glomerular filtration &
DESCRIPTION
glomerularTRANSCRIPT
Glomerular Filtration & Acute Renal Failure

Renal Blood Flow
• Majority of RBF is directed to the cortex, with only a small proportion delivered to the medulla
• Thus the medulla is very sensitive to reduction in RBF & oxygen delivery that may induce hypoxia, and result in tubular damage, causing acute renal failure – Acute Kidney Injury / AKI
• Main determinant of overall RBF :– State of vasoconstriction of the renal arterial tree

Glomerular Filtration
• Process of filtration occurs across a complex barrier consisting of– Thin fenestrated endothelial lining of the glomerular
capillary– The glomerular basement membrane– The foot processes of the epithelial cells
• This filtration barrier allows free passage of solutes– Up to a molecular weight of around 60,000D– But retain cells and protein within the circulation

Afferent art.
Efferent art
Pgc = 45 mmHgPt = 10 mmHgπgc = 25 mmHgPuf = 10 mmHg
• An overall expression of GFR: GFR = Kf X P uf Kf= ultrafiltration coefficient, made up of the product of the hydraulic
permeability of the filtration membrane times the surface area available for filtration
• Factors which interfere with any of these determinants of glomerular filtration may lead to an abrupt fall in GFR and thus acute renal failure unless adequate compensatory responses occur
• The most important physiological determinant is the capillary hydrostatic pressure, which may be reduced by
– Reduction in perfusion pressure reaching the afferent arteriole– Increase in afferent arteriolar tone– A decrease in efferent arteriolar tone
• Pressure in the tubular system may rise significantly during ureteric obstruction, thus reducing the GFR
• Changes in plasma oncotic pressure are less important in altering GFR in physiological or pahological conditions
• Pathologies involving the glomeruli may lead to alteration in the ultrafiltration coefficient and impair GFR by
– Decreasing the hydraulic permeability– Obliterating the total capillary surface area available for filtration– E.g. glomerulonephritis, DM


• In the normal kidney minor perturbations in levels of individual substances do not have significant net effects on GFR because of compensatory changes in other factors which tend to maintain a haemodynamic steady state
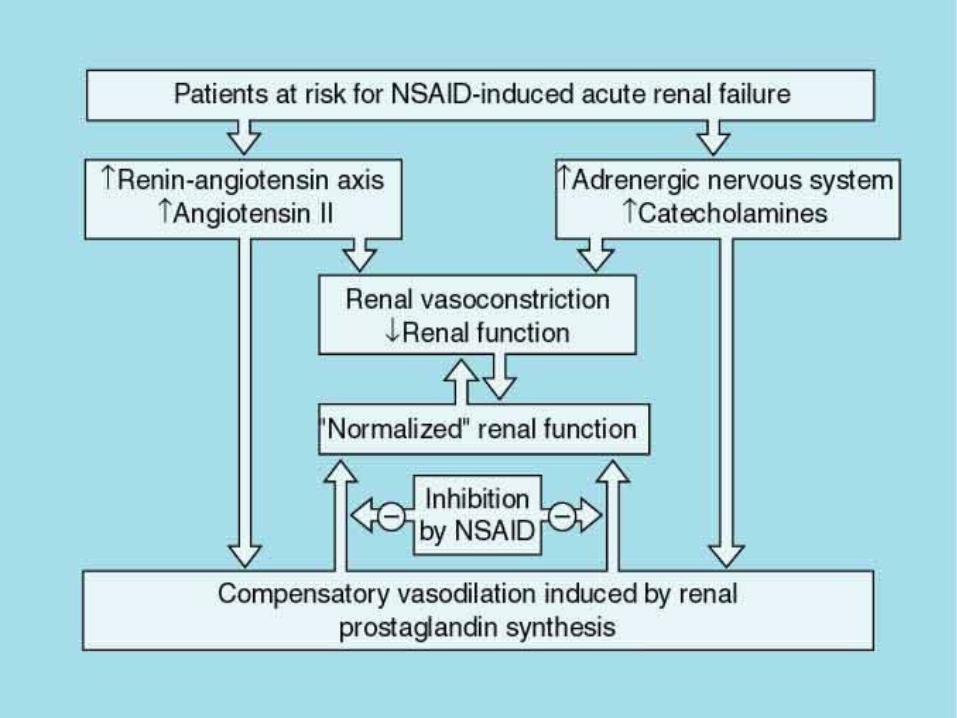
• If renal function is impaired, particularly because of a low renal perfusion pressure, maintenance of GFR is highly dependent on intrinsic compensatory mechanisms such as afferent arteriolar vasodilatation (PG) and efferent arteriolar vasoconstriction (AII)
• Factors that interfere with these mechanisms – NSAIDS, ACE-I, ARB – blunt these compensatory responses and may precipitate ARF

