vision is the art of seeing what is basic invisible to
TRANSCRIPT

BASIC ABDOMINAL ULTRASOUND
• “VISION IS THE ART OF SEEING WHAT IS
INVISIBLE TO OTHERS.”- JONATHON SWIFT
• AMY BOSSUNG DVM, IVUSS CERT
• MOBILE SONOGRAPHER

MY EXPERIENCE - HOW I STARTED
• Small Animal Practitioner for 21 years
• Ultrasound was in it’s beginnings
• Fortunate to have an employer/mentor
• Started with a used machine
• Went to my first seminar – 3 people
• Started scanning
• Radiologist reviews of exams -VHS

BLAST FROM THE PAST
• Eventually we upgraded machine
• Continued to take advantage of education
packages with each upgrade
• Read everything I could
• Put the probe on anything I could.

MY EXPERIENCE – HOW I STARTED
• Started scanning in 1995.
• In 2006 expanded to mobile ultrasound work by starting
Animage, Inc to meet a growing need in the area.
• Completed IVUSS Certification program in 2010.
• IVUSS – International Veterinary Ultrasound Society -
Website IVUSS.org
• Today I work part time in general practice and part time
performing mobile ultrasound exams for local veterinarians.

REFERENCES/RESOURCES
• Nyland and Matton
• Penninck and d’Anjou
• Sonopath.com
• VIN
• ACVR Ultrasound Society
• Journal - Veterinary Radiology and
Ultrasound
• Conference Notes

A GROWING FIELD
“Today, ultrasonography is an
integral part of the
diagnostic approach in
academic institutions as well
as in private practice.”- Atlas
of Small Animal
Ultrasonography,Penninck/d'
Anjou

BASIC PRINCIPLES OF SOUND
Diagnostic ultrasound is the use of high frequency sound waves to produce an image from within the
body.
Diagnostic sound waves are above the range of
human hearing.
Audible sound - < 0.2 mHz
Ultrasound waves - 2-10 mHz (10-100 x more)
Human hearing has a limited range of 20 Hz to
20 kilohertz (kHz). Ultrasound is
considered those frequencies greater than 20 kHz, while diagnostic
ultrasound utilizes frequencies greater than 1
megahertz (MHz).

BASIC PRINCIPLES OF SOUND
• Sound energy is a form of
mechanical energy that travels
in a longitudinal wave in cycles
of compressions and
rarefactions.
• Sound transmission requires
medium such as air, liquid or
tissue.
• Each wave has a wavelength,
speed of travel and frequency.

BASIC PRINCIPLES OF SOUND
• A cycle is the time required for one
complete compression and rarefaction
• Frequency is the # of cycles per second
• Frequency measured in Hertz where 1
Hz = 1 cycle/sec
• Wavelength is distance in millimeters
that the sound wave travels in one
cycle

BASIC PRINCIPLES OF ULTRASOUND
• Speed of sound depends on the density and stiffness of the
medium through which it travels.

BASIC PRINCIPLES OF SOUND
• Speed of travel of sound in
soft tissue is fairly constant
value at 1540 m/s which
means wavelength and
frequency are inversely
related.
• As such the higher the
frequency of the sound
waves produced the
shorter the wavelength.
• Higher frequencies =
shorter wavelengths
• Lower frequency = longer
wavelengths

BASIC PRINCIPLES OF SOUND
Velocity of sound is independent of frequency and does not change through a homogenous structure.
Sound travels at the same speed (1540 m/s) through soft tissue whether you use a 2.0 mHz or 10 mHz probe
Velocity is calibrated into the machine which calculates the distance to the imaged structure based on how long it takes to receive reflected echos.

BASIC PRINCIPLES OF SOUND
• Acoustic Impedance – opposition or resistance to the flow of sound
through a medium

BASIC PRINCIPLES OF SOUND
• The difference in acoustic impedance
between tissues is important.
• The greater the difference between
acoustic impedance between adjacent
tissues the greater the reflection of sound
waves at the interface.
• If there is no acoustical impedance
difference between adjacent tissues (i.e.
they have the same acoustical impedance)
their boundary will not produce an echo
and the tissue will appear the same. (Ex
liver lobes)

BASIC PRINCIPLES OF SOUND
• Though it sounds contradictory the higher the density and
greater the velocity of sound through a medium the greater
the resistance to sound transmission
• Example bone: Speed of sound through bone is 4080 m/s
but it has a high density (inability to compress and rarefact)
and therefore has a high acoustical impedance and a high
degree of sound reflection thus creating a shadow.

BASIC PRINCIPLES OF SOUND

BASIC PRINCIPLES OF SOUND
• In contrast air has a low speed of sound (330 m/sec) and a
low impedance. However there is 99% reflection of sound
at soft tissue-air interfaces
• Why? Reflection of sound depends on an acoustical
mismatch. The greater the difference in acoustical
properties the greater the reflection.
• This is why you need coupling gel between the transducer
and skin and why you cannot image aerated lungs.

BASIC PRINCIPLES OF SOUND-TISSUE INTERACTION/IMAGE PRODUCTION
• Basis of ultrasound imaging is sound waves are generated
and travel through tissue.
• The interaction of the sound with the tissues determines
what we see on the screen.
• The sound waves as they travel through tissue undergo
either reflection, refraction or absorption.
• The reflected waves that return to the probe are
responsible for the image.

