prior authorization review panel mco policy …...acupuncture for weight loss body plethysmography...
TRANSCRIPT
Prior Authorization Review Panel MCO Policy Submission
A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
Plan: Aetna Better Health Submission Date: 04/01/2019
Policy Number: 0039 Effective Date: Revision Date: 03/12/12018
Policy Name: Weight Reduction Medications and Programs
Type of Submission – Check all that apply: New Policy Revised Policy
Annual Review – No Revisions* *All revisions to the policy must be highlighted using track changes throughout the document. Please provide any clarifying information for the policy below:
CPB 0039 Weight Reduction Medications and Programs
Clinical content was last revised on 03/12/18 No additional non-clinical updates were made by Corporate since the last PARP submission.
Name of Authorized Individual (Please type or print):
Dr. Bernard Lewin, M.D.
Signature of Authorized Individual:
Proprietary
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 1 of 38
-->
(https://www.aetna.com/)
Weight Reduction Medicationsand Programs
Clinical Policy Bulletins Medical Clinical Policy Bulletins
Policy History
Last Re
view
03/12/2018
Effective: 02/14/2000
Next
Review: 01/10/2019
Review
Histor
y
Definitions
Additional Information
Number: 0039
Policy
*Please see amendment for Pennsylvania Medicaid at the end of this CPB.
Note: Many Aetna plan benefit descriptions specifically exclude services and
supplies for or related to treatment of obesity or for diet and weight control. Under
these plans, claims for weight reduction medications and for physician supervision
of weight reduction programs will be denied based on that exclusion. Please check
benefit plan descriptions for details.
Aetna considers the following medically necessary treatment of obesity when
criteria are met:
1. Weight reduction medications, and
2. Clinician supervision of weight reduction programs.
Weight Reduction Medications:
Note: Many Aetna benefit plans specifically exclude coverage of weight reduction
medications under the pharmacy benefit and/or under the health benefits plan. The
medical necessity criteria set forth below do not apply to health plans that
specifically exclude services and supplies for or related to treatment of obesity or
for diet or weight control. Under these plans, claims for weight loss drugs will be
03/28/2019
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 2 of 38
denied based on this exclusion. For members whose medical policies do not
exclude weight reduction medications or services and supplies for or related to
weight reduction programs, Aetna covers these drugs under the medical benefit,
not the pharmacy benefit. Please check benefit plan descriptions for details.
Weight reduction medications are considered medically necessary for members
who have failed to lose at least one pound per week after at least 6 months on a
weight loss regimen that includes a low-calorie diet, increased physical activity, and
behavioral therapy, and who meet either of the following selection criteria below:
I. Member has a body mass index * (BMI) greater than or equal to 30 kg/m²; or
II. Member has a BMI greater than or equal to 27 kg/m² with any of the
following obesity-related risk factors considered serious enough to warrant
pharmacotherapy:
A. Coronary heart disease
B. Dyslipidemia:
1. HDL cholesterol less than 35 mg/dL, or
2. LDL cholesterol greater than or equal to 160 mg/dL, or
3. Triglycerides greater than or equal to 400 mg/dL
C. Hypertension (systolic blood pressure [SBP] higher than 140 mm Hg or
diastolic blood pressure [DBP] higher than 90 mm Hg on more than one
occasion)
D. Obstructive sleep apnea
E. Type 2 diabetes mellitus.
Weight reduction medications are considered experimental and investigational
when these criteria are not met.
* Body Mass Index (BMI) = weight (kg) / [height (m)]²
Calculate Your Body Mass
Index (http://www.nhlbi.nih.gov/guidelines/obesity/BMI/bmicalc.htm)
03/28/2019
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 3 of 38
The following medications have been approved by the FDA for weight reduction:
▪ Benzphetamine [Didrex],
▪ Diethylpropion [Tenuate],
▪ Liraglutide [Saxenda],
▪ Lorcaserin [Belviq],
▪ Naltrexone and bupropion [Contrave]
▪ Orlistat [Xenical, Alli],
▪ Phendimetrazine [Bontril]
▪ Phentermine [Adipex-P], and
▪ Phentermine and topiramate [Qsymia].
For reauthorization criteria for weight reduction medications, see Aetna Pharmacy
CPB on Antiobesity Agents.
For Aetna’s clinical policy on surgical management of obesity,
see CPB 0157 - Obesity Surgery (../100_199/0157.html).
Clinician Supervision of Weight Reduction Programs:
Up to a combined limit of 26 individual or group visits by any recognized provider
per 12-month period are considered medically necessary for weight reduction
counseling in adults who are obese (as defined by BMI ≥ 30 kg/m2**). The number
of medically necessary visits for obese children are left to the discretion of the
member's physician.
** For a simple and rapid calculation of BMI, please click below and it will take you
to the Obesity Education Initiative:
BMI = weight (kg) ¸ [height (m)]
Calculate Your Body Mass Index
² (http://www.nhlbi.nih.gov/guidelines/obesity/BMI/bmicalc.htm)
The following services are considered medically necessary for the evaluation of
overweight or obese individuals:
03/28/2019
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 4 of 38
▪ Complete blood count
▪ Comprehensive history and physical examination
▪ Dexamethasone suppression test and 24-hour urinary free cortisol measures if
symptoms suggest Cushing's syndrome.
▪ Electrocardiogram (EKG) -- adult
▪ Glucose tolerance test (GTT)
▪ Hand x-ray for bone age -- child
▪ Lipid profile (total cholesterol, HDL-C, LDL-C, triglycerides)
▪ Metabolic and chemistry profile (serum chemistries, liver tests, uric acid) (SMA
20)
▪ Thyroid function tests (T3, T4, TSH)
▪ Urinalysis
Very Low-Calorie Diets (VLCD):
For obese members who have been prescribed a very low-calorie diet (VLCD) (less
than 799 Kcal/day) (e.g., Optifast, Medifast), the following services are considered
medically necessary for up to 16 weeks after initiation of the VLCD:
1. EKG after 50 lbs of weight loss; and
2. Lipid profile at the beginning and end of the VLCD program; and
3. Serum chemistries and liver function tests (SMA 20) weekly during the rapid
weight loss phase of the VLCD, then every 2 weeks thereafter up to 16 weeks.
Note: VLCDs extending beyond 16 weeks are subject to medical review to
determine if additional services are medically necessary.
Notes: Prepackaged food supplements or substitutes and grocery items are
generally excluded from coverage under most benefit plans. Diagnostic tests
required by, for or as a result of non-covered weight loss programs (e.g., those not
requiring physician supervision) are not covered. Please check benefit plan
descriptions for details.
Excluded Services:
The following interventions/procedures are considered experimental and
investigational for weight reduction:
03/28/2019
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 5 of 38
▪ Acupuncture for weight loss
▪ Body plethysmography (diagnostic study)
▪ Low-level laser therapy
▪ Dual-energy X-ray (DEXA) body composition (diagnostic study)
▪ Fat mass and obesity-associated (FTO) genotyping
▪ FTO genotyping
▪ Gastric electrical stimulation (see
CPB 0678 - Gastric Pacing and Gastric Electrical
Stimulation (../600_699/0678.html) )
▪ Human chorionic gonadotropin (HCG) or vitamin injections for weight loss
▪ Indirect calorimetry (also known as oxygen uptake analysis; diagnostic study)
▪ Normobaric hypoxic conditioning.
Whole body calorimetry and composition and whole body bioimpedance analysis
are considered experimental and investigational for weight reduction and other
indications.
Hospital confinement is considered not medically necessary for a weight reduction
program.
Note: Under most benefit plans, the following services and supplies for weight
reduction are specifically excluded from coverage (please check benefit plan
descriptions for details)
▪ Exercise programs or use of exercise equipment
▪ Rice diet or other special diet supplements (e.g., amino acid supplements,
Optifast liquid protein meals, NutriSystem pre-packaged foods, Medifast foods,
or phytotherapy), see CPB 0061 - Nutritional Support (0061.html)
▪ Weight Watchers, Jenny Craig, Diet Center, Zone diet, or similar programs.
Background
03/28/2019
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html 03/28/20
Page 6 of 38
Weight reduction medications should be used as an adjunct to caloric restriction,
exercise, and behavioral modification, when these measures alone have not
resulted in adequate weight loss. Factors influencing successful weight loss are
weight loss during dieting alone, adherence to diet, eating habits, motivation and
personality.
Weight loss due to weight reduction medication use is generally temporary. In
addition, the potential for development of physical dependence and addiction is
high. Because of this, their use to aid in weight loss is not regarded as therapeutic,
but rather involves a risk/benefit ratio, which makes it medically inappropriate in
most cases.
Individuals who cannot maintain weight loss through behavioral weight loss therapy
and are at risk of medical complications of obesity are an exception to this; for
these persons, the risk of physical dependence or other adverse effects may
present less of a risk than continued obesity. For such individuals, use of weight
reduction medication may need to be chronic.
Tests with weight loss drugs have shown that initial responders tend to continue to
respond, while initial non-responders are less likely to respond even with an
increase in dosage. If a person does not lose 2 kg (4.4 lb) in the first four weeks
after initiating therapy, the likelihood of long-term response is very low. If weight is
lost in the initial 6 months of therapy or is maintained after the initial weight loss
phase, this should be considered a success and the drug may be continued.
Orlistat is a reversible inhibitor of gastric and pancreatic lipases. Binding of orlistat
to these enzymes forms inactive intermediates in the gut. This non‐systemic action
does not allow fat to be broken down and absorbed. Rather, an oil phase that
includes triglycerides and cholesterol is excreted in feces. This effect may lead to
weight loss.
Xenical (orlistat) is indicated for obesity management including weight loss and
weight maintenance when used in conjunction with a reduced‐calorie diet. It is also
indicated to reduce the risk for weight regain after prior weight loss.
19
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html 03/2
Page 7 of 38
Orlistat is available as Xenical in 120mg capsules and as Alli in 60mg capsules. Alli
is available over‐the‐counter. Recommended dosage of Xenical is one 120-mg
capsule three times a day with each main meal containing fat (during or up to 1
hour after the meal).
Supplementation with fat‐soluble vitamins (A, D, E, K) and beta carotene is
recommended in some patients as these may not be adequately absorbed when
given orlistat therapy.
Comorbidities associated with obesity appear to be improved through weight loss in
orlistat treated patients. However, studies are limited in time span and comparison
with other pharmacologic agents is needed to determine place in therapy.
Dosage reductions of hypoglycemic agents may be necessary when glycemic
control is improved with weight loss.
Risk of cholelithiasis increases with substantial weight loss.
Pharmacologic treatment of exogenous obesity should be adjunctive to caloric
restriction, increased physical activity, and behavioral modification.
Other than orlistat (Xenical), which is approved for use in adolescents aged 12
years or older, weight reduction medications have not been proven to be safe and
effective for treatment of obesity in children and adolescents. Orlistat (Xenical) is
contraindicated in persons with chronic malabsorption syndromes and cholestasis.
Qsymia is contraindicated in pregnancy, glaucoma,
hyperthyroidism, hypersensitivity to sympathomimetic amines, and within 14 days
of taking monoamine oxidase inhibitors. Belviq is contraindicated in pregnancy.
Other drugs listed in this policy are contraindicated in the following conditions:
hypertension, atherosclerosis, coronary artery disease, and stroke.
Ioannides-Demos et al (2006) stated that there is limited safety and effectiveness
data for amfepramone (diethylpropion) and phentermine and their approvals for the
management of obesity are limited to short-term use. The authors stated that,
although the benefit-risk profiles of sibutramine and orlistat appear positive,
sibutramine continues to be monitored because of long-term safety concerns. The
safety and effectiveness of currently approved drug therapies have not been
evaluated in children and elderly patient populations.
