screening ct angiography of the aorta, visceral branch vessels,...
TRANSCRIPT

J A C C : C A R D I O V A S C U L A R I M A G I N G VO L . - , N O . - , 2 0 1 6
ª 2 0 1 6 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
P U B L I S H E D B Y E L S E V I E R
I S S N 1 9 3 6 - 8 7 8 X / $ 3 6 . 0 0
h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j c m g . 2 0 1 6 . 0 4 . 0 1 0
Screening CT Angiography of the Aorta,Visceral Branch Vessels, and PelvicArteries in Fibromuscular Dysplasia
Michael A. Bolen, MD,a,b Ellen Brinza, BS,b Rahul D. Renapurkar, MD,a Esther S.H. Kim, MD,b Heather L. Gornik, MDbABSTRACT
Fro
Oh
of
thi
Ma
OBJECTIVES This study sought to evaluate the diagnostic yield of a dedicated computed tomography angiography
(CTA) protocol of the chest, abdomen, and pelvis in patients with fibromuscular dysplasia (FMD).
BACKGROUND FMD is an uncommon vascular disease that may result in stenosis, dissection, or aneurysm of
nearly all arterial distributions, typically affecting medium-sized arteries. Findings from the United States Registry for
Fibromuscular Dysplasia have suggested the potential need to perform screening imaging of the aorta and medium
branch vessels.
METHODS A total of 113 consecutive patients enrolled in our institutional FMD registry who received a tailored CTA
protocol at our institution between March 2013 and June 2015 were included in this study. Arterial phase contrast-
enhanced images were obtained on a dual-source scanner using high pitch and electrocardiogram trigger. Images were
analyzed by 2 readers.
RESULTS Abnormalities including beading, aneurysm, dissection, and stenosis/occlusion were noted in aortic, renal,
mesenteric, and iliac distributions. The most commonly affected vessels were the renal arteries (n ¼ 76 [67%]), followed
by the lower extremity/iliac arteries (n ¼ 37 [32%]). Aortic abnormalities were less frequently encountered (n ¼ 3 [3%]),
including 1 case with mild dilation (4.2 cm) of the ascending aorta and 2 cases of dissection involving the descending
aorta, 1 with mild dilation (4.4 cm). Incremental findings beyond those known at patient intake were commonly noted,
including new areas of arterial beading (n ¼ 55 [49%]), new aneurysms (n ¼ 21 [19%]), and new dissections (n ¼ 3 [3%]).
Reformatted images were crucial, affecting final assessment in 56% of cases evaluated by reader 1 and 36% evaluated by
reader 2.
CONCLUSIONS Screening chest, abdomen, and pelvis CTA in patients with FMD showed substantial and incremental
diagnostic yield. Reformatted images should routinely be included in imaging analysis. Abnormalities in the aorta were
not common, so screening of the thoracic aorta may not be indicated. (J Am Coll Cardiol Img 2016;-:-–-) © 2016 by
the American College of Cardiology Foundation.
F ibromuscular dysplasia (FMD) is a vascular dis-ease that may result in stenosis, dissection, oraneurysm of nearly all arterial distributions,
with the renal and extracranial carotid and vertebralarteries most commonly affected (1). Medium-sizedarteries are typically affected, and the disease ofteninvolves multiple vascular territories within an
m the aImaging Institute, Cleveland Clinic, Cleveland, Ohio; and the bHear
io. Dr. Kim is a paid consultant for Philips Ultrasound. Dr. Gornik is a mem
America, a nonprofit organization. All other authors have reported that th
s paper to disclose.
nuscript received January 22, 2016; revised manuscript received April 5,
individual patient. The etiology of this disease is un-clear. It is believed to be neither an inflammatory noran atherosclerotic process, but genetic and environ-mental risk factors may play a role in the condition(2). The clinical presentation is driven by the vascularbeds affected. Renal involvement usually presentswith hypertension, and carotid artery involvement
t and Vascular Institute, Cleveland Clinic, Cleveland,
ber of the medical advisory board of the FMD Society
ey have no relationships relevant to the contents of
2016, accepted April 14, 2016.

ABBR EV I A T I ON S
AND ACRONYMS
CT = computed tomography
CTA = computed tomography
angiography
DSA = digital subtraction
angiography
FMD = fibromuscular dysplasia
MRA = magnetic resonance
angiography
Bolen et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 6
CTA Screening for Vascular Abnormalities in FMD - 2 0 1 6 :- –-
2
is often heralded by pulsatile tinnitus, head-ache (generally the migraine type), and tran-sient ischemic attack or stroke (often due tocarotid or vertebral artery dissection). FMDmay also be discovered incidentally in anasymptomatic patient who is imaged foranother clinical indication.
