oulu 2015 d 1303 university of oulu p.o. box 8000 fi...
TRANSCRIPT
UNIVERSITY OF OULU P .O. Box 8000 F I -90014 UNIVERSITY OF OULU FINLAND
A C T A U N I V E R S I T A T I S O U L U E N S I S
Professor Esa Hohtola
University Lecturer Santeri Palviainen
Postdoctoral research fellow Sanna Taskila
Professor Olli Vuolteenaho
University Lecturer Veli-Matti Ulvinen
Director Sinikka Eskelinen
Professor Jari Juga
University Lecturer Anu Soikkeli
Professor Olli Vuolteenaho
Publications Editor Kirsti Nurkkala
ISBN 978-952-62-0854-1 (Paperback)ISBN 978-952-62-0855-8 (PDF)ISSN 0355-3221 (Print)ISSN 1796-2234 (Online)
U N I V E R S I TAT I S O U L U E N S I S
MEDICA
ACTAD
D 1303
ACTA
Tarja Tanner
OULU 2015
D 1303
Tarja Tanner
HEALTHY YOUNG ADULTS' ORAL HEALTH AND ASSOCIATED FACTORSCROSS-SECTIONAL EPIDEMIOLOGICAL STUDY
UNIVERSITY OF OULU GRADUATE SCHOOL;UNIVERSITY OF OULU,FACULTY OF MEDICINE;MEDICAL RESEARCH CENTER OULU;OULU UNIVERSITY HOSPITAL;FINNISH DOCTORAL PROGRAM IN ORAL SCIENCES FINDOS


A C T A U N I V E R S I T A T I S O U L U E N S I SD M e d i c a 1 3 0 3
TARJA TANNER
HEALTHY YOUNG ADULTS' ORAL HEALTH AND ASSOCIATED FACTORSCross-sectional epidemiological study
Academic dissertation to be presented with the assent ofthe Doctora l Train ing Committee of Health andBiosciences of the University of Oulu for public defence inthe Leena Palotie auditorium (101A) of the Faculty ofMedicine (Aapistie 5 A), on 19 August 2015, at 12 noon
UNIVERSITY OF OULU, OULU 2015

Copyright © 2015Acta Univ. Oul. D 1303, 2015
Supervised byDocent Vuokko AnttonenProfessor Leo TjäderhaneDoctor Pertti Patinen
Reviewed byDocent Sisko HonkalaProfessor Dowen Birkhed
ISBN 978-952-62-0854-1 (Paperback)ISBN 978-952-62-0855-8 (PDF)
ISSN 0355-3221 (Printed)ISSN 1796-2234 (Online)
Cover DesignRaimo Ahonen
JUVENES PRINTTAMPERE 2015
OpponentProfessor Liisa Suominen

Tanner, Tarja, Healthy young adults' oral health and associated factors. Cross-sectional epidemiological studyUniversity of Oulu Graduate School; University of Oulu, Faculty of Medicine; MedicalResearch Center Oulu; Oulu University Hospital; Finnish Doctoral Program in Oral SciencesFINDOSActa Univ. Oul. D 1303, 2015University of Oulu, P.O. Box 8000, FI-90014 University of Oulu, Finland
Abstract
The aim of this epidemiological study was to investigate the oral health situation and associatedfactors among a group of Finnish healthy males born in the early 1990s.
A pilot study was carried out in two garrisons of the Finnish Defence Forces in July 2010 toevaluate and time the various parts of the protocol (n = 256 men and women). In the main study,oral health of 13,564 men and 255 women who entered the military service in 2011 was screenedfor restorative treatment need (DT), dental history (DMFT) and periodontal status (CPI and BOP).In this cross-sectional study, a representative sample of the entire group of draftees in 2011 wasachieved by examining all conscripts in 15 out of 20 garrisons and every fifth conscript inalphabetical order randomising the subjects in the five largest garrisons. Also 8,539 men answereda questionnaire covering their smoking and snuffing habits and alcohol use as well as otherbehaviour and background factors. BOP was available on 6,596 conscripts.
The findings suggested stagnation in the improvement or even deterioration of the caries statusin young healthy males. Among the study group of young male adults, caries burden waspolarised, mainly due to primary caries. Prevalence of smoking was alarmingly high (39.6%).Smoking significantly increased the odds for restorative treatment need, high BOP or high CPI andwas associated with other behaviour related to poor health. Snuffing and alcohol use were notassociated with caries prevalence, BOP and CPI in the study group. The importance of the placeof residence to caries experience was evident, but the impact decreased when health behaviourswere included in the statistical analyses. Sociodemographic factors were associated with oralhealth among young men. In conclusion, health behaviour of young Finnish males does notsupport good oral health, and therefore caries control continues to be a challenge. Both healthbehaviours and environmental factors are associated with oral health, which should be consideredin oral health promotion.
Keywords: alcohol use, dental caries, epidemiology, health behaviour, periodontalinfection, smoking, snuffing, sociodemographic factors, socioeconomic factors, youngadults


Tanner, Tarja, Terveiden nuorten aikuisten suun terveys ja siihen liittyvät tekijät.Epidemiologinen poikkileikkaustutkimusOulun yliopiston tutkijakoulu; Oulun yliopisto, Lääketieteellinen tiedekunta; Medical ResearchCenter Oulu; Oulun yliopistollinen sairaala; Suun terveystieteiden tohtoriohjelma FINDOSActa Univ. Oul. D 1303, 2015Oulun yliopisto, PL 8000, 90014 Oulun yliopisto
Tiivistelmä
Tämän epidemiologisen tutkimuksen tavoitteena oli tutkia 1990-luvulla syntyneiden perustervei-den suomalaisten nuorten miesten suun terveyden tilannetta ja siihen vaikuttavia taustatekijöitä.
Pilottitutkimuksessa heinäkuussa 2010 testattiin tutkimusprotokolla ja arvioitiin sen soveltu-vuus epidemiologiseen tutkimukseen. Pilottitutkimus tehtiin kahdessa Puolustusvoimien varus-kunnassa, ja siihen osallistui yhteensä 256 varusmiestä
Epidemiologinen tutkimus tehtiin tammikuussa ja heinäkuussa 2011 kahdessakymmenessävaruskunnassa. Kliininen tarkastus tehtiin kaikille alokkaille lukuun ottamatta viittä suurintavaruskuntaa, joissa tutkimukseen valittiin joka viides alokas. Tutkimukseen osallistui yhteensä13 564 miestä ja 255 naista. Heiltä selvitettiin korjaavan hoidon tarve (DT) ja hoidon historia(DMFT) sekä korkein parodontaalisen hoidon tarve indeksihampaista (CPI). Ikenien vuotoin-deksi (BOP) mitattiin 6 596 varusmieheltä. Kliinisen tarkastuksen lisäksi 8 539 varusmiestä vas-tasi kyselyyn, jolla selvitettiin muun muassa heidän tupakointi-, nuuskaus- ja alkoholinkäyttötot-tumuksiaan sekä muuta terveyskäyttäytymistä ja sosioekonomisia ja -demografisia taustatietoja.
Tulosten perusteella suomalaisten nuorten miesten kariologinen tilanne ei ole enää parantu-nut vaan jopa hieman huonontunut aiempiin tutkimuksiin verrattuna. Karieskertymä on pola-risoitunut tutkimusjoukossa, ja suurin osa löydöksistä oli uusia kariesleesioita. Varusmiehistäjopa 39,6 % tupakoi päivittäin. Tupakoinnin ja lisääntyneen kariologisen ja parodontaalisen hoi-don tarpeen sekä huonon terveyskäyttäytymisen välillä havaittiin yhteys. Nuuskaaminen ja alko-holin käyttö eivät vaikuttaneet todettuun kariologisen ja parodontaalisen hoidon tarpeeseen täs-sä tutkimuksessa.
Varusmiehen asuinpaikka vaikutti kariologisen hoidon tarpeeseen, mutta vaikutus väheni,kun terveyskäyttäytyminen otettiin analyyseihin mukaan. Myös varusmiehen omalla sekä hänenvanhempiensa koulutustaustalla oli vaikutusta nuorten miesten suun terveyteen.
Tutkimuksen perusteella voidaan sanoa, että suomalaisten nuorten miesten terveyskäyttäyty-minen ei tue hyvää suun terveyttä, jonka takia karieksen hallinta tulee olemaan haastavaa myöstulevaisuudessa. Sekä terveyskäyttäytyminen että ympäristö vaikututtavat suun terveyteen, mikäon tärkeä pitää mielessä terveyden edistämistyössä.
Asiasanat: alkoholin käyttö, epidemiologia, karies, nuoret aikuiset, nuuskaus,parodontaali-infektio, sosiodemografiset tekijät, sosioekonomiset tekijät,terveyskäyttäytyminen, tupakointi


To Emma, Anni and Toni

9
Acknowledgements This study was carried out at the Faculty of Medicine, Oral Health Sciences and Medical Research Center, Oulu University Hospital and University of Oulu and The Finnish Defence Forces, during the years 2010 to 2015. This research was carried out in co-operation with the Finnish Doctoral Program in Oral Sciences (FINDOS). This study period has been interesting and, most of all a learning experience.
I wish to express my deepest gratitude to my supervisors Docent Vuokko Anttonen D.D.S, Ph.D, Professor Leo Tjäderhane D.D.S, Ph.D. and Commander Pertti Patinen D.D.S, Ph.D. for guiding me throughout this process.
My main supervisor Docent Vuokko Anttonen has been the best supervisor who I ever could get. Her never-ending enthusiasm, optimism and constructive criticism have been essential driving forces in completing this work. During my student hood I could never believe to be scientist in some day. But when Vuokko introduced me the idea of study of conscripts, suddenly I wasn´t so sure my future plan anymore. Vuokko is such a supervisor which young research need. She opened even her home to offer facilities to our “science camps”. For that I would also like to offer my special thanks to Vuokko`s husband, Hannu.
I am grateful to Professor Leo Tjäderhane for his excellent guidance in scientific work and critical thinking. He is also an excellent writer and I have learned much about his detailed comments about my texts. I really appreciated his passionate attitude towards science.
I am grateful to Commander Pertti Patinen, Chief Dental Officer in Finnish Defence Forces who also made this research possible. I appreciate his personality and skills to showed value of this study which helped to get permission to do it in Finnish Defence Forces. He has maintained excellent relationships between university of Oulu and Finnish Defence Forces during the project. Also his valuable comments have made this research much better.
My re-examiners Docent Sisko Honkala and Professor Dowen Birked deserve acknowledgement for their careful revision, expert and reassuring comments. Mrs. Outi Hiltunen is acknowledged for the linguistic revision. I also thank the people in my follow-up group: Professor Kirsi Sipilä, Professor Pertti Pirttiniemi and Docent Tuomo Heikkinen.
The value of co-operation is immeasurable. I would like to offer my special thanks to Jari Päkkilä, MSc, for patiently guiding me through all the statistical dilemmas. I really appreciated his tireless efforts to give answers to my countless questions on SPSS. I would like to also thank my colleague Antti Kämppi, who has
10
shared the same pain and joy of PhD project as I. His energetic and enthusiastic personality has given me a lot of energy during the project. I would like to sincerely thank all of our experts, Professor Marjo-Riitta Järvelin, Periodontologist Kaisa Karjalainen, D.D.S, Ph.D, and Radiologist Jukka Rosberg D.D.S, for sharing their time and knowledge to this epidemiological study. To our great sorrow, Jukka passed away during the project. I want to own this book also to the memory of our dear colleague, Jukka.
I gratefully acknowledge the dental staff at the dental clinics of the Finnish Defense Forces for their enthusiasm and work in conducting the field survey, as well as the medical conscripts for their assistance. Especially I would like to thank Jukka Leinonen, D.D.S, Ph.D, who helped me to do oral examinations of conscripts in Jaeger Brigade in January 2011. I also want to express thanks to Mrs. Mari Saario at the Centre for Military Medicine, Finnish Defence Forces for her co-operation in collecting data. I am grateful to Mr. Matti Paadar for his work in getting the computers needed for the field survey and Dr. Ahti Niinimaa for his contribution in developing the computer program used in this study, and preparing the computers for delivery. I really appreciate the time and effort given by Mr. Juhani Vänttilä and Mr. Eino Kemppainen for delivering the computers to the garrisons in December 2010.
I thank all my siblings, relatives, friends and colleagues as well as my godchildren Miko, Reeta, Eino, Hilla, Helvi and Aaron for being part of my life. I wish to acknowledge the help provided by my uncle Esko. He has offered lodging to me and my family in Oulu every time we required it during my Ph.D. project. I wish to thank my parents, Lilja and Vesa, for good start to my life and imparting a positive attitude to study.
Last but foremost I wish to thank my family. Word of thanks is not enough for my beloved husband Toni whose never-ending support, encouragement and love mean everything to me. I remember very well when my Ph.D project started because in the same autumn you married me. That day and ever since were unique days with you. I loved to be a parent with you to our amazing girls, Anni and Emma. Their searing criticism and unconditional love is confusing me every day. You, you do I love.
This study was support financially by Finnish Doctoral Program in Oral Sciences, FINDOS; an EVO grand form the University of Oulu, foundation of Emil Aaltonen; foundation of Tyyni Tani, University of Oulu; research grant from the Finnish Dental Society Apollonia, the society of Finnish Female Dentists and the Finnish Association for Dentists in Public Health, which are gratefully acknowledged.
10th May, 2015 Tarja Tanner
11
Abbreviations and definitionsBOP Bleeding on Probing = bleeding indexBW Bitewing radiographyCI Confidence IntervalCE Clinical examination CPI Community Periodontal IndexDT Number of decayed permanent teeth needing restorative treatmentDMFT Number of decayed, missing and filled permanent teeth FT Number of filled permanent teeth GTK Geological Survey of FinlandHU-DBI Hiroshima University – Dental Behavioral InventoryICC1 Intra-class correlation coefficientICC2 Inter-class correlation coefficientID IdentificationICDAS International Caries Detection and Assessment SystemMT Number of missing permanent teeth due to dental caries OR Odds ratioREC Gingival recessionSD Standard DeviationSES Socioeconomic statusWHO World Health Organization
12
13
List of original papers This thesis is based on the following publications, which are referred throughout the text by their Roman numerals:
I Anttonen V, Tanner T, Kämppi A, Päkkilä J, Tjäderhane L, Patinen P (2012) A methodological pilot study on oral health of young, healthy males. Dent Hypotheses 3:106–111.
II Tanner T*, Kämppi A*, Päkkilä J, Patinen P, Rosberg J, Karjalainen K, Järvelin M-R, Tjäderhane L, Anttonen V (2013) Prevalence and polarization of dental caries among young, healthy adults – Cross-sectional epidemiological study. Acta Odontol Scand 71:1436–1442. (*These two authors contributed equally to this work)
III Tanner T, Kämppi A, Päkkilä J, Järvelin M-R, Patinen P, Tjäderhane L, Anttonen V (2014) Association of smoking and snuffing with dental caries occurrence in a young male population in Finland: A cross-sectional study. Acta Odontol Scand 72:1017–1024.
IV Tanner T, Päkkilä J, Karjalainen K, Kämppi A, Järvelin M-R, Patinen P, Tjäderhane L, Anttonen V (2015) Smoking, alcohol use, socio-economic background and oral health among young Finnish adults. Community Dent Oral Epidemiol Apr 24 doi: 10.1111/cdoe.12163. [Epub ahead of print]
In addition, some unpublished data are presented.

14
15
Contents
AbstractTiivistelmäAcknowledgements 9Abbreviations and definitions 11List of original papers 131 Introduction 192 Review of the literature 21
2.1 Trends in caries occurrence in adolescents in the industrialised countries .................................................................................................. 212.1.1 Polarisation of dental caries among young adults ........................ 21
2.2 Periodontal health of young people ........................................................ 222.3 Young adults and use of intoxicants ....................................................... 232.4 Snuffing/use of smokeless tobacco, dental caries and periodontal
health ...................................................................................................... 242.5 Alcohol use, dental caries and periodontal health .................................. 252.6 Health behaviours in association with the use of intoxicants ................. 252.7 Health behaviours, dental caries and periodontal health ........................ 262.8 Sociodemographic factors and use of intoxicants .................................. 262.9 Sociodemographic factors, dental caries and periodontal health............ 272.10 Oral health studies among conscripts ..................................................... 28
3 Hypotheses and aims of the studies 314 Subjects and methods 33
4.1 Subjects ................................................................................................... 334.1.1 Pilot study (I) ............................................................................... 344.1.2 Other studies (Studies III–V) ....................................................... 35
4.2 Oral health screening .............................................................................. 364.2.1 Oral health screening in the pilot study (I) .................................. 364.2.2 Training and calibrating the dentists (II–IV) ............................... 374.2.3 Oral health screening (II–IV) ....................................................... 38
4.3 Questionnaire .......................................................................................... 404.3.1 Pilot study (I) ............................................................................... 414.3.2 Studies III and IV ......................................................................... 41
4.4 Factors associated with the place of residence (III)................................ 42
16
4.5 Statistical analyses .................................................................................. 424.5.1 Study I (pilot) ............................................................................... 424.5.2 Study II ......................................................................................... 424.5.3 Study III ....................................................................................... 434.5.4 Study IV ....................................................................................... 44
4.6 Ethical issues .......................................................................................... 455 Results 47
5.1 Pilot study (I) .......................................................................................... 475.1.1 Timing of different sections of the clinical inspection and
answering questionnaire ............................................................. 475.1.2 Remarks concerning the questionnaire, study design and
protocol ...................................................................................... 475.2 Calibration of the dentists (II) ................................................................ 485.3 Distribution of the mean DMFT and DT values (II) .............................. 48
5.3.1 Polarisation of dental caries (II) ................................................... 505.3.2 Tooth-wise distribution of DT, FT and MT components (II) ....... 51
5.4 Use of intoxicants (III, IV) ..................................................................... 515.4.1 Prevalence of smoking, snuffing and alcohol use (III, IV) .......... 515.4.2 Background factors associated with smoking and snuffing (III) .....525.4.3 Mean DT, DMFT, CPI and BOP values according to the
use of alcohol and smoking (IV) ................................................ 565.5 Background factors associated with DT and DMFT (III, IV) ................ 57
5.5.1 Effect of the use of intoxicants on DT and DMFT (III, IV) ........ 585.6 Distribution of BOP and CPI values ....................................................... 595.7 Background factors associated with CPI and BOP values (IV).............. 60
5.7.1 Effect of the use of intoxicants on CPI and BOP (IV) ................. 605.8 Smokers’ use of dental services and proposition of acute care (IV) ....... 625.9 The main findings (I–IV) ........................................................................ 62
6 Discussion 656.1 Validation of the epidemiological study (I) ............................................ 65
6.1.1 Randomisation (I–IV) .................................................................. 666.1.2 Validation of the examiners (II) ................................................... 666.1.3 Validation of the study protocol (I-IV) ........................................ 676.1.4 Subjective treatment need (I) ....................................................... 686.1.5 Validation of the questionnaire (I, III, IV) ................................... 68
6.2 DT and DMFT among young adults (II) ................................................ 696.2.1 Caries polarisation (II) ................................................................. 70
17
6.3 BOP and CPI among young adults (IV) ................................................. 716.4 Prevalence of smoking, snuffing and alcohol use (III, IV) ..................... 726.5 Smoking, snuffing, dental caries and associated factors (III) ................. 736.6 Background factors associated with DT, DMFT, BOP and CPI ............. 75
6.6.1 Snacking and tooth brushing (III) ................................................ 756.6.2 Smoking (III, IV) ......................................................................... 766.6.3 Snuffing (III) ................................................................................ 776.6.4 Alcohol use (IV) .......................................................................... 786.6.5 Education level (III, IV) ............................................................... 796.6.6 Urban–rural residence (III) .......................................................... 796.6.7 Language of the municipality of residence (III) .......................... 796.6.8 Fluoride level in drinking water (III) ........................................... 806.6.9 Using dental services (IV) ........................................................... 81
6.7 Strengths and weaknesses of the study ................................................... 827 Summary and conclusions 83
7.1 Practical relevance and future studies .................................................... 83References 85Appendices 97Original papers 107
18

19
1 Introduction In the early 1990s, young people in Finland had reached and even exceeded the oral health goal set by WHO (DMF < 2 for 12-year-olds) (Nordblad et al. 2004). Therefore, an individual recall system replaced regular dental check-ups at public health clinics in Finland. Recently, the decline in caries prevalence, however, has shown signs of levelling or even deterioration, particularly in terms of childhood caries in Finland and also elsewhere (Nordblad et al. 2004, Pitts et al. 2006).
The causes for this stagnation of improvement in Finland can be speculated. In the early 1990s, health promotion, including the promotion of oral health, was the first which was cut when the economic recession caused a reduction in the resources of the public health services. Simultaneously, individual recall intervals became a common practice. It has been reported that low examination rates in public health is weakly associated with caries prevalence (Suominen-Taipale et al. 2009). Conventional methods such as brushing with fluoride toothpaste and restricting sugar use play an important role in caries control (Ellwood et al. 2008, Zero et al. 2008). However, during the past decades, dietary habits of young people have changed worldwide. Unhealthy snacking of processed foods, take-away type meals and beverages is more common than ever before (Popkin 2006). This kind of a trend increases the intake of refined carbohydrates, added sugars and fats among young adults (Popkin 2006). Finnish young people, especially boys and men, are brushing their teeth more rarely compared to other countries in Europe. Less than half of adolescents report brushing their teeth twice a day (Maes et al. 2004, Honkala et al. 2012). Such dietary and oral hygiene behaviours are harmful to young adults’ oral health.
The effect of fluoride in drinking water disappeared with the improving dental status (Seppä et al. 1998, 2002), most likely due to the common use of topical fluorides in Finland from the 1970s onwards. At the moment, drinking water is not fluoridated in Finland and the level of fluoride in drinking water is low, between 0 and 0.3 mg/l, in most parts of the country. Only in the south-eastern and south-western regions the level of fluoride in drinking water is high, > 0.8 mg/l (Lahermo & Backman 2000).
Socioeconomic status (SES) is known to be associated with health. The Swedish-speaking minority have higher SES and better health than their Finnish-speaking counterparts (NIHW 2006). Finland is officially a bilingual (Finnish and Swedish) country. Of the total population of 5.4 million, 5.4% are Swedish-speaking (Statistics Finland 2011). The majority of the Swedish-speaking people live in the southern, south-western and western parts of the country.

20
Smoking and alcohol use are well-known risk factors to general health. High blood pressure, tobacco smoking, including second-hand smoke, and alcohol use were the three leading risk factors in the global disease burden in 2010 (Lim et al. 2012). In 2005, alcohol consumption in Finland by adults (15 years and older) was on average 12.5 litres of pure alcohol. The mean alcohol consumption is almost the same as in Europe (12.2 l). (WHO 2011a). In 2013, about 16% of Finns aged 15–64 reported smoking daily. Daily smokers accounted for 19% of men and 13% of women. (Helldán et al. 2013). Prevalence of smoking differ around the world, being the highest in Europe (32%), followed by the regions of Western Pacific (28%), Americas (21%), Easter Mediterranean (19%), South-East Asia (18%) and Africa (10%) (WHO 2011b). Different kinds of smokeless tobacco products are also used worldwide. In Europe, the most common smokeless tobacco product is the Swedish moist snuff, called snus. In South-East Asia and parts of Africa, smokeless tobacco is often chewing tobacco combined with nuts, usually areca or betel nuts. Chewing tobacco and dry or moist snuff are often used in the North America. (SCENIHIR 2008). Import and marketing of snuff are banned within the entire European Union (EU) region since 1992, apart from Sweden who was the only country in the EU who applied for and was granted a special exemption to manufacture and market Swedish snus when it joined the EU in 1995, partly due to its longstanding tradition of snus use. In 2013, 2.9% of 15–64-year-old Finnish men used snuff daily and 3.8% occasionally, but among Finnish adult women snuffing is very rare (Helldán et al. 2013).
Military service is obligatory for Finnish men under 28 years of age, unless they have some physical or mental disability preventing the service. Since 1995 also Finnish women have had the possibility to do voluntary military service. Around 25,000 young adults, 79% of the males in each cohort, enter the service annually. The military service attendance rate is by far the highest in Finland compared to other countries, therefore comprising an excellent study group for epidemiological studies. (Siilasmaa et al. 2010). Conscripts’ obligatory general health inspection and oral health screening is performed during their first week of military service.
The main aim of this study was to investigate young men’s oral health situation and health behaviours, and particularly their use of intoxicants. This study includes information from both the clinical examination and a questionnaire covering background factors and health habits. With the comprehensive study population of males born in the early 1990s in Finland, the present study is a useful epidemiological study on oral health and health behaviour among young adults.
21
2 Review of the literature
2.1 Trends in caries occurrence in adolescents in the industrialised countries
Oral health of young people has dramatically improved in the industrialised countries since the 1950s when the first epidemiological studies were published (Marthaler 2004). The changes in the distribution of caries occurrence included an overall decline in prevalence and severity in child population, increasing polarisation of dental caries and concentration of caries in pit and fissure lesions (Burt 1998). There is a number of different reasons for the decline in caries prevalence. Perhaps the main reasons were frequent use of fluoride toothpaste and other topical fluoride products (Bratthal et al. 1996, Seppä et al. 1998) as well as effective prevention policies (Burt 1998). However, the reasons for the decline vary in different countries and should be topics for epidemiological studies (Bratthall et al. 1996).
The positive trend in the improvement of caries status took a turn in the early 1990s, when it was reported that decrease in caries was showing signs of levelling or even deterioration (Spencer et al. 1994, Hugoson et al. 1995). Since the beginning of the 1990s, oral health has shown signs of deterioration, particularly in terms of childhood caries, in Finland and elsewhere (Marthaler 2004, Nordblad et al. 2004, Pitts et al. 2006, Anttonen et al. 2008, Hopcraft et al. 2009, Anttonen et al. 2011).
2.1.1 Polarisation of dental caries among young adults
Polarisation of dental caries describes the distribution of caries burden in population. WHO (1997) recommends the following criteria for registering dental caries: sound, decayed (D or Decayed), filled (F or Filled) and missing teeth (M or Missing due to dental caries), excluding wisdom teeth. At the tooth level, D represents both primary and secondary caries lesions as well as teeth needing endodontic treatment or extraction. M represents teeth missing due to dental caries and F represents restored teeth (WHO 1997).
Sheiham & Sabbah (2010) explained that polarisation increases when DMFT (decayed, missing and/or filled teeth) values improve and the number of individuals with no restorative treatment need increases. This information may be used in estimating the need for dental resources. According to a previous study among conscripts in Finland in 1993 (Läärä 1999), the worst 10% of the subjects
22
accounted for 50% of all decayed teeth and the worst 100 subjects (3.5%) had 24% of all decayed teeth. Compared to the previous study by Ankkuriniemi (1979), where the worst 16.7% of subjects had more than half (52.5%) of all caries lesions, polarisation was more pronounced in the study by Läärä (1999). In the Health 2000 study focusing on the Finnish adult population, 25% of subjects had 90% of the caries lesions (Suominen-Taipale et al. 2008). Polarisation of dental caries has also been reported among first-year university students in Finland (Peltola et al. 2006). Oral health of university students improved from 1982 to 2002. The mean DMFT index decreased significantly during those two decades, yet the number of decayed teeth increased slightly (Peltola et al. 2006). Elsewhere, for example in Brazil, oral health of young males improved between 1999 and 2003 (Bastos et al. 2007). Caries prevalence decreased by 18.6% and caries severity by 26.7%, which led to an increase in dental caries polarisation (Bastos et al. 2007).
2.2 Periodontal health of young people
Gingivitis associated with dental plaque formation is the most common form of gingival disease among the young, but there are also other reasons for gingivitis (Novak 2006). Some gingival diseases lead to periodontitis especially if the person has some risk factors (Novak 2006). Gingival bleeding has been shown to predict future periodontitis in follow-up studies both among young adults and among adults (Albandar et al. 1998, Schätzle et al. 2003).
Periodontitis is an inflammatory disease of the supporting tissues of the teeth caused by microorganisms and affected by individual tissue response. Periodontitis is a result of progressive destruction of the periodontal ligament and alveolar bone with pocket formation, recession or both (attachment loss) (Novak 2006). Young people do not have much attachment loss or bone destruction unless they have aggressive periodontitis. Prevalence of localised aggressive periodontitis varies among the young because of genetic and ethnic factors from 0.1 to 4.3% in the European population (Saxby 1984, Levin et al. 2006). According to the review article by Susin et al. (2014), prevalence of aggressive periodontitis in Northern and Central Europe is 0.1%, 0.5% in the South European population, and between 1% and 5% in the African population. In North America, aggressive periodontitis affects 0.1–0.2% of Caucasians, 0.5–1.0% of Hispanics and 2.6% of African-American people. The disease prevalence in South America is between 0.3% and 2.0% and in the Asian population between 0.2% and 1.0% (Susin et al. 2014).

