perspectives on demand side financing, social safety nets and the mdgs dr. adnan a. khan director...
TRANSCRIPT

Perspectives on Demand Side Financing, Social Safety Nets and the MDGs
Dr. Adnan A. KhanDirector
Research and Development Solutions, Islamabad
LEAD Workshop on Demand Side Financing, Social Safety Nets and MDGs
15th February 2013

Key Consideration
Health
Access to HealthcareHealthcare
? ?
?

The Issue
Enabling the poor to actually
pay for and consume a
good or serviceEffective Demand
Supply
Purchasing Power
Demand for Health care

RAND Experiment
• Large Scale, Multi Year experiment, in the 1970s, in the US
• Participants who paid for their healthcare, used around 30% fewer healthcare services
• Cost sharing and decreased use was similar for highly effective and less effective services
• Free care led to better care of hypertension, vision and dental health, particularly for the poorest and sickest patients
• Overall health/ longevity was unchanged

Composition of Outpatient Visits in Pakistan
Acute Care; 91%
Preventive; 2%
Chronic
Care; 6%
Source: Multiple Studies

Financing of Health in Pakistan
Private OOP; 60%
Lo-cal NGOs; 6%
Donor; 3%
Public Sector; 26%
Health In-
surance; 6%
Source: National Health Accounts 2007-8Public Sector
0%
20%
40%
60%
80%
100%
15%
11%
56%
19%
Preventive 5%
Inpatients 15%
Outpatients 3%
Overheads 4%

Private Funding and Preventive Health
• 90%+ goes to curative healthcare• 50-60% of family planning is self paid• 35%+ birthing services are self paid• 3% of childhood immunization are in the
private sector

Options for Health Financing: Out of Pocket Payments
Advantages Issues
Low CostMay ignore important but unrealized needs such as preventive services
Client Need BasedCan be expensive, particularly for hospitalizations and chronic illnesses
Specific in Location and Need
Increased unnecessary services such as unneeded Caesarean sections and Injections
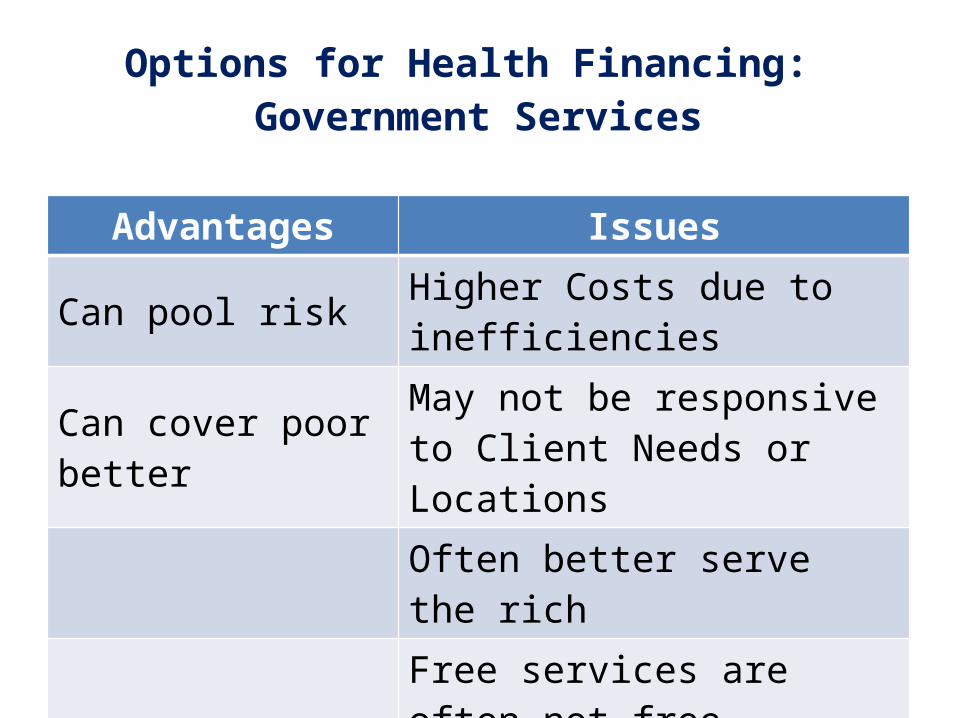
Options for Health Financing: Government Services
Advantages Issues
Can pool risk Higher Costs due to inefficiencies
Can cover poor better May not be responsive to Client Needs or LocationsOften better serve the richFree services are often not freeEthics of regressive taxes paying for inefficient services

