prevalence of malaria infection in some localities of ... of malaria infection in some localities of...
TRANSCRIPT

Prevalence of malaria infection in some
localities of Fayoum governorate
Thesis
Submitted for fulfillment for Master Degree of
Medical Parasitology
By
Gomaa Desoky Eimam Hassanien
M.B., B.CH.
Demonstrator of Medical Parasitology
Faculty of Medicine
Fayoum University
Under supervision of
Prof. Dr. Maysa Mohamed Kamel
Professor of Medical Parasitology
Faculty of Medicine
Cairo University
Prof. Dr. Naglaa Abd –Elkhalek Al -shirbiny
Assistant Professor of Community Medicine
Faculty of Medicine
Fayoum University
Dr. Samr Sayed Attia
Lecturer of Medical Parasitology
Faculty of Medicine
Cairo University
Faculty of Medicine
Cairo University
2014

Acknowledgements
I offer my deepest thanks to Prof. Dr. Mona Mahmoud Hamed,
Head of Parasitology Department, Faculty of Medicine, Cairo
University, for her kind support and persistent encouragement.
I would like to express the deepest appreciation to my supervisor
Professor Dr. Maysa Mohamed Kamel, Professor of Medical
Parasitology, Faculty of Medicine, Cairo University, who gave me the
chance to start this work and to continue, with her encouragement,
scientific suggestions throughout this research work and extremely
unlimited efforts for revising this work.
I owe sincere thanks and everlasting gratitude to Dr.Naglaa Abd –
Elkhalek Al –shirbiny, Assistant Professor of Community Medicine ,
Faculty of Medicine, Fayoum University, for her moral support, valuable
suggestions and her guidance in the epidemiological aspect of this thesis .
Special thanks are extended to Dr. Samr Sayed Attia, Lecturer of
Medical Parasitology , Faculty of Medicine ,Cairo University, who gave
me help and provided me with facilities throughout the practical part of
this work and extremely unlimited efforts for revising and rewriting this
work.
Special thanks are extended to Dr. Gomaa Said
Mohamed,assistant Lecturer of Measurement and Evaluation , Faculty of
Education ,Fayoum University, for the statistical analysis of the data
reported in this thesis..
Also, I would like to express profound gratitude to Prof. Dr. Abd
El-Hamid Abd El-Tawab Sabry, Professor of Medical Parasitology,
Faculty of Medicine, Fayoum University, for his moral support.
I also appreciate the assistance I received from all staff members
in Parasitology Department, Faculty of Medicine, Fayoum University,
throughout my work.
Finally, special deep rooted heartily thanks to my mother for her
love and support throughout my life. I also wish to thank my wife
Dr.Shimaa for her support and understanding during my study.

Abstract
The present work was carried on 600 cases, 500 from household
cases from El-Khaldia and Abo-Shanab villages, Abshoy
District ,Fayoum governorate and 100 selected cases from Fayoum Fever
Hospital in order to find prevalence of malaria infection in some
localities of Fayoum governorate.. Diagnosis of malaria was done by thin
and thick blood film for all cases in addition to malaria RDT applied to
the 100 selected cases. Three cases were diagnosed by malaria RDT;
while one case was positive by thick blood film.All positive cases were
imported from Sudan.
Key Words: malaria, RDT, blood film, Fayoum, imported.

I
List of Abbreviations
ACC Automated cell counter
AIDS Acquired Immunodeficiency Syndrome
An.multicolor Anopheles multicolor
DBL Duffy binding like
DLL depolarized laser light
DNA Deoxyribonucleic acid
ELISA Enzyme-Linked Immunosorbent Assay
FCM Flow cytometer
HIV Human Immunodeficiency Virus
HRP-II histidine-rich protein II
IFA Immunofluorescence antibody testing
IFU Instruction for use
IRMA Immunoradiometric assay
LAMP loop-mediated isothermal amplification
LDH lactate dehydrogenase
LDMS laser adsorption mass spectrometry
LED light emitting diode
ml Milliliter
MOHP Ministry of Health and Population
P. falciparum Plasmodium falciparum
PCR Polymerase chain reaction
PfEMP1 plasmodium falciparum erythrocyte membrane protein 1
pLDH pan-malaria lactate dehydrogenase
QBC Quantitative buffy coat
RDT Rapid diagnostic test

II
SD Standard deviation
UN United Nation
UNMIS United Nation Missions In Sudan
VCS volume, conductivity, and scatter
WBC(s) White blood cell (s )
WHO The World Health Organization
μm A micrometre or micron

III
LIST OF FIGURES
Figure Title Page
1 Malaria rapid test device positive for Plasmodium
falciparum 38
2 Malaria rapid test device negative for all Plasmodium
species 38
3 Malaria pf /pan rapid test. 39
4 Age groups of the household cases 41
5 Age groups of the selected cases 42
6 Gender distribution of household cases. 43
7 Gender distribution of selected cases. 44
8 History of travelling abroad in selected cases. 45
9 Drug intake in the household cases. 46
10 Drug intake in the selected cases. 47
11 Clinical symptoms detected in the household cases 48
12 Clinical symptoms detected in the selected cases 48
13 Clinical signs detected in the household cases 49
14 Clinical signs in the selected cases 50
15 Thick blood film showing ring stage of plasmodium
falciparum. 51
16 malaria (Pf/Pan) One Step Rapid Test applied for 100
selected cases 52
17 Malaria rapid test negative for all plasmodium species 53
18 Malaria rapid test positive for plasmodium falciparum 53

IV
LIST OF TABLES
Table Title Page
1 Malaria in Egypt from 1960-2003. 6
2 Malaria in Egypt from 2004-2010. 7
3 Recorded indigenous malaria cases in Fayoum
governorate (1971- 2004) 8
4 Recorded imported malaria in Egypt from 1998-2004. 12
5 Age distribution of household cases 41
6 Age distribution of selected cases 42
7 Gender distribution of the household cases 43
8 Gender distribution of the selected cases 43
9 Number and percentage of household cases with
history of travel to Sudan 44
10 History of intake of anti-malaria drug in household
cases 45
11 Frequency of intake of anti-malaria drug in household
cases 46
12 Clinical signs detected in the household cases 49
13 Clinical signs detected in the selected cases 50
14 Distribution of positive cases as regard different
characteristics (history and clinical examination) 54

V
Contents
Titles Pages
Introduction 1
Aim of the work 3
Review of Literature 4
Prevalence of malaria 4
Imported malaria, 9
Taxonomy 12
Life cycle and methods of transmission 13
Anopheline vector 51
Clinical picture of malaria 17
Diagnosis 21
Materials and methods 32
Results 40
Discussion 56
Summary and Conclusion 66
Recommendations 69
References 70
Arabic Summary

Introduction
1
Introduction
Forty-one percent of the world's population lives in areas where malaria is
transmitted (e.g., parts of Africa, Asia, the Middle East, Central and South
America) (WHO, 2002).About 3.3 billion people -half of the world's population-
are at risk of malaria leading to about 250 million malaria cases and nearly one
million deaths every year. People living in the poorest countries are the most
vulnerable (WHO, 2009).
About Ninety-percent of all malaria deaths in the world today occur in
Africa South of the Sahara. This is because the majority of infections in Africa
are caused by Plasmodium falciparum, which is considered as the most
dangerous of the four human malaria parasites. The vector of falciparum malaria
(Anopheles gambiae) is widely spreaded in Africa and considered as the most
difficult vector to control. An estimated one million people in Africa die from
malaria each year and most of these are children under 5 years old
(Daoud,2003).
Malaria control in Egypt achieved a considerable progress in the last few
decades due to widespread indoor residual spraying (IRS) with long-lasting
insecticides and introduction of artemisinin combination therapy with
artemether-lumefantrine (Coartem©).These procedures led to a decrease in
malaria caseload from about 85000 cases in 1960 to 5400 cases in 1970, with a
preponderance of P.vivax cases(MOHP,2006).After application of intensive
control measures, only 4 indigenous cases caused by falciparum were reported
in 1997(WHO, 2006). There were few annual imported malaria cases from
1998-2003(Dawoud, 2003). In 2005, Ministry of health in Egypt reported 23
cases of imported malaria from Sierra Leon and Sudan (WHO, 2006).
It has been shown that malaria infection increased with the decrease of
socioeconomic level of families, educational level of examined individuals and
among unemployed or students. The infection increased among those living in

Introduction
2
muddy or bad constructed houses near the breeding places of mosquitoes. Also,
it decreased significantly among individuals who owned animal sheds (Dahesh
et al., 2009).
However, there are many factors which may contribute to re-emergence
of the disease in Egypt. Such factors include infection of local Anopheline
mosquitoes by imported cases, continuous movement of populations between
Aswan governorate and Sudan as well as the influx of large populations from
Africa and Asia to Egyptian governorates for educational and religious
purposes. Another risk factor is the environmental change brought about by
water-sources development projects as Toshka and El Salam Canals (Hassan
et al.,2003).

AIM OF WORK
3
AIM OF WORK
The present work aimed to:
1- Study the prevalence of malaria in some localities in Fayoum
governorate ; in addition to study the demographic criteria of the
examined population incorporated in this study.
2- Determine the likelihood of acquisition of malaria infection in this
area using thin and thick blood film, in addition to malaria pf/pan one
step rapid test to detect plasmodium antigen in blood samples.
Review of Literature
3
Review of Literature
Malaria prevalence in the world
The global human population has grown geometrically during the
20th century from approximately 1 to 6 billion. These demographics have
important implications for the percentage of the human population exposed
to all-cause malaria risk through time. The percentage of the global
population at risk has decreased from 77% at the turn of the 20th
century to a
low of 46% in 1994. This figure increased to 48% in 2002 due to population
growth in an unchanged geographic distribution. In absolute terms the
numbers of people at risk has increased consistently from 0.9 to 3 billion
over the same period (1900-2002). At the turn of the 21st century, it is
estimated that 48% of the global population remain exposed to the risk of
malaria, a situation that has deteriorated since the early 1990s and a figure
substantially higher than the 40% widely cited (Hay et al., 2004).
Almost 300 million clinical cases of malaria occur worldwide each
year and over a million people die. Almost 90% of these deaths occur in sub-
Saharan Africa, where young children are the most affected. Malaria is
directly responsible for one in five childhood deaths in Africa and indirectly
contributes to illness and deaths from respiratory infections, diarrhoeal
disease and malnutrition (World Health Report, 1999).
According to WHO malaria report in 2011,the number of reported
cases of malaria decreased more than 50% in 35 of the 53 countries
ongoing transmission between 2000 and 2010 while decreased 25%-50% in
the other 4 countries.In 2010, the Europe region reported only 176
indigenous cases.The number of cases continued to fall least in countries
with the highest incidence rates, indicating that greater attention should be

Review of Literature
4
given to countries which harbour most of malaria burden outside Africa
(WHO,2011).
There were 8 countries in the pre-eliminating stage of malaria control
in 2011 and 9 countries are implementing elimination programmes
nationwide.
A further 8 countries including Bahamas, Egypt, Georgia, Iraq,
Jamica, Oman, Russian federation and Syria have interrupted transmission
and are in the prevention of reintroduction phase (WHO, 2011).
An estimated 3.3 bilion people were at risk of malaria in 2010,
2.1bilion were at low risk (> 1reported case per 1000 population ),94% of
whom were living in geographic regions other than the WHO African
region.The remaining 1.2 bilion were at high risk (< 1reported case per 1000
population ) and were living mostly in WHO African region (47%) and
South East Asia (37%) (WHO,2011). Approximately 81%, or 174 milion
cases, wer in Africa and 13% in South East Asian region. There were an
estimated 655000 malaria deaths in 2010,of which 91% were in Africa.
Approximately86% of malaria deaths occurred in children under 5 years of
age (WHO, 2011).

Review of Literature
5
Malaria situation in Egypt
The present distribution of malaria cases in Egypt as reported by the
Ministry of Health is demonstrated in table (1).
Table (1): Malaria in Egypt from 1960 – 2003 (MOHP, 2006).
% Of malaria in the
examined slides
Plasmodium
Falciparum
Plasmodium
Vivax No.of +ve No.of slides Year
21.3 1996 83205 85201 400000 1960
1.2 144 7853 7997 674044 1965
0.88 153 5241 5394 609329 1970
0.12 46 1759 1805 1399101 1975
0.02 4 370 374 1332541 1980
0.006 19 53 72 1180900 1985
0.006 69 2 71 1145251 1990
0.27 298 15 313 1139859 1995
0 0 0 0 1107560 2000
0 0 0 0 1567223 2001
0 0 0 0 1357223 2002
0 0 0 0 1041767 2003
The last focus of malaria in Egypt was in Fayoum which became free
from transmission of malaria since 1998 and Egypt was certificated as free
of malaria. There were few annual imported malaria cases since the year
1998.
As regards malaria situation in Egypt from the period 2004-2010;All
the detected cases were imported as shown in Table (2) (WHO, 2012).

Review of Literature
6
Table (2): Malaria in Egypt from 2004-2010 (WHO, 2012)
Imported
cases
Confirmed
microscopically
Examined
microscopically
Suspected Year
43 43 - 43 2004
23 23 - 23 2005
29 29 - 29 2006
30 30 23402 30 2007
80 80 34880 80 2008
94 94 41344 94 2009
85 85 664294 85 2010
Malaria situation in Fayoum governorate:
Fayoum governorate is considered as a large agricultural area. It lies
90 Km south-east of Cairo. It is composed of six districts, Fayoum, Sinnuris,
Ebshawy,Youssef-Elsdek, Tamiya and Itsa.
The main problem in malaria transmission in Fayoum goveronorate is
the high level of subsoil water leading to formation of many swamps and
pools creating suitable environmental conditions for Anopheline
vectors(Harb,1994).
Also, the favourable meterological conditions , mainly optimum temperature
and relative humidity leading to the extension of the transmission season to
8 months a year from the end of March to the end of
November(Bassiouny,1996).
Two main Anopheline vectors in Fayoum governorate were
responsible for the transmission of malaria; Anopheles sergenti and
Anopheles pharoensis(Shehata et al.,1989).

Review of Literature
7
Table (3) Recorded indigenous malaria cases in Fayoum governorate (1971-
2004) (Bassiouny, 2001).
Year Number of malaria cases
P. falciparum P. vivax
1971 208 489
1972 264 888
1973 8 250
1974 6 129
1975 175 1102
1976 205 242
1977 120 271
1978 131 555
1979 42 271
1980 9 193
1981 3 109
1982 103 68
1983 5 28
1984 52 111
1985 11 4
1986 41 22
1987 10 10
1988 218 0
1989 200 0
1990 69 1
1991 21 4
1992 9 2
1993 13 3
1994 473 23
1995 290 16
1996 69 2
1997 4 0
1998 0 0
1999 0 0
2000 0 0
2001 0 0
2002 0 0
2003 0 0
2004 0 0
The early eradication of P.vivax first before P.falciparum was due to higher
sensitivity of P.vivax than P.falciparum to chloroquine(Bassiouny, 2001).

