powerpoint presentationmedicine2.keele.ac.uk/val/presentation.pdf · so you may be asking who is...
TRANSCRIPT
1

Slide 2
I feel very privileged to be here in this auditorium and our wonderful new building. To use the phrase of the young, born in another time, it is pretty awesome ! I also bear a deep sadness as I think of Helen Lester, such a key lead for academic primary care and for the college who died earlier this year. Helen was the last to receive a similar college honour: the James McKenzie award. How lucky I have been to have survived, to date, through the same illness. She was so less fortunate: one of the profound inequities of life. So I wish very much to hold her in our thoughts today and I dedicate this lecture to her memory. Helen was a wonderful speaker and these words encapture I feel the legacy she has left us.
“As pines keep the shape of the wind even when the wind has fled and is no longer there so words guard the shape of man even when man has fled and is no longer there.”(ref) from "Mr. Stratis Thalassinos Describes a Man" Georges Seferis
Helen was wonderful in shaping her words and arguments and will live on in our minds for what she achieved . Just as the achievements of Sir William Pickles have lived on 44 years after his death.
2

Slide 3: Acknowledgements
I am also grateful for all those who have supported me in being here today . Before I start I really want to acknowledge them
The Keele team:
Mike Lancaster for his invaluable help with these graphics and Steven Harper for his technical expertise .
My critical Keele friends: Peter Coventry, Simon Gay, Andy Hassell, Bob McKinley, Kay Mohanna , Sarah Yardley for their time and invaluable input to the dress rehearsal.
Sir Denis Pereira Gray for his kind and generous support in providing background bibliography and advice.
Family, friends and colleagues for being here today.
3

Slide 4: First let me explain the title ?
Some who know me well as a medical educationalist, will have heard it before. It has very much been my mantra over the years: an old Hebrew proverb: “Do not confine children to your own learning for they were born in another time.”
Why do we always harp back to how we were educated regretting what has been lost. The world as viewed through the eyes of the young is so very different now and will be even more so in the future.
We face the same challenge as general practice changes. There is a strong , and natural, tendency to look back to the old arguably unsustainable values and we struggle to look forward.
We have to recognise that the different values adopted by the younger generations may be better placed for the future world.
So you may be asking who is this little fellow flying up into the sky?
4

Slide 5 : Le Petit Prince
,
Well, he’s Le Petit Prince. As I contemplated the gap we have at Keele between our expectations for ,and those of ,our students (most notably a very significant disconnect around electronic communication as our students seem to have long ago abandoned email), then Le Petit Prince came to mind .
A treasured rather grubby novel from my youth as you see here from the cover. This is a charming story narrated by the French author Antoine de Exupery of his encounter, when he was stranded in the Sahara desert following a plane crash, with the Little Prince who was visiting earth from his tiny asteroid B-612 (where the sun sets 47 times a day).
I recalled his frustrated exposition of the generation gap. It related to this drawing : to his fury interpreted by adults as “ a hat” . In fact it was this: “ a boa constrictor digesting an elephant”.
There was no attempt to understand his interpretation. He was advised to abandon drawing and concentrated of geography , history, mathematics and grammar!
5

The ongoing revelations of the small isolated world of the Prince’s planet compared to earth hold hidden messages for adults. They seem to me only too well to illustrate the gap between our understanding as adult educators and that of those we are preparing for the future. He will therfore help guide us through this lecture :
5
Slide 6: Overview :
So what am I aiming to do?
Firstly of course Sir William Pickles; to acknowledge why he was so ahead of his time and then explain why I have chosen to focus on undergraduate education and bemoan secondary care dominance in this field and our seeming inability to change this.
Secondly I will explore my view of the implications of how exponential world change will impact on future health care and the role of doctors . Your visions may be different and , sadly, traditionally in this forum there is no discussion .
Please feel free to twitter or email as I would be interested in your views . I have not yet mastered facebook!
And then to three key areas I have selected to explore related to some of my educational research which suggests there is potential to work to reduce distance and increase understanding : I will discuss:
6
The generation gap focusing on global awareness as a key to reducing cultural differences and health inequities
The doctor –patient relationship arguing for a move away from the patient centred formulaic models to acknowledge the flexibility needed to facilitate the two way doctor patient interaction
The individual : It seems increasingly clear to me that unless we understand our own individuality and background , we cannot develop the resilience needed to face the implications of world change
This all relates to the opportunities fostered within generalist practice so I will conclude with recommendations for change .
6
Slide 7 William Pickles
There can be no doubt that Sir William Pickles was a remarkable man for his time.
He was the son of a general practitioner and a Leeds man, as is my father. We share the Yorkshire background.
Sir William attended Leeds Grammar School and then Leeds Medical School qualifying in 1910.
From 1913 until the end of his professional life he was a General Practitioner in Wensleydale, North Yorkshire.
He was global though. He travelled widely as a ship’s doctor, survived two world wars serving in the navy during the second one .
But his Wensleydale practice and community was his main stay throughout his career. It was from there that he achieved fame both for himself and General Practice .
7