REFLECTION
• Responsible for the image
• Depends on the acoustical
mismatch (ie bone-soft tissue and
air-soft tissue interface)
• Depends on angle of incidence
(sound striking perpendicular will
have more sound reflected back
to the transducer)
• Depends on the reflecting
structures size (higher frequency
transducers can reflect sound
from smaller structures)
Structures that are small and
irregular with respect to the
sound wave cause scatter of
the sound

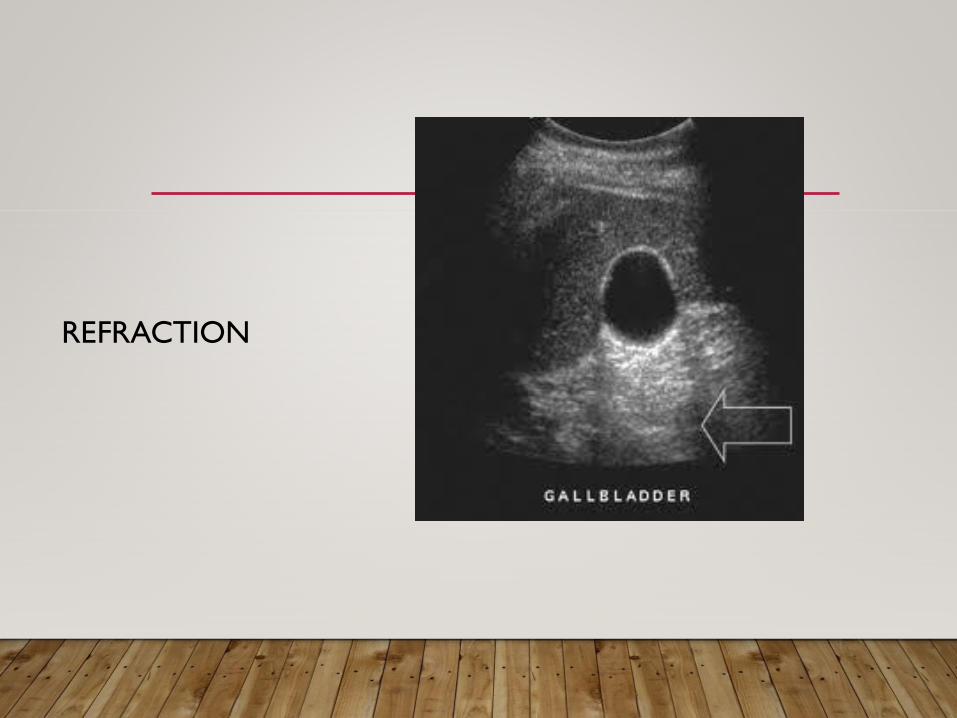
REFRACTION
• Change in direction of
sound as it travels from
one medium to another
where the speed of travel
is different.
• Usually occurs where
there is a fluid filled or
rounded structure such as
the gall bladder or kidney.
REFRACTION

ABSORPTION
ABSORPTION
• Sound waves that are absorbed by
the tissue and converted to heat by
frictional forces in the tissue.
ATTENUATION
• Decrease in the intensity or
loss of energy of the
ultrasound beam due to
absorption, reflection,
refraction and scatter
• High frequency sounds
attenuate to a higher degree
thus have less energy for
deeper structures to reflect

GENERATING THE IMAGE
• Machine
-Holds the computer and amplifier
• Transducer
-pizoelectric crystals in special housing,
connects to the machine with cable
• Monitor screen
-displays the image

GENERATING THE IMAGE
• Transducer (Probe)
• Pizoelectric crystals within
transducer converts electrical
energy into sound energy
• Multi frequency – 5-8 or 3-8 mHz
most common
• Voltage applied intermittently so
crystals produce sound 1% of time
and 99% is spent receiving echos

TRANSDUCER TYPES
• Linear array
• -rectangular image
• -usually higher frequency 7.5-12
mHz
• -used for superficial structures
that need higher resolution
• -feline abdomen, thyroid glands

TRANSDUCER TYPES
• Sector probes
-curvilinear
-pie shape image
-multifrequency
-most commonly used;
work horse
• Phased array probe
-used in cardiac imaging

SECTOR PROBES

REMEMBER
TRANSDUCER FREQUENCY RELATION
HIGHER FREQUENCY=INCREASED RESOLUTION
AND DECREASED DEPTH
LOWER FREQUENCY=DECREASED RESOLUTION
AND INCREASED DEPTH

HIGH RES LOW DEPTH

LOW RES MORE DEPTH

RESOLUTION
• Spatial Resolution
–ability to distinguish two points as separate in space.
- sub categorized to axial and lateral
• Axial resolution – ability to differentiate two points along
the length of the beam
-improves image quality and detail
-higher frequency probes have better axial resolution

RESOLUTION
• Lateral Resolution
-ability to differentiate
two points lying side by
side perpendicular to the
sound beam
-higher frequencies have
higher lateral resolution
-best at the focal zone
ULTRASOUND MODES
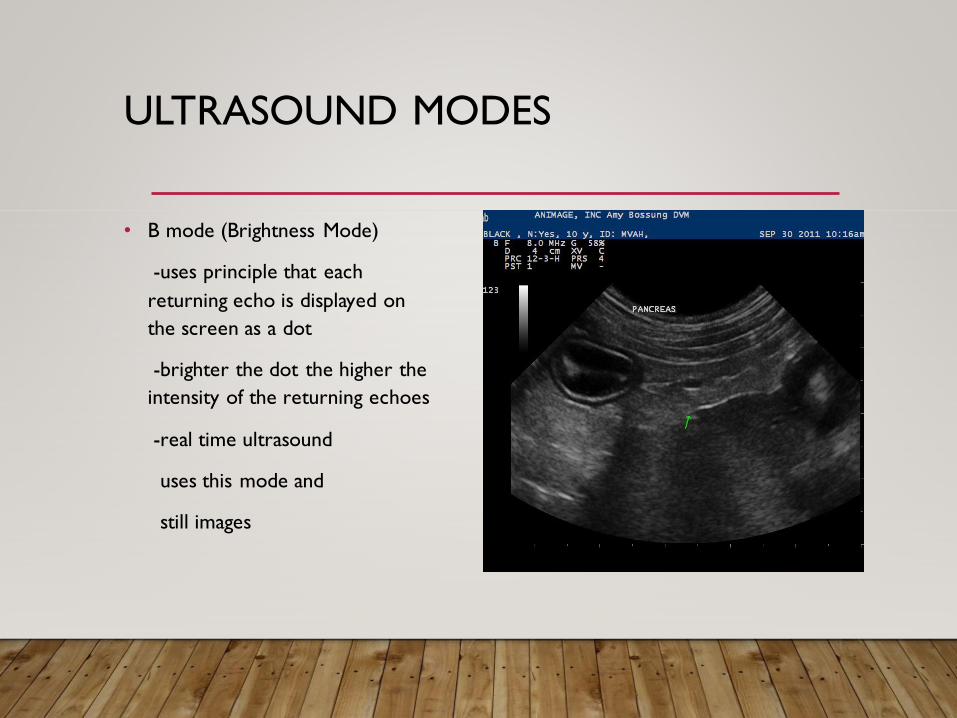
• B mode (Brightness Mode)
-uses principle that each
returning echo is displayed on
the screen as a dot
-brighter the dot the higher the
intensity of the returning echoes
-real time ultrasound
uses this mode and
still images