Review of Literature
8
In Fayoum governorate, it seems that malaria control achieved
significant progress when widespread indoor residual spraying (IRS) with
long-lasting insecticides and introduction of artemisinin combination therapy
with artemether-lumefantrine (Coartem©) and this led to disappearance of
clinical cases of indigenous malaria and interruption of malaria transmission
(MOHP,2006).
The researchers in the Military Fever Hospital, Egypt diagnosed thirty
six patients as having malarial disease. Twenty of them were recruited from
Peace Keeping Mission Forces in Africa and sixteen cases presented with
prolonged fever coming from different locations in Egypt. Their results
showed that 12.5% of them were from Fayoum governorate. The diagnosis
was by the use of bone marrow smears as they were negative by peripheral
blood examination (El-Bahnasawy et al., 2010).
Imported malaria, 2001–2010
Imported malaria refers to infections acquired outside and brought
into a national territory. The character of imported malaria and the problems
it possess for countries in the prevention of reintroduction and malaria-free
stages has changed over the period 2001–2010. Factors influencing the
change include the reduction of malaria incidence in tourist destinations, an
increase in the number of countries recently classified as malaria-free and
new patterns of travel and international migration prior to year 2000, the
importation of malaria into non-endemic countries as “traveller‟s malaria”
was primarily a matter for foreign tourists returning home after visiting
endemic areas(WHO, 2012).
Since 2000, the problem has grown and changed in at least four ways:
(i) in non-endemic countries with large and relatively affluent immigrant
populations (e.g. countries in North America and Western Europe),
immigrants returning home to endemic areas to visit friends and relatives

Review of Literature
01
have become a high-risk group among travellers; (ii) non endemic countries
take refugees from malaria-endemic areas; (iii)malaria cases are imported
with returning members of national armed forces and UN peacekeeping
forces; and (iv) malaria infections are often brought into countries by
temporary migrant workers (WHO, 2012).
Imported malaria was reported by 91 countries between 2001and
2010; the largest total numbers of cases were in the United States of
America (12701) in the Region of the Americas, the United Arab Emirates
(20 452) in the Eastern Mediterranean Region, France (48 580) and the
United Kingdom (17 063) in the European Region and Australia (3355) in
the Western Pacific Region. Between 2001 and 2010, 45 countries in the
European Region reported a striking and consistent decline in imported
malaria cases and deaths, for reasons that have not yet been investigated
(WHO, 2012).
Critical for malaria control is whether imported cases lead to local
outbreaks of malaria, transmitted by indigenous Anopheline mosquitoes. The
risk can be high, for example when temporary agricultural workers infected
with malaria are recruited for harvesting during the malaria transmission
season. However, while malaria outbreaks are commonly documented, they
are less frequently investigated to understand the precise circumstances of
the outbreak and to identify the local vectors. In the European Region, local
transmission from imported cases has been reported in Republic of Moldova
(2003), Ukraine (2003),France (2006, 2008–2010), Italy (2007), Greece
(2009– 2010) and Spain (2010) .In all these instances, local outbreaks were
limited to fewer than 10 cases (WHO, 2012).
In the Region of the Americas, the United States of America reported
an outbreak of eight cases of P. vivax in Palm Beach County, Florida, in
2003, probably originating from a single infected person. Immigration was

Review of Literature
00
the cause of a large outbreak of P. falciparum malaria that occurred in
Jamaica between September 2006 and December 2009, in which there were
406 confirmed cases. In the Bahamas, 19 P. falciparum cases were identified
on the island of Great Exuma between May and June 2006, apparently
brought to the island by Haitian immigrants. These outbreaks in the
Americas were contained by a swift reaction from public health authorities
(WHO, 2012).
In other parts of the world: three cases arising from local P.
falciparum transmission were reported in Singapore in 2003; Oman, which
interrupted transmission in 2004, has experienced several subsequent
outbreaks of P. vivax and P. falciparum brought in by migrant workers from
the Indian subcontinent; and Morocco, certified malaria-free in 2007,
recorded two cases of “airport malaria” in 2009 (WHO, 2011).
Other countries which eliminated malaria many years ago, including
the Maldives, Mauritius and Tunisia, continued to invest effort in preventing
the reintroduction of malaria. For the growing number of countries
progressing to the prevention of reintroduction and malaria-free stages, the
nature of malaria control will change, moving towards outbreak
preparedness, surveillance and rapid response and studies of malaria risk and
receptivity (WHO, 2011).
The Imported Malaria cases in Egypt were recorded by Dawoud( 2003).
Blood samples were taken from ship passengers travelling between
Aswanwady Half , sent to fever hospitals , examined for malaria parasites.
The reported data are shown in table (4).

Review of Literature
01
Table (4): Recorded Imported Malaria cases 1998-2004 in Egypt
(Dawad,2003).
Year No of
examined
slides
Positive P.falciparum P.vivax
1998 32403 24 23 1 (5 from Egypt)
1999 28992 38 37 1 (3 from Egypt )
2000 26581 17 17 0 (3 from Egypt )
2001 26341 9 10 1 ………………..
2002 25785 9 9 1 (1 from Egypt )
2003 23813 45 44 1 (37 from Egypt )
3.2-Taxnomy
Phylum: Apicomplexa
Class: Aconoidasida
Order: Haemosporida
Family: Plasmodiidae
Genus: Plasmodium
Species: falciparum, ovale, vivax and malariae. )Marchiafava & Celli,
1885).
Plasmodium knowlesi. P. knowlesi is one of the species of Plasmodium most
recently identified as an agent of human malaria (Cox-Singh et al., 2008).

Review of Literature
02
3. Life cycle of malaria:
3.3.1-Pre-erythrocytic development
The small motile Plasmodium sporozoites are injected by the feeding
female Anopheline during the phase of probing (Rosenberg et al.1990).
After injection, sporozoites enter the circulation and rapidly target the
hepatic parenchymal cells and begin a phase of asexual reproduction. This
stage lasts on average between 5.5 (P. falciparum) and 15 days (P. malariae)
before the hepatic schizont ruptures to release merozoites into the
bloodstream (Smith et al., 2004). In P. vivax and P. ovale infections a
proportion of the intrahepatic parasites do not develop, but instead they rest
inert as sleeping forms or „hypnozoites‟ causing the relapses which
characterize infections with these two species. During the hepatic phase of
development, asexual multiplication takes place and many thousands of
merozoites are released from each ruptured infected hepatocyte. However, as
only a few liver cells are infected, this phase is asymptomatic for the human
host (Smith et al., 2008).
3.3.2-Asexual blood-stage development
The merozoites liberated from ruptured hepatocytes invade red cells
rapidly. The process of invasion involves attachment of the merozoite to the
erythrocyte surface, orientation so that the apical complex (which protrudes
slightly from one end of the merozoite and contains the rhoptries, the
micronemes and dense granules) abuts the red cell .Interiorization takes
place by a wriggling or boring motion inside a vacuole composed of the
invaginated erythrocyte membrane.Inside the erythrocyte, the parasite lies
within the erythrocyte cytosol enveloped by its own plasma membrane and a
surrounding parasitophorous vacuolar membrane. The attachment of the
merozoite to the red cell is mediated by the attachment of one or more of a

Review of Literature
03
family of erythrocyte binding proteins, localized to the micronemes of the
merozoite apical complex, to a specific erythrocyte receptor. In P. vivax this
is related to the Duffy blood group antigen Fya or Fyb (Miller et al., 1976).
After approximately 12–14 h of development, P. falciparum parasites
begin to exhibit a high molecular weight strain-specific variant antigen,
Plasmodium falciparum erythrocyte membrane protein 1 (PfEMP1) on the
exterior surface of the infected red cell which mediates attachment of the
infected erythrocyte to vascular endothelium (Leech et al.,1984).
Approximately 36 h after merozoite invasion (or 54 h in P. malariae),
repeated nuclear division takes place to form a schizont. As the red cell
ruptures, from 6 to 36 merozoites are released destroying the remnants of the
red cell. The released merozoites rapidly re-invade other red cells and start a
new asexual cycle. The process of gametocytogony takes about 7–10 days
in P. falciparum. Thus, there is an interval of 1 week between the peaks of
asexual and sexual stage parasitaemia in acute falciparum malaria. In
contrast, P.vivax begins gametocytogenesis immediately and the process of
gametocytogony in the blood stage infection takes only 4 days. Symptomatic
P. vivax infections are therefore more likely to present with patent
gametocytaemia and was able to transmit infection to mosquitoes before
treatment than acute P. falciparum infections (Leech et al., 1984).
3.3.3- Sexual stages and development in the mosquito
Following ingestion in the blood meal of a biting female Anopheline
mosquito, the motile male microgametes separate and seek the female
macrogamete. Within 24 h the enlarging zygote becomes motile and forms
the ookinete which penetrates the wall of the mosquito mid-gut (stomach)
where it encysts as an oocyst. (Ghosh et al.,2000).

Review of Literature
04
The oocyst finally bursts to liberate myriads of sporozoites into the
coelomic cavity of the mosquito. The sporozoites then migrate to the
salivary glands to await inoculation into the next human host during feeding.
The development of the parasite in the mosquito is termed sporogony, and
takes between 8 and 35 days depending on the ambient temperature and
species of parasite and mosquito. The longevity of the mosquito is a critical
factor in determining its vectorial capacity (Ghosh et al., 2000).
3.4-Methods of transmission:
1. From female anopheline mosquitoes to humans: Malaria infection in
humans is initiated with the bite of an infectious female mosquito, which
injects sporozoites of Plasmodium species into the circulation. These
sporozoites rapidly bind and invade liver cells and undergo rapid
multiplication, leading to the release of thousands of infectivemerozoites
(Raether et al.1989).
2. From humans to anopheline mosquitoes: The journey of Plasmodium within
the mosquito begins as the mosquito ingests gametocytes with the blood of
an infected host (Ghosh et al., 2003).
3. From humans to humans : Plasmodium is sometimes transmitted by means
other than the bite of a mosquito. The blood cycle may be initiated by
blood transfusion, by malaria therapy of certain paralytic disease, by
syringe-passed infection among drug addicts, or, rarely, by congenital
infection (Schmidt and Roberts, 1985).
3.5-Anopheline vector
Malaria is transmitted only via Anopheline mosquitoes. In principle,
reducing or eliminating mosquito populations should stop disease
transmission. In practice, this approach is difficult to implement, especially
in sub-Saharan Africa, where mosquitoes can easily grow in environments

Review of Literature
05
such as small pools of water, which are extremely difficult to manage or
target with insecticides. Insecticide campaigns might reduce mosquito
populations temporarily, but leave a largely intact biological niche, where
mosquitoes can continue to thrive (Ghosh et al., 2003).
Anopheles gambiae is the principal mosquito vector of malaria in
Africa (Land, 2003).
Anopheles multicolor: Plasmodium infection rates determined by
enzyme-linked immunosorbent assay (ELISA) were compared for Anopheles
sergentii and An. multicolor Cambouliu in Siwa Oasis, Egypt, an area with
low-level Plasmodium vivax transmission, and in Bahariya and Farafra, two
other Egyptian oases which appear to be free of malaria. Initial testing
indicated that 4.4% (23 of 518) and 0.8% (4 of 518) of the An. sergentii were
positive for P. vivax and P. falciparum, respectively, and that 1.4% (1 of 71)
of the An. multicolor was positive for P. falciparum (Kenawy et al., 1990).
Anopheles pharoensis : Plasmodium vivax and P.falciparum
epidemiology were studied for parasitological and entomological samples
collected during the period 1989 and 1990, respectively, from Gambella, South
West Ethiopia. Of the total population examined (n = 1091), 147 (13.5%) were
found to be positive for malaria parasites. Prevalence rates among males and
females were 13.8% and 13.1%, respectively.The mosquito species responsible
for malaria transmission were the indoor-resting A. gambiae and A.
pharoensis. The parasite infection rates of these species were 0.76% and 0.46%
and they were found to be the exclusive vectors of P. falciparum and P. vivax,
respectively (Nigatu et al., 1992).
Anopheles sergenti: Detection and identification of malaria
sporozoites is usually done by two immunoassay: immunoradiometric assay

Review of Literature
06
(IRMA) and the enzyme-linked immunosorbent assay (ELISA) using the
species-specific monoclonal antibodies is routinely performed. Afield study
analyzed (573) anopheline mosquitoes of A. sergenti (463), A. pharoensis
(81) and A. multicolor (29) collected from Siwa-oases and Fayoum
governorate (two known active malaria foci in Egypt), for detection of P.
falciparum and P. vivax sporozoites. P. falciparum sporozoites were
detected by both IRMA and ELISA tests in two A. sergenti mosquitoes (one
from Siwa 1/389 = (0.26%) and one from Fayoum governorate 1/74 =
(1.35%)). No P. vivax sporozoites were detected. This finding is important in
explaining the malaria transmission and provides first incrimination of An.
sergenti as the responsible vector of malaria in Siwa-oasis, Egypt (Shehata et
al., 1989).
3.6-Clinical picture of malaria
3.6.1-Uncomplicated malaria
Incubation period ranges from 9 days in P. falciparum to 30 days in P.
malariae infections. As far as the degree of previous protection possessed by
the infected subject is concerned, it is known that effective immunity
prolongs incubation period and reduces level of parasitemia and clinical
manifestations. Low asymptomatic parasitemia may persist in migrants from
endemic areas long after their arrival in the host country ( Harinasuta and
Bunnang,1988).Delayed clinical presentation of P. falciparum has been
described as long as 2, 4 or even 8 years (Szmitko et al., 2008) after subjects
have left malaria-endemic areas.Prolonged incubation period may also be
caused by the use of antimalarial drugs that, although ineffective, may
impact on the parasite multiplication rate (D'Ortenzio et al., 2008).
The clinical manifestations of malaria are dependent on the previous
immune status of the host. In areas where endemicity of P. falciparum
malaria is stable, severe malaria most commonly occurs in children up to 5

Review of Literature
07
years of age, while is less common in older children and adults because of
the acquisition of partial immunity. In areas of lower endemicity, the age
distribution of severe malaria is less well defined and may also occur in
adult semi-immune (Cook et al., 2009).
The first symptoms of malaria, common to all the different malaria
species, are nonspecific and mimic a flu-like syndrome. The hallmark of
malaria is fever. Up to two days before the onset of fever, prodromal
symptoms, such as malaise, anorexia, lassitude, dizziness, with a desire to
stretch limbs and yawn, headache, backache in the lumbar and sacroiliac
region, myalgias, nausea, vomiting and a sense of chillness may be
experienced (Warrell, 1993).
In P. vivax and P. ovale infection, if left untreated, asexual cycles
become synchronous after 5 to 7 days causing periodic febrile paroxysms.
The classical malaria paroxysm presents three stages: a cold stage, followed
by a hot stage with a terminal sweating stage. The cold stage is typically
characterized by a sudden onset with a feeling of extreme coldness. The
subject may shiver and his or her teeth may chatter. In virtue of an intense
peripheral vasoconstriction phenomenon, the skin is cold, dry, pale,
cyanosed and sometimes goose-pimpled. (Cook et al., 2009).
In P. falciparum malaria, the onset of fever occurs few days after
prodromal symptoms started during the last days of the incubation period
(normal range 9-14 days). At first, fever is irregular, but usually occurs daily. It
may be intermittent or continuous, and shows no sign of periodicity until the
illness has continued for a week or more. The symptoms present in the
prodromal phase continue and increase configuring a flu-like syndrome.
Anorexia, dyspepsia, epigastric discomfort, nausea, vomiting and watery
diarrhoea are frequent and may be misdiagnosed as a gastrointestinal infection.
Herpes labialis may be present. A dry cough and an increase in the respiration

Review of Literature
08
rate may be observed, arising the suspect of an acute respiratory infection.
When periodic febrile paroxysms occur, they may be daily (quotidian), every
third day (tertian) or at about 36-hour intervals (subtertian) (Taylor and
Strickland, 2003).
P. malariae causes the mildest and most persistent form of malaria
infection after an incubation period that is never less than 18 days, but that
may be up to 30-40 days, prodromal symptoms resembling those of vivax
malaria precedes the onset of fever. The clinical picture of the primary attack
is similar to that of vivax malaria. The onset is often insidious, but febrile
paroxysms, often occurring in the late afternoon, show well synchronized
schizogony from an early stage and are typically separated by intervals of 72
hours(quartan malaria) ( Harinasuta and Bunnang,1988).
Left untreated, the acute attack is self limiting but may last for several
months before spontaneous remission occurs. Severe complications of P.
malariae infection are rarely observed. However, recrudescences may occur,
more frequently during the first year and then at longer intervals, even after
30-50 years. P. malariae has no hypnozoite form, so recrudescences arise
from persisting blood stage. Asymptomatic P. malariae parasitaemia in
blood donors may cause transfusion malaria ( Harinasuta and
Bunnang,1988).
P. malariae infection is associated with development of a nephrotic
syndrome.P. Malariae parasitemia is common in children, but not in adults.
Transient clinical remissions with period of asymptomatic proteinuria are
frequent but progressive deterioration and development of renal failure often
occurs within 3 to 5 years (Taylor and Strickland, 2003).
Knowlesi malaria (a simian parasite) is the most common locally acquired
human malaria in Malaysian Borneo (~70% of malaria cases) (Daneshvar et al.,
2009). with the disease also reported from other countries of Southern and

Review of Literature
11
Eastern Asia.( Baird,2009). On the basis of clinical features, it is not possible to
distinguish knowlesi malaria from vivax or falciparum malaria (Daneshvar et
al., 2009).The development of hyperparasitemia and other complications are
fairly common (Baird, 2009).

