body plethysmography - ssu.ac.ir · pdf filethe primary function of whole-body plethysmographs...
TRANSCRIPT

The primary function of whole-body plethysmographs is themeasurement of intrathoracic gasvolume (TGV) and volume change.Different models of whole-bodyplethysmograph (or “body box”)are used to measure changes inlung volume, from mL to L.
The first reports ofplethysmography describedmeasurement of thoracic gasvolume (TGV) [1] and airwayresistance (Raw) [2]. Volumechanges of mL were measured interms of associated changes in boxand alveolar pressures (PA), usingthe constant-volume variable-pressure box. Changes in lungvolume during compression anddecompression of thoracic gas weremeasured while the subjectbreathed entirely within the box.
An alternative volume-displacement body box measuredvolume changes of the thoraxdirectly, including the mass of gas
flowing into and out of the lung andsimultaneous compression anddecompression of thoracic gas(“Mead box”), with the subjectbreathing in and out across the wallof the box [3]. The Mead box
BODY PLETHYSMOGRAPHY03
30 THE BUYERS’ GUIDE TO RESPIRATORY CARE PRODUCTS
BODY PLETHYSMOGRAPHYM.D. Goldman
CorrespondenceM.D. Goldman
University of California Los AngelesDepartment of Medicine
Center for Health Sciences, Los AngelesCA 90095
USA
E-mail: [email protected]
TLC
RV
Box Volume Change
Mou
th fl
ow
Figure 1. A schematic representation offorced vital capacity in a patient withchronic obstructive pulmonary disease in a"Mead" box. Not changes in box volume atzero mouth flow. See text for discussion.TLC: total lung capacity; RV: residualvolume.
BG-03 Plethysmography 6/8/07 20:26 Page 30

measured changes in TGV duringvital capacity (VC) efforts. Thisresults in a “different” VC to thatobtained by integration of airflow.Figure 1 illustrates schematicallythat the VC estimated from mouthflow is less than the difference in boxvolume between TLC and residualvolume (RV), which includescompression of thoracic gas duringexpiration and decompression of thistrapped gas during initialinspiratory effort at RV.
Subsequent technology combinedthe above approaches, using apressure-compensated volume-displacement or integrated-flow box[4–9]. In the combination box,
subjects breathe either across thewall of the box to the outside (totalthoracic displacements) or within thebox to measure compressionvolumes only. Pressure change in thebox is added to the volumedisplaced through the box wall toprovide a measure of thoracicvolume displacements. Thepressure-compensated integratedflow is commonly called a“transmural” box and offers thegood frequency response of thepressure box with an ability tomeasure a wide range of volumedisplacements. Advances in theunderstanding of chronic obstructivepulmonary disease (COPD) have ledto renewed interest in the evaluation
of compression of TGV to betterunderstand dynamic events duringthe respiratory cycle; somemanufacturers offer this transmuralbox (table 1).
Principles of whole-bodyplethysmography
The body box consists of a rigidchamber, comparable in size andshape to an enclosed telephonebooth, in which the subject sits.Pressure transducers measure thepressure across apneumotachograph (flow), pressureacross the wall of the box, andpressure at the airway opening.
BODY PLETHYSMOGRAPHY
THE BUYERS’ GUIDE TO RESPIRATORY CARE PRODUCTS 31
03
Manufacturer Cosmed Medisoft/Pulmolink Viasys/Jaeger ZAN/nSpirehealth
Unique1 feature Regression Raw Panting Raw “instantaneous” Therm/Pres compNumber of testsa Unique sequencingb Raw (within breath)c Variable orifice flowd
Wheelchair access2 Yes Yes Yes No
Pressure-compensated No Yes No Yesintegrated-flow model3
Warm-up required4 No Yes Yes No
Compensation chamber Optional Optional Yes No
Optional5 PFTs Add unit Yes Yes Yes
Information from manufacturers (Cosmed, Medisoft/Pulmolink, Viasys/Jaeger, and ZAN/nSpirehealth) was provided in May, 2007.Specifications are subject to change from descriptions provided by manufacturers at that time. Specifications for Biomedin andMedGraphics plethysmographs were not available in response to direct enquiries, but may be available from their websites. Allmanufacturers provide all alternative measures of Raw (and sGaw) described below. All provide box calibration with a motorisedsyringe. All correct measured TGV for equipment deadspace. All provide user-choice of measuring sequence. All provide a wide varietyof optional additional pulmonary function testing, requiring extra costs for built-in or added-on PFT equipment. Manufacturers’specifications included below should be verified by personal correspondence with representatives of each company.1: Unique features of each manufacturer are best explained and verified by direct correspondence with company representatives. a: Cosmed provides all the usual measures of Raw listed in the text and in addition “Total Regression and Balanced Regression”measures. Any number of Raw tests can be included in one measure. b: Medisoft (mainland Europe) and Pulmolink (UK) provide forpanting Raw as primary choice, but also offer tidal breathing methods. They allow VC to be done before or after shutter closure, and torestart procedure if desired. VC measures can be imported and aligned at measured TLC. Software in US models differs from Europeanmodels. c: The “instantaneous Raw” described in the text below is provided with the same technical procedures and parameter listings.An additional graphic and numerical display of resistance as a function of absolute thoracic gas volume (R/V display) within the tidalbreathing excursions is provided. Pre- and post-bronchodilator measures can be superimposed on the same graphic representation. d: Rigid security glass walls with good thermal conductivity provide for patent-pending electronic compensation of both thermal andpressure signals, allowing rapid testing to begin without the usual 2-min warm-up. Unique variable-orifice flow meter provides very lowflow resistance and independence from humidity effects. Electronics in US models differs from European models.2: Extra-cost option where available.3: The pressure-compensated integrated-flow (“transmural box”) model is constructed separately (as an extra-cost option) from the usualconstant-volume body plethysmograph (“DuBois Box”) construction.4: Requirement for warm-up is a function of available software and hardware. The specific demands of each body plethysmograph,whether the “usual DuBois box” or “transmural box” should be discussed with the manufacturer’s technical experts. Differentmanufacturers state their requirements in rather different ways. Verification with manufacturer’s representatives is required.5: Options include DL,CO; resistance by interruption, also called resistance by occlusion; P0.1 measures; lung compliance measures; andautomated bronchial provocation testing. Cosmed provides these options through connection to its Quark PFT unit. Other manufacturersprovide some options available as built-in extra-cost features, and some as external add-on measurement techniques. Specific options arebest discussed directly with manufacturers’ representatives.
