accountable care organizations- creating a care … care organizations- creating a care community...
TRANSCRIPT
Accountable Care Organizations- Creating a Care Community Webinar: September 11, 2013
Presented by:
Adele Allison, National Director of Government Affairs, SuccessEHS, Inc.
The following questions and answers were raised during the AAOMS Webinar “Accountable Care Organizations-Creating a Care Community” broadcasted on September 11, 2013. This Webinar provided a general overview of Accountable Care Organizations (ACOs) including the history and progression of the United States’ physician reimbursement system, which included the federal government’s desired reformation. This webinar educated OMS and administrators about the rules governing assignment of Medicare beneficiaries; the 33 quality measures that must be reported by ACOs; how commercial carriers are moving to this type of delivery model; and the health IT considerations necessary for successful participation.
Q: How will ACOs affect OMS practices directly? A: As discussed in the webinar, ACOs may be contracted to private payers, government
payers or both. If an ACO has contracted with Medicare, it will be subject to the Final Rule issued by CMS on Oct. 20, 2011. ACOs will be most effective where they have aligned the governance and operational structure, the participant values, and the providers throughout the care continuum including OMS. The more comprehensively the full continuum is in sync with the goals and mission of the ACO, the more successful the ACO will be in increasing the quality of care and decreasing the cost.
Quite often, oral-related care is overlooked in the development of a holistic delivery system. Yet, OMS is very much part of the community. Depending on the ACO vision and contractual relationships with payers, OMS may be deemed more or less of a priority. However, the more fully integrated into the ACO an OMS is will be a direct function of quality patient care. On the lower end of the integration spectrum, the involvement may be limited to simple referral management and tracking, as well as care coordination. Tighter integration can lead to supporting streamlined communication, data-sharing through use of electronic health records (EHRs) and health information exchange (HIE), and even shared-risk and opportunity through value-based reimbursement models, such as shared-savings and capitation.
In the long-term, an OMS will be best positioned by embracing the underpinnings of the ACO to succeed under health care reform. Regardless of the long-term viability of the ACO model of care delivery, getting the patient the right care, in the right care setting, at the right time, for the right price, will survive.
Q: How does an ACO apply to me as an oral and maxillofacial surgeon if I have opted out
of Medicare? A: The ACO model actually pre-dates CMS getting into the mix. In fact, there were over
150 ACOs in existence prior to CMS launching its contracting. As of July, 2013, there were 488 ACOs nationwide of which only 253 were contracted to CMS for Medicare— 55 having contracts with both Medicare and private payers. So, while many may have contractual relationships with Medicare, many have no relationship with Medicare and thus would have no impact on this election to opt-out. However, if an OMS contracts with an ACO, he/she is part of a single legal entity (TIN) that has the ability to contract with payers, including Medicare. Thus, an ACO contractual relationship could potentially change an opt-out election to opt and require you to accept reimbursement arrangements made by the ACO for Medicare beneficiaries. I would encourage you to fully understand the risk-sharing models for which any ACO may contract, since it will be linked to your financial destiny.
Q: What would be the benefit for an oral surgeon to be part of an ACO if they do not
want to participate in Medicare? A: As discussed in the question above regarding the impact on OMS practices directly, OMS
is part of the care continuum and should be part of the community’s delivery system. In the U.S., health care represents an intricate schema of the economy with the Federal government spending around 24 percent of its budget on health care alone, 16 percent on Medicare. The CBO is predicting Medicare to grow to 20 percent of the Federal budget by 2020. In the U.S., health care is impacted by legal, economic, social, political, cultural, technological and very personal systems. Generally, providers enjoy autonomy in the practice of medicine and dentistry.
The government has assumed a leadership role in reforming health care under the
Affordable Care Act (ACA); both how it is delivered and how it is provisioned. This is part of an effort to create and purchase value, or value-based purchasing (VBP). ACA has triggered a sweeping trend of VBP models among governmental and commercial payers. Over time, VBP models of care delivery will replace our blanket fee-for-service system. The ACO is a VBP model that is being embraced by CMS and commercial payers alike. According to a survey of national payers performed by Booz & Company, virtually every major payer was either involved in planning or seriously considering ACOs.