Review of Literature
10
4-Diagnosis of malaria infection
4.1- Microscopic diagnosis using stained thin and thick peripheral blood
smears (PBS):
Malaria is conventionally diagnosed by microscopic examination of
stained blood films using Giemsa, Wright's, or Field's stains (Warhurst and
Williams, 1996). This method has changed very little since Laverran's
original discovery of the malaria parasite, and improvements in staining
techniques by Romanowsky in the late 1,800s. More than a century later,
microscopic detection and identification of Plasmodium species in Giemsa-
stained thick blood films (for screening of malaria parasite), and thin blood
films (for species' confirmation) remains the gold standard for laboratory
diagnosis (Bharti et al., 2006). The wide acceptance of this technique by
laboratories all around the world can be attributed to its simplicity, low cost,
its ability to identify the presence of parasites, the infecting species, and
assess parasite density-all parameters useful for the management of malaria.
Recently, a study showed that conventional malaria microscopic diagnosis at
primary healthcare facilities in Tanzania could reduce the prescription of
antimalarial drugs, and also appeared to improve the appropriate
management of non-malarial fevers (Ngasala et al., 2008). However, the
staining and interpretation processes are labor intensive, time consuming,
and require considerable expertise and trained healthcare workers,
particularly for identifying species accurately at low parasitemia or in mixed
malarial infections
The most important shortcoming of microscopic examination is its
relatively low sensitivity, particularly at low parasite levels. Although the
expert microscopist can detect up to 5 parasites/µl, the average microscopist
detects only 50-100 parasites/µl (Payne, 1988). This has probably resulted in
underestimating malaria infection rates, especially cases with low

Review of Literature
11
parasitemia and asymptomatic malaria. The ability to maintain required
levels of in malaria diagnostics expertise is problematic, especially in remote
medical centers in countries where the disease is rarely seen (Ohrt et
al.,2002). Microscopy is laborious and ill-suited for high-throughput use,
and species determination at low parasite density is still challenging.
Therefore, in remote rural settings, e.g. peripheral medical clinics with no
electricity and no health-facility resources, microscopy is often unavailable
(Erdman et al., 2008).
Concerning diagnosis, the identification of P. knowlesi infection by
using microscopy only is difficult because it is very similar to P.
malariae( Lee et al., 2009).Polymerase Chain Reaction (PCR) is currently
the method of choice to obtain a certain diagnosis.(Cox-Singh et al.,2008).
4.2-Quantitative Buffy Coat technique:
The Quantative buffy coat (QBC) technique was designed to enhance
microscopic detection of parasites and simplify malaria diagnosis
(Clendennen et al., 1995). This method involves staining parasite
deoxyribonucleic acid (DNA) in micro-hematocrit tubes with fluorescent
dyes, e.g. acridine orange, and its subsequent detection by epi-fluorescent
microscopy. Briefly, finger-prick blood is collected in a hematocrit tube
containing acridine orange and anticoagulant. The tube is centrifuged at
12,000 gram for 5 min and immediately examined using an epi-fluorescent
microscope (Chotivanich et al., 2006). Parasite nuclei fluoresces bright
green, while cytoplasm appears yellow-orange. The QBC technique has been
shown to be a rapid and sensitive test for malaria diagnosing in numerous
laboratories settings (Bhandari et al.,2008). While it enhances sensitivity for
P. falciparum, it reduces sensitivity for non-falciparum species and
decreases specificity due to staining of leukocyte DNA (Moody et al., 2002).

Review of Literature
12
Recently, it has been shown that acridine orange is the preferred
diagnostic method (over light microscopy and immunochromatographic
tests) in the context of epidemiologic studies in asymptomatic populations in
endemic areas, probably because of increased sensitivity at low parasitemia
(Ochola LB et al., 2006). Although the QBC technique is simple, reliable, it
requires specialized instrumentation and it is more costly than conventional
light microscopy, also it is poor at determining species and numbers of
parasites (Tangpukdee et al., 2009).
4.3-Rapid diagnostic tests (RDTs):
Since the World Health Organization (WHO) recognized the urgent
need for new, simple, quick, accurate and cost-effective diagnostic tests for
determining the presence of malaria parasites to overcome the deficiencies
of light microscopy, numerous new malaria-diagnostic techniques have been
developed (WHO, 1996). This, in turn, has led to an increase in the use of
RDTs for malaria, which are fast and easy to perform, and do not require
electricity or specific equipment (Bell et al., 2006).
Currently, 86 malaria RDTs are available from 28 different
manufacturers (WHO, 2008). Unlike conventional microscopic diagnosis by
staining thin and thick peripheral blood smears, and QBC technique, RDTs
are all based on the same principle and detect malaria antigen in blood
flowing along a membrane containing specific anti-malaria antibodies; they
do not require laboratory equipment. Most tests target a P. falciparum-
specific protein, e.g. histidine-rich protein II (HRP-II) or lactate
dehydrogenase (LDH). Some tests detect P. falciparum specific and pan-
specific antigens (aldolase or pan-malaria pLDH) and distinguish non-P.
Falciparum infections from mixed malaria infections. Although most RDT
products are suitable for P. falciparum malaria diagnosis, some also claim
that they can effectively and rapidly diagnose P. vivax malaria (Lee et al.,

Review of Literature
13
2009). Recently, a new RDT method has been developed for detecting P.
knowlesi (McCutchan et al., 2008).
RDTs provide an opportunity to extend the benefits of parasite-based
diagnosis of malaria beyond the confines of light microscopy, with potentially
significant advantages in the management of febrile illnesses in remote malaria-
endemic areas. RDT performance for diagnosis of malaria has been reported as
excellent (Doderer et al., 2007). However, some reports from remote malaria-
endemic areas have shown wide variations in sensitivity (Murray et al., 2008).
Murray and co-authors recently discussed the reliability of RDTs in an "update
on rapid diagnostic testing for malaria in their research (Murray et al., 2008).
Overall, RDTs appears a highly valuable, rapid malaria-diagnostic tool for
healthcare workers; however it must be used in conjunction with other
methods to confirm the results, characterize infection and monitor treatment.
In malaria-endemic areas where no light microscopy facility exists that may
benefit from RDTs, improvements are required for ease of use, sensitivity
for non-falciparum infection, stability, and affordability. The WHO is now
developing guidelines to ensure lot-to-lot quality control, which is essential
for the community's confidence in this new diagnostic tool (WHO, 2008). As
the simplicity and reliability of RDTs have been improved for use in rural
endemic areas, RDT diagnosis in non-endemic regions is becoming more
feasible, which may reduce time-to-treatment for cases of imported malaria
(Erdman et al., 2008).

Review of Literature
14
4.4-Serological tests
Diagnosis of malaria using serological methods is usually based on
the detection of antibodies against asexual blood stage malaria parasites.
Immunofluorescence antibody testing (IFA) has been a reliable serologic test
for malaria in recent decades (She et al., 2007).The literature clearly
illustrates the reliability of IFA, so that it was usually regarded as the gold
standard for malarial serology testing (Doderer et al., 2007). IFA is useful in
epidemiological surveys, for screening potential blood donors, and
occasionally for providing evidence of recent infection in non-immunes.
Until recently, it was a validated method for detecting Plasmodium-specific
antibodies in various blood bank units, which was useful for screening
prospective blood donors, so avoiding transfusion-transmitted malaria
(Mungai et al.,1978).
In France, for example, IFA is used as part of a targeted screening
strategy, combined with a donor questionnaire (Oh et al., 2008). The
principle of IFA is that, following infection with any Plasmodium species;
specific antibodies are produced within 2 weeks of initial infection, and
persist for 3-6 months after parasite clearance. IFA uses specific antigen or
crude antigen prepared on a slide, coated and kept at -30 until used, and
quantifies both IgG and IgM antibodies in patient serum samples. Titers >
1 : 20 are usually deemed positive, and < 1 : 20 unconfirmed. Titers > 1 :
200 can be classified as recent infections (Chotivanich et al., 2008).
In conclusion, IFA is simple and sensitive, but time-consuming. It
cannot be automated, which limits the number of sera that can be studied
daily. It also requires fluorescence microscopy and trained technicians;
readings can be influenced by the level of training of the technician,
particularly for serum samples with low antibody titers. Moreover, the lack
of IFA reagent standardization makes it impractical for routine use in blood-

Review of Literature
15
transfusion centers and for harmonizing inter-laboratory results (Tangpukdee
et al.,2009).
4.5-Molecular dignostic methods
4.5.1-PCR technique:
PCR-based techniques are a recent development in the molecular
diagnosis of malaria and have proven to be one of the most specific and
sensitive diagnostic methods, particularly for malaria cases with low
parasitemia or mixed infection (Morassin et al., 2002). The PCR technique
continues to be used extensively to confirm malaria infection, follow-up
therapeutic response, and identify drug resistance (Chotivanich et al., 2008).
It was found to be more sensitive than QBC and some RDTs (Makler et al.,
1998). Regarding the gold standard method for malaria diagnosis, PCR has
shown higher sensitivity and specificity than conventional microscopic
examination of stained peripheral blood smears, and now seems to be the
best method for malaria diagnosis (Morassin et al., 2002).
PCR can detect as few as 1-5 parasites/µl of blood (≤ 0.0001% of
infected red blood cells) compared with around 50-100 parasites/µl of blood
by microscopy or RDT. Moreover, PCR can help detect drug-resistant
parasites, mixed infections, and may be automated to process large numbers
of samples (Hawkes et al., 2007). Some modified PCR methods are proving
reliable as nested PCR, real-time PCR, and reverse transcription PCR, and
appear to be useful second-line techniques when the results of traditional
diagnostic methods are unclear for patients presenting with signs and
symptoms of malaria. They also allow accurate species determination
(Hawkes and Kain,2007).
Recently, the PCR method has become widely accepted for
identifying P. knowlesi infections (Cox-Singh et al., 2008). Although PCR

Review of Literature
16
appears to have overcome the two major problems of malaria diagnosis-
sensitivity and specificity- the utility of PCR is limited by complex
methodologies, high cost, and the need for specially trained technicians.
PCR, therefore, is not routinely implemented in developing countries
because of the complexity of the testing and the lack of resources to perform
these tests adequately and routinely. Quality control and equipment
maintenance are also essential for the PCR technique, so that it may not be
suitable for malaria diagnosis in remote rural areas or even in routine clinical
diagnostic settings (Hanscheid et al., 2008).
4.5.2-Loop mediated isothermal amplification (LAMP) technique:
It detects 18s ribosome RNA gene of P.falciparum. Observations suggest
that LAMP is more reliable and useful for routine screening for malaria
parasites in regions where vector-borne diseases, such as malaria, are endemic.
LAMP appears to be easy, sensitive, quick and lower in cost than PCR.
However, reagents require cold storage, and further clinical trials are needed to
validate the feasibility and clinical utility of LAMP (Erdman et al., 2008).
4.5.3-Microarrays:
Publication of the Plasmodium genome offers many malaria-
diagnostic opportunities (Doolan et al., 2008). The principle of the
microarrays technique parallels traditional Southern hybridization.
Hybridization of labeled targets divided from nucleic acids in the test sample
to probes on the array enables the probing of multiple gene targets in a single
experiment. Ideally, this technique would be miniaturized and automated for
point-of-care diagnostics (Holland et al., 2005). A pan-microbial
oligonucleotide microarray has been developed for infectious disease
diagnosis and has identified P. falciparum accurately in clinical specimens
(Palacios et al., 2007). This diagnostic technique, however, is still in the
early stages of development (Erdman et al., 2008).

Review of Literature
17
4.5.4- Flow cytometry (FCM) assay:
Flow cytometry has been used for malaria diagnosis (Izumiyama et
al., 2009). Briefly, the principle of this technique is based on detection of
hemozoin, which is produced when the intra-erythrocytic malaria parasites
digest host hemoglobin and crystallize the released toxic heme into
hemozoin in the acidic food vacuole. Hemozoin within phagocytotes can be
detected by depolarization of laser light, as cells pass through a flow-
cytometer channel. This method may provide a sensitivity of 49-98%, and a
specificity of 82-97%, for malarial diagnosis (Padial et al., 2005), and is
potentially useful for diagnosing clinically unsuspected malaria. The
disadvantages are its labor intensiveness, the need for trained technicians,
costly diagnostic equipment, and that false-positives may occur with other
bacterial or viral infections. Therefore, this method should be considered a
screening tool for malaria.
4.5.5-Automated blood cell counters (ACC):
An ACC is a practical tool for malaria diagnosis, with 3 reported
approaches. The first approach used a Cell-Dyn® 3500 apparatus to detect
malaria pigment (hemozoin) in monocytes, and showed a sensitivity of 95%
and specificity of 88%, compared with the gold-standard blood smear. The
second method also used a Cell-Dyn® 3500, and analyzed depolarized laser
light (DLL) to detect malaria infection, with an overall sensitivity of 72%
and specificity of 96% . The third technique used a Beckman Coulter ACC
to detect increases in activated monocytes by volume, conductivity, and
scatter (VCS), with 98% sensitivity and 94% specificity Although
promising, none of the 3 techniques is routinely available in the clinical
laboratory; further studies are required to improve and validate the
instrument and its software. These methods show apromising accuracy for

Review of Literature
18
detection of malaria parasite so that they would become avaluable and
routine malaria diagnostic method (Briggs et al., 2006).
4.5.6-Mass spectrophotometry:
` A novel method for in vitro detection of malaria parasites, with a sensitivity
of 10 parasites/µl of blood, has been reported recently. It comprises a
protocol for cleanup of whole blood samples, followed by direct ultraviolet
laser desorption mass spectrometry (LDMS). For malaria diagnosis, the
principle of LDMS is to identify a specific biomarker in clinical samples. In
malaria, heme from hemozoin is the parasite-specific biomarker of interest.
LDMS is rapid, high throughput, and automated. Compared with the
microscopic method, which requires a skilled microscopist and up to 30-60
min to examine each peripheral blood smear, LDMS can analyze a sample in
< 1 min However, the remote rural areas without electricity are inhospitable
for existing high-tech mass spectrometers. Future improvements in
equipment and techniques should make this method more practicable (Scholl
et al., 2004).
4.6-Culturing:
The methodological breakthrough for culturing the asexual
intraerythrocytic stages of Plasmodium falciparum parasites published over
35 years ago by Trager and Jensen (1976) is still used in most malaria
laboratories today (Butcher, 1979 and Schuster, 2002).
These basic culturing procedures have been essential to almost all
molecular, genomic, and immunological and biochemical studies of malaria
over the last 30 years and has been critical to the development of much-
needed drugs and vaccines. The procedure for maintaining P.falciparum in
vitro generally involves growing the parasites in static cultures in the
presence of human erythrocytes at low O2 conditions (& Hurd et al., 2003).
Review of Literature
21
One drawback of growing P. falciparum using static tissue culture flask
methods is the low yield of parasite material for the study of native parasite
molecules or organelles (Radfar et al., 2009).
Cultures of 5 ml (in T25 flasks) to ml (in T150 flasks) can be routinely
maintained at a 4–5% haematocrit and up to 5–10% parasitaemia. Further
bulking-up of parasite cultures requires establishing multiple flasks, which
becomes time consuming and labour intensive since each flask requires at
least one or two daily media changes, depending on parasitaemia levels
( Hurd et al., 2003).There have been few endeavours to develop large-scale
cultures of malaria parasites (Hurd et al., 2003). Most notable was the deep 7
L cultures of P. falciparum in large 15 Litre vessels whereby cells were kept
in suspension by stirring.
However, medium needs to be replenished by continuous flow and the
assemblage and dismantling of this large-scale apparatus was cumbersome
(Moloney et al., 1990). More recently, hollow-fibre capillary bioreactors have
been used to obtain asynchronous cultures of P. falciparum with high
parasitaemia, although these systems are of relatively low volume (Li et al.,
2003)
Radfar et al.,( 2009) reported a detailed stepwise protocol for the
production of synchronous parasite cultures at high parasitaemia. This
method used static cultures maintained at low haematocrit (0.8–1.5%) to
seed additional flasks to reach parasitaemia as high as 60%.
Other reliable malaria-diagnostic tests have been developed and
introduced and some tests are commercially available, for example, enzyme
linked immunosorbent assay (ELISA)/enzyme immunoassay (EIA) , latex
agglutination assay and post-mortem organ diagnosis (investigating malaria
parasites in tissue autopsy, e.g. liver and spleen , kidney and brain) have
also been described.However, parasite culture, molecular techniques,

Review of Literature
20
serology techniques and pathological diagnostic techniques, although
sometimes useful in research laboratories, but are not practical or
appropriate for the routine clinical diagnosis of malaria (Sachanonta et al.,
2008).

