thoracic trauma tresna
DESCRIPTION
Thoracic TraumaTRANSCRIPT
Thoracic Trauma
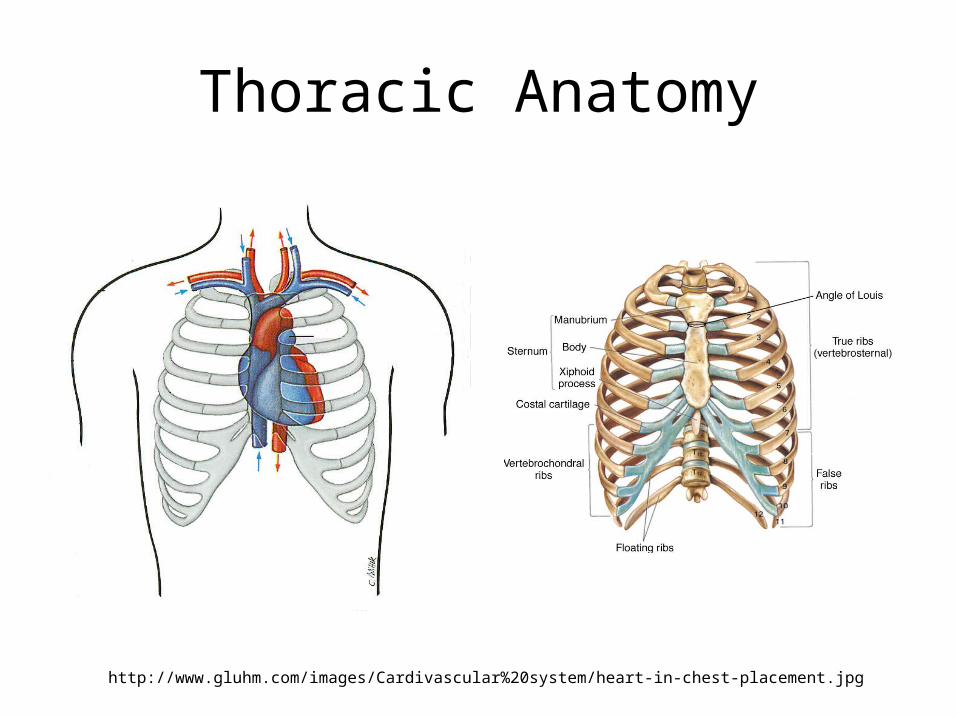
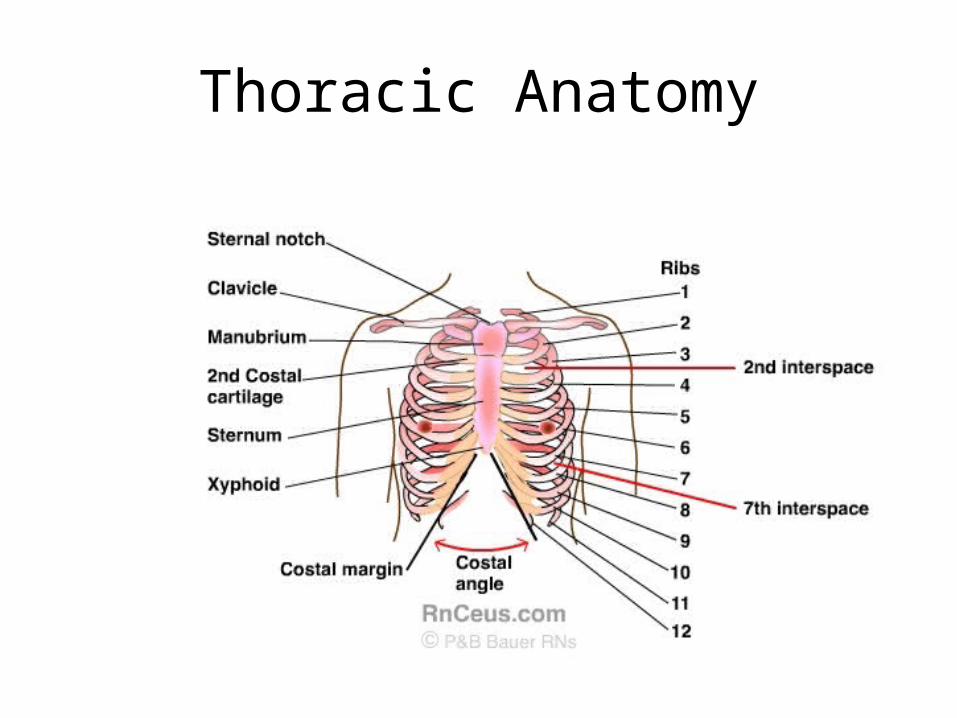
Thoracic Anatomy
http://www.gluhm.com/images/Cardivascular%20system/heart-in-chest-placement.jpg
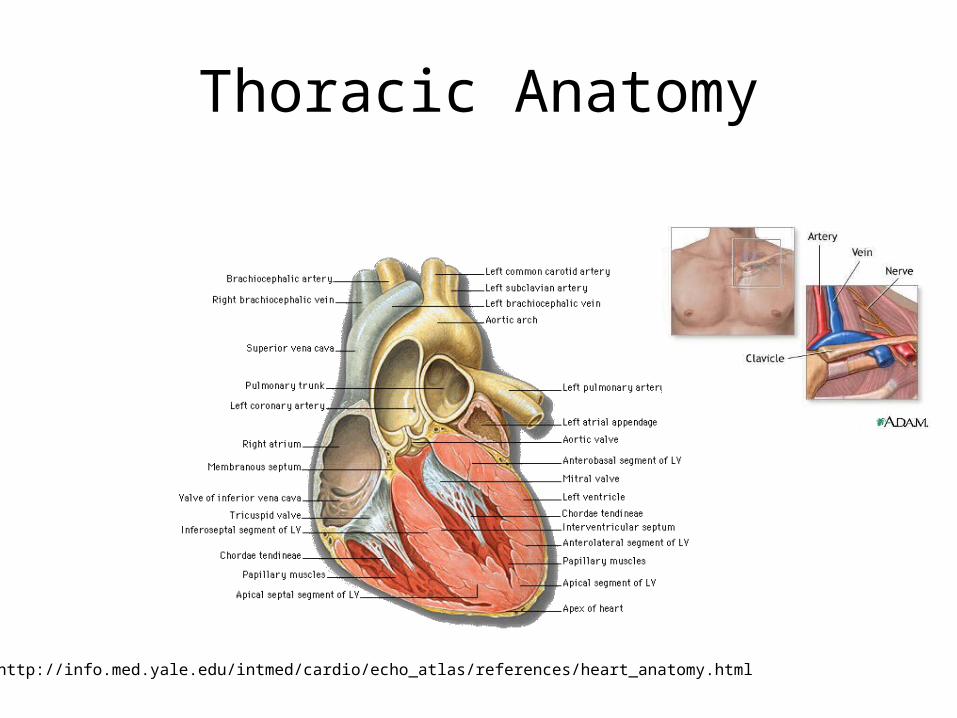
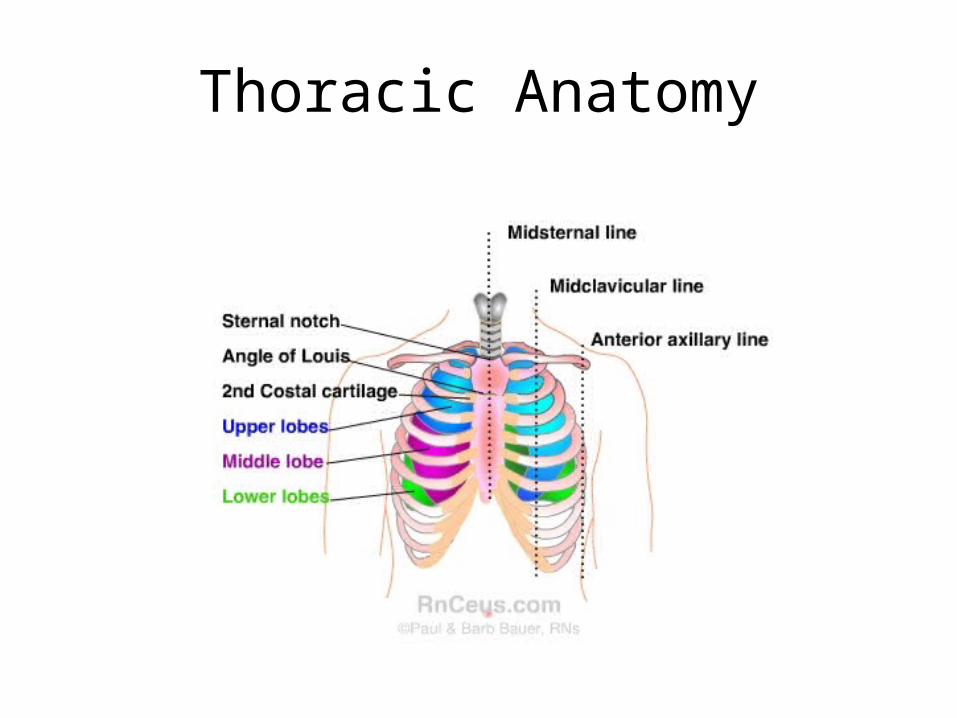
Thoracic Anatomy
http://info.med.yale.edu/intmed/cardio/echo_atlas/references/heart_anatomy.html

Thoracic Anatomy
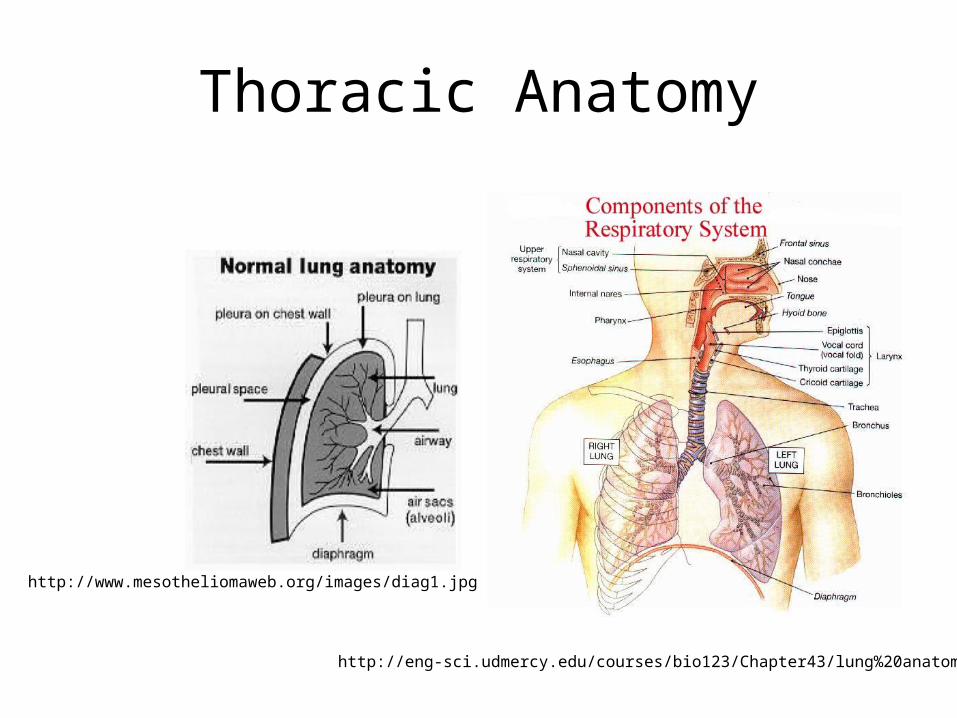
Thoracic Anatomy
http://www.mesotheliomaweb.org/images/diag1.jpg
http://eng-sci.udmercy.edu/courses/bio123/Chapter43/lung%20anatomy.html
Thoracic Anatomy
Thoracic Anatomy
Thoracic Trauma• 25% of nonmilitary trauma
related deaths.• Mortality 5% for isolated chest
trauma• Two or more organ systems
1/3 mortality• Nearly all penetrating injuries
result in pneumothorax with hemothorax in more than 75% of cases.
• Of penetrating trauma, 1/3 will be associated with abdominal injuries.
• Mechanisms of blunt trauma: compression, direct trauma, and accel/decel forces.
• 25% kematian terkait trauma non militer.
• Kematian 5% untuk trauma dada terisolasi
• Dua atau lebih sistem organ 1/3 kematian
• Hampir semua luka tembus mengakibatkan pneumotoraks dengan hemothorax di lebih dari 75% kasus.
• Trauma penetrasi, 1/3 akan terkait dengan cedera perut.
• Mekanisme trauma tumpul: kompresi, trauma langsung, dan pasukan accel / Decel.
Diagnosing Thoracic Injuries
• Symptoms: Chest pain and SOB.
• Physical Exam.• Look for six major
conditions.• Think of mechanism of
injury.• Don’t forget about liver
and spleen.
• Gejala: Nyeri dada dan SOB.
• Ujian Fisik.• Carilah enam syarat
utama.• Pikirkan mekanisme
cedera.• Jangan lupa tentang
hati dan limpa.
Chest Wounds• Lethal six injuries:
– Airway obstruction– Tension pneumothorax– Pericardial tamponade– Open pneumothorax– Massive hemothorax– Flail chest
• The Box: bounded by nipples bilat, costal margin inferiorly, and thoracic inlet superiorly– Have high suspicion of
cardiac injury
• Lethal enam luka:• obstruksi jalan napas• ketegangan