Autoregulation of RBF & GFR
• The myogenic mechanism– Intrinsic capacity of the afferent arteriolar smooth muscle cells to
increase their state of contraction in response to an increase in renal perfusion pressure
– This response, probably mediated by vasoactive agents produced by endothelial cells acting on smc in the afferent arteriole, serves to blunt the transmission of changed arteriolar pressure into the glomerular capillary bed
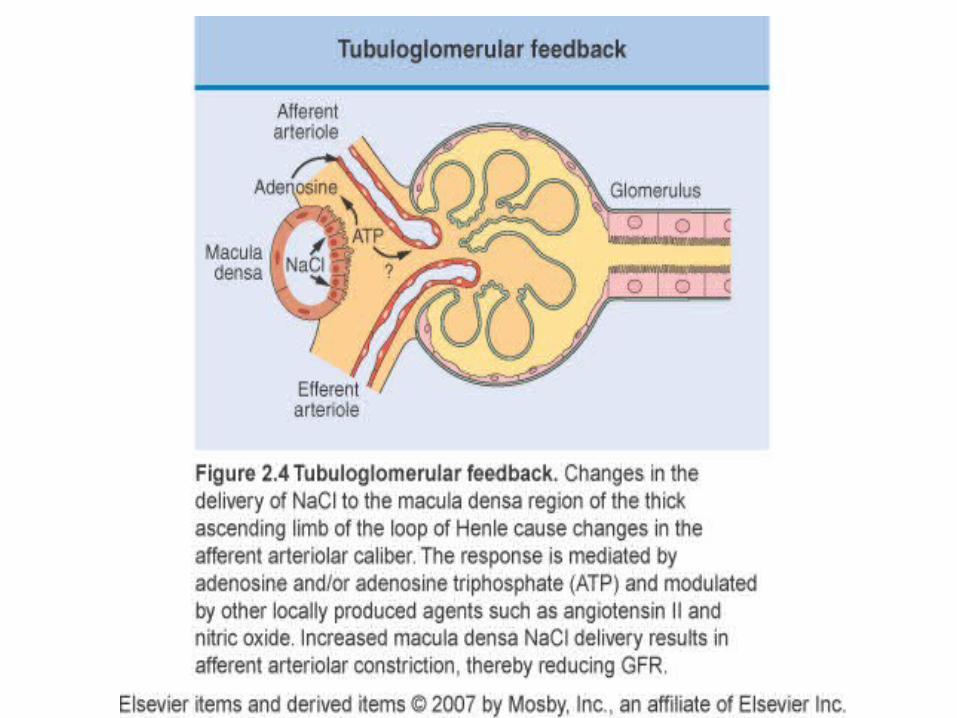
• The Tubuloglomerular feedback (TGF)– GFR in individual nephrons is regulated according to the rate of solute
flow through that (distal tubule) nephron– The ionic composition (and indirectly the flow rate) of the tubular fluid
can be sensed by the macula densa– Which signals directly to the vascular structures of the glomerulus to
influence GFR– During periods of avid tubular NaCl reabsorption, the [Na] of the luminal
fluid is reduced at the macula densa• Filtration in the corresponding glomerulus is increased, primarily by dilatation
of the afferent arteriole– When NaCl concentration and fluid delivery are high at the macula
densa, • afferent arteriole tone is increased and single nephron GFR falls
– The mediator of the vasoconstrictor response involved in TGF appears to be locally produced Adenosine, acting via the A1 receptor on the afferent arteriole


Renal secretion and clearance• The rate at which a solute (s) is excreted by the kidney
(Es) is given by the product of the concentration of the solute in the urine (Us) and the urine flow rate (V), which is the urine volume over a defined period
Es = Us X V mmol/min, mg/min
• The renal clearance (Cs) of solute (s) is defined as the apparent volume of plasma from which the substance is completely removed per unit time during passage through the kidneys.
• It is equivalent to the ratio of the excretion rate to the simultaneous plasma concentration for that substance (Ps)
Cs = (Us X V) / Ps ml/min,

Measuring the glomerular filtration rate
Inulin is freely filtered at the glomerulus and undergoes no reabsorption or secretionDuring its passage through the tubular system. GFR = inulin clearance


• In practice, an endogenous molecule whose behavior approximates that of inulin is used for clinical determination of GFR
• CREATININE• For a given individual, the amount of creatinine
entering the circulation per day is dependent almost exclusively on the skeletal muscle mass.
• As long as renal function is stable, this same daily amount will be excreted in the urine
• Cr, like inulin is freely filtered at the glomerulus and undergoes no tubular reabsorption, although there is a small degree of secretion by the tubules when renal function is impaired; may increase to 30% at low GFR


