fmea applied to the phenomenon of retained objects after surgery project managers dr. joan burtner...
TRANSCRIPT
FMEA Applied to the FMEA Applied to the Phenomenon of Phenomenon of
Retained Objects After SurgeryRetained Objects After Surgery
Project ManagersProject ManagersDr. Joan Burtner and Dr. Laura Dr. Joan Burtner and Dr. Laura
MoodyMoody
Mercer University School of Mercer University School of EngineeringEngineering
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 2
Presentation OverviewPresentation Overview
IntroductionIntroduction Motivation for the StudyMotivation for the Study Healthcare Failure Modes and Healthcare Failure Modes and
Effects Analysis Case StudyEffects Analysis Case Study Typical ResultsTypical Results Select RecommendationsSelect Recommendations Questions/CommentsQuestions/Comments
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 3
IntroductionIntroduction
To Err is HumanTo Err is Human – Call for action with – Call for action with respect to reducing medical errorsrespect to reducing medical errors
Case study courses at Mercer Case study courses at Mercer University School of Engineering University School of Engineering emphasize real-world projects emphasize real-world projects
Clients: MD and RN responsible for Clients: MD and RN responsible for administering Quality programs at a administering Quality programs at a hospital in the southeasthospital in the southeast
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 4
What is an FMEA?What is an FMEA? Failure Modes and Effects AnalysisFailure Modes and Effects Analysis ““FMEA is a team-based problem-solving FMEA is a team-based problem-solving
tool intended to help users identify and tool intended to help users identify and eliminate, or reduce the negative eliminate, or reduce the negative effects of, potential failures before they effects of, potential failures before they occur in systems, subsystems, product occur in systems, subsystems, product or process design, or the delivery of a or process design, or the delivery of a service.” service.” The Certified Quality Engineer The Certified Quality Engineer HandbookHandbook, page 233, page 233
CQE Body of Knowledge (Reliability and Risk CQE Body of Knowledge (Reliability and Risk Management)Management)
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 5
What is a Healthcare FMEA?What is a Healthcare FMEA? Motivation for the HFMEAMotivation for the HFMEA
Joint Commission on the Accreditation of Healthcare Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) Standard LD.5.2 requires facilities Organizations (JCAHO) Standard LD.5.2 requires facilities to select at least one high-risk process for proactive risk to select at least one high-risk process for proactive risk assessment annuallyassessment annually
FMEA vs HFMEAFMEA vs HFMEA HFMEA combines the detectability and criticality steps of HFMEA combines the detectability and criticality steps of
a traditional FMEAa traditional FMEA HFMEA uses a hazard score in place of the risk priority HFMEA uses a hazard score in place of the risk priority
number (RPN) that is associated with a traditional FMEAnumber (RPN) that is associated with a traditional FMEA Hazard Score obtained from the Hazard Matrix Table Hazard Score obtained from the Hazard Matrix Table
developed by the Department of Veteran’s Affairs developed by the Department of Veteran’s Affairs National Center for Patient SafetyNational Center for Patient Safety
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 6
Project Timeline 2005-2006Project Timeline 2005-2006
Preliminary researchPreliminary research Journal articles and booksJournal articles and books Materials provided by southeastern hospitalMaterials provided by southeastern hospital
Operating room observationsOperating room observations Process flow and documentationProcess flow and documentation
High-LevelHigh-Level Detailed counting proceduresDetailed counting procedures
Healthcare Failure Modes and Effects Healthcare Failure Modes and Effects AnalysisAnalysis
Consultation with MD and RNConsultation with MD and RN
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 7
Project TeamProject Team Clients: Upper level administrators at a Clients: Upper level administrators at a
southeastern hospitalsoutheastern hospital Chief Quality Officer (Physician)Chief Quality Officer (Physician) Performance Improvement Coordinator of Performance Improvement Coordinator of
