tmo em crianças avanços no transplante da leucemia ...sbtmo.org.br/userfiles/fck/file/aulas_i...
TRANSCRIPT

TMO em Crianças
Avanços no Transplante da Leucemia Linfóide Aguda
Maria Lucia M. Lee

Biology and clinical application of CAR T cells for B cellmalignancies
Int J Hematol (2016) 104:6–17
SNC
Citocinas

ÍNDICES DE REMISSÃO: 95 – 98% SLE : 76 – 87 % SG : 85 - 90%
Cenário Atual da LLA Pediátrica
JCO 2015

Masculino, 4 anos Masc, 6a5m
• LI : 7500/mm3
• SNC 1
• IF: LLA comum
• Cariótipo: 46 , XY
• BM : bcr-abl p 190 : neg
ETV6 – RUN X1 : neg
Protocolo IC BFM 2002 - RI
D8: < 1000 bl/mm3
D15 : MO – M1
D 33 : MO – M1
Recidiva Mo Isolada: 7 meses pós FT
6 irmãos não compatíveis
• LI: 3400/mm3
• SNC 1
• IF: LLA pré B
• Cariótipo e BM: não avaliáveis
• Protocolo IC BFM 2002 – RS
• D8 : > 1000bl/mm3- AR
• D15 : M0 M3
• D33: MO 27% blastos – TMO?
• D64: MO M1
• CONDUTA: TMO NA? Filho único

Quando Indicar TMO ?
“HSCT should therefore be considered for patients in whom this procedure is likely to result in superior long term disease free survival (DFS) when compared with
other therapeutic modalities"Principles and Practice
of Pediatric Oncology, 6th edition

TMO em LLA Pediátrica
PRIMEIRA REMISSÃO
• Falha Indutória
• Lactentes
• Ph+
• Hipodiploides
• ETP
• DRM Positiva final indução
RECAÍDAS
• Muito Precoces
• Precoces
• Tardias ?
• Mo isoladas
• Mo combinadas
• Extramedulares ?
• LLA – T extramedularisolada?

FALHA INDUTORIA GRUPO ALTÍSSIMO RISCO
98%
2%
95 %
< 5%
1a Remissão: de quem estamos falando?

INDICAÇÕES EM PRIMEIRA REMISSÃO
INDICAÇÃO
Particularidades da doença
Particularidades
do
paciente
Modalidade do TMO
Particularidadesda avaliação da
resposta
• 3a,masc, LI: 3400/mm3
• SNC 1
• IF: LLA pré B
• Cariótipo e BM: não avaliáveis
• Protocolo IC BFM 2002 – RS
• D8 : > 1000bl/mm3- AR
• D15 : M0 M3
• D33: MO 27% blastos – TMO?
• D64: MO M1
• CONDUTA: TMO NA? Filho único

1a Remissão: de quem estamos falando?
95%
5%
SUBGRUPO PACIENTES
ALTÍSSIMO RISCO

De quem estamos falando?
Carrol WL, 2005

Blood. 2007;109:926-935
Risk- and response-based classification of childhood B-precursor acute lymphoblastic leukemia: a combined analysis of prognostic markers from the
Pediatric Oncology Group (POG) and Children’s Cancer Group (CCG)Kirk R. Schultz, D. Jeanette Pullen, Harland N. Sather et al
Falha IndutóriaHipodiploidia < 44 crPh+/bcr-abl
Near-haploid and low-hypodiploid acute lymphoblastic leukemia:two distinct subtypes with consistently poor prognosis
• Cariótipo < 40 cromossomos, distribuição bimodal
• Near haploide : 24 – 30 cr ( media 5a)
• Low hipodiploide : 31 – 39 cr ( em crianças necessita de investigação mut p 53 familiar)( media 11, 5 a)
• Alterações nas vias RAS, TK, RB1, IKZF3, IKZF2
• “It is not clear whether hematopoietic stem cell transplantation in CR1 is beneficial in near-haploid and low hypodiploid ALL."
Blood. 2017;129(4)

