fisiopatologia del metabolismo del ferro e implicazioni ... · fisiopatologia del metabolismo del...
TRANSCRIPT
DG - 1PBM Ovest Milanese 16 Febbraio 2018
Fisiopatologia del metabolismo del ferro e implicazioni terapeutiche
Domenico GirelliDipartimento di Medicina, Università di Verona
Centro di Riferimento per i Disordini del Metabolismo del FerroEuroBloodNet (European Reference Network for Rare Hematological Diseases)

anemianeuromuscolar impairment
iron overloadtoxic organ damage
low excess
Iron: essential but potentially dangerous
easily exchange electronsFe3+ ↔ Fe2+
useful redox properties
key-component of enzymes crucial for O2 transport and
energy production (Hb, cytochromes…)
free radicals generation (Fe2++ H202 → Fe3+ + OH- + OH•)
strict regulation of body iron content needed
DG - 2PBM Ovest Milanese 16 Febbraio 2018
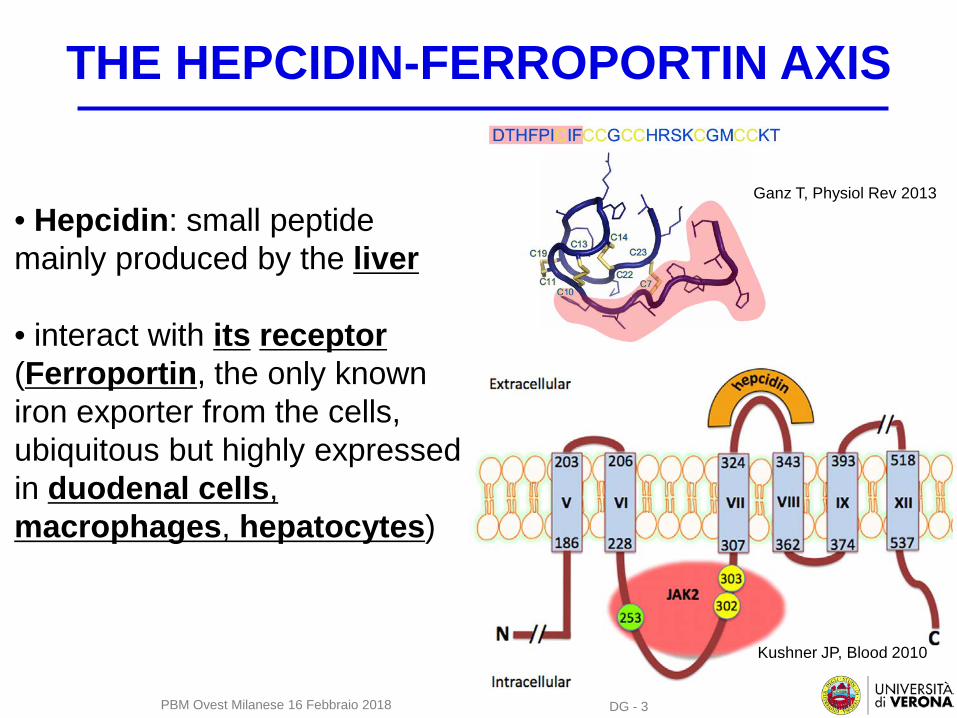
THE HEPCIDIN-FERROPORTIN AXIS
Ganz T, Physiol Rev 2013
• Hepcidin: small peptide mainly produced by the liver
• interact with its receptor(Ferroportin, the only known iron exporter from the cells, ubiquitous but highly expressed in duodenal cells, macrophages, hepatocytes)
Kushner JP, Blood 2010
DG - 3PBM Ovest Milanese 16 Febbraio 2018