The greatest benefit of participation is becoming part of a bigger community in voice and governance as this paradigm shift occurs within your market. For procedural specialists, such as OMS, ACOs can provide volume and margin stabilization at a time when specialists are facing volume declines due to aggressive care management and utilization controls– something that will grow under health care reform.
Q: When is the best time to become engaged with an ACO? A: Early. Initially, risk-modeling may have limited or no downside, as with the one-sided
Medicare Shared-Savings Program ACO. This will allow providers to come together and own their destiny, defining what works and what does not work before reimbursement assumes a more structured risk-model. It also helps with the mental shift of moving from volume-based reimbursement to value-based.
Q: My hospital’s ACO includes a physician from every specialty except oral and
maxillofacial surgery. How can I approach the ACOs in our area about including oral and maxillofacial surgery into the model?
A: The key to incorporation of OMS into an ACO that is overlooking OMS lay in creating a
value-proposition. An ACO is essentially a cultural shift. You must demonstrate and focus on ways that OMS can help achieve the ACO triple aim of enriching the patient experience, improving the patient’s overall health, and reducing the cost of care.
Q: What are the ramifications if asked to join an ACO, but I reject the offer to participate
with a payer? A: Your ability to reject an ACO payer contract will be governed by your ACO participation
agreement, so read it carefully. Under some payer contracts, the OMS may continue with a direct provider-payer contractual arrangement. With other contracts, the OMS would be obliged to participate at an “upstream” level through the ACO. Payment reform models are coming to governmental and private payers alike and can include such arrangements as simple managed fee-for-service to full risk-sharing.
You need to evaluate your readiness to embrace new payment models such as shared-
savings, global payments, bundled payments, episodic payments and both full and partial capitation. Some of these arrangements will require tighter clinical and financial integration with providers in your community. A well governed ACO should bring OMS the strongest value that can be achieved with ease and the least amount of financial investment and reduced risk.

Q: Do ACOs only apply to Medicare reimbursement? A: No. Each ACO’s payer mix can vary from only having a single contract such as with CMS
for Medicare to multiple contracts. As of July, 2013, of 488 identified ACOs in the U.S., only 52 percent had contracts with Medicare; 11 percent had contracts with both CMS and private payers.
Q: Which commercial payers have formed ACOs and are they operating the same as
Medicare ACOs? A: Great question! There is no single source that maintains a full handle on this rapidly
evolving market. Some good sources that periodically report on ACOs are:
The American Academy of Physical Medicine and Rehabilitation (AAPM&R) – www.aapmr.org. They maintain a list of ACOs by state.
Leavitt Partners – www.leavittpartners.com. They provide a periodic report on the ACO trends.
