research article the expression of cd14 cd16 monocyte
TRANSCRIPT
Hindawi Publishing CorporationEvidence-Based Complementary and Alternative MedicineVolume 2013 Article ID 416932 6 pageshttpdxdoiorg1011552013416932
Research ArticleThe Expression of CD14+CD16+ Monocyte Subpopulation inCoronary Heart Disease Patients with Blood Stasis Syndrome
Ye Huang1 Jing-Shang Wang2 Hui-jun Yin2 and Ke-ji Chen2
1 Emergency Department Xiyuan Hospital China Academy of Chinese Medical Sciences Beijing 10091 China2Department of Cardiovascular Disease Xiyuan Hospital China Academy of Chinese Medical Sciences Beijing 100091 China
Correspondence should be addressed to Hui-jun Yin huijunyinaliyuncom
Received 6 March 2013 Revised 31 May 2013 Accepted 9 June 2013
Academic Editor Hao Xu
Copyright copy 2013 Ye Huang et alThis is an open access article distributed under theCreative CommonsAttribution License whichpermits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Blood stasis syndrome (BSS) a comprehensive pathological state is one of the traditional Chinesemedicine syndromes of coronaryheart disease (CHD) In our previous study we investigated that Fc120574RIIIA (also called CD14+CD16+ monocyte subpopulation)is one of the differentially expressed genes related to CHD patients and its possible role in the atherosclerotic formation andplaque rupture However whether or not the deregulation of CD14+CD16+monocyte subpopulation expression is implicated in thepathogenesis of CHD patients with BSS has not yet been elucidated In this study we found that there was no significant differencebetween CHDpatients with BSS and non-BSS in CD14+CD16+monocyte subpopulation at gene level Moreover the protein level ofCD14+CD16+ monocyte subpopulation in CHD patients with BSS was increased significantly when compared to the CHD patientswith non-BSS Additionally the level of inflammatory cytokines downstream of CD14+CD16+ monocyte subpopulation such asTNF-120572 and IL-1 in sera was much higher in CHD patients with BSS than that in CHD patients with non-BSS Taken together theseresults indicated that CD14+CD16+ monocyte subpopulation was implicated in the pathogenesis of CHD patients with BSS whichmay be one of the bases of the essence of BSS investigation
1 Introduction
The way of disease-syndrome combination is an importantstyle to diagnose and treat disease in traditional Chinesemedicine (TCM) clinical practice today Study on the bloodstasis syndrome (BSS) is the most active field of inte-gration of traditional and western medicine research inChina [1] To normalize and standardize the BSS the wayof disease-syndrome combination is used to explore theessence of BSS which will be the inevitable tendency inthe future Study on CHD with BSS initiated by researchteam of Chen keji is the model of the way of disease-syndrome combination In our previous study we foundthat Fc receptor III A of immunoglobulin G (Fc120574RIIIAalso called CD14+CD16+ monocyte subpopulation) is one ofthe differentially expressed genes related to coronary heartdisease (CHD) patients using the oligonucleotide microarraytechnique [2] and high level of Fc120574RIIIA in CHD patientsobserved previously was verified by both mRNA level and itsprotein content [3] Our recent study suggested an important
role of Fc120574RIIIA in the atherosclerotic formation by elevatingthe adhesive efficiency of monocytes to HUVECs in vitroby increasing expression of inflammatory cytokines andalso by kindling the atherosclerotic plaque destabilizationin ApoEminusminus mouse [4] Additionally we also investigatedthat traditional Chinese medicine of activation of bloodand dissolving stasis effective components of ChuanxiongRhizome and Red Peony Root could stabilize the atheroscle-rotic plaque by suppressing inflammation and its target wasrelative with Fc120574RIIIA [5] However whether or not thederegulation of the expression of CD14+CD16+ monocytesubpopulation is implicated in the pathogenesis of CHDpatients with BSS has not yet been elucidated
2 Methods
21 Patients and Healthy Control All patients with coronaryheart disease were the inpatients of Beijing Anzhen Hospitalfrom May 2010 to December 2010 diagnosed by a diameter
2 Evidence-Based Complementary and Alternative Medicine
Table 1 Characteristics of the CHD patients with BSSnon-BSS and healthy individuals participated in the study
CHD patientsBSS patients Non-BSS patients Healthy control 119875 value(119899 = 50) (119899 = 50) (119899 = 40)
Age (year) 5300 plusmn 643 5292 plusmn 603 4950 plusmn 871 0507Sex (malefemale) 3614 3317 2812 0804BMI (kgm2) 2550 plusmn 277 2510 plusmn 257 2429 plusmn 157 0509SAP (119899) 12 13 mdash mdashACS (119899) 38 37 mdash mdash
UAP (119899) 31 31 mdash mdashAMI (119899) 7 6 mdash mdash
Hypercholesterolemia (gt230mgdL) (yesno) 743 545 mdash mdashHypertension (yesno) 3119 3020 mdash mdashDiabetes (yesno) 2030 2030 mdash mdashMonocyte count (mmolL) 038 plusmn 011 037 plusmn 020 036 plusmn 011 0891BMI bodymass index SAP stable angina pectoris ACS acute coronary syndromeUAP unstable angina AMI acutemyocardial infarctionData are expressedas mean plusmn SD
stenosis of at least 50 from standard selective coronaryangiography [6 7] These CHD patients were selected intoblood stasis syndrome (BSS) group and non-BSS group basedon the standard diagnostic criteria established by the SpecialCommittee of Promoting Blood Circulation and RemovingBlood Stasis ChineseAssociation of IntegrativeMedicine [8]Patients with severe valvulopathy serious primary diseasessuch as liver or kidney dysfunction malignant tumorsmedication history of antiplatelet therapy and women inpregnancy or lactation stage were excluded from enroll-ment Forty age- and sex-matched healthy individuals fromthe physical examination center of Xiyuan Hospital wereselected as a control group These individuals were withoutany history of chest pain or evidence of cardiac or othersystemic disease verified by history examination chest filmelectrocardiogram and blood routine examination and nonewas taking anymedication Our studywas in accordancewiththe Helsinki Declaration with ethical approval granted bythe Ethics Committee at Xiyuan Hospital China Academyof Chinese Medical Sciences and a written informed consentwas obtained from all study participants The clinical charac-teristics of the participants are shown in Table 1
22 Blood Samples Peripheral blood was collected from theCHD patients with BSSnon-BSS and healthy subjects understandardized conditions Blood from CHD patients wasdrawn before coronary angiography was performed For theanalyses of cytometry or mRNA expression or flow cytom-etry 2mL ethylenediaminetetraacetate- (EDTA-) anticoag-ulated blood was taken and immediately analyzed For thedetection of inflammatory cytokines by ELISA assay bloodwas centrifuged at 3000 rpm for 20min and serum wasfrozen at minus80∘C until analysis
23 RT-PCR Fc120574RIIIA mRNA expression was investigatedby the quantitative real-time polymerase chain reaction(PCR) assay Total RNA samples were extracted from leuko-cytes using Trizol reagent (Invitrogen USA) according to
the manufacturerrsquos protocol The purity and integrity of RNAwere determined on a UV spectrophotometer (EppendorfGermany) by 260ndash280 nm absorbance ratio and agarosegel electrophoresis (15) and ethidium bromide stainingrespectively cDNA preparations were performed at 42∘Cfor 1 h with reverse transcriptase 2120583L RNase 2 120583L of anoligo (dT) primer and 10mM of each dNTP in a totalvolume of 50 120583L of 1x first strand cDNA synthesis bufferincubated at 70∘C for 10min PCR assays were carried outin a PCR (ABI 7500 USA) 15 120583L of cDNA mixture wassubjected to amplification in a 20120583L mixture The followingprimer sequenceswith the predicted size were used for ampli-fication Fc120574RIIIA forward 51015840-TGTTCAAGGAGGAAG-ACCCT-31015840 reverse 51015840-GAAGTAGGAGCCGCTGTCTT-31015840GAPDH forward 51015840-GGGTGTGAACCATGAGAAGT-31015840reverse 51015840-GGCATGGACTGTGGTCATGA-31015840 PCR condi-tions were as follows initial denaturation at 94∘C for 15minfollowed by 40 cycles of denaturation for 15 s at 94∘C anneal-ing at 60∘C for 34 sec extending at 72∘C for 15 sec and a finalextension at 72∘C for 10min Glyceraldehydes-3-phosphatedehydrogenase (GAPDH) was used as an internal control inall PCR reactions The PCR products were subjected to 2agarose gel electrophoresis The relative mRNA expressionlevel of the target gene in each individual was calculated usingthe comparative cycle time (119862t) method [9]
24 Flow Cytometry Fc120574RIIIA protein level was assessed byflow cytometry Ethylenediaminetetraacetic-Acid- (EDTA-)anticoagulated peripheral blood (PB) samples were collectedfrom all patients and healthy controls for flow cytomet-ric analysis performed previously described [10] BrieflyPB samples were stained with saturating concentrations offluorescein-isothiocyanate- (FITC-) conjugated anti-CD14monoclonal antibody (mAb) (BD Biosciences Lot 74003)and phycoerythrin- (PE-) conjugated anti-CD16 mAb (BDBiosciences Lot 73903) or isotype-matched control mAb for20min at room temperature in the dark After erythrocyteswere lysed by incubation with lysing solution for 8min PB
Evidence-Based Complementary and Alternative Medicine 3
P lt 001 P lt 005
Cont BSS Non-BSS0
sCD
14 co
nten
t (U
mL)
10
5
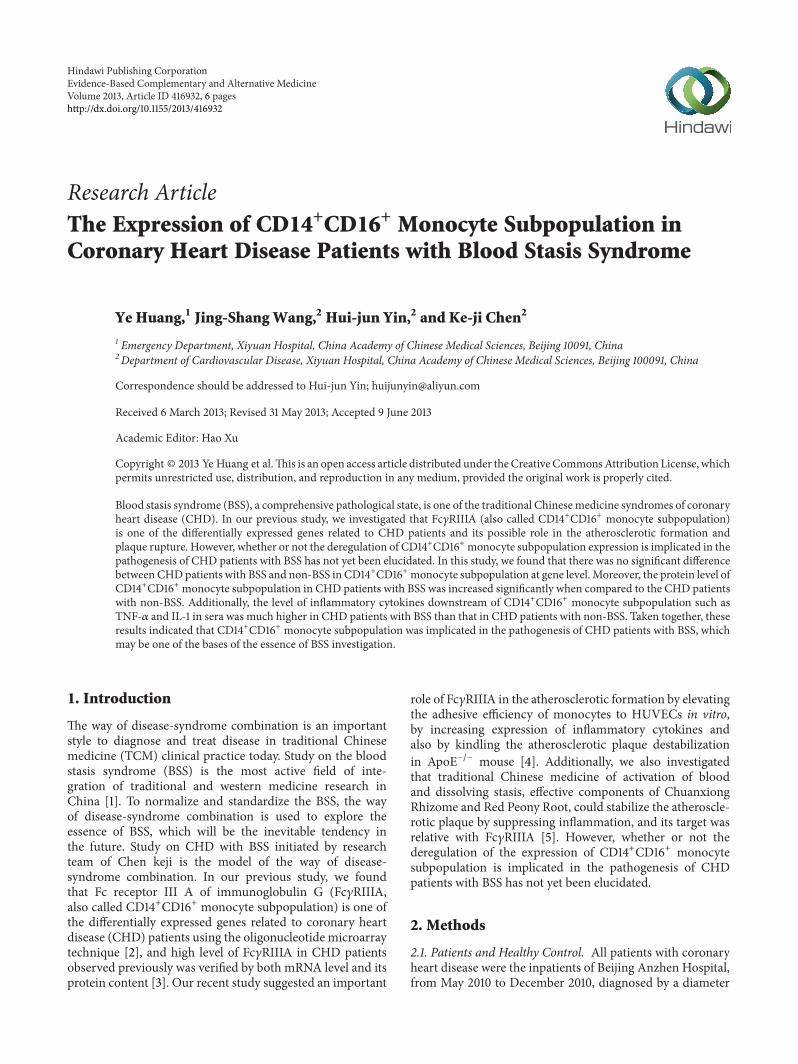
Figure 1 The significant level of soluble CD14 in sera in CHDpatients with BSS by ELSIA assay Results were presented as mean plusmnSD
