palinopsia revamped 10-7-2014
DESCRIPTION
healthTRANSCRIPT

Accepted Manuscript
Palinopsia Revamped: A Systematic Review of the Literature
David Gersztenkorn, MD, MS Andrew G. Lee, MD
PII: S0039-6257(14)00128-3
DOI: 10.1016/j.survophthal.2014.06.003
Reference: SOP 6524
To appear in: Survey of Ophthalmology
Received Date: 4 April 2014
Revised Date: 23 June 2014
Accepted Date: 24 June 2014
Please cite this article as: Gersztenkorn D, Lee AG, Palinopsia Revamped: A Systematic Review of theLiterature, Survey of Ophthalmology (2014), doi: 10.1016/j.survophthal.2014.06.003.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT1
Palinopsia Revamped: A Systematic Review of the Literature
David Gersztenkorn, MD, MSa, Andrew G. Lee, MD
b
aCenter for Biomedical Engineering, The University of Texas Medical Branch, Galveston, TX, USA
bDepartment of Ophthalmology, Houston Methodist Hospital, Houston, TX, USA, Department of
Neurology, Houston Methodist Hospital, Houston, TX, USA, Departments of Ophthalmology, Neurology,
and Neurosurgery, Weill Cornell Medical College, Department of Ophthalmology, The University of Texas
Medical Branch, Galveston, TX, USA, Houston, TX, USA, Baylor College of Medicine, Houston, TX, USA,
Department of Ophthalmology, The University of Iowa Hospitals and Clinics, Iowa City, Iowa, USA, The
University of Texas MD Anderson Cancer Center, Houston, TX, USA
Corresponding author: Andrew G. Lee, Department of Ophthalmology, Houston Methodist Hospital,
6560 Fannin St. Suite 450, Houston, TX, 77030
Email address: [email protected]

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT2
Abstract
Palinopsia, the persistence or recurrence of visual images after the stimulus has been removed, is a non-
specific term that describes multiple types of visual symptoms with a wide variety of etiologies. For
example, palinopsia may be the presenting symptom of a potentially life-threatening posterior cortical
lesion, yet it may also be a benign medication side effect. We comprehensively review all published
cases and subdivide palinopsia into two clinically significant categories: illusory palinopsia and
hallucinatory palinopsia.
Key Words: Palinopsia; Visual Perseveration; Cerebral Polyopia; Akinetopsia; Hallucinogen Persisting
Perception Disorder; Persistent Migrainous Aura; Persistent Visual Aura; Positive Spontaneous Visual
Phenomena; Visual Snow; Saccadic Suppression
Abbreviations:
HPPD: Hallucinogen persisting perception disorder
CSD: Cortical spreading depression
AVM: Arteriovenous malformation
PCA: Alzheimer variant posterior cortical atrophy
LGN: Lateral geniculate nucleus
MT/MST: Medial temporal/medial superior temporal area
LSD: Lysergic acid diethylamide

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT3
1. Introduction
Palinopsia (Greek: palin for "again" and opsia for "seeing"), defined by Bender et al as “the
persistence or recurrence of visual images after the stimulus has been removed”17
, encompasses many
different visual symptoms. The heterogeneous group of symptoms cannot be accurately classified as
either visual illusions or visual hallucinations, leading to ambiguity in the nosology of palinopsia and of
related terms such as akinetopsia, illusory visual spread, and cerebral polyopia. Palinopsia is
synonymous with visual perseveration137
.
Kolmel first subdivided palinopsia in 1982 based on the latency between the observation of the
true image and the appearance of the palinoptic image81
. Palinopsia may be described as “immediate”
for a latency up to a few seconds or “delayed” for a latency greater than a few seconds. While this
temporal relationship is important, there is now ample evidence to show that it should not be the
primary factor for categorization.
After thoroughly reviewing the 127 cases of palinopsia in the literature (Appendix), we discuss
its symptomology, etiology, pathophysiology, diagnostic evaluation, prognosis, and treatment. We split
palinopic symptoms into two clinically relevant categories. Hallucinatory palinopsia describes
afterimages that are not usually affected by environmental conditions of light or motion and are long-
lasting, isochromatic, and high resolution. This category of palinopsia represents a dysfunction in visual
memory and is caused by posterior cortical lesions or seizures. Illusory palinopsia describes afterimages
that are unformed, indistinct, or low resolution and are affected by ambient light and motion. This
category of palinopsia represents a dysfunction in visual perception and is a result of migraines,
prescription drugs, illicit drugs, or head trauma.
2. Symptomology
2.1. Physiological afterimages
Palinopsia should be distinguished from physiological afterimages, a common and benign
phenomenon. Physiological afterimages regularly appear after viewing a bright stimulus and shifting
visual focus. These afterimages occur in the same location in the visual field as the original stimulus and
lack clarity. The generation of physiological afterimages relies on the intensity and contrast of the
original stimulus, the time of fixation, and the retinal adaptation state11,17,137
. Physiological afterimages
are almost always the complementary color (negative afterimage) to the original stimulus, but can very
briefly be the same color (positive afterimage) when viewing an exceptionally bright stimulus. A stimulus
consistently produces the same afterimage, which varies in size based on the distance between the
person and the background17
. Physiological afterimages can be seen with either eye open, with both
eyes open, or with both eyes shut, and are often revived by blinking. Physiological afterimages are
thought to derive mainly from photobleaching of the retina24,147
, although newer evidence indicates
contribution from cerebral processes131
.
2.2. Palinopsia subtypes
We describe eight categories of symptoms which are all defined as palinopsia. Notably,
palinoptic images are almost always isochromatic (positive afterimage) to the original stimulus.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT4
2.2.1. Formed image perseveration
Patients may report a single, stationary object remaining fixed in their visual field. The
perseverated images are realistic, with the same color, resolution, and clarity as the original stimulus.
Some patients even try to reach out and touch the afterimage. The palinopsia usually lasts at least 15
seconds, but can persist for several hours or days. For example, a patient sees a picture of a wasp, and
then an identical copy of the wasp is superimposed on the patient’s field of view for a few hours82
. A
typical complaint is retaining the examiner’s fingers in the field of view (Figure 1a). These afterimages
may occur at the original location of the stimulus or appear elsewhere in the visual field, often in a visual
field deficit. The perseverated images are not affected by the length of fixation or external conditions
such as stimulus intensity, contrast, or color. The palinoptic image may appear immediately after
viewing the original image or be temporally delayed. If delayed, the image will usually appear within a
few minutes. On occasion, the perseverated image is part of an object or multiple objects that are close
together.
2.2.2. Scene perseveration
Patients may describe seeing a previously-viewed, short, and stereotyped action which
continuously replays for several minutes. For example, a patient might view a person running his hand
through his hair, and minutes later, sees the same action-sequence repeated many times35
.The
palinoptic scene usually appears within minutes after the original scene, with the same color and clarity.
Scene perseveration may occur in a visual field deficit or be superimposed on an intact visual field. Our
understanding of visual memory considers a short scene as a unit of memory, similar to an image21, thus
scene perseveration is probably mechanistically related to formed image perseveration.
2.2.3. Categorical incorporation
Palinopsia also refers to a patient seeing an object or feature and then superimposing it onto
comparable objects or people. For example, a patient sees a man with a beard and incorporates the
same beard on every subsequent person viewed104
. Or a person sees the spire of a building and
perceives the spire on the top of other structures154
(Figure 1b). The episodes of categorical
incorporation usually last a few minutes. The perseverated images have the same characteristics as the
original stimulus and are not affected by fixation, light, contrast, or motion. Categorical incorporation
highlights the brain’s use of constructs to process the external world.
2.2.4. Illusory visual spread/patterned visual spread
Illusory visual spread or patterned visual spread is a rare type of palinopsia that describes the
spread of a pattern to other objects in a single field of view. For example, a patient sees a checkered
pattern on a lamp, which then spreads to other objects, such as the floor or a desk. The visual spread is
not influenced by contextual clues, differentiating it from categorical incorporation. Illusory visual
spread was renamed to patterned visual spread for clarity.
2.2.5. Prolonged indistinct afterimage

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT5
After viewing a bright stimulus or a light and then looking away, some patients report seeing a
prolonged afterimage in the same location in the visual field as the original stimulus. The indistinct or
unformed perseverated image or light is typically isochromatic to the original stimulus, but can fade to
different colors over time. For example, after viewing a light-post, a bright outline of the post stays in
one’s visual field for several minutes122
. Stimulus intensity, background contrast, and fixation length
affects the generation and severity of these perseverated images. Photophobia frequently co-exists,
which can hamper a patient’s ability to perform outdoor activities. Afterimages from lights tend to have
a longer duration than the indistinct afterimages from other bright objects. Patients often complain of
trouble with camera flashes, which may stay in their visual field for ten minutes or longer140
. Palinoptic
prolonged light afterimages of the complementary color are differentiated from physiological
afterimages based on afterimage intensity and duration.
2.2.6. Light streaking
Light streaking occurs when relative motion between a person and a light source causes streaks
to appear behind the light, usually persisting for several seconds before fading. This type of palinopsia
commonly occurs with a bright light on a dark background. Difficulty with night driving is a common
complaint, as vision is obscured by multiple streaks from the headlights of oncoming cars1. The streaking
can appear anywhere in the visual field, depending on the location of the light movement.
2.2.7. Visual trailing
Some patients report that an object in motion leaves copies in its wake, colloquially called visual
trailing or ghosting (Figure 1c). The perseverated images left behind the moving object may be discrete
and discontinuous such as in a film reel or in a multiple-exposure photograph, or the afterimages may
be blurred together such as in a long-exposure photograph. Delayed image elimination after motion has
been described as “seeing Neo dodge bullets in the movie, The Matrix”132
. The perseverated images last
a few seconds and are identical in shape and color to the original stimulus, but they are often less
intense. Visual trailing is sometimes more noticeable in the temporal fields. Some patients report that
the afterimages catch-up and integrate with the original stimulus after motion ceases. Most cases
describe visual trails during movement of an object; however there are also reports from the movement
of the observers’ head or eyes66,117
.
2.2.8. Variant image perseveration
There are a few people who report palinopsia with many of the features of formed image
perseveration (Section 2.2.1.), but with some important differences. One variant consists of a formed
perseverated image that is similar to the original but fades after only a couple of seconds. Another
variant consists of a formed afterimage that is black or translucent. These variants usually lack the
realistic clarity of formed image perseveration, and the generation of the palinoptic images is affected
by fixation time, motion, stimulus intensity, or contrast.
2.3. Palinopsia symptom groups
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT6
We divide the subtypes of palinopsia into two symptomatic groups. Illusory palinopsia consists
of prolonged indistinct afterimages, light streaking, visual trailing, and momentary formed image
perseveration. The palinopsia is exposed or exacerbated based on environmental parameters and often
occurs continuously or predictably such as in the morning or during light adaptation. These perseverated
images appear in the same location in the visual field as the original stimulus and are likely due to
sustained awareness of the previously-viewed object. Illusory palinopsia is similar to a visual illusion: the
distorted perception of a real external stimulus.
Hallucinatory palinopsia consists of formed image perseveration, scene perseveration,
categorical incorporation, and patterned visual spread. The perseverated images or scenes can appear
anywhere in the visual field regardless of the location of the original stimulus, have high resolution, and
are typically not reliant on environmental parameters such as contrast, light, and motion. These formed,
high-fidelity afterimages or scenes are likely the projection of an already-encoded visual memory.
Hallucinatory palinopsia is similar to a complex visual hallucination: the creation of a formed visual
stimulus where none exists.
Those who report multiple types of palinopsia usually have all of their symptoms from the same
group, which suggests etiologic and mechanistic similarity. Patients with variant formed image
perseveration have characteristics from both groups, the significance of which will be discussed later
(Section 4.2.).
2.4. Associated symptoms
Patients with both groups of palinopsia often have visual illusions and hallucinations such as
visual snow, micropsia, macropsia, teleopsia, pelopsia, dysmetropsia (“Alice in Wonderland” syndrome),
oscillopsia, phosphenes, and photopsias. Some patients briefly think that the perseverated images are
real, but palinopsia is not associated with delusional ideation or psychosis. Below are terms that are
symptomatically related to palinopsia.
2.4.1. Cerebral polyopia
Cerebral diplopia or polyopia occurs when a patient sees two or more duplicated images
arranged in ordered rows or columns after fixation on an object18,73,153
. The polyopic images occur
monocular bilaterally and binocularly, differentiating it from ocular polyopia. Cerebral polyopia is
sometimes confused with visual trailing, however in cerebral polyopia, the rows or columns of
duplicated images move with the original object, or the polyopic images disappear during motion. In
palinoptic polyopia, movement causes each polyopic image to leave a perseverated image in its wake,
creating hundreds of palinoptic images (entomopia)75,97
.
2.4.2. Akinetopsia
Akinetopsia is defined as a failure to perceive motion, which can occur with or without
palinopsia. Akinetopic palinopsia (visual trailing) is often described as stroboscopic vision. Motion
appears fragmented and afterimages are left at the previous location where the moving object was
observed. Depth perception affects motion perception, and two patients with akinetopic palinopsia had
decreased stereopsis53,94
.
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT7
2.4.3. Visual allesthesia
Visual allesthesia occurs when fixation on an object causes its duplication in the opposite
hemifield. If the patient looks away from the original image and the duplicated image is still retained,
then the patient has visual allesthesia and formed image perseveration palinopsia.
2.4.4. Entoptic phenomena
Entoptic phenomena are the observation of real, physiologic processes within the eye. Examples
include squiggly lines representing white blood cells moving through retinal capillaries or tree-like
outlines representing the retinal vasculature. Entoptic phenomena are the continuous viewing of new
stimuli, different from the persistent or recurrence of a previously viewed stimulus (palinopsia). Entoptic
phenomena may be the result of visual pathway hypersensitivity causing the perception of normally
subthreshold stimuli.
3. Etiology and pathophysiology
Palinopsia has a wide variety of etiologies and mechanisms, which relate to the previously-
defined symptomatic groups.
3.1. Etiology: Post-geniculate cortical lesions
We found 44 cases of palinopsia from posterior visual pathway lesions, and all but three
described hallucinatory palinopsia (formed image perseveration, categorical incorporation, scene
perseveration, patterned visual spread). There were 17 cases of cerebrovascular accidents (CVAs) 10,35,38,57,61,85-87,104,106,111,122,145,146,A
, 26 cases of space-occupying lesions, one case of idiopathic gliosis37
, and
one case of cortical dysplasia113
(Appendix). Of the 26 cases of palinopsia from a space-occupying lesion,
14 were neoplasms17,30,77,82,89,91,104,111,151,153
, five were infectious lesions, five were arteriovenous
malformations (AVMs)45,69,84,122
, and one was an aneurysm17
. Of the infectious causes, there were three
abscesses (in the setting of acute myeloid leukemia116
, Kartagener syndrome98
, and Noonan
syndrome11
), one tuberculoma149
, and one case of neurocysticercosis10
.
Palinopsia, once considered a disorder of the non-dominant parieto-occipital lobe, has since
been shown to occur from lesions in the dominant or non-dominant temporal, parietal, or occipital
lobes. There are 24 reported cases of palinopsia with lesions in the occipital cortex, five in the parietal
cortex, two in the temporal cortex, eight in the occipito-parietal area, five in the occipito-temporal area,
and one in the occipito-parieto-temporal area. There were 35 cases with right-sided pathology, nine
with left-sided pathology, and one lesion was midline. The predominance of right-sided lesions might be
from anatomical or functional differences in visual memory encoding26
. Palinopsia from post-geniculate
cortical lesions is caused by focal cortical hyperactivity, which may be from cortical deafferentation,
epileptic discharges, or cortical irritation.
3.1.1. Pathophysiology: Cortical deafferentation hyperexcitability
Palinopsia commonly occurs in the setting of posterior visual pathway deafferentation causing
homonymous visual field deficits, of which patients are frequently unaware (hemianopic anosagnosia).