Histologically, FMD is classified dependingon which layer of the vessel wall is predom-inantly involved. Medial fibroplasia is themost common subtype, seen in >80% of pa-
TABLE 1 X-Ray Parameters
Lateral Width,* cm Tube Potential, kV Tube Current, mA
<32 100 260
32–38 120 220
39–45 120 300
>45 NA NA
*Skin-to-skin measurement at diaphragm from anteroposterior scout.
NA ¼ not applicable.
tients (2). Angiographically, the appearance of medialfibroplasia resembles a string of beads, with beadedareas larger in caliber than the unaffected portion ofthe artery (3). Less common subtypes of FMD includeintimal fibroplasia, which is a more focal processcharacterized by smooth or bandlike areas of nar-rowing, and perimedial and adventitial fibroplasia(4). A recent American Heart Association scientificstatement proposed a simplified angiography-basedFMD classification, with FMD lesions characterizedas either multifocal (previously primarily medialfibroplasia) or focal (2).
To further the understanding of the clinical char-acteristics, epidemiology, management, and out-comes of patients with FMD, a multicenter registrywas instituted in 2008 (1), and initial data from thefirst 447 patients entered into the United StatesRegistry for Fibromuscular Dysplasia were reported in2012 (1). Notable findings in this group includedaneurysm in 17% of patients (with 20% of these casesinvolving the aorta) and dissection in 20%. Further-more, because the entire aortic and visceral branchcirculation was not imaged in all cases, the preva-lence of aneurysms may have been underestimated.Based on these initial findings, in 2013 our institutionbegan imaging all patients with a diagnosis of FMD toscreen for aortic and/or visceral branch vessel andpelvic arterial abnormalities (5). A specializedcomputed tomography angiography (CTA) protocol isused for this one-time screening of patients who hadnot previously undergone comprehensive assessmentof the aorta or visceral and pelvic branch vessels. Forthis study, we reviewed the first 113 patients imagedwith this protocol to evaluate the imaging techniqueand analysis, categorize pathological findings, andassess for possible effects on clinical management.
METHODS
This retrospective study was approved by the localinstitutional review board, with a waiver of individ-ual consent. From March 2013 to June 2015, a total of360 patients with an established diagnosis of FMD
who were enrolled in our institutional FMD registrywere seen for new patient or follow-up visits. Amongthese patients, a total of 113 consecutive patients(31%) who had not previously undergone tomo-graphic imaging of the aorta or visceral and pelvicbranch vessels underwent the specialized CTA pro-tocol and were included in this study.
IMAGING TECHNIQUE. Imaging was performed on acommercially available second-generation dual-source computed tomography (CT) scanner (SiemensSomatom Flash, Siemens Healthcare, Erlangen,Germany). The full scan range extended from thethoracic inlet to the ischial tuberosities. High-pitch(pitch ¼ 3.2) imaging was performed during the arte-rial phase. Patient electrocardiogram was used totrigger initiation of table motion as well as detectorrotation, timed for table positioning at the level of theaortic root and proximal ascending aorta during thediastolic phase. The average estimated dose-lengthproduct was 273.1 � 91 mGy$cm, corresponding toan effective dose of approximately 4 mSv. Contrast(111 � 12 ml) (Omnipaque 350, GE Healthcare, Chicago,Illinois) was administered intravenously according topatient weight as determined by manufacturer-provided software (P3t Cardiac version 1.0, MEDRADInc., Pittsburgh, Pennsylvania), after a test bolus scan(20 ml) was obtained at the midabdominal level toassess time to peak enhancement. Techniques forradiation dose minimization included lower tube po-tential and tube current settings based on patient size(Table 1). In all cases, 18g intravenous access was ob-tained. Images were reconstructed to a slice thicknessof 1 mm (increment ¼ 1 mm) and 3 mm (increment ¼ 3mm), with medium smooth kernel (B31f).