Transplant Outcomes for Children with Hypodiploid AcuteLymphoblastic Leukemia
Biol Blood Marrow Transplant. 2015 ; 21(7)

Outcome of children with hypodiploid ALL treated with risk-directed therapy based on MRD levels
Blood 2015;126
Estudos Total 15 e Total 16 : 2,2% Hipodiploide
20 pacientes : Todos alcançaram RCCDRM NEG no D29 : 14/20,13 QT INTENSIVA : SLE 85%1 – TMO alo : óbito por toxic
> 0,01% : 6/20 pts ( 1com DRM > 1%)

Coustan-Smith et al, Lancet Oncol 2009
Early T-cell precursor leukaemia: a subtype of very high-riskacute lymphoblastic leukaemia ( 11 -12% população pediátrica)
SG SLE Falha ind ou rec
SJRH
AEIOP

Outcome for children and young people with Early T-cell precursor acute lymphoblastic leukaemia treated on a
contemporary protocol, UKALL 2003
British Journal of Haematology 2014; 166
35 pts = 16% grupo T

Outcome for children and young people with Early T-cell precursor acute lymphoblastic leukaemia treated on a
contemporary protocol, UKALL 2003
British Journal of Haematology 2014; 166

De quem estamos falando ?
98%
2%
Falha Indutória

Outcomes after Induction Failure in Childhood Acute Lymphoblastic Leukemia
Martin Schrappe, M.D., Stephen P. Hunger, M.D., Ching-Hon Pui, M.D.,et al.
N Engl J Med 2012;366
14 cooperative study groups between 1985 and 2000
44.017 pts – 1041 ( 2,4%)
"Pediatric ALL with induction failure is highly heterogeneous."

Outcomes after Induction Failure in Childhood Acute Lymphoblastic Leukemia
N Engl J Med 2012;366
624 pts

Outcomes after Induction Failure in Childhood Acute Lymphoblastic Leukemia
Pacientes LLA pB sem rg MLL < 6 anos
N Engl J Med 2012;366
" our analysis showed no benefit of allogeneic transplantation in patients younger than 6 years of age who had precursor B-cell ALL and induction failure and no high-risk cytogenetic features ."

Outcomes after Induction Failure in Childhood Acute Lymphoblastic Leukemia
Pacientes LLA pB sem rg MLL > 6 anos
N Engl J Med 2012;366

Outcomes after Induction Failure in Childhood Acute Lymphoblastic Leukemia
Pacientes com LLA T
N Engl J Med 2012;366

Doença Residual Miníma é o mais importantedeterminante prognóstico?
Coustan-Smith. Blood 96 (8): 2691-6, 2000
Estudos Total XIIIA e XIII St. Jude:Impacto da DRM no final indução

