urinary system 4 glomerular disease ii professor john simpson
TRANSCRIPT
Urinary system 4Glomerular disease II
Professor John Simpson

The possible clinical presentations
• acute nephritis (aka acute nephritic syndrome)• rapidly progressive GN (acute nephritis with acute renal
failure) • nephrotic syndrome• chronic renal failure• proteinuria and/or haematuria
• but overlaps occur and the same patients can have different presentations at different stages of his/her disease
• and some of these presentations can also be due to non-glomerular disease

Last lecture on situations where filter clogs up or leaks a bit
This one mainly on what happens when the glomerular filter leaks a lot over a significant period of time, causing the nephrotic syndrome

Nephrotic syndrome
The syndrome always consists of 3 things -
• massive proteinuria (usually > 3.5 g/day)– predominantly albuminuria
• hypoalbuminaemia (usually < 3 g/dl)
• oedema (often severe)
• and, usually also, hyperlipidaemia
Nephrotic syndrome (NS)
• always the result of severe and prolonged damage to the glomerular filter
• that results in massive proteinuria
• which leads to hypoalbuminaemia
• and therefore reduced plasma colloid osmotic pressure
• and that causes (Starling equation) oedema, which may be severe (anasarca)
Other plasma proteins also leak
• transferrin microcytic anaemia
• antithrombin III thrombosis
• IgG susceptibility to infection
• lipoprotein lipase altered lipoprotein metabolism, hyperlipidaemia

Why these proteins?
– it’s the smallest plasma proteins which leak most
– (liver initially compensates by producing more albumen, but only for limited time)
– - and why hyperlipidaemia?
Causes of nephrotic syndrome
• anything which causes severe prolonged filter damage• glomerulonephritis (GN), including
– proliferative GN– membranous GN– minimal change GN– FSGS– membranoproliferative GN
• non GN glomerular disease, including– diabetes mellitus– amyloidosis– myeloma
Proliferative GN
• any proliferative GN which does not resolve - – GN (streptococcal and other infections,
autoimmune etc), whether diffuse, RPGN or focal
• but other GNs are more common causes of NS
Membranous GN
• commonest cause of NS in white adults, but also seen in all other races: mostly middle-aged/elderly
• Ag/Ab complexes again - long term deposition
• in most cases, Ag in complex is unknown (“idiopathic membranous GN”), but…
Known immune complex associations in membranous GN
• infections (hepatitis B, quartan malaria, syphilis, schistosomiasis)
• drugs (e.g. penicillamine, NSAIDs)
• inorganic metals (gold, mercury)
• malignant tumours (e.g. lung, lymphoma, colon)
• autoimmune diseases (espec. SLE)

Membranous GN - uniform diffuse thickening of glomerular capillary wall

Membranous GN
• accumulation of electron-dense, immune complex deposits along outside of GBM
• paradoxically the thickened GBM is very leaky• epithelial cell component of filter probably also
damaged
• no cell proliferation – because Ag/Ab reactions are on outside of GBM, thus away from mesangial & endothelial cells and PMNs



Membranous GN
• tends to have an indolent course
• sometimes, proteinuria decreases for a time (so nephrotic syndrome will disappear)
• a few (mainly younger patients) resolve (espec. if “association” can be dealt with)
• but most drift into chronic renal failure (“chronic GN”) over 2-20 years
Minimal change GN
• most common cause of NS in children in the “west”, but also occurs in adults – also seen in Africa
• peak ages 2 – 10
• NS sometimes accompanies URT infection or immunisation without lag time
• NS extremely responsive to steroids (almost diagnostic of the disease)