This small red book ‘Epidemiology in a Country Practice’ , is an account of this research which tracked the spread of disease within his community, and led him to academic recognition . He was able to track infections across his practice and make important deductions on the mode of spread.
Sir Denis Pereira Gray kindly summarised for me what he felt were William Pickle’s keys to success? This was the answer:
His meticulous observation of his professional life
He was ahead of the field—few GPs were writing in the BMJ and Lancet in the 1930s
This led to his progression from a service GP into academic life
He was highly respected and this was honoured by the University of Leeds
He was International recognised: he delivered a Cutter Lecture at Harvard
He was a natural choice to be the first President of the College
I wonder given his experience of two wars and huge change in general practice as the NHS was established whether he would agree with what I am to say today or feel it was unnecessary concern and just say “one has to adapt”. Certainly he represents a generation who survived exponential world change as did my father who was studying at Leeds University during the second world war and ,aged 91, is in the audience today.
7

Here are my father and late mother whose war romance was described recently in the Leeds alumni journal
Which was searching for war romances. They report:
“The most enduring romance came from Donald Vincent (chemistry 1942) and Hazel Vincent (Chemistry 1943)
Who last year celebrated the 70th anniversary of their wartime romance when they met across a bench in the organic chemistry laboratory” … They married in 1944 and have been followed in Leeds by a son and grandaughter.
8
Slide 9 Denis
Here are those 4 graduates, my mother and father , brother David and daughter Katherine all here in the audience today along with my other brother Bob and my son Sam both of whom strayed from the family Leeds tradition.
Why am I dwelling on William Pickle’s Leeds University association? Well I have chosen to focus on his progression into academic life; a pathway I followed almost serendipitously after 12 years as a GP in Kent.
Dennis Periera Gray made this comment :
That Sir William was awarded an honorary degree at Leeds when most went to specialists and still do.
This resonates with my experience :
9
Slide 10 :
I have been privileged to be the Head of the Medical School at Keele for three years.
Just take a look at the Deans of UK medical schools; now 34 in number. The figures are dismal. As far as recollections go back over more than 20 years there have only been four GP deans; one recruited from Australia. . Yet GPs are excellent educators and do so much to support undergraduate teaching. At least a third of all GPs teach medical students. Why this failure to achieve this level of influential leadership?
Well I feel as a college we take some responsibility.
We have failed to recognise, despite quite substantial published evidence, that if we are to recruit the brightest and best into what is after all, I would argue, the most difficult speciality, we must engage much more proactively with medical students.
We need to link much more closely with the Society for Academic Primary Care (where much of the UG education leadership occurs) and Medical School Council.
10