pneumotoraks• tamponade perikardial• Buka pneumotoraks• hemothorax besar• flail chest• The Box: dibatasi oleh
puting bilat, inferior batas kosta, dan cerukan dada superior
• Memiliki kecurigaan yang tinggi cedera jantung
Inspection
• Chest Wall: look for signs of injury such as contusions, flail chest, open chest wounds.
• Neck: Distended neck veins, subcutaneous emphysema, swelling and cyanosis
• Abdomen: scaphoid abdomen
• Dada Wall: mencari tanda-tanda cedera seperti memar, flail chest, luka dada terbuka.
• Leher: buncit vena leher, emfisema subkutan, pembengkakan dan sianosis
• Abdomen: perut skafoid
Physical Exam
• Palpation: trachea position, tenderness, or crepitus.
• Percussion: dullness for hemothorax and hyperresonance for pneumothorax
• Auscultation: Equal breath sounds, bowel sounds high in chest.
• Palpasi: Posisi trakea, nyeri, atau krepitus.
• Perkusi: kusam untuk hemothorax dan hyperresonance untuk pneumothorax
• Auskultasi: suara nafas yang sama, usus suara tinggi dalam dada.
Pneumothorax• Can cause severe symptoms
if:– Tensions pneumothorax– Occupies >40% of hemithorax– Pt in shock or preexisting
cardiopulmonary disease.• Occasionally can be
delayed.• Can repeat film in 6hrs and.• Occult Pneumo: requires
chest tube if patient is going on a ventilator.
• Dapat menyebabkan gejala berat jika:
• ketegangan pneumotoraks• Menempati> 40% dari
hemithorax• Pt shock atau riwayat
penyakit kardiopulmoner.• Kadang-kadang dapat
ditunda.• Dapat mengulangi film 6hrs
dan.• Okultisme Pneumo:
memerlukan tabung dada jika pasien yang sedang terjadi ventilator.
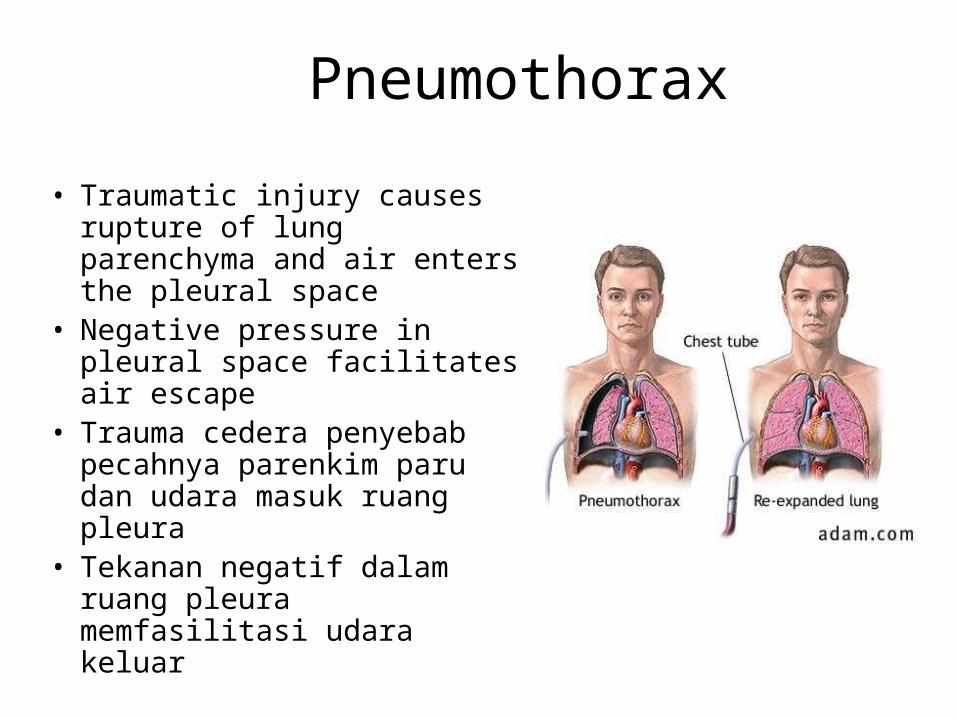
Pneumothorax
• Traumatic injury causes rupture of lung parenchyma and air enters the pleural space
• Negative pressure in pleural space facilitates air escape
• Trauma cedera penyebab pecahnya parenkim paru dan udara masuk ruang pleura
• Tekanan negatif dalam ruang pleura memfasilitasi udara keluar
Pneumothorax – Types• Simple Pneumothorax –
air seen on CXR with no vital sign derangements and no mediastinal shift.