23
2.3 Young adults and use of intoxicants
The Adolescent Health and Lifestyle Survey has monitored the use of alcohol and tobacco products in the adolescent population aged 12 to 18 years every two years since 1977 in Finland (Kinnunen et al. 2013). Among 18-year-old boys, prevalence of smoking has decreased from 34.5% in 1981 to 18.7% in 2013 whereas occasionally or daily snuffing has increased from 5.1% in 1981 to 14.5% in 2013 (Kinnunen et al. 2013). In recent studies on Finnish conscripts, prevalence of smoking was around 30% (Bingham et al. 2010, Mattila et al. 2012), i.e. somewhat higher than the previous figures among Finnish young adults Kinnunen et al. 2013). Additionally, monthly and weekly alcohol use has decreased among 18-year-old boys during the recent years (Kinnunen et al. 2013). Most boys (72%) in this age group used alcohol monthly or more often and 34% used alcohol every week, which was the lowest figure in the 21st century (Kinnunen et al. 2013). According to a recent WHO report from Europe and North America, 15-year-old adolescents seem to consume more alcohol in other countries than in Finland (Ferreira et al. 2012). Smoking, dental caries and periodontal health
The influence of smoking on general health, including oral health, is well known (Samet et al. 2004, Ylöstalo et al. 2004). There are some studies showing an association between dental caries and smoking (Axelsson et al. 1998, Rooban et al. 2011). On the other hand, there are also studies in which that association is unclear or even missing (Vellappally et al. 2007, Hugoson et al. 2012). The association between smoking and dental caries has been explained by, for example, poor oral hygiene and harmful dietary habits associated with smoking (Bruno-Ambrosius et al. 2005, Hellqvist et al. 2009).
The deteriorating effect of smoking on periodontal disease is also well known among the young (Ylöstalo et al. 2004, Levin et al. 2006, Thomson et al. 2007, Heikkinen et al. 2008) even with short-term or low tobacco consumption (Rosa et al. 2008). Tomar & Asma (2000) reported in their epidemiological study that smokers have four times more periodontitis than non-smokers. In addition, Machuca et al. (2000) found that deeper probing depths and greater bleeding values were recorded among smoking conscripts compared to non-smoking conscripts. Smoking cessation may be associated with relatively rapid improvement in the periodontium among young adults (Thomson et al. 2007). Smokers indeed have less gingival bleeding on probing than non-smokers eventually because smoking masks the effects of inflammation (Novak & Novak 2006, Shimazaki et al. 2006).
24
2.4 Snuffing/use of smokeless tobacco, dental caries and periodontal health
Different kind of smokeless tobacco products are used worldwide. In Europe, the most common smokeless tobacco product is moist snuff used on oral mucosa, usually in the sulcus under the upper lip, called snus (in Swedish). In parts of Africa and South-East Asia, smokeless tobacco is often chewing tobacco together with, for example, areca or betel nuts. In the US, dry or moist snuff or chewing tobacco are often used. (SCENIHR 2008). A common factor to all smokeless tobacco products is that they are addictive (WHO 2008, 2011b). The nicotine concentration in the products varies by more than 100-fold. The plasma levels of nicotine and the speed of delivery depend on the pH and buffering capacity of saliva. When pH in the oral cavity rises, more nicotine is absorbed through the buccal mucosa (Fant et al. 1999). The buffering agents include slaked lime, bicarbonate, ash, etc. (SCENIHIR 2008). The products also vary by several carcinogens, such as tobacco-specific nitrosamines (TSNA), benzo[α]pyrene, arsenic, nickel, formaldehyde, radioactive polonium-210, and other toxicants. The Swedish snus contains tobacco, water, sodium carbonate, sodium chloride and moisturiser. (SCENIHIR 2008). It contains small amounts of fermentable carbohydrates and has high pH value and a low level of tobacco-specific nitrosamines (Lee 2011). Many kinds of smokeless tobacco products are also used widely in North America (SCENIHIR 2008). Some chewing tobacco products used in the US contain sucrose (Tomar & Winn 1999, SCENIHIR 2008). In South-East Asia several smokeless tobacco products are widely used; for example, pan masala contains betel nuts, areca nuts, catechu, lime, spice flavourings, saccharine and other additives, gutka contains pan masala with tobacco and zarda is prepared by boiling pieces of tobacco leaves in water with slaked lime (Sinha et al. 2006).
There are only a few studies on the association between snuffing and dental caries. The results are contradictory and vary from increasing the risk of dental caries (Tomar & Winn 1999) to a neutral effect (Hugoson et al. 2012). According to a study by Tomar & Winn (1999), among US adult men, chewing tobacco may be a risk factor in the development of root-surface and coronal caries. Hugoson et al. (2012) found that snuffing does not increase the risk of dental caries. They also proposed that the salivary buffer capacity of snuffers is greater than non-users, which may help the remineralisation process of caries lesions and also further inhibition of the cariogenic microflora. The reasons for the contradictory results may be due to the different compositions of smokeless tobacco products in different countries.
25
Already in the 1990s, Tomar & Winn (1999) reported that gingival recession and enhanced collagenase activity have increased among the individuals using smokeless tobacco in the US. In Sweden, no association was found between periodontal disease and snuffing (Wickholm et al. 2004, Rolandsson et al. 2005, Bergström et al. 2006, Hugoson & Rolandsson 2011). However, Montén et al. (2006) reported a significant association between the use of snuff and gingival recessions in the maxillary anterior tooth region. Mechanical and/or chemical trauma to the gingiva might be causative factors for the development of recession.
2.5 Alcohol use, dental caries and periodontal health
The association between alcohol use and oral health has been investigated mostly among adult populations, and studies conducted on young adolescents are difficult to find. Among adults an association has been found between dental caries occurrence and alcohol use (Jansson 2008, Nguyen et al. 2008). Reports on the association of alcohol use to periodontal health vary from increased risk (Jürgensen et al. 2012, Lages et al. 2012) to limited effect (Okamoto et al. 2006) or no effect (Jansson 2008).
2.6 Health behaviours in association with the use of intoxicants
According to many previous studies, poor oral hygiene and harmful dietary habits are associated with smoking among adolescent (Bruno-Ambrosius et al. 2005, Honkala et al. 2011) and young adults (Hellqvist et al. 2009). Engström et al. (2010) also found that the dietary habits of snuffers are more harmful than those of non-users (less fruit and vegetables and more alcohol). Smoking (Paavola et al. 2004) and snuffing (Engström et al. 2010) have been reported to be associated with alcohol consumption, whereas alcohol abuse is particularly found with tobacco use (Li et al. 2007).
Dental attendance of smokers is lower than that of non-smokers (Drilea et al. 2005, Hellqvist et al. 2009, Bloom et al. 2012). Poor dental attendance can also be an explaining factor for poor oral health of smokers and those with heavy alcohol consumption compared to non-smokers and non-drinkers. The same has been shown to be true for adults with the highest alcohol consumption compared with those with moderate use (Jansson 2008).
26
2.7 Health behaviours, dental caries and periodontal health
Conventional oral hygiene habits, such as removal of plaque by brushing with fluoride toothpaste and restriction of sugar consumption, play an important role in caries control (Ellwood et al. 2008, Zero et al. 2008). The role of food intake in caries development has widely been studied for decades, and its impact on oral health is beyond dispute. Most of the studies have investigated the impact of sugar and sugar substitutes on dental caries (Gupta et al. 2013, Moynihan & Kelly 2014) but also the effect of eating and snacking frequency (Popkin et al. 2006, Nguyen et al. 2008).
Many previous studies have found that good oral hygiene and a healthy diet are also associated with good periodontal health (Axelsson 1998, Bawadi et al. 2011, Tomofuji et al. 2011). It is clear on the basis of experimental and epidemiologic studies that microbial plaque is the direct cause of gingivitis and poorer oral hygiene increases the prevalence of gingivitis (Beck & Arbes 2006).
Dental attendance has also been associated with dental caries and periodontal health. Nguyen et al. (2008) reported how former or never regular attendance significantly increase caries occurrence among men. In addition, former and never regular attenders had a significantly higher DMFT value but fewer filled teeth than always regular attenders (Aldossary et al. 2015). On the other hand, low examination rates in public health have been shown to be associated with slightly poorer dental health as for dental caries (Suominen-Taipale et al. 2009).
Herman et al. (2009) reported that regular dental attendance is significantly associated with healthier periodontium (CPI=0).
2.8 Sociodemographic factors and use of intoxicants
A recent Swedish study among 34,707 adults presented profiles of smokers and snuff users (Engström et al. 2010). A typical snuffer was reported to be alike non-tobacco users apart from heavier alcohol use and lower use of fruits and vegetables. An average snuffer is a young man who is skilled manual worker with intermediate education. He has also a good self-perceived general and mental health. In contrast, a typical smoker is a middle-aged manual worker with low education and very low income level who consume large amounts of alcohol and less often fruit and vegetables. A typical smoker has also low BMI and sedentary lifestyle in leisure time as well as perceived poor general and mental health. (Engström et al. 2010). Sociodemographic factors are significantly associated with the use of tobacco

27
products also among Finnish young people (Honkala et al. 2011, Mattila et al. 2012). A low educational status increases the risk of smoking (Honkala et al. 2011, Mattila et al. 2012). The odds for the use of snus were significantly higher among those living in the capital area or large cities than in rural areas (Mattila et al. 2012). The use of snuff is associated with higher intensity sport activity organised by sports clubs or teams. Sports requiring more individual performance and maximal oxygen intake (e.g., running, swimming, cycling, or cross-country skiing) are not associated with any use of tobacco products. (Mattila et al. 2012).
Bonevski et al. (2014) have prepared separate profiles of smokers, alcohol users and risky alcohol users with a smoking habit based on 267,153 Australians aged 45 and over. Factors associated with tobacco use alone were female gender, younger age, lower individual- and area-level socioeconomic status, depression and psychological distress. Factors associated with alcohol use alone were old age, male gender, higher socioeconomic status and lower psychological distress and no recent depression treatment. Factors associated with concurrent risky alcohol consumption together with tobacco use included being middle-aged, male, having low educational status, being unemployed, and living in lower-socioeconomic areas, having or having had treatment for depression and high distress. (Bonevski et al. 2014).
2.9 Sociodemographic factors, dental caries and periodontal health
Sociodemographic factors (socioeconomic status, SES) are among the most important factors associated with oral health, even in the 21st century. The topic has widely been studied in the past decades, and the impact of SES has not changed even with new information technology. It seems that no matter how socioeconomic status is measured, the differences in oral health always exist (Schou & Uitenbroek 1995, Schwendicke et al. 2015).
Educational background in the family and family income are both associated with oral health (Ankkuriniemi 1979, Läärä 1999, Ceylan et al. 2004, Häkkinen et al. 2006, Bastos et al. 2007, Polk et al. 2010, Costa et al. 2012, Hugoson et al. 2012, Buchwald et al. 2013). Polk et al. (2010) suggested that the impact of socioeconomic disparity on caries experience may be explained by individual oral hygiene habits (tooth brushing and flossing), preventive interventions (sealant use and fluoride exposure) and recent history of dental attendance.
Furthermore, the place of residence is associated with oral health (Ankkuriniemi 1979, Läärä 1999, Ceylan et al. 2004, Hopcraft et al. 2009, Kämppi et al. 2013). Hopcraft et al. (2009) found that Australian conscripts who had lived most
28
of their lives in areas with access to fluoridated drinking water had about 25% lower caries experience than those without fluoride exposure. Also among the Finnish conscripts in the 1970s, oral health situation varied in different parts of Finland, and the fluoride level in drinking water was associated with good oral health (Ankkuriniemi 1979). Living in an urban or rural area affects oral health (Läärä 1999, Ceylan et al. 2004). According to the studies on Finnish conscripts (Läärä 1999, Kämppi et al. 2013), living in an urban area significantly decreases the number of decayed teeth. Ceylan et al. (2004) found only a weak correlation between oral health and urbanisation. The reason for a better oral health status in urban areas may be the bigger proportion of well-educated inhabitants compared to rural areas (OSF 2012). In addition, people who live in urban areas use more dental services, which also affects oral health (Aldossary et al. 2015). Läärä (1999) has stated that the importance of socioeconomic differences is almost fundamental. The reasons for them may be so deeply buried in the society or in the subjects’ personality that the health care system alone is not able to diminish the differences (Läärä 1999).
2.10 Oral health studies among conscripts
Conscripts form an excellent study population for cross-sectional studies because their age and general health are quite similar. In the army, it is also easy to investigate a large number of people in a short period of time.
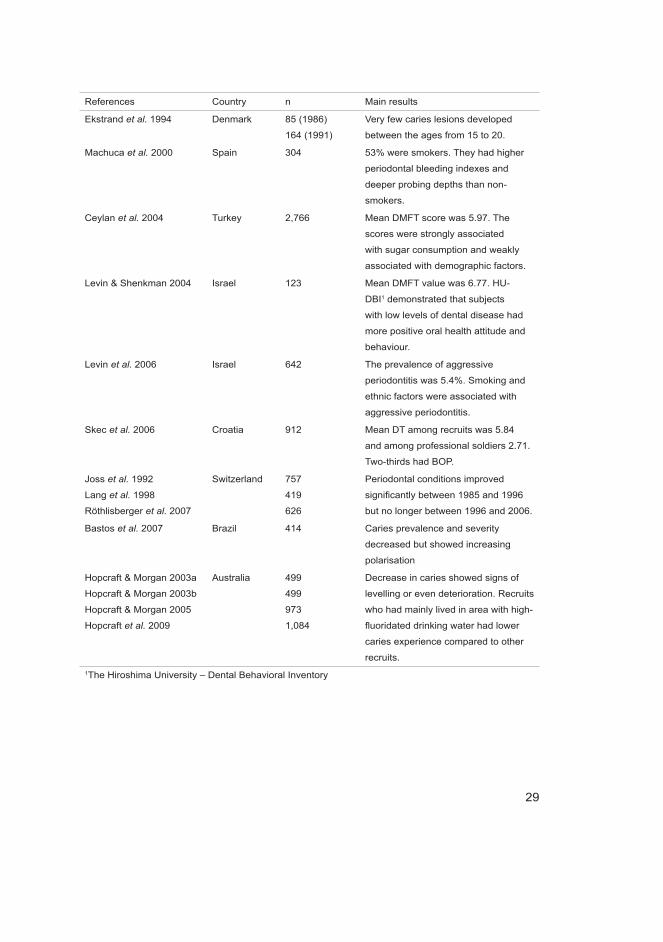
Conscripts’ oral health has been investigated in two studies in Finland and in some studies elsewhere (Table 1).
Table 1. Studies of conscripts’ oral health in Finland and elsewhere.
References Country n Main results
Ankkuriniemi 1979 Finland 3,344 Mean DT, MT and FT values were
4.34, 1.22 and 10.28.
About 75% had gingival bleeding
(BOP).
Läärä 1999 Finland 2,850 Mean DT and DMFT values were 1.98
and 6.75. Caries burden was strongly
polarised.
29
References Country n Main results
Ekstrand et al. 1994 Denmark 85 (1986)
164 (1991)
Very few caries lesions developed
between the ages from 15 to 20.
Machuca et al. 2000 Spain 304 53% were smokers. They had higher
periodontal bleeding indexes and
deeper probing depths than non-
smokers.
Ceylan et al. 2004 Turkey 2,766 Mean DMFT score was 5.97. The
scores were strongly associated
with sugar consumption and weakly
associated with demographic factors.
Levin & Shenkman 2004 Israel 123 Mean DMFT value was 6.77. HU-
DBI1 demonstrated that subjects
with low levels of dental disease had
more positive oral health attitude and
behaviour.
Levin et al. 2006 Israel 642 The prevalence of aggressive
periodontitis was 5.4%. Smoking and
ethnic factors were associated with
aggressive periodontitis.
Skec et al. 2006 Croatia 912 Mean DT among recruits was 5.84
and among professional soldiers 2.71.
Two-thirds had BOP.
Joss et al. 1992
Lang et al. 1998
Röthlisberger et al. 2007
Switzerland 757
419
626
Periodontal conditions improved
significantly between 1985 and 1996
but no longer between 1996 and 2006.
Bastos et al. 2007 Brazil 414 Caries prevalence and severity
decreased but showed increasing
polarisation
Hopcraft & Morgan 2003a
Hopcraft & Morgan 2003b
Hopcraft & Morgan 2005
Hopcraft et al. 2009
Australia 499
499
973
1,084
Decrease in caries showed signs of
levelling or even deterioration. Recruits
who had mainly lived in area with high-
fluoridated drinking water had lower
caries experience compared to other
recruits.1The Hiroshima University – Dental Behavioral Inventory

30
31
3 Hypotheses and aims of the studiesIn his article on caries prevalence during the past five decades, Marthaler (2004) expressed the need for continuous epidemiological research on the topic. The previous comprehensive epidemiological study on young men’s oral health in Finland dates back more than 15 years (Läärä 1999).
Our hypothesis was that oral health among young males in Finland has deteriorated compared to the study conducted in 1993 among a similar study group (Läärä 1999) and that polarisation has become weaker. The second hypothesis was that the prevalence of smoking and snuffing and consumption of alcohol may be at the same level as among older adolescents in Finland (Kinnunen et al. 2013). Furthermore, we hypothesised that the prevalence of dental caries and periodontal disease are higher among smokers, snuffers and alcohol users than among non-users. It was also hypothesised that smoking and snuffing are associated with other harmful oral health habits such as consumption of sugar products and neglecting brushing. Harmful oral health behaviour was hypothesised to have a stronger association with caries occurrence compared to smoking, snuffing, alcohol use and sociodemographic factors.
The specific aims were:1. To investigate the restorative treatment history and need among the healthy
young male population born in the early 1990s. 2. To study if polarisation of dental caries among the study population still exists.3. To investigate the prevalence of smoking, snuffing and alcohol use among the
male population born in the early 1990s in Finland and their association with dental caries occurrence and periodontal disease indicated.
4. To study the association of smoking and snuffing with oral health behaviours and factors related to the place of residence.
5. To study the impact of smoking, snuffing and alcohol consumption, own and parents’ education and poor dental attendance on oral health.
6. To study the association of smoking, snuffing and alcohol consumption and dental caries and risk of periodontal disease indicated.

32
33
4 Subjects and methods
4.1 Subjects
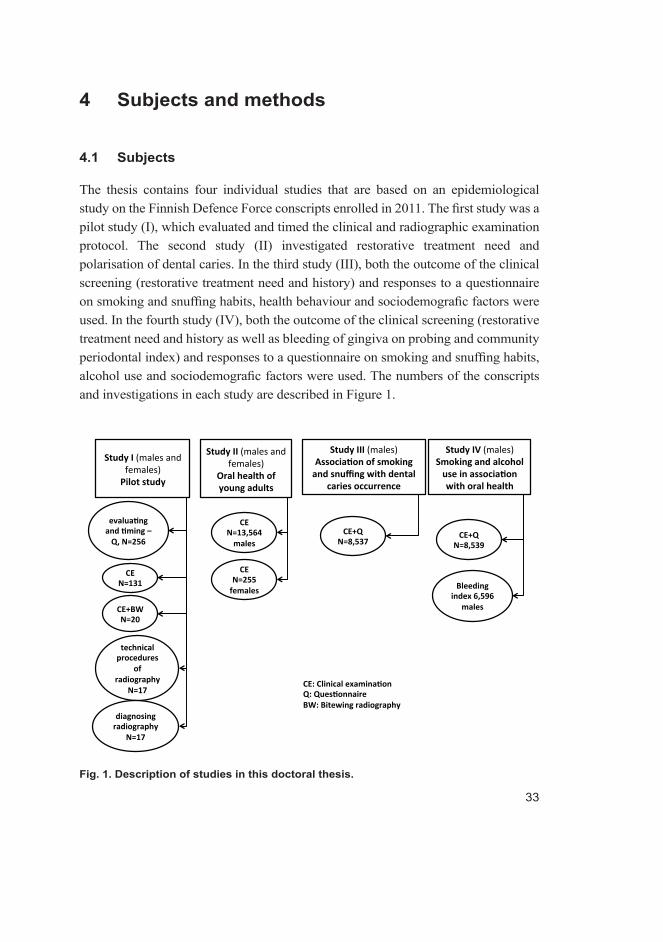
The thesis contains four individual studies that are based on an epidemiological study on the Finnish Defence Force conscripts enrolled in 2011. The first study was a pilot study (I), which evaluated and timed the clinical and radiographic examination protocol. The second study (II) investigated restorative treatment need and polarisation of dental caries. In the third study (III), both the outcome of the clinical screening (restorative treatment need and history) and responses to a questionnaire on smoking and snuffing habits, health behaviour and sociodemografic factors were used. In the fourth study (IV), both the outcome of the clinical screening (restorative treatment need and history as well as bleeding of gingiva on probing and community periodontal index) and responses to a questionnaire on smoking and snuffing habits, alcohol use and sociodemografic factors were used. The numbers of the conscripts and investigations in each study are described in Figure 1.
Fig. 1. Description of studies in this doctoral thesis.
34
4.1.1 Pilot study (I)
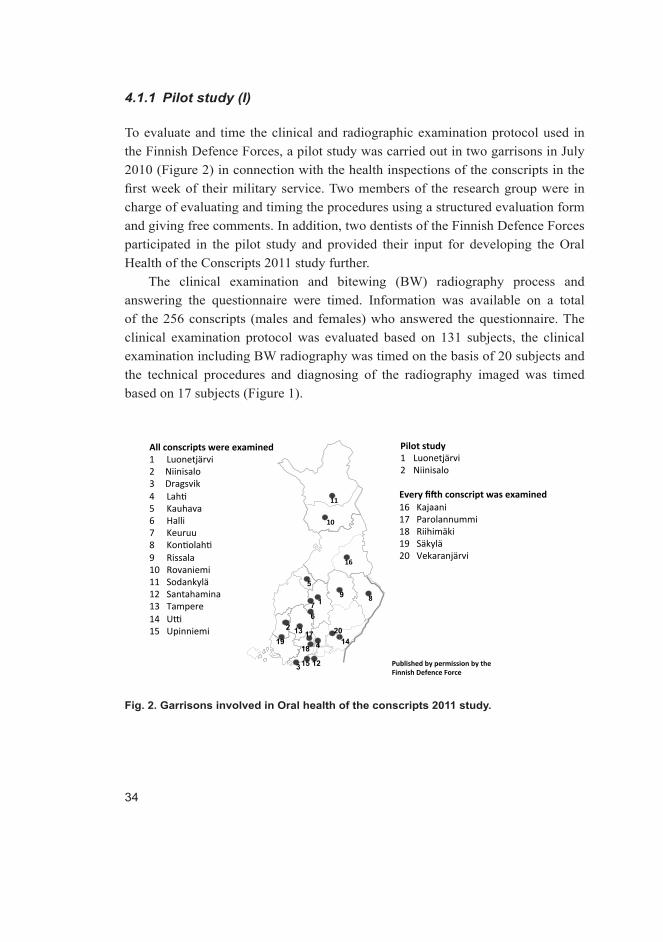
To evaluate and time the clinical and radiographic examination protocol used in the Finnish Defence Forces, a pilot study was carried out in two garrisons in July 2010 (Figure 2) in connection with the health inspections of the conscripts in the first week of their military service. Two members of the research group were in charge of evaluating and timing the procedures using a structured evaluation form and giving free comments. In addition, two dentists of the Finnish Defence Forces participated in the pilot study and provided their input for developing the Oral Health of the Conscripts 2011 study further.
The clinical examination and bitewing (BW) radiography process and answering the questionnaire were timed. Information was available on a total of the 256 conscripts (males and females) who answered the questionnaire. The clinical examination protocol was evaluated based on 131 subjects, the clinical examination including BW radiography was timed on the basis of 20 subjects and the technical procedures and diagnosing of the radiography imaged was timed based on 17 subjects (Figure 1).
9 1 7
3
2 6
5
13
12 15
14 20
19 18 4 17
Fig. 2. Garrisons involved in Oral health of the conscripts 2011 study.
35
4.1.2 Other studies (Studies III–V)
On the basis of the pilot study, an epidemiological cross-sectional study was designed in the spring of 2010 and carried out in 20 garrisons’ health centres (of a total 24) of the Finnish Defence Forces in January and July 2011 (Figure 2). A representative sample of the entire group of draftees in 2011 was achieved by examining all conscripts in 15 garrisons and every fifth conscript in alphabetical order randomising the subjects in the five largest garrisons (Figure 2). The study sample was randomised in the five largest garrisons because of the limited personnel resources. Because the conscripts enter the inspection unit-by-unit in alphabetical order, randomisation was done by selecting every fifth person in alphabetical order. Where the person chosen was absent, the next person was selected. That kind of randomising included both sexes. Four garrisons were excluded from the study because of the limited personnel in the dental service. However, those garrisons were small, the total number of excluded conscripts not exceeding 600. The clinical examination was carried out during the first two weeks of the service. The number of the dropouts was non-existent – all of those who were in the service were obligated to attend the examination when ordered.
The screened study population consisted of 13,564 males and 255 females born in 1990, 1991 or 1992 (mean age 19.6 years). In Finland, new draftees enter the service twice a year, and consequently the study was carried out twice, in January and in July. The outcome of the screening of dental caries prevalence and history (n = 13,564) was used in Study II.
The population in Study III comprised 8,537 male conscripts on whom there were data available from both the clinical screening and the questionnaire. Because the proportion of the female conscripts was small among the study group, their data were excluded from the analyses (Figure 1).
The population in Study IV comprised 8,539 male subjects whose dental caries and CPI data and responses to the questionnaire were used. The value of bleeding index (BOP) was available on 6,529 conscripts (Figure 1).