Doença Residual Miníma é o mais importante determinante prognóstico?
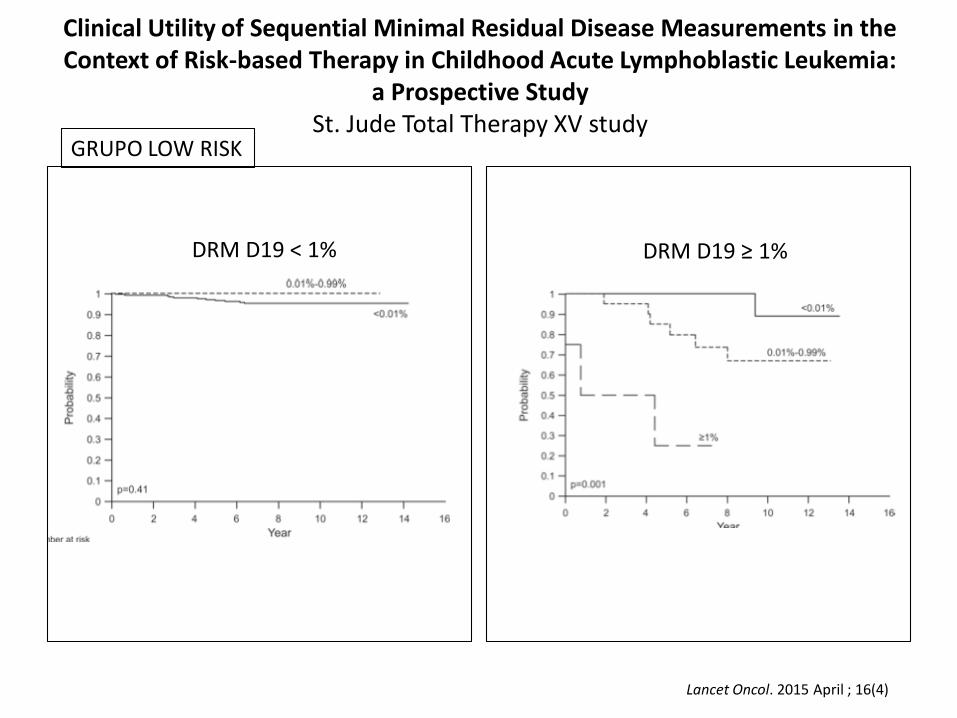
Clinical Utility of Sequential Minimal Residual Disease Measurements in the Context of Risk-based Therapy in Childhood Acute Lymphoblastic Leukemia:
a Prospective Study St. Jude Total Therapy XV study
GRUPO LOW RISK
DRM D19 < 1% DRM D19 ≥ 1%
Lancet Oncol. 2015 April ; 16(4)

Molecular response to treatment redefines all prognostic factors in childrenand adolescents with B-cell precursor acute lymphoblastic leukemia:
results in 3184 patients of the AIEOP-BFM ALL 2000 study
TP1 <10-4
>10-3 (TP2)
TP1 >10-4 MAS TP2 <10-3
MRD Estratificação Risco • SR = MRD NEG no D33 e 78
( 42%)• RI= >10-4(TP1) <10-3 (TP2) (51,7% )• HR = MRD > 10-³ no D78
( 6%)
SLE
Conter et al. Blood 15(16), 2010
Inc
acu
mre
cid
iva

Late MRD response determines relapse risk overall and in subsets of childhood T-cell ALL: results of the AIEOP-BFM-ALL 2000 study
Blood. 2011
MRD < 10-4 em TP1 e TP2
MRD > 10-3 em TP2
MRD + em TP1 ou TP2 MASTP2 < 10-3
DRM em TP2 x Recidiva

ESTUDOS NOPHO ALL-92 and ALL-2000
Leukemia (2010) 24, 345–35

Childhood high-risk acute lymphoblastic leukemia in first remission: results after chemotherapy or transplant from the
AIEOP ALL 2000 study Estimates of EFS in 312 children with HR- ALL by HR criteria
(hierarchical order).
BLOOD. 2014 ; 123 ( 10 )Critérios Grupo Alto Risco: DRM ≥ 10 -3 no D78 ( HR MRD), D33 falha indutória, t( 4;11), PRP