Our current objective for the year, as stated in the RCGP strategy , to “Contact 20% of medical schools to offer talks on GP as a career” is far from enough.
10
Slide 11
The responsibility as Dean though is quite awesome:
“We live in a world where change is exponential and we are helping to prepare students for jobs that don’t yet exist, using technologies that have not yet been invented, in order to solve problems that we don’t know are problems yet.
In short, we have a responsibility to prepare our students for a lifetime of uncertainty, change, challenge and emergent or self-created opportunity”.
And a huge burden to bear as an educator if you see it that way. Nobody could have foreseen what now exists and who are we to assume that we can for see medicine in 20-30 years time?
Many of my peers now take me aside to point out, in essence, what a poor job I am doing!
Masked by comments which start with “what do you think Val?: Why are they (their
11
junior doctors) so “Inexperienced? They have no knowledge (certainly of anatomy). There is no professional commitment. “ What are you doing? It was SO different in our day.
Yet in my day the wards were full of post myocardial infarction patients who were treated with 28 days on complete bed rest. One of my consultants insisted the cure for haematemesis was to get the patient to suck ice in peace with the curtains drawn round the bed. The pace was relatively slow. The average hospital stay approaching 12 days. It is now 3 days. None of the high technology, high bed turn over and current pressures of the modern NHS and European directives.
11
As a college we hold, I believe, a huge responsibility for training our future doctors by the very virtue of what we do.
For the purpose of this lecture I have chosen to work with the definition of generalist practice offered by Joanna Reeve and her Liverpool colleagues.
“Generalist practice is decision-making which is person-focused, not disease-focused, which is continuous and not episodic, which integrates the biographical and the biotechnical knowledge… all with a view to supporting health as a resource for living and not an end in itself.”
This for me not only captures the essence of what we do but provides an excellent platform for students to learn some of the skills essential for this uncertain future.
I will be returning to this definition throughout the talk to illustrate the contribution generalism can make .
I would emphasise though the interest of my secondary care colleagues in the need for generalism in hospitals too. These are skills now much in need in both settings.
12
Slide 13 So time to move on to contemplate with Le Petit Prince the implications for the future.
You might like to hold in your minds what you feel are the challenges we, or our young, face globally. Yours might differ from my three top choices so feedback later would be really most welcome.
Mine our :
Transformation of knowledge
Reversal of world dominance
Climate change
13
The transformation of knowledge; by this I mean the changes we are seeing in the holding, processing and transmission of knowledge . Probably the most significant change in my life time and I cannot envisage what is to come. Nor have I found to date anyone who can.
This slide shows a characterisation used by Richard and Sylvia Cruess in one of their seminal papers on professionalism. Their intent is to demonstrate the power doctors have held for generations as the one who held all the knowledge. A power which has been gradually erased by the internet and IT technology.
Does it matter? Well it certainly seems to worry medical students both in the UK and internationally . One of our students, when I was in Manchester, Thomas Mole, did a project for me interviewing students in Manchester , Kerala, India and Mansoura, Egypt on their views on patient centredness and professionalism .
Thematic analysis of the transcripts revealed that students globally felt frustrated and upset by the loss of power they had perhaps anticipated would be there for them. It was an international issue as illustrated by these quotes:
14
A South Indian, Female said:
Doctors get irritated easily because of these [educated] patients who are coming, they’re having some knowledge of the disease…
And a Manchester, White British Male,
“Patients come in …wanting …treatment and …that’s what sometimes doctors find very frustrating.”
There was a sense of bereavement at the loss of power, or possibly security , they perceived medicine offered them.
14
Slide 15:
And undoubtedly professional values and attitudes will change. To me this cartoon depicts it all.
Who leads? Certainly future doctors will need to follow rather than lead as other health professionals gain more power and status as the rather impotent surgeon in this team dynamic illustrates.
Where will knowledge be held and how will it be transmitted ? We used to carry around huge textbooks. Everything now is on iphones. What next?
And above all the impact the communication of knowledge is having on Professionalism. The new social media are causing, often unwittingly , students and doctors to find themselves in challenging and unprofessional situations which lead to fitness to practise procedures and even, dismissal from the course . This seems to be an increasing international experience,
15
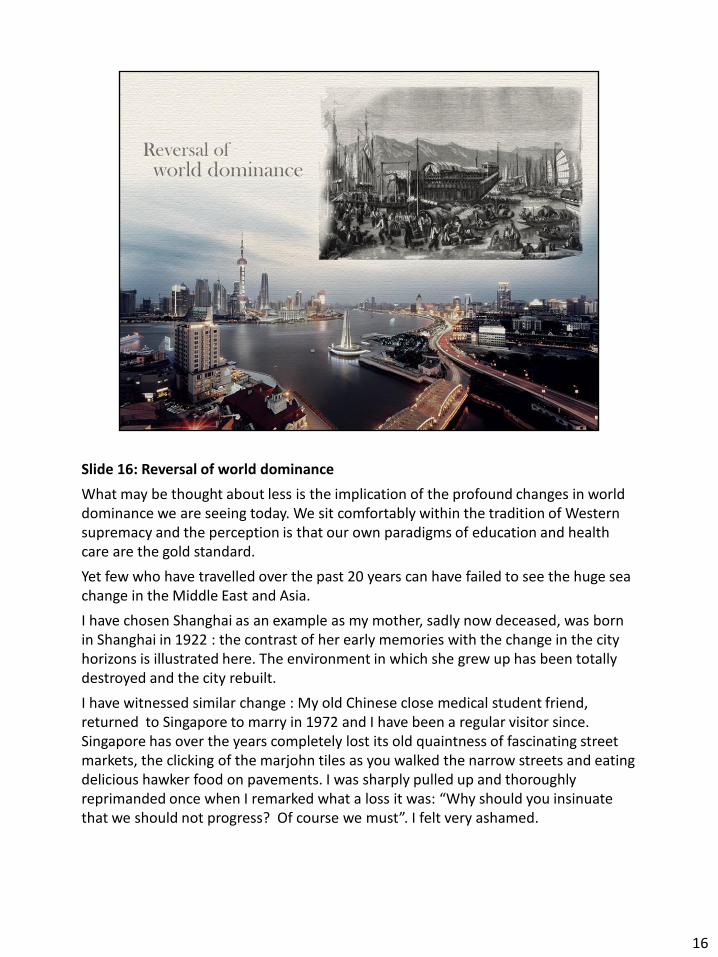
Slide 16: Reversal of world dominance
What may be thought about less is the implication of the profound changes in world dominance we are seeing today. We sit comfortably within the tradition of Western supremacy and the perception is that our own paradigms of education and health care are the gold standard.
Yet few who have travelled over the past 20 years can have failed to see the huge sea change in the Middle East and Asia.
I have chosen Shanghai as an example as my mother, sadly now deceased, was born in Shanghai in 1922 : the contrast of her early memories with the change in the city horizons is illustrated here. The environment in which she grew up has been totally destroyed and the city rebuilt.
I have witnessed similar change : My old Chinese close medical student friend, returned to Singapore to marry in 1972 and I have been a regular visitor since. Singapore has over the years completely lost its old quaintness of fascinating street markets, the clicking of the marjohn tiles as you walked the narrow streets and eating delicious hawker food on pavements. I was sharply pulled up and thoroughly reprimanded once when I remarked what a loss it was: “Why should you insinuate that we should not progress? Of course we must”. I felt very ashamed.
16