ULTRASOUND MODES
• M mode (Motion mode)
-single ultrasound beam in a fixed position and records
how the dimensions of the section being interrogated
change with time
-used with cardiac
imaging

VOCABULARY
• Normal relative echogenicity of organs
Spleen Most hyperechoic
Liver
Renal Cortex
Renal Medulla Least hypoechoic

VOCABULARY -ARTIFACTS
• Acoustic Shadow – most
common with bone,
calcification and gas
-structures reflect and/or
absorb about 100% of
ultrasound beam
-dark area distal to structure
(anechoic-black)
- see most commonly with rib
shadows; skin air interface

ACOUSTIC SHADOW
BLADDER CALCULI

VOCABULARY - ARTIFACTS
• Acoustic Enhancement (through transmission)
-hyperechoic (bright area) distal to a structure that has
lower attenuation than the surrounding structure
-most common with cysts and gall bladder or fluid filled
viscus
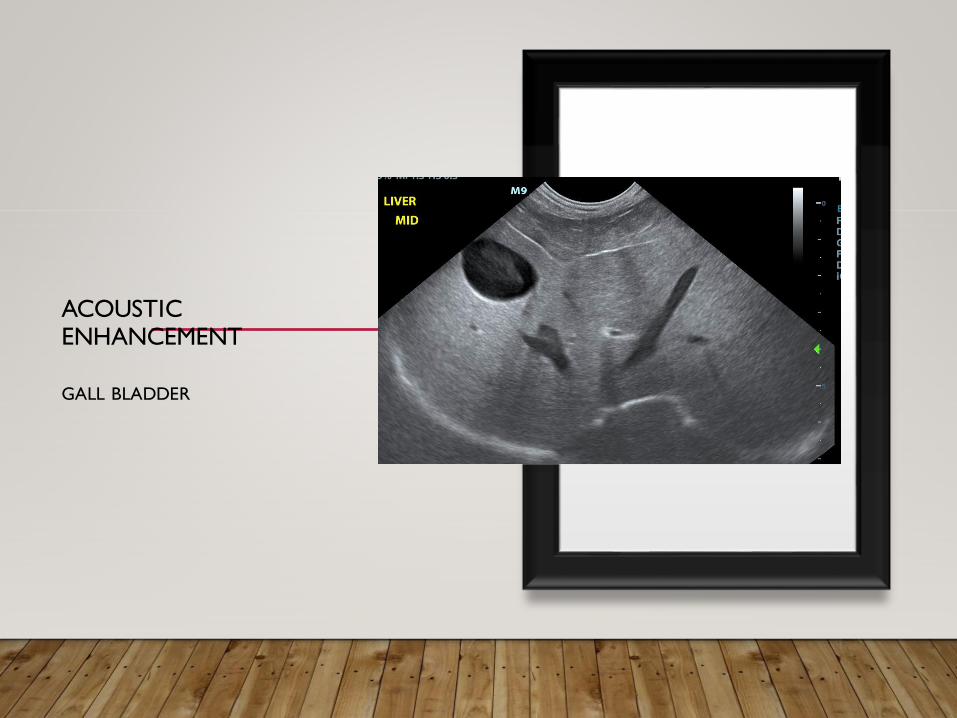
ACOUSTIC ENHANCEMENT
GALL BLADDER

VOCABULARY - ARTIFACTS
• Reverberation
-reflection of ultrasound beam back and forth between two reflective
surfaces
-most common with lung wall interfaces, GI gas, metallic foreign bodies
-comet tail or ring down is special form of reverberation. Seen with gas
bubbles intestines or in lungs

REVERBERATION

VOCABULARY - ARTIFACTS
• Mirror image artifact
-illusion of a duplicate image on the other side of a reflective
surface
-caused by altered echoes
- that are “late” returning to the transducer
-transducer interprets these as coming from a deeper area
because the echoes take longer to return
-most common with liver at diaphragm (looks like liver is in
the thorax)

MIRROR IMAGE ARTIFACT

MIRROR IMAGE ARTIFACT EXAMPLE

VOCABULARY ARTIFACTS
• Side lobe artifact
-causes anatomy outside the main beam to show up as if
in the main beam
-a highly reflective surface outside the main beam can
result in echoes returning to the transducer
-slice thickness or grating is another type of this artifact
-common with gall bladder or urinary bladder, mimics
sediment or colon looks like it is in the bladder

SIDE LOBE AND SLICE THICKNESS

VOCABULARY ARTIFACTS
• Refraction
-bending of sound beam
along margin of rounded
organ or structure
-common with kidney
edge of kidney or gall
bladder

REFRACTION

DOPPLER
• color flow Doppler ultrasound - a form of pulse wave
Doppler in which the energy of the returning echoes is
displayed as an assigned color.
Red=towards probe; Blue=away from probe
• continuous wave Doppler ultrasound - a technique in
which the transducer emits and receives the ultrasound
beam continuously, enabling the measurement of high
velocity blood flow, such as occurs through heart valve
stenoses. Measures continuously.

DOPPLER
• spectral Doppler ultrasound - a form of ultrasound
image display in which the spectrum of flow velocities is
represented graphically on the Y-axis and time on the X-
axis; both pulse wave and continuous wave doppler are
displayed in this way
• pulse wave Doppler ultrasound - a technique in which
the transducer emits ultrasound in pulses. Measures
velocity at a certain point in time.
• continuous wave Doppler ultrasound - a technique
in which the transducer emits and receives the ultrasound
beam continuously, enabling the measurement of high
velocity blood flow, such as occurs through heart valve
stenoses. Measures continuously.