Materials and methods
23
Materials and methods
Study population
The present study was conducted on a total of 600 cases from Fayoum
governorate during a period of 13 months from March 2013 to March 2014.Out
of these 600 cases;500 cases were collected randomly from inhabitants of Abo –
Shanab and EL-Khaldia villages of Abshoy District. The remaining 100 cases
were selected from Fayoum Fever Hospital and were presenting with symptoms
suggestive of malaria as headache, fever or darkening of urine.
Sampling
Blood samples were collected from all cases included in the study.
Samples were collected in sterile syringes labeled with patient name and date of
collection.
Thin and thick blood films were immediately prepared and stained. The
remaining whole blood samples were transferred to clean sterile dry tubes
containing EDTA. Blood specimens were stored at 2°C-8°C for up to 3 days or
at -20°C for longer storage.
Plan of work
All cases included in the present study were subjected to the following:
1. History taking, symptoms and clinical examination.
2. Laboratory examination (blood film) for detection of different malarial
stages.
3. Immunological methods: by malaria pf/pan one step rapid test for detection
of plasmodium antigens in blood samples was performed only for 100 blood
samples obtained from 100 selected cases in Fayoum Fever Hospital.

Materials and methods
22
1- History taking and clinical examination.
Clinical data were obtained from each case in the present study according
to a clinical sheet that included the following items:
Personal history: name,age,sex and residence.
History of travelling abroad.
Present history(symptoms): rigors, fever,sweating,headache and darkening of
urine.
History of intak anti-malaria drug .
General examination for pallor and jaundice.
Abdominal examination for detection of splenomegaly.
2- Laboratory examination
(I) Giemsa staining preparation: (Clendennen et al., 1995 ).
Reagents:
1. Giemsa Stain: Concentrated liquid stock.
2. Absolute Methanol: acetone-free.
3. Phosphate Buffer Solution pH 7.2 (Giemsa buffer): used for dilution of
Giemsa stock.
Preparation of Phosphate Buffer Solution (Giemsa buffer):
Phosphate buffer solution (67 mmol / L, pH 7.2) was prepared according
to Hawkey and Lewis (2004) as follow:
1. Solution A: was prepared by adding 9.5 grams of disodium hydrogen
phosphate (anhydrous salt) (Oxford Lab., India) to 1 liter of distilled water to
obtain 67 mmol / L Na2HPO4.

Materials and methods
23
2. Solution B: was prepared BY dissolving 9.2 grams of sodium dihydrogen
phosphate (Oxford Lab., India) in 1 liter of distilled water to obtain 67 mmol
/ L NaH2PO4.
3. Phosphate Buffer Solution was prepared by mixing 72 ml of solution A
with 28 ml of solution B and 900 ml of distilled water .
Working solution was prepared by adding1 part of stock Giemsa solution
to 20 parts of phosphate buffer (pH 7.2). The prepared buffer should be clear
with no precipitates.
Blood samples were collected from all cases included in the present study and
examined (Chotivanich et al.,2006).
1. A clean glass slide was prepared.
2. Date,name and age of patient was written on slide .
3. The patient's finger was cleaned with 70% ethyl alcohol and allowed to dry
4. The side of fingertip was picked with a sharp sterile lancet to obtain blood
drops.
(II) Preparation of thin blood film :(Cheesbrough,1999).
A- The smooth edge of a spreader slide was placed in a drop of blood.
B- The angle between slide and spreader was adjusted to 45°.
C- The blood was smeared with a swift and steady sweep along the surface.
D- The film was allowed to air-dry and was fixed with absolute methanol.
E- The sample was stained with diluted Giemsa (1 : 20, vol/vol) for 20 min
F- The sample was washed by briefly dipping the slide in and out of a jar of
buffered water.

Materials and methods
24
G- The slide was then allowed to air-dry in a vertical position and examined
under a light microscope X100.
(III) Preparation of thick blood film: (Salako et al.,1999)
A- A blood spot was stirred in a circular motion with the corner of the slide.
B- Blood spot was allowed to dry without fixative.
C- The spot was stained with diluted Giemsa (1 : 20, vol/vol)for 20 min.
D- The slide was washed by placing the film in buffered water for 3Min.
E- The slide was allowed to air-dry in a vertical position and was examined
using a light microscope X1000.
3- Immunological methods:
Detection of Plasmodium falciparum and non-falciparum Plasmodium
antigens was done using the commercially available malaria pf/pan one step
rapid test[Abon Biopharm (Hangzhou) co.,Ltd,China].
The Malaria (Pf/Pan) One Step Rapid Test is a lateral flow chromatographic
immunoassay for the simultaneous detection and differentiation of antigens of
Plasmodium species in human blood samples or serum samples.
Test principle (Cooke et al., 1999)
The Malaria (Pf/Pan) One Step Rapid Test is a lateral flow
chromatographic immunoassay. The lysis buffer contains a detergent that lyses
the red blood cells and releases various Plasmodium antigens, which migrate by
capillary action across the strip held in the cassette. If plasmodium histidine rich
protein-II (pHRP-II) is present in the specimen, it will bind to the pHRP II-gold
conjugates. The immunocomplex is then captured on the membrane by the pre-
coated anti-pHRP-II antibodies, forming a burgundy colored Pf band, indicating
a plasmodium falciparum positive test result .

Materials and methods
25
If pLDH (plasma lactate dehydrogenase) is present in the specimen, it
will bind to the pLDH gold conjugates. The immunocomplex is then captured on
the membrane by the pre-coated anti pLDH antibody, forming a burgundy
colored band, indicating a Plasmodium positive test result. In the absence of pf
band, a positive test result for any of the other three Plasmodia can be
recommended .
Reagents
The Malaria (Pf/Pan) One Step Rapid Test comprises the following:
1) A burgundy colored conjugate pad containing mouse anti- pHRP-II antibody
conjugated with colloid gold (pHRP II-gold conjugates)and mouse anti-
pLDH antibody conjugated with colloid gold (pLDH-gold conjugates)
2) A nitrocellulose membrane strip containing two test bands (pf and pan bands)
and a control band (C band). Pf band is pre-coated with monoclonal anti-
pLDH antibody and polyclonal anti-pHRP-II antibodies by which the
infection with Plasmodia falciparum can be detected, the pan band is
precoated with monoclonal anti-pLDH antibody and polyclonal anti-pHRP-II
antibodies by which the infection with Plasmodim vivax,Plasmodium ovale
or Plasmodium malariae can be detected. While the control band (C band) is
coated with goat anti-mouse IgG .
3) Pipette dropper
4) Desiccant
5) Buffer
6) Package Inser
7) Timer
8) Lancing device for whole blood test.
Materials and methods
26
Methods (According to the manufacturer instructions)
The specimen and test components were brought to room temperature
before use. then the following steps were done:
1- The specimen was mixed well prior to assay.
2- The pouch was opened at the notch and device was removed. the test device
was Placed on a clean, flat surface .
3- The device was labeled with specimen’s ID number
4- The mini plastic dropper was filled with 10 µL of blood specimen
5- The dropper was hold vertically, the entire specimen was dispensed into the
center of the sample well -1(w1) making sure that there were no air bubbles .
6- Three drops (about 100-150 µL) of Lysis Buffer were added to W2
7- After five minutes, 1 full drop of buffer was added toW1.
8- The results were read after 15 minutes
Interpretation of results
Presence of C band was indicator of validity of the test.
Positive test for plasmodium falciparum infection was indicated by
development of pf band In addition to C band.
Positive test for Plasmodium vivax,Plasmodium ovale or Plasmodium
malariae was Indicated by development of pan band in addition to C band.
Negative test for all species was indicated by absence of pf and pan bands in
addition to the presence of C band.

Materials and methods
27
Figure (1): Malaria rapid test device positive for Plasmodium falciparum.
Figure (2): Malaria rapid test device negative for all Plasmodium species.

Materials and methods
28
Figure (3):Malaria p.f / pan rapid test device.

RESULTS
04
RESULTS
The present study was conducted on a total of 600 cases from Fayoum
governorate during a period of 13 months from March 2013 to March 2014. Out
of these 600 cases, 500 cases were randomly from inhabitants of Abo –Shanab
and EL-Khaldia villages of Abshoy District in a random manner. The remaining
100 were selected from Fayoum Fever Hospital and were presenting with
symptoms suggestive of malaria as headache, fever or darkening of urine. The
data collection lasted for six months from June 2013 to December 2013.
The examined populations were subjected to complete history taking and
detailed general examination. Blood samples were collected from all cases
included in the study and were subjected to thin and thick blood films in
addition to malaria pf/pan one step rapid test aiming at detection of malaria
antigens.
All data were collected and statistically analysed and presented as follow:
I. Demographic criteria of the examined population.
II. Clinical history.
III. Clinical examination.
IV. Results of thin and thick blood films.
V. Results of malaria pf/pan one step rapid test.

RESULTS
04
Demographic criteria of examined populations:
Age distribution
The examined population's ages ranged from 1 to 90 year.
The mean (average) age for all 600 cases participated in the study was
23.73±17.89 years old.
The mean (average) age of household cases was 23.30 ± 17.70. Two
hundreds and thirteen of them (42.6%) were below eighteen years old and 287
(58.4%) were above eighteen years old as shown in table (5) and Figure (4) .As
regard 100 selected cases it was found that ages ranged from 1 to 83 years with
mean of 25.89±18.70 years old. Twenty nine of selected cases (29%) were
below eighteen years old and 71 of them (71%) were above eighteen years old
as shown in figure (5) and table (6). .
Table (5): Age distribution of household cases.
Age Frequency Percentage
Child
Adult
213
287
42.6%
58.4%
Total examined populations 500 100 %
Figure (4): Age groups of the household cases
42.6
58.4
0
10
20
30
40
50
60
70
80
90
100
Childern Adult
pe
rce
nta
ge
Age

RESULTS
04
Table (6): Age distribution of selected cases.
Age Frequency Percentage
Child
Adult
29
71
29%
71%
Total examined populations 100 100 %
Figure (5): Age groups of the selected cases
Gender distribution:
Among the household cases, 160 (32%) were males and 340 were females
(68%) as shown in table (7) and figure (6).While among the 100 selected cases
,16 of them (16%) were males and 84 (84%) were females as shown in figure (7)
and table(8).

RESULTS
04
Table (7): Gender distribution of household cases.
Gender Frequency Percentage
male
female
160
340
32%
68%
Total examined populations 500 100 %
Figure (6): Gender distribution of household cases.
Table (8): Gender distribution of the selected cases.
Gender Frequency
Percentage
Male
Female
16
84
16%
84%
Total examined populations 100 100 %

RESULTS
00
Figure (7): Gender distribution of the selected cases.
Figure (7): Gender distribution of the selected cases.
History of travelling to malaria endemic area:
Out of 500 household cases, 80 cases (16%) gave a history of travel to Sudan as
shown in table (9). Nine persons (9%) of the selected cases from Fayoum Fever
Hospital gave a history of travel to Sudan as shown in figure (8).
Table (9): Number and percentage of household cases with history of travel to
Sudan .
Travelling abroad Frequency
(Total= 500) Percentage.
Yes
No
80
420
16%
84%
Total examined population 500 100 %

RESULTS
04
Figure (8): History of travelling abroad in the selected cases
History of intake anti-malaria drug:
Out of 500 household cases, 120 cases (24%) gave a history of intake
anti- malaria drug as shown in table (10).
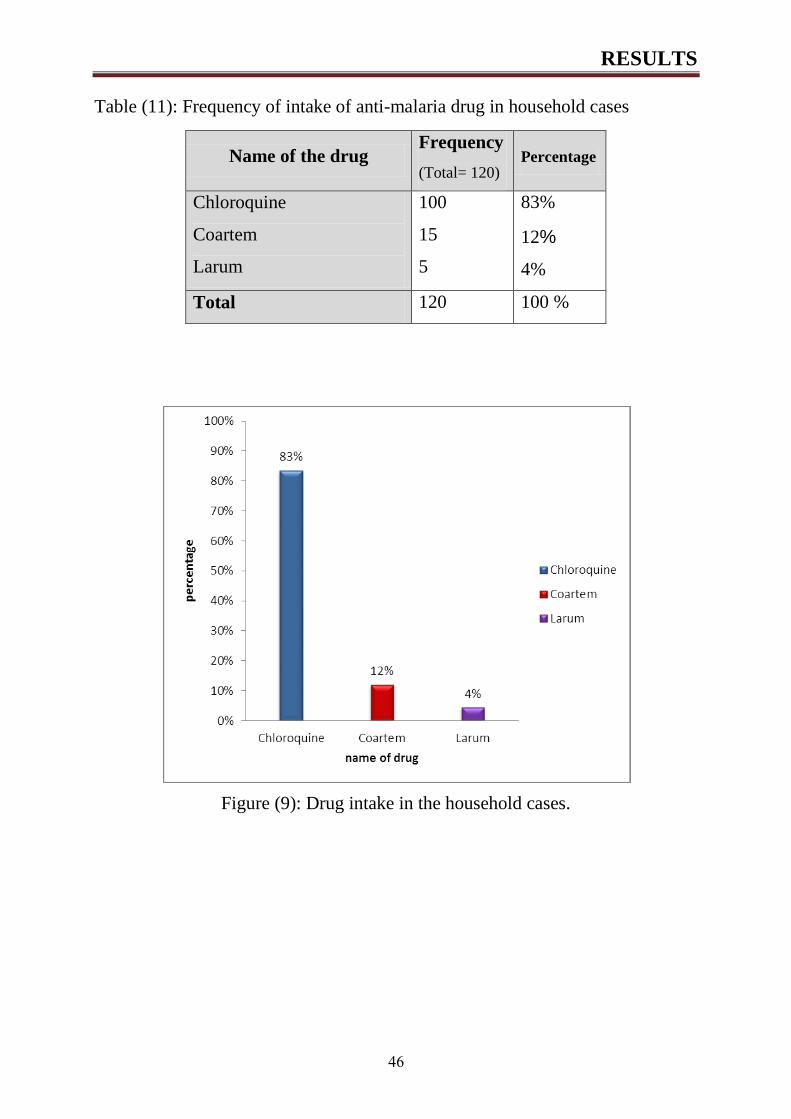
Chloroquine was given to 100 cases (83%), 15 cases received
Coartem(12%) and 5 cases (4%) received Larum as shown in table (11) and
Figure (9). Regarding the 100 selected cases, only 3 cases (3%) received
Coartem. These data are demonstrated in figure (10).
Table (10): History of intake of anti-malaria Drug in household cases
Intake of anti- malaria drug Frequency
(Total= 500) Percent.
Yes
No
120
380
24%
76%
Total examined patients 500 100 %
RESULTS
04
Table (11): Frequency of intake of anti-malaria drug in household cases
Name of the drug Frequency
(Total= 120) Percentage
Chloroquine
Coartem
Larum
100
15
5
83%
12%
4%
Total 120 100 %
Figure (9): Drug intake in the household cases.