BG-03 Plethysmography 6/8/07 20:26 Page 31

In the variable-pressure box,changes in PA are inferred fromchanges in box pressure. A shutterclose to the mouth can be closed toocclude the airway transiently,during which voluntary respiratoryefforts performed against theclosed shutter are recorded(Mueller and Val Salvamanoeuvres), allowing changes inPA to be estimated by the change inmouth pressure (Pm). Pm is plottedagainst simultaneous box pressurechanges during respiratory effortsagainst a closed shutter to measureabsolute TGV. The relationshipbetween alveolar and box pressuremeasured during respiratory efforts against a closed shutter isextended to dynamic events duringbreathing to measure Raw, definedas the relationship between airflowand PA.
Three different types of whole-bodyplethysmograph have been used tomeasure changes in thoracicvolume: large volume changesduring the VC, or only those thatresult from compression/decompression of gas in the lungs.Different transducer sensitivitiesand mechanical arrangements areused to achieve this. The constant-volume (variable-pressure) bodybox measures small volumechanges due to compression/decompression of gas in the lungs.The constant-pressure (volume-displacement) body box (Mead box)measures only large changes inlung volume due to gas flow intoand out of the lungs. The pressure-corrected variable-volume bodybox, (transmural), combines theadvantages of the other types. Thesensitivity and rapid frequencyresponse of transmural boxesprovide measures of large slowvolume changes in the lungs duringbreathing as well as TGV and Raw,but not all manufacturers currentlyprovide this technology (table 1).The use of the pure volume-displacement body box (Mead box)does not provide the sine qua non ofclinical plethysmography, namelymeasurement of TGV and Raw. Itwill not be further discussed.
Box pressure transducers mustregister very small changes inpressure. If the total chambervolume of the box is ~800 L, andTGV is ~4 L, and respiratory effortsagainst the closed shutter producechanges in alveolar pressure of 2 kPa, then the change in TGV dueto compression/decompression is~80 mL. This 80 mL compressionvolume “signal” will cause achange in box pressure of 0.01 kPa.Thus mouth pressure changes are200 times box pressure changes.This ratio is directly related to theratio of TGV to box chambervolume.
With such sensitive transducers tomeasure changes in box pressure, itis logical that small changes inambient room air pressure maycause an artefact in box pressureduring patient testing. If the wallsof the box are very rigid and thebox is properly sealed, this can becompensated for by computeralgorithms. Alternatively, a physicalcompensation can be made forchanges in ambient room airpressure, using a “compensationchamber” (similar to the originalDuBois box). Table 1 lists methodsused by different manufacturers. Anadditional source of possible errorin box pressure is slowly occurringpressure changes unrelated torespiratory manoeuvres, such asheating of the interior caused by thepresence of a person inside thechamber. These changes may becompensated for by softwarealgorithms or by periodicallyventing the box to the room, orboth.
In practical use, the box pressuretransducer is calibrated in terms of changes in TGV by rapidintroduction and withdrawal of30–50 mL air into the box chamber,commonly using a motor-drivensyringe. After calibration, changesin box pressure reflect changes inTGV due to compression/decompression of thoracic gas.Changes in calibrated box pressureare usually recorded in terms of avolume change known as “shift
BODY PLETHYSMOGRAPHY03
32 THE BUYERS’ GUIDE TO RESPIRATORY CARE PRODUCTS
BG-03 Plethysmography 6/8/07 20:26 Page 32

volume”. Shift volume is the changein TGV due to compression/decompression during occludedrespiratory efforts, and also duringbreathing within the body box.Calibration of the body box isnormally done without a subject inthe chamber, and must be correctedfor the subject’s body volume, usingthe subject’s body mass to calculatethe final adjusted calibrationcoefficient.
Figures 2a and b are schematicrepresentations of a variable-pressure constant-volumeplethysmograph and a pressure-corrected integrated-flowplethysmograph. Frequencyresponse of box volume changes isachieved by adding a signalproportional to box pressure to theintegrated pneumotachographsignal in the wall of the box. Such apressure-corrected plethysmographpermits accurate measurement ofchanges in TGV during forcedexpiration manoeuvres. Occlusionof the pneumotachograph in thewall of the plethysmograph androuting the mouthflowpneumotachygraph back into thebox chamber converts the flowplethysmograph back into avariable-pressure plethysmograph,allowing more sensitivemeasurements of TGV and Raw.
The box pressure change requiredto drive air through a flow meter inthe wall of the box reflectscompression/decompression of boxair that does not reach equilibriumuntil box pressure has returned toatmospheric, as noted by Mead [3].Thus, as the subject breathes roomair through a tube across the wall ofthe box, changes in TGV expand orcompress box air, andsimultaneously displace some air inor out of the box across the flowmeter in its wall. The volumechange due to compression ordecompression of box air isaccounted for by adding anelectrical signal proportional to boxpressure to the integrated flowacross the wall of the box (thus,“pressure-corrected”) [4–7].
BODY PLETHYSMOGRAPHY
THE BUYERS’ GUIDE TO RESPIRATORY CARE PRODUCTS 33
03
Shutter
ControlledMechanical Leak
CalibrationSyringe
ReferenceChamber
V’Pm
PV
P
VL
Raw
Raw
TGV
CalibrationSyringe
ReferenceChamber
P
Shutter
V’Pm
VP
VL
Raw
Raw
TGV
a)
b)
Figure 2. Schematic representation of: a) a variable-pressure constant-volumeplethysmograph; and b) a pressure-corrected integrated-flow plethysmograph. (a) illustratesthe controlled mechanical leak to room air and optional reference chamber. The subjectbreathes through a pneumotachygraph entirely within the box chamber. Recording of volumedisplacements of the thorax is limited to compression and decompression of thoracic gas.Calibration of plethysmographic pressure is done via a motorised syringe inserting andwithdrawing 30–50 mL of air into the box chamber at a frequency of 1–3 Hz. (b) Arrowsillustrate differences in the pressure-corrected integrated-flow plethysmograph showing thesubject’s breathing through the wall of the box to room air with an additionalpneumotachygraph recording changes in box volume. Recording of volume displacements ofthe thorax includes mass of gas airflow into and out from the lung, and compression/decompression of thoracic gas V': flow; PA: alveolar pressure; Pm: mouth pressure; VL: lungvolume; Raw: airway resistance; TGV: thoracic gas volume; �V: change in volume; �P:change in pressure.