8/2019
medical/data/1_99/0039.html 03/28/ http://www.aetna.com/cpb/ Proprietary
Page 8 of 38
On October 8, 2010, Abbott Laboratories announced that that it was withdrawing its
diet drug Meridia (sibutramine) from the United States, Australian and Canadian
markets as a consequence of heightened concerns that the medication can trigger
heart attack or stroke, especially in patients with underlying cardiovascular disease.
Dual-energy X-ray (DEXA) was developed for the diagnosis of osteoporosis and
was employed originally to clinically significant locations of the forearm, femoral
neck, and lumbar spine. With body composition measurements by means of DEXA,
a controlled x-ray beam scans the entire body to ascertain bone mineral content,
body fat and lean tissue mass. The comprehensive view of body composition
provided by DEXA is thought to be the method of choice for evaluating body
composition by its advocates because of its speed, ease of application as well as
relatively low-dose of ionizing radiation. Its purported uses entail determining
appropriate nutritional support during disease progression and monitoring response
to therapeutic interventions.
Available evidence does not support the use of whole body DEXA for managing
obesity. There is a lack of reliable evidence demonstrating that whole body DEXA
measurement improves the management of persons with obesity over simpler
methods of measuring body composition (including BMI and anthropomorphic
measures), such that clinical outcomes are significantly improved. Published data
have focused on the level of agreement between whole body DEXA and various
other methods of measuring body composition, and on the use of DEXA as an
endpoint in research studies. Well-designed studies are needed to assess
the clinical value of whole body DEXA scanning (Ball and Altena, 2004; Williams et
al, 2006; Ritz et al, 2007; Pineau et al, 2007; Pineau et al, 2009).
There is currently no established role for whole body bioimpedance for weight
reduction or other indications. Current ACC/AHA guidelines on obesity mention no
role for bioimpedance analysis (Jensen, et al., 2013). Current NICE
obesity guidance (NICE, 2014) states: “Do not use bioimpedance as a substitute for
BMI as a measure of general adiposity.”
Balázs (2010) stated that the rapidly increasing prevalence of over-weight and
diabetes mellitus is a serious global threat to healthcare. Nowadays, medicinal plants
and natural treatments are becoming more and more popular. Diabetes has
historically been treated with plants or plant-derived formulations in different cultures,
mainly in China, Asia and India. Different mechanisms for the anti-diabetic
2019

Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html 03/28/
Page 9 of 38
effect of plants has been proposed: increased release of insulin, reduction of
intestinal glucose absorption, as well as enhancement of glycogen synthesis. The
scientific evidences for most of these plants are still incomplete. The large market
for plant remedies has resulted in an array of unauthorized products or marketed as
dietary supplements and, at the same time, no reliable pharmaceutical-grade
products are registered for this purpose.
Borel et al (2012) conducted a prospective intervention study in 104 viscerally
obese men classified according to their glucose tolerance status. They were
followed for one year while participating in a healthy eating-physician
activity/exercise lifestyle modification program while their insulin sensitivity was
tracked. The goals of the study were to evaluate glucose tolerance as well as to
evaluate the respective contribution so fo changes in body fat distribution versus
changes in cardiorespiratory fitness (CRF) to the improvements in indices of
plasma glucose/insulin homeostasis. The results showed insulin sensitivity
improved in assocication with decreases inboth visceral (VAT) and subcutaneous
adiposity (SAT) as well as improvement in CRF, regardless of baseline glucose
tolerance. The results of this study also showed that reduction in VAT was
associated with an improvement in homeostasis model assessment of insulin
resistance, whereas reduction in SAT was rather associated with improvement of
the insulin sensitivity index of Matsuda. The authors concluded that a one-year
lifestyle intervention improved plasma glucose/insulin homeostasis in viscerally
obese men, including those with normal glucose tolerance status at baseline.
Garvey et al (2012) conducted a placebo-controlled, double-blind, 52-week extension
study to evaluate the long-term efficacy and safety of controlled-release
phentermine/topiramate (PHEN/TPM CR) in overweight and obese subjects with
cardiometabolic disease. Subjects were randomly assigned to placebo, 7.5 mg
phentermine/46 mg controlled-release topiramete, or 15 mg phentermine/92 mg
controlled-release topiramate. Of the 676 extension study participants, 84%
completed the study. At week 108 PHEN/TPM-CR was associated with significant,
sustained weight loss. Significantly more PHEN/TPM CR-treated subjects at each
dose achieved ≥ 5%, ≥ 10%, ≥ 15%, and ≥ 20% weight loss compared with placebo
(P < 0.001). The authors therefore concluded that PHEN/TPM CR, in conjunction with
lifestyle modification, may provide a well-tolerated and effective option for the
sustained treatment of obesity complicated by cardiometabolic disease.
2019
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html 03/28/
Page 10 of 38
Mulholland et al (2012) stated that evidence from the literature supports the safe
use of very-low-energy diets (VLED) for up to 3 months in supervised conditions for
patients who fail to meet a target weight loss using a standard low-fat, reduced-
energy approach. There is, however, a need for longer-term outcomes on obesity and
associated morbidities following a VLED. These researchers investigated longer-term
outcomes from studies using VLED, with a minimum duration of 12 months,
published between January 2000 and December 2010. Studies conducted in both
children and adults, with a mean/median BMI of greater than or equal to 28 kg/m2
were included. PubMed, Medline, Web of Science and Science Direct were searched.
Reference lists of studies and reviews were manually searched. Weight loss or
prevention of weight gain and morbidities were the main outcomes assessed. A
total of 32 out of 894 articles met the inclusion criteria. The duration of the studies
ranged from 12 months to 5 years. Periods of VLED ranged from 25 d to 9 months.
Several studies incorporated aspects of behavior therapy, exercise, low-fat diets, low-
carbohydrate diets or medication. Current evidence demonstrated significant weight
loss and improvements in blood pressure, waist circumference and lipid profile in the
longer term following a VLED. Interpretation of the results, however, was restricted
and conclusions with which to guide best practice were limited due to heterogeneity
between the studies. The authors concluded that the present review clearly identified
the need for more evidence and standardized studies to assess the longer-term
benefits from weight loss achieved using VLED.
Indirect calorimetry is designed to measure an individual’s oxygen consumption.
Using this measurement, the device calculates a person’s resting energy
expenditure (REE), also known as resting metabolic rate (RMR). Clinicians
supposedly can screen for abnormally low metabolic rates, teach energy balance,
and identify the precise caloric intake needed for weight loss. Clinical applications
of indirect calorimetry include obesity treatment, as well as treating obesity related
diseases such as diabetes, dysmetabolic syndrome X, hypothyroidism,
hyperthyroidism, hypertension, cardiovascular disease, as well as sleep apnea.
Under strict laboratory protocol, indirect calorimetry can also be used to measure
basal metabolic rate.
Published studies of indirect calorimetry in weight management have focused on its
accuracy (Frankenfeld, et al., 2010; Henes, et al., 2015; Wilms, et al., 2010). There
is a lack of reliable evidence that indirect calorimetry measurements result in
improved clinical outcomes in obesity management.
2019

Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 11 of 38
McDoniel, et al., (2008) evaluated the efficacy of a weight management program
using indirect calorimetry to set energy goals. Fifty-four overweight, active duty adult
employees of the US Air Force (age 18-46 years, BMI 25.2–35.6 kg/m2)
participated in this quasi-experimental control design study. All participants were
enrolled in a four-session US Air Force ‘Sensible Weigh’ group weight control
program. Treatment participants received a personalized nutrition energy goal
message developed using measured resting metabolic rate (RMR) from a hand-
held indirect calorimeter (MedGem®). Usual care participants received a nutritional
message using a standard care equation (25 kcal/day × body weight) to set energy
intake goals. Investigators reported that treatment participants lost significantly more
weight than usual care participants (p ≤ 0.05). Ten of the 54 subjects dropped from
the study before completion. Difference in weight loss between the treatment and
usual care group were –4.3 kg ± 3.3 vs. –1.8 kg ± 3.2, respectively. The
investigators reported that were no significant differences in reported food intake or
energy expenditure between groups. The investigators posited that a possible
reason why experimental individuals experienced greater weight loss from
measured resting metabolic rate may be that the individualized nutrition message
influenced psychobehavioral constructs (i.e. motivation, self-efficacy, etc.) for
weight loss change. The investigators noted that study limitations include small
sample size, short duration, and small treatment effect. An additional issue is the
generalizability of the findings, given that, at the time of the study, the Air Force had
regulations that all personnel maintain a desired body weight and body fat
percentage, or these individuals could be discharged from service. The
investigators stated that future research is needed to determine the long-term
efficacy of using indirect calorimetry as part of a comprehensive weight control
program.
An UpToDate review on “Palliative care: Assessment and management of anorexia
and cachexia” (Bruera and Dev, 2013) states that “Handheld indirect calorimetry,
which is more accurate than equations at estimating basal energy needs but less
precise than traditional devices used in the research setting, may be useful in the
outpatient setting. Close to one-half of cancer patients being evaluated in an
outpatient cachexia clinic are noted to be hypermetabolic by indirect calorimetry.
These assessments are appropriate in the research setting but have little if any
utility in the clinic”.
03/28/2019

Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 12 of 38
Whiting et al (2014) stated that capsaicinoids are a group of chemicals naturally
occurring in chilli peppers with bioactive properties that may help to support weight
management. These investigators conducted a meta-analysis investigating the
potential effects of capsaicinoids on energy intake, clarified previous observations
and formed evidence-based conclusions about possible weight management roles.
Medical databases (Medline, Web of Knowledge and Scopus) were systematically
searched for papers. Search terms were: 'capsaicin (*)' or 'red pepper' or 'chilli(*)' or
'chili(*)' with 'satiety' or 'energy intake'. Of the 74 clinical trials identified, 10 were
included, 8 of which provided results suitable to be combined in analysis (191
participants). From the studies, 19 effect sizes were extracted and analyzed using
MIX meta-analysis software. Data analysis showed that capsaicinoid ingestion prior
to a meal reduced ad libitum energy intake by 309.9kJ (74.0kcal) during the meal (p
< 0.001). However, results should be viewed with some caution as heterogeneity
was high (I(2) = 75.7 %). Study findings suggested a minimum dose of 2 mg of
capsaicinoids is needed to contribute to reductions in ad libitum energy intake,
which appears to be attributed to an altered preference for carbohydrate-rich foods
over foods with a higher fat content. The authors concluded that meta- analysis
findings suggested that daily consumption of capsaicinoids may contribute to weight
management through reductions in energy intake. Subsequently, there may be
potential for capsaicinoids to be used as long-term, natural weight-loss aids. They
stated that further long-term randomized trials are now needed to investigate these
effects.
In a systematic review, Onakpoya et al (2014a) evaluated the evidence for or
against the effectiveness of glucomannan, a soluble fiber, in body weight
reduction. Electronic searches were conducted in Medline, Embase, Amed, and
The Cochrane Library. Hand searches of bibliography were also conducted.
Outcomes of interest were body weight and BMI. Studies involving only over-
weight and/or obese participants were included. Two reviewers independently
determined the eligibility of studies and assessed the reporting quality of included
randomized controlled trials (RCTs), using the CONSORT and PRISMA guidelines.