36
4.2 Oral health screening
4.2.1 Oral health screening in the pilot study (I)
Two dentists of the Defence Forces carried out the oral inspections according to the Defence Forces’ protocol and criteria. The protocol was timed, evaluated and commented by two independent dentists from the research group (the author being one) not working for the Defence Forces. The observations were recorded to a feedback form (Appendix 1). The two dentists were advised to inspect as many conscripts as possible because the aim was to evaluate and time the protocol. A probe, an oral mirror and the light of the dental unit were used for the examinations. The oral health screening aimed at determining the need for restorative treatment for each conscript according to the criteria of the Defence Forces (Table 2). In the criteria, 1 stands for a healthy tooth without fillings, 2 means a sound tooth with a filling, 3–5 stand for decayed teeth (4 with a filling), 6 means that the tooth has been extracted because of dental caries, 7 means that the tooth is missing per se, and 8–9 mean that a prosthetic structure has replaced the tooth/teeth. Periodontal diseases were classified following the WHO guidelines (1997). The Mildoc® computer program of the Finnish Defence Forces was used to record the oral findings, which were registered by a dental assistant. The Finnish evidence-based guidelines for controlling dental caries (Evidence-based guidelines 2009) were used as the criteria for taking the BW radiographs. According to those criteria, BW radiography is indicated in the presence of even one active caries lesion having penetrated into dentin. BW radiographs were advised to be taken only when clinically indicated. The conventional number 2 oral films of Kodak Insight Dental Film® (Kodak Insight Dental Film®, Eastman Kodak CO, Rochester, NY, USA) and Minray DC SL-9® X-ray devices (CompareNetworks, Inc. San Francisco, CA, USA) were used. The exposure time was 0.28 seconds. The films were processed in an automatic Dürr Dental Periomat Plus® processor (Dürr Dental Periomat Plus®, Dürr Dental AG, Bietigheim-Bissingen, Germany) using fresh processing solutions (Periomat Intra, Dürr Dental AG, Bietigheim-Bissingen, Germany). In one garrison, digital radiography was used, using the same exposure device with 0.16 s exposure time and the Digora scanning system (Soredex, Tuusula, Finland). All films were developed and findings diagnosed and recorded as so-called “second status” after clinical examination.
37
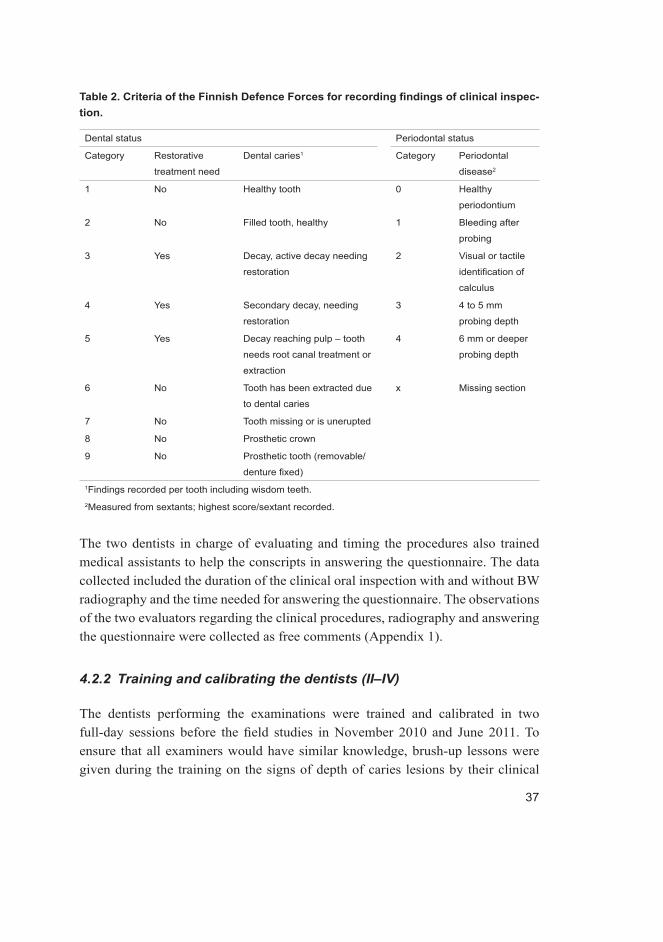
Table 2. Criteria of the Finnish Defence Forces for recording findings of clinical inspec-tion.
Dental status Periodontal status
Category Restorative
treatment need
Dental caries1 Category Periodontal
disease2
1 No Healthy tooth 0 Healthy
periodontium
2 No Filled tooth, healthy 1 Bleeding after
probing
3 Yes Decay, active decay needing
restoration
2 Visual or tactile
identification of
calculus
4 Yes Secondary decay, needing
restoration
3 4 to 5 mm
probing depth
5 Yes Decay reaching pulp – tooth
needs root canal treatment or
extraction
4 6 mm or deeper
probing depth
6 No Tooth has been extracted due
to dental caries
x Missing section
7 No Tooth missing or is unerupted
8 No Prosthetic crown
9 No Prosthetic tooth (removable/
denture fixed)1Findings recorded per tooth including wisdom teeth.2Measured from sextants; highest score/sextant recorded.
The two dentists in charge of evaluating and timing the procedures also trained medical assistants to help the conscripts in answering the questionnaire. The data collected included the duration of the clinical oral inspection with and without BW radiography and the time needed for answering the questionnaire. The observations of the two evaluators regarding the clinical procedures, radiography and answering the questionnaire were collected as free comments (Appendix 1).
4.2.2 Training and calibrating the dentists (II–IV)
The dentists performing the examinations were trained and calibrated in two full-day sessions before the field studies in November 2010 and June 2011. To ensure that all examiners would have similar knowledge, brush-up lessons were given during the training on the signs of depth of caries lesions by their clinical
38
appearance according to criteria of ICDAS, International Caries Detection and Assesment System (Ismail et al. 2007) and activity (Nyvad et al. 1999). WHO criteria were used in registering lesions in the field study according to the protocol of the Defence Forces. Lessons during training were targeted to provide information on clinical signs of lesions needing restorative treatment. The lessons were available to the examiners throughout the field study on the website of the Institute of Dentistry, University of Oulu, designed for this purpose. Following the lessons, and to practice their diagnostic skills, the dentists determined the treatment need for 30 previously photographed and radiographed extracted teeth with a variety of caries lesions using the WHO criteria (1997) and the protocol of Finnish Defence Forces (Table 2).
The same teeth were used in the calibration sessions in November 2010 and June 2011, after which they were sectioned to gain a golden standard. The teeth were cut in two halves revealing the most affected site using a high speed drill and a long and narrow diamond bur. After that they were photographed and the lesion depth was determined. This lesion depth served as the golden standard. The photographs and radiographs of the teeth were presented to the trainees through a PowerPoint presentation using a PC and a data projector. A consensus about the treatment need for all 30 teeth based on the clinical findings and supported by radiographic findings was achieved among the entire group in both sessions. The treatment need for the teeth recorded by the trainees in both sessions was collected for the analyses of inter-examiner and intra-examiner agreement.
4.2.3 Oral health screening (II–IV)
All the dentists working in the Defence Forces, a dentist conscript doing his military service and two external researchers (both DDS) (n = 15) carried out the oral health examinations. The dental examinations were carried out in the dental units of the garrison dental clinics.
Dental caries
The dental unit light, a probe and an oral mirror were used for the examination. The probe was used to study the tooth surface structures tactilely. The aim of the oral examination was to record the restorative treatment need at the tooth level for each conscript according to the 1997 criteria for epidemiological studies by WHO (1997) (e.g. sound teeth, decayed teeth, filled teeth and missing teeth as a result of

39
caries) excluding wisdom teeth, and following the protocol of the Defence Forces. The outcome achieved using the Defence Forces’ protocol was analysed as such but was also adjusted to gain the DT and DMFT values (Table 2). At the tooth level, D represented primary and secondary caries lesions as well as teeth needing endodontic treatment or extraction. M represented teeth missing due to dental caries and F represented restored teeth. If the tooth was both decayed and filled it was registered as decayed (D). In borderline cases, the trainees were advised to choose the alternative representing a more severe option.
Periodontal health
Periodontal health was examined for index teeth (dd. 16, 11, 26, 36, 31 and 46) using a gingival probe. The examination was advised to be carried out step by step around each tooth as advised in the WHO criteria for epidemiological studies (WHO 1997) with a force of about 20 g. The force was demonstrated to the examiners in a calibration session using a digital scale. Each sextant was to be examined only if there were two or more teeth present. If the index tooth of the sextant was missing, all the remaining teeth in that sextant were examined and the highest score was recorded as the bleeding on probing (BOP) score of the sextant. Three indicators of periodontal status were examined and recorded for every index tooth: gingival bleeding, calculus and depth of the periodontal pocket. Gingival bleeding was evaluated visually with an oral mirror after probing all index teeth. The number of bleeding sextants was registered. Gingival bleeding, calculus and the depth of the pockets were registered using Community Periodontal Index (CPI). CPI was coded using the numbers from 0 to 4 or the letter X (0 = Healthy; 1 = Bleeding observed, directly or by using oral mirror, after probing; 2 = Calculus detected during probing with pocket depth < 4 mm; 3 = Probing depth of 4–5 mm; 4 = Probing depth of 6 mm or more; and X = Excluded sextant [less than two teeth present]) (WHO 1997).
Bitewing radiographs
Bitewing radiographs were taken of every fifth conscript with clinical indication for radiography, which meant at least one clinically detected active caries lesion having penetrated into dentin. The dentists were advised to use the information on the radiographs to support their clinical findings. The Mildoc® oral health status computer program of the Finnish Defence Forces was used to record the oral findings. Recording the findings was carried out by a dental assistant.
40
4.3 Questionnaire
In connection with the oral inspection, the conscripts answered a computer-based questionnaire developed in the Institute of Dentistry, University of Oulu, Finland, for investigating individual background factors and health behaviour (Appendix 2). The modified form of the questionnaire has been used in studies on schoolchildren (Anttonen et al. 2008, 2011). Responses to the questionnaire could be analysed individually or as summary variables with or without combining clinical dental findings with the analyses. Answering the questionnaire was voluntary and by answering it, the conscripts gave their permission for using their personal military records. All records on oral health and on some general health issues (body mass index [BMI] and diagnoses of systemic diseases) as well as on issues connected with the military service (i.e., unit and court of the service) were collected into separate databases from Mildoc® for investigating data collection. These data were united with data from the questionnaire and prepared for analyses. All IDs (identifications) of the conscripts were excluded from the data before analyses. The key to the IDs was held by the University of Oulu and the Defence Forces as agreed in the project agreement between the parties.
The questionnaire comprised a total of 50 questions. The core of the questionnaire was formed by questions used in earlier studies on dietary and oral hygiene issues (questions 17 to 37) (Anttonen et al. 2008, 2011). Four new questions on the use of energy and sports drinks, smoking and consumption of alcohol and snuff were included in this section (questions 26 to 29). In addition, the following questions were added to the questionnaire: background information on social relationships, own education and education of parents, professions of parents and place of residence (questions 1 to 12), free-time activities (13, 14), general health and medication (15, 16), sources of information of received oral health promotion (38), presence of dental symptoms/toothache (39, 40), issues concerning dental attendance and received treatment, and estimated need for dental treatment (41 to 44, 47, 48), pain in the temporomandibular joints (TMJs) and facial area (45, 46), dental fear (49), and well-being in association with oral health (50). It was pointed out in the questionnaire that the questions concerned the period before entering the service, if not specified differently. The alternative answers to the questions were of the following types: Yes / No or Never or hardly ever / Every day or almost every day / Occasionally. The alternative was chosen by clicking on it on the computer screen. The program made it difficult for the

41
respondents to skip the questions but eventually it was possible. This information was automatically recorded and saved as a dBase file format for later statistical analyses.
4.3.1 Pilot study (I)
As a convenience sample, conscripts from the garrisons of Luonetjärvi and Niinisalo answered the questionnaire in Study I. The conscripts answered the questionnaire while waiting for their turn for the oral inspection and when the computer in the waiting area was available. Two laptop computers with the questionnaires were provided for both garrisons. Responding was timed (minutes and seconds) and any problems related to the questionnaire were registered to the feedback form (Appendix 1).
4.3.2 Studies III and IV
Three computers with the questionnaire program installed were provided per dentist to enable as many draftees as possible to answer the questionnaire while they were waiting.
In Study III the responses to the following questions were used: Do you smoke? (Not at all / 1–5 cigarettes daily / 10–20 cigarettes daily / > 20 cigarettes daily); Do you use snuff? (Never or hardly ever / Every day or almost every day / Occasionally); What is your education? (Comprehensive school / Vocational school / University of applied sciences / Vocational school and matriculation exam or upper secondary school / Matriculation exam or upper secondary school / College or university / Other); How often do you eat/drink the following snacks: Sweets / Crisps / Soft drinks / Energy drinks? (Never or hardly ever / Every day or almost every day / Occasionally during the week); and How often do you brush your teeth? (Never or hardly ever / Occasionally / Every day). For those persons who reported brushing their teeth every day, a new question opened: How many times a day do you brush your teeth? (Once a day / Twice a day / More than twice a day).
In Study IV, the responses to the following questions were used: Do you smoke? Do you consume alcohol? What is your education? What is your mother’s/father’s education? How often do you brush your teeth? How many times a day do you brush your teeth? How long ago did you visit an oral hygienist or a dentist? Did you visit a dentist last time because of toothache?
42
4.4 Factors associated with the place of residence (III)
In Study III, data from some other sources were pooled and prepared for analyses in addition to data from Mildoc®. Postal addresses including the province of the individual were collected from the database of the Defence Forces. Data on the mean fluoride level in the drinking water (mg/l) and the main language spoken (Finnish/Swedish) in each municipality were pooled with the original data as well. Data on the fluoride levels in all Finnish municipalities were purchased from the Geological Survey of Finland (GTK, an agency under the Finnish Ministry of Employment and the Economy) (Lahermo & Backman 2000). The fluoride levels used were those calculated from the combined values of streams, springs and dug and drilled wells in each municipality (Lahermo & Backman 2000). The mean fluoride values were categorised into three groups: 0–0.30 mg/ml, > 0.30–0.80 mg/ml and > 0.80 mg/ml. The conscripts were also divided into four groups according to the main language spoken in their place of residence (Finnish only, mainly Finnish [> 50%], mainly Swedish [> 50%], Swedish only).
4.5 Statistical analyses
4.5.1 Study I (pilot)
The results of Study I were descriptive and were executed with SPSS (version 16.0, SPSS, Inc., Chicago, Il, USA) and the R software (version 2.11.1 patched; a language and environment for statistical computing; R Foundation for Statistical Computing, Vienna, Austria, URL http://www.R-project.org).
4.5.2 Study II
For statistical analyses, only the data concerning the conscripts born in 1990, 1991 or 1992 were investigated (about 97% of all examined were males). To illustrate the level of treatment need, the mean DMFT and DT (SD) values were calculated for males and females. Data on third molars were excluded from the analyses. The distribution of the DMFT and DT values among both genders was illustrated using bar plots. Because the proportion of the female conscripts was small (1.8%) they were excluded from the rest of the analyses. To study the distribution of the DT values among the male conscripts in different DMFT categories, the DMFT values were categorised as follows: DMFT1 = 0, DMFT2

43
= 1, DMFT3 = 2–4, DMFT4 = 5–9, DMFT5 > 9. The frequencies and proportions of filled and decayed teeth were calculated. A Lorenz curve was drawn to describe caries polarisation. Restorative treatment need was also presented according to the Defence Forces’ criteria.
To estimate the intra- and inter-examiner agreement on treatment decisions, the examiners estimated the treatment need of 30 extracted teeth with a variety of caries lesions in two separate sessions on the basis of the criteria of WHO (1997), as described above. To describe the inter-examiner agreement, ICC1 values (inter-class correlation coefficient) were calculated in both sessions and their means (min, max) were presented. For validation, the consensus treatment decision of the entire group was considered as the golden standard. To investigate the intra-examiner agreement of the examiners, ICC2 values were calculated for the treatment decisions of each examiner in the two calibration sessions and their means (min, max) were presented.
All analyses were executed and figures drawn using SPSS (version 16.0 and 18.0 SPSS) and the R software (version 2.13.2 patched).
4.5.3 Study III
For statistical modelling, the DT and DMFT values were categorised as follows: DT = 0 or DT > 0, and DMFT ≤ 1 or DMFT > 1.
For the statistical analyses, the responses to the questions regarding smoking and using snuff were dichotomised as follows: those not smoking and those smoking 1–5 cigarettes daily or more, and those not using snuff and those using snuff at least occasionally during the week. A new variable was created to allow analysing persons according to their smoking and snuffing habits (no smoking/no snuffing, smoking/no snuffing, no smoking/snuffing and smoking/snuffing).
The confounding variables were dichotomised as follows: those eating/drinking snacks at least occasionally during the week and the rest. The two questions dealing with tooth brushing were linked together and categorised into three groups as follows: those brushing teeth two times daily or more, those brushing teeth daily, and the rest. The education level was categorised into three groups: vocational school, matriculation exam or upper secondary school, and the rest.
Cross tabulation was used to analyse the association between smoking/using snuff and other health behaviours and the education level. The significance between the groups was tested by chi-squared tests. The mean DT and DMFT values were investigated in four groups and the differences between the groups
44
were analysed with one-way ANOVA. Statistical significance was determined at p < 0.05. For analysing the risk (OR, 95% CI) of the occurrence of dental caries (bivariate responses DT = 0 or DT > 0, and DMFT ≤ 1 or DMFT > 1), smoking (No/Yes) and snuffing (No/Yes), generalised linear mixed models with logit link function were conducted (Faraway 2006). In these models, the garrison was treated as a random effect. The initial models included all independent variables and first-order interactions between health behaviours and smoking/snuffing. Those terms for which the regression coefficient did not reach statistical significance (p < 0.05) were eliminated from the final models. All analyses were executed and figures drawn using the SPSS software (versions 20.0) and R software (version 2.15.1 Patched).
4.5.4 Study IV
For statistical modelling, the DT and DMFT values were dichotomised as follows; DT = 0 or DT > 0, and DMFT ≤ 1 or DMFT > 1. The numbers of bleeding sextants were dichotomised as ≤ 2 and the rest. The value of the highest periodontal treatment need (CPI) was dichotomised as CPI ≥ 2 and the rest. In addition, the responses to the questions about smoking were categorised in two ways: those not smoking at all, those smoking 1–5 cigarettes daily and those smoking more than 10 cigarettes daily; and again those not smoking at all and the rest. Consumption of alcohol was categorised as follows: those consuming alcohol more than once a week (Intensive), those consuming alcohol at least once a month but not more than once a week (Moderate) and those consuming alcohol less than once a month or not at all (No alcohol).
A new variable was created to allow analysing persons according to the combined effect of smoking and alcohol consumption (No smoking/No alcohol, No smoking/Moderate alcohol, No smoking/Intensive alcohol, Smoking/No alcohol, Smoking/Moderate alcohol, Smoking/Intensive alcohol).
The responses to the two questions dealing with tooth brushing were combined. The responses were also categorised into three groups: those brushing teeth two times daily or more frequently, those brushing teeth daily, and the rest. The education level was categorised into three groups: vocational or upper secondary school, matriculation exam, and the rest. For statistical analysis, the responses to the question on the length of the period since the last visit to dentist were categorised in two ways; Less than a year ago / 1–2 years ago / 3–4 years ago / 5 years ago or more, or Do not remember / Less than 3 years ago and the rest.

45
The mean DT, DMFT, BOP and CPI values were investigated in six categories. The difference between the groups was determined statistically significant at p < 0.05. Generalized linear mixed models with logit link function were conducted (Faraway 2006) for analysing the risk (OR, 95% CI) of the occurrence of dental caries (DT), caries prevalence and treatment history (DMFT), gingival bleeding (BOP) and community periodontal index (CPI). In these models, the garrison was considered as a random effect. The terms for which the regression coefficient did not reach statistical significance were eliminated from the final models. The analyses were conducted on the basis of the responses of the conscripts who answered all questions. The smokers’ use of dental services and the proposition of acute care were illustrated using a mosaic graphics. All analyses were executed and figures drawn using the SPSS software (version 21.0) and R software (version 2.15.1 Patched).
4.6 Ethical issues
The data were collected from the archives of the records of the Finnish Defence Forces and by permission of the conscripts and the Finnish Defence Forces. For identification, ID numbers were created for all the conscripts. The key to the IDs and patient records is kept in the archives of the Defence Forces. The conscripts gave their consent to use their patient and military records by answering the voluntary computer-assisted questionnaire. The main research plan was evaluated by the Ethical Committee of the Northern Ostrobothnia Hospital District, and who gave its positive consent on 30 March 2010. The Centre for Military Medicine of the Finnish Defence Forces gave its permission for the study in June 2010 (AG14218/23.6.2010).