• Tension Pneumothorax – continued air leakage into closed space causes significant lung collapse, compression of mediastinum, and compression of opposite hemi-thorax
• Pneumotoraks sederhana - udara terlihat pada CXR tanpa kekacauan tanda vital dan tidak ada pergeseran mediastinum.
• Ketegangan Pneumotoraks - kebocoran udara terus ke ruang tertutup menyebabkan kolaps paru yang signifikan, kompresi mediastinum, dan kompresi berlawanan hemi-thorax
Pneumothorax – Types• Open Pneumothorax –
from penetrating injury– If significant enough in size
will cause “Sucking Chest Wound”
• Spontaneous Pneumothorax – typically occurs in tall, slender teenagers due to congenital area of lung weakness.– Also seen asthma, COPD,
restrictive lung dz
• Buka Pneumotoraks - dari cedera penetrasi
• Jika cukup signifikan dalam ukuran akan menyebabkan "Mengisap Dada Luka"
• Pneumotoraks spontan - biasanya terjadi pada tinggi, remaja ramping karena wilayah bawaan kelemahan paru-paru.
• Juga terlihat asma, PPOK, membatasi dz paru
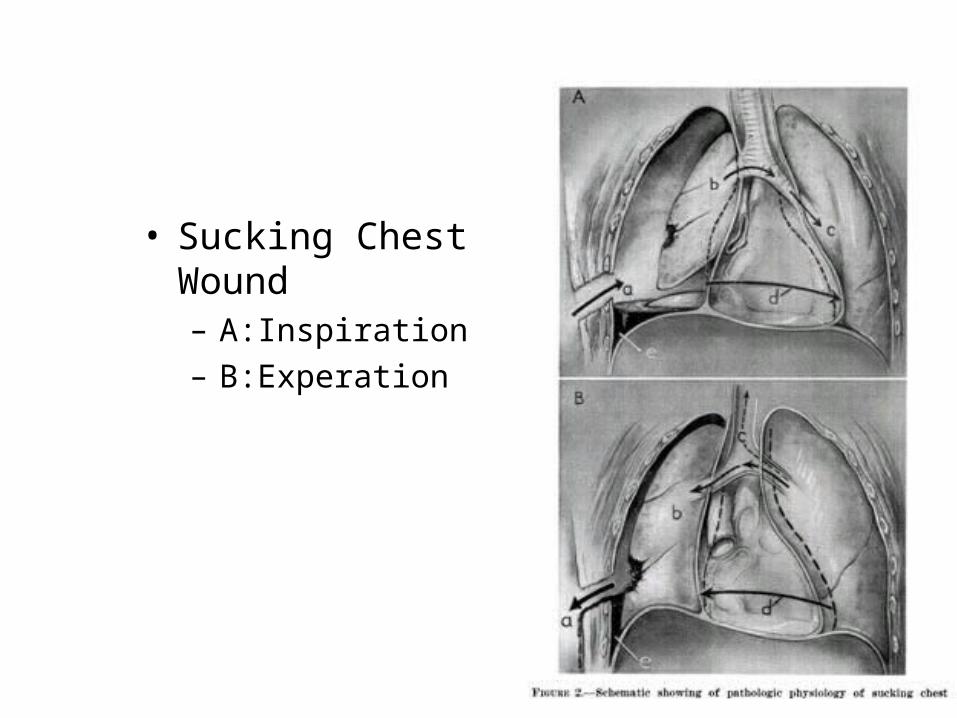
• Sucking Chest Wound– A:Inspiration– B:Experation
Pneumothorax – Exam findings• Simple Pneumothorax
– Diminished lung sounds (hilangnya suara paru)
– Tachycardia – Tachypnea– Dyspnea– Pleuritic chest pain– Hyper-resonant to
percussion
• Tension Pneumothorax– JVD– Tracheal shift (Deviasi
trakea)– Diminished SpO2
– Absent breath sounds– Diminished breath sounds
on opposite side (hilangya suara napas disebelah)
– Hypotension– Narrowing pulse pressure
(tekanan nadi sempit)
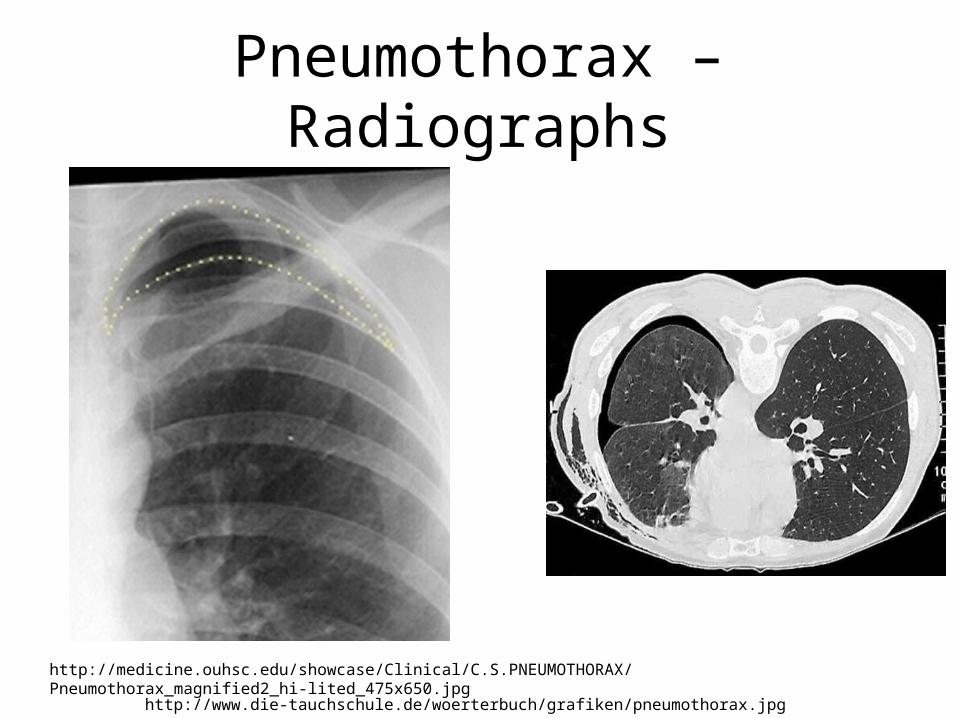
Pneumothorax – Radiographs
http://medicine.ouhsc.edu/showcase/Clinical/C.S.PNEUMOTHORAX/Pneumothorax_magnified2_hi-lited_475x650.jpg
http://www.die-tauchschule.de/woerterbuch/grafiken/pneumothorax.jpg
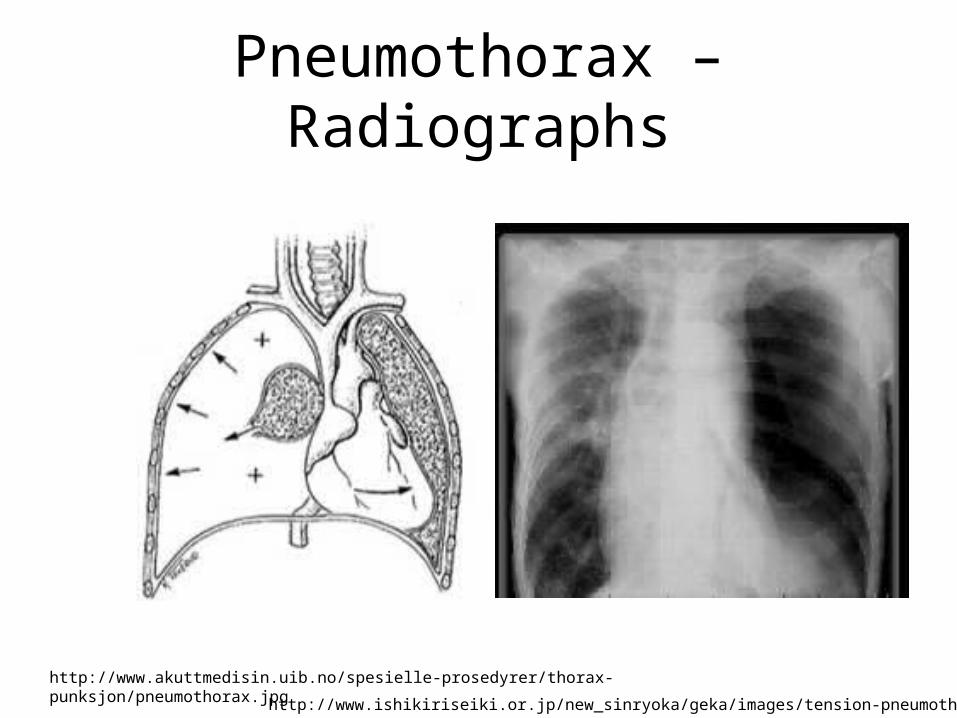
Pneumothorax – Radiographs
http://www.akuttmedisin.uib.no/spesielle-prosedyrer/thorax-punksjon/pneumothorax.jpg http://www.ishikiriseiki.or.jp/new_sinryoka/geka/images/tension-pneumothorax1.jpg