A total of 18 trials were identified, and 9 were included. There was a variation in
the reporting quality of the included RCTs. A meta-analysis (random effect model)
of 8 RCTs revealed a non-statistically significant difference in weight loss between
glucomannan and placebo (mean difference [MD]: -0.22 kg; 95 % confidence
interval [CI]: -0.62, 0.19; I(2) = 65 %). Adverse events included abdominal
discomfort, diarrhea, and constipation. The authors concluded that the evidence
03/28/2019

Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 13 of 38
from available RCTs does not show that glucomannan intake generates statistically
significant weight loss. They stated that future trials should be more rigorous and
better reported.
Onakpoya et al (2014b) noted that several slimming aids being sold as food
supplements are widely available. One of them is pyruvate. Its effectiveness in
causing weight reduction in humans has not been fully established. The objective of
this systematic review was to examine the effectiveness of pyruvate in reducing
body weight. Electronic and non-electronic searches were conducted to identify all
relevant human RCTs. The bibliographies of all located articles were also
searched. No restrictions in language or time were applied. Two independent
reviewers extracted the data according to predefined criteria. A fixed-effect model
was used to calculate MD and 95 % CI. A total of 9 trials were identified and 6
were included. All had methodological weaknesses. The meta-analysis revealed a
statistically significant difference in body weight with pyruvate compared to placebo
(MD: -0.72 kg; 95 % CI: -1.24 to -0.20). The magnitude of the effect is small, and
its clinical relevance is uncertain. Adverse events included gas, bloating, diarrhea,
and increase in low-density lipoprotein (LDL) cholesterol. The authors concluded
that the evidence from RCTs does not convincingly show that pyruvate is effective
in reducing body weight; limited evidence exists about the safety of pyruvate. They
stated that future trials involving the use of this supplement should be more
rigorous and better reported.
The FDA has approved liraglutide [rDNA origin] injection (Saxenda), a once-daily
injection of a glucagon-like peptide-1 (GLP-1) receptor agonist, for chronic weight
management (Novo Nordisk, 2014). Liraglutide is indicated as an adjunct to a
reduced-calorie diet and increased physical activity for chronic weight management
in adults with obesity (BMI ≥30 kg/m2) or who are overweight (BMI ≥27 kg/m2) in
the presence of at least one weight-related comorbid condition (e.g., hypertension,
type 2 diabetes mellitus, or dyslipidemia) (FDA, 2014).
The labeling of Saxenda states that liraglutide should not be used with insulin (FDA,
2014). It also states that the the effects of liraglutide on cardiovascular morbidity
and mortality have not been established. The labeling states that the safety and
efficacy of coadministration with other products for weight loss have not been
established. In addition, liraglutide has not been studied in patients with a history of
pancreatitis.
03/28/2019

Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html 03/2
Page 14 of 38
Liraglutide for chronic weight management is contraindicated in the following
conditions: personal or family history of medullary thyroid carcinoma (MTC) or
multiple endocrine neoplasia syndrome type 2 (MEN 2); patients with a prior
serious hypersensitivity reaction to liraglutide or to any of the product components;
and pregnancy (FDA, 2014).
The FDA approval of liraglutide was based upon the SCALE (Satiety and Clinical
Adiposity−Liraglutide Evidence in Non-diabetic and Diabetic adults) phase 3 clinical
trial program, which included study participants who have obesity (BMI ≥30 kg/m2) or
who are overweight (BMI ≥27 kg/m2) with comorbidities (Novo Nordisk, 2014).
Trial data showed that liraglutide, in combination with a reduced-calorie diet and
increased physical activity, resulted in significantly greater weight loss than diet and
physical activity alone.
The SCALE phase 3 clinical trial program of the safety and effectiveness of
liraglutide for chronic weight management included three clinical trials that included
approximately 4,800 obese and overweight patients with and without significant
weight-related conditions (FDA, 2014). All patients received counseling regarding
lifestyle modifications that consisted of a reduced-calorie diet and regular physical
activity.
Results from a clinical trial that enrolled patients without diabetes showed that
patients had an average weight loss of 4.5 percent from baseline compared to
treatment with a placebo at one year (FDA, 2014). In this trial, 62 percent of
patients treated with liraglutide lost at least 5 percent of their body weight compared
with 34 percent of patients treated with placebo. Results from another clinical trial
that enrolled patients with type 2 diabetes showed that patients had an average
weight loss of 3.7 percent from baseline compared to treatment with placebo at one
year. In this trial, 49 percent of patients treated with liraglutide lost at least 5 percent
of their body weight compared with 16 percent of patients treated with placebo.
The FDA approved labeling states that patients using liraglutide should be
evaluated after 16 weeks to determine if the treatment is working (FDA, 2014). If a
patient has not lost at least 4 percent of baseline body weight, liraglutide should be
discontinued, as it is unlikely that the patient will achieve and sustain clinically
meaningful weight loss with continued treatment.
8/2019
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html 03/28/2019
Page 15 of 38
Saxenda is a glucagon-like peptide-1 (GLP-1) receptor agonist and should not be
used in combination with any other drug belonging to this class, including Victoza, a
treatment for type 2 diabetes (FDA, 2014). Saxenda and Victoza contain the same
active ingredient (liraglutide) at different doses (3 mg and 1.8 mg, respectively).
However, Saxenda is not indicated for the treatment of type 2 diabetes, as the
safety and efficacy of Saxenda for the treatment of diabetes has not been
established.
Saxenda has a boxed warning stating that thyroid C-cell tumors have been
observed in rodent studies with liraglutide but that it is unknown whether liraglutide
causes thyroid C-cell tumors, including medullary thyroid carcinoma (MTC), in
humans (FDA, 2014). Liraglutide causes dose-dependent and treatment-duration-
dependent thyroid C-cell tumors at clinically relevant exposures in both genders of
rats and mice. It is unknown whether liraglutide causes thyroid C-cell tumors,
including MTC, in humans, as the human relevance of liraglutide-induced rodent
thyroid C-cell tumors has not been determined.
The labeling states that liraglutide is contraindicated in patients with a personal or
family history of MTC or in patients with multiple endocrine neoplasia syndrome
type 2 (MEN 2) (FDA, 2014). The labeling states that patients should be counseled
regarding the risk of MTC with use of liraglutide and informed of symptoms of
thyroid tumors (e.g., a mass in the neck, dysphagia, dyspnea, persistent
hoarseness). The labeling states that routine monitoring of serum calcitonin or
using thyroid ultrasound is of uncertain value for early detection of MTC in patients
treated with liraglutide.
In clinical trials, the most common adverse reactions, reporting in ≥5%, were:
nausea, hypoglycemia, diarrhea, constipation, vomiting, headache, decreased
appetite, dyspepsia, fatigue, dizziness, abdominal pain, and increased lipase (Novo
Nordisk, 2014).
Serious side effects reported in patients treated with liraglutide for chronic weight
management include pancreatitis, gallbladder disease, renal impairment, and
suicidal thoughts (FDA, 2014). Liraglutide can also increase heart rate and should
be discontinued in patients who experience a sustained increase in resting heart
rate.
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 16 of 38
Based on spontaneous postmarketing reports, acute pancreatitis, including fatal
and non-fatal hemorrhagic or necrotizing pancreatitis, has been observed in
patients treated with liraglutide (Novo Nordisk, 2014). After initiation of liraglutide,
patients should be observed for signs and symptoms of pancreatitis (including
persistent severe abdominal pain, sometimes radiating to the back and which may
or may not be accompanied by vomiting). If pancreatitis is suspected, liraglutide
should promptly be discontinued and appropriate management should be initiated.
If pancreatitis is confirmed, liraglutide should not be restarted.
Substantial or rapid weight loss can increase the risk of cholelithiasis; however, the
incidence of acute gallbladder disease was greater in liraglutide-treated patients
than in placebo-treated patients even after accounting for the degree of weight loss
(Novo Nordisk, 2014). If cholelithiasis is suspected, gallbladder studies and
appropriate clinical follow-up are indicated.
When liraglutide is used with an insulin secretagogue (e.g., a sulfonylurea) serious
hypoglycemia can occur (Novo Nordisk, 2014). The labeling recommends lowering
the dose of the insulin secretagogue to reduce the risk of hypoglycemia.
Renal impairment has been reported postmarketing, usually in association with
nausea, vomiting, diarrhea, or dehydration, which may sometimes require
hemodialysis (Novo Nordisk, 2014). The labeling recommends using caution when
initiating or escalating doses of liraglutide in patients with renal impairment.
Serious hypersensitivity reactions (e.g., anaphylaxis and angioedema) have been
reported during postmarketing use of liraglutide (Novo Nordisk, 2014). The labeling
recommends that patients stop taking liraglutide and seek medical advice if
symptoms of hypersensitivity reactions occur.
The labeling states that patients treated with liraglutide should be monitored for the
emergence or worsening of depression, suicidal thoughts or behavior, and/or any
unusual changes in mood or behavior (Novo Nordisk, 2014). Liraglutide should be
discontinued in patients who experience suicidal thoughts or behaviors. Liraglutide
should be avoided in patients with a history of suicidal attempts or active suicidal
ideation.
03/28/2019

Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 17 of 38
The labeling states that nursing mothers should either discontinue liraglutide for
chronic weight management or discontinue nursing (Novo Nordisk, 2014). The
labeling states that the safety and effectiveness of liraglutide have not been
established in pediatric patients and is not recommended for use in pediatric
patients.
The FDA is requiring the following post-marketing studies for liraglutide for chronic
weight management (FDA, 2014): clinical trials to evaluate dosing, safety, and
efficacy in pediatric patients; a study to assess potential effects on growth, sexual
maturation, and central nervous system development and function in immature rats;
an MTC case registry of at least 15 years duration to identify any increase in MTC
incidence related to liraglutide; and an evaluation of the potential risk of breast
cancer with liraglutide in ongoing clinical trials. In addition, the cardiovascular safety
of liraglutide is being investigated in an ongoing cardiovascular outcomes trial.
The FDA approved Saxenda with a Risk Evaluation and Mitigation Strategy
(REMS), which consists of a communication plan to inform health care
professionals about the serious risks associated with Saxenda (FDA, 2014).
Lingwood (2013) stated that there is a critical need for improved technologies to
monitor fluid balance and body composition in neonates, particularly those
receiving intensive care. Bioelectrical impedance analysis (BIA) meets many of the
criteria required in this environment and appears to be effective for monitoring
physiological trends. These researchers reviewed the literature regarding the use
of bioelectrical impedance in neonates. It was found that prediction equations for
total body water, extracellular water and fat-free mass have been developed, but
many require further testing and validation in larger cohorts. Alternative
approaches based on Hanai mixture theory or vector analysis are in the early
stages of investigation in neonates. The authors concluded that further research is
needed into electrode positioning, bioimpedance spectroscopy and Cole analysis in
order to realize the full potential of this technology.
de Miguel-Etayo et al (2013) noted that nutrition, physical activity and behavior-
modifying techniques are widely applied components of interventions treating
obesity. These investigators reviewed available information on the short- and long-
term effects of intervention treatment on body fat composition of overweight and
obese children and adolescents and, to obtain a further understanding on how
different body composition techniques detect longitudinal changes. A total of 13
03/28/2019

Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 18 of 38
papers were included; 7 included a multi-disciplinary intervention component, 5
applied a combined dietary and physical activity intervention and 1 a physical
activity intervention. Body composition techniques used included anthropometric
indices, BIA, and dual energy X-ray absorptiometry. Percentage of fat mass
change was calculated in when possible. Findings suggested, no changes were
observed in fat free mass after 16 weeks of nutritional intervention and the lowest
decrease on fat mass percentage was obtained. However, the highest fat mass
percentage with parallel increase in fat free mass, both assessed by DXA was
observed in a multi-component intervention applied for 20 weeks. The authors
concluded that more studies are needed to determine the best field body
composition method to monitor changes during overweight treatment in children
and adolescents.