46
47
5 Results
5.1 Pilot study (I)
5.1.1 Timing of different sections of the clinical inspection and answering questionnaire
In the pilot study, the clinical inspections of 131 conscripts were timed from the moment the draftee entered the dental office to the moment he left it. The mean time spent for the clinical oral inspection per conscript was 2 minutes 48 seconds (range: from 1 min 55 s to 3 min 11 s). Exposing of radiographs added 1 minute 1 second. It took about 5 minutes and 30 seconds per conscript to develop, diagnose and record the radiographic findings. Answering the questionnaire took on an average 10 minutes 47 seconds (range: from 6 min 26 s to 15 min 27 s).
5.1.2 Remarks concerning the questionnaire, study design and protocol
On the basis of the duration of the inspection (about 3 min) and time spent on answering the questionnaire (about 11 min), the need of three computers per dentist was established to enable as many conscripts as possible to participate in the survey. Most of the questions in the questionnaire caused no comments by the respondents. However, they asked if migraine or pollen allergy were considered chronic illnesses (yes and no, respectively) and if net poker was considered a computer game (yes). Conscripts who had split their time between divorced parents also queried which parent they should report as having shared accommodation with (the one in whose home they got their mail). They also wondered how a conscript having both studied and worked during the past six months before the service should report his main job (yes). Furthermore, they questioned if one dose of alcohol per week was considered as use of alcohol (yes).
On the basis of the open-form comments, the protocol and criteria needed to be clarified to all the participants. The need for training in radiographic techniques and diagnosing was also recognised. Similarly, the criteria for determining the need for restorative, periodontal or endodontic treatment and radiography were considered essential.
48
Furthermore, the need for guidelines on how to record additional oral findings in a structured manner was brought up. Therefore, the number of gingival bleeding sextants, presence of traumatised and deciduous teeth, oral mucosal piercing, and the existence of active orthodontic treatment devices were decided to be added to the recording practice. Trained auxiliary staff was also considered necessary in each inspection team. At least one person for assisting in clinical inspections, one for helping with the questionnaire and, if possible, one for developing X-rays was also advised. Collecting and preparing data from several databases caused no difficulties.
About 40% of the participants were estimated having a need for dental treatment. Toothache or some other dental symptoms were reported by 14.6% and sensitivity of the teeth due to temperature changes or after exposure to acidic or sour food or drink by 26.5%. Therefore, the future study was considered indicated.
5.2 Calibration of the dentists (II)
The intra-examiner agreement on the treatment need in vitro before the field surveys was good ICC1 = 0.733 (min = 0.315, max = 0.846) before the January survey and ICC1 = 0.717 (min = 0.583, max = 0.861) before the July survey. The inter-examiner agreement on the treatment need was also good (ICC2 = 0.717; min = 0.275, max = 0.935).
5.3 Distribution of the mean DMFT and DT values (II)
The DMFT index of 78.7% of the conscripts was > 0 (men 78.6% and women 78.8%). The mean values of DMFT, DT and FT were 4.1 (SD = 4.2), 1.4 (SD = 2.5) and 2.7 (SD = 2.9), respectively. Almost half of the men (45.1%) and four in ten of the women (37.3%) had restorative treatment need. The restorative treatment need (DT) increased with increasing restorative history (DMFT). Those with low DMFT (≤ 4) had only some, if any, lesions needing restorative treatment, comparing to those with DMFT 5–9 [the median DT = 2 (n = 3,544)] or those with DMFT > 9 [the median DT = 5 (n = 1,517)] (Table 3, Figure 3).
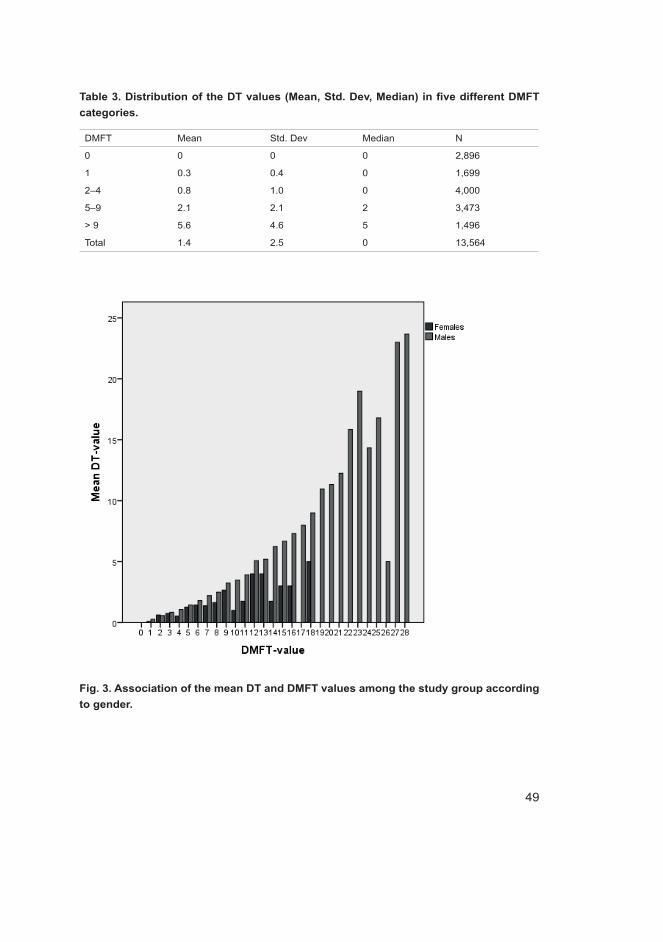
49
Table 3. Distribution of the DT values (Mean, Std. Dev, Median) in five different DMFT categories.
DMFT Mean Std. Dev Median N
0 0 0 0 2,896
1 0.3 0.4 0 1,699
2–4 0.8 1.0 0 4,000
5–9 2.1 2.1 2 3,473
> 9 5.6 4.6 5 1,496
Total 1.4 2.5 0 13,564
Fig. 3. Association of the mean DT and DMFT values among the study group according to gender.
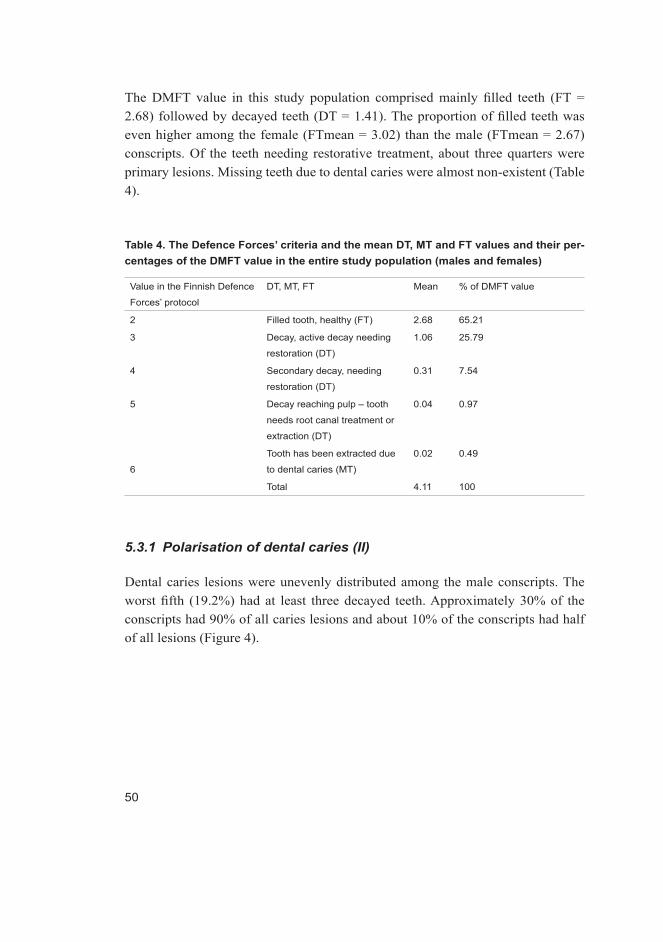
50
The DMFT value in this study population comprised mainly filled teeth (FT = 2.68) followed by decayed teeth (DT = 1.41). The proportion of filled teeth was even higher among the female (FTmean = 3.02) than the male (FTmean = 2.67) conscripts. Of the teeth needing restorative treatment, about three quarters were primary lesions. Missing teeth due to dental caries were almost non-existent (Table 4).
Table 4. The Defence Forces’ criteria and the mean DT, MT and FT values and their per-centages of the DMFT value in the entire study population (males and females)
Value in the Finnish Defence
Forces’ protocol
DT, MT, FT Mean % of DMFT value
2 Filled tooth, healthy (FT) 2.68 65.21
3 Decay, active decay needing
restoration (DT)
1.06 25.79
4 Secondary decay, needing
restoration (DT)
0.31 7.54
5 Decay reaching pulp – tooth
needs root canal treatment or
extraction (DT)
0.04 0.97
6
Tooth has been extracted due
to dental caries (MT)
0.02 0.49
Total 4.11 100
5.3.1 Polarisation of dental caries (II)
Dental caries lesions were unevenly distributed among the male conscripts. The worst fifth (19.2%) had at least three decayed teeth. Approximately 30% of the conscripts had 90% of all caries lesions and about 10% of the conscripts had half of all lesions (Figure 4).
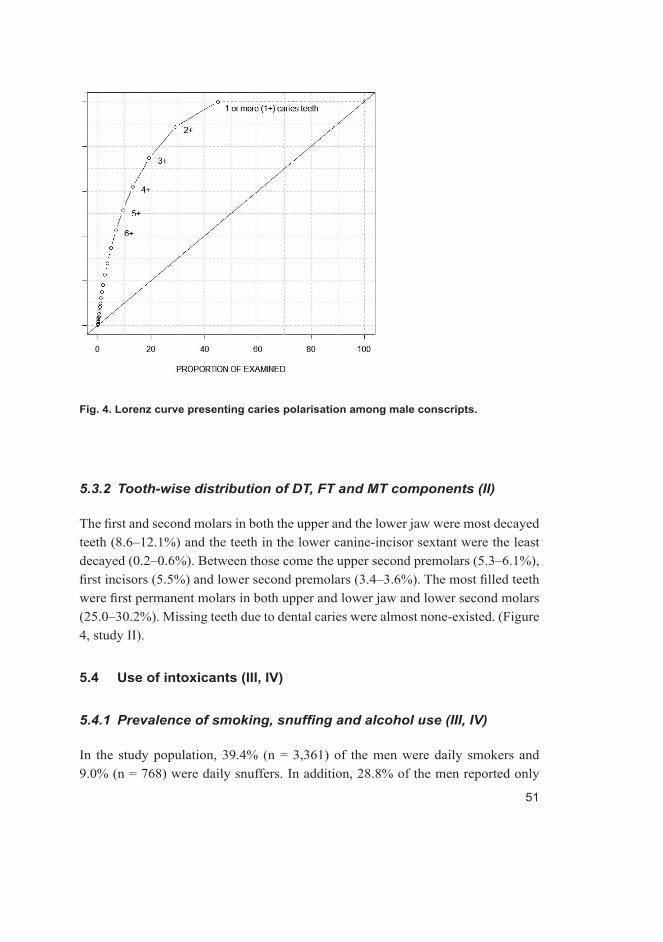
51
Fig. 4. Lorenz curve presenting caries polarisation among male conscripts.
5.3.2 Tooth-wise distribution of DT, FT and MT components (II)
The first and second molars in both the upper and the lower jaw were most decayed teeth (8.6–12.1%) and the teeth in the lower canine-incisor sextant were the least decayed (0.2–0.6%). Between those come the upper second premolars (5.3–6.1%), first incisors (5.5%) and lower second premolars (3.4–3.6%). The most filled teeth were first permanent molars in both upper and lower jaw and lower second molars (25.0–30.2%). Missing teeth due to dental caries were almost none-existed. (Figure 4, study II).
5.4 Use of intoxicants (III, IV)
5.4.1 Prevalenceofsmoking,snuffingandalcoholuse(III,IV)
In the study population, 39.4% (n = 3,361) of the men were daily smokers and 9.0% (n = 768) were daily snuffers. In addition, 28.8% of the men reported only
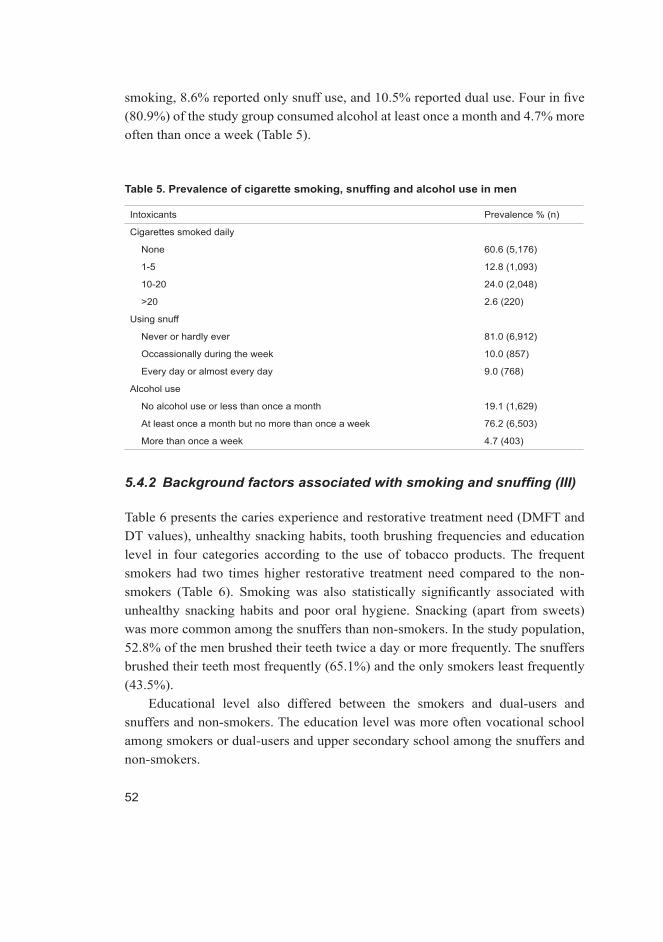
52
smoking, 8.6% reported only snuff use, and 10.5% reported dual use. Four in five (80.9%) of the study group consumed alcohol at least once a month and 4.7% more often than once a week (Table 5).
Table 5. Prevalence of cigarette smoking, snuffing and alcohol use in men
Intoxicants Prevalence % (n)
Cigarettes smoked daily
None 60.6 (5,176)
1-5 12.8 (1,093)
10-20 24.0 (2,048)
>20 2.6 (220)
Using snuff
Never or hardly ever 81.0 (6,912)
Occassionally during the week 10.0 (857)
Every day or almost every day 9.0 (768)
Alcohol use
No alcohol use or less than once a month 19.1 (1,629)
At least once a month but no more than once a week 76.2 (6,503)
More than once a week 4.7 (403)
5.4.2 Backgroundfactorsassociatedwithsmokingandsnuffing(III)
Table 6 presents the caries experience and restorative treatment need (DMFT and DT values), unhealthy snacking habits, tooth brushing frequencies and education level in four categories according to the use of tobacco products. The frequent smokers had two times higher restorative treatment need compared to the non-smokers (Table 6). Smoking was also statistically significantly associated with unhealthy snacking habits and poor oral hygiene. Snacking (apart from sweets) was more common among the snuffers than non-smokers. In the study population, 52.8% of the men brushed their teeth twice a day or more frequently. The snuffers brushed their teeth most frequently (65.1%) and the only smokers least frequently (43.5%).
Educational level also differed between the smokers and dual-users and snuffers and non-smokers. The education level was more often vocational school among smokers or dual-users and upper secondary school among the snuffers and non-smokers.

53
Table 6. The mean DT and DMFT values, prevalence (%) of unhealthy snacking habits (crisps, soft drinks, energy drinks), tooth brushing frequencies and education levels in four categories according to the use of tobacco products; n = 8,537.
Associated variables No smoking
& no
snuffing
n = 4,445
(52.1%)
Smoking
but no
snuffing
n = 2,467
(28.9%)
No smoking
but snuffing
n = 731
(8.6%)
Smoking &
snuffing
n = 894
(10.5%)
P-value
Mean DT (SD) 1.07 (2.05) 2.23 (3.29) 1.03 (1.67) 1.94 (2.89) < 0.001
Mean DMFT (SD) 3.55 (3.78) 5.43 (4.85) 3.79 (3.59) 4.98 (4.40) < 0.001
Eating sweets at least
occasionally
during the week (%)
(n = 6,232)
75.7 70.7 69.6 72.9 < 0.001
Eating crisps at least
occasionally during the week
(%) (n = 5,071)
55.6 64.6 57.2 65.5 < 0.001
Drinking soft drinks at least
occasionally during the week
(%) (n = 7,419)
83.4 91.6 86.7 91.9 < 0.001
Drinking energy drinks at
least occasionally during the
week (%) (n = 4,405)
39.2 64.5 60.7 70.5 < 0.001
Brushing teeth (%)
at least two times daily
(n = 4,508)
55.9 43.5 65.1 53.0
once a day (n = 3,133) 35.5 41.1 28.2 37.4
less frequently than daily
(n = 896)
8.6 15.4 6.7 9.6 < 0.001
Education (%)
Vocational school (n = 3,756) 35.1 59.5 38.6 50.3
Matriculation exam or upper
secondary school
(n = 3,500)
55.1 18.5 48.0 26.8
Other
(n = 1,281)
9.8 21.9 13.4 22.8 < 0.001

54
According to the generalised linear mixed model, smoking was associated with other harmful health behaviours such as snuffing, consuming energy or soft drinks, eating potato chips, and brushing teeth less than twice a day. The odds for smoking decreased significantly with high educational status (Table 7). The smoking frequencies between the provinces or between the urban and rural areas were similar, and the language of the municipality of residence was not associated with smoking either. The odds for the use of snuff were significantly higher among those smoking, using energy drinks or living in urban areas. Furthermore, living in the Western Finland border provinces and Swedish speaking municipalities increased the risk of using snuff (Table 7, Figure 5). Brushing teeth two times a day or more often was associated with snuffing. The risk factors did not have combined effects on the restorative treatment need, smoking and snuffing.

55
Table 7. Odds ratios and 95% confidence intervals (95% CI) from generalised linear mixed model for smoking and snuffing.
Smoking Snuffing
Explanatory factor OR 95% CI OR 95% CI
Smoking - 2.07 (1.82, 2.34)
Snuffing 2.09 (1.85, 2.37) -
Energy drinks 2.06 (1.85, 2.28) 1.94 (1.71, 2.21)
Soft drinks 1.35 (1.14, 1.60) 1.02 (0.84, 1.24)
Crisps 1.03 (0.93, 1.15) 0.95 (0.84, 1.07)
Tooth brushing
Two times or more daily
Daily
Less frequently than daily
1
1.31
1.41
(1.18, 1.46)
(1.20, 1.66)
1
0.73
0.58
(0.64, 0.83)
(0.47, 0.72)
Rural 1.12 (0.98, 1.28) 0.77 (0.67, 0.90)
Language of home municipality
Finnish
Mainly Finnish
Mainly Swedish
or Swedish only
1
1.15
1.15
(0.90, 1.61)
(0.80, 2.15)
1
1.39
2.40
(1.05, 1.85)
(1.52, 3.79)
Education
Vocational school
Matriculation exam or upper secondary school
Other
1
0.26
1.32
(0.23, 0.29)
(1.15, 1.51)
1
1.09
1.18
(0.95, 1.25)
(1.00, 1.39)
Province
Varsinais-Suomi
Lapland
Ostrobothnia
North Ostrobothnia
Kanta-Häme
Satakunta
South Karelia
Central Ostrobothnia
Pirkanmaa
Central Finland
Uusimaa
North Savo
Kainuu
South Ostrobothnia
North Karelia
South Savo
Päijät-Häme
Kymenlaakso
1
1.36
1.02
1.93
1.20
1.08
1.96
1.77
1.32
1.16
1.39
1.85
1.65
1.41
1.62
1.93
1.86
1.57
(0.93, 1.97)
(0.63, 1.64)
(1.35, 2.75)
(0.77, 1.87)
(0.77, 1.52)
(1.13, 3.40)
(0.99, 3.16)
(0.96, 1.83)
(0.82, 1.65)
(1.04, 1.85)
(1.26, 2.71)
(0.91, 2.98)
(0.99, 2.00)
(1.05, 2.50)
(1.22, 3.05)
(1.24, 2.78)
(0.93, 2.65)
1
2.24
1.70
1.58
1.16
1.09
0.87
0.80
0.95
0.83
0.86
0.91
0.51
0.50
0.56
0.49
0.52
0.33
(1.65, 1.86)
(1.07, 2.72)
(1.17, 2.13)
(0.73, 1.86)
(0.75, 1.57)
(0.44, 1.70)
(0.40, 1.62)
(0.67, 1.33)
(0.59, 1.18)
(0.65, 1.14)
(0.61, 1.34)
(0.21, 1.23)
(0.32, 0.78)
(0.35, 0.89)
(0.28, 0.86)
(0.33, 0.84)
(0.15, 0.72)
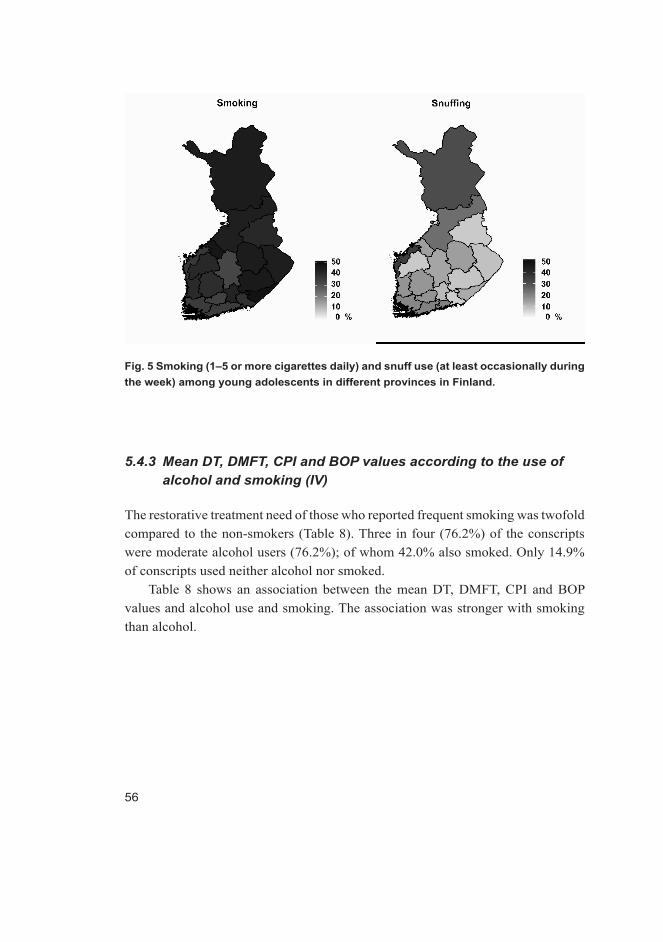
56
Fig. 5 Smoking (1–5 or more cigarettes daily) and snuff use (at least occasionally during the week) among young adolescents in different provinces in Finland.
5.4.3 Mean DT, DMFT, CPI and BOP values according to the use of alcohol and smoking (IV)
The restorative treatment need of those who reported frequent smoking was twofold compared to the non-smokers (Table 8). Three in four (76.2%) of the conscripts were moderate alcohol users (76.2%); of whom 42.0% also smoked. Only 14.9% of conscripts used neither alcohol nor smoked.
Table 8 shows an association between the mean DT, DMFT, CPI and BOP values and alcohol use and smoking. The association was stronger with smoking than alcohol.
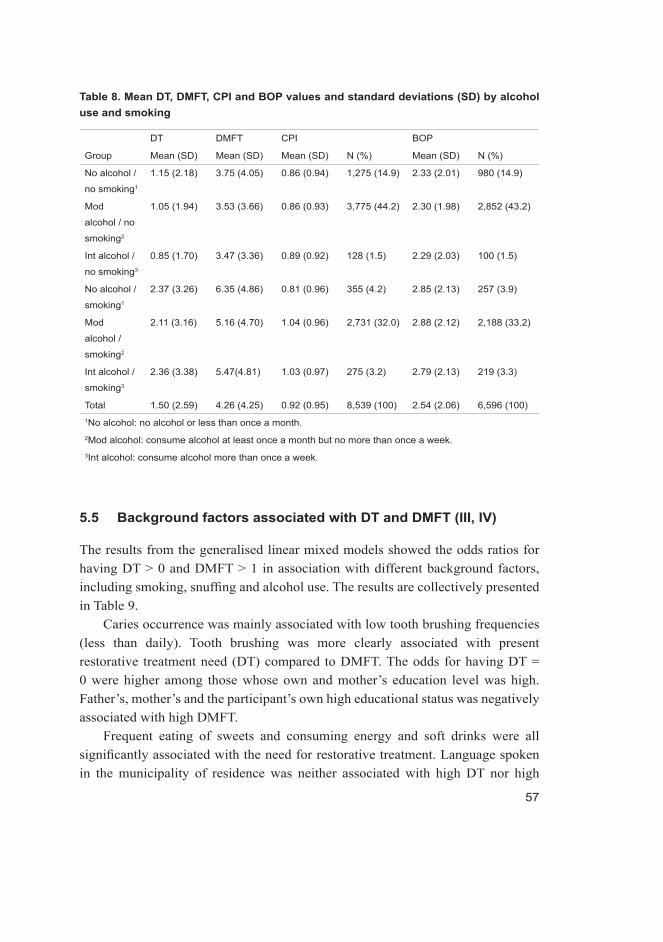
57
Table 8. Mean DT, DMFT, CPI and BOP values and standard deviations (SD) by alcohol use and smoking
DT DMFT CPI BOP
Group Mean (SD) Mean (SD) Mean (SD) N (%) Mean (SD) N (%)
No alcohol /
no smoking1
1.15 (2.18) 3.75 (4.05) 0.86 (0.94) 1,275 (14.9) 2.33 (2.01) 980 (14.9)
Mod
alcohol / no
smoking2
1.05 (1.94) 3.53 (3.66) 0.86 (0.93) 3,775 (44.2) 2.30 (1.98) 2,852 (43.2)
Int alcohol /
no smoking3
0.85 (1.70) 3.47 (3.36) 0.89 (0.92) 128 (1.5) 2.29 (2.03) 100 (1.5)
No alcohol /
smoking1
2.37 (3.26) 6.35 (4.86) 0.81 (0.96) 355 (4.2) 2.85 (2.13) 257 (3.9)
Mod
alcohol /
smoking2
2.11 (3.16) 5.16 (4.70) 1.04 (0.96) 2,731 (32.0) 2.88 (2.12) 2,188 (33.2)
Int alcohol /
smoking3
2.36 (3.38) 5.47(4.81) 1.03 (0.97) 275 (3.2) 2.79 (2.13) 219 (3.3)
Total 1.50 (2.59) 4.26 (4.25) 0.92 (0.95) 8,539 (100) 2.54 (2.06) 6,596 (100)1No alcohol: no alcohol or less than once a month.2Mod alcohol: consume alcohol at least once a month but no more than once a week.3Int alcohol: consume alcohol more than once a week.
5.5 Background factors associated with DT and DMFT (III, IV)
The results from the generalised linear mixed models showed the odds ratios for having DT > 0 and DMFT > 1 in association with different background factors, including smoking, snuffing and alcohol use. The results are collectively presented in Table 9.
Caries occurrence was mainly associated with low tooth brushing frequencies (less than daily). Tooth brushing was more clearly associated with present restorative treatment need (DT) compared to DMFT. The odds for having DT = 0 were higher among those whose own and mother’s education level was high. Father’s, mother’s and the participant’s own high educational status was negatively associated with high DMFT.
Frequent eating of sweets and consuming energy and soft drinks were all significantly associated with the need for restorative treatment. Language spoken in the municipality of residence was neither associated with high DT nor high