Slide 17
These changes are fully reflected in the economic forecasts. This Financial Times front page hit me a month ago.
It demonstrates the average upgrade (in blue) and downgrade (in red) of economies since 2007.
From left to right, Latin America, Asia and Eastern Europe have gained. Of those in decline Europe has fared the worst.
It seems inevitable to me that we are preparing our young for work in a new world where Asia dominates. This is a fundamental challenge given we see ourselves today as the model and brand to inform development.
Let me read you a quote from an American article:
“Here are the stark numbers. By 2020 India will be graduating four times as many college graduates as the United States.
By 2030, China will have 200 million college graduates—more than the entire U.S. workforce.
The central question before us is how do we compare with our global competitors in supporting and investing in our most valuable asset, our children? They are investing more than ever in their future while the United States is fighting to keep up.”
17
Slide 18
I am not going to dwell on my third choice: climate change. The announcement last week that we have the highest recorded carbon dioxide levels is enough. Some forecast that by the end of the century we will no longer have a sustainable planet
Perhaps in the West we are in denial. My work though in South Asia developing the MRCGP[INT] examination has highlighted to me though the overwhelming reality of times to come . Catastrophic floods, drought, crop failure and energy rationing seem to be increasingly common.
Yet as Lord Nigel Crisp so has so eloquently highlighted we have so much to learn from the developing world. I am humbled, at times overwhelmed, by the resilient resourcefulness of my South Asia colleagues who faced with electricity cuts : sometimes one hour on one hour off in intense heat, poor resources, gas shortage and the consequent political unrest with endless security threats and killings manage to achieve at a superb level. I have learnt much including relatively minor practicalities : for example a mobile phone makes an excellent torch when you are trying to locate the toilet!
18
Slide 21
I thank Kay Mohanna for this quote which aptly illustrates the point. The question is
Will the young automatically adapt or do we have the moral obligation as educators to provide them with the skills? Should we confine them to our own learning or make every effort to prepare them for these future changes we can predict are on the horizon? If so as generalists I will argue we have the skills both to do this and embed generalist primary care principles in their learning which , I believe, is hugely important for future global health .
19

Slide 22
I would be so interested in your thoughts at this stage but my curiosity needs to be set aside in the formalites of this setting. BUT when I went to re read the Lancet report on Health Professionals for a new century and find this quote: :
I was reassured to find this
Read quote
“All health professionals in all countries should be educated to mobilise knowledge and to engage in critical reasoning and ethical conduct so that they are competent to participate in patient and population-centred health systems as members of locally
responsive and globally connected teams.”
This supports my argument to date : I particularly like the term “mobilise knowledge”;
The emphasis on “critical reading and ethical conduct”, in patient and population-centred health systems of course supports my argument for generalist practice and I will come back to the locally responsive and globally connected teams .
20
Slide 21:
So now we move on with the little Prince to our credibility as educators.
As the story goes when this famous Turkish astronomer discovered a new planet in 1909
and presented his finding at the International Conference of Astronomy now one believed him on account of the way he dressed.
He tried again in 1920 in this elegant suit and this time everyone was in total agreement with his findings.
In the interest of internationalism though I am going to stick with the cultural dress.
21
Slide 21:
So now we move on with the little Prince to our credibility as educators.
As the story goes when this famous Turkish astronomer discovered a new planet in 1909
and presented his finding at the International Conference of Astronomy now one believed him on account of the way he dressed.
He tried again in 1920 in this elegant suit and this time everyone was in total agreement with his findings.
In the interest of internationalism though I am going to stick with the cultural dress.
22
Morally I feel responsible as an educator to try and close some of the distance between us and our future doctors : to let go of our time and set about closing the distance illustrated by “le chapeau” and the poor elephant being digested by the boa constrictor. “ As intimated in my overview I want to look to change supported by my research in three areas
Distance between :
- generations and cultures; - doctor and patient ; - within individuals
23

“ As intimated in my overview I want to look to change supported by my research in three areas
Distance between :
- generations and cultures; - doctor and patient ; - within individuals
I hope this will synthesise into 3 memorable take home messages
24
Slide 24
Firstly global awareness, Le Petit Prince spends a great deal of time on asteroid B-612 caring for his planet: decoking his volcanoes, weeding, fighting the baobab trees and cherishing his one tender rose.
How can we work to decrease the distance between generations and between cultures?
Within the college we have a strong force moving us in this direction.
25
Slide 25 :
That is : The junior international committee composed of GP trainees and those in their first 5 years of practice : shown here at their recent annual conference on the 5th floor terrace here at Euston Square:
They represent the voice of a young generation keen to develop global health and international exchange both within and beyond Europe. They are a great source of inspiration and motivation to the international Committee and have an unrelenting persistence which will drive us forward. They have the vision for what lies ahead.
They have highlighted that the RCGP curriculum for vocational training (front cover on the right) does not contain even one learning objective related to global health. In collaboration with the other Royal colleges, some of whom have fared a little better but none well, they argue that this has to change. The RCGP curriculum must become more globally orientated.
Similar work has taken place inspired by students at medical schools and both groups have published their findings in the Lancet
And the journal of the Royal Society of Medicine.
However although I totally support their views and the need for more internationally orientated knowledge base, my firm belief is that this is not the crux of the problem.
26

The undergraduate group published in the Lancet and the postgraduate group in the Royal Society of Medicine arguing for more global knowledge and skills in their curricula.
26