Talma et al (2013) stated that BIA is a practical method to estimate percentage
body fat (% BF). In this systematic review, these researchers evaluated validity,
responsiveness, reliability and measurement error of BIA methods in estimating %
BF in children and adolescents. They searched for relevant studies in PubMed,
Embase and Cochrane through November 2012. Two reviewers independently
screened titles and abstracts for inclusion, extracted data and rated methodological
quality of the included studies. These investigators performed a best evidence
synthesis to synthesize the results, thereby excluding studies of poor quality. They
included 50 published studies. Mean differences between BIA and reference
methods (gold standard [criterion validity] and convergent measures of body
composition [convergent validity]) were considerable and ranged from negative to
positive values, resulting in conflicting evidence for criterion validity. These
investigators found strong evidence for a good reliability, i.e., (intra-class)
correlations greater than or equal to 0.82. However, test-retest mean differences
ranged from 7.5 % to 13.4 % of total % BF in the included study samples, indicating
considerable measurement error. The authors concluded that the findings of this
systematic review suggested that BIA is a practical method to estimate % BF in
children and adolescents. However, they stated that validity and measurement
error were not satisfactory.
Goldberg et al (2014) stated that the sensory and gastro-intestinal changes that
occur with aging affect older adults' food and liquid intake. Any decreased liquid
intake increases the risk for dehydration. This increased dehydration risk is
compounded in older adults with dysphagia. The availability of a non-invasive and
easily administered way to document hydration levels in older adults is critical,
03/28/2019

Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 19 of 38
particularly for adults in residential care. This pilot study investigated the
contribution of BIA to measure hydration in 19 older women in residential care: 13
who viewed themselves as healthy and 6 with dysphagia. Mann-Whitney U
analyses documented no significant between-group differences for total body water
(TBW), fat free mass (FFM), Fat Mass (FM), and % BF. However, when compared
to previously published data for age-matched women, the TBW and FFM values of
the 2 participant groups were notably less, and FM and % BF values were notably
greater than expected. The authors concluded that if results are confirmed through
continued investigation, such findings may suggest that long-term care facilities are
unique environments in which all older residents can be considered at-risk for
dehydration and support the use of BIA as a non-invasive tool to assess and
monitor their hydration status.
Buffa et al (2014) defined the effectiveness of bioelectrical impedance vector
analysis (BIVA) for assessing 2-compartment body composition. These researchers
performed a systematic literature review using MEDLINE database up to February
12, 2014. The list of papers citing the first description of BIVA, obtained from
SCOPUS, and the reference lists of included studies were also searched. Selection
criteria included studies comparing the results of BIVA with those of other
techniques, and studies analyzing bioelectrical vectors of obese, athletic, cachectic
and lean individuals. A total of 30 articles met the inclusion criteria. The ability of
classic BIVA for assessing 2-compartment body composition has been mainly
evaluated by means of indirect techniques, such as anthropometry and BIA. Classic
BIVA showed a high agreement with body mass index, which can be interpreted in
relation to the greater body mass of obese and athletic individuals, whereas the
comparison with BIA showed less consistent results, especially in diseased
individuals. When a reference method was used, classic BIVA failed to accurately
recognize FM % variations, whereas specific BIVA furnished good results. The
authors concluded that specific BIVA is a promising alternative to classic BIVA for
assessing 2-compartment body composition, with potential application in nutritional,
sport and geriatric medicine.
Haverkort et al (2015) noted that BIA is a commonly used method for the evaluation
of body composition. However, BIA estimations are subject to uncertainties. These
researchers explored the variability of empirical prediction equations used in BIA
estimations and evaluated the validity of BIA estimations in adult surgical and
oncological patients. Studies developing new empirical prediction equations and
studies evaluating the validity of BIA estimations compared with a reference
03/28/2019
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 20 of 38
method was included. Only studies using BIA devices measuring the entire body
were included. Studies that included patients with altered body composition or a
disturbed fluid balance and studies written in languages other than English were
excluded. To illustrate variability between equations, fixed normal reference values
of resistance values were entered into the existing empirical prediction equations of
the included studies and the results were plotted in figures. The validity was
expressed by the difference in means between BIA estimates and the reference
method, and relative difference in %. Substantial variability between equations for
groups (including men and women) was found for TBW and FFM. The gender-
specific existing general equations assume less variability for TBW and FFM. BIA
mainly under-estimated TBW (range relative difference -18.8 % to +7.2 %) and
FFM (range relative differences -15.2 % to +3.8 %). Estimates of the FM
demonstrated large variability (range relative difference -15.7 % to +43.1 %). The
authors concluded that application of equations validated in healthy subjects to
predict body composition performs less well in oncologic and surgical patients.
They suggested that BIA estimations, irrespective of the device, can only be useful
when performed longitudinally and under the same standard conditions.
Ketogenic Diets for Weight Loss:
Gibson et al (2015) stated that VLEDs and ketogenic low-carbohydrate diets
(KLCDs) are 2 dietary strategies that have been associated with a suppression of
appetite. However, the results of clinical trials investigating the effect of ketogenic
diets on appetite are inconsistent. To evaluate quantitatively the effect of ketogenic
diets on subjective appetite ratings, these researchers conducted a systematic
literature search and meta-analysis of studies that assessed appetite with visual
analog scales (VAS) before (in energy balance) and during (while in ketosis)
adherence to VLED or KLCD. Individuals were less hungry and exhibited greater
fullness/satiety while adhering to VLED, and individuals adhering to KLCD were
less hungry and had a reduced desire to eat. Although these absolute changes in
appetite were small, they occurred within the context of energy restriction, which is
known to increase appetite in obese people. Thus, the clinical benefit of a
ketogenic diet is in preventing an increase in appetite, despite weight loss, although
individuals may indeed feel slightly less hungry (or more full or satisfied). Ketosis
appears to provide a plausible explanation for this suppression of appetite. The
authors concluded that future studies should investigate the minimum level of
03/28/2019

Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 21 of 38
ketosis required to achieve appetite suppression during ketogenic weight loss diets,
as this could enable inclusion of a greater variety of healthy carbohydrate-
containing foods into the diet.
Medium-Chain Triglycerides for Weight Loss:
Bueno and colleagues (2015) examined the effect of replacing dietary long-chain
triacylglycerols (LCTs) with medium-chain triacylglycerols (MCTs) on body
composition in adults. These researchers conducted a meta-analysis of RCTs, to
examine if individuals assigned to replace at least 5 g of dietary LCTs with MCTs for
a minimum of 4 weeks show positive modifications on body composition. They
systematically searched, through July 2013, the CENTRAL, EMBASE, LILACS, and
MEDLINE databases for RCTs that investigated the effects of MCT intake on body
composition in adults. Two authors independently extracted data and assessed risk
of bias. Weighted mean differences (WMDs) were calculated for net changes in
the outcomes. These investigators assessed heterogeneity by the Cochran Q test
and I(2) statistic and publication bias with the Egger's test. Pre-specified sensitivity
analyses were performed. A total of 11 trials were included, from which 5
presented low risk of bias. In the overall analysis, including all studies, individuals
who replaced dietary LCT with MCT showed significantly reduced body weight
(WMD, -0.69 kg; 95 % CI: -1.1 to -0.28; p = 0.001); body fat (-0.89 kg; 95 % CI:
-1.27 to -0.51; p < 0.001), and WC (-1.78 cm; 95 % CI: -2.4 to -1.1; p < 0.001). The
overall quality of the evidence was low-to-moderate. Trials with a cross-over
design were responsible for the heterogeneity. The authors concluded that despite
statistically significant results, the recommendation to replace dietary LCTs with
MCTs must be cautiously taken, because the available evidence is not of the
highest quality.
Mumme and Stonehouse (2015) conducted a systematic review and meta-analysis
of RCTs comparing the effects of MCTs, specifically C8:0 and C10:0, to long-chain
triglycerides (LCTs) on weight loss and body composition in adults. Changes in
blood lipid levels were secondary outcomes. Randomized controlled trials of
greater than 3 weeks' duration conducted in healthy adults were identified
searching Web of Knowledge, Discover, PubMed, Scopus, New Zealand Science,
and Cochrane CENTRAL until March 2014 with no language restriction. Identified
trials were assessed for bias. Mean differences were pooled and analyzed using
inverse variance models with fixed effects. Heterogeneity between studies was
calculated using I(2) statistic. An I(2) > 50 % or p < 0.10 indicated heterogeneity. A
03/28/2019

Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 22 of 38
total of 13 trials (n = 749) were identified. Compared with LCTs, MCTs decreased
body weight (-0.51 kg [95 % CI: -0.80 to -0.23 kg]; p < 0.001; I (2) = 35 %); waist
circumference (-1.46 cm [95 % CI: -2.04 to -0.87 cm]; p < 0.001; I (2) = 0%), hip
circumference (-0.79 cm [95 % CI: -1.27 to -0.30 cm]; p = 0.002; I (2) = 0 %), total
body fat (standard mean difference -0.39 [95 % CI: -0.57 to -0.22]; p < 0.001; I(2) =
0%), total subcutaneous fat (standard mean difference -0.46 [95 % CI: -0.64 to
-0.27]; p < 0.001; I(2) = 20 %), and visceral fat (standard mean difference -0.55 [95
% CI: -0.75 to -0.34]; p < 0.001; I(2) = 0 %). No differences were seen in blood lipid
levels. Many trials lacked sufficient information for a complete quality assessment,
and commercial bias was detected. Although heterogeneity was absent, study
designs varied with regard to duration, dose, and control of energy intake. The
authors concluded that replacement of LCTs with MCTs in the diet could potentially
induce modest reductions in body weight and composition without adversely
affecting lipid profiles. However, they stated that further research is needed by
independent research groups using large, well-designed studies to confirm the
effectiveness of MCT and to determine the dosage needed for the management of
a healthy body weight and composition.
FTO Genotyping:
Xiang and colleagues (2016) noted that studies have suggested that the fat mass and
obesity-associated (FTO) genotype is associated with individual variability in weight
loss in response to diet/lifestyle interventions, but results are inconsistent. These
investigators provided a summary of the literature evaluating the relation between the
FTO genotype and weight loss in response to diet/lifestyle interventions. They
performed a search of English-language articles in the PubMed and Embase
databases (through April 30, 2015). Eligible studies were diet/lifestyle weight-loss
intervention studies conducted in adults that reported changes in body weight or BMI
by the FTO variant rs9939609 (or its proxy). Differences in weight loss between FTO
genotypes across studies were pooled with the use of fixed- effect models. A meta-
analysis of 10 studies (comprising 6,951 participants) that reported the results of
additive genetic models showed that individuals with the FTO TA genotype and AA
genotype (those with the obesity-predisposing A allele) had 0.18-kg (95 % CI: -0.09
to 0.45-kg; p= 0.19; NS) and 0.44-kg (95 % CI: 0.09- to
0.79-kg; p = 0.015) greater weight loss, respectively, than those with the TT
genotype. A meta-analysis of 14 studies (comprising 7,700 participants) that
reported the results of dominant genetic models indicated a 0.20-kg (-0.43- to 0.04-
kg) greater weight loss in the TA/AA genotype than in the TT genotype (p = 0.10).