According to an analysis released in June, 2013, by Premier Health Alliance of 85 ACO payer arrangements:
Type of Plan Capitation Shared-Savings
with Downside
Risk
Shared-Savings
with Upside
Only Risk
Bundled
Payments
Care
Management
Fees
Provider-Owned
Plan (50% or less
ownership)
1
Provider-Owned
Plan (Over 50%
ownership)
1 1 2 1 3
Self-Insured
Employers 1 4 2
Commercial 2 8 6 1 11
Medicaid 1 2 2 1 4
Medicare
Advantage 2 2 3 1 5
Medicare MSSP 1 13
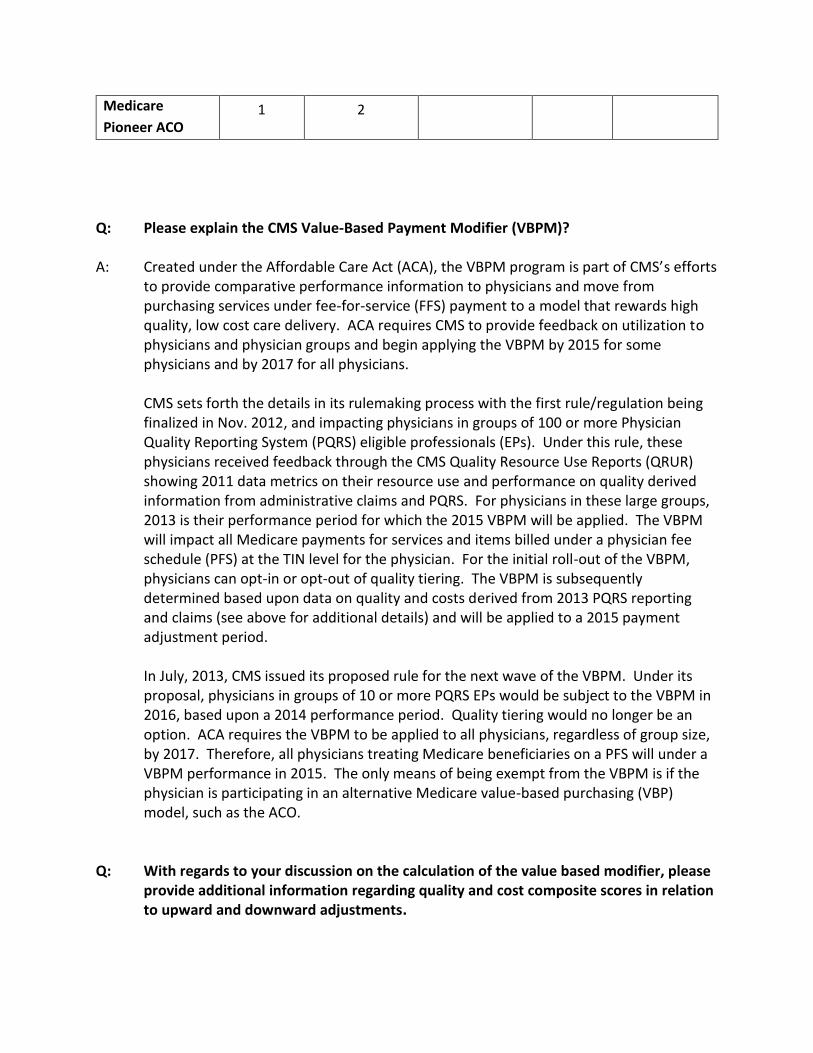
Medicare
Pioneer ACO 1 2
Q: Please explain the CMS Value-Based Payment Modifier (VBPM)? A: Created under the Affordable Care Act (ACA), the VBPM program is part of CMS’s efforts
to provide comparative performance information to physicians and move from purchasing services under fee-for-service (FFS) payment to a model that rewards high quality, low cost care delivery. ACA requires CMS to provide feedback on utilization to physicians and physician groups and begin applying the VBPM by 2015 for some physicians and by 2017 for all physicians.
CMS sets forth the details in its rulemaking process with the first rule/regulation being
finalized in Nov. 2012, and impacting physicians in groups of 100 or more Physician Quality Reporting System (PQRS) eligible professionals (EPs). Under this rule, these physicians received feedback through the CMS Quality Resource Use Reports (QRUR) showing 2011 data metrics on their resource use and performance on quality derived information from administrative claims and PQRS. For physicians in these large groups, 2013 is their performance period for which the 2015 VBPM will be applied. The VBPM will impact all Medicare payments for services and items billed under a physician fee schedule (PFS) at the TIN level for the physician. For the initial roll-out of the VBPM, physicians can opt-in or opt-out of quality tiering. The VBPM is subsequently determined based upon data on quality and costs derived from 2013 PQRS reporting and claims (see above for additional details) and will be applied to a 2015 payment adjustment period.