We were privileged to have Richard Horton visit Keele recently to help debate with staff and students how we might increase the emphasis in our curriculum on global and cultural awareness, social accountability and sustainability. His list of key factors was this: “People, human rights, justice and knowledge”. To my delight as it very much mirrors my priorities. Although yes I do agree that knowledge is key, this is a relatively easy “fix” and not the whole issue. I would like to argue, using some of my educational research over the years, for the responsibilities we have for “people” . My firm belief is that we have perhaps an even greater responsibility to patients, the health economy and our young to tackle this if we are to reduce the distance between cultures both within and between generations . Take this piece of research published in 2008 in medical education.
27
Jane Roberts, an increasingly prominent academic GP, and I decided to explore how year 2 medical students were adapting to their own ethnic mix and the patients they were meeting in their early clinical experience encounters. Jane worked in Stockton on Tees where Newcastle Medical School has a campus and I was working in Manchester. Both our student cohorts had a similar ethnic mix but the context of their encounters differed as Stockton on Tees has a high level of white ethnicity and social deprivation whereas Manchester had a high level of ethnic minority patients alongside deprivation in the inner city. Both campuses were using small group teaching and ensuring that the groups were composed a mix of gender and ethnicity. We carried out 7 focus groups across the two campuses asking students as part of the protocoltoe discuss their interpretation of the terms “race”, “ethnicity” , “culture” and “cultural diversity”. These four themes emerged from our qualitiative analysis of the transcripts using grounded theory. Tom Sanders a sociologist then at Manchester and now at Keele, externally validated the scripts and brought a sociological theory perspective to the interpretation. We found that for students, discussion of race beyond the confines of medical discourse was problematic. An interesting process of dealing with 4 referees all who took a different perspective on our work followed. There was clear discomfort with our title for the first of the 4 themes “white fear” but we stuck to our guns as this was clear from the transcripts . white students were uncomfortable with discussing race, ethnicity and culture, because they felt they lacked knowledge and this “ignorance” might be perceived as racist; A discomfort I feel may well pervade the postgraduate world of training and clinical practice in
28
health care teams themselves. Ethnic minority students felt at a distance, peripheral and marginalised within the student body . This linked well with Lave and Wenger’s theories of Communities of Practice and Legitimate Peripheral Participation which argues that to gain professional acceptance students need to mve for a peripheral to a central position to achieve full acceptance . They did not carry the protection afforded by being part of a long established and white dominated organisation. This is where professional boundaries became challenging and difficult : social practices , such as alcohol creating significant barriers Students were comfortable talking about disease and different racial demographic prevalence:
We were fond of this quote :
“African sleeping sickness in microbiology that’s kind of cultural awareness isn’t it?
Rare and dodgy diseases like that.”
but not to talk freely about their different backgrounds and cultural beliefs. We concluded that if students are to develop professional holistic values towards patient care, they need more support in understanding their own personal values and uncertainties. Which brings me to another piece of research in this area:
28