03/28/2019
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 23 of 38
In addition, differences in weight loss between the AA genotype and TT genotype
were significant in studies with a diet intervention only, adjustment for baseline BMI or
body weight, and several other subgroups. However, the relatively small number of
studies limited these stratified analyses, and there was no statistically significant
difference between subgroups. The authors concluded that the findings of this meta-
analysis suggested that individuals carrying the homozygous FTO obesity-
predisposing allele may lose more weight through diet/lifestyle interventions than non-
carriers; and clinical applications of these findings need further investigations. They
stated that these findings provided some support for considering genetic variability in
response to diet/lifestyle interventions in the development of more effective strategies
for weight loss; nevertheless, more studies are needed to explore which types of
diet/lifestyle interventions most powerfully facilitate the FTO genetic effect on weight
loss.
Normobaric Hypoxic Conditioning:
Hobbins and colleagues (2017) stated that normobaric hypoxic conditioning (HC) is
defined as exposure to systemic and/or local hypoxia at rest (passive) or combined
with exercise training (active). Hypoxic conditioning has been previously used by
healthy and athletic populations to enhance their physical capacity and improve
performance in the lead up to competition. Recently, HC has also been applied
acutely (single exposure) and chronically (repeated exposure over several weeks) to
over-weight and obese populations with the intention of managing and potentially
increasing cardio-metabolic health and weight loss. At present, it is unclear what the
cardio-metabolic health and weight loss responses of obese populations are in
response to passive and active HC. Exploration of potential benefits of exposure to
both passive and active HC may provide pivotal findings for improving health and
well-being in these individuals. These researchers carried out a systematic literature
search for articles published between 2000 and 2017. Studies investigating the
effects of normobaric HC as a novel therapeutic approach to elicit improvements in
the cardio-metabolic health and weight loss of obese populations were included.
Studies investigated passive (n = 7; 5 animals, 2 humans), active (n
= 4; all humans) and a combination of passive and active (n = 4; 3 animals, 1
human) HC to an inspired oxygen fraction between 4.8 and 15.0 %, ranging
between a single session and daily sessions per week, lasting from 5 days up to 8
months. Passive HC led to reduced insulin concentrations (-37 to -22 %) in obese
animals and increased energy expenditure (+12 to +16 %) in obese humans,
whereas active HC led to reductions in body weight (-4 to -2 %) in obese animals
03/28/2019
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html 03/28/2019
Page 24 of 38
and humans, and blood pressure (BP; -8 to -3 %) in obese humans compared with
a matched workload in normoxic conditions. Inconclusive findings, however, exist
in determining the impact of acute and chronic HC on markers such as
triglycerides, cholesterol levels, and fitness capacity. More importantly, most of the
studies that included animal models involved exposure to severe levels of hypoxia
(= 5.0 %; simulated altitude greater than 10,000 m) that are not suitable for human
populations. The authors concluded that normobaric HC demonstrated observable
positive findings in relation to insulin and energy expenditure (passive), and body
weight and BP (active), which may improve the cardio-metabolic health and body
weight management of obese populations. However, they stated that further
evidence on responses of circulating biomarkers to both passive and active HC in
humans is needed.
Appendix
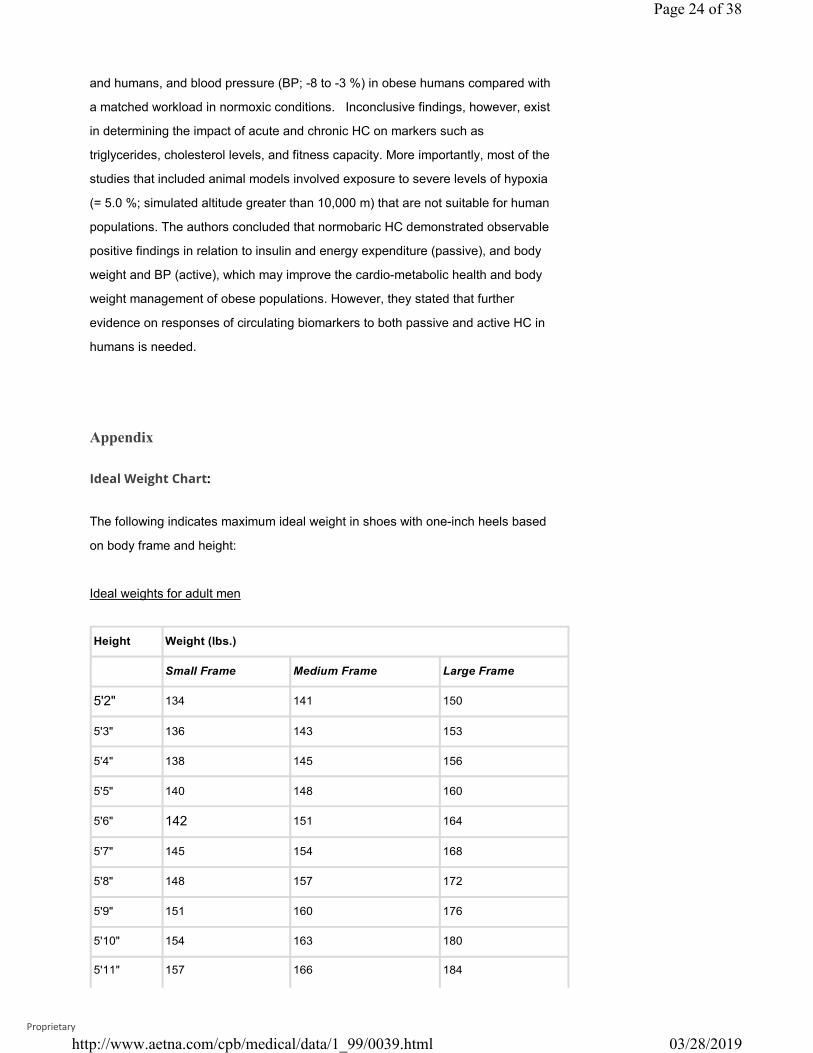
Ideal Weight Chart:
The following indicates maximum ideal weight in shoes with one-inch heels based
on body frame and height:
Ideal weights for adult men
Height Weight (lbs.)
Small Frame Medium Frame Large Frame
5'2" 134 141 150
5'3" 136 143 153
5'4" 138 145 156
5'5" 140 148 160
5'6" 142 151 164
5'7" 145 154 168
5'8" 148 157 172
5'9" 151 160 176
5'10" 154 163 180
5'11" 157 166 184
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 25 of 38
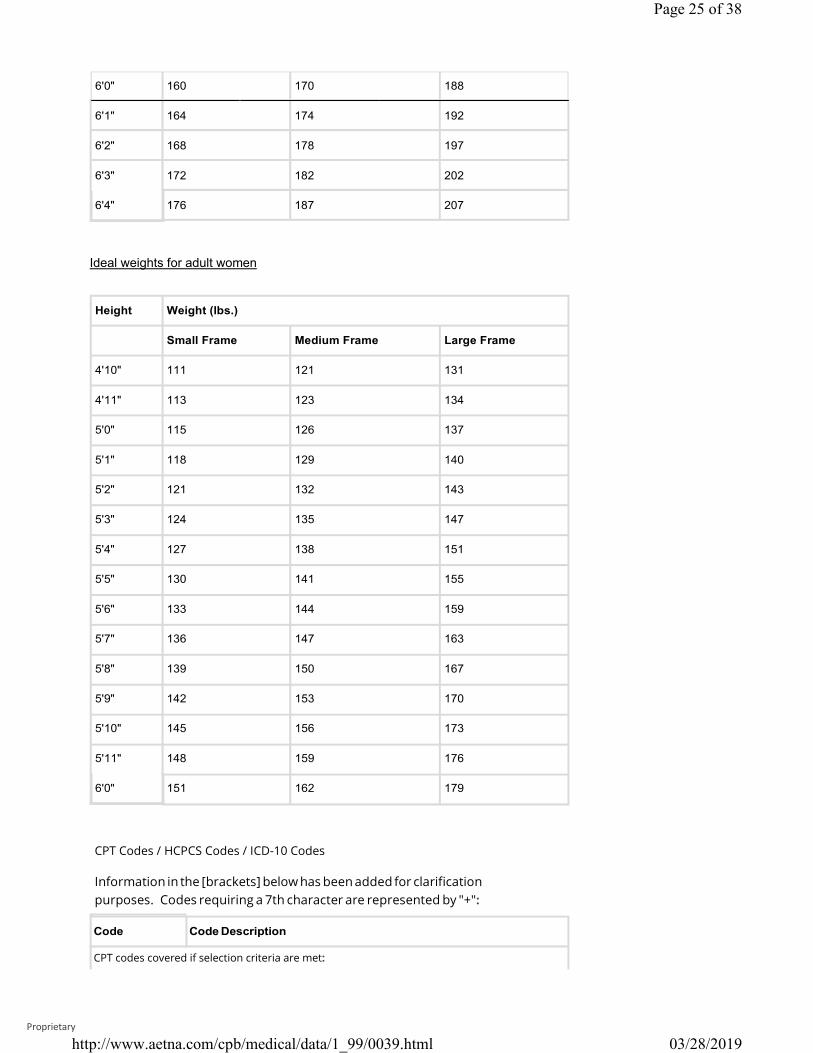
6'0" 160 170 188
6'1" 164 174 192
6'2" 168 178 197
6'3" 172 182 202
6'4" 176 187 207
Ideal weights for adult women
Height Weight (lbs.)