In July, 2013, CMS issued its proposed rule for the next wave of the VBPM. Under its
proposal, physicians in groups of 10 or more PQRS EPs would be subject to the VBPM in 2016, based upon a 2014 performance period. Quality tiering would no longer be an option. ACA requires the VBPM to be applied to all physicians, regardless of group size, by 2017. Therefore, all physicians treating Medicare beneficiaries on a PFS will under a VBPM performance in 2015. The only means of being exempt from the VBPM is if the physician is participating in an alternative Medicare value-based purchasing (VBP) model, such as the ACO.
Q: With regards to your discussion on the calculation of the value based modifier, please
provide additional information regarding quality and cost composite scores in relation to upward and downward adjustments.

A: CMS Quality tiering is at the heart of shifting from the purchasing of services (volume-based revenue model) to becoming a purchaser of value (performance-based revenue model). Providers will be plotted against the national mean based on two scores:
1. Quality of Care Composite Score. This score is developed through reporting clinical
data to CMS under the Physician Quality Reporting System (PQRS) in six national priority domains establish in the National Quality Strategy: clinical care, patient experience, population/community health, patient safety, care coordination and efficiency.
2. Cost Composite Score. This score is created from five per capita cost measures on Medicare beneficiaries: total per capita costs (Medicare Parts A and B) and the total per capita costs for beneficiaries with one or more of four target chronic diseases (Diabetes, CAD, COPD and heart failure).
These two composite scores are combined to create the Value-Based Purchasing Modifier (VBPM) for quality tiering. To do so, CMS will classify the scores into categories of high, average and low. To do this, CMS will measure the composites precisely at the 5.0 percent level of significance (e.g., a 95 percent confidence interval) and classify those scores that are at least one standard deviation above and below the mean into high/low categories. CMS will compare the quality composite classification with the cost composite classification to arrive at a VBPM adjustment set forth in the table below.
Table 1. Calculation of the Value Modifier Using the Quality-Tiering Approach
Quality/Cost Low Cost Average Cost High Cost
High Quality +2.0x* +1.0x* +0.0%
Medium Quality +1.0x* +0.0% -0.5%
Low Quality +0.0% -0.5% -1.0%
* Eligible for an additional +1.0x if reporting clinical data for quality measures and average beneficiary risk score in
the top 25 percent of all beneficiary risk scores.
Any upward payment (reward) will be budget neutral to CMS, using revenue generated
from downward payment adjustments for poor performers. To do this, CMS will first
aggregate the downward payment adjustments in Table 1 with the -1.0 percent
adjustments from groups of physicians that fall within “Category 2,” because they did
not participate in PQRS reporting. This amount will then solve for the upward payment
adjustment factor of “x” noted in Table 1.

Example:
1. CMS determines the aggregate projected amount of the downward payment
adjustments.
2. CMS calculates the payment adjustment factor – let us say it is 0.75 percent.
3. The High Quality/Low Cost groups of physicians would receive a 1.5 percent
upward adjustment based upon 2.0 x 0.75 (see cell in Table 1 highlighted
yellow).
Q: What is Health IT? A: Health Information Technology (health IT, or HIT) is the design, development, use and
maintenance of computerized information systems for management of health care data by and between consumers, providers, health care organizations, insurers and the government.
Q: In what ways is Health IT necessary for participation in an ACO? A: Health IT will be decisive in determining ACO winners and losers and the course of unity
for a common purpose as a health community. Within an ACO, health IT will be used to create evidence-based care plans, ensure patient safety, streamline provider-provider and provider-patient communications, manage transitions of care and referrals, and implement care delivery strategies that integrate medical, dental and social services through a provider-led care team. ACO success, sophistication and achievement will greatly depend on the ability to measure performance and utilization, continue process improvement, electronically coordinate care, effectively communication among the ACO stakeholders and engage the patient. ACO accomplishments can only be met through adoption of a robust health IT infrastructure to support a common goal.