IMAGE ANALYSIS. All cases were analyzed on adedicated workstation using manufacturer’s software(Agfa Healthcare, Mortsel Belgium) by a cardiovas-cular radiologist with fellowship training and 7 years’CT reading experience (M.B.). Aortic size wasassessed with the use of multiplanar reformattedimages oriented orthogonal to the aorta centerline.Images were analyzed for the presence of beading,aneurysm, or dissection, first with axial thin-slice

TABLE 2 Baseline Clinical Characteristics
Value
Age, yrs 55.6 � 10.1(range 29–76)
Female 112/113 (99)
Body mass index, kg/m2 25.9 � 6.3
Past medical history and/or presenting symptom at diagnosis
Symptom
Headache* 86/112 (77)
Pulsatile tinnitus† 57/103 (55)
Hypertension* 60/111 (54)
Dizziness† 45/96 (47)
Neck pain† 43/94 (46)
Dissection 46/109 (42)
Aneurysm 18/110 (16)
Flank or abdominal pain† 16/98 (16)
Transient ischemic attack* 16/109 (15)
Stroke* 13/111 (12)
Horner syndrome* 11/107 (10)
Myocardial infarction (any cause, includingcoronary artery dissection)*
11/111 (10)
Post-prandial abdominal pain† 9/99 (9)
Arm or leg claudication* 9/109 (8)
Amaurosis fugax* 2/110 (2)
Renal infarction* 1/76 (1)
Renal insufficiency or failure* 1/77 (1)
Mesenteric ischemia* 1/109 (1)
Additional risk factors
Hyperlipidemia* 44/77 (57)
Tobacco smoking history* 33/111 (30)
Physical examination findings
Carotid bruit 48/110 (44)
Femoral bruit 18/74 (24)
Epigastric (abdominal) bruit 17/107 (16)
Vascular bed involvement‡
Extracranial carotid 98/107 (92)
Coronary 13/19 (68)
Renal 47/73 (64)
Lower extremity 9/15 (60)
Vertebral§ 36/79 (46)
Upper extremity 2/5 (40)
Mesenteric 10/48 (21)
Intracranialk 14/95 (15)
Aorta 2/14 (14)
Type of FMD
Multifocal 108/113 (96)
Focal 2/113 (2)
Multifocal plus focal 2/113 (2)
Could not be determined 1/113 (1)
Values are mean � SD or n/N (%) unless otherwise indicated. *Past history ofcomorbidity or clinical sign/symptom, or observed during presentation at time ofFMD diagnosis. †Presenting sign or symptom at time of FMD diagnosis. ‡Includesonly patients with imaging performed before study computed tomography angi-ography. All vascular beds were not imaged in all patients. Thus, denominatorsrepresent the total number of patients for whom imaging data were available foranalysis. §Excludes patients with only limited vertebral artery assessment by ca-rotid duplex examination or inadequate imaging of the vertebral arteries to allowfor conclusive assessment for FMD. kIntracranial involvement including cerebralaneurysms or dissections.
FMD ¼ fibromuscular dysplasia.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 6 Bolen et al.- 2 0 1 6 :- –- CTA Screening for Vascular Abnormalities in FMD
3
images, then with coronal and sagittal reformattedimages in both thin slice (1 mm, 1-mm increment) andmaximum intensity projection (8 mm, 1-mm incre-ment). The investigators noted whether recon-structed images changed their initial interpretationand led to new findings (e.g., an aneurysm or newregion of beading) or increased the reader’s confi-dence in the finding (i.e., changed assessment frompossible to convincing beading). A second reader withcardiovascular imaging fellowship training and 4years’ CT experience (R.R.) analyzed 25 randomlyselected cases to assess inter-reader variability.
Aneurysm was diagnosed when the arterial diam-eter measured $150% the diameter of the adjacentnormal artery. FMD (multifocal, string-of-beads type)was diagnosed when characteristic sequential areasof dilation greater in dimension than the adjacentnormal vessel and separated by areas of narrowingwere identified; these areas were graded as possible,convincing, or absent. Segments of focal concentricstenosis were also diagnosed as FMD (focal type).Dissection was diagnosed when the contrast-filledlumen was separated into true and false compo-nents by the intimal flap.
CLINICAL DATA COLLECTION. All patients includedin this retrospective imaging study had been seen inthe FMD clinic at our institution and had previouslyconsented and been enrolled in the United StatesRegistry for Fibromuscular Dysplasia (1). Informationabout past medical history, presenting signs andsymptoms, and physical examination findings wascollected at the time of patients’ enrollment into theregistry and was extracted from the local registrydatabase for this study. Regarding vascular bedinvolvement, all previous imaging studies performedbefore the time of the study CTA were included foranalysis, including data captured at baseline andduring previous follow-up visits at our center. Heartrate was obtained from the office visit closest to thedate of the CTA, and all incremental findings from theimaging study were reported separately.