Suzanne Vaughan , a sociologist has being doing a phD supervised by Tom Sanders and myself and Prof Nick Crossley at Manchester who has expertise in analysing social networks . Suzanne has worked with year 4 clinical medical students who have weekly PBL sessions : she worked across the 4 NHS trusts where they are placed and asked students within their PBL group for information on who they connected with within the PBL group , individually for study and revision (an ego network as outlined here) and socially . The focus of her work is on ethnicity and achievement and this is just part of a larger study. This is an ego network of Luhman (factious name) a male Asian students struggling somewhat with clinical medicine: linking o the previous slide having difficulties with legitimatising participation. You can see that his ego network is all Asian, predominantly male. The red circle is his mother. We are learning a lot : of particular note is achievement seems to be better if the study networks include a more senior role model who can help reduce the distance but where they are and where they need to be . However there is a clear overall pattern we believe to be of concern:
29
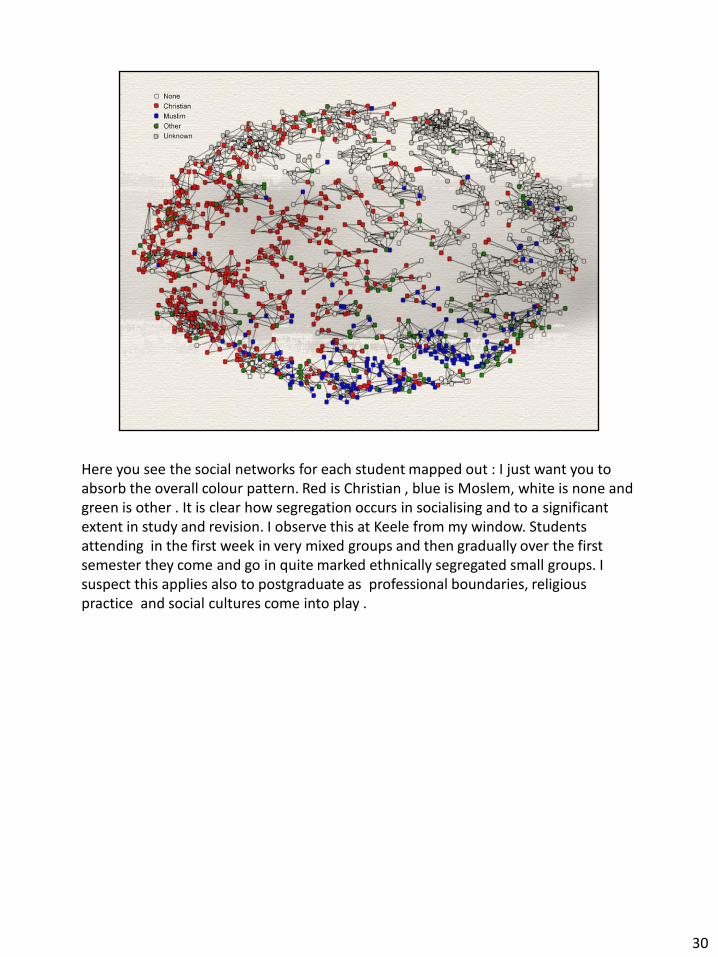
Here you see the social networks for each student mapped out : I just want you to absorb the overall colour pattern. Red is Christian , blue is Moslem, white is none and green is other . It is clear how segregation occurs in socialising and to a significant extent in study and revision. I observe this at Keele from my window. Students attending in the first week in very mixed groups and then gradually over the first semester they come and go in quite marked ethnically segregated small groups. I suspect this applies also to postgraduate as professional boundaries, religious practice and social cultures come into play .
30
Does this matter in terms of the global awareness and preparing students and trainees for “another time” . I would argue yes and that the words of Trevor Philips, Former chair of the Equality and Human Rights Commission, may seem controversial but we need to take heed as evidence suggest they apply to higher education as much as they do to primary and secondary schools. I am not suggesting that social engineering is feasible but that there is a great a need to address cultural and global awareness locally as there is to do so globally .
31
So in terms of preparing the young for global awareness , I believe this is a crucial message : “Global awareness needs to be locally responsive and globally connected”. We need to understand what is happening on our own doorstep and nurture the cultural complexity of our population. The Lancet commission came to a similar conclusion: i.e. we need “Patient and population-centred health systems as members of locally responsive and globally connected teams . Arthur Kleinmann is one of my heroes in this field so I add this quote : “ If you can’t see that your own culture has its own set of interests, emotions and biases, how can you expect to deal successfully with someone else’s culture.” I would add, having worked now within England in the South , North and Midlands , in inner deprived cities and an affluent commuter belt the are huge contrasts within our own society . This was certain apparent in the focus groups Jane and I did. So yes the RCGP curriculum does need to embrace knowledge of global health systems and global is also local.
32
And where else but best to explore and address this than generalist practice : back to the Reeves et al definition : that in an arena which integrates biographical and biotechnical knowledge . But I want to move now to the distance between the doctor and patient .
33
Slide 34
Le petit prince meets this business man : a model of rigidity as he does not even lift his head to greet the Prince. He is too busy counting stars.
I use this as contrast to argue that we need a much more flexible approach to the doctor : patient interaction.
The probably unintended consequence of patient centredness has been the development of fixed frameworks for consultation models which have, on the whole, taken the focus from the doctor side of the interaction. Yet it is a two way interaction.
If we force fixed models on students it can be damaging.
Indeed I am haunted by a quote from Sarah Yardley’s fascinating PhD on “understanding authentic early patient contact in undergraduate medical education”. A student said, after her first interview with a patient
“I was aware that I was not a professional and had to leave my own personality behind “.
This is far from our intention when preparing them for clinical practice.
34
Slide 35
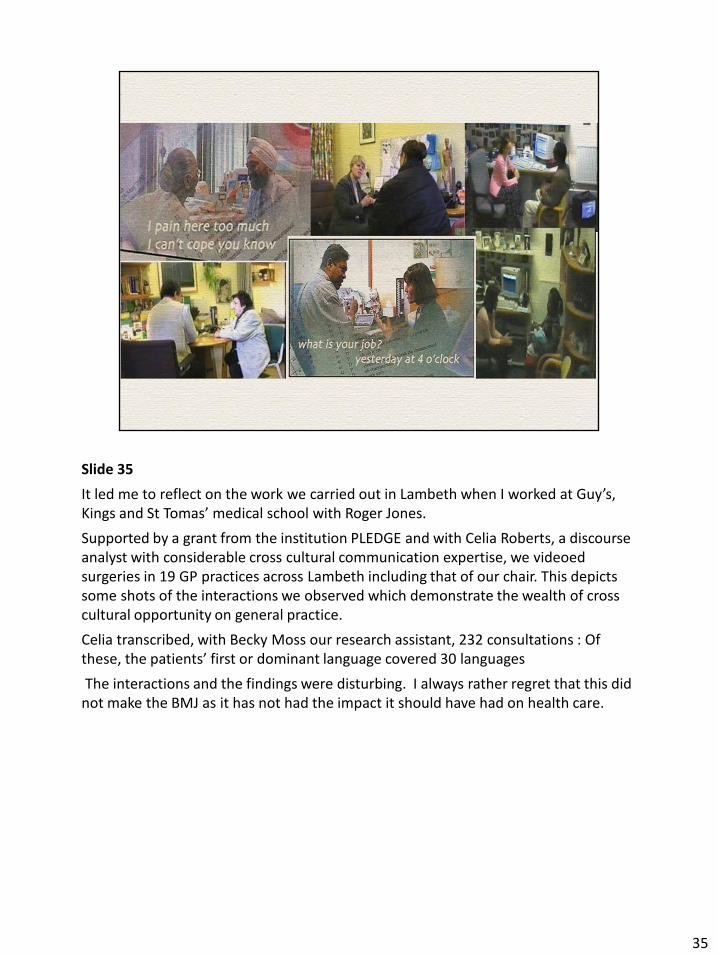
It led me to reflect on the work we carried out in Lambeth when I worked at Guy’s, Kings and St Tomas’ medical school with Roger Jones.
Supported by a grant from the institution PLEDGE and with Celia Roberts, a discourse analyst with considerable cross cultural communication expertise, we videoed surgeries in 19 GP practices across Lambeth including that of our chair. This depicts some shots of the interactions we observed which demonstrate the wealth of cross cultural opportunity on general practice.
Celia transcribed, with Becky Moss our research assistant, 232 consultations : Of these, the patients’ first or dominant language covered 30 languages
The interactions and the findings were disturbing. I always rather regret that this did not make the BMJ as it has not had the impact it should have had on health care.
35
Slide 36
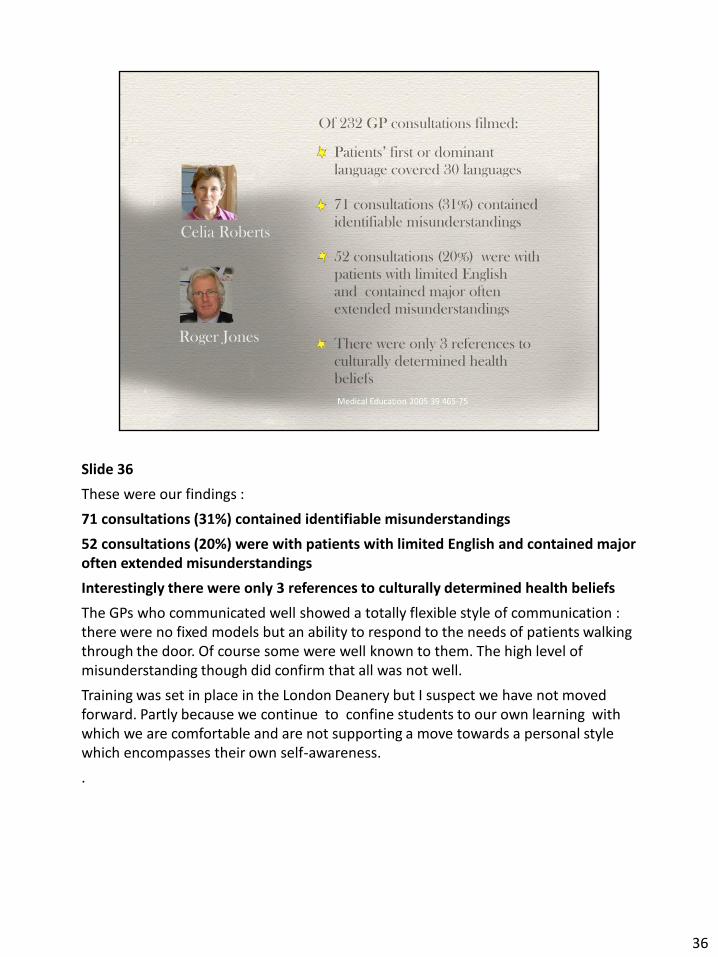
These were our findings :
71 consultations (31%) contained identifiable misunderstandings
52 consultations (20%) were with patients with limited English and contained major often extended misunderstandings
Interestingly there were only 3 references to culturally determined health beliefs
The GPs who communicated well showed a totally flexible style of communication : there were no fixed models but an ability to respond to the needs of patients walking through the door. Of course some were well known to them. The high level of misunderstanding though did confirm that all was not well.
Training was set in place in the London Deanery but I suspect we have not moved forward. Partly because we continue to confine students to our own learning with which we are comfortable and are not supporting a move towards a personal style which encompasses their own self-awareness.
.
36

