work-related upper limb wrulds - givengain
TRANSCRIPT

in terms of Circular Instruction 180
regarding compensation for work-related
upper limb disorders (WRULDs)
(Compensation for Occupational Injuries
and Diseases Act, 1993
(Act No 130 of 1993), as Amended)
WRULDs
The Compensation
Commissioner’s Guidelines for
Health Practitioners & Employers
to manage
Work-related Upper Limb Disorders

INDEX
SUMMARY: QUICK REFERENCE TO THE EFFECTIVE MANAGEMENT OF WRULDs
SECTION A: INTRODUCTION AND DEFINITION
1 INTRODUCTION 8
1.1 Aim . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
1.2 History . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
1.3 The impact of WRULDs on the economy . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
1.4 Why it is important to prevent WRULDs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
1.5 What is covered by Circular Instruction 180 and what not? . . . . . . . . . . . . . . . 9
1.6 Occupational injuries vs. diseases. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
1.7 Compensation and prevention (COIDA & OHSA/MHSA) . . . . . . . . . . . . . . . . . 10
2 DEFINITION 11
SECTION B-1: FOR HEALTHCARE WORKERS
3 THE CLASSIFICATION OF WRULDS ACCORDING TO SPECIFIC TYPES OF BODY TISSUE 13
3.1 Tendon-related disorders (tendinopathies) . . . . . . . . . . . . . . . . . . . . . . . . . . 13
3.2 Nerve-related disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
3.3 Bursa-related disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
3.4 Blood vessel disorders . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
3.5 Other . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
SECTION B-2: FOR HEALTHCARE WORKERS
4 SHOULDER 17
4.1 Relevant anatomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
4.2 Rotator cuff syndrome (impingement syndrome) . . . . . . . . . . . . . . . . . . . . . . 18
4.3 Other work-related shoulder conditions . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
5 ELBOW 21
5.1 Anatomy of the elbow . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 21
5.2 Lateral humeral epicondylitis (‘tennis elbow’) . . . . . . . . . . . . . . . . . . . . . . . . 22
5.3 Medial epicondylitis (‘golfer’s elbow’) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
5.4 Other elbow conditions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22
6 WRIST, HAND AND FINGER DISORDERS 23
6.1 Anatomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
6.2 De Quervain’s tenosynovitis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23
6.3 Trigger finger / thumb . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
6.4 Carpal tunnel syndrome . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25
6.5 Tendinopathy of the common flexors / extensors . . . . . . . . . . . . . . . . . . . . . . 27
6.6 Other work-related hand and wrist conditions . . . . . . . . . . . . . . . . . . . . . . . . 27
SECTION C-1: FOR HEALTHCARE WORKERS
7 PRINCIPLES OF DIAGNOSIS 29
7.1 Occupational (and other relevant) history, symptoms, signs and
special investigations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 29
7.1.1 Relevant symptoms, clinical signs and progression of the disorder. . . . 29
7.1.2 The history of occupational exposure to the risk factors. . . . . . . . . . . . 31
7.1.3 Relevant facts from the medical, family and social history

as well as the investigation of other potential causes . . . . . . . . . . . . . . 32
7.1.4 Health risk assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
7.1.5 Special investigations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32
7.2 Duration of exposure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
8 MANAGEMENT OF WRULDs 34
8.1 Clinical significance of the diagnosis of tendinosis . . . . . . . . . . . . . . . . . . . . 34
8.2 Treatment modalities. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
8.2.1 Employee education . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 35
8.2.2 Anti-inflammatory strategies. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
8.2.3 Therapeutic strategies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
8.2.4 Reasonable job accommodations . . . . . . . . . . . . . . . . . . . . . . . . . . . . 36
8.2.5 Surgery as a last resort . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
8.3 Algorithms . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 37
Algorithm A . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 38
Algorithm B . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39
Algorithm C . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
9 EVALUATION OF IMPAIRMENT 41
SECTION C-2: FOR THE EMPLOYER
10 REPORTING WRULDs TO THE COMPENSATION COMMISSIONER 43
11 BENEFITS 44
11.1 Temporary total disablement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
11.2 Permanent disablement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
11.3 Medical aid . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
12 CLAIM PROCESSING 44
SECTION D: FOR THE EMPLOYER
13 REPORTING TO THE INSPECTORATE OF LABOUR 46
STEP 1: Notify the Inspectorate of Labour . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
STEP 2: Obtain an ergonomic assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
STEP 3: Compile a plan of action . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
STEP 4: Implement the plan of action and review it at appropriate intervals. . . . . . . . 47
Algorithm D . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 48
SECTION E-1: FOR THE EMPLOYER
14 A PRACTICAL APPROACH TO IDENTIFY AND ASSESS RISKS IN THE WORKPLACE WHICH MAY CAUSE WRULDs 50
14.1 Ergonomics and its practice . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
14.2 Ergonomic analysis – practical steps . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50
14.3 Principles of task/workplace assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . 51
14.3.1 Heed concerns of workers and supervisors . . . . . . . . . . . . . . . . . . . . . 51
14.3.2 Gain better understanding of jobs and tasks . . . . . . . . . . . . . . . . . . . . 51
14.3.3 Identify existing and potential hazards . . . . . . . . . . . . . . . . . . . . . . . . 52
14.3.4 Determine underlying causes of hazards . . . . . . . . . . . . . . . . . . . . . . 52
14.4 Recommend changes and monitor hazard controls (personal protective
equipment, engineering controls, policies, procedures) . . . . . . . . . . . . . . . . . 52
14.5 Workplace observation considerations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
14.6 Assessing working environment for WRULDs. . . . . . . . . . . . . . . . . . . . . . . . . 52
14.6.1 Ergomax risk calculator . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 52
14.6.2 Using the risk calculator . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53

14.7 TASK RISKS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
14.7.1 Highly repetitive movements . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53
14.7.2 Movements requiring force . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 54
14.7.3 Movements at the extremes of reach . . . . . . . . . . . . . . . . . . . . . . . . . 54
14.7.4 Static muscle loading . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
14.7.5 Awkwardly sustained postures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55
14.7.6 Contact stress . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
14.7.7 Vibration. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
14.7.8 Load exposure . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
14.7.9 Cold Exposure. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57
14.8 Additional guidelines to WRULDs assessment. . . . . . . . . . . . . . . . . . . . . . . . 57
14.9 Ergonomic range of motion with safe working zones . . . . . . . . . . . . . . . . . . . 58
14.9.1 Wrist range of motion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
14.9.2 Elbow range of motion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
14.9.3 Shoulder range of motion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58
14.10 HUMAN RISKS – Human variables affecting WRULDs risk exposure . . . . . . . . 59
14.10.1 Gender . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
14.10.2 Age . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
14.10.3 Body mass index (BMI) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
14.10.4 Exposure history . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
14.11 Worked examples . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
14.11.1 Industrial setting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 59
14.11.2 Office setting . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
14.12 Ergonomic intervention strategies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
14.12.1 Deciding how to reduce risks . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 60
14.12.2 Ergonomic principles . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 61
SECTION E-2: FOR THE EMPLOYER
15 OCCUPATIONAL HEALTH PROGRAMME 64
15.1 Health risk assessment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64
15.1.1 Medical surveillance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65
SECTION E-3: FOR THE EMPLOYER
16 NEGOTIATE A POLICY ON THE PREVENTION AND MANAGEMENT OF WRULDs 67
16.1 Aim . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
16.2 Risk assessments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 67
16.3 Information, education and training . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
16.4 Work routine . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
16.5 Notification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
16.6 Responding to diagnosed conditions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68
16.7 Redeployment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
16.8 Monitoring and review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69
SECTION F: AMINISTRATION AND RESOURCES
17 CIRCULAR INSTRUCTION 180 71
18 W.CL 301: FIRST MEDICAL REPORT 74
19 W.CL 302: PROGRESS/FINAL MEDICAL REPORT 77
20 REPORTING – THE CONTACT DETAILS 80
21 GETTING FURTHER ADVICE 82
22 CHECKLIST: WRULDs IN THE WORKPLACE 85
23 BIBLIOGRAPHY 92

FiguresFigure 1. WRULDs is an umbrella term 11
Figure 2. Tendinosis is the painful degeneration of a tendon, typically caused by overuse (e.g. repetitive
movements, etc.), injury or aging 13
Figure 3. Posterior view of the shoulder complex 19
Figure 4. Anterior view of the shoulder complex 20
Figure 5. Anterior view of the muscles that move the wrist, hand and digits 24
Figure 6. Posterior view of the muscles that move the wrist, hand and digits 25
Figure 7. Trigger finger generally results from swelling within a tendon sheath, restricting tendon
motion. A bump (nodule) may also form 26
Figure 8. The carpal tunnel 26
Figure 9. Early detection and prevention of WRULDs are very important. It is important to be on
the look-out for the ‘fog’ – the level of which indicates perception and awareness of
symptoms. The fog may partly obscure a volcano of WRULDs ready to explode! 64
TablesTable 1. Direct and indirect costs associated with WRULDs 9
Table 2. Bonar’s classification of overuse tendon conditions 14
Table 3. The work-relatedness of musculo-skeletal disorders: Physical work risk factors 17
Table 4. Muscles involved in shoulder (glenohumeral and scapular) movements 18
Table 5. Job activities and tasks typically associated with rotator cuff syndrome 18
Table 6. Muscles that move the humerus, radius and ulna 21
Table 7. Job activities and tasks typically associated with elbow conditions 22
Table 8. Muscles involved in hand, wrist and digit movements 23
Table 9. Job activities and tasks typically associated with De Quervain’s tenosynovitis 24
Table 10. Job activities and tasks typically associated with carpal tunnel syndrome 26
Table 11. Job activities and tasks typically associated with tendinopathy of the common flexors /
extensors 27
Table 12. Job activities and tasks typically associated with hand and wrist conditions 27
Table 13. Symptoms and signs of WRULDs 30
Table 14. Progression of WRULDs 30
Table 15. The risks associated with the development of WRULDs are increased by the following home
or work-based activities 31
Table 16. Example of a template to summarise exposure to risk factors 31
Table 17. Work system factors to be assessed 32
Table 18. Common misconceptions about tendinopathies and its management 34
Table 19. Implications of the diagnosis of tendinosis compared with tendonitis 35
Table 20. The following treatment modalities can be utilised depending on the status of the disorder 36
Table 21. The following documentation should be submitted to the Compensation Commissioner by the
employer individually liable or the mutual association concerned 43
Table 22. Various components of an ergonomics survey 47
Table 22. Some of the main measures that employers can take to prevent WRULDs 62

ACKNOWLEDGEMENTSThe Compensation Office is grateful to the members of its Technical Committee on Occupational Diseases (TCOD)
for their valuable contribution in compiling these comprehensive guidelines and Circular Instruction 180.
These guidelines are the result of consultations with various professional interest groups. We are grateful for the
valuable contributions from:
Afrox Occupational Healthcare (Medical Standards Committee)
Chief Inspector of Mines (Dept of Minerals and Energy)
CSIR Mining Technology
Department of Human Kinetics and Ergonomics, Rhodes University
Department of Labour (Occupational Health & Safety)
Department of Public Health (UCT) – Prof Rodney Ehrlich
Ergomax (Pty) Ltd
Ergonomic Society of South Africa (ESSA)
International Ergonomics Society (Section for Industrial Developing Countries)
Mines Occupational Health Advisory Committee (MOHAC)
National Centre for Occupational Health (NCOH)
Occupational Therapy Association of South Africa (OTASA)
Orthopaedic Association of South Africa
South African Chamber of Commerce (SACOB)
South African Society of Occupational Health Nurses (SASOHN)
South African Society of Occupational Medicine (SASOM)
South African Society of Physiotherapy
South African Society of Surgery of the Hand
Sport Science Institute (UCT) – Prof Tim Noakes
Workability Prevention, Assessment & Work Rehabilitation Services
We acknowledge various institutions around the world who gave permission to quote directly from their publications
and for the use of their illustrations.
Any comments or additional information which can assist the Compensation Commissioner in updating and improv-
ing these guidelines, are being welcomed. Please submit comments in electronic format to the medical officers of
the Compensation Commissioner ([email protected]).
DR MMUSO RAMANTSI
Chief Medical Officer
Compensation Commissioner
9 April 2004
Pretoria

SUMMARYQuick reference to the effective management
of WRULDs

Page | 2 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
Definition
WRULDs is a collective term for a
group of occupational diseases that
comprise musculo-skeletal disorders
caused by exposure in the workplace
affecting the muscles, tendons,
nerves, blood vessels, joints and
bursae of the hand, wrist, arm and
shoulder. These are syndromes
associated with characteristic
symptoms and physical signs (e.g.
rotator cuff syndrome, epicondylitis
at the elbow, tenosynovitis and nerve
entrapments such as carpal tunnel
syndrome)
1. What are work-related upper limb disorders(WRULDs)?
Classification of WRULDs according to theeffect on specific tissue
Tendon-related disorders Nerve-related disorders Bursa-related disorders
Blood vessel disorders Other
wor
k-related upper limb disordersRSI
Overusesyndrome
& OCDCTD

Page | 3 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
Shoulder conditions
Fractures around the shoulder
joint
Levator scapulae syndrome
Pectoralis major strains
Rotator cuff syndrome
(Impingement syndrome,
bicipital tendinosis,
infraspinatus tendinosis,
partial tear of the rotator cuff,
subacromial bursitis, subdel-
toid bursitis, subscapularis
tendinosis,
supraspinatus tendinosis)
Rupture of the long head of
the biceps
Elbow conditions
Cubital tunnel syndrome
Lateral humeral epicondylitis
(‘tennis elbow’)
Medial numeral epicondylitis
(‘golfer’s elbow’)
Olecranon bursitis (‘beat
elbow’)
Forearm, wrist, hand and fin-ger conditions
Anterior & posterior
interosseous syndrome
Carpal tunnel syndrome
De Quervain’s tenosynovitis
Guyon (ulnar) tunnel
syndrome
Intersection syndrome
Pronator teres syndrome
Radial tunnel syndrome
Tendinosis / Tenosynovitis of
extensor/flexor tendons
Trigger finger / thumb
White finger (Raynaud’s syn-
drome, vibration syndrome)
2. Some definitive diagnoses of WRULDs*
3. Principles in the diagnosis of WRULDs
(* those marked bold are the more common conditions)
Section 65 (1) (a) of the Compensation for Occupational Injuries and Diseases Act, (No. 130 of 1993) states that
an employee will be entitled to compensation if it is proven to the satisfaction of the Director General that the
employee has contracted a disease mentioned in Schedule 3 and that such a disease has arisen out of and in the
course of his or her employment. Schedule 3 states that musculo-skeletal conditions caused by specific work
activities or a work environment where particular risk factors are present will be regarded as an occupational
disease. Examples of such activities or environment include:
(a) rapid or repetitive motion
(b) forceful exertion
(c) excessive mechanical force concentration
(d) awkward or non-neutral postures
(e) vibration
Compensation for WRULDs caused by exposure to these risk factors are covered in Circular Instruction 180.
Musculo-skeletal diseases which are not of the upper limbs (e.g. neck, lower limbs, etc.) are not covered in the
Compensation Commissioner’s guidelines or in Circular Instruction 180, but can still be reported in terms of
Section 65 (1) (a) of the Compensation for Occupational Injuries and Diseases Act, 1993.

Burning sensation
Fatiguability
Loss of grip strength
Loss of normal sensation
Stiffness and cramps
Muscle weakness
Pain
Paraesthesia (tingling)
Sensation of cold
Swelling
Page | 4 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
WRULDs tend to be progressive and the development of these disorders can be divided into three broad stages:
Stage 1 Pain, aching and tiredness of the limb are experienced during work, but these symptoms improve
overnight. This stage is most often reversible with rest alone. Sometimes guided exercise and
treatment to address muscular problems are required for a cure
Stage 2 Recurrent pain, aching and tiredness of the limb occur earlier in the day, persist at night and
may disturb sleep. Physical signs of the specific disorder (e.g. swelling) may be visible. These
patients should be referred for physiotherapy and ergonomic assessment to prevent recurrence
Stage 3 Persistent pain, aching, weakness and fatigue of the limb are experienced even if the person had
not been working for some time. Sleep is often disturbed. This can be irreversible if not treated
appropriately
Rapid or repetitive motion
Movements requiring force exertion
Excessive mechanical force concentration
Awkward or non-neutral postures (movementsat extremes of reach, static muscle loading,awkwardly sustained postures, contact stress)
Cold environment or handling chilled or frozenproducts
Vibration
Gender (Females are more at risk)
Age (Older employees are more at risk)
Abnormal body mass index
Prolonged duration of exposure
Poor work organisation (low level of controlover work rate, no breaks, etc.)
Psychosocial stress at work and fatigue
History of occupational exposure to risk factors
Relevant symptoms
Family, medical and social history
Progression of WRULDs
4. The Medical Officers in the Compensation Officewill determine if a diagnosis of a WRULD wasmade according to the acceptable medical standards:
Although symptoms will vary according to the type of disorder, common symptoms include the following:

Page | 5 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
Perform special investigations
if it is essential for the accurate diagnosis and treatment of the disorder
to investigate and eliminate other causes
Examples
High resolution ultrasound, X-rays, strength testing, range of motion testing, electromyography (EMG)analysis, isokinetic dynamometry
Get prior authorisation for MRI scans from the Compensation Commissioner
Clinical signs
Health risk assessment supporting the clinical findings
Although clinical signs will vary according to the type of disorder, common signs include the following:
Crepitus (crackling sound in subcuta-neous tissue)
Muscle spasm
Muscle weakness
Reduction in range of movement
Swelling
Tender trigger points in muscles
Tenderness
Please note that:
• Symptoms may not always be accompanied by objective signs.
• Any one symptom or sign on its own is not indicative of WRULDs
and some may be common with normal function.
• Very few sufferers experience all the symptoms.
• The symptoms do not appear in any particular order.
Special investigations
COM
PEN
SATI
ONIS
M
Disability
Disorders, injuriesand diseases
requiring medical interventions
Pronounced symptoms make itdifficult to continue usual
activities
Soreness, pain, persistent aches and painsaffect well-being and performance
Occasional movement or posture problems, intermittent discomfort, fatigue, small aches
Fatigue and tiredness, uneasiness and discomfort generally considered ‘normal’ after a full day’s work
VERSUS PREVEN
TIONISM
5. The importance of preventative strategies
Early detection and prevention of WRULDs are very
important – Koemar (1994) described early signs of
WRULDs as the ‘fog’ slumbering in the valley in front
of the mountain. The ‘fog’ may partly obscure a
volcano of WRULDs ready to explode!

Page | 6 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
Various treatment modalities can be utilised, depending on the status of the disorder. The Compensation
Commissioner will pay for reasonable medical costs once a case has been accepted. A full motivation of the
diagnosis will prevent unnecessary correspondence and delays in adjudication of claim. Health professionals
are encouraged to follow the Compensation Commissioner’s algorithms in managing WRULDs. (See the
Compensation Commissioner’s ‘Guideline for occupational health practitioners & employers to manage work-
related upper limb disorders (WRULDs)’ in terms of Circular Instruction 180)
6. Reporting to the Compensation Commissioner
W. CL. 1 EMPLOYER’S REPORT OF AN OCCUPATIONAL DISEASE OR
W. CL . 305 EMPLOYEE AFFIDAVIT FOR AN OCCUPATIONAL DISEASE (WHEN THE EMPLOYER DOES NOT TIMEOUSLYSUBMIT THE EMPLOYER’S REPORT OF AN OCCUPATIONAL DISEASE (W. CL.1))
W. CL. 14 NOTICE OF AN OCCUPATIONAL DISEASE AND CLAIM FOR COMPENSATION (SIGNED BY THE EMPLOYEE)
W. CL. 110 EXPOSURE HISTORY OR AN APPROPRIATE EMPLOYMENT HISTORY (PLEASE NOTE THAT THE NEW W. CL. 110 FORM SHOULD BE USED)
W. CL. 301 FIRST MEDICAL REPORT IN RESPECT OF A WORK-RELATED UPPER LIMB DISORDER (WRULD)WHEN WRULDS ARE REPORTED, W. CL. 301 MUST BE USED INSTEAD OF THE USUAL W. CL. 22 (FIRSTMEDICAL REPORT IN RESPECT OF AN OCCUPATIONAL DISEASE)
ALL OTHER REPORTS THAT MAY BE RELEVANT TO THE DIAGNOSIS AND TREATMENT OF THE CONDITION (E.G. AN ERGONOMIC ASSESSMENT SUPPORTED BY PHOTOGRAPHS, VIDEO CLIPS, ETC.)
W. CL. 6 RESUMPTION REPORT (EVEN IF THE EMPLOYEE IS AT WORK)
W. CL. 302 PROGRESS/FINAL MEDICAL REPORT IN RESPECT OF A WORK-RELATED UPPER LIMB DISORDER (WRULD)WHEN WRULDS ARE REPORTED, W. CL. 302 MUST BE USED INSTEAD OF THE USUAL W. CL. 26(PROGRESS/FINAL MEDICAL REPORT IN RESPECT OF AN OCCUPATIONAL DISEASE)
As long as the case is open, the employer must submit the following reports on a monthly basis to the Compensation
Commissioner or Mutual Association or employer individually liable, as the case may be, until the employee’s con-
dition has become stabilised, when a Final Medical Report (W.Cl. 302) should be submitted.
The following documentation should be submitted to the Compensation Commissioner, or the employer individual-
ly liable, or the mutual association concerned:
7. Treatment modalities
A. EMPLOYEE EDUCATION
B. ANTI - INFLAMMATORY STRATEGIES
CRYOTHERAPY (ICE)
NON-STEROID ANTI-INFLAMMATORY DRUGS
ELECTROTHERAPEUTIC MODALITIES
(PHYSIOTHERAPY)
INFILTRATION WITH CORTICOSTEROIDS (DUBIOUS
VALUE)
C. THERAPEUTIC STRATEGIES
INITIAL TREATMENT MAY INCLUDE REST
IMMOBILISE – SPLINTAGE (OCCUPATIONAL THERAPY)
MOBILISE (PHYSIOTHERAPY)
MOBILISE – EXERCISE TO APPROPRIATELY
STRENGTHEN MUSCLES (WORKING IN A PROPER
WAY WILL ALSO STIMULATE COLLAGEN
FORMATION)
EDUCATION – GOOD WORK HABITS, PACING, JOINTCONVERSATION TECHNIQUES AND SELF-MANAGEMENT (OCCUPATIONAL THERAPY)
D. REASONABLE JOB ACCOMODATION
TEMPORARY JOB CHANGE
WORK STATION REDESIGN (LAYOUT, HEIGHTS,ETC.)
TOOL AND EQUIPMENT ADAPTATION (CHANGE HANDLE DESIGN, USE OF JIGS, ETC.)
JOB TASK MODIFICATIONS
RETRAINING AND REASSIGNMENT
WORK SCHEDULE MODIFICATIONS
JOB ENLARGEMENT
ROTATION
E. PSYCHOLOGICAL EVALUATION
F. SURGERY (AS LAST RESORT)

SECTION A:Introduction and
Definition

1. Introduction
Page | 8 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
1.1 Aim
The aim of these guidelines is to give the office of the
Compensation Commissioner and health professionals
dealing with work-related upper limb disorders
(WRULDs) guidance on how to define, diagnose,
manage and report these disorders. It also advises
employers on preventative measures to be taken where
such disorders occur in the workplace and how to
report these to the Department of Labour.
1.2 History
Work-related upper limb disorders (WRULDs) are not a
new phenomenon. They were identified as long ago as
1713 by Ramazzini, an Italian doctor generally
regarded as the father of occupational medicine, who
recognised that serious disease could be caused by
“violent and irregular motions and unnatural postures
of the body”. Ramazzini described symptoms of
WRULD in scribes and clerks, noting that the
“incessant driving of the pen over paper causes
intense fatigue of the hand and the whole arm because
of the continuous strain of the muscles and tendons.”
In the 19th century the condition was recorded
amongst artists, musicians, seamstresses, milkmaids
and smiths. A range of popular terms exists to
describe musculo-skeletal problems associated with
particular occupations: telegraphist’s cramp, hop
picker’s gout, fisherwoman’s finger, upholsterer’s
hand, gamekeeper’s thumb, cotton-twister’s hand,
tennis elbow and, more recently, pizza-cutter’s wrist
and Nintendonitis.1 More recently alternative terms
have been used, i.e. overuse syndrome, repetitive
strain injury (RSI) and cumulative trauma disorder
(CTD). Circular Instruction 180 uses the umbrella
term, work-related upper limb disorders.
Recently musculo-skeletal disorders affecting the upper
limbs have received considerable attention around the
world, following financial claims for damages from
employees considered to have developed WRULDs.
Important differences of opinion still exist, for instance as
to how the disorders should be defined. The term
‘repetitive strain injury’ (RSI) is medically imprecise. A
more descriptive title would be ‘regional pain syndrome’.2
Controversy also arises as to whether certain disorders,
such as carpal tunnel syndrome, are related to workplace
ergonomic factors. Although some of these conditions are
known to be related to non-occupational causes, such as
pregnancy or rheumatoid arthritis, occupational factors
play an important aetiological role in other cases.3
Most of the information regarding WRULDs is
available from developed countries and although many
recommendations will be applicable to developing
countries, there is a need for research on WRULDs in
the South African context. This is particularly
pertinent in industrially developing countries (IDCs)
where there is a high prevalence of manual labour.
This is likely to result in more musculo-skeletal
disorders than is reported in advanced countries.4
1.3 The impact of WRULDs on the economy
No statistics are available for South Africa regarding
the impact of WRULDs on health care and the
economy.5 However, internationally WRULDs are
having an alarming impact, causing significant
occupational health problems, estimated to affect many
millions of employees annually.6
The Unites States of America’s Bureau of Statistics
(1999) reported that among major disabling injuries
and illnesses, the average days away from work were
highest for carpal tunnel syndrome (27 days),
fractures (20 days), and amputations (18 days). Among
the leading events and exposures, repetitive motion
such as grasping tools, lifting bricks and typing,
resulted in the longest absences from work – an
average of 17 days. Conservative estimates calculate
the cost of work-related musculo-skeletal disorders in
the USA at between $13 and $20 billion annually.7
There is substantial evidence within the European
Union that WRULDs are a significant problem with
respect to ill health and associated costs within the
workplace. It is likely that the size of the problem will
increase as more employees are becoming exposed to
1 London Hazard Centre (1997). Ch 4, p1.
2 NIOSH (1997). p 23.
3 HSE (1996). Introduction, p 1.
4 Scott P et al. (2002)
5 SAMOSA (2002)
6 Personal communication – Prof PA Scott, Department of Human Kinetics and
Ergonomics, Rhodes University, South Africa
7 NIOSH (1997)

Page | 9 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
workplace risk factors for these disorders within the
European Union.8
Where data do exist (e.g. in the Nordic countries and
the Netherlands) the cost has been estimated at
between 0.5% and 2% of Gross National Product.9
In Britain, the Health and Safety Executive (HSE)
estimated that WRULDs incurred approximate costs of
£1.25 billion per year10.
Although there are limited records on the incidence of
WRULDs in South Africa, it is very likely to be
substantially higher than that reported for the USA
and Europe. This is due to the excessive physical
demands placed on employees in industrially
developing countries.
The direct costs for compensation of musculo-skeletal
disorders are appreciated far more than the indirect
costs associated with disruptions in productivity and
quality, worker replacement costs, training and other
work absence costs. It is believed that the direct costs
due to compensated work-related musculo-skeletal
disorders are a relatively low proportion of the total
costs.11
1.4 Why it is important to prevent WRULDs
WRULDs may have severe consequences if prompt
action is not taken, such as:
Decreased productivity due to pain and increased
fatigue.
Inability to work. Well motivated and productive
people have had to give up work because of pain
and disablement from WRULDs. Others have been
so badly affected that simple household tasks
become difficult.
Lost production when employees take time off
sick.
Compensation claims from those who have to stop
working because of WRULDs.
The Occupational Health and Safety Act and the
Mine Health and Safety Act require employers to
assess health and safety risks, and to put meas-
ures in place to ensure the health and safety of
employees.
Failure to comply could lead to legal action against
the employer by the Department of Labour, who
administers the Occupational Health and Safety
Act, or the Department of Minerals and Energy,
who administers the Mine Health and Safety Act.
1.5 What is covered by Circular Instruction180 and what not?
Section 65 (1) (a) of the Compensation for
Table 1. Direct and indirect costs associated with WRULDs
DIRECTCOSTS ±20%
MEDICAL EXPENSES
EMPLOYEES COMPENSATION PREMIUMS
LOST WORKDAYS
PAID LEAVE
INDIRECTCOSTS ±80%
LOSS OF INJURED WORKER’S PRODUCTION
TIME LOST BY UNINJURED EMPLOYEES
TEMPORARY RE-PLACEMENT
TRAINING AND RE-TRAINING
REPORTING AND CLAIMS
MANAGEMENT TIME
WORKER / MANAGEMENT DISCUSSIONS
LITIGATION PROCESSES
8 European Agency for Safety and Health at Work (1999). Summary p. 7
9 European Agency for Safety and Health at Work (1999). Ch 2.3, p. 23
10 HSE (1996). Ch 2.3, p. 23
11 Hagberg M et al. (1995).