Small Frame Medium Frame Large Frame
4'10" 111 121 131
4'11" 113 123 134
5'0" 115 126 137
5'1" 118 129 140
5'2" 121 132 143
5'3" 124 135 147
5'4" 127 138 151
5'5" 130 141 155
5'6" 133 144 159
5'7" 136 147 163
5'8" 139 150 167
5'9" 142 153 170
5'10" 145 156 173
5'11" 148 159 176
6'0" 151 162 179
CPT Codes / HCPCS Codes / ICD-10 Codes
Information in the [brackets] below has been added for clarification purposes. Codes requiring a 7th character are represented by "+":
CPT codes covered if selection criteria are met:
03/28/2019
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 26 of 38
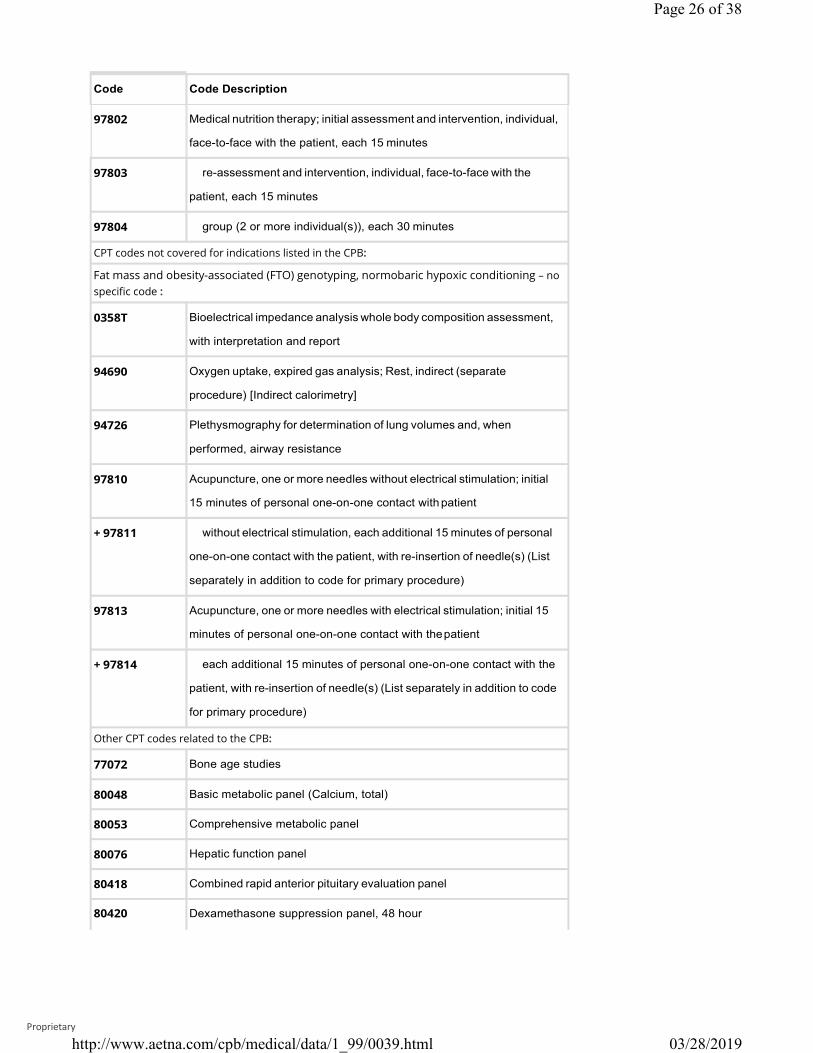
Code Code Description
97802 Medical nutrition therapy; initial assessment and intervention, individual,
face-to-face with the patient, each 15 minutes
97803 re-assessment and intervention, individual, face-to-face with the
patient, each 15 minutes
97804 group (2 or more individual(s)), each 30 minutes
CPT codes not covered for indications listed in the CPB:
Fat mass and obesity-associated (FTO) genotyping, normobaric hypoxic conditioning – no specific code :
0358T Bioelectrical impedance analysis whole body composition assessment,
with interpretation and report
94690 Oxygen uptake, expired gas analysis; Rest, indirect (separate
procedure) [Indirect calorimetry]
94726 Plethysmography for determination of lung volumes and, when
performed, airway resistance
97810 Acupuncture, one or more needles without electrical stimulation; initial
15 minutes of personal one-on-one contact with patient
+ 97811 without electrical stimulation, each additional 15 minutes of personal
one-on-one contact with the patient, with re-insertion of needle(s) (List
separately in addition to code for primary procedure)
97813 Acupuncture, one or more needles with electrical stimulation; initial 15
minutes of personal one-on-one contact with thepatient
+ 97814 each additional 15 minutes of personal one-on-one contact with the
patient, with re-insertion of needle(s) (List separately in addition to code
for primary procedure)
Other CPT codes related to the CPB:
77072 Bone age studies
80048 Basic metabolic panel (Calcium, total)
80053 Comprehensive metabolic panel
80076 Hepatic function panel
80418 Combined rapid anterior pituitary evaluation panel
80420 Dexamethasone suppression panel, 48 hour
03/28/2019
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 27 of 38
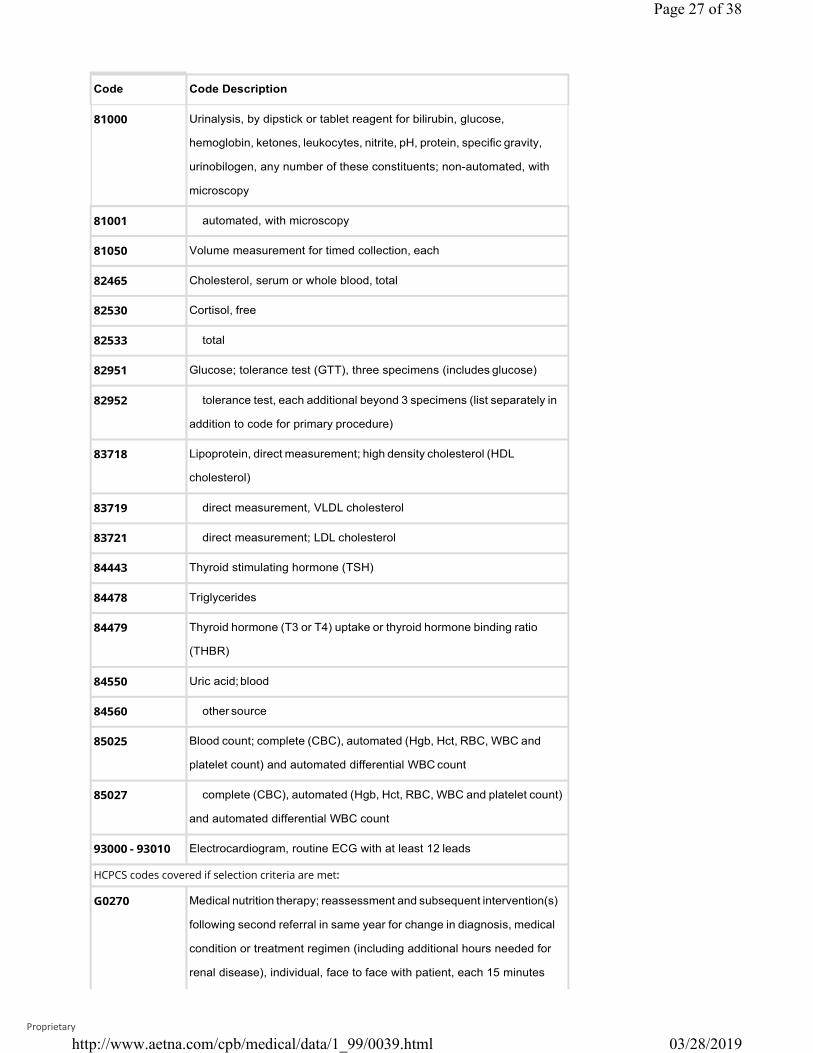
Code Code Description
81000 Urinalysis, by dipstick or tablet reagent for bilirubin, glucose,
hemoglobin, ketones, leukocytes, nitrite, pH, protein, specific gravity,
urinobilogen, any number of these constituents; non-automated, with
microscopy
81001 automated, with microscopy
81050 Volume measurement for timed collection, each
82465 Cholesterol, serum or whole blood, total
82530 Cortisol, free
82533 total
82951 Glucose; tolerance test (GTT), three specimens (includes glucose)
82952 tolerance test, each additional beyond 3 specimens (list separately in
addition to code for primary procedure)
83718 Lipoprotein, direct measurement; high density cholesterol (HDL
cholesterol)
83719 direct measurement, VLDL cholesterol
83721 direct measurement; LDL cholesterol
84443 Thyroid stimulating hormone (TSH)
84478 Triglycerides
84479 Thyroid hormone (T3 or T4) uptake or thyroid hormone binding ratio
(THBR)
84550 Uric acid; blood
84560 other source
85025 Blood count; complete (CBC), automated (Hgb, Hct, RBC, WBC and
platelet count) and automated differential WBC count
85027 complete (CBC), automated (Hgb, Hct, RBC, WBC and platelet count)
and automated differential WBC count
93000 - 93010 Electrocardiogram, routine ECG with at least 12 leads
HCPCS codes covered if selection criteria are met:
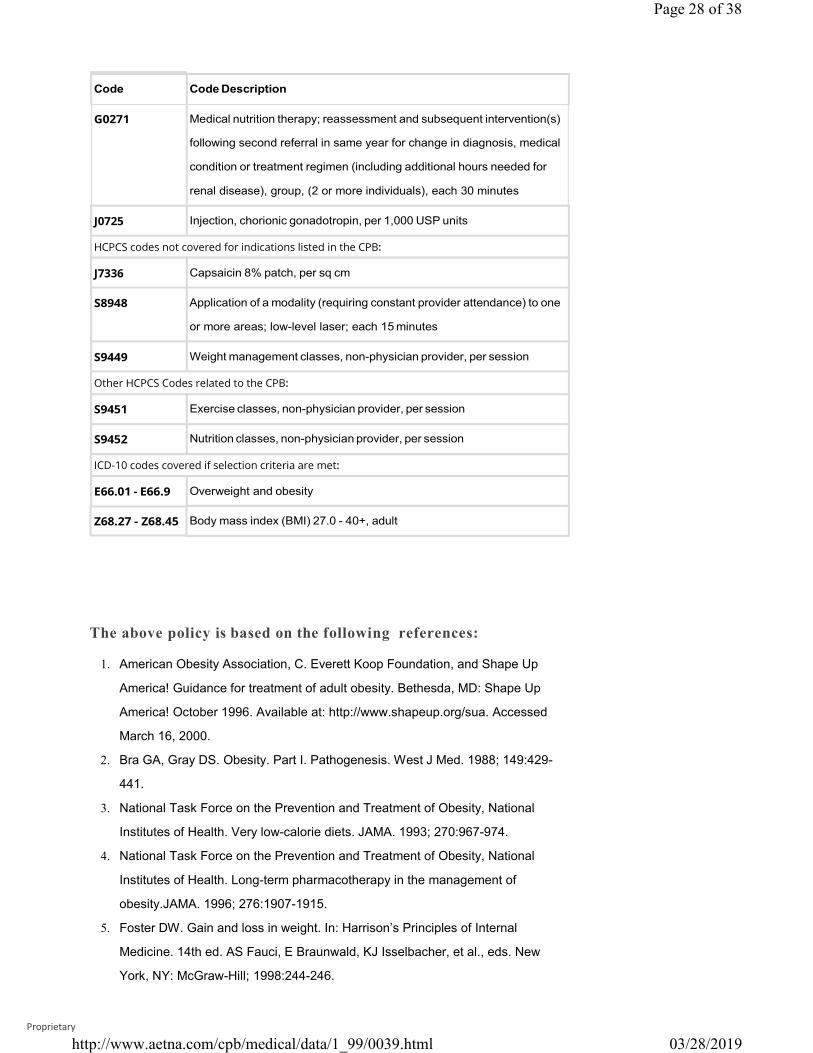
G0270 Medical nutrition therapy; reassessment and subsequent intervention(s)
following second referral in same year for change in diagnosis, medical
condition or treatment regimen (including additional hours needed for
renal disease), individual, face to face with patient, each 15 minutes
03/28/2019
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 28 of 38
J0725
HCPCS codes not covered for indications listed in the CPB:
J7336
Other HCPCS Codes related to the CPB:
ICD-10 codes covered if selection criteria are met:
The above policy is based on the following references:
1. American Obesity Association, C. Everett Koop Foundation, and Shape Up
America! Guidance for treatment of adult obesity. Bethesda, MD: Shape Up
America! October 1996. Available at: http://www.shapeup.org/sua. Accessed
March 16, 2000.
2. Bra GA, Gray DS. Obesity. Part I. Pathogenesis. West J Med. 1988; 149:429-
441.
3. National Task Force on the Prevention and Treatment of Obesity, National
Institutes of Health. Very low-calorie diets. JAMA. 1993; 270:967-974.
4. National Task Force on the Prevention and Treatment of Obesity, National
Institutes of Health. Long-term pharmacotherapy in the management of
obesity.JAMA. 1996; 276:1907-1915.
5. Foster DW. Gain and loss in weight. In: Harrison’s Principles of Internal
Medicine. 14th ed. AS Fauci, E Braunwald, KJ Isselbacher, et al., eds. New
York, NY: McGraw-Hill; 1998:244-246.
03/28/2019
/data/1_99/0039.html
Proprietary
http://www.aetna.com/cpb/medical
Page 29 of 38
6. U.S. Department of Agriculture and U.S. Department of Health and Human
Services. Nutrition and your health: Dietary guidelines for Americans. 3rd ed.
Home and Garden Bulletin. No. 232. Washington, DC: U.S. Government
Printing Office; 1990.