Surgical Services (Registered Nurse)Surgical Services (Registered Nurse) Faculty at Mercer UniversityFaculty at Mercer University
Dr. Joan Burtner – Certified Quality EngineerDr. Joan Burtner – Certified Quality Engineer Dr. Laura Moody – Human Factors EngineerDr. Laura Moody – Human Factors Engineer
Students enrolled at Mercer UniversityStudents enrolled at Mercer University Industrial Engineering SeniorsIndustrial Engineering Seniors Industrial Management SeniorsIndustrial Management Seniors
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 8
Preliminary ResearchPreliminary Research Factors associated with retained objectsFactors associated with retained objects
Emergency surgeryEmergency surgery Unplanned change in surgical procedureUnplanned change in surgical procedure Patient obesity (higher mean body-mass-Patient obesity (higher mean body-mass-
index)index) Most likely causes for discrepancies in Most likely causes for discrepancies in
countscounts Intensity/complexity of the environment Intensity/complexity of the environment Non-standardized methods for Non-standardized methods for
performing countsperforming counts Poor communication among the Poor communication among the
Operating Room (OR) team membersOperating Room (OR) team members
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 9
Site-Specific ObservationsSite-Specific Observations
Forms used by southeastern hospitalForms used by southeastern hospital Qualitative assessment of processQualitative assessment of process
Two people have to witness the count Two people have to witness the count for it to be validfor it to be valid
Lap sponges are mainly lost in cases Lap sponges are mainly lost in cases with obese people and/or abdominal with obese people and/or abdominal surgeriessurgeries
Sponges will do more damage to the Sponges will do more damage to the patient than instruments if left inside patient than instruments if left inside the body, due to decompositionthe body, due to decomposition
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 10
Healthcare FMEA Step #1Healthcare FMEA Step #1
Define the process that will be Define the process that will be examined and define the scopeexamined and define the scope Process - Counting of surgical tools and Process - Counting of surgical tools and
sponges prior to, during and after sponges prior to, during and after operationsoperations
Goal - Provide client with possible Goal - Provide client with possible recommendations for performing this task recommendations for performing this task that will attempt to prevent surgical tools that will attempt to prevent surgical tools and sponges from being left inside patientsand sponges from being left inside patients
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 11
Healthcare FMEA Step #2Healthcare FMEA Step #2
Assemble the TeamAssemble the Team ISE StudentsISE Students ISE ProfessorsISE Professors IDM StudentsIDM Students MD MD RNRN
ExpertiseExpertise Subject-matterSubject-matter Process ImprovementProcess Improvement
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 12
Healthcare FMEA Step #3Healthcare FMEA Step #3
Graphically represent the processGraphically represent the process Two flows generatedTwo flows generated
High-Level process flowHigh-Level process flow Detailed counting procedure process Detailed counting procedure process
flowflow Only partial graphics will be Only partial graphics will be
presented due to proprietary presented due to proprietary reasonsreasons
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 13
Healthcare FMEA Step #4Healthcare FMEA Step #4
Conduct a hazard analysisConduct a hazard analysis Define potential failures at each step in each Define potential failures at each step in each
processprocess Define causes for failures at each step in processDefine causes for failures at each step in process Assign severity rating:Assign severity rating:
catastrophic, major, moderate, minor catastrophic, major, moderate, minor Determine probability scoreDetermine probability score Determine hazard scoreDetermine hazard score Eliminate, control, or accept failure mode Eliminate, control, or accept failure mode Actions for eliminate or controlActions for eliminate or control Who is responsible?Who is responsible?