58
DMFT values. Living in a rural area increased the risk of the occurrence of dental caries compared with living in a city. Living in an area where the fluoride level in drinking water was more than 0.3 mg/ml was a protective factor against dental caries. Regular dental attendance was positively associated with high DMFT values but negatively with high DT values (Table 9).
5.5.1 Effect of the use of intoxicants on DT and DMFT (III, IV)
Smoking was associated both with the restorative treatment need and with DMFT and the odds for having caries lesions increased with the increasing number of daily cigarettes. Using snuff did not affect the occurrence of dental caries lesions but it had a slight association with a high DMFT index. Alcohol use was associated neither with present restorative treatment need nor with DMFT (Table 9).
Table 9. Odds ratios and 95% confidence intervals (95% CI) from generalised linear mixed model for DT > 0 and DMFT > 1according to the different explanatory factors.
DT > 0 (n = 3,912) DMFT > 1 (n = 5,579)
Explanatory factor OR (95% CI) OR (95% CI)
Brushing
Two times or more daily
Daily
Less frequently than daily
1
1.18 (1.07, 1.30)
1.98 (1.69, 2.31)
1
1.03 (0.93, 1.14)
1.59 (1.33, 1.90)
Alcohol
No alcohol or less than once a month
At least once a month, no more than
once a week
More than once a week
1
0.90 (0.80, 1.02)
0.83 (0.65, 1.05)
1
0.97 (0.85, 1.09)
1.06 (0.82, 1.38)
Smoking
No
1–5 cigarettes daily
More than 10 cigarettes daily
1
1.57 (1.37, 1.81)
1.63 (1.45, 1.83)
1
1.28 (1.10, 1.49)
1.50 (1.32, 1.70)
Snuffing 1.06 (0.94, 1.19) 1.18 (1.04, 1.35)
Eating sweets 1.22 (1.10, 1.37) 1.29 (1.15, 1.44)
Consuming energy drinks 1.13 (1.02, 1.25) 1.14 (1.03, 1.26)
Consuming soft drinks 1.16 (1.00, 1.34) 1.21 (1.04, 1.40)
Eating crisps 0.96 (0.87, 1.07) 0.95 (0.86, 1.06)
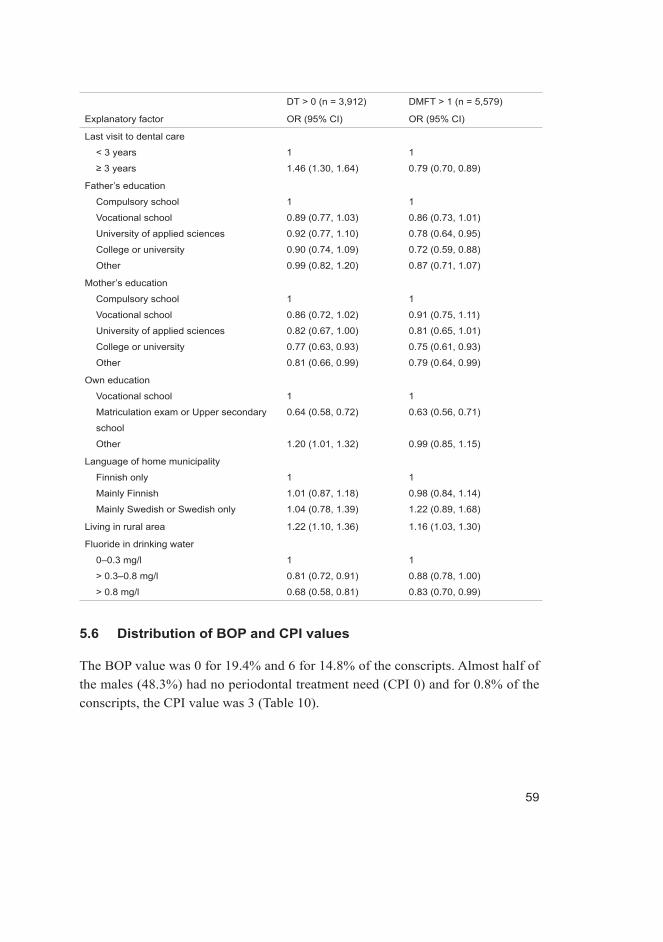
59
DT > 0 (n = 3,912) DMFT > 1 (n = 5,579)
Explanatory factor OR (95% CI) OR (95% CI)
Last visit to dental care
< 3 years
≥ 3 years
1
1.46 (1.30, 1.64)
1
0.79 (0.70, 0.89)
Father’s education
Compulsory school
Vocational school
University of applied sciences
College or university
Other
1
0.89 (0.77, 1.03)
0.92 (0.77, 1.10)
0.90 (0.74, 1.09)
0.99 (0.82, 1.20)
1
0.86 (0.73, 1.01)
0.78 (0.64, 0.95)
0.72 (0.59, 0.88)
0.87 (0.71, 1.07)
Mother’s education
Compulsory school
Vocational school
University of applied sciences
College or university
Other
1
0.86 (0.72, 1.02)
0.82 (0.67, 1.00)
0.77 (0.63, 0.93)
0.81 (0.66, 0.99)
1
0.91 (0.75, 1.11)
0.81 (0.65, 1.01)
0.75 (0.61, 0.93)
0.79 (0.64, 0.99)
Own education
Vocational school
Matriculation exam or Upper secondary
school
Other
1
0.64 (0.58, 0.72)
1.20 (1.01, 1.32)
1
0.63 (0.56, 0.71)
0.99 (0.85, 1.15)
Language of home municipality
Finnish only
Mainly Finnish
Mainly Swedish or Swedish only
1
1.01 (0.87, 1.18)
1.04 (0.78, 1.39)
1
0.98 (0.84, 1.14)
1.22 (0.89, 1.68)
Living in rural area 1.22 (1.10, 1.36) 1.16 (1.03, 1.30)
Fluoride in drinking water
0–0.3 mg/l
> 0.3–0.8 mg/l
> 0.8 mg/l
1
0.81 (0.72, 0.91)
0.68 (0.58, 0.81)
1
0.88 (0.78, 1.00)
0.83 (0.70, 0.99)
5.6 Distribution of BOP and CPI values
The BOP value was 0 for 19.4% and 6 for 14.8% of the conscripts. Almost half of the males (48.3%) had no periodontal treatment need (CPI 0) and for 0.8% of the conscripts, the CPI value was 3 (Table 10).
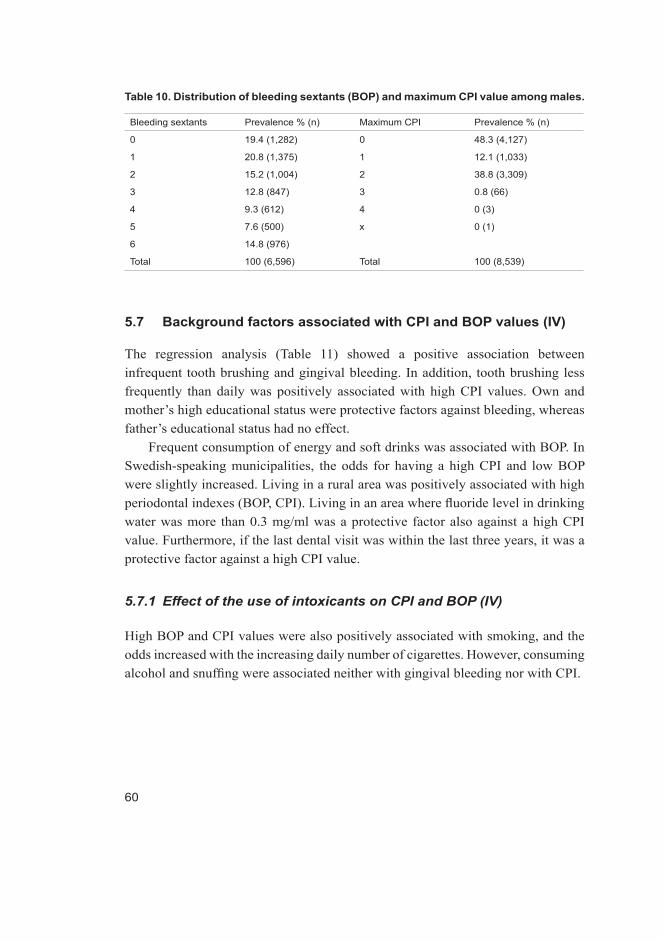
60
Table 10. Distribution of bleeding sextants (BOP) and maximum CPI value among males.
Bleeding sextants Prevalence % (n) Maximum CPI Prevalence % (n)
0 19.4 (1,282) 0 48.3 (4,127)
1 20.8 (1,375) 1 12.1 (1,033)
2 15.2 (1,004) 2 38.8 (3,309)
3 12.8 (847) 3 0.8 (66)
4 9.3 (612) 4 0 (3)
5 7.6 (500) x 0 (1)
6 14.8 (976)
Total 100 (6,596) Total 100 (8,539)
5.7 Background factors associated with CPI and BOP values (IV)
The regression analysis (Table 11) showed a positive association between infrequent tooth brushing and gingival bleeding. In addition, tooth brushing less frequently than daily was positively associated with high CPI values. Own and mother’s high educational status were protective factors against bleeding, whereas father’s educational status had no effect.
Frequent consumption of energy and soft drinks was associated with BOP. In Swedish-speaking municipalities, the odds for having a high CPI and low BOP were slightly increased. Living in a rural area was positively associated with high periodontal indexes (BOP, CPI). Living in an area where fluoride level in drinking water was more than 0.3 mg/ml was a protective factor also against a high CPI value. Furthermore, if the last dental visit was within the last three years, it was a protective factor against a high CPI value.
5.7.1 Effect of the use of intoxicants on CPI and BOP (IV)
High BOP and CPI values were also positively associated with smoking, and the odds increased with the increasing daily number of cigarettes. However, consuming alcohol and snuffing were associated neither with gingival bleeding nor with CPI.

61
Table 11. Odds ratios and 95% confidence intervals (95% CI) from generalised linear mixed model for DT > 0 and DMFT > 1 for bleeding on probing (BOP >2) and Community Periodontal Index (CPI>2) according to different explanatory factors.
Explanatory factor BOP > 2 (n = 2,881)
OR (95% CI)
CPI ≥ 2 (n = 5,465)
OR (95% CI)
Brushing
Two times or more daily
Daily
Less frequently than daily
1
1.23 (1.11, 1.38)
2.32 (1.94, 2.77)
1
1.02 (0.92, 1.12)
1.19 (1.01, 1.40)
Alcohol
No alcohol or less than once a month
At least once a month, no more than
once a week
More than once a week
1
1.00 (0.87, 1.14)
0.88 (0.68, 1.15)
1
1.05 (0.93, 1.19)
1.00 (0.78, 1.28)
Smoking
No
1–5 cigarettes daily
More than 10 cigarettes daily
1
1.19 (1.01, 1.40)
1.45 (1.28, 1.65)
1
1.33 (1.15, 1.54)
1.86 (1.64, 2.11)
Snuffing 0.96 (0.84. 1.10) 1.06 (0.94. 1.20)
Eating sweets 1.02 (0.90, 1.16) 0.85 (0.76, 0.95)
Consuming energy drinks 1.13 (1.01, 1.26) 1.00 (0.90, 1.11)
Consuming soft drinks 1.24 (1.05, 1.47) 0.99 (0.86, 1.15)
Eating crisps 1.01 (0.90, 1.13) 1.00 (0.90, 1.11)
Last visit to dental care
< 3 years
≥ 3 years
1
1.12 (0.98, 1.28)
1
1.37 (1.21, 1.55)
Father’s education
Compulsory school
Vocational school
University of applied sciences
College or university
Other
1
0.93 (0.79, 1.09)
0.96 (0.78, 1.18)
0.93 (0.75, 1.15)
1.06 (0.86, 1.31)
1
1.06 (0.91, 1.23)
1.06 (0.88, 1.27)
1.24 (1.02, 1.50)
1.05 (0.87, 1.28)
Mother’s education
Compulsory school
Vocational school
University of applied sciences
College or university
Other
1
0.84 (0.69, 1.02)
0.81 (0.65, 1.01)
0.77 (0.62, 0.96)
0.75 (0.60, 0.94)
1
0.85 (0.70, 1.02)
0.76 (0.62, 0.93)
0.82 (0.67, 1.01)
0.88 (0.71, 1.09)
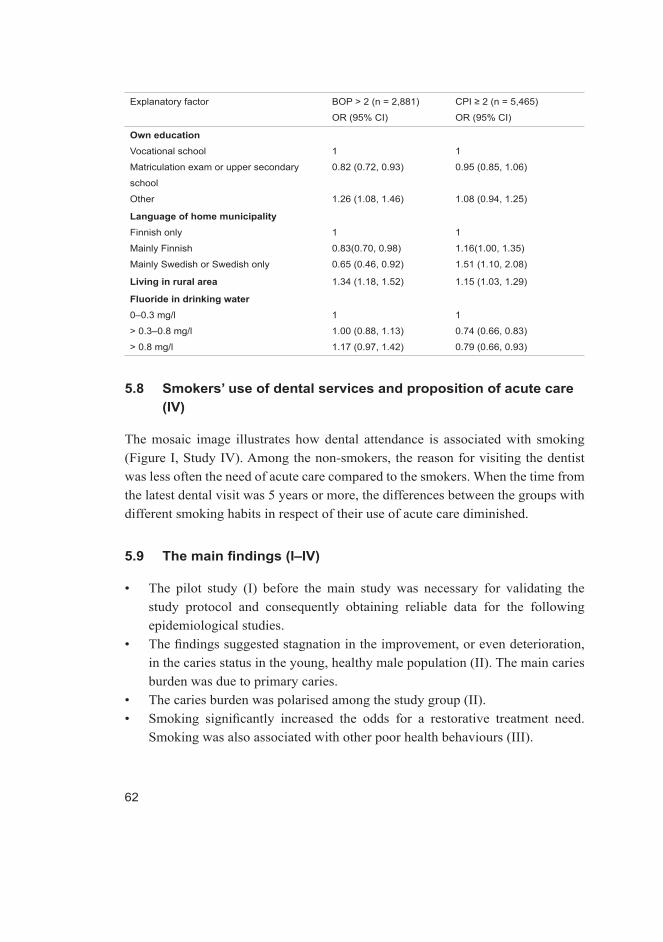
62
Explanatory factor BOP > 2 (n = 2,881)
OR (95% CI)
CPI ≥ 2 (n = 5,465)
OR (95% CI)
Own educationVocational school
Matriculation exam or upper secondary
school
Other
1
0.82 (0.72, 0.93)
1.26 (1.08, 1.46)
1
0.95 (0.85, 1.06)
1.08 (0.94, 1.25)
Language of home municipalityFinnish only
Mainly Finnish
Mainly Swedish or Swedish only
1
0.83(0.70, 0.98)
0.65 (0.46, 0.92)
1
1.16(1.00, 1.35)
1.51 (1.10, 2.08)
Living in rural area 1.34 (1.18, 1.52) 1.15 (1.03, 1.29)
Fluoride in drinking water0–0.3 mg/l
> 0.3–0.8 mg/l
> 0.8 mg/l
1
1.00 (0.88, 1.13)
1.17 (0.97, 1.42)
1
0.74 (0.66, 0.83)
0.79 (0.66, 0.93)
5.8 Smokers’ use of dental services and proposition of acute care (IV)
The mosaic image illustrates how dental attendance is associated with smoking (Figure I, Study IV). Among the non-smokers, the reason for visiting the dentist was less often the need of acute care compared to the smokers. When the time from the latest dental visit was 5 years or more, the differences between the groups with different smoking habits in respect of their use of acute care diminished.
5.9 The main findings (I–IV)
• The pilot study (I) before the main study was necessary for validating the study protocol and consequently obtaining reliable data for the following epidemiological studies.
• The findings suggested stagnation in the improvement, or even deterioration, in the caries status in the young, healthy male population (II). The main caries burden was due to primary caries.
• The caries burden was polarised among the study group (II).• Smoking significantly increased the odds for a restorative treatment need.
Smoking was also associated with other poor health behaviours (III).

63
• Snuffing was not associated with caries prevalence in the study group. The snuffers had better health habits compared to the smokers. The use of snuff was associated with the geographical location of the place of residence (III).
• The effect of the place of residence on caries experience remained, but the impact decreased when health behaviour factors were included in the statistical analyses (III).
• Consuming alcohol was not associated with caries experience and BOP in the studied population (IV).
• The participant’s own and mother’s education level were associated with their oral health (III, IV).
• The smokers used dental services more rarely than the non-smokers and the reason for their visit was more often toothache than among the non-smokers (IV).
64

65
6 DiscussionMandatory military service with obligatory health screening in Finland provides an excellent opportunity to conduct epidemiological studies on specific age cohorts; in this nationwide study on those born in the early 1990s. Hence, a great advantage of the present study is its uniquely large study population, representative of the healthy, young Finnish males. The study population of 13,564 men comprised 13.5% of the total size of the male birth cohorts (100,502) born between 1990 and 1992, and 53.7% of all the males born in 1990–1992 who entered the military service in 2011. The total number of conscripts in 2011 was 26,492 (born in 1983–1993) of which 96.9% were born in 1990–1992 (25,243 men, 428 women).
The number of those men not entering the military service or entering civil service instead of the military one is approximately 1,700 annually. The reason for not entering the service is most often problems with the physical or mental health. Mental problems (Kisely et al. 2011) are associated with the restorative treatment need and the same is true for asthma (Alavaikko et al. 2011) and juvenile diabetes (Twetman et al. 2002). Those are also the large subgroups exempted from the military service. Therefore, the oral health situation among young men may actually be even worse than presented here. The mean DT and DMFT values would have probably been even higher if those groups were included in the study population.
The proportion of those choosing the civil service (7.0% of men in that age group) instead of the military service has increased in Finland (Siilasmaa et al. 2010). These facts must be kept in mind when considering the outcome of this study and they could be topics for future study.
6.1 Validation of the epidemiological study (I)
According to the pilot study, the study protocol and obtaining the data had no major deficiencies. A standardised protocol, guidelines, calibration, and radiological education of the dentists were, however, emphasised. Following the WHO guidelines (1997) and the simple protocol of the Finnish Defence Forces, could be accomplished a cross-sectional national epidemiological study during the mandatory military service of conscripts.

66
6.1.1 Randomisation (I–IV)
The pilot study enabled to determine that all conscripts can be inspected in all but five garrisons (Kajaani, Säkylä, Vekaranjärvi, Parola and Riihimäki). This means that the oral health and health behaviours of more than 14,000 draftees could be analysed. In the theses of both Ankkuriniemi (1979) and Läärä (1999), similar random samplings were used. The numbers of the participants were 3,936 and 2,850, respectively. Thus, the number of the participants in the present study considerably exceeds those earlier studies, ensuring its reliability in all parts of the country. Any other type of randomisation would have been complicated because the oral inspection was a part of the health inspection with a strict time limit. Female and male conscripts serve in the same units, so randomisation included both genders. The study protocol allowed data on the female conscripts to be investigated separately because the proportion of the female conscripts was small. However, generalisation was not possible due to the small sample size.
In the epidemiological study, the study group was randomized as planned after the pilot study. Three garrisons of county of Kymeenlaakso (Hamina, Lappeenranta, Kotka) and one from county of North Karelia (Onttola) were excluded from the study because of the limited personnel resources. However, those garrisons were small, and the total number of conscripts serving in them did not exceed 600. Therefore, the bias in the results caused by the exclusion of the participants can be considered minimal. From these counties other garrisons (2+1) were included. In addition, the oral health examination was obligatory and carried out during the first week of the military service. This limited the number of the dropouts to a minimum, increasing the value of this study.
6.1.2 Validation of the examiners (II)
Screening of the dental treatment need of the conscripts entering the service has been part of the Defence Forces’ protocol for decades. Practically all examiners were experienced and most were at least familiar with the protocol and criteria, which helped to manage the tight schedule. Again the mean time spent for the clinical oral inspection was short, less than 3 minutes which might have affected the quality of the caries registration. The existing protocol was easily converted into a collection of data valid for research purposes by training and calibrating the examiners and introducing them to the WHO criteria for epidemiological studies (1997). The good intra- and inter-examiner agreement of examiners reinforcing
67
the validity of this study but it might have been better to use clinical calibration. Otherwise Piovesan et al. (2013) found that laboratorial training of examiners for using a visual caries detection system in epidemiological study was feasible. However, the short and simultaneous screening period (about one week) and long distances between the garrisons made impossible to use of a clinical golden standard during the examinations. In the research of Ankkuriniemi (1979), the calibration was carried out clinically, but the research of Läärä (1999) did not include any calibration. However, a large enough dataset collected from public health records by non-calibrated examiners is not inferior to those obtained from examinations by calibrated examiners (Hausen et al. 2001). It can therefore be concluded that the way data was collected in this study produced reliable and useful data for investigating the oral health of young males. In addition, the results are comparable with the results of the previous studies on Finnish conscripts (Ankkuriniemi 1979, Läärä 1999).
6.1.3 Validation of the study protocol (I–IV)
The time limit in the dental inspection per draftee allows estimating the need for restorative treatment tooth-wise (DMFT, DT). The lack of the study protocol was that the examiners were not registered different stage of dental caries lesions only those that needing a restoration. So in truth, there must have been more caries, both clinically and radio-graphically. Both cariological findings and periodontal health were recorded as specified in the WHO criteria for epidemiological studies (WHO 1997). Data on wisdom teeth were excluded from the analyses because the need for treatment in them was generally registered as caries by some dentists in the Defence Forces, even in cases where the cause could have been, for example, pericoronitis. The outcome as to the restorative treatment need with and without wisdom teeth is different, as wisdom teeth become decayed easily. This issue was only detected afterwards and did not come up during the pilot study.
Recording BOP in the index teeth allows analysing the proportion of the infected areas. CPI had been recorded by military dentists before but BOP had not been used before. Therefore, the dentists had to be introduced to its use during the education sessions by a periodontologist. Some additional findings, such as the presence of traumatised and deciduous teeth as well as of active orthodontic treatment and piercings, were considered valuable and were included in the protocol after the pilot study.
68
In the pilot study, the recommendation was to take BW radiographs when clinically indicated, which allowed estimating the need for radiography as well as the time required by it. According to the pilot study, this would have meant radiography of about 40% of the conscripts, which was not possible within the time limit. Therefore in the epidemiological study following the pilot study, BW radiographs were taken only from every fifth draftee with a clinical indication for radiography. Conventional radiographs were taken in all but one garrison, where the system had been digitised. With respect to radiography, the dentists needed to be educated both technique and diagnostics practices before the field survey. The radiographs were also later analysed in detail by a radiologist.
6.1.4 Subjective treatment need (I)
According to the pilot study, the prevalence of self-estimated oral symptoms and the need for dental treatment were reasonably high (about 40% reported oral symptoms), considering that these youngsters had been entitled to dental care free of charge all their lives (Ministry of Social Affairs and Health 1972). The same was also true for clinical findings.
There was also a reason to believe that caries still exists because the oral health behaviour of young adults has not been beneficial during the 1990s and the first decade of the 2000s, but rather the opposite (Anttonen et al. 2008, 2011). The generation concerned had also suffered from the reductions in the oral health promotion resources carried out in the early 1990s. There are no recent epidemiological studies available on young adults, as the latest one was performed 15 years ago (Läärä 1999.) This study also indicated, as proposed by Marthaler (2004), that research is needed to investigate the occurrence of caries in the industrialised world in an era after a strong decline in the prevalence of caries. According to these views, together with the alarming findings of the pilot study, a national epidemiological study on young adults was considered indicated and most valuable.
6.1.5 Validation of the questionnaire (I, III, IV)
The pilot study revealed that answering the questionnaire took three times longer than the clinical examination. Therefore, the need of three computers per dentist was established to enable as many draftees as possible to answer the questionnaire. In the pilot study, the questionnaire was only available in Finnish. Because
69
Finland has two official languages, Finnish and Swedish, the questionnaire was also translated into Swedish after the pilot study. Also there was some lacks of the questionnaire which were noticed afterwards. There was no data collected on the use of fluoride toothpaste, which is very important in for dental caries. Also the question of smoking was categorised in inexact way when the option “5 to 10 cigarettes per day” was missing. Answering the questionnaire took place during the first two weeks in the military service when the military service, i.e. the change in the environment, had not yet affected the habits of the conscripts.
6.2 DT and DMFT among young adults (II)
According to the results of the present study, almost half of the Finnish young men born in the early 1990s had at least one tooth needing restorative treatment, even with third molars excluded. Women’s mean DMFT and DT values were lower compared to men’s and they had more restorations (higher FT values than men), indicating their higher dental attendance and treatment rate. In the Health 2000 survey, the mean DT of men (1.4) was double to that of women (0.7) (Suominen-Taipale et al. 2008), which is in accordance with the findings in the present study (1.4 v. 0.8). However, the proportion of the female conscripts was very small. Since the military service is voluntary for women, they most likely do not form a representative sample as to their oral health and, therefore, generalisations must be avoided.
In the present study, the mean DMFT value (4.1) was smaller than in the studies by Läärä (6.8) (1999) and Ankkuriniemi (15.8) (1979). It must be reminded that in Ankkuriniemi’s and Läärä’s studies the third molars were included in the analyses but in the present study they were not. Thus, the results are not directly comparable. The proportion of the conscripts with DT= 0 was 54.9% (wisdom teeth excluded) in this study which is more than respective figure in study by Ankkuriniemi [(23.7%) 1979], and almost same as in the study by Läärä [(44.0%) 1999]. In the Health 2000 survey (Suominen-Taipale et al. 2008), the mean DT value for men was 1.0 and for women 0.3 among 30–44 year olds. Compared to Health 2000 survey (Suominen-Taipale et al. 2008), the caries status was worse in our study group even though the conscripts here were over 10 years younger at the time of the examination. According to the first results from the Health 2011 survey (Suominen et al. 2012), the caries status of Finnish men (30–44 years old) has become slightly worse during the last decade. In 2000, about one-third (29.0%) had at least one tooth needing restorative treatment (Suominen-Taipale et al. 2008) when the corresponding figure
70
in 2011 was 35.0% (Suominen et al. 2012). This could be a sign of deterioration of young males’ oral health. The reason for that can be speculated: the 1970s and 1980s are regarded as the era of health promotion, in particular among children (Nordblad et al. 2004). The youngest age group in the Oral Health 2000 survey lived their school age and teenage during this period, which can also be seen in their oral health situation now. In comparison, the present study group lived their childhood at a time of the economic recession when resources also for oral health promotion were reduced. Good oral health of the young has been regarded as a truism. Simultaneously, dietary changes (Popkin 2006) have taken place and tooth brushing frequency still stays low (Honkala et al. 2015).
Mandatory military service similar to that in Finland exists in Israel, Greece and Turkey but has been replaced by professional military forces in most Western countries (Siilasmaa et al. 2010). According to the results of the present study, caries prevalence among Finnish conscripts was at the same level as among conscripts in Brazil (Bastos et al. 2007) and in Australia (Hopcraft et al. 2009) but lower than among conscripts in Israel (Levin &Shenkman 2004), Turkey (Ceylan et al. 2004) and Croatia (Skec et al. 2006).
6.2.1 Caries polarisation (II)
In the present study, one-third of the study group carried 90% of the total caries burden and the worst 10% about half of it. Compared to the previous studies, polarisation was more pronounced than in the 1970s (Ankkuriniemi 1979) and similar to that in the 1990s (Läärä 1999) when the respective age cohorts were studied but distinctly weaker than in the Health 2000 study carried out on the Finnish adult (30–44 years) population (Suominen-Taipale et al. 2008). When the number of individuals with no cavities increases, the mean DMFT values decrease and polarisation becomes more pronounced (Sheiham & Sabbah 2010). This observation appears to be the case in the present study when compared to the Health 2000 study – the increased caries prevalence leads to less pronounced polarisation, which is also a sign of deterioration in the oral health of young males. In addition, the distribution of intact, filled, decayed and removed teeth in the present study were in accordance with the findings of Ankkuriniemi (1979) and Batchelor et al. (2004). The DT value here mainly consists of primary caries lesions (75.2% of all decayed teeth), which indicates a heavy treatment need also in the future.