BG-03 Plethysmography 6/8/07 20:26 Page 33
Pressure-corrected integrated-flowbody (transmural) boxes providesensitive recordings of pressure andvolume events over a wide range ofvolume displacements, includingmaximal expiratory flow volumecurves and measurement of TGV,specific airway resistance (sRaw)and Raw with the same instrument.They permit evaluation ofdifferences between thoracic gascompression and airway closure,the so-called “trapped gas” [10].
Clinical use ofplethysmography
After the subject has entered theplethysmograph, the door is closedwith an airtight seal. Some bodyboxes require ~2 min for chamberpressure to equilibrate duringwarming and humidification ofchamber air by the subject. Duringthis initial period, theplethysmograph cabin is ventedperiodically to room air via asolenoid-operated valve. Afterequilibration of box pressure, thesubject is asked to close his/her lipstightly around the mouthpiece andbreathe normally through thepneumotachygraph. The patient sitserect with head and neck in aneutral posture. A nose-clip isapplied to close the nares. Patientsmay require reassurance inadapting to breathing within anairtight box, prior to making clinicalmeasurements.
Clinical body box measurementsinclude three measuring sequenceswhose order may be defined by theuser. sRaw is usually measured first,followed by measurement of TGVand finally, measurement of slowand forced vital capacities.
Measurement of TGV
As described initially by DuBois etal. [1], measurement of TGV is donein the body box using BoyleMariotte’s law relating pressure andvolume changes under isothermalconditions. During compression of
thoracic gas, PA rises, and theproduct of pressure and volumeremains constant. In the body box,respiratory efforts against the closedshutter produce changes in alveolarpressure, which are closely similarto Pm changes, and are associatedwith reciprocal changes in TGV:TGV is decompressed andcompressed, causing correspondingchanges in box pressure, which arerecorded in terms of the change inTGV, denoted as “shift volume”.
In normal subjects, change in Pm
closely approximates that in PA
during panting efforts [1]. However,in patients with airflow obstruction,significant differences betweenchanges in oesophageal pressureand Pm occur during panting effortsagainst a closed shutter [11–16]. Ifpanting efforts are done slowly (1 Hz), it is possible to measurechanges in PA from Pm. Pm (PA) isplotted against simultaneous boxpressure changes (measured as shiftvolume) during respiratory effortsagainst a closed shutter to measureabsolute TGV.
Boyle Mariotte’s law states that theproduct of pressure and volume isconstant under isothermalconditions. In the body box,respiratory efforts against the closedshutter change PA and TGV bysmall amounts. These changes areshown in equation (1):
PAxTGV = (PA – �PA)x(TGV + �TGV) (1)
After expanding and rearrangingequation (1):
TGV = (�V / �PA)x(PA – �PA) (2)
The terms in equation (2) aredefined as follows:
TGV is the absolute intrathoracicgas volume to be measured(calculated).
PA is alveolar pressure at rest(before any occluded respiratoryefforts). It is important to note
BODY PLETHYSMOGRAPHY03
34 THE BUYERS’ GUIDE TO RESPIRATORY CARE PRODUCTS
Shift Volume mL
3
2
1
0
-1
-2
-3
Mou
th P
ress
ure
k
Pa
-40 -20 0 20 40
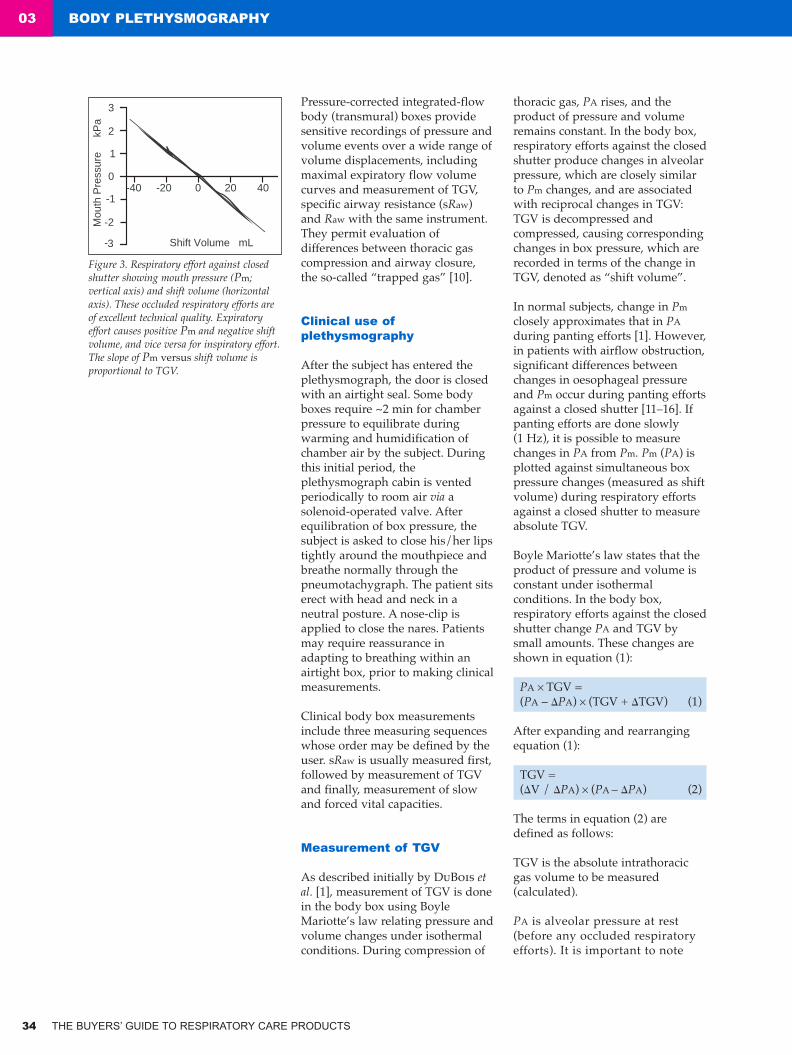
Figure 3. Respiratory effort against closedshutter showing mouth pressure (Pm;vertical axis) and shift volume (horizontalaxis). These occluded respiratory efforts areof excellent technical quality. Expiratoryeffort causes positive Pm and negative shiftvolume, and vice versa for inspiratory effort.The slope of Pm versus shift volume isproportional to TGV.