mononuclear cells were resuspended in PBS with 1 fetalcalf serum The surface expression of CD14 and CD16 on PBmonocytes was performed by a fluorescence-activated cellsorter (FACS) cytometer (Becton Dickinson) The test datawere obtained by FS versus SS gate and analyzed by Expo32special software Monocytes were identified by gating CD14+events and all additional analyses were performed on thispopulation Fc120574RIIIA protein content defined by the percent-age of CD16 on the monocyte population (CD14+CD16+)was measured
25 Enzyme-Linked Immunosorbent Assay (ELISA) Concen-trations of TNF-120572 (RampD USA Lot 1007143) IL-1 (RampDUSA Lot 1007155) and soluble CD14 (sCD14) (RampD USALot 1010179) in sera were determined by double-antibodysandwich avidin-biotin peroxidase complex enzyme-linkedimmunosorbent assay (ABC-ELISA) according to manufac-turerrsquos instructions
26 Statistical Analysis All data are expressed as mean plusmnSD The SPSS Statistics 150 package was utilized to analyzethe data Differences among groups were analyzed usingthe one-way analysis of variance (ANOVA) followed bymultiple comparisons by LSD test Difference was consideredsignificant at 119875 lt 005
3 Results and Discussion
BSS is a pathological state which is the outwardmanifestationof some certain pathological stage of various diseases Dueto lack of objective diagnosis criteria the essence of BSSis studied into the bottleneck stage Recently based onthe way of disease-syndrome combination much effective
Cont BSS Non-BSS0
2
1
Relat
ive e
xpre
ssio
n le
vel
lowast
lowast
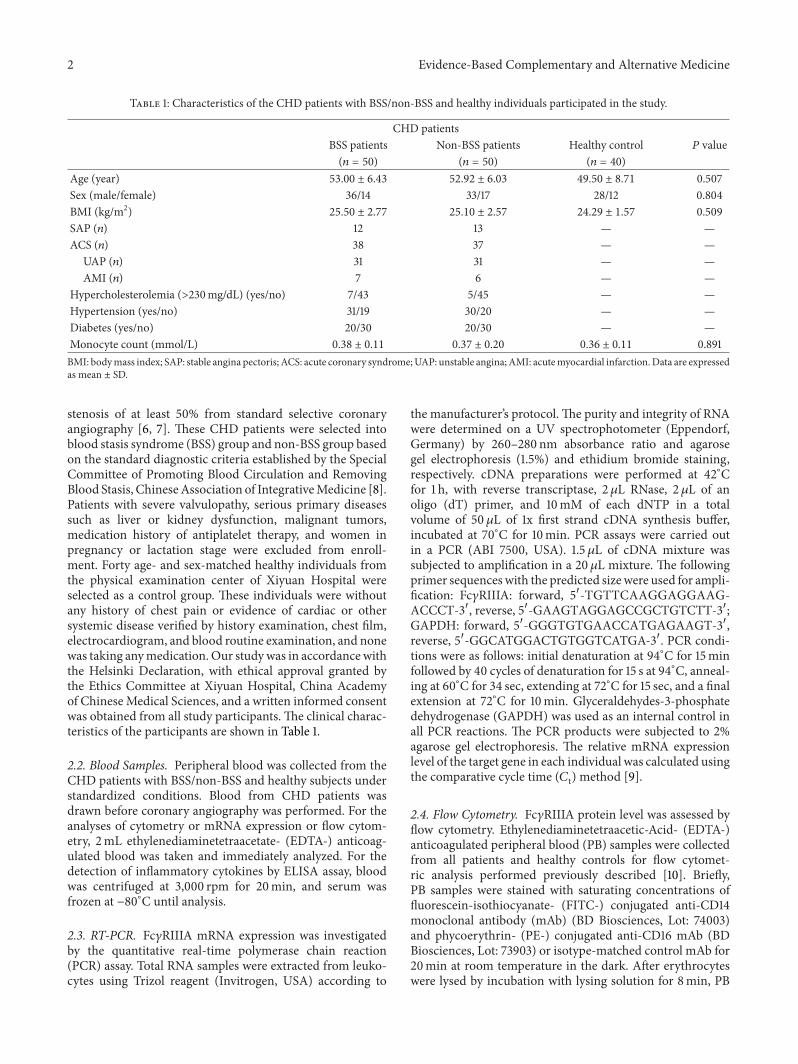
Figure 2 The mRNA level of CD14+CD16+ monocyte subpopula-tion in leukocytes in CHDpatients with BSS by qRT-PCR lowast119875 lt 001compared to the control group Results were presented as mean plusmnSD
exploration of the essence of BSS was the foundation of BSSobjective diagnosis criteria construction During the past 50years we found a correlation between CHD with BSS andinflammatory hemodynamics platelet andmicrocirculation[11]
Atherosclerosis a chronic inflammatory immune stateis chiefly responsible for the development of CHD Variousleukocytes have been shown to influence atherogenesisMonocytes and their descendant macrophages are centralprotagonists in the development of atherosclerosis [12]Monocyte migration to the vessel wall is an initial event inthe growth of atherosclerotic lesions [13] Once monocytesare activated adhesion to endothelial cells was inducedby the transform of phenotype which led to myocardiuminjury inducing the proinflammatory cytokines such as TNF-120572 and IL-1 synthesis to initiate the inflammatory cascadereaction and oxidative stress injury producing matrix met-alloproteinase (MMP) and releasing many media to induceplaque instability and even fracture [14 15] Thereforemonocytes played the key role in the chronic inflammation-immunoreaction of the arterial vessels In our study weinvestigated that there was no significant difference of mono-cyte count based on CBC count among CHD patients withBSS non-BSS and healthy control (Table 1) However thelevel of sCD14 which is the indicator of activated monocyte[16] was obviously increased in CHD patients with BSScompared to non-BSS and healthy control (Figure 1) Theincreased level of sCD14 in sera in CHD patients withBSS indicated monocytes activation To demonstrate thecorrelation between deregulated expression of CD14+CD16+monocyte subpopulation and pathogenesis of CHDwith BSSits mRNA expression at the leukocyte level was assessed Asshown in Figure 2 relative expression level of CD14+CD16+
4 Evidence-Based Complementary and Alternative Medicine
105
105
104
104
103
103
102
102
Cont BSS Non-BSS
CD16
-PE
105
104
103
102
CD16
-PE
105
104
103
102
CD16
-PE
CD14-FITC
105
104
103
102
CD14-FITC
105
104
103
102
CD14-FITC
(a)
P lt 001 P lt 005
Cont BSS Non-BSS
16
8
0
CD14
+CD
16+
mon
ocyt
e (
)
(b)
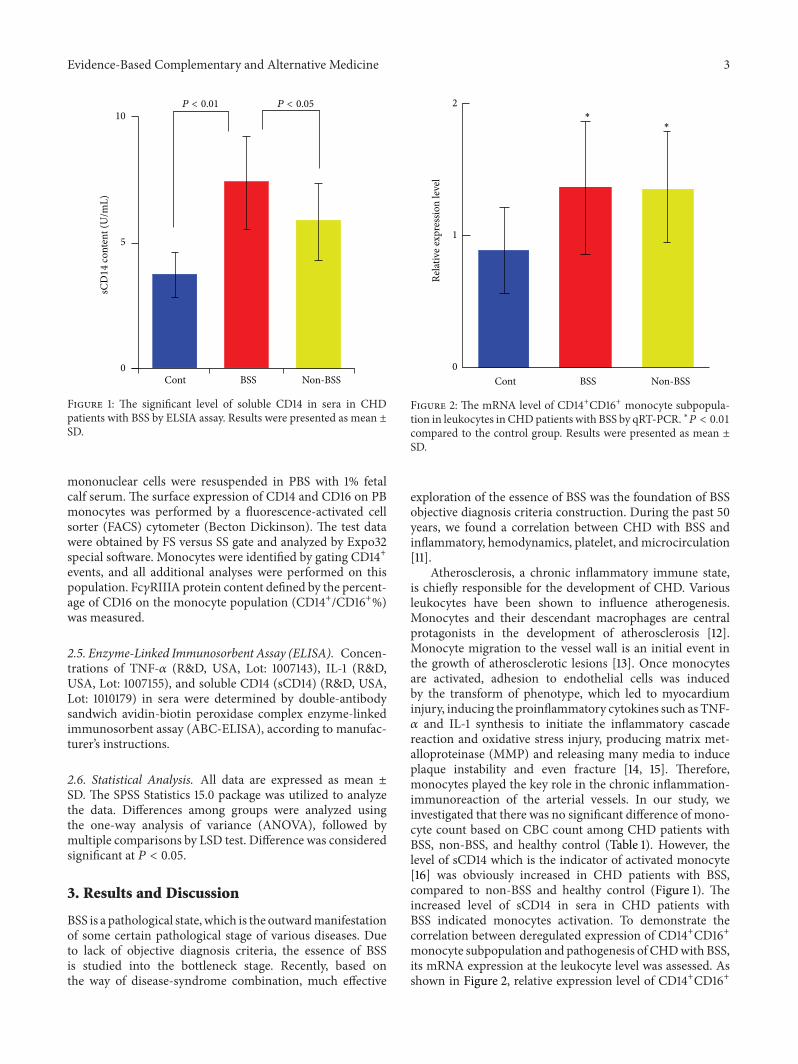
Figure 3The protein level of CD14+CD16+ monocyte subpopulation in CHD patients with BSS by FACS analysis (a) Representation data ofFACS analysis of CD14+CD16+monocyte subpopulationWhole peripheral blood samples from patients and healthy individuals were stainedwith FITC-conjugated anti-CD14 antibody and PE-conjugated anti-CD16 antibody followed by FACS (b) The percentage of CD14+CD16+monocoyte subpopulation in the whole CD14-positive cells Results were presented as mean plusmn SD
monocyte subpopulation in both CHD patients with BSS andnon-BBS was largely increased by 99 and 77 respectivelycompared to the healthy control (119875 lt 001) However therewas no significant difference of this relative expression levelbetween CHDpatients with BSS and non-BSS (Figure 2)Theexpression of biological traits was controlled by gene andthe biological traits were reflected by protein To investigatewhether or not the expression change of CD14+CD16+mono-cyte subpopulation in both CHD patients with BSS and non-BSS at its protein level therefore we further analyzed theprotein level of CD14+CD16+ on monocyte member using2-color immunofluorescent staining (Figure 3(a)) The FACSresults showed that the protein level of CD14+CD16+ onmonocyte member was significantly increased in the CHDpatients with BSS when compared to the CHD patients withnon-BSS and the healthy control (119875 lt 001 or 119875 lt 005Figure 3(b))
TNF-120572 is one of the cytokines with various biologicalactivation and one previous study confirms that increasedlevel of TNF-120572 was existed in the monocytemacrophagesmooth muscle cells and endothelial cells in the atheroscle-rotic plaque and this high level was correlated to theseverity of atherosclerosis [17] IL-1 was released by activemonocytemacrophage which induced the releasing of manycytokines and growth factors by monocytemacrophage andthe expression of adhesion molecules such as ICAM-1 Addi-tionally IL-1 could stimulate vascular endothelium to pro-duce many inflammatory factors such as TNF-120572 aggravatedlocal inflammatory reaction and promote the developmentof atherosclerosis [18 19] Additionally previous studiesindicated that the circulation of CD14+CD16+ monocytescould spontaneously produce TNF and IL-1 [20] which couldprovoke cell proliferation and migration of smooth musclecells and macrophages in the atherosclerotic plaque [21]
Evidence-Based Complementary and Alternative Medicine 5
TNF-120572
lowast
lowast
lowast
lowast
IL-1
Cont BSS Non-BSS
Cyto
kine
cont
ent (
pgm
L)
120
60
0
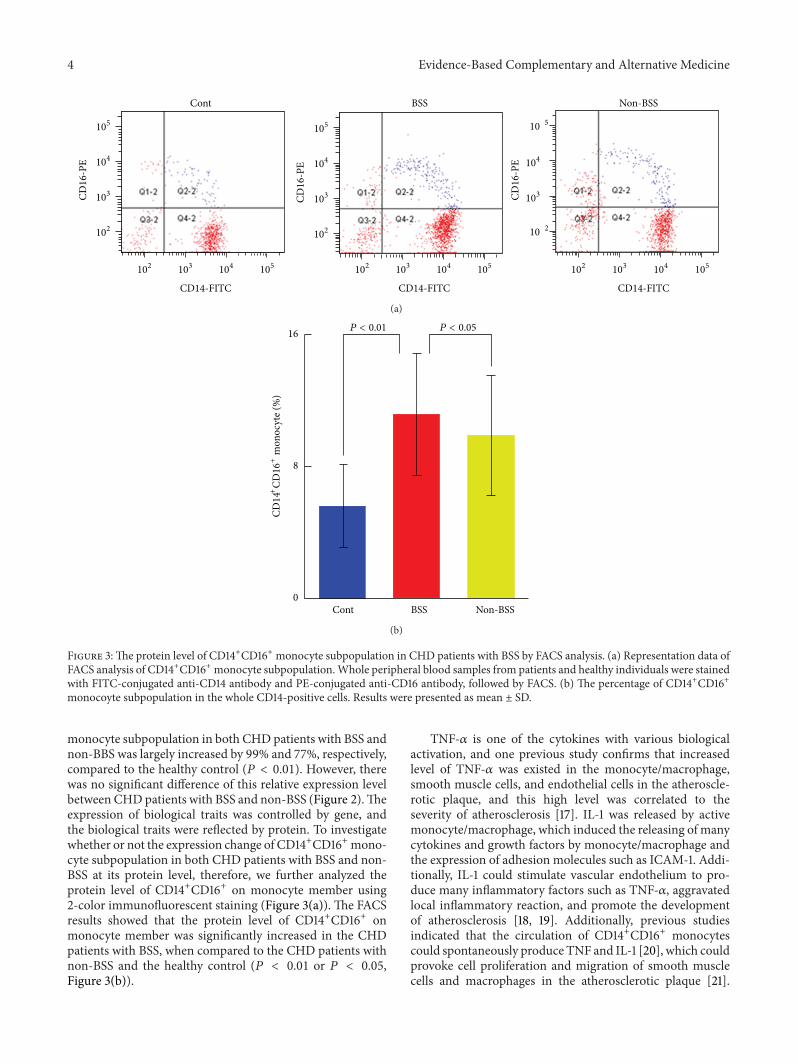
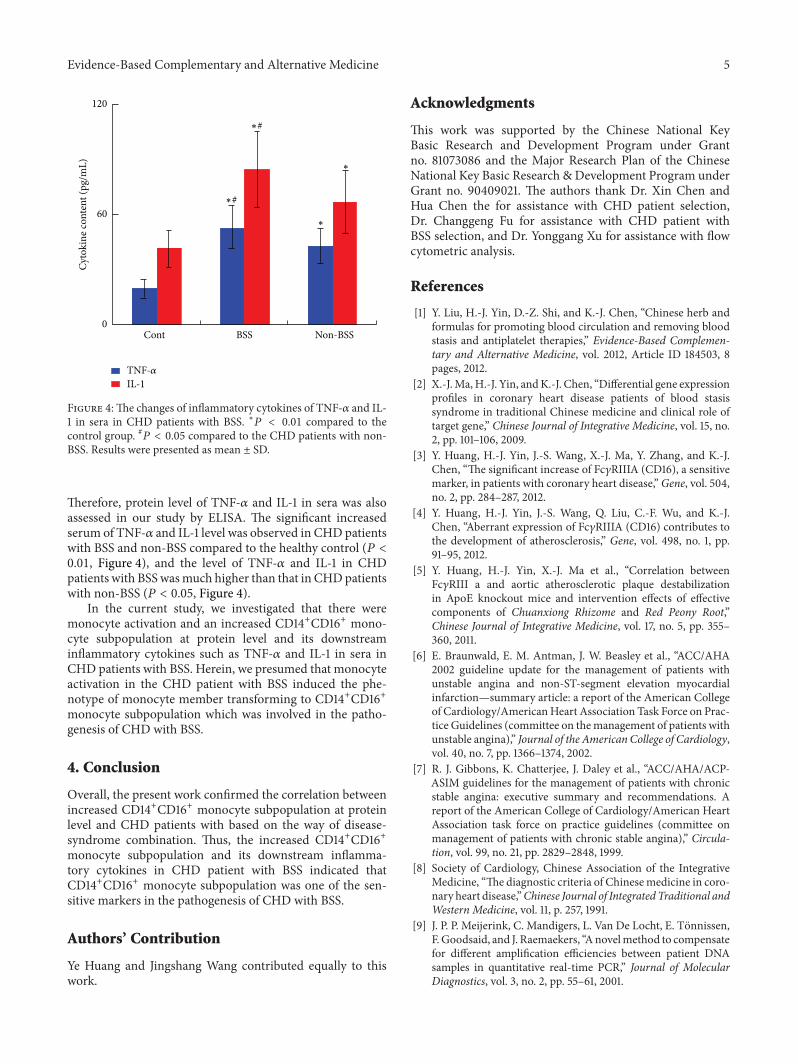
Figure 4The changes of inflammatory cytokines of TNF-120572 and IL-1 in sera in CHD patients with BSS lowast119875 lt 001 compared to thecontrol group 119875 lt 005 compared to the CHD patients with non-BSS Results were presented as mean plusmn SD
Therefore protein level of TNF-120572 and IL-1 in sera was alsoassessed in our study by ELISA The significant increasedserum of TNF-120572 and IL-1 level was observed in CHD patientswith BSS and non-BSS compared to the healthy control (119875 lt001 Figure 4) and the level of TNF-120572 and IL-1 in CHDpatients with BSSwasmuch higher than that in CHDpatientswith non-BSS (119875 lt 005 Figure 4)
In the current study we investigated that there weremonocyte activation and an increased CD14+CD16+ mono-cyte subpopulation at protein level and its downstreaminflammatory cytokines such as TNF-120572 and IL-1 in sera inCHD patients with BSS Herein we presumed that monocyteactivation in the CHD patient with BSS induced the phe-notype of monocyte member transforming to CD14+CD16+monocyte subpopulation which was involved in the patho-genesis of CHD with BSS
4 Conclusion
Overall the present work confirmed the correlation betweenincreased CD14+CD16+ monocyte subpopulation at proteinlevel and CHD patients with based on the way of disease-syndrome combination Thus the increased CD14+CD16+monocyte subpopulation and its downstream inflamma-tory cytokines in CHD patient with BSS indicated thatCD14+CD16+ monocyte subpopulation was one of the sen-sitive markers in the pathogenesis of CHD with BSS
Authorsrsquo Contribution
Ye Huang and Jingshang Wang contributed equally to thiswork
Acknowledgments
This work was supported by the Chinese National KeyBasic Research and Development Program under Grantno 81073086 and the Major Research Plan of the ChineseNational Key Basic Research amp Development Program underGrant no 90409021 The authors thank Dr Xin Chen andHua Chen the for assistance with CHD patient selectionDr Changgeng Fu for assistance with CHD patient withBSS selection and Dr Yonggang Xu for assistance with flowcytometric analysis
References
[1] Y Liu H-J Yin D-Z Shi and K-J Chen ldquoChinese herb andformulas for promoting blood circulation and removing bloodstasis and antiplatelet therapiesrdquo Evidence-Based Complemen-tary and Alternative Medicine vol 2012 Article ID 184503 8pages 2012
[2] X-JMaH-J Yin andK-J Chen ldquoDifferential gene expressionprofiles in coronary heart disease patients of blood stasissyndrome in traditional Chinese medicine and clinical role oftarget generdquo Chinese Journal of Integrative Medicine vol 15 no2 pp 101ndash106 2009
[3] Y Huang H-J Yin J-S Wang X-J Ma Y Zhang and K-JChen ldquoThe significant increase of Fc120574RIIIA (CD16) a sensitivemarker in patients with coronary heart diseaserdquoGene vol 504no 2 pp 284ndash287 2012
[4] Y Huang H-J Yin J-S Wang Q Liu C-F Wu and K-JChen ldquoAberrant expression of Fc120574RIIIA (CD16) contributes tothe development of atherosclerosisrdquo Gene vol 498 no 1 pp91ndash95 2012