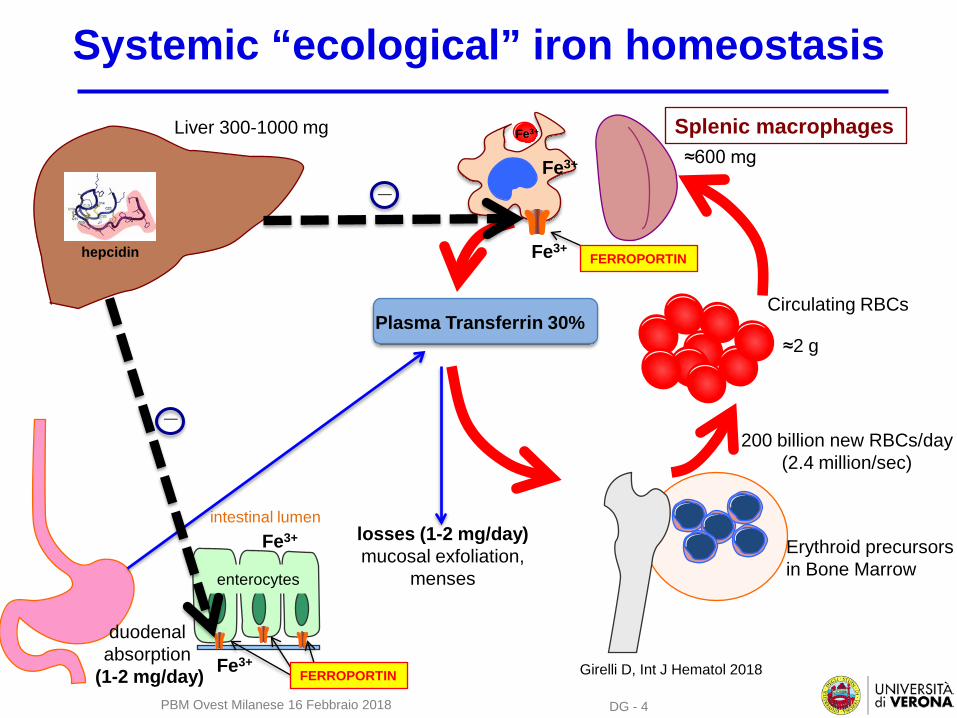
Systemic “ecological” iron homeostasis
≈2 g
≈600 mg
Erythroid precursors in Bone Marrow
Fe3+
Fe3+
Fe3+
FERROPORTIN
Splenic macrophages
Circulating RBCsPlasma Transferrin 30%
losses (1-2 mg/day)mucosal exfoliation,
menses
duodenal absorption
(1-2 mg/day)
enterocytes
intestinal lumenFe3+
Fe3+FERROPORTIN Girelli D, Int J Hematol 2018
Liver 300-1000 mg
hepcidin
_
_
200 billion new RBCs/day (2.4 million/sec)
DG - 4PBM Ovest Milanese 16 Febbraio 2018
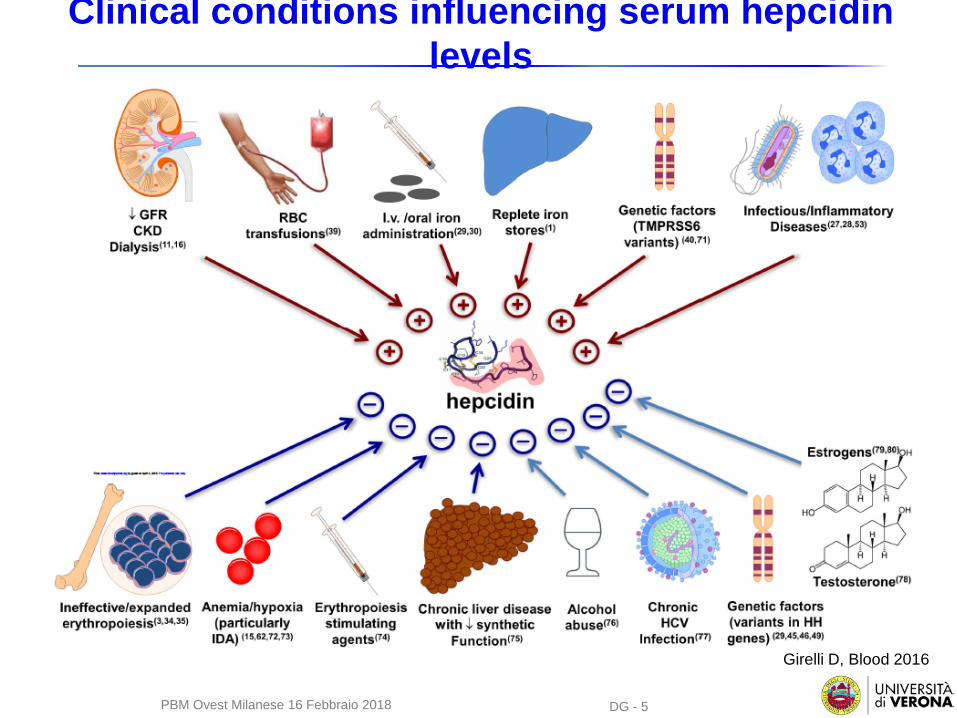
Clinical conditions influencing serum hepcidin levels
Girelli D, Blood 2016
DG - 5PBM Ovest Milanese 16 Febbraio 2018
DG - 6
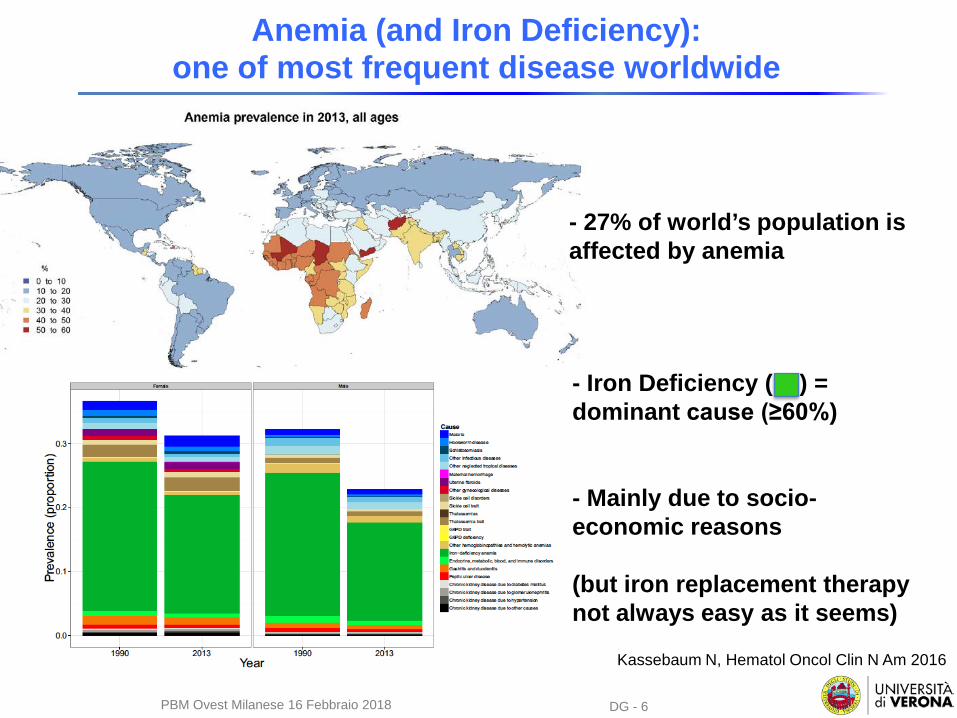
Anemia (and Iron Deficiency): one of most frequent disease worldwide
DG - 6
Kassebaum N, Hematol Oncol Clin N Am 2016
- 27% of world’s population is affected by anemia
- Iron Deficiency ( ) = dominant cause (≥60%)
- Mainly due to socio-economic reasons
(but iron replacement therapy not always easy as it seems)
PBM Ovest Milanese 16 Febbraio 2018
DG - 7
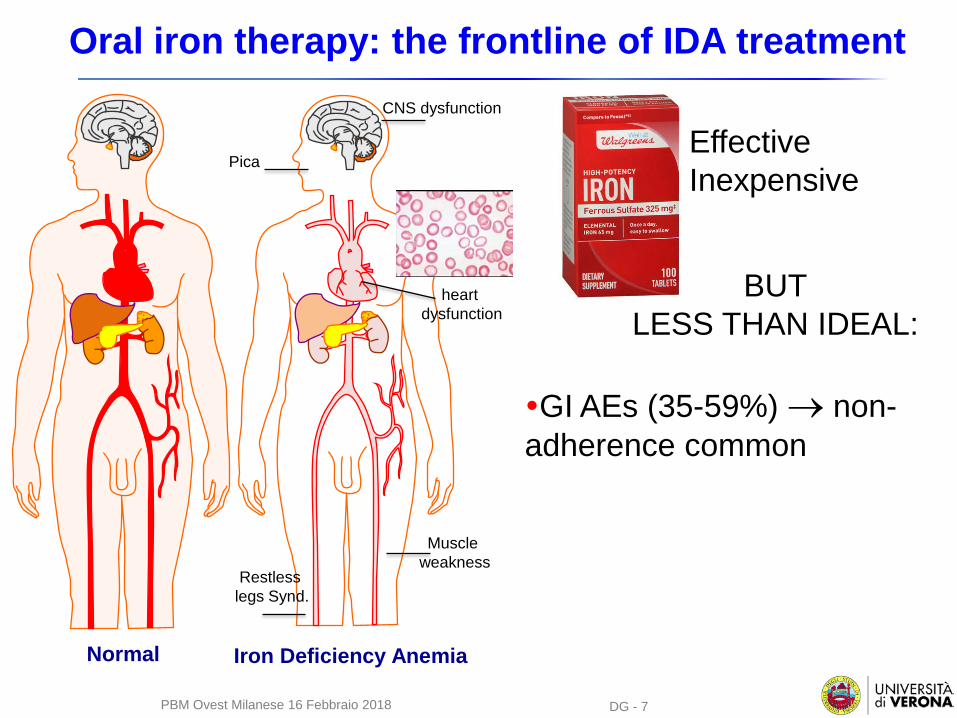
Oral iron therapy: the frontline of IDA treatmentCNS dysfunction
heart dysfunction
Muscle weakness
Restless legs Synd.