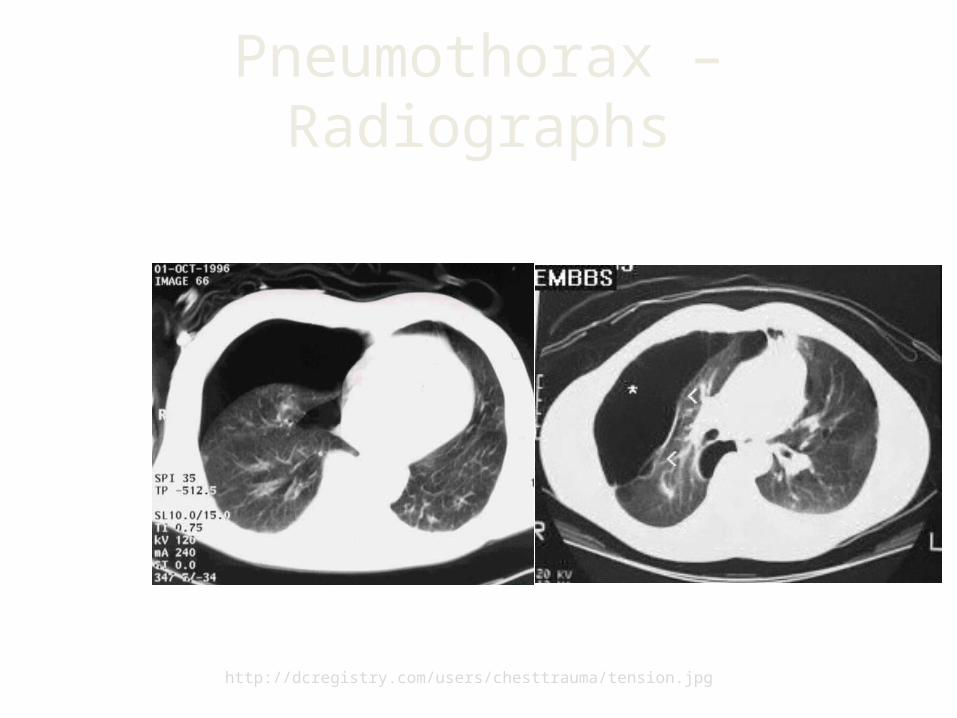
Pneumothorax – Radiographs
http://dcregistry.com/users/chesttrauma/tension.jpg
Pneumothorax – Treatment• All types of pneumothorax
– ABCs, supportive care, early notification
– High flow oxygen– Rapid transport if unstable
vitals
• Open pneumothorax– Occlusive dressing placed
• Consider securing only on three sides
– Watch for signs of tension pneumothorax
• * Semua JENIS pneumotoraks
• ABC, perawatan suportif, PEMBERITAHUAN Mutasi
• Tinggi, Aliran Oksigen• Transportasi CEPAT Severe
Tanda-Tanda penting stabil• Buka pneumotoraks• Ganti oklusif ditempatkan• Pertimbangkan
mengamankan hanya FUNDS Tiga Sisi
• Perhatikan Tanda-Tanda tension pneumothorax
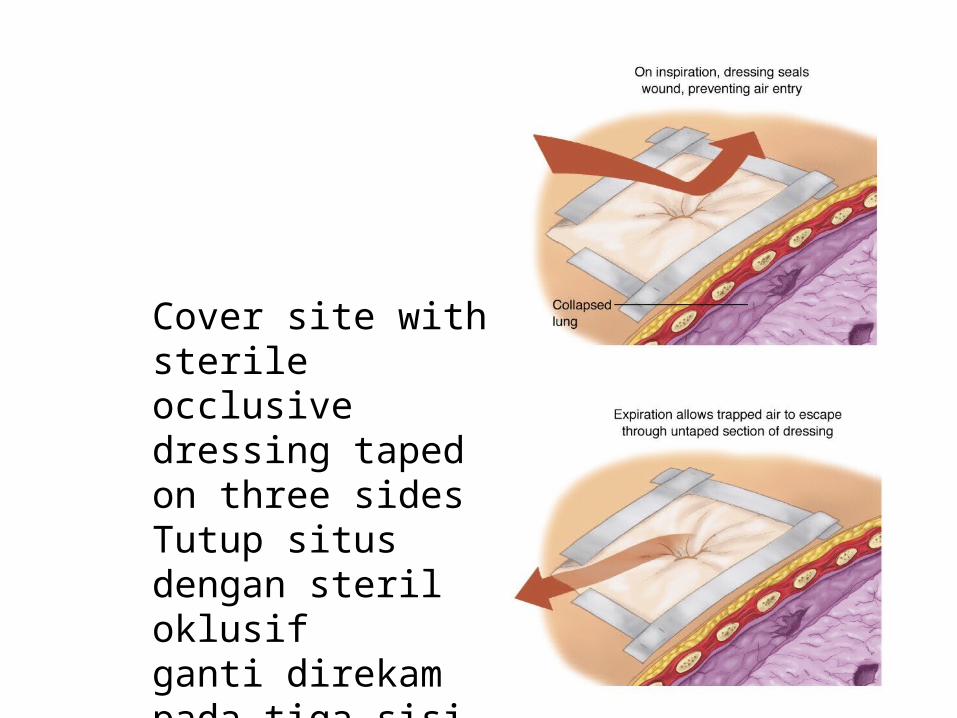
Cover site with sterile occlusive dressing taped on three sidesTutup situs dengan steril oklusifganti direkam pada tiga sisi
Pneumothorax – Treatment• Tension Pneumothorax
– Acute life threatening emergency
– Needle decompression affected side
• 2nd intercostal space mid-clavicular line -OR-
• 4th or 5th intercostal space at mid-axillary line
• Place above rib to avoid neurovascular bundle
– All needle decompressions will need chest tube upon arrival at hospital
• ketegangan Pneumotoraks• Kehidupan akut mengancam
darurat• Jarum dekompresi
mempengaruhi sisi• 2nd interkostal ruang mid-
klavikularis line-OR-• Ruang interkostal 4 atau 5 di
garis mid-aksilaris• Tempat di atas tulang rusuk
untuk menghindari bundel neurovaskular
• Semua dekompresi jarum akan membutuhkan tabung dada setelah tiba di rumah sakit
Tension Pneumothorax• Clinical diagnosis• Dyspnea, hypoperfusion,
distended neck veins, diminished breath sounds, hyperresonant percussion, tracheal deviation.
• Decompress with 14 gauge catheter – 2nd intercostal space
midclavicular line– If no improvement then
look for other cause (ie Cardiac Tamponade)
• Chest Tube
• diagnosis klinis• Dyspnea, hipoperfusi,
distensi vena leher, suara nafas berkurang, perkusi hyperresonant, deviasi trakea.
• Dekompresi dengan 14 ukuran kateter
• 2nd ruang interkostal linea• Jika tidak ada perbaikan
kemudian mencari penyebab lainnya (misalnya tamponade jantung)
• dada Tabung
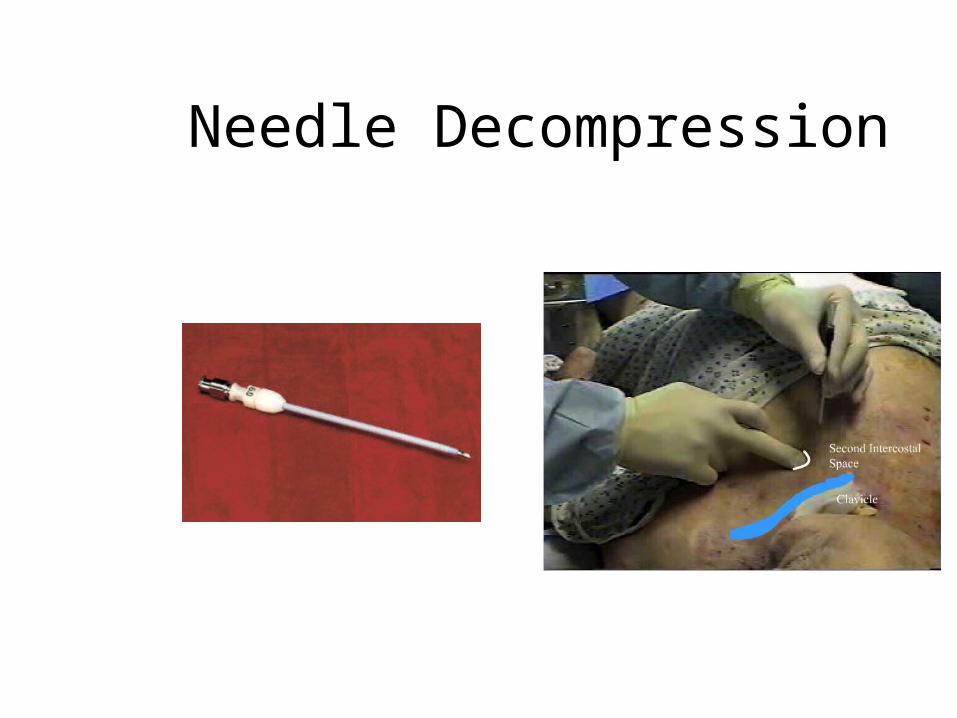
Needle Decompression
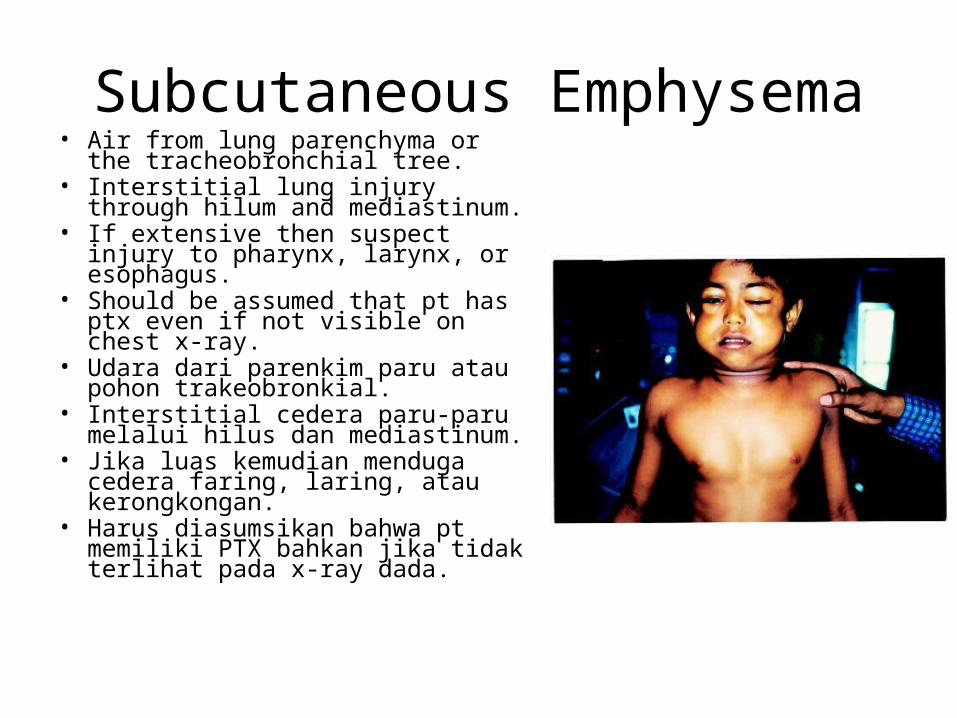
Subcutaneous Emphysema• Air from lung parenchyma or the
tracheobronchial tree.• Interstitial lung injury through hilum
and mediastinum.• If extensive then suspect injury to
pharynx, larynx, or esophagus.• Should be assumed that pt has ptx
even if not visible on chest x-ray.• Udara dari parenkim paru atau
pohon trakeobronkial.• Interstitial cedera paru-paru melalui
hilus dan mediastinum.• Jika luas kemudian menduga cedera
faring, laring, atau kerongkongan.• Harus diasumsikan bahwa pt
memiliki PTX bahkan jika tidak terlihat pada x-ray dada.
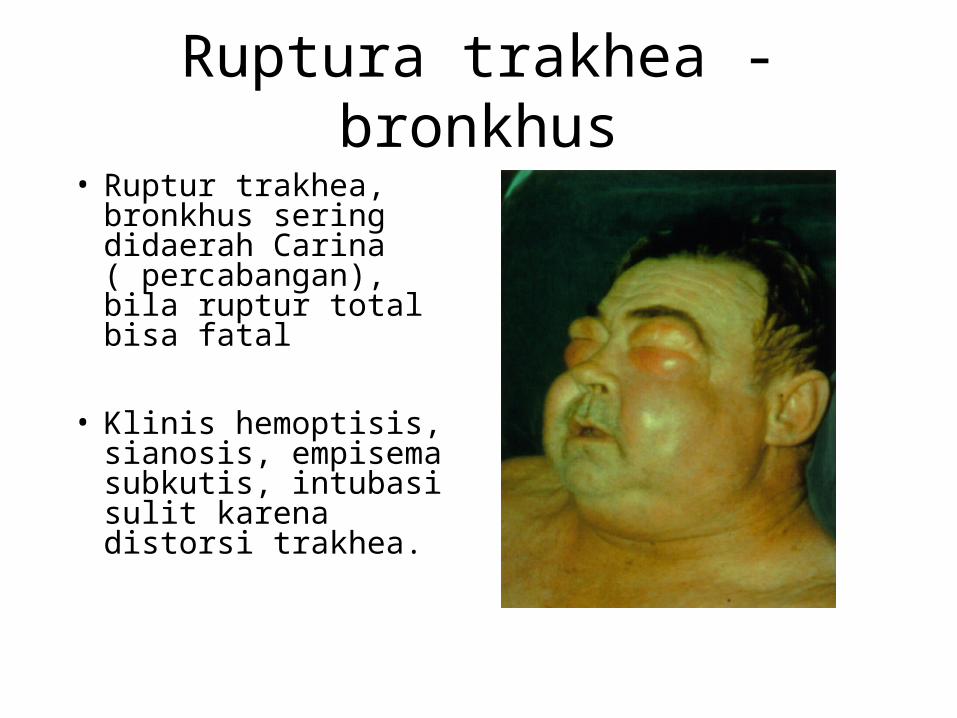
Ruptura trakhea - bronkhus• Ruptur trakhea,
bronkhus sering didaerah Carina ( percabangan), bila ruptur total bisa fatal
• Klinis hemoptisis, sianosis, empisema subkutis, intubasi sulit karena distorsi trakhea.
Hemothorax
• Most frequently from lung injury.
• 5-15% of pts admitted with chest trauma require thorocotomy.
• Upright film: 200-300 mL of blood.
• Treatment: Chest tube.
• Paling sering dari cedera paru-paru.
• 5-15% dari Poin mengaku dengan trauma dada memerlukan thorocotomy.
• Film Tegak: 200-300 mL darah.
• Pengobatan: tabung Dada.
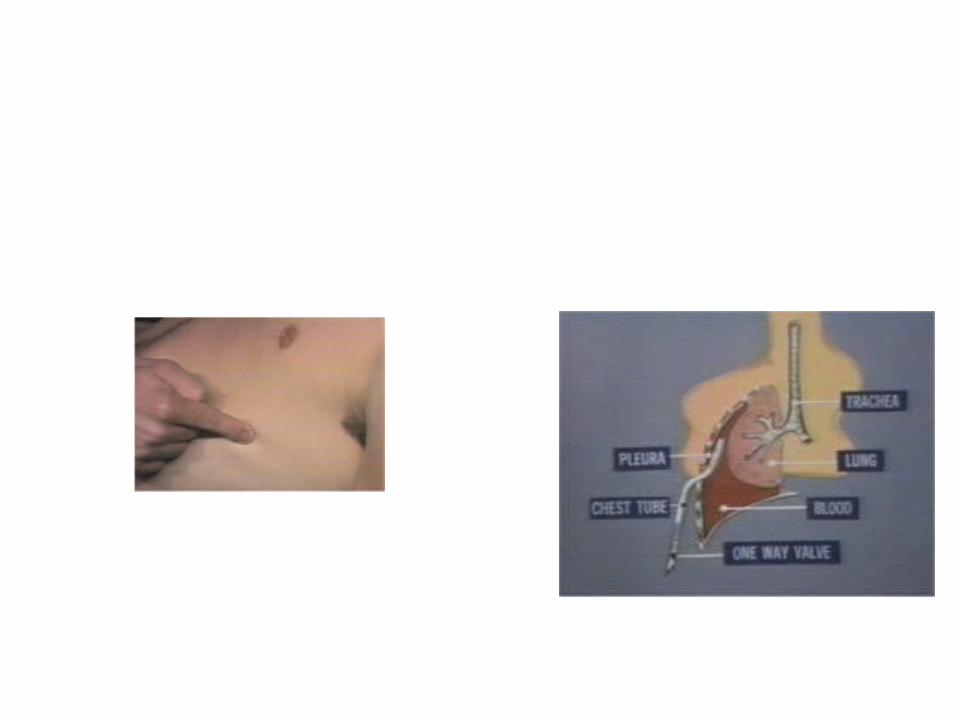
Chest Tube
• Site: anterior axillary line.
• 2-3cm incision 1-2cm below interspace.
• Extend down to intercostal muscles.
• 24F or 28F tube for pnuemothorax.
• 32F or 40F tube form hemothorax.
• Situs: garis aksilaris anterior.
• 2-3cm sayatan 1-2cm bawah sela.
• Perluas ke otot interkostal.
• Tabung 24F atau 28F untuk pnuemothorax.
• 32F atau 40F tabung bentuk hemothorax.
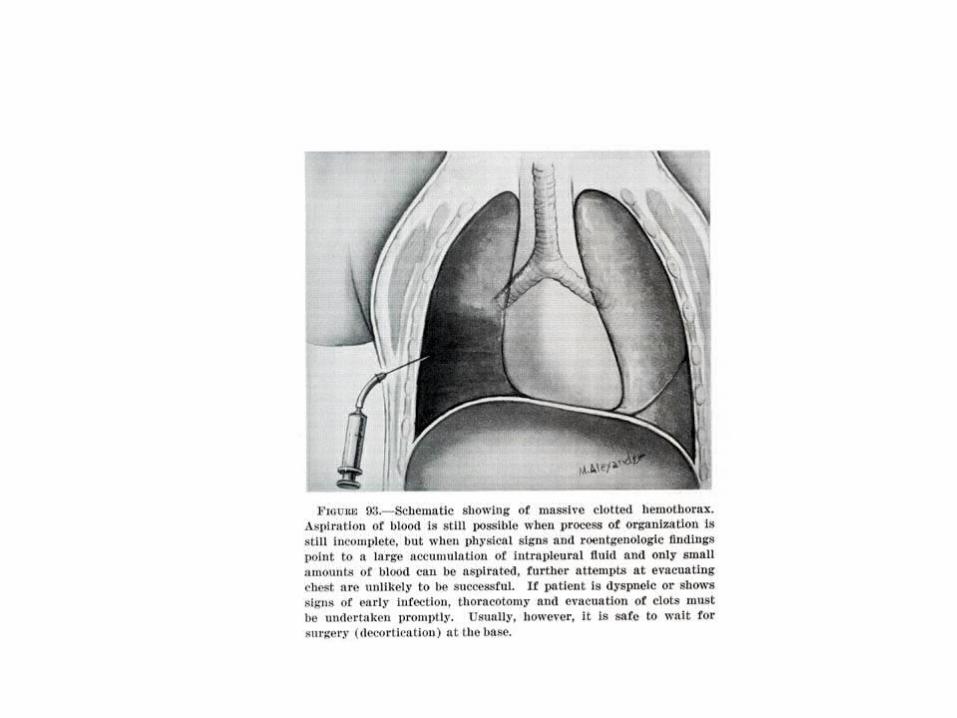
Massive Hemothorax
• Each hemithorax can hold 40-50% of blood volume.
• Defined: 1500 mL or more.
• Cause: Injury to lung parenchyma, intercostal artery or internal mammary artery
• Setiap hemithorax dapat menyimpan 40-50% dari volume darah.
• Ditetapkan: 1500 mL atau lebih.
• Penyebab: Cedera parenkim paru, arteri interkostal atau arteri mamaria interna
Massive Hemothorax
• Life threatening– Hypovolemia causing
inadequate preload– Hypoxia– Compresses the vena cava.
• Chest x-ray-Aerated lung surrounded by fluid.
• Treat: Chest tube operation
• mengancam kehidupan• Hipovolemia
menyebabkan preload memadai
• hipoksia• Kompres vena cava.• Dada rontgen paru-Aerasi
dikelilingi oleh cairan.• Treat: tabung Dada
operasi
Cardiac Tamponade
• Caused by blunt and penetrating trauma.
• Stab wounds to midchest most common cause.
• Pericardial sack has poor compliance.– 150-200 mL can result in
tamponade.
• Disebabkan oleh trauma tumpul dan tajam.
• Luka tusuk midchest penyebab paling umum.
• Kantong perikardial memiliki kepatuhan miskin.
• 150-200 mL dapat mengakibatkan tamponade.
Cardiac Tamponade• Obstruction of venous
return leading to hypoperfusion and distended neck veins.
• Becks Triad : JVD,hypotension, muffled hear tones
• Treat: Fluid bolus and Pericardiocentesis– As little as 5-10 mL can
improve cardiac performance
• Obstruksi aliran balik vena menyebabkan hipoperfusi dan distensi vena leher.
• Becks Triad: JVD, hipotensi, teredam mendengar nada
• Treat: Cairan bolus dan Pericardiocentesis
• Sesedikit 5-10 mL dapat meningkatkan kinerja jantung
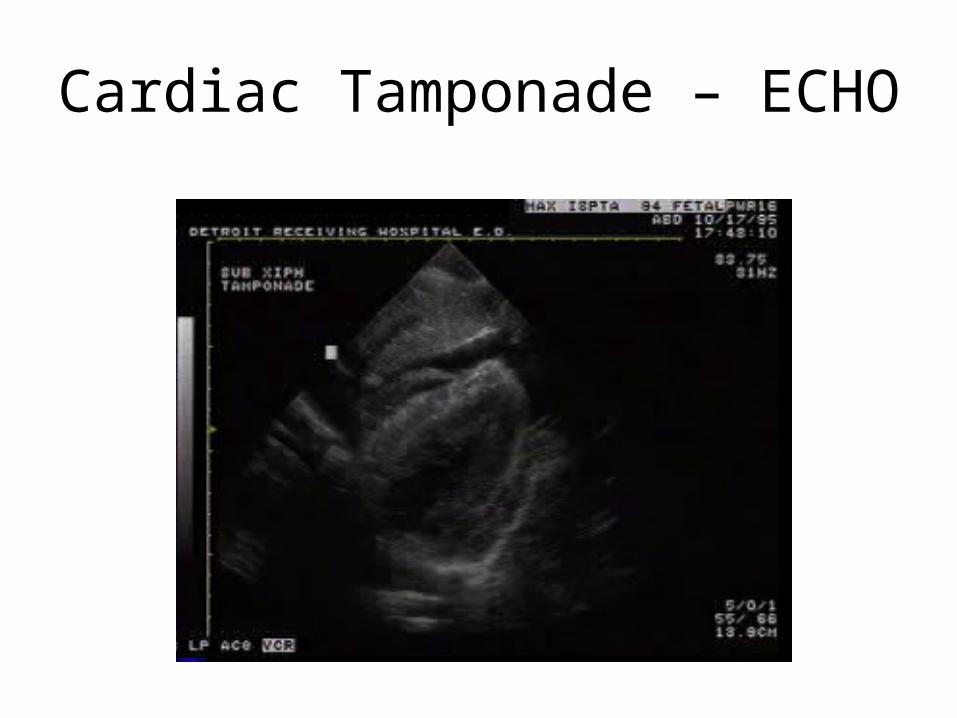
Cardiac Tamponade – ECHO
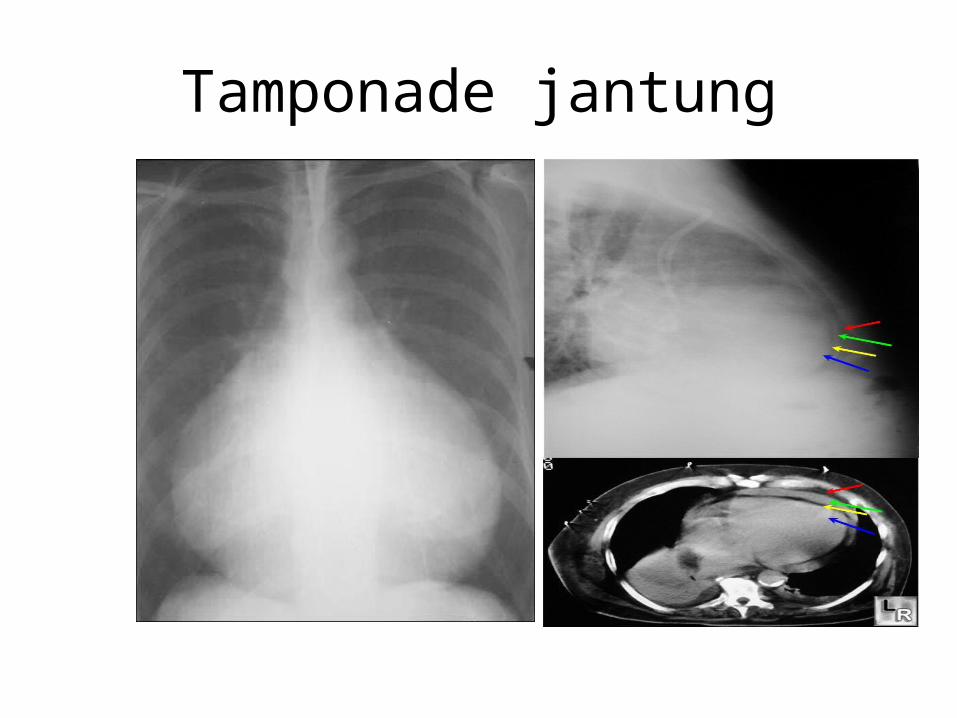
Tamponade jantung
Chest Wall Injuries• Soft tissue with bleeding:
control with pressure. Explore in OR.
• Open Chest Wounds– If exceeds 2/3 are of trachea
then air will enter through chest wall
– Cover with air tight dressing but may cause tension pneumothorax.
– Do not insert chest tube through tract.
• Tissue loss
• Jaringan lunak dengan perdarahan: kontrol dengan tekanan. Jelajahi di OR.
• Buka Luka Dada• Jika melebihi 2/3 adalah
trakea maka udara akan masuk melalui dinding dada
• Tutup dengan saus kedap udara tetapi dapat menyebabkan tension pneumothorax.
• Jangan memasukkan tabung dada melalui saluran.
• kehilangan jaringan
Bony Injuries• Simple rib fractures: 50% will
not appear on x-ray. Look for complications:
• Hemopneumothorax• Contusion
• 1st and 2nd rib fractures: requires significant force. Look for other injuries.
• Multiple: If 9,10,11 then think liver spleen injury.
• Flail Chest: Segmental fx or 3 or more adjacent ribs. Paradoxical movement. Hypoxemia from underlying contusion.
• Sederhana rusuk patah tulang: 50% tidak akan muncul pada x-ray. Carilah komplikasi:
• Hemopneumothorax• luka memar• 1 dan patah tulang rusuk 2:
membutuhkan kekuatan yang signifikan. Carilah cedera lainnya.
• Beberapa: Jika 9,10,11 kemudian berpikir cedera limpa hati.
• Flail Dada: Segmental fx atau 3 atau lebih yang berdekatan rusuk. Gerakan paradoksal. Hipoksemia dari luka memar yang mendasarinya.
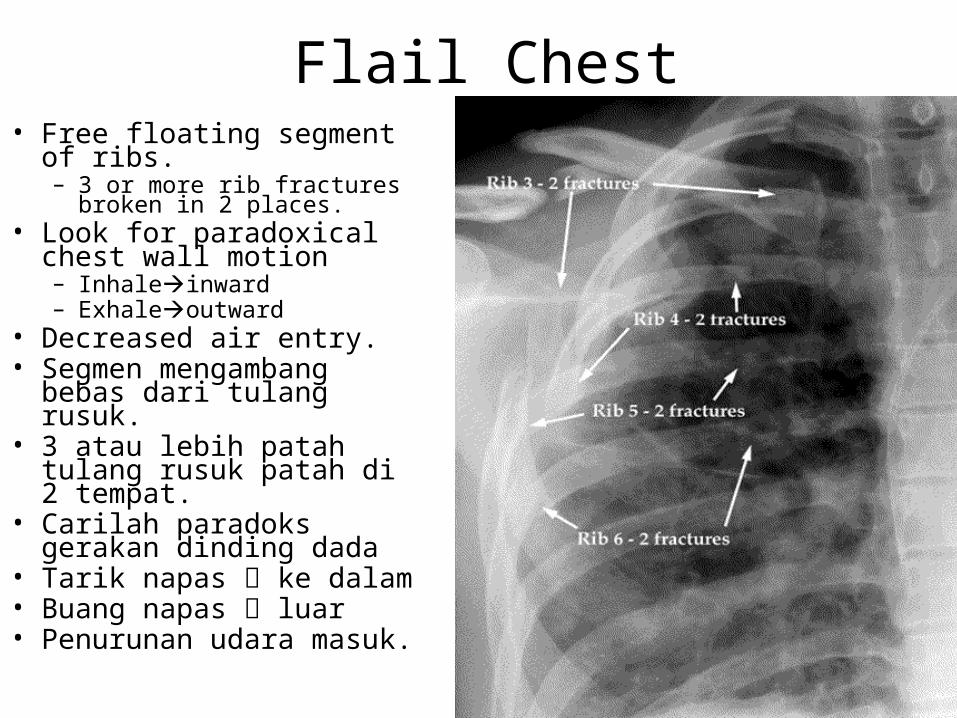
Flail Chest• Free floating segment of
ribs.– 3 or more rib fractures
broken in 2 places.• Look for paradoxical chest
wall motion– Inhaleinward– Exhaleoutward
• Decreased air entry.• Segmen mengambang
bebas dari tulang rusuk.• 3 atau lebih patah tulang
rusuk patah di 2 tempat.• Carilah paradoks gerakan
dinding dada• Tarik napas ke dalam• Buang napas luar• Penurunan udara masuk.
Flail Chest Treatment
• Analgesia and intercostal nerve block.
• Belts and adhesive tape inhibit expansion.
• Restrict IV fluids.• Ventilatory support:
shock, 3 or more injuries, head injury, pulmonary disease, >65 yrs.
• Analgesia dan blok saraf interkostal.
• Ikat pinggang dan pita perekat menghambat ekspansi.
• Batasi cairan IV.• Dukungan ventilasi:
shock, 3 atau lebih cedera, cedera kepala, penyakit paru,> 65 thn.
Consider Ventilatory Support• Respiratory failure from flail
chest.• Shock• Multiple injuries• Comatose• Requiring multiple
transfusions• Elderly• Preexisting pulmonary
disease• RR >30-35• Po2 <50 on room air
• Kegagalan pernapasan dari flail chest.
• syok• beberapa luka• pingsan• Membutuhkan beberapa
transfusi• tua• Riwayat penyakit paru• RR> 30-35• Po2 <50 pada ruang udara
Sternal Fractures
• Incidence 3%.• Normal vitals and
normal EKG. Repeat EKG in 6 hrs
• Insiden 3%.• Tanda-tanda vital
normal dan EKG normal. Ulangi EKG pada 6 hrs
Injuries to Lung
• Pulmonary Contusion
– Significant source or morbidity and mortality.
– Hemorrhage and edema without laceration.
– Caused by compression-decompression injury.
• Memar paru• Sumber yang signifikan
atau morbiditas dan mortalitas.
• Perdarahan dan edema tanpa laserasi.
• Disebabkan oleh cedera kompresi-dekompresi.
Pulmonary Contusion
• Pathological changes: capillary damage causes interstitial and intraalveolar extravasation of blood and edema.
• First hemorrhage then edema.
• Pt becomes hypoxic, hypercarbic, and acidotic.
• Perubahan patologis: kerusakan kapiler menyebabkan ekstravasasi interstitial dan intraalveolar darah dan edema.
• Perdarahan pertama kemudian edema.
• Pt menjadi hipoksia, hypercarbic, dan asidosis.
Diagnosis and Treatment
• Chest x-ray: areas of opacification seen within 6 hrs.
• Maintain adequate ventilation.
• Usually require support if more than 28% of lung volume.
• Rontgen dada: daerah kekeruhan terlihat dalam 6 jam.
• Pertahankan ventilasi yang memadai.
• Biasanya membutuhkan dukungan jika lebih dari 28% dari volume paru-paru
Pneumomediastinum• Hamman sign: crunching,
rasping sound, synchronous with heartbeat
• Suspect if subcutaneous emphysema in neck.
• Traumatic pneumomediastinum is usually asymptomatic.
• Must look for injury to the larynx, trachea, major bronchi, pharynx or esophagus.
• Hamman tanda: berderak, serak suara, sinkron dengan detak jantung
• Curiga jika subkutan emphysema di leher.
• Pneumomediastinum Traumatic biasanya tanpa gejala.
• Harus mencari cedera pada laring, trakea, bronkus utama, faring atau esofagus.
Lung Injuries
• Hematoma: parenchymal tears filled with blood. Can form abscess.
• Lacerations: major hemorrhage from sharp ends of fractured ribs.
• Air embolism: air from injured bronchus forced into vessel.
• Hematoma: air mata parenkim penuh dengan darah. Dapat membentuk abses.
• Laserasi: perdarahan besar dari ujung tajam patah tulang rusuk.
• Emboli udara: pesawat dari bronkus terluka dipaksa kapal.
Tracheobronchial Injury• Caused by rapid
deceleration. • Expiration against closed
glottis or compression against vertebral column.
• Signs and Symptom: dyspnea, hemoptysis, Hamman sign, and sternal tenderness.
• 10% asymptomatic.• Injury occurs within 2cm of
carina or at origin of lobar bronchi.
• Disebabkan oleh perlambatan cepat.
• Kadaluarsa melawan glotis tertutup atau kompresi terhadap tulang punggung.
• Tanda dan Gejala: dyspnea, hemoptisis, Hamman tanda, dan nyeri sternum.
• 10% tanpa gejala.• Cedera terjadi dalam 2cm
dari carina atau asal lobar bronkus.
Diaphragmatic Injury
• Mostly penetrating trauma.
• 4-5% from blunt trauma.
• 80-90% on left in blunt trauma.
• Often Intraop diagnosis in penetrating trauma.
• Sebagian penetrasi trauma.
• 4-5% dari trauma tumpul.
• 80-90% di kiri dalam trauma tumpul.
• Sering Intraop diagnosis pada trauma tembus.
Penetrating Injury to Heart• Factors affecting survival:
weapon used, size of myocardial injury, artery damage and presence of tamponade.
• 1/3 can be saved.• Signs of life in OR: 70%
gunshot and 85% stab wound survival.
• If no sign of life in field-do not resuscitate.
• Faktor yang mempengaruhi kelangsungan hidup: senjata yang digunakan, ukuran cedera miokard, kerusakan arteri dan adanya tamponade.
• 1/3 dapat disimpan.• Tanda-tanda kehidupan
di OR: 70% tembak dan 85% hidup luka tusuk.
• Jika tidak ada tanda-tanda kehidupan di lapangan tidak resusitasi.
Heart Injury Cont…• Usually rapidly fatal from
massive hemorrhage.• <1/4 of patients reach
hospital.
• Beck’s triad: distended neck veins, hypotension, muffled heart tones.
• Other causes: tension pneumothorax, myocardial dysfunction and systemic air embolism.
• Biasanya cepat fatal dari perdarahan masif.
• <1/4 pasien mencapai rumah sakit.
• Beck triad: distensi vena leher, hipotensi, bunyi jantung melemah.
• Penyebab lain: tension pneumothorax, disfungsi miokard dan emboli udara sistemik.
Diagnosing
• X-ray:most patients have normal silhouettes. Pericardium is noncompliant.
• EKG: nonspecific• Echo: pericardial fluid
• X-ray: kebanyakan pasien memiliki siluet normal. Perikardium adalah patuh.
• EKG: nonspesifik• Echo: cairan perikardial
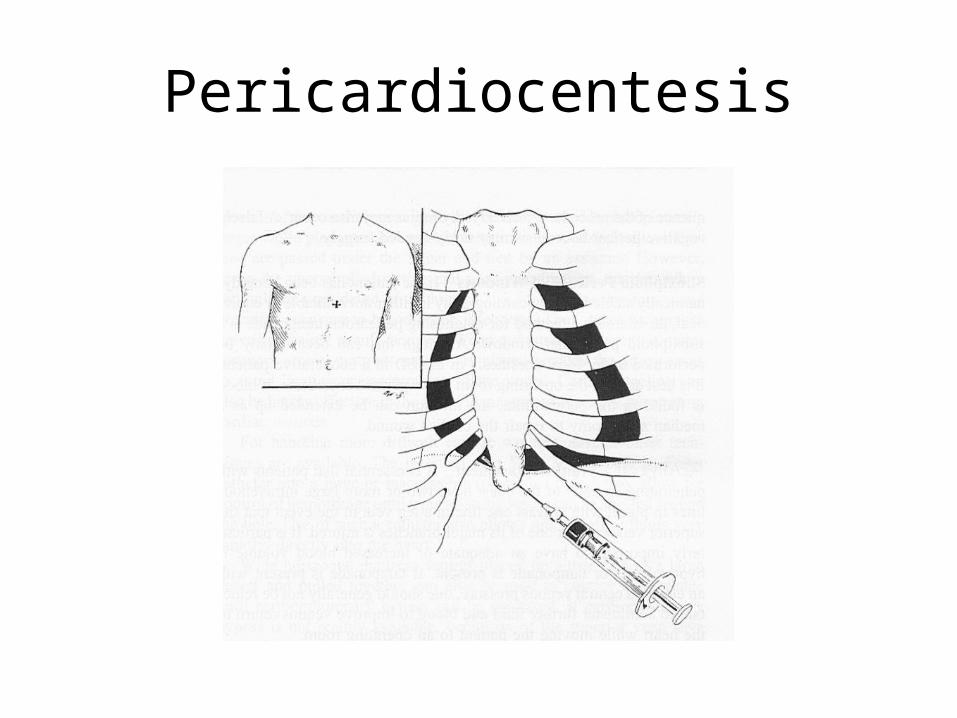
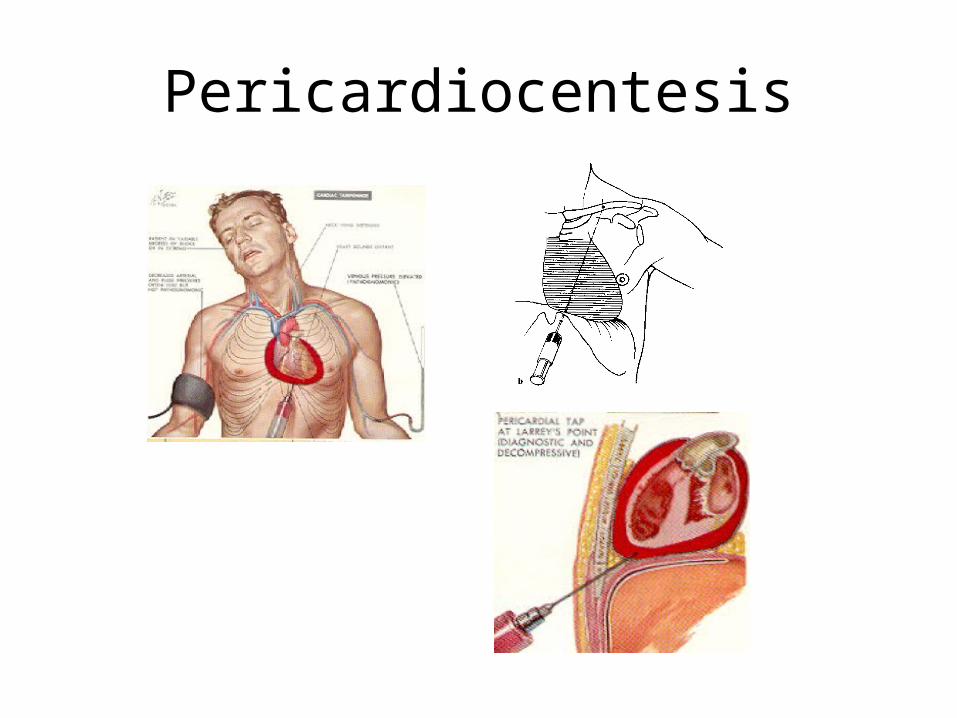
Pericardiocentesis• Paraxiphoid approach• Can direct needle toward
left scapula or right scapula (less likely to damage ventricle).
• Up and back at 45 degrees for 4-5 cm.
• Aspirate every 1-2mm.• Removal of 5-10 mL can
increase stroke volume by 25-50%.
• pendekatan Paraxiphoid• Dapat mengarahkan
jarum ke arah kiri atau kanan scapula scapula (cenderung kerusakan ventrikel).
• Dan kembali pada 45 derajat selama 4-5 cm.
• Aspirasi setiap 1-2mm.• Penghapusan 5-10 mL
dapat meningkatkan volume stroke sebesar 25-50%.
Pericardiocentesis
Pericardiocentesis

Indications For Thoracotomy/Median Sternotomy
• Hemodynamic instability with penetrating chest wound
• Massive hemothorax >1500cc• Persistent htx >200cc/hr x 4hrs or
persistent large htx despite chest tube
• Persistent air leak/tracheobronchial fistula with inability to ventilate patient
• Cardiac tamponade• Esophageal injury• Great vessel injury
• Ketidakstabilan hemodinamik dengan luka dada tembus
• Besar hemothorax> 1500cc• Persistent HTX> 200cc/hr x
4 jam atau HTX besar persisten meskipun tabung dada
• Persistent kebocoran udara / fistula tracheobronchial dengan ketidakmampuan untuk ventilasi pasien
• tamponade jantung• terserang cedera• Cedera kapal besar
Thoracotomy Indicated for Cont Bleeding In:
• Pts losing more than 1500mL in first 4-8hrs.
• Chest tube drains 200-300mL per hour.
• Chest continues to be more than half full on x-ray with functioning chest tube.
• Poin kehilangan lebih dari 1500ml di pertama 4-8hrs.
• Dada tabung saluran 200-300ml per jam.
• Dada terus menjadi lebih dari setengah penuh pada x-ray dengan berfungsi tabung dada.