[5] Y Huang H-J Yin X-J Ma et al ldquoCorrelation betweenFc120574RIII a and aortic atherosclerotic plaque destabilizationin ApoE knockout mice and intervention effects of effectivecomponents of Chuanxiong Rhizome and Red Peony RootrdquoChinese Journal of Integrative Medicine vol 17 no 5 pp 355ndash360 2011
[6] E Braunwald E M Antman J W Beasley et al ldquoACCAHA2002 guideline update for the management of patients withunstable angina and non-ST-segment elevation myocardialinfarctionmdashsummary article a report of the American Collegeof CardiologyAmericanHeart Association Task Force on Prac-tice Guidelines (committee on themanagement of patients withunstable angina)rdquo Journal of the American College of Cardiologyvol 40 no 7 pp 1366ndash1374 2002
[7] R J Gibbons K Chatterjee J Daley et al ldquoACCAHAACP-ASIM guidelines for the management of patients with chronicstable angina executive summary and recommendations Areport of the American College of CardiologyAmerican HeartAssociation task force on practice guidelines (committee onmanagement of patients with chronic stable angina)rdquo Circula-tion vol 99 no 21 pp 2829ndash2848 1999
[8] Society of Cardiology Chinese Association of the IntegrativeMedicine ldquoThe diagnostic criteria of Chinesemedicine in coro-nary heart diseaserdquoChinese Journal of Integrated Traditional andWestern Medicine vol 11 p 257 1991
[9] J P P Meijerink C Mandigers L Van De Locht E TonnissenFGoodsaid and J Raemaekers ldquoAnovelmethod to compensatefor different amplification efficiencies between patient DNAsamples in quantitative real-time PCRrdquo Journal of MolecularDiagnostics vol 3 no 2 pp 55ndash61 2001
6 Evidence-Based Complementary and Alternative Medicine
[10] T Gremmel C W Kopp D Seidinger et al ldquoThe formationofmonocyte-platelet aggregates is independent of on-treatmentresidual agonistsrsquo-inducible platelet reactivityrdquo Atherosclerosisvol 207 no 2 pp 608ndash613 2009
[11] K-J Chen ldquoExploration on the possibility of reducing cardio-vascular risk by treatment with Chinese medicine recipes forpromoting blood-circulation and relieving blood-stasisrdquo ZhongGuo Zhong Xi Yi Jie He Za Zhi vol 28 no 5 p 389 2008
[12] M J Pittet and F K Swirski ldquoMonocytes link atherosclerosisand cancerrdquo European Journal of Immunology vol 41 no 9 pp2519ndash2522 2011
[13] K JWoollard and FGeissmann ldquoMonocytes in atherosclerosissubsets and functionsrdquo Nature Reviews Cardiology vol 7 no 2pp 77ndash86 2010
[14] B Pamukcu G Y H Lip A Devitt H Griffiths and EShantsila ldquoThe role of monocytes in atherosclerotic coronaryartery diseaserdquo Annals of Medicine vol 42 no 6 pp 394ndash4032010
[15] P Saha B Modarai J Humphries et al ldquoThemonocytemacro-phage as a therapeutic target in atherosclerosisrdquo Current Opin-ion in Pharmacology vol 9 no 2 pp 109ndash118 2009
[16] C Kruger C Schutt U Obertacke et al ldquoSerum CD14 levelsin polytraumatized and severely burned patientsrdquo Clinical andExperimental Immunology vol 85 no 2 pp 297ndash301 1991
[17] P Barath M C Fishbein J Cao J Berenson R H Helfantand J S Forrester ldquoDetection and localization of tumor necrosisfactor in human atheromardquoAmerican Journal of Cardiology vol65 no 5 pp 297ndash302 1990
[18] F Merhi-Soussi B R Kwak D Magne et al ldquoInterleukin-1plays a major role in vascular inflammation and atherosclero-sis in male apolipoprotein E-knockout micerdquo CardiovascularResearch vol 66 no 3 pp 583ndash593 2005
[19] K Isoda S Sawada N Ishigami et al ldquoLack of interleukin-1 receptor antagonist modulates plaque composition inapolipoprotein E-deficient micerdquo Arteriosclerosis Thrombosisand Vascular Biology vol 24 no 6 pp 1068ndash1073 2004
[20] M Frankenberger T Sternsdorf H Pechumer A Pforte andH W L Ziegler-Heitbrock ldquoDifferential cytokine expressionin human blood monocyte subpopulations a polymerase chainreaction analysisrdquo Blood vol 87 no 1 pp 373ndash377 1996
[21] N de Bont M G Netea C Rovers et al ldquoLPS-inducedrelease of IL-1120573 IL-1Ra IL-6 and TNF-120572 in whole bloodfrom patients with familial hypercholesterolemia no effectof cholesterol-lowering treatmentrdquo Journal of Interferon andCytokine Research vol 26 no 2 pp 101ndash107 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
2 Evidence-Based Complementary and Alternative Medicine
Table 1 Characteristics of the CHD patients with BSSnon-BSS and healthy individuals participated in the study
CHD patientsBSS patients Non-BSS patients Healthy control 119875 value(119899 = 50) (119899 = 50) (119899 = 40)
Age (year) 5300 plusmn 643 5292 plusmn 603 4950 plusmn 871 0507Sex (malefemale) 3614 3317 2812 0804BMI (kgm2) 2550 plusmn 277 2510 plusmn 257 2429 plusmn 157 0509SAP (119899) 12 13 mdash mdashACS (119899) 38 37 mdash mdash
UAP (119899) 31 31 mdash mdashAMI (119899) 7 6 mdash mdash
Hypercholesterolemia (gt230mgdL) (yesno) 743 545 mdash mdashHypertension (yesno) 3119 3020 mdash mdashDiabetes (yesno) 2030 2030 mdash mdashMonocyte count (mmolL) 038 plusmn 011 037 plusmn 020 036 plusmn 011 0891BMI bodymass index SAP stable angina pectoris ACS acute coronary syndromeUAP unstable angina AMI acutemyocardial infarctionData are expressedas mean plusmn SD
stenosis of at least 50 from standard selective coronaryangiography [6 7] These CHD patients were selected intoblood stasis syndrome (BSS) group and non-BSS group basedon the standard diagnostic criteria established by the SpecialCommittee of Promoting Blood Circulation and RemovingBlood Stasis ChineseAssociation of IntegrativeMedicine [8]Patients with severe valvulopathy serious primary diseasessuch as liver or kidney dysfunction malignant tumorsmedication history of antiplatelet therapy and women inpregnancy or lactation stage were excluded from enroll-ment Forty age- and sex-matched healthy individuals fromthe physical examination center of Xiyuan Hospital wereselected as a control group These individuals were withoutany history of chest pain or evidence of cardiac or othersystemic disease verified by history examination chest filmelectrocardiogram and blood routine examination and nonewas taking anymedication Our studywas in accordancewiththe Helsinki Declaration with ethical approval granted bythe Ethics Committee at Xiyuan Hospital China Academyof Chinese Medical Sciences and a written informed consentwas obtained from all study participants The clinical charac-teristics of the participants are shown in Table 1
22 Blood Samples Peripheral blood was collected from theCHD patients with BSSnon-BSS and healthy subjects understandardized conditions Blood from CHD patients wasdrawn before coronary angiography was performed For theanalyses of cytometry or mRNA expression or flow cytom-etry 2mL ethylenediaminetetraacetate- (EDTA-) anticoag-ulated blood was taken and immediately analyzed For thedetection of inflammatory cytokines by ELISA assay bloodwas centrifuged at 3000 rpm for 20min and serum wasfrozen at minus80∘C until analysis
23 RT-PCR Fc120574RIIIA mRNA expression was investigatedby the quantitative real-time polymerase chain reaction(PCR) assay Total RNA samples were extracted from leuko-cytes using Trizol reagent (Invitrogen USA) according to
the manufacturerrsquos protocol The purity and integrity of RNAwere determined on a UV spectrophotometer (EppendorfGermany) by 260ndash280 nm absorbance ratio and agarosegel electrophoresis (15) and ethidium bromide stainingrespectively cDNA preparations were performed at 42∘Cfor 1 h with reverse transcriptase 2120583L RNase 2 120583L of anoligo (dT) primer and 10mM of each dNTP in a totalvolume of 50 120583L of 1x first strand cDNA synthesis bufferincubated at 70∘C for 10min PCR assays were carried outin a PCR (ABI 7500 USA) 15 120583L of cDNA mixture wassubjected to amplification in a 20120583L mixture The followingprimer sequenceswith the predicted size were used for ampli-fication Fc120574RIIIA forward 51015840-TGTTCAAGGAGGAAG-ACCCT-31015840 reverse 51015840-GAAGTAGGAGCCGCTGTCTT-31015840GAPDH forward 51015840-GGGTGTGAACCATGAGAAGT-31015840reverse 51015840-GGCATGGACTGTGGTCATGA-31015840 PCR condi-tions were as follows initial denaturation at 94∘C for 15minfollowed by 40 cycles of denaturation for 15 s at 94∘C anneal-ing at 60∘C for 34 sec extending at 72∘C for 15 sec and a finalextension at 72∘C for 10min Glyceraldehydes-3-phosphatedehydrogenase (GAPDH) was used as an internal control inall PCR reactions The PCR products were subjected to 2agarose gel electrophoresis The relative mRNA expressionlevel of the target gene in each individual was calculated usingthe comparative cycle time (119862t) method [9]
24 Flow Cytometry Fc120574RIIIA protein level was assessed byflow cytometry Ethylenediaminetetraacetic-Acid- (EDTA-)anticoagulated peripheral blood (PB) samples were collectedfrom all patients and healthy controls for flow cytomet-ric analysis performed previously described [10] BrieflyPB samples were stained with saturating concentrations offluorescein-isothiocyanate- (FITC-) conjugated anti-CD14monoclonal antibody (mAb) (BD Biosciences Lot 74003)and phycoerythrin- (PE-) conjugated anti-CD16 mAb (BDBiosciences Lot 73903) or isotype-matched control mAb for20min at room temperature in the dark After erythrocyteswere lysed by incubation with lysing solution for 8min PB
Evidence-Based Complementary and Alternative Medicine 3
P lt 001 P lt 005
Cont BSS Non-BSS0
sCD
14 co
nten
t (U
mL)
10
5
Figure 1 The significant level of soluble CD14 in sera in CHDpatients with BSS by ELSIA assay Results were presented as mean plusmnSD