Pica
Normal Iron Deficiency Anemia
Effective Inexpensive
GI AEs (35-59%) → non-adherence common
BUTLESS THAN IDEAL:
PBM Ovest Milanese 16 Febbraio 2018
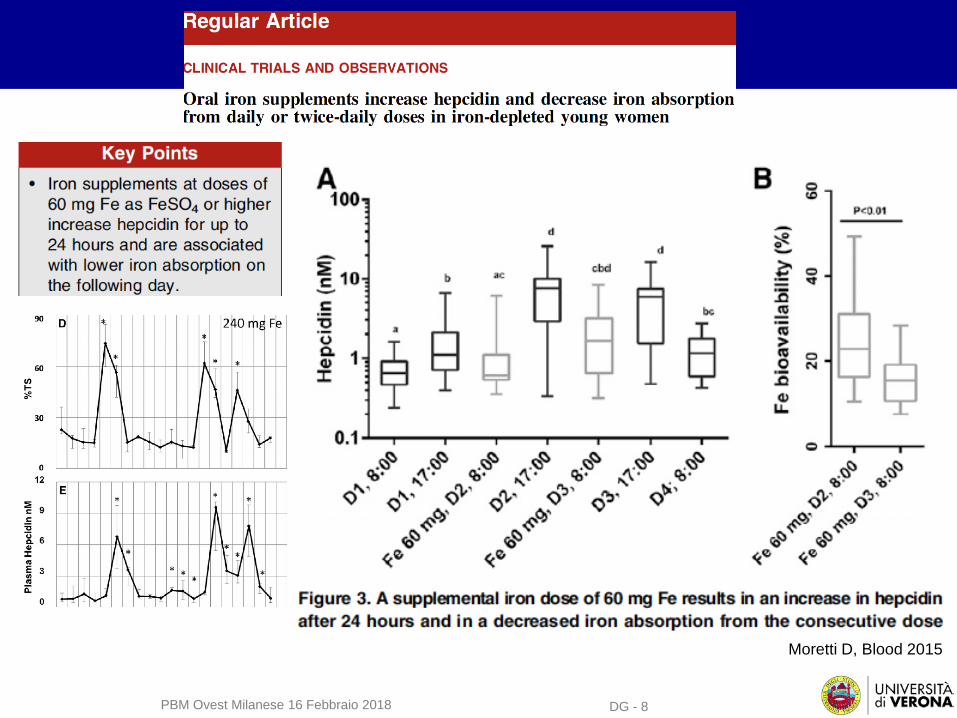
Moretti D, Blood 2015
DG - 8PBM Ovest Milanese 16 Febbraio 2018
DG - 9
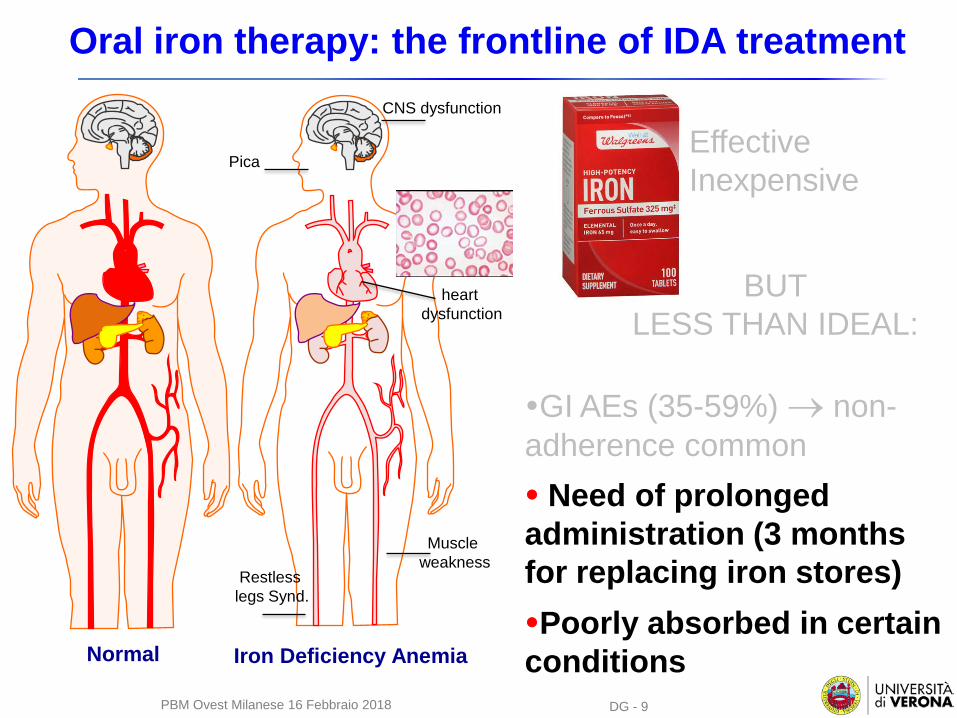
Oral iron therapy: the frontline of IDA treatmentCNS dysfunction
heart dysfunction
Muscle weakness
Restless legs Synd.