Q: Is it possible to obtain a glossary of all the acronyms provided in today’s webinar? A: Yes, please see attached glossary beginning on page 10 of this document. Q: Do you think Policy-Making will evolve to include oral health more fully? A: Yes. It is the policymaking under CMS that outlines many of the details that impact
delivery system design. Ultimately, federal healthcare policymaking answers to the White House under the cabinet position known as the Secretary of Health and Human Services (HHS). Under HHS, there are 12 agencies (e.g., FDA, ONC, HRSA, CMS, etc.).

Provider policymaking, known as rules or regulations, will always come from their governmental payer – the Centers for Medicare and Medicaid Services (CMS). We have seen the advocacy efforts by such entities as the ADA and the National Network for Oral Health Access (NNOHA) result in oral health clinical quality measures (CQMs) being added to the Meaningful Use program. Nevertheless, oral health professionals will always struggle to strike a balance due to a statutory limitation in the Social Security Act (§ 1862(a)(12)), since Medicare does not cover general dental care or most dental procedures such as cleanings, fillings, tooth extractions or dentures.
Q: Do you think ACOs will be here for the long-term? A: It is hard to say. CMS contracted with 32 Pioneer ACOs, intended to promote more
advanced markets with multi-payer collaboration. While all 32 demonstrated value to CMS in the first year, nine abandoned the Pioneer ACO model halfway through their contracts. Seven of these moved into the CMS Medicare Shared-Savings Program (MSSP) ACO model with less risk; two dropped out completely owing $4 million to Medicare; and, many lessons were learned. Despite the growing trend, ACOs will need to advance payment model design and continue to improve health IT infrastructures for long-term sustainability. Regardless, the goal of coming together as a community of providers to promote health and wellness, manage chronic disease and acute care, and be accountable for the quality and costs will survive.
Polling Questions in Order of Presentation (Correct answers in Bold)
1. All of the following are accurate statements about the evolution of provider reimbursement
in the U.S., except:
a. Capitation can create provider adverse selection risk
b. Current fee schedules are derived using a % of Health Insurance Association of
America (HIAA)
c. RBRVS fees use a three-part formula of work, expense and risk
d. The Medicare dental exclusion was last updated in 1980
e. Under ACA, CMS is now contracting with ACOs
2. Which of the following statements applies to the Affordable Care Act and Value-Based
Purchasing (VBP):
a. The government is seeking to become a purchaser of value
b. ACA requires CMS to being applying a Value-Based Purchasing Modifier (VBPM) by
2015
c. Value is defined as a function of Quality and Cost
d. Quality is defined by clinical data, cost by claims data
e. All of the above apply
3. All of the following are true statements about the Accountable Care Organization model of
care delivery, except:
a. ACOs are unique legal entities
b. ACOs are a model of VBP
c. ACOs use health IT to increase quality and efficiency
d. The number of new ACOs forming is tapering off
e. Commercial and CMS ACOs require performance reporting
4. All of the following are true statements about the CMS contracted ACO, except:
a. CMS has 3 types of ACOs – Medicare Shared-Savings Program, Advanced Payment,
and Pioneer
b. Shared-Savings ACOs can have 1-sided or 2-sided risk
c. CMS ACOs have 44 performance measures
d. EHR adoption is weighted twice over the other measures
e. 7 measures are linked directly to patient experience
5. Which of the following statements applies to Oral Surgeons and ACOs:
a. Many associate Oral Surgery with Dentistry
b. Medicare is a big ACO focus, which does not cover dental
c. Oral Surgeons need to identify the value proposition for ACOs
d. Integration can start simple and grow with time
e. All of the above applies

888.879.7302 • www.SuccessEHS.com
Page1
Term Description
Accountable Care Organization (ACO)
A type of payment and delivery reform model that seeks to tie provider reimbursement to quality metrics and reduction in the total cost of care for an assigned population of patients (E.g. Medicare). An ACO is a unique legal entity with its own TIN wherein a group of coordinated health care providers provide care to a defined patient population. The ACO may use a range of payment models (capitation, fee‐for‐service with asymmetric or symmetric shared savings, etc.). The ACO is accountable to the patients and the third‐party payer for the quality, appropriateness, and efficiency of the health care provided. CMS defines an ACO as “an organization of health care providers that agrees to be accountable for the quality, cost, and overall care of Medicare beneficiaries who are enrolled in the traditional fee‐for‐service program who are assigned to it.”