Occupational Injuries and Diseases Act, (No. 130 of
1993) states that an employee will be entitled to
compensation if it is proven to the satisfaction of the
Director General that the employee has contracted a
disease mentioned Schedule 3 and that such a
disease has arisen out of and in the course of his or
her employment. Schedule 312 states that musculo-
skeletal diseases caused by specific work activities or
work environment where particular risk factors are
present will be regarded as an occupational disease.
Examples of such activities or environment include:
(a) rapid or repetitive motion
(b) forceful exertion
(c) excessive mechanical force concentration
(d) awkward or non-neutral postures
(e) vibration
Compensation for WRULDs caused by exposure to these
risk factors are covered in Circular Instruction 180.
Musculo-skeletal diseases which are not of the upper
limbs (e.g. neck, lower limbs, etc.) are not covered in
these guidelines or in Circular Instruction 180, but
can still be reported in terms of Section 65 (1) (a) of
the Compensation for Occupational Injuries and
Diseases Act, 1993.
It is necessary to emphasise the importance of referring
employees to adequately trained and experienced
health professionals when a WRULD is suspected.
These include occupational medicine practitioners,
physiotherapists, occupational therapists, ergonomists,
and orthopaedic specialists, amongst others.
1.6 Occupational injuries vs. diseases
A case of WRULD will be regarded as an occupational
disease and not as an ‘injury’ – and should therefore
be reported as such.
However, if a case of WRULD develops as a result of
an occupational injury (e.g. a fracture into the wrist
joint with the consequent development of carpal
tunnel syndrome), the WRULD should be considered
part of the injury and the Compensation Commissioner
should be notified in the subsequent progress reports
of the occupational injury.
1.7 Compensation and prevention (COIDA & OHSA/MHSA)
WRULDs must be reported to the Compensation
Commissioner so that payment of medical costs, sick
leave and compensation can be considered in terms of
the COID Act (Table 20, p. 43).
WRULDs should also be reported to the Provincial
Executive Manager of Labour (in terms of the Occu-
pational Health and Safety Act) or to the Regional
Principal Inspector of Mines (in terms of the Mine
Health and Safety Act) so that they can ascertain
whether the health hazards causing this disease were
reduced through ergonomic improvement.
Useful forms and templates are included as addenda
to these guidelines. These templates may be used or
adapted to suit individual circumstances. It is not
compulsory to use these forms or templates, but it is
highly recommended.
Page | 10 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
12 Amendment of Schedule 3 as published in Government Gazette [Number 26302 – 30 April 2004]

2. Definition
Work-related upper limb disorders are occupationally-
induced conditions that develop over time to affect
the musculo-skeletal and peripheral nervous system of
the upper limbs.
Previously a number of other terms have been used
which probably describe the same entities, but in the
strictest sense do not overlap completely,13 such as
repetitive strain injury (RSI), cumulative trauma
disorder (CTD), occupational overuse syndrome (OOS),
occupational cervico-brachial disorder (OCD), etc. For
the purpose of this instruction the umbrella term,
work-related upper limb disorders (WRULDs), will be
used. This can be represented simply by Figure 1
(HSE, 1996) shown below.
The symptoms of pain and loss of motion can be the
result of fatigued muscles, overloaded muscles,
muscle imbalances, degeneration of tendons and their
attachments, inflamed tendon sheaths or compressed
nerves.
There is controversy surrounding the work-relatedness
of many musculo-skeletal disorders, and it is likely
that many of those reported in the workplace have a
multifactorial origin with psychosocial and contribut-
ing individual factors. There is, however, strong
evidence of a causal relationship between at least
some of these conditions, and repetitive, forceful work
involving the body parts affected and/or the sustained
postures adopted during work.
Circular Instruction 180 states that WRULDs are caused,
aggravated or precipitated by one or more of the
following risk factors, singly or in combination:
Highly repetitive movements
Movements requiring force
Movements at the extremes of reach
Static muscle loading
Awkwardly sustained postures
Contact stress (e.g. uncomfortable gripping and
twisting, sharp edges to hand tools, desk edges, etc.)
Vibration
In terms of this instruction, upper limb musculo-
skeletal disorders will be presumed to be work-related
(Table 3, p. 17) if the nature of the work performed
includes exposure to the relevant risk factors.
Work-related musculo-skeletal disorders of body parts
other than the upper limbs are not covered in Circular
Instruction 180 or these guidelines, but it will be con-
sidered in terms of Section 65 (1) (b) of the Compens-
ation for Occupational Injuries and Diseases Act.
Page | 11 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
wor
k-related upper limb disordersRSI
Overusesyndrome
& OCDCTD
Figure 1. WRULDs is an umbrella term
WRULDs is a collective term for a group of occupational
diseases that comprise musculo-skeletal disorders caused by
exposure in the workplace affecting the muscles, tendons,
nerves, blood vessels, joints and bursae of the hand, wrist, arm
and shoulder. These are syndromes associated with
characteristic symptoms and physical signs (e.g. rotator cuff
syndrome, epicondylitis at the elbow, tenosynovitis and nerve
entrapments such as carpal tunnel syndrome).
13 HSE (1996). Section 1, p 1.

SECTION B-1:For healthcare workers
Classification

3. The classification of WRULDs according to specific types of body tissue
WRULDs can be classified according to the
specific types of body tissue that are involved.14
Various degrees of, and variations of the following
conditions can be the result of overuse:
Tendon-related disorders
Nerve-related disorders
Bursa-related disorders
Blood vessel disorders
Other
Page | 13 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
14 European Agency for Safety and Health at Work (1999). Ch 2.1, p 16.
15 Personal communication with Prof Tim Noakes (UCT Sports Science Institute)
16 Used with the permission of Mayo Foundation for Medical Education and
research (© 1998–2002)
17 Khan, K (2000).
18 Perugia L et al (1986 )
19 Evans, G (1997)
One factor that may interfere with optimal treatment
is that common tendinopathies may be mislabelled as
tendonitis. Advances in the understanding of tendon
pathology indicate that conditions that have been tra-
ditionally labelled as lateral epicondylitis, rotator cuff
tendonitis, etc., are in fact tendinosis. An increasing
body of evidence supports the notion that these over-
use tendon conditions do not involve inflammation
(“-itis”), but collagen degeneration (“-osis”). If this is
correct, then the traditional approach to treating
tendinopathies as an inflammatory tendonitis is likely
to be flawed.17
Tendinosis is intratendinous collagen degeneration
commonly due to aging, microtrauma (e.g. chronic
overuse with repetitive movements), or vascular com-
promise.
The term tendinosis was first used by German
researchers in the 1940s. Perugia18 noted the
‘remarkable discrepancy between the terminologies
generally adopted for these conditions (which are
obviously inflammatory since the ending itis is used)
and their histopathologic substratum, which is largely
degenerative.’
Thus, occupational health practitioners must shift
their perspective and acknowledge that tendinosis is
the pathology being treated in most cases and that
treatment needs to combat collagen breakdown rather
than inflammation. Tendinosis may require a reason-
able period of relative rest and attention to strength-
ening with the aim of first breaking the tendinosis
cycle. Once this is done, the patient uses modalities
that optimise collagen production and maturation so
that the tendon achieves the necessary tensile
strength for normal function.
Examples: Epicondylitis (tennis and golfer’s elbow),
rotator cuff impingement syndrome of the shoulder, etc.
Tenosynovitis: Rapid, repetitive movements of the
upper extremities, particularly the hands and fingers,
can cause inflammation of the synovial lining of the
tendon sheath.19 The consequent swelling causes pain
and impedes movement of the tendon in the sheath.
3.1 Tendon-related disorders(tendinopathies)
Khan (2000) and Noakes (2002)15 stated that numerous
investigators worldwide have shown that the pathology
underlying overuse tendinopathies is primarily tendi-
nosis (i.e. collagen degeneration).
Figure 2. Tendinosis is the painful degeneration of a tendon, typicallycaused by overuse (e.g. repetitivemovements, etc.), injury or aging16
Bursa
Muscle
Tendon
© Mayo Foundation for Medical Education and Research. All rights reserved.

It is called tenosynovitis. Repeated exposure ultimately
causes the growth of scar tissue and results in pain,
reduced mobility and weakness. 20
Examples: Trigger finger, De Quervain’s tenosynovitis,
etc.
Tendonitis is inflammation of tendons and of tendon-
muscle attachments.21 It is a rather rare condition,
but may occur occasionally in the Achilles tendon in
conjunction with a primary tendinosis.22 Many
clinicians and medical publications still mistakenly
use the term tendonitis (inflammation), when they
actually mean tendinosis (degeneration).
3.2 Nerve-related disorders
Repeated or prolonged pressure or irritation can cause
damage to the nerve that supplies the muscle or
passes through it. The nerve irritation causes paraes-
thesia (numbness, tingling) and changes in sensation
in the areas supplied by the nerve.23
Examples: Carpal tunnel syndrome (by far the most
common), cubital tunnel syndrome, Guyon tunnel
syndrome, pronator teres syndrome, radial tunnel
syndrome, anterior interosseous nerve syndrome,
posterior interosseous nerve entrapment etc.
3.3 Bursa-related disorders
Bursas are ‘cushions’ which protect muscles, tendons
and skin from friction against bones (e.g. at the elbow
and shoulder, during movements of the joints).24 (See
Figure 2). Overexertion can lead to inflammation in
these bursas and causes a dull aching pain, called
bursitis.25 It can also cause an effusion within the sac
of the bursa.
Examples: Olecranon bursitis (beat elbow), subacro-
mial burisits, subdeltoid bursitis, etc.
3.4 Blood vessel disorders
Work-related blood vessel disorders are usually due to
vibration or hammering. Exposure to vibration at the
hand interface and its effects on biological tissues are
well established and it is generally recognised that
excessive exposure may result in disturbances to
Page | 14 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
Table 2. Bonar’s classification of overuse tendon conditions
PATHOLOGIC MACROSCOPIC HISTOLOGICAL F INDINGDIAGNOSIS PATHOLOGY
TENDINOSIS INTRATENDINOUS DEGENERATION COLLAGEN DISORIENTATION, DISORGANISATION, AND FIBRE
COMMONLY DUE TO AGING, MICRO- SEPARATION BY INCREASED MUCOID GROUND SUBSTANCE,
TRAUMA, OR VASCULAR COMPROMISE INCREASED PROMINENCE OF CELLS AND VASCULAR SPACES
WITH OR WITHOUT NEOVASCULARISATION, AND FOCAL
NECROSIS OR CALCIFICATION
PARTIAL RUPTURE SYMPTOMATIC DEGENERATION OF THE DEGENERATIVE CHANGES AS NOTED ABOVE WITH SUPER-
OR TENDINIT IS TENDON WITH VASCULAR DISRUPTION, IMPOSED EVIDENCE OF TEAR, INCLUDING FIBROBLASTIC AND
INFLAMMATORY REPAIR RESPONSE MYOFIBROBLASTIC PROLIFERATION, HAEMORRHAGE, AND
ORGANISING GRANULATION TISSUE
PARATENDONITIS INFLAMMATION OF THE OUTER LAYER MUCOID DEGENERATION IS SEEN IN THE AREOLAR TISSUE: A
( INCLUDING OF THE TENDON (PARATENDON) ALONE SCATTERED MILD MONONUCLEAR INFILTRATE WITH OR
TENOSYNOVIT IS) WHETHER OR NOT THE PARATENDON WITHOUT FOCAL FIBRIN DEPOSITION AND FIBRINOUS EXUDATE
IS LINED BY SYNOVIAL
PARATENDONITIS PARATENDONITIS ASSOCIATED WITH DEGENERATIVE CHANGES AS NOTED IN TENDINOSIS WITH
( INCLUDING INTRATENDINOUS DEGENERATION MUCOID DEGENERATION WITH OR WITHOUT FIBROSIS AND
TENOSYNOVIT IS) SCATTERED INFLAMMATORY CELLS IN THE PARATENON
WITH TENDINOSIS ALVEOLAR TISSUE
20 Bridger, RS (1995). p. 135
21 HSE (1996). Ch 3, p. 5
22 Khan, K (2000)
23 Bridger, RS (1995). p. 136
24 Bridger, RS (1995). p. 136
25 House of Commons (1998). p. 12
Source: Khan (2000)

finger blood circulation and also neurological and
locomotor functions of the hand and arm.26&27
Examples: Raynaud’s phenomenon, hand-arm vibra-
tion syndrome, hypothenar hammer syndrome, etc.
3.5 Other
The effect of work on muscles and joints are problem-
atic (e.g. static loading can cause muscle imbal-
ances28 and trigger points29). (Keep in mind that
static loading of proximally situated muscles may be
more affected than tendons situated more distally).
Muscles and joints form, per definition, part of upper
limb disorders, such as tension neck syndrome,
muscle sprain and strain (biceps strain, torn
muscles), myalgia and myositis, and osteoarthritis.
But the effect of work on muscles and joints are very
controversial and fall outside the scope of these
guidelines. The same applies to musculo-skeletal
‘injuries’, because in these guidelines we are only
dealing with ‘occupational diseases/disorders’ of the
upper limb.
Page | 15 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
26 European Agency for Safety and Health at Work (1999). Ch 5.6, p. 70
27 Mennen (1999)
28 Pheasant et al. (1991)
29 MacKinnon et al. (1997)

SECTION B-2:For healthcare workers
Shoulder, Elbow, Wrist,Hand and Fingers

CARPAL TUNNEL SYNDROME
TENDINOSIS
HAND-ARM VIBRATION SYNDROME
SHOULDER
4. Shoulder
4.1 Relevant anatomy
Healthy shoulder function is essential for many work-ing tasks. Manual materials handling (MMH) tasks,particularly those involving lifting and lowering ofloads, may place considerable cumulative stress onthe shoulder joint. Sound knowledge of the functionalanatomy and dynamic forces acting around the shoul-der joint is important to understand the pathologicalprocesses that commonly affect this area. The shoul-der (glenohumeral) joint is a ball and socket joint and
stability of this joint is provided by static and dynam-
ic constraints. Static constraints include the gleno-
humeral ligaments, glenoid labrum and capsule. The
dynamic constraints are predominantly the rotator
cuff musculature (refer Figure 3. p.17 and Figure 4,
p. 18). An understanding of the musculature involved
in certain shoulder movements will help to determine
the structures likely to be more strained. Presented in
Table 4 are movements of the shoulder complex and
the muscles involved in these movements.
Page | 17 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
BODY PART STRONG EVIDENCE EVIDENCE INSUFFICIENT EVIDENCE OF RISK FACTOR EVIDENCE NO EFFECT
Table 3. The work-relatedness of musculo-skeletal disorders: Physical work risk factors
NECK AND NECK/SHOULDER
REPETITION QFORCE QPOSTURE QVIBRATION Q
REPETITION QFORCE QPOSTURE QVIBRATION Q
REPETITION QFORCE QPOSTURE QCOMBINATION QHAND/WRIST
ELBOW
REPETITION QFORCE QPOSTURE QVIBRATION QCOMBINATION Q
REPETITION QFORCE QPOSTURE QCOMBINATION Q
VIBRATION QSource: NIOSH (1997)

Page | 18 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
30 Bridger RS. (1995). Ch 5, p. 140 31 Uhthoff HK et al. (1991)
4.2 Rotator cuff syndrome (impingement syndrome)
The shoulder is particularly prone to damage where
persons are executing repetitive overhead move-
ments.30 The same applies to static loading and/or sus-
tained postures. They are prone to develop bursal side
tears secondary to impingement in the rotator cuff
region.31 (See Figure 2, p.14)
Table 4. Muscles involved in shoulder (glenohumeral and scapular) movements
MOVEMENT PRIME MOVERS SECONDARY MOVERS
FLEXION ANTERIOR DELTOID PECTORALIS MAJOR (CLAVICULAR HEAD)
CORACOBRACHIALIS
EXTENSION LATISSIMUS DORSI TERES MINOR
TERES MAJOR TRICEPS
POSTERIOR DELTOID
ABDUCTION MID DELTOID ANTERIOR/POSTERIOR DELTOID
SUPRASPINATUS SERRATUS ANTERIOR
ADDUCTION PECTORALIS MAJOR TERES MAJOR
LATISSIMUS DORSI
EXTERNAL ROTATION INFRASPINATUS POSTERIOR DELTOID
TERES MINOR
INTERNAL ROTATION SUBSCAPULARIS ANTERIOR DELTOID
PECTORALIS MAJOR
LATISSIMUS DORSI
TERES MAJOR
GLE
NO
HU
ME
RA
L
RETRACTION RHOMBOID MAJOR/MINOR
TRAPEZIUS
PROTRACTION SERRATUS ANTERIOR PECTORALIS MINOR
UPWARD ROTATION TRAPEZIUS
SERRATUS ANTERIOR
DOWNWARD ROTATION RHOMBOIDS LATISSIMUS DORSI
PECTORALIS MINOR
ELEVATION TRAPEZIUS
LEVATOR SCAPULAE
RHOMBOIDS
DEPRESSION LATISSIMUS DORSI
PECTORALIS MINOR
SC
AP
ULA
R
Source: Scott, P. et al. (2002)
Table 5. Job activities and tasks typically associated with rotator cuff syndrome
B E LT C O N V E Y O R A S S E M B LY
L I F T I N G
PA C K I N G
C A R R Y I N G L O A D O N S H O U L D E R S
O V E R H E A D A S S E M B LY
P U N C H P R E S S O P E R AT I O N
C O N S T R U C T I O N W O R K
O V E R H E A D PA I N T I N G
R E A C H I N G
E L E C T R I C A L W O R K
O V E R H E A D W E L D I N G
W O R K W I T H T H E A R M S AW AY F R O M T H E B O D Y
Source: Guild R, et al. (2001)

Figure 3. Posterior view of the shoulder complex35
Page | 19 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
Shoulder pain exacerbated by abduction against
resistance is a sign of rotator cuff lesions. Although an
active range of movement of the joint is limited by
pain, passive range of motion remains approximately
normal.32 Acute rotator cuff tendinosis is diagnosed if
the symptoms are of 12 weeks duration or less.
Chronic rotator cuff rupture presents a marked
difficulty initiating abduction with weakness and
limitation of movement.33 Pain is usually experienced
towards the end of the active range of movement.34 An
understanding of the ‘painful arc’ is a useful diagnos-
tic tool. Pain is usually reproduced in the range of 70o
to 120o abduction.
Rotator cuff syndrome (impingement syndrome)includes the following conditions:
Bicipital tendinosis
Infraspinatus tendinosis
Partial tear of the rotator cuff
Subacromial bursitis
Subdeltoid bursitis
Subscapularis tendinosis
Supraspinatus tendinosis
Tendonisis of the shoulder
4.3 Other work-related shoulder conditions
Rupture of the long head of the biceps
Pectoralis major strains
Levator scapulae syndrome
Fractures around the shoulder joint
32 Cyriax J (1988)
33 Vecchio P et al. (1995)
34 Cyriax J (1988)
35 Taken from Tortora (2002)
First thoracic vertebra
ClavicleAcromion of scapula
Spine of scapula
DELTOID
Long head of triceps brachii
SUPRASPINATUS (cut)
Scapula
TERES MAJORCORACOBRACHIALIS
Humerus
LATISSIMUS DORSI
Spinous process offirst lumbar vertebra
Iliac crestThoracolumbar fascia
Levator scapulae (cut)
RHOMBOIDEUS MINOR (cut)
DELTOID (cut)
INFRA-SPINATUS
TERES MINORRHOMBOIDEUS MAJOR (cut)
TERES MAJOR
Humerus

Figure 4. Anterior view of the shoulder complex36
Page | 20 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
36 Taken from Tortora (2002)
DELTOID (cut)
SUPRASPINATUS
SUBSCAPULARIS
PECTORALIS MAJOR (CUT)
TERES MAJOR
Biceps brachii (cut)CORACOBRACHIALIS
LATISSIMUS DORSI
Brachialis
Biceps brachii (cut)
Radius
Ulna
10th rib
Internal intercostals
External intercostals
Serratus anterior
Sternum
Pectoralis minor
PECTORALIS MAJOR (cutcut)
2ND ribSerratus anterior
Coracoid process of scapulaSubclaviusClavicle

5. Elbow
5.1 Anatomy of the elbow
Use of the upper limb during many work activities
demands a well-functioning elbow. Refer to Figure 3,
Figure 4, Figure 5 and Figure 6 while reading through
the table below which lists the muscles involved in
the movement of the humerus, radius and ulna.
Epicondylitis is a common and well-defined clinical
entity affecting the elbow. It is a tendinosis charac-
terised by pain at the epicondyle, due to intratendi-
nous degeneration of the tendon-bone attachment. It
is more frequent laterally (‘tennis elbow’) than
medially (‘golfer’s elbow’). Epicondylitis is due to
unusual force, repetition, forceful gripping or
repeated supination and pronation.37
Entrapment neuropathies of the forearm should
always be suspected with ‘resistant’ tennis elbow
(e.g. radial tunnel syndrome can mimic lateral
epicondylitis).38
Page | 21 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
Table 6. Muscles that move the humerus, radius and ulna
MOVEMENT PRIME MOVERS SECONDARY MOVERSFLEXION PECTORALIS MAJOR (CLAVICULAR HEAD)
ANTERIOR DELTOID
CORACOBRACHIALIS
EXTENSION PECTORALIS MAJOR (STERNOCOSTAL HEAD)
LATISSIMUS DORSI
POSTERIOR DELTOID
TERES MAJOR
TERES MINOR
ABDUCTION LATERAL DELTOID SUPRASPINATUS
ADDUCTION PECTORALIS MAJOR INFRASPINATUS
LATISSIMUS DORSI TERES MAJOR
TERES MINOR
CORACOBRACHIALIS
MEDIAL ROTATION PECTORALIS MAJOR TERES MAJOR
LATISSIMUS DORSI
ANTERIOR DELTOID
SUBSCAPULARIS
LATERAL ROTATION POSTERIOR DELTOID
INFRASPINATUS
TERES MINOR
HU
ME
RU
S
F LEXION BICEPS BRACHII
BRACHIALIS
BRACHIORADIALIS
EXTENSION TRICEPS BRACHII
ANCONEUS
PRONATION PRONATOR TERES
PRONATOR QUADRATUS
SUPINATION SUPINATORRA
DIU
S A
ND
ULN
A
Source: Scott et al. (2002)
37 HSE (1996). Ch 4, p. 1 38 HSE (1996)

5.2 Lateral humeral epicondylitis (‘tenniselbow’)
Lateral elbow pain is very common in manual employ-
ees with the most common cause being overuse. This
condition has traditionally been referred to as ‘lateral
epicondylitis’. The primary pathological process
involved in this condition is degeneration of the
extensor carpi radialis brevis (refer Table 6 and Table
8). Although a common disorder, there are many other
injuries which can affect the elbow and which impede
movements of the humerus, radius and ulna.39
Wrist dorsiflexion, such as in the power grasp, and
exposure of the arms to high forces and repetitive
tasks can lead to degeneration at the attachment of
the extensor muscles of the wrist to the lateral
humeral epicondyle.
This condition also often starts with an acute direct
injury to the site of the muscle origin which progresses
to an epicondylitis.
5.3 Medial epicondylitis (‘golfer’s elbow’)
Overuse of the finger flexors and the wrist
flexors/pronators, as in repetitive work with the elbow
flexed, leads to pain in the common proximal flexor
origin on the medial aspect of the elbow.40
5.4 Other elbow conditions
Olecranon bursitis (beat elbow)41
Cubital tunnel syndrome
Page | 22 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
39 Scott, P. et al (2002)
40 Williams N (1993) 41 HSE (1996). Ch 4, p. 11
Table 7. Job activities and tasks typically associated with elbow conditions
EPICONDYLIT IS
DRILLERS
CARPENTERS
POLISHERS
TURNING SCREWS
SMALL PARTS ASSEMBLY
HAMMERING
REPETITIVE WRIST EXTENSION
REPETITIVE WRIST GRASP
COMPUTER USERS
CUBITAL TUNNELSYNDROME
RESTING FOREARM NEAR ELBOW ON A HARD SURFACE
RESTING FOREARM NEAR ELBOW ON SHARP EDGE
RESTING FOREARM NEAR ELBOW WHILE REACHING OVER OBSTRUCTION
REPETITIVE OR STATIC ELBOW FLEXION
Source: Bridger (1995); Guild et al. (2001)