Pica
Normal Iron Deficiency Anemia
Effective Inexpensive
GI AEs (35-59%) → non-adherence common
BUTLESS THAN IDEAL:
Need of prolonged administration (3 months for replacing iron stores)Poorly absorbed in certain conditions
PBM Ovest Milanese 16 Febbraio 2018
DG - 10
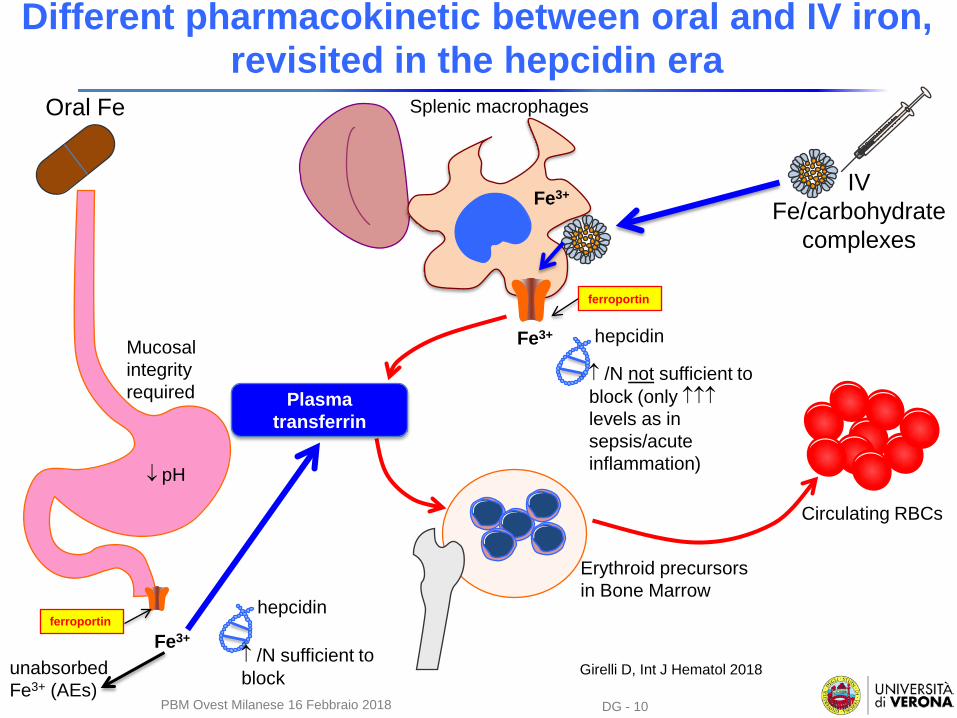
Different pharmacokinetic between oral and IV iron, revisited in the hepcidin era
Erythroid precursors in Bone Marrow
Fe3+
Fe3+
ferroportin
Splenic macrophages
Circulating RBCs
Plasma transferrin
Oral Fe
IVFe/carbohydrate
complexes
Mucosal integrityrequired
↓ pH
ferroportin
Fe3+
unabsorbed Fe3+ (AEs)
↑ /N sufficient to block
hepcidin
hepcidin
↑ /N not sufficient to block (only ↑↑↑levels as in sepsis/acute inflammation)
Girelli D, Int J Hematol 2018
PBM Ovest Milanese 16 Febbraio 2018
DG - 11
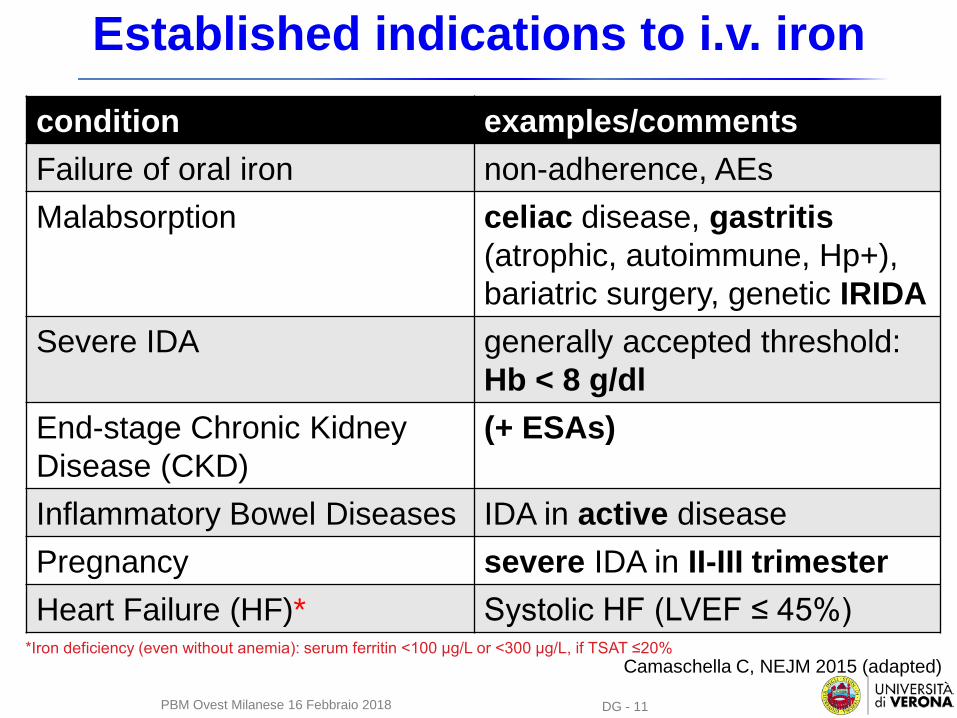
Established indications to i.v. ironcondition examples/commentsFailure of oral iron non-adherence, AEs Malabsorption celiac disease, gastritis
(atrophic, autoimmune, Hp+), bariatric surgery, genetic IRIDA
Severe IDA generally accepted threshold: Hb < 8 g/dl
End-stage Chronic Kidney Disease (CKD)
(+ ESAs)
Inflammatory Bowel Diseases IDA in active diseasePregnancy severe IDA in II-III trimester Heart Failure (HF)* Systolic HF (LVEF ≤ 45%)