RESULTS
04
Figure (10): Drug intake in the selected cases.
III-Symptoms detected by history taking and clinical examination of the
examined population incorporated in the study.
Out of 500 population, 416 persons (83.2%)had elevated body
temperature ,80 person (16%) had rigors, 47 persons (9.4%) had sweating, 18
persons (3.6%)had darkening of urine with no cerebral coma (0%) as shown in
figure (11).As regard the 100 selected cases, 99 (99%) had elevated body
temperature ,19 person (19%) had rigors, 12 persons (12%) had sweating, 4
persons (3.6%)had darkening of urine; while cerebral coma was absent (0%) as
shown in figure (12).

RESULTS
04
Figure (11): clinical symptoms detected in the household cases.
Figure (11): Clinical symptoms detected in the household cases
Figure (12): clinical symptoms detected in the selected cases.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
temperature rigors sweating darkeningof urine
fever withcoma
Pe
rcen
tage
Symptoms

RESULTS
04
Signs detected by clinical examination of populations incorporated in the
study:
Out of 500 population 43 persons (8.6%) had splenomegaly, 33 person
(6.6%) had hepatomegaly and 329 persons (65.9%) had pallor as shown in table
(12) and figure (13).
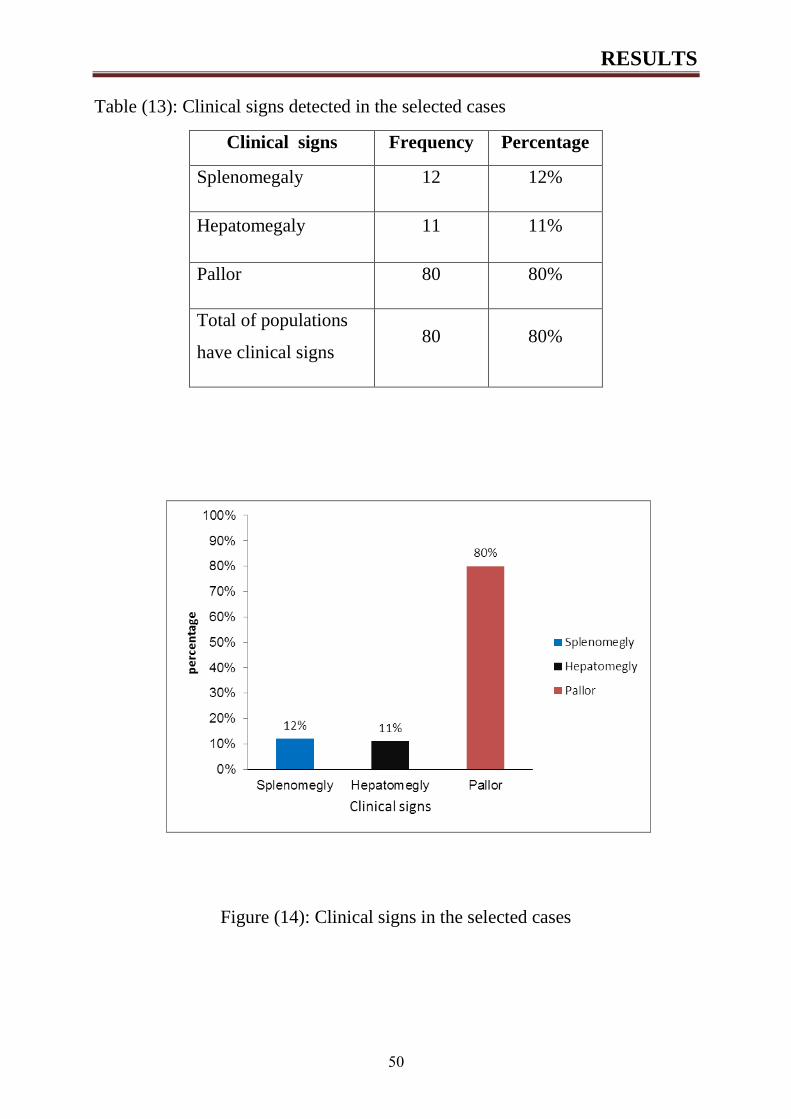
As regard 100 selected cases, it was found that 12 persons (12%) had
splenomegaly, 11 person (11%) had hepatomegaly and 80 persons (80%) had
pallor as shown in figure (14) and table (13).
Table (12): Clinical signs detected in household cases
Clinical signs Frequency Percentage
Splenomegaly 43 8.6%
Hepatomegaly 33 6.6%
Pallor 329 65.9%
Figure (13): Clinical signs detected in household case
RESULTS
44
Table (13): Clinical signs detected in the selected cases
Clinical signs Frequency Percentage
Splenomegaly 12 12%
Hepatomegaly 11 11%
Pallor 80 80%
Total of populations
have clinical signs 80 80%
Figure (14): Clinical signs in the selected cases
RESULTS
44
Results of microscopic examination of blood films
Blood samples were taken from all cases in the study. Thick and thin
blood films were prepared, stained with Giemsa and examined under oil
immersion lens at magnification of 1000 X. Microscopic examination of blood
films of the 500 cases revealed absence of Plasmodium stages in all cases
(100%). Ring stage of Plasmodium falciparum detected by thick blood film of
one of the 100 selected cases as shown in figure (15).
Figure (15): Thick blood film showing ring stage of Plasmodium falciparum
(magnification X1000).

RESULTS
44
Results of immunological test (One step rapid test):
Blood samples were obtained from 1oo selected cases from Fayoum
Fever Hospital and were tested using malaria (Pf/Pan) One Step Rapid Test to
detect Plasmodium falciparum antigen and other Plasmodium species. Three
cases (3%) were positive for Plasmodium falciparum antigen as shown in figure
(18) figure (20), but were negative for all species as shown in figure (19).
Figure (16): malaria (Pf/Pan) One Step Rapid Test applied for 100 selected cases

RESULTS
44
Figure (17): Malaria rapid test negative for all Plasmodium species.
Figure (18): Malaria rapid test positive for Plasmodium falciparum.

RESULTS
40
Distribution of positive cases as regard different characteristics (history
and clinical examination) (N=3)
Regarding demographic criteria of positive cases, it was found that the
mean (average) age was 32.7 ±11.2 and all cases were males. Regarding
travelling abroad, it was found that they came from Sudan after one visit.
Regarding clinical symptoms of positive cases it was found that all three cases
(100%) presented with fever, rigors and sweating with absence of darkening of
urine, cerebral coma, hepatomegaly and splenomegaly. All these are shown in
table (14) and figure (21).
Table (14): Distribution of positive cases as regard different characteristics
(history and clinical examination) (N=3)
Variable Mean SD
Age (Years) 32.7 11.2
Variable N %
Male gender 3 100.0
Fever 3 100.0
Rigor 3 100.0
Sweating 3 100.0
Dark urine 0 0.0
Coma 0 0.0
Hepatomegally 0 0.0
Splenomegally 0 0.0
History of drug taking
Coartem for 4 weeks
immediately after return from
sudan
3 100%
RESULTS
44
Statistical Analysis
Data was collected, coded, translated to English to facilitate data
manipulation and double entered into Microsoft Excel and data analysis
was performed using SPSS software version 22 under windows 7.
Simple descriptive analysis in the form of numbers and percentages for
qualitative data, and arithmetic means as central tendency measurement,
standard deviations as measure of dispersion for quantitative parametric
data was done.

Discussion
65
Discussion
About 3.3 billion people; half of the world's population-are at risk of malaria
leading to about 250 million malaria cases and nearly one million deaths every
year. People living in the poorest countries are the most vulnerable (WHO,
2009). Forty-one percent of the world's population lives in areas where malaria
is transmitted (e.g., parts of Africa, Asia, the Middle East, Central and South
America) (WHO, 2002).
The present study was conducted on a total of 600 cases from Fayoum
governorate during a period of 13 months from March 2013 to March 2014.Out of
these 600 cases,500 cases were selected from inhabitants of Abo –Shanab and
EL-Khaldia villages of Abshoy District in a random sampling. The remaining 100
were selected from Fayoum Fever Hospital and were chosen from those having
symptoms suggestive of malaria as headache, fever or darkening of urine.
All cases included in the present study were subjected to history taking, clinical
examination and laboratory examination (thin and thick blood film) for detection
of different malaria stages. Also, immunological method was done by malaria
pf/pan one step rapid test for detection of Plasmodium antigens in blood samples
collected from 100 selected cases in Fayoum Fever Hospital.
Blood samples were collected from all cases included in the study. Samples
were collected in sterile syringes labeled with patient name and date of
collection. For laboratory examination of samples thin and thick blood films
were immediately prepared and stained. The remaining whole blood samples
were transferred to clean sterile dry tubes containing EDTA. Blood specimens
were stored at 2°C-8°C for up to 3 days or at -20°C for longer storage.
Regarding age and gender, the examined cases ranged from 1 to 90 years with
average age of 23.73±17.89 years old. One hundred and sixty of participants
(32%) were males and three hundred and forty (68%) were females in the

Discussion
65
household cases and as regard 100 selected cases, Sixteen (16%) were males and
eighty four (84%) were females.
As regard gender and age of exposure to malaria; Rahman et al., (1993) showed
that males above 18 years old were more exposed to malaria than females and
those less than 18 years old were less exposed.
Canada statistics 2013 analysis indicated that the rate of imported
Plasmodium infection in males was twice that of females(Nelder et
al.,2013) .Also,predominance of men in imported malaria is well represented,
for example Western Australia , 80% of all cases are men (Baas,2006);
Amsterdam, the Netherlands(69%)(Smith,2008).
Risk of infection is often greater in men because they are more likely to migrate
to malaria-endemic areas for agricultural or mining work and more likely to
sleep outdoors during peak biting times of vector (Reuben, 1993).
Out of 500 household cases, 80 (16%) gave history of travel to malaria endemic
areas in addition to 9 cases of selected cases from Fayoum Fever Hospital. All
these cases gave history of travel to Sudan. Malaria appears to have been caught by
travel of persons to endemic country (Sudan) for working as in the present study,
all the three positive cases detected in the present work gave a history of traveling
to Sudan and this was in accordance with the Malaria Control Program reports that
published on WHO website in 2008.In this report, 23 cases of malaria were
discovered in Egypt in 2005, but they were imported from Sierraleon and Sudan.
They came immediately from the quarantine so no period of relapse.
In contrast, the researchers in the Military Fever Hospital, Egypt diagnosed
thirty six patients as having malarial disease. Twenty of them were recruited
from Peace Keeping Mission Forces in Africa and sixteen cases presented with
prolonged fever coming from different locations in Egypt. Their results showed
that two locally acquired cases were malaria positive. The detection of these two

Discussion
65
locally acquired cases in this study was diagnosed by the use of bone marrow
smears as they were negative by peripheral blood examination and that El-Gabal
El-Ahmar area (Cairo) was the most extensively infected region (37.4%). El-
Sharkia and El-Fayoum Governorates were next in order (18.7%) and (12.5%).
(El-Bahnasawy et al.,2010)
Malaria is an important threat not only for autochthonous populations, but also
for non-immune individuals travelling or working in malaria endemic areas.
According to the 2011 international travel and health book; approximately 125
million international travellers visit malaria-endemic countries yearly and over
10,000 cases are reported having malaria after returning home (WHO, 2011).
The incidence of imported malaria cases among UK travellers visiting West
Africa varied from 52 to 196 cases/1,000 traveller per year between 2003 and
2006 (Behrens et al.,2008). In a cohort of the French general population,
followed from 1994 to 1998, the incidence of malaria imported from endemic
areas was 178 cases per 1,000 travellers per year (Malvay et al., 2006).
In the French Armed Forces, the annual incidence rate was 14 per 1,000 people
per year in 2006. Amongest French soldiers who served in Ivory Coast between
1998 and 2007, the annual malaria incidence rate ranged from 37 to 388 cases
per 1,000 people per years (Gaeten et al., 2013).
Non-immune travellers should be protected from malaria by chemoprophylaxis and
prophylactic measures against mosquito bites (including insecticide-impregnated bed
nets, repellents and insecticide-treated long-sleeved clothes and pants). In malaria-
endemic areas, the use of most of these prophylactic measures is mandatory for non-
immune employees of most major international groups and soldiers.
However, the effectiveness of these measures is limited by the lack of compliance
(Sagui et al.,2011) even among military personnel (Michel et al.,2007) and even if

Discussion
65
the chemoprophylaxis is adapted to the chemosusceptibility of Plasmodium
falciparum(Henry,2007).
The increased number of malaria cases, occurring among traveller populations,
has been frequently attributed to behavioral factors. Machault et al., (2008)
stated that the lack of compliance with protective measures was identified as the
second most important factor that determined the malaria incidence rate among
non-immune travellers after environmental factors.
In Fayoum Goveronorate, it seems that malaria control achieved significant
progress when widespread indoor residual spraying (IRS) with long-lasting
insecticides and introduction of artemisinin combination therapy with
artemether-lumefantrine (Coartem©) and this led to absence of clinical cases of
endogenous malaria and interruption of malaria transmission (MOHP, 2006).
As regard the symptoms of malaria , out of 500 household populations, four
hundreds and sixteen persons (83.2%)had elevated body temperature, eighty
person (16%) had rigors, forty seven persons (9.4%) had sweating, eighteen
persons (3.6%)had darkening of urine and none with cerebral coma(0%).
As regard the 100 selected cases, ninety-nine (99%) had elevated body
temperature, 19 person (19%) had rigors, twelve persons (12%) had sweating,
four persons (4%) had darkening of urine and none with cerebral coma (0%).
Malaria paroxysms are defined by intense chills, fever and sweating caused by
new merozoites burst from the erythrocytes and infect more cells (Sadanand,
2010 ).
The study was in line with (Genton and D’ Acremont , 2001) who said that in
general, the majority of patients experience fever (>92%), chills (79%),
headaches (70%), and diaphoresis (64%) .
In the present study, fever was a constant symptom in malaria positive patients
and this was in accordance with the universal screening symptom for malaria in