Slide 37
Ian McWhinney, stated this very clearly back in 1996 :
“We can only attend to a patient’s feelings and emotions if we know our own but self-knowledge is neglected in medical education.
As educators I fear we have ignored these wise words.
37

It is good to see Janet Lefroy who so successfully leads our communication skills programme at Keele working to develop this flexibility by increasing challenge to students across the year . I am grateful to her for use of this quote :
It illustrates the frustrations students can feel as we confine them to our own time
38
So take home message 2 is the need decrease the distance bwteen the doctor and patient in the interaction and the oly way to do this is as pointed out by Albert Schweitzer :
39
Slide 40
And back again to generalist practice. I like the use of “person centred interaction” as carefully phrased here
The “person” can be interpreted as both doctor and patient centred which leads me to my final point about helping students understand their own personal identity and develop the resilience needed for the exponential change I believe they will face.
40

Slide 41
Here I use Le Petit Prince’s struggle to conquer the baobab tree : an enemy to his attempts to preserve his planet as a foreground to illustrate the resilience students need.
Qualitative research is making us increasingly aware of challenges and difficulties students face in the workplace culture of the hidden curriculum: that is the unintended, and sometimes undesirable learning, which takes place in the NHS environment.
Students tend to divorce their learning in the medical school from that required in actual practice. Indeed having learnt certain ethical values these can then be challenges again by clinicians “confined to their time” perhaps. A commonly found example is the practice of learning how to do intimate examinations when a patient is under anaesthetic. We teach the absolute necessity of asking the patient’s permission before the operation. In the operating theatre they experience being told that they must examine a patient
By a powerful surgeon knowing they had to anticipated this and agreed consent. Very hard to stand up for themselves and a source of distress.
The Francis report now highlights even more for us that students must develop the strength and resilience to challenge in the unsatisfactory health care within the NHS culture. They need the assertive, negotiation skills and courage to do this.
41