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT8
Of the 43 patients with homonymous visual field deficits, 40 (93%) described hallucinatory palinopsia
(Appendix). This palinoptic mechanism is thought to be similar to visual release hallucinations (Charles-
Bonnet Syndrome)37
which are due to neuronal hyperexcitabiity, often from ocular vision loss.
Hallucinatory palinopsia is due to focal cortical hyperexcitability from cortical visual loss. Visual release
hallucinations are distinguished from palinopsia by content (if the formed image or scene actually
occurred). Deafferentation hyperexcitability is a well-studied phenomenon, also seen in neuropathic
pain and phantom limb syndrome. Molecular changes include a presynaptic increase in
neurotransmitter vesicle size and number, increased post-synaptic receptor sensitivity, and alterations
in extracellular neurotransmitter concentrations27
.
3.1.2. Pathophysiology: Epileptic discharges
Palinopsia may occur during a seizure aura, the ictal phase, and post-ictally, with the epileptic
discharges confirmed by electroencephalogram (EEG) 18,50,91,111
. The seizures can originate in the
temporal, parietal, or occipital lobe, depending on the lesion location. The discharge may stay localized
or spread, although there is rarely seizure generalization70,111. Some visual seizures do not have the
commonly associated motor and sensory symptoms, and there are case reports of palinopsia as the only
symptom of the seizure111
. The palinoptic seizure may leave the primary visual pathway unaltered152
or
the patients may report visual field loss related to the seizure, with the palinopsia appearing in the field
deficit85
.
3.1.3. Pathophysiology: Focal cortical irritation
Palinopsia after neurosurgical procedures or cerebrovascular events is attributed, in part, to
focal cortical irritation70,85,154
. Hayashi et al report palinopsia is associated with perilesional
hyperperfusion, which could reflect focal cortical instability and hyperactivity61
.
3.2. Etiology: Metabolic or systemic disease
There are seven case reports of palinopsia in the setting of a metabolic or systemic disease:
three from uncontrolled diabetes causing hyperglycemic seizures25,72,106
, two attributed to transient
ischemic attacks117,140
, one from carnitine deficiency causing secondary seizures80
, and one in Leber
hereditary optic neuropathy (the only report of palinopsia from ocular vision loss)117
. All of these
patients had visual field deficits or seizures, suggesting a similar mechanism to palinopsia caused by
post-geniculate cortical lesions (sections 3.1.1. and 3.1.2.). These patients all reported hallucinatory
palinopsia (Appendix).
3.3. Etiology: Idiopathic seizures
Epileptic discharges are commonly associated with palinopsia, but the seizure is usually
secondary to an easily diagnosable cortical lesion or metabolic disturbance (section 3.1. and 3.2.). There
are six cases of palinopsia from idiopathic seizures17,75,107,115,133,141
, five of which reported hallucinatory
palinopsia (Appendix).
3.4. Etiology: Diffuse cortical pathology

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT9
There are nine cases of palinopsia from diffuse cortical pathology: three from multiple
sclerosis8,71,117
(MS), three from posterior cortical atrophy (PCA) variant of Alzheimer disease33,145
, one
from a primary B cell lymphoma with unremarkable neuroimaging135
, one from Creutzfeld-Jacob disease
(CJD)119, and one from an epileptic ion channel mutation42 (Appendix). The patients with the ion channel
mutation, CJD, and primary B-cell lymphoma had epileptic discharges (section 3.1.2.), and these patients
described hallucinatory palinopsia. All of the patients with multiple sclerosis experienced the black or
translucent variant of formed image perseveration. One patient developed unilateral, monocular
palinopsia after a bout of optic neuritis, perhaps indicating a pre-chiasmatic lesion117
. To note, one
patient with MS had focal white matter enhancement but still was included in the diffuse cortical
pathology group8. The PCA cases will be discussed later (Section 5.3.3.).
3.4.1. Pathophysiology: Demyelination
MS causes inflammatory demyelination in the CNS, affecting the anterior and posterior visual
pathways. Demyelination is associated with increased inflammatory cytokines and synaptic
hyperexcitability123.
3.5. Etiology: Drug-induced
3.5.1. Illicit drugs
There are 14 cases of palinopsia attributed to the intake of illicit drugs, all of which reported
illusory palinopsia1,9,53,76,92,94,102,140
(Appendix). One case described both types of palinopsia. After taking
hallucinogens, as many as 50% of people experience “flashbacks”, a spontaneous and often transitory
feeling of being under the influence of the drug which occurs any time after drug ingestion. If these
experiences are prolonged, pervasive, and recurrent, it is known as hallucinogen persisting perception
disorder (HPPD). Lysergic acid diethylamide (LSD ) is the most common cause of HPPD, which occurs in
about 5% of past users. Psylocibin (psychedelic mushrooms), 3,4 methylenedioxy-N-
methylamphetamine (MDMA or ecstasy), and cannabis (marijuana) have also been implicated41
. The
visual symptoms of HPPD include illusory palinopsia (light streaking, visual trailing, prolonged indistinct
afterimages, prolonged light afterimages, momentary formed image perseveration), dysmetropsia,
oscillopsia, visual snow, halos, entopic phenomena, and photopsias2,14
.
HPPD is more commonly and thoroughly described in the psychiatric literature and palinoptic
symptoms are often not defined as palinopsia. Patients are often reluctant to admit drug use, and
palinopsia from HPPD is likely relatively common. The relationship between the number and strength of
hallucinogen doses and HPPD is not clear, but there are reports of HPPD after minimal hallucinogen use,
sometimes after just one dose2,59,94
.
3.5.2. Prescription drugs
There are 27 case reports of palinopsia from prescription drugs. All except two of the patients
described illusory palinopsia, which would often co-exist with other visual illusions and unformed
hallucinations (Appendix). These symptoms typically occur during drug initiation or dose increase and
resolve after drug discontinuation. There are four published cases solely from trazodone along with nine
unpublished cases that occurred during clinical trials1,66
. There are eight cases from

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT10
nefazodone48,65,67,83,108,127
, which is rarely used because of serious adverse effects. There is one case of
palinopsia from mirtazepine68
, two cases from topiramate46,49
, and one case from zosuquidar124
. There
are three cases of palinopsia from risperidone5, which caused a relapse of HPPD. There are three cases
of clomiphene-induced palinopsia along with more complaints of “visual disturbances” in FDA reports120.
Clomiphene caused permanent symptoms. There are also three cases from a combination of the
aforementioned drugs46,88,132
. There are single reports of palinopsia from maprotiline and interleukin-2,
although there was a questionable link between the symptoms and the drugs51,64
.
3.5.3. Pathophysiology: Diffuse neurotransmitter and neurotransmitter receptor alterations
The illusory palinopsia induced by drugs is mainly caused by antidepressants and HPPD after
LSD, both of which act primarily on the serotonergic system. The main target of LSD is the 5HT2a
receptor, and Abraham et al found that HPPD is associated with 5HT2a receptor excitotoxicity3.
Additionally, nefazodone and trazodone are 5HT2a receptor antagonists. Le Grand et al found that
serotonin depletion leads to cortical hyperexcitability90
.
Drugs such as topiramate or clomiphene also cause palinopsia but are not considered to be
strongly associated with the serotonergic system. The symptoms may be related to a disruption in
GABAnergic transmission, which is facilitated by the 5HT2a receptor129
. Topiramate is also known to
modulate cortical excitability12
, and Abraham et al found cortical disinhibition in HPPD4. Regardless, the
neuropharmacology of the visual system is exceedingly complex and neurotransmitter profiles are
largely unstudied.
Illusory palinopsia is strikingly dependent on external light or the motion of an object. Light and
motion perception are dynamic operations involving processing and feedback from structures
throughout the central nervous system: retina, lateral geniculate nucleus (LGN), V1-V5, superior
colliculus, frontal eye fields, Edinger-Westphal nucleus, etc. We approach illusory palinopsia by
considering the impact of diffuse neuronal excitability alterations on physiological mechanisms for light
and motion perception.
3.5.3.1. Dysfunction in light perception
Light perception depends on the external parameters of the stimulus as well as internal
conditions such as neuronal depolarization sensitivity, retinal adaptation state, and cortical adaptation
state. Light contrast and intensity is mostly processed in V1, although processing and feedback from
many other structures throughout the visual pathway affect light perception55
. For example, retinal
ganglion cells can merge neural signals to increase light sensitivity and alter the perception of the
signal44
. Olsen et al show that layer 6 of V1, an area with many corticothalamic neurons, is especially
important in light and contrast perception114, highlighting the significance of the feedback loops.
Dysregulated cortico-thalamo-retinal feedback could cause failed cortical and retinal/geniculate light
adaptation resulting in prolonged positive and negative light afterimages, respectively103
.
3.5.4.2. Dysfunction in motion perception
Motion perception requires high-level cortical processing and precise coordination between
multiple regions of the brain, with a large emphasis on MT/MST (medial temporal/medial superior

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT11
temporal areas). Visual trailing is reported during object movement, observer movement, and eye
movement, with or without fixation, suggesting a dysfunction in global motion processing mechanisms.
Visual masking and corollary discharges are inhibitory mechanisms which reduce normal motion blur
from object movement and from eye movement. They are best studied in saccades (saccadic
suppression) but are also present in smooth pursuit and blinking15,28,29,32,52,143,150
.
Visual masking is a phenomenon characterized by the reduction in visibility of an object caused
by the appearance of a second object in space or time. The presentation of a second stimulus can
obscure the perception of a previous stimulus, or the leading edge of a moving object can mask the back
end of the same object which removes visual trails43,99,112
. The masked visual trails are removed from
perceptual awareness but are still processed, helping determine the direction of the motion. Perhaps
persistent, diffuse neuronal hyperexcitability causes failed visual masking and blurred visual trails.
Kilpatrick et al report that visual trailing could result from a group of V1 neurons that stay persistently
active79
. There is currently debate whether visual masking involves active or passive cortical
inhibition84,99,150
.
A corollary discharge is an internal duplicated copy of an efferent signal which notifies other
neurons of impending muscle movement. Corollary discharges help integrate eye movements with
neuro-anatomically segregated processes such as visual attention39
. A well-characterized saccadic
corollary discharge originates in the superior colliculus, synapses in the pulvinar, and proceeds to
MT/MST to inhibit motion processing during the saccade150
. The visual system then integrates pre-
suppression and post-suppression images to create seamless motion105
. A failure to assimilate this
information could result in discontinuous visual trails and akinetopsia. Perhaps diffuse hyperexcitability
causes prominent pre-suppression images, or incomplete/inappropriate corollary discharges do not
properly activate the cortical areas associated with image integration. Shepherd reports that enhanced
motion after-effects in migraineurs are associated with extended suppression130
.
3.6. Etiology: Migraine
There are six cases of palinopsia from migraines, all of which described illusory
palinopsia47,96,117,134,B
. These illusory palinoptic symptoms are often continuous and co-exist with the
other simple visual hallucinations and visual illusions of a migraine aura such as dysmetropsia,
oscillopsia, photopsias, entoptic phenomena, and visual snow. When aura symptoms persist in
migraineurs, the condition is defined by The International Classification of Headache Disorders (ICHD) as
persistent visual aura without infarction142
. Persistent visual aura is further subdivided into typical aura
symptoms (homonymous, gradually developing) such as scotomas and teichopsia and atypical aura
symptoms (diffuse, continuous) such as illusory palinopsia, visual snow, visual trailing, and oscillopsia148
.
Belcastro et al performed a case control study of 200 migraineurs and found that momentary
palinopsia (variant formed image perseveration) occurred in 14.2% of migraineurs with aura and 6.6% of
migraineurs without aura16
. These paroxysmal perseverated images could appear at a different location
in the visual field than the original stimulus, would usually only last a couple of seconds, and occurred a
few times per month. The patients in this study did not complain of other visual symptoms. To note, a
patient on topiramate can have migraine-induced palinopsia, or a patient with migraines can have
topiramate-induced palinopsia.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT12
3.6.1. Pathophysiology: Cortical spreading depression
Cortical spreading depression (CSD), the presumed cause of a migraine aura, is a wave of intense
depolarizing electrical activity that slowly spreads across cortical grey matter, followed by 1/2 to 2
minutes of suppressed neuronal activity and electrical silence, with eventual repolarization. During the
electrical silence, there is reduced cerebral blood flow, ion homeostasis, decreased extracellular pH, and
intracellular swelling136
. The intense electrical activity could be clinically related to the positive
symptoms (scintillations, tinnitus, tingling) and the subsequent silence to the negative symptoms
(scotomas, hearing loss, paresthesias) of a migraine aura. Following the electrical silence and negative
symptoms, the neuronal repolarization and hyperexcitability would clinically manifest as photophobia,
phonophobia, and cutaneous allodynia. Migraineurs have significant interictal fluctuations in cortical
excitability36
, and most evidence points to a hyperexcitable state being associated with the generation
of the wave of CSD, causing the aura22,23,126,136,138
and perhaps the headache13,110,126
.
The pathophysiology of persistent visual aura is not well-established. Chen et al report ictal
visual cortex excitability potentiation in persistent visual aura compared to ictal habituation in other
migraine types34. Perhaps ictal potentiation and failed cortical adaptation primes the cortex for CSD
wave reverberation, causing the spontaneous and focal symptoms (teichopsia and scotoma) in
persistent aura19,47,148
. Chen et al also report greater interictal visual cortex hyperexcitability in
persistent visual aura than in episodic migraine34
, which could be an effect of the ictal potentiation.
Diffuse, persistent alterations in neuronal excitability would impair light or motion processing, causing
continuous symptoms (illusory palinopsia, visual snow, dysmetropsia, oscillopsia, photophobia). These
diffuse symptoms supports accumulating evidence that emphasizes the role of the thalamus and
brainstem in migraine pathogenesis6,58,109,118
.
The momentary formed perseverated images in as many as 10% of migraineurs are
symptomatically similar to the longer-lasting formed perseverated images from epileptic discharges,
cortical deafferentation, and focal cortical irritation. These migrainous afterimages could represent
localized, transient cortical hyperactivity during a peak in the cyclical cortical excitability state.
Interestingly, Belcastro et al found that migraineurs with these momentary perseverated images
reported significantly fewer migraine attacks (4.3 vs 14.4 attacks/year) than the patients who did not
complain of palinopsia16
. Perhaps the relatively mild, localized, and non-propagating focal electrical
discharge, which generates the momentary afterimage, functions as a failsafe. This could hinder the
production of intensely depolarizing waves of CSD that are associated with the wave propagation, the
prolonged repolarization time, and the subsequent teichopsia, scotoma, and headache.
3.7. Etiology: Head trauma
There are four reports of palinopsia arising after a head injury, all of which described illusory
palinopsia1,50,96,117
. Patients with palinopsia from a traumatic head injury often complain of similar visual
illusions and simple hallucinations as the patients with persistent visual aura and HPPD.
3.7.1 Pathophysiology: Diffuse cortical irritation
Traumatic brain injuries can cause focal or diffuse cortical hyperactivity. Focal hyperactivity and
epilepsy typically require a structural lesion from the head injury101
. The majority of concussion