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 14
Process Flow and Process Flow and DocumentationDocumentation
High-Level ProcessHigh-Level Process Highlights overall operating room Highlights overall operating room
proceduresprocedures Reviewed and approved by RNReviewed and approved by RN
Detailed Counting ProceduresDetailed Counting Procedures Highlights the specific counting procedures Highlights the specific counting procedures
for sponges, sharps, and instrumentsfor sponges, sharps, and instruments Reviewed and approved by RNReviewed and approved by RN
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 15
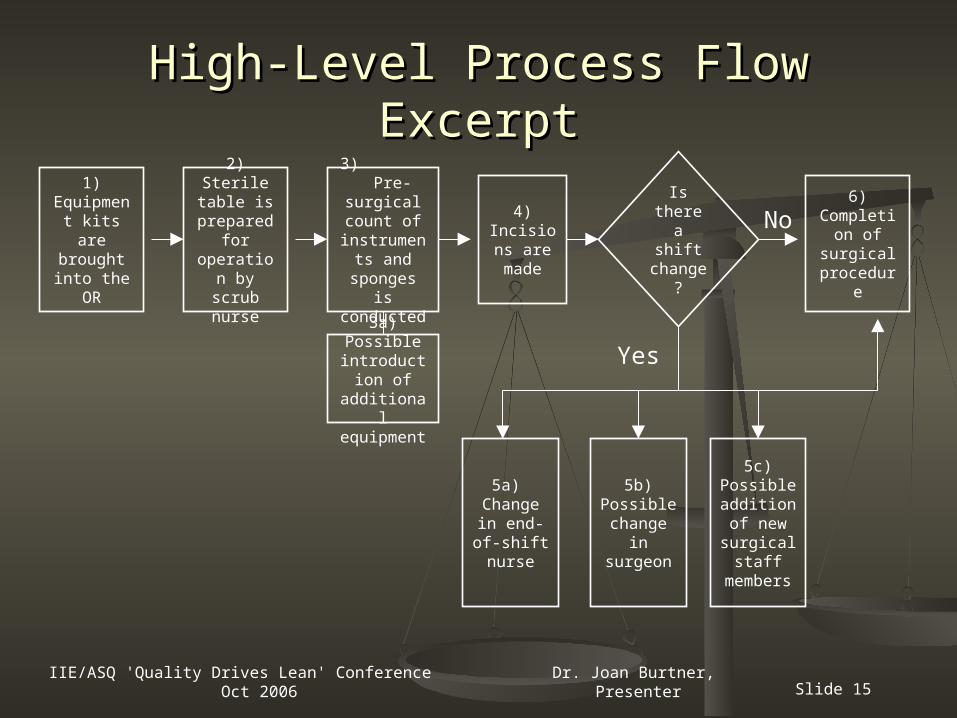
High-Level Process Flow ExcerptHigh-Level Process Flow Excerpt
Is there a shift change
?
Yes
6) Completio
n of surgical
procedure
3a) Possible
introduction of
additional equipment
No1)
Equipment kits are brought into the
OR
2) Sterile table is
prepared for
operation by scrub
nurse
3) Pre-
surgical count of
instruments and
sponges is conducted
4) Incisions
are made
5a) Change
in end-of-shift
nurse
5b) Possible change
in surgeon
5c) Possible addition of new surgical
staff members
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 16
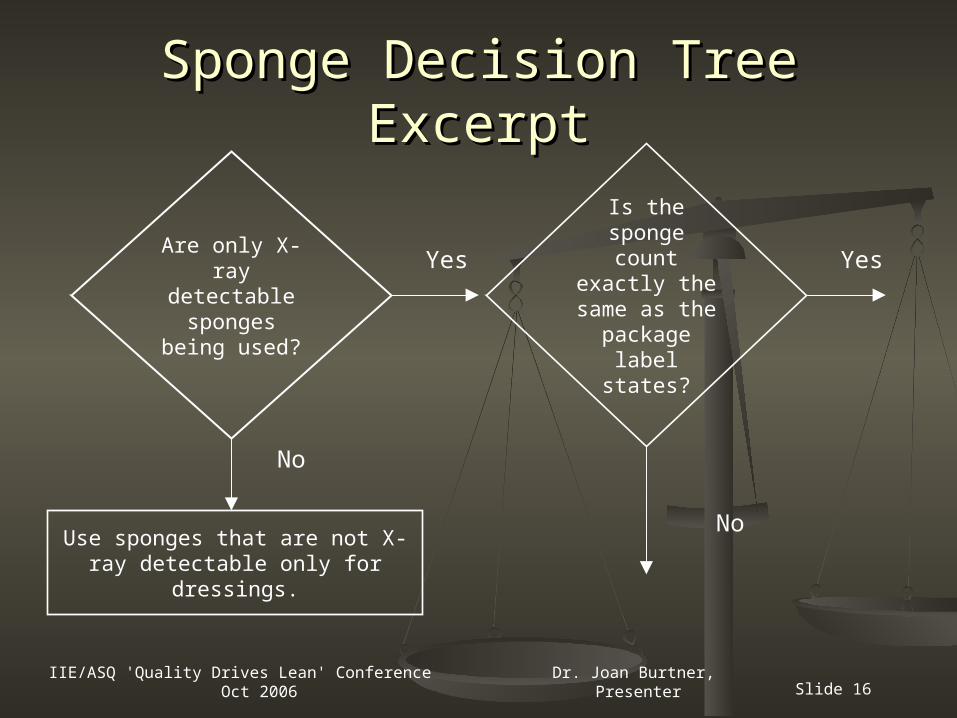
Sponge Decision Tree ExcerptSponge Decision Tree Excerpt
Is the sponge count
exactly the same as the
package label states?
YesAre only X-
ray detectable sponges
being used?