BG-03 Plethysmography 6/8/07 20:26 Page 34

Figure 4. Specific resistance loops in a) anormal subject; b) a subject with increasedlarge airway resistance; and c) a patientwith chronic airflow obstruction.
that at resting end-expiratorylung volume (EELV) with theairway open to atmosphere, PA
is not “zero” but rather is equal to atmospheric pressure, ~100kPa.
�PA is the change in alveolarpressure during the occludedrespiratory effort, measured aschange in Pm.
�TGV (or �V) is the change inthoracic gas volume during theoccluded respiratory effort. Thischange in volume, as noted above,will be 40–80 mL. It is equal andopposite to the change in boxvolume occurring simultaneously inthe airtight body box. This“volume” change is measured bythe box pressure transducer, as theshift volume.
Because �PA is very smallcompared to PA (~2%) it is usuallyomitted in the differential term.
The measurement procedure fordetermining TGV requiressubstantial subject cooperation,making respiratory efforts whileventilation is interrupted by theclosed shutter. Therefore, TGV mayvary from test to test.
In contrast, residual volume (RV)and total lung capacity (TLC)require less subject coordination. Aninspiratory capacity (IC) effort maybe made immediately after shutteropening following the TGVmeasurement, to measure TLC. RVmay then be obtained bysubtracting a subsequent slow VC(SVC) from TLC, or alternatively bysubtracting an independentlymeasured SVC from TLC, to avoidintegrator drift during exhalation toRV in the box.
Control of shutter closure in mostbody boxes includes a program toreopen after a defined occlusionduration or number of zero-pressure crossings, to minimisepatient discomfort and avoid thesubject experiencing fear when(s)he is trying to breathe but the
shutter is closed! Subjects shouldalways be informed to remove themouthpiece from their mouth in theevent the shutter does not open or ifthe subject senses substantialdifficulty breathing. The shiftvolume and the corresponding Pm
changes during shutter closure aredisplayed on an X–Y graph infigure 3, demonstrating excellentquality and patient cooperation.
As in all pulmonary functionevaluations, it is recommended thatthree replicates of the measurementof TGV are recorded and saved.Measurement quality is reflected inlarge part by the variability ofreplicate trials. QUANJER et al. [17]suggest a maximal deviation of 5%between the individual trials.
Measurement of sRaw
Thermal and humidity effects ariseduring inspiration ofplethysmographic air andexpiration of warm humid alveolarair. Electronic compensation forthermal and humidity effectspermits tidal breathing duringmeasurement of sRaw [18]; andcurrent whole-bodyplethysmographs commonlyincorporate algorithms tocompensate for these effects.
Mouth flow during spontaneousbreathing is continuously recordedfrom the pneumotachygraph anddisplayed on a graphic X–Y
BODY PLETHYSMOGRAPHY
THE BUYERS’ GUIDE TO RESPIRATORY CARE PRODUCTS 35
03
Shift Volume mL
Flow
L·
s-1
2
1
0
-1
-2
a) b) c)
BG-03 Plethysmography 6/8/07 20:26 Page 35

display versus the shift volumeproduced by thoracic compressionand decompression as shown infigure 4. As noted above, shiftvolume excludes lung volumechange due to gas flow in and outof the lung. The sRaw loop isinfluenced by Raw and TGV and itsinclination rotates clockwise ifeither Raw or TGV or both areincreased.
During assessment of sRaw, therelationship between airflow andshift volume described by DUBOIS etal. [2] defines not Raw, but sRaw.Currently, sRaw is most oftendefined during tidal breathing,without rapid shallow respirations.sRaw is given by the slope of themouth pressure versus shift volumeloops shown in figure 4 (correctedby the body box computer to referto “dry” gas). Different numerical“slopes” may be calculated from thesRaw loop shown for a patient withchronic airflow obstruction (fig. 4c),depending on which portion of theloop is chosen.
Subjects should sit upright andavoid neck flexion or rotation. Fiveto ten sRaw loops should berecorded as one trial. Normally,three replicate trials are recordedand saved. Optimal quality of therecording is achieved when sRaw
loops are regular and reproduciblewith the loop nearly closed,although patients with significantairflow obstruction manifest openloops during expiration.
While loops shown in figures 4aand b appear as nearly linear flatloops, the sRaw loop is complex inthe presence of peripheral airwaydisease, as described by DUBOIS etal. [2]. Since the sRaw loop includesvarying flows throughout the tidalbreathing respiratory cycle,different investigators have useddifferent portions of the loop toapproximate a “representative”value for the entire cycle.
The total specific resistance (sRtot)[19] and effective specific resistance(sReff) [20] are both utilised inclinical laboratories in Europe. InNorth America, the linear portion ofthe sRaw loop between inspiratoryand expiratory flow rates of 0.5 L·s-1
[21, 22] provides a linearapproximation of sRaw.
This last linear approximation(sR0.5) is shown in figure 5. It ismeasured between near end-inspiratory volume and the firstportion of expiration. sR0.5
standardises the flow at whichresistance is measured; and offersless interindividual variability.
In contrast, the sRtot, as describedby ISLAM and ULMER [19], isdetermined by a straight linebetween maximal inspiratory andmaximal expiratory shift volume,and is more sensitive to peripheralairways disease, but manifestsgreater variability from test to test.