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT13
symptoms stem from diffuse neuronal dysfunction60
which probably causes diffuse neuronal
hyperexcitability7. Heron et al documented illusory palinopsia, along with other visual illusions and
unformed hallucinations after six days of perceptual isolation62
.
3.8. Etiology: Psychiatric conditions
There are four cases in the literature that report palinopsia from psychiatric conditions:
schizophrenia100
, psychotic depression56
, and Capgras and Cotard Syndrome74
, and peduncular
hallucinosis78. The patient with psychotic depression described repetitively seeing a visual hallucination
(not palinopsia), the patient with peduncular hallucinosis described complex visual hallucinations (not
palinopsia), and the patient with Capgras and Cotard syndrome described repeatedly seeing his
Doppelganger while psychotic, consistent with the syndrome of subjective doubles (not palinopsia). The
patient with schizophrenia reported palinopsia while not overtly psychotic, stating that the palinopsia
worsened when stressed, tired, or prior to a psychotic episode.
3.9. Idiopathic palinopsia
There are five cases of idiopathic palinopsia20,104,117
. There are ICHD classifications for typical
visual aura with non-migraine headache, typical visual aura with no headache, and persistent visual aura
without infarction142
. Therefore, palinopsia without the associated migraine headache could conceivably
be analogous to persistent aura with non-migraine headache or persistent aura with no headache.
Cortical spreading depression also occurs during acute cortical insults40
, so palinopsia and other visual
illusions and hallucinations could theoretically arise from insignificant or silent infarctions.
3.10 Visual snow clinical syndrome
Schankin at al recently dubbed “visual snow clinical syndrome” to describe patients with
refractory symptoms, which they characterized as visual snow along with momentary formed image
perseveration (86%), photopsia (63%), floaters (81%), visual trailing (60%), photophobia (74%),
nyctalopia (68%), tinnitus (62%), blue field entopic phenomena (79%), concentration problems (60%),
and lethargy (55%)125
. Schankin et al report that 59% of the patients have a history of migraines, 87%
have a history of headaches, and 36% describe symptoms starting directly after a migraine125
. Various
combinations of the aforementioned symptoms, with or without visual snow, often co-exist with other
diffuse illusory symptoms (oscillopsia, halos, dysmetropsia) in atypical persistent visual aura, in HPPD, as
a prescription drug side effect, after head trauma, or can be idiopathic1,20,29,47,50,53,65,88,94,96,117,120,134.
The atypical persistent visual aura with the diffuse, illusory symptoms is often harder to treat
than the typical persistent visual aura with scotomas and teichopsia148
. If these continuous and
refractory symptoms (which often agitate the patient) represent a clinical entity, then perhaps more
information on symptom pathogenesis and treatment is needed to determine if visual snow should be
classified separately from the associated persistent diffuse symptoms (including illusory palinopsia) with
the same etiologies.
4. Relationship between pathophysiology, etiology, and symptomology
4.1. Correlation between pathophysiology, etiology, and symptomology

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT14
Reflecting the etiology and symptomology, we now split the pathophysiology of palinopsia into
two categories: dysfunction of visual memory and dysfunction of visual perception (Figure 2).
4.1.1. Dysfunction of visual memory
Hallucinatory palinopsia (formed image perseveration, scene perseveration, categorical
incorporation, patterned visual spread) is indicative of a dysfunction in visual memory, focal cortical
hyperactivity due to post-geniculate lesions or seizures. Cortical deafferentation, epileptic discharges, or
focal irritation cause unregulated or uncontrolled depolarizations and persistent or recurrent activation
of post-geniculate neurons that function in visual memory encoding, processing, or retrieval50
(Figure 2),
Environmental conditions or external parameters will not usually alter the afterimage, implying that the
objects, features, or scenes are already encoded in visual memory. The perseverated images can occur
at a different location in the visual field as the original stimulus and are isochromatic, high-resolution,
and long-lasting.
Cortical deafferentation and focal irritation usually cause a few episodes of palinopsia,
suggesting there is quick cortical compensation to reduce the hyperexcitability. If seizures are persistent,
then continual palinoptic episodes occur. Symptoms may present in a patient with EEG-diagnosed
seizures and visual field deficits, after a neurosurgical procedure. This suggests that the focal neuronal
hyperactivity from each mechanism is additive. Of the 56 patients with focal, posterior visual pathway
lesions or seizures, 52 (93%) described hallucinatory palinopsia (Appendix).
In categorical incorporation, contextual data from visual association circuits is externally
superimposed onto other objects, indicating pathology in visual memory and processing. All of the
hallucinatory palinopsia symptoms can occur concomitantly in a patient with one lesion, which supports
current evidence that objects, features, and scenes are all units of visual memory21
, perhaps at different
levels of processing. This alludes to neuroanatomical integration in visual memory creation and storage.
4.1.2. Dysfunction of visual perception
Illusory palinopsia (visual trailing, light streaking, prolonged indistinct afterimages, momentary
formed image perseveration) is indicative of a dysfunction of visual perception, probably caused by
diffuse, persistent alterations in excitability which can occur after head trauma, after hallucinogen use,
and in migraineurs. There could be a dysfunction in adaptation and feedback between the anterior and
posterior visual pathways. The altered brain state likely affects physiological mechanisms of light or
motion perception, as the perseverated images are heavily dependent on parameters such as eye
fixation, stimulus intensity, background contrast, and motion (Figure 2). Symptoms are often continuous
or predictable and occur at the same location in the visual field as the original stimulus. These
perseverated images tend to be blurry or short-lived. Of the 50 cases of palinopsia that are idiopathic or
attributed to migraines, HPPD, prescription drugs, or head trauma, 47 (94%) described illusory
palinopsia (Appendix).
Symptoms are often worse with high stimulus intensity, a high contrast ratio, and a dark-
adapted state. One patient frequently has symptoms that represent dysfunction in light and motion
perception, even though light and motion are processed via different pathways. This suggests diffuse or
global involvement of visual pathway. Some evidence suggests that patients with persistent illusory

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT15
phenomena also have high rates of cognitive deficits125
, which implies an altered brain state beyond the
visual pathway.
4.2. Overlap in dysfunction of visual memory and visual perception
There is mechanistic commonality in palinopsia since all the proposed mechanisms focus on
dysfunction of neuronal excitability and activity. The features of each symptomatic group are typical
descriptions, not strict guidelines, and there are cases that describe patients with characteristics from
both groups. We used the clarity and duration of the perseverated images as the predominant
determining factors. For example, one case reported hallucinatory palinopsia lasted 30-90 seconds but
was more pronounced after fixation and with high contrast37
. Another case of hallucinatory palinopsia
(from trazodone) described blurred but formed afterimages that required movement, were worse in the
morning, swirled, and lasted 15minutes66
. One patient had unpredictable, paroxysmal episodes of visual
trailing1. A patient with PCA and severe occipital pole atrophy reported that objects would appear in the
complementary color of a previously-viewed bright stimulus33
, which is probably a mix of patterned
visual spread and prolonged physiological afterimages.
The long-lasting black or translucent afterimages in multiple sclerosis and the momentary
afterimages common in migraineurs do not quite fit into either group. These perseverated images are
affected by external parameters and often co-exist with illusory symptoms16,71,B
. The brief, positive, and
formed afterimages in migraineurs were included in illusory palinopsia to simplify the clinical and
prognostic picture. Yet if caused by transient, focal cortical hyperactivity from CSD, they are
mechanistically more similar to hallucinatory palinopsia. Further study of these afterimages in relation
to alterations in cortical excitability could help expose mechanisms associated with the encoding of
visual memory.
5. Clinical encounter
It is important to recognize that palinopsia is a collection of symptoms, not a diagnosis. The
diversity in the etiologies of palinopsia necessitates a thorough history, physical exam, and work-up.
5.1. Clinical history
The clinical history of the palinopsia provides much prognostic information. One should
determine if the palinopsia is illusory or hallucinatory, inquiring about the length, content, and color of
the persisting images or scenes, the time delay between the original stimulus and the palinoptic image,
the number of episodes, the time of day, the place in the visual field where the original and
perseverated image occurred, and if light or motion exacerbates or exposes the palinopsia.
One should take a careful headache history since migraines, cerebrovascular accidents, visual
seizures, and neoplasms can all cause palinopsia. The examiner should ask about the associated
headache symptoms and ask about symptoms related to possible ictal events such as focal neurological
signs, tongue biting, incontinence, nausea/vomiting, and other positive and negative visual phenomena.
Patients complaining of black or translucent afterimages should specifically be asked about findings
associated with multiple sclerosis such as optic neuritis or spasticity.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT16
A detailed medical and surgical history is important, with emphasis on ophthalmological,
neurological, and psychiatric illnesses and procedures and their relationship to the onset of the
palinopsia. The examiner should also get a detailed prescription drug history, looking for
antidepressants, topiramate, clomiphene, contraceptives, and risperidone. One should ask about a
history of head trauma and a past hallucinogenic drug use, especially in a patient who complains of
illusory palinopsia with a clinical history that does not suggest any other etiologies.
5.2. Physical exam
Palinopsia necessitates proper ophthalmological and neurological physical exams. Visual acuity,
pupils, tonometry, extraocular movements, external exam, and anterior chamber exam are usually
noncontributory. Bedside or formal visual fields may show deficits in cases with structural lesions.
Funduscopy is typically normal but may reveal papilledema if the underlying etiology causes significant
mass effect. The neurological exam including cranial nerves, deep tendon reflexes, sensation, motor,
and cerebellar testing is often normal since the pathology (if present) is often in the visual pathway.
5.3 Work-up and Diagnosis
Visual fields and neuroimaging should usually be obtained in patients with palinopsia. Routine
labs such as a complete metabolic panel and complete blood count may be done to check for metabolic
disturbances or hint at the presence of a neoplasm. Other diagnostic tests such as structural or
functional neuroimaging, EEG, electroretinogram, visual evoked potential, lumbar puncture, or drug
screen should be performed on an as-needed basis, depending on the clinical history, the results of the
preliminary work-up, the working diagnosis, and the symptom persistence.
5.3.1. Hallucinatory palinopsia
It is generally easy to diagnose the primary cause of hallucinatory palinopsia, the symptoms
indicative of a dysfunction of visual memory. Neuroimaging will usually reveal cortical lesions. In
patients with unremarkable neuroimaging, blood tests and clinical history will often expose the
pathology. An EEG can be performed if epileptic discharges are suspected by the clinical history, or there
is a long latency between the original and palinoptic image, multiple recurrences of the same
perseverated image or scene, or continual episodes of hallucinatory palinopsia.
One should be cognizant of hallucinatory palinopsia symptoms, which can be the presenting
symptom of a potentially life-threatening illness116,154. If the primary work-up is negative, there should
be a short follow-up. One patient who experienced an episode of formed image perseveration with
unremarkable neuroimaging was diagnosed five months later with a glioblastoma multiforme82
. Another
patient was later diagnosed with CJD119
. Occasionally, hallucinatory palinopsia is drug-related or caused
by TIAs, and the patient would continue to have negative diagnostic testing.
5.3.2. Illusory palinopsia Illusory palinopsia, symptoms indicative of a dysfunction in visual perception, is usually due to
pharmaceutical drugs, HPPD, migraines, or head trauma. The physical exam and work-up are almost
always non-contributory, and diagnosis is largely based on information from the clinical history.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT17
Palinopsia is attributed to a prescription drug if symptoms begin after initiation or dose increase.
Continuous illusory palinopsia in a migraineur is usually persistent migrainous aura. HPPD is a diagnosis
of exclusion in patients with a history of hallucinogen use. Migraines and HPPD are probably the most
common causes of palinopsia, despite the paucity of case reports in the literature.
If the history and work-up do not reveal an etiology, then the idiopathic palinopsia may be
analogous to the cerebral state in persistent visual aura with non-migraine headache or persistent visual
aura with no headache. Because of the subjective nature of the symptoms and the absence of organic
findings, doctors are sometimes dismissive of patients with illusory palinopsia, which may cause the
patients considerable distress. There is substantial evidence in the literature verifying the symptom
legitimacy, so validating the patient’s symptoms can alleviate anxiety.
5.3.3. Exceptions to palinopsia groupings
Five patients (with schizophrenia, infarction, neoplasm, HPPD, idiopathic) had symptoms from
both groups (Appendix), and a few patients had a diagnosis in the opposite group as would be
predicated by symptomology. Patients with illusory palinopsia from cortical lesions or seizures usually
have other alarming symptoms such as neurological deficits or complex visual hallucinations37,75
.
Unidirectional visual trails, symptoms confined to part of a visual field, or homonymous field loss
suggests focal cortical pathology. One patient had a left-sided infarction in MT/MST causing only
rightward akinetopic visual trails57
. Two patients with PCA had severe right-sided parietal atrophy and
only leftward akinetopic visual trails144
. Another patient with occipital and LGN infarctions had light
streaking confined to the quadrant with the field deficit145
.
Risk factors for possible serious pathology include old age, vasculopathy, a history of cancer, and
a history of radiation. It is reasonable to order neuroimaging in illusory palinopsia, as migraine aura
symptoms can mimic seizures or posterior cortical lesions63,113,122,128
. In a young patient with illusory
palinopsia and no other worrisome symptoms or signs, neuroimaging is low-yield but may provide the
patient peace of mind. Belcastro et al reported that as many as 10% of migraineurs have isolated
episodes of momentary formed image perseveration16
. If this data is corroborated, then these patients
might not need additional neuroimaging.
There are not any reported cases of palinopsia from cancer-associated retinopathy or
metabolic/toxic retinopathy, but there are reports of related illusory symptoms in these occult
conditions. Further retinal work-up might be indicated in a patient presenting with palinopsia and a
suggestive clinical history.
5.4. Treatment
Palinopsia from CVAs typically resolves spontaneously and treatment should be directed at the
vasculopathic risk factors. Neoplasms, AVMs, or abscesses require treatment of the underlying
condition, which usually also resolves the palinopsia. Palinopsia due to seizures generally resolves after
correcting the primary disturbance and/or treating the seizures. The literature reports success with
carbamazepine or phenytoin, but newer, less toxic drugs with similar seizure-aborting ability could likely
be used. In persistent hallucinatory palinopsia, a trial of an anti-epileptic drug may be attempted since