*Iron deficiency (even without anemia): serum ferritin <100 µg/L or <300 µg/L, if TSAT ≤20%Camaschella C, NEJM 2015 (adapted)
PBM Ovest Milanese 16 Febbraio 2018
DG - 12
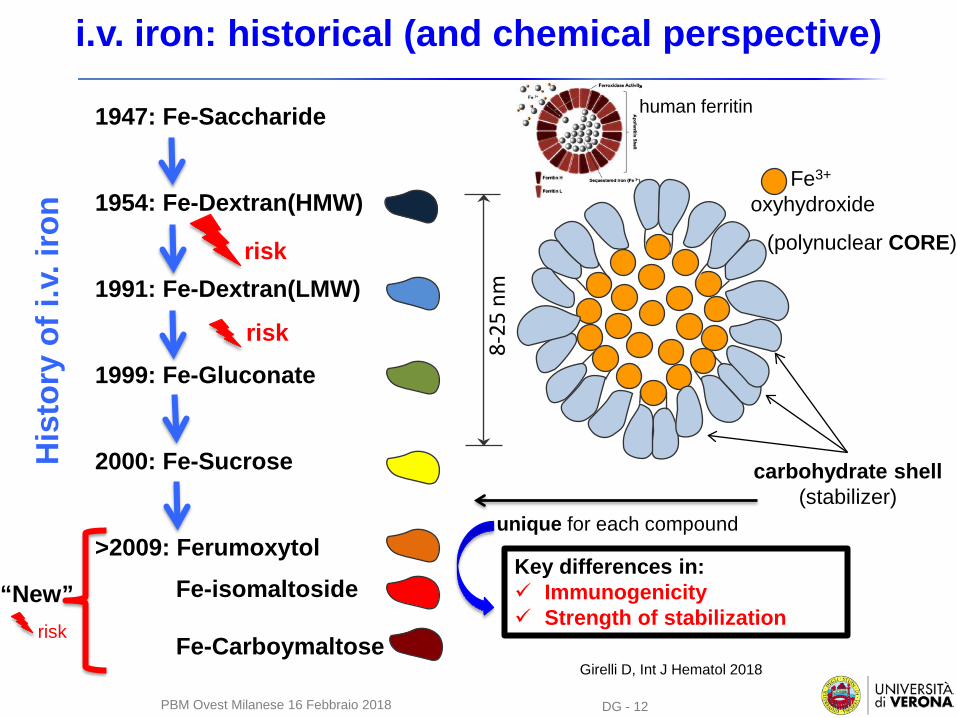
i.v. iron: historical (and chemical perspective)
human ferritin1947: Fe-Saccharide
1954: Fe-Dextran(HMW)
1991: Fe-Dextran(LMW)
1999: Fe-Gluconate
2000: Fe-Sucrose
>2009: FerumoxytolFe-isomaltoside
Fe-Carboymaltose
“New”
8-25
nm
Fe3+
oxyhydroxide
(polynuclear CORE)
carbohydrate shell(stabilizer)
unique for each compound
Key differences in: Immunogenicity Strength of stabilization
His
tory
of i
.v. i
ron
risk
risk
risk
Girelli D, Int J Hematol 2018
PBM Ovest Milanese 16 Febbraio 2018
DG - 13
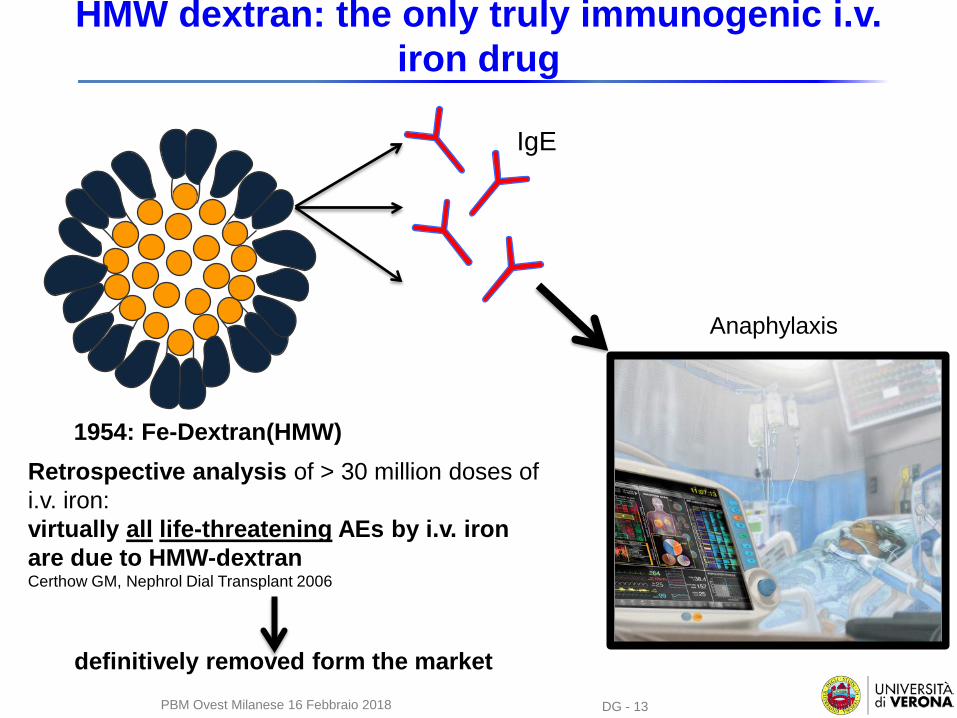
HMW dextran: the only truly immunogenic i.v. iron drug
1954: Fe-Dextran(HMW)
IgE
Anaphylaxis
Retrospective analysis of > 30 million doses of i.v. iron: virtually all life-threatening AEs by i.v. iron are due to HMW-dextranCerthow GM, Nephrol Dial Transplant 2006
definitively removed form the marketPBM Ovest Milanese 16 Febbraio 2018
DG - 14
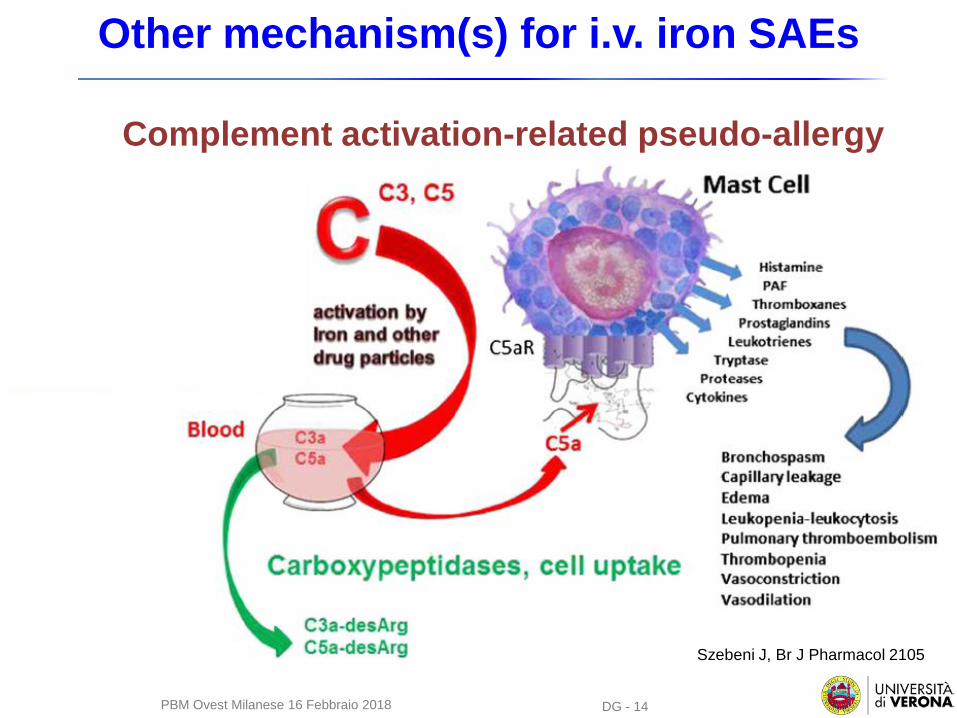
Other mechanism(s) for i.v. iron SAEs
Szebeni J, Br J Pharmacol 2105
Complement activation-related pseudo-allergy