Use sponges that are not X-ray detectable only for dressings.
Yes
No
No
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 17
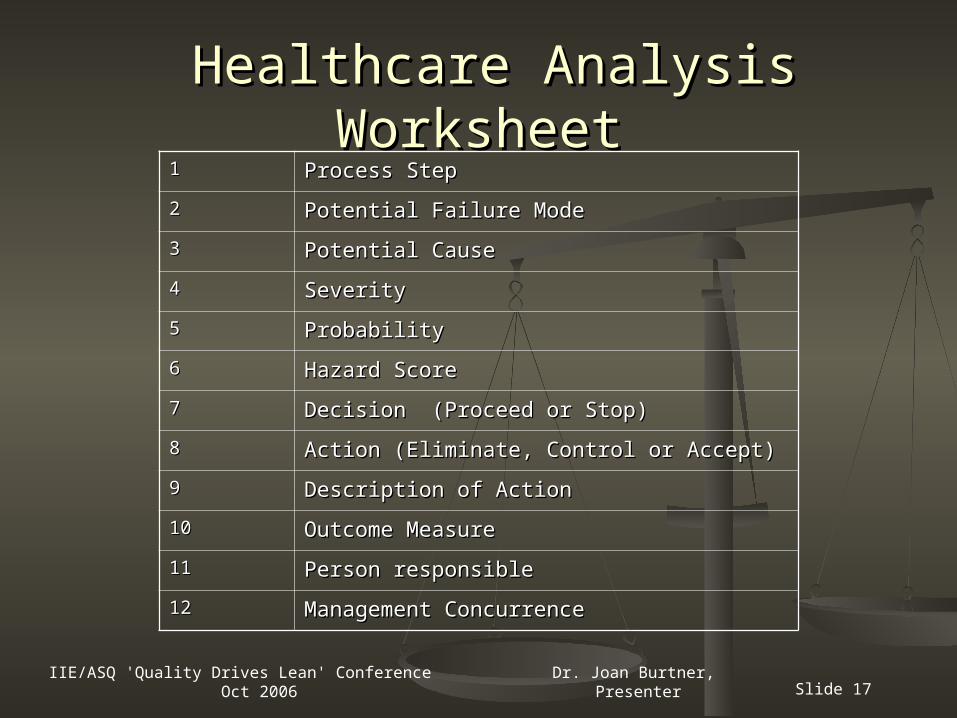
Healthcare Analysis WorksheetHealthcare Analysis Worksheet11 Process StepProcess Step
22 Potential Failure ModePotential Failure Mode
33 Potential CausePotential Cause
44 SeveritySeverity
55 ProbabilityProbability
66 Hazard ScoreHazard Score
77 Decision (Proceed or Stop)Decision (Proceed or Stop)
88 Action (Eliminate, Control or Accept)Action (Eliminate, Control or Accept)
99 Description of ActionDescription of Action
1010 Outcome MeasureOutcome Measure
1111 Person responsiblePerson responsible
1212 Management ConcurrenceManagement Concurrence
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 18
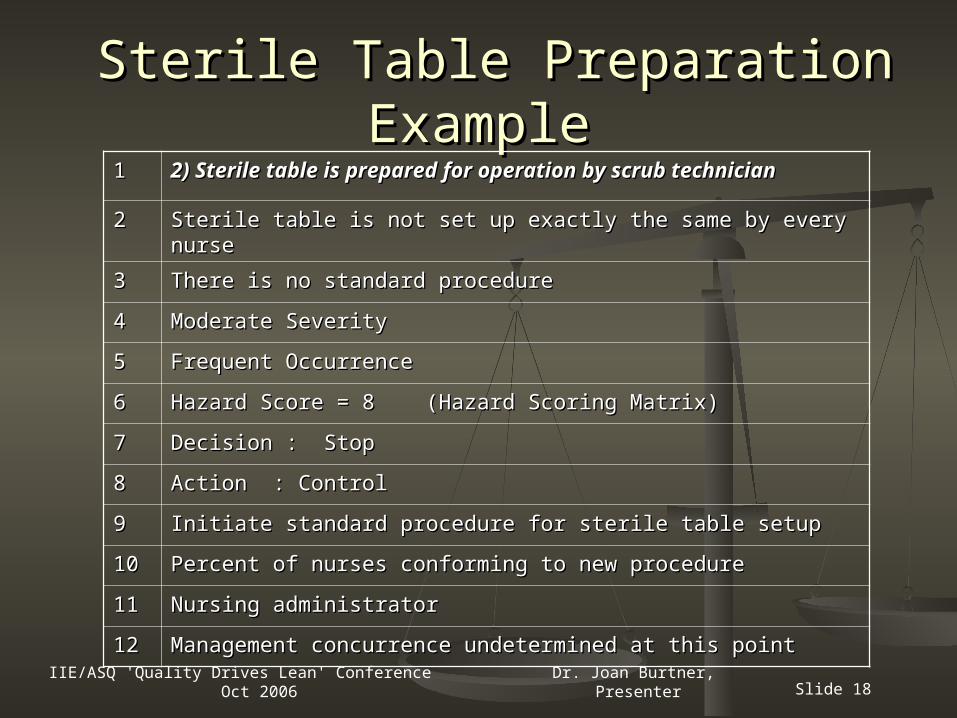
Sterile Table Preparation ExampleSterile Table Preparation Example11 2) Sterile table is prepared for operation by scrub 2) Sterile table is prepared for operation by scrub
techniciantechnician
22 Sterile table is not set up exactly the same by every nurseSterile table is not set up exactly the same by every nurse
33 There is no standard procedureThere is no standard procedure
44 Moderate SeverityModerate Severity
55 Frequent OccurrenceFrequent Occurrence
66 Hazard Score = 8 (Hazard Scoring Matrix)Hazard Score = 8 (Hazard Scoring Matrix)
77 Decision : StopDecision : Stop
88 Action : Control Action : Control