Discussion
56
research studies (D’Acremont et al., 2010). In Fayoum, where the present study
was carried out, local clinical officers state that they must inquire about fever to
capture all cases of malaria.
On the contrary; Murray et al., (2007) stated that fever is not always a feature of
malaria, and signs may be unusual if prophylaxis has been given, and is partly
effective. Also; Sakaria et al., (2013) stated that the classic presentation of
malaria with paroxysms of fever is seen only in 50-70% of the patients. In
addition, Abdel-Wahab et al., (2012) studied the use of fever alone as a
presumptive prompt for anti-malarial treatment would result in a huge over-
treatment burden.
Bejon et al., (2010) reported that the clinical signs of malaria may be
nonspecific and parasitaemia accompanied by clinical symptoms consistent with
malaria does not necessarily imply clinical malaria especially in endemic areas.
In addition, Yaw et al.,(2014)stated that in non-endemic areas, peripheral
parasitaemia accompanied by fever could be used to define clinical malaria, In
endemic areas this is not so since over 60% of individuals could always have
asymptomatic parasitaemia. Illnesses such as typhoid fever, which companying
fever, could be confuse with clinical malaria because of accompanying
parasitaemia.
Out of 500 population forty three persons (8.6%)had splenomegaly, thirty three
person (6.6%) had hepatomegaly and three hundred and twenty-nine persons
(65.9%) had pallor and as regard 100 selected cases, it was found that twelve
persons (12%)had splenomegaly ,eleven person (11%) had hepatomegaly and
eighty persons (80%)had pallor.
There was absence of hepatomegaly ,splenomegaly , jaundice and cerebral coma
in the three positive cases, which had been reported in the literatures as common
signs associated with a complication of falciparum malaria (WHO,2010) and

Discussion
56
this was in contrast to El-Bahnasawy et al.,(2010).Their study was conducted in
Military Fever Hospital, Egypt where they found that cerebral coma occurred
and one patient died. This difference in the apparent complication maybe due to
early diagnosis and treatment by the use of multi-drug regimen (Coartem) in our
study in contrast to the monotherapy based one such as Chloroquine or
Mefloquine.
Of particular interest was the high percentage of pallor (80%) among the
selected cases but this was not due to malaria as pallor was absent in the three
positive cases. Pallor is most probably due to anemia due to low socioeconomic
levels.
The lack of classical severe malaria syndromes in malarial patients has
important implications for the surveillance of malaria, considering that many
healthcare facilities with limited resources throughout sub-Saharan Africa often
rely on clinical presentation and the ascertainment of coma, seizures and renal
failure for severe malaria diagnosis and management decisions in adults
(Reyburn et al.,2004). The data confirm the emphasis of WHO that reliance on
clinical features alone for the diagnosis of severe malaria is inaccurate
(WHO,2010).
As regard intake of chemoprophylaxis regimen in the 500 random population, it
was found that 105 (17%) of cases had a history of intake of chemoprophylaxis
regimen in the form of Chloroquine in100cases (95%), and Larum (Mefloquine
hydrochloride) 5 cases(5%). Because of its long half-life, mefloquine is the
preferred chemoprophylactic agent against Plasmodium falciparum malaria in
UNMIS. However, its side effects, which include vomiting, dizziness, syncope,
extra systoles, tinnitus, and emotional problems, cause some people refuse or
cease mefloquine.
In the present study, some of population (3%) received antimalarial drug; Coartem
(artemether-lumefantrine ) as a therapeutic agent and this was in line with WHO

Discussion
56
guidelines that documented that artemisinin derivatives should not be used as
monotherapies for the treatment of uncomplicated malaria because this can
promote resistance to this critically important class of antimalarial agents (WHO,
2011). However, in a randomized single-blinded clinical trial, dihydroartemisinin-
piperaquine was found to be superior to artemether-lumefantrine for reducing the
risk of recurrent parasitemia and gametocytemia. It also fostered better hemoglobin
recovery in the treatment of uncomplicated Plasmodium falciparum malaria
(Kamya et al., 2007).
In contrary to this, El-Bahnasawy et al.,(2010) said that monotherapy such
chloroquine or mefloquine is drug of choice for local cases.
Malaria diagnosis has for a long time, and particularly at community level,
depended on clinical diagnosis. However, this is unreliable due to the non-
specific nature of signs and symptoms of malaria leading to over-diagnosis and
over-treatment (Reyburn, 2010). Misdiagnosis can lead to inappropriate or
delayed treatment that has been implicated in malaria-associated deaths in
developed countries (Kain and Keystone,199).
Our results showed that the differences in detection rates of microscopy and
ABON PLUS (RDT) test are 0.16%, and 3% respectively. On the other hand,
reported studies from different countries of South Asia: Sri Lanka (Fernando et
al., 2004), Pakistan (Iqbal et al., 2003) .and Thailand. (Pattanasin et al.,2003)
that demonstrated 38%, 42%, 53% malaria positive cases were diagnosed among
studied groups using microscopy and RDTs. Also;Abdel-Wahab et al.,(2012)
showed that the differences in detection rates of microscopy, RDT test (45%,
42.5% respectively) in 120 clinically suspected cases.
Species differentiation in the positive samples by blood film examination
showed presence of P.falciparum in travellers coming from Sudan and this
coincides with reports on the high levels of P. falciparum disease activity in
Sudan.

Discussion
56
Accurate identification of malaria parasites to the species level is imperative so
that the patient receives appropriate therapy, particularly when the patient has
relapsing malaria caused by P. vivax and P. ovale It is also important because of
the severe morbidity and mortality associated with P. falciparum and growing
resistance to antimalarial therapy. Furthermore, it is vital to obtain follow-up
specimens from malaria-positive patients to monitor therapy outcome and detect
drug failure (Palmer et al., 2003).
Self-diagnosis of febrile illness with reliable malaria RDTs could accelerate
early therapy with the standby treatment, preventing complications and death, or
avoid unnecessary use of antimalarial (Magill,2006).
In the present study, the three cases were positive for Plasmodium falciparum by
malaria pf/pan one step rapid test in contrast to the thick smears which gave one
positive result.
In general, the screening of Giemsa stains (GS) by light microscopy is still
considered the gold standard (Jonkman, 1995). Microscopy is the preferred
diagnostic test for patients with severe febrile illness. This method is cheap and
simple but labor intensive and time consuming and requires well-trained
personnel (Reyburn,2004), particularly for the detection of low levels of
parasites (Gilles,1993). In resource-poor areas, microscopic diagnosis has been
shown to be insensitive and nonspecific, especially when parasitemias are low or
mixed infections are present(Amexo,2004,).. Because sensitivity of RDTs is low
when the parasite density <100/µl, the diagnosis of afebrile or atypical malaria
with low parasitemia mainly depended on microscopy ( Moody ,2002). The
sensitivity of thick-film microscopy is 10 to 30 parasites/μl of blood
(Gilles,1993). Therefore, lack of personnel experience in microscopic diagnosis
of malaria may bring the possibility of high false negative rates in the
microscopy test.

Discussion
56
In the present study, positive RDT with negative blood films may be explained
by treatment that clears parasitaemia with persistent of antigenaemia.
(WHO,2004). Other possible reasons include persistence of antigens due to
sequestration of malaria parasites from peripheral blood (Reyburn ,2006),
incomplete treatment, delayed clearance of circulating antigen (free or in
antigen-antibody complexes), and cross reaction with non- falciparum malaria,
rheumatoid factor or heterophile antibodies( Moody and Chiodini ,2002).
Thus, the slightly better RDT performance in our study is most likely due to two
facts. First, the study population consisted of non-immune, returning Sudan
travelers who typically have higher parasitemia levels than other studies’
populations in malaria endemic areas. Second, we compared the RDT to single
blood smears performed under “real world” conditions (rather than the gold
standard three tests read by expert malariologists) and finally hemolysis of the
blood during transport.
On the contrary, the successful implementation of RDT has been bedeviled by
poor product performance, inadequate methods to determine the quality of
products (Bell et al., 2006). Another group described the limitations of RDTs as
having: the inability to diagnose non falciparum malaria, variable heat stability
and safety risks related to blood sampling (especially HIV and hepatitis B). Also
of equal concern is that negative RDT results are often ignored and patients are
treated anyway (Christopher et al., 2008).
Therefore, it is important that the instruction for use (IFU) clearly mentions that
reading test results should be performed within the time specified in the IFU and
any test line becoming visible beyond the recommended reading time should be
ignored and this occurs clearly For One Step even reading a few minutes too late
resulted in some false positive P. falciparum test lines observed by the second
observer and explaining the low interobserver agreement.

Discussion
56
False negative results of RDTs have been attributed to possible genetic
heterogeneity of HRP2 or LDH expression, deletion or mutation of HRP2 or
LDH gene, presence of blocking antibodies, or immune-complex formation and
also inability of Optimal test to detect parasitaemia levels blow 100 parasites/μl
of blood (Chaijaroenkul , 2011).
However, limitations should be considered in this study. The present study used
a limited and selected number of samples, precluding calculation of predictive
values and providing wide confidence intervals for non-falciparum results.
Besides, the present study has not used a collection of samples comprising all
four human Plasmodium species at different parasite densities for providing
relevant data on diagnostic accuracy.

SUMMARY AND CONCLUSION
66
SUMMARY AND CONCLUSION
Malaria infection is a life threatening protozoan infection and is associated
with several adverse health outcomes. Almost 300 million clinical cases of
malaria occur worldwide each year and over a million people die. Almost
90% of these deaths occur in sub-Saharan Africa, where young children are
the most affected. Malaria is directly responsible for one in five childhood
deaths in Africa and indirectly contributes to illness and deaths from
respiratory infections, diarrhoeal disease and malnutrition. Fayoum
goveronorate had the Last focus of malaria which has been eradicated from
Egypt since 1998 according to WHO records .
The present study was designed to study the prevalence of malaria in some
localities in Fayoum governorate ; in addition to study the demographic
criteria of the examined population incorporated in this study and to
determine the likelihood of acquisition of malaria infection in this area using
thin and thick blood film, in addition to malaria pf/pan one step rapid test to
detect plasmodium antigen in blood samples.
Blood samples were collected randomly from 500 inhabitants of Abo —
Shanab and EL-Khaldia villages of Abshoy district and 100 selected cases
from Fayoum Fever Hospital in Fayoum governorate, Egypt during a period
of 13 months from March 2013 to March 2014. Thin and thick blood films
were immediately prepared and stained.
All cases included in the present study were subjected to history
taking ,clinical examination, laboratory examination(blood film ) for
detection of different malaria stages and immunological method by malaria
pf/pan one step rapid test for detection of plasmodium antigens in blood
samples was carried out only to the 100 selected cases in Fayoum Fever
Hospital.
In the current work, the examined populations ages ranged from 1 to 90
years. The mean (average) age for population participated in the study was
23.73±17.89 years old.

SUMMARY AND CONCLUSION
66
As regard the 500 household cases, 213 of participants (42.6%) were below
eighteen years old and 287 of them (58.4%) were above eighteen years old,
160 of them (32%) were males and 340 were females (68%).As regard the
100 selected cases it was found that ages ranged from 1 to 83 years with
mean (average) age 25.89±16.43 years old. Twenty nine of them (29%) were
below eighteen years old and seventy one (71%) was above eighteen years
old. Sixteen (16%) were males and eighty four (84%) were females.
History of travelling abroad to malaria endemic area showed that eighty
populations (1 6%) have been traveled and as regard the 100 selected cases it
was found that nine case (9%) have been travelled to Sudan.
History of intake anti-malaria Drug showed that one hundred and twenty
populations (24%) had a history of intake antimalaria drug out of one
hundred and twenty persons received malaria drug, 100 person (84%)
received chloroquine, 5 persons (4%) received larum and 15 persons (12%)
received coartem and as regard 100 selected cases it was found that 3
populations (3%) received Coartem.
Symptoms detected by history taking and clinical examination showed that
out of the 500 household cases, it was found that 416 persons (83.2%)had
elevated body temperature ,80 person (16%) had rigors, 47 persons (9.4%)
had sweating, 18 persons (3.6%) had darkening of urine with no cerebral
coma (0%).Regarding the 100 selected cases, 99 (99%) had elevated body
temperature ,19 person (19%) had rigors, 12 persons (12%) had sweating, 4
persons (4%)had darkening of urine; while cerebral coma was absent (0%).
Signs detected by clinical examination among the household cases showed
that it was found that 43 persons (8.6%) had splenomegaly, 33 person(6.6%)
had hepatomegaly and 329 persons (65.9%) had pallor. As regard the 100
selected cases, it was found that 12 persons (12% have splenomegaly, 11
person (11 %) had hepatomegaly and three 380 persons (80%) had pallor.
Demographic criteria of the three positive cases showed tha the mean
(average) age was 32.7 ±11.2 and all cases were males. Regarding clinical
symptoms of positive cases it was found that all three cases (100%)

SUMMARY AND CONCLUSION
66
presented with fever, rigors and sweating with absence of darkening of
urine , cerebral coma, hepatomegaly and splenomegaly.
Microscopic examination of thin and thick blood films obtained from the
500 house hold cases showed absence of Plasmodium stages while
microscopic examination showed ring stage of Plasmodium falciparum in
one case in the 100 selected cases. Using the malaria (pf/pan) rapid step test
among the 100 selected cases, it was found that three cases detected as
positive for Plasmodium falciparum antigen. None of the cases are positive
for other plasmodium species.
The results of the present study pointed to the prevalence of malaria
infection in some localities of Fayoum governorate and this was among
workers returning from Sudan. Also, RDT of malaria gave higher detection
rate (3%) in comparison to thick and thin blood films results which showed
lower detection (0.16%) for diagnosis of malaria.
In the present study, positive RDT with negative blood films may be
explained by treatment that clears parasitaemia with persistent of
antigenaemia. Other possible reasons include persistence of antigens due to
sequestration of malaria parasites from peripheral blood, incomplete
treatment, delayed clearance of circulating antigen (free or in antigen-
antibody complexes), and cross reaction with non- falciparum malaria,
rheumatoid factor or heterophile antibodies.

RECOMMENDATIONS
96
RECOMMENDATIONS
Malaria control programme should be strengthened along South Egypt
and Fayoum governorate and Oases to prevent reintroduction of malaria.
Combination of RDT and blood film examination is recommended for
accurate laboratory diagnosis of Plasmodium parasite. Thus, proper
treatment and control of infection can be achieved.
PCR is needed to evaluate validity of ABON PLUS test in diagnosis of
malaria.
Non-immune travellers should be protected from malaria by chemoprophylaxis
and prophylactic measures against mosquito bites (including insecticide-
impregnated bed nets, repellents and insecticide-treated long-sleeved clothes
and pants). .
Attention must be paid to prevention of mosquito vector of malaria in
suspected areas.