PBM Ovest Milanese 16 Febbraio 2018
DG - 15
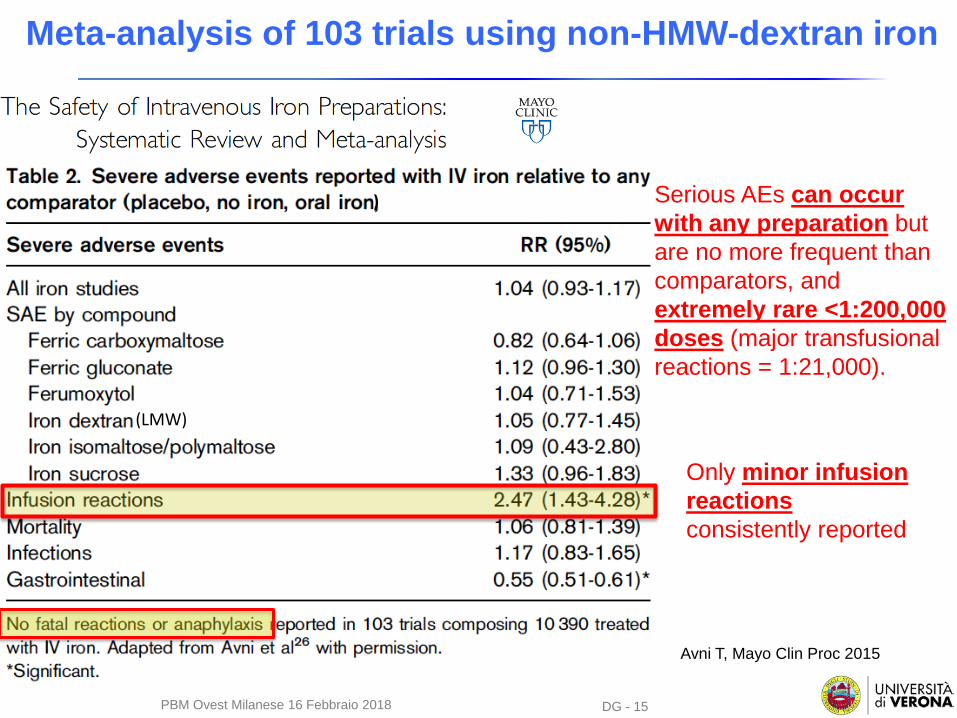
Meta-analysis of 103 trials using non-HMW-dextran iron
Serious AEs can occur with any preparation but are no more frequent than comparators, and extremely rare <1:200,000 doses (major transfusional reactions = 1:21,000).
Avni T, Mayo Clin Proc 2015
(LMW)
)
Only minor infusion reactions consistently reported
PBM Ovest Milanese 16 Febbraio 2018
DG - 16
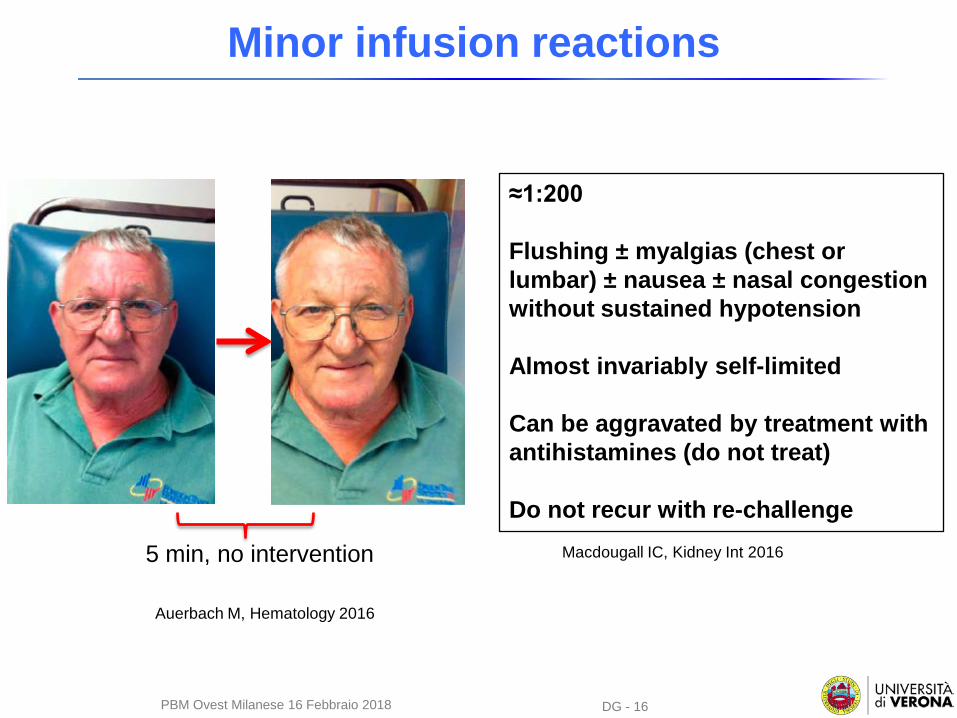
Minor infusion reactions
≈1:200
Flushing ± myalgias (chest or lumbar) ± nausea ± nasal congestion without sustained hypotension
Almost invariably self-limited
Can be aggravated by treatment with antihistamines (do not treat)
Do not recur with re-challenge
Auerbach M, Hematology 2016
5 min, no intervention Macdougall IC, Kidney Int 2016
PBM Ovest Milanese 16 Febbraio 2018
DG - 17
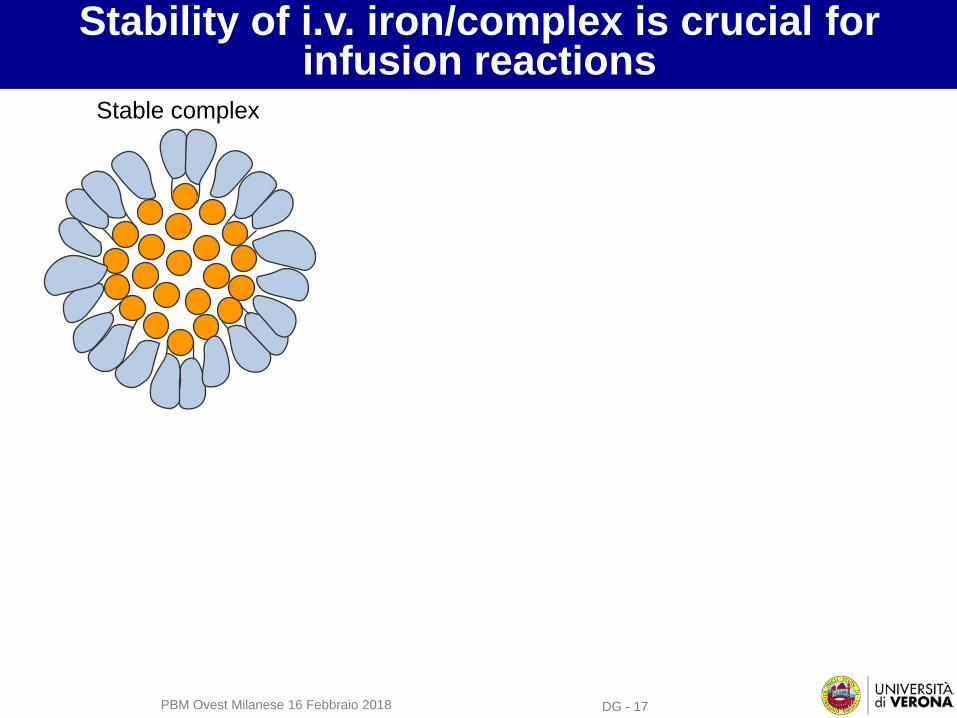
Stability of i.v. iron/complex is crucial for infusion reactions
Stable complex
PBM Ovest Milanese 16 Febbraio 2018
DG - 18
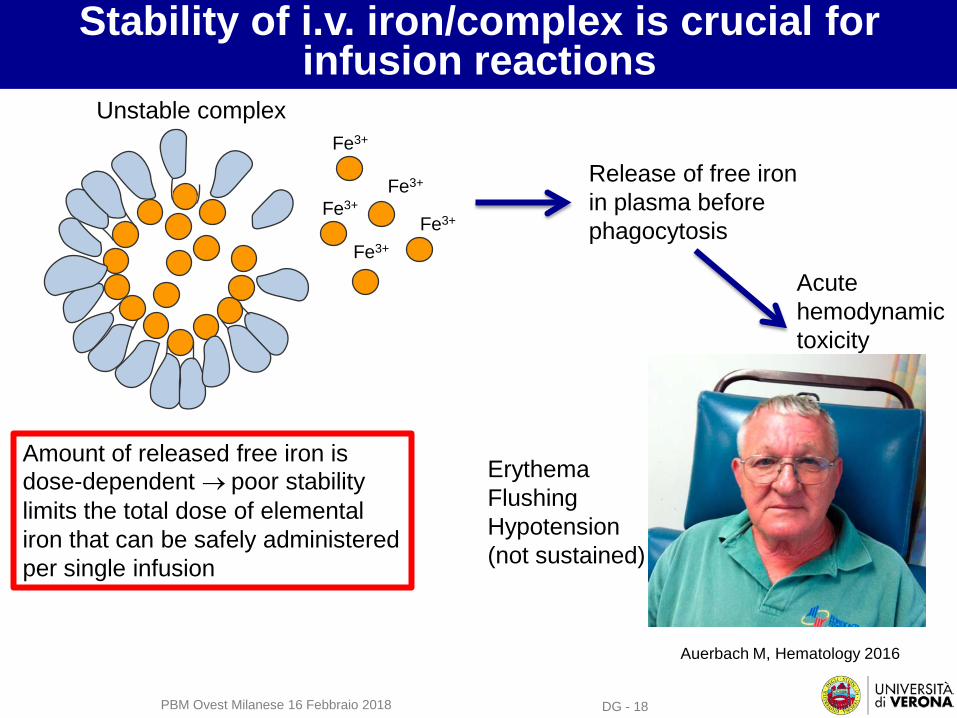
Stability of i.v. iron/complex is crucial for infusion reactions
Fe3+
Fe3+
Fe3+
Fe3+
Fe3+
Unstable complex
Release of free iron in plasma before phagocytosis
Acute hemodynamic toxicity