6. Wrist, hand and finger disorders
6.1 Anatomy
Although the wrist and hand are frequently trauma-
tised during work, there is a tendency to overlook the
severity of the injuries to these areas, with the result
that a number of important conditions are not
diagnosed. Overuse conditions to the wrist are
common, while direct trauma to the hand and digits is
another concern. Presented in Figure 5 (p. 24) and
Figure 6 (p. 25) are the musculature of the wrist,
hand and digits. The anterior compartment muscles
function as flexors, and the posterior compartment
muscles function as extensors. Outlined below in
Table 8, are the muscles involved in various wrist,
hand and digit movements.
6.2 De Quervain’s tenosynovitis
De Quervain’s tenosynovitis is sometimes called
stenosing tenosynovitis of the abductor pollices
longus and extensor pollices brevis tendons. The
patient presents with pain over the styloid process of
the radius. A common and well-recognised variant of
De Quervain’s tenosynovitis is characterised by a
localised swelling at the base of the thumb and thick-
ening of the fibrous sheath or reticulum. Sometimes a
palpable nodule, of which the precise cause is
unknown, can be felt in the course of the abductor
pollicis longus and extensor pollicis brevis tendons.42
This condition can result from overuse of the thumb,
such as in the repetitive grasping of a straight handled
Page | 23 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
42 HSE (1996). Ch 4, p. 6
Table 8 Muscles involved in hand, wrist and digit movements
MOVEMENT PRIME MOVERS SECONDARY MOVERS
FLEXION FLEXOR CARPI RADIALIS
FLEXOR CARPI ULNARIS PALMARIS LONGUS
FLEXOR DIGITORUM PROFUNDUS
EXTENSION EXTENSOR CARPI RADIALIS
EXTENSOR CARPI RADIALIS BREVIS
EXTENSOR DIGITORUM
EXTENSOR CARPI ULNARIS
EXTENSOR POLLICIS BREVIS
EXTENSOR INDICIS
ABDUCTION ABDUCTOR POLLICIS LONGUS FLEXOR CARPI RADIALIS
EXTENSOR CARPI RADIALIS
EXTENSOR POLLICIS LONGUS
ADDUCTION FLEXOR CARPI ULNARIS
EXTENSOR CARPI ULNARIS
TH
E W
RIS
T A
ND
HA
ND
F LEXION FLEXOR DIGITORUM SUPERFICIALIS (MIDDLE PHALANX)
FLEXOR POLLICIS LONGUS (THUMB)
FLEXOR DIGITORUM PROFUNDUS
EXTENSION EXTENSOR DIGITORUM
EXTENSOR DIGITI MINIMI (L ITTLE FINGER)
EXTENSOR POLLICIS BREVIS (THUMB) ABDUCTOR POLLICIS BREVIS (THUMB)
EXTENSOR POLLICIS LONGUS (THUMB)
EXTENSOR INDICIS ( INDEX FINGER)
ABDUCTION ABDUCTOR POLLICIS LONGUS (THUMB)
DIG
ITS
Source: Scott et al. (2002)

tool (e.g. screwdriver, endo files of dentist). The
tendons of the muscles of the forearm are stretched
and rub against the radial styloid, causing inflamma-
tion of the tendon sheath and leading to pain and
localised swelling (tenosynovitis of the first dorsal
compartment of the wrist) over the lateral aspect of
the distal radius.43 Incidentally, this condition is also
common in post-partum women.
Diagnostic criteria suggest pain and tenderness
localised to the radial aspect of the wrist plus a
positive Finkelsteins’s test (ask patient to make a fist
over his thumb, and ulnarly deviating wrist – sharp
pain at this site is produced by active extension and
abduction of the thumb against resistance).44
Page | 24 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
43 Bridger RS (1995). p. 145
44 HSE (1996). Ch 4, p. 6 45 Taken from Tortora (2002)
Figure 5. Anterior view of the muscles that move the wrist, hand and digits45
Table 9. Job activities and tasks typically associated with De Quervain’s tenosynovitis
B U F F I N G
G R I N D I N G
P O L I S H I N G
S A N D I N G
E N D O F I L I N G ( D E N T I S T )
P U S H I N G
P R E S S I N G
S AW I N G
U S E O F P L I E R S
U S E O F S M A L L T O O L S
‘ T U R N I N G ’ C O N T R O L S A S O N M O T O R C Y C L E
I N S E R T I N G S C R E W S I N H O L E S
F O R C E F U L H A N D W R I N G I N G
Source: Guild et al. (2001)
Biceps brachii
Brachialis
Brachial arteryMedian nerve
PRONATOR TERESBRACHIORADIALIS
SUPINATORPALMARIS LONGUSFLEXOR CARPI RADIALISFLEXOR CARPI ULNARIS
PRONATOR TERES (cut)
FLEXOR DIGITORUM SUPERFICIALIS
FLEXOR POLLICIS LONGUS
ABDUCTOR POLLICIS LONGUS
PRONATOR QUADRATUS
flexor retinaculum
MetacarpalsTendon of flexor digitorum superficialis
Tendon of flexor digitorum profundus
(a) Anterior superficial view (b) Anterior deep view
Palmaris longusPronator teresFlexor carpi radialisFlexor digitorum superficialisFlexor carpi ulnaris
FLEXOR DIGITORUM PROFUNDUS
Medial epicondyle of humerusTendon of biceps brachii

De Quervain’s tenosynovitis must be differentiated
from degenerative arthritis of the trapeziometacarpal
joint. The Grind Test is used to differentiate, which
will usually be negative in De Quervain’s, but positive
in degenerative arthritis. (The Grind Test is performed
by holding the thumb’s proximal phalanx and the
metacarpal phalangeal joint in the examiner’s hands
and forcefully pushing against trapeziometacarpal
joint, while also rotating it slightly, to cause a grind-
ing motion).47 It must also be differentiated from
Intersection48 and Wartenberg’s syndromes.49
6.3 Trigger finger / thumb
Trigger finger or thumb is tenosynovitis and/or tendi-
nosis of the finger’s or the thumb’s flexor tendons,
causing an inability to move the fingers or thumb
smoothly and the locking of the affected digit, with or
without pain. This stenosing tenosynovitis can be
caused by using hand tools that have sharp edges
pressing into the tissue or whose handles are too far
apart for user.50 Repetitive movements with repeated
or prolonged gripping or pinching can also cause oper-
ating trigger finger. 51
Concomitant diseases and/or reasons for trigger finger
(e.g. rheumatoid arthritis, diabetes, etc.) should be
investigated as part of the differential diagnosis.52
6.4 Carpal tunnel syndrome
A totally different range of conditions that are loosely
associated with the overuse syndromes, are the condi-
tions which result from direct or indirect pressure on
nerves, of which carpal tunnel syndrome is the most
frequently encountered.
Page | 25 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
46 Taken from Tortora (2002)
47 Wheeless CR (1996)
48 Intersection syndrome is a painful condition that affects the thumb side of
the forearm where two muscles (abductor pollicis longus and extensor
pollicis brevis) cross over – or intersect – two underlying wrist tendons
(extensor carpi radialis longus and brevis)
49 Wartenberg's syndrome: Radial sensory nerve entrapment causing significant
pain in the lower third of the forearm.
50 Guild R, et al. (2001)
51 House of Commons (1998). p. 13
52 Channas M, et.al. (1995)
Figure 6. Posterior view of the muscles that move the wrist, hand and digits46
Triceps brachii
ANCONEUSEXTENSOR CARPI ULNARIS
EXTENSOR CARPI RADIALIS BREVIS
EXTENSOR DIGITI MINIMI
FLEXOR CARPI ULNARISFLEXOR DIGITORUM
PROFUNDUS
ABDUCTOR POLLICISLONGUS
Tendon of extensor carpi ulnaris
Extensor retinaculumCarpals
Tendon of extensorindicis
Dorsal interosseiTendons of extensordigitorum
Tendon of extensordigiti minimi
EXTENSOR DIGITORUM
HumerusBRACHIORADIALIS
EXTENSOR CARPIRADIALIS LONGUS
Medial epicondyle of humerusLateral epicondyle of humerus
Olecranon of ulna
SUPINATOR
Tendon of pronator terres
EXTENSOR POLLICIS LONGUSEXTENSOR POLLICIS
LONGUS EXTENSOR INDICIS(a) Posterior superficial view
(b) Posterior deep view
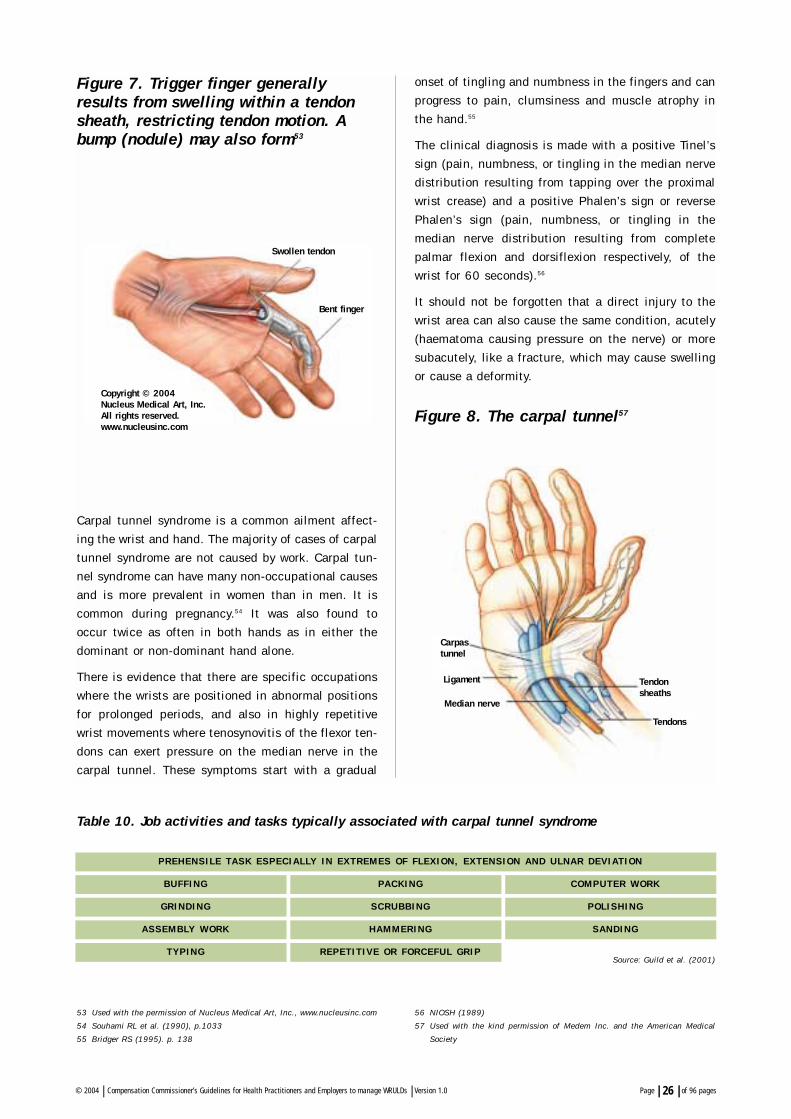
Figure 7. Trigger finger generallyresults from swelling within a tendonsheath, restricting tendon motion. Abump (nodule) may also form53
Carpal tunnel syndrome is a common ailment affect-
ing the wrist and hand. The majority of cases of carpal
tunnel syndrome are not caused by work. Carpal tun-
nel syndrome can have many non-occupational causes
and is more prevalent in women than in men. It is
common during pregnancy.54 It was also found to
occur twice as often in both hands as in either the
dominant or non-dominant hand alone.
There is evidence that there are specific occupations
where the wrists are positioned in abnormal positions
for prolonged periods, and also in highly repetitive
wrist movements where tenosynovitis of the flexor ten-
dons can exert pressure on the median nerve in the
carpal tunnel. These symptoms start with a gradual
onset of tingling and numbness in the fingers and can
progress to pain, clumsiness and muscle atrophy in
the hand.55
The clinical diagnosis is made with a positive Tinel’s
sign (pain, numbness, or tingling in the median nerve
distribution resulting from tapping over the proximal
wrist crease) and a positive Phalen’s sign or reverse
Phalen’s sign (pain, numbness, or tingling in the
median nerve distribution resulting from complete
palmar flexion and dorsiflexion respectively, of the
wrist for 60 seconds).56
It should not be forgotten that a direct injury to the
wrist area can also cause the same condition, acutely
(haematoma causing pressure on the nerve) or more
subacutely, like a fracture, which may cause swelling
or cause a deformity.
Figure 8. The carpal tunnel57
Page | 26 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
53 Used with the permission of Nucleus Medical Art, Inc., www.nucleusinc.com
54 Souhami RL et al. (1990), p.1033
55 Bridger RS (1995). p. 138
56 NIOSH (1989)
57 Used with the kind permission of Medem Inc. and the American Medical
Society
Table 10. Job activities and tasks typically associated with carpal tunnel syndrome
B U F F I N G
G R I N D I N G
A S S E M B LY W O R K
T Y P I N G
P R E H E N S I L E TA S K E S P E C I A L LY I N E X T R E M E S O F F L E X I O N , E X T E N S I O N A N D U L N A R D E V I AT I O N
PA C K I N G
S C R U B B I N G
H A M M E R I N G
R E P E T I T I V E O R F O R C E F U L G R I P
C O M P U T E R W O R K
P O L I S H I N G
S A N D I N G
Source: Guild et al. (2001)
Copyright © 2004Nucleus Medical Art, Inc.All rights reserved.www.nucleusinc.com
Swollen tendon
Bent finger
Carpastunnel
Ligament
Median nerve
Tendonsheaths
Tendons

6.5 Tendinopathy of the common flexors / extensors of the forearm
Page | 27 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
Table 11. Job activities and tasks typically associated with tendinopathy of the common flexors / extensors of the forearm
Table 12. Job activities and tasks typically associated with hand and wrist conditions
T E N D I N O PAT H Y ( E . G . T E N D I N O S I S ,T E N O S Y N O V I T I S )
PUNCH PRESS OPERATION POLISHING
ASSEMBLY WORK SANDING
WIRING PUNCH PRESS OPERATION
PACKAGING SAWING
USE OF PLIERS CUTTING
BUFFING USE OF PLIERS
GRINDING FORCEFUL HAND WRINGING
‘TURNING’ CONTROLS SUCH INSERTING SCREWS IN HOLES
AS ON MOTORCYCLE
G U Y O N T U N N E L S Y N D R O M E
( B I K E R ’ S F I N G E R )
R E P E AT E D / P R O L O N G E D P R O L O N G E D F L E X I O N O F A N D
P R E S S U R E O N T H E O U T S I D E O F E X T E N S I O N O F T H E W R I S T
T H E PA L M B R I C K L AY I N G
C A R P E N T R Y S O L D E R I N G
U S E O F P L I E R S H A M M E R I N G
P R O N AT O R T E R E S S Y N D R O M E
S O L D E R I N G B U F F I N G
S A N D I N G G R I N D I N G
P O L I S H I N G
W H I T E F I N G E R( R AY N A U D ’ S S Y N -
D R O M E , V I B R AT I O N S Y N D R O M E )
Source: Guild et al. (2001)
Source: Guild et al. (2001)
W O R K I N G W I T H C H A I N S AW, J A C K H A M M E R S , U S I N G V I B R AT I N G T O O L
T H AT I S T O O S M A L L F O R T H E H A N D , O F T E N I N A C O L D
E N V I R O N M E N T
6.6 Other work-related hand and wrist conditions
Radial tunnel syndrome
Guyon (ulnar) tunnel syndrome
Pronator teres syndrome
Anterior and posterior interosseous syndrome
Intersection syndrome

SECTION C-1:For healthcare workers
Diagnosis, management &evaluation of impairment

7. Principles of Diagnosis
WRULDs caused by rapid or repetitive motion, force-
ful exertion, excessive mechanical force concentra-
tion, awkward or non-neutral postures and vibration
have been included in Schedule 3 of the
Compensation for Occupational Injuries and Diseases
Act, 1993.
In Circular Instruction 180 these risk factors are men-
tioned in more detail, namely highly repetitive move-
ments, movements requiring force, movements at the
extremes of reach, static muscle loading, awkwardly
sustained postures, contact stress (e.g. uncomfortable
gripping and twisting, sharp edges to hand tools, desk
edges, etc.) and vibration. (See 14.7, p. 53 on how to
assess for these risk factors.)
The implication is that employees only have to prove
that they are exposed to these risk factors at work and
it will be presumed that they developed the specific
WRULD as a result of their work, provided investiga-
tions for potential other causes have been reasonably
excluded. This will have to correlate with their job and
the specific condition – employees cannot claim they
have tendinosis of the elbow if they do repetitive
movements with their legs!!
According to Circular Instruction 180 the following
criteria should be applied to confirm the diagnosis:
a. A diagnosis of a WRULD by the medical practition-
er.
b. Medical history and clinical signs indicating –
– site and distribution
– quality (type, character)
– severity (intensity, frequency, duration) and
– progression of the symptoms according to the
type of disorder
c. Functional ability report by an occupational thera-
pist and / or physiotherapist, where necessary.
d. Occupational exposure to known risk factors and a
chronological relationship between the WRULD
and the work environment.
e. Confirmatory tests/investigations (e.g. X-rays,
strength testing, range of motion testing, nerve
conduction tests), where appropriate.
The medical officers in the Compensation Office will
determine whether the diagnosis of WRULD was made
according to acceptable criteria.
7.1 Occupational (and other relevant) history, symptoms, signs and specialinvestigations
7.1.1 Relevant symptoms, clinical signs and progres-sion of the disorder
The presence of specific symptoms and objective
signs (accurately described and evaluated) associated
with this alleged, specific disorder is necessary to
make a definitive diagnosis. Pain, swelling and func-
tion should be evaluated.
The progression of the injury over a period of time is
important to help determine the prognosis.
When the worker is examined, there must be an exam-
ination routine. It is important that both the uninjured
and injured sides are examined. Try and reproduce the
symptoms, assess for referred pain, examine the spine
and perform functional testing. It is important that
the area be palpated, that ligaments are tested and
that nerve function be assessed.
It is not the purpose of these guidelines to go into
depth on how to examine the upper limb. However,
occupational health practitioners are advised to famil-
iarise themselves thoroughly with the Southampton
examination schedule for the diagnosis of musculo-
skeletal disorders of the upper limb.58
Page | 29 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
58 Palmer K et al. (2000)

Table 13 – Symptoms and signs of WRULDs
Page | 30 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
SYMPTOMS
STAGE 1
Although symptoms will vary according to the type of disorder, common symptoms and signs include the following:
B U R N I N G S E N S AT I O N
FAT I G U A B I L I T Y
L O S S O F G R I P S T R E N G T H
L O S S O F N O R M A L S E N S AT I O N
S T I F F N E S S A N D C R A M P S
M U S C L E W E A K N E S S
PA I N
PA R A E S T H E S I A ( T I N G L I N G )
S E N S AT I O N O F C O L D
S W E L L I N G
PA I N , A C H I N G A N D T I R E D N E S S O F T H E L I M B I S E X P E R I E N C E D W H E N W O R K -
I N G , B U T T H E S E S Y M P T O M S I M P R O V E O V E R N I G H T. T H I S S TA G E I S M O S T
O F T E N R E V E R S I B L E W I T H R E S T A L O N E . S O M E T I M E S G U I D E D E X E R C I S E A N D
T R E AT M E N T T O A D D R E S S M U S C U L A R P R O B L E M S A R E R E Q U I R E D F O R A C U R E .
STAGE 2
R E C U R R E N T PA I N , A C H I N G A N D T I R E D N E S S O F T H E L I M B O C C U R E A R L I E R I N
T H E D AY, P E R S I S T AT N I G H T A N D M AY D I S T U R B S L E E P. P H Y S I C A L S I G N S O F
T H E S P E C I F I C D I S O R D E R ( E . G . S W E L L I N G ) M AY B E V I S I B L E . T H E S E PAT I E N T S
S H O U L D B E R E F E R R E D F O R P H Y S I O T H E R A P Y A N D W O R K A S S E S S M E N T T O
P R E V E N T R E C U R R E N C E .
STAGE 3
P E R S I S T E N T PA I N , A C H I N G , W E A K N E S S A N D FAT I G U E O F T H E L I M B A R E
E X P E R I E N C E D E V E N I F T H E P E R S O N H A D N O T B E E N W O R K I N G F O R S O M E
T I M E . S L E E P I S O F T E N D I S T U R B E D . T H I S C A N B E I R R E V E R S I B L E I F N O T
T R E AT E D A P P R O P R I AT E LY.
C R E P I T U S ( C R A C K L I N G S O U N D I N S U B C U TA N E O U S T I S S U E )
M U S C L E S PA S M
M U S C L E W E A K N E S S
R E D U C T I O N O F R A N G E M O V E M E N T
S W E L L I N G
T E N D E R T R I G G E R P O I N T S I N M U S C L E S
T E N D E R N E S S
S IGNS
Please note that:
Symptoms may not always be accompanied by objective signs.
Any one symptom or sign on its own is not indicative of WRULDs and some may be common with normal function.
Very few sufferers experience all the symptoms.
The symptoms do not appear in any particular order.
Table 14. Progression of WRULDs – WRULDs tend to be progressive and the development of the disorder can be divided into three broad stages
Source: London Hazard Centre (1997)

7.1.2 The history of occupational exposure to the riskfactors
A summary is needed of the current working environ-
ment with respect to the flow of work and the actions
required by the employee to complete the work.
Summarise the exposure to the risk factors (See Table
16 and 17). The summary table should be completed
by the medical practitioner when completing the
Medical Reports for WRULDs (W.Cl. 301 & W.Cl. 302
forms).
Refer to the posture/s adopted by the employee to
conduct the work, the force and motion required, and
the exposure to vibration. Consider which of these fac-
tors contributed to the alleged upper limb disorder in
relation to the frequency of the movements, duration,
strength and range of movement.
Page | 31 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
R A P I D O R R E P E T I T I V E M O T I O N
M O V E M E N T S R E Q U I R I N G F O R C E E X E R T I O N
E X C E S S I V E M E C H A N I C A L F O R C E C O N C E N T R AT I O N
AW K W A R D O R N O N - N E U T R A L P O S T U R E S
( M O V E M E N T S AT E X T R E M E S O F R E A C H , S TAT I C
M U S C L E L O A D I N G , AW K W A R D LY S U S TA I N E D
P O S T U R E S , C O N TA C T S T R E S S )
C O L D E N V I R O N M E N T O R H A N D L I N G C H I L L E D O R
F R O Z E N P R O D U C T S
V I B R AT I O N
G E N D E R ( F E M A L E S A R E M O R E AT R I S K )
A G E ( O L D E R E M P L O Y E E S A R E M O R E AT R I S K )
A B N O R M A L B O D Y M A S S I N D E X
P R O L O N G E D D U R AT I O N O F E X P O S U R E
P O O R W O R K O R G A N I S AT I O N ( L O W L E V E L O F C O N -
T R O L O V E R W O R K R AT E , N O B R E A K S , E T C . )
P S Y C H O S O C I A L S T R E S S AT W O R K A N D FAT I G U E
Table 15. The risks associated with the development of WRULDs are increased bythe following home or work-based activities
Table 16. Example of a template to summarise the exposure to risk factors
RISK FACTOR PERCENTAGE OF BRIEFLY DESCRIBE THE JOB TASK WHERE THIS RISK WORKING DAY FACTOR OCCURS AND QUANTIFY IN TERMS OF
REPETITIONS/DURATION/ STRENGTH REQUIRED/RANGE OF MOVEMENT, ETC.
R E P E T I T I V E M O V E M E N T S
M O V E M E N T S R E Q U I R I N GF O R C E
M O V E M E N T S AT T H EE X T R E M E S O F R E A C H
S TAT I C M U S C L E L O A D I N G
AW K W A R D LY S U S TA I N E DP O S T U R E S
C O N TA C T S T R E S S
V I B R AT I O N
L O W T E M P E R AT U R E S( C O L D )

Page | 32 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
Table 17. Work system factors to be assessed
PHYSICAL PROPERTYPOSTURE
STRENGTH & RANGE REPETITION/ DURATIONOF MOVEMENT FREQUENCY(AMPLITUDE / MAGNITUDE)
F O R C E F O R C E G E N E R AT E D F R E Q U E N C Y O F T I M E T H AT F O R C E I SO R A P P L I E D A P P L I C AT I O N A P P L I E D
P O S T U R E J O I N T A N G L E F R E Q U E N C Y T I M E H E L D
M O T I O N V E L O C I T Y, A C C E L E R AT I O N F R E Q U E N C Y O F M O T I O N T I M E O F M O T I O N E X P O S U R E
V I B R AT I O N A C C E L E R AT I O N F R E Q U E N C Y W I T H W H I C H T I M E O F V I B R AT I O NV I B R AT I O N O C C U R S E X P O S U R E
Source: European Agency for Safety and Health at Work (1999)
Note:
Acute injuries can develop into chronic injuries if there is inadequate rehabilitation before returning to work.
When this progression of an acute injury is reported to the Compensation Commissioner, one must continue to
handle it as an occupational injury and not as an occupational disease (WRULD), because it was reported as an
injury in the first place (thus use W. Cl. 5 to complete progress medical reports).
State the period(s) the employee worked in previous
environments with exposures related to his/her
disease (start with the most recent employer mention-
ing the period of exposure, the occupation, the type of
exposure, the year first exposed, the duration / years
of exposure (which may not be the same as the years
in an occupation), the frequency of exposure (e.g.
once per week for an hour or 8 hours every day).
If necessary, attach photos, diagrams and/or extra
reports to explain the employee’s work actions.
7.1.3 Relevant facts from the medical, family andsocial history as well as the investigation ofother potential causes
It is important that all non-vocational activities (e.g.
sport) are investigated to determine how these
conditions contribute to the development of any of the
symptoms. An upper limb disorder may be seen as a
consequence of activities performed at work, but it
could also be caused by the worker’s domestic or
recreational activities and not work.
Previous injuries, leisure activities, lifestyle issues
and other non work-related activities which could lead
to the development of this disorder, should thus be
determined.
Proof should also be given that other potential causes
have been investigated, where appropriate (e.g.
hypothyroidism, diabetes, pregnancy, rheumatologic
disorders, etc., in the case of carpal tunnel syndrome;
and X-rays to exclude neck pathology where
indicated).
7.1.4 Health risk assessment
The medicine practitioner who makes the definitive
diagnosis should familiarise himself with the alleged
work environment, work process and work actions.
7.1.5 Special investigations
Special investigations should be carried out if
considered essential for the accurate diagnosis
and treatment of the injury (e.g. high resolution
ultrasound X-rays, strength testing, range of

motion testing, electromyography (EMG) analysis,
isokinetic dynamometry, etc.). The Compensation
Commissioner will not pay for magnetic resonance
imaging (MRI) scan if prior authorisation had not
been obtained from the medical officers in the
Compensation Commissioner’s office.
7.2 Duration of exposure
WRULDs take a period of time to develop and gener-
ally a job which involves exposure to the mentioned
risk factors, should be performed for more than 6
months before the condition develops. However, each
case should be evaluated on its own merit.
Page | 33 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0

