detection of glomerular and non glomerular hematuria using...
TRANSCRIPT

Detection of glomerular and non
glomerular hematuria using
flowcytometry
IRA PUSPITAWATIDEPARTEMEN PATOLOGI KLINIK DAN KEDOKTERAN LABORATORIUMFKKMK UGM-RSUP DR SARDJITO YOGYAKARTA

Introduction
Hematuria
Very important feature in kidney disease
Variation in hematuria prevalence

Introduction
Woolhander, et al. JAMA. 1989;262(9):1214-1219
• Prevalence of asymptomatic hematuria was 0,19-16,1%.
Woolhander, et al 1989
• Prevalence of asymptomatic hematuria was 13% among >35 years old man and postmenopousal woman.
Mohr, et al, 1986
• Prevalence of occult haematuriawas 20.1% among men over 60 years of age screening for bladder cancer using dipstick.
Britton, et al
1989

Hematuria4
• Gross hematuriaMacroscopic
• More than 5 RBC/ high-power field (hpf) on microscopic analysis of 2 or 3 properly collected urine specimens.
Microscopic
Karnath, et al. Hospital Physician 2007;62: 20-26; Grossted, et al. American Family Physician. 2007. 63

5Hyodo et al.and Pellet et al.showed that more than 80-90% of the microhematurias were rated as glomerular hematuria
Microscopic hematuria is thus predominantly associated with glomerular disease.
Identification of the type RBC in urine diagnose the etiology
Hyudo, et al. Nephron 1999;82:312-323

6Etiology of Hematuria
RENAL
Glomerular
Thin basement membrane
disease (benign familial hematuria)
IgA nephropathy
Alport’s syndrome
Other glomerulonephritides
Nonglomerular
Polycystic kidney disease
Medullary sponge kidney
Papillary necrosis
Pyelonephritis Sickle cell disease
Renal cell carcinoma
EXTRARENAL
Upper urinary tract
Nephrolithiasis
Ureteral cancer
Lower urinary tract
CystitisBladder cancer
Bladder stones
Prostate cancer
Schistosomiasis
otherVigorous exercise
Coagulation related
Factitious
False hematuria
Karnath, et al. Hospital Physician 2007;62: 20-26

7
Early detection of hematuria and differentiaton between glomerular and non glomerular type.
Essential for determination of correct line of investigation and management
Avoid unnecessary invasive diagnostic procedures such as cystoscopy and radiologicalinvestigations.
Dinda, Indian J Nephrol 2001;11: 37-38

8Glomerular vs Non Glomerular
GlomerularNon Glomerular
Evaluation of Urine RBC morphology

Glomerular vs Non Glomerular
1.Glomerular erythrocytes are smaller than
nonglomerular erythrocytes
2.The smaller glomerular erythrocytes vary greatly
in both shape and size whereas nonglomerular
erythrocytes are uniform in size and shape.
3.Glomerular erythrocytes usually have lost a large
amount of their hemoglobin pigment and are pale.
4.Erythrophagocytes and RBC cast commonly
accompany glomerular hematuria.
Smith dan Fairley. Semin Nephrol 2005. 25:127-135

Glomerular vs Non Glomerular
Glomerular Non Glomerular
Non Glomerular HematuriaGlomerular Hematuria

Glomerular
ErythrophaghocyteRBC cast
Glomerular bleeding
Glomerular

Glomerular Hematuria

13Glomerular hematuria Dysmorphic Erythrocyte

14Glomerular bleeding
Glomerular bleeding is associated with more than 80% dysmorphic RBC.
Kohler, et al. Kidney International, Vol. 40 (1991), pp. 115—120
No clear cut definition of dysmorphic erythrocyte

15Dysmorphic vs Isomorphic RBC
• Variously shaped blebs or
projections at the cell
membrane. Classify as
acanthocytes, G1 cells, or
D cells based.
DysmorphicRBC
•Uniform and no more than two types
Isomorphic RBC
Kohler, et al. Kidney International, Vol. 40 (1991), pp. 115—120; Kidney International, Vol. 21(1982),
pp. 105—108; Letgen, et al. Pediatric Nephrology 1995: 9(4); 435–437|