Auerbach M, Hematology 2016
ErythemaFlushingHypotension(not sustained)
Amount of released free iron is dose-dependent → poor stability limits the total dose of elemental iron that can be safely administered per single infusion
PBM Ovest Milanese 16 Febbraio 2018
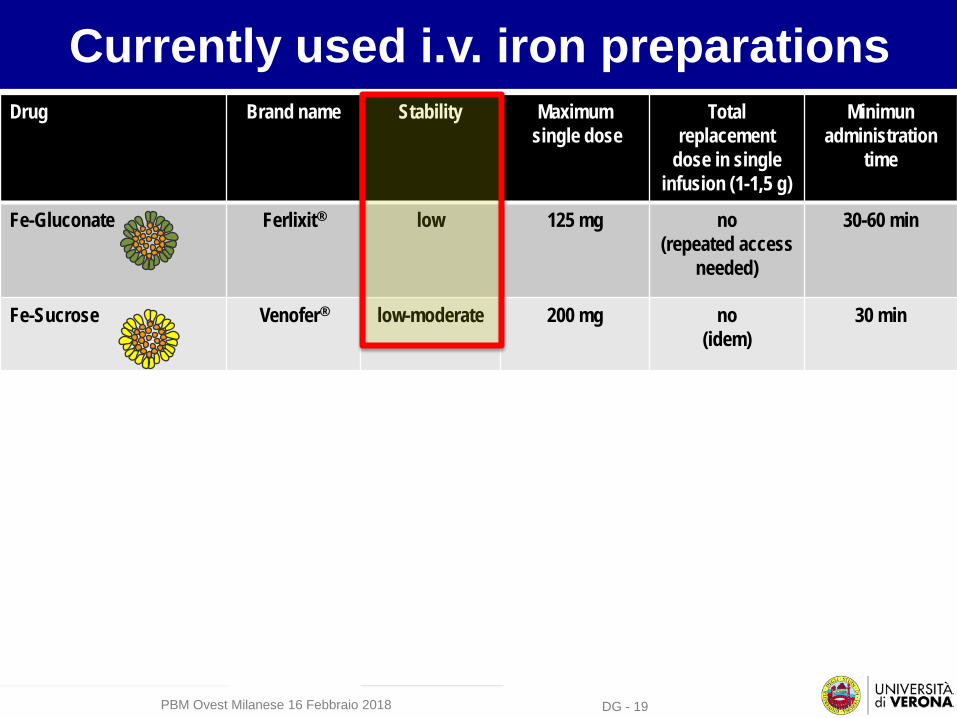
Currently used i.v. iron preparationsDrug Brand name Stability Maximum
single doseTotal
replacement dose in single
infusion (1-1,5 g)
Minimunadministration
time
Fe-Gluconate Ferlixit® low 125 mg no(repeated access
needed)
30-60 min
Fe-Sucrose Venofer® low-moderate 200 mg no(idem)
30 min
Fe-Carboxymaltose Ferinject® high 1000 mg yes 15 min
Fe-isomaltoside Monofer® high 20 mg Fe/Kg yes 15 min
Ferumoxytol Feraheme® high 510 mg yes/no 15 min
“Third generation”
DG - 19PBM Ovest Milanese 16 Febbraio 2018
DG - 20
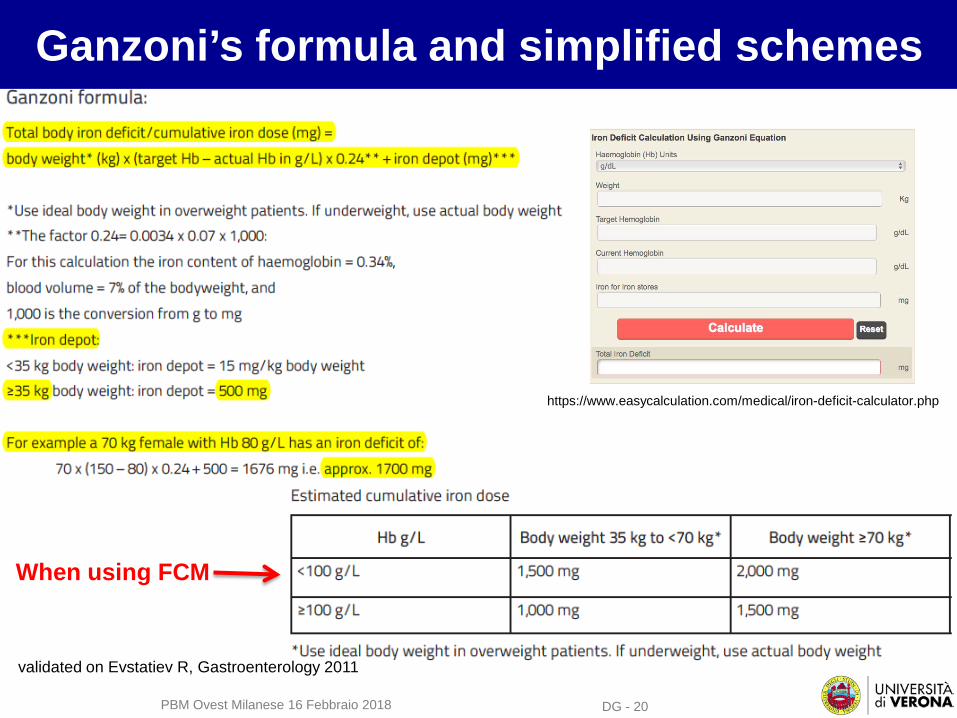
Ganzoni’s formula and simplified schemes
https://www.easycalculation.com/medical/iron-deficit-calculator.php
When using FCM
validated on Evstatiev R, Gastroenterology 2011
PBM Ovest Milanese 16 Febbraio 2018
DG - 21
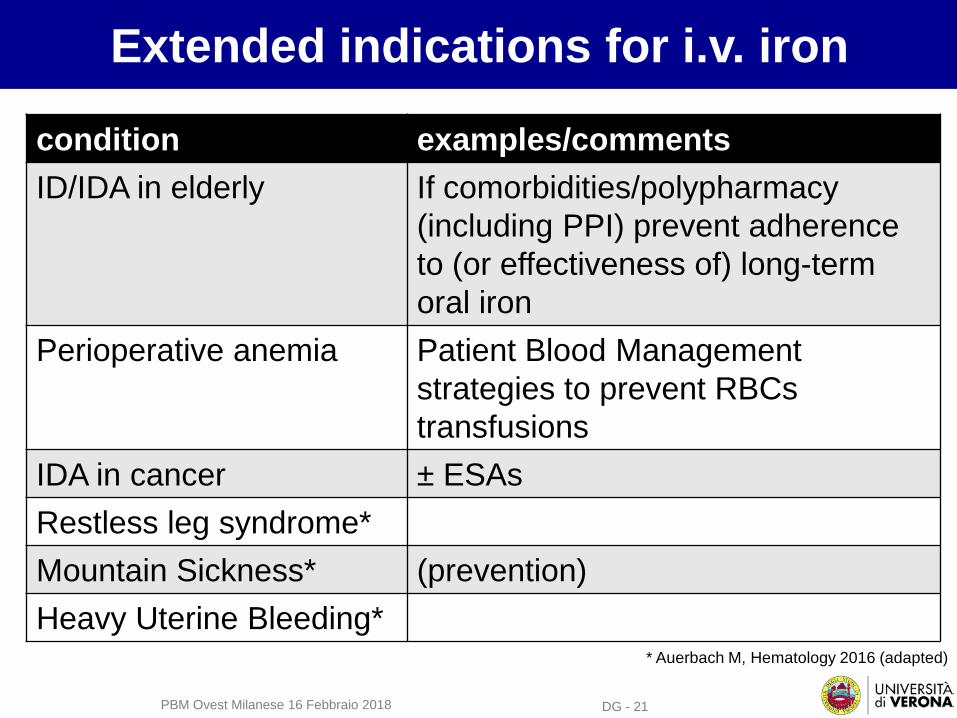
Extended indications for i.v. iron
condition examples/commentsID/IDA in elderly If comorbidities/polypharmacy