8. Management OF WRULDs
Definitions:
Occupational health practitioner (OHP): A
registered nursing sister with an extra
qualification in occupational health, also
often referred to as the occupational
health nurse (OHN).
Occupational medicine practitioner (OMP):
A medical doctor with an extra qualifica-
tion in occupational health.
Page | 34 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
59 Personal communication with Prof Tim Noakes (UCT Sport Science Institute)
60 Khan K (2000) 61 Khan K (2000)
8.1 Clinical significance of the diagnosis oftendinosis
Evidence supports the notion that overuse tendon con-
ditions do not primarily involve inflammation, but
degeneration.59 If this is correct, then the traditional
approach to treating tendinopathies as an inflammato-
ry ‘tendonitis’ is likely flawed. Current scientific data
(Table 18) will help physicians avoid common miscon-
ceptions about tendinopathies and their management.60
If we accept that a worker with overuse tendinopathy
has a disorder that is due to collagen degeneration,
then the diagnosis has various implications for the
management of these disorders (Table 19).61
Table 18. Common misconceptions about tendinopathies and its management
MISCONCEPTION
TENDINOPATHIES ARE SELF-LIMITING CONDITIONS THAT TAKE
ONLY A FEW WEEKS TO RESOLVE
EVIDENCE-BASED FINDING
TENDINOPATHIES OFTEN PROVE RECALCITRANT TO
TREATMENT AND MAY TAKE MONTHS TO RESOLVE
IMAGING APPEARANCE CAN PREDICT PROGNOSIS
IMAGING DOES NOT PREDICT PROGNOSIS; IT ADDS
TO THE LIKELIHOOD OF A DIAGNOSIS OF TENDINOPATHY BUT
DOES NOT PROVE IT
CYST-LIKE ULTRASONOGRAPHIC ABNORMALITIES IN
TENDONS ARE INDICATIONS FOR SURGERY
SURGERY IS GENERALLY NOT INDICATED.
AS LAST RESORT, SURGERY SHOULD BE BASED ON
CLINICAL GROUNDS; CYST-LIKE ULTRASONOGRAPHIC
FINDINGS CAN BE FOUND IN ASYMPTOMATIC EMPLOYEES
SURGERY PROVIDES RAPID RELIEF OF SYMPTOMS
IN ALMOST ALL SUBJECTS
AFTER SURGERY (WHERE IT WAS CLINICALLY INDICATED AS
LAST RESORT), RETURN TO REPETITIVE WORK TAKES A
MINIMUM OF 4-6 MONTHS; NOT ALL PATIENTS DO WELL
Source: Khan K (2000)

8.2 Treatment modalities
Khan (1998) presented a new paradigm in the manage-
ment of tendinopathies in sports medicine. This
approach has a record of clinical effectiveness and
recent research adds further scientific support.62
This approach in sports medicine was therefore
adapted for these guidelines to fit occupational health
and the management of WRULDs, since the under-
lying mechanism of tissue damage is presumably the
same, namely repetitive movements, overuse, excessive
force and overloading.
Prof Tim Noakes (2002) of the Sport Science Institute
(University of Cape Town) agrees that this assumption
is justified and that it is supported by sound scientific
research.63
Tendinopathies have caused long-lasting frustration
for employees, employers and occupational health
practitioners, because they attributed the pathology to
tendonitis, rather than tendinosis. Occupational
health practitioners should acknowledge that the
cause is most often due to tendinosis, rather than
tendonitis, and treat the problem using a fundamen-
tally different paradigm. Advice and suggestions for
employees along these lines of clinical thought can
help them recover more quickly and prevent surgery.
8.2.1 Employee education
The occupational health practitioner should take the
time to explain and illustrate the pathology of
tendinosis, especially since textbooks and websites
have yet to embrace this pathology and its clinical
implications. Employees who have symptoms of short
duration, but are still able to engage in work, are the
ones who need the most education. They are likely to
continue to do repetitive work without undergoing
appropriate treatment, and thus worsen the
tendinosis.64
Page | 35 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
62 Khan (1998)
63 Personal communication with Prof Tim Noakes (December 2002) 64 Khan (2000)
Table 19. Implications of the diagnosis of tendinosis compared with tendonitis
TRAIT OVERUSE TENDINOSIS OVERUSE TENDONITIS
PREVALENCE COMMON RARE
TIME FOR RECOVERY, EARLY PRESENTATION 6-10 WEEKS SEVERAL DAYS TO 2 WEEKS
TIME FOR FULL RECOVERY, CHRONIC 3-6 MONTHS 4-6 WEEKSPRESENTATION
LIKELIHOOD OF FULL RECOVERY FROM CHRONIC SYMPTOMS TO RESUMEREPETITIVE WORK ~80% 99%
FOCUS OF CONSERVATIVE THERAPY ENCOURAGEMENT OF COLLAGEN- ANTI-INFLAMMATORY MODALITIESSYNTHESIS MATURATION AND AND DRUGSSTRENGTH
ROLE OF SURGERY AS LAST RESORT EXCISE ABNORMAL TISSUE NOT KNOWN
PROGNOSIS FOR RECOVERY AFTER SURGERY 70%-85% 95%
TIME TO RECOVER FROM SURGERY 4-6 MONTHS 3-4 WEEKS
Source: Khan K (2000)

8.2.2 Anti-inflammatory strategies
Common anti-inflammatory strategies include:
Cryotherapy (ice)
Electrotherapeutic modalities (physiotherapy)
Non-steroidal anti-inflammatory drugs (NSAIDs)
Corticosteroid injections
Employees with tendinosis may benefit from cryo-
therapy, because ice has a vasoconstrictive role, and
abnormal neovascularisation is a feature of the pathol-
ogy. Because a strong clinical impression exists that
ice is helpful in tendinopathies, this modality should
not be discarded.65
Limited evidence exists to support the use of NSAIDs
and corticosteroids in treating tendinosis.66, 67 NSAIDs
on the other hand are effective in the treatment of
tenosynovitis, which is an inflammatory condition.
Corticosteroid injection has lost favour in managing
tendinosis, because tendinosis is not an inflammatory
condition.68, 69 It may still have a role to play in the
treatment of tenosynovitis.
8.2.3 Therapeutic strategies
Therapeutic strategies are used to improve the
individual’s functional capacity and some of the
modalities which are used, include:
Initial treatment may include rest
Immobilise – splinting (occupational therapy)
Physiotherapy modalities, e.g. ultrasound for
tenosynovitis
Mobilise – stretches to improve flexibility (physio-
therapy)
Mobilise – exercise to appropriately strengthen
muscles (physiotherapy)
Education – good work habits, pacing, joint con-
servation techniques and self-management (occu-
pational therapy)
8.2.4 Reasonable job accommodations
Temporary job change
Work station redesign (layout, heights, etc)
Page | 36 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
65 Khan (2000)
66 Almekinders et al. (1998)
67 Khan(2000)
68 Shrier et al. (1996)
69 Khan(2000)
Table 20. The following treatment modalities can be utilised depending on the statusof the disorder
A. EMPLOYEE EDUCATION
B. INFLAMMATORY STRATEGIES
CRYOTHERAPY (ICE)
NON-STEROID ANTI-INFLAMMATORY DRUGS
ELECTROTHERAPEUTIC MODALITIES
(PHYSIOTHERAPY)
INFILTRATION WITH CORTICOSTEROIDS
C. THERAPEUTIC STRATEGIES
INITIAL TREATMENT MAY INCLUDE REST
IMMOBILISE – SPLINTAGE
(OCCUPATIONAL THERAPY)
MOBILISE (PHYSIOTHERAPY)
MOBILISE – EXERCISE TO APPROPRIATELY
STRENGTHEN MUSCLES
EDUCATION – GOOD WORK HABITS, PACING, JOINT
CONVERSATION TECHNIQUES AND
SELF-MANAGEMENT (OCCUPATIONAL THERAPY)
D. REASONABLE JOB ACCOMODATION
TEMPORARY JOB CHANGE
WORK STATION REDESIGN (LAYOUT, HEIGHTS,
ETC.)
TOOL AND EQUIPMENT ADAPTATION (CHANGE HAN-
DLE DESIGN, USE OF JIGS, ETC.)
JOB TASK MODIFICATIONS
RETRAINING AND REASSIGNMENT
WORK SCHEDULE MODIFICATIONS
JOB ENLARGEMENT
ROTATION
E. PSYCHOLOGICAL EVALUATION
F. SURGERY (AS LAST RESORT)

Tool and equipment adaptation (change handle
design, use of jigs etc)
Job task modification
Retraining and reassignment
Work schedule modifications (half day initially,
build up to full day)
Job enlargement (inclusion of additional duties to
reduce repetitiveness of performing a single task only)
Rotation
8.2.5 Surgery as a last resort
Surgery has been considered the treatment of last
resort for tendinopathies, and this certainly applies, if not
more so, for a confirmed case of tendinosis. Surgery
can be used to excise tissue affected by tendinosis,
but surgery has not been proven to stimulate collagen
synthesis or maturation. Reviews suggest that surgery
in tendinosis has a 75% to 85% success rate.70, 71
Therefore, an important implication of tendinopathy’s
underlying pathology being tendinosis is that conser-
vative management must progress slowly. Because
surgical treatment of tendinosis is not without failure,
and recovery takes a minimum of 4 to 6 months, this
treatment should be reserved for failure of a high-
quality programme of conservative management.72 If
surgery is required, rehabilitation should start pre-
surgery in order to improve post-surgery recovery. This
includes physiotherapy, occupational therapy and
exercise therapy.
8.3 Algorithms
Algorithms A, B and C73 (p. 38 – 40) offer OHNs and
OMPs guidelines on how to manage a possible case of
WRULD.
The rationale behind these algorithms in managing
WRULDs is:
That of a typical occupational health clinic in an
industrial setting
With an occupational nursing practitioner as the
primary contact
And the visiting occupational medicine practition-
er or general practitioner as secondary contact
Where this is not the case, these algorithms will still
give a health practitioner a good idea of the process to
be followed in managing and reporting a WRULD to
the Compensation Commissioner. See ‘Reporting’
(p. 43) for forms which should be used.
Page | 37 | of pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
70 Coleman BD; Khan KM; Maffulli, et al. (2000)
71 Coleman BD; Khan KM; Kiss ZS, et al. (2000)
72 Khan(2000)
73 Adapted for South African circumstances from a NIOSH Health Hazard
Evaluation Report (HETA 89-307-2009) by Afrox Occupational Healthcare
ALGORITHM A
PRIMARY CONTACT: GUIDELINES FOR THE OCCUPATIONAL NURSING PRACTITIONER
WHEN A WRULD IS SUSPECTED. THE OCCUPATIONAL HEALTH NURSING PRACTITIONER
HAS AN IMPORTANT ROLE IN EVALUATING AND SCREENING ORDINARY MUSCLE ACHES
AND PAINS FOR POTENTIAL WRULDs.
ALGORITHM B
SECONDARY CONTACT: GUIDELINES FOR THE OCCUPATIONAL HEALTH MEDICINE
PRACTITIONER BEFORE A WRULD IS REPORTED TO THE COMPENSATION
COMMISSIONER
THE DOCTOR USUALLY EVALUATES THOSE EMPLOYEES NOT RESPONDING TO THE
OHN’S CONSERVATIVE MANAGEMENT. THE DOCTOR NOW HAS THE TASK TO EVALUATE
THE WORK-RELATEDNESS OF THE SYMPTOMS, AND THEN HAS TO DECIDE IF AN OCCU-
PATIONAL INJURY OR AN OCCUPATIONAL DISEASE (WRULDs) SHOULD BE REPORTED
TO THE COMPENSATION COMMISSIONER.
ALGORITHM CGUIDELINES TO THE OCCUPATIONAL HEALTH MEDICINE PRACTITIONER WHEN REPORT-
ING A CASE OF WRULD TO THE COMPENSATION COMMISSIONER
ALGORITHM D GUIDELINES TO THE EMPLOYER IN REPORTING WRULDs TO THE DEPT OF LABOUR
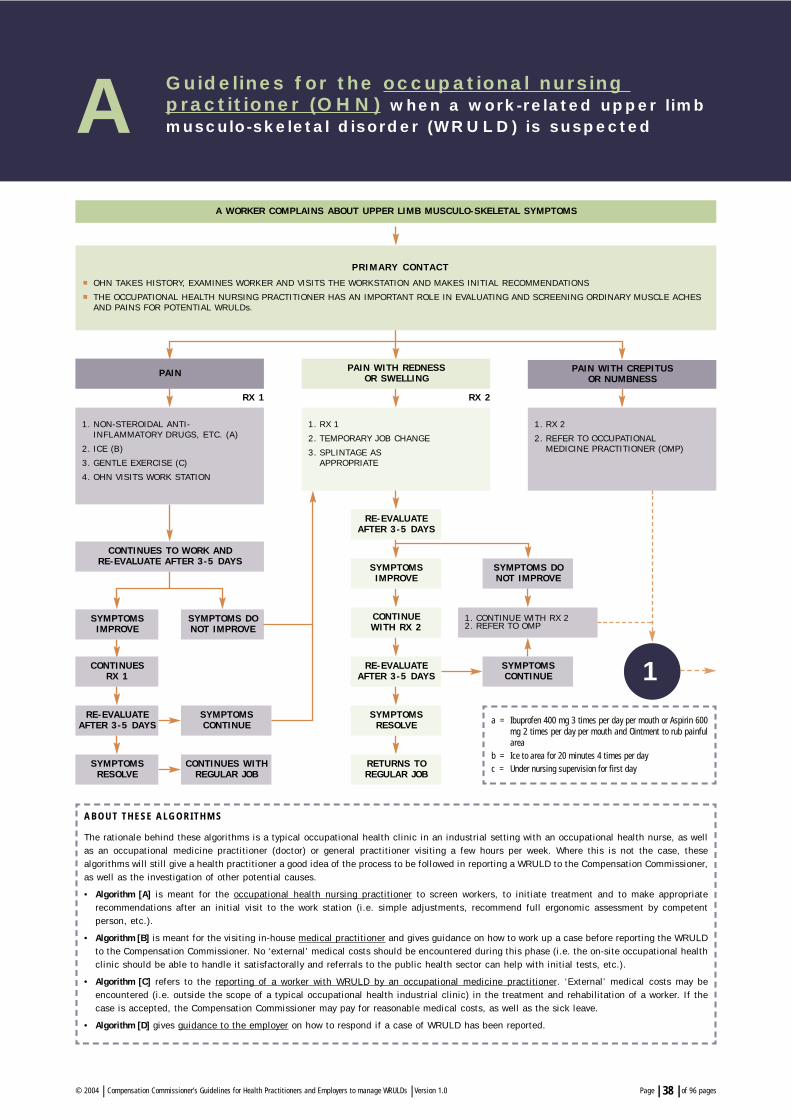
Page | 38 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
A Guidelines for the occupational nursing practitioner (OHN) when a work-related upper limbmusculo-skeletal disorder (WRULD) is suspected
A WORKER COMPLAINS ABOUT UPPER L IMB MUSCULO-SKELETAL SYMPTOMS
1. RX 1
2. TEMPORARY JOB CHANGE
3. SPLINTAGE AS APPROPRIATE
1. RX 2
2. REFER TO OCCUPATIONALMEDICINE PRACTITIONER (OMP)
PAIN
CONTINUES TO WORK AND RE-EVALUATE AFTER 3-5 DAYS
SYMPTOMSIMPROVE
SYMPTOMSIMPROVE
CONTINUESRX 1
CONTINUE WITH RX 2
RE-EVALUATE AFTER 3-5 DAYS
RE-EVALUATE AFTER 3-5 DAYS
RE-EVALUATE AFTER 3-5 DAYS
SYMPTOMSRESOLVE
SYMPTOMSRESOLVE
SYMPTOMS DONOT IMPROVE
SYMPTOMS DONOT IMPROVE
SYMPTOMSCONTINUE
SYMPTOMSCONTINUE
CONTINUES WITHREGULAR JOB
RETURNS TOREGULAR JOB
PAIN WITH CREPITUS OR NUMBNESS
1. NON-STEROIDAL ANTI-INFLAMMATORY DRUGS, ETC. (A)
2. ICE (B)
3. GENTLE EXERCISE (C)
4. OHN VISITS WORK STATION
RX 1 RX 2
ABOUT THESE ALGORITHMS
The rationale behind these algorithms is a typical occupational health clinic in an industrial setting with an occupational health nurse, as wellas an occupational medicine practitioner (doctor) or general practitioner visiting a few hours per week. Where this is not the case, these algorithms will still give a health practitioner a good idea of the process to be followed in reporting a WRULD to the Compensation Commissioner,as well as the investigation of other potential causes.
• Algorithm [A] is meant for the occupational health nursing practitioner to screen workers, to initiate treatment and to make appropriate recommendations after an initial visit to the work station (i.e. simple adjustments, recommend full ergonomic assessment by competent person, etc.).
• Algorithm [B] is meant for the visiting in-house medical practitioner and gives guidance on how to work up a case before reporting the WRULDto the Compensation Commissioner. No ‘external’ medical costs should be encountered during this phase (i.e. the on-site occupational healthclinic should be able to handle it satisfactorally and referrals to the public health sector can help with initial tests, etc.).
• Algorithm [C] refers to the reporting of a worker with WRULD by an occupational medicine practitioner. ‘External’ medical costs may beencountered (i.e. outside the scope of a typical occupational health industrial clinic) in the treatment and rehabilitation of a worker. If thecase is accepted, the Compensation Commissioner may pay for reasonable medical costs, as well as the sick leave.
• Algorithm [D] gives guidance to the employer on how to respond if a case of WRULD has been reported.
a = Ibuprofen 400 mg 3 times per day per mouth or Aspirin 600mg 2 times per day per mouth and Ointment to rub painfularea
b = Ice to area for 20 minutes 4 times per day c = Under nursing supervision for first day
PAIN WITH REDNESS OR SWELLING
1
P R I M A R Y C O N TA C T
OHN TAKES HISTORY, EXAMINES WORKER AND VISITS THE WORKSTATION AND MAKES INITIAL RECOMMENDATIONS
THE OCCUPATIONAL HEALTH NURSING PRACTITIONER HAS AN IMPORTANT ROLE IN EVALUATING AND SCREENING ORDINARY MUSCLE ACHESAND PAINS FOR POTENTIAL WRULDs.
1. CONTINUE WITH RX 22. REFER TO OMP

SECONDARY CONTACT
DOCTOR TAKES MEDICAL, OCCUPATIONAL AND SOCIAL HISTORY AND DOES A PHYSICAL EXAMINATION, MAKES A PSYCHOLOGICAL IMPRESSION,AS WELL AS A WORKING DIAGNOSIS AND VISITS THE WORKSTATION.
THE DOCTOR USUALLY EVALUATES THOSE WORKERS NOT RESPONDING TO THE OHN’S CONSERVATIVE MANAGEMENT. THE DOCTOR NOW HAS THE TASK TO EVALUATE THE WORK-RELATEDNESS OF THE SYMPTOMS, AND THEN NEEDS TO DECIDE IF AN OCCUPATIONALINJURY OR AN OCCUPATIONAL DISEASE (WRULD) SHOULD BE REPORTED TO THE COMPENSATION COMMISSIONER.
Page | 39 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
NO SYMPTOMS
B Guidelines for the occupational medicine practitioner (OMP) before a work-related upperlimb disorder (WRULD) is reported to theCompensation Commissioner
REFERRAL FROM ONP TO OMP / GENERAL PRACTIT IONER
S Y M P T O M S R E M A I N O R W O R S E N
1. OMP VISITS WORKSTATION & GIVESADVICE
2. NSAID INJECTION (D)
3. PHYSIO / OCCUPATIONAL THERAPY (E)
4. REST FOR 2-3 WORKING DAYS
5. CONTINUE RX 1
6. SPLINTAGE AS APPROPRIATE
IMPROVED SYMPTOMS – RETURNS TOREGULAR OR TEMPORARY JOB
BACK TO REGULAR JOB
CONTINUES WITH TEMPORARY JOB
NO SYMPTOMS
RE-EVALUATE IN 3-7 DAYS
MANAGE FURTHER AND REFER TO TER-T IARY LEVEL IF NECESSARY. THE
COMPENSATION COMMISSIONER WILL NOT
ACCEPT RESPONSIBIL ITY FOR ANYCLAIMS OR MEDICAL EXPENSES.
RE-EVALUATE IN 3-7 DAYS
STILL MILD SYMPTOMS
NOT CONVINCING EVIDENCE OF WRULD SOUND EVIDENCE OF WRULD
DO NOT REPORT TO COMPENSATION COMMISSIONER
REPORT TO COMPENSATIONCOMMISSIONER (G)
IN GAUTENG – PLEASE ALSO REPORT TO SAMOSA (H)
WORSENINGSYMPTOMS
MUCH IMPROVED OR NO SYMPTOMS
BACK TO TEMPORARY JOB APPROPRIATE MEDICAL
WORK UP (F )
RE-EVALUATE IN 3-7 DAYS
RX 3
d = Diclofenac 50 – 75 mg IMI e = Consider physiotherapy and/or occupational therapy where these services are available (e.g. at the day hospital - the
Compensation Commissioner will not pick up these costs at this stage).f = Where appropriate, do special investigations to exclude other non work-related causes (e.g.ESR, thyroid functions,
rheumatoid screening in the case of carpal tunnel syndrome; X-rays of the neck may be necessary to exclude cervical spondylosis; X-rays of a specific joint may also be indicated, etc). The Compensation Commissioner is notresponsible for these costs!
g = Please inform the worker beforehand that medical costs will only be paid if the case is accepted. Huge amounts ofcompensation will most probably not be forthcoming.
h = SA Occupational Musculo-skeletal Disorder Surveillance Action Group (SAMOSA),National Centre for OccupationalHealth, Johannesburg. (Tel/Fax 011 725 5978; [email protected]).
NO IMPROVEMENT IN SYMPTOMS
2
1
RE-EVALUATE IN 3-7 DAYS
SYMPTOMS REMAIN OR WORSEN

C Guidelines for the occupational medicine practitioner (OMP) when a WRULD is reported tothe Compensation Commissioner
Page | 40 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
EVALUATE PROGRESS FOR 2-3 MONTHS
PREVENTATIVE MEASURES
IN ORDER TO COMPLY WITH THE OCCUPATIONAL HEALTH ANDSAFETY ACT AND THE MINE HEALTH AND SAFETY ACT, THE
EMPLOYER SHOULD NOTIFY THE PROVINCIAL EXECUTIVEMANAGER (DEPT LABOUR) OR THE REGIONAL PRINCIPAL
INSPECTOR OF MINES (DME) . SEE ALGORITHM D.
REPORT TO THE COMPENSATION COMMISSIONER WITH COPIES TO THE DEPT LABOUR / DME
NO IMPROVEMENT
1. PHYSIOTHERAPY / CCCUPATIONAL THERAPY
2. RX 3
3. REST / SICK LEAVE FOR 7 DAYS (I)
4. INFILTRATE WITH STEROID INJECTION WHERE INDICATED (J)
1. EXTENDED PERIOD OF REST (I) FOR 1–2 MONTHS (SICK LEAVE AT 75% OF SALARY PAID BYCOMPENSATION COMMISSIONER).
2. CONTINUED PHYSIOTHERAPY AND/OR OCCUPATIONAL THERAPY AND/OR EXERCISE THERAPY, WITH RELAX-ATION, STRETCHING, STRENGTHENING, POSTURE CORRECTION AND GENTLE EXERCISE PLUS
3. REFERRAL TO ORTHOPAEDIC SURGEON FOR POSSIBLE SURGERY PLUS
4. PRE- AND POST-SURGERY REHABILITATION BY OCCUPATIONAL THERAPIST / PHYSIOTHERAPIST /BIOKINETHESIST.
CONTINUED MEDICAL MANAGEMENT
NO / MILD SYMPTOMS ORGREAT IMPROVEMENT
RE-EVALUATE AFTER 7 DAYS
CONSIDER EXTENDING THEPERIOD OF REHABIL ITATION
CONTINUE WITH MEDICAL TREATMENT AS APPROPRIATE (RX 5) AND START WITH COUNSELLING IN CO-OPERATION WITHTHE EMPLOYER’S EMPLOYEE ASSISTANCE PROGRAMME (EAP)
START INDUCTION PROGRAMME AT WORK (K)
IF RECURRENCE OF SYMPTOMS
IF NO RECURRENCE OF SYMPTOMS
NO OR L ITTLE IMPROVEMENTOF SYMPTOMS
CONSIDER PERMANENTALTERNATIVE WORK
PLACEMENT; COMPLETE F INAL MEDICAL REPORT
(W.CL. 302) & DESCRIBEPERMANENT IMPAIRMENT
IF RECURRENCE OF SYMPTOMS
NO SYMPTOMS OR GREATIMPROVEMENT AFTER RX 6
START INDUCTION PROGRAMME AT WORK (K)
CONSIDER PERMANENT ALTERNATIVE PLACEMENT
AND/OR RETURN TO PROPER ADJUSTED WORK
ENVIRONMENT
EVALUATE PROGRESS FOR 2-3 MONTHS
COMPLETE F INAL MEDICALREPORT (W.CL. 302)
NO OR L ITTLE IMPROVEMENT OF SYMPTOMSNO SYMPTOMS OR GREAT IMPROVEMENT AFTER RX 5
CONSIDER PERMANENT ALTERNATIVE PLACEMENT AND/ORRETURN TO PROPER ADJUSTED WORK ENVIRONMENT
i = Rest (i.e. sick leave) should be part of a well-planned rehabilitation programme under the supervision of physiotherapist / occupational therapist / biokinethesist.j = Example: 1 ml Depot Medrol with 2 ml of Lignocaine injected into tendon sheath.k = Return to temporary job for 1-6 months and start with supervised work hardening programme (e.g. with help of ergonomist, physiotherapist, occupational therapist or OHP)
3
2
RX 4
RX 5
RX 6
9. Evaluation of impairment
Should an employee be unable to perform the required
work at the level achieved prior to the development of
this condition, he/she could be deemed ‘unfit’ to con-
tinue in that position, but permanent disability might
not necessarily be awarded, as the Compensation
Commissioner assesses impairment and permanent
disability in comparison with the open labour market
and not for a specific job or position.
When the Final Medical Report (W. Cl. 302) is received
from the treating doctor, after maximum medical
improvement has been reached, impairment will be
determined by the medical officers of the Compensation
Commissioner, in accordance with Internal Instruction
157 for residual impairment of the function of the mus-
cles, tendons, joints or nerves involved.
Maximum medical improvement should preferably be
reached after a reasonable recovery period not exceed-
ing 12 months, and failure to perform work effective-
ly after the following process has been followed:
a. Thorough investigations, which include:
i. Medical assessment
ii. Functional capacity evaluation
iii. Job analysis/ergonomic assessment
b. An integrated treatment plan, which includes:
i. Medical treatment [medication, surgical inter-
vention (where indicated) and / or acute reha-
bilitation (e.g. physiotherapy, occupational
therapy, etc.)]
ii. Vocational rehabilitation, which includes
– Optimising the person’s functional ability
(i.e. ability to perform tasks) through reha-
bilitation that includes work hardening,
work conditioning, etc.
– Addressing problem areas identified in the
job analysis / ergonomic assessment by
allowing alterations in the way in which
work is performed through reasonable
accommodation. Reasonable accommoda-
tion would include workplace environment
adaptation, tool and equipment adaptation,
workstation redesign, job task modification,
retraining and reassignment, and work
schedule modifications.
Permanent disablement will thus be awarded only if
objective and verifiable clinical signs and symptoms
are present after optimum treatment had been admin-
istered, and no further recovery can reasonably be
expected.
In case of nerve conditions, documented abnormal
sensory and/ or motor latencies are important.
Therefore a full sensory evaluation should be
performed. (It is important to note that neural
dysfunction can occur in the absence of abnormal
nerve conduction tests.74)
Grip strength is one of the few objective measura-
ble signs of muscular dysfunction, provided the
measuring instrument is properly calibrated.
Observable muscle wasting is also an objective
sign.
Causalgia and other sensory abnormalities, if accu-
rately and reliably described, will be considered in
the assessment of impairment and disablement.
However, it is expected that most employees will
recover and return to work and that only a very small
percentage will suffer any permanent residual impair-
ment if the worker was properly managed as suggest-
ed in these guidelines.
Page | 41 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
74 Greening and Lynn (1998)

SECTION C-2:For the employer
CompensationCommissioner

10. Reporting WRULDs to the CompensationCommissioner
Table 21. The following documentation should be submitted to the CompensationCommissioner by the employer individually liable or the mutual association concerned
Page | 43 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
W. CL. 1 EMPLOYER’S REPORT OF AN OCCUPATIONAL DISEASE OR
W. CL . 305 EMPLOYEE AFFIDAVIT FOR AN OCCUPATIONAL DISEASE (WHEN THE EMPLOYER DOES NOT TIMEOUSLYSUBMIT THE EMPLOYER’S REPORT OF AN OCCUPATIONAL DISEASE (W. CL.1))
W. CL. 14 NOTICE OF AN OCCUPATIONAL DISEASE AND CLAIM FOR COMPENSATION (SIGNED BY THE EMPLOYEE)
W. CL. 110 EXPOSURE HISTORY OR AN APPROPRIATE EMPLOYMENT HISTORY (PLEASE NOTE THAT THE NEW W. CL.110 FORM SHOULD BE USED)
W. CL. 301 FIRST MEDICAL REPORT IN RESPECT OF A WORK-RELATED UPPER LIMB DISORDER (WRULD)WHEN WRULDs ARE REPORTED, W. CL. 301 MUST BE USED INSTEAD OF THE USUAL W. CL. 22 (FIRSTMEDICAL REPORT IN RESPECT OF AN OCCUPATIONAL DISEASE)
ALL OTHER REPORTS THAT MAY BE RELEVANT TO THE DIAGNOSIS AND TREATMENT OF THE CONDITION (E.G. AN ERGONOMICASSESSMENT SUPPORTED BY PHOTOGRAPHS, VIDEO CLIPS, ETC.)
W. CL. 6 RESUMPTION REPORT (EVEN IF THE EMPLOYEE IS AT WORK)
W. CL. 302 PROGRESS/FINAL MEDICAL REPORT IN RESPECT OF A WORK-RELATED UPPER LIMB DISORDER (WRULD)WHEN WRULDs ARE REPORTED, W. CL. 302 MUST BE USED INSTEAD OF THE USUAL W. CL. 26(PROGRESS/FINAL MEDICAL REPORT IN RESPECT OF AN OCCUPATIONAL DISEASE)
As long as the case is open, the employer must submit the following reports on a monthly basis to the Compensation
Commissioner or Mutual Association or employer individually liable, as the case may be, until the employee’s con-
dition has become stabilised, when a Final Medical Report (W.Cl. 302) should be submitted.