The sReff was introduced byMATTHYS and ORTH [20]. Thisnumerical parameter is used tointegrate effects of variable flowsand nonlinearities of mouth
BODY PLETHYSMOGRAPHY03
36 THE BUYERS’ GUIDE TO RESPIRATORY CARE PRODUCTS
Shift Volume mL
2
1
0
-1
-2
-40 -20 0 20 40
+0.5 L·s-1
-0.5 L·s-1Flow
L·
s-1
Figure 5. A specific airway resistance (sRaw) loop during tidal breathing shown in a patientwith chronic airflow obstruction. The straight line is drawn tangent to a part of the sRaw loopbetween 0.5 L·s-1 inspiratory flow (above 0 flow) and 0.5 L·s-1 expiratory flow (below 0 flow).This tangent is only one way of choosing a numerical value for sRaw.
BG-03 Plethysmography 6/8/07 20:26 Page 36

flow-shift volume loops duringtidal breathing, using the quotientof the integrated shiftvolume–volume loop (flow resistivework of breathing) and theintegrated flow–volume loop. Thisratio reflects larger central airwayssomewhat more prominently thansRtot.
The reciprocal of sRaw is denotedspecific conductance (sGaw). Theconversion of sRaw to sGaw is basedon the original observations ofBriscoe and DuBois [23] that themajor determinant of Raw in normalsubjects is lung volume and,accordingly, that the relationshipbetween lung volume andconductance is linear within andbetween individuals. Thus, sGaw isa “volume-normalised” expressionfor airway conductance.
Since both resistance and restingEELV may change during bronchialor therapeutic challenge, sRaw andsGaw provide useful practicalassessments of airway responsivity,even in the absence of adetermination of absolute TGV.Such measures of airway responseduring tidal breathing are oftenconsidered preferable to spirometricassessments [24].
Calculation of airway resistance,Raw, is simply by dividing sRaw byTGV. Thus as noted above,calculation of Raw requires choosinga numerical approximation to thesRaw loop, and knowledge of TGV,determined by respiratory effortsagainst a closed shutter.
In practice, measurements of TGVare conveniently performedimmediately after the sRaw
breathing loops; and threereplicates are recommended.Quality of the measurement isreflected in part by the variabilityof replicate trials and, in part, byhow closely thePm–plethysmograph pressuretracing approximates a straight line.
By definition, inaccuracy in thedetermination of TGV will cause a
proportional error in Raw
calculations. For this reason, andbecause it is technically moredemanding for patients withairflow obstruction to makerespiratory efforts against a closedshutter than for tidal breathing,some clinicians restrict theirattention to sRaw and sGaw [19, 20,25, 26].
In many patients with COPD, Raw
appears to be nearly within normallimits, due to compensatory lunghyperinflation, especially whenmeasured between 0.5 L·s-1
inspiratory and expiratory flow. Inthese cases, sRaw and sGaw stillshow abnormality, because of theincreased TGV maintained duringtidal breathing.
Spirometric measurements may bemade in the body box after TGVhas been determined. An IC effortimmediately after shutterreopening defines absolute TLC.This may be followed immediatelyby a maximal forced expiratoryeffort to define forced expiratoryvolume in one second and forcedVC (FVC). These spirometric dataare recorded from the flow meterin the pressure box.
Using the transmural box it ispossible to view the maximalexpiratory flow–volume curve withrespect to volume displacements ofthe thorax, including compressioneffects, during forced expiration[27]. This is more reliable fordetecting expiratory flow limitation(EFL) during resting breathing thanspirometry using integrated mouthflow as the volume axis.
The VC measured from thoracicwall displacements in atransmural box is greater thanthat measured for integrated flow. This is not an artefact, andreflects compression of trappedgas, as shown schematically infigure 1.
Further discussion is provided inthe European Respiratory Monograph[28].
Clinical interpretation andemerging concepts of bodyplethysmography
Clinical utility of whole-bodyplethysmography is discussed byBRUSASCO and PELLEGRINO [29] andphysiological considerations arepresented in detail by PRIDE andMACKLEM [30].
The raison d’être of whole-bodyplethysmography is themeasurement of lung volumes.Accordingly, the first acknowledgedclinical benefit of bodyplethysmography is the definitionof restrictive lung disease [31].Normative data for TGV andpulmonary subdivisions allowdefinition of restrictive lung diseaseas distinct from obstructive, in thepresence of a reduced VC.
Definition of abnormally increasedlung volumes in obstructive lungdisease is a further appropriateclinical use of whole-bodyplethysmography. Because lungvolumes measured by gas dilutiontechniques measure only thevolume of ventilated airspaces,when plethysmography iscombined with dilution measures oflung volumes, the volume oftrapped gas is estimated by thedifference betweenplethysmographic and dilutionalTGV. The difference between FVCmeasured by transmural boxvolume change and that measuredby integrated mouth flow alsoprovides an estimate of trapped gasvolume.
The voluntary rapid shallowobstructed respiratory effortsdescribed by DUBOIS et al. [1]overestimate TGV because thechange in Pm underestimates thechange in PA [12, 13], in thepresence of intrathoracic airwayobstruction. In patients with airflowobstruction, changes in Pm
significantly underestimate those inthe oesophagus, taken to be equalto PA changes during respiratoryefforts against a closed shutter.Increased airflow obstruction,
BODY PLETHYSMOGRAPHY
THE BUYERS’ GUIDE TO RESPIRATORY CARE PRODUCTS 37
03
BG-03 Plethysmography 6/8/07 20:26 Page 37

increased compliance of the upperextrathoracic airways and increasedrate of panting all combine to causethe underestimation of PA changeby Pm, and consequentoverestimation of TGV. Thesestudies have resulted in arecommendation of panting at 1 Hzto optimise the measurement ofTGV.
The simplest form of BoyleMariotte’s Law used in manualcalculations of TGV [1] has beenevaluated by COATES et al. [32]who included calculation of TGVusing the complete BoyleMariotte’s law equation anddemonstrated errors in the orderof 3% during panting and 2–9%during a single inspiratory effortagainst a closed shutter asrecommended for children [33].Such discrepancies are not likelyto influence clinical decisions, butare easily avoided using moderncomputational methods inautomated whole-bodyplethysmographs [34].