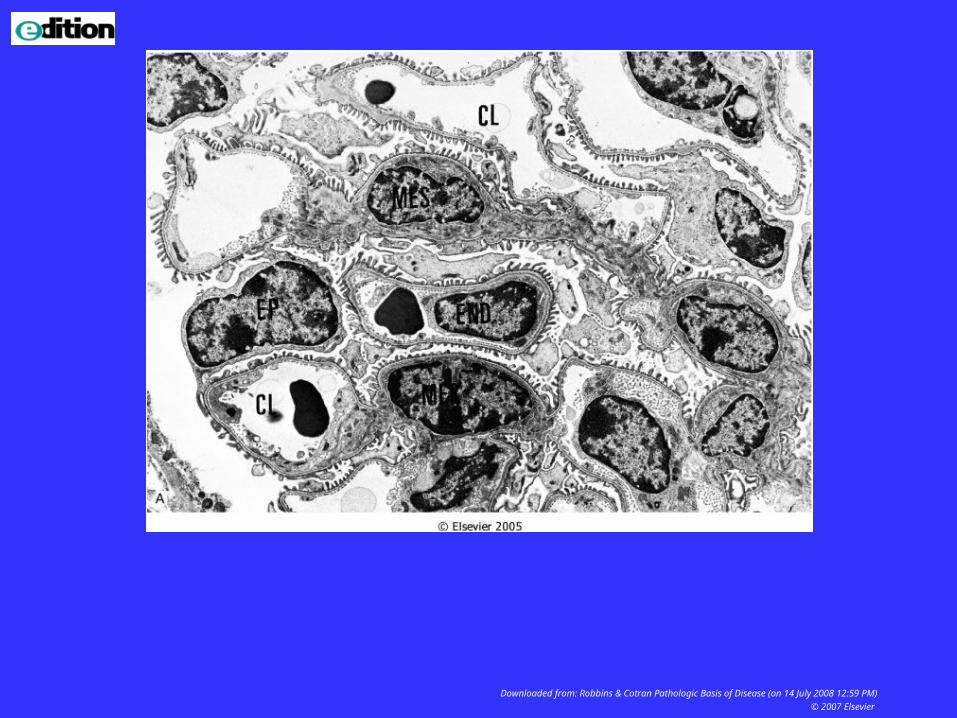
Minimal change GN
• little to see by light microscopy: may be fat in renal tubular cells (= lipoid nephrosis)
• EM shows loss of foot processes of epithelial cells
• no local immune reactants• probably cytokine-like material from distant
immune reaction targets the epithelial cells• good prognosis



Minimal change GN
• classically, recurrent episodes of NS
• in children, often resolves by puberty
• if patient becomes steroid resistant, diagnosis probably wrong
• in a few adults, this type of GN associated with lymphomas or leukaemias
FSGS (focal and segmental glomerulosclerosis)
• commonest cause of NS in blacks• proteinuria often heavy enough to cause NS• most cases progress to renal failure within
months – year or two• associations include HIV infection, heroin
addiction, IgA GN etc– but also “idiopathic”


Focal GN in patients with HIV
• HIVAN common
• often seen before AIDS
• probably due to anti-HIV Abs
• typical lesion is collapsing type of FSGS
• usually proteinuria, often severe enough for nephrotic syndrome
• prognosis, in terms of eventual renal failure, worse in adults
Other renal problems in patients with AIDS
• post-infectious GN
• renal infection (pyelonephritis, TB etc)
• reactions to antiviral drugs – e.g. interstitial nephritis
• renal failure (acute or chronic)
• tumours

Back to causes of nephrotic syndrome

Membranoproliferative GN – mesangiocapillary GN in US textbooks
• rare GN, but commonest one in hepatitis C – also not uncommon in schistosomiasis
• microscopically rather like a mixture of proliferative and membranous GNs– i.e. both cellular proliferation and capillary wall
thickening
• clinical presentation usually NS: often profound hypocomplementaemia (? role of nephritic factors)
• renal failure within 10 years

Nephrotic syndrome also associated with non-GN disease
• diabetes mellitus
• amyloid
• myeloma and other paraproteinaemias
• pathogeneses unclear, though all must be damaging GBM filter to cause chronic massive proteinuria.

Diabetic nephropathy
• diabetic glomerular disease• common after DM present 10 years+• especially in poorly controlled type 1 DM• patients may also have diabetic
retinopathy• always proteinuria, sometimes bad
enough to cause NS• at least 50% cases will progress to end
stage renal failure within 10 years

Diabetic nephropathy
• uniform thickening of GBM
• diffuse global increase in mesangial matrix (connective tissue in mesangium)
• segmental nodular excess of mesangial matrix (Kimmelstiel-Wilson lesions)
• pathogenesis unclear, but probably related to degree of hyperglycaemia
Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 14 July 2008 12:59 PM)
© 2007 Elsevier


Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 29 January 2007 12:01 PM)
© 2005 Elsevier


Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 29 January 2007 12:01 PM)
© 2005 Elsevier
Amyloid
• 80 - 90% patients with secondary amyloidosis (TB, chronic suppuration, rheumatoid arthritis, myeloma etc) get renal amyloidosis
• glomerular deposits of amyloid material cause proteinuria, again often heavy enough to cause nephrotic syndrome
• (amyloid also found in vessels)• progression to chronic renal failure within 1-2
years