mononuclear cells were resuspended in PBS with 1 fetalcalf serum The surface expression of CD14 and CD16 on PBmonocytes was performed by a fluorescence-activated cellsorter (FACS) cytometer (Becton Dickinson) The test datawere obtained by FS versus SS gate and analyzed by Expo32special software Monocytes were identified by gating CD14+events and all additional analyses were performed on thispopulation Fc120574RIIIA protein content defined by the percent-age of CD16 on the monocyte population (CD14+CD16+)was measured
25 Enzyme-Linked Immunosorbent Assay (ELISA) Concen-trations of TNF-120572 (RampD USA Lot 1007143) IL-1 (RampDUSA Lot 1007155) and soluble CD14 (sCD14) (RampD USALot 1010179) in sera were determined by double-antibodysandwich avidin-biotin peroxidase complex enzyme-linkedimmunosorbent assay (ABC-ELISA) according to manufac-turerrsquos instructions
26 Statistical Analysis All data are expressed as mean plusmnSD The SPSS Statistics 150 package was utilized to analyzethe data Differences among groups were analyzed usingthe one-way analysis of variance (ANOVA) followed bymultiple comparisons by LSD test Difference was consideredsignificant at 119875 lt 005
3 Results and Discussion
BSS is a pathological state which is the outwardmanifestationof some certain pathological stage of various diseases Dueto lack of objective diagnosis criteria the essence of BSSis studied into the bottleneck stage Recently based onthe way of disease-syndrome combination much effective
Cont BSS Non-BSS0
2
1
Relat
ive e
xpre
ssio
n le
vel
lowast
lowast
Figure 2 The mRNA level of CD14+CD16+ monocyte subpopula-tion in leukocytes in CHDpatients with BSS by qRT-PCR lowast119875 lt 001compared to the control group Results were presented as mean plusmnSD
exploration of the essence of BSS was the foundation of BSSobjective diagnosis criteria construction During the past 50years we found a correlation between CHD with BSS andinflammatory hemodynamics platelet andmicrocirculation[11]
Atherosclerosis a chronic inflammatory immune stateis chiefly responsible for the development of CHD Variousleukocytes have been shown to influence atherogenesisMonocytes and their descendant macrophages are centralprotagonists in the development of atherosclerosis [12]Monocyte migration to the vessel wall is an initial event inthe growth of atherosclerotic lesions [13] Once monocytesare activated adhesion to endothelial cells was inducedby the transform of phenotype which led to myocardiuminjury inducing the proinflammatory cytokines such as TNF-120572 and IL-1 synthesis to initiate the inflammatory cascadereaction and oxidative stress injury producing matrix met-alloproteinase (MMP) and releasing many media to induceplaque instability and even fracture [14 15] Thereforemonocytes played the key role in the chronic inflammation-immunoreaction of the arterial vessels In our study weinvestigated that there was no significant difference of mono-cyte count based on CBC count among CHD patients withBSS non-BSS and healthy control (Table 1) However thelevel of sCD14 which is the indicator of activated monocyte[16] was obviously increased in CHD patients with BSScompared to non-BSS and healthy control (Figure 1) Theincreased level of sCD14 in sera in CHD patients withBSS indicated monocytes activation To demonstrate thecorrelation between deregulated expression of CD14+CD16+monocyte subpopulation and pathogenesis of CHDwith BSSits mRNA expression at the leukocyte level was assessed Asshown in Figure 2 relative expression level of CD14+CD16+
4 Evidence-Based Complementary and Alternative Medicine
105
105
104
104
103
103
102
102
Cont BSS Non-BSS
CD16
-PE
105
104
103
102
CD16
-PE
105
104
103
102
CD16
-PE
CD14-FITC
105
104
103
102
CD14-FITC
105
104
103
102
CD14-FITC
(a)
P lt 001 P lt 005
Cont BSS Non-BSS
16
8
0
CD14
+CD
16+
mon
ocyt
e (
)
(b)
Figure 3The protein level of CD14+CD16+ monocyte subpopulation in CHD patients with BSS by FACS analysis (a) Representation data ofFACS analysis of CD14+CD16+monocyte subpopulationWhole peripheral blood samples from patients and healthy individuals were stainedwith FITC-conjugated anti-CD14 antibody and PE-conjugated anti-CD16 antibody followed by FACS (b) The percentage of CD14+CD16+monocoyte subpopulation in the whole CD14-positive cells Results were presented as mean plusmn SD
monocyte subpopulation in both CHD patients with BSS andnon-BBS was largely increased by 99 and 77 respectivelycompared to the healthy control (119875 lt 001) However therewas no significant difference of this relative expression levelbetween CHDpatients with BSS and non-BSS (Figure 2)Theexpression of biological traits was controlled by gene andthe biological traits were reflected by protein To investigatewhether or not the expression change of CD14+CD16+mono-cyte subpopulation in both CHD patients with BSS and non-BSS at its protein level therefore we further analyzed theprotein level of CD14+CD16+ on monocyte member using2-color immunofluorescent staining (Figure 3(a)) The FACSresults showed that the protein level of CD14+CD16+ onmonocyte member was significantly increased in the CHDpatients with BSS when compared to the CHD patients withnon-BSS and the healthy control (119875 lt 001 or 119875 lt 005Figure 3(b))
TNF-120572 is one of the cytokines with various biologicalactivation and one previous study confirms that increasedlevel of TNF-120572 was existed in the monocytemacrophagesmooth muscle cells and endothelial cells in the atheroscle-rotic plaque and this high level was correlated to theseverity of atherosclerosis [17] IL-1 was released by activemonocytemacrophage which induced the releasing of manycytokines and growth factors by monocytemacrophage andthe expression of adhesion molecules such as ICAM-1 Addi-tionally IL-1 could stimulate vascular endothelium to pro-duce many inflammatory factors such as TNF-120572 aggravatedlocal inflammatory reaction and promote the developmentof atherosclerosis [18 19] Additionally previous studiesindicated that the circulation of CD14+CD16+ monocytescould spontaneously produce TNF and IL-1 [20] which couldprovoke cell proliferation and migration of smooth musclecells and macrophages in the atherosclerotic plaque [21]
Evidence-Based Complementary and Alternative Medicine 5
TNF-120572
lowast
lowast
lowast
lowast
IL-1
Cont BSS Non-BSS
Cyto
kine
cont
ent (
pgm
L)
120
60
0
Figure 4The changes of inflammatory cytokines of TNF-120572 and IL-1 in sera in CHD patients with BSS lowast119875 lt 001 compared to thecontrol group 119875 lt 005 compared to the CHD patients with non-BSS Results were presented as mean plusmn SD
Therefore protein level of TNF-120572 and IL-1 in sera was alsoassessed in our study by ELISA The significant increasedserum of TNF-120572 and IL-1 level was observed in CHD patientswith BSS and non-BSS compared to the healthy control (119875 lt001 Figure 4) and the level of TNF-120572 and IL-1 in CHDpatients with BSSwasmuch higher than that in CHDpatientswith non-BSS (119875 lt 005 Figure 4)
In the current study we investigated that there weremonocyte activation and an increased CD14+CD16+ mono-cyte subpopulation at protein level and its downstreaminflammatory cytokines such as TNF-120572 and IL-1 in sera inCHD patients with BSS Herein we presumed that monocyteactivation in the CHD patient with BSS induced the phe-notype of monocyte member transforming to CD14+CD16+monocyte subpopulation which was involved in the patho-genesis of CHD with BSS
4 Conclusion
Overall the present work confirmed the correlation betweenincreased CD14+CD16+ monocyte subpopulation at proteinlevel and CHD patients with based on the way of disease-syndrome combination Thus the increased CD14+CD16+monocyte subpopulation and its downstream inflamma-tory cytokines in CHD patient with BSS indicated thatCD14+CD16+ monocyte subpopulation was one of the sen-sitive markers in the pathogenesis of CHD with BSS
Authorsrsquo Contribution
Ye Huang and Jingshang Wang contributed equally to thiswork
Acknowledgments
This work was supported by the Chinese National KeyBasic Research and Development Program under Grantno 81073086 and the Major Research Plan of the ChineseNational Key Basic Research amp Development Program underGrant no 90409021 The authors thank Dr Xin Chen andHua Chen the for assistance with CHD patient selectionDr Changgeng Fu for assistance with CHD patient withBSS selection and Dr Yonggang Xu for assistance with flowcytometric analysis
References
[1] Y Liu H-J Yin D-Z Shi and K-J Chen ldquoChinese herb andformulas for promoting blood circulation and removing bloodstasis and antiplatelet therapiesrdquo Evidence-Based Complemen-tary and Alternative Medicine vol 2012 Article ID 184503 8pages 2012
[2] X-JMaH-J Yin andK-J Chen ldquoDifferential gene expressionprofiles in coronary heart disease patients of blood stasissyndrome in traditional Chinese medicine and clinical role oftarget generdquo Chinese Journal of Integrative Medicine vol 15 no2 pp 101ndash106 2009
[3] Y Huang H-J Yin J-S Wang X-J Ma Y Zhang and K-JChen ldquoThe significant increase of Fc120574RIIIA (CD16) a sensitivemarker in patients with coronary heart diseaserdquoGene vol 504no 2 pp 284ndash287 2012
[4] Y Huang H-J Yin J-S Wang Q Liu C-F Wu and K-JChen ldquoAberrant expression of Fc120574RIIIA (CD16) contributes tothe development of atherosclerosisrdquo Gene vol 498 no 1 pp91ndash95 2012
[5] Y Huang H-J Yin X-J Ma et al ldquoCorrelation betweenFc120574RIII a and aortic atherosclerotic plaque destabilizationin ApoE knockout mice and intervention effects of effectivecomponents of Chuanxiong Rhizome and Red Peony RootrdquoChinese Journal of Integrative Medicine vol 17 no 5 pp 355ndash360 2011