71
6.3 BOP and CPI among young adults (IV)
BOP and CPI indexes were used to describe periodontal disease in this study. Using the highest CPI index to describe periodontal health is recommend by WHO (1997), but this has some limitations. CPI has been recommended for epidemiological surveys (WHO 1997) but not to studies on risk factors for periodontitis. Page & Eke (2007) described that CPI does not estimate the prevalence of periodontitis but it enables to estimate treatment need. A more detailed examination would be valuable but in the survey context, a cost-benefit evaluation needs to be taken into account (Cascaes et al. 2009). Albandar et al. (1998) found in follow-up studies among young adults that BOP is important signal and predict future periodontitis. In this study, BOP was available for 76.5% of the conscripts but the CPI value was available for the whole study group. The BOP scoring was included the protocol of the Finnish Defence Forces first time in this study (Table 2). Perhaps it was difficult to the dentists register it, even if it was taught in the calibration sessions.
According to a review article by Susin et al. (2014), the prevalence of aggressive periodontitis varies significantly between different geographic locations and between different ethnicities. In Northern Europe and Central Europe, the prevalence of aggressive periodontitis is 0.1% (Susin et al. 2014), which is almost same than the corresponding figure in this study. In a previous study from Finland, the prevalence of periodontitis has been 15.0% among adolescents (Heikkinen 2011), 9.6% among conscripts (Ankkuriniemi 1979) and 48% among adults aged 30–44 (Suominen-Taipale et al. 2008). In the Health 2000 survey (Suominen-Taipale et al. 2008), 68.0% of females and males in younger age groups had gingivitis, which is lower than the corresponding figure in this study (80.6%). The results of this study are closer to the results of international (Susin et al. 2014) rather than of national studies (Ankkuriniemi 1979, Suominen-Taipale et al. 2008, Heikkinen 2011). Possible reasons to this can only be speculated. Measurement methods and populations differ between the studies, which makes comparisons difficult. Different measurements cause also under-estimation or overestimation of real need for periodontal treatment (Costa et al. 2009). In this study, the BOP and CPI values were not in line with each other either, and it is difficult to determine which one would be more reliable. Zappa et al. (1995) investigated the reliability of single and double probing attachment level measurements and found that the false positive rate was significantly lower than the false negative rate. Thus, it can be estimated that the prevalence of periodontitis was at least 0.8% in this
72
study population. Although the prevalence of periodontitis may sound low, the population-based problem is significant since about one per cent of males in this age group already needs periodontal treatment.
6.4 Prevalence of smoking, snuffing and alcohol use (III, IV)
Hypothesis that the use of intoxicants in this age group may be at the same level, or even higher, as reported in previous studies in Finland (Kinnunen et al. 2013) seems to be true especially when concerning smoking and snuffing. Here, 80.9% consumed alcohol at least once a month, 39.6% were daily smokers and 19.0% used snuff occasionally or every day, when the corresponding figures in the study by Kinnunen et al. (2013) were 72.0%, 18.7% and 14.5% among 18-year-olds. The results of this study also support the finding that the trend is increasing: in Finland daily smoking has increased in the last decade among young men, which can be seen from the results from Bingham et al. (2010) (30.0%) and Mattila et al. (2012) (34.2%) and here (39.6%). Most adult smokers begin smoking before 18 years of age (U.S. Department of Health and Human Services 2012), which means that the increasing trend of smoking among Finnish young men should be taken seriously.
The level of alcohol use in this study (80.9%) was also similar than among Finnish male university students in 2011 (80.7%), but the level of smoking was significantly lower (9.5%) in the study by Pohjola et al. (2014). Randomisation and maximising the attendance to examinations with no dropouts can be considered to improve the reliability of the results in this study. In addition, the conscripts represent males from different parts of the country and from the different education levels. This may explain the differences between the results concerning smoking compared to previous studies from Finland (Bingham et al. 2010, Mattila et al. 2012, Pohjola et al. 2014). At the same time, studies from other countries show that smoking has decreased (Gallus et al. 2011, Filion et al. 2012, Hugoson et al. 2012, Verlato et al. 2014), except for among people with lower socioeconomic status (SES) (Filion et al. 2012, Verlato et al. 2014).
The timing of the on-going five-year project in the Finnish Defence Forces to support non-smoking and non-snuffing in military service (Siitonen & Heikkilä 2013) is good, considering the high levels of smoking and snuffing. In many garrisons, there is still a positive attitude towards smoking because it is thought to be part of the military culture. The change in habits also requires change in attitudes and culture (Siitonen & Heikkilä 2013). Preventive work should be done continuously and at every level of society.
73
6.5 Smoking, snuffing, dental caries and associated factors (III)
One of the main findings of this study was that the restorative treatment need among the smokers was higher, even two-fold, compared to the non-smokers. The dental caries experience of the dual-users was almost as poor as that of the smokers, whereas the caries occurrence of the snuffers and the non-users was almost the same. Smoking also seemed to associate with other harmful oral health behaviours like snacking and infrequent tooth brushing. Snuff use was also associated with snacking, but also with the most frequent tooth brushing compared to both the smokers and those neither smoking nor snuffing.
Our results are contradictory to those by Hugoson et al. (2012), who in 2003 found that there are no statistically significant differences in the restorative treatment need between the snuff users, smokers and non-users. In previous decades (1983 and 1993), findings similar to ours have been reported in cross-sectional studies, the dental caries experience being significantly lower among the snuffers than other groups (Hugoson et al. 2012).
It is good to notice that different kinds of smokeless tobacco products are used in different parts of the world, which means that the results of this study are only comparable to studies about the Swedish “lip snuff”. In addition, the study groups are not directly comparable as to the age of the participants and the sizes of the study population. In this study, the study population was considerably larger and younger than in the study by Hugoson et al. (2012). It would be important to get epidemiological data of Swedish snuff use also from other countries in Europe. There are only few studies of association between snuff use, dental caries and periodontal health among young adults and they all are from the Nordic countries. Further investigations are needed: follow-up studies would be valuable. Holmén et al. (2013) investigated the use of tobacco products (both cigarette smoking and snuff use) in their longitudinal study from Sweden. They found that the use of tobacco products are associated with increased caries prevalence among the young, irrespective of socioeconomic and geographic factors. Health habits of the young were not included in the analyses (Holmen et al. 2013).
The findings in this study are in accordance with previous studies where the non-smokers brushed their teeth more frequently than the smokers did (Hellqvist et al. 2009, Honkala et al. 2011). Here, the snuffers used more snacks, apart from sweets, compared to the non-smokers. Harmful dietary habits of snuffers have also been found in Sweden where the snuffers used less fruit and vegetables and more alcohol than the non-users (Engström et al. 2010).

74
The low restorative treatment need of snuffers is one of the most interesting finding in this study. Perhaps snuffers’ more favourable brushing habits is one explanation to that. Another reason could be that the salivary buffer capacity of snuffers is higher compared to non-users. Higher buffer capacity may favour remineralisation of caries lesions and promote inhibition of the cariogenic microflora. (Hugoson et al. 2012). According to the study by Hellqvist et al. (2012), some nicotine-containing snuffs increase the plaque pH, and some nicotine-free snuffs lower the pH. Therefore, pH changes may affect the caries risk both positively and negatively, depending on the product used (Hellqvist et al. 2012).
Snuffing was more common in the provinces near to the western borders of Finland and in urban areas, perhaps due to the easier access to the snuff products. It was hoped that the total ban of selling snuff in 1995 would end or at least decrease snuff use in Finland, but on the contrary, the increase in use continued (Huhtala et al. 2006). In Finland, it is possible to import snuff for personal use, and users usually import it from Sweden. This study and previous studies among young Finnish adults (Kinnunen et al. 2013) show that snuffing has increased over the past three decades. Perhaps snuffing is considered as less harmful than smoking (Lee 2011) and the negative health effects are poorly known. Snuff use is more common among physically active persons, and snuff use is suggested to be part of the culture in some sports clubs (Mattila et al. 2012). In particular in areas where snuff is easily available, it is also well accepted. Furthermore, Finland has banned smoking in several environments, such as educational establishments, workplaces and restaurants, which may have caused to increasing use of snuff.
Conversations around health effects of snuff use are complicated because there are no long-time follow-up studies of snuff use from a young age. In addition, dual use (snuff with other tobacco products) is relatively common (Kinnunen et al. 2013), which may interfere the research of health effects of snuff use. Roosar et al. (2008) followed a cohort up to 29 years and found that snuff use is not associated with an increased incidence of cancer overall but tentatively with an excess incidence of the combined category of oral and pharyngeal and of total smoking-related cancer. It is clear that snuff and other smokeless tobacco products are not products that would promote oral and general health. The health effects of snuff use should not be compared to effects of smoking but effects of non-use. Furthermore, it should be kept in mind that the health effects of smokeless tobacco differ between different products.
Among the present study population, the education level of 85.0% of the subjects was vocational school, matriculation exam or upper secondary school; therefore, the focus in the analyses was on them. The high education level of the
75
conscripts was a significant protective factor against smoking, but the educational background among the snuffers varies. Findings of this study are in accordance with study by Engström et al. (2010), who found that a low educational background is significantly more common among the smokers than the snuffers. Social determinants associated with smoking were not investigated in this study. Perhaps in the army, the surrounding community affects more individuals compared to the civilian world. The study by Schultz et al. (2007) proposes that unhealthy social norms provide people with no motivation to improve their health habits, and may even encourage those who have a healthy diet to change their health behaviour for the worse, i.e. to eating less healthy in an attempt to conform to the majority. A supportive environment, however, can encourage changing unhealthy eating habits to more positive (Burger et al. 2011). It is likely that the same phenomena can also be seen among other health behaviours such as smoking.
6.6 Background factors associated with DT, DMFT, BOP and CPI
6.6.1 Snacking and tooth brushing (III)
In this study, infrequent tooth brushing was the most and smoking the second most important factor associated with an increased risk of dental caries. In addition, frequent eating of unhealthy snacks increased the risk of caries experience. Unhealthy dietary and oral hygiene habits were associated with the risk of periodontal disease indicated by BOP and CPI. These findings are in line with previous studies which have reported that good oral hygiene and healthy diet are associated with good periodontal health (Bawadi et al. 2011, Tomofuji et al. 2011). Both clinical and epidemiologic studies indicate that microbial plaque is the direct cause of gingivitis (Beck & Arbes 2006). The role of food intake in caries development has been widely studied for decades, and its impact on oral health is beyond dispute. Most studies deal with the association of sugar and sugar substitutes with dental caries (Gupta et al. 2013, Moynihan & Kelly 2014). In addition, the frequencies of eating and snacking have been studied (Nguyen et al. 2008, Catteau et al. 2013). Catteau et al. (2013) found that the regular use of sweet snacks and/or sweet drinks was associated with high caries rate. Nguyen et al. (2008) found that regular healthy diet decreased the occurrence of caries.
Brushing teeth twice a day is the main preventive measure against dental caries and a common habit among the young in most European countries. The
76
tooth brushing frequency of Finnish young people, especially males, has stayed among the lowest in Europe (Maes et al. 2004, Honkala et al. 2012), as less than half of the young men in Finland brush their teeth twice a day. Here, about 53% of the conscripts (males) brushed their teeth twice a day, a figure slightly higher than in the recent previous study among 15-year-olds (Honkala et al. 2012). It has been shown that tooth brushing habit is adopted already in childhood and will not change easily later in life (Kuusela et al. 1996, Åstrøm & Jacobsen 1998, Åstrøm 2004). This study also supports the idea that a low tooth brushing frequency plays the most important role in caries development (the main risk factor in this study).
Between the Health 2000 (Suominen-Taipale et al. 2004) and Health 2011 (Suominen et al. 2012) surveys, tooth brushing twice a day has increased from 50.0% to 63.0% among Finnish men aged 30–44, which is a good signal of a changing attitude towards oral health in the last decade. The subjects of the Oral Health 2000 and 2011 surveys have lived their school age and teens in the 1970s and 1980s, which are regarded as the golden era of children’s oral health promotion in Finland (Nordblad et al. 2004), as mentioned above. After that, the preventive dentistry resources were reduced because of the economic recession in the 1990s. Additionally, perhaps the study population of the Health 2011 survey was aware of the alarming situation in Finnish people’s oral health and have changed their health habits accordingly. Health topics seem to be interesting now and get much attention in the Finnish media. It can be concluded that effective health promotion is also needed in the future because the good health habits are associated with both caries occurrence and periodontal health (Ellwood et al. 2008, Zero et al. 2008, Bawadi et al. 2011, Tomofuji et al. 2011).
6.6.2 Smoking (III, IV)
In the present study, smoking was associated both with restorative treatment need and with DMFT, and the odds increased with the increasing number of daily cigarettes. The influence of smoking on dental caries may be due to smoking being associated with other unhealthy oral health habits. Earlier studies have established an association between smoking and dental caries due to, for example, poor oral hygiene and harmful dietary habits (Bruno-Ambrosius et al. 2005). According to the review article by Benedetti et al. (2013), the overall poor quality of cross-sectional studies produced no validation for an association between smoking and dental caries. Prospective studies on the topic are needed like the study by Bernabé et al. (2014). They found that smoking was independently associated with caries

77
development (DT increment), but not to caries treatment (FT or MT increments) in Finnish adults over 4 years (Bernabé et al. 2014).
Evidence indicates that cigarette smoking is one of the most significant risk factors for periodontal disease (Tomar & Asma 2000, Ylöstalo et al. 2004, Thomson et al. 2007, Heikkinen et al. 2008). On the other hand, according to many previous studies, smokers have less gingival inflammation than non-smokers, which may be caused by alterations in the inflammatory response or from alterations in the vascular response of the gingival tissue (Novak & Novak 2006). The results of this study are in accordance with previous studies where a negative association between smoking and periodontal health among young adults has been reported even with short-term or low tobacco consumption (Machuca et al. 2000, Ylöstalo et al. 2004, Thomson et al. 2007, Heikkinen et al. 2008, Rosa et al. 2008). Thomson et al. (2007) found that smoking cessation may be associated with relatively rapid improvement in the periodontium among young adults. That should be taken into account in the health promotion for young men.
6.6.3 Snuffing(III)
Using snuff did not affect the occurrence of dental caries lesions but it had a slight association with a high DMFT value. The snuffers had more filled teeth compared to the non-users and the difference was statistically significant. It might be that the snuffers have used more dental services before, which can be seen in the higher DMFT values compared to the non-users. However, the dental attendance of the snuffers was not analysed in this study. Hellqvist et al. (2015) found that the daily use of snus neither increased nor decreased the risk of the dental caries among Swedish adult population.
In this study, snuffing did not increase the risk of periodontal disease indicated by BOP and CPI. The results are in line with previous studies from Sweden (Rolandsson et al. 2005, Bergström et al. 2006, Hugoson & Rolandsson 2011). Montén et al. (2006) also reported that snuffing was not associated with the presence of periodontal disease, except for a significantly higher prevalence of gingival recessions in the maxillary anterior tooth region. They were not registered in this study. Montén et al. (2006) suggested that gingival recession may indicate mechanical and/or chemical trauma caused by snuffing.
78
6.6.4 Alcohol use (IV)
Alcohol use was not associated with the present restorative treatment need or with the caries history. Our results are partly contradictory to the results of Läärä (1999), who found that dental caries is significantly related to the use of alcohol when analysed separately. Also in some previous studies, an association between dental caries occurrence and alcohol use has been reported (Jansson 2008, Nguyen et al. 2008). However the use of alcohol has been shown to be a weaker predictor for caries experience than smoking (Läärä 1999).
Alcohol consumption was only weakly associated with BOP and CPI. The results are in line with Swedish study by Jansson (2008), where alcohol consumption was not associated with periodontal health. On the other hand, Jansson (2008) reported that heavy alcohol users have more calculus than moderate users, which may be a sign of a need for periodontal care in the future (Schätzle et al. 2003). In addition according to a study from Brazil (Lages et al. 2012) high alcohol consumption was associated with prevalence and severity of periodontitis but smoking emphasised these findings. The results between the studies are not directly comparable to this study because the study designs are different. In those studies, the study populations were middle-aged and alcohol use was not investigated in an exact detail (Jansson 2008, Lages et al. 2012). In addition, the study of Jansson (2008) categorised alcohol use differently (centilitres pure alcohol per day) than in our study. By Lages (2012) the categorisation of alcohol use was similar to ours (frequency of alcohol use).
The association between alcohol use and dental health among young adults is a complicated but an interesting topic. At first, it is hard to find studies among young adults because most of the studies have been made among adult population and have applied many different ways to categorise alcohol use. Second, there are no longitudinal studies on the topic. Most of the conscripts used alcohol occasionally in this study. However, it takes on average 15 to 20 years of intensive alcohol use to develop chronic illness, alcoholism, with clinical evidence (WHO 1992). Alcohol can influence host defences and immunity in many ways even with acute use (Szabo 1999). This study provided information about the frequencies of alcohol use but we do not know how severe the alcohol use among conscripts is. In this study, the association of smoking with oral health was much greater than the association of alcohol use. Perhaps the effects of alcohol use on dental health become visible only after years of regular use, but the further research are needed.
79
6.6.5 Education level (III, IV)
In this age group, the high education level of both participants and mothers seemed to decrease the prevalence of high DT, DMFT, BOP and CPI values, whereas father’s high educational level was associated only to caries occurrence (DMFT). Häkkinen et al. (2006) found that mother’s and own educational level were connected to general health, especially among boys which are in accordance with findings of this study. On the other hand, López et al. (2006) reported that the education level of both parents affects to periodontal health among high school students. It might be that even though information about healthy behaviour is available to everyone, instructions and examples of parents make a big difference to health behaviour of males. Behavioural health habits, along with many other habits, are adopted in the childhood and adolescence, and they may be difficult to be changed later on and may require extensive and tailored intervention (Busch et al. 2015). Health promotion should be given continuously because continuous oral health promotion is considered more efficient than short-term intervention among children (Tolvanen et al. 2010).
6.6.6 Urban–rural residence (III)
In the present study, living in a rural area increased the risk of restorative treatment need, caries occurrence and high BOP and CPI values. The cause for lower caries occurrence in urban areas may be associated with differences in the socioeconomic situation in urban and rural areas. The proportion of well-educated inhabitants is larger in cities compared to rural areas (OSF 2012), which affects health behaviours positively (Häkkinen et al. 2006, López et al. 2006). The study by Wierzbicka et al. (2002) also reported that tooth brushing at least twice a day is relatively more frequent in urban than in rural areas, which may diminish the DT, DMFT, BOP and CPI values. The effect of the place of residence on caries occurrence has also registered in Finland (Kämppi et al. 2013).
6.6.7 Language of the municipality of residence (III)
The language of the conscript’s home municipality was not associated with high DT and DMFT values in this study. However, Kämppi et al. (2013) found from the same study population that young males living in Swedish-speaking areas have significantly better oral health than their peers in Finnish-speaking areas. In this
80
study, the language of the conscript’s municipality of residence lost its effect on the DT and DMFT values when other independent variables were included in the models. Therefore, the present study offers a more profound aspect on the issue. The importance of sociodemographic factors remains, but the effect decrease when health behaviours are included in the analyses.
An interesting finding in the present study is that living in Swedish-speaking municipalities was associated with the risk of a high CPI and low BOP value. According to a previous study (Hermann et al. 2009), regular dental attendance was associated with low CPI values. Among this study population did not found an association between a dentist density and high DT (Kämppi et al. 2013) or CPI values of conscripts. Perhaps conscripts living in Swedish-speaking municipalities use dental services less often than those living in Finnish-speaking municipalities. However, the association between dental attendance and CPI values was not investigated in this study.
6.6.8 Fluoride level in drinking water (III)
Living in an area where fluoride level in drinking water is high decreased the risk of the restorative treatment need, caries occurrence, high BOP and high CPI. This is in line with a previous study from Australia (Hopcraft et al. 2009), which reported that conscripts who have lived most of their lives in an area with access to fluoridated drinking water (fluoride concentration greater than 0.5 ppm) had significantly lower (about 25%) caries experience than among those without fluoride exposure. Ankkuriniemi (1979) also found a connection between a low DMFT index and high fluoride level in drinking water but did not find an association between a high fluoride level in drinking water and low level of periodontal diseases. Yet, he found a geographical distribution of periodontal diseases in the country, although the distribution was not as clear as with dental caries. The prevalence of periodontitis was higher in the provinces of North Karelia and Varsinais-Suomi whereas the prevalence of dental caries was higher only in eastern Finland (Ankkuriniemi 1979). The reasons for this can only be speculated. Perhaps good periodontal health correlates with a good caries status – both are infectious diseases. Ainamo (1970) found that decayed tooth surfaces and surplus of fillings cause more attachment loss than calculus. The effect of the fluoride level in drinking water on caries status of the young disappeared when dental health improved (Seppä et al. 2002). In Finland, own wells are one of the main sources of drinking water in rural and partly also in urban areas. But there are only some areas in the south-eastern and

81
south-western Finland where endemic fluoride in drinking water is high (0.5–2.0 mg/l) (Lahermo and Backman 2000). It will be interesting to see if the association between fluoride levels and the caries status is or is not confirmed in future studies.
6.6.9 Using dental services (IV)
When the time from the latest dental visit exceeded three years, the odds for high CPI and DT values increase and the odds for high DMFT values decreased. High BOP values were not associated with dental attendance in this study. The conscripts with irregular dental attendance had more untreated cariological and periodontal diseases compared to regular users of dental services whose high DMFT value may indicate restorative work done. The results are in line with those of Läärä (1999) and Nguyen et al. (2008), who found that regular dental attendance was a significant predictive factor for good caries status among men. Sound teeth have been reported to be associated with regular dental attendance with long intervals which is opposite to filled teeth when annual check-ups have been reported (Ankkuriniemi 1979, Vehkalahti et al. 2008). In addition, the former and never regular attenders had a significantly higher DMFT score and numbers of decayed and missing teeth but fewer filled teeth than the always regular attenders (Aldossary et al. 2014). These findings are also in line with ours. Our findings also agree with the studies by Ankkuriniemi (1979) and Hermann et al. (2009), who found that more frequent dental visits are also associated with periodontal health.
In Finland, every citizen under 18 of age has the legal right to free dental care. That right had just ended for the study population of the present study. Due to that, dental attendance between the conscripts varied considerably. In this study, the smokers used dental services more rarely than the non-smokers, which is in accordance with the study by Bloom et al. (2012) and Hellqvist et al. (2009). Oral health of the smokers was significantly worse compared to the non-smokers in this study, which could be associated with non-regular dental attendance. Läärä (1999) found that conscripts with poor oral health were less willing to visit a dentist. In addition, high dental fear have been reported to be associated with smoking (Pohjola et al. 2014), which may be one reason to the non-regular dental attendance of the smokers also in this study. It could also be possible that smokers’ attitude to health may be indifferent and therefore they end up using acute care.

82
6.7 Strengths and weaknesses of the study
A great advantage of the present study was its uniquely large study population. Furthermore, studies on this age group, like the present one, are hard to find in the literature. Thus, this study offers epidemiological evidence of oral health of young people in the 2010s. The value of this study was also combining the clinical findings with self-reported factors. This epidemiological study was carried out carefully with a calibration of examiners and a pilot study, which increases the validity of this study. Otherwise, the variation between the examiners was quite high, which may decrease the validity of this study. Also data on initial caries was missing which underestimated the prevalence of dental caries in the study population. A shortcoming is also the lack of information about the history of smoking, snuffing and alcohol consumption among the study group. This epidemiological, cross-sectional study shows only the current situation of the conscripts’ lifestyle and oral health. Longitudinal studies on the topic would be most valuable.
83
7 Summary and conclusionsIt can be concluded that the present study offers epidemiological data from an era subsequent to that when the caries status was constantly improving. Our findings suggest stagnation in the improvement, or even deterioration of the caries status of the healthy, young adult male population in Finland, despite the free dental care available to all Finns under 18 years of age.
Compared to the adult population in the Oral Health 2011 study, the dental caries situation was poorer in the present study. The caries burden was still polarised among the study group. Yet, the polarisation was weaker in this study than in the previous national survey (Suominen-Taipale et al. 2008), as one might expect given the apparently higher caries level.
The trend of increasing daily smoking was quite alarming among young Finnish men and may cause a threat to their health in the future, also increasing the sickness burden and pressure on health care. Smoking was more common than among 18-years-old Finnish males now than in a previous study (Kinnunen et al. 2013). Smoking was associated both with poor oral health and with dental attendance, which should be noted in health promotion. The smokers had a higher risk of dental caries and future periodontal treatment need compared to the non-smokers, snuffers and alcohol users. On the other hand, dietary habits of the snuffers seemed harmful too but were compensated by the snuffers’ good tooth brushing frequency. The consequences of smoking on oral health may be seen even after a short use, but the effect of alcohol use takes more time to become visible. The present study group consumed alcohol moderately, and it had only a slight effect on oral health.
According to this study, the place of residence increased the odds for using snuff in Finland because of the easier access to snuff products near the Swedish border. Similar geographical distributions were not found among the smokers.
7.1 Practical relevance and future studies
Smoking seems to be associated with poor oral hygiene and harmful dietary habits. These also increase the risk of dental caries and periodontal disease. Apparently more weight should be put on investigating the smoking habits in addition to other health behaviours of young adults when estimating their risk of dental caries and periodontal disease. Both health behaviours and environmental factors are associated with oral health, which should be considered in oral health promotion.

84
We know that health habits of young Finnish males do not support good oral health, and therefore caries control continues to be a challenge. That is why new ways for oral health promotion targeted in particular to men should be developed and investigated. During the field survey of the present study, we collected specific data not only on oral health but also on health habits of this study group. Our valuable data provide the possibility of investigating health behavioural patterns associated with oral health among the young. We hope that this information facilitates ways to maintain and promote oral health of the young in our country and elsewhere. Good oral health promotes good general health.
The questionnaire and the psychological and fitness tests of the Finnish Defence Forces offer much more information than used in this study. It would be valuable to investigate even more background factors’ (e.g. dietary and snacking behaviours’) association with oral health in detail. That might help us to understand the complex web of factors associated with people’s oral health.
85
ReferencesAlavaikko S, Jaakkola MS, Tjäderhane L, Jaakkola JJ (2011) Asthma and caries: a systematic
review and meta-analysis. Am J Epidemiol 174:631–641.Albandar JM, Kingman A, Brown LJ, Löe H (1998) Gingival inflammation and subgingival
calculus as determinants of disease progression in early-onset periodontitis. J Clin Periodonto 25:231–237.
Aldossary A, Harrison VE, Bernabe E (2015) Long-term patterns of dental attendance and caries experience among British adults: a retrospective analysis. Eur J Oral Sci 123:39–45.
Ainamo J (1970). Concomitant periodontal disease and dental caries in young adult males Suom Hammaslääk 66:303–366 (In Finnish).
Ankkuriniemi O (1979) The dental status and need for dental treatment among Finnish conscripts [dissertation]. University of Helsinki, Finland.
Anttonen V, Hausen H, Seppä L, Niinimaa A (2008) effect of dietary habits on laser fluorescence values of visually sound occlusal surfaces among Finnish schoolchildren. Int J Paediatr Dent 18:124–130.
Anttonen V, Seppä L, Niinimaa A, Hausen H (2011) Dietary and oral hygiene intervention in secondary school pupils. Int J Paediatr Dent 21:81–88.
Åstrøm AN, Jakobsen R (1998) Stability of dental health behavior: a 3-year prospective cohort study of 15-, 16- and 18-year-old Norwegian adolescents. Community Dent Oral Epidemiol 26:129–138.
Åstrøm AN (2004) Stability of oral health-related behaviour in a Norwegian cohort between the ages of 15 and 23 years. Community Dent Oral Epidemiol 32:354–362.
Axelsson P (1998) Needs-related plaque control measures based on risk prediction. In: Lang N, Attstrom R, Loe H. Proceedings of the European Workshop on Mechanical Plaque Control Chicago: Quintessence, pp. 190–247.
Axelsson P, Paulander J, Lindhe J (1998) Relationship between smoking and dental status in 35-, 50-, 65-, and 75-year-old individuals. J Clin Periodontol 25:297–305.
Bastos JL, Nomura LH, Peres MA (2007) Dental caries and associated factors among young male adults between 1999 and 2003 in Southern Brazil. Community Dent Health 24:122–127.
Batchelor PA, Sheiham A (2004) Grouping of tooth surfaces by susceptibility to caries: a study in 5–16 year-old children. BMC Oral Health 4:2. doi: 10.1186/1472-6831-4-2
Bawadi HA, Khader YS, Haroun TF, Al-Omari M, Tayyem RF (2011) The association between periodontal disease, physical activity and healthy diet among adults in Jordan. J Periodontal Res 46:74–81.
Beck JD, Arbes SJ Jr (2006) Epidemiology of Gingival and Periodontal Diseases. In: Newman MG, Takei HH, Klokkevold PR, Carranza FA editors. Carranza’s Clinical Periodontology, tenth edition. Saunders Elsevier, St. Louis, Missouri, pp. 115–120.
Benedetti G, Campus G, Strhmenger L, Lingström P (2013) Tobacco and dental caries: a systematic review. Acta Odontol Scand 71:363–371.