Myeloma and other paraproteinaemias
• glomeruli trap abnormal proteins (Bence-Jones and other paraproteins)
• GBM gets damaged and becomes leaky
• proteinuria, if severe and prolonged, causes nephrotic syndrome
It’s not always nephrotic syndrome!
• patients with ALL of the diseases (GN and non-GN) causing nephrotic syndrome may at times have less severe proteinuria, so no nephrotic syndrome
• and, in some, the proteinuria sometimes disappears entirely
“Chronic” GN
• may result from ANY GN failing to resolve – but also may appear “de novo”
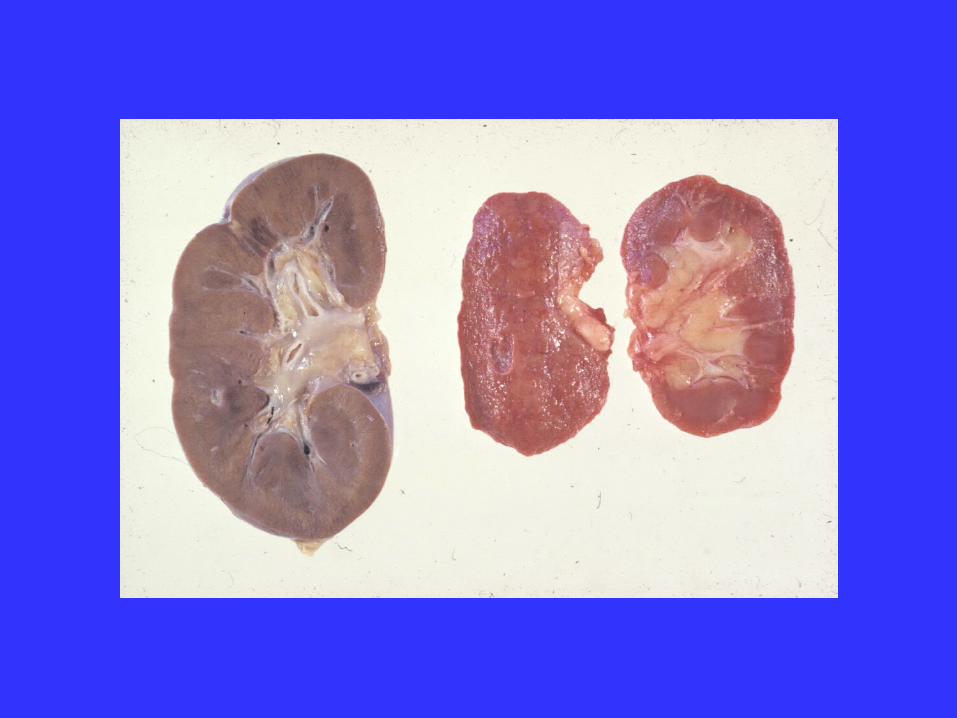
• glomeruli become fibrosed (global glomerulosclerosis) with secondary tubular loss, so kidneys shrink
• rate of glomerular loss determines how quickly renal function deteriorates
• GNs thus one cause of “end-stage” kidney (or “granular contracted kidney) and so chronic renal failure
• most patients hypertensive & require renal replacement therapy
• diabetes, amyloid and, less commonly hypertension can also cause chronic renal failure by gradually replacing functioning glomeruli

Downloaded from: Robbins & Cotran Pathologic Basis of Disease (on 14 July 2008 12:59 PM)
© 2007 Elsevier
The possible clinical presentations
• acute nephritis (aka acute nephritic syndrome)• rapidly progressive GN (acute nephritis with acute renal
failure) • nephrotic syndrome• chronic renal failure• proteinuria and/or haematuria
• but overlaps occur and the same patients can have different presentations at different stages of his/her disease
• and some of these presentations can also be due to non-glomerular disease

- and finally

Systemic disease and the kidneys
• (depends on how “systemic” is defined) • SLE (and other non-organ specific autoimmune
diseases) – glomerulonephritis• DM, amyloid, myeloma – nephrotic syndrome• infective endocarditis - GN • Henoch-Schonlein purpura – IgA GN• HIV, TB, schistosomiasis• etc etc

- and many of these diseases affect the kidneys in more than one way
e.g. Diabetes and the kidney
In addition to diabetic nephropathy (glomerulosclerosis), diabetes also associated with
• pyelonephritis (bacterial infection of kidney)• increased risk of atheroma and thus renal
ischaemia• increased risk of hypertension and thus
arteriosclerotic renal disease (nephrosclerosis)• increased risk of papillary necrosis (especially if
pyelonephritis present)