[6] E Braunwald E M Antman J W Beasley et al ldquoACCAHA2002 guideline update for the management of patients withunstable angina and non-ST-segment elevation myocardialinfarctionmdashsummary article a report of the American Collegeof CardiologyAmericanHeart Association Task Force on Prac-tice Guidelines (committee on themanagement of patients withunstable angina)rdquo Journal of the American College of Cardiologyvol 40 no 7 pp 1366ndash1374 2002
[7] R J Gibbons K Chatterjee J Daley et al ldquoACCAHAACP-ASIM guidelines for the management of patients with chronicstable angina executive summary and recommendations Areport of the American College of CardiologyAmerican HeartAssociation task force on practice guidelines (committee onmanagement of patients with chronic stable angina)rdquo Circula-tion vol 99 no 21 pp 2829ndash2848 1999
[8] Society of Cardiology Chinese Association of the IntegrativeMedicine ldquoThe diagnostic criteria of Chinesemedicine in coro-nary heart diseaserdquoChinese Journal of Integrated Traditional andWestern Medicine vol 11 p 257 1991
[9] J P P Meijerink C Mandigers L Van De Locht E TonnissenFGoodsaid and J Raemaekers ldquoAnovelmethod to compensatefor different amplification efficiencies between patient DNAsamples in quantitative real-time PCRrdquo Journal of MolecularDiagnostics vol 3 no 2 pp 55ndash61 2001
6 Evidence-Based Complementary and Alternative Medicine
[10] T Gremmel C W Kopp D Seidinger et al ldquoThe formationofmonocyte-platelet aggregates is independent of on-treatmentresidual agonistsrsquo-inducible platelet reactivityrdquo Atherosclerosisvol 207 no 2 pp 608ndash613 2009
[11] K-J Chen ldquoExploration on the possibility of reducing cardio-vascular risk by treatment with Chinese medicine recipes forpromoting blood-circulation and relieving blood-stasisrdquo ZhongGuo Zhong Xi Yi Jie He Za Zhi vol 28 no 5 p 389 2008
[12] M J Pittet and F K Swirski ldquoMonocytes link atherosclerosisand cancerrdquo European Journal of Immunology vol 41 no 9 pp2519ndash2522 2011
[13] K JWoollard and FGeissmann ldquoMonocytes in atherosclerosissubsets and functionsrdquo Nature Reviews Cardiology vol 7 no 2pp 77ndash86 2010
[14] B Pamukcu G Y H Lip A Devitt H Griffiths and EShantsila ldquoThe role of monocytes in atherosclerotic coronaryartery diseaserdquo Annals of Medicine vol 42 no 6 pp 394ndash4032010
[15] P Saha B Modarai J Humphries et al ldquoThemonocytemacro-phage as a therapeutic target in atherosclerosisrdquo Current Opin-ion in Pharmacology vol 9 no 2 pp 109ndash118 2009
[16] C Kruger C Schutt U Obertacke et al ldquoSerum CD14 levelsin polytraumatized and severely burned patientsrdquo Clinical andExperimental Immunology vol 85 no 2 pp 297ndash301 1991
[17] P Barath M C Fishbein J Cao J Berenson R H Helfantand J S Forrester ldquoDetection and localization of tumor necrosisfactor in human atheromardquoAmerican Journal of Cardiology vol65 no 5 pp 297ndash302 1990
[18] F Merhi-Soussi B R Kwak D Magne et al ldquoInterleukin-1plays a major role in vascular inflammation and atherosclero-sis in male apolipoprotein E-knockout micerdquo CardiovascularResearch vol 66 no 3 pp 583ndash593 2005
[19] K Isoda S Sawada N Ishigami et al ldquoLack of interleukin-1 receptor antagonist modulates plaque composition inapolipoprotein E-deficient micerdquo Arteriosclerosis Thrombosisand Vascular Biology vol 24 no 6 pp 1068ndash1073 2004
[20] M Frankenberger T Sternsdorf H Pechumer A Pforte andH W L Ziegler-Heitbrock ldquoDifferential cytokine expressionin human blood monocyte subpopulations a polymerase chainreaction analysisrdquo Blood vol 87 no 1 pp 373ndash377 1996
[21] N de Bont M G Netea C Rovers et al ldquoLPS-inducedrelease of IL-1120573 IL-1Ra IL-6 and TNF-120572 in whole bloodfrom patients with familial hypercholesterolemia no effectof cholesterol-lowering treatmentrdquo Journal of Interferon andCytokine Research vol 26 no 2 pp 101ndash107 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Evidence-Based Complementary and Alternative Medicine 3
P lt 001 P lt 005
Cont BSS Non-BSS0
sCD
14 co
nten
t (U
mL)
10
5
Figure 1 The significant level of soluble CD14 in sera in CHDpatients with BSS by ELSIA assay Results were presented as mean plusmnSD
mononuclear cells were resuspended in PBS with 1 fetalcalf serum The surface expression of CD14 and CD16 on PBmonocytes was performed by a fluorescence-activated cellsorter (FACS) cytometer (Becton Dickinson) The test datawere obtained by FS versus SS gate and analyzed by Expo32special software Monocytes were identified by gating CD14+events and all additional analyses were performed on thispopulation Fc120574RIIIA protein content defined by the percent-age of CD16 on the monocyte population (CD14+CD16+)was measured
25 Enzyme-Linked Immunosorbent Assay (ELISA) Concen-trations of TNF-120572 (RampD USA Lot 1007143) IL-1 (RampDUSA Lot 1007155) and soluble CD14 (sCD14) (RampD USALot 1010179) in sera were determined by double-antibodysandwich avidin-biotin peroxidase complex enzyme-linkedimmunosorbent assay (ABC-ELISA) according to manufac-turerrsquos instructions
26 Statistical Analysis All data are expressed as mean plusmnSD The SPSS Statistics 150 package was utilized to analyzethe data Differences among groups were analyzed usingthe one-way analysis of variance (ANOVA) followed bymultiple comparisons by LSD test Difference was consideredsignificant at 119875 lt 005
3 Results and Discussion
BSS is a pathological state which is the outwardmanifestationof some certain pathological stage of various diseases Dueto lack of objective diagnosis criteria the essence of BSSis studied into the bottleneck stage Recently based onthe way of disease-syndrome combination much effective
Cont BSS Non-BSS0
2
1
Relat
ive e
xpre
ssio
n le
vel
lowast
lowast
Figure 2 The mRNA level of CD14+CD16+ monocyte subpopula-tion in leukocytes in CHDpatients with BSS by qRT-PCR lowast119875 lt 001compared to the control group Results were presented as mean plusmnSD
exploration of the essence of BSS was the foundation of BSSobjective diagnosis criteria construction During the past 50years we found a correlation between CHD with BSS andinflammatory hemodynamics platelet andmicrocirculation[11]
Atherosclerosis a chronic inflammatory immune stateis chiefly responsible for the development of CHD Variousleukocytes have been shown to influence atherogenesisMonocytes and their descendant macrophages are centralprotagonists in the development of atherosclerosis [12]Monocyte migration to the vessel wall is an initial event inthe growth of atherosclerotic lesions [13] Once monocytesare activated adhesion to endothelial cells was inducedby the transform of phenotype which led to myocardiuminjury inducing the proinflammatory cytokines such as TNF-120572 and IL-1 synthesis to initiate the inflammatory cascadereaction and oxidative stress injury producing matrix met-alloproteinase (MMP) and releasing many media to induceplaque instability and even fracture [14 15] Thereforemonocytes played the key role in the chronic inflammation-immunoreaction of the arterial vessels In our study weinvestigated that there was no significant difference of mono-cyte count based on CBC count among CHD patients withBSS non-BSS and healthy control (Table 1) However thelevel of sCD14 which is the indicator of activated monocyte[16] was obviously increased in CHD patients with BSScompared to non-BSS and healthy control (Figure 1) Theincreased level of sCD14 in sera in CHD patients withBSS indicated monocytes activation To demonstrate thecorrelation between deregulated expression of CD14+CD16+monocyte subpopulation and pathogenesis of CHDwith BSSits mRNA expression at the leukocyte level was assessed Asshown in Figure 2 relative expression level of CD14+CD16+
4 Evidence-Based Complementary and Alternative Medicine
105
105
104
104
103
103
102
102
Cont BSS Non-BSS
CD16
-PE
105
104
103
102
CD16
-PE
105
104
103
102
CD16
-PE
CD14-FITC
105
104
103
102
CD14-FITC
105
104
103
102
CD14-FITC
(a)
P lt 001 P lt 005
Cont BSS Non-BSS
16
8
0
CD14
+CD
16+
mon
ocyt
e (
)
(b)
Figure 3The protein level of CD14+CD16+ monocyte subpopulation in CHD patients with BSS by FACS analysis (a) Representation data ofFACS analysis of CD14+CD16+monocyte subpopulationWhole peripheral blood samples from patients and healthy individuals were stainedwith FITC-conjugated anti-CD14 antibody and PE-conjugated anti-CD16 antibody followed by FACS (b) The percentage of CD14+CD16+monocoyte subpopulation in the whole CD14-positive cells Results were presented as mean plusmn SD
monocyte subpopulation in both CHD patients with BSS andnon-BBS was largely increased by 99 and 77 respectivelycompared to the healthy control (119875 lt 001) However therewas no significant difference of this relative expression levelbetween CHDpatients with BSS and non-BSS (Figure 2)Theexpression of biological traits was controlled by gene andthe biological traits were reflected by protein To investigatewhether or not the expression change of CD14+CD16+mono-cyte subpopulation in both CHD patients with BSS and non-BSS at its protein level therefore we further analyzed theprotein level of CD14+CD16+ on monocyte member using2-color immunofluorescent staining (Figure 3(a)) The FACSresults showed that the protein level of CD14+CD16+ onmonocyte member was significantly increased in the CHDpatients with BSS when compared to the CHD patients withnon-BSS and the healthy control (119875 lt 001 or 119875 lt 005Figure 3(b))