86
Bernabé E, Delgado-Angulo EK, Vehkalahti MM, Aromaa A, Suominen AL (2014) Daily smoking and 4-years caries increment in Finnish adults. Community Dent Oral Epidemiol 42:428–434.
Bergström J, Keilani H, Lundholm C, Rådestad U (2006) Smokeless tobacco (snuff) use and periodontal bone loss. J Clin Periodontl 33:549–554.
Bingham CM, Jallinoja P, Lahti-Koski M, Absetz P, Paturi M, Pihlajamäki H, Sahi T, Uutela A (2010) Quality of diet and food choices of Finnish young men: A sociodemographic and health behaviour approach. Public Health Nutrition 13:980–986.
Bloom B, Adams PF, Cohen RA, Simile C (2012) Smoking and oral health in dentate adults aged 18–64. NCHS Data Brief. 85:1–8.
Bonevski B, Regan T, Paul C, Baker AL, Bisquera A (2014) Associations between alcohol, smoking, socioeconomic status and comorbidities: Evidence from the 45 and UP Study. Drug Alcohol Rev. 33:169–176.
Bratthall D, Hänsel-Petersson G, Sundberg H (1996) Reason for the caries decline: what do the experts believe? Eur J Oral Sci 104:416–422.
Bruno-Ambrosius K, Swanholm G, Twetman S (2005) Eating habits, smoking and toothbrushing in relation to dental caries: a 3-year study in Swedish female teenagers. Int J Paediatr Dent 15:190–196.
Buchwald S, Kocher T, Biffar R, Harb A, Holtfreter B, Meisel P (2013) Tooth loss and periodontitis by socioeconomic status and inflammation in a longitudinal population-based study. J Clin Periodontol 40:203–211.
Burger JM, Shelton M (2011) Changing everyday health behaviors through descriptive norm manipulations. Social Influence 6:69–77.
Burt BA (1998) Prevention policies in the light of the changed distribution of dental caries. Acta Odontol Scand 56:179–186.
Busch V, De Leeuw JR, Zuithoff NP, Van Yperen TA, Schrijvers AJ (2015) A Controlled Health Promoting School Study in the Netherlands: Effects After 1 and 2 Years of Intervention. Health Promot Pract Jan 7. pii: 1524839914566272. [Epub ahead of print].
Cascaes AM, Peres KG, Peres MA (2009) Periodontal disease is associated with poor self-rated oral health among Brazilian adults. J Clin Periodontol 36:25–33.
Catteau C, Blaizot A, Duhamel A, Delzenne A, Devillers A, Frimat P (2013) Dental status and factors in an occupational health service in Northern France [Article in French, summary in English]. Sante Publique 25:747–755.
Ceylan S, Acikel CH, Okcu KM, Kilic S, Tekbas OF, Ortakoglu K (2004) Evaluation of the dental health of the young adult male population in Turkey. Mil Med 169:885–889.
Costa FO, Guimaraes AW, Cota LO, Pataro AL, Sequndo TK, Cortelli SC, Costa JE (2009) Impact of different periodontitis care definitions on periodontal research. J Oral Sci 51:199–206.
Costa SM, Martins CC, Bonfim ML, Zina LG, Paiva SM, Pordeus IA (2012) A systematic review of socioeconomic indicators and dental caries in adults. Int J Environ Res Public Health 9:3540–3574.
Drilea SK, Reid BC, Li CH, Hyman JJ, Manski RJ (2005) Dental visits among smoking and nonsmoking US adults in 2000. Am J Health Behav. 29:462–471.
87
Ekstrand KR, Carvalho JC, Thylstrup A (1994) Restorative caries treatment patterns in Danish 20-year-old males in 1986 and 1991. Community Dent Oral Epidemiol 22:75–79.
Ellwood R, Fejerskov O, Cury J, Clarkson B (2008) Fluorides in caries control. In: Fejerskov O, Kidd E, editors: Dental caries, 2nd edition. Oxford: Blackwell Munksgaard, pp. 288–327.
Engström K, Magnusson C, Galanti MR (2010) Socio-demographic, lifestyle and health characteristics among snus users and dual tobacco users in Stockholm County, Sweden. BMC Public Health 10:619. doi: 10.1186/1471-2458-10-619.
Evidence based guidelines for controlling dental caries (2009). Finnish Medical Society (Duodecim). Available from: http://www.kaypahoito.fi/web/kh/suositukset/naytaartikkeli/tunnus/hoi50078 [in Finnish]
Fant RV, Henninqfield JE, Nelson RA, Pickworth WB (1999) Pharmacokinetics and pharmacodynamics of moist snuff in humans. Tobacco Control. 8:387–392.
Faraway JJ (2006) Extending the Linear Model with R Generalized Linear, Mixed Effects and Nonparametric Regression Models. Boca Raton, Chapman & Hall/CRC.
Ferreira M, Kuntsche E, de Looze M, Baska T, Simons-Morton B, ter Bogt, Nic Gabbainn S (2012) Chapter 5. Alcohol use. In: Currie C, Zanotti C, Morgan A, Currie D, de Looze M, Roberts C, Samdal O, Smith ORF, Barnekow V editors. Social determinants of health and well-being among young people. Health Behaviour in School-aged Children (HBSC) study: international report from the 2009/2010 survey. Health Policy for Children and Adolescents, No. 6. Copenhagen: WHO Regional Office for Europe, pp. 151–162. Available from: http://www.euro.who.int/__data/ assets/pdf_file//0003/163857/Social-determinants-of-health-and-well-being -among-young-people.pdf
Filion KB, Steffen LM, Duval S, Jacobs DR Jr, Blacburn H, Luepker RV (2012) Trend in smoking among adults from 1980 to 2009: the Minnesota heart survey. Am J Public Health 102:705–713.
Gallus S, Muttarak R, Martínez-Sánchez JM, Zuccaro P, Colombo P, La Vecchia C (2011) Smoking prevalence and smoking attributable mortality in Italy, 2010. Prev Med 52:434–438.
Gupta P, Gupta N, Pawar A, Birajdar S, Natt A, Singh H (2013) Role of sugar and sugar substitutes in dental caries: A Review. ISRN Dent 29:519421. doi: 10.1155/2013/519421.
Hausen H, Karkkainen S, Seppä L (2001) Caries data collected from public health records compared with data based on examinations by trained examiners. Caries Res 35:360–365.
Heikkinen AM, Pajukanta R, Pitkäniemi J, Broms U, Sorsa T, Koskenvuo M, Meurman JH (2008) The effect of smoking on periodontal health of 15- to 16-year-old adolescents. J Periodontol 79:2042–2047.
Heikkinen AM (2011) Oral health, smoking and adolescence. Academic Dissertation, University of Helsinki, Finland.
88
Helldán A, Helakorpi S, Virtanen S, Uutela A (2013) Health Behaviour and Health among the Finnish Adult Population. National Institute for Health and Welfare (THL), Report 21/2013, 204 pages. Helsinki 2013. pp. 3, 12–15, 68. Available from: https://www.julkari.fi/bitstream/handle/10024/110841/ URN_ISBN_978-952-302-051-1.pdf?sequence=1
Hellqvist L, Rolandsson M, Birkhed D, Hugoson A (2009) Tobacco use in relation to socioeconomic factors and dental care habits among Swedish individuals 15–70 years of age, 1983–2003. Int J Dent Hyg 7:62–70.
Hellqvist L, Boström A, Lingström P, Hugoson A, Rolandsson M, Birkhed D (2012) Effect of nicotine-free and nicotine-containing snus on plaque pH in vivo. Swed Dent J 36:187–194.
Hellqvist L, Rolandsson M, Hugoson A, Lingström P, Birkhed D (2015) Dental caries and associated factors in a group of Swedish snus users. Swed Dent J 39:47–54.
Hermann P, Gera I, Borbély J, Fejérdy P, Madléna M (2009) Periodontal health of an adult population in Hungary: findings of a national survey. J Clin Periodontol 36:449–457.
Holmén A, Strömberg U, Magnusson K, Twetman S (2013) Tobacco use and caries risk among adolescents – a longitudinal study in Sweden. BMC Oral Health 13:31. doi: 10.1186/1472-6831-13-31.
Honkala S, Honkala E, Newton T, Rimpelä A (2011) Toothbrushing and smoking among adolescents- aggregation of health damaging behaviours. J Clin Periodontol 38:442–448.
Honkala S, Honkala E, Levin KA (2012). Chapter 4: Oral health. In: Currie C, Zanotti C, Morgan A, Currie D, de Looze M, Roberts C, Samdal O, Smith ORF, Barnekow V editors. Social determinants of health and well-being among young people. Health Behaviour in School-aged Children (HBSC) study: international report from the 2009/2010 survey. Health Policy for Children and Adolescents, No. 6. Copenhagen: WHO Regional Office for Europe, 123–128. Available from: http://www.euro. who.int/__data/assets/pdf_file//0003/163857/Social-determinants-of-health-and-well-being-among-young-people.pdf
Honkala S, Vereecken C, Niclasen B, Honkala E (2015) Trends in toothbrushing in 20 countries or regions between 1994 and 2010. Eur J Public Health 25(Suppl. 2):20–23.
Hopcraft MS, Morgan M (2003a) Exposure to fluoridated drinking water and dental caries experience in Australian army recruits, 1996. Community Dent Oral Epidemiol 31:68–74.
Hopcraft M, Morgan M (2003b) Dental caries experience in a young adult military population. Aust Dent J 48:125–129.
Hopcraft M, Morgan MV (2005) Dental caries experience in Australian Army recruits 2002–2003. Aust Dent J 50:16–20.
Hopcraft MS, Yapp KE, Mahoney G, Morgan MV (2009) Dental caries experience in young Australian Army recruits 2008. Aust Dent J 54:316–322.
Hugoson A, Koch G, Bergendal T, Hallonsten AL, Slotte C, Thorstensson B, Thorstensson H (1995) Oral health of individuals aged 3–80 years in Jonkoping, Sweden in 1973, 1983 and 1993. II. Review of clinical and radiographic findings. Swed Dent J 19:243–260.

89
Hugoson A, Rolandsson M (2011) Periodontal disease in relation to smoking and the use of Swedish snus: epidemiological studies covering 20 years (1983–2003). J Clin Periodontol 38:809–816.
Hugoson A, Hellqvist L, Rolandsson M, Birkhed D (2012) Dental caries in relation to smoking and use of Swedish snus: epidemiological studies covering 20 year (1983–2003). Acta Odontol Scand 70:289–296.
Huhtala H, Rainio S, Rimpelä A (2006) Adolescent snus use in Finland in 1981–2003: trend, total sales ban and acquisition. Tob Control 15:392–397.
Häkkinen U, Järvelin MR, Rosenqvist G, Laitinen J (2006) Health, schooling and lifestyle among young adults in Finland. Health Econ 15:1201–1216.
Ismail AI, Sohn W, Tellez M, Amaya A, Sen A, Hasson H, Pitts NB (2007) The International Caries Detection and Assessment System (ICDAS): an integrated system for measuring dental caries. Community Dent Oral Epidemiol 35:170–178.
Jansson L (2008) Association between alcohol consumption and dental health. J Clin Periodontol 35:379–384.
Joss A, Weber HP, Gerber C, Siegrist B, Curilovic Z, Saxer UP, Lang NP (1992) Periodontal conditions in Swiss Army recruits. Schwe Monatsschr Zahnmed 102:541–548.
Jürgensen N, Petersen PE, Ogawa H, Matsumoto S (2012) Translating science into action: periodontal health through public health approaches. Periodontol 2000 60:173–187.
Kämppi A, Tanner T, Päkkilä J, Patinen P, Järvelin MR, Tjäderhane L, Anttonen V (2013) The geographical distribution of dental caries prevalence and associated factors in young adults in Finland. Caries Res 47:346–354.
Kinnunen JM, Lindfors P, Pere L, Ollila H, Samposalo H, Rimpelä A (2013) The Adolescent Health and Lifestyle Survey 2013. Adolescent smoking, alcohol and substance use in 1977–2013. Sosiaali- ja terveysministeriön raportteja ja muistioita 16, pp. 20–40, Helsinki (In Finnish). Available from: http://www.stm.fi/c/ document_library/get_file?folderId=6511574&name=DLFE-26851.pdf
Kisely S, Quek LH, Pais J, Lalloo R, Johnson NW, Lawrence D (2011) Advanced dental disease in people with severe mental illness: systematic review and meta-analysis. Br J Psychiatry 199:187–193.
Kuusela S, Honkala E, Rimpelä A (1996). Toothbrushing frequency between ages 12 and 18 – Longitudinal prospective studies of Finnish adolescents. Community Dent Health 13:34–39.
Läärä M (1999) Polarization of dental caries and the explanatory background factors in a Finnish conscript population. Academic dissertation, University of Turku, Finland.
Lages EJP, Costa FO, Lages EMB, Cota LOM, Cortelli SC, Nobre-Franco GC, Cyrino RM, Cortelli JR (2012) Risk variables in the association between frequency of alcohol consumption and periodontitis. J Clin Periodontol 39:115–122.
Lahermo P, Backman B (2000) The Occurrence and Geochemistry of Fluorides with Special Reference to Natural Waters in Finland. Report of Investigation 149. Geological Survey of Finland. Available from: http://arkisto.gsf.fi/tr/tr149/tr149.pdf.
90
Lang NP, Joss A, Saxer C, Wallkamm B, Brägger U, Schürch E, Hofer B, Schimd B, Luterbacher S, Etter T, Christensen M, Attström R (1998) Periodontal conditions of Swiss army recruits – positive effects of prevention –oriented dentistry. Acta Med Dent Helvetica 3:81–86 (In German with an English abstrakt).
Lee PN (2011) Summary of the epidemiological evidence relating snus to health. Reg Toxicol Pharmacol 59:197–214.
Levin L, Shenkman (2004) The relationship between dental caries status and oral health attitudes and behaviour in young Israeli adults. J Dent Educ 68:1185–1191.
Levin L, Baev V, Lev R, Stabholz A, Ashkenazi M (2006) Aggressive periodontitis among young Israeli army personnel. J Periodontol 77:1392–1396.
Li TK, Volkow ND, Baler RD, Egli M (2007) The biological bases of nicotine and alcohol co-addiction. Biol Psychiatry 61:1–3.
Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H et al. (2012) A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380:2224–2260.
López R, Fernández O, Baelum V (2006) Social gradients in periodontal diseases among adolescents. Community Dent Oral Epidemiol 34:184–196.
Machuca G, Rosales I, Lacalle JR, Machuca C, Bullón P (2000) Effect of cigarette smoking on periodontal status of healthy young adults. J Periodontol 71:73–78.
Maes L, Maser M, Honkala S (2004). Oral health. In: Currie C, Roberts C, Morgan A, Smith R, Settertobult W, Samdal O, Barnekow, Rasmussen V editors. Young People’s Health in Context. Health Behaviour in School-aged Children (HBSC) study: international report from the 2001/2002 survey. Health Policy for Children and Adolescents, No. 4. Denmark, World Health Organization Regional Office for Europe, pp. 130–132. Available from: http://www.who.int /immunization/hpv/target/young_peoples_health_in_context_who_2011_2012.pdf
Marthaler TM (2004) Changes in dental caries 1953–2003. Caries Res 38:173–181.Mattila VM, Raisamo S, Pihlajamäki H, Mäntysaari M, Rimpelä A (2012) Sports activity
and the use of cigarettes and snus among young males in Finland in 1999–2010. BMC Public Health 12:230. doi: 10.1186/1471-2458-12-230.
Ministry of Social Affairs and Health, Finland (1972) Primary Health Care Act (66/1972), Helsinki, Finland. Available from: http://www.finlex.fi/fi/laki/ajantasa/1992/19920734
Montén U, Wennström JL, Ramberg P (2006) Periodontal conditions in male adolescents using smokeless tobacco (moist snuff). J Clin Periodontol 33:863–868.
Moynihan P, Kelly S (2014) Effect on caries of restricting sugars intake: systematic review to inform WHO guidelines. J Dent Res. 93:8–18.
National Institute for Health and Welfare (NIHW/THL) (2006) Health for the population from the Community. Helsinki (in Finnish) Available from: http://www.julkari.fi/bitstream/handle/10024/102825/10kansanterveys2006.pdf?sequence=1
Nguyen L, Häkkinen U, Knuuttila M, Järvelin MR (2008) Should we brush twice a day? Determinants of dental health among young adults in Finland. Health Econ 17:267–286.
91
Nordblad A, Suominen-Taipale L, Rasilainen J, Karhunen T (2004) In: Oral Health Care at Health Centers from the 1970’s to the year 2000. Saarijärvi, Finland: Gummerus; STAKES Reports (National Institute for Health and Welfare, THL); Saarijärvi, Finland: Gummerus (In Finnish with an English summary).
Novak MJ (2006) Classification of Diseases and Conditions Affecting the Periodontium In: Newman MG, Takei HH, Klokkevold PR, Carranza FA editors. Carranza’s Clinical Periodontology, tenth edition. St. Louis, Missouri: Saunders Elsevier, St. Louis, Missouri, pp. 100–106. ISBN 13 978-1-4160-2400-2
Novak MJ, Novak KF (2006) Smoking and Periodontal Disease. In: Newman MG, Takei HH, Klokkevold PR, Carranza FA editors. Carranza’s Clinical Periodontology, tenth edition. St. Louis, Missouri: Saunders Elsevier, St. Louis, Missouri, pp. 251–255. ISBN 13 978-1-4160-2400-2
Nyvad B, Machiuiskiene V, Baelum V (1999) Reliability of a new caries diagnostic system differentiating between active and inactive caries lesions. Caries Res 33:252–260.
Official Statistics of Finland (OSF) (2013): Tobacco statistics [e-publication]. Helsinki: National Institute for Health and Welfare (THL). Available from:http://www.stat.fi/til/tupk/index_en.html
Okamoto Y, Tsuboi S, Suzuki S, Nakagaki H, Ogura Y, Maeda K, Tokudome S (2006) Effects of smoking and drinking habits on the incidence of periodontal disease and tooth loss among Japanese males: a 4-yr longitudinal study: J Periodontal Res 41:560–566.
Paavola M, Vartiainen E, Haukkala A (2004) Smoking, Alcohol Use, and Physical Activity: A 13-Year Longitudinal Study Ranging from Adolescence into Adulthood. J Adolesc Health 35:238–244.
Page RC, Eke PI (2007) Case definitions for use in population based surveillance of periodontitis. J Periodontol 78:1387–1399.
Peltola JS, Ventä I, Haahtela S, Lakoma A, Ylipaavalniemi P, Turtola L (2006) Dental and oral radiographic findings in first year university students in 1982 and 2002 in Helsinki, Finland. Acta Odontol Scand. 64:42–46.
Piovesa C, Moro BLP, Lara JS, Ardenghi TM, Guedes RS, Haddad AE, Braga MM, Mendes FM (2013) Laboratorial training of examiners for using a visual caries detection system in epidemiological surveys. BMC Oral Health 13:49. doi: 10.1186/1472-6831-13-49.
Pitts N, Chestnutt I, White D, Chadwick B, Steele J (2006) The dentinal caries experience of children in the United Kingdom, 2003. Br Dent J 200:313–320.
Pohjola V, Rannanautio L, Kunttu K, Virtanen JI (2014) Dental fear, tobacco use and alcohol use among university students in Finland: a national survey. BMC Oral Health 14:86. doi: 10.1186/1472-6831-14-86.
Polk DE, Weyant RJ, Manz MC (2010) Socioeconomic factors in adolescents’ oral health: are they mediated by oral hygiene behaviors or preventive interventions? Community Dent Oral Epidemiol 38:1–9.
Popkin BM (2006) Global nutrition dynamics: the world is shifting rapidly toward a diet linked with noncommunicable diseases. Am J Clin Nutr 84:289–298.
Rolandsson M, Hellqvist L, Linqvist L, Hugoson A (2005) Effects of snuff on the oral health status of adolescent males: a comparative study. Oral Health Prev Dent 3:77–85.
92
Rooban T, Vidya K, Joshua E, Rao A, Ranganathan S, Rao UK, Ranganathan K (2011) Tooth decay in alcohol and tobacco abusers. J Oral Maxillofac Pathol 15:14–21.
Roosar A, Johansson ALV, Sandborgh-Englund G, Axéll T, Nyrén O (2008) Cancer and mortality among users and nonusers of snus. Int J Cancer 123:168–173.
Rosa GM, Lucas GQ, Lucas ON (2008) Cigarette smoking and alveolar bone in young adults: a study using digitized radiographs. J Periodontol 79:232–244.
Röthlisberger B, Kuonen P, Salvi GE, Gerber J, Pjetursson BE, Attström R, Joss A, Lang NP (2007) Periodontal conditions in Swiss army recruits: a comparative study between the years 1985, 1996 and 2006. J Clin Periodontol 34:860–866.
Samet JM, Norman LA, Wilbanks C editors (2004) The Health Consequences of Smoking: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2004. Available from: http://www.cdc.gov/tobacco/ data_statistics/sgr/2004/
Saxby M (1984) Prevalence of juvenile periodontitis in a British school population. Community Dent Oral Epidemiol 12:185–187.
SCENIHR (Scientific Committee on Emerging and Newly-Identified Health Risks) (2008) Scientific opinion on the Health Effects of Smokeless Tobacco Products, 6 February 2008. European Commission. Available from: http://ec.europa.eu/health/archive/ph_risk/committees/04_scenihr/docs/scenihr_o_013.pdf
Schou L, Uitenbroek D (1995) Social and behavioural indicators of caries experience in 5-year-old children. Community Dent Oral Epidemiol 23:276–281.
Schultz PW, Nolan JM, Cialdini RB, Goldstein NJ, Griskevicius V (2007) The constructive, destructive and reconstructive power of social norms. Psychol Sci 18:429–434.
Schwendicke F, Dörfer CE, Schlattmann P, Page LF, Thomson WM, Paris S (2015) Socioeconomic inequality and caries: a systematic review and meta-analysis. J Dent Res 94:10–18.
Schätzle M, Löe H, Bürgin W, Anerud A, Boysen H, Lang NP (2003) Clinical course of chronic periodontitis. I. Role of gingivitis. J Clin Periodontol 30(10):887–901.
Seppä L, Kärkkäinen S, Hausen H (1998) Caries frequency in permanent teeth before and after discontinuation of water fluoridation in Kuopio, Finland. Community Dent Oral Epidemiol 26:256–262.
Seppä L, Hausen H, Kärkkäinen S, Larmas M (2002) Caries occurrence in a fluoridated and a nonfluoridated town in Finland: A retrospective study using longitudinal data from public dental records. Caries Res 36:308–314.
Sheiham A, Sabbah W (2010) Using universal patterns of caries for planning and evaluating dental care. Caries Res 44:141–150.
Shimazaki Y, Saito T, Kiyohara Y, Kato I, Kubo M, Iida M, Yamashita Y (2006) The influence of current and former smoking on gingival bleeding: The Hisayama Study. J Periodontol 77:1430–1435.
Skec V, Macan JS, Susac M, Jokic D, Brajdic D, Macan D (2006) Influence of oral hygiene on oral health of recruits and professionals in the Croatian Army. Mil Med 171:1006–1009.
93
Siilasmaa R, Ahtisaari M, Ala-Pietilä P, Junger M, Komi K, Ojajärvi A, Parkkinen M, Räty A, Siimes O, Virtanen V (2010) Finnish mandatory military service. A Report 2010, Ministry of Defence, Helsinki, Finland (in Finnish).
Siitonen S, Heikkilä R (2013) Tupakoimattomuuden edistäminen puolustusvoimissa v. 2012–2017. Ann Med Milit Fenn 1:41–43 (In Finnish).
Sinha DN, Dobe M, Rahman K (2006) Smokeless tobacco use and its implications in WHO South East Asia Region. Indian J Public Health 50:68–73.
Spencer AJ, Davies M, Slade G, Brennan D (1994) Caries prevalence in Australia. Int Dent J 44:415–423.
Statistics Finland (2011): Population. 2011. Available from: http://stat.fi/tup/suoluk/suoluk-vaesto_en.html
Suominen L, Vehkalahti M and Knuuttila M (2012) Oral health In: Koskinen S, Lundqvist A, Ristiluoma N, editors. Health, functional capacity and welfare in Finland in 2011. National Institute for Health and Welfare (THL), Helsinki, pp. 102–107(In Finnish with an English summary). Available from: http://www.julkari.fi/bitstream /handle/10024/90832/Rap068_2012_netti.pdf
Suominen-Taipale L, Nordblad A, Vehkalahti M, Aromaa A (2008) Oral health of Finnish adults. Health 2000 Survey. Publications of the National Public Health Institute B25/2008. Helsinki: Hakapaino Oy, 2008. Available from: http://www.terveys2000.fi/julkaisut/oral_health.pdf
Suominen-Taipale AL, Widström E, Sund R (2009) Association of examination rates with children’s national caries indices in Finland. Open Dent J 3:59–67.
Susin C, Haas AN, Albandar JM (2014) Epidemiology and demographics of aggressive periodontitis. Periodontol 2000 65:27–45.
Szabo G (1999) Consequences of alcohol consumption on host defence. Alcohol 34:830–841.
Thomson WM, Broadbent JM, Welch D, Beck JD, Poulton R (2007) Cigarette smoking and periodontal disease among 32-year-olds: a prospective study of a representative birth cohort. J Clin Periodontol 34:828–834.
Tolvanen M, Lahti S, Hausen H (2010) Changes in toothbrushing frequency in relation to changes in oral health-related knowledge and attitudes among children – a longitudinal study. Eur J Oral sci. 118:284–289.
Tomar SL, Asma S (2000) Smoking-attributable periodontitis in the United States: findings from NHANES III. National Health and Nutrition Examination Survey. J Periodontol 71:743–751.
Tomar SL, Winn DM (1999) Chewing tobacco use and dental caries among U.S. men. J Am Dent Assoc 130:1601–1610.
Tomofuji T, Furuta M, Ekuni D, Irie K, Azuma T, Iwasaki Y, Morita M (2011) Relationships between eating habits and periodontal condition in university students. J Periodontol 82:1642–1649.
94
Twetman S, Johansson I, Birkhed D, Nederfors T (2002) Caries incidence in young type 1 diabetes mellitus patients in relation to metabolic control and caries-associated risk factors. Caries Res 36:31–35.
U.S. Department of Health and Human Services (2012) Preventing tobacco use among youth and young adults: A report of the surgeon general. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health;2012:2.
Vehkalahti M, Varsio S, Hausen H (2008). Dental status. In: Suominen-Taipale L, Nordblad A, Vehkalahti M, Aromaa A editors. Oral health in the Finnish adult population. Health 2000 survey. Publications of the National Public Health Institute B25/2008. Helsinki: Hakapaino Oy, pp. 73–81. Available from: http://www.terveys 2000. fi /julkaisut/oral_health.pdf
Vellappally S, Fiala Z, Smejkalová J, Jacob V, Shriharsha P (2007) Influence of tobacco use in dental caries development. Cent Eur J Public Health 15:116–121.
Verlato G, Accordini S, Nguyen G, Marchetti P, Cazzoletti L, Ferrari M et al. (2014) Socioeconomic inequalities in smoking habits are still increasing in Italy. BMC Public Health 14:879. doi: 10.1186/1471-2458-14-879.
WHO (1992) The classification of mental and behavioral disorders. Clinical descriptions and diagnostic guidelines. Geneva: World Health Organization, 1992.
WHO (1997) Oral health surveys – basic methods, 5th ed. Geneva: World Health Organization, pp. 42–51. Available from; http://www.icd.org/content/publications/WHO-Oral-Health-Surveys-Basic-Methods-5th-Edition-2013.pdf
WHO (2008) The scientific basis of tobacco product regulation. Second report of a WHO Study Group. WHO Technical Report Series 951. Geneva: World Health Organization. Available from: http://www.who.int/tobacco /global_interaction/tobreg/publications/9789241209519.pdf
WHO (2011a) Global status report on alcohol and health. Geneva: World Health Organization. Available from: http://apps.who.int/iris/ bitstream/10665/44499/1/9789241564151_eng.pdf
WHO (2011b) Report on the global tobacco epidemic: Warning about the dangers of tobacco. Geneva: World Health Organization. Available from: http://www.who.int/tobacco/global_report/2011/en/
Wickholm S, Soder PO, Galanti MR, Soder B, Klinge B (2004) Periodontal disease in a group of Swedish adult snuff and cigarette users. Acta Odontol Scand 62:333–338.
Wierzbicka M, Petersen PE, Szatko F, Dybiebanska E, Kalo I (2002) Changing oral health status and oral health behaviour of schoolchildren in Poland. Community Dent Health 19:234–250.
Ylöstalo P, Sakki T, Laitinen J, Järvelin MR, Knuuttila M (2004) The relation of tobacco smoking to tooth loss among young adults. Eur J Oral Sci 112:121–126.
Zappa V, Simona C, Graf H, Case D, Thomas J (1995) Reliability of single and double probing attachment level measurements. J Clin Periodontol 22:764–771.