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT18
there could be undiagnosed seizures. Drugs that reduce cortical excitability could also potentially treat
palinopsia caused by deafferentation or irritation.
Palinopsia from prescription drugs is treated by discontinuing the offending agent, although this
is only necessary in drugs reported to cause permanent symptoms (clomiphene and oral
contraceptives). If symptoms are not bothersome and there is a positive therapeutic response, the
patient may elect to continue the drug. There is no standard treatment for HPPD, and no randomized
controlled trials have been performed. The condition is generally benign, so treatment is based on the
patient’s distress and willingness to try multiple trials of different drugs. Case series of 7-9 patients show
an 80%+ cure rate from benzodiazepines, clonidine, and haloperidol for HPPD59
. Given the side-effect
profile of haloperidol and the abuse potential of benzodiazepines, these drugs are not optimal for
treating a benign condition. Additionally, Lerner et al report that the trailing phenomenon is
“remarkably refractory” to clonazepam93
. There are reports of selective serotonin reuptake inhibitors
and risperidone exacerbating HPPD5,59
.
There is even less evidence for treating persistent migrainous aura without infarction. There are
single cases which report successful treatment with lamotrigine, nimodipine, topiramate, verapamil,
divalproex sodium, gabapentin, furosemide, and acetazolamide, as these drugs have mechanisms that
decrease neuronal excitability34,134
. Others report treatment failure from the same drugs. Some report
that treating the migraine improves the persistent aura symptoms, while others report no effect47. The
focal, typical persistent visual aura symptoms are usually easier to treat than the diffuse atypical
persistent visual aura symptoms148
.
It is not clear if the etiology of the illusory palinopsia affects treatment efficacy, but given the
symptom similarity, it is reasonable to try the same pharmaceuticals to treat the illusory symptoms from
persistent migrainous aura, HPPD, head trauma, and idiopathic palinopsia. Based on the available
evidence and side-effect profile, clonidine might be an attractive treatment option. Richter et al show
that clonidine suppresses CSD in rats121, and indirect evidence shows that clonidine reduces cortical
hyperexcitability31,95
. Other drugs with relatively benign side effect profiles may also be attempted, if
desired by the patient. Since many patients report improvement from sunglasses, one could suggest
trying the FL-41 tinted lenses which have shown some efficacy in treating visually sensitive
migraineurs151
.
6. Conclusion
Palinopsia is not a diagnosis, but a broad term that describes a heterogeneous group of
symptoms. We divided the symptoms into two clinically relevant categories. Hallucinatory palinopsia
consists of formed image perseveration, scene perseveration, categorical incorporation, and patterned
visual spread. These symptoms typically arise from post-geniculate cortical lesions and various seizure
etiologies and resolve after treating the underlying pathology. The perseverated images are long-lasting,
high clarity, isochromatic, and not typically affected by light or motion. Hallucinatory palinopsia is the
result of posterior visual pathway deafferentation, epileptic discharges, or focal cortical irritation, which
likely cause focal cortical hyperexcitability or hyperactivity and inappropriate and persistent activation
of a visual memory circuit (Figure 2). If no etiology is found, these alarming symptoms warrant further
testing or prompt follow-up. This was previously considered a dorsal stream disorder in the non-

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT19
dominant parieto-occipital l lobe, but the predominance of lesions in certain cortical areas is more likely
due to the uneven distribution or functional variation of visual cortex-hippocampal neurons.
Illusory palinopsia consists of momentary formed image perseveration, prolonged indistinct
afterimages, light streaking, and visual trailing (Figure 2). The perseverated images short-lived or
unformed, occur in the same location in the visual field as the original stimulus, and are affected by
fixation, light, and motion. Migraines (persistent migrainous aura), HPPD, prescription drugs, and head
trauma are the known etiologies, but the palinopsia can also be idiopathic. Combinations of the illusory
palinoptic symptoms often co-exist with simple visual hallucinations and with other diffuse, illusory
symptoms such as visual snow, dysmetropsia, and oscillopsia. These symptoms are presumably related
to a diffuse modification in neuronal sensitivity or excitability. More evidence is needed on the efficacy
of pharmaceuticals for these various symptoms and diagnoses, but clonidine, gabapentin,
acetazolamide, magnesium, or calcium channel blockers could be possible treatment options.
7. Method of literature search
We conducted a PubMed and Web of Science search of the English language literature using the
search terms palinopsia, paliopsia, visual perseveration, cerebral polyopia, illusory visual spread, visual
trails, visual snow, visual trailing, hallucinogen persisting perception disorder, positive spontaneous
visual phenomena, akinetopsia, and dyskinetopsia from 1968 to the present. Reference lists from
retrieved articles were examined for additional citations. The accepted definition of palinopsia was
described in 1968, and neuroimaging was not available which caused difficulty in diagnosis before that
time. Cases that did not adequately describe symptoms were excluded from numerical analysis
(Appendix). Non-case articles describing palinoptic mechanisms were reviewed as needed.
8. Disclosures
The authors report no proprietary or commercial interests in any product or concept discussed
in this article.
9. References
1. Abert B, Ilsen PF. Palinopsia. Optometry. 2010;81(8):394-404
2. Abraham HD. Visual phenomenology of the LSD flashback. Arch Gen Psychiatry. 1983;40(8):884-9
3. Abraham HD, Aldridge AM, Gogia P. The psychopharmacology of hallucinogens.
Neuropsychopharmacology. 1996;14(4):285-98
4. Abraham HD, Duffy FH. Stable quantitative EEG difference in post-LSD visual disorder by split-half
analysis: evidence for disinhibition. Psychiatry Res. 1996;67(3):173-87
5. Abraham HD, Mamen A. LSD-like panic from risperidone in post-LSD visual disorder. J Clin
Psychopharmacol. 1996;16(3):238-41
6. Akerman S, Holland PR, Goadsby P J. Diencephalic and brainstem mechanisms in migraine. Nat Rev
Neurosci. 2011;12(10):570-84
7. Alwis DS, Johnstone V, Yan E, Rajan R. Diffuse traumatic brain injury and the sensory brain. Clin Exp
Pharmacol Physiol. 2013;40(7):473-83
8. Anbarasan D., Howard J. Acute exacerbation of multiple sclerosis presenting with facial
metamorphopsia and palinopsia. Mult Scler. 2013;19(3):369-71
9. Anderson WH, O'Malley JE. Trifluoperazine for the "trailing" phenomenon. Jama. 1972;220(9):1244-5

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT20
10. Ardila A, Botero M, Gomez J. Palinopsia and visual allesthesia. Int J Neurosci. 1987;32(3-4):775-82
11. Arnold RW, Janis B, Wellman S, Crouch E, Rosen C. Palinopsia with bacterial brain abscess and
Noonan syndrome. Alaska Med. 1999;41(1):3-7
12. Aurora SK, Barrodale PM, Vermaas AR, Rudra CB. Topiramate modulates excitability of the occipital
cortex when measured by transcranial magnetic stimulation. Cephalalgia. 2010;30(6):648-54
13. Aurora SK, Wilkinson F. The brain is hyperexcitable in migraine. Cephalalgia. 2007;27(12):1442-53
14. Baggott MJ, Coyle JR, Erowid E, Erowid F, Robertson LC. Abnormal visual experiences in individuals
with histories of hallucinogen use: a Web-based questionnaire. Drug Alcohol Depend. 2011;114(1):61-6
15. Barnes GR. Cognitive processes involved in smooth pursuit eye movements. Brain Cogn.
2008;68(3):309-26
16. Belcastro V, Cupini LM, Corbelli I et al. Palinopsia in patients with migraine: a case-control study.
Cephalalgia. 2011;31(9): 999-1004
17. Bender MB, Feldman M, Sobin A J. Palinopsia. Brain. 1968;91(2): 321-38
18. Bender MB, Sobin AJ. Polyopia and palinopsia in homonymous fields of vision. Trans Am Neurol
Assoc. 1963;88:56-9
19. Bereczki D, Kollar J, Kozak N et al. Cortical spreading edema in persistent visual migraine aura.
Headache. 2008;48(8):1226-9
20. Blythe IM, Bromley JM, Ruddock KH, Kennard C, Traub M. A study of systematic visual perseveration
involving central mechanisms. Brain. 1986;109(4):661-75
21. Brady TF, Konkle T, Alvarez GA. A review of visual memory capacity: Beyond individual items and
toward structured representations. J Vis. 2011;11(5):1-34
22. Brigo F, Storti M, Nardone R et al. Transcranial magnetic stimulation of visual cortex in migraine
patients: a systematic review with meta-analysis. J Headache Pain. 2012;13(5):339-49
23. Brigo F, Storti M, Tezzon F, Manganotti P, Nardone R. Primary visual cortex excitability in migraine: a
systematic review with meta-analysis. Neurol Sci. 2013;34(6): 819-30
24. Brindley GS. Two new properties of foveal after-images and a photochemical hypothesis to explain
them. J Physiol. 1962;164:168-79
25. Brust JC, Behrens MM. "Release hallucinations" as the major symptom of posterior cerebral artery
occlusion: a report of 2 cases. Ann Neurol. 1977;2(5):432-6
26. Burgess N, Maguire EA, O'Keefe J. The human hippocampus and spatial and episodic memory.
Neuron. 2002;35(4):625-41
27. Burke W. The neural basis of Charles Bonnet hallucinations: a hypothesis. J Neurol Neurosurg
Psychiatry. 2002;73(5):535-41
28. Burr D. Motion smear. Nature. 1980;284(5752):164-5
29. Burr D. Vision: in the blink of an eye. Curr Biol. 2005;15(14), R554-6
30. Bynke H. Visual perseveration following temporal lobe surgery Case report. Neuro-Ophthalmology.
1985;4(1):47-53
31. Calligaris L, Vidoni A, Bruno I, Vidoni M, Barbi E. Efficacy of clonidine in hyperammonemia induced
hyperexcitability syndrome. Paediatr Anaesth. 2013;23(2):202-4
32. Cambron M, Anseeuw S, Paemeleire K, Crevits L. Saccade behavior in migraine patients. Cephalagia.
2011;31(9):1005-14
33. Chan D, Crutch SJ, Warrington EK. A disorder of colour perception associated with abnormal colour
after-images: a defect of the primary visual cortex. J Neurol Neurosurg Psychiatry. 2001;71(4):515-7
34. Chen WT, Lin YY, Fuh JL, Hamalainen MS, Ko YC, Wang SJ. Sustained visual cortex hyperexcitability in
migraine with persistent visual aura. Brain. 2011;134(8):2387-95
35. Cleland PG, Saunders M, Rosser R. An unusual case of visual perseveration. J Neurol Neurosurg
Psychiatry. 1981;44(3):262-3

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT21
36. Cosentino G, Fierro B, Vigneri S et al (in press). Cyclical changes of cortical excitability and
metaplasticity in migraine: evidence by a rTMS study. Pain.
37. Cummings JL, Syndulko K, Goldberg Z, Treiman DM. Palinopsia reconsidered. Neurology. 1982;
2(4):444-7
38. Curio M, Popovic J, Pignatti R, Sacco L. Case report - Palinopsia in a patient with a left pericalcarine
cavernous haemangioma. Swiss Archives of Neurology and Psychiatry. 2012;163(7): 255-6
39. Deubel H, Schneider WX. Saccade target selection and object recognition: evidence for a common
attentional mechanism. Vision Res. 1996;36(12): 1827-37
40. Dreier JP. The role of spreading depression, spreading depolarization and spreading ischemia in
neurological disease. Nat Med. 2011;17(4):439-47
41. Dubois J, Vanrullen R. Visual trails: do the doors of perception open periodically? PLoS Biol.
2011;9(5):e1001056
42. Engelsen BA, Tzoulis C, Karlsen B et al. POLG1 mutations cause a syndromic epilepsy with occipital
lobe predilection. Brain. 2008;131(3):818-28
43. Enns JT, Di Lollo V. What's new in visual masking? Trends Cogn Sci. 2000;4(9):345-52
44. Enroth-Cugell C, Robson JG. The contrast sensitivity of retinal ganglion cells of the cat. J Physiol.
1966;187(3):517-52
45. Eretto PA, Schoen FS, Krohel GB, Pechette D. Palinoptic visual allesthesia. Am J Ophthalmol.
1982;93(6):801-3
46. Evans RW. Reversible palinopsia and the Alice in Wonderland syndrome associated with topiramate
use in migraineurs. Headache. 2006;46(5):815-8.
47. Evans RW, Aurora SK. Migraine with persistent visual aura. Headache. 2012;52(3):494-501
48. Faber RA, Benzick JM. Nafazodone-induced palinopsia. J Clin Psychopharmacol. 2000;20(2):275-6
49. Fontenelle LF. Topiramate-induced palinopsia. Int J Neuropsychiatry Clin Neurosci. 2008;20(2):249-
50
50. Fournier AV, Zackon DH. Palinopsia: a case report and review of the literature. Can J Ophthalmol.
200;35(3):154-7
51. Friedman DI, Hu EH, Sadun AA. Neuro-ophthalmic complications of interleukin 2 therapy. Arch
Ophthalmol. 1991;109(12):1679-80
52. Furman M, Gur M. And yet it moves: perceptual illusions and neural mechanisms of pursuit
compensation during smooth pursuit eye movements. Neurosci Biobehav Rev. 2012; 36(1):143-51
53. Gaillard MC, Borruat FX. Persisting visual hallucinations and illusions in previously drug-addicted
patients. Klin Monbl Augenheilkd. 2003;220(3):176-8
54.Garcia-Perez MA, Peli E. Visual Contrast Processing is Largely Unaltered during Saccades. Front
Psychol. 2011;2:247
55. Gardner JL, Sun P, Waggoner RA et al.Contrast adaptation and representation in human early visual
cortex. Neuron. 2005;47(4):607-20
56. Gates TJ, Stagno SJ, Gulledge AD. Palinopsia posing as a psychotic depression. Br J Psychiatry.
1988;153:391-3
57. Gottlieb D. The unidirectionality of cerebral polyopia. J Clin Neuroophthalmol. 1992;12(4):257-62
58. Granziera C, Daducci A, Romascano D et al (in press). Structural abnormalities in the thalamus of
migraineurs with aura: A multiparametric study at 3 T. Hum Brain Mapp.
59. Halpern JH, Pope HG. Hallucinogen persisting perception disorder: what do we know after 50 years?
Drug Alcohol Depend. 2003;69(2):109-19
60. Hardman JM, Manoukian A. Pathology of head trauma. Neuroimaging Clin N Am. 2002;12(2):175-87
61. Hayashi R, Shimizu S, Watanabe R, Katsumata Y, Mimura M. Palinopsia and perilesional
hyperperfusion following subcortical hemorrhage. Acta Neurol Scand. 2002;105(3):228-31