Grupo 3 : DRM TP2 ≥ 10 -2, FI D33, t (4;11) e PRP
SG QUIMIO: 54,7% TMO 1 RC : 50,5% SLD QUIMIO: 54,7% TMO 1 RC : 50,5%
Childhood high-risk acute lymphoblastic leukemia in first remission: results after chemotherapy or transplant from the
AIEOP ALL 2000 study
BLOOD. 2014 ; 123 ( 10 )
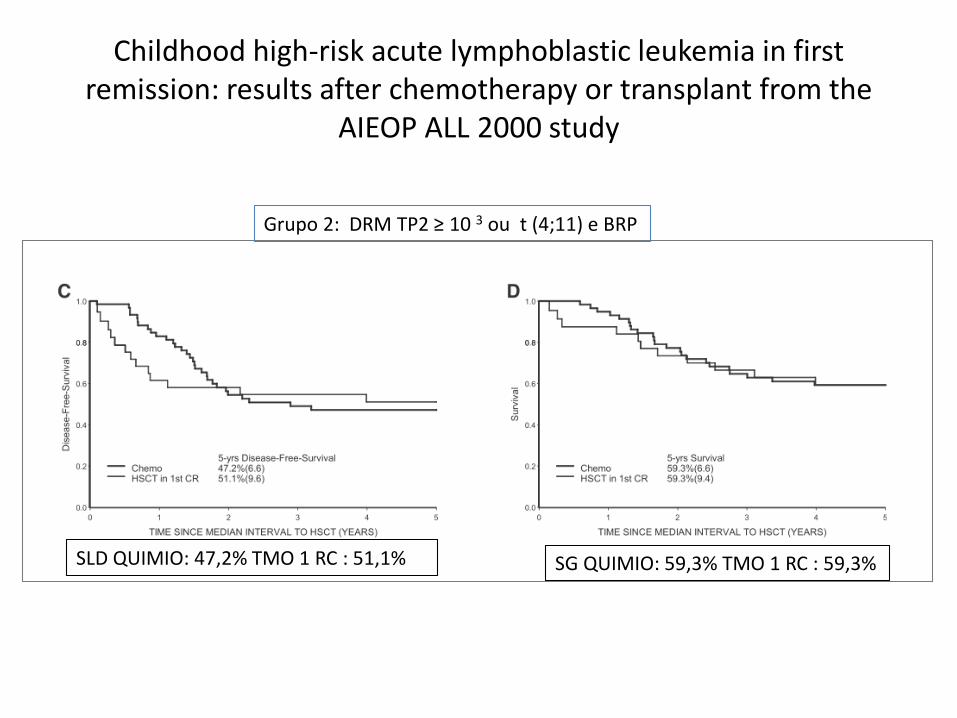
Grupo 2: DRM TP2 ≥ 10 3 ou t (4;11) e BRP
Childhood high-risk acute lymphoblastic leukemia in first remission: results after chemotherapy or transplant from the
AIEOP ALL 2000 study
SLD QUIMIO: 47,2% TMO 1 RC : 51,1% SG QUIMIO: 59,3% TMO 1 RC : 59,3%

TMO nas Recidivas
• 15 - 20% ainda recidivam
• 9 casos/milhão/ano
• Considerada ainda a principal causa de morte
associada ao cancer infantil
• Número significativo ocorre em pacientes que
não são caracterizados inicialmente com
aspectos desfavoráveis.

Recidivas : o que considerar?
• Muito Precoces
• Precoces
• Tardias ?
• Mo isoladas
• Mo combinadas
• Extramedulares ?
• LLA – T extramedular isolada?

Fatores Prognósticos na Recidiva
TEMPO DA 1ª RCC
FENÓTIPO
BLASTO
SÍTIO DA RECAIDA

Estudo RECAÍDA 15 St JUDE

Factors Influencing Survival After Relapse From Acute
Lymphoblastic Leukemia: A Children's Oncology Group Study
RECAIDA ISOLADA MO x TEMPO
Leukemia 2008;14:2142-50
> 36 mSobrevida : 43%
Sobrevida : 18,4 %
< 18 mSobrevida : 11,5 %

Factors Influencing Survival After Relapse From Acute
Lymphoblastic Leukemia: A Children's Oncology Group Study
RECAIDA MO COMBINADA x TEMPO
> 36 mo
Sobrevida :
60,3%
< 18 mo
Sobrevida: 11,6%
Leukemia 2008;14:2142-50
Sobrevida:
39,8%

Factors Influencing Survival After Relapse From Acute
Lymphoblastic Leukemia: A Children's Oncology Group Study
RECAIDA ISOLADA SNC x TEMPO
>36 moSobrevida: 78,2%
< 18 moSobrevida: 43,5%
Leukemia 2008;14:2142-50
Sobrevida: 68%