• Plasma Cr only starts to increase when approximately 50% of renal function (GFR) is already lost
• Each such relationship is specific to a given individual with a particular muscle mass, making comparison of plasma Cr between patients of different body size / muscle mass difficult
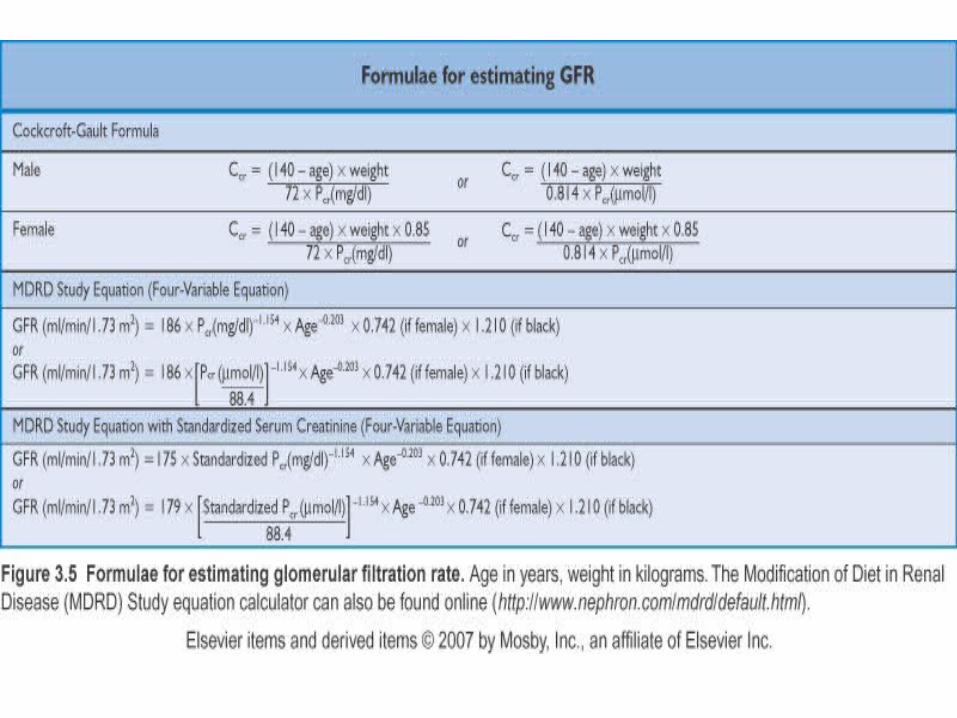
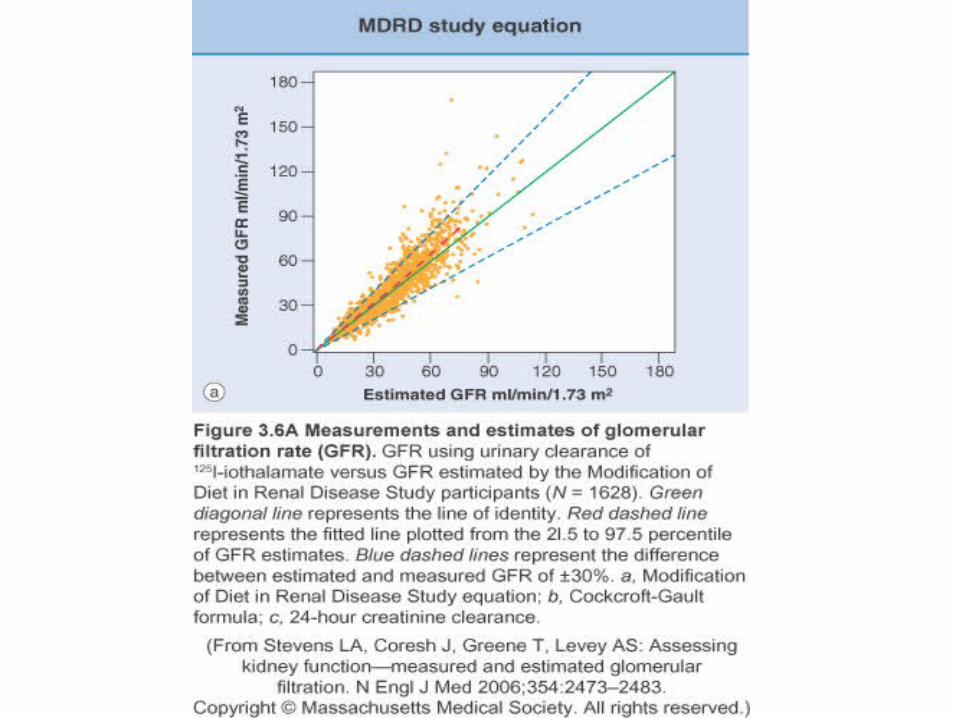
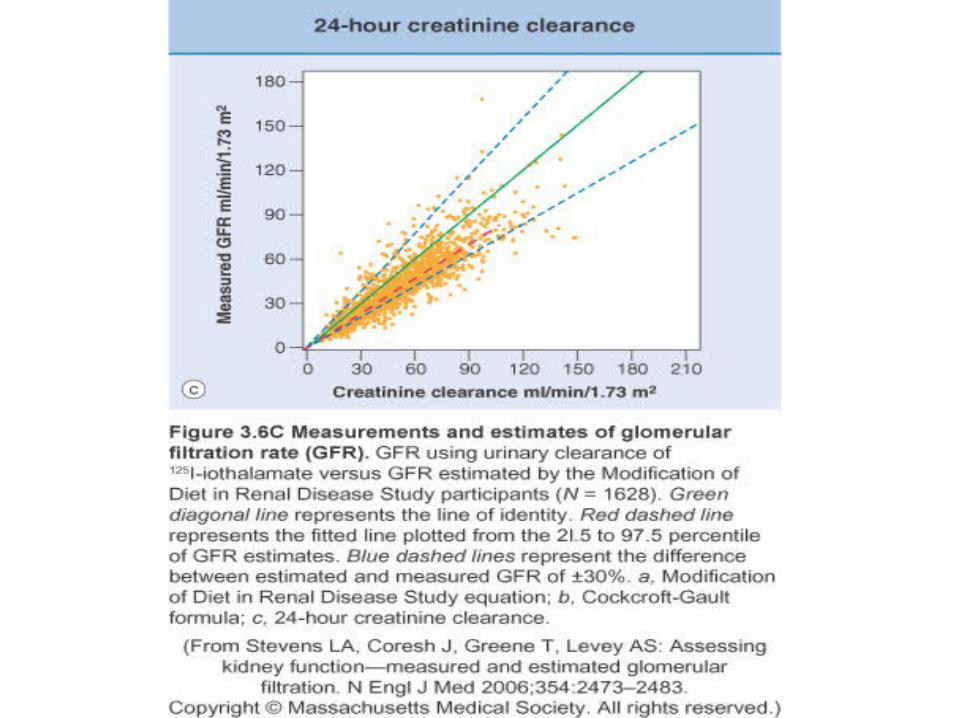
• Crockcroft & Gault formula: Estimated GFR (ml/min) = (140 – age) X weight (kg)
72 X plaama [Cr] (mg/dl)
X0.85 for women
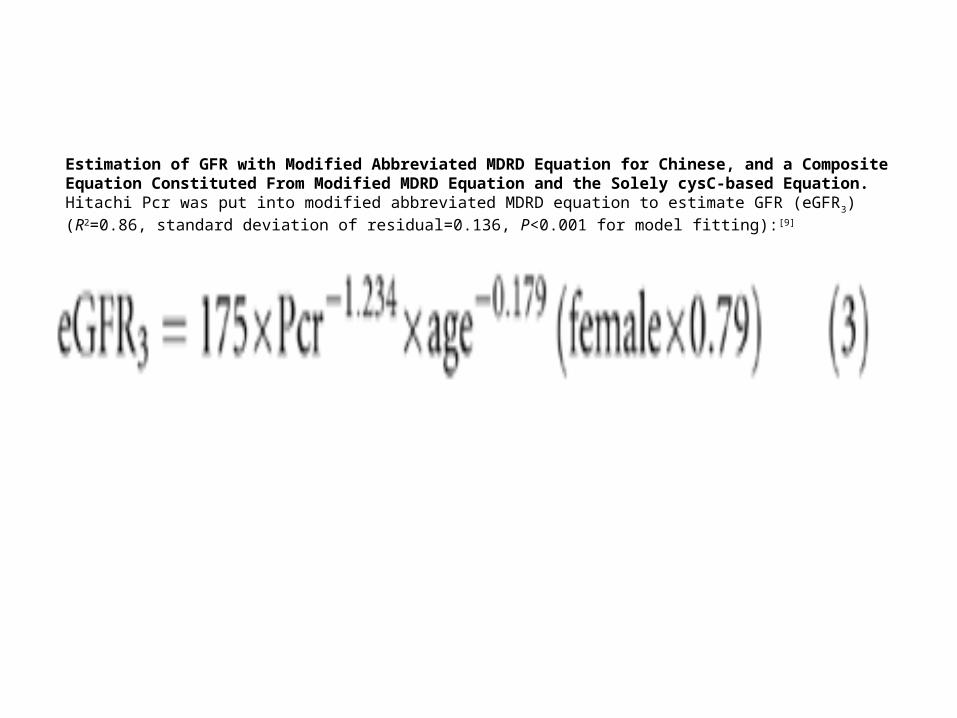
Estimation of GFR with Modified Abbreviated MDRD Equation for Chinese, and a Composite Equation Constituted From Modified MDRD Equation and the Solely cysC-based Equation. Hitachi Pcr was put into modified abbreviated MDRD equation to estimate GFR (eGFR3) (R2=0.86, standard deviation of residual=0.136, P<0.001 for model fitting):[9]

Urea • Synthesized in the liver from amino acid metabolism• Freely filtered at the glomerulus, but• Undergoes approximately 50% reabsorption during
passage through the nephron.• The clearance of urea is approximately half the GFR,
and plasma urea varies inversely with GFR• The fraction of filtered urea that is reabsorbed is not
constant, being greater during conditions of dehydration and low urine flow rate
• It is also related to the amount of protein absorbed from the gut, and to the protein catabolic rate



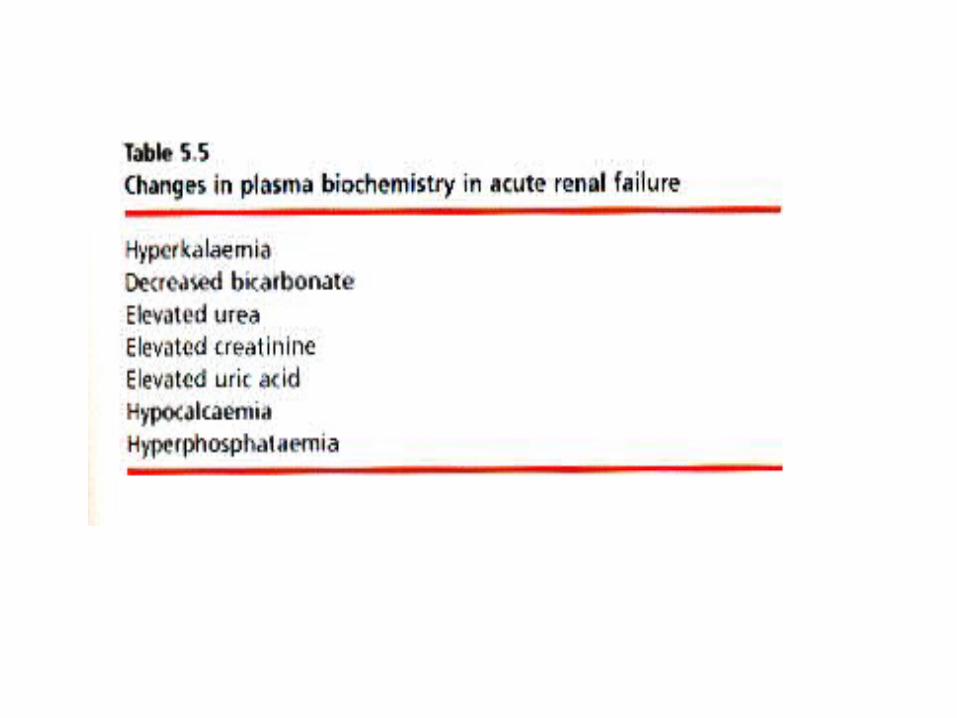
Acute Renal FailureAcute Kidney Injury

• ARF is a clinical term that encompasses many causes of abrupt renal impairment;
• that is, a fall in GFR over a period of hours to days which results in impaired fluid & electrolyte homeostasis and the accumulation of nitrogenous wastes.
• The most common causes are haemodynamic, immunological, toxic & obstructions.
• Major predisposing factors include volume depletion, drugs, and radiocontrast agents.
• Elderly, diabetic, and chronically hypertensive patients are at particular risk because of their predisposition to underlying vascular disease & poor renal autoregulatory responses
• In the hospital population, hypotension, heart failure, sepsis, and aminoglycoside use are common additional factors
• Sustained circulatory failure leading to ischemia-induced ATN accounts for the majority of cases of ARF








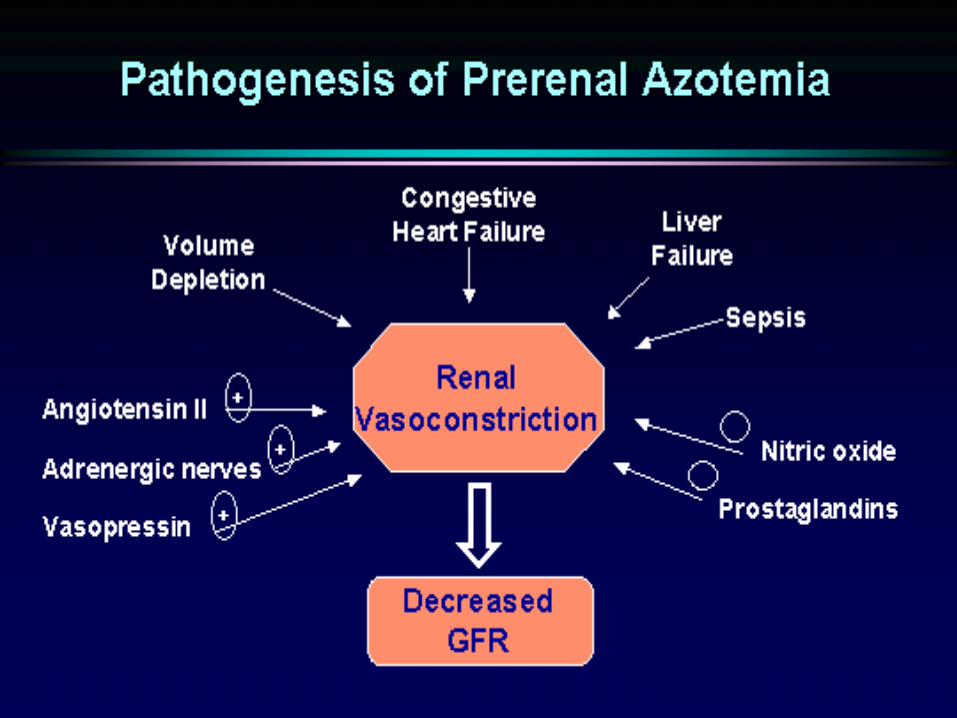
• In volume depletionvolume depletion, there is a decrease in renal plasma flow, decrease in the intraglomerular capillary pressure. Filtration fraction will remain the same under these circumstances and GFR will fall. This is before the neurohumoral responses kick in.
• In response to this change in renal plasma flow, renal blood flow, we have activation of the renin angiotensin system, angiotensin II causing vasoconstriction and then a response as well of vasodilatory prostaglandins causing a reduction in the vasoconstriction in the afferent arteriole.
• This results in actually a further decline in the glomerular plasma flow but because of the vasoconstriction in the efferent arteriole, intraglomerular pressure is restored to normal, filtration fraction actually rises, and GFR is maintained at a normal level; at the expense though of an increase in sodium reabsorption and urea reabsorption triggered both by the increase in angiotensin levels and the increase in filtration fraction.




FE (urea) <35% >35%






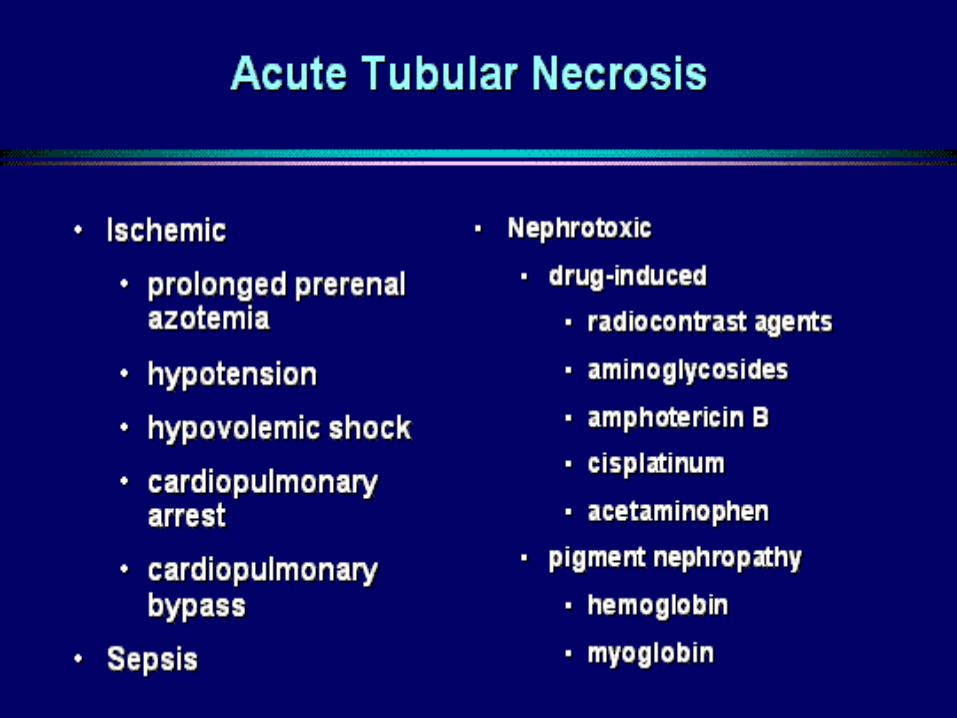
Acute Tubular Necrosis
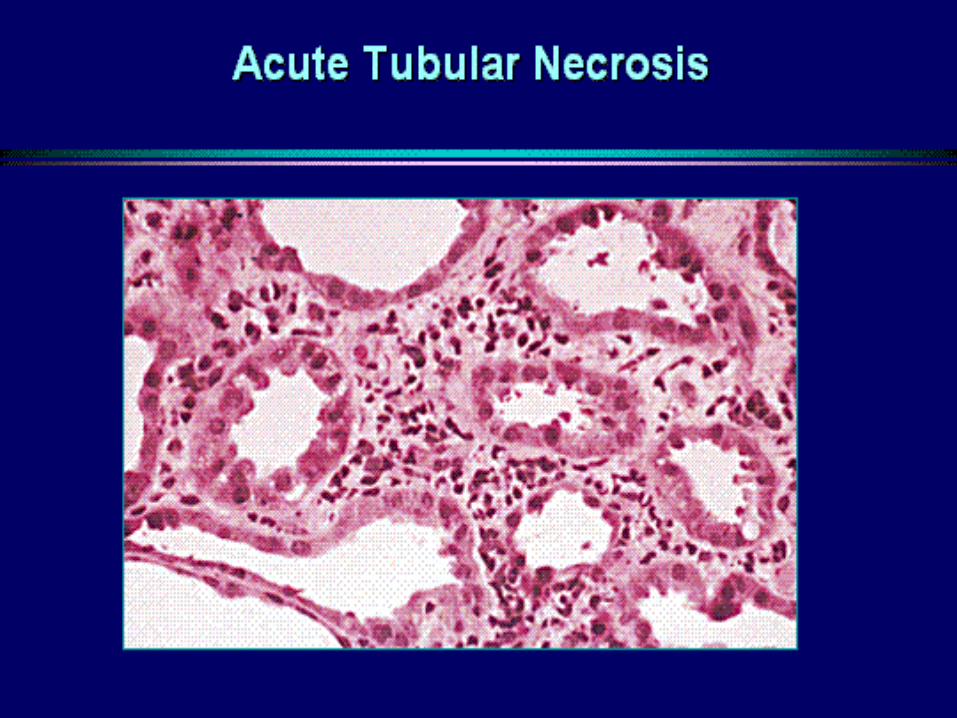


ATN: Urine sedimentThe urine sediment classically has many tubular epithelial cells and granular casts, as shown here with the classic muddy brown casts of ATN.


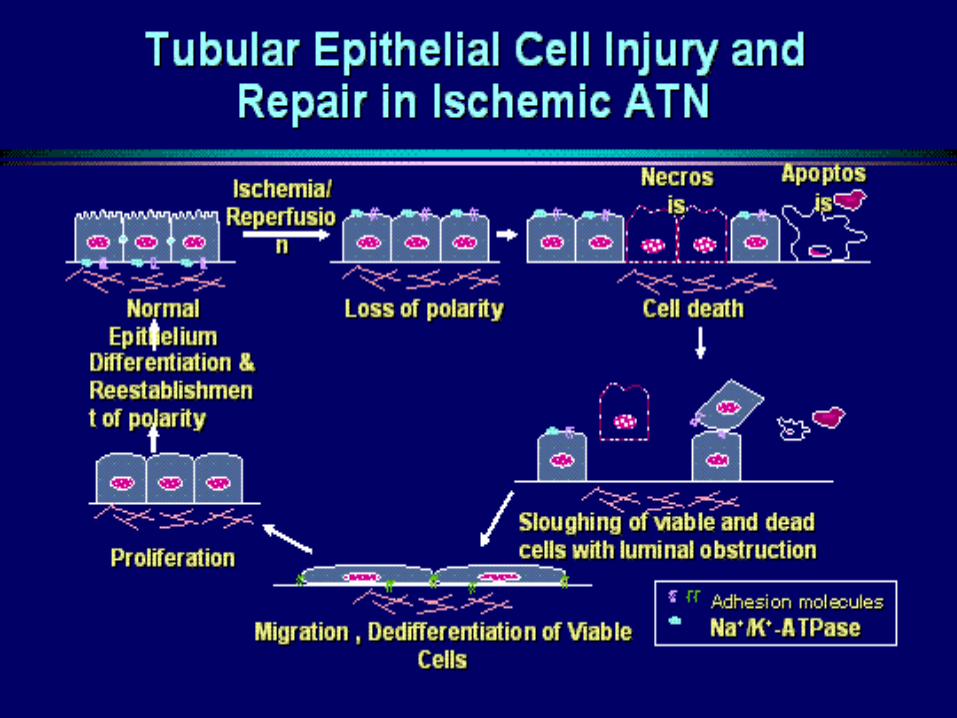
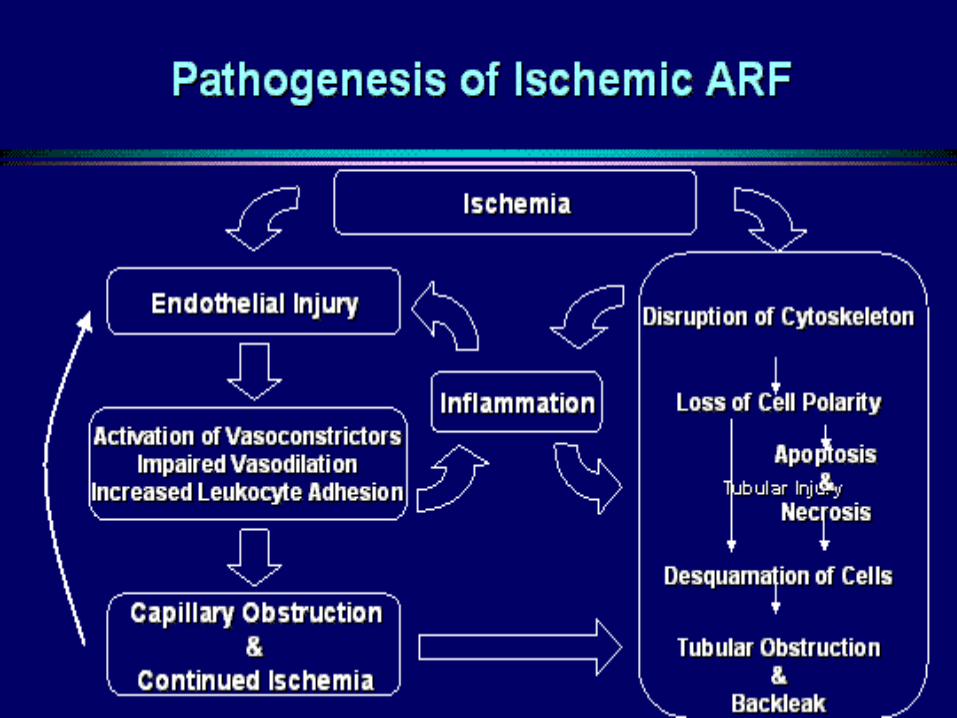

• As a result of the endothelial injury, there is activation of vasoconstrictors, impaired vasodilatation, endothelin release, and nitric oxide inhibition.
• There is increased expression of adhesion molecules and increased leukocyte adhesion.
• This goes on to cause capillary obstruction, continued ischemia, which extends the tubular injury, goes back and actually feeds back for further endothelial injury, but importantly, both the tubular cell injury and the endothelial injury trigger an inflammatory response that also amplifies the injury to the kidney.
• It has been shown that blocking of this inflammatory response can actually ameliorate the injury and shorten the course of acute renal failure in animal models.


• Inflammation and leukocyte activation in ischemic ATN
• There is local production of inflammatory mediators, so we have cytokines, complement, platelet activating factor, metabolites of arachidonic acid, the production of reactive oxygen species, and expression of the adhesion molecules.
• The activated leukocytes then infiltrate into the interstitium, have further release of these mediators, bringing in more lymphocytes and monocytes, further injury, maintaining and extending the injury. When you look at a patient who has ATN histologically, the pathologist will frequently say there is ATN, but there is also interstitial nephritis. The interstitial nephritis does not mean there are two processes going on. The interstitial nephritis that is seen, the interstitial inflammation, is part and parcel of the ATN.

• ATN is not just a disease of the kidneys, • The inflammatory process that is triggered in the kidney has systemic
effects. This is shown in animal models• Renal ischemia raises systemic tumor necrosis factor levels.• At the heart, there is increased expression of ICAM-1, one of the adhesion
molecules, that develops in the rats following ischemia, but not in the sham animals. There is infiltration of the cardiac tissue by inflammatory cells. You can demonstrate that there is change in cardiac contractility.
• That there is an increase in apoptosis of the cardiac myocytes. This is seen increasing progressively with duration of ischemia that is independent of the magnitude of azotemia that develops, but is not seen with nephrectomy despite the more severe degree of azotemia with nephrectomy - so that is not a factor of the renal failure causing the injury to the heart. It is the renal ischemic injury, and this can also be seen in cytotoxic injury.
• Renal ischemia reperfusion injury alters the expression of sodium channels and water channels in the lung with a decreased expression of the epithelial sodium channel and aquaporins, which is associated with a decrease in the clearance of lung water, so that increased lung water and respiratory compromise may occur independent of oliguria in patients with acute renal failure.



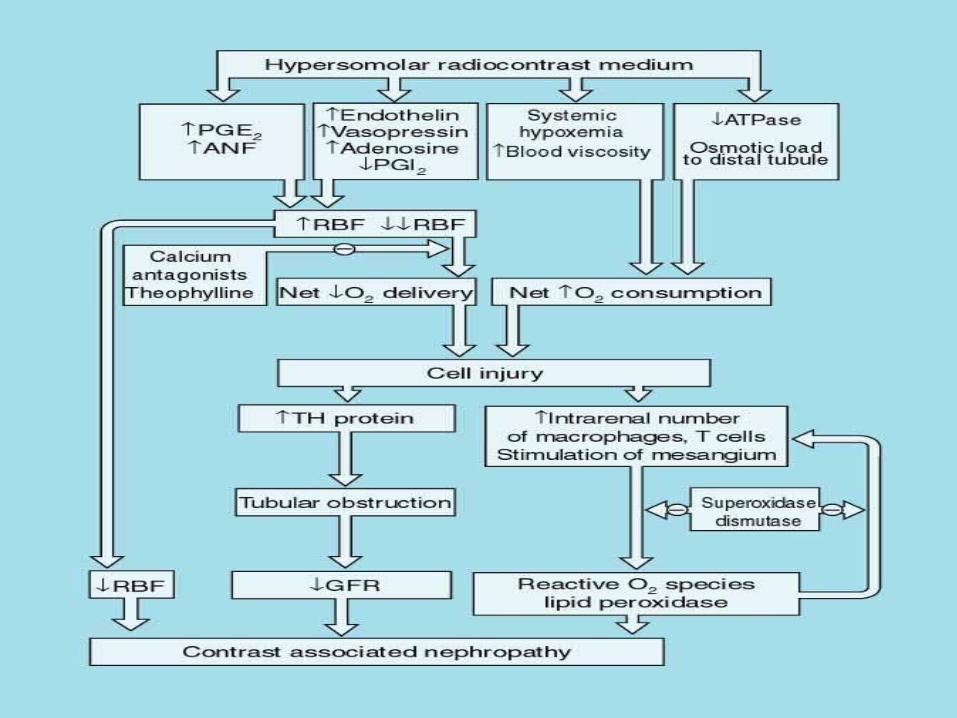
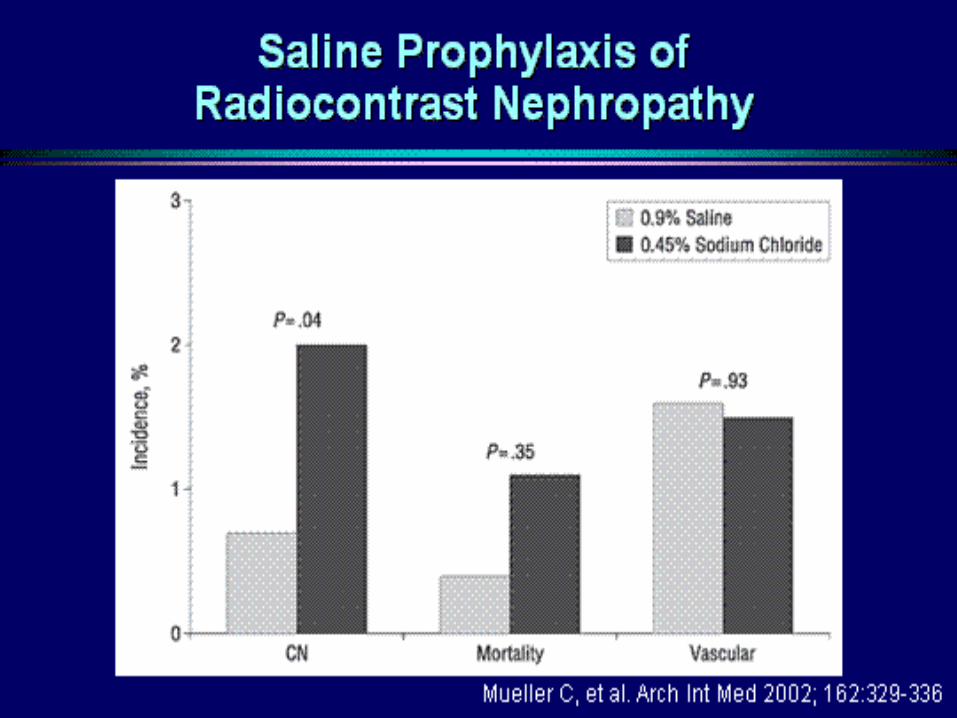
• Radiocontrast nephropathy. • Is an increase of serum creatinine of 25% at 48 hours or
72 hours; or 50% increase or 100% increase, or is it an increase of 0.5 or increase of 1 mg/dL?
• Increases in serum creatinine are associated with an increase in mortality, but a decrease in the number of patients.
• Even an increase in serum creatinine of less than 50%, namely, a 25% to 50% increase in creatinine, is associated with a doubling in mortality. There is about a five-fold increase in mortality in patients who have a 50% to 100% increase in serum creatinine. So small changes may be important.



The first group received normal saline at 1 mL/kg per hour for 12 hours, pre and post procedure, a second group that received saline plus mannitol, and a third group that received the same volume load plus furosemide.