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT22
62. Heron W, Doane BK, Scott TH. Visual disturbances after prolonged perceptual isolation. Can J
Psychol. 1956;10(1):13-8
63. Hoffman JA. LSD flashbacks. Arch Gen Psychiatry. 1984;41(6):631-2
64. Hori H, Terao T, Nakamura J. Visual perseveration: a new side effect of maprotiline. Acta Psychiatr
Scand. 2002;101(6): 476-7
65. Horton JC, Trobe JD. Akinetopsia from nefazodone toxicity. Am J Ophthalmol. 1999;128(4):530-1
66. Hughes MS, Lessell S. Trazodone-induced palinopsia. Arch Ophthalmol. 1990;108(3):399-400
67. Hundal KS, Chen S, Moore W, Tranos P, Joshi N. Dyskinetopsia during light adaptation associated
with nefazodone treatment. Eye (Lond). 2003;17(9):1040-2.
68. Ihde-Scholl T, Jefferson JW. Mitrazapine-associated palinopsia. J Clin Psychiatry. 2001 62(5):373
69. Jacobs L. Visual allesthesia. Neurology. 1980;30(10):1059-63
70. Jacobs L, Feldman M, Bender MB. The persistence of visual or auditory percepts as symptoms of
irritative lesions of the cerebrum of man. Z Neurol. 1972;203(3): 211-8
71. Jacome DE. Palinopsia and bitemporal visual extinction on fixation. Ann Ophthalmol. 1985;17(4),
251-2
72. Johnson SF, Loge RV. Palinopsia due to nonketotic hyperglycemia. West J Med. 1988;148(3):331-2
73. Jones MR, Waggoner R, Hoyt WF. Cerebral polyopia with extrastriate quadrantanopia: report of a
case with magnetic resonance documentation of V2/V3 cortical infarction. J Neuroophthalmol.
1999;19(1):1-6
74. Joseph AB. Cotard's syndrome in a patient with coexistent Capgras' syndrome, syndrome of
subjective doubles, and palinopsia. J Clin Psychiatr. 1986;47(12):605-6
75. Kataoka H, Ueno S. Cerebral polyopia and palinopsia in a patient with occipital lobe epilepsy.
Epilepsy Behav. 2009 14(4):684-6
76. Kawasaki A, Purvin V. Persistent palinopsia following ingestion of lysergic acid diethylamide (LSD).
Arch Ophthalmol. 1996;114(1):47-50
77. Khan AN, Sharma R, Khalid S et al. Palinopsia from a posteriorly placed glioma--an insight into its
possible causes. BMJ Case Rep. 2011;2011:bcr0820103273
78. Killer HE, Buettner UW. Mulitple Visual hallucinations and pseudohallucinations in on individual
patient: when the world is turning upside down and the television keeps falling to the ground while the
dwarfs are parading on the ceiling. Ophthalmologica. 2005;219(2):115-8
79. Kilpatrick ZP, Bard Ermentrout G. Hallucinogen persisting perception disorder in neuronal networks
with adaptation. J Comput Neurosci. 2012;32(1):25-53
80. Kim H, Chu K, Jung KH et al. Acquired encephalopathy associated with carnitine deficiency after
cefditoren pivoxil administration. Neurol Sci. 2012;33(6):1393-6
81. Kolmel HW. Visual illusions and hallucinations. Baillieres Clin Neurol. 1993;2(2):243-64
82. Kondziella D, Maetzel H. The sting in the tail: syncope and palinopsia. J Neurol. 2006;253(5):657-8
83. Kraus RP. Visual "trails" with nefazodone treatment. Am J Psychiatry. 1996;153(10):1365-6
84. Kupersmith MJ, Berenstein A, Nelson PK, ApSimon HT, Setton A. Visual symptoms with dural
arteriovenous malformations draining into occipital veins. Neurology. 1999;52(1):156-62
85. Lance JW. Simple formed hallucinations confined to the area of a specific visual field defect. Brain.
1976;99(4):719-34
86. Landis T, Cummings JL., Benson DF, Palmer, EP. Loss of topographic familiarity. An environmental
agnosia. Arch Neurol. 1986;43(2):132-6
87. Lang C. Palinoptic phenomena as an error mechanism in resolving alexia without agraphia. A case
report. Eur Neurol. 1985;24(4): 248-53
88. Lauterbach EC, Abdelhamid A, Annandale JB. Posthallucinogen-like visual illusions (palinopsia) with
risperidone in a patient without previous hallucinogen exposure: possible relation to serotonin 5HT2a
receptor blockade. Pharmacopsychiatry. 2002;33(1):38-41

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT23
89. Lazaro RP. Palinopsia: rare but ominous symptom of cerebral dysfunction. Neurosurgery.
1983;13(3):310-3
90. le Grand SM, Supornsilpchai W, Saengjaroentham C, Srikiatkhachorn A. Serotonin depletion leads to
cortical hyperexcitability and trigeminal nociceptive facilitation via the nitric oxide pathway. Headache.
2011;51(7) 1152-60
91. Lefebre C, Kolmel HW. Palinopsia as an epileptic phenomenon. Eur Neurol. 1989;29(6):323-7
92. Leo H, Melanie S, Martin R, Anil B, Martin G. Hallucinogen Persisting Perception Disorder (HPPD) and
flashback- are they identical?. J Alcoholism Drug Depend. 2013;1:4
93. Lerner AG, Gelkopf M, Skladman I et al. Clonazepam treatment of lysergic acid diethylamide-induced
hallucinogen persisting perception disorder with anxiety features. Int Clin Psychopharmacol.
2003;18(2):101-5
94. Levi L, Miller NR. Visual illusions associated with previous drug abuse. J Clin Neuroophthalmol.
1990;10(2):103-10
95. Liu B, Eisenach JC. Hyperexcitability of axotomized and neighboring unaxotomized sensory neurons
is reduced days after perineural clonidine at the site of injury. J Neurophysiol. 2005;94(5):3159-67
96. Liu GT, Schatz NJ, Galetta SL et al. Persistent positive visual phenomena in migraine. Neurology.
1995;45(4):664-8
97. Lopez JR, Adornato BT, Hoyt WF. 'Entomopia': a remarkable case of cerebral polyopia. Neurology.
1993;43(10):2145-6
98. Lunardi P, Tacconi L, Missori P, Salvati M. Palinopsia: unusual presenting symptom of a cerebral
abscess in a man with Kartagener's syndrome. Clin Neurol Neurosurg. 1991;93(4):337-9
99. Marinovic W, Arnold DH. An illusory distortion of moving form driven by motion deblurring. Vision
Res. 2013;88:47-54
100. Marneros A, Korner J. Chronic palinopsia in schizophrenia. Psychopathology. 1993;26(5-6): 236-9
101. McCrory PR, Berkovic SF. Concussive convulsions. Incidence in sport and treatment
recommendations. Sports Med. 1998;25(2): 131-6
102. McGuire PK, Cope H, Fahy TA. Diversity of psychopathology associated with use of 3,4-
methylenedioxymethamphetamine ('Ecstasy'). Br J Psychiatry. 1994;165(3):391-5
103. McLelland D, Baker P, Ahmed B, Bair W. Neuronal responses during and after the presentation of
static visual stimuli in macaque primary visual cortex. J Neurosci. 2010;30(38):12619-31
104. Meadows JC, Munro SS. Palinopsia. J Neurol Neurosurg Psychiatry. 1977;40(1): 5-8
105. Melcher D, Colby CL. Trans-saccadic perception. Trends Cogn Sci. 2008;12(12):466-73
106. Michel EM, Troost BT. Palinopsia: cerebral localization with computed tomography. Neurology.
1980;30(8):887-9
107. Mitsueda-Ono T, Ikeda A, Noguchi E et al. Epileptic polyopia with right temporal lobe epilepsy as
studied by FDG-PET and MRI: a case report. J Neurol Sci. 2006;247(1): 109-11
108. Mosberian P, Leung M, Hollander Y, Remick RA. Nefazodone-induced visual disturbances. Can J
Psychiatry. 1999;44(9):925-6
109. Moulton EA, Burstein R, Tully S et al. Interictal dysfunction of a brainstem descending modulatory
center in migraine patients. PLoS One. 2008;3(11):e3799
110. Mulleners WM, Chronicle EP, Palmer JE, Koehler PJ, Vredeveld JW. Visual cortex excitability in
migraine with and without aura. Headache. 2001;41(6):565-72
111. Muller T, Buttner T, Kuhn W, Heinz A, Przuntek H. Palinopsia as sensory epileptic phenomenon.
Acta Neurol Scand. 1995;91(6):433-6
112. Ogmen H. A theory of moving form perception: Synergy between masking, perceptual grouping,
and motion computation in retinotopic and non-retinotopic representations. Adv Cogn Psychol.
2007;3(1-2):67-84

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT24
113. Ogunyemi A, Adams D. Migraine-like symptoms triggered by occipital lobe seizures: response to
sumatriptan. Can J Neurol Sci. 1998;25(2):151-3
114. Olsen SR, Bortone DS, Adesnik H, Scanziani M. Gain control by layer six in cortical circuits of vision.
Nature. 2012;483(7387):47-52
115. Ossola M, Romani A, Tavazzi E, Pichiecchio A, Galimberti CA. Epileptic mechanisms in Charles
Bonnet syndrome. Epilepsy Behav. 2010;18(1-2):119-22
116. Patterson MC, Bunce IH, Eadie MJ. Cerebral abscess in leukaemia: an unusual presentation of a rare
complication. Clin Exp Neurol. 1985;21:257-62
117. Pomeranz HD, Lessell S. Palinopsia and polyopia in the absence of drugs or cerebral disease.
Neurology. 2000;54(4):855-9
118. Prescot A, Becerra L, Pendse G et al. Excitatory neurotransmitters in brain regions in interictal
migraine patients. Mol Pain. 2009;5:34
119. Purvin V, Bonnin J, Goodman J. Palinopsia as a presenting manifestation of Creutzfeldt-Jakob
disease. J Clin Neuroophthalmol. 1989;9(4):242-8
120. Purvin VA. Visual disturbance secondary to clomiphene citrate. Arch Ophthalmol. 1995;113(4):482-
4
121. Richter F, Mikulik O, Ebersberger A, Schaible HG. Noradrenergic agonists and antagonists influence
migration of cortical spreading depression in rat-a possible mechanism of migraine prophylaxis and
prevention of postischemic neuronal damage. J Cereb Blood Flow Metab. 2005;25(9):1225-35
122. Ritsema ME, Murphy MA. Palinopsia from posterior visual pathway lesions without visual field
defects. J Neuroophthalmol. 2007;27(2):115-7
123. Rossi S, Furlan R, De Chiara V et al. Interleukin-1beta causes synaptic hyperexcitability in multiple
sclerosis. Ann Neurol. 2012;71(1):76-83
124. Rubin EH, de Alwis DP, Pouliquen I et al. A phase I trial of a potent P-glycoprotein inhibitor,
Zosuquidar.3HCl trihydrochloride (LY335979), administered orally in combination with doxorubicin in
patients with advanced malignancies. Clin Cancer Res. 2002; 8(12):3710-7
125. Schankin CJ, Maniyar FH, Digre KB, Goadsby PJ (in press). 'Visual snow' - a disorder distinct from
persistent migraine aura. Brain.
126. Schoenen J. Neurophysiological features of the migrainous brain. Neurol Sci. 2006;27(Suppl 2): 77-
81
127. Schwartz K. Nefazodone and visual side effects. Am J Psychiatry. 1997;154(7):1038
128. Shams PN, Plant GT. Migraine-like visual aura due to focal cerebral lesions: case series and review.
Surv Ophthalmol. 2011;56(2):135-61
129. Shen RY, Andrade R. 5-Hydroxytryptamine2 receptor facilitates GABAergic neurotransmission in rat
hippocampus. J Pharmacol Exp Ther. 1998;285(2):805-12
130. Shepherd AJ. Increased visual after-effects following pattern adaptation in migraine: a lack of
intracortical excitation? Brain. 2001;124(11):2310-8
131. Shimojo S, Kamitani Y, Nishida S. Afterimage of perceptually filled-in surface. Science.
2001;293(5535):1677-80
132. Sierra-Hidalgo F, de Pablo-Fernandez E. Palinopsia induced by topiramate and zonisamide in a
patient with migraine. Clin Neuropharmacol. 2013;36(2):63-4
133. Silva JA, Tekell JL, Penny G, Bowden CL. Resolution of palinopsia with carbamazepine. J Clin
Psychiatry. 1997;58(1):30
134. Simpson JC, Goadsby PJ, Prabhakar P. Positive persistent visual symptoms (visual snow) presenting
as a migraine variant in a 12-year-old girl. Pediatr Neurol. 2013;49(5):361-3
135. Smith PE, Shah P, Sharpe J, Todd A, Goringe AP. Palinopsia. Lancet. 2003;361(9363):1098
136. Somjen GG. Mechanisms of spreading depression and hypoxic spreading depression-like
depolarization. Physiol Rev. 2001;81(3):1065-96

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT25
137. Stagno SJ, Gates TJ. Palinopsia: a review of the literature. Behav Neurol. 1991;4(2):67-74
138. Stankewitz A, May A. Cortical excitability and migraine. Cephalalgia. 2007;27(12):1454-6
139. Sun YT, Lin CC. Sequential appearance and disappearance of hemianopia, palinopsia and
metamorphopsia: a case report and literature review. Acta Neurol Taiwan. 2004;13(2):77-83
140. Sunness JS. Persistent afterimages (palinopsia) and photophobia in a patient with a history of LSD
use. Retina. 2004;24(5):805
141. Swash M. Visual perseveration in temporal lobe epilepsy. J Neurol Nuerosurg Psychiatry. 1979;
42(6):569-71
142. The International Classification of Headache Disorders, 3rd edition (beta version). Cephalagia.
2013;33(9)629-808
143. Thiele A, Henning P, Kubischik M, Hoffmann KP. Neural mechanisms of saccadic suppression.
Science. 2002;295(5564):2460-2
144. Tsai PH, Mendez MF. Akinetopsia in the posterior cortical variant of Alzheimer disease. Neurology.
2009;73(9):731-2
145. Van der Stigchel S, Nijboer TC, Bergsma DP, Barton JJ, Paffen CL. Measuring palinopsia:
characteristics of a persevering visual sensation from cerebral pathology. J Neurol Sci. 2012;316(1-
2):184-8
146. Vaphiades, MS, Celesia GG, Brigell MG. Positive spontaneous visual phenomena limited to the
hemianopic field in lesions of central visual pathways. Neurology. 1996;47(2):408-17
147. Virsu V. Retinal mechanisms of visual adaptation and afterimages. Med Biol. 1978;56(2):84-96
148. Wang YF, Fuh JL, Chen WT, Wang SJ. The visual aura rating scale as an outcome predictor for
persistent visual aura without infarction. Cephalalgia. 2008;28(12):1298-1304
149. Werring DJ, Marsden CD. Visual hallucinations and palinopsia due to an occipital lobe tuberculoma.
J Neurol Neurosurg Psychiatry. 1999;66(5):684
150. Wurtz RH. Neuronal mechanisms of visual stability. Vision Res. 2008;48(20):2070-89
151. Wilkins AJ, Patel R, Adjamian P, Evans BJ. Tinted spectacles and visually sensitive migraine.
Cephalagia. 2002;22(9):711-9
152. Young WB, Heros DO, Ehrenberg, B. L., Hedges TR. Metamorphopsia and palinopsia. Association
with periodic lateralized epileptiform discharges in a patient with malignant astrocytoma. Arch Neurol.
1989;46(7):820-2
153. Zakaria A, Lalani I, Belorgey L, Jay Foreman P. Focal occipital seizures with cerebral polyopia.
Epileptic Disord. 2006;8(4):295-7
154. Ziaei M, Elgohary MA, Bremner FD. Palinopsia as the initial manifestation of non-hodgkin's
lymphoma. Int Ophthalmol. 2013;33(5):553-6
Other Cited Material
A. Metz RJ, Pieri V, Diederich NJ. Object-specific and “side inversed” palinopsia limited to the
hemianopic field in occipital infarction. Poster session presented at: 16th
Meeting of the European
Neurological Society; 2006 May 27-31; Luxembourg, LUX
B. Abdulfattah Q, Swanson JW. Migraine headache and palinopsia. Poster session presented at: 47th
Annual Scientific Meeting American Headache Society; 2005 Jun 23-5; Philadelphia, PA