7. Goldstein DJ, Potvin JH. Long-term weight loss: The effect of pharmacologic
agents. Am J Clin Nutr. 1994;60(5):647-657.
8. Silverstone T. Appetite suppressants: A review. Drugs. 1992;43(6):820-836.
9. United States Pharmacopeial Convention, Inc. Appetite suppressants
(systemic). In: USP DI: Drug Information for the Health Care Professional.
19th ed. Rockville, MD: United States Pharmacopeial Convention; 1999: 452-
459.
10. No author listed. Weight control. In: Introductory Nutrition and Diet Therapy.
2nd ed. MM Eschleman, ed. Philadelphia, PA: J.B. Lippincott Co.
;1991;368.
11. No author listed. Metabolic drugs: Drugs used in obesity. In: AMA Drug
Evaluations Subscription. DR Bennett, ed. Chicago, IL: American Medical
Association (AMA); 1992: III/MET 6:7.
12. Scheen AJ, Desaive C, Lefebvre PJ. Therapy for obesity--today and
tomorrow. Baillieres Clin Endocrinol Metab. 1994;8(3):705-727.
13. Bjorntorp P. Treatment of obesity. Int J Obes Relat Metab Disord. 1992;16
(suppl 3):S81-S84.
14. Bray GA. Use and abuse of appetite-suppressant drugs in the treatment of
obesity. Ann Intern Med. 1993;119(7 pt 2):707-713.
15. Mosby-Year Book, Inc. Mosby’s GenRx: The Complete Reference for Generic
and Brand Drugs. 8th ed. St. Louis, MO: Mosby; 1998.
16. American Society of Health-System Pharmacists, Inc. American Hospital
Formulary Service Drug Information 98. Bethesda, MD: American Society of
Health-System Pharmacists; 1998.
17. U.S. Department of Health and Human Services, National Institutes of Health
(NIH). Clinical guidelines on the identification, evaluation, and treatment of
overweight and obesity in adults. National Heart, Lung, and Blood Institute and
National Institute of Diabetes and Digestive and Kidney Diseases. Bethesda,
MD: NIH; June 1998.
18. Jarvis M, McNaughton L, Seddon A, Thompson D. The acute 1-week effects
of the Zone diet on body composition, blood lipid levels, and performance in
recreational endurance athletes. J Strength Cond Res. 2002;16(1):50-57.
19. Haller C, Schwartz JB. Pharmacologic agents for weight reduction. J Gend
Specif Med. 2002;5(5):16-21.
03/28/2019
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Page 30 of 38
20. Shepherd TM. Effective management of obesity. J Fam Pract. 2003;52(1):34-
42.
21. Heshka S, Anderson JW, Atkinson RL, et al. Weight loss with self-help
compared with a structured commercial program: A randomized
trial. JAMA. 2003;289(14):1792-1798.
22. Institute for Clinical Systems Improvement (ICSI). Pharmacological
approaches to weight loss in adults. Technology Assessment Report No. 71.
Bloomington, MN: ICSI; February 2003.
23. Asp N G, Bjorntorp P, Britton M, et al. Obesity - problems and interventions.
SBU Report No. 160. Stockholm, Sweden: Swedish Council on Technology
Assessment in Health Care (SBU); 2002.
24. O’Meara S, Riemsma R, Shirran L, et al. A rapid and systematic review of the
clinical effectiveness and cost-effectiveness of orlistat in the management of
obesity. Health Technol Assess. 2001;5(18):1-81.
25. NHS Centre for Reviews and Dissemination (CRD). The prevention and
treatment of childhood obesity. Effective Health Care. York, UK: CRD; 2002; 7
(6).
26. U.S. Preventive Services Task Force. Screening for obesity in adults:
Recommendations and rationale. Ann Intern Med. 2003;139(11):930-932.
27. U.S. Preventive Services Task Force. Behavioral counseling in primary care to
promote a healthy diet: Recommendations and rationale. Am J Prev Med.
2003;24(1):93-100.
28. U.S. Preventive Services Task Force. Behavioral counseling in primary care to
promote physical activity: Recommendation and rationale. Ann Intern Med.
2002;137(3):205-207.
29. American Gastroenterological Association medical position statement on
obesity. Gastroenterology. 2002;123(3):879-881.
30. National Institute for Clinical Excellence (NICE). Guidance on the use of
orlistat for the treatment of obesity in adults. Technology Appraisal
Guidance No.22. London, UK: NICE; 2001.
31. O'Meara S, Riemsma R, Shirran L, et al. The clinical effectiveness and cost-
effectiveness of sibutramine in the management of obesity: A technology
assessment. Health Technol Assess. 2002;6(6):1-97.
32. Shekelle P, Morton S, Maglione M. Ephedra and ephedrine for weight loss
and athletic performance enhancement: Clinical efficacy and side effects.
Evidence Report/Technology Assessment 76. Rockville, MD: Agency for
Healthcare Research and Quality (AHRQ); 2003.
03/28/2019
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html 03/28/2019
Page 31 of 38
33. McTigue K, Harris R, Hemphill MB, et al. Screening and interventions for
overweight and obesity in adults. Preventive Services Task Force Systematic
Evidence Review No. 21. Rockville, MD: Agency for Healthcare Research and
Quality (AHRQ); 2003.
34. Jain A. What works for obesity? A summary of the research behind obesity
interventions. London, UK: BMJ Publishing Group Ltd.; April 30, 2004.
35. Institute for Clinical Systems Improvement (ICSI). Diet programs for weight
loss in adults. Technology Assessment Report
No.83.Bloomington, MN: ICSI; August2004.Availableat:http://www.icsi.org/knowledge/detail.asp?
catID=107&itemID=1742. Accessed September 21, 2004.
36. Avenell A, Broom J, Brown TJ, et al. Systematic review of the long-term effects
and economic consequences of treatments for obesity and implications for
health improvement. Health Technol Assess. 2004;8(21): iii-iv, 1-182.
37. O'Meara S, Riemsma R, Shirran L, et al. A systematic review of the clinical
effectiveness of orlistat used for the management of obesity. Obes Rev.
2004;5(1):51-68.
38. Padwal R, Li SK, Lau DC. Long-term pharmacotherapy for obesity and
overweight. Cochrane Database Syst Rev. 2004;(3):CD004094.
39. Pittler MH, Ernst E. Dietary supplements for body-weight reduction: A
systematic review. Am J Clin Nutr. 2004;79(4):529-536.
40. Smartt P. Evidence based review of weight loss medicines: A report
commissioned by the New Zealand Accident Compensation Corporation
(ACC). NZHTA Report. Christchurch, New Zealand: New Zealand Health
Technology Assessment (NZHTA); 2004;7(6).
41. Day P. What is the evidence for the safety and effectiveness of surgical and
non-surgical interventions for patients with morbid obesity? NZHTA Technical
Brief Series. Christchurch, New Zealand: New Zealand Health Technology
Assessment (NZHTA); 2005;4(1).
42. Institute for Clinical Systems Improvement (ICSI). Diet programs for weight loss
in adults. Technology Assessment Report No. 83. Bloomington, MN: ICSI;
March 2004.
43. Institute for Clinical Systems Improvement (ICSI). Behavioral therapy
programs for weight loss in adults. Technology Assessment Report
No.87. Bloomington,MN:ICSI; January2005. Available at:
http://www.icsi.org/knowledge/detail.asp?catID=107&itemID=1993. Accessed
February 7, 2006.
44. Institute for Clinical Systems Improvement (ICSI). Treatment of obesity in
children and adolescents. Technology Assessment Report
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html 03/28/2019
Page 32 of 38
No.90. Bloomington, MN: ICSI;2005. Available at:
http://www.icsi.org/knowledge/detail.asp?catID=107&itemID=2243. Accessed
February 7, 2006.
45. McTigue K M, Hess R, Ziouras J. Diagnosis and treatment of obesity in the
elderly. Health Technology Assessment. Rockville, MD: Agency for Healthcare
Research and Quality (AHRQ); December 18, 2003. Available at:
http://www.cms.hhs.gov/mcd/viewtechassess.asp?where=search&tid=23.
Accessed January 15, 2008.
46. Shekelle PG, Morton SC, Maglione MA, et al. Pharmacological and surgical
treatment of obesity. Evidence Report/Technology Assessment No. 103.
Prepared by the Southern California–RAND Evidence-Based Practice Center,
Santa Monica, CA, under contract no. 290-02-0003. AHRQ Publication No. 04-
E028-2. Rockville, MD: Agency for Healthcare Research and Quality; July
2004.
47. Snow V, Barry P, Fitterman N, et al. Pharmacologic and surgical management
of obesity in primary care: A clinical practice guideline from the American
College of Physicians. Ann Intern Med. 2005:142(7):525-531.
48. Li Z, Maglione M, Tu W, et al. Meta-analysis: Pharmacologic treatment of
obesity. Ann Intern Med. 2005;142(7):532-546.
49. Tsai AG, Wadden TA. Systematic review: An evaluation of major commercial
weight loss programs in the United States. Ann Intern Med. 2005;142(1):56-
66.
50. Whitlock EP, Williams SB, Gold R, et al. Screening and interventions for
childhood overweight: A summary of evidence for the US Preventive Services
Task Force. Pediatrics. 2005;116(1): e125-e144.
51. Wadden TA, Berkowitz RI, Womble LG, et al. Randomized trial of lifestyle
modification and pharmacotherapy for obesity. N Engl J Med. 2005;353
(20):2111-2120.
52. Swedish Council on Technology Assessment in Healthcare (SBU).
Interventions to prevent obesity: A systematic review. Stockholm, Sweden;
SBU; 2005.
53. Ioannides-Demos LL, Proietto J, Tonkin AM, McNeil JJ. Safety of drug
therapies used for weight loss and treatment of obesity. Drug Saf. 2006;29
(4):277-302.
54. Abell TL, Minocha A, Abidi N. Looking to the future: Electrical stimulation for
obesity. Am J Med Sci. 2006;331(4):226-232.
55. Dixon JB. Weight loss medications--where do they fit in? Aust Fam Physician.
2006;35(8):576-579.
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html 03/28/2019
Page 33 of 38
56. Blissmer B, Riebe D, Dye G, et al. Health-related quality of life following a
clinical weight loss intervention among overweight and obese adults:
Intervention and 24-month follow-up effects. Health Qual Life Outcomes.
2006; 4:43.
57. Arterburn DE, DeLaet DE, Schauer DP. Obesity. In: BMJ Clinical Evidence.
London, UK: BMJ Publishing Group; July 2005.
58. National Institute for Health and Clinical Excellence (NICE). Obesity: The
prevention, identification, assessment and management of overweight and
obesity in adults and children. Clinical Guideline 43. London, UK: NICE; 2006.
59. Lambert M-L, Kohn L, Vinck I, et al. Pharmacological and surgical treatment of
obesity. Residential care for severely obese children in Belgium. KCE Reports
36. Brussels, Belgium: Belgian Health Care Knowledge Centre (KCE); 2006.
60. Dansinger ML, Tatsioni A, Wong JB, et al. Meta-analysis: The effect of dietary
counseling for weight loss. Ann Intern Med. 2007;147(1):41-50.
61. Wilfley DE, Stein RI, Saelens BE, et al. Efficacy of maintenance treatment
approaches for childhood overweight: A randomized controlled trial. JAMA.
2007;298(14):1661-1673.
62. Whitlock EP, O'Connor EA, Williams SB, et al. Effectiveness of weight
management programs in children and adolescents. Evidence
Report/Technology Assessment No. 170. Prepared by the Oregon
Evidence-based Practice Center under Contract No. 290-02-0024. AHRQ
Publication No. 08-E014. Rockville, MD: Agency for Healthcare Research
and Quality (AHRQ); September 2008.