(including PPI) prevent adherence to (or effectiveness of) long-term oral iron
Perioperative anemia Patient Blood Management strategies to prevent RBCs transfusions
IDA in cancer ± ESAs Restless leg syndrome*Mountain Sickness* (prevention)Heavy Uterine Bleeding*
* Auerbach M, Hematology 2016 (adapted)
PBM Ovest Milanese 16 Febbraio 2018
DG - 22
Take-home messages
New (“third generation”) i.v. iron drugs are characterized by higher stability of the carbohydrate shell and by improved safety profiles
They allow easy and convenient schedules, with complete replacement of iron in 1 or 2 administrations.
This drives a paradigm shift in the treatment of one of the most common disease worldwide, with extending indications (to be confirmed).
PBM Ovest Milanese 16 Febbraio 2018

The Verona Interdisciplinary Group on Iron Disorders
Participants Units1. Internal Medicine2. Clinical Chemistry & Molecular Biology3. Blood Bank / Transfusional Service4. Radiology5. Pathology6. Gastroenterology
http://www.gimferverona.org
Fabiana Busti, Paola Capelli, Annalisa Castagna, Michela Corbella, Massimo Delledonne, Giorgio Gandini, Alejandro Giorgetti, Giacomo Marchi, Oliviero Olivieri, Roberto Pozzi-Mucelli, Monica Rizzi, Alice Vianello, Luciano Xumerle.
DG - 23PBM Ovest Milanese 16 Febbraio 2018