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Figure 1- Examples of palinopsia symptom types. (A) Formed image perseveration: an examiner’s hand
persists in the visual field. (B) Categorical incorporation: a spire is incorporated on to other buildings.
(C) Visual trailing: a ball in motion leaves images in its wake. Photographs courtesy of Kelli X. Gross, MD.
Figure 2- Flowchart contrasting the two types of palinopsia. Hallucinatory palinopsia is caused by a
dysfunction in visual memory and illusory palinopsia is caused by a dysfunction in visual perception.
HPPD = hallucinogen persisting perception disorder.
Appendix- Details the 129 cases of palinopsia we found in the literature. * = Cases of seizure or post-
geniculate cortical lesions not causing hallucinatory palinopsia; ** = Cases of prescription drug, illicit
drug, idiopathic, migraine, or head trauma not causing illusory palinopsia; X = Not included in numerical
analysis due to inadequate symptom description or describing non-palinoptic symptoms.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Dysfunction of Visual Memory Dysfunction of Visual Perception
EtiologyPost-geniculate cortical lesions
Various seizure etiologies, Seizures of
unknown etiology
Patho-physiology
Cortical deafferentation
Focal cortical
irritation
Epileptic discharges
Focal activation of post-geniculate neurons which represent images or
scenes already encoded in visual memory
Type of Palinopsia
Formed image perseveration
Categorical incorporation
Scene perseveration
Patterned visual spread
Symptom Features
High resolution, formed, episodic, not affected by environmental conditions,
lasts more than a few seconds
Associated Symptoms
Complex visual hallucinations, homonymous field deficits
MigraineRx
drugs
Diffuse, persistent neuronal
perceptual abnormalities
Diffuse, persistent neuronal hyperexcitability throughout the visual pathway causing perceptual abnormalities
Diffuse cortical
irritation
Diffuse neurotransmitter or receptor alterations,
GABA/5HT2a?
Cortical spreading depression
HPPDHead
trauma
Focal, transient peak in cortical
activity or excitability
Visual trailing
Light streaking
Prolonged indistinct
afterimages
Variant single image perseveration
Low resolution, persistent, continuous or predictable
Visual snow, halos, oscillopsia, akinetopsia,
entoptic phenomena
Simple visual hallucinations, dysmetropsia, cerebral polyopia, photophobia,
metamorphopsia
Affected by light and motion
Transient, paroxysmal
?
Hallucinatory Palinopsia Illusory palinopsia

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Author/
year Primary Etiology
Palinopsia
Mechanism Diagnostic
Visual Field
Defect Type of Palinopsia Description of Palinopsia Other Visual Sx
Simpson,
2013134
Migraine
cortical spreading
depression
Sx occurred directly after
severe migraine
prolonged
indistinct
afterimages, light
streaking, visual
trails
Bright lights can leave afterimages that persist for
several hours, visual trails. Unformed single color
afterimages when moveing field of vision. Topiramate
resolved migraine sx but did not affect visual sx
phosphenes,
photopsia, visual snow,
photophobia
Sierra-
Hidalgo,
2013132
Topiramate,
zonisamide
diffuse neurotrans-
mitter/receptor Δs
Sx started with drug and
resolved with drug d/c visual trails
Stroboscopic vision for an hour only in AM, objects
moved like agents avoiding bullets in the Matrix.
Increasing frequency so topiramte was d/c. Mild sx
from zonisamide.
Not associated with
migranie or aura
Ziaei,
2013154
Central occiput NHL
irritative hyper-
excitability, edema
CT/FLAIR: signs of
compression, resolved
after chemo
enlarged blind
spot, arcuate
scotoma
categorical
incorporation
Categorical incorporation of church spiral over
buildings, complete resolution after chemotherapy.
Palinopsia was presenting symptom of NHL.
Anabrasan,
20138 Multiple sclerosis
possible MS
demylineation
L tempero-occipital
enhancement; oligoclonal
bands on CSF
variant image
perseveration
Immediate, translucent or black afterimages lasting
seconds to minutes. Improved spontaneously after a
few weeks. Visual sx were MS presentation metamorphopsia
Leo, 201392
HPPD
diffuse neurotrans-
mitter/receptor Δs diagnosis of exclusion
akinetopic visual
trails
Moving objects like "stroboscopic photography"; non-
descript afterimages of objects he had seen previously photopsias
Van der
Stigchel,
2012145
R V1/ thalamic
infarction deafferentation MRI displayed infarctions
L homonymous
field deficit
formed image
perseveration;
light streaks
Formed image perseveration (words) would move to
defective quandrant. Light streaking in defective
quadrant. Closing eyes removed afterimages
Curio,
201238
L occipital
hemangioma
epileptic discharge
irritative hyper-
excitability,
deafferentation
MRI: showed lesion,
resolved with AED
R transient
homonymous VF
deficits
formed image
perseveration
After a cortical hemorrhage, immediate palinopsia for a
few minutes with objects and faces. After 1 week of sx,
started on keppra despite negative EEG and sx
disappeared
Kim, 201280
Carnitine def., 2°
seizure epileptic discharge
Decreased plasma
carnitine, R occipital lesion
formed image
perseveration
After a seizure, noted "persistence of afterimages"
which were vivid and indistinguishable from the real
stimulus Left hemineglect
Evans,
201247
Migraine
cortical spreading
depression
MRI/A unremarkable;
clinical migraine sx which
improved with tx
light streaking,
unknown
Long history of migraines and "constant afterimages" or
tracers, more noticeable in light. Migraine and
palinopsia improved on topiramate
visual snow, blue field
entopic phenomena
Khan,
201177
R parieto-tempero-
occipital GBM
deafferentation,
irritative
hyperexcitability
MRI displayed GBM;
palinopsia resolved after
neoplasm debulking
L homonymous
quadrantanopia
large blind spot
formed image
perseveration
Palinopsia presenting sign of GBM; Delayed palinopsia
of wife or TV in left visual field persisting for about
15minutes. Palinopsia resolved after neoplasm
debulking
Abert,
20101 HPPD
diffuse neurotrans-
mitter/receptor Δs diagnosis of exclusion
akinetopic visual
trails
Described 2 episodes in past 6 months of a "reel of film
in slow motion", perceiving motion as "frame by frame"
Head trauma
diffuse cortical
hyperexcitability
Sx occurred directly after
head trauma
light streaking,
prolonged
indistinct
afterimages
Multiple copies of brightly colored opaque isochromatic
"streamers" near moving bright lights
Trazadone
diffuse neurotrans-
mitter/receptor Δs
Sx disappeared after
trazadone d/c
akinetopic and
blurred visual
trails
6 mo after starting trazadone, c/o stroboscopic vision
and "visual trails" lasting for ~1/2 hr each morning.
Also occurrs during exposure to bright light
HPPD/trazodone
diffuse neurotrans-
mitter/receptor Δs
Sx started over 40 years
ago after LSD use, recent
trazodone use
prolonged
indistinct
afterimages,
akinetopic trails
Motion causes isochromatic, translucent, isointense
distinct trailing images in all fields of gaze. Constant for
40 years after LSD, recently started trazadone.
Metamorphopsia,
halos

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Ossola,
2010115
Seizure of unknown
etiology epileptic discharge
EEG: PLEDS over R parietal
region; Sx resolved with
phenytoin/lorazepam
left
homonymous
field deficit
formed image and
scene
perseveration
Delayed palinopic images and scenes from 30minutes
before, lasting about 30seconds, more often in
hemianopic field. Occurred during end of ictal event CVH
Kataoka,
200975
*
Seizure of unknown
etiology epileptic discharge
EEG: R occipital seizure
discharge; improved with
treatment
non-akinetopic,
discrete visual
trails
Cerebral polyopia w/ unmoving objects, motion would
cause trails and shapes to Δ . Valproate/ gabapentin
resolved polyopia and improved palinopsia
cerebral
polyopia/entomopia
Tsai, 2009144
Posterior corticl
atrophy diffuse atrophy
SPECT: posterior parieto-
occipital hypometabolism
akinetopsia visual
trails
Leftward moving objects were percieved as successive
images side by side. No palinopsia on eye movement
Posterior corticl
atrophy diffuse atrophy MRI: parietal atrophy
akinetopsia visual
trails
Multiple images only when objects moved leftward, not
present on eye movement.
Fontenelle,
200849
Topiramate
diffuse neurotrans-
mitter/receptor Δs
Sx started after topiramate
dose increase
akinetopic visual
trails
Pt c/o stroboscopic vision, images lasted a few sec and
episodes occurred several times a day.
Engelson,
200842
X
POLG1 mutation, 2°
seizure epileptic discharge
POLG1 mutation, R
occipital focus, seizures,
status epilepticus no description No details of the palinopsia were given dysmetropsia
Ritsema,
2007122
L occipital AVM; 2°
seizure
epileptic discharge
irriration
hyperexcitability
Sx after AVM hemorrhage,
during a seizure aura
formed image
perseveration
Immediate formed image perseveration of TV, etc in
defective visual field photopsia
*
L anterior optic
radiation infarction unknown
2 small hyperintensities
within periatrial white
matter
prolonged
indistinct
afterimages
Prolonged indistinct light afterimages, esp when
looking at a white wall. Would also see outline of bright
images such as a lightpost, images would last ~60sec
Kondziella,
200682
R temporo-occipital
GBM unknown
CT showed GBM 5 months
after palinopsia
formed image
perseveration
Delayed palinopsia- wasp in central vision for 2 hrs, CT
originally negative, palinopsia GBM presentation
Mitsuedo-
Ono,
2006107
Seizure of unknown
etiology epileptic discharge
Dx by EEG and clinical
seizure signs; resolved with
AED
scene
perseveration
Seizure episodes lasting about 10seconds occuring
multiple times per day; pt would see a replay of a scene
he had just viewed CVH, cerebral polyopia
Evans,
200646
Topiramate, trazadone
diffuse neurotrans-
mitter/receptor Δs
sx after inc topiramate,
resolved with dose dec visual trails
Multiple afterimages when looking at a moving hand or
person, episodes each morning for about an hr
Topiramate
diffuse neurotrans-
mitter/receptor Δs
sx occurred with dose inc,
resolved with dose dec
visual trails, light
streaking
Shadow images of moving objects or lights, trouble
with night driving. Sx only at night or in dark
Metz, 2006A R occipital infarction
deafferentation,
irritation
hyperactivity
MRI: recent infarction,
clinical sx of CVA
left
homonymous
field deficit
formed image
perseveration
3 days post infarction, patient noted duplicated objects
in her hemianopic field from objects seen in her intact
field. Went away by day 5 SVH, visual allesthesia
Killer,
200578
X
Peduncular
hallucinosis
neurotransmitter
alterations
CT: subcortical
encephalopathy not palinopsia described repetitive visual hallucinations CVH
Abdulfattah,
2005B Migraine
cortical spreading
depression clinical sx of migraine
variant formed
image
perseveration
After a severe migraine, c/o persistence of images in
visual fields for a couple seconds, worse when moving.
Persisted for a few months and slowly resolved.
Sunness,
2004140
HPPD
diffuse neurotrans-
mitter/receptor Δs diagnosis of exclusion
prolonged
indistinct
afterimages
2yr history of prominent fluorescent green afterimages
after viewing bright lights, 1+ year since last LSD use photophobia
Sun, 2004139
TIA
deafferentation,
irritative
hyperexcitability
SPECT: hypoperfusion in R
occipitotemporal region, sx
appeared after TIA
transient L
homonymous
field deficit
scene
perseveration
Immediate palinopsia of waving fingers lasting 3min, in
defective field. This resolved after 1 day and patient
then c/o metamorphopsia for 12 hours