95
Zero D, Moynihan P, Lingstrom P, Birkhead D (2008) The role of dietary control. In: Fejerskov O, Kidd E, editors: Dental caries, 2nd edition. Blackwell Munksgaard, Oxford 329–352.

96
97
Appendices
Appendix I – Feedback form of the pilot study
Garrison __________________________________________________________
Clinical oral inspection too approximately _______minute without BW radiographyIncluding BW radiography, clinical inspection too approximately _______minutes Radiographs were diagnosed during the inspection Yes/NoRadiographs were diagnosed afterwards Yes/No
Comments regarding the clinical inspection and radiography:____________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Answerin the computer-based questionnaire took approximately _______ minutesComments regarding the questionnaire and answering it:________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Please return the filled form and the USB memory stick to X.XXXXXXX.XXXXXXXX, Institute of Dentistry, POB 5281, 90014 University of Oulu, Finland

98
Appendix II – Questionnaire
29th March 2010Covering letter to study of Oral health of conscripts 2011
We kindly ask you to take part to this national study of Oral health of conscripts 2011. The aim of this study is to get information about the oral health situation and treatment need of conscripts born beginning of 1990s.
Information from the questionnaire will be used in this study. In addition we ask permission to use information from your clinical examinations included in your military service. In this study all information will be used so that conscripts can´t be identified from their answers.
By answering this questionnaire you also give permission to use information from your clinical examinations in this study.
Pertti Patinen Vuokko AnttonenChief Dental Officer in Senior Researcher (PhD), Finnish Defence Forces University of Oulu
1. Do you live
In a city? In the countryside?
2. Your education:
Comprehensive school
Vocational school
University of applied sciences
Vocational school and matriculation exam or gymnasium
Matriculation exam or gymnasium
College or university
Other
3. What did you do before the service? /
Studied/
Worked
Was unemployed (>6kk)/
Took a year off (travelling
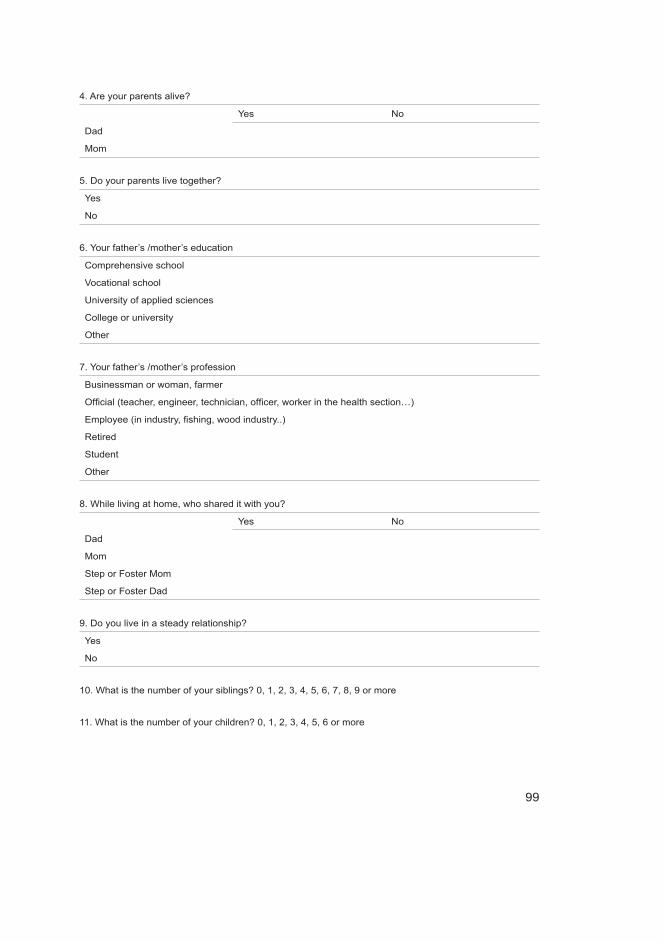
99
4. Are your parents alive?
Yes No
Dad
Mom
5. Do your parents live together?
Yes
No
6. Your father’s /mother’s education
Comprehensive school
Vocational school
University of applied sciences
College or university
Other
7. Your father’s /mother’s profession
Businessman or woman, farmer
Official (teacher, engineer, technician, officer, worker in the health section…)
Employee (in industry, fishing, wood industry..)
Retired
Student
Other
8. While living at home, who shared it with you?
Yes No
Dad
Mom
Step or Foster Mom
Step or Foster Dad
9. Do you live in a steady relationship?
Yes
No
10. What is the number of your siblings? 0, 1, 2, 3, 4, 5, 6, 7, 8, 9 or more
11. What is the number of your children? 0, 1, 2, 3, 4, 5, 6 or more

100
12. During past 6 months how often have you
Never or hardly ever Every day or almost
every day
Occasionally
Exercised or done sports?
Been to movies or theatre or
sports events or played music
or read?
Spent time with friends,
played with friends?
Been to bars or pubs?
Watched TV or played
computer games?
Been in nature or gone fishing
or hunting?
Done handicrafts (wood work,
metal work, painting etc.)?
Done motor sports (car, motor
cycle)?
13. How often do you do physical exercise?
Never
1–2 times a month
1–2 times a week
3–4 times a week
more than 5 times a week
14. During past 12 months how often have you been temporarily sick (common cold etc.)?
Less than once a year
1–2 times a year
3–4 times a year
more than 5 times a year
15. Do you have a chronic illness requiring regular medication? Yes/No
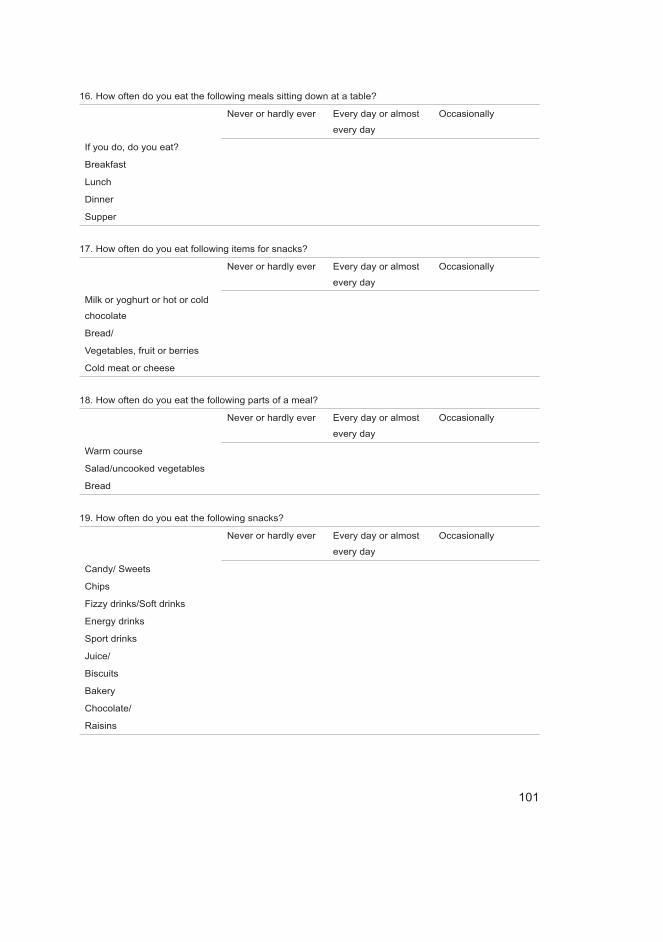
101
16. How often do you eat the following meals sitting down at a table?
Never or hardly ever Every day or almost
every day
Occasionally
If you do, do you eat?
Breakfast
Lunch
Dinner
Supper
17. How often do you eat following items for snacks?
Never or hardly ever Every day or almost
every day
Occasionally
Milk or yoghurt or hot or cold
chocolate
Bread/
Vegetables, fruit or berries
Cold meat or cheese
18. How often do you eat the following parts of a meal?
Never or hardly ever Every day or almost
every day
Occasionally
Warm course
Salad/uncooked vegetables
Bread
19. How often do you eat the following snacks?
Never or hardly ever Every day or almost
every day
Occasionally
Candy/ Sweets
Chips
Fizzy drinks/Soft drinks
Energy drinks
Sport drinks
Juice/
Biscuits
Bakery
Chocolate/
Raisins
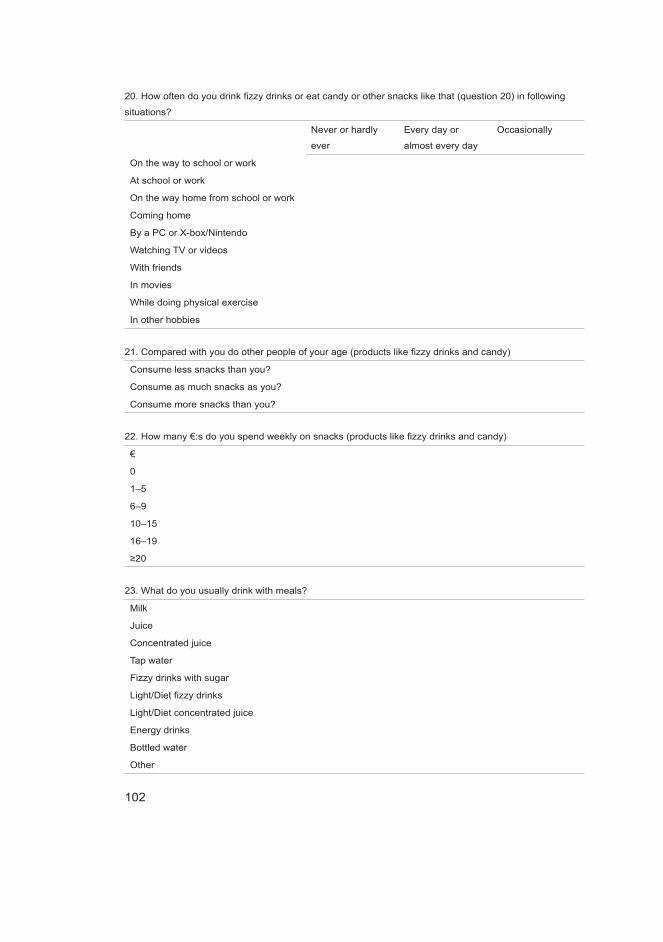
102
20. How often do you drink fizzy drinks or eat candy or other snacks like that (question 20) in following
situations?
Never or hardly
ever
Every day or
almost every day
Occasionally
On the way to school or work
At school or work
On the way home from school or work
Coming home
By a PC or X-box/Nintendo
Watching TV or videos
With friends
In movies
While doing physical exercise
In other hobbies
21. Compared with you do other people of your age (products like fizzy drinks and candy)
Consume less snacks than you?
Consume as much snacks as you?
Consume more snacks than you?
22. How many €:s do you spend weekly on snacks (products like fizzy drinks and candy)
€
0
1–5
6–9
10–15
16–19
≥20
23. What do you usually drink with meals?
Milk
Juice
Concentrated juice
Tap water
Fizzy drinks with sugar
Light/Diet fizzy drinks
Light/Diet concentrated juice
Energy drinks
Bottled water
Other

103
24. What do you usually drink to quench thirst
Milk
Juice
Concentrated juice
Tap water
Fizzy drinks with sugar
Light/Diet fizzy drinks
Light/Diet concentrated juice
Energy drinks
Bottled water
Other
25. Do you use
Never or hardly ever Every day or almost
every day
Occasionally
Energy drinks?
Sports drinks?
26. Do you smoke?
No
1–5 cigarettes daily
10–20 cigarettes daily
>20 cigarettes daily
27. Do you consume alcohol?
No
Less than once a month
About once a month
About every other week
About every week
More than once a week
28. Do you use snuff?
Never or hardly ever
Every day or almost every day
Occasionally
29. If you use chewing gum, how often?
Never or hardly ever
Every day or almost every day
Occasionally
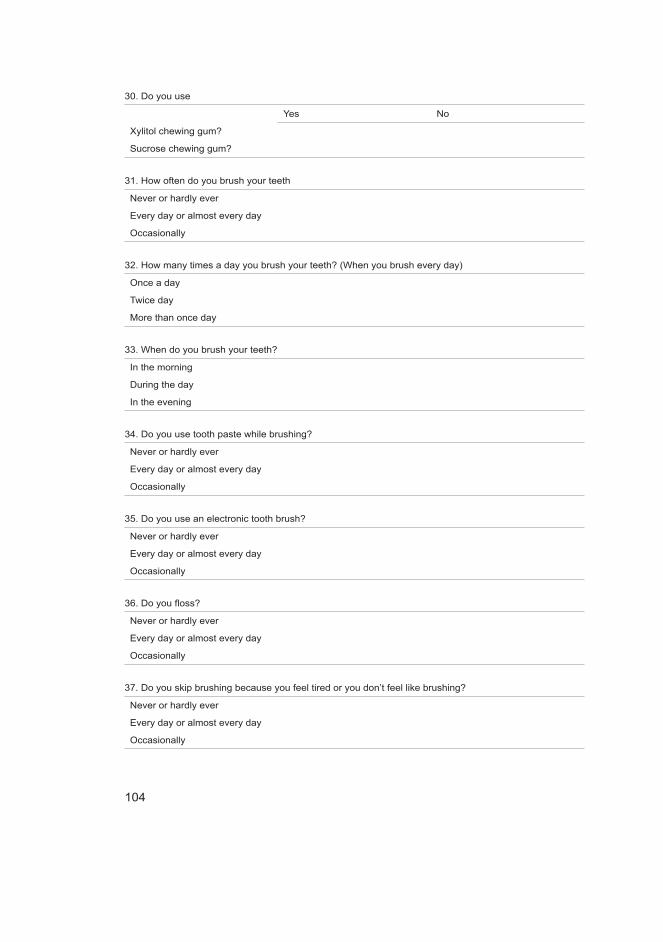
104
30. Do you use
Yes No
Xylitol chewing gum?
Sucrose chewing gum?
31. How often do you brush your teeth
Never or hardly ever
Every day or almost every day
Occasionally
32. How many times a day you brush your teeth? (When you brush every day)
Once a day
Twice day
More than once day
33. When do you brush your teeth?
In the morning
During the day
In the evening
34. Do you use tooth paste while brushing?
Never or hardly ever
Every day or almost every day
Occasionally
35. Do you use an electronic tooth brush?
Never or hardly ever
Every day or almost every day
Occasionally
36. Do you floss?
Never or hardly ever
Every day or almost every day
Occasionally
37. Do you skip brushing because you feel tired or you don’t feel like brushing?
Never or hardly ever
Every day or almost every day
Occasionally
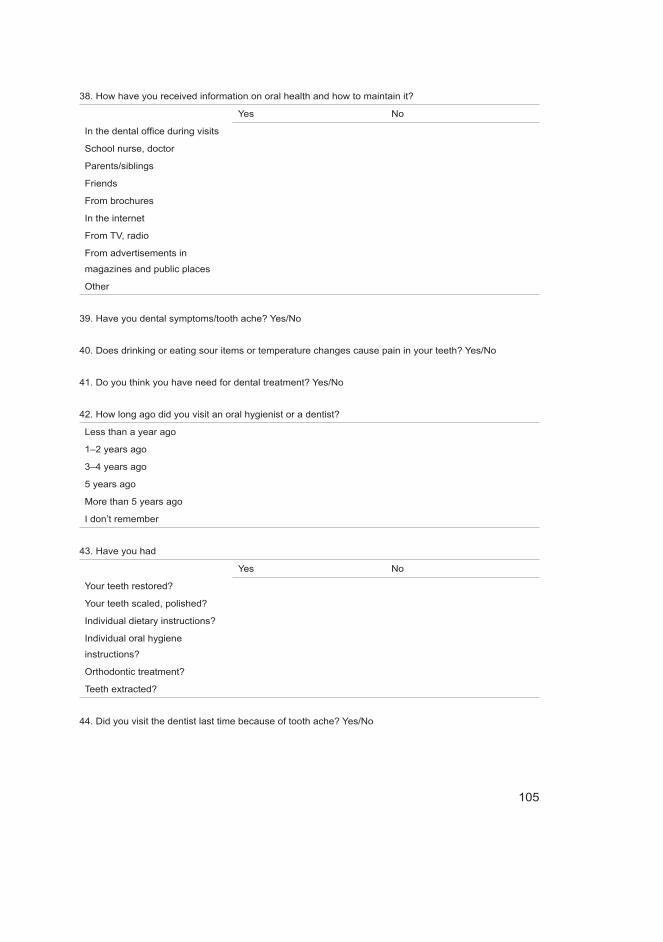
105
38. How have you received information on oral health and how to maintain it?
Yes No
In the dental office during visits
School nurse, doctor
Parents/siblings
Friends
From brochures
In the internet
From TV, radio
From advertisements in
magazines and public places
Other
39. Have you dental symptoms/tooth ache? Yes/No
40. Does drinking or eating sour items or temperature changes cause pain in your teeth? Yes/No
41. Do you think you have need for dental treatment? Yes/No
42. How long ago did you visit an oral hygienist or a dentist?
Less than a year ago
1–2 years ago
3–4 years ago
5 years ago
More than 5 years ago
I don’t remember
43. Have you had
Yes No
Your teeth restored?
Your teeth scaled, polished?
Individual dietary instructions?
Individual oral hygiene
instructions?
Orthodontic treatment?
Teeth extracted?
44. Did you visit the dentist last time because of tooth ache? Yes/No
106
45. During past 12 months have you had pain
Not at all Occasionally Quite often Often/all the
time
In your face?
In your jaws?
46. Have you had following symptoms in your temporomandibular joints?
Not at all Occasionally Quite often Often/ all the
time
Pain at rest
Pain while moving the
mandible
Noise (rattling and cracking)
of the joints
Difficulty in opening the mouth
47. Do you have your teeth checked regularly? Yes/No
48. Do you usually visit
A private dentist?
A municipal dentist?
49. Do you find visiting a dentist
Not at all scary?
A little/somewhat scary?
Very scary?
50. Does your dentition influence your wellbeing?
Dentition has a positive influence on wellbeing (e.g. beautiful teeth)
Dentition has a negative influence on wellbeing (e.g. symptoms, or feel ashamed of the appearance)
No influence

107
Original papersI Anttonen V, Tanner T, Kämppi A, Päkkilä J, Tjäderhane L, Patinen P (2012) A
methodological pilot study on oral health of young, healthy males. Dent Hypotheses 3:106–111.
II Tanner T, Kämppi A, Päkkilä J, Patinen P, Rosberg J, Karjalainen K, Järvelin M-R, Tjäderhane L, Anttonen V (2013) Prevalence and polarization of dental caries among young, healthy adults – Cross-sectional epidemiological study. Acta Odontol Scand 71:1436–1442.
III Tanner T, Kämppi A, Päkkilä J, Järvelin M-R, Patinen P, Tjäderhane L, Anttonen V (2014) Association of smoking and snuffing with dental caries occurrence in a young male population in Finland: A cross-sectional study. Acta Odontol Scand 72:1017–1024.
IV Tanner T, Päkkilä J, Karjalainen K, Kämppi A, Järvelin M-R, Patinen P, Tjäderhane L, Anttonen V (2015) Smoking, alcohol use, socio-economic background and oral health among young Finnish adults. Community Dent Oral Epidemiol Apr 24 doi: 10.1111/cdoe.12163. [Epub ahead of print]
Reprinted with permission from Wolters Kluwer – Medknow (I)Reprinted with permission from Informa Healthcare (II-III). Reprinted with permission from John Wiley & Sons Ltd (IV)
Original publications are not included in the electronic version of the dissertation.


A C T A U N I V E R S I T A T I S O U L U E N S I S
Book orders:Granum: Virtual book storehttp://granum.uta.fi/granum/
S E R I E S D M E D I C A
1288. Karsikas, Sara (2015) Hypoxia-inducible factor prolyl 4-hydroxylase-2 in cardiacand skeletal muscle ischemia and metabolism
1289. Takatalo, Jani (2015) Degenerative findings on MRI of the lumbar spine :prevalence, environmental determinants and association with low back symptoms
1290. Pesonen, Hanna-Mari (2015) Managing life with a memory disorder : the mutualprocesses of those with memory disorders and their family caregivers following adiagnosis
1291. Pruikkonen, Hannele (2015) Viral infection induced respiratory distress inchildhood
1292. Vähänikkilä, Hannu (2015) Statistical methods in dental research, with specialreference to time-to-event methods
1293. Sipola-Leppänen, Marika (2015) Preterm birth and cardiometabolic risk factors inadolescence and early adulthood
1294. Koskenkorva, Timo (2015) Outcome after tonsillectomy in adult patients withrecurrent pharyngitis
1295. Pietilä, Riikka (2015) Angiopoietin 1 and 2-regulated Tie2 receptor translocationin endothelial cells and investigation of Angiopoietin-2 splice variant 443
1296. Timlin, Ulla (2015) Adolescent's adherence to treatment in psychiatric care
1297. Aatsinki, Sanna-Mari (2015) Regulation of hepatic glucose homeostasis andCytochrome P450 enzymes by energy-sensing coactivator PGC-1α
1298. Rissanen, Ina (2015) Nervous system medications and suicidal ideation andbehaviour : the Northern Finland Birth Cohort 1966
1299. Puurunen, Johanna (2015) Androgen secretion and cardiovascular risk factors inwomen with and without PCOS : studies on age-related changes and medicalintervention
1300. Pakanen, Lasse (2015) Thrombomodulin and catecholamines as post-mortemindicators of hypothermia
1301. Mäkelä, Mailis (2015) Hoitoon ja kohteluun kohdistuva tyytymättömyys :potilaslain mukaiset muistutukset
1302. Nordström, Tanja (2015) Predisposing factors and consequences of adolescentADHD and DBD : a longitudinal study in the Northern Finland Birth Cohort1986

UNIVERSITY OF OULU P .O. Box 8000 F I -90014 UNIVERSITY OF OULU FINLAND
A C T A U N I V E R S I T A T I S O U L U E N S I S
Professor Esa Hohtola
University Lecturer Santeri Palviainen
Postdoctoral research fellow Sanna Taskila
Professor Olli Vuolteenaho
University Lecturer Veli-Matti Ulvinen
Director Sinikka Eskelinen
Professor Jari Juga
University Lecturer Anu Soikkeli
Professor Olli Vuolteenaho
Publications Editor Kirsti Nurkkala
ISBN 978-952-62-0854-1 (Paperback)ISBN 978-952-62-0855-8 (PDF)ISSN 0355-3221 (Print)ISSN 1796-2234 (Online)
U N I V E R S I TAT I S O U L U E N S I S
MEDICA
ACTAD
D 1303
ACTA
Tarja Tanner
OULU 2015
D 1303
Tarja Tanner
HEALTHY YOUNG ADULTS' ORAL HEALTH AND ASSOCIATED FACTORSCROSS-SECTIONAL EPIDEMIOLOGICAL STUDY
UNIVERSITY OF OULU GRADUATE SCHOOL;UNIVERSITY OF OULU,FACULTY OF MEDICINE;MEDICAL RESEARCH CENTER OULU;OULU UNIVERSITY HOSPITAL;FINNISH DOCTORAL PROGRAM IN ORAL SCIENCES FINDOS