The foregoing review of themeasurement of TGV emphasisedthe cooperation required of thepatient, including panting effortsagainst a closed shutter at acontrolled low frequency andmaintenance of an open glottisduring obstructed respiratoryefforts. Emerging concepts mayavoid these constraints in the futureby measuring TGV during tidalbreathing without obstructedrespiratory efforts [35]. Since sRaw isexpressed numerically by theproduct of TGV and Raw, additionof a known resistance in therespiratory path would permitdetermination of TGV bysubtraction. Because Raw = sRaw /TGV, sRaw is the product of TGVand Raw. By adding a knownresistance it is possible to compute:
sRaw1 = RawxTGV (3)
and
sRaw2 = (Raw + Radded)xTGV (4)
Thus: sRaw2 – sRaw1 = RaddedxTGV (5)
Or: TGV = (sRaw2 – sRaw1) / Radded (6)
The advantage of estimating lungvolume in this manner is that tidalbreathing only is required.However, TGV must be constantbetween tidal breathing withoutand with the added resistance. Itremains to be determined whethermodern computer-assisted bodyboxes will provide comparable TGVresults during respiratory effortsagainst a closed shutter and duringtidal breathing without and withadded resistance. This approachappears worthy of furtherinvestigation as it presents aconvenient approach to themeasurement of TGV that is likelyto be more easily applicable to awide variety of patients.
Calculation of Raw in a body boxdemands the constraints and linearapproximations described above,and a single number defining“resistance” is not entirelysatisfactory in patients withsubstantial peripheral airflowobstruction. Nonhomogeneous lungmechanical properties, EFL andairway closure all contribute to thecomplex shapes of sRaw loops. Thecomplex shape of the sRaw loopitself provides more informationthan approximations of the sRawslope in determining patients’pathophysiology.
Plethysmographic sRaw can bemeasured both during rapidshallow breathing (panting) andduring tidal breathing. The initialdescription of sRaw [2] utilisedrapid shallow breathing tominimise thermal effects. This hadthe advantage of resulting in fullopening of the vocal cords [36].However, controlling pantingfrequency at a rate of 1 Hz [17–22],increases the likelihood of variableglottic opening [36].
The clinical utility ofplethysmographic measurements of
Raw and sRaw is attested to by thefact that they have been consideredthe “gold standard” for decades forassessing airway function. Inpatients with significant airflowobstruction, sGaw is commonlyassessed. This permits lunghyperinflation to be taken intoaccount. Normative values areavailable for Raw, sRaw, and theirreciprocals, Gaw and sGaw [37–40].
The choice of which measure ofresistance is clinically most usefulvaries among different investigatorsand between countries. Someinvestigators emphasise Rtot
because it includes effects ofmultiple mechanical abnormalitiesassociated with advancedperipheral airway obstruction.Against this is the disadvantage oftest-to-test variability, due to itsderivation from only two points(maximal inspiratory andexpiratory shift volumes) of thesRaw loop.
Other investigators prefer Reff,because it integrates the entireranges of flow, shift volume andlung volume of the complete tidalbreath, and may thus be expected tooffer less within-individualvariability.
Others argue against both theseapproaches because of theirsensitivity to nonflow-resistivemechanical effects due tocompression of nonventilating airspaces, dynamic expiratoryintrathoracic airway compression,and EFL during tidal breathing.
These mechanical abnormalities, arelargely excluded from the calculationof R0.5. North American cliniciansutilise R0.5, from a standardised flowrange between late inspiration, +0.5L·s-1, and early expiration, 0.5 L·s-1,on the sRaw loop (fig. 5). Thiscalculation results in a lower Raw
than either Reff or Rtot because it isminimally affected by dynamicairway compression or compressionof nonventilating airspace. It maymanifest less test-to-test variabilitywithin an individual.
BODY PLETHYSMOGRAPHY03
38 THE BUYERS’ GUIDE TO RESPIRATORY CARE PRODUCTS
BG-03 Plethysmography 6/8/07 20:26 Page 38

The effects of dynamic airwaycompression and compression ofnonventilating airspaces lead to adependence of Rtot and Reff onbreathing pattern itself, namely thedegree to which patients withchronic airflow obstruction “force”their expiratory effort.
During resting tidal breathing innormal individuals, expiratoryairflow is largely produced bystored elastic energy in the chestwall. In patients with chronicairflow obstruction, activeexpiratory muscle recruitment ismuch more likely. Such patientscommonly utilise active expiratorymuscle effort to aid expiratoryairflow and manifest EFL, evenduring resting tidal breathing [41].The degree of expiratory muscleeffort may change with bronchial ortherapeutic challenge, and willdirectly influence calculated Reff
and Rtot because greater effortscause greater shift volumes withoutcorresponding increases inexpiratory airflow in the presenceof expiratory flow limitation.
Thus, there are marked differencesbetween “instantaneous” airflowresistance during inspiration andexpiration in patients with chronicairflow obstruction. Numericalrepresentation of the mechanicalabnormalities that occur separatelyduring expiration is not possibleusing R0.5, Rtot or Reff due to thedefinition of these quantities basedon the sRaw loops. Instead, graphicdisplay of the sRaw loop is requiredto appreciate the prominence ofsuch abnormalities during theexpiratory phase [2, 42–44].
Current computer-assistedplethysmography makes it possibleto calculate “instantaneous” valuesof airflow resistance, provided TGVis known. As noted above, duringbreathing within the body box,airflow resistance in the lungrequires compression of thoracicgas during expiration andexpansion of thoracic gas duringinspiration, resulting in the “shiftvolumes” measured by the pressure
change in the plethysmograph.Calculation of Raw requiresmeasures of PA and airflow. Duringfree breathing, shift volume can beused to record an index of changesin PA, because shift volume is theproduct of TGV and the change inalveolar pressure, divided by initialPA. In other words, the fractionalchange in PA integrated over TGVcauses a change in TGV equal toshift volume, which, in turn, resultsin box pressure change. In this way,shift volume provides an index ofchanges in PA provided TGV isknown. It is again emphasised,however, that box pressure changeduring breathing is not equal tochange in PA. It is much smaller inmagnitude, and reflects thefractional change in PA modified bythe ratio of TGV to box volume.
Instantaneous PA during freebreathing may be estimated bycomputer, continuously in time,from measured signals of shiftvolume, volume and airflow afterrespiratory efforts against a closedshutter have been utilised tocalculate TGV. Instantaneous Raw
(iRaw) is then defined by the ratio ofinstantaneous PA to instantaneousairflow. This computer calculationhas only recently beenimplemented, and displays Raw
throughout the tidal breath, exceptat end-expiration and end-inspiration, where iRaw isundefined because airflow is zero.