REFERENCES
07
REFERENCES
Abdel-Wahab, M.; Ismail, K. and El-Sayed, N. (2012): Laboratory diagnosis
of malaria infection in clinically suspected cases using microscopic
examination, OptiMAL Rapid Antigen test and PCR. P.U.J., 5(1):59-66.
Amexo, M.R.; Tolhurst, G. and Barnish, I. (2004): Malaria misdiagnosis:
effects on the poor and vulnerable. Lancet, 364(9448):1896-1898.
Baas, M.C.; Wetsteyn , J.C.; Van Gool, T. (2006):Patterns of imported
malaria at the Academic Medical Center, Amsterdam, The Netherlands. J.
Travel. Med., 13(1): 2–7.
Baird, J.K. (2009): Neglect of Plasmodium vivax malaria. Trends Parasitol.,
23(11):533-539.
Bassiouny, H.K. (1996): Determination of epidemiological factors causing
the persistence of malaria transmission in Fayoum goveronorate, final report
Alexandria, WHO Reginal Office for the Eastern Mediteranean.
Bassiouny, H.K. (2001): Bioenvironmental and meteorological factors
related to the persistence of malaria in Fayoum goveronorate aretrosoective
study. East. Medit. Health J., 7(6):895-906.
Behrens, R.; Carroll, B.; Smith , V. and Alexander, N. ( 2008): Declining
incidence of malaria imported into the UK from West Africa. Malar. J.,
7:235.
Bejon, P.;Williams ,T.N.; Liljander, A.; Noor, A.M.; Wambua, J.;
Ogada, E. Olotu, A.; Osier, F.H.; Hay, S.I.; Färnert, A. and Marsh,
K.(2010): Stable and unstable malaria hotspots in longitudinal cohort studies
in Kenya. PLoS Med.,7(7): 10.
Bell, D.; Wongsrichanalai, C. and Barnwell, J. (2006): Ensuring quality
and access for malaria diagnosis: how can it be achieved? In: Evaluating
Diagnostics Review. Available from www.nature.com/reviews/micro.
Bhandari, P.L.; Raghuveer, C.V.; Rajeev, A. and Bhandari, P.D. (2008):
Comparative study of peripheral blood smear, quantitative buffy coat and

REFERENCES
07
modified centrifuged blood smear in malaria diagnosis. Ind. J. Pathol.
Microbiol., 51(1):108–112.
Bharti, A.R.; Patra, K.P.; Chuquiyauri, R.; Kosek, M.; Gilman, R.H.L. and
lanos-Cuentas, A. (2006): Polymerase chain reaction detection of
Plasmodium vivax and Plasmodium falciparum DNA from stored serum
samples: implications for retrospective diagnosis of malaria. Am. J. Trop.
Med. Hyg., 77(3):444–446.
Briges, C.; Costa, A.D.; Freeman, L.; and Aucamp, I. (2006):
Development of an automated malaria discriminant factor using VCS
technology. Am. J. Clin. Path., 126(5):691-698.
Butcher, G.A. (1979): Factors affecting the in vitro culture of Plasmodium
falciparum and Plasmodium knowlesi. Bull. World Health Organ., 57 (S1):
17–26.
Chaijaroenkul, W.; Wongchai, T.; Ruangweerayut, R. and Na-
Bangchang, K. (2011): Evaluation of rapid diagnostics for Plasmodium
falciparum and P. vivax in Mae Sot malaria endemic area, Thailand. Korean
J. Parasitol., 49(1): 33-38.
Cheesbrough, M. (1999): District laboratory practice in tropical countries.
Cambridge: Cambridge University Press. pp, 178-309.
Chotivanich, K.; Silamut, K. and Day, N.P.J. (2006): Laboratory diagnosis
of malaria infection-a short review of methods. Aust. J. Med. Sci., 27:11–15.
Chotivanich, K.; Silamut, K.U.; Domsangpetch, R.; Stepniewska, K.A.;
ukrittayakamee, S.; Looareesuwan , S. and White, N.J. (2008) : Ex-vivo
short-term culture and developmental assessment of Plasmodium vivax.
Trans. R. Soc. Trop. Med. Hyg., 95(6):677–680.
Christopher, J.; Hopkins, H.; Ansah, E.; Leslie, T. and Reyburn, H.
(2008): Opportunities and threats in targeting antimalarials for the AMFm:
the Role of Diagnostics. Discussion paper prepared for the Consultative
Forum on AMFm- the Affordable Medicine Facility- malaria Available at
www.rrf.org.

REFERENCES
07
Clendennen, T.E.; Long, G.W. and Baird, K.J. (1995): QBC and Giemsa
stained thick blood films: diagnostic performance of laboratory technologists.
Trans. R. Soc. Trop. Med. Hyg., 89(2):183–184.
Cook, G.C.; Manson, P. and Zumla, A. (2009): Malaria. In: Manson's
tropical diseases. 22nd: Saunders; pp., 1201-1300.
Cooke, A.H.; Chiodin, P.L. and Doherty, T. (1999): Comparison of a
parasite lactate dehydrogenase base immunochromotographic antigen
detection assay with microscopy for the detection of malaria parasite in
human blood samples. Am. J. Trop. Med. Hyg., 60 (2):173.
Cox-Singh, J. Davis, T.M.; Lee, K.S.; Shamsul, S.S; Matusop, A.; Ratnam,
S.; Rahman, H.A.; Conway, D.J. and Singh, B. (2008):Plasmodium knowlesi
malaria in humans is widely distributed and potentially life threatening. Clin.
Infect. Dis., 46(2):165–171.
D’Acremont, V.; Lengeler, C. and Genton, B. (2010): Reduction in
the proportion of fevers associated with Plasmodium falciparum
parasitaemia in Africa: a systematic review. Malar. J., 9:240.
Dahesh, S.M.; Bassiouny, H.K. and El-Masry, S.A. (2009):
Socioeconomic and environmental factors affecting malaria infection in
Fayoum Governorate, Egypt. J. Egypt Soc. Parasitol., 39(2):511-523.
Daneshvar, C.; Davi, T.M.; Cox-Singh, J.; Rafa'ee, M.Z.; Zakaria, S.K.
and Divis, P.C. (2009): Clinical and laboratory features of human
Plasmodium knowlesi infection. Clin. Infect. Dis., 49(6):852-860.
Daoud, A.I.E. (2003): Malaria situation in Egypt, formal report by Ministry
of Health.
Doderer, C.; Heschun, A.; Guntz, P.; Cazenave, J.P.; Hansmann, Y.;
Senegas , A.; Pfaff, A.W.; Abdelrahman, T. and Candolfi, E. (2007): A new
ELISA kit which uses a combination of Plasmodium falciparum extract and
recombinant Plasmodium vivax antigens as an alternative to IFAT for
detection of malaria antibodies. Malar. J., 6:19.
Dollan, D.L.; Mu, Y.; Unal, B. and Sundresh, S. (2008): Profiling
humoral immune response to P. falciparum infection with protein
microarrays. Proteomics, 8(22):4680-4694.

REFERENCES
07
D'Ortenzio, E.; Godineau, N.; Fontanet, A.; Houze, S.; Bouchaud, O.
and Matheron, S. (2008): Prolonged Plasmodium falciparum infection in
immigrants, Paris. Emerg. Infect. Dis., 14:323-326.
El-Bahnasawy, M.; Dabbous, H. and Morsy, T. (2010): Imported malaria
as a threat to Egypt. J. Egypt. Soc. Parasitol., 40(3):773-788.
Erdman, L.K. and Kain, K.C. (2008): Molecular diagnostic and surveillance
tools for global malaria control. Travel Med. Infect. Dis., 6(1-2):82–99.
Fernando, S.D.; Karunaweera, N.D. and Fernando, W.P. (2004):
Evaluation of a rapid whole blood immunochromatographic assay for the
diagnosis of Plasmodium falciparum and Plasmodium vivax malaria. Ceylon
Med. J., 49(1):7-11.
Gaeten,V.; Machault, T.; Meili, B.; Jean-Paul, B. and Christophe, R.
(2013): Environmental determinant of malaria cases among travellers. Malar.
J., 12: 87.
Genton, B. and D’Acremont, V. (2001): Clinical features of malaria in
returning travelers and migrants In : Travelers’ malaria.Schlagenhauf, P.
Hamilton: BC Decker: 371–392.
Ghosh, A.; Edwards, M.J. and Jacobs-Lorena, M. (2000): The journey of
the malaria parasite in the mosquito: hopes for the new century. Parasitol.
Today, 16(5): 196 - 201.
Ghosh, A.; Srinivasan, P.; Abraham, E.G.; Fujioka, H. and Jacobs-
Lorena, M. (2003): Molecular strategies to study Plasmodium-mosquito
interactions. Trends Parasitol., 19 (2): 94 - 101.
Gilles, H. M. (1993): Diagnostic methods in malaria. In: H. M. Gilles and D.
A. Warrell (eds.), Bruce-Chwatt's essential malariology, 3rd edition. Edward
Arnold, London, United Kingdom. pp., 78-95
Hanscheid, T.; Melo-Cristino, J. and Pinto, B.G. (2008): Automated
detection of malaria pigment in white blood cells for the diagnosis of malaria
in Portugal. Am. J. Trop. Med. Hyg., (64):290–292.
Harb, M. (1994): Malaria situation in Egypt. Annual report, Ministry Of
Health and Population, Cairo.

REFERENCES
07
Harinasuta, T. and Bunnang, D. (1988): The clinical features of malaria.
In: Wernsdorfer, W.H. and McGregor, I. (eds), Malaria: principles and
practice of malariology. Churchill Livingstone. pp., 709-734.
Hassan, M. A.; Kenawy, H.; Abdelsattar, A. and Sowielm, M. (2003):
GIS-based prediction of malaria risk in Egypt. East. Mediterr. Health J.,
9(4):549.
Hawkes, M. and Kain, K.C. (2007): Advances in malaria diagnosis. Expert
Rev. Anti Infect. Ther., 5(3): 485-495.
Hay, S.I.; Guerra, C.A.; Tatem A.J.; Noor, A.M and Snow, R.W. (2004):
The global distribution and population at risk of malaria: past, present and
future. Lancet Infect. Dis., 4(6): 327 – 336.
Henry, M.; Diallo, .;, Bordes, J.; Ka, S.; Pradines, B.; Diatta, B.;
M'Baye, P.; Sane, M.; Thiam, M.; Gueye, P . ; Wade, B.; Touze, J.;
Debonne, J.; Rogier C.; and Fusai, T.(2007): Urban malaria in Dakar,
Senegal: chemosusceptibility and genetic diversity of Plasmodium
falciparum isolates. Am. J. Trop. Med. Hyg., 75:146–151.
Holland, C.A. and Kiechle, F.L. (2005): Point of care molecular diagnostic
systems-past, present and future. Curr. Opin. Microbiol., 8(5):504-509.
Hurd, H.; Al-Olayan, E. and Butcher, G.A. (2003): In vitro methods for
culturing vertebrate and mosquito stages of Plasmodium. Microbes Infect.,
5(4): 321–327.
Iqbal, J.; Muneer, A.; Khalid, N. and Ahmed, M.A. (2003): Performance
of the OptiMAL test for malaria diagnosis among suspected malaria patients
at the rural health centers. Am. J. Trop. Med. Hyg., 68:624-628.
Izumiyama, S.; Omura, M.; Takasaki, T.; Ohmae, H. and Asahi, H.
(2009): Plasmodium falciparum development and validation of a measure of
intraerythrocytic growth using SYBR Green I in a flow cytometer. Exp
Parasitol., 121(2):144-150.
Jonkman, A.R.A.; Chibwe, C.O.; Khoromana, U.L.; Liabunya, M.E.;
Chaponda, G.E.; Kandiero, M.E. and Molyneux, T. E. (1995): Cost-

REFERENCES
07
saving through microscopy based versus presumptive diagnosis of malaria in
adult outpatients in Malawi. Bull. World Health Organ., 73:223-227.
Kain, K.C. and Keystone, J.S. (1998): Malaria in travelers. Epidemiology,
disease, and prevention. Infect. Dis. Clin. North Am., 12:267–284.
Kamya, M.R.; Yeka, A.; Bukirwa, H.; Lugemwa, M. and Rwakimari,
J.B. (2007): Artemether-lumefantrine versus dihydroartemisinin-piperaquine
for treatment of malaria: A randomized trial. Plos Clinical Trials 2.
Kenawy, M.A.; Beier, B.C.; Asiago, C.M.; El Said, S.E. and Roberts,
C.R. (1990): Interpretation of low-level Plasmodium infection rates
determined by ELISA for anophelines (Diptera: Culicidae) from Egyptian
oases. J. Med. Entomol., 27(4): 681 - 685.
Land, K.M. (2003): The mosquito genome: perspectives and possibilities.
Trends Parasitol., 19(3):103-105.
Lee, K.S.; Cox-Singh, J. and Singh, B. (2009): Morphological features and
differential counts of Plasmodium knowlesi parasites in naturally acquired
human infections. Malar. J., 8:73.
Leech, J.H.; Barnwell, J.W.; Aikawa, M.; Miller, L.H.; and Howard, R.
J. (1984a): Plasmodium falciparum malaria: association of knobs on the
surface of infected erythrocytes with a histidine-rich protein and the
erythrocyte skeleton. J. Cell Biol., 98(4): 1256-1264.
Leech, J. H.; Barnwell, J. W.; Aikawa, M.; Miller, L. H.; and Howard,
R. J. (1984b): Identification of a strain-specific malarial antigen exposed on
the surface of Plasmodium falciparum-infected erythrocytes. J. Exp. Med.,
159(6):1567-1575.
Li, T.; Glushakova, S. and Zimmerberg, J. (2003): A new method for
culturing Plasmodium falciparum shows replication at the highest
erythrocyte densities. J. Infect. Dis., 187(1):159–162.
Machault, V.; Orlandi-Pradines, E.; Michel, R.; Pagès, F.; Texier, G.;
Pradines, B.; Fusaï, T.; Boutin, J. and Rogier, C. (2008): Remote sensing and
malaria risk for military personnel in Africa. J. Travel Med., 15(4):216–220.

REFERENCES
07
Magill, A.J. (2006): Malaria: diagnosis and treatment of falciparum malaria
in travelers during and after travel. Curr. Infect. Dis. Rep., 8(1): 35–42.
Makler, M.T.; Palmer, C.J. and Ager, A.L. (1998): A review of practical
techniques for the diagnosis of malaria. Ann. Trop. Med. Parasitol.,
92(4):419–433.
Malvy, D.; Pistone, T.; Rezvani, A.; Lancon, F.; Vatan, R.; Receveur,
M.C.; Durand, I.; Hercberg, S. and El Hasnaoui, A.(2006): A. Risk of
malaria among French adult travellers. Travel Med. Infect. Dis., 4(5):259–
269.
Marchiafava, E. and Celli, A. (1885): Nouve recherché sulla infezione
malarica.Arch.Sci. infezione malarica. Arch. Sci. Med. Torino., 9:311–340.
McCutchan, T.F.; Piper, R.C. and Makler, M.T. (2008): Use of malaria rapid
diagnostic test to identify Plasmodium knowlesi infection. Emerg. Infect.
Dis., 14:1750–1752.
Michel, R.; Ollivier, L.; Meynard, J.; Guette, C.; Migliani, R. and
Boutin, J. (2007): Outbreak of malaria among policemen in French
Guiana. Mil. Med., 172:977–981.
Miller, L.H.; Roberts, T.; Shahabuddin, M. and McCutchan, T.F.
(1976): Analysis of sequence diversity in the Plasmodium falciparum
merozoite surface protein-1 (MSP-1). Mol. Biochem. Parasitol., 59(1): 1 - 14.
Ministry Of Health and Population – MOHP (2006): Egypt, malaria
report May, Cairo
Moloney, M.B.; Pawluk, A.R. and Ackland, N.R.(1990): Plasmodium
falciparum growth in deep culture. Trans. R. Soc. Trop. Med. Hyg., 84:516–
518.
Moody, A. (2002): Rapid diagnostic tests for malaria parasites. Clin.
Microbiol. Rev., 15(1):66–78.
Moody, A. and Chiodini, P.L. (2002):Non-microscopic method for malaria
diagnosis using OptiMAL IT: A second-generation dip-stick for malaria
pLDH antigen detection. Br. J. Biomed. Sci., 59(4):228–231.