RESULTS
Baseline characteristics at the time of imaging aresummarized in Table 2. Of the 113 patients included inthe study, 112 (99%) were women, with a mean age of55.6 � 10.1 years (range 29 to 76 years) at the time ofthe imaging study. Common signs and symptomsincluded headache (77%), hypertension (54%), pul-satile tinnitus (55%), dizziness (47%), and neck pain(46%). Multifocal FMD was by far the most commontype of FMD (96% of patients). A history of dissectionwas noted in 42% of patients, and 16% had a known

TABLE 3 Distributio
Tomography Angiogr
VascularTerritory
Thoracic/abdominal ao
Renal arteries
Right renal
Left renal
Bilateral
Splenic artery
Celiac artery
Superior mesenteric art
Lower extremity artery
Right common iliac
Left common iliac
Right external iliac
Left external iliac
Right internal iliac
Left internal iliac
Values are n (%).
Bolen et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 6
CTA Screening for Vascular Abnormalities in FMD - 2 0 1 6 :- –-
4
aneurysm. Among patients who had previously un-dergone renal imaging, FMD was present in 64%.Carotid involvement was found in 92% of patientswho underwent carotid artery imaging, and vertebralartery involvement was noted in 46% of patients. Themakeup of this patient cohort may have been skewedby the imaging protocol. Performing screening thor-acoabdominal aorta and branch vessel CTA in patientswithout prior tomographic imaging of this region mayhave led to a larger fraction of patients with cere-brovascular involvement by FMD. Conversely, pa-tients with renal or other thoracoabdominal aorticbranch vessel involvement at the time of diagnosismore likely would have undergone prior imaging ofthis area and therefore would not have undergone thescreening imaging evaluated in this study. The rela-tively high frequency of upper extremity, lower ex-tremity, and coronary artery involvement on imagingstudies likely reflects the small number of patientswho underwent dedicated imaging studies of thesevascular territories, generally for investigation ofsigns and symptoms, increasing the likelihood ofvascular bed involvement.
FREQUENCY AND DISTRIBUTION OF VASCULAR
ABNORMALITIES. Abnormalities including beading,aneurysm, dissection, and stenosis/occlusion werenoted in aortic, renal, mesenteric, iliac, and coronarydistributions (Table 3). The most commonly affected
n of Vascular Abnormalities Detected by Protocol Computed
aphy of Aorta and Visceral/Pelvic Branches
PatientsAffected Abnormalities
rta 5 (4) 2 cases >4 cm, dissection 2(both affecting descending aorta)
76 (67) Aneurysm 2, beading 67, beading plus aneurysm6, focal 1
67 (59)
57 (50)
48 (42)
16 (14) Aneurysm 8, beading 5, beading plus aneurysm 3
15 (13) Aneurysm 3, beading 9, beading plus ostialstenosis 2, ostial occlusion 1
ery 10 (9) Beading 6, aneurysm plus dissection 1, beadingplus stenosis 1, beading plus dissection 1,aneurysm 1
37 (32) Beading 29, dissection 2, beading plus dissection2, occlusion 1, beading plus aneurysm 2,diffuse ectasia 1
1 (1)
2 (2)
21 (18)
28 (24)
5 (4)
8 (7)
vessels were the renal arteries (n ¼ 76 [67%]), fol-lowed by the lower extremity/iliac arteries (n ¼ 37[32%]). Aneurysms of the aortic branch vessels rangedin size from 5 to 14 mm. Aortic abnormalities wereless frequently encountered (n ¼ 3 [3%]), including 1case with mild dilation (4.2 cm) of the ascending aortaand 2 cases of dissection involving the descendingaorta, with mild dilation (4.4 cm) in 1 of these cases.Aortic valve morphology suggested a trileaflet valvein all but 1 case, which appeared bicuspid (confirmedat the time of transthoracic echocardiography). Ex-amples of the various vascular abnormalities areshown in Figures 1 to 4.
Incremental findings yielded by CTA imaging werecommonly noted, including beading (multifocal FMD)(n ¼ 55 [49%]) or focal stenosis (focal FMD) (n ¼ 1[1%]) in a new vascular territory, and new aneurysms(n ¼ 21 [19%]) or new dissections (n ¼ 3 [3%]).