Pathways Through Relapses and Deaths of Children With Acute Lymphoblastic Leukemia: Role of Allogeneic Stem Cell Transplantation in
Nordic Data Pathways Through Relapses and Deaths of Children With Acute Lymphoblastic Leukemia: Role of Allogeneic Stem- Cell Transplantation in
Nordic Data
J Clin Oncol 2006 ; 24
SLE x Tempo /Sítio recaída

Pathways Through Relapses and Deaths of Children With Acute Lymphoblastic Leukemia: Role of Allogeneic Stem Cell Transplantation
in Nordic Data Pathways Through Relapses and Deaths of Children With Acute Lymphoblastic Leukemia: Role of Allogeneic Stem- Cell Transplantation
in Nordic Data
J Clin Oncol 2006 ; 24
SLE x Risco Inicial

Outcome After Relapse Among Children With Standard-Risk Acute Lymphoblastic Leukemia: Children’s Oncology
Group Study CCG-1952
J Clin Oncol 2007;25:5800-5807
Recaida Medular Isolada

Transplant Outcomes for Children with T-Cell Acute Lymphoblastic Leukemia in Second Remission: A Report of the CIBMTR
Biol Blood Marrow Transplant. 2015 December ; 21(12):
Rec Extra Mo 15% x 45% Rec Mo SLD Extra Mo 56 % x 35 % Rec Mo
Numero de Pacientes: 229Número de Centros: 99Idade: mediana 10 a ( 2 – 18)

Results of Trial ALL-REZ BFM 90
A: Rec MO Precoce ( isolada/comb.)
B:Rec. MO Tardia
C:Rec. Extra Mo Isolada
PPG: Rec MO muito precoce ou T .
Muito Precoce: Dentro de 18 meses após Dx
Precoce: Após 18 meses do Dx e menos 6 meses após término Tto.
Tardia: Após 6 meses término Tto.
J Clin Oncol 2010 28:2339-2347.

Excellent prognosis of late relapses of ETV6/RUNX1-positive
childhood acute lymphoblastic leukemia: lessons from the
FRALLE 93 Protocol
43/713 ETV6/RUNX1 –
recidivaram ( 19,4%)
Haematologica 2012
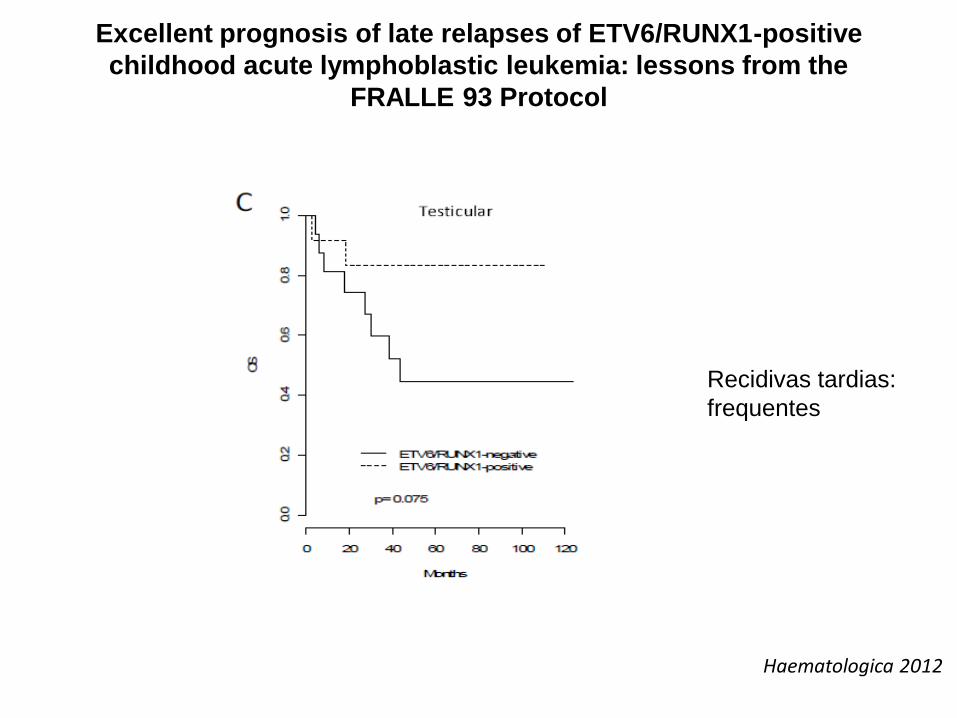
Excellent prognosis of late relapses of ETV6/RUNX1-positive
childhood acute lymphoblastic leukemia: lessons from the
FRALLE 93 Protocol
Recidivas tardias:
frequentes
Haematologica 2012