63. Orozco LJ, Buchleitner AM, Gimenez-Perez G, et al. Exercise or exercise
and diet for preventing type 2 diabetes mellitus. Cochrane Database Syst
Rev. 2008;(3):CD003054.
64. Ball SD, Altena TS. Comparison of the BOD POD and dual energy x-ray
absorptiometry in men. Physiol Meas. 2004;25(3):671-678.
65. Williams JE, Wells JC, Wilson CM, et al. Evaluation of Lunar Prodigy dual-
energy X-ray absorptiometry for assessing body composition in healthy
persons and patients by comparison with the criterion 4-component
model. Am J Clin Nutr. 2006;83(5):1047-1054.
66. Ritz P, Sallé A, Audran M, Rohmer V. Comparison of different methods to
assess body composition of weight loss in obese and diabetic patients.
Diabetes Res Clin Pract. 2007;77(3):405-411.
67. Pineau JC, Guihard-Costa AM, Bocquet M. Validation of ultrasound
techniques applied to body fat measurement. A comparison between
ultrasound techniques, air displacement plethysmography and
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html 03/28/2019
Page 34 of 38
bioelectrical impedance vs. dual-energy X-ray absorptiometry. Ann Nutr
Metab. 2007;51(5):421-427.
68. Pineau JC, Filliard JR, Bocquet M. Ultrasound techniques applied to body
fat measurement in male and female athletes. J Athl Train. 2009;44(2):142
147.
69. U.S. Food and Drug Administration (FDA). Meridia (sibutramine
hydrochloride) information. Postmarketing drug safety information for
patients and providers. Rockville, MD: FDA; updated October 8, 2010.
70. Rogovik AL, Chanoine JP, Goldman RD. Pharmacotherapy and weight-loss
supplements for treatment of paediatric obesity. Drugs. 2010;70(3):335
346.
71. Whitlock EP, O'Connor EA, Williams SB, et al. Effectiveness of weight
management interventions in children: A targeted systematic review for
the USPSTF. Pediatrics. 2010;125(2): e396-e418.
72. Balazs A. Role of phytotherapy in the prevention and treatment of obesity.
Orv Hetil. 2010;151(19):763-773.
73. Borel AL, Nazare JA, Smith J, et al. Improvement in insulin sensitivity
following a 1-year lifestyle intervention program in viscerally obese men:
Contribution of abdominal adiposity. Metabolism. 2012;61(2):262-72.
74. Garvey WT, Ryan DH, Look M, et al. Two-year sustained weight loss and
metabolic benefits with controlled-release phentermine/topiramate in
obese and overweight adults (SEQUEL): A randomized, placebo-controlled,
phase 3 extension study. Am J Clin Nutr. 2012;95(2):297-308.
75. Mulholland Y, Nicokavoura E, Broom J, Rolland C. Very-low-energy diets
and morbidity: A systematic review of longer-term evidence. Br J Nutr.
2012;108(5):832-851.
76. Fioravante M, Alegre SM, Marin DM, et al. Weight loss and resting energy
expenditure in patients with chronic hepatitis C before and during
standard treatment. Nutrition. 2012;28(6):630-634.
77. Bruera E, Dev R. Palliative care: Assessment and management of anorexia
and cachexia. UpToDate [serial online]. Waltham, MA: UpToDate; reviewed
October 2013.
78. Yanovski SZ, Yanovski JA. Long-term drug treatment for obesity: A
systematic and clinical review. JAMA. 2014;311(1):74-86.
79. Whiting S, Derbyshire EJ, Tiwari B. Could capsaicinoids help to support
weight management? A systematic review and meta-analysis of energy
intake data. Appetite. 2014; 73:183-188.
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html 03/28/
Page 35 of 38
80. Onakpoya I, Posadzki P, Ernst E. The efficacy of glucomannan
supplementation in overweight and obesity: A systematic review and meta-
analysis of randomized clinical trials. J Am Coll Nutr. 2014a;33(1):70- 78.
81. Onakpoya I, Hunt K, Wider B, Ernst E. Pyruvate supplementation for weight
loss: A systematic review and meta-analysis of randomized clinical trials.
Crit Rev Food Sci Nutr. 2014b;54(1):17-23.
82. Novo Nordisk Inc. Novo Nordisk receives FDA approval for Saxenda
(liraglutide [rDNA origin] injection) for chronic weight management. Press
Relsease. Plainsboro, NJ: Novo Nordisk; December 24, 2014.
83. U.S. Food and Drug Administration (FDA). FDA approves weight-
management drug Saxenda. Press Release. Silver Spring, MD: FDA;
December 23, 2014.
84. Jensen MD, Ryan DH, Apovian CM, et al.; American College of
Cardiology/American Heart Association Task Force on Practice Guidelines;
Obesity Society. 2013 AHA/ACC/TOS guideline for the management of
overweight and obesity in adults: A report of the American College of
Cardiology/American Heart Association Task Force on Practice Guidelines
and The Obesity Society. Circulation. 2014;129(25 Suppl 2):S102-S138.
85. National Institute for Health and Care Excellence (NICE). Obesity:
Identification, assessment and management of overweight and obesity in
children, young people and adults. NICE Clinical Guidance No. 189.
London, UK: NICE; November 2014.
86. Lingwood BE. Bioelectrical impedance analysis for assessment of fluid
status and body composition in neonates -- the good, the bad and the
unknown. Eur J Clin Nutr. 2013;67 Suppl 1: S28-S33.
87. de Miguel-Etayo P, Moreno LA, Iglesia I, et al. Body composition changes
during interventions to treat overweight and obesity in children and
adolescents: A descriptive review. Nutr Hosp. 2013;28(1):52-62.
88. Talma H, Chinapaw MJ, Bakker B, et al. Bioelectrical impedance analysis to
estimate body composition in children and adolescents: A systematic
review and evidence appraisal of validity, responsiveness, reliability and
measurement error. Obes Rev. 2013;14(11):895-905.
89. Goldberg LR, Heiss CJ, Parsons SD, et al. Hydration in older adults: The
contribution of bioelectrical impedance analysis. Int J Speech Lang Pathol.
2014;16(3):273-281.
2019
Proprietary
http://www.aetna.com/cpb/medical/data/1_99/0039.html 0
Page 36 of 38
90. Buffa R, Mereu E, Comandini O, et al. Bioelectrical impedance vector
analysis (BIVA) for the assessment of two-compartment body composition.
Eur J Clin Nutr. 2014;68(11):1234-1240.
91. Haverkort EB, Reijven PL, Binnekade JM, et al. Bioelectrical impedance
analysis to estimate body composition in surgical and oncological patients:
A systematic review. Eur J Clin Nutr. 2015;69(1):3-13.
92. Gibson AA, Seimon RV, Lee CM, et al. Do ketogenic diets really suppress
appetite? A systematic review and meta-analysis. Obes Rev. 2015;16(1):64
76.
93. Bueno NB, de Melo IV, Florêncio TT, Sawaya AL. Dietary medium-chain
triacylglycerols versus long-chain triacylglycerols for body composition in
adults: Systematic review and meta-analysis of randomized controlled
trials. J Am Coll Nutr. 2015;34(2):175-183.
94. Mumme K, Stonehouse W. Effects of medium-chain triglycerides on weight
loss and body composition: A meta-analysis of randomized controlled trials.
J Acad Nutr Diet. 2015;115(2):249-263.
95. Wilms B, Schmid SM, Ernst B, et al. Poor prediction of resting energy
expenditure in obese women by established equations. Metabolism.
2010;59(8):1181-1189.
96. Henes ST, Johnson A, Toner M, et al. Assessing Resting Metabolic Rate in
Overweight and Obese Adolescents with a Portable Indirect Calorimeter: A
Pilot Study for Validation and Reliability. Nutr Clin Pract. 2016;31(3):355- 361.
97. Frankenfield D, Roth-Yousey L, Compher C. Comparison of predictive
equations for resting metabolic rate in healthy nonobese and obese
adults: A systematic review. J Am Diet Assoc. 2005;105(5):775-789.
98. McDoniel SO, Nelson HA, Thomson CA. Employing RMR technology in a 90
day weight control program. Obes Facts. 2008;1(6):298-304.
99. Xenical (orlistat) Prescribing Information. South San Francisco, CA:
Genentech USA, Inc. August 2015.
100. Livingstone KM, Celis-Morales C, Lara J, et al. Associations between FTO
genotype and total energy and macronutrient intake in adults: A
systematic review and meta-analysis. Obes Rev. 2015;16(8):666-678.
101. Paravattil B, Wilby KJ, Turgeon R. Topiramate monotherapy for weight
reduction in patients with type 2 diabetes mellitus: A systematic review
and meta-analysis. Diabetes Res Clin Pract. 2016; 114:9-14.
3/28/2019
Proprietary
03/28/2019
Page 37 of 38
102. Khera R, Murad MH, Chandar AK, et al. Association of pharmacological
treatments for obesity with weight loss and adverse events: A systematic
review and meta-analysis. JAMA. 2016;315(22):2424-2434.
103. Xiang L, Wu H, Pan A, et al. FTO genotype and weight loss in diet and
lifestyle interventions: A systematic review and meta-analysis. Am J Clin
Nutr. 2016;103(4):1162-1170.
104. Livingstone KM, Celis-Morales C, Papandonatos GD, et al. FTO genotype
and weight loss: Systematic review and meta-analysis of 9563 individual
participant data from eight randomised controlled trials. BMJ. 2016;354:
i4707.
105. Croghan IT, Ebbert JO, Schroeder DR, et al. A randomized, open-label pilot
of the combination of low-level laser therapy and lorcaserin for weight loss.
BMC Obes. 2016; 3:42.
106. Stavrou S, Nicolaides NC, Papageorgiou I, et al. The effectiveness of a
stress-management intervention program in the management of
overweight and obesity in childhood and adolescence. J Mol Biochem.
2016;5(2):63-70.
107. Xiang L, Wu H, Pan A, et al. FTO genotype and weight loss in diet and
lifestyle interventions: A systematic review and meta-analysis. Am J Clin
Nutr. 2016;103(4):1162-1170.
108. Hobbins L, Hunter S, Gaoua N, Girard O. Normobaric hypoxic conditioning
to maximize weight loss and ameliorate cardio-metabolic health in obese
populations: A systematic review. Am J Physiol Regul Integr Comp Physiol.
2017;313(3):R251-R264.
http://www.aetna.com/cpb/medical/data/1_99/0039.html
Proprietary
Page 38 of 38
Copyright Aetna Inc. All rights reserved. Clinical Policy Bulletins are developed by Aetna to assist in administering plan
benefits and constitute neither offers of coverage nor medical advice. This Clinical Policy Bulletin contains only a partial,
general description of plan or program benefits and does not constitute a contract. Aetna does not provide health care
services and, therefore, cannot guarantee any results or outcomes. Participating providers are independent contractors in
private practice and are neither employees nor agents of Aetna or its affiliates. Treating providers are solely responsible
for medical advice and treatment of members. This Clinical Policy Bulletin may be updated and therefore is subject to
change.
Copyright © 2001-2019 Aetna Inc.
http://www.aetna.com/cpb/medical/data/1_99/0039.html 03/28/2019
AETNA BETTER HEALTH® OF PENNSYLVANIA
Amendment to Aetna Clinical Policy Bulletin Number: 0039 Weight
Reduction Medications and Programs
There are no amendments for Medicaid.
www.aetnabetterhealth.com/pennsylvania annual 04/01/2019
Proprietary