Beacon Community Funded under HITECH grant through the Office of National Coordinator (ONC), there are 17
communities in the U.S. designed to build and strengthen their existing health information
technology infrastructure and exchange capabilities. These communities demonstrate the vision
of a future where hospitals, clinicians, and patients are meaningful users of health IT and
together the community achieves measurable improvements in health care quality, safety,
efficiency, and population health. Beacons exist in the following communities: Brewer, ME;
Spokane, WA; Indianapolis, IN; Grand Junction, CO; New Orleans, LA; Stoneville, MS; Cincinnati,
OH; Tulsa, OK; Hilo, HI; Danville, PA; Providence, RI; San Diego, CA; Detroit, MI; Rochester, NY;
Concord, NC; Salt Lake City, UT; and, Buffalo, NY.
Certificate Authority (CA)
A certificate authority (CA) is an authority in a network that issues and manages security credentials and public keys for message encryption. As part of a public key infrastructure (PKI), a CA checks with a registration authority (RA) to verify information provided by the requestor of a digital certificate. If the RA verifies the requestor’s information, the CA can then issue a certificate. Depending on the public key infrastructure implementation, the certificate includes the owner’s public key, the expiration date of the certificate, the owner’s name, and other information about the public key.
Certification Criteria Certification of Health IT products provides assurance to purchasers and other users that an EHR system, or other relevant technology, offers the necessary technological capability, functionality, and security to help them meet the meaningful use criteria established for a given stage. Certified EHR Technology (CEHRT) are tested and certified to meet ONC standards for functionality, security, confidentiality and interoperability. CEHRT that meets Stage 1 Meaningful Use criteria is deemed 2011 Edition certified. CEHRT that meets Stage 2 Meaningful Use criteria is 2014 Edition certified. All eligible professionals (EPs) must use CEHRT 2014 Edition technology for Meaningful Use effective in 2014, regardless of the stage for which they are working to achieve.
Clinical Document Architecture (CDA)
The HL7 Clinical Document Architecture (CDA) is an XML‐based markup standard intended to specify the encoding, structure and semantics of clinical documents for purposes of exchange between different systems.
Consolidated CDA (CCDA)
The single ONC standard for communicating the summary of care for Meaningful Use. The CCDA encompasses a communication standard that accommodates all data elements CMS asks that providers give their patients after an office visit. It offers a library of reusable CDA templates, setting the stage for streamlined development and rapid implementation of Health Information Exchange (HIE). These templates facilitate incremental interoperability and easier machine‐to‐machine communication for the transfer and storage of data.
Continuity of Care CCD is an HL7 CDA implementation of the Continuity of Care Record (CCR). It is generally possible to convert a CCR document into a CCR, however it is not always possible to perform the

888.879.7302 • www.SuccessEHS.com
Page2
Document (CCD) inverse transformation as some CCD features are not supported in CCR. A CCD is a document that contains the most relevant and timely core health information about a patient. This document is transmitted electronically from one caregiver to another. It contains various sections such as patient demographics, insurance information, diagnoses and problem list, medications, allergies and care plan. These represent a "snapshot" of a patient's health data in a human‐readable format.
Continuity of Care Record (CCR)
Like CCD, CCR is another form of HL7 document that contains the most relevant and timely core health information about a patient. This document is transmitted electronically from one caregiver to another. It contains various sections such as patient demographics, insurance information, diagnoses and problem list, medications, allergies and care plan. These represent a "snapshot" of a patient's health data.