Prognostic Value of Minimal Residual Disease Quantification Before Allogeneic Stem-Cell Transplantation in Relapsed Childhood Acute
Lymphoblastic Leukemia: The ALL-REZ BFM Study Group
Clin Oncol 2008 ; 27:377-384
Pacientes em Primeira ou Segunda Recidiva

Prognostic Value of Minimal Residual Disease Quantification Before Allogeneic Stem-Cell Transplantation in Relapsed Childhood Acute
Lymphoblastic Leukemia: The ALL-REZ BFM Study Group
• Nas Recidivas Risco Intermediário: Recidivas Mo de pB combinadas precoces ou > 6 m FT; • Mo tardia de pB• Extra Mo isoladas muito precoces ( pB ou T)

Prognostic Value of Minimal Residual Disease Quantification Before Allogeneic Stem-Cell Transplantation in Relapsed Childhood Acute
Lymphoblastic Leukemia: The ALL-REZ BFM Study Group
Clin Oncol 2008 ; 27:377-384
Grupo Alto risco/ 3 RCC

Use of Allogeneic Hematopoietic Stem-Cell Transplantation Based on Minimal Residual Disease Response Improves Outcomes for Children With Relapsed
Acute Lymphoblastic Leukemia in the Intermediate-Risk Group
Clin Oncol 2013; 31
DRM < 10 -3
DRM > 10-3

Outcome of pediatric acute lymphoblastic leukemia with very laterelapse: a retrospective analysis by the Tokyo Children’s Cancer
Study Group (TCCSG)
Int J Hematol (2015) 101:52–57

Outcome of pediatric acute lymphoblastic leukemia with very laterelapse: a retrospective analysis by the Tokyo Children’s Cancer
Study Group (TCCSG)
“our results demonstrated that the risk ofsecond relapse in very late relapsed ALL was lower than that of late relapsed ALL, and suggested that these patients should be treated without allogeneic HSCT even when first relapse occurs in the bone marrow."
Int J Hematol (2015) 101:52–57

Phase I/Phase II Study of Blinatumomab in Pediatric Patients With Relapsed/Refractory Acute Lymphoblastic Leukemia
J Clin Oncol 2016; 34
Dose I ciclo : 5/15 μ/m2 ( 70 pts)Idade: mediana 8a ( <1 – 17)

RCC após 2 ciclos: 39% pts
Phase I/Phase II Study of Blinatumomab in Pediatric Patients With Relapsed/Refractory Acute Lymphoblastic Leukemia
J Clin Oncol 2016; 34

CASO 1
• LI: 3400/mm3, 4 anos
• SNC 1
• IF: LLA pré B
• Cariótipo e BM: não avaliáveis
• Protocolo BFM IC 2002 – RS
• D8 : > 1000bl/mm3- AR
• D15 : M0 M3
• D33: MO 27% blastos – TMO?
• D64: MO M1
• CONDUTA: Completou tratamento, FT em 1RCC – 8 anos
• LI : 7500/mm3, 6a 5m• SNC 1• IF: LLA comum• Cariótipo: 46 , XY• BM : bcr-abl p 190 : neg
ETV6 – RUN X1 : negProtocolo IC BFM 2002 - RID8: < 1000 bl/mm3D15 : MO – M1D 33 : MO – M1Recidiva Mo Isolada: 7 meses pós FT6 irmãos não compatíveis –
Refratariedade

OBRIGADA [email protected]