Raw calculated in this mannerincludes nonlinearities in flowresistance and effects of EFL and acontribution of compression oftrapped gas to flow resistance. EFLcontributes variably to apparentRaw as a function of respiratoryeffort: the greater the expiratorymuscle effort, the larger thecalculated expiratory Raw at a fixedflow rate. Compression of trappedgas during expiration anddecompression during inspirationalso contribute to the total dynamicPA burden during breathing. Thedegree of trapped gas in patientswith airflow obstruction is likely toreflect small airway obstruction
more importantly than obstructionof larger more central airways.
In summary, most commerciallyavailable body boxes at presentprovide useful measures of absolutelung volumes at RV, FRC, and TLC,and measures of resistance toairflow. Absolute lung volumes (atTLC) are the gold standarddefinition of restrictive lungdisease. Airflow resistance is asimple name, but its evaluationduring breathing in a body boxrequires careful attention to thecomplex effects of dynamiccompression of intrathoracicairways during expiration,expiratory flow limitation duringresting breathing, EFL, andcompression of nonventilatedairspaces. It is up to the individualphysician to choose calculated“airway resistance” measures thatincorporate his or her perceptionsof the important physiologicalissues encountered in patients withobstructive lung disease. ■
BODY PLETHYSMOGRAPHY
THE BUYERS’ GUIDE TO RESPIRATORY CARE PRODUCTS 39
03
BG-03 Plethysmography 6/8/07 20:26 Page 39

BODY PLETHYSMOGRAPHY03
40 THE BUYERS’ GUIDE TO RESPIRATORY CARE PRODUCTS
1. DuBois AB, Botelho Sy, Bedell GN,Marshall R, Comroe JH Jr. A rapidplethysmographic method formeasuring thoracic gas volume: acomparison with a nitrogen washoutmethod for measuring functionalresidual capacity in normal subjects. J Clin Invest 1956; 35: 322–326.
2. DuBois AB, Botelho SY, Comroe JHJr. A new method for measuringairway resistance in man using abody plethysmograph: values innormal subjects and in patients withrespiratory disease. J Clin Invest1956; 35: 327–335.
3. Mead J. Volume displacement bodyplethysmograph for respiratorymeasurements in human subjects. J Appl Physiol 1960; 15: 736–740.
4. Grimby G, Takishima T, Graham W,Macklem P, Mead J. Frequencydependence of flow resistance inpatients with obstructive lung disease.J Clin Invest 1968; 47: 1455–1465.
5. Clement J, Van De Woestijne KP.Pressure correction in volume andflow-displacement bodyplethysmography. J Appl Physiol1969; 27: 895–897.
6. Stanescu D, DeSutter P, Van DeWoestijne K. Pressure-corrected flowbody plethysmograph. Am Rev RespirDis 1972; 105: 304–305.
7. Leith D, Mead J. Principles of BodyPlethysmography. Bethesda, MD,National Heart and Lung Institute,Division of Lung Disease, 1974.
8. Peslin R. Body plethysmography. In: Techniques in the Life Sciences:Respiratory Physiology. 4th Edn.County Clare, Ireland, ElsevierScientific Publishers, 1984; pp. 1–26.
9. Coates A, Peslin R, Rodenstein D,Stocks J. Measurement of lungvolumes by plethysmography. EurRespir J 1997; 10: 1415–1427.
10. Davis C, Campbell EJ, Openshaw P,Pride NB, Woodroof G. Importanceof airway closure in limiting maximalexpiration in normal man. J ApplPhysiol 1980; 48: 695–701.
11. Bohadana AB, Peslin R, Hannhart B,Teculescu D. Influence of pantingfrequency on plethysmographicmeasurements of thoracic gasvolume. J Appl Physiol 1982; 52:739–747.
12. Stanescu D, Rodenstein D,Caugerghs M, Van De Woestijne K.Failure of body plethysmography inbronchial asthma. J Appl Physiol:
Respirat Environ Exercise Physiol1982; 52: 939–948.
13. Rodenstein D, Stanescu D, FrancisC. Demonstration of failure of bodyplethysmography in airwayobstruction. J Appl Physiol: RespiratEnviron Exercies Physiol 1982; 52:949–954.
14. Shore S, Huk O, Mannix S, MartinJ. Effect of panting frequency onthe plethysmographicdetermination of thoracic gasvolume in chronic obstructivepulmonary disease. Am Rev RespirDis 1983; 128: 54–59.
15. Begin P, Peslin R. Influence ofpanting frequency on thoracic gasvolume measurements in chronicobstructive pulmonary disease. AmRev Respir Dis 1984; 130: 121–123.
16. Brown R, Slutsky A. Frequencydependence of plethysmographicmeasurement of thoracic gasvolume. J Appl Physiol 1984; 57:1865–1871.
17. Quanjer P, Tammeling G, Cotes J,Pedersen O, Peslin R, Yernault J.Standardized lung function testing:Lung volumes and forced ventilatoryflows. Eur Respir J 1993; 6: Suppl.16, 5–40.
18. Buchheim FW, Krause W.Elektronische Feuchte- undTemperaturkompensation bei derGanzkoörperplethysmographie[Electronic humidity- and temperaturecompensation in wholebodyplethysomography]. BiomedizinischeTechnik 1971; 16: 3.
19. Islam M, Ulmer W. Diagnostic valueof ‘closing volume’ in comparison to‘airway resistance/lung volume plot’.Respiration 1974; 31: 449–458.
20. Matthys H, Orth U. ComparativeMeasurements of AirwayResistance. Respiration 1975; 32:121–134.
21. Lord P, Edwards J. Variation inairways resistance when definedover different ranges of airflows.Thorax 1978; 33: 401–405.
22. Hantos Z, Galgoczy G, Daroczy B,Dombos K. Computation of theequivalent airway resistance: acomparison with routine evaluationsof plethysmographic measurements.Respiration 1978; 36: 64–72.