TNF-120572 is one of the cytokines with various biologicalactivation and one previous study confirms that increasedlevel of TNF-120572 was existed in the monocytemacrophagesmooth muscle cells and endothelial cells in the atheroscle-rotic plaque and this high level was correlated to theseverity of atherosclerosis [17] IL-1 was released by activemonocytemacrophage which induced the releasing of manycytokines and growth factors by monocytemacrophage andthe expression of adhesion molecules such as ICAM-1 Addi-tionally IL-1 could stimulate vascular endothelium to pro-duce many inflammatory factors such as TNF-120572 aggravatedlocal inflammatory reaction and promote the developmentof atherosclerosis [18 19] Additionally previous studiesindicated that the circulation of CD14+CD16+ monocytescould spontaneously produce TNF and IL-1 [20] which couldprovoke cell proliferation and migration of smooth musclecells and macrophages in the atherosclerotic plaque [21]
Evidence-Based Complementary and Alternative Medicine 5
TNF-120572
lowast
lowast
lowast
lowast
IL-1
Cont BSS Non-BSS
Cyto
kine
cont
ent (
pgm
L)
120
60
0
Figure 4The changes of inflammatory cytokines of TNF-120572 and IL-1 in sera in CHD patients with BSS lowast119875 lt 001 compared to thecontrol group 119875 lt 005 compared to the CHD patients with non-BSS Results were presented as mean plusmn SD
Therefore protein level of TNF-120572 and IL-1 in sera was alsoassessed in our study by ELISA The significant increasedserum of TNF-120572 and IL-1 level was observed in CHD patientswith BSS and non-BSS compared to the healthy control (119875 lt001 Figure 4) and the level of TNF-120572 and IL-1 in CHDpatients with BSSwasmuch higher than that in CHDpatientswith non-BSS (119875 lt 005 Figure 4)
In the current study we investigated that there weremonocyte activation and an increased CD14+CD16+ mono-cyte subpopulation at protein level and its downstreaminflammatory cytokines such as TNF-120572 and IL-1 in sera inCHD patients with BSS Herein we presumed that monocyteactivation in the CHD patient with BSS induced the phe-notype of monocyte member transforming to CD14+CD16+monocyte subpopulation which was involved in the patho-genesis of CHD with BSS
4 Conclusion
Overall the present work confirmed the correlation betweenincreased CD14+CD16+ monocyte subpopulation at proteinlevel and CHD patients with based on the way of disease-syndrome combination Thus the increased CD14+CD16+monocyte subpopulation and its downstream inflamma-tory cytokines in CHD patient with BSS indicated thatCD14+CD16+ monocyte subpopulation was one of the sen-sitive markers in the pathogenesis of CHD with BSS
Authorsrsquo Contribution
Ye Huang and Jingshang Wang contributed equally to thiswork
Acknowledgments
This work was supported by the Chinese National KeyBasic Research and Development Program under Grantno 81073086 and the Major Research Plan of the ChineseNational Key Basic Research amp Development Program underGrant no 90409021 The authors thank Dr Xin Chen andHua Chen the for assistance with CHD patient selectionDr Changgeng Fu for assistance with CHD patient withBSS selection and Dr Yonggang Xu for assistance with flowcytometric analysis
References
[1] Y Liu H-J Yin D-Z Shi and K-J Chen ldquoChinese herb andformulas for promoting blood circulation and removing bloodstasis and antiplatelet therapiesrdquo Evidence-Based Complemen-tary and Alternative Medicine vol 2012 Article ID 184503 8pages 2012
[2] X-JMaH-J Yin andK-J Chen ldquoDifferential gene expressionprofiles in coronary heart disease patients of blood stasissyndrome in traditional Chinese medicine and clinical role oftarget generdquo Chinese Journal of Integrative Medicine vol 15 no2 pp 101ndash106 2009
[3] Y Huang H-J Yin J-S Wang X-J Ma Y Zhang and K-JChen ldquoThe significant increase of Fc120574RIIIA (CD16) a sensitivemarker in patients with coronary heart diseaserdquoGene vol 504no 2 pp 284ndash287 2012
[4] Y Huang H-J Yin J-S Wang Q Liu C-F Wu and K-JChen ldquoAberrant expression of Fc120574RIIIA (CD16) contributes tothe development of atherosclerosisrdquo Gene vol 498 no 1 pp91ndash95 2012
[5] Y Huang H-J Yin X-J Ma et al ldquoCorrelation betweenFc120574RIII a and aortic atherosclerotic plaque destabilizationin ApoE knockout mice and intervention effects of effectivecomponents of Chuanxiong Rhizome and Red Peony RootrdquoChinese Journal of Integrative Medicine vol 17 no 5 pp 355ndash360 2011
[6] E Braunwald E M Antman J W Beasley et al ldquoACCAHA2002 guideline update for the management of patients withunstable angina and non-ST-segment elevation myocardialinfarctionmdashsummary article a report of the American Collegeof CardiologyAmericanHeart Association Task Force on Prac-tice Guidelines (committee on themanagement of patients withunstable angina)rdquo Journal of the American College of Cardiologyvol 40 no 7 pp 1366ndash1374 2002
[7] R J Gibbons K Chatterjee J Daley et al ldquoACCAHAACP-ASIM guidelines for the management of patients with chronicstable angina executive summary and recommendations Areport of the American College of CardiologyAmerican HeartAssociation task force on practice guidelines (committee onmanagement of patients with chronic stable angina)rdquo Circula-tion vol 99 no 21 pp 2829ndash2848 1999
[8] Society of Cardiology Chinese Association of the IntegrativeMedicine ldquoThe diagnostic criteria of Chinesemedicine in coro-nary heart diseaserdquoChinese Journal of Integrated Traditional andWestern Medicine vol 11 p 257 1991
[9] J P P Meijerink C Mandigers L Van De Locht E TonnissenFGoodsaid and J Raemaekers ldquoAnovelmethod to compensatefor different amplification efficiencies between patient DNAsamples in quantitative real-time PCRrdquo Journal of MolecularDiagnostics vol 3 no 2 pp 55ndash61 2001
6 Evidence-Based Complementary and Alternative Medicine
[10] T Gremmel C W Kopp D Seidinger et al ldquoThe formationofmonocyte-platelet aggregates is independent of on-treatmentresidual agonistsrsquo-inducible platelet reactivityrdquo Atherosclerosisvol 207 no 2 pp 608ndash613 2009
[11] K-J Chen ldquoExploration on the possibility of reducing cardio-vascular risk by treatment with Chinese medicine recipes forpromoting blood-circulation and relieving blood-stasisrdquo ZhongGuo Zhong Xi Yi Jie He Za Zhi vol 28 no 5 p 389 2008
[12] M J Pittet and F K Swirski ldquoMonocytes link atherosclerosisand cancerrdquo European Journal of Immunology vol 41 no 9 pp2519ndash2522 2011
[13] K JWoollard and FGeissmann ldquoMonocytes in atherosclerosissubsets and functionsrdquo Nature Reviews Cardiology vol 7 no 2pp 77ndash86 2010
[14] B Pamukcu G Y H Lip A Devitt H Griffiths and EShantsila ldquoThe role of monocytes in atherosclerotic coronaryartery diseaserdquo Annals of Medicine vol 42 no 6 pp 394ndash4032010
[15] P Saha B Modarai J Humphries et al ldquoThemonocytemacro-phage as a therapeutic target in atherosclerosisrdquo Current Opin-ion in Pharmacology vol 9 no 2 pp 109ndash118 2009
[16] C Kruger C Schutt U Obertacke et al ldquoSerum CD14 levelsin polytraumatized and severely burned patientsrdquo Clinical andExperimental Immunology vol 85 no 2 pp 297ndash301 1991
[17] P Barath M C Fishbein J Cao J Berenson R H Helfantand J S Forrester ldquoDetection and localization of tumor necrosisfactor in human atheromardquoAmerican Journal of Cardiology vol65 no 5 pp 297ndash302 1990
[18] F Merhi-Soussi B R Kwak D Magne et al ldquoInterleukin-1plays a major role in vascular inflammation and atherosclero-sis in male apolipoprotein E-knockout micerdquo CardiovascularResearch vol 66 no 3 pp 583ndash593 2005
[19] K Isoda S Sawada N Ishigami et al ldquoLack of interleukin-1 receptor antagonist modulates plaque composition inapolipoprotein E-deficient micerdquo Arteriosclerosis Thrombosisand Vascular Biology vol 24 no 6 pp 1068ndash1073 2004
[20] M Frankenberger T Sternsdorf H Pechumer A Pforte andH W L Ziegler-Heitbrock ldquoDifferential cytokine expressionin human blood monocyte subpopulations a polymerase chainreaction analysisrdquo Blood vol 87 no 1 pp 373ndash377 1996
[21] N de Bont M G Netea C Rovers et al ldquoLPS-inducedrelease of IL-1120573 IL-1Ra IL-6 and TNF-120572 in whole bloodfrom patients with familial hypercholesterolemia no effectof cholesterol-lowering treatmentrdquo Journal of Interferon andCytokine Research vol 26 no 2 pp 101ndash107 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
4 Evidence-Based Complementary and Alternative Medicine
105
105
104
104
103
103
102
102
Cont BSS Non-BSS
CD16
-PE
105
104
103
102
CD16
-PE
105
104
103
102
CD16
-PE
CD14-FITC
105
104
103
102
CD14-FITC
105
104
103
102
CD14-FITC
(a)
P lt 001 P lt 005
Cont BSS Non-BSS
16
8
0
CD14
+CD
16+
mon
ocyt
e (
)
(b)
Figure 3The protein level of CD14+CD16+ monocyte subpopulation in CHD patients with BSS by FACS analysis (a) Representation data ofFACS analysis of CD14+CD16+monocyte subpopulationWhole peripheral blood samples from patients and healthy individuals were stainedwith FITC-conjugated anti-CD14 antibody and PE-conjugated anti-CD16 antibody followed by FACS (b) The percentage of CD14+CD16+monocoyte subpopulation in the whole CD14-positive cells Results were presented as mean plusmn SD