12. Claim Processing
The Office of the Compensation Commissioner will
consider and adjudicate upon the liability of all
claims. The medical officers in the Compensation
Commissioner’s office are responsible for the medical
assessment of a claim and for the confirmation of the
acceptance or rejection of a claim.
Page | 44 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
11. Benefits
Benefits will be payable according to the
Compensation for Occupational Injuries and Diseases
Act, 1993, as amended.
11.1 Temporary total disablement
Payment for reasonable temporary total or partial dis-
ablement will be made on the basis of medical reports
for as long as such disablement continues, for a peri-
od not exceeding 24 months.
11.2 Permanent disablement
Permanent disablement will be assessed when a Final
Medical Report is received, after a reasonable recov-
ery period not exceeding 24 months, and failure to
perform work effectively after the appropriate course
of treatment and rehabilitation.
11.3 Medical aid
Medical expenses shall be provided for a period of not
more than 24 months from the date of diagnosis. This
period may be extended if, in the opinion of the
Director General, further medical aid will reduce the
extent of the disablement. The medical aid covers the
costs of diagnosing a WRULD and any necessary treat-
ment provided by any healthcare provider. The
Compensation Commissioner will decide on the need
for, the nature and the sufficiency of the medical aid
supplied.

SECTION D:For the employer
Inspectorate of Labour

13. Reporting to the Inspectorate of Labour
The employer should not only report a case of WRULD
to the Compensation Commissioner, but also to the
nearest Inspectorate of the Department of Labour.
The employer must be able to demonstrate to the
Inspectorate what is being done to reduce the risk of
WRULDs.
The General Administrative Regulations of the
Occupational Health and Safety Act (No 85 of
1993), provides for investigation and recording of
incidents and occupational disease.75
Section 8(1) provides that employers must provide
and maintain a workplace that is safe and without
risk to the health of their employees.
Section 8(2) (d) also provides for a risk assess-
ment of the working environment.
The same is true of section 8(2)(e) dealing with
training of and information to employees.
In discussions with the Chief Inspectorate of Labour
during the drafting of these guidelines, the following
practical steps were tabled by the Inspectorate to
guide employers in adhering to the above-mentioned
requirements (see Algorithm D).
Recommended action steps to prevent,reduce and eliminate WRULDs in theworkplace)
Page | 46 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
75 Regulations 6 and 8.
STEP 1: NOTIFY THE NEAREST INSPECTORATE OF
LABOUR WITHIN 14 DAYS OF DEFINITIVE
DIAGNOSIS BEING MADE
STEP 2: OBTAIN AN ERGONOMIC ASSESSMENT
STEP 3: COMPILE A SUBSEQUENT PLAN OF ACTION
STEP 4: IMPLEMENT THE PLAN OF ACTION AND
REVIEW IT AT APPROPRIATE INTERVALS
W. CL. 1 EMPLOYER’S REPORT OF AN
OCCUPATIONAL DISEASE OR
W. CL. 305 EMPLOYEE AFFIDAVIT FOR AN
OCCUPATIONAL DISEASE (WHEN THE
EMPLOYER DOES NOT TIMEOUSLY SUBMIT
THE EMPLOYER’S REPORT OF AN
OCCUPATIONAL DISEASE (W. CL.1))
W. CL. 301 FIRST MEDICAL REPORT IN RESPECT OF A
WORK-RELATED UPPER LIMB DISORDER
(WRULD)
W. CL. 302 PROGRESS/FINAL MEDICAL REPORT IN
RESPECT OF A WORK-RELATED UPPER
LIMB DISORDER (WRULD) (MONTHLY)
The improvement of the employee’s working condi-
tions by reducing the ergonomic risks is not only a
legal requirement as stated above, but is also part and
parcel of the employee’s integrated treatment plan
(see p. 41). Determination of impairment is also not
feasible if task and equipment adaptations were not
considered as part of the final report.
STEP 1: Notify the Inspectorate of Labour
The Inspectorate of Labour must be notified within 14
days of definitive diagnosis being made. Copies of the
following forms which was sent to the Compensation
Commissioner, should be sent to the nearest Provincial
Executive Manager of Labour.
STEP 2: Obtain an ergonomic assessment
It is recommended that the employer obtain an
ergonomic assessment of the workplace if WRULD is
diagnosed.
An ergonomics report can only be compiled by an ergono-
mist or one with knowledge of ergonomics and who is
competent to do so – this may be a “safety officer”, an
occupational health practitioner, a physiotherapist, an
occupational therapist or an occupational hygienist.
NOTE:
The Compensation Commissioner will not be liable to pay
for any ergonomic reports.
The costs of ergonomic reports should be carried by
the employer. It is the employer’s responsibility to
assess the health hazards in the workplace according

to the Occupational Health and Safety Act and the
Mine Health and Safety Act.
Therefore employers are required to examine their own
organisation to assess whether other employees are
likely to be at risk of developing WRULDs as a result
of the jobs they do, the environment they work in and
any other organisational factors.
A practical approach to identify and assess risks in
the workplace which may cause WRULDs is discussed
in detail in the next chapter. (See 14, p. 50)
STEP 3: Compile a plan of action
If an ergonomic assessment (see Step 2 above) was
done, the employer should compile a plan of action to
eliminate / reduce the ergonomic risks which may lead
to the development of WRULDs. Such a plan should
have the following elements:
A plan to implement the ergonomic recommenda-
tions (see Step 2 above)
A plan to manage the health surveillance of
employees (see 15, p. 64)
A plan to negotiate a health and safety policy on
the prevention of WRULDs (see 16, p. 67)
The Chief Inspectorate of Labour advises employers to
have such a plan of action ready within 3 months of
the definitive diagnosis being made.
STEP 4: Implement the plan of action andreview it at appropriate intervals
Having adopted a step-by-step approach in identifying
locations in their organisation which have the
potential for WRULDs, as well as identifying those at
risk, employers must now implement appropriate
measures for purposes of prevention and control.
The Chief Inspectorate of Labour advises employers to
implement such a plan of action (see Step 3 above)
and to have the following available within 6 months of
the definitive diagnosis being made:
A review of progress made regarding the
implementation of the ergonomic plan of action,
especially the progress made to adjust/modify the
job to the person and not attempts to fit the
person to the job.
A summary of progress made in the implement-
ation of an occupational health programme
(including a health risk assessment and a medical
surveillance programme).
The negotiated policy on the prevention of WRULDs
signed by the management, labour union represen-
tatives and an occupational health practitioner.
Page | 47 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
Table 22. Various components of an ergonomic survey
ORGANISATIONALFACTORS
• ORGANISATION OF WORK
• JOB ROTATION
• MANAGEMENT STYLE
• WORK RATE
• MONITORING
• CONSULTATION
• BONUS SYSTEMS
• STRESS, ETC.
ENVIRONMENTAL FACTORS
• COLD TEMPERATURES • VIBRATION, ETC.
TASK ANALYSIS • INDICATE A BRIEF DESCRIPTION OF THE TASK
INDIVIDUALFACTORS
• PHYSICAL CONDITION
• TRAINING
• PERSONAL PROTECTIVE
EQUIPMENT, ETC.
HUMAN – TASKINTERACTION
• USE OF FORCE
• REPETITIVE MOVEMENTS
• RAPID MOVEMENTS
• TWISTING MOVEMENTS
• AWKWARD POSTURES
• OVERSTRETCHING
• LACK OF REST BREAKS
• STATIC LOADING
• DESIGN OF TOOLS AND
EQUIPMENT, ETC.

Page | 48 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
STEP 1: WITHIN 14 DAYS OF DEFINIT IVE DIAGNOSIS BEING MADE
A COPY OF THE NOTIFICATION OF A WRULD TO THE COMPENSATION COMMISSIONER SHOULD BE SENT TO THEPROVINCIAL EXECUTIVE MANAGER OF LABOUR (OHS ACT) WITHIN 14 DAYS OF THE DIAGNOSIS BEING MADE.
STEP 2: OBTAIN AN ERGONOMIC ASSESSMENT
STEP 3: COMPILE A PLAN OF ACTION
PLAN OF ACTION
OCCUPATIONAL HEALTH PLANSHOULD MAKE PROVISION FOR
EDUCATION, HEALTH RISK ASSESSMENT AND MEDICAL
SURVEILLANCE
NEGOTIATE A POLICY ONPREVENTION OF WRULDs
WITH EMPLOYEES
ERGONOMIC REPORT
• ORGANISATIONAL FACTORS • TASK ANALYSIS • INDIVIDUAL FACTORS • HUMAN – TASK INTERACTION • ENVIRONMENTAL FACTORS
3 REPORT THE FOLLOWING TO THE PROVINCIAL EXECUTIVE MANAGER OF THE DEPARTMENT OF LABOUR
(OCCUPATIONAL HEALTH AND SAFETY ACT)
DETAILED ERGONOMIC PLAN OF ACTION
WITH TIME-SCALE
STEP 4: IMPLEMENT THE PLAN OF ACTION AND REVIEW IT AT APPROPRIATE INTERVALS
THE EMPLOYER WILL SUBMIT A REPORT CONTAINING:
PROGRESS MADE WITH HEALTH RISK ASSESSMENT
AND MEDICAL SURVEILLANCE
THE NEGOTIATED POLICY ON PREVENTION OF WRULDs
A REVIEW ON PROGRESS MADE REGARDING THE
IMPLEMENTATION OF THEERGONOMIC PLAN OF ACTION
D The employer reporting WRULDs to theDepartment of Labour

SECTION E-1For the employer
Ergonomic plan of action

14 A practical approach to identify and assess risksin the workplace which may cause WRULDs
14.1 Ergonomics and its practice
“Ergonomics is the scientific discipline concerned
with the fundamental understanding of interactions
among humans and other elements of a system, and
the profession that applies theory, principles, data
and methods to design in order to optimise human
well-being and overall system performance”.
International Ergonomics Association (IEA) 2000.
Ergonomics is a rigorous, applied science and at an
international level all registered ergonomists must
have at least an MSc in Ergonomics. Often “safety
officers”, occupational health professionals, physio-
therapists, occupational therapists and occupational
hygienists are able to conduct basic ergonomic
surveys or analyses, but not just anyone can offer
ergonomically sound intervention strategies in more
complicated cases. There is a growing number of
guidelines being written for occupational health
professionals on the basic principles of basic
ergonomics, but we urge occupational health profes-
sionals and employers to recognise their limitations
and call in a qualified ergonomist on a regular basis.
Ergonomic enhancements can, and should, play a
major role in furthering the health and safety of
workers and improving the quality and quantity of
productivity. This improved productivity is essential
for the economy of the country and will be achieved
not by the workers being pushed to work harder, but
by running companies on sound ergonomics principles
resulting in improved worker efficiency and less
physical and mental stress being placed on workers.
Physical ergonomics is concerned with human anatomical,
anthropometric, physio-logical and biomechanical
characteristics as they relate to physical activity.
Relevant topics include working postures, materials
handling, repetitive movements, heavy work, work-
related musculo-skeletal disorders, workplace layout,
safety and health.
Cognitive ergonomics is concerned with mental
processes, such as perception, memory, reasoning,
and motor response, as they affect interactions among
humans and other elements of a system. Relevant
topics include mental workload, decision-making,
skilled performance, human-computer interaction,
work stress and training as these may relate to the way
humans work in systems.
Organisational ergonomics is concerned with the
optimisation of socio-technical systems, including
their organisational structures, policies, and processes.
Relevant topics include human system considerations
in communication, human resource management,
work design, design of working times, teamwork,
participatory design, community ergonomics, cooperative
work, new work paradigms, virtual organisations,
tele-work, and quality management. While the emphasis
in any ergonomic investigation may be more in one
domain than the other, it is important to realise that
no thorough evaluation of a work site should ever be
exclusively in one area: a holistic approach is the very
essence of any ergonomic assessment.
With the growing awareness of ergonomics in industrial
developing countries it is important that the limited
number of ergonomists establish a “functional
partnership” with other professionals involved in
addressing the challenging problem of improving the
often horrendous working conditions, as well as the
health and safety of people working under these
conditions.
Ergonomic principles applied systematically will
ensure improved working conditions, thereby reducing
the risks of injuries and illness arising from working
under poor conditions. A prime objective of ergonomics
is to increase worker efficiency and reduce the like-
lihood of excessive physical and/or mental strain
being placed on the worker, thereby improving
productivity, with obvious benefits for workers and the
organisation.
14.2 Ergonomic analysis – practical steps
Changing social attitudes have made most jobs/tasks
non-gender specific. If the person performing a job
has the physical and mental capability to successful-
Page | 50 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0

ly and safely complete the task, by law he/she has the
right to perform that job. Concurrent with these
trends, is the need to develop safe, efficient environ-
ments which allow for adjustability to accommodate
persons of varying physical dimensions and skill
capabilities. When taking into account subject specif-
ic factors like gender, age and cultural background,
the problem of fitting the task to the user becomes
difficult.
The complexity of an ergonomic assessment is limited
only by the physical resources available to the
investigator. Many thorough ergonomic assessments
have been completed with a ruler, weigh scale and
(sometimes) photographic equipment. Although some
of the data reduction is computation intensive, insight
may be gained from easily obtainable information.
An existing job design will as a rule determine:
the types of tasks performed
how tasks are performed
the order in which tasks are completed
the type of equipment needed to complete the task
One must always keep these factors in mind when
assessing a task. Generally, the types of tasks
performed are the only factors which remain fixed.
However, how tasks are performed and the order in
which these tasks are completed, may be factors
which can be adjusted to improve overall task
performance and decrease risk for injury or error.
Although the type of equipment required for the task
is often a fixed variable, suggestions for alterations to
equipment may be necessary, especially if equipment
design is deemed responsible for causing acute or
chronic injury to the worker.
The following criteria have been identified as necessary
for a well-designed job (Stones, 198976):
Allows worker to vary body position to avoid
physical strain
Allows worker to frequently change mental tasks to
avoid mental fatigue
Gives worker a sense of accomplishment
Provides adequate work/rest ratios which allows
the person adequate time to complete the task and
recover in order to continue to the next task
Allows an adjustment period (warm-up) for physi-
cally demanding tasks (habitualise to the working
conditions)
Prompts worker as to what tasks to do and how to
complete them
In order to successfully make recommendations for
improved manners in which a task/skill is to be per-
formed, these criteria should be satisfied. Depending
upon the specific job being considered, some of the
listed criteria will rank higher in importance than oth-
ers. However, the following should be considered: The
ultimate goal of an ergonomic analysis is to ensure
that a person is satisfied physically, psychologically,
and socially with their work situation.
14.3 Principles of task/workplace assessment
14.3.1 Heed concerns of workers and supervisors
The most efficient form of ergonomic assessment is to
ask all individuals (involved in completing a task)
about their specific concerns and suggestions for cor-
recting the situation. Workers involved directly with a
task will as a rule delineate specific problems for the
safe and successful completion of the task.
Management and supervisors will detail specific per-
formance standards expected of the worker.
Performance expectations may be a fixed variable or
one that is presently unacceptable from a human per-
formance point of view.
14.3.2 Gain better understanding of jobs and tasks
For optimal understanding of a job or task, one should
perform it oneself. This may not however always be
feasible, especially where complicated or dangerous
tasks are being assessed. First-hand experience could,
however, be invaluable when assessing a task. In
attempting a skill or job, one must always be aware of
the physical and mental demands involved. For
example, is the task physically reasonable; can the
task be performed for an extended period of time; is
there evidence of physical or mental stress?
Cognisance of these questions allows for better
decision-making on task components to be considered
in greater detail.
Page | 51 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
76 Stones (1989)
14.3.3 Identify existing and potential hazards
There are several checklist-type surveys which can be
used to organise the assessment of a task. These
checklists are discussed in more detail later in this
chapter. The scope of an ergonomic assessment is
generally limited to specific or potential hazards.
14.3.4 Determine underlying causes of hazards
Use the Ergomax’s (Pty) Ltd. checklist (see 14.7 –
14.10) to determine factors contributing to a claimed
WRULD. The total score will enable one to determine
potential risk and the area/s which are deemed high risk.
14.4 Recommend changes and monitor hazard controls (personal protectiveequipment, engineering controls, policies, procedures)
Once causal factors have been identified, they should
be monitored on at least a weekly basis. If changes
have been done, it is important that these changes be
monitored and assessed.
14.5 Workplace observation considerations
The first inspection of a worksite or task will provide
one with basic information for initiating a more
comprehensive ergonomic assessment. It should be
kept in mind that a worker may alter work habits or
execution of skills if there is any suspicion of being
observed. Observations should be as discreet as
possible and if management and employees agree, a
video or still photography record could be obtained
(this process could be sensitive, particularly when
workers’ union or management policies are
considered).
The following has been adapted from Stewart (1989)77
and is based on the U.S.A. National Safety Council’s
report on poor common working practices. These
include items to be noted on initial inspection, more
specifically for an industrial setting.
Using equipment without authority or previous
instruction/certification
Operating at unsafe speeds, rates or repetitions
Removing guards or other safety devices, or
rendering them ineffective
Using hands or body instead of tools or push sticks
Overloading, crowding or failing to balance
materials, or handling materials in other unsafe
ways, including improper lifting techniques
Repairing or adjusting equipment which are in
motion, under pressure, or electrically charged
Failing to use or maintain, or improperly using
personal protective equipment or safety devices
Creating unsafe, unsanitary or unhealthy
conditions by improper personal hygiene, by using
compressed air for cleaning clothes, by poor
housekeeping, or by smoking in unauthorised areas
Standing or working under suspended loads,
scaffolds, shafts or open hatches
14.6 Assessing working environment forWRULDs
Many employers find a checklist useful in deciding:
If other employees are at risk of developing
WRULDs
Whether they need to take more precautions; and
What to do.
Following a step-by-step approach in assessing
potential WRULDs in their organisation and identify-
ing those at possible risk, employers must implement
the appropriate measures needed to prevent or control
the risk of WRULDs:
Useful checklists are supplied with kind permission of
the Health and Safety Executive (HSE) in the United
Kingdom. One does not need any specialist knowledge
to complete these. “Yes” entries in the checklist imply
that action is required. The more “Yes” entries, the
more urgently one should act. Risks may be much
higher than average where several things are present in
the same job which may cause WRULDs.
14.6.1 Ergomax risk calculator
Ergomax (Pty) Ltd developed a WRULDs risk
calculator which could be used to assess and score
(as percentage) the critical ergonomics risk factors
an employee is exposed to (Kennedy 2004)78
Page | 52 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
77 Stewart (1989) 78 Kennedy (2004)

(see 14.7 – 14.10). The calculator may also be used
as a preventative tool in assessing various workstation
tasks.
In situations where only one risk factor can be
identified, a more in-depth ergonomic assessment of
that particular risk factor is required. The calculator
may score the one risk as low and not give a true
reflection of the severity of the risk. Although one
isolated factor is rarely evident, the likelihood should
nevertheless be considered.
Ergomax’s risk calculator is available on their website:
http:\\www.ergomax.co.za. It can also be done manu-
ally on the following page.
14.6.2 Using the risk calculator
The Total WRULDs Risk Score (TWRS) is obtained by
adding the score for each Task Risk Score (TRS) and
each Human Risk Score (HRS) and multiplying this by
50 to get a percentage score. The following formula
can thus be used:
Page | 53 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
79 Kennedy (2004) 80 Kilbom (1994)
The task risks discussed below score as either:
TWRS = 50 X [(TRS / 36) + (HRS / 18)]
T W R S = T O TA L W R U L D s R I S K S C O R E A S
P E R C E N TA G E
T R S = T O TA L TA S K R I S K S C O R E ( A D D T O G E T H E R
A L L 9 TA S K R I S K S )
H R S = T O TA L H U M A N R I S K S C O R E ( A D D
T O G E T H E R A L L H U M A N R I S K S )
Any score above 30% is deemed to predispose the
employee to WRULDs.
One can then review the risk data sheet and deter-
mine where the greater risks are. Obviously factors
such as age and gender cannot be adjusted for. The
variables relevant to these human factors need there-
fore to be modified (Kennedy 2004)79.
14.7 TASK RISKS
In Circular Instruction 180 various risk factors are
mentioned that could contribute to the development
of WRULDs. In this section these task risk factors are
defined and practical tools are suggested on how
these task risks could be assessed and scored.
1 = L O W R I S K
2 = M E D I U M R I S K
4 = H I G H R I S K
Note: if a risk is not present, the score is 0
If there is immediate danger, shut down and “lock
out” any hazardous items which cannot be brought to
a safe operating standard until repaired.
14.7.1 Highly repetitive movements
Repetition is a matter of definition (“more than once
per time unit”) and what is low or high depends on
the specific activities or body part involved.
A concern is that in numerically describing the
frequency of an activity one presumes that the actions
occur at regular intervals during the recording time.
Yet, in reality, this is commonly not the case for an
average working day: certain activities may run
concurrently during some periods and may seldomly
occur during others.
Ergomax’s risk calculator is based on data published
by Kilbom (1994)80. Both the number of hand manip-
ulations per 8-hour work shift and the task cycle time
have been used to rate this factor. Task cycle times of
30 sec or less were defined as high repetition; cycle
times greater than 30 sec as low repetition. For hand
manipulations, high repetitiveness was described as
more than 20,000 manipulations per 8-hour work
shift; medium repetitiveness as between 10,000 and
20,000 manipulations per 8-hour work shift, and low
repetitiveness as less than 10,000 manipulations per
8-hour work shift.
These guidelines also consider other areas of the
upper extremity. Each area may have a different abil-
ity to tolerate repetitious activity. At the same rate of
repetitions some specific acts such as pinching may
be less well tolerated than others. This is an example
of complexities that current guidelines may not
address adequately.