QUESTIONS????CLEAR AS MUD???

ULTRASOUND EXAM
• Patient Prep
-Fasting 10-12 hours, do not withhold water.
-dorsal or lateral recumbency. I start dorsal and then shift
to lateral as I need to for certain views.
-V trough is helpful, patient comfort
-quiet dark room without interruptions
-sedation as needed; don’t be afraid to sedate; motion,
panting, tense abdominal wall all can decrease image quality.

ULTRASOUND EXAM
• Patient Prep
-Clip hair, decrease air trapping (air
decreases exam quality)
-coupling gel, improves contact and
sound transmission; should use for
high quality exam
-no enemas or barium (decreases
quality of exam)

ULTRASOUND EXAM
• Always have a standard starting point.
-some start at bladder some at liver.
• Always follow same routine so you don’t forget any organs.
-resist the temptation to go right to the lesion
• Usually work in a clockwise fashion around abdomen
• Keep a list of organs and image views by machine

HEPATOBILIARY • Liver
-place probe subxiphoid
-liver size is subjective; no standard
measures for liver.
-radiographs superior to ultrasound
for mild changes in liver size but
extreme hepatomegaly or
microhepatica can subjectively be
assessed.
-falciform fat ventral to liver. Usually
iso or hyperechoic to liver but can
mimic liver parenchyma.

LIVER SCAN
PROBE PLACEMENT

LIVER VIEWS
• Right liver
• Right caudal liver with right kidney
• Mid liver – midline (CBD, PV, CVC, AO maybe visible) plus cineloop
• Left liver
• Transverse mid liver (with gall bladder)
• Transverse right and left liver (optional)
• Liver spleen comparison (either in same image if possible or on split
screen)

HEPATOBILIARY
• Liver parenchyma
-normal echogenicity - equal to (isoechoic) or slightly more
echogenic (hyperechoic) than the renal cortex of right kidney and
less than (hypoechoic) to the spleen. Always compare with these
views.
-Cats compare echogenicity of liver to falciform fat and not spleen.
-homogenous, coarser than spleen
• Liver capsule
-smooth, hyperechoic, caudoventral borders are sharp.

NORMAL LIVER

HEPATOBILIARY
• Liver
-anechoic/hypoechoic tubular structures are portal and
hepatic veins and caudal vena cava
-intrahepatic portal vein branches have hyperechoic walls
(fatty and fibrous tissue) that distinguish them from hepatic
veins
-Note: hepatic veins can appear to have a hyperechoic wall if
sound beam is perpendicular to the wall. Portal veins will be
hyperechoic throughout.

NORMAL LIVER

HEPATOBILIARY
• Gallbladder
-lies to right of midline
-generally only portion of normal biliary tract seen
on ultrasound in dogs. Cats can see CBD with higher
frequencies. GB to cystic duct to CBD to duodenal
papilla to duodenum
-variably shaped, larger with fasting, usually ovoid tear
dropped shaped. Cats can be bilobed.
-wall is thin, smooth uniform
-usually anechoic due to fluid bile with distal acoustic
enhancement
-biliary sludge can be echogenic and have variable
consistency (fluid, inspissated, mucocele)

GALLBLADDER

GALL BLADDER SLUDGE

GALL BLADDER PATHOLOGYMUCOCELE

GALL BLADDER PATHOLOGY
CHOLECYSTITIS CALCULUS

FOCAL HEPATIC LESIONS
• classify by size, shape, number, margination, relative
echogenicity and texture.

FOCAL HEPATIC LESIONS
• Cysts, abscesses, primary or metastatic neoplasia, hematomas,
granulomas, infarts, extramedullary hematopoiesis, nodular
hyperplasia.
• Cysts will be anechoic with distal acoustic enhancement.
• Other lesions can all appear similar on ultrasound. Needle
biopsy can help to distinguish. Correlate with history, exam,
blood work etc
• Target lesion: hyperechoic nodule with surrounding hypoechoic
rim. High correlation with metastatic lesion.

FOCAL HEPATIC LESIONSREGENERATIVE NODULES

FOCAL HEPATIC LESIONS
MULTIFOCAL
NODULES CYST

FOCAL HEPATIC LESIONSHEPATOCELLULAR CARCINOMA

DIFFUSE HEPATIC DISEASE
• Diffuse parenchymal abnormalities can be a little more
difficult to detect.
• Compare echogenicity to right kidney and spleen: Is it
hyperechoic, hypoechoic, isoechoic?
• Echotexture : Is it homogenous or heterechoic?
• Subjective size assessment.

DIFFUSE HEPATIC DISEASE
HYPERECHOIC LIVER HYPOECHOIC LIVER
Significantly darker than the
spleen.
Portal vessels would stand
out.
Leptospirosis and
cholangiohepatitis or
hepatitis

DIFFUSE LIVER DISEASE
HETERECHOIC/MIXED
ECHOGENICITY

DIFFUSE LIVER DISEASE
HEPATOCUTANEOUS
SYNDROME TARGET LESION
DIFFUSE HEPATIC DISEASE
DIFFUSE
HYPERECHOIC• Steroid hepatopathy
• Lipidosis
• Other vacuolar hepatopathies
• Chronic hepatitis
• Fibrosis
• Cirrhosis
• Lymphoma
• Mast Cell Tumor
DIFFUSE HYPOECHOIC• Passive Congestion
• Acute hepatitis or cholangiohepatitis
• Lymphoma
• Leukemia
• Histiocytic neoplasms
• Amyloidosis

DIFFUSE HEPATIC DISEASE
MIXED ECHOGENICITY
• Steroid hepatopathy +/- benign
nodular regeneration or other
processes
• Hepatitis
• Lymphoma
• Hepatocellular carcinoma
• Metastasis
• Necrosis
• Amyloidosis

SPLEEN
• Left cranial abdomen, usually tongue shaped and triangular on
transverse views
• Position can be variable but head is usually dorsal and have to scan
under ribs in this area to visualize
• Echogenicity – homogenous normally with a finer texture than the
liver
• Thin hyperechoic capsule, should be smooth
• Hyperechoic to liver and renal cortex
• Splenic veins can be seen exiting at the hilus (clue to distinguishing
from liver)

SPLEEN
• Images to acquire
Longitudinal Splenic head
Transverse Splenic head
Longitudinal Mid-Body Spleen
Transverse Mid-Body Spleen

SPLEEN
• Cat spleens are small
homogenous and smooth
but don’t compare to
liver.
• Splenomegaly with normal
echogenicity is often
caused by sedation.