monocyte subpopulation in both CHD patients with BSS andnon-BBS was largely increased by 99 and 77 respectivelycompared to the healthy control (119875 lt 001) However therewas no significant difference of this relative expression levelbetween CHDpatients with BSS and non-BSS (Figure 2)Theexpression of biological traits was controlled by gene andthe biological traits were reflected by protein To investigatewhether or not the expression change of CD14+CD16+mono-cyte subpopulation in both CHD patients with BSS and non-BSS at its protein level therefore we further analyzed theprotein level of CD14+CD16+ on monocyte member using2-color immunofluorescent staining (Figure 3(a)) The FACSresults showed that the protein level of CD14+CD16+ onmonocyte member was significantly increased in the CHDpatients with BSS when compared to the CHD patients withnon-BSS and the healthy control (119875 lt 001 or 119875 lt 005Figure 3(b))
TNF-120572 is one of the cytokines with various biologicalactivation and one previous study confirms that increasedlevel of TNF-120572 was existed in the monocytemacrophagesmooth muscle cells and endothelial cells in the atheroscle-rotic plaque and this high level was correlated to theseverity of atherosclerosis [17] IL-1 was released by activemonocytemacrophage which induced the releasing of manycytokines and growth factors by monocytemacrophage andthe expression of adhesion molecules such as ICAM-1 Addi-tionally IL-1 could stimulate vascular endothelium to pro-duce many inflammatory factors such as TNF-120572 aggravatedlocal inflammatory reaction and promote the developmentof atherosclerosis [18 19] Additionally previous studiesindicated that the circulation of CD14+CD16+ monocytescould spontaneously produce TNF and IL-1 [20] which couldprovoke cell proliferation and migration of smooth musclecells and macrophages in the atherosclerotic plaque [21]
Evidence-Based Complementary and Alternative Medicine 5
TNF-120572
lowast
lowast
lowast
lowast
IL-1
Cont BSS Non-BSS
Cyto
kine
cont
ent (
pgm
L)
120
60
0
Figure 4The changes of inflammatory cytokines of TNF-120572 and IL-1 in sera in CHD patients with BSS lowast119875 lt 001 compared to thecontrol group 119875 lt 005 compared to the CHD patients with non-BSS Results were presented as mean plusmn SD
Therefore protein level of TNF-120572 and IL-1 in sera was alsoassessed in our study by ELISA The significant increasedserum of TNF-120572 and IL-1 level was observed in CHD patientswith BSS and non-BSS compared to the healthy control (119875 lt001 Figure 4) and the level of TNF-120572 and IL-1 in CHDpatients with BSSwasmuch higher than that in CHDpatientswith non-BSS (119875 lt 005 Figure 4)
In the current study we investigated that there weremonocyte activation and an increased CD14+CD16+ mono-cyte subpopulation at protein level and its downstreaminflammatory cytokines such as TNF-120572 and IL-1 in sera inCHD patients with BSS Herein we presumed that monocyteactivation in the CHD patient with BSS induced the phe-notype of monocyte member transforming to CD14+CD16+monocyte subpopulation which was involved in the patho-genesis of CHD with BSS
4 Conclusion
Overall the present work confirmed the correlation betweenincreased CD14+CD16+ monocyte subpopulation at proteinlevel and CHD patients with based on the way of disease-syndrome combination Thus the increased CD14+CD16+monocyte subpopulation and its downstream inflamma-tory cytokines in CHD patient with BSS indicated thatCD14+CD16+ monocyte subpopulation was one of the sen-sitive markers in the pathogenesis of CHD with BSS
Authorsrsquo Contribution
Ye Huang and Jingshang Wang contributed equally to thiswork
Acknowledgments
This work was supported by the Chinese National KeyBasic Research and Development Program under Grantno 81073086 and the Major Research Plan of the ChineseNational Key Basic Research amp Development Program underGrant no 90409021 The authors thank Dr Xin Chen andHua Chen the for assistance with CHD patient selectionDr Changgeng Fu for assistance with CHD patient withBSS selection and Dr Yonggang Xu for assistance with flowcytometric analysis
References
[1] Y Liu H-J Yin D-Z Shi and K-J Chen ldquoChinese herb andformulas for promoting blood circulation and removing bloodstasis and antiplatelet therapiesrdquo Evidence-Based Complemen-tary and Alternative Medicine vol 2012 Article ID 184503 8pages 2012
[2] X-JMaH-J Yin andK-J Chen ldquoDifferential gene expressionprofiles in coronary heart disease patients of blood stasissyndrome in traditional Chinese medicine and clinical role oftarget generdquo Chinese Journal of Integrative Medicine vol 15 no2 pp 101ndash106 2009
[3] Y Huang H-J Yin J-S Wang X-J Ma Y Zhang and K-JChen ldquoThe significant increase of Fc120574RIIIA (CD16) a sensitivemarker in patients with coronary heart diseaserdquoGene vol 504no 2 pp 284ndash287 2012
[4] Y Huang H-J Yin J-S Wang Q Liu C-F Wu and K-JChen ldquoAberrant expression of Fc120574RIIIA (CD16) contributes tothe development of atherosclerosisrdquo Gene vol 498 no 1 pp91ndash95 2012
[5] Y Huang H-J Yin X-J Ma et al ldquoCorrelation betweenFc120574RIII a and aortic atherosclerotic plaque destabilizationin ApoE knockout mice and intervention effects of effectivecomponents of Chuanxiong Rhizome and Red Peony RootrdquoChinese Journal of Integrative Medicine vol 17 no 5 pp 355ndash360 2011
[6] E Braunwald E M Antman J W Beasley et al ldquoACCAHA2002 guideline update for the management of patients withunstable angina and non-ST-segment elevation myocardialinfarctionmdashsummary article a report of the American Collegeof CardiologyAmericanHeart Association Task Force on Prac-tice Guidelines (committee on themanagement of patients withunstable angina)rdquo Journal of the American College of Cardiologyvol 40 no 7 pp 1366ndash1374 2002
[7] R J Gibbons K Chatterjee J Daley et al ldquoACCAHAACP-ASIM guidelines for the management of patients with chronicstable angina executive summary and recommendations Areport of the American College of CardiologyAmerican HeartAssociation task force on practice guidelines (committee onmanagement of patients with chronic stable angina)rdquo Circula-tion vol 99 no 21 pp 2829ndash2848 1999
[8] Society of Cardiology Chinese Association of the IntegrativeMedicine ldquoThe diagnostic criteria of Chinesemedicine in coro-nary heart diseaserdquoChinese Journal of Integrated Traditional andWestern Medicine vol 11 p 257 1991
[9] J P P Meijerink C Mandigers L Van De Locht E TonnissenFGoodsaid and J Raemaekers ldquoAnovelmethod to compensatefor different amplification efficiencies between patient DNAsamples in quantitative real-time PCRrdquo Journal of MolecularDiagnostics vol 3 no 2 pp 55ndash61 2001
6 Evidence-Based Complementary and Alternative Medicine
[10] T Gremmel C W Kopp D Seidinger et al ldquoThe formationofmonocyte-platelet aggregates is independent of on-treatmentresidual agonistsrsquo-inducible platelet reactivityrdquo Atherosclerosisvol 207 no 2 pp 608ndash613 2009
[11] K-J Chen ldquoExploration on the possibility of reducing cardio-vascular risk by treatment with Chinese medicine recipes forpromoting blood-circulation and relieving blood-stasisrdquo ZhongGuo Zhong Xi Yi Jie He Za Zhi vol 28 no 5 p 389 2008
[12] M J Pittet and F K Swirski ldquoMonocytes link atherosclerosisand cancerrdquo European Journal of Immunology vol 41 no 9 pp2519ndash2522 2011
[13] K JWoollard and FGeissmann ldquoMonocytes in atherosclerosissubsets and functionsrdquo Nature Reviews Cardiology vol 7 no 2pp 77ndash86 2010
[14] B Pamukcu G Y H Lip A Devitt H Griffiths and EShantsila ldquoThe role of monocytes in atherosclerotic coronaryartery diseaserdquo Annals of Medicine vol 42 no 6 pp 394ndash4032010
[15] P Saha B Modarai J Humphries et al ldquoThemonocytemacro-phage as a therapeutic target in atherosclerosisrdquo Current Opin-ion in Pharmacology vol 9 no 2 pp 109ndash118 2009
[16] C Kruger C Schutt U Obertacke et al ldquoSerum CD14 levelsin polytraumatized and severely burned patientsrdquo Clinical andExperimental Immunology vol 85 no 2 pp 297ndash301 1991
[17] P Barath M C Fishbein J Cao J Berenson R H Helfantand J S Forrester ldquoDetection and localization of tumor necrosisfactor in human atheromardquoAmerican Journal of Cardiology vol65 no 5 pp 297ndash302 1990
[18] F Merhi-Soussi B R Kwak D Magne et al ldquoInterleukin-1plays a major role in vascular inflammation and atherosclero-sis in male apolipoprotein E-knockout micerdquo CardiovascularResearch vol 66 no 3 pp 583ndash593 2005
[19] K Isoda S Sawada N Ishigami et al ldquoLack of interleukin-1 receptor antagonist modulates plaque composition inapolipoprotein E-deficient micerdquo Arteriosclerosis Thrombosisand Vascular Biology vol 24 no 6 pp 1068ndash1073 2004
[20] M Frankenberger T Sternsdorf H Pechumer A Pforte andH W L Ziegler-Heitbrock ldquoDifferential cytokine expressionin human blood monocyte subpopulations a polymerase chainreaction analysisrdquo Blood vol 87 no 1 pp 373ndash377 1996
[21] N de Bont M G Netea C Rovers et al ldquoLPS-inducedrelease of IL-1120573 IL-1Ra IL-6 and TNF-120572 in whole bloodfrom patients with familial hypercholesterolemia no effectof cholesterol-lowering treatmentrdquo Journal of Interferon andCytokine Research vol 26 no 2 pp 101ndash107 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Evidence-Based Complementary and Alternative Medicine 5
TNF-120572
lowast
lowast
lowast
lowast
IL-1
Cont BSS Non-BSS
Cyto
kine
cont
ent (
pgm
L)
120
60
0
Figure 4The changes of inflammatory cytokines of TNF-120572 and IL-1 in sera in CHD patients with BSS lowast119875 lt 001 compared to thecontrol group 119875 lt 005 compared to the CHD patients with non-BSS Results were presented as mean plusmn SD