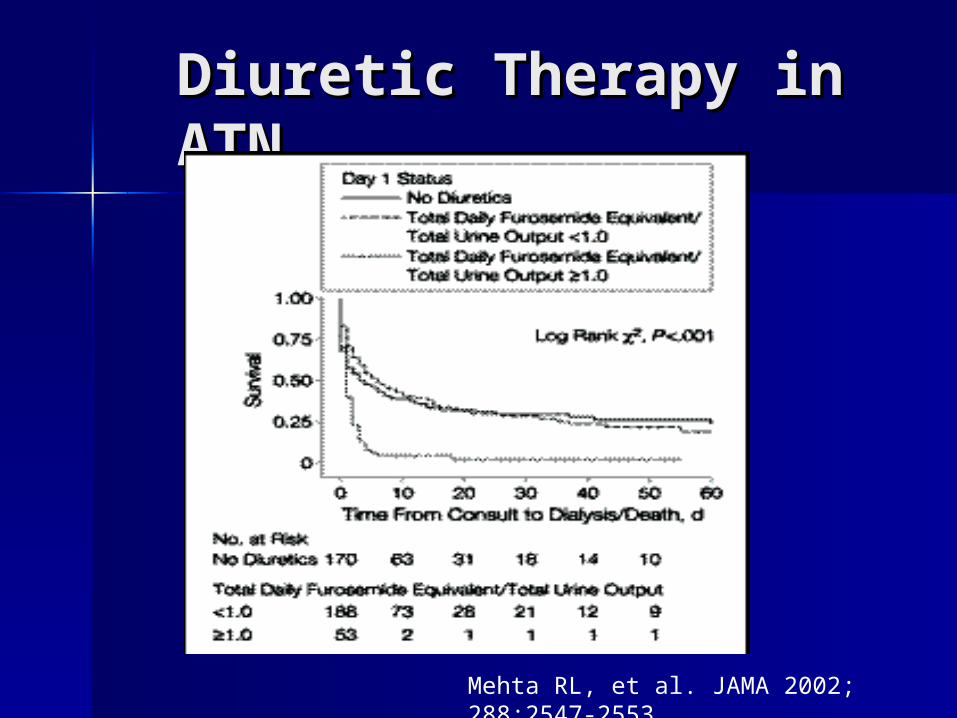
Diuretic Therapy in Diuretic Therapy in ATNATN
Mehta RL, et al. JAMA 2002; 288:2547-2553






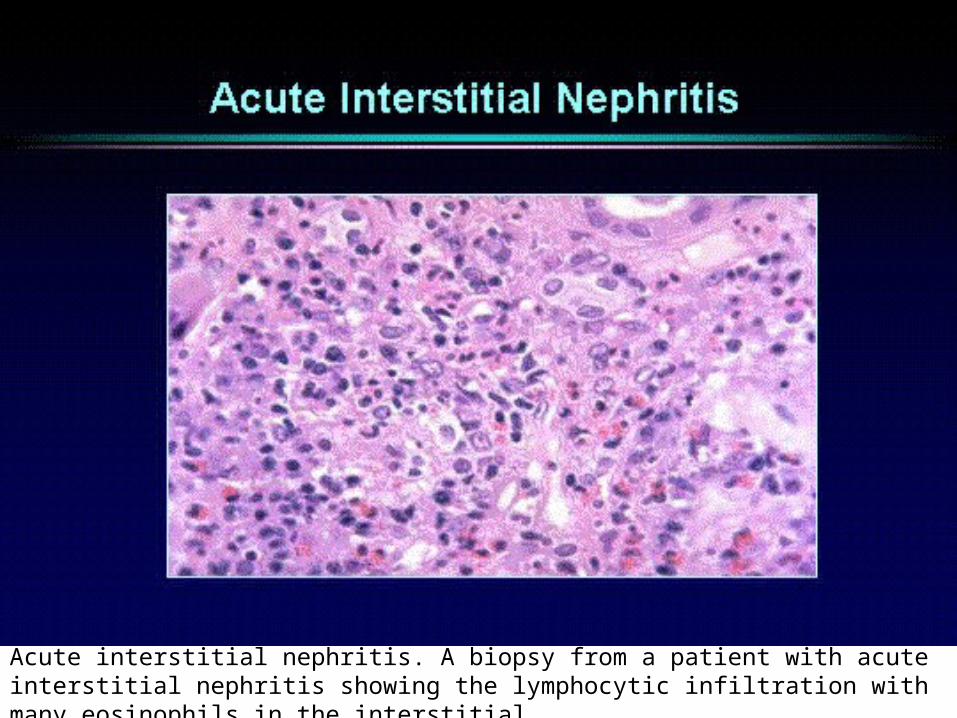
Acute interstitial nephritis. A biopsy from a patient with acute interstitial nephritis showing the lymphocytic infiltration with many eosinophils in the interstitial.



White cell cast

Hansel stain of the urine showing eosinophiluria

Acute glomerulonephritis. The characteristic finding that should tip you off to this is the presence of dysmorphic red cells and red blood cell casts in the urine.

Illustrating the histologic finding in atheroembolic disease of an arteriole with a characteristic cholesterol plaque in the atheromatous embolus here, and this is surrounded by a reactive process; and, as time goes on, you get an inflammatory process and then obliteration of the vasculature.


• The renal manifestations of atheroembolic disease may be subacute renal failure where the renal failure progresses slowly, frequently in a stuttering fashion over a period of days to weeks, frequently after an angiographic manipulation.
• Sometimes confused with contrast nephropathy. However, contrast nephropathy will usually have its onset within 24-36 hours and will have the peak serum creatinine in 3-5 days whereas atheroembolic disease may not have its onset for several days after the catheter manipulation.
• There may be a fulminant atheroembolism, fulminate showering with acute renal failure that may be oliguric or anuric.
• You may just see exacerbation of hypertension in a patient with preexisting hypertension.
• The patients may develop proteinuria. They may actually develop nephrotic syndrome, which is associated with a histology of focal and segmental glomerulosclerosis.
• They may present with hematuria or they may have renal infarction.




Anticoagulation may precipitate recurrent showers of atheroemboli.
Late recovery of renal function may occur.