16

17Dysmorphic vs Isomorphic

18Dysmorphic vs Isomorphic
Yu Chu Su. 2017. Scientific report 7:40521, 1-10

19Dysmorphic vs Isomorphic
The shapes of isomorphic RBCs can change in response to the
osmolarity of urine.
The isomorphic RBCs swell to spheres (Fig. 2B-07) in urine
with a low specific gravity, and they shrink to the shape of a
spiked disk (Fig. 2B-11 and B-12) or a spiked sphere (Fig. 2B-
13) in urine with a high specific gravity.
Yu Chu Su. 2017. Scientific report 7:40521, 1-10
Some “dysmorphic” cells could be easily and reversibly induced by
changes of osmolality, pH or coverslip (Kohler, et al, 1991)

20Achantocyturia
Sumber: Kohler, et al. Kidney International 1991: 40; pp. 115—120
One irreversible cell type, a ringform with vesicle-shaped
protrusions (acanthocyte), was found almost in glomerular disease
and was not induced by journey of the renal tubules (changes in
osmolality, pH or the investigation procedur.

21
Achanthocyte in urine ≥ 5% (specificity 98%, sensitivity 52%) was found almost in glomerular disease.
Kohler, et al. Kidney International, Vol. 40 (1991), pp. 115—120
Glomerular Bleeding

22PROBLEMS
Dysmorphic RBC
Isomorphic RBC
Classification and Interpretation
sometimes not easy
Underinterpretation of dysmorphic
RBC

Dysmorphic erythrocyte
23
Phase-contrast microscopy is considered the gold
standard for the differentiation between
glomerular and non-glomerular hematuria.
Limited availability

Supra vital stain using brightfield
microscope
Cutoff ≥20% dysmorphic erythrocyte for diagnosing glmerular heusing supravital stain and brightfield microscope specificity
82%, sensitivity 100%.
Pemeriksaan yang sederhana ini memiliki efisiensi yang setara
dengan mikroskop fase kontras.
Prinsip pengecatan supravital dilakukan dengan menggunakan
cat kristal violet 1%, safranin 0,5% dan normal saline, selanjutnya
cat akan dicampurkan dengan sedimen urin hasil sentrifugasi
dengan perbandingan 1:1

25PROBLEMS
Laboratory interpretation
Nephrologist
- Nephrologist found a higher number of Renal tubular epithelial (RTE), granular
cast, hyaline cast and RTE cast compared to medical technologist.
- Nephrologist reported the presence of acanthocytes in 7 samples that were
not detected by laboratory personels.
Discrepancies
Tsai, et al (2005). Am. J. Kidney Dis. 46: 820-829

26
Urinalysis report usually
lack a description of
dysmorphic RBCs,
Tools that can give information related with the dysmorphic RBC
Urine Flowcytometry

PROBLEMS
The drawbacks of microscopic urinalysis high inter-observer variability, low sensitivity, and time consuming
Automation of Urine analyzer

Principle of Urine Flowcytometry

Classify by 3 level information
Forward scatter light (Fsc)
Side scatter light (Ssc)
Fluorescence light (Fl)
Describe particle size
Describe complexity of particle
Describe material genetic of particle
Classifying
type of
particle


31

32Principle of UF in detecting dysmorphic RBC
• The majority size of the RBC population
RBC-P70Fsc
• The width of the RBC size distribution
RBC-Fsc-DW
RBC Information from UF