REFERENCES
00
Morassin, B.; Fabre, R.; Berry, A. And Magnaval, J.F. (2002): One year's
experience with the polymerase chain reaction as a routine method for the
diagnosis of imported malaria. Am. J. Trop. Med. Hyg., 66(5):503–508.
Mungai, M.; Tegtmeier, G.; Chamberland, M. and Parise, M. (2001):
Transfusion-transmitted malaria in the United States from 1963 through
1999. N. Engl. J. Med., 344(26):1973–1978.
Murray, C.K.; Gasser, R.A.; Magill, A.J. and Miller, R.S. (2008): Update
on Rapid Diagnostic Testing for Malaria. Clin. Microbiol. Rev., (21): 97–
110.
Murray, L.; Ian, W.; Tom, T. and Chee, K.C. (2007): Malaria:treatment and
prophylaxis, cerebral malaria (Plasmodium falciparum), Oxford Hand Book
of Clinical Medicine. Oxford University Press, England, 385.
Nelder, M.; Russell, C.; Williams, D.; Johnson, K. and Li, L. (2013):
Spatiotemporal Dynamics and Demographic Profiles of
Imported Plasmodium falciparum and Plasmodium vivax Infections in
Ontario, Canada (1990–2009). PLoS ONE 8(9): e76208.(Canada statistics,
chronological index ).
Ngasala, B.; Mubi, M.; Warsame, M.; Petzold, M.G.; Massele, A.Y.;
Gustafsson, L.L.; Tomson, G.; Premji, Z. and Bjorkman, A. (2008) : Impact
of training in clinical and microscopy diagnosis of childhood malaria on anti-
malarial drug prescription and health outcome at primary health care level in
Tanzania: a randomized controlled trial. Malar. J., 7:199.
Nigatu, W.; Abebe, M. and Dejene, A. (1992):Plasmodium vivax and P.
falciparum epidemiology in Gambella, South-West Ethiopia. Trop. Med.
Parasitol., 43(3): 181 - 185.
Ochola, L.B.; Vounatsou, P.; Smith, T.; Mabaso, M.L. and Newton, C.R.
(2006): The reliability of diagnostic techniques in diagnosis and management
of malaria in absence of a gold standard. Lancet Infect. Dis., (6):582–588.
Oh, J.S.; Kim, J.S.; Lee, C.H.; Nam, D.H.; Kim, S.H.; Park, D.W.; Lee, C.K.;
Lim, C.S. and Park, G.H. (2008):Evaluation of a malaria antibody enzyme
immunoassay for use in blood screening. Mem. Inst. Oswaldo Cruz.,
103(1):75–78.

REFERENCES
07
Ohrt, C.; Sutamihardia, M.A.; Tang, D. and Kain, K.C. (2002): Impact of
microscopy error on estimates of protective efficacy in malaria prevention
trials. J. Infect. Dis., 186(4):540–546.
Padial, M.M.; Subirats, M. and Puente, S. (2005): Sensitivty to laser light
depolarization analysis for detection of malaria in blood samples. J. Med.
Microbiol., 54(Pt 5):449-452.
Palacios, G.; Quan, P.L. and Jabado, O.J. (2007): Panmicrobial
oligonucleotide array for diagnosis of infectious diseases. Emerg. Infect.
Dis., 13(1):73-81.
Palmer, C.J.; Bonilla, J.A. and Bruckner, D.A. (2003): Multicenter study
to evaluate the OptiMAL test for rapid diagnosis of malaria in U.S.
Hospitals. J. Clin. Microbiol., 41(11):5178-5182.
Pattanasin, S.; Proux, S. and Chompasuk, D. (2003): Evaluation of a new
Plasmodium lactate dehydrogenase assay (OptiMAL-IT) for the detection of
malaria. Trans. R. Soc. Trop. Med. Hyg., 97(6):672-674.
Payne, D. (1988): Use and limitations of light microscopy for diagnosing
malaria at the primary health care level. Bull. WHO, 66(5):621–628.
Radfar, A.;Mendez, D.;Moneriz, C.;Linares, M.; Marin-Garcia, P.;
Puyet, A.; Diez, A. and Bautista, J.M. (2009):Synchronous culture of
Plasmodium falciparum at high parasitemia levels. Nat. Protoc., (4):1899–
1915. Correct this reference in the text Radfar not Radfa
Raether, W.; Enders, B. and Hoffman, J. (1989): Antimalarial activity of
new floxacrine-related acridinedione derivatives:studies on blood
schizontocidal action of potential candidates against P.berghei in mice and P.
falciparum in vivo and in vitro. Parasitol. Res., 75(8):619-626.
Rahman, W.A.; Abu Hassan, A.; Adanan, C.R. and Abdul Hamid, K.
(1993): Malaria transmission in remote village located in northern peninsular
Malaysia near the malaysia-Tailand border. Trop. Biomed., (9):83-89.
Reuben, R. (1993): Women and malaria-special risks and appropriate
control strategy. Soc. Sci. Med., 37(4): 473–480.

REFERENCES
07
Reybun, H.R.; Mbita, C.; Drakel, I.; Carneiro, E.; Mwakasungula, O.;
Mwerind, K. ; Saganda, J.; Shao, A.; Kitua, R. and Olom, B.M.(2004):
Overdiagnosis of malaria in patients with severe febrile illness in Tanzania: a
prospective study. BMJ, 329:1212.
Reyburn, H. (2010): New WHO guidelines for the treatment of malaria.
BMJ, 340:c2637.
Reyburn, H.; Ruanda, J.; Mwerinde, O.; Drakele, C. (2006): The
contribution of microscopy to targeting antimalarial treatment in a low
transmission area of Tanzania:aprospective study. Malar J., 5:4.
Rosenberg, R.;Wirtz, R.A.; Schneide, I. and Burge, R. (1990):An
estimation of the number of malaria sporozoites ejected by a feeding
mosquito. Trans. Roy. Soc.Trop. Med. Hyg., 84(2):209-212.
Sachanonta, N.; Medana, I., M.; Roberts, R. and Jones, N. (2008):
Hostvascular endothelial growth factor is tropic for Plasmodium falciparum-
infected red cell. Asian Pac. J. Allergy Immunol., 26(1):37-45
Sadanand, S. (2010): Malaria: An Evaluation of the Current State of Research
on Pathogenesis and Antimalarial Drugs. Yale J. Biol. Med., 83: 185–191.
Sagui, E.; Resseguier, N.; Machault, V.; Ollivier, L.; Orlandi-Pradines,
E.; Texier, G.; Pages, F.;Michel, R.; Pradines, B.; Briolant, S.;
Buguet ,A.; Tourette-Turgis, C. and Rogier, C. (2011):Determinants of
compliance with anti-vectorial protective measures among non-immune
travellers during missions to tropical Africa. Malar. J., 10:232.
Sakaria, A.; Mahajan, S.; Desai, R. and Shah, K. (2013): Delayed
cerebellar ataxia: A rare self limiting complication of Plasmodium
falciparum malaria. Adv. Biomed Res., 2:27
Salak, L.A.; Akinyanju, O. and Afolabi, B.M. (1999): Comparison of the
standard Giemsa –stained thick blood film with Quantative Buffy Coat
Tecnique in malaria diagnosis in Nigeria. Niger Q.J. Hosp. Med., 9:256-269.
Schmidt, G.D. and Roberts, L.S. (1985): Phylum Apicomplexa: Malaria
and piroplasms.149 –178. In: Schmidt GD, Roberts LS. Foundations of
ParasitologyTimes ,Mirror/Mosby College Publishing, St. Louis, Missouri.

REFERENCES
77
Scholl, P.F.; Kongkasuriyachai, D. and Demirev, P.A. (2004): Rapid
detection of malaria infection in vivo by laser desorption mass spectrometry.
Am. J. Trop. Med. Hyg., 71:546–551
Schuste, F. (2002): Cultivation of Plasmodium spp. Clin. Microbiol. Rev.,
15(3): 335-364.
She, R.C.; Rawlins, M.L.;Mohl, R.; Perkins, S.L.; Hill, H.R. and Litwin,
C.M. (2007): Comparison of immunofluorescence antibody testing and two
enzyme immunoassays in the serologic diagnosis of malaria. J. Travel Med.,
14(2):105–111.
Shehata, M.G.; Kenawy, M.A.; El Said, S.M.; Beier, J.C. and Gwadz, R.
(1989): Anopheles sergenti (Theobald) a potential malaria vector in Egypt.
Ann. Parasitol. Hum. Comp., 64(1): 72 - 76.
Smith, A.D.; Bradley, D.J.; Smith, V.; Behrens, R.; Chiodini, P.;
(2008): Imported malaria and high risk groups: observational study using UK
surveillance data 1987-2006. B.M.J., 337.
Szmitko, P.E.; Kohn, M.L. and Simor, A.E. (2008): Plasmodium
falciparum malaria occurring 8 years after leaving an endemic area. Diagn.
Microbiol. Infect. Dis., 63(1):105-107.
Tangpukdee, N.; Duangdee, C.; Wilairatana, P. and Krudsood, S.
(2009): Malaria diagnosis: a brief review. Korean J. Parasitol., 47(2): 93-102.
Taylor, T.E. and Strickland, G.T. (2003): In: Hunter's tropical medicine
and emerging infectious diseases. Hunter GW, Strickland GT. Eighth (eds).
Philadelphia: Saunders. pp, 614-643.
Warhurst, D.C and Williams, J.E. (1996): Laboratory diagnosis of malaria. J.
Clin. Pathol., (49):533–538.
Warrell, D.A.; Looareesuwan, S.; Warrell, M.J.; Kasemsarn, P.;
Intaraprasert, R. and Bunnag, D. (1993): Dexamethasone proves
deleterious in cerebral malaria. A double-blind trial in 100 comatose patients.
N. Engl. J. Med., (306):313-319.
World Health Organization (1996): WHO information consultation on
recent advances in diagnostic techniques and vaccines for malaria: a rapid

REFERENCES
77
dipstick antigen capture assay for the diagnosis of falciparum malaria. Bull
World Health Organ., (74):47–49.
World Health Organization (1999): The World Health Report 1999:WHO
Library Cataloguing in Publication Data.The world health report 1999:
Making a difference. World Health Organization. Geneva, Switzerland.
World Health Organization (2002): The World Health Report: reducing
risks, promoting healthy life. Geneva, World Health Organization.
World Health Organization (2004): Africa malaria report, 2003. World
Health Organization, Geneva, Switzerland.
World Health Organization (2006): Guidelines for the treatment of
malaria, (1):133–143. World Health Organization, Geneva, Switzerland.
World Health Organization (2008): List of known commercially available
antigen-detecting malaria RDTs. World Health Organization, Geneva,
Switzerland.
World Health Organization (2009): The World Health Report 2009:10
facts on malaria.
World Health Organization (2011): Guidelines for the treatment of
malaria, (2):13–15. World Health Organization, Geneva, Switzerland.
World Health Organization (2011): International travel and health book.
World Health Organization, Geneva, Switzerland.
World Health Organization (2012): WHO Global Malaria
Programme .World Health Organization, Geneva, Switzerland.
World Health Organization (2012): WHO malaria report 2011.World
Health Organization, Geneva, Switzerland.
Yaw, A.; Afrane, G.; Andrew, K. and Guiyun, Y. (2014):Clinical malaria
case definition and malaria attributable fraction in the highlands of western
Kenya. Malar. J., 13(1): 405

الملخص العربي
٠ؼزجش شع االس٠ب األشاع اطف١١خ از رذد ح١بح األسب، ب ػالت طح١خ
١ حبخ ظبثخ ثزا اشع غبج١ز ف أفش٠م١ب 033خ١خ،فبن ب٠مشة
حبالد فبح مذ 5ح١ثب ٠ى االؽفبي اوثش ػشػخ ف سؤي ػ فبح حبخ ى
زشبس اإلطبثخ ثشع االس٠ب ف ثؼغ بؽك طذ ز اذساسخ ؼشفخ ذ ا
كما تم استخداموزه ؼشفخ اظفبد اذ٠خشاف١خ الشخبص اذساسخ ,حبفظخ اف١
)االث ثس(السريع وحيد الخطوة واختبار المجهري لجميع حاالت الدراسة الفحص
ا ثطش٠مخ ىشف ػ از١د١بد اجالصد٠ ف ػ١بد اذ ئخ شخض از٠ اخز
زمبح سزشف ح١بد اف١ اشزجخ ف١ اإلطبثخ ثبالس٠ب إو١١ى١ب
شخض اخزا ثطش٠مخ ػشائ١خ لش٠ز اث 533شخض ث١ 033لذ ر فحض
شخض اخزا ثطش٠مخ زمبح سزشف ح١بد 033شت اخبذ٠خ ثبالػبفخ ا
-0الس٠ب إو١١ى١ب رزشاذ اػبس اشخبص اذساسخ اف١ اشزجخ ف١ اإلطبثخ ثب
خذ خالي 03 ,90 ثؼذي احشاف 30 ,30سخ، ثزسؾ ػش 03
%( لذ سبفشا ا ا اسدا دخ 05شخض ) 90االسزمظبء أ ب٠مشة
س٠ب %( لذ ربا أد٠خ ؼبدح ال32شخض) 033ثءح ثبالس٠ب خذ ا٠ؼب ا
5,%( شخض ربا اىسر03١)05 ,%(92شخض ربا اىسو٠) 033
%( اىسر١ ابئخ حبخ 0اشخبص )0ث١ب ربي .%( ربا ا١ش2أشخبص)
ازب٠ؼخ سزشف ح١بد اف١
%( ٠ؼب رؼخ 9شخض ) 20رج١ خالي افحض االو١١ى ا ب ٠مشة
%( ٠ؼب 50شخض ) 030,%( ٠ؼب رؼخ ثبىجذ0شخض ) 00 ,ثبطحبي
شخض 03شحة اخ ث١ اشخبص اذساسخ اض١خ ث١ب خذ ا ب ٠مشة
93,%( ٠ؼب رؼخ ثبىجذ00شخض ) 00 ,%( ٠ؼب رؼخ ثبطحبي 03)
. اح١بد%( ٠ؼب شحة اخ ث١ اشخبص اذساسخ ازمبح 93شخض )
%( ٠ؼب 90شخض ) 203رج١ خالي افحض االو١١ى ا ب ٠مشة
%( شخض 0)23%( ٠ؼب اشػشخ 00شخض ) 93اسرفبع دسخخ احشاسح
٠ؼب اؼشق غ غ١بة اؼبػفبد ث اغ١جثخ اخ١خ ث١ اشخبص اذساسخ
%( ٠ؼب 00شخض ) 00ا ب ٠مشة رج١ خالي افحض االو١١ى ,اض١خ
%( 03شخض ) 03%(٠ؼب اشػشخ 00) 00 اسرفبع دسخخ احشاسح
٠ؼب اؼشق ف اشخبص اذساسخ ازمبح اح١بد

خالي افحض ادش ثأسزخذا افحض ادش ره د١غ حبالد اذساسخ
٠ىشف االز١د١بد از رزدب ؽف١١بد االس٠ب اخزجبس ح١ذ اخطح اسش٠غ از
أظشد ازبئح إطبثخ ثالس حبالد ثبالس٠ب ثبسزخذا اخزجبس ح١ذ اخطح
%( ، حبخ احذح ثبسزخذا افحض ادش 0اسش٠غ)االث ثس( ثؼذي )
و احبالد %( ، وبذ االس٠ب ز١دخ ا ألطبثخ ثطف١ افب سجبس، وبذ16.ثؼذي )
٠ؼض زا افبسق ا ا اؼالج لذ اصاي اطف١ غ ثمبء االز١د١بد ,افذح اسدا
ا احظبس اطف١ اذسح اطشف١خ ا ز١دخ رفبػ غ ؼب اشبر٠ذ ادسب
.ا١ز١شف١١خ

دراسة انتشار االصابة بمرض المالريا في بعض مناطق محافظة الفيوم تـوطـئة لمحصـول عمـي درجـة المـاجـسـتير في عمـم الطفيمـيات الطبية رسالـة
مقدمـة مـن
الطـبيـب / جمعة دسوقى امام حسانين بكالوريوس الطب والجراحة
الطبيةمعيد بقسم الطفيميات جامعـة الفيــوم –كمية الطب
تحت إشــراف
أ.د / مايسة محمد كامل الطفيميــات الطبيـةأستـاذ عمـم جامعـة القاهـرة –كميـة الطـب
أ.د.م / نجالء عبد الخالق الشربيني أستـاذ مساعد طب المجتمع
جامعـة الفيــوم –كميـة الطـب
د / سمر سيد عطية مـدرس عمـم الطفيميــات الطبيـة
جامعـة القاهرة –كميـة الطـب
كميـة الطـب جامعـة القاهـرة
م 2012