EFFECT OF RECONSTRUCTIONS. The use of refor-matted images affected final assessment in 63 of the113 cases (56%) evaluated by reader 1 and 9 of the 25cases (36%) evaluated by reader 2.
The inter-reader agreement (Table 4) was reason-ably good, with the readers showing exact agreementin grading of beading (not present, possible, orconvincing) in 80% to 88% of cases. When the“possible” and “convincing” groups were classified aspositive, the readers showed 84% to 96% agreementin diagnosis. All cases of dissection showed concor-dant analysis, and only 3 subcentimeter aneurysmswere discrepant, with the remaining 22 aneurysmsconcordant (88% agreement). The renal arteriesshowed the lowest exact agreement (80%) betweenreaders, although the agreement was excellent (96%)when the scores of “possible” and “convincing” werecombined.
DISCUSSION
A high prevalence of aneurysms has been reported inpatients with FMD (1). At our institution, we use CTAto assess a wide expanse of vascular territory in pa-tients with documented FMD, and this study is thefirst to our knowledge to report the outcomes of thisscreening approach. A significant number ofabnormal vascular findings were made, many of thesenot known at the time of patient intake, although asurprisingly low number of aortic abnormalities wereidentified.
IMAGING TECHNIQUES TO SCREEN FOR VASCULAR
ABNORMALITIES IN PATIENTS WITH FMD. Invasivetechniques such as digital subtraction angiography(DSA) would likely improve the detection of subtlevascular abnormalities in this patient population.

FIGURE 1 Renal Artery Images From 3 Patients With FMD
Possible beading consistent with multifocal FMD (A, pink arrows) demonstrated on coronal maximum intensity projection image of the right renal artery. Convincing
FMD (pink arrows) demonstrated on multiplanar reformatted (B) and volume-rendered images (C) of the right renal artery in 2 different patients. Aneurysms also noted
in the right renal artery (B, green arrow) and left renal artery (C, green arrow). FMD ¼ fibromuscular dysplasia.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 6 Bolen et al.- 2 0 1 6 :- –- CTA Screening for Vascular Abnormalities in FMD
5
A review of DSA in potential renal donors demon-strated an FMD incidence of 3.8% (6) versus 2.6%with CTA (7), suggesting that DSA may be an attrac-tive option when there is high suspicion that inter-vention will be required. However, the risk, time, andcost associated with this approach make it a lessappealing option for the assessment of large vascularterritories. Some investigators have reported robustperformance with CTA versus DSA in the assessment
FIGURE 2 Iliac Artery and Mesenteric Artery Involvement in Patien
Volume-rendered image from a patient with convincing findings of FMD
intensity projection image from a patient with occluded celiac trunk and
FMD ¼ fibromuscular dysplasia.
of FMD (8) and renal artery stenosis, even withslightly older-generation CT scanners (9,10). Alter-natively, ultrasonography with color flow Doppler canbe used to identify areas of turbulence and somecases of abnormal arterial morphology. However,Doppler ultrasonography is strongly dependent onuser skill and satisfactory sonographic windows,which can be challenging in the assessment of renaland visceral branch arteries (2).
ts With FMD
in both external iliac arteries (A, green arrow). Sagittal maximum
focal stenosis of the superior mesenteric artery (B, pink arrow).

FIGURE 3 Dissections in Patients With FMD
Axial images from a patient with dissection of the common iliac arteries (A and B, pink arrows). Axial image from a patient with descending aortic dissection
(C, pink arrow). FMD ¼ fibromuscular dysplasia.
Bolen et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 6
CTA Screening for Vascular Abnormalities in FMD - 2 0 1 6 :- –-
6
Magnetic resonance angiography (MRA) is anotherpossible technique for the detection of vascular ab-normalities across multiple vascular territories. Thismodality offers the additional benefit of increasedfunctional (e.g., flow) measurements, all without theneed for ionizing radiation. However, MRA is moretime intensive than CTA, and its spatial resolution isslightly inferior to that of CTA, which might limit itsability to detect abnormalities. In studies of patientswith spontaneous coronary artery dissection, MRA
FIGURE 4 Vessel Dilation in Patients With FMD
Axial maximum intensity projection image of a patient with a 9-mm spl
ascending aorta (B, green arrow). FMD ¼ fibromuscular dysplasia.
detected a 25% prevalence of extracoronary abnor-malities (11), whereas CTA detected a 69% prevalence(12). Additionally, magnetic resonance imaging is noteffective for evaluating calcium deposition and maylead to difficulties in differentiating between athero-sclerosis and FMD or in evaluating mixed processes(e.g., atherosclerosis plus FMD).FREQUENCY OF ABNORMALITIES. Because this wasthe first study to evaluate the diagnostic yield ofscreening aortic and branch vessel angiography in
enic artery aneurysm (A, green arrow) and mildly dilated (4.2 cm)
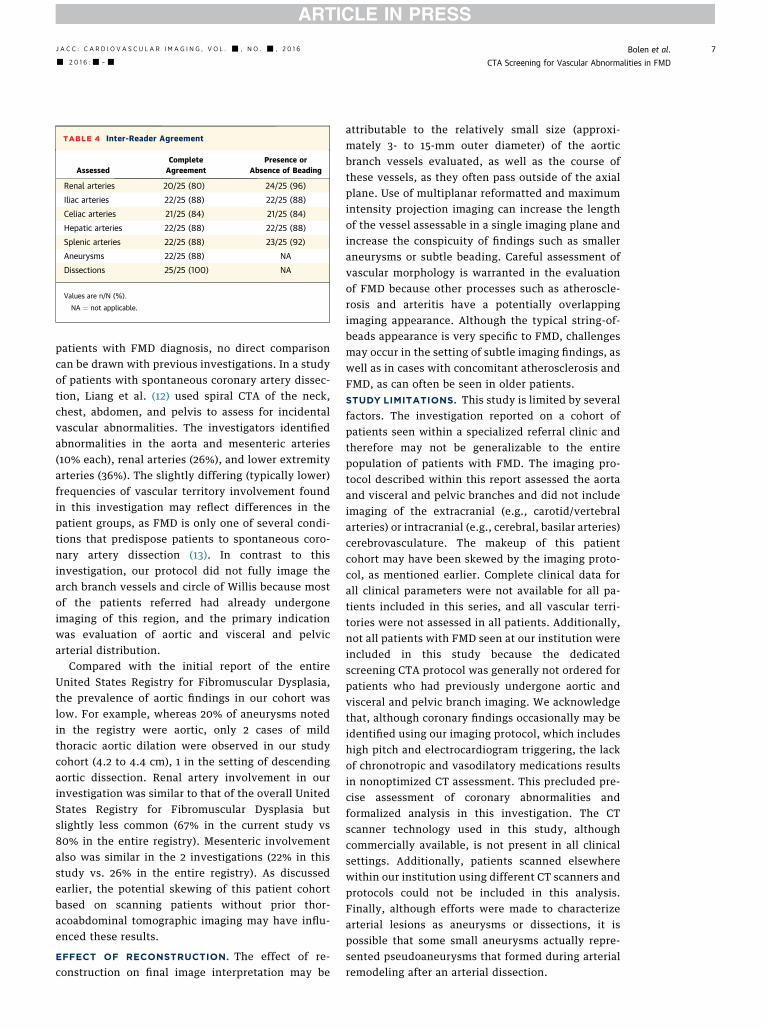
TABLE 4 Inter-Reader Agreement
AssessedCompleteAgreement
Presence orAbsence of Beading
Renal arteries 20/25 (80) 24/25 (96)
Iliac arteries 22/25 (88) 22/25 (88)
Celiac arteries 21/25 (84) 21/25 (84)
Hepatic arteries 22/25 (88) 22/25 (88)
Splenic arteries 22/25 (88) 23/25 (92)
Aneurysms 22/25 (88) NA
Dissections 25/25 (100) NA
Values are n/N (%).
NA ¼ not applicable.
J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 6 Bolen et al.- 2 0 1 6 :- –- CTA Screening for Vascular Abnormalities in FMD
7
patients with FMD diagnosis, no direct comparisoncan be drawn with previous investigations. In a studyof patients with spontaneous coronary artery dissec-tion, Liang et al. (12) used spiral CTA of the neck,chest, abdomen, and pelvis to assess for incidentalvascular abnormalities. The investigators identifiedabnormalities in the aorta and mesenteric arteries(10% each), renal arteries (26%), and lower extremityarteries (36%). The slightly differing (typically lower)frequencies of vascular territory involvement foundin this investigation may reflect differences in thepatient groups, as FMD is only one of several condi-tions that predispose patients to spontaneous coro-nary artery dissection (13). In contrast to thisinvestigation, our protocol did not fully image thearch branch vessels and circle of Willis because mostof the patients referred had already undergoneimaging of this region, and the primary indicationwas evaluation of aortic and visceral and pelvicarterial distribution.
Compared with the initial report of the entireUnited States Registry for Fibromuscular Dysplasia,the prevalence of aortic findings in our cohort waslow. For example, whereas 20% of aneurysms notedin the registry were aortic, only 2 cases of mildthoracic aortic dilation were observed in our studycohort (4.2 to 4.4 cm), 1 in the setting of descendingaortic dissection. Renal artery involvement in ourinvestigation was similar to that of the overall UnitedStates Registry for Fibromuscular Dysplasia butslightly less common (67% in the current study vs80% in the entire registry). Mesenteric involvementalso was similar in the 2 investigations (22% in thisstudy vs. 26% in the entire registry). As discussedearlier, the potential skewing of this patient cohortbased on scanning patients without prior thor-acoabdominal tomographic imaging may have influ-enced these results.
EFFECT OF RECONSTRUCTION. The effect of re-construction on final image interpretation may be
attributable to the relatively small size (approxi-mately 3- to 15-mm outer diameter) of the aorticbranch vessels evaluated, as well as the course ofthese vessels, as they often pass outside of the axialplane. Use of multiplanar reformatted and maximumintensity projection imaging can increase the lengthof the vessel assessable in a single imaging plane andincrease the conspicuity of findings such as smalleraneurysms or subtle beading. Careful assessment ofvascular morphology is warranted in the evaluationof FMD because other processes such as atheroscle-rosis and arteritis have a potentially overlappingimaging appearance. Although the typical string-of-beads appearance is very specific to FMD, challengesmay occur in the setting of subtle imaging findings, aswell as in cases with concomitant atherosclerosis andFMD, as can often be seen in older patients.STUDY LIMITATIONS. This study is limited by severalfactors. The investigation reported on a cohort ofpatients seen within a specialized referral clinic andtherefore may not be generalizable to the entirepopulation of patients with FMD. The imaging pro-tocol described within this report assessed the aortaand visceral and pelvic branches and did not includeimaging of the extracranial (e.g., carotid/vertebralarteries) or intracranial (e.g., cerebral, basilar arteries)cerebrovasculature. The makeup of this patientcohort may have been skewed by the imaging proto-col, as mentioned earlier. Complete clinical data forall clinical parameters were not available for all pa-tients included in this series, and all vascular terri-tories were not assessed in all patients. Additionally,not all patients with FMD seen at our institution wereincluded in this study because the dedicatedscreening CTA protocol was generally not ordered forpatients who had previously undergone aortic andvisceral and pelvic branch imaging. We acknowledgethat, although coronary findings occasionally may beidentified using our imaging protocol, which includeshigh pitch and electrocardiogram triggering, the lackof chronotropic and vasodilatory medications resultsin nonoptimized CT assessment. This precluded pre-cise assessment of coronary abnormalities andformalized analysis in this investigation. The CTscanner technology used in this study, althoughcommercially available, is not present in all clinicalsettings. Additionally, patients scanned elsewherewithin our institution using different CT scanners andprotocols could not be included in this analysis.Finally, although efforts were made to characterizearterial lesions as aneurysms or dissections, it ispossible that some small aneurysms actually repre-sented pseudoaneurysms that formed during arterialremodeling after an arterial dissection.

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: FMD
is a diffuse arteriopathy that involves medium-sized
arteries in multiple vascular territories throughout the
body, most commonly the renal and cerebrovascular
arteries. A high prevalence of arterial aneurysm and
dissection has been previously demonstrated among
patients with FMD. Use of a specialized screening CTA
protocol of the chest, abdomen, and pelvis in a single-
center group of patients with FMD diagnosis provided
important incremental information about aortic
branch vessels; however, aortic abnormalities were
uncommon in this group (3%). Reformatted images
had a significant effect on final interpretations.
TRANSLATIONAL OUTLOOK: Additional studies
are needed to validate the findings and determine
whether screening CTA can be limited to the abdomen
and pelvis in patients with a diagnosis of FMD.