Therefore protein level of TNF-120572 and IL-1 in sera was alsoassessed in our study by ELISA The significant increasedserum of TNF-120572 and IL-1 level was observed in CHD patientswith BSS and non-BSS compared to the healthy control (119875 lt001 Figure 4) and the level of TNF-120572 and IL-1 in CHDpatients with BSSwasmuch higher than that in CHDpatientswith non-BSS (119875 lt 005 Figure 4)
In the current study we investigated that there weremonocyte activation and an increased CD14+CD16+ mono-cyte subpopulation at protein level and its downstreaminflammatory cytokines such as TNF-120572 and IL-1 in sera inCHD patients with BSS Herein we presumed that monocyteactivation in the CHD patient with BSS induced the phe-notype of monocyte member transforming to CD14+CD16+monocyte subpopulation which was involved in the patho-genesis of CHD with BSS
4 Conclusion
Overall the present work confirmed the correlation betweenincreased CD14+CD16+ monocyte subpopulation at proteinlevel and CHD patients with based on the way of disease-syndrome combination Thus the increased CD14+CD16+monocyte subpopulation and its downstream inflamma-tory cytokines in CHD patient with BSS indicated thatCD14+CD16+ monocyte subpopulation was one of the sen-sitive markers in the pathogenesis of CHD with BSS
Authorsrsquo Contribution
Ye Huang and Jingshang Wang contributed equally to thiswork
Acknowledgments
This work was supported by the Chinese National KeyBasic Research and Development Program under Grantno 81073086 and the Major Research Plan of the ChineseNational Key Basic Research amp Development Program underGrant no 90409021 The authors thank Dr Xin Chen andHua Chen the for assistance with CHD patient selectionDr Changgeng Fu for assistance with CHD patient withBSS selection and Dr Yonggang Xu for assistance with flowcytometric analysis
References
[1] Y Liu H-J Yin D-Z Shi and K-J Chen ldquoChinese herb andformulas for promoting blood circulation and removing bloodstasis and antiplatelet therapiesrdquo Evidence-Based Complemen-tary and Alternative Medicine vol 2012 Article ID 184503 8pages 2012
[2] X-JMaH-J Yin andK-J Chen ldquoDifferential gene expressionprofiles in coronary heart disease patients of blood stasissyndrome in traditional Chinese medicine and clinical role oftarget generdquo Chinese Journal of Integrative Medicine vol 15 no2 pp 101ndash106 2009
[3] Y Huang H-J Yin J-S Wang X-J Ma Y Zhang and K-JChen ldquoThe significant increase of Fc120574RIIIA (CD16) a sensitivemarker in patients with coronary heart diseaserdquoGene vol 504no 2 pp 284ndash287 2012
[4] Y Huang H-J Yin J-S Wang Q Liu C-F Wu and K-JChen ldquoAberrant expression of Fc120574RIIIA (CD16) contributes tothe development of atherosclerosisrdquo Gene vol 498 no 1 pp91ndash95 2012
[5] Y Huang H-J Yin X-J Ma et al ldquoCorrelation betweenFc120574RIII a and aortic atherosclerotic plaque destabilizationin ApoE knockout mice and intervention effects of effectivecomponents of Chuanxiong Rhizome and Red Peony RootrdquoChinese Journal of Integrative Medicine vol 17 no 5 pp 355ndash360 2011
[6] E Braunwald E M Antman J W Beasley et al ldquoACCAHA2002 guideline update for the management of patients withunstable angina and non-ST-segment elevation myocardialinfarctionmdashsummary article a report of the American Collegeof CardiologyAmericanHeart Association Task Force on Prac-tice Guidelines (committee on themanagement of patients withunstable angina)rdquo Journal of the American College of Cardiologyvol 40 no 7 pp 1366ndash1374 2002
[7] R J Gibbons K Chatterjee J Daley et al ldquoACCAHAACP-ASIM guidelines for the management of patients with chronicstable angina executive summary and recommendations Areport of the American College of CardiologyAmerican HeartAssociation task force on practice guidelines (committee onmanagement of patients with chronic stable angina)rdquo Circula-tion vol 99 no 21 pp 2829ndash2848 1999
[8] Society of Cardiology Chinese Association of the IntegrativeMedicine ldquoThe diagnostic criteria of Chinesemedicine in coro-nary heart diseaserdquoChinese Journal of Integrated Traditional andWestern Medicine vol 11 p 257 1991
[9] J P P Meijerink C Mandigers L Van De Locht E TonnissenFGoodsaid and J Raemaekers ldquoAnovelmethod to compensatefor different amplification efficiencies between patient DNAsamples in quantitative real-time PCRrdquo Journal of MolecularDiagnostics vol 3 no 2 pp 55ndash61 2001
6 Evidence-Based Complementary and Alternative Medicine
[10] T Gremmel C W Kopp D Seidinger et al ldquoThe formationofmonocyte-platelet aggregates is independent of on-treatmentresidual agonistsrsquo-inducible platelet reactivityrdquo Atherosclerosisvol 207 no 2 pp 608ndash613 2009
[11] K-J Chen ldquoExploration on the possibility of reducing cardio-vascular risk by treatment with Chinese medicine recipes forpromoting blood-circulation and relieving blood-stasisrdquo ZhongGuo Zhong Xi Yi Jie He Za Zhi vol 28 no 5 p 389 2008
[12] M J Pittet and F K Swirski ldquoMonocytes link atherosclerosisand cancerrdquo European Journal of Immunology vol 41 no 9 pp2519ndash2522 2011
[13] K JWoollard and FGeissmann ldquoMonocytes in atherosclerosissubsets and functionsrdquo Nature Reviews Cardiology vol 7 no 2pp 77ndash86 2010
[14] B Pamukcu G Y H Lip A Devitt H Griffiths and EShantsila ldquoThe role of monocytes in atherosclerotic coronaryartery diseaserdquo Annals of Medicine vol 42 no 6 pp 394ndash4032010
[15] P Saha B Modarai J Humphries et al ldquoThemonocytemacro-phage as a therapeutic target in atherosclerosisrdquo Current Opin-ion in Pharmacology vol 9 no 2 pp 109ndash118 2009
[16] C Kruger C Schutt U Obertacke et al ldquoSerum CD14 levelsin polytraumatized and severely burned patientsrdquo Clinical andExperimental Immunology vol 85 no 2 pp 297ndash301 1991
[17] P Barath M C Fishbein J Cao J Berenson R H Helfantand J S Forrester ldquoDetection and localization of tumor necrosisfactor in human atheromardquoAmerican Journal of Cardiology vol65 no 5 pp 297ndash302 1990
[18] F Merhi-Soussi B R Kwak D Magne et al ldquoInterleukin-1plays a major role in vascular inflammation and atherosclero-sis in male apolipoprotein E-knockout micerdquo CardiovascularResearch vol 66 no 3 pp 583ndash593 2005
[19] K Isoda S Sawada N Ishigami et al ldquoLack of interleukin-1 receptor antagonist modulates plaque composition inapolipoprotein E-deficient micerdquo Arteriosclerosis Thrombosisand Vascular Biology vol 24 no 6 pp 1068ndash1073 2004
[20] M Frankenberger T Sternsdorf H Pechumer A Pforte andH W L Ziegler-Heitbrock ldquoDifferential cytokine expressionin human blood monocyte subpopulations a polymerase chainreaction analysisrdquo Blood vol 87 no 1 pp 373ndash377 1996
[21] N de Bont M G Netea C Rovers et al ldquoLPS-inducedrelease of IL-1120573 IL-1Ra IL-6 and TNF-120572 in whole bloodfrom patients with familial hypercholesterolemia no effectof cholesterol-lowering treatmentrdquo Journal of Interferon andCytokine Research vol 26 no 2 pp 101ndash107 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 Evidence-Based Complementary and Alternative Medicine
[10] T Gremmel C W Kopp D Seidinger et al ldquoThe formationofmonocyte-platelet aggregates is independent of on-treatmentresidual agonistsrsquo-inducible platelet reactivityrdquo Atherosclerosisvol 207 no 2 pp 608ndash613 2009
[11] K-J Chen ldquoExploration on the possibility of reducing cardio-vascular risk by treatment with Chinese medicine recipes forpromoting blood-circulation and relieving blood-stasisrdquo ZhongGuo Zhong Xi Yi Jie He Za Zhi vol 28 no 5 p 389 2008
[12] M J Pittet and F K Swirski ldquoMonocytes link atherosclerosisand cancerrdquo European Journal of Immunology vol 41 no 9 pp2519ndash2522 2011
[13] K JWoollard and FGeissmann ldquoMonocytes in atherosclerosissubsets and functionsrdquo Nature Reviews Cardiology vol 7 no 2pp 77ndash86 2010
[14] B Pamukcu G Y H Lip A Devitt H Griffiths and EShantsila ldquoThe role of monocytes in atherosclerotic coronaryartery diseaserdquo Annals of Medicine vol 42 no 6 pp 394ndash4032010
[15] P Saha B Modarai J Humphries et al ldquoThemonocytemacro-phage as a therapeutic target in atherosclerosisrdquo Current Opin-ion in Pharmacology vol 9 no 2 pp 109ndash118 2009
[16] C Kruger C Schutt U Obertacke et al ldquoSerum CD14 levelsin polytraumatized and severely burned patientsrdquo Clinical andExperimental Immunology vol 85 no 2 pp 297ndash301 1991
[17] P Barath M C Fishbein J Cao J Berenson R H Helfantand J S Forrester ldquoDetection and localization of tumor necrosisfactor in human atheromardquoAmerican Journal of Cardiology vol65 no 5 pp 297ndash302 1990
[18] F Merhi-Soussi B R Kwak D Magne et al ldquoInterleukin-1plays a major role in vascular inflammation and atherosclero-sis in male apolipoprotein E-knockout micerdquo CardiovascularResearch vol 66 no 3 pp 583ndash593 2005
[19] K Isoda S Sawada N Ishigami et al ldquoLack of interleukin-1 receptor antagonist modulates plaque composition inapolipoprotein E-deficient micerdquo Arteriosclerosis Thrombosisand Vascular Biology vol 24 no 6 pp 1068ndash1073 2004
[20] M Frankenberger T Sternsdorf H Pechumer A Pforte andH W L Ziegler-Heitbrock ldquoDifferential cytokine expressionin human blood monocyte subpopulations a polymerase chainreaction analysisrdquo Blood vol 87 no 1 pp 373ndash377 1996
[21] N de Bont M G Netea C Rovers et al ldquoLPS-inducedrelease of IL-1120573 IL-1Ra IL-6 and TNF-120572 in whole bloodfrom patients with familial hypercholesterolemia no effectof cholesterol-lowering treatmentrdquo Journal of Interferon andCytokine Research vol 26 no 2 pp 101ndash107 2006
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom