standard operating procedure 3 (sop 3)
TRANSCRIPT
Enteral Feeding Page 1 of 18 Version 1.2 May 2018
Standard Operating Procedure 3 (SOP 3)
Enteral Feeding - Children, Young People and Families
Why we have a procedure?
Children who are unable to meet their nutritional requirements orally but have a functioning gut are increasingly being enterally fed. An enteral tube is used to deliver a nutritionally complete feed via a tube. The use of Enteral Tube feeding is important and rapidly growing in the community setting. Most children requiring Enteral Feeding receive it directly into their stomach via either a Gastrostomy tube or a Nasogastric tube.
What overarching policy the procedure links to?
Children’s Community Nursing Team Operational Policy
Which services of the trust does this apply to? Where is it in operation?
Group Inpatients Community Locations
Mental Health Services all
Learning Disabilities Services all
Children and Young People Services all
Who does the procedure apply to?
This Enteral Feeding procedure is intended to provide information to all healthcare professionals involved with Enteral Feeding within community settings. This procedure has been developed for use by all clinical staff working in Black Country Partnership Foundation Trust. Where the task(s) incorporated within this policy are delegated to non-clinical staff, the registered nurse providing the training for these staff will retain accountability and responsibility to follow the guidance within this policy (NMC 2006, 2008). All staff working in Community Services aim to ensure that children and adults requiring Enteral Feeding receive quality and safe evidenced based care by ensuring that practice complies with the latest national and local guidance.
Enteral Feeding Page 2 of 18 Version 1.2 May 2018
When should the procedure be applied?
The decision to commence artificial feeding will be taken following discussion within a multi-disciplinary team which include the consultant in charge and dietician and in conjunction with the parents/carers and individual. The decision must be clearly documented in the medical record including an individual risk assessment.
How to carry out this procedure
Inserting a Nasogastric Tube At any point during this procedure you have a variance you must stop and contact team leader and/ or community paediatrician for further advice in management
Intervention Rationale
Ensure consent is completed recorded and contained within the records
The Code: Standards of conduct, performance and ethics for nurses and midwives (2008) NMC
Read care plan and feeding regime To ensure up to date person specific instructions are in place
Collect equipment (Nasogastric tube (portex or silk as per care plan), 50ml syringe ( enteral use – purple) , pH indicator paper (marked with CE and intended to test gastric aspirate), water to flush, tape to secure, dressing to protect child’s face
Adherence to evidence based practice
Wash your hands before and after the procedure
As per Hand Hygiene Policy
Wear non-sterile non-latex gloves As per Infection Control Assurance Policy
Explain to the child/young person that you are going to pass the Nasogastric tube
To put the child at their ease
Position child as per care plan
Enteral Feeding Page 3 of 18 Version 1.2 May 2018
Intervention Rationale
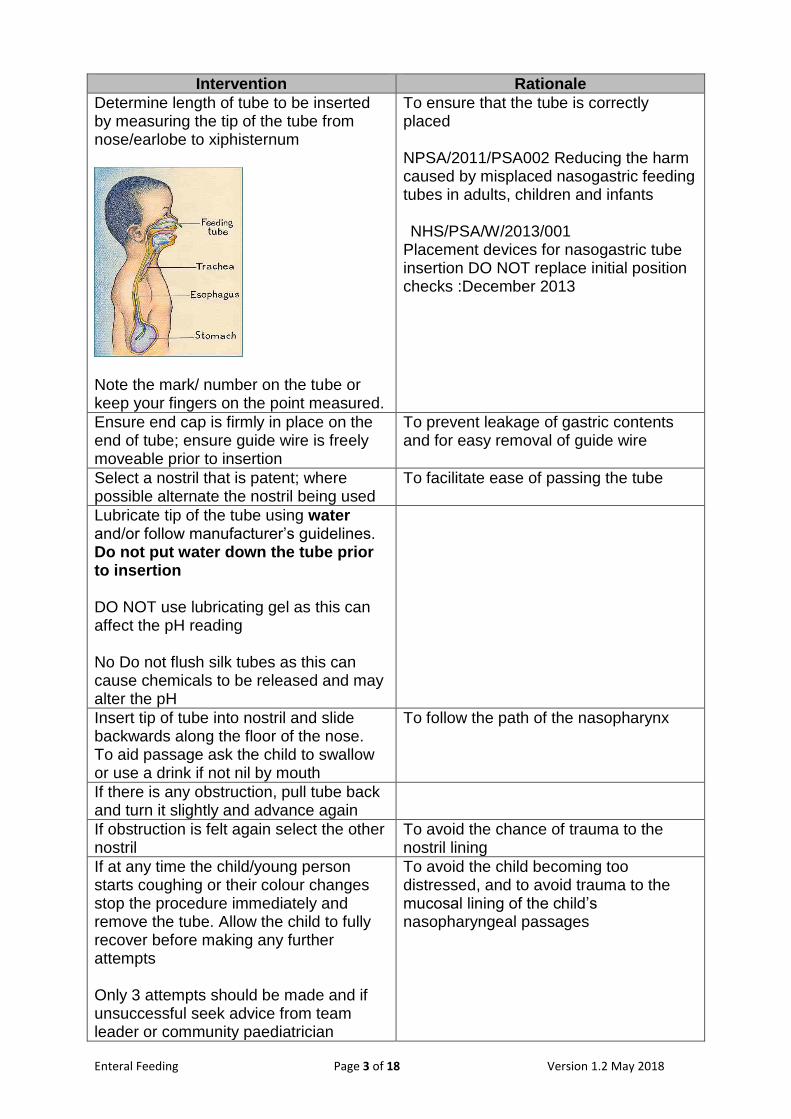
Determine length of tube to be inserted by measuring the tip of the tube from nose/earlobe to xiphisternum
Note the mark/ number on the tube or keep your fingers on the point measured.
To ensure that the tube is correctly placed NPSA/2011/PSA002 Reducing the harm caused by misplaced nasogastric feeding tubes in adults, children and infants NHS/PSA/W/2013/001
Placement devices for nasogastric tube insertion DO NOT replace initial position checks :December 2013
Ensure end cap is firmly in place on the end of tube; ensure guide wire is freely moveable prior to insertion
To prevent leakage of gastric contents and for easy removal of guide wire
Select a nostril that is patent; where possible alternate the nostril being used
To facilitate ease of passing the tube
Lubricate tip of the tube using water and/or follow manufacturer’s guidelines. Do not put water down the tube prior to insertion DO NOT use lubricating gel as this can affect the pH reading No Do not flush silk tubes as this can cause chemicals to be released and may alter the pH
Insert tip of tube into nostril and slide backwards along the floor of the nose. To aid passage ask the child to swallow or use a drink if not nil by mouth
To follow the path of the nasopharynx
If there is any obstruction, pull tube back and turn it slightly and advance again
If obstruction is felt again select the other nostril
To avoid the chance of trauma to the nostril lining
If at any time the child/young person starts coughing or their colour changes stop the procedure immediately and remove the tube. Allow the child to fully recover before making any further attempts Only 3 attempts should be made and if unsuccessful seek advice from team leader or community paediatrician
To avoid the child becoming too distressed, and to avoid trauma to the mucosal lining of the child’s nasopharyngeal passages

Enteral Feeding Page 4 of 18 Version 1.2 May 2018
Intervention Rationale
Advance the tube until you reach the point where the tube was measured
To facilitate correct positioning of the tube
Secure the tube in position using a skin barrier product such as hydrocolloid dressings to protect the skin and adhesive dressing and tape to secure.( as per care plan and BCPFT wound care formulary)
To ensure that the tube remains in the correct position, to avoid it migrating into the lung
Prior to use the position of the tube must be confirmed by aspirating up to 5mls and using the PH test ensuring the readings are between 1-5.5 DO NOT administer anything down the tube if above 5.5 unless a multidisciplinary risk assessment has been undertaken
To ensure that it is in the stomach and minimise risk of aspiration
Detach the syringe from the tube remembering to replace the end cap of the tube
Once the tube is in the correct position, if there is a guide wire remove and retain as per manufacturers’ guidance and close the port. Seek dieticians recommended instruction regarding flushing
Document the procedure (including the following) in the child’s individual record • Date and time of insertion and when it would be due to be replaced • Tube type (which should be radio opaque and have measured markings
through its length) • Nose to ear to Xiphoid measurement • Nostril used Left or Right • Aspirate obtained Y or N • The actual value of the pH result (i.e. it is not acceptable to record ‘within
range’ or similar) • Method for securing the tube and dressing used • External tube length remaining – or numbered marking on the tube at the level
of the nostril • Inserted by • Tube change due
Ongoing care: - Check skin integrity where nasal gastric tube is secured - Check nasal passages are patent - Regular personal hygiene can take the form of baths/showers, however, ensure
the feeding port is closed
Enteral Feeding Page 5 of 18 Version 1.2 May 2018
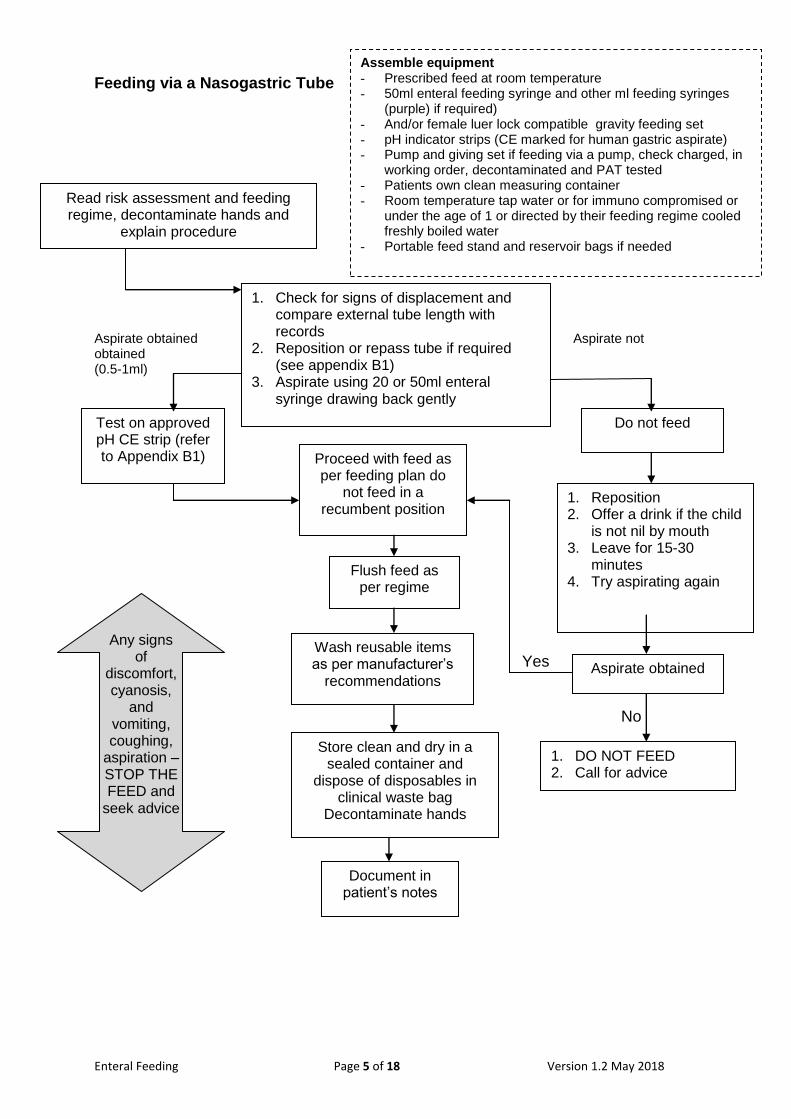
Feeding via a Nasogastric Tube Aspirate obtained Aspirate not obtained (0.5-1ml)
Yes No
1. Check for signs of displacement and compare external tube length with records
2. Reposition or repass tube if required (see appendix B1)
3. Aspirate using 20 or 50ml enteral syringe drawing back gently
Read risk assessment and feeding regime, decontaminate hands and
explain procedure
Test on approved pH CE strip (refer to Appendix B1) Proceed with feed as
per feeding plan do not feed in a
recumbent position
Flush feed as per regime
Wash reusable items as per manufacturer’s
recommendations
Store clean and dry in a sealed container and
dispose of disposables in clinical waste bag
Decontaminate hands
Document in patient’s notes
Any signs of
discomfort, cyanosis,
and vomiting, coughing,
aspiration – STOP THE FEED and
seek advice
Do not feed
1. Reposition 2. Offer a drink if the child
is not nil by mouth 3. Leave for 15-30
minutes 4. Try aspirating again
1. DO NOT FEED 2. Call for advice
Aspirate obtained
Assemble equipment - Prescribed feed at room temperature - 50ml enteral feeding syringe and other ml feeding syringes
(purple) if required) - And/or female luer lock compatible gravity feeding set - pH indicator strips (CE marked for human gastric aspirate) - Pump and giving set if feeding via a pump, check charged, in
working order, decontaminated and PAT tested - Patients own clean measuring container - Room temperature tap water or for immuno compromised or
under the age of 1 or directed by their feeding regime cooled freshly boiled water
- Portable feed stand and reservoir bags if needed
Enteral Feeding Page 6 of 18 Version 1.2 May 2018
Management and Feeding via a Gastrostomy Site and Tube 1.0 Care of a PEG Gastrostomy Tube The site at all times must be kept clean and dry Care of the tube may vary according to manufacturer’s guidelines. A PEG is not routinely removed in the community but may fall out. Should the tube fallout the child will need to be seen in hospital as soon as possible to assess if any intervention is necessary with regards to the retaining disc. In the event of it falling out follow the procedure as outlined in the management of a PEG gastrostomy Care plan. If there are any of the below signs or symptoms feeds should be stopped and medical advice sought. This is particularly relevant in the first 72 hours following initial insertion due to the small but significant risk of peritonitis caused by leakage between the stomach and peritoneum prior to the tract becoming established. There is also a rare but significant possibility of peritonitis with and established stoma if the peg becomes dislodged. Many children have gastric leakage which does not usually require urgent medical review. Immediate post –insertion care. In the first 72 hours always stop feeding and seek team leader / medical advice if there is: • Pain on feeding • Prolonged or severe pain post-procedure • Fresh bleeding • External leakage of gastric contents • Signs of infection i.e. discharge swelling, heat, redness, pain, and offensive
smell 1.1 Care for the First 10 Days Following Insertion The site at all times must be kept clean and dry Baths must be avoided within the first 10 days until the stoma tract is formed to avoid infection. Inspect the skin for signs of redness, swelling, irritation, skin breakdown and leakage and report any concerns to Consultant/Nutritional Care Team. Please refer to instruction from the Nutritional Care nurse and Consultant on length of time that pH testing is required prior to administration of feed. If the child has a PEG tube that falls out, medical attention must be sought immediately.
Enteral Feeding Page 7 of 18 Version 1.2 May 2018
1.2 Daily Care after 10 days and before 28 days
Intervention Rationale
Inform the child what is about to happen Ensure consent is obtained and documented
• Always wash and dry hands before touching the tube
• wear non-sterile non-latex gloves and apron
• Leave external fixation device in place until advised to loosen
Note the position of the external fixator device so that it can be returned to the same position on the tube after cleaning
• Clean skin around stoma site and under fixation device with sterile water using gauze and ensure the skin is dried thoroughly afterwards
The Code: Standards of conduct, performance and ethics for nurses and midwives (2008)
As per Infection Control Assurance Policy Please refer to instruction from the Nutritional Care nurse and Consultant
• Inspect the skin for signs of redness, swelling, irritation, skin breakdown and leakage and report any concerns to Consultant/Nutritional Care Team
• Dispose of equipment • Document all interventions in the
child’s record
As per Infection Control Assurance Policy
Enteral Feeding Page 8 of 18 Version 1.2 May 2018
Intervention Rationale
When cleaning extension tubes always follow the manufacturer’s guidelines Clean the site with water and dry thoroughly.
• In one movement, daily- gently advance the tube (5mm) and turn tube 360°to ascertain free movement and then gently retract tube back to original place (this depends on tube manufacturer’s guidelines).
• If rotation causes pain or tube will not turn, stop and contact and report to Team Leader/Consultant/Nutritional Care Team for further instruction
• The need for a dressing will depend on the child’s skin condition and will require individual assessment as per Trust guidelines.
• Document in the child’s record • If the child has a PEG tube that
falls out, medical attention must be sought as per care plan
1.3 Checking the Position of the Gastrostomy Tube Positioning of the Tube The position of a gastrostomy tube only needs to be checked once following a planned or emergency change. The responsibility for ensuring correct tube placement lies with the registered nurse, parent or carer caring for that child, and he/she must be satisfied that the tube is correctly placed before commencing or continuing with feeding or medicine administration via the Gastrostomy tube.
Enteral Feeding Page 9 of 18 Version 1.2 May 2018
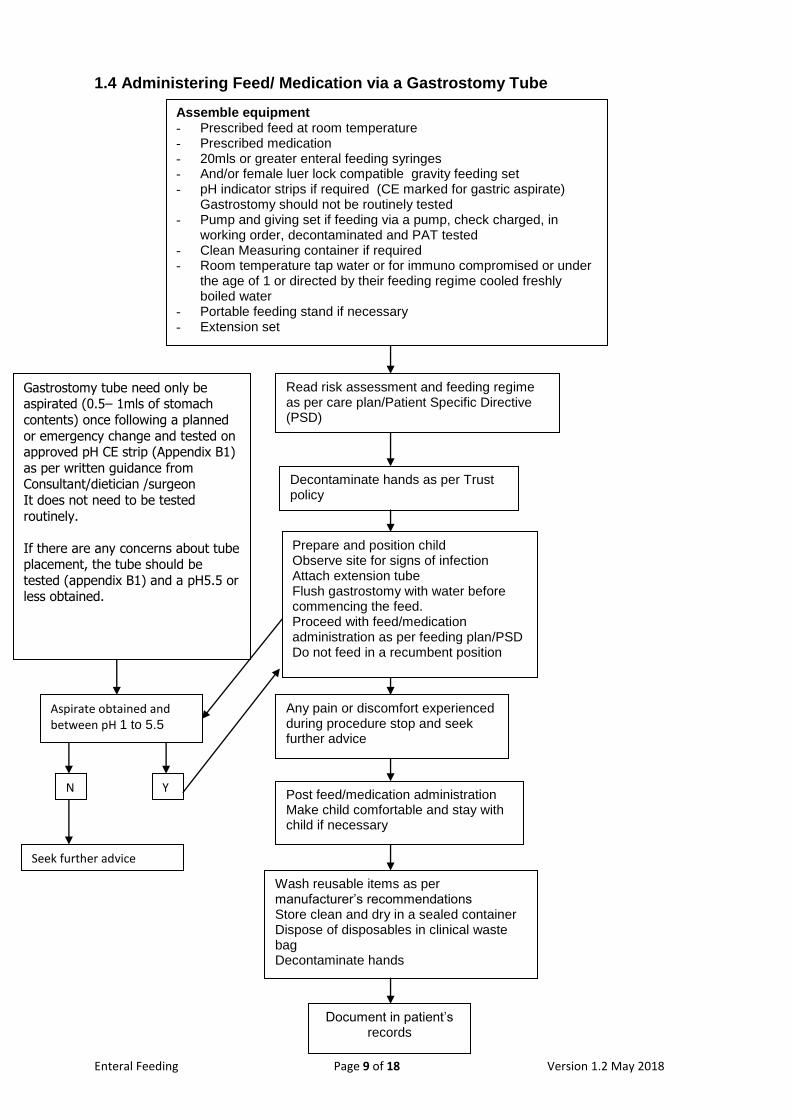
1.4 Administering Feed/ Medication via a Gastrostomy Tube
Read risk assessment and feeding regime as per care plan/Patient Specific Directive (PSD)
Decontaminate hands as per Trust policy
Assemble equipment - Prescribed feed at room temperature - Prescribed medication - 20mls or greater enteral feeding syringes - And/or female luer lock compatible gravity feeding set - pH indicator strips if required (CE marked for gastric aspirate)
Gastrostomy should not be routinely tested - Pump and giving set if feeding via a pump, check charged, in
working order, decontaminated and PAT tested - Clean Measuring container if required - Room temperature tap water or for immuno compromised or under
the age of 1 or directed by their feeding regime cooled freshly boiled water
- Portable feeding stand if necessary - Extension set
Gastrostomy tube need only be aspirated (0.5– 1mls of stomach
contents) once following a planned
or emergency change and tested on approved pH CE strip (Appendix B1)
as per written guidance from Consultant/dietician /surgeon
It does not need to be tested
routinely.
If there are any concerns about tube placement, the tube should be
tested (appendix B1) and a pH5.5 or less obtained.
Aspirate obtained and between pH 1 to 5.5
Prepare and position child Observe site for signs of infection Attach extension tube Flush gastrostomy with water before commencing the feed. Proceed with feed/medication administration as per feeding plan/PSD Do not feed in a recumbent position Flush post feed as per regime
Y N
Seek further advice
Wash reusable items as per manufacturer’s recommendations Store clean and dry in a sealed container Dispose of disposables in clinical waste bag Decontaminate hands
Document in patient’s records
Post feed/medication administration Make child comfortable and stay with child if necessary
Any pain or discomfort experienced during procedure stop and seek further advice
Enteral Feeding Page 10 of 18 Version 1.2 May 2018
1.5 Care of Balloon Gastrostomy As per 1.2 and additional care Do not insert syringes directly into the main port of a button device. Priming should be carried out before, interim and post administering feeds or medicines. Wash reusable items as per manufacturer’s recommendations and in care plan. 2.0 Checking Balloon Inflation This is undertaken on a weekly basis to ensure it is secure and remains in situ
Check the recommended volume of the balloon as per care plan
Decontaminate hands
Wear non-sterile non-latex gloves and apron
Ensure equipment includes sterile water, luer slip syringe x 2 (not an enteral syringe) including a replacement tube
Position child as per care plan
Attach luer slip syringe onto the balloon valve of the gastrostomy. It is advisable to hold on to the tube, ensuring it remains in the child’s stomach
Gently draw back the plunger on the syringe until no more water comes out of the internal balloon
Check volume of water
Discard syringe in clinical waste
Using the sterile water and other luer syringe, insert recommended volume via the valve to re-inflate balloon
Dispose of equipment
Document in the child’s record including volumes of water removed and replaced
If the volume removed is 0.5 mls or more less than the volume inserted, seek advice from the health care professional as the device may need changing
3.0 Replacing a balloon Gastrostomy tube Only registered nursing staff or health care professionals deemed competent and delegated by the registered nurse or parents who have received appropriate training are able to replace balloon Gastrostomy tubes.
Intervention Rationale
If the Gastrostomy tube falls out then it must be replaced within the hour by a person trained to carry out this procedure Parents/carers must be aware of what to do, who to contact or where to go if tube falls out The procedure for changing the Gastrostomy tube will depend on each individual care plan but is usually undertaken every 3– 6 months as per manufacturer’s guidelines A replacement tube must be kept with the
Enteral Feeding Page 11 of 18 Version 1.2 May 2018
child at all times Replacing a balloon device
• Equipment required - replacement tube, sterile water, gloves and plastic apron, 2 x luer slip syringes, pH CE strips and 50ml enteral feeding tube and gauze
• Wash and dry hands before touching the tube
• Put on non-sterile non-latex gloves and apron
• Prepare the equipment. • Inflate the replacement device
balloon to confirm patency. Deflate and remove all air
• Using an empty syringe remove all the water from the balloon in situ and note amount removed
• Position thumb and forefinger 5cms apart either side of the tube to stabilise the exit site, gently remove the tube
• Clean site with sterile water check for signs of infection
• Gauze may be used to apply gentle pressure around the Gastrostomy site to absorb gastric content during procedure.
• Lubricate the tip of the replacement device with water or manufacturer supplied lubricant
• gently retract the tube from the stomach
• Using a new syringe inflate the balloon with sterile water as per care plan
• Gently pull back the device to ensure the balloon is inflated and is internally retaining the device
• Clean and dry the stoma site • Aspirate fluid from the feeding port
and test it on pH paper (ref: policy no. 20) If the pH value is 1-5.5 the tube is in the correct position .If the pH is more than 5.5 tape the tube down and contact the managing healthcare professional – do not use the tube as may not be in the correct position. Record in child’s health records
• Dispose of equipment
Enteral Feeding Page 12 of 18 Version 1.2 May 2018
• Document details in the child’s record including device make and size removed and replaced, volume of water removed and replaced. ( retain manufacturers instruction sticker and place in notes) and next change due date
4.0 Unblocking a Gastrostomy Tube in Situ To unblock a Gastrostomy tube the following can be attempted and may need to be repeated if the blockage is not fully dispersed. Unblocking a Gastrostomy tube may take several attempts to achieve. Do not use force as the tube may burst. Ensure the patient is relaxed
Use a clean 50ml syringe gently flush the tube using warm water (at least 10mls) using a gentle push/pull technique
Gently squeeze the tube between fingers and along its length (i.e. milking the tube)
If the blockage persists, very gently draw back on the syringe and then attempt to flush as before. After three attempts and blockage persists escalate to Team Leader
This should be considered ‘urgent’ if the only route for medication is through the gastrostomy
Document your actions and the outcome in the child’s record 5.0 Management of Over Granulation at Gastrostomy Site There are multiple causes for over granulation around the gastrostomy site. On detection of over granulation escalate to Team Leader to enable a thorough assessment and management plan. 6.0 Other Care
The child’s dietician and the medical team must be contacted for further assessment and management where staff and/or parents report problems of vomiting, diarrhoea, constipation, abdominal distension, cramps, nausea or dehydration, weight loss or rapid weight gain
Regularly inspect the skin for signs of redness, swelling, offensive odour, irritation, skin breakdown and leakage obtain a swab and report to Team Leader/Consultant/Nutritional Care Team
In the event of recurrent burst balloons or leaking valve ports, a swab of surrounding skin area must be obtained or gastric aspirate taken and must be sent to check for the presence of yeasts. If yeasts are present this should be treated. A microbiology form should be completed and the specimen transported according to the standard operating procedure for transportation of specimens by a healthcare worker
Ensure oral hygiene is maintained at all times as per care plan
It is essential to always promote oral feeding when assessed as safe to do so by a multi-disciplinary team and is clearly documented and regularly reviewed
All efforts must be made to keep the patient at home and avoidable admission to hospital

Enteral Feeding Page 13 of 18 Version 1.2 May 2018
Report any problems with Medical Devices to Nutricia, report onto Datix, Dieticians and follow Medical Devices Policy
Management of Jejunostomy Tube Procedure: Care and Management of a Jejunostomy Tube Background and relevant information Care and management of Jejunostomy tubes may be undertaken by a registered practitioner or a non-registered practitioner who has been delegated the task and have achieved the required competencies in all aspects of the care. Nasojejunal and Nasoduodenal tubes In the event of a patient having nasojejunal or nasoduodental tubes an individual standard operational procedure will be developed. Specific training and competencies checks will be delivered per patient. PEG-J In the event of a patient having Peg-J an individual standard operational procedure will be developed. Specific training and competencies checks will be delivered per patient.
Additional Information/ Associated Documents
The Royal Marsden Hospital Manual of Clinical Nursing Procedures (2004) Chapter 24. Nutritional Support. Pages 420-440
Definitions and Glossary of Terms
Aspiration Taking a sample of gastric contents for pH testing
Balloon A water filled balloon holds some gastrostomy tubes securely in the stomach
Body mass index (BMI) Weight (in kilograms) divided by height (in metres). Used as a measure of nutritional status in conjunction with a BMI centile chart for children
Bolus feeding A measured amount of feed that is given slowly by syringe (gravity) over 15/20 minutes or via a feeding pump over a set time period
Centile chart Used to assess an infant/child’s physical development. The lines of growth on the chart are called centiles. The number of the centile (from one to a hundred) predicts the percentage of infants/children who are below that measurement for a particular age e.g. if a baby falls within the 10th centile, it means 10% of all babies will be smaller and 90% will be bigger. A baby would be expected to follow the centile if displaying a ‘normal’ growth trend
Clinical waste Used medical equipment for disposal
Continuous feeding A volume of feed delivered by a feeding pump at a constant rate over a period of time
Decanting Pouring feed from the original container into the giving set container
Dysmotility When muscles in the gastrointestinal tract (oesophagus, stomach, small and large intestines) are not working
Enteral Feeding Page 14 of 18 Version 1.2 May 2018
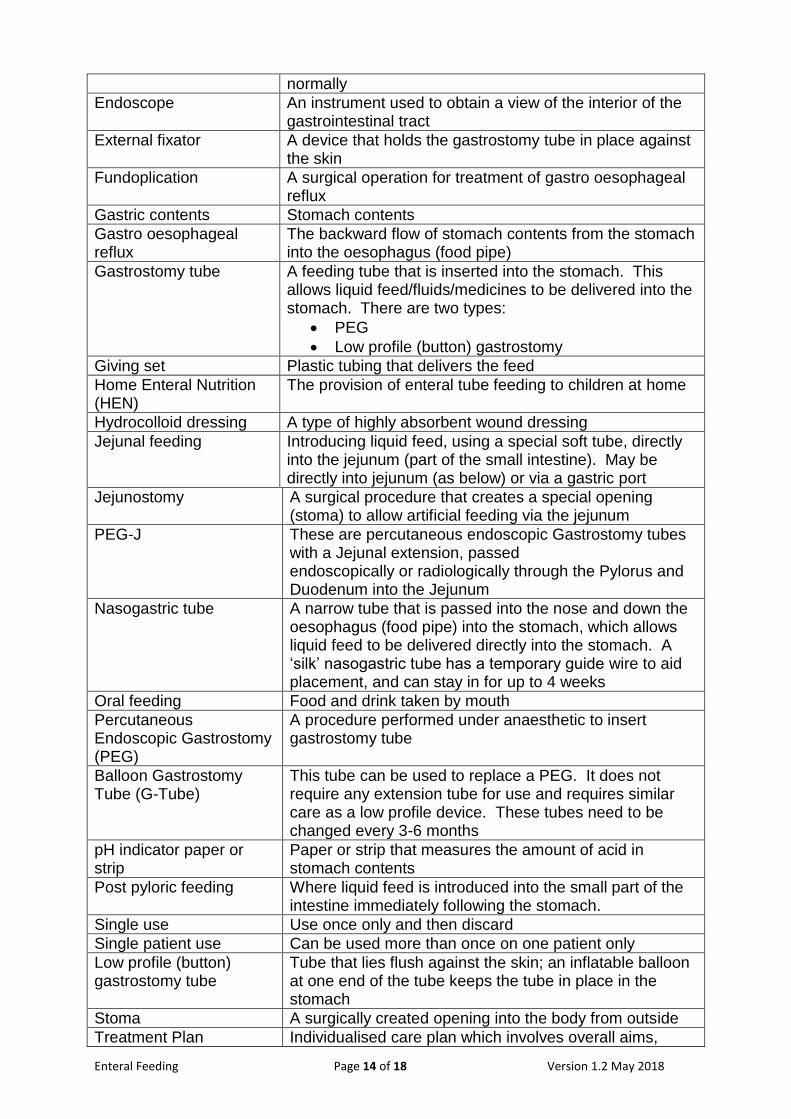
normally
Endoscope An instrument used to obtain a view of the interior of the gastrointestinal tract
External fixator A device that holds the gastrostomy tube in place against the skin
Fundoplication A surgical operation for treatment of gastro oesophageal reflux
Gastric contents Stomach contents
Gastro oesophageal reflux
The backward flow of stomach contents from the stomach into the oesophagus (food pipe)
Gastrostomy tube A feeding tube that is inserted into the stomach. This allows liquid feed/fluids/medicines to be delivered into the stomach. There are two types:
PEG
Low profile (button) gastrostomy
Giving set Plastic tubing that delivers the feed
Home Enteral Nutrition (HEN)
The provision of enteral tube feeding to children at home
Hydrocolloid dressing A type of highly absorbent wound dressing
Jejunal feeding Introducing liquid feed, using a special soft tube, directly into the jejunum (part of the small intestine). May be directly into jejunum (as below) or via a gastric port
Jejunostomy A surgical procedure that creates a special opening (stoma) to allow artificial feeding via the jejunum
PEG-J These are percutaneous endoscopic Gastrostomy tubes with a Jejunal extension, passed endoscopically or radiologically through the Pylorus and Duodenum into the Jejunum
Nasogastric tube A narrow tube that is passed into the nose and down the oesophagus (food pipe) into the stomach, which allows liquid feed to be delivered directly into the stomach. A ‘silk’ nasogastric tube has a temporary guide wire to aid placement, and can stay in for up to 4 weeks
Oral feeding Food and drink taken by mouth
Percutaneous Endoscopic Gastrostomy (PEG)
A procedure performed under anaesthetic to insert gastrostomy tube
Balloon Gastrostomy Tube (G-Tube)
This tube can be used to replace a PEG. It does not require any extension tube for use and requires similar care as a low profile device. These tubes need to be changed every 3-6 months
pH indicator paper or strip
Paper or strip that measures the amount of acid in stomach contents
Post pyloric feeding Where liquid feed is introduced into the small part of the intestine immediately following the stomach.
Single use Use once only and then discard
Single patient use Can be used more than once on one patient only
Low profile (button) gastrostomy tube
Tube that lies flush against the skin; an inflatable balloon at one end of the tube keeps the tube in place in the stomach
Stoma A surgically created opening into the body from outside
Treatment Plan Individualised care plan which involves overall aims,
Enteral Feeding Page 15 of 18 Version 1.2 May 2018
monitoring and review plan
Professional lead Consultant in charge, Key worker, Lead Nurse
Priming Removing air from a tube with water
Single use syringes
Granulation A product of the skin healing process
Over granulation Is defined as an excess of granulation tissue which is in excess
7.1 Enteral Feeding The decision to commence artificial feeding will be taken following discussion within a multi-disciplinary team which include the consultant in charge and dietician and in conjunction with the parents/carers and individual. The decision must be clearly documented in the medical record including an individual risk assessment. 7.2 Cautions
• There is an increased risk of nasogastric tube misplacement or migration in children who have a reduced level of consciousness, confusion, and cognitive impairment with agitation, impaired swallow or experience bouts of retching or vomiting
• With nasogastric tubes there is an increased risk of aspiration due to gastric reflux in children with a history of gastro-oesophageal reflux, reduced level of consciousness, impaired swallow, or who have mobility problems and remain supine during feeding
• Nasogastric tube insertion can be difficult for individuals with altered anatomy or severe physical difficulties. In these situations the individualised care plan must be contain guidance from the professional lead
• Children taking antacids, H2 antagonists or proton pump inhibitors are likely to have a stomach pH greater than 6 in which case it may be difficult to confirm tube placement with the necessary accuracy. The need to continue this medicine should be reviewed by the prescriber against the need to feed via Nasogastric tube. Additionally individual risk assessments on a case by case basis may be required. Patient specific standard operating procedure may have to be developed
• In the rare occasions continuous pump feeding via a Nasogastric tube is required, a risk assessment must be undertaken owing to the high risk of tube misplacement and resultant aspiration. Overnight continuous pump feeding will not be supported in the community unless the individual is monitored on a one to one basis
7.3 Administration of Medication via an Enteral Tube In all cases the prescriber must provide directions regarding the preparation and administration of all medicines via enteral tubes, including instructions for crushing tablets or altering medicines. Guidance should be obtained from pharmacy, prior to administration to minimise drug errors. The administration of drugs via enteral feed tubes will by its nature be unlicensed if the medication is in any way altered, such as a tablet being crushed. For this reason
Enteral Feeding Page 16 of 18 Version 1.2 May 2018
the prescriber must seek guidance from the adult/child Pharmacists who will give guidance about best practice in administering medicines by this route. The formulation of the medication will be considered, as a liquid formulation is often preferable. This may be either as syrup or as dissolved dispersible tablets. However, if tablets/capsules are an appropriate formulation, the prescriber must indicate the method of preparation required for the administration of the drug. A Pharmacist must be consulted to discuss compatibility of medications prescribed for administration via enteral routes. 7.4 Infection Control and Hygiene Regardless of the route of administration there are risks of bacterial contamination. Healthcare workers must be aware of these risks (NICE, 2012) and it is important to prevent contamination and infection by adhering to standard (universal) infection control precautions. As per Infection Control Assurance Policy. 7.5 Preparation and Storage of Feed Feeds must be stored according to manufacturers’ instruction and standard food hygiene regulations. These include checking use by date on feed, and recording the date opened. Sterile feeds to be disposed of after 24 hours of opening and made up feeds disposed of after 4 hours. Wherever possible, use pre-packed ready to use feeds. Only use decanting if directed through the feeding regime contained within the plan of care directed by the consultant and dietician. Associated Documents • Waste Management Policy • Management of Medical Devices Policy • Infection Control Assurance Policy • Birmingham Children’s Hospital (2009) Gastrostomy Site Care • Birmingham Children’s Hospital (2013) Insertion of a Gastrostomy (Button) Skin
Level Devise • Birmingham Children’s Hospital (2013) Insertion of a Gastrostomy Tube • Birmingham Children’s Hospital (2013) Insertion of a nasogastric feeding tube in
infants and children
Where do I go for further advice or information?
• Team Leader, Dietician, Nutricia (homeward)
Training and Competencies
All staff working with enteral feeds must be trained and competent in the preparation and delivery of enteral feeding systems. Competencies must be updated and recorded in the personal file annually
All parents/carers and individuals must be trained and deemed competent in administering enteral feeds in the community or prior to discharge from hospital to enable shared care
Training must be given by a registered Nurse who has up to date knowledge and skills to ensure safe evidenced based practice
Enteral Feeding pump training will be provided by Nutricia. On the rare occasion of an alternative pump being used the dischargingprovider/ manufacturer must ensure health professionals, parent/carers and individuals

Enteral Feeding Page 17 of 18 Version 1.2 May 2018
are trained. Nutricia is accountable for pat testing and maintenance of equipment
Refer to the Trust’s Mandatory and Risk Management Training Needs Analysis for further details on training requirements, target audiences and update frequencies. Monitoring / Review of this Procedure In the event of planned change in the process(es) described within this document or an incident involving the described process(es) within the review cycle, this SOP will be reviewed and revised as necessary to maintain its accuracy and effectiveness. Equality Impact Assessment Please refer to overarching policy Data Protection Act and Freedom of Information Act Please refer to overarching policy
Enteral Feeding Page 18 of 18 Version 1.2 May 2018
Standard Operating Procedure Details
Review and Amendment History
Version Date Description of Change
1.2 Feb 2018 Minor amendments made to flowchart (1.4); In line with nutritional care, advice from the dieticians and advice from the Community Children’s Nurses network forum.
1.1 Dec 2016 Minor amendments made to flowchart (1.4)
1.0 Mar 2015 New SOP for BCPFT
Unique Identifier for this SOP is BCPFT-CYPF-SOP-OP-3
State if SOP is New or Revised Revised
Policy Category Children’s Services
Executive Director whose portfolio this SOP comes under
Director of Nursing, AHPs and Governance
Policy Lead/Author Job titles only
Team Leader, Community Paediatric Specialist Team
Committee/Group Responsible for Approval of this SOP
CYPF Quality and Safety Steering Group
Month/year consultation process completed
N/A
Month/year SOP was approved February 2018
Next review due February 2020
Disclosure Status ‘B’ can be disclosed to patients and the public
Key Words for this SOP enteral, feeding, nutrition, children, community, see-saw team, palliative, paediatric,
Consultant Paediatrician Signature
Dietician Signature