99 Initiate standard procedure for sterile table setupInitiate standard procedure for sterile table setup
1010 Percent of nurses conforming to new procedurePercent of nurses conforming to new procedure
1111 Nursing administratorNursing administrator
1212 Management concurrence undetermined at this pointManagement concurrence undetermined at this point
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 19
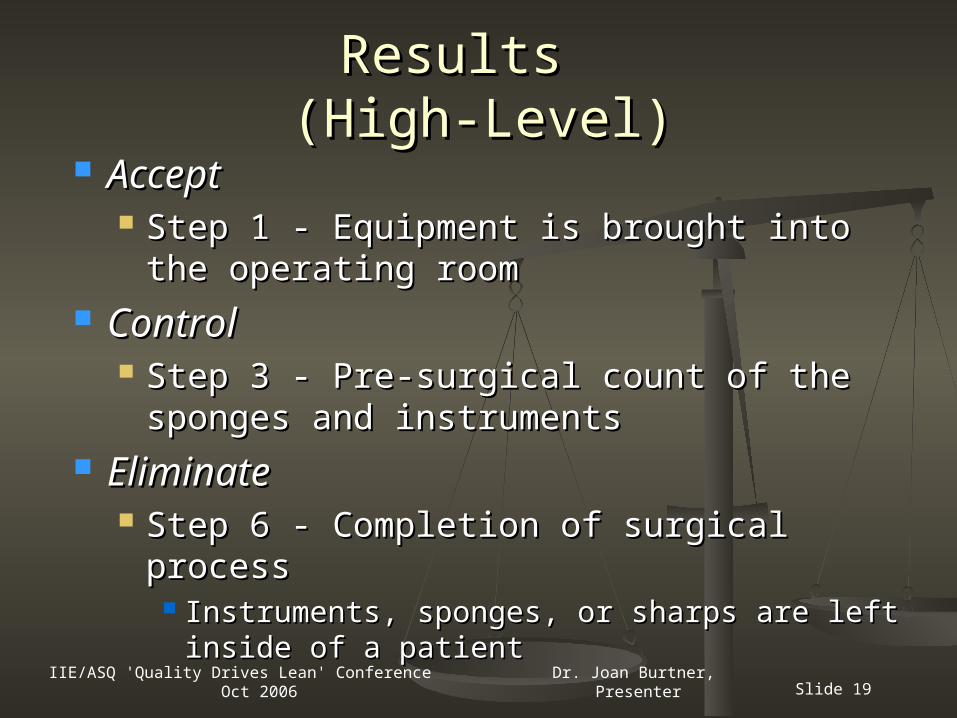
Results Results (High-Level)(High-Level)
AcceptAccept Step 1 - Equipment is brought into the Step 1 - Equipment is brought into the
operating roomoperating room ControlControl
Step 3 - Pre-surgical count of the Step 3 - Pre-surgical count of the sponges and instrumentssponges and instruments
EliminateEliminate Step 6 - Completion of surgical processStep 6 - Completion of surgical process
Instruments, sponges, or sharps are left Instruments, sponges, or sharps are left inside of a patientinside of a patient

IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 20
ResultsResults(Detailed Counting Procedures)(Detailed Counting Procedures)
AcceptAccept Step 2a - Sponges are not completely Step 2a - Sponges are not completely
separated during the countseparated during the count
ControlControl Step 11 - Object has left sterile field, Step 11 - Object has left sterile field,
circulator must retrieve and verify with the circulator must retrieve and verify with the scrub nursescrub nurse
EliminateEliminate Step 10 - The scrub nurse continually Step 10 - The scrub nurse continually
counts needles during the procedurecounts needles during the procedure
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 21
Recommendations for FutureRecommendations for Future
Review FMEA worksheets Review FMEA worksheets Institute recommendations and testInstitute recommendations and test Continue to monitor process flow Continue to monitor process flow
periodicallyperiodically Revise as necessaryRevise as necessary
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 22
The project managers would like to The project managers would like to acknowledge the exceptional efforts of acknowledge the exceptional efforts of the members of the student team as the members of the student team as
well as the professionalism of our well as the professionalism of our community partners at a hospital in community partners at a hospital in
the southeast.the southeast.
AcknowledgementsAcknowledgements
IIE/ASQ 'Quality Drives Lean' Conference Oct 2006 Dr. Joan Burtner, Presenter Slide 23
Questions or Comments?Questions or Comments?
Dr. Joan BurtnerDr. Joan BurtnerASQ Certified Quality EngineerASQ Certified Quality Engineer
Associate Professor of Industrial EngineeringAssociate Professor of Industrial EngineeringMercer University Macon, GAMercer University Macon, GA
(478) 301-4127(478) [email protected][email protected]