33Principle of UF in detecting dysmorphic RBC
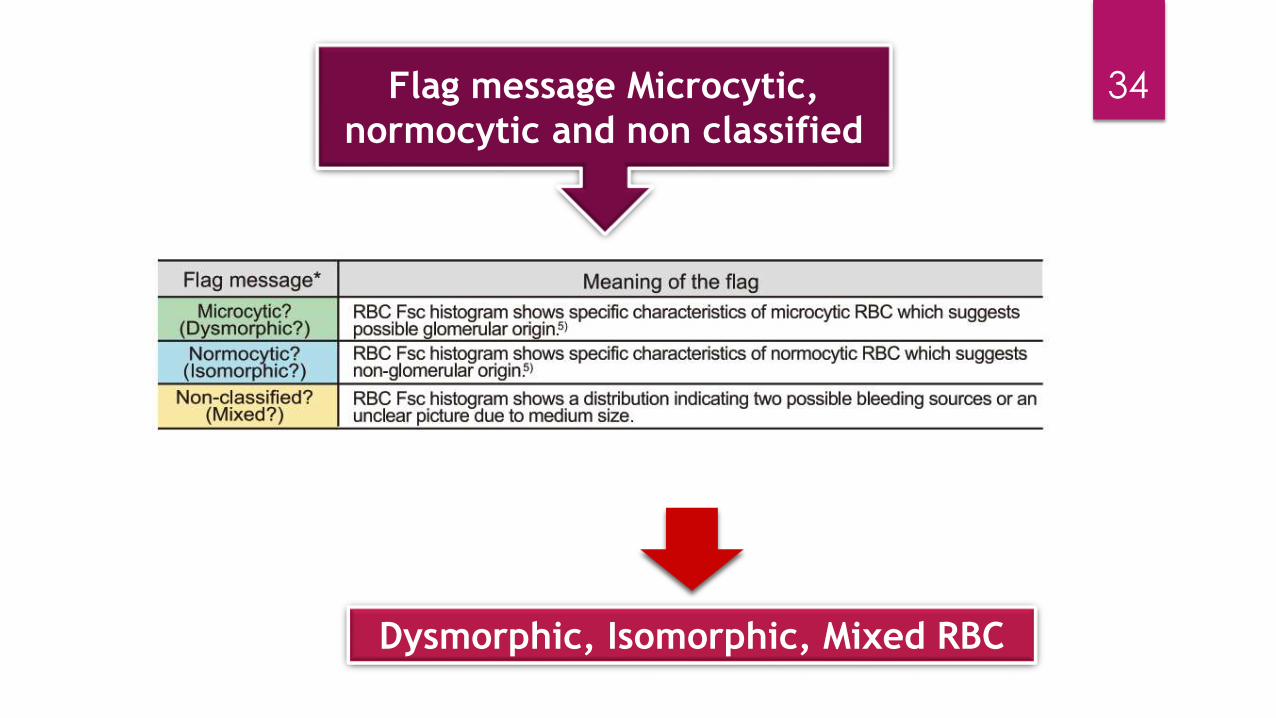
34Flag message Microcytic,
normocytic and non classified
Dysmorphic, Isomorphic, Mixed RBC

Principle of UF in detecting dysmorphic RBC35

RBC Morphology from UF
36

37Glomerular Hematuria

38Non Glomerular Hematuria

Study of Dysmorphic RBC using Urine
Flowcytometry
39
Shayanfar, et al 2013
UF 100i had sensitivity 76%, specificity 93%, 92% NPV, 78% PPV in detecting RBC
Some sample with dysmorphic RBC flag normal RBC but small manual reviewed

40Study of Dysmorphic RBC using Urine
Flowcytometry
Hyodo, et al 1999
Sensitivity and specificity of UF100 in detecting glomerular hematuria were 90,3% and 92,5% respectively (Study 1)
Sensitivity and specificity of UF100 in detecting glomerular for hematuria were 100% and 86,6% respectively (Study 2)
Hyodo, et al. Nephron 1999;82:312-323

41Study of Dysmorphic RBC using Urine
Flowcytometry
Yu, Chu Su, et al. 2017
Modified urinalysis protocol with an increased
relative centrifuge force and concentration factor
↑recovery ratio of dysmorphic erythrocyte 34,7%
42% p=0,001
Correlation between dysmorphic RBC counts by the modified urinary protocol and Sysmex UF-1000i urinary flow cytometer (r ≥ 0.898, P < 0.001).