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Smith,
2003135
B-cell NHL, secondary
seizure
epileptic discharge,
irritative
hyperexcitability
palinopsia resolved after
adding carbamazepine to
valproate and chemo
scene
perseveration,
categorical
incorporation
Categorical incorporation with body parts lasting a few
minutes. Repeated scene of a nurse walking. Sx
resolved after adding carbamazepine to valproate.
Symptoms did not return after chemotherapy
cerebral polyopia,
oscillopsia
Gaillard,
200353
HPPD
diffuse neurotrans-
mitter/receptor Δs diagnosis of exclusion
momentary
afterimages
Persistence of an object for several seconds after
shifting gaze onto a white wall
visual snow, blue field
entoptic
HPPD
diffuse neurotrans-
mitter/receptor Δs diagnosis of exclusion dyskinetopsia
Complained of stroboscopic vision (dyskinetopsia) and
difficulty in depth perception decreased stereopsis
Hundal,
200367
Nefazodone
diffuse neurotrans-
mitter/receptor Δs
Sx started after dose
increase
visual trails, light
streaks
Moving objects leave short-lived trails, during fixation,
light adaptation, resolves after 20-30min in bright
conditions
Hayashi,
200261
R parietal hematoma
deafferentation,
irritative hyper-
excitability
Sx occurred after CVA, CT:
subcortical hemorrhage
left
homonymous
field deficit
formed image
perseveration;
scene
perseveratio
Immediate and delayed palinopsia 2-5 days after
hemorrhagic CVA, images (fingers) and scenes
perseverated mostly in the left VF for ~15min. Also
heard examiners voice photopsia
Rubin,
2002124
X Zosuquidar zosuquidar tox no description No details of the palinopsia were given
Idhe-Scholl,
200168
Mirtazepine
diffuse neurotrans-
mitter/receptor Δs
sx occurred with dose inc,
resolved with dose dec visual trails
Saw "visual trails" from moving objects. Less intense
color, slightly blurred, faded after 30sec-1minute.
Worse in lateral visual fields.
Chan,
200133
Posterior corticl
atrophy Diffuse atrophy
MRI: atrophy restricted to
the occipital pole
constricted
peripheral field
patterned visual
spread
After seeing intense color, subsequent objects would
immediately appear in the opposite color for 30-60 sec
Hori, 200064
**
Maprotiline, possible
2° seizure unknown
Maprotiline dec seizure
threshold, pt on other rx
that inc. maprotiline lvl
formed image
persev., patterned
visual spread
Would see perseverated words, pattern on ceiling
spread to arms. Disappeared 1 week after maprotline
d/c
Fournier,
200050
Head trauma
possible diffuse
cortical
hyperexcitability
visal deficits occurred 7+
months after head
trauma/LoC
left
homonymous
field deficit
unidirectional
akinetopic visual
trails
After focusing on an object, would see afterimages
when moving head left like "a strobe light", images
looked real and lasted about 15sec occansional micropsia
Faber,
200048
Nefazodone
diffuse neurotrans-
mitter/receptor Δs
sx started with trazodone,
resolved with dose dec visual trails blur
Pt saw "visual trails of moving objects", same color and
size as original, occured at night or in dim light
Lauterbach,
200088
Trazadone/risperidone
diffuse neurotrans-
mitter/receptor Δs
Sx after dose incr of both
rx, resolved after drug d/c
visual trails and
light streaking
Eminating light from objects and "streamers" would
follow moving objects. Would persist after closing eyes halos around objects
Pomeranz,
2000117
Possible TIA
deafferentation,
irritative
hyperexcitability
patient had stroke 2
months later and a h/o
TIAs
hand motion
only
formed image,
scene
perseveration
2 days after grid laser treatment for diabetic macular
edema, pt saw repeated scenes and images, saw a
woman superimposed on her visual field.
LHON deafferentation
MRI negative; LHON
diagnostic test
nonspecific
vision loss
formed image
perseveration
Shortly after vision loss, pt had immediate palinopsia,
worse when tired or moving. A pink car remained for
30min
Multiple sclerosis
optic neuritis
demylineation
unremarkable
neuroimaging; started after
optic neuritis
variant image
perseveration
Pt saw black and white outlines in same place in VF as
original object, outline of foot. Only with unaffected
eye, improved over time
Idiopathic unknown
unremarkable
neuroimaging
visual trails,
prolonged
indistinct
afterimages
After viewing a bright stimuli, would see isochromatic
afterimages for a few seconds. Motion would cause
trailing
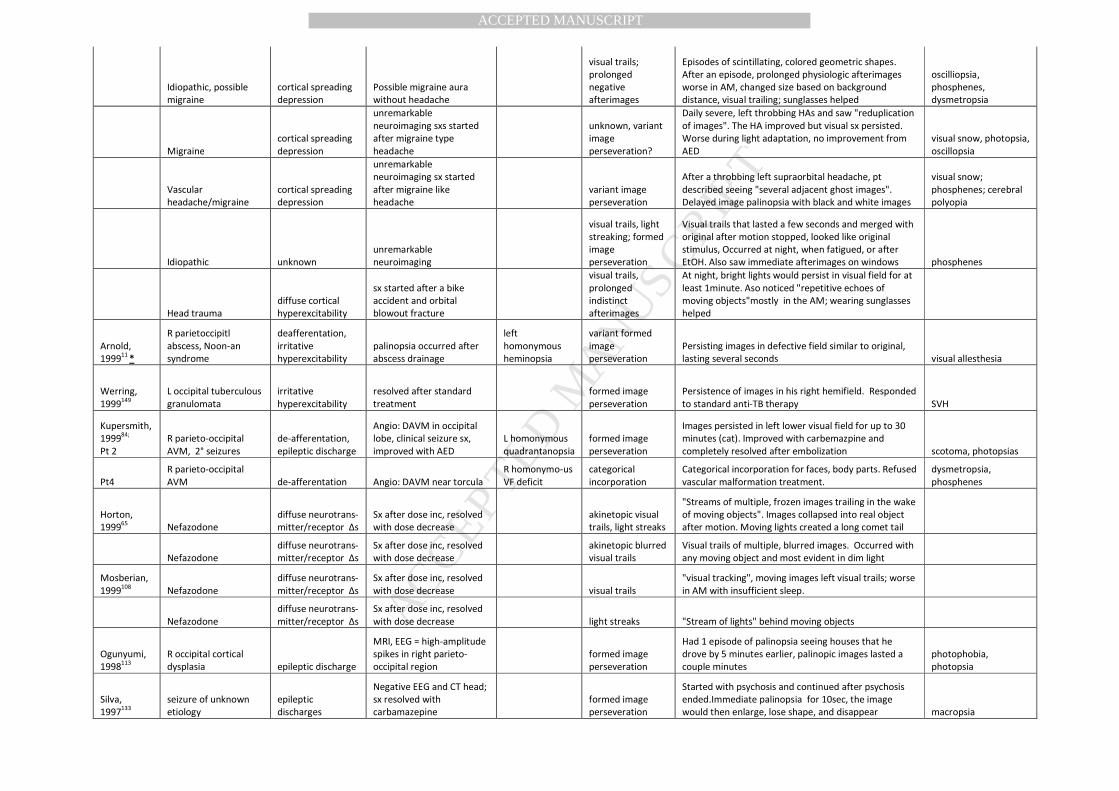
MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Idiopathic, possible
migraine
cortical spreading
depression
Possible migraine aura
without headache
visual trails;
prolonged
negative
afterimages
Episodes of scintillating, colored geometric shapes.
After an episode, prolonged physiologic afterimages
worse in AM, changed size based on background
distance, visual trailing; sunglasses helped
oscilliopsia,
phosphenes,
dysmetropsia
Migraine
cortical spreading
depression
unremarkable
neuroimaging sxs started
after migraine type
headache
unknown, variant
image
perseveration?
Daily severe, left throbbing HAs and saw "reduplication
of images". The HA improved but visual sx persisted.
Worse during light adaptation, no improvement from
AED
visual snow, photopsia,
oscillopsia
Vascular
headache/migraine
cortical spreading
depression
unremarkable
neuroimaging sx started
after migraine like
headache
variant image
perseveration
After a throbbing left supraorbital headache, pt
described seeing "several adjacent ghost images".
Delayed image palinopsia with black and white images
visual snow;
phosphenes; cerebral
polyopia
Idiopathic unknown
unremarkable
neuroimaging
visual trails, light
streaking; formed
image
perseveration
Visual trails that lasted a few seconds and merged with
original after motion stopped, looked like original
stimulus, Occurred at night, when fatigued, or after
EtOH. Also saw immediate afterimages on windows phosphenes
Head trauma
diffuse cortical
hyperexcitability
sx started after a bike
accident and orbital
blowout fracture
visual trails,
prolonged
indistinct
afterimages
At night, bright lights would persist in visual field for at
least 1minute. Aso noticed "repetitive echoes of
moving objects"mostly in the AM; wearing sunglasses
helped
Arnold,
199911
*
R parietoccipitl
abscess, Noon-an
syndrome
deafferentation,
irritative
hyperexcitability
palinopsia occurred after
abscess drainage
left
homonymous
heminopsia
variant formed
image
perseveration
Persisting images in defective field similar to original,
lasting several seconds visual allesthesia
Werring,
1999149
L occipital tuberculous
granulomata
irritative
hyperexcitability
resolved after standard
treatment
formed image
perseveration
Persistence of images in his right hemifield. Responded
to standard anti-TB therapy SVH
Kupersmith,
199984;
Pt 2
R parieto-occipital
AVM, 2° seizures
de-afferentation,
epileptic discharge
Angio: DAVM in occipital
lobe, clinical seizure sx,
improved with AED
L homonymous
quadrantanopsia
formed image
perseveration
Images persisted in left lower visual field for up to 30
minutes (cat). Improved with carbemazpine and
completely resolved after embolization scotoma, photopsias
Pt4
R parieto-occipital
AVM de-afferentation Angio: DAVM near torcula
R homonymo-us
VF deficit
categorical
incorporation
Categorical incorporation for faces, body parts. Refused
vascular malformation treatment.
dysmetropsia,
phosphenes
Horton,
199965
Nefazodone
diffuse neurotrans-
mitter/receptor Δs
Sx after dose inc, resolved
with dose decrease
akinetopic visual
trails, light streaks
"Streams of multiple, frozen images trailing in the wake
of moving objects". Images collapsed into real object
after motion. Moving lights created a long comet tail
Nefazodone
diffuse neurotrans-
mitter/receptor Δs
Sx after dose inc, resolved
with dose decrease
akinetopic blurred
visual trails
Visual trails of multiple, blurred images. Occurred with
any moving object and most evident in dim light
Mosberian,
1999108
Nefazodone
diffuse neurotrans-
mitter/receptor Δs
Sx after dose inc, resolved
with dose decrease visual trails
"visual tracking", moving images left visual trails; worse
in AM with insufficient sleep.
Nefazodone
diffuse neurotrans-
mitter/receptor Δs
Sx after dose inc, resolved
with dose decrease light streaks "Stream of lights" behind moving objects
Ogunyumi,
1998113
R occipital cortical
dysplasia epileptic discharge
MRI, EEG = high-amplitude
spikes in right parieto-
occipital region
formed image
perseveration
Had 1 episode of palinopsia seeing houses that he
drove by 5 minutes earlier, palinopic images lasted a
couple minutes
photophobia,
photopsia
Silva,
1997133
seizure of unknown
etiology
epileptic
discharges
Negative EEG and CT head;
sx resolved with
carbamazepine
formed image
perseveration
Started with psychosis and continued after psychosis
ended.Immediate palinopsia for 10sec, the image
would then enlarge, lose shape, and disappear macropsia

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Schwartz,
1997127
Nefazodone
diffuse neurotrans-
mitter/receptor Δs
Sx started after dose
increase visual trails
Patient noticed ghost shadows on moving objects for
~30min after waking, went away after 6 weeks
Vaphadies,
1996146
R occipital infarction deafferentation
MRI: right occipital infarct,
EEG negative
L homonymous
deficit
formed image
perseveration
Saw fragments of objects in defective field that were
recently seen in intact field, lasted 3 days after CVA
X R occipital infarction deafferentation MRI
L homonymous
deficit no description No details of the palinopsia were given phosphenes, CVH
Kawasaki,
199676
HPPD
diffuse neurotrans-
mitter/receptor Δs
Diagnosis of exclusion,
occurred after wisdom
tooth extraction
prolonged
physiological
afterimages
4 mo after LSD use, received fentanyl, methohexital,
midazolam, dexamethasone, and lidocaine for a
surgery. Prolonged physiologic afterimages, more vivid
in bright lights. No resolution in 3+ yrs
HPPD
diffuse neurotrans-
mitter/receptor Δs diagnosis of exclusion
prolonged
physiological
afterimages
2 mo after LSD ingestion, negative afterimages more
prominent with high contrast, lasted up to 1 min.
Precipitated by hot baths photopsia, phosphenes
HPPD
diffuse neurotrans-
mitter/receptor Δs diagnosis of exclusion visual trails
Pt noted a "series of images that trailed behind the
moving object for a few seconds". Occurred with any
object in motion, constant, unchanged after 6mo
Kraus,
199683
Nefazodone
diffuse neurotrans-
mitter/receptor Δs
Sx after dose inc, resolved
with dose decrease
visual trails, light
streaks
Visual trails from moving objects lasting ~1sec, more
apparent at night, occur when turning her head
Abraham,
19965 HPPD/risperidone
diffuse neurotrans-
mitter/receptor Δs
sx in close proximity to
risperidone dose increase visual trails
Pt used LSD ~35 times, had HPPD visual trailing. Panic
attacks and worse flashbacks after risperidone
HPPD/risperidone
diffuse neurotrans-
mitter/receptor Δs
started in close proximity
as risperidone initiation visual trails
Continuous visual symptoms of non-descript
"afterimages", visual trails, and halos. Worsened after
starting risperidone which also caused a panic attack halos
HPPD/risperidone
diffuse neurotrans-
mitter/receptor Δs
started in close proximity
as risperidone initiation
visual trails,
prolonged
indistinct
afterimages
A week after his last LSD trip, pt experienced visual
trails and intensification/prolongation of light. Many
years later, respiradone caused flashbacks/panic
attacks intensification of light
Muller,
1995111
R occipital infarction,
2° seizure
epileptic discharge,
deafferentation
EEG during palinopsia: Δ
focus with sharp waves in R
temporal area; resolved
with phenytoin
left
homonymous
field deficit
formed image
perseveration
Immediate and delayed palinopsia of faces and other
scenic after-images. No other signs of seizure.
R occipitotemp-oral
mets, 2° seizure
epileptic discharge,
deafferentation
EEG= R sharp waves;
resolved with AED
left
homonymous
field deficit
formed image
perseveration
Pt saw images of delayed palinopic images of people
from minutes before.
R occipitotemp-oral
mets, 2° seizure
epileptic discharge,
deafferentation
EEG: R occipitotemporal
delta focus, paroxysmal
bilateral theta/delta
waves; resolved with AED
left
homonymous
field deficit
scene
perseveration
For weeks, patient reported complete visual scenes
from seconds or minutes before such as a soccer player
throwing a ball in his hemianopic field.
Purvin,
1995120
Clomiphene
diffuse neurotrans-
mitter/receptor Δs
Palinopsia occurred after
clomiphene dose increase visual trails
Noticed prolongation of afterimages of moving targets.
Worse in high-contrast images in bright light. Visual
disturbance never abated
shimmering,
oscillopsia,
photophobia
Clomiphene
diffuse neurotrans-
mitter/receptor Δs
after clomiphene dose
increase visual trails?
4 mo after starting clomiphene, "abnormal
prolongation of afterimages" for moving objects; worse
after entering bright room, not resolved 4 years later
shimmering,oscillopsia,
photophobia

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Clomiphene
diffuse neurotrans-
mitter/receptor Δs
Palinopsia occurred after
clomiphene dose increase visual trails
Pt described stroboscopic vision. Symptoms worsened
during light adaptation and during menses, persisted
for 7 years after d/c clomiphene
blurred vision,
photophobia, visual
snow
Liu, 199596
X
Head trauma,
migraine
diffuse cortical
hyperexcitability
clinical diagnosis, SPECT:
biparietal hypoperfusion no description
After a MVA, developed a persistence of afterimages.
Resolved with nortryptaline and carbamazepine visual snow
McGuire,
1994102
X MDMA
diffuse neurotrans-
mitter/receptor Δs diagnosis of exclusion no description No details of the palinopsia were given
Marnenos,
1993100
Schizophrenia unknown
started with schizophrenia
onset, worsened before
psychosis
formed image
perseveration;
visual trails
Immediate and delayed afterimages, same size, shape,
and color. Visual trails with eye movement. Palinopsia
worsening when tired, stressed, or before psychotic
episode; lasted for 5+ years
CVH, photopsia,
teleopsia, oscillopsia
Gottlieb,
199257
*
Infarctions post-CABG,
largest R parietal deafferentation
CT: multiple infarctions;
normal EEG
left
homonymous
field deficit
unidirectional
visual trails eye
scanning
Palinopsia induced by leftward horizontal scanning of
an objects, lasting 5-10 seconds. Increasing the contrast
made it worse; misdiagnosed as polyopia micropsia
Lunardi,
199198
L occipital abscess,
Kartagener's
syndrome
deafferentation,
irritative
hyperactivity
edema
CT: left occipital abscess
with perilesional edema;
resolved with drainage
R homonymous
quadrantanopsia
categorical
incorporation
1 episode of categorical incorporation with faces and
clothes lasting 10mintes, went away after abscess
drainage
Friedman,
199151
X IL-2 unknown
unremarkable
neuroimaging (CT) no description
"persistent image overlapping the true image lasting
several minutes", began 11 days after IL-2 scintillating scotoma
Levi, 199094
pt2 HPPD
diffuse neurotrans-
mitter/receptor Δs diagnosis of exclusion
akinetopsia visual
trails
Moving objects a series of still pictures, episodes last
~1hr, multiple times/day. Precipitated by stress or by
describing phenomenon to others, lasted 1+ years decreased stereopsis
pt4 HPPD
diffuse neurotrans-
mitter/receptor Δs diagnosis of exclusion
light streaking;
formed image
perseveration
2 yrs after last drug use, moving lights in dark appeared
as streaks; After looking at an object, a life-like image
stayed for secs to mins, even after closing eyes
pt6 HPPD
diffuse neurotrans-
mitter/receptor Δs diagnosis of exclusion
light streaking,
visual trails
During a stressful period, noticed streaking of moving
objects, did not occur if tracking object with eyes.
Worse with bright objects in dark settings.
Hughes,
199066
** Trazadone
diffuse neurotrans-
mitter/receptor Δs
Sx after dose inc, resolved
with dose decrease
formed image
perseveration
Immediate palinopsia, worse in temporal fields, lasting
up to 15min. She or the object (door, crib) had to be
moving. Only in the morning, frequent, intense
Trazadone
diffuse neurotrans-
mitter/receptor Δs
MRI: 1.5cm frontal lobe
meningioma; palinopsia
resolved with rx d/c
akinetopic visual
trails
Saw "strobelike afterimages" of objects in motion.
Worse in peripheral visual fields and with insufficient
sleep.
Trazadone
diffuse neurotrans-
mitter/receptor Δs
Sx after dose inc, resolved
with dose decrease
akinetopic visual
trails
Strobe images in AM. After fixating on a door and
moving his gaze, he would see multiple images of the
door "march" across the room. Episodes lasted 15mins
Purvin,
1989119
Creutzfeld-Jacob
disease
deafferentation,
possible epileptic
discharge
Unremarkable
neuroimaging; EEG:
marked slowing, periodic
sharp wave discharges;
L and R
homonymous VF
deficits
formed image
perseveration;
categorical
incorporation
Immediate palinopsia with mustard label, palinopsia
would last for a few minutes up to an hour, anywhere
in his visual field. Categorical incorporation with
houses. Presenting symptom of CJD photopsia