Bolen et al. J A C C : C A R D I O V A S C U L A R I M A G I N G , V O L . - , N O . - , 2 0 1 6
CTA Screening for Vascular Abnormalities in FMD - 2 0 1 6 :- –-
8
CONCLUSIONS
Use of a specialized screening CTA imaging protocolof the aorta and medium branch vessels in patientswith FMD yielded useful incremental findings. Theoverall frequency of abnormalities observed waswithin the expected range for visceral branch andlower extremity arteries. Infrequent abnormalitiesin the thoracic aorta suggest that screening imagingin this patient population may be more appropri-ately limited to abdomen and pelvic aorta andbranch vessel CTA. Confidence in this finding maybe increased by correlating these results with find-ings from other centers. This screening CTA proto-col was performed with a reasonable estimatedradiation dose and contrast volume. Reformattedimage processing had a notable effect on imageanalysis.
ACKNOWLEDGMENTS The authors appreciate theeditorial contribution of Megan M. Griffiths and theCT scanning expertise of Stacie Kuzmiak.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Michael A. Bolen, Cardiovascular Imaging Laboratory,J1-4, Imaging Institute, Cleveland Clinic, 9500 Euclid
Avenue, Cleveland, Ohio 44195. E-mail: [email protected].
RE F E RENCE S
1. Olin JW, Froehlich J, Gu X, et al. The UnitedStates Registry for Fibromuscular Dysplasia: re-sults in the first 447 patients. Circulation 2012;125:3182–90.
2. Olin JW, Gornik HL, Bacharach JM, et al.,American Heart Association Council on PeripheralVascular Disease; American Heart AssociationCouncil on Clinical Cardiology; American HeartAssociation Council on Cardiopulmonary, CriticalCare, Perioperative and Resuscitation; AmericanHeart Association Council on Cardiovascular Dis-ease in the Young; American Heart AssociationCouncil on Cardiovascular Radiology and Inter-vention, American Heart Association Council onEpidemiology and Prevention; American HeartAssociation Council on Functional Genomics andTranslational Biology; American Heart Associa-tion Council for High Blood Pressure Research;American Heart Association Council on the Kidneyin Cardiovascular Disease; American Heart Asso-ciation Stroke Council. Fibromuscular dysplasia:state of the science and critical unansweredquestions: a scientific statement from the Amer-ican Heart Association. Circulation 2014;129:1048–78.
3. Slovut DP, Olin JW. Fibromuscular dysplasia.N Engl J Med 2004;350:1862–71.
4. Harrison EG Jr., McCormack LJ. Pathologicclassification of renal arterial disease in renovas-cular hypertension. Mayo Clin Proc 1972;46:161–7.
5. O’Connor SC, Gornik HL. Recent developmentsin the understanding and management of fibro-muscular dysplasia. J Am Heart Assoc 2014;3:e001249.
6. Cragg AH, Smith TP, Thompson BH, et al. Inci-dental fibromuscular dysplasia in potential renaldonors: long-term clinical follow-up. Radiology1989;172:145–7.
7. McKenzie GA, Oderich GS, Kawashima A,Misra S. Renal artery fibromuscular dysplasia in2640 renal donor subjects: a CT angiographyanalysis. J Vasc Interv Radiol 2013;24:1477–80.
8. Sabharwal R, Vladica P, Coleman P. Multi-detector spiral CT renal angiography in the diag-nosis of renal artery fibromuscular dysplasia. Eur JRadiol 2007;61:520–7.
9. Kim TS, Chung JW, Park JH, Kim SH, Yeon KM,Han MC. Renal artery evaluation: comparison of
spiral CT angiography to intra-arterial DSA. J VascInterv Radiol 1998;9:553–9.
10. Beregi JP, Elkohen M, Deklunder G, Artaud D,Coullet JM, Wattinne L. Helical CT angiographycompared with arteriography in the detection ofrenal artery stenosis. AJR Am J Roentgenol 1996;167:495–501.
11. Toggweiler S, Puck M, Thalhammer C, et al.Associated vascular lesions in patients with spon-taneous coronary artery dissection. Swiss MedWkly 2012;142:w13538.
12. Liang JJ, Prasad M, Tweet MS, et al.A novel application of CT angiography to detectextracoronary vascular abnormalities in patientswith spontaneous coronary artery dissection.J Cardiovasc Comput Tomogr 2014;8:189–97.
13. Yip A, Saw J. Spontaneous coronary arterydissection—a review. Cardiovasc Diagn Ther 2015;5:37–48.
KEY WORDS aneurysm, arterial dissection,computed tomography angiography,fibromuscular dysplasia