42Dysmorphic RBC Detection
Chu Su, et al (2016) proposed modified urinalysis protocol increases the
detection rate of dysmorphic red blood cells:
a. Relative Centrifuge Force (RCF) with higher recovery ratios for formed
elements in urine sediment is preferable to increase the cell count
accuracy.
The Recovery ratio of RBCs from the sediment suspension at an RCF of
500×g (49.8%) was significantly higher (P <0.001) than that at an RCF
of 400x g (44.2%).
b. Use optimal RCF setting (500xg) for the recovery of dysmorphic RBCs
in cases of haematuria. The increased concentration factor (20-fold)
for urine sedimen.
c. Apply Stenheimer malbin stainning.
Yu Chu Su. 2017. Scientific report 7:40521, 1-10
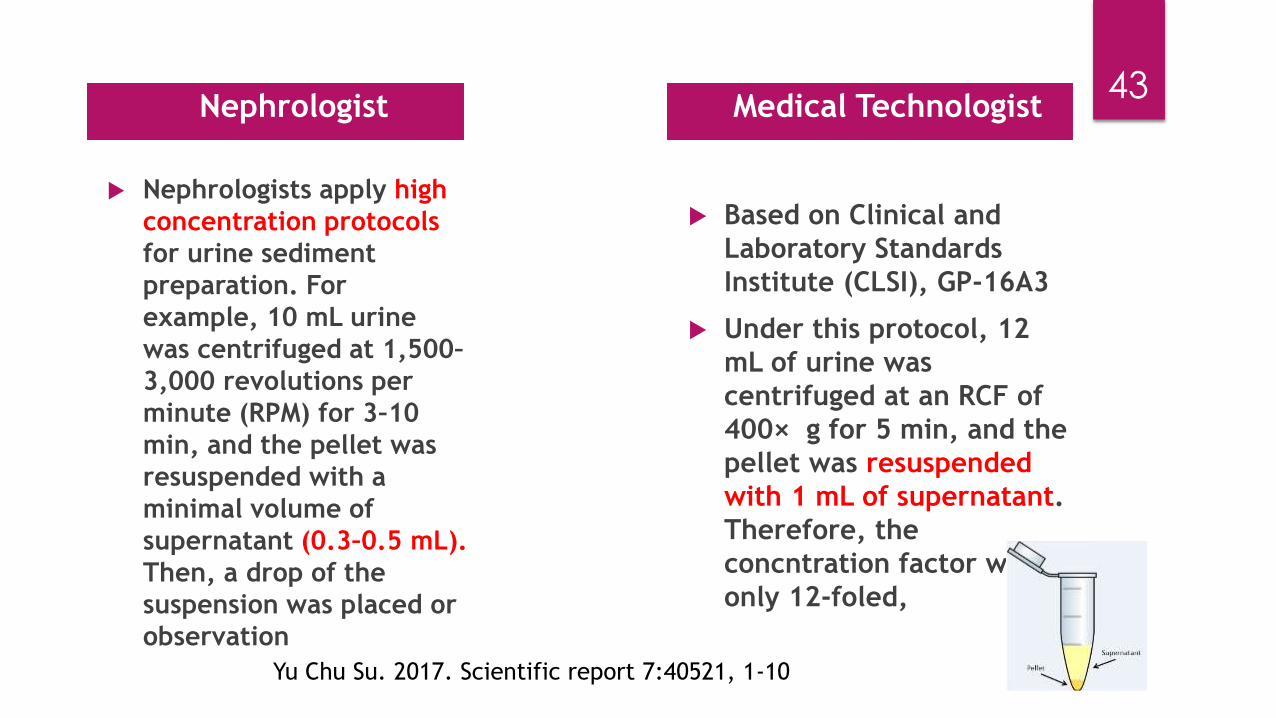
43 Nephrologist
Nephrologists apply high
concentration protocols
for urine sediment
preparation. For
example, 10 mL urine
was centrifuged at 1,500–
3,000 revolutions per
minute (RPM) for 3–10
min, and the pellet was
resuspended with a
minimal volume of
supernatant (0.3–0.5 mL).
Then, a drop of the
suspension was placed or
observation
Medical Technologist
Based on Clinical and
Laboratory Standards
Institute (CLSI), GP-16A3
Under this protocol, 12
mL of urine was
centrifuged at an RCF of
400× g for 5 min, and the
pellet was resuspended
with 1 mL of supernatant.
Therefore, the
concntration factor was
only 12-foled,
Yu Chu Su. 2017. Scientific report 7:40521, 1-10

1. Differentiating glomerular and non glomerular hematuria is an
important steps in urinalysis.
2. Urine flowcytometry can help us in differentiating glomerular
and non glomerular hematuria based on RBC P70 FSc that give
information related with the majority size of RBC population
and RBC FSc-DW that give information related with the width of
RBC variation.
3. Manual review is needed to confirm the Dysmorphic RBC.
Conclusions
4
4