Repetition calculator: highly repetitive movements
How often does the repetition occur during an 8-hour
shift or per minute? (Count the number of upper limb
movements the employee makes in one minute)
Ergonomic solutions for force
To reduce the risk of injury, design tasks that min-
imise stress on the body:
Use rollers to move objects
Use mechanical lifting aids
Use two or more people to help lift or move heavy
loads
Use hand carts or dollies with large diameter
wheels for moving objects
If possible use larger muscle groups to complete
the task
14.7.3 Movements at the extremes of reach
Extreme reach is defined as the working area that
occurs outside of your wrist, elbow or shoulder cir-
cumference zone.
For example, if you were to sit at a desk with your
upper arms relaxed and your elbows bent at 90
degrees and you move your forearms in a semi-circle
(like windscreen wipers of a car) that would be your
zone of convenient reach. Obviously this applies in
both the horizontal and vertical directions.
Movements at the extremes of reach predispose the
employee to arm injury due to the static nature the
shoulder muscles have to endure to hold the arm in an
extended position. Furthermore, the further one
reaches, the more the facet joints of the vertebral
bodies are loaded. This increases the shearing forces
within the spine and in turn stresses the surrounding
soft tissue which may result in neck and lower back
pain.
Reach risk calculator: extremes of reach
How far from the centre of the hip to the centre of the
object does the movement occur?
(Measure the distance from the middle of the hip joint
Page | 54 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
SCORE LOW MEDIUM HIGH(1 POINT) (2 POINTS) (4 POINTS)
REPETITIONS <10,000 10,001 – >20,001PER 8-HOUR SHIFT 20,000
OR OR OR OR
REPETITIONS 20 – 30 31 – 41 >41PER MINUTE
Ergonomic solutions for repetitiveness
Repetitive motions can have cumulative effects. To
reduce the risk of injury, perform tasks so as to min-
imise stress on the body:
Implement frequent short rest breaks
Minimise the number of motions between opera-
tions
Use conveyors, chutes, slides and turntables to
change direction of material flow
Prevent movements occurring at the extreme range
of motions
14.7.2 Movements requiring force
Force is defined as any muscular contraction that
requires extended effort over a given time period.
Forcefulness is also a matter of definition and what is
low or high depends on the specific activities or body
part involved. Not everyone has the ability to measure
force as this is often expensive. For the purpose of
these guidelines any force exerted over an extended
time period places the employee at risk.
Force risk calculator: movements requiring force
How long does the forceful movement last during an
8-hour shift?
(Time the duration of the movement, for example if
one has to turn a screwdriver for half and hour every
hour, then the total risk for this category would be 4
hours or 240 minutes)
SCORE LOW MEDIUM HIGH(1 POINT) (2 POINTS) (4 POINTS)
EXERTION OF FORCE PER MINUTE PER 8-HOUR SHIFT 1-120 121- 240 >240

to the middle of the object being manipulated)
Page | 55 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
Static muscle risk calculator
How long is the static posture held?
(Time the duration the employee has to hold his arms
above his head, for example if one has to turn a
screwdriver for half and hour above one’s head, every
hour, then the total risk for this category would be 4
hours or 240 minutes)
Ergonomic solutions for reach
Keep working zones within “safe working parame-
ter” (see diagrams in section 14.9, p. 55)
Avoid obstacles which necessitate employees lean-
ing over in order to reach controls
Place objects used most frequently within safe
working zones
14.7.4 Static muscle loading
Static postures may be defined as postures that are
held for longer than 30 seconds, without the limb
moving.
Fixed postures also result in static (isometric) muscle
contractions. A muscle that is actively involved in
concentric and eccentric contractions converts glu-
cose and oxygen into carbon dioxide and water, liber-
ating energy in the process. Muscles therefore require
a regular blood supply in order to replenish fuel and
remove waste products. The rhythmic pumping action
of an active muscle facilitates this flow of blood.
However, during sustained isometric contractions a
muscle occludes the blood vessels within it, resulting
in diminished blood supply. The muscle is thus
starved of oxygen and waste products accumulate as
oxygen-independent metabolic processes take place.
Discomfort and fatigue occur rapidly for this reason,
as well as the increased risk of WRULDs.
For example, if one has to fit a light bulb above your
head, you would have to hold your arms above your
head continually in order to position and screw in the
bulb. This results in a static muscle posture of the
shoulder muscles and fatigue sets in quickly.
Ergonomic solutions for static muscle loading
Try avoiding the static posture where possible
Allow lifting devices, jigs or turntables to hold and
move the load whilst handling it
Increase the number of rest breaks
14.7.5 Awkward sustained postures
Postures that are not within the normal reach zones of
the employee are considered to be awkward.
This variable needs to be measured individually for each
employee assessed, as we all have various working
postures. The time spent working in this posture will
need to be considered to calculate the risk exposure.
For example, if one has to fully bend one’s wrist in
order to thread material through a sewing machine,
this wrist posture will be deemed awkward.
Risk calculator: awkward postures
How long is the awkward posture maintained?
(Time the duration the employee has to hold his hands
in an awkward position, for example if one has to turn
a screwdriver for half and hour, with hand bent every
hour, then the total risk for this category would be 4
hours or 240 minutes)
SCORE LOW MEDIUM HIGH(1 POINT) (2 POINTS) (4 POINTS)
MEASUREMENT IS 150 – -599 600 – 750 >750 MMTAKEN FROM THE MM MMPERPENDICULAR DISTANCE BETWEEN THE CENTRES OF THE HIP TO CENTRE OF THE OBJECT BEING LIFTED (MILLIMETRES)
SCORE LOW MEDIUM HIGH(1 POINT) (2 POINTS) (4 POINTS)
MINUTES PER 8-HOUR SHIFT 1-120 121-240 >240
SCORE LOW MEDIUM HIGH(1 POINT) (2 POINTS) (4 POINTS)
MINUTES PER 8-HOUR SHIFT 1-120 121-240 >240

Ergonomic solution for awkward postures
Keep working zones within “safe working parame-
ter” (see diagrams in section 14.9, p. 55)
Avoid obstacles which necessitate employees lean-
ing over in order to stretch and reach controls
Design hand-held tools to accommodate the angle
of use, instead of the employee having to bend his
wrist, for example
14.7.6 Contact stress
Contact stress is defined as the time spent leaning/
pressing the upper limb against an uncomfortable
surface (e.g. uncomfortable gripping and twisting,
sharp edges to hand tools, desk edges, etc.)
The risk calculator considers the time spent in con-
tact with the object. For example, if one leans one’s
elbows on the desk all day to type, the contact stress
for the elbows will be considered a high risk
Contact stress calculator
How long is contact made with an object?
(For example: Time how long the employee has to lean
his hand against his desk in order to type)
Page | 56 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
Ergonomic solutions for contact stress
Avoid employees having to lean against objects or
machinery
Design appropriate surface edges for employee to
work against. (Round square edges)
Proven adequate Personal Protective Equipment
(PPE) for employees who have to hold tools for
extended periods
14.7.7 Vibration
Vibration is defined as any hand-held tool or working
surface that shakes, pulsates whilst in use.
The calculation of vibration exposure is often costly
and difficult to administer. For ease of use, Ergomax
uses length of time exposure to vibrations. Obviously
exposure limits will vary according to the area of the
body affected and the frequency of vibrating cycles
per second exposure. Vibration exposure can affect
your upper limbs when using hand-held power tools,
hand-guided tools or holding material being processed
by machinery.
Vibration risk exposure
How long is the employee exposed to vibrations?
(Time how long the employee has to stand or use
vibrating equipment.)
SCORE LOW MEDIUM HIGH(1 POINT) (2 POINTS) (4 POINTS)
MINUTES PER 8-HOUR SHIFT 1-120 121-240 >240
SCORE LOW MEDIUM HIGH(1 POINT) (2 POINTS) (4 POINTS)
MINUTES PER 8-HOUR SHIFT 1-120 121-240 >240
Ergonomic solution for vibration
Minimise exposure to vibrations from hand-held
tools.
Consider using anti-vibration gloves when using
vibrating tools
Maintain tools regularly
Vibration exposure
Note: the best way to quantify vibration exposure is to
calculate the daily vibration exposure. This, however,
is often difficult, as suppliers often do not indicate
the vibration magnitude. The vibration exposure is
dependant on the duration of exposure to a reference
period of 8 hours, thereby allowing different expo-
sures to be compared. It is currently recommended
that preventative measures and health surveillance be
provided when workers’ daily vibration exposure regu-
larly exceeds 2.8m/s2 A(*8).
It is possible to calculate the vibration exposure when
the vibration magnitude of the tool is known. For
example, information from a supplier of a chainsaw
states that vibration magnitude is 9.7 m/s2. The
equipment is used for 2 hours daily.

Using A(8) = ahw√t/8
where: t is the daily exposure time; ahw is the vibration
magnitude
A(8) = 9.7√2/8
Average for 8 hours = 4. 8m/s2
14.7.8 Load exposure
Load is defined as the weight of the object being lifted.
Obviously, the heavier the load, the more strenuous
and dangerous the task. The introduction of mechan-
ical devices for handling heavy materials, the division
of heavy items into smaller objects or two workers
involved in handling one heavy item reduces the
fatigue caused by handling heavy weights, and worker
productivity is improved. The risk of back injuries is
also greatly reduced.
Load risk calculator
What is the weight of the load lifted or handled?
(Weigh the tool or load that the employee has to
operate or lift)
Page | 57 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
SCORE LOW MEDIUM HIGH(1 POINT) (2 POINTS) (4 POINTS)
KILOGRAM < 5KG 5,1 – 7 KG >7KG
SCORE LOW MEDIUM HIGH(1 POINT) (2 POINTS) (4 POINTS)
MINUTES PER 8-HOUR SHIFT 1-120 121-240 >240
Ergonomic solutions for load
Minimise the load as far as reasonably possible
Lift loads within safe range of motion zones
Lift directly in front of the body
Eliminate or reduce lifts occurring in confined
spaces
Decrease frequency of lift
14.7.9 Cold exposure
Cold is defined as the environment temperature being
below 18 degrees Celsius where discomfort is felt.
In general, when it is too cold, or when we touch cold
materials, our hands can become numb. Due to the
physiological changes that occur due to cold expo-
sure, one is more likely to misjudge the amount of
force required to complete work and normally exert
too much force. A cold environment also makes our
bodies less flexible. Every movement made and every
position held takes more effort.
Cold risk calculator
How long does the employee spend working in a cold
environment?
(Time the length of shift the employee is working in a
cold environment)
Ergonomic solutions for cold environments
Minimise the exposure to cold environments as far
as reasonably possible
Allow adequate personal protective equipment
against the cold.
14.8 Additional guidelines to WRULDs assessment
a.) Do not operate equipment unless authorised to do
so. Ask the operator for a demonstration. If the
operator of any piece of equipment does not know
what dangers may be present, this is cause for con-
cern. Never ignore any item because you do not
have the necessary knowledge to make an accurate
judgement of safety.
b.) Look up, down, around and inside. Be methodical
and thorough. Do not spoil your limited inspection
opportunities with a “once-over-lightly” approach.
c.) Clearly describe each hazard and its exact location
in your rough notes. Allow recording of all findings
before they are forgotten or inspection is interrupted.
d.) Ask questions, but do not unnecessarily disrupt
work activities. This may interfere with efficient
assessment of the job function and may also create
a potentially hazardous situation.

e.) Consider the static and dynamic conditions of the
item you are inspecting. If a machine is shut
down, consider postponing the inspection until it
is functioning again.
f.) Discuss as a group: ‘Can any problem, hazard or
accident generate from this situation when looking
at the equipment, the process or the environment?’
Determine appropriate corrections or controls.
14.9 Ergonomic range of motion with safeworking zones
The following sketches may be used as a quick
reference to describe safe working zones for various
movements of the upper limb. Any movements
occurring outside the “safe working zone” is deemed
awkward and should be avoided where possible.
14.9.1 Wrist range of motion:81
Flexion/ Extension
Page | 58 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
81 Drawings and diagrams taken from Luttgens, K. & Hamilton, N. (1997).
Kinesiology: Scientific Basis of Human Motion, 9th Ed., Madison, WI: Brown
& Benchmark.
00 degrees neutral
500
Flexion
Safe working zone
Hyper extension
600
1800
1400
900
Safeworking
zone
00
Neutral
100 or lessHyper extension
Flexion
900
Safe working zone
00 Neutral
Inward rotation (internal)
Outward rotation (external)
900
900
900
500Safe working zone
00 Neutral
900
1800
Hyper extension
Forw
ard
flexi
on
14.9.2 Elbow range of motion
Elbow flexion extension
Radial and ulnar flexion
900
200
Safeworking
Neutral00
300
Radialflexion
Ulnarflexion
900
14.9. Shoulder range of motion
Internal and external rotation
Note: any work occurring above shoulder height is
deemed awkward for the purpose of these guidelines.
Shoulder flexion extension

14.10 Human risks – Human variables affecting WRULDs risk exposure
The human risks discussed below score slightly
differently than the task risks as each human risk has
independent associated risks:
14.10.1 Gender
Depending on one’s gender, the exposure or likelihood
of the development of WRULDs varies. Due to physio-
logical differences, females appear to be more predis-
posed to certain WRULDs relative to their male coun-
terparts. Use the table below to score the relevant
risk.
For female employees add a score of 2 to the total
human variable score.
14.10.2 Age
As one ages certain physiological and biomechanical
changes occur. For example one looses 1 percent of
one’s total strength capability each year from the age
of 25 onwards. These physiological changes,
associated with ageing, may increase the likelihood of
developing WRULDs in certain individuals.
Page | 59 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
SCORE LOW MEDIUM HIGH(1 POINT) (2 POINTS) (4 POINTS)
AGE (YEARS) 20-39 40-50 >51
SCORE LOW MEDIUM HIGH(0 POINT) (3 POINTS) (5 POINTS)
AGE (YEARS) 19-27 28-32 >32
SCORE LOW MEDIUM HIGH(3 POINTS) (5 POINTS) (7 POINTS)
PERIOD (YEARS) <2 2-5 >5
14.10.3 Body mass index (BMI)
Body mass index (BMI) is derived from the calculation
of body mass divided by height squared.
BMI = kg/m2
Body mass index can be used to indicate whether one
is overweight, obese, underweight or normal. It will,
however, overestimate fatness in people who are mus-
cular or athletic. One generally makes use of the BMI
index as a quick reference to the body composition of
an individual, instead of the lengthy process of meas-
uring ones fat content versus lean body mass. Women
will tend to score higher due to the physiological con-
stitution of their bodies.
14.10.4 Exposure history
Exposure history considers the environment in which
the employee has worked that have exposed him/her
to the risk factors of WRULDs. If the employee has
worked in an environment which has previously
exposed him/her to any of the seven task risk factors,
indicate the length of time he/she has been exposed.
14.11 Worked examples:
14.11.1 Industrial setting
An employee in a warehouse has to lift and place
more than 480 boxes on a conveyor belt above shoul-
der height each hour. The duration of the shift is eight
hours and the employee is required to complete this
task for the entire shift. The conveyor system is 1.8 m
above the ground. Each box is held briefly (3 sec)
whilst the conveyor partitioning moves into place in
order for the employee to load the box.
Task criteria:
Lifts occur 8 times per minute
Movements requiring force is throughout the shift
Static posture is held for 24 sec per minute
Awkward postures occur throughout the shift
Contact stress occurs for 36 sec per minute
The weight of the load is 8 kg
The distance that the box has to be moved is
1.8 m
There is no vibration exposure

Human criteria
The employee’s age is 42 yrs, is a female and has
been exposed to one or more of the seven risk fac-
tors for approximately 5 years. Her height is 1.61
and weight is 74 kg.
BMI = 74/1.61m2
= 74/2.592
Total WRULDs Risk Score:
TWRS = 50 X [(TRS / 32) + (HRS / 18)]
= 50 X [(18/32) + (12/18)]
= 50 X [0.5625 +0.6666]
= 50 X 1.2291
= 61.45 %
14.11.2 Office setting
An employee is involved in editing magazine articles
and spends about 5 hours a day typing. She is 53
years old; height 168 m and weight is 63kg. Her
keyboard is placed 45 cm from the centre of her hip.
She has to hold her arms up in order to type on her
keyboard, due to the height of the desk. As a
consequence she has to rest her elbows on the edge of
her desk. She makes over 100 repetitions with her
fingers each minute. She has been at this job her
whole working career.
Task criteria:
Repetitive movements occur more than 100 times
per minute
She types for 5 hours a day (force)
Her keyboard is placed 450 mm from the centre of
her hip (reach)
Her shoulder muscles have to hold her arms up
whilst typing (static)
She rests her elbows on the desk whilst typing
(contact)
Human criteria
The employee’s age is 53 yrs, is a female. Her
height is 1.68 m and weight is 63 kg.
BMI = 63/1.68m2
= 63/2.8224
= 22.3
Total WRULDs Risk Score:
TWRS = 50 X [(TRS / 32) + (HRS / 18)]
= 50 X [(22/32) + (13/18)]
= 50 X [0.6875 +0.7222]
= 50 X 1.409
= 70.46 %
14.12 Ergonomic intervention strategies
14.12.1 Deciding how to reduce risks
Approaches to problems can include people-based
solutions (e.g. training, adding variety to the job,
appropriate treatment of the individual and reschedul-
ing rest breaks) as well as alterations to workstations,
tools or the work environment. However, no single
approach is successful all the time and as such,
several solutions need to be investigated.
Often straightforward and inexpensive changes are all
that is required. Again, remember to consult the
workers who are actually doing the job. They should
know what the difficulties are and may have good
ideas on how to modify the task.
Unusual WRULDs problems may require more
complex solutions, for example where risks are high,
or where several interacting risk factors exist. Here,
approaches such as redesigning workstations,
providing better tools, or supplying sub-components
already assembled may help. If not, one may have to
consider fundamental changes of approach such as
automation, or changing from assembly-line to other
production methods. One could also consider intro-
ducing job rotation – which implies workers in a team
exchanging jobs at intervals to provide greater variety.
Remember, if one introduces new tools, equipment or
working methods, workers will have to be trained in
order to get the best results (both for health and
safety, as well as productivity).
An employer should make sure that staff knows who is
Page | 60 | of pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0

responsible for taking action to reduce the risks for
WRULDs.
14.12.2 Ergonomic principles
The following main ergonomic principles must be
taken into consideration when implementing an
ergonomic plan of action
a) Avoid the risk altogether (e.g. by not using a par-
ticular tool or process)
b) Combat risks at source rather than applying pallia-
tive measures
c) Adapt work to the individual, especially as regards
the design of workplaces, the choice of work
equipment and the choice of working and produc-
tion methods, with a view to eliminating monoto-
nous work and work at a predetermined rate
d) Take advantage of technological and technical
progress to improve working methods and make
them safer
e) Ensure that the measures form part of a coherent
policy of reducing risks, which takes account of
the way work is organised, working conditions, the
working environment and any relevant social fac-
tors
f) Give priority to measures which protect the whole
workforce
g) Ensure that workers understand what they need to
do by providing information and training
h) Ensure an active health and safety culture
throughout the entire workplace
i) Conduct regular evaluations of the situation in
order to be pro-active to potential problems
Page | 61 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0

Table 23. Some of the main measures that employers can take to prevent WRULDs
A qualified ergonomist can be of great value in providing expertise and advice so that WRULDs can be eliminated
from the workplace:
Improving the work environment Improving task and equipment design
Page | 62 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
THE PHYSICAL WORK ENVIRONMENT CAN BE A SOURCEOF STRESS AND STRAIN TO WORKERS. EMPLOYERSCAN HELP TO REDUCE THESE STRESSES BY:
a ) Ensur ing no ise leve ls a re kept as low as poss ib le .
b ) Improv ing l i gh t ing leve ls and remov ing i r r i ta t ingf l i cke rs o r g la res .
c ) Improv ing tempera tu re and vent i l a t ion .
d ) Prov id ing we l l des igned pro tec t i ve c lo th ing and reg -u la r b reaks in a warmer env i ronment fo r worke rswho have to work in co ld cond i t ions o r w i th f rozenfoods .
e ) P rov id ing su i tab le res t a reas away f rom the works ta -t ion fo r worke rs to have recupera t i ve b reaks .
f ) Encourag ing f lu id in take a t a l l t imes but pa r t icu la r -l y in hot env i ronments .
g ) Reduc ing the need to use v ib ra t ing too ls .
h ) P rov id ing v ib ra t ion absorb ing g r ips on too ls and bymainta in ing them in a good s ta te o f repa i r.
THIS CAN BE DONE BY APPLYING GOOD ERGONOMIC PRINCI-PLES IN THE DESIGN OF TOOLS, EQUIPMENT, WORKSTA-TIONS, TASKS AND WORK METHODS. IMPROVEMENTS CANBE ACHIEVED BY:
a) Selecting tools and equipment appropriate for the job andsuitable for the individual who has to use them.
b) Maintaining tools in a condition which makes them easy touse, e.g. keeping them sharpened or lubricated.
c) Providing powered versions of tools.
d) Selecting tools with handles which allow the worker to workwith the limbs in a ‘natural’ alignment.
e) Redesigning workstation so that everything is within reach,or so that controls are easier to use.
f) Providing seats, equipment, etc., that can be adjusted tomeet individual needs and by providing training in how toadjust them.
g) Giving the worker an appropriate space in which to work.
h) Redesigning the task to minimise repetitive movements andstatic handling and/or sustained postures.
i) Automating the task.
j) Redesigning the work method to avoid overreaching andother awkward postures.
Improving work organisation Taking account of the individual
WORK SHOULD BE ORGANISED IN SUCH A WAY THATEMPLOYEES’ HEALTH AND SAFETY IS NOT PUT AT RISK.WORK ORGANISATION CAN BE IMPROVED IN A NUMBER OFWAYS, FOR EXAMPLE BY:
a) Improving communication between management and staff.
b) Consulting employees and their representatives about theirjobs and any changes they may suggest (participatoryergonomics).
c) Ensuring that jobs which pose a risk and which cannot becompletely eliminated are rotated so that no individualspends long periods on that task.
d) Ensuring that all employees have sufficient variety in thedemands of their task, thus ensuring different muscles andpostures being utilised and making their jobs more satisfying.
e) Providing adequate rest breaks with pause exercises to prevent the build-up of fatigue, and by ensuring that thebreaks are in fact taken, i.e. improving the work-to-restratio.
f) Identifying and limiting stress factors in the workplace.
g) Discussing the control of work pace and the overall plan forthe day with the workers.
h) Removing task rate and payment by results systems thatmake earnings dependent on excessive work rates.
i) Removing bonus, performance or monitoring schemes whichmake workers push themselves beyond their capacities.
j) Having proper monitoring and reporting procedures forsymptoms of WRULDs as well as appropriate work harden-ing programmes.
EMPLOYERS NEED TO ENSURE THAT WORKERS ARE NOT ATRISK THROUGH LACK OF TRAINING OR BECAUSE OF INDIVIDUAL FACTORS. THEY CAN HELP PROTECT THEIREMPLOYEES FROM DEVELOPING WRULDs BY:
a) Providing information and training about WRULDs and howto recognise the symptoms.
b) Providing information and training about how to avoidWRULDs through safe working techniques and safe workingpostures.
c) Advising employees on the importance of taking breaksbefore the onset of fatigue and of varying their work routines.
d) Informing employees of the importance of reporting symptoms of WRULDs as soon as possible.
e) Providing information on how to report symptoms ofWRULDs.
f) Ensuring that workstations and equipment can be fullyadjusted to accommodate people of very different sizes,heights or with particular needs.
g) Ensuring that workstations and equipment can be adjustedto the needs of people with disabilities.
h) Ensuring that males or females, left or right-handed work-ers, do not have to use equipment and tools designed forother groups.
i) Ensuring that new employees or those returning from a longbreak are allowed to build up their work rate gradually.
j) Ensuring that the wearing of personal protective equipmentor clothing (e.g. gloves) does not increase the risk ofWRULDs.
Care should be taken that this does not result in an over-eager-ness to report WRULDs in the hope of receiving compensation.

SECTION E-2FOR THE EMPLOYER
Occupational healthprogramme

15 Occupational health programme
Page | 64 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
Figure 9. Early detection andprevention of WRULDs
COM
PEN
SATI
ONIS
M
Early detection and prevention of WRULDs are very important – Koemar (1994) described early signs of WRULDs as the ‘fog’ slumbering in the valley in front of
the mountain! The ‘fog’ may partly obscure a volcano of WRULDs ready to explode!
Disability
Disorders, injuriesand diseases
requiring medical interventions
Pronounced symptoms make itdifficult to continue usual
activities
Soreness, pain, persistent aches and painsaffect well-being and performance
Occasional movement or posture problems, intermittent discomfort, fatigue, small aches
Fatigue and tiredness, uneasiness and discomfort generally considered ‘normal’ after a full day’s work
VERSUS PREVEN
TIONISM
Health risk assessment, adequate medical surveillance
and relevant health education and training should
form an integral part of an institution’s occupational
health programme.
15.1 Health risk assessment
As part of risk assessment, employers should check
whether any of their employees are already displaying
symptoms of WRULDs. However, it is important to
note that:
Many employees may not recognise their own
symptoms as WRULDs.
Many employees will be unaware of the serious
nature of WRULDs even if they do suspect the
symptoms.
Many employees will continue to work, regardless
of their symptoms.
Many employees will be unaware of the importance
of reporting their symptoms early.
Many employees will be afraid to report their
symptoms.
Early detection and prevention of WRULDs (Figure 9)
are very important. It is important to be on the look-out
for the ‘fog’ – the level of which indicates perception
and awareness of symptoms. The fog may partly
obscure a volcano of WRULDs ready to explode!82
Employers should take account of these problems
when trying to assess the extent of any existing
problem in their organisation.
One way to find out whether employees have WRULD
symptoms is for employers to look at their accident
book and at sickness absence records and to consult
their occupational health service if one is available.
However, since many employees will not recognise or
report symptoms, as already indicated, employers will
probably need to carry out a health survey of their
employees. This should be done in an open and trans-
parent way and employers will need to explain the pur-
pose of the survey and demonstrate a commitment to
resolving any problems, whilst guaranteeing employ-
ment security to anyone found to have symptoms. If
employees suspect that the real motive behind the
survey is to weed out people with problems, they will
82 Koemer (1994)

not have any confidence in the survey and are unlikely
to take part.
The survey itself will have to be appropriate to the
purpose and set out in a way that is easy to understand.
The language used should be simple, with translations
available in any other languages in common use
amongst the workforce. (See 15.1.1, p. 65) An example
of a simple form which incorporates questions about
symptoms with reference to different parts of the body
as well as questions about the job can be viewed on
the next page.
The role of trade unions is vital in ensuring that
surveys are done properly and are not used to weaken
job security and discriminate against employees. The
employer should consult the union at every step along
the way and obtain agreement for the method to be
employed.
15.1.1 Medical surveillance
Health surveillance can play an important role in the
prevention of WRULDs, by detecting symptoms early,
so that remedial action can be taken. It should be seen
as an essential backup to the preventive measures
taken to design WRULDs out of the workplace.
Employers should at the very least set up an internal
reporting system so that symptoms of WRULDs can be
monitored, recognised early, and treated before the
condition progresses to a more serious state. In order
for such a system to be effective, it must be explained
properly to employees so that they understand the
purpose of the system, how to recognise symptoms of
WRULDs, how to report them and what would happen
if they do report them. Employees are unlikely to
report symptoms if they think their future employment
will be at risk, so the system must be seen as a
positive element of the employer’s approach to
WRULDs prevention.
Some employers have tried to introduce pre-
employment screening in an attempt to weed out
people who may be susceptible to WRULDs. Not only
could this amount to discrimination under the law, but
the evidence shows that there is no reliable test
available. There is no scientific evidence to show that
pre-employment and preplacement screening can
predict the risk of developing a work-related musculo-
skeletal disorder. The principle must be to make the
workplace safe for everyone and not to try and select
a workforce of super-resilient men and women.
The Musculo-skeletal Wellness Questionnaire
(currently only available in English and Afrikaans) can
help you assess / screen potential WRULDs in the
workplace.
More detailed scientific musculo-skeletal questionnaires
are available for occupational health practitioners and
ergonomists, e.g. the Nordic Questionnaire which has
been adapted by the CSIR for the South African
mining industry.
Page | 65 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0

SECTION E-3For the employer
A policy on the prevention and
management of WRULDs

16 Negotiate a policy on the prevention and management of WRULDs
It is recommended that an employer negotiate a poli-
cy on the prevention and management of WRULDs.
This negotiated policy could be signed by the manage-
ment, health and safety committee representatives,
labour union representatives and an occupational
health practitioner.
The Trade Union Congress in the United Kingdom
(TUC) has published a model policy on the prevention
of WRULDs, which has been adapted with their kind
permission. As with all model policies, it is not some-
thing merely to be accepted and filed away, but
should be discussed, fully understood and adapted as
a living policy. This means that if such a policy is
introduced, the health and safety committee should
monitor its implementation and effectiveness.
The following model policy for the prevention and
management of WRULDs could be used as an example
by employers when developing their own custom-made
policy, which should be relevant for their own unique
circumstances:83
16.1 Aim
The aim of this agreement is to provide a healthy and
safe working environment and prevent the develop-
ment of WRULDs. The employer and the union recog-
nise that there must be a programme of preventive
action which should include the following commit-
ments:
a.) Management commitment to reduce the risk of
WRULDs.
b.) To consult the union on the development of the
programme.
c.) To provide resources for the information, instruc-
tion and training to be given to management, those
involved in design of work areas, supervisors and
employees on WRULD, its symptoms and its pre-
vention.
d.) To conduct risk assessments for tasks identified as
potentially hazardous by agreement with manage-
ment and the union, or subsequently through a
regular programme covering every aspect of work,
or in the event of significant changes to work
systems, work methods, equipment, environment
or training.
e.) To set up a competent Health and Safety working
group on WRULDs to oversee the implementation
of the WRULD prevention policy.
f.) To implement changes identified as necessary by
such risk assessments and review the implementa-
tion of these changes (e.g. an agreement on suit-
able rest breaks and pause exercises when neces-
sary during continuous repetitive work (dependent
on the intensity of the work).
g.) Clear procedures for early reporting of symptoms
and no victimisation or harassing of employees
who develop WRULDs or report symptoms.
h.) Clear procedures for dealing with diagnosed cases.
i.) An agreement that employees with WRULD symp-
toms will be offered temporary or permanent rede-
ployment and/or time off for recovery, as stated in
the Compensation for Occupational Injuries and
Diseases Act.
j.) An agreement that the employer will pay for any
reasonable treatment or investigations that are
required until the case is accepted by the
Compensation Commissioner, when these expenses
can be claimed from the Commissioner.
k.) To use an agreed occupational health practitioner
experienced in WRULDs to monitor staff on a
regular basis.
l.) A commitment to monitor and review the policy.
16.2 Risk assessments
The following factors which are known to cause or
contribute to WRULDs will be taken into account, in
terms of work equipment, workplaces and methods:
a) Frequency and duration of repetitive movements.
b) Force used in performing the movements.
Page | 67 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
83 Used and adapted with the kind permission of the London Hazard Centre.

c) Absence of adequate recuperative breaks.
d) Awkward postures, particularly degree of fixed
muscle loading in the trunk, shoulders and arms.
e) Static work load.
f) Degree of stress involved in the job contributed to
by its boring and monotonous nature or lack of
opportunity for initiative, responsibility or individ-
uality.
g) Sudden changes in work rate or fast pace of work.
h) Individual monitoring of work, leading to stress
and work pressure.
i) Vibration, temperature, lighting and glare.
The risk assessment will involve union and management
assessors and reports by competent persons, who should
also assist in implementing the preventive programme.
The employees concerned will be involved in the risk
assessment and be provided with a copy of it.
16.3 Information, education and training
The employer will consult with the union regarding an
education programme for employees, which will
include:
a) Ergonomic principles associated with work equip-
ment, workstations, work patterns, etc.
b) Ways of making necessary adjustments to furni-
ture, equipment, lighting, etc.
c) Regular monitoring of the workplace to ensure it
remains ergonomically sound
d) Exercises for eyes, shoulders, hands, arms, etc., to
prevent excessive strain on the muscles
e) Information on potential hazards associated with
methods of work and the importance of safe work
rates and adequate rest breaks
f) Information on management’s health and safety
policy
g) Information on health and safety reporting and
monitoring systems as well as the signs, symptoms
and management of WRULDs
h) Training of managers and supervisors in the sym-
pathetic handling of known or potential cases
16.4 Work routine
Management and the union agree that a reasonable
work rate varies with the capabilities of individual
employees, the demands of the task and environmen-
tal factors. The availability of rest breaks and pause
exercises (e.g. quick stretching exercises done at the
workstation for 60 seconds every 30 minutes) in work
involving WRULDs risk factors is necessary to avoid
the accumulation of fatigue and strain which con-
tribute to WRULDs. Breaks in work involving WRULDs
risk factors will therefore be provided on the basis of
an assessment of the overall situation and adjusted
accordingly. These breaks and pause exercises should
be in addition to personal health and meal breaks.
16.5 Notification
A notification system will be set up as follows:
a) Employees will be encouraged to report signs and
symptoms of WRULDs.
b) Incidences of such signs and symptoms will be
logged in the accident book.
c) Line managers will have responsibility for monitor-
ing the incidence of signs and symptoms and pro-
posing remedial action, including reviewing the
risk assessment, for employees for whom they are
responsible.
d) Safety representatives will be informed periodical-
ly of the incidence of signs and symptoms in their
area of responsibility and whenever the incidence
rises appreciably.
e) Annual statistics will be supplied to the health and
safety committee.
16.6 Responding to diagnosed conditions
When a case of WRULDs is medically diagnosed, man-
agement will assess necessary action on the basis of
medical advice, including:
a) The extent and nature of the condition
b) The possible causes of the condition
c) The course of treatment recommended
d) The length of time needed for rehabilitation, and
e) The limitations placed on employment in terms of
both tasks and recommended duration of work
Page | 68 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0

The following steps will be taken:
a) A review of the risk assessment of the job involved
by a competent person to be agreed on by both
management and union.
b) Provision of the assessment and reports to the
employee concerned.
c) Implementation, as appropriate, of changes, train-
ing and treatment necessary to enable the employ-
ee to return to his/her position, or of suitable
retraining and redeployment.
d) The granting of access to the workplace to health
professionals who are treating the employee.
e) Training of the employee in the application of
ergonomic and preventive principles.
f) The employer will report a case of WRULD 14 days
after the definitive diagnosis by a doctor to the
Compensation Commissioner and the Dept of
Labour / Minerals and Energy Affairs, as is
required by the COID Act..
g) The employer will submit the subsequently
required reports to the Dept of Labour / Minerals
and Energy Affairs, 3 and 6 months respectively,
after the date the definitive diagnosis was made.
16.7 Redeployment
Where the employee is redeployed, the following will
apply:
a) Job security will be a primary objective and
employees who have to take sick leave will
receive time off with pay until the
Compensation Commissioner reimburses the
company for the temporary total disablement.
(The COID Act determines that an employer will
pay 75% of the employee’s salary for three
months)
b) There will be full consultation with the employee
on career options and procedures prior to any deci-
sions being taken
c) Detailed job descriptions of prospective positions
will be provided to the employee, their treating
medical practitioner and their union
d) Modifications to prospective positions to make
them suitable in the light of the nature of the
condition and treatment will be undertaken where
necessary
e) A gradual return to work will be allowed with no
pressure to return to work until fully ‘fit’
16.8 Monitoring and review
Regular monitoring and annual review of this
policy will be carried out by the health and safety
committee and any difficulties reported to the
person responsible for the implementation of the
policy.
Page | 69 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0

SECTION FADMINISTRATION &
RESOURCES

17Circular Instruction 180 regarding the Compensation
of Work-related Upper Limb Disorders (WRULDs),
Compensation for Occupational Injuries and Diseases
Act, 1993 (Act no 130 of 1993), as amended.
Published in the Government Gazette (23 April 2004)
No. 26270; General notices: Notice 498 of 2004
Circular Instruction 180

Page | 72 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
CIRCULAR INSTRUCTION NO. 180
Circular Instruction 180 regarding the compensationof work-related upper limb disorders (WRULDs)Compensation for Occupational Injuries and Diseases Act, 1993
(Act no 130 of 1993), as amended
The following circular instruction is issued to clarify the compensation of claims for work-related upper limb
disorders (WRULDs) and supersedes all previous instructions in this regard. The Compensation Commissioner‘s
“Guidelines for medical practitioners and employers on how to manage Work-Related Upper Limb Disorders
(WRULDs)” can also be used for further reference. These guidelines are available on the Department of Labour web-
site – www.labour.gov.za – through the CC web page under Occupational Diseases.
1. Definition
WRULDs is a collective term for a group of occupational diseases that consist of musculo-skeletal disorders caused
by exposure in the workplace affecting the muscles, tendons, nerves, blood vessels, joints and bursae of the hand,
wrist, arm and shoulder. These are syndromes associated with characteristic symptoms and physical signs (e.g. rota-
tor cuff syndrome, epicondylitis at the elbow, tenosynovitis and nerve entrapments such as carpal tunnel syndrome).
Previously other terms had been used, such as repetitive strain injury (RSI), cumulative trauma disorder (CTD),
occupational overuse syndrome (OOS), occupational cervico-brachial disorder (OCD), etc. For the purpose of this
instruction the umbrella term, work-related upper limb disorders (WRULDs), will be used.
WRULDs are caused, aggravated or precipitated by one or more of the following risk factors, singly or in combination:
Highly repetitive movements
Movements requiring force
Movements at the extremes of reach
Static muscle loading
Awkward sustained postures
Contact stress (e.g. uncomfortable gripping and twisting, sharp edges to hand tools, desk edges, etc.)
Vibration
In terms of this instruction, upper limb musculo-skeletal disorders will be presumed to be work-related if the nature
of the work performed includes exposure to the relevant risk factors.
2. Diagnosis
The following criteria should be used to confirm the diagnosis:
A diagnosis of WRULD by the medical practitioner.
Medical history and clinical signs indicating - site and distribution, quality (type, character), severity (intensi-
ty, frequency, duration) and progression of the symptoms according to the type of disorder
Functional ability report by an occupational therapist and / or physiotherapist, where necessary
Occupational exposure to known risk factors and a chronological relationship between the WRULD and the work
environment.
The confirmatory tests/investigations (e.g. x-rays, strength testing, range of motion testing, nerve conduction
tests), where appropriate.
The medical officers in the Compensation Office will determine whether the diagnosis of WRULD was made accord-
ing to acceptable medical standards.

Page | 73 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
3. Impairment
Impairment will be determined, in accordance with the internal instructions 157 for residual impairment of the
function of the muscles, tendons, joints or nerves involved, after maximum medical improvement has been reached.
4. Benefits
Benefits will be payable according to the Compensation for Occupational Injuries and Diseases Act, 1993 (Act
number 130 of 1993), as amended.
• Temporary total disablement
Payment for reasonable temporary total or partial disablement will be made on the basis of medical reports for
as long as such disablement continues, for a period not exceeding 24 months.
• Permanent disablement
Permanent disablement will be assessed when a Final Medical Report is received, after a reasonable recovery
period not exceeding 24 months, and failure to perform work effectively after the appropriate course of
treatment and rehabilitation.
• Medical aid
Medical expenses shall be provided for a period of not more than 24 months from the date of the diagnosis. This
period may be extended if, in the opinion of the Director General, further medical aid will reduce the extent of
the disablement. The medical aid covers the costs of diagnosing a WRULD and any necessary treatment
provided by any healthcare provider. The Compensation Commissioner will decide on the need for, the nature
and the sufficiency of the medical aid supplied.
5. Reporting
The following documentation should be submitted to the Compensation Commissioner, or the employer individual-
ly liable, or the mutual association concerned:
W.Cl.1 Employer’s Report of an Occupational Disease
W.Cl.14 Notice of an Occupational Disease and Claim for Compensation
W.Cl.301 First Medical Report in respect of a Work-Related Upper Limb Disorder (WRULD)
All other reports that may be relevant to the diagnosis and treatment of the condition (e.g. an ergonomic
assessment supported by photographs, video clips, etc.)
W.Cl.302 Progress / Final Medical Report in respect of a Work-Related Upper Limb Disorder (WRULD)
Progress medical reports must be submitted monthly to the Compensation Commissioner.
W.Cl. 110 Exposure History or an appropriate employment history
W.Cl.6 Resumption Report (monthly as long as the case is open, even if the employee is at work)
6. Claim Processing
The Office of the Compensation Commissioner will consider and adjudicate upon the liability of all claims. The
medical officers in the Compensation Commissioner’s office are responsible for the medical assessment of a claim
and for the confirmation of the acceptance or rejection of a claim.
DIRECTOR GENERAL: LABOUR
Date: 9 March 2004
Published in the Government Gazette (23 April 2004) No. 26270, General notices: Notice 498 of 2004

18First medical report in respect of a work-related upper
limb disorder (WRULD), published in the Government
Gazette (21 May 2004) No. 26384
W.CL 301: First MedicalReport

1. Date symptoms first started: 2. Date of first consultation: 3. Date of specific diagnosis:
4. Specific diagnosis of this upper limb disorder:
5. The symptoms the employee experiences (tick the appropriate box/es):
Burning sensation Fatiguability Loss of grip strength
Loss of normal sensation Muscle weakness Pain
Paraesthesia (tingling) Sensation of cold Swelling
Stiffness and cramps
Describe:
6. The clinical signs found on examination (tick the appropriate box/es):
Crepitus (crackling sound in subcutaneous tissue) Muscle spasm
Muscle weakness Reduction of range movement
Swelling Tender trigger points in muscles
Tenderness
Describe:
7. Is the employee left or right handed?* Sex:* Age:
8. Height of employee: Weight of employee: Body mass index:
9. Which special medical investigation/s and/or job analysis / ergonomic assessments were done to prove the diagnosis and/or what other poten-tial causes of the above-mentioned upper limb disorder have been investigated / eliminated? (Where applicable, please attach these reports.
10. Does the employee suffer from any other diseases? (If so, please specify)
11. Describe the nature of any previous injuries sustained and/or abnormalities to the employee’s upper limb/s?
Employee: Surname: Identity number:
First names:
Address: Code:
Employer:
Address: Code:
FIRST MEDICAL REPORT IN RESPECT OF A WORK-RELATED UPPER LIMB DISORDER (WRULD)
Compensation for Occupational Injuries and Diseases Act, 1993 (Act number 130 of 1993)[Section 6A(b) – Commissioner’s rules, forms and particulars – Annexure 25]
This form must be completed by a medical practitioner and sent to the Compensation Commissioner, PO Box 955, Pretoria, 0001
Right Left Male Female years
cm kg
Claim number:
W.CI. 301
Please turn over and complete reverse side.*Encircle correct answer

I certify that I have by examination of the employee, satisfied myself of the above-mentioned facts.
Signature Registered address with HPCSA:
(Medical Practitioner):
Name (printed):
Qualifications: Code:
Practice number: Date (Important):
12. Appraise the job or summarise the job analysis / ergonomic assessment of the job which has allegedly caused the disorder, in terms ofthese risk factors (Where applicable, attach photos, diagrams and/or job analysis / ergonomic assessment):
13. How long has the employee been doing this job? years months
14. Explain how this alleged occupational disease progressed over a period of time in terms of function (i.e. signs and symptoms with relationto job tasks) [E.g. wrist pain started after 8 hours of sewing 6 months ago (no clinical signs). Currently increased pain after 30 minutes of sewing with pain keeping her out of
sleep. Positive Phalen and Tinel tests and reduction in grip strength.]
15. Have any of the employee’s colleagues, performing a similar job, complained of similar symptoms? If yes, explain.
16. Explain how this condition was managed before this specific diagnosis was made in terms of:
a) The Person Medically (e.g. medication, surgery, etc.):
Functionally (e.g. rehabilitation, etc.):
b) The Job Task adaptation (e.g. job rotation, shorter hours, etc.):
Equipment adaptation (e.g. extended handle on tool used, etc.):
17. Is the employee currently fit to work?* If yes, is he/she performing his/her* or ?
If the employee is performing alternate/adapted work, is this position* or ?
Yes No
Yes No Alternate/Adapted workUsual work
Temporary Permanent
Risk factor Percentage of Briefly describe the job task where this risk factor occurs and quantify in terms of repetitions / working day duration / strength required / range of movement, etc.
Repetitive movements
Movements requiring force
Movements at the extremes of reach
Static muscle loading
Awkward sustained postures
Contact stress
Vibration
Low temperatures
IMPORTANT: • All questions must be answered in full (use extra paper if necessary).
• Full motivation of diagnosis will prevent unnecessary correspondence and delays in adjudication of claim.
• The form must be forwarded to the employer within 14 days after the specific diagnosis was made. The employer must forward this report to the Compensation Commissioner.
• Please submit medical accounts separately. Attach a copy of this report to your account.
• It is advisable to consult the Compensation Commissioner’s “Guidelines for Managing Work-Related Upper Limb Disorders” before reporting this condition.
• The employer must submit a copy of this report to the Provincial Executive Manager of the Department of Labour (Occupational Health and Safety Act) or the Regional Principal Inspector of Mines (Mine Health and Safety Act)
• The employer must submit a Progress Medical Report (W.Cl. 302) and a Resumption Report (W.Cl. 6) on a monthly basis to the Compensation Commissioner or Mutual Association or employer individually liable, as the case may be, until the employee’s condition has become stabilised, when a Final Medical Report (W.Cl. 302) should be submitted.
*Encircle correct answer
W.CI. 301

19Progress/Final medical report in respect of a work-
related upper limb disorder (WRULD), published in
the Government Gazette (21 May 2004) No. 26384
W.CL 302: Progress/Final medical report

B. COMPLETE THE FOLLOWING SECTION ONLY IF THE EMPLOYEE IS CURRENTLY NOT WORKING DUE TO THIS CONDITION
3. Is the employee still in the employment of the above-mentioned employee? If yes, answer the following questions:
a. Since when is the employee not working because of this occupational disease? (Date)
b. When do you expect the employee to return to work? (Date)
c. Will the employee be returning to his/her usual job?**
i. If yes, are there any task adaptations?* If yes, please explain (e.g. job rotation, shorter hours)
ii. If yes, are there any equipment adaptations? ** If yes, please explain (e.g. extended handle on tool used)
d. Is the employee returning to an alternate position?** If yes, is this position or ?**
e. What arrangements have been made with the employer regarding the employee’s re-introduction to work (e.g. work hardening, shorter hours, etc.)?
Employee: Surname: Identity number:
First names:
Address:
Employer:
Address:
Specific diagnosis: Date of specific diagnosis:
Code:
Code:
A. CURRENT CLINICAL CONDITION OF EMPLOYEE (Complete this section)
1. Since the previous Medical Report, is there an improvement in the severity of the symptoms the employee is experiencing and clinical signs found on examination?** Explain.
2. Describe how the employee’s condition has been managed since the previous report (mention dates of procedures, tests, etc.) in terms ofthe following:
a. Medically (e.g. medication, surgery, etc.)
b. Functionally (e.g. rehabilitation, etc.)
PROGRESS / FINAL* MEDICAL REPORT IN RESPECT OF A WORK-RELATED UPPER LIMB DISORDER (WRULD)
Compensation for Occupational Injuries and Diseases Act, 1993 (Act number 130 of 1993)[Section 6A(b) – Commissioner’s rules, forms and particulars – Annexure 26]
This form must be completed by a medical practitioner and sent to the Compensation Commissioner, PO Box 955, Pretoria, 0001
YES NO
YES NO
YES NO
Claim number:
YES NO
YES NO
YES NO
TEMPORARY PERMANENT
*Delete which is not applicable **Encircle the correct answerW.CI. 302 Please turn over and complete reverse side.

I certify that I have by examination of the employee satisfied myself of the above-mentioned facts.
Signature Registered address with HPCSA:
(Medical Practitioner):
Name (printed):
Qualifications: Code:
Practice number: Date (Important):
D. PROGNOSIS (Complete this section)
11. Has the employee’s condition been optimally managed since the previous Medical Report in terms of medical treatment and actions taken in response to the functional capacity and job analysis / ergonomics assessments? If no, please explain.
12. a. Has the employee’s condition become stabilised (i.e. reasonable medical intervention will not improve the employee’s condition)?
b. If yes, has there been any permanent anatomical defect and/or impairment of functions as a result of this occupational disease? If yes, describe this in detail and substantiate by special reports where necessary.
7. Did the employee receive a planned re-introduction when returning to work?**
8. Are you aware of any adaptation to the workplace that are planned / implemented by the employer to prevent other employees from developing WRULDs?**
9. Are you aware of an occupational health programme that is in place to assess the health risks causing WRULDs and to do adequate medical surveillance and health education?**
10. Are you aware of a company policy to address WRULDs?**
C. COMPLETE THE FOLLOWING SECTION ONLY IF THE EMPLOYEE IS CURRENTLY AT WORK:
4. Was the employee off work for more than 2 days due to this condition?**
If yes, the period the employee was not at work, was from (inclusive) to (Dates)
5. Has the employee returned to his/her usual job?**
a. If yes, are there any task adaptations?* If yes, please explain (e.g. job rotation, shorter hours)
b. If yes, are there any equipment adaptations? ** If yes, please explain (e.g. extended handle on tool used)
6. Has the employee returned to an alternate position?** If yes, is this position** or ?
If yes, then analyse the job that the employee has returned to in terms of the risk factors below:
Risk factor Percentage of Briefly describe the job task where this risk factor occurs and quantify in terms of working day repetitions / duration / strength required / range of movement, etc.
Repetitive movements
Movements requiring force
Movements at the extremes of reach
Static muscle loading
Awkward sustained postures
Contact stress
Vibration
Low temperatures
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
TEMPORARY PERMANENT
YES NO
YES NO
YES NO
IMPORTANT: • All questions must be answered in full (use extra paper if necessary).
• The form must be forwarded to the employer who will send it to the Compensation Commissioner.
• Please submit medical accounts separately. Attach a copy of this report to your account.
• It is advisable to consult the Compensation Commissioner’s “Guidelines for Managing Work-Related Upper Limb Disorders” before completing this report.
• The employer must submit a copy of this report to the Provincial Executive Manager of the Department of Labour (Occupational Health and Safety Act) or the Regional Principal Inspector of Mines (Mine Health and Safety Act).
• A Progress Medical Report (W.Cl. 302) and a Resumption Report (W.Cl. 6) must be submitted by the employer on a monthly basis to the Compensation Commissioner or Mutual Association or employerindividually liable, as the case may be, until the employee’s condition has become stabilised, when a Final Medical Report (W.Cl. 302) should be submitted.
**Encircle correct answerW.CI. 302

20The contact details of the Compensation
Commissioner and the Provincial Executive Managers
of the Department of Labour
Reporting – the contactdetails

Page | 81 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
REPORTING – The contact details1
The employer must submit the necessary forms to the Compensation Commissioner.
The employer must also notify the Provincial Executive Manager of the Department of Labour (Occupational
Health and Safety Act) of a case of WRULD.
The employer must submit a Progress Medical Report (W.Cl. 302) and a Resumption Report (W.Cl. 6) on a
monthly basis to the Compensation Commissioner or Mutual Association or employer individually liable, as the
case may be, until the employee’s condition has become stabilised, when a Final Medical Report (W.Cl. 302)
should be submitted.
REGION POSTAL ADDRESS PHONE FAX
E A S T E R N C A P E P R I VAT E B A G X 9 0 0 5 0 4 3 7 0 1 3 1 2 8 0 4 3 7 2 2 1 0 1 2E A S T L O N D O N5 2 0 0
F R E E S TAT E P. O . B O X 5 2 2 0 5 1 5 0 5 6 2 0 3 0 5 1 4 4 8 5 3 2 9B L O E M F O N T E I N9 3 0 0
G A U T E N G N O R T H P R I VAT E B A G 3 9 3 0 1 2 3 0 9 5 0 6 5 0 1 2 3 2 0 2 3 6 7P R E T O R I A0 0 0 1
G A U T E N G S O U T H P O B O X 4 5 6 0 0 1 1 4 9 7 3 0 4 7 0 1 1 4 9 7 3 2 2 5J O H A N N E S B U R G2 0 0 0
K W A Z U L U - N ATA L P O B O X 9 4 0 0 3 1 3 6 6 2 0 2 2 0 3 1 3 0 5 9 5 4 0D U R B A N4 0 0 0
L I M P O P O P R I VAT E B A G X 9 3 6 8 0 1 5 2 9 0 1 6 0 7 0 1 5 2 9 0 1 6 0 8P O L O K WA N E0 7 0 0
M P U M A L A N G A P R I VAT E B A G X 7 2 6 3 0 1 3 6 5 5 8 7 0 1 0 1 3 6 5 5 8 8 3 8W I T B A N K1 0 3 5
N O R T H E R N C A P E P R I VAT E B A G X 5 0 1 2 0 5 3 8 3 8 1 5 0 2 0 5 3 8 3 2 9 3 8 6K I M B E R L E Y8 3 0 1
N O R T H W E S T P R I VAT E B A G X 2 0 4 0 0 1 8 3 8 7 8 1 0 0 0 1 8 3 8 4 2 5 9 7M M A B AT H O ( E X T. 1 0 1 )2 7 4 5
W E S T E R N C A P E P R I VAT E B A G X 8 7 2 0 2 1 4 2 1 0 8 0 2 0 2 1 4 2 5 2 3 9 2C A P E T O W N8 0 0 0
COMPENSATION COMMISSIONER
P O B O X 9 5 5 T E L : 0 1 2 3 2 1 0 2 4 5
P R E T O R I A FA X : 0 1 2 3 2 4 4 4 5 1
0 0 0 1 E - M A I L : I N F O @ W C O M P. G O V. Z A
W E B : W W W. L A B O U R . G O V. Z A
DEPARTMENT OF LABOUR: CHIEF INSPECTOR
OCCUPATIONAL HEALTH AND SAFETY
PROVINCIAL EXECUTIVE MANAGERS OF THE DEPARTMENT OF LABOUR
P R I VAT E B A G X 1 1 7 T E L : 0 1 2 3 0 9 4 3 7 7
P R E T O R I A FA X : 0 1 2 3 2 0 0 9 2 3
0 0 0 1 W E B : W W W. L A B O U R . G O V. Z A
1 As on 1 April 2004

21In many cases employer, line managers or supervisors
will be quite capable of assessing WRULD risks and
taking appropriate action. However, an employer
should get further advice if:
There is uncertainty whether a significant risk exists;
Simple and cheap corrective measures are not
available;
The right action to handle a risk is not obvious; or
If numerous employees are developing WRULDs.
Where help is needed, and no one else in the organi-
sation has the answer, an employer should seek expert
advice. The following organisations (in alphabetical
order) may be able to point an employer in the right
direction:
Getting further advice