23. Briscoe W, DuBois AB. Therelationship between airwayresistance, airway conductance andlung volume in subjects of different
age and body size. J Clin Invest1958; 37: 1279–1285.
24. Van Noord J, Clement J, Van deWoestijne K, Demedts M. Totalrespiratory resistance and reactanceas a measurement of response tobronchial challenge with histamine.Am Rev Respir Dis 1989; 139:921–925.
25. Jaeger M, Otis A. Measurement ofairway resistance with a volumedisplacement body plethysmograph.J Appl Physiol 1964; 19: 813–820.
26. Krell W, Agrawal K, Hyatt R. Quietbreathing vs. panting methods fordetermination of specific airwayconductance. J Appl Physiol 1984;57: 1917–1922.
27. Coates A, Desmond K, Demizio D,Allen P, Beaudry P. Sources of errorin flow-volume curves: effect ofexpired volume measured at themouth vs that measured in a bodyplethysmograph. Chest 1988; 94:976–982.
28. Goldman MD, Smith HJ, Ulmer WT.Whole-body plethysmography. In:Gosselink R, Stam H, eds. LungFunction Testing. Eur Respir Mon2005; 31; pp. 15–43.
29. Brusasco V, Pellegrino R.Mechanics of ventilation. In: GibsonG, Geddes D, Costabel U, Sterk P,Corrin B, eds. Respiratory Medicine.3rd Edn. Vol. I. Edinburgh,Saunders, 2003; pp. 299–315.
30. Pride N, Macklem P. Lungmechanics in disease. In: MacklemP, Mead J, eds. Handbook ofPhysiology. The Respiratory System.Mechanics of Breathing. Section 3,Vol. III, part 2. Bethesda, MD,American Physiological Society,1986; pp. 659–692.
31. American Thoracic Society. Lungfunction testing: selection ofreference values and interpretativestrategies. Am Rev Respir Dis 1991;144: 1202–1208.
32. Coates A, Desmond K, Demizio D.The simplified version of Boyle’s lawleads to errors in the measurementof thoracic gas volume. Am J Respir Crit Care Med 1995; 152:942–946.
33. Desmond K, Demizio D, Allen P,Beaudry P, Coates A. An alternativemethod for the determination offunctional residual capacity in aplethysmograph. Am Rev Respir Dis1988; 137: 273–276.
REFERENCES
BG-03 Plethysmography 6/8/07 20:26 Page 40
PRODUCT LISTINGS
BODY PLETHYSMOGRAPHY
THE BUYERS’ GUIDE TO RESPIRATORY CARE PRODUCTS 41
03
34. Peslin R, Gallina C, Rotger M.Methodological factors in thevariability of lung volume andspecific airway resistance measuredby body plethysmography. Bull EurPhysiopathol Respir 1987; 23:323–327.
35. Agrawal A, Agrawal KP. Bodyplethysmographic measurement ofthoracic gas volume without pantingagainst a shutter. J Appl Physiol1996; 81: 1007–1011.
36. Jackson A, Gulesian P, Mead J.Glottic aperature during panting withvoluntary limitation of tidal volume. J Appl Physiol 1975; 39: 834–836.
37. Ulmer WT, Reichel G, Nolte D, IslamMS. Die Lungenfunktion.Physiologie, Pathophysiologie,Methodik [Lung function. Physiology,pathophysiology, methodology].Thieme 1991: 5.
38. Ulmer WT, Nolte D, Lecheler J,Schaefer T. Die Lungenfunktion.Methodik und klinische anwendung[Lung function. Methodology and
clinical application]. Thieme 2001; 6:86–95.
39. Matthys H, Zaiss AW, Theissen JL,Virchow JC Jr, Werner P.Definitionen, soll- und messwertezur diagnose obstruktiver, restriktiversowie gemischterventilationsstörungen für dieklinische lungenfunktionsdiagnostik[Definitions, predicted values andmeasures for diagnosis ofobstructive, restrictive as well ascombined ventilatory disorders forclinical lung function diagnostics].Atemw-Lungenkrkh 1995; 21:130–138.
40. Van der Velden K, Nietzman-Lammering K, Hoek R, Zanen P,Stam H. Comparison of airwayresistance measured with threedifferent techniques. Eur Respir J2003; 22: Suppl. 45, 576s. Abstract3621.
41. Pellegrino R, Wilson O, Jenouri G,Rodarte J. Lung mechanics duringinduced bronchoconstriction. J ApplPhysiol 1996; 81: 964–975.
42. Jaeger M, Bouhuys A. Loopformation in pressure vs flowdiagrams obtained by bodyplethysmographic techniques. BodyPlethymsmography. Prog Resp Res1969; 4: 116–130.
43. Nitta K, Mochizuki M. Study of thetime displacement between airflowand box pressure curves in bodyplethysmography. Med Biol Engin1967; 5: 481–487.
44. Ulmer W, Reif E, Weller W. Dieobstruktiven Atemwegserkrankungen[Obstructive airway disease].Thieme 1969; Stuttgart.
REFERENCES Continued
Phone: ++ 1 651 484 4874www.medgraphics.com
Elite™ Series Plethysmograph
The Elite™ Series Plethysmograph, Winner of the MedicalDesign Excellence Award, offers complete spirometry,diffusing capacity, lung volumes by nitrogen washout and/orPlethysmography, and airway resistance in a networked orstand-along system. The Elite’s unique “zero-clearance” doorwraps around the system, allowing it to operate in smallspaces whileaccommodating patientsof all sizes, frompediatric to adult. TheElite’s clear chamberimproves patientcomfort by providing anopen field of vision, andmakes testingaccessible for allambulatory andwheelchair-boundpatients.
MasterScope Body
www.viasyshealthcare.comPhone: +49 (0) 931 4972 0
MasterScope Body, the Gold-Standard for airway resistance measurements with optimised computer assisted loop compensation and wireless bluetooth connection to the box.
� Comprehensive PFT differential diagnostics including� Airway resistance, total lung volumes� Spirometry, Flow/volume, MVV� Animation for children
� Clear differentiation of obstructive,restrictive and combined diseases
� Reversibility, Pre/post comparison
� Bronchial challenge testing
� Compliant with all international guidelines
BG-03 Plethysmography 6/8/07 20:27 Page 41