Options for Health Financing: Insurances
Advantages IssuesPool risk Selection and Moral HazardCan cover poor better Often better serve the rich
What do you coverHow do you get people to go for essential but unwanted services
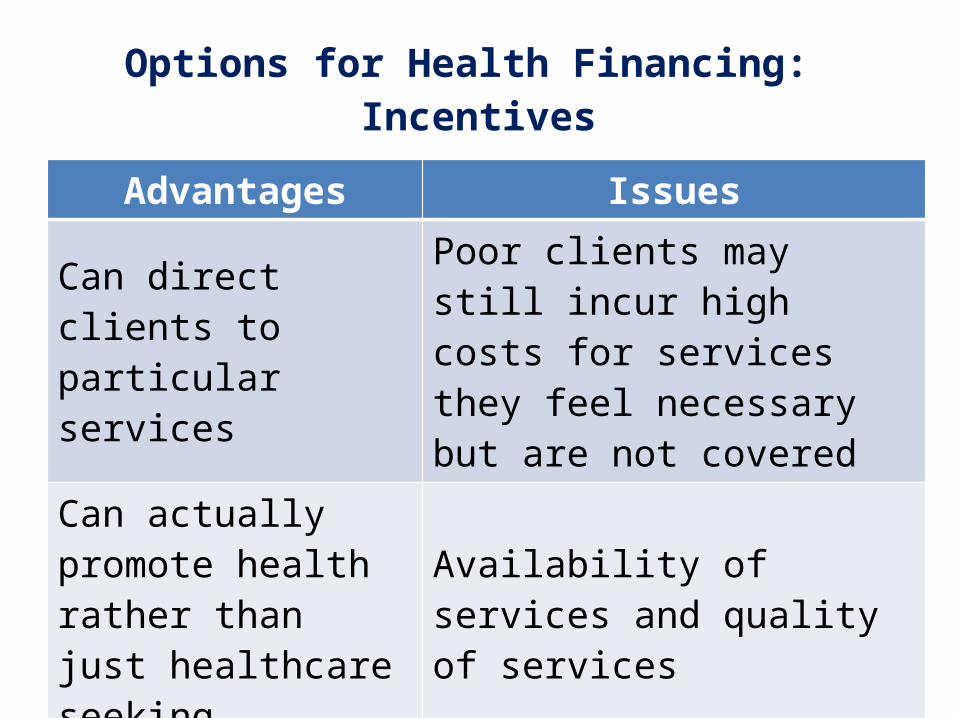
Options for Health Financing: Incentives
Advantages Issues
Can direct clients to particular services
Poor clients may still incur high costs for services they feel necessary but are not covered
Can actually promote health rather than just healthcare seeking
Availability of services and quality of services
TransparencyIncrease market competition among providers
Advantages to health are indirect
Community Insurance and Reproductive Health
• Some evidence for increase skilled birth attendance (China Cooperative Medical System)
• Maternal Health, Infant and Child Mortality (Cost Rica), although more in depth analysis shows benefits entirely due to maternal schooling, economic status and location/ proximity to clinics

Issues in Improving Health via Healthcare and Access Approaches
• Information asymmetry• Client costs are from provider (fees and
supplies), transport, opportunity – what do you cover
• Not all care sought leads to health

Vouchers: Bangladesh
• Vouchers for maternal health services in multiple underserved districts
• Increased client satisfaction• Increased ANC, facility deliveries, PNC but not FP• Increased facility use by the poor• Decreased differences between poor and rich• Rich still used government facilities more than the poor• Successes less than anticipated• Limited success related to poor service quality and
choice

Vouchers: Bangladesh
• Location: Dijanpour• Vouchers for birthing services• Increased client satisfaction• Increased facility deliveries and EMOC use• Increased birthing information

Vouchers: Cambodia
• Vouchers for in 3 rural districts• Increased facility deliveries 3 fold• Increase occurred in voucher and self pay
clients (slightly more for vouchers)• More improvements seen among the poor

Summing it up
• Demand side financing changes health behaviors +/- provides health financing
• May help the poor• May promote health and progress towards MDGs• Limited application unless services are available• Experience thus far mainly with covering
services/ commodities – not for transport, opportunity costs
• Sustainability• How long does it take to change behaviors?

Challenges
• Dependency of recipients and misuse• Targeting the poor• Administrative costs/Quality control• Systematic corruption• Lack of suppliers• Sustainability of demand side financing
schemes

Options for Sustained DSF and SSN
Social Enterprise Models
• Provide subsidized health care based on a revenue generating framework
• Trained Community Health Entrepreneur (TCHE) in India provides basic healthcare services in rural areas.
• The Health Entrepreneur is expected to generate their own sales through providing health care services at the doorsteps.
• Small scale pilots exist such as Packard Foundation’s “Marvi” project in Umerkot with the help of HANDS

Social Enterprise ModelsAdvantages Issues
Requires less investmentNeed to train people for leadership and entrepreneurial skills
Build self reliance in communities
Create and implement strict price controls
Workers have incentive to provide service
Requires some procurement support for medicines and equipment
Workers make effort at convincing people to access health care
Will be dependent on the ability and motivation of the worker

Social Franchising
• Green Star Social Marketing and Marie Stopes International and others have worked through their franchise centers
• Marie Stopes Society (MSS) - a subsidiary of the Marie Stopes International works through its Suraj Franchise Model in Pakistan to provide IUCD vouchers that can be utilized at Suraj franchises

Social FranchisingAdvantages Issues
Increase access for poor and underserved
Requires strong monitoring mechanisms
Good quality services Selection and Moral HazardCan be run by local health care providers Avoid costs of fixed facilities

Key Questions
• How can we reach the poor and underserved?• How can we identify the deserving?• Is there a possibility for public –private
partnerships to serve the poor and improve efficiency?
• Can the public sector fund/subsidize private sector for better service choice and quality?
• How should we use indigenous knowledge?• Can economic development support DSF
measures?
Key Questions
• What are the roles of key macroeconomic variables in supporting and promoting SSN– Education– Employments– Price Stability– Infrastructure
• Does food security affect SSN?• What can be done to improve SSN Conflict and
Security concerns?• Are vouchers the only solution we have?

Thank You