SPLENOMEGALY
• Subjective assessment
• Dogs may be more rounded and organs may extend further caudal
and to the right.
• Cats look fat like a sausage; may fold on itself
• Can be due to sedation (normal echogenicity) but also can be seen
with extramedullary hematopoiesis, infectious disease, splenic torsion
or malignant infiltration (lymphoma or mast cell disease.
• Mast cell disease can be a common cause of splenic enlargement in
the cat.

SPLEEN
• May have diffuse or focal disease
• Note shape of spleen and appearance of capsule
• Describe lesions similar to focal liver lesions
-size, shape, number, relative echogenicity, margination,
texture if lesion breaks capsule continuity.

SPLEEN LESIONS
DIFFUSE DISEASE
• Hypoechoic
-Lymphoma
-Mast cell disease
-multiple myeloma
-splenic torsion (diffuse lacy
appearance)
-congestion
DIFFUSE DISEASE
• Heterechoic (mixed echogenic)
-Hemangiosarcoma
-Hemangioma
-Hematoma
-Nodular hyperplasia
-Extramedullary hematopoiesis

SPLEEN LESIONS
FOCAL LESIONS• Hypoechoic
-Metastatic neoplasia
-Primary neoplasia
-Nodular hyperplasia
-Extramedullary hematopoiesis
-Abscess
-Infarction
-Cyst
FOCAL LESIONS• Heterechoic (mixed echogenic)
-Hemangiosarcoma
-Hemangioma
-Hematoma
• Complex lesions
-anechoic, hypoechoic and
hyperechoic
-often what hemangiosarcomas
look like

SPLEEN LESIONS
Hyperechoic Focal Lesions
• Nodular hyperplasia
• Extramedullary hematopoiesis
• Dystrophic mineralization
• Fibrosis of chronic inflammation
• Myelolipomas – perivascular fat/fibrous capsular invaginations. Can get
very large.
Important to note benign and malignant disease can account for
similar lesions on ultrasound.

SPLEEN FOCAL LESIONS
HYPERPLASIA BENIGN LESION

FOCAL SPLENIC LESION AND MASSHIGH GRADE SARCOMA

FOCAL SPLENIC LESIONS MASS HEMATOMA

FOCAL SPLENIC LESIONMYELOLIPOMA
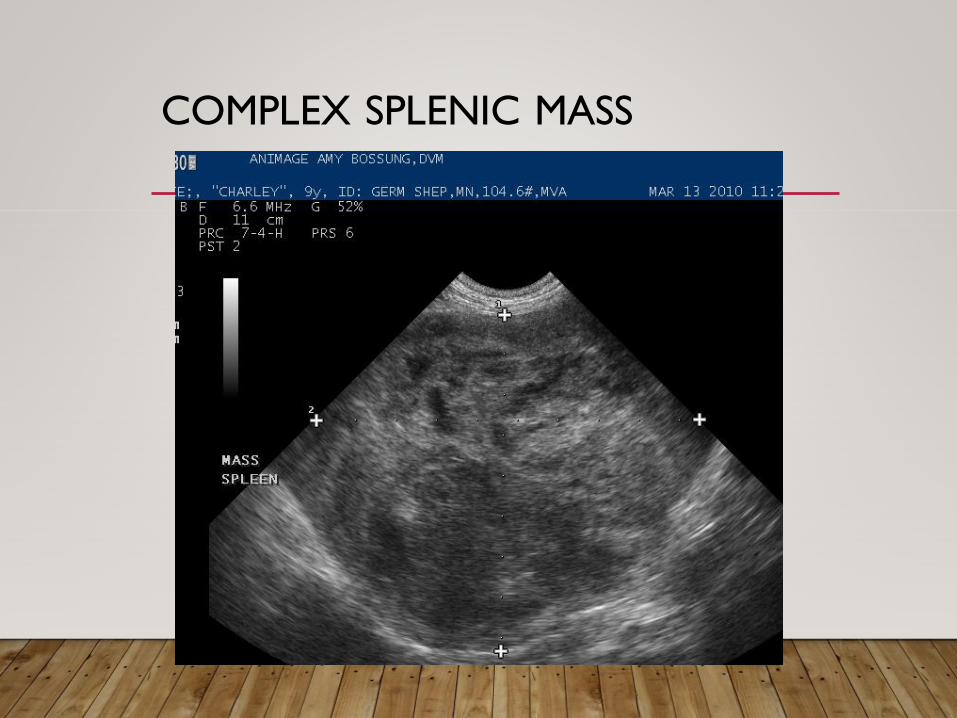
COMPLEX SPLENIC MASS

FELINE SPLEEN

KIDNEY IMAGING
• Image both longitudinally
and transversely
• Transverse image to see
renal pelvis and look for
renal pelvic dilation.
• Feline: 2 –5 mm (length)
• Canine: 3 – 8 mm (Length)
weight dependent

KIDNEY IMAGES
Longitudinal Midline
Longitudinal cineloop
Transverse mid kidney for renal pelvis

KIDNEY IMAGING
• Left kidney
•Lies caudal to the last rib directly behind the spleen
•Retroperitoneal location
•Usually easy to find
• Right kidney
•Lies partially under the rib cage
•Can be obscured by bowel gas
•Located dorsally below the epaxial muscles
•Tip: will be caudal to the right caudate liver lobe

KIDNEY IMAGING
• Indications:
•Abnormal size
•Altered shape and contour
•Azotemia (except pre-renal from dehydration)
•Hematuria
•Abnormal urinalysis
•Unable to palpate or visualize kidneys in a patient with suspected renal
disease.

KIDNEY IMAGING
• Renal cortex more echogenic
than the medulla
• Renal cortex (left) hypoechoic
to the spleen
• Renal cortex (right) hypo or
isoechoic to the liver
• Renal cortex
-coarsely stippled
-arcuate arteries are bright
echoic spots in cortex
• Renal Pelvis
- not seen usually
-peripelvic fat is hyperechoic
and can shadow

NORMAL KIDNEY
NORMAL KIDNEY

NORMAL FELINE KIDNEY

KIDNEY IMAGING
• Diffuse renal parenchymal disease may result in changes in
renal size, shape, and/or echogenicity, or may show no
changes at all.
• Most commonly seen ultrasound change of diffuse renal
disease is increased cortical echogenicity, with enhanced
cortico-medullary definition
• Loss of corticomedullary definition can also be seen
especially in severe cases.

DIFFUSE RENAL DISEASE

RENAL LYMPHOMA

KIDNEY IMAGING
• Chronic renal disease may result in a decrease in size, irregular
capsule, increased cortical thickness, loss of corticomedullary
definition
• Differentials for diffuse chronic renal disease -
nephrocalcinosis, glomerulonephritis, chronic pyelonephritis,
congenital renal dysplasia, end stage kidney disease, and
chronic interstitial nephritis.
• Enlarged, hyperechoic kidneys may indicate FIP, amyloidosis,
acute tubular necrosis (as seen with ethylene glycol toxicity),
and lymphosarcoma

CHRONIC KIDNEY DISEASE
CORTICAL
THICKENING RENAL INFARCT

KIDNEY IMAGING
• Medullary rim sign - a hyperechoic line at the cortico-
medullary junction is visible. This is now considered a non-
specific finding, and can be seen in patients without renal
disease.

KIDNEY IMAGING
• Focal renal disease may be due to cysts, abscesses, hematomas,
primary and metastatic neoplasia, and infarcts.
• Reduced cortical echogenicity or multifocal hypoechoic nodules or
masses have been described with lymphoma as well diffuse
hyperechogenicity.
• Other renal neoplasia such as carcinoma usually result in focal mass
lesions of mixed echogenicity.
• Entire renal structure can be infiltrated by neoplasia making it difficult
to recognize as a kidney
• Can’t differentiate tumor type on ultrasound exam alone, consider
other differentials such as abscess, hematoma, and necrosis as well.

KIDNEY PATHOLOGYRENAL MASS FOCAL

KIDNEY PATHOLOGYPOLYCYSTIC KIDNEY

KIDNEY IMAGING
• Hydronephrosis
•Gradual dilation of ureters, pelvis and medulla due to
obstruction.
•Progressive dilation and replacement of kidney with an
anechoic fluid-filled structure
•Cortex becomes compressed and thin
• Perinephric pseudocysts
•Normal appearing kidney with anechoic cyst surrounding the
cortex

KIDNEY IMAGING
HYDRONEPHROSIS/HY
DROURETER CANINE
HYDRONEPHROSIS
FELINE

KIDNEY IMAGING
Ureter Calculus

KIDNEY IMAGING
Perinephric pseudocyst

KIDNEY IMAGING
• Pyelonephritis
•Dilation to renal pelvis and ureter (more echogenic fluid)
•Hyperechoic renal cortex and medulla
• Renolithiasis
•Almost always in the renal pelvis
•Look for acoustic shadowing of stone
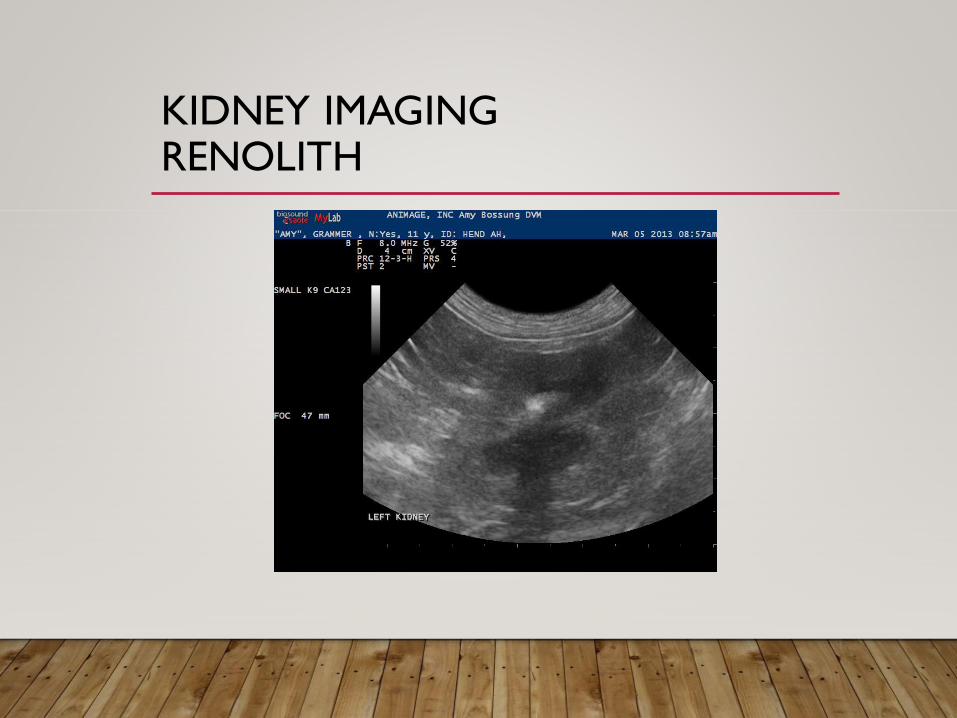
KIDNEY IMAGINGRENOLITH

KIDNEY IMAGING
• Neoplasia can usually be diagnosed with a fine needle
biopsy
• Diffuse disease needs a wedge biopsy

URINARY BLADDER
• Anechoic fluid-filled structure in the caudal
abdomen
• Size is dependent on volume of urine in the
lumen
• Sometimes falls back into the pelvis
• Should be imaged transversely and longitudinally
• Acoustic window for the caudal aorta, caudal vena cava,
sublumbar lymph nodes, and uterus.

URINARY BLADDER IMAGING
• Images to acquire
Longitudinal Midline Body
Longitudinal Midline Trigone
and Proximal Urethra
(still image and cineloop)
Transverse Mid-body
Urinary Bladder

URINARY BLADDER
• Sonographic appearance
-Outer hyperechoic serosa
-Hypoechoic smooth muscle and mucosa
-Wall image should be uniform
-Normal thickness 1-2 mm when distended; appears more thickened when
empty
-Colon may impinge and distort the wall
• Ureters should not be seen entering trigone; may see ureter papilla or ureter jet
• Anatomy – Apex, body, trigone, proximal urethra

NORMAL BLADDER
LONGITUDINAL BODY
LONGITUDINAL BODY
WITH URETHRA

NORMAL BLADDER
Transverse
Mid Body

URINARY BLADDER LESIONS
• Calculi (stones)
•Highly echogenic with have acoustic shadowing
•Gravity-dependent (turn the patient)
• Neoplasia
•Project from the wall into the lumen
•Can also cause diffuse irregular thickening
•Usually mixed echogenicity
FNA of TCC is not recommended due to tumor seeding
• Blood clots
•Irregular, hypo/hyperechoic masses
•May be mobile or adhered to bladder wall
• Can use color doppler to help distinguish clot from neoplasia

URINARY BLADDER LESIONS
MULTIPLE CALCULI
PROBALE AMM. URATE MULTIPLE CALCULI

URINARY BLADDER LESIONS
FOCAL TRANSITIONAL
CELL CARCINOMA
TRANSITIONAL CELL
CARCINOMA

URINARY BLADDER TCC
URINARY BLADDER LESIONS
• Cystitis may cause thickening or irregularity of the mucosa, mainly
involving the cranioventral bladder wall. Blood clots may be associated
with cystitis, as are calculi and echogenic urine sediment.
• Can see polypoid cystitis
-more of a stalk versus wide attachment
-can mimic neoplasia
• Bladder rupture is not reliably diagnosed on ultrasound exam alone.
although the presence of free abdominal fluid is easily seen. If saline or
sterile water is injected into the bladder while scanning, flow may be seen
through a defect in the bladder wall. Positive contrast cystography is more
reliable for the diagnosis of bladder rupture, however.

URINARY BLADDER LESIONS
CYSTITIS CYSTITIS

URINARY BLADDER LESIONS
BLADDER RUPTURE

URINARY BLADDER RUPTURE

FEMALE REPRODUCTION
• Uterus
-Tubular structure with layering
-Dorsal to urinary bladder – good place to start
-Follows up to kidneys
-Typically not seen well except if diseased or during estrus cycle
• Ovaries
-Located caudal and medial to caudal pole of kidney
-small oval; varying appearance dependent on cycle; may look cystic

FEMALE REPRODUCTION
• Pyometra
-large tubular fluid filled structure
-fluid is usually echogenic and “swirly”
• Hydrometra
-anechoic fluid smaller diameter of uterus
• Neoplasia

FEMALE REPRODUCTION
HYDROMETRA PYOMETRA

MALE REPRODUCTION
Prostate
• Found caudal to urinary bladder along
midline/ urethra
• Use urinary bladder as landmark
• Scan in transverse and longitudinal fashion
• Neutered male prostate will be small well marginated and
hypoechoic

MALE REPRODUCTIONPROSTATE

MALE REPRODUCTION
Normal
Prostate

MALE REPRODUCTION
• Benign Prostatic Hypertrophy
•Increase echogenicity
•Small anechoic cavitations are normal
•Almost always symmetrical, well defined.
• Prostatitis
•Hyperechoic – like BPH
•Multiple anechoic cavitary lesions
•Usually painful

MALE REPRODUCTION
PROSTATE - BPH

MALE REPRODUCTION
BENIGN PROSTATIC
HYPERPLASIA PARAPROSTATIC CYST

MALE REPRODUCTION
• Prostatic Abscess
-often a sequelum to prostatitis or BPH
-irregular echogenic fluid filled area
-fluid is echogenic due to blood, WBC’s and bacteria accumulation
• Paraprostatic Cyst
-”one to many bladders”
-finding two or more anechoic structures in the caudal abdomen. Can
become infected.

MALE REPRODUCTION
• Prostatic Neoplasia (Adenocarcinoma)
-often coexists with and is thought to be a sequelum to
infection.
-may see periprostatic effusion
-increased size, irregular margin, multiple hyperechoic foci
-may see dystrophic calcification (shadows)
-image sublumbar lymph nodes (common area to
metastasize)

MALE REPRODUCTION
• Testes Normal Anatomy
-coarse to medium stippled eco pattern
-rete testes: 0.2 mm wide linear structure on long axis
-epididymus: hypoechoic and stippled relative to testes
-testicular tunic: bright echogenic covering

MALE REPRODUCTIONNORMAL TESTES

MALE REPRODUCTION
• Testicular neoplasia
-Sertoli cell tumor: hyperechoic/mixed echogenic mass,
extensive organ distortion
-Interstitial Cell Tumor: focal hypoechoic, well marginated
mass
-Seminoma: coarse hypoechoic mass (variable), disrupt testes
architecture, may have fluid
• Other testicular disorders: orchitis/epididymitis, retained
testicles, granulomatous infiltrates
GASTROINTESTINAL IMAGING
• Patient prep important
• Gas will cause artifact and limit imaging
• Cannot “run” the whole bowel
• Normal sonographic appearance
● 5 sonographic layers
Serosa (hyperechoic)
Muscularis (hypoechoic)
Submucosa (hyperechoic)
Mucosa (hypoechoic)
Lumen - often filled with gas (hyperechoic)
• Duodenum, jejunum, ileum, and colon can be
individually distinguished

GASTROINTESTINAL IMAGING
• Normal wall thickness:
Canine Feline
Stomach 3-5 mm Stomach 2 mm
Small Intestine 2-4 mm Small Intest 2 mm
Colon 2.5-3 mm Ileum 3 mm
Duodenum 3-5 mm Colon 1.5 mm
(usu about .1mm thicker than SI)
• Stomach 3-5 contractions/min
• Small Intestine 1-3 contractions/min

GI IMAGING STOMACH
NORMAL STOMACH ADENOCARINOMA

GASTROINTESTINAL IMAGING
NORMAL INTESTINES DUODENUM

GASTROINTESTINAL IMAGING
NORMAL ILEUM NORMAL ILEUM

GASTROINTESTINAL IMAGING
Most common pathology I see
• Mass lesions: neoplasia – lymphoma, mast cell tumor,
adenocarcinoma; less common granulomatous lesions
• Thickened bowel wall associated with IBD or lymphoma
(mostly see in cats)
• Intussusception
• Jejunal lymphadenopathy
• Foreign bodies

GASTROINTESTINAL IMAGING
THICKENED SM
INTESTINE IBD OR LYMPHOMA

GASTROINTESTINAL IMAGING
• Stomach
-5 layers as intestines; limited by luminal gas
-rugal folds can be visible
-measure wall between rugal folds
-wall thickness 3-5 mm
-large fluid distended stomach concerns for obstruction or possible
motility disorder
-stomach and duodenum should have 4-5 peristaltic contractions per
minute; jejunum contracts 1-3 times minute

GI IMAGING STOMACH
NORMAL STOMACH ADENOCARCINOMA

GASTROINTESTINAL IMAGING
Mass lesions
• expansive area with loss of intestinal wall layering
• May be symmetrical (more common with lymphoma) or
asymmmetrical (more common with adenocarcinoma)
• Lymphoma can have an infiltrative pattern that causes wall
thickening but retains clear wall layering

GASTROINTESTINAL IMAGING
ILEUM MASS
LYMPHOMA

GASTROINTESTINAL IMAGING
Intussusception
• Telescoping of bowel within itself
• Can occur anywhere along intestinal tract
• Characteristic ultrasound appearance
• Cross section shows a multilayered, concentric, target like lesion due to
multiple layers of bowel “stacked” on top of each other
• Often has hyperechoic mesentery within the center due to mesentery
telescoping with the intestine.
• Inflammation and edema may distort the image however

GASTROINTESTINAL IMAGING
INTUSSUSCEPTION
LONGITUDINAL

GASTROINTESTINAL IMAGING
INTUSSUSCEPTION
TRANSVERSE

GASTROINTESTINAL IMAGING
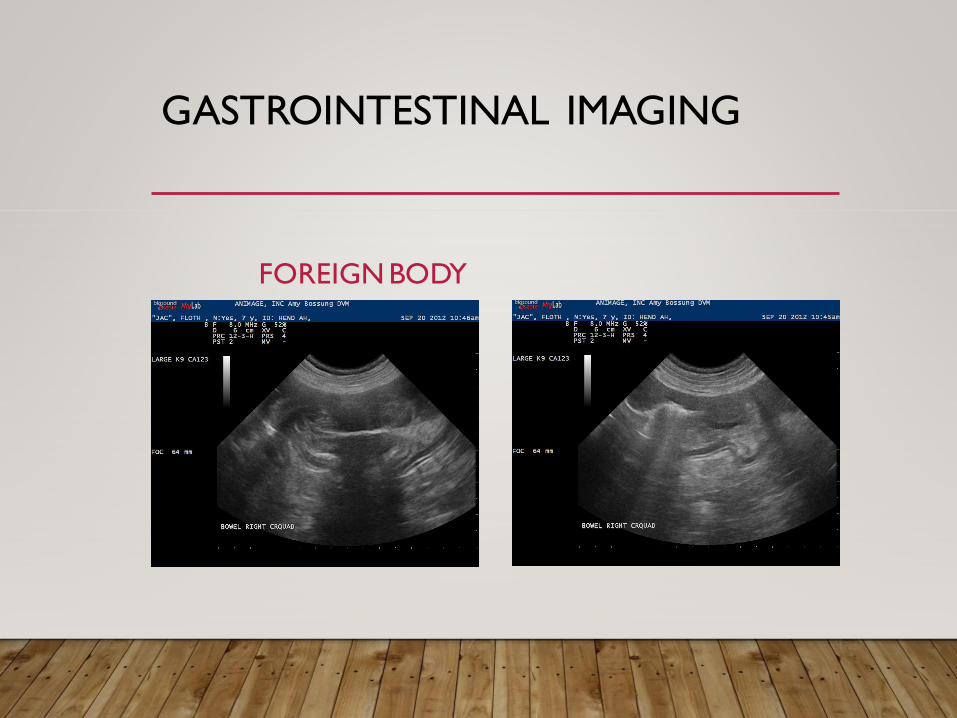
Foreign Bodies
• Linear foreign bodies
-plication of bowel; sometimes can see the hyperechoic linear line
within the lumen
• Other foreign bodies will have a variable appearance and depends on
the type and acoustic impedance of the material
-hyperechoic with strong shadow or “dirty” shadow
• Dilated fluid filled intestines proximal to the suspected foreign body
GASTROINTESTINAL IMAGING
FOREIGN BODY

GASTROINTESTINAL IMAGING
Jejunal lymphadenopathy
• Ovoid to elongated homogenous; can see them with newer machines
• Reactive nodes get a mild heterechoic look but still remain ovoid
shaped
• Neoplastic infiltration node will get larger and often as wide as they
are long and are often hypoechoic or have a mixed echogenic
appearance.
• Maybe able to find lymphoma here if the intestines are thickened but
there isn’t a mass to aspirate

GASTROINTESTINAL IMAGING
REACTIVE JEJUNAL LN
JEJUNAL LNS
LYMPHOMA

GASTROINTESTINAL IMAGING
REACTIVE - LN FLUID IN CECALAREA

THE END
“Man cannot discover new oceans unless he has the courage to
lose sight of the shore.”- Andre Gide