Page | 83 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
Getting futher adviceIn many cases employers, line managers or supervisors will be quite capable of assessing WRULD risks and taking
appropriate action. However, an employer should get further advice if:
There is uncertainty whether a significant risk exists
Simple and cheap corrective measures are not available
The right action to handle a risk is not obvious or
If numerous employees are developing WRULDs.
Where help is needed, and no one else in the organisation has the answer, an employer should seek expert advice.
The following organisations (in alphabetical order) may be able to point an employer in the right direction:
AFROX OCCUPATIONAL HEALTHCARE
At ten t ion : Dr S te fanus Snyman
PO BOX 474 TEL: 082 557 1056
GOODWOOD FAX: 086 670 1842
CAPE TOWN E-MAIL: [email protected]
7459 WEB: WWW.OCCHEALTH.GIVENGAIN.NET
CSIR MINING TECHNOLOGYAt ten t ion : Mr Schu Schut te
Dr Bel inda Dias
P O BOX 91230 TEL: 011 358 0202 / 011 358 0291
AUCKLAND PARK FAX: 011 482 3267
2006 E-MAIL: [email protected]
WEB: WWW.CSIR.CO.ZA/MININGTEK
ERGOMAX (PTY) LTD(ERGONOMIC CONSULTANTS)
At ten t ion : Dale Kennedy
UNIT B6 TEL: 021 702 2001 OR 011 791 1616
WESTLAKE SQUARE FAX: 021 701 1117
WESTLAKE MOBILE: 082 462 54 86 OR 072 321 9227
7945 E-MAIL: [email protected] OR
WEB: WWW.ERGOMAX.CO.ZA
ERGONOMIC SOCIETY OF SOUTH AFRICA (ESSA)
can advise on f inding a consultant ergonomist (a special ist in ensuring a good ‘ f i t ’ between
employees and their ‘ job’ requirements) .
At ten t ion : Jon James
C/O DEPARTMENT OF HUMAN KINETICS AND ERGONOMICS
RHODES UNIVERSITY TEL: 046 6038468
GRAHAMSTOWN E-MAIL: J . [email protected]
6140 WEB: WWW.ERGONOMICS-SA.ORG.ZA
OCCUPATIONAL THERAPYASSOCIATION OF
SOUTH AFRICA (OTASA)At ten t ion : Mrs B . Badenhors t
PO BOX 11695 TEL: 012 342 6731
HATFIELD FAX: 012 342 5400
0028 E-MAIL: [email protected]
WEB: WWW.OTASA.ORG.ZA
SOUTH AFRICAN SOCIETY OFOCCUPATIONAL HEALTH
NURSES (SASOHN)At ten t ion : L inda Stokes
P.O.BOX 18793 TEL: 011-8923174
SUNWARD PARK E-MAIL: : [email protected]
1470 WEB: WWW.SASOHN.ORG.ZA

Page | 84 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
SOUTH AFRICAN SOCIETY OFOCCUPATIONAL MEDICINE
(SASOM)At ten t ion : Dr F iona Robinson
(Tel : 011 315 1926)Pro f Mary Ross
(Tel : 011 358 9183)
PO BOX 16179 TEL: 012 667 5160/1
LYTTLETON FAX: 012 667 5160
0140 E-MAIL: [email protected]
WEB: WWW.SASOM.ORG.ZA
SOUTH AFRICAN SOCIETY OFPHYSIOTHERAPY
At ten t ion : Sai ra Khan
P O BOX 92125 TEL: 011 4851467
NORWOOD FAX: : 011 4851613
2117 E-MAIL: [email protected]
WEB: WWW.PHYSIOSA.ORG.ZA
WORKABIL ITY – PREVENTION,ASSESSMENT & WORK
REHABIL ITATION SERVICESAt ten t ion : L indsay Scot t
L ize S labber t
PO BOX 51784 TEL 021 551 9108
WEST BEACH FAX: 021 5519108
7449 E-MAIL: [email protected]

22This checklist is reproduced with the permission of
the Health & Safety Executive. HSE (1998)
Checklist: WRULDs inthe workplace

Page | 1 | of Checklist© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
INITIAL ASSESSMENT YES NO
CHECKLIST: WRULDs IN THE WORKPLACE1
Company / Department:
Workstation: Completed by:
Task:
Worker: Date:
RISK FACTOR TICK YOURANSWER ACTION REQUIRED
If you have no ticks in the “YES” column onthis page, you are unlikely to have anyWRULDs. You need not go on to the followingpages.
However, if you have any ticks in the “YES”column on this page, there may be a risk ofWRULDs in your workplace. You should go onand complete the full risk assessment on thefollowing pages.
** ‘Awkward’ includes ‘staying in one position for a long
time’ and ‘holding things for a long time’
ARE THERE ANY WARNING SIGNS OF UPPER LIMB DISORDERS? For example:
Gripping (a tool or work piece)?
Squeezing (e.g. tool handles)?
Twisting?
Reaching?
Moving things (pushing, pulling, lifting)?
Finger/hand movements (e.g. keyboard work)?
Actual cases of possible WRULDs in this or similar work?
Complaints by employees, e.g. aches and pains in hands, wrists, arms, shoulder, etc.? Ask youremployees if they have any of these symptoms.
Home-made, improvised changes to workstations or tools? (e.g. handles cushioned or madelonger)
DOES THE JOB INVOLVE MUCH
FREQUENTorFORCEFULorAWKWARD**
1 This checklist is reproduced with the permission of the Health & Safety Executive. HSE (1998)

Page | 2 | of Checklist© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
FULL RISK ASSESSMENT
RISK FACTOR YES NO POSSIBLE SOLUTIONS
Are there any factors in the job that make WRULDs likely, such as NEED FOR MUCH FORCE?
Does the job involve: RECOMMENDATIONS FOR ACTION
1. Strong force at the same time as Redesign workstation or tool, e.g. awkward movements or posture • Reposition supply of components to reduce (e.g. static loading, bent wrists, reaching requiredwork with arms raised or fully • Move controls to more convenient positionextended)?
2. Forceful use of hand/forearm • Redesign job, workstation, and/or tools to avoid muscles? over-use of the hand or forearm
• Maintain tools for ease of use.(e.g. keep them sharp and lubricated
• Assess improved job rotation / sharing
3. Trying to make do with ill-fitting • Improve quality of components, or provide suitablecomponents by forcing them into tools for fitting themplace?
4. Tools not ideal for repetitive or • Replace domestic or DIY hand tools with tools designed frequent use – particularly if for repetitive industrial use squeezing, twisting or hammering • Redesign tool handles to achieve even distribution of actions are required? force across the hand (adequate size of the handle and
power grip preferable to pinch grip) and straight rather than bent wrists. Consider replacing hand tools with power tools. Reduce squeezing forces by using weaker springs in triggers, etc.
5. Using equipment designed for a • Redesign equipment or tool (e.g. counter-balancing to larger or stronger person (e.g. reduce force required)women using tools designed • Provide powered version for men)?

Page | 3 | of Checklist© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
RISK FACTOR YES NO POSSIBLE SOLUTIONS
Are there any factors in the job that make WRULDs likely, such as RAPID, AWKWARD OR FREQUENT MOVEMENTS?
Does the job involve: RECOMMENDATIONS FOR ACTION
1. Machine pacing • Self-pacing is preferable(e.g. to keep up with conveyor)?
2. Frequent repetitions of the • Re-plan work, e.g. break up pause/repetition cyclessame small number of or spread movement across both hands. Consider movements? adding extra activities to job, to give variety. Consider
scope for automation or use of power tools.
3. Awkward movements such as • Redesign workstation, controls or shape of tool handlestwisting or rotation of wrist, movements of wrist from side to side,very bent fingers and wrist, or hand or arm movements beyond a comfortable range?
4. Pressure on employees to work • Consider need for such systems (but employees mayfast, e.g. perform piecework or resist change). Better training in WRULD risks may bonus system? help.

Page | 4 | of Checklist© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
RISK FACTOR YES NO POSSIBLE SOLUTIONS
Are there any factors in the job that make WRULDs likely, such as AWKWARD OR STATIC POSTURE?
Does the job involve: RECOMMENDATIONS FOR ACTION
1. Cramped body position, and/or • Improve space available to worker. Provide adjustablenot enough space to change workstation (especially chair) for employees who are posture? above or below average height or shape.
2. Arms stretching out or at shoulder • Move materials or controls to more convenient position.height or above for long periods?
3. Work at awkwardly high or low • Move materials or controls to more convenient position.height (crouching, stooping, or reaching up)?
4. Poor posture for any other reason? • Has worker been trained in good working techniques and posture?
• Is there a need for better seating (adjustable to correctheight for individual) footrests, etc.?
• Sitting versus standing position?

Page | 5 | of Checklist© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
RISK FACTOR YES NO POSSIBLE SOLUTIONS
Are there any factors in the job that make WRULDs likely, such as AWKWARD OR STATIC POSTURE?
Does the job involve: RECOMMENDATIONS FOR ACTION
1. No changes to work routine or • If possible, vary tasks to provide changes in activity.variation of tasks? If not, check that there is adequate rest breaks
2. No breaks or infrequent breaks? • Check that breaks are taken, especially if work involvescontinuous effort such as holding tools, or rapidlyrepeated movements (e.g. typing)
• Pause exercises, e.g. quick stretches / movements atworkstation for 60 seconds every 30 minutes
3. Worker not able to have short • Redesign work to make short breaks possiblepauses when desired?
Are there any factors in the job that make WRULDs likely, such as NO SPECIAL ARRANGEMENT FOR NEW EMPLOYEES?
1. People having to work at full pace • Allow recruits to build up their work rate sensibly as immediately on starting (or they gain experienceresuming) the job?
2. No training in risks of WRULDs • Provide training in skills, posture and warningand ways employees can reduce symptoms for all those at riskrisks?
Does the job involve: RECOMMENDATIONS FOR ACTION

Page | 6 | of Checklist© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
RISK FACTOR YES NO POSSIBLE SOLUTIONS
Are there any factors in the job that make WRULDs likely, such as POOR ENVIRONMENTAL CONDITIONS
1. In dim light, shadow or flickering • Provide better lighting so that employees do not havelight? to adopt awkward postures to see properly
2. In cold or otherwise adverse • Cold (e.g. handling frozen foods) may increase the riskconditions? of WRULDs. If it is not possible to warm the working
environment, check that protective clothing is welldesigned and does not affect posture or grip
3. With tools that vibrate? • Consider whether job can be done another way to avoidneed for high-vibration tools. Or provide vibration-absorbing grip and minimise vibration by proper maintenance.
Is the job performed: RECOMMENDATIONS FOR ACTION

23This bibliography contains more references than
referred to in the text. Various individuals and profes-
sional interest groups commented on the draft docu-
ments in developing these guidelines and most of
them mentioned additional sources and references.
We considered it valuable to include everything in this
bibliography.
Bibliography

Page | 93 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
Bibliography
Alfredson H, Pietila T, Jonsson P, Heavy-load eccen-
tric calf muscle training for the treatment of chronic
Achilles tendinosis. Am J Sports Med 1998;
26(3):360-366.
Almekinders LC, Temple JD. Etiology, diagnosis, and
treatment of tendonitis: an analysis of the literature.
Med Sci Sports Exerc 1998; 30(8):1183-1190.
Andersson BJG, Ortengren R, Nachemson A, Elfstrom
G. Lumbar disc pressure and myoelectric back muscle
activity during sitting. Studies on an experimental
chair. Scandinavian Journal of Rehabilitation
Medicine 1974; 6:104-114.
Andersson BJG, Ortengren R, Nachemson A, Elfstrom
G. Lumbar disc pressure and myoelectric back muscle
activity during sitting. Studies on an office chair.
Scandinavian Journal of Rehabilitation Medicine
1974; 6:115-121.
Bauer W, Wittig T. Influence of screen and copyholder
positions on head posture, muscle activity and user
judgment. Applied Ergonomics 1998; 29(3):185-
192.
Bendix T. Seated trunk posture at various seat inclina-
tions, seat heights and table heights. Human Factors
1984; 26(6):695-703.
Bergqvist U, Wolgast E, Nilsson B, Voss M. Musculo-
skeletal disorders among visual display employees;
individual, ergonomic and work organizational factors.
Ergonomics 1995; 38(4):763-776.
Black KM, McClure P, Polansky M. The influence of
different sitting positions on cervical and lumbar pos-
ture. Spine 1996; 21(1):65-70.
Branton P. Backshapes of seated persons – how close
can the interface be designed? Applied Ergonomics
1984; 15(2):105-107.
Bridger RS, Wilkinson D, van Houweninge T. Hip joint
mobility and spinal angles in standing and in different
sitting postures. Human factors 1989; 31(2):229-
241.
Bridger RS. Introduction to Ergonomics. Singapore:
McGraw-Hill, 1995.
Bridger RS. Postural adaptations to a sloping chair
and work surface. Human Factors 1988; 30(2):237-
247.
British Standards 5940. Office furniture part 1 –
design and dimensions of office workstations, desks,
tables and chairs. 1980.
Brukner P, Kahn K. Clinical Sports Medicine. Sydney:
McGraw-Hill Book Company, 1993.
Brukner P, Khan K. Clinical Sports Medicine. Sydney:
McGraw-Hill, 1993.
Butler D. Mobilisation of the nervous systems.
Melbourne: Churchill Livingstone, 1991.
Carson R. Ergonomically designed chairs adjust to
individual demands. Occupational Health and Safety
1993; June:71-75.
Carter JB, Banister EW. Musculo-skeletal problems in VDT
work: A review. Ergonomics 1994; 37(10):1623-1648.
Channas M, et.al. Dupuytren's Disease, Carpal Tunnel
Syndrome, Trigger Finger, and Diabetes Mellitus, J
Hand Surg [Am] 1995; 20:109-114.
Clement DB, Taunton JE, Smart GW. Achilles tendinitis
and peritendinitis: etiology and treatment. Am J
Sports Med 1984;12(3):179-184.
Corlett EN, Bishop RP. A technique for assessing pos-
tural discomfort. Ergonomics 1976; 19(2):75-182.
Curwin SL, Stanish WD. Tendinitis: Its Etiology and
Treatment. Toronto: Collamore Press, 1984
Cyriax J. Textbook of Orthopaedic Medicine (Volume
1): Diagnosis of soft tissue lesions. London: Bailliere
Tindall, 1988.
De Wall M, Van Riel M, Aghina J, Burdof A, Snijders
C. Improving the sitting posture of CAD/CAM employ-
ees by increasing VDU monitor working height.
Ergonomics 1992; 35(4):427-436.
Dickenson CE, Campion K, Foster AF, Newman SJ,
O’Rourke AMT, Thomas PG. Questionnaire develop-
ment: an examination of the Nordic Musculo-
skeletal Questionnaire. Applied Ergonomics 1992;
23(3):197–201.
Guild R, Ehrlich RI, Johnston JR, Ross MH. Handbook
of Occupational Health Practice in the South African
Mining Industry. Johannesburg: SIMRAC, 2001.
Elvey RL. Physical evaluation of the peripheral nervous
system in disorders of pain and dysfunction. Journal
of Hand Therapy 1997; April-June:122-129.

European Agency for Safety and Health at Work. Work-
Related Upper Limb Musculo-skeletal Disorders.
Buckle P, Devereux, J. (eds.). Luxembourg: Office for
Official Publications of the European Communities,
1999.
Evans G. Tenosynovitis in Industry: Menace or
Misnomer. British Medical Journal 1987; 294:1569-
1570.
Farbach P, Chapman L. VDT work duration and mus-
culo-skeletal discomfort. American Association of
Occupational Health Nurses 1990; 38(1):32-36.
Faucett J, Rempel D. VDU related musculo-skeletal
symptoms: Interaction between work posture and psy-
chosocial work factors. American Journal of Industrial
Medicine 1994; 26:597-612.
Goetschel G. A review of the development of an
ergonomically balanced chair. Journal of Manipulative
and Physiological Therapeutics 1987; 10(3):65-69.
Golding A. Workstation design and postural stress:
Part 2 Case study. South African Journal of
Physiotherapy 1990; 46(2):13-17.
Grant R, Forrester C, Hides J. Screen based keyboard
operation: The adverse effects on the neural system.
Australian Physiotherapy 1995; 41(2):99-107.
Greening J, Lynn B. Vibration sense in the upper limb
in patients with repetitive strain injury and a group of
at-risk office employees. International Archives of
Occupational and Environmental Health 1998;
71:29-34.
Greenspan JD. Nociceptors and the peripheral nervous
systems role in pain. Journal of Hand Therapy 1997;
(April-June):78-85.
Gur S, Ron S, Heicklen-Klein A. Objective evaluation
of visual fatigue in VDU employees. Journal of
Occupational Medicine [British] 1994; 44:201-204.
Hagberg M, Silverstein BA, Wells RV, Smith MJ,
Hendrick HW, Carayon P, Pérusse M. Work related
musculo-skeletal disorders: a reference for preven-
tion. Kuorinka I & Forcier L (eds). London: Taylor and
Francis, 1995.
Health and Safety Executive. Review Of Diagnostic
Criteria For Work Related Upper Limb Disorders
(WRULD). Silman AJ, Newman J (eds.). London: HSE
Books, 1996.
Health and Safety Executive. Upper limb disorders:
Assessing the risk. Sadbury: Health and Safety
Executive, 1998.
Hedge A, Powers JR. Wrist postures while keyboard-
ing: Effects of a negative slope keyboard system and
full motion forearm supports. Ergonomics 1995;
38(3):508-517.
Hedman TP, Fernie GR. Mechanical response of the
lumbar spine to seated postural loads. Spine 1997;
22(7):734-743.
Hendrikse J. Vibration and human task performance.
Address at the SASOHN Congress: Midrand, 15-17
November 1995.
Higgs PE, Mackinnon SE. Repetitive Motion Injuries.
Annu. Rev. Med. 1995; 46:1-16.
Hölmich P, Uhrskou P, Ulnits L, Effectiveness
of active physical training as treatment for long-
standing adductor-related groin pain in athletes:
randomised trial. Lancet 1999; 353(9151):439-
443.
House of Commons. Work-Related Upper Limb
Disorders. Research Paper 1998/51. Sleator A, Gore
D, Vidler G (eds.). London: House of Commons
Library, 1998.
Jacobs K. Ergonomics for Therapists (2nd edition).
Boston: Butterworth-Heinemann, 1999.
Karh O, Kansi P, Kuorinka I. Correcting working pos-
tures in industry: a practical method for analysis.
Applied Ergonomics 1997; 33(8):1055-1063.
Karlqvist LK, Hagberg M, Koster M, Wenemark M,
Anell R. Musculo-skeletal symptoms among com-
puter-assisted design (CAD) operators and evaluation
of a self-assessment questionnaire. Interna-tional
Journal of Occupational and Environmental Health
1996; 2(3):185-194.
Kennedy, D. Valuable contributions and editing of the
final document and assessment forms. Ergomax (Pty)
Ltd. Cape Town, South Africa, 2004
Kennedy, D. WRULD’s Risk Calculator. Ergomax (Pty)
Ltd. Cape Town South Africa, 2004.
Khan K. A New Paradigm for a Difficult ClinicalProblem. The Physician and Sportmedicine 2000, 28(5).
Khan K. The effect of mechanical loading on the mus-culo-skeletal system: clinical and laboratory studies.Melbourne: University of Melbourne, 1998.
Kietrys D. McClure P, Kelley Fitzgerald G. The rela-tionship between head and neck posture and VDTscreen height in keyboard operators. Physical Therapy1998; 78(4):395-403.
Page | 94 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0

Kilbom Å. Repetitive work of the upper extremity: PartI – Guidelines for the practitioner. InternationalJournal of Industrial Ergonomics 1994. 14: 51-57.
Kilbom Å. Repetitive work of the upper extremity: PartII – The Scientifica Basis (knowledge base) for theguide. International Journal of Industrial Ergonomics1994. 14: 59-86.
Kroemer K, Kroemer H, Kroemer-Elbert K. Ergonomics– How to design for ease and efficiency (2nd edition).New Jersey: Prentice-Hall, 2000.
Kroemer K, Kroemer H, Kroemer-Elbert K.Ergonomics: How to design for ease and efficiency.New Jersey: Prentice-Hall Incorporated, 1994.
London Hazard Centre. RSI Hazard Handbook.London: Interchange Studios, 1997.
Lowe W. Orthopedic Massage: A Model for alternativetreatment of cumulative trauma disorders. AAOHNJournal 1999; 47:175-181.
Luttgens K, Hamilton N. Kinesiology: Scientific Basisof Human Motion, 9th Ed., Madison (WI): Brown &Benchmark, 1997
MacKinnon SE, Novak CB. Clinical commentary:Pathogenesis of cumulative trauma disorder. TheJournal of Hand Surgery [American] 1994; 19A(5):873 – 883.
MacKinnon SE, Novak CB. Repetitive strain in theworkplace. The Journal of Hand Surgery [American]1997; 22(A):2-18.
Malchaire, JB, Cock NA. Risk prevention and controlstrategy for upper limb musculo-skeletal disorders.TUBT Newsletter June 1999; 11(12): 27-31.
Marcus M, Gerr F. Upper extremity musculo-skeletalsymptoms among female office employees: As-socia-tions with video display terminal use and occupation-al psychosocial stressors. America Journal ofIndustrial Medicine 1996. 29:161-170.
Martin C, Andrew-Tuthill DM. Office Ergonomics:Measurements for success. AAOHN Journal 1999;47:479-492.
Marxhausen P. Computer related repetitive straininjuries. Lincoln: University of Nebraska, 1996.
McAtamney L, Corlett EN. RULA: A survey method forthe investigation of work-related upper limb disorders.Applied Ergonomics 1993; 24(2):91-99.
Mennen U. Neurovascular assessment of the hand.CME 1999; 14:1007-1018.
Nachemson AL. Disc pressure measurements. Spine1981; 6(1):1231-1244.
Naqvi SAA. Study of forward sloping seats for VDU work-stations. Journal of Human Egology 1994; 23:41-49.
Niesen-Vertommen SL, Taunton JE, Clement DB, Theeffect of eccentric versus concentric exercise in themanagement of Achilles tendonitis. Clin J Sport Med1992; 2(2):109-113.
NIOSH. Health Hazard Evaluation Report of PerdueFarms (Lewiston & Robertsonville, North Carolina).Kiken S, Cincinnati: NIOSH Publication number HETA89-307-2009, 1989.
NIOSH. Musculoskeltal Disorders (MSDs) and workplacefactors – A critical review of epidemiologic evidence forwork-related musculo-skeletal disorders of the neck,upper limb, and low back. Bernard PB (ed). Cincinnati:DHHS (NIOSH) Publication No. 97B141, 1997.
Occhipinti E, Colombini D. Assessment of exposure torepetitive upper limb movement: an IEA con-sensus document. TUBT Newsletter June 1999; 11(12): 22-26.
Palmer K, Walker-Bone K, Linaker C, Reading I,Kellingray S, Coggon D, Cooper C. The Southamptonexamination schedule for the diagnosis of musculo-skeletal disorders of the upper limb. Ann Rheum Dis2000; 59:5–11.
Pascarelli E, Kella J. Soft-tissue injuries related touse of the computer keyboard. Journal ofOccupational Medicine [American] 1993;(A)35(5):522-532.
Perugia L, Postacchini F, Ippolito E. The Tendons:Biology, Pathology, Clinical Aspects. Milan: EditriceKurtis, 1986.
Pheasant S. Ergonomics, Work and Health. Basing-
stoke: MacMillan Academic and Professional Ltd.,
1991.
Quintner JL, Elvey RL. Understanding RSI: A Review
of the role of peripheral neural pain and hyperalgesia.
The Journal of Manual and Manipulative Therapy
1993; 1(3):99-105.
Robinson AJ. Central nervous system pathways for
pain transmission and pain control: Issues rele-vant to
the practicing clinician. Journal of Hand Therapy
1997; (April-June):64-77.
Rossignol A, Morse E, Summers V, Pagnotto L. Video
display terminal use and reported health symptoms
among Massuchusetts clerical employees. Journal of Oc-
cupational Medicine [American] 1987; (A)29:112-118.
SAMOSA (South African Musculo-skeletal Disorder
Surveillance Action Group). Musculo-skeletal
Disorders. Johannesburg: SAMOSA (NCOH), 2002.
Page | 95 | of 96 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0

Page | 96 | of 9 pages© 2004 | Compensation Commissioner’s Guidelines for Health Practitioners and Employers to manage WRULDs | Version 1.0
Schuldt K, Ekholm J, Harms-Ringdahl K, Nemeth G,
Arborellus UP. Effects of change in sitting work pos-
ture on static neck and shoulder muscle activity.
Ergonomics 1986; 29(12):1525-1537.
Scott J, Huskisson EC. Graphic presentation of pain.
Pain 1976; 2:175-184.
Scott, P, Christie C. Work-related upper limb disor-
ders: Functional Anatomy. Department of Human
Kinetics and Ergonomics, Rhodes University, Grahams
Town, South Africa, 2002
Scott, P, Christie, C, James, J, Todd, A. Valuable con-
tributions and editing of the final document and
assessment forms. Department of Human Kinetics and
Ergonomics, Rhodes University, Grahams Town, South
Africa, 2002
Shacklock M. Neurodynamics. Physiotherapy 1995;
81(1):9-16.
Shrier I, Matheson GO, Kohl HW III. Achilles ten-
donitis: are corticosteroid injections useful or harm-
ful? Clin J Sport Med 1996; 6(4):245-250.
Sluiter JK, Rest KM. Criteria document for evaluating
the work-relatedness of upper-extremity musculo-
skeletal disorders. Scandinavian Journal of Work,
Environment and Health 2001; 27 (Supple-
ment)(1):1-102.
Snyman ISDeW. Repetitive Strain Injuries – An
Overview. Cape Town: Afrox Occupational Healthcare,
2001.
Soderberg GL, Blanko MK, Cosentino TL, Kurdelmeier
KA. An EMG analysis of posterior trunk musculature
during flat and anteriorly inclined sitting. Human fac-
tors 1986; 28(4):483-491.
Souhami RL, Moxham J. Textbook of Medicine.
Edinburgh: Churchill Livingstone, 1990
Stewart KA. Effective workplace inspections.
Canadian centre for Occupational Health and Safety.
1989; (No. P87-1E).
Stewart KA. Ergonomics and basic guide. Canadian
centre for Occupational Health and Safety. 1989.
Taptagaporn S, Sotoyama M, Saito S, Suzuki T, Saito
S. Visual comfort in VDT Workstation design. Journal
of Human Ergology 1995; June:84-88.
Tortora GJ. Principles of Human Anatomy. Ninth
Edition. New York: John Wiley and Sons, Inc., 2002.
Tozzi GA. Musculo-skeletal disorders in Europe:
Unions show a lead. TUBT Newsletter June 1999; No
11(12): 12-21.
U.S. Department of Energy. ErgoEASER – Ergonomics
Education, Awareness, System Evaluation And
Recording Tool. Washington: Pacific Northwest
National Laboratory, 1999.
Uhthoff HK, Sarkar K. Shoulder pain and reflex sym-
pathetic dystrophy. Curr Opinion Rheum 1991;
3:240-246.
Van der Merwe J, Cochrane J. Ergonomics in occupa-
tional health. Occupational Health [South Africa]
2000; Vol.6:25-27.
Vecchio, P. Shoulder pain in a community-based
rheumatology clinic. British Journal of Rheu-matology
1995; 34:440-442.
Wheeless CR. Wheeless' Textbook of Orthopaedics.
Internet: Medmedia, 1996.
Williams N. WRULDs: encouraging an Ergonomics
approach. Occupational Health 1993; 401-404.
Wilson A. Effective Management of Musculo-skeletal
Injury – A clinical Ergonomics approach to pre-ven-
tion, treatment and rehabilitation. Churchill
Livingston, 2002.