Data Use and Reciprocal Support Agreement (DURSA)
The legal multi‐party trust agreement that is entered into voluntarily by all entities, organizations and Federal agencies that desire to engage in electronic health information exchange (HIE) with other members of the Nationwide Health Information Network Exchange now known as eHealth Exchange.
Digital Certificate A digital certificate is an electronic “credit card” that establishes an individual’s credentials when doing business or other transactions on the Web. It is issued by a certificate authority (CA). It contains the certificate holder’s name, a serial number, expiration dates, a copy of the certificate holder’s public key (used for encrypting messages and digital signatures), and the digital signature of the certificate‐issuing authority so that a recipient can verify that the certificate is real. Some digital certificates conform to a standard known as X.509. Digital certificates can be kept in registries so that authenticating users can look up other users’ public keys (See also: certificate authority, registration authority, and public key infrastructure).
Direct Exchange Born from the ONC’s “Direct Project,” Direct enables exchange of health information through a “push” transport where a sender pushes information to one or more known recipients – similar to email. Direct messages act as containers of health information and use digital certificates to protect these messages in transit and to express a trust relationship between those exchanging information. Security/trust agents (STAs) such as Health Information Service Providers (HISPs) to provide the necessary services for exchange using Direct.
eHealth Exchange (Exchange)
A group of federal agencies and non‐federal organizations that came together under a common mission and purpose to improve patient care, streamline disability benefit claims, and improve public health reporting through secure, trusted, and interoperable health information exchange (HIE). Participating organizations mutually agree to support a common set of standards and specifications that enable the establishment of a secure, trusted, and interoperable connection among all participating Exchange organizations for the standardized flow of information, by:
Sending health information to other participating organizations
Finding and requesting copies of healthcare information from other participating organizations‐‐where permitted by law and policy
Matching patients to their data without a national patient identifier
Subscribing to receive updates to health information
888.879.7302 • www.SuccessEHS.com
Page3
Electronic Health Record (EHR)
An electronic record of health‐related information on an individual that conforms to nationally recognized interoperability standards and that can be created, managed, and consulted by authorized clinicians and staff across more than one health care organization. EHRs create a longitudinal view of the patient’s health information.
Electronic Medical Record (EMR)
An electronic record of health‐related information on an individual that can be created, gathered, managed, and consulted by authorized clinicians and staff within a single health care organization.
Health Information Exchange (HIE)
Used as both a noun and a verb, HIE is the electronic movement of health‐related information among organizations according to nationally recognized standards. The goal of health information exchange is to facilitate access to and retrieval of clinical data to provide safer, timelier, efficient, effective, equitable, patient‐centered care. Health information exchange organizations (HIOs) provide the capability to electronically move clinical information between disparate health care information systems while maintaining the meaning of the information being exchanged. HIOs also provide the infrastructure for secondary use of clinical data for purposes such as public health, clinical, biomedical, and consumer health informatics research as well as institution and provider quality assessment and improvement. Most HIOs currently are regional health information organizations (RHIOs).
Health Information Organization (HIO)
An organization that oversees and governs the exchange of health‐related information among organizations according to nationally recognized standards. (See also: health information exchange (HIE) and regional health information organization (RHIO).)
Health Information Service Provider (HISP)
HISPs provide the framework for secure exchange of clinical messages over the Internet between disparate EHRs. HISPs use Direct protocols and structure an interface to verify Direct addresses and ensure that messages are accurately sent and received on both ends of the exchange.
Health Level 7 (HL7) A non‐profit organization involved in the development of international healthcare informatics interoperability standards. "HL7" is also used to refer to some of the specific standards created by the organization.
Integrating the Healthcare Enterprise (IHE)
An initiative by healthcare professionals and the industry to improve the way computer systems in healthcare share information. IHE promotes the coordinated use of established standards to address specific clinical need in support of optimal patient care.