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Young,
1989152
R parietal astrocytoma
epileptic
discharges
EEG: PLEDs in R parietal
region, resolved with AED
formed image
perseveration;
categorical
incorporation
Immediate palinopsia in her left field. Categorical
incorporation with beards, eyes. Palinopsia was
presenting symptom of neoplasm
CVH, cerebral
polyopia,
dyschromotopsia,
dysmetropsia,
metamorphosia
Lefebre,
198991
R parieto-occipital
astrocytoma
epileptic discharge,
deafferentation
EEG: pt noticed palinopsia
1s after first sharp wave in
R temperoparietal region
upper left
quadrantanopsia
formed image
perseveration;
categorical
incorporation
6 mo after astrocytoma debulking, immediate and
delayed palinopsia in VF deficit. Images lasted secs to
hrs, sometimes translucent, stayed with eye closure.
Categorical incorporation of taxi sign onto other cars.
Johnson,
198872
Hyperglycemia, 2°
seizure
epileptic discharge;
deafferentation
EEG: L occipital focus,
seizure sx; resolved after
glucose normalized
right
homonymous
field deficit
formed image
perseveration
Had spells that included seizure sx, SVH, and immediate
palinopsia with formed images SVH, visual allesthesia
Gates,
198856
X Depression
neurotransmitter
alterations
CT: large left occipital lobe
infarction
R homonymo-us
VF deficit not palinopsia
Pt. with psychosis had repetitive episodes of
"hallucinated" pac-man moving towards VF deficit SVH
Ardila,
198710
L occipital
neurocysticercosis
cyst
epileptic discharge
irriration hyper-
excitability,
deafferentation
palinopsia started 1 day
after GTC, resolved with
anti-epileptic
transient right
homonymous
field deficit
scene
perseveration
During tx for neurocysticorcosis, had a GTC seizure and
afterwards had scene perseveration of orderly bringing
tray into the room with same speed, color, shape,
lasted about 30min in right visual field.
visual allesthesia,
cerebral polyopia, SVH
R occipital infarction
deafferentation;
irritation
hyperexcitability CT: right occipital infarction
left
homonymous
field deficit
scene and variant
formed image
perseveration
Long history of vascular headaches with momentary
image perseveration; after a CVA, got neuro signs, VF
deficits, and scene perseveration
dysmetropsia,
proposagnosia,
oscillopsia
Blythe,
198620
Idiopathic
rheumatological
disease unknown
unremarkable
neuroimaging, high ESR, sx
started while pregnant;
mildly improved on
carbamazepine
prolonged
indistinct
afterimages, light
streaking
After an unclear rheumatologic/neurologic insults, pt
noticed positive prolonged light afterimages, light
streaking. Worse for high contrast images, continuous,
depedent on brightness and stimulus exposure length.
Flash of camera would last 10-20minutes.
visual snow,
photophobia
Landis,
198686
R occipito-parietal
infarction
deafferentation,
irritation
hyperexcitability
CT: R occipitotemporal
infarction, EEG: slow wave
activity in R posterior
temporal region
left
homonymous
field deficit
categorical
incorporation,
scene
perseveration
Categorical incorporation with dog face. Repeated
scene of man walking. Palinopsia worsened over next
10 months
CVH, metamorphopsia,
prosopagnosia,
photopsia
Joseph,
198674
X Capgras and Cotard
syndrome of
subjective doubles unknown not palinopsia
Overtly psychotic man would look in mirror and see
two images of himself, one he dubbed an imposter CVH
Jacome,
198571
Multiple sclerosis
unknown/possible
MS demylineation
neuroimaging
unremarkable; VEP:
probable bilateral
retrochiasmal optic neuritis
bitemporal
visual extinction
on fixation
prolonged
indistinct
afterimages, light
streaking, variant
formed image
perseveration
After fixation, black images would momentarily appear
in her temporal visual fields seconds to minutes after
seeing object. Bright lights persisted for several hours;
images removed with head shaking or blinking
bilateral INO,
photophobia,
photopsia
Patterson,
1985116
R occipital abcess,
AML deafferentation
CT showed abscess and
autopsy, palinopsia was
presenting sx
left
homonymous
field deficit
categorical
incorporation
formed image
perseveratn
Severe headache then categorical incorporation with
boots on TV; delayed image perseveration with an
elephant on a billboard; palinopsia occurred over 10
days blurry vision
Lang, 198587
L occipital infarction deafferentation
CT: showed infarction,
palinopsia started after
right
homonymous
field deficit
formed image
perseveration
After a heart attack and a subsequent CVA, patient
noticed perseverated, moving letters to the point that
he could not read; resolved after 4 months

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Bynke,
198430
R temporal glioma
deafferentation,
irritative
hyperexcitability
CT: glioma, palinopsia after
tumor debulking
L homonymous
field deficit
formed image
perseveration
For weeks after operations, would see objects (red
roses) stationary in visual field for 10minutes.
Lazaro,
198389
R occipital GBM deafferentation
CT showed GBM;
presented as palinopsia
left
homonymous
field deficit
categorical
incorporation
1 episode of categorical incorporation with people,
lasting several minutes. Palinopsia was part of
presentation of GBM
transient visual
obscurations,
metamorphopsia
Cummings,
198237
R parieto-occipital
gliosis
irritation
hyperexcitability,
deafferentation
palinopsia started
immediately after surgery,
unaffected by phenyyoin
left
homonymous
field deficit
formed image
perseveration
After fixation, image persisted for 30-90 secs, worse
during high contrast; immediate or delayed, also
occured based on thought; daily for 6 years
micropsia, simple
visual hallucinations
Eretto,
198245
R occipital AVM, 2°
seizure
epileptic discharge
irritative
hyperexcitability
palinopsia started after
surgery, improved with
anti-epileptic
formed image
perseveration
Patient reports seeing a negative afterimage for a few
seconds, then the image jumped to the opposite VF
and turned positive, new image lasted a few minutes
macropsia, visual
allesthesia
Cleland,
198135
R parietal infarction
epileptic discharge,
deafferentation
CT: Right post. parietal
infarction, EEG: right
temporal abnormality
L homonymo-us
quadrant-
anopsia
scene
perseveration
Saw action of man walk in left VF repeated at twice the
speed for ~10min. Similar symptoms with a child
waving and brother putting hand in hair vision misty
Michel,
1980106
R occipital infarction,
maybe tumor deafferentation
CT: dec density in R
occipital lobe, no EEG;
asymptomatic after
radiation
subtle left
homonymous
deficit
patterned visual
spread,
categorical
incorporation
Cateogorical incorporation with faces, clothes, money.
patterned visual spread with a banana all over a wall
and a $20 bill
Hyperglycemia, 2°
seizure
epileptic discharge,
deafferentation
CT showed infarction;
palinopsia resolved after
glucose normalization
congruous left
homonymous
field deficit
formed image
perseveration;
categorical
incorporation
After looking at a picture, it persisted in left field of
vision. Categorical incorporation with faces. Blood
sugar was 534 when admitted to hospital
L occipital infarction
deafferentation,
irritation
hyperactivity
CT showed infarction, only
episode close proximity
after CVA
right
homonymous
field deficit
formed image
perseveration
After seeing objects on the table, he would look away
but still saw the objects floating in space, thought
palinopic images were real. Only had 1 episode
Jacobs,
198069
R parieto-occipital
AVM, 2° seizures
epileptic discharge,
irritative
hyperexcitability
angiogram: AVM; EEG:
right parietoccipital focus,
clinical seizure sx, resolved
with AED
formed image
perseveration
Immediate and delayed palinopsia 2 weeks after
neurosurgical procedure, objects would remain 3-
15minutes after stimulus was removed, the palinoptic
would be smaller and oscillate vertically
left homonymous
hemichromatopsia,
visual allesthesia
Swash,
1979141
Seizure of unknown
etiology epileptic discharge
EEG: episodic theta activity
in L temporal area; clinical
sx of seizure
formed image
perseveration
Patient would stare blankly into space for a few
seconds and have immediate afterimages that
persisted for several minutes
X
seizure of unknown
etiology epileptic discharge
CT negative; EEG:
sharpened theta wave
activity on the left not palinopsia
3 yr h/o seizures where his whole visual field would
remain fixed for several minutes until slowly fading
away; attacks stopped after phenytoin treatment
Meadows,
1977104
R occipitotemporal
infarction
deafferentation;
irritatiive
hyperexcitability
right occipitotemporal
infarct on autopsy
homonymous
left upper
quadrantanopsia
formed image
perseveration;
patterned visual
spread,
categorical
incorporation
categorical incoporation with beards superimposed on
people, delayed afterimage of candle; died a week later
from infarction
R occipitotemporal
meningioma, 2°
seizure epileptic discharge
Sx started with d/c of AED
and resolved by restarting
the AED
left
homonymous
field deficit
formed image
perseveration
Delayed palinopsia after stopping phenyyoin, saw
husbands face and a window in her defective visual
field CVH

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
** Idiopathic deafferentation normal EEG, Tc brain scan
L homonynous
quadrantanopsia
formed image
perseveration
1 episode of delayed palinopsia with barley lasting for 5
minutes
Brust,
197725
Hyperglcyemia, 2°
seizures
epileptic discharge
irritative
hyperexcitability
EEG: R occipitotemporal
spikes, Sx resolved with
glucose normalization and
AEDs
transient left
homonymous
field deficit
formed image
perseveration;
scene
perseveration
Patient with 390-700mg/dL blood sugars would have
seizures. After ictal activity, he would get transient
scotomas in left VF and see images or scenes in the
scotoma that he saw minutes to years before.
phosphenes,
metamorphopsia,
faces "melt"
Lance,
197685
pt 7 R occipital infarction
deafferentation;
irritative
hyperexcitability
Tc scan: R occipital
infarction; palinopsia
occurred after CVA
left
homonymous
field deficit
scene
perseveration
After seeing a man walk past on his left side, would see
the repetition of the scene in VF deficit
dysmetropsia,
metamorphopsia, CVH,
cerebral polyopia
pt 9
R occipital infarction,
2° seizure
epileptic discharge,
deafferentation
Palinopsia resolved after
AED
left
homonymous
field deficit
scene
perseveration;
formed image
perseveration
4 months after an occipital lobe infarction, saw
repeated scenes of people walking on both sides (visual
allesthesia), often in VF deficit
simple and CVH,
metamorphopsia
Anderson,
19729 HPPD
diffuse neurotrans-
mitter/receptor Δs
diagnosis of exclusion;
resolved with
trifluoperazine
akintopsia visual
trails
After ~65 hallucinogen doses in previous month, pt saw
motion as stroboscopic vision. Described it as constant,
worsened by light and concentration
photopsia, SVH,
depersonalization
Bender,
196817
pt 1
R posterior
hemisphere
metastasis deafferentation
angiogram: R occipital
lesion, palinopsia resolved
as VFD enlarged
left
homonymous
field deficit
formed image
perseveration
Delayed palinopsia of objects seen in recent past (clock,
eyes) in left VF lasting a few minutes, usually in same
location, persisted after eye closure
dysmetropsia, SVH,
visual allesthesia
pt 2
R occipital
meningioma
epileptic discharge,
deafferentation
angiogram: right occipital
meningioma, clinical sx of
seizure
L homonymous
quadrantanopsia
formed image
perseveration,
prolonged
indistinct
afterimages
"Shimmering of images" and seizures with intermittant
palinopic images in VF deficit for 4 years. Palinopsia
progressively worsened in frequency, length, and
became more delayed (30sec to eventually 30minutes)
dysmetropsia,
metamorphopsia,
cerebral polyopia
pt 3
R parieto-occipital
glioma
epileptic discharge,
deafferentation
angiogram: right parieto-
occipital glioma, clinical sx
of seizure
left
homonymous
field deficit
formed image
perseveration,
categorical
incorporation
Palinopic letters, zebra, hands in left visual field. False
images lasted 10-15seconds and would disppear and
re-appear over 20minutes, palinoptic images occurred
only at presentation of tumor
pt 4
Seizure of unknown
etiology
epileptic discharge,
deafferentation
normal angiogram, EEG:
bilateral occipito-temporal
spikes
transient,
homonymous
field deficits
formed image
perseveration
Patient not oriented to time/place. Stationary, fixed
palinopic images lasting a few minutes, not specific to a
part of visual field. Occurred with transient visual field
deficits and with eyelids opened or closed.
cerebral polyopia,
dysmetropsia, CVH,
achromotopsia,
metamorphopsia
pt 10
L parietal
ependymoma, 2°
seizures
epileptic discharge
irritation
hyperexcitability
Angiography, biopsy,
clinical seizure sx
formed image
perseveration
Two months after operation for neoplasm removal,
noticed enlarged perseverated images; also noticed
ringing in ears at same time macropsia
pt 11
R occipital lobe
aneursym
deafferentation,
irritation
hyperexcitability
Palinopsia occurred after
procedure to treat
aneursym
left
homonymous
field deficit
formed image
perseveration
For two years after operation, had photopsia and
immediate palinopsia in left visual field with
afterimages lasting about 1 minute SVH
pt 5-9, 12 no description Did not adequately describe symptom or etiology