National eHealth Collaborative (NeHC)
A public‐private partnership focused on accelerating progress toward widespread, secure and interoperable nationwide health information exchange to improve health and healthcare. NeHC’s neutrality and diverse multi‐stakeholder participation provides a unique platform for collaboration. NeHC educates, connects, and encourages healthcare stakeholders to advance health information technology and health information exchange nationwide through its NeHC University web‐based education program, its Consumer Consortium on eHealth, its support of the Nationwide Health Information Network Exchange now known as the eHealth Exchange, its collaborative online community and its ongoing study of leading health information exchanges. National eHealth Collaborative is a cooperative agreement partner of the ONC.

888.879.7302 • www.SuccessEHS.com
Page4
Patient Consent There are five generally accepted models for defining patient consent to participate in an HIE.
The non‐consent model does not require any agreement on the part of the patient to participate
in an HIE. The opt‐out model allows for a predetermined set of data to be automatically included
in an HIE but a patient may still deny access to information in the exchange. The opt‐out with
exceptions exchange enables the patient to selectively exclude data from an HIE, limit
information to specific providers, or limit exchange of information to exchange only for specific
purposes. The opt‐in model requires patients to specifically affirm their desire to have their data
made available for exchange within an HIE. The opt‐in with restrictions model allows patients to
make all or some defined amount of their data available for electronic exchange.
Private HIE The term “private” HIE generally refers to HIEs which operate under the governance of an
integrated delivery network (IDN) or a single healthcare system. The term “enterprise HIE” is
often substituted in this context.
Provider Directory Provider directories are like an electronic “yellow pages” of healthcare providers. A provider
directory is a core requirement for accomplishing secure directed exchange to a previously
unknown entity.
Public Key Infrastructure (PKI)
A PKI (public key infrastructure) enables users of a basically unsecure public network such as the
Internet to securely and privately exchange data and money through the use of a public and a
private cryptographic key pair that is obtained and shared through a trusted authority. The
public key infrastructure provides for a digital certificate that can identify an individual or an
organization and directory services that can store and, when necessary, revoke the certificates.
Push and Send Push and send refers to one‐directional electronic messaging such as those for which “The Direct
Project” has developed standards and specifications for secure transport. In push messaging, as
in email, the receiver of the message must be a known entity.
Query / Retrieve A more advance form of HIE, query/retrieve refers to a messaging pattern in which a query is
initiated from one participating health information organization to another, requesting a list of
available documents meeting the given query parameters for a particular patient for later
retrieval.
Record Locator Service (RLS)
In an HIE, a record locator service is the part of the system that determines what records exist
for a patient‐member and where the source data is located. The record locator service includes
the following distinct functions: managing participating provider identities; maintaining and
publishing a patient index; matching patients using an algorithm; looking up patient record
locations (but not the records themselves); communicating securely and maintaining an audit
log; and managing patient consent to record sharing (under state laws and ARRA).
Regional Health Information Organization (RHIO)
A health information organization that brings together health care stakeholders within a defined
geographic area and governs health information exchange among them for the purpose of
improving health and care in that community.

888.879.7302 • www.SuccessEHS.com
Page5
Registration Authority (RA)
A registration authority (RA) is an authority in a network that verifies user requests for a digital
certificate and tells the certificate authority (CA) to issue it. RAs are part of a public key
infrastructure (PKI), a networked system that enables companies and users to exchange
information and money safely and securely. The digital certificate contains a public key that is
used to encrypt and decrypt messages and digital signatures.
Standards & Interoperability Framework (S&I)
A set of integrated functions, processes, and tools being guided by the healthcare and
technology industry to achieve harmonized interoperability for healthcare information
exchange.
Statewide HIE The state HIE provides alignment of architecture, technology and policy throughout an individual
state. Currently there are fifty‐six states and territories planning and coordinating state level
exchanges through a State Designated Entity. The state HIE typically manages funding provided
by the Office of the National Coordinator (ONC) and assists specific HIEs within the state.
Extensible Markup Language (XML)
A set of rules to encode documents in a machine readable format. XML is used over the Internet
and by web services.