But faced with the future, resilience has to be more than this. I am fond of this quote.
Slide 41
Here I use Le Petit Prince’s struggle to conquer the baobab tree : an enemy to his attempts to preserve his planet as a foreground to illustrate the resilience students need.
Qualitative research is making us increasingly aware of challenges and difficulties students face in the workplace culture of the hidden curriculum: that is the unintended, and sometimes undesirable learning, which takes place in the NHS environment.
Students tend to divorce their learning in the medical school from that required in actual practice. Indeed having learnt certain ethical values these can then be challenges again by clinicians “confined to their time” perhaps. A commonly found example is the practice of learning how to do intimate examinations when a patient is under anaesthetic. We teach the absolute necessity of asking the patient’s permission before the operation. In the operating theatre they experience being told that they must examine a patient
By a powerful surgeon knowing they had to anticipated this and agreed consent. Very hard to stand up for themselves and a source of distress.
The Francis report now highlights even more for us that students must develop the strength and resilience to challenge in the unsatisfactory health care within the NHS culture. They need the assertive, negotiation skills and courage to do this.
But faced with the future, resilience has to be more than this. I am fond of this quote.
41

Slide 42
“Those who learnt to operate in a vastly changing global environment,
Those who can walk on quick sand and dance with electrons:
Those who amass an array of valid experiences;
Those who see connections where others see chaos will flourish and find opportunity in every experience.
I am very taken with this but have to confess, we need a better understanding of both the attitudinal behaviours that we should be using for selection and how to help students identify these skills within their own identity.
A recent story made me think perhaps it is an undefinable ability to respond innovatively
Insert joke
42
I am not saying that developing this resilience is the answer I believe Einstein is correct
Understanding one’s own values and attitudes is a sense a liberation which would give students the courage to share their cultural beliefs more and overcome the barriers Jane Roberts and myself identified
43
So back to generalist practice again ; If we can overcome these distances the I believe we can support health as a resource for living and not as an end in itself.
44
Slide 45
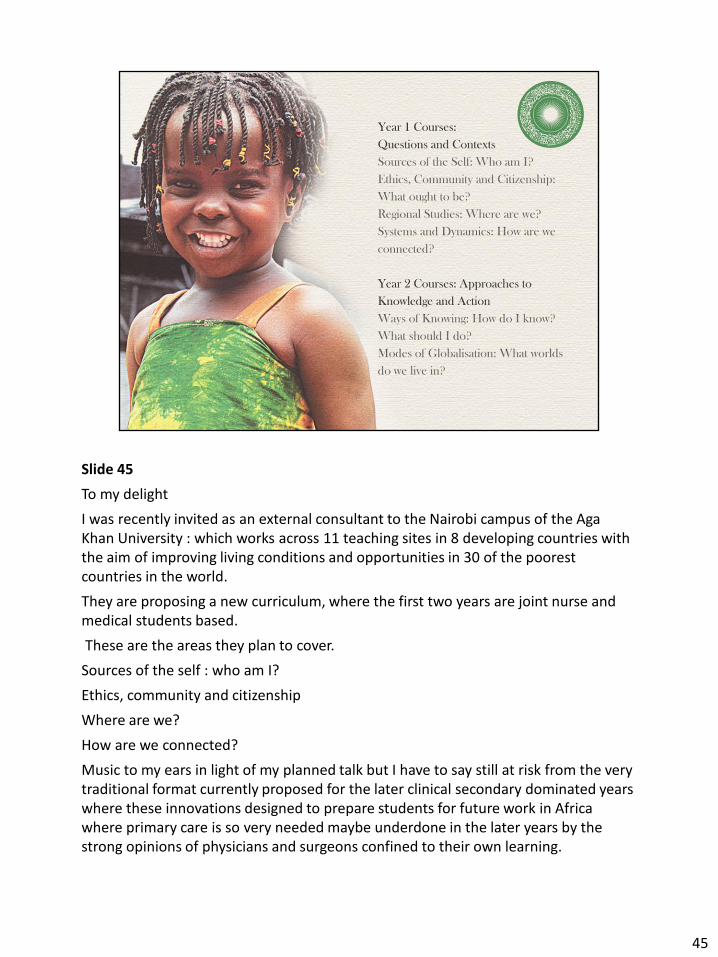
To my delight
I was recently invited as an external consultant to the Nairobi campus of the Aga Khan University : which works across 11 teaching sites in 8 developing countries with the aim of improving living conditions and opportunities in 30 of the poorest countries in the world.
They are proposing a new curriculum, where the first two years are joint nurse and medical students based.
These are the areas they plan to cover.
Sources of the self : who am I?
Ethics, community and citizenship
Where are we?
How are we connected?
Music to my ears in light of my planned talk but I have to say still at risk from the very traditional format currently proposed for the later clinical secondary dominated years where these innovations designed to prepare students for future work in Africa where primary care is so very needed maybe underdone in the later years by the strong opinions of physicians and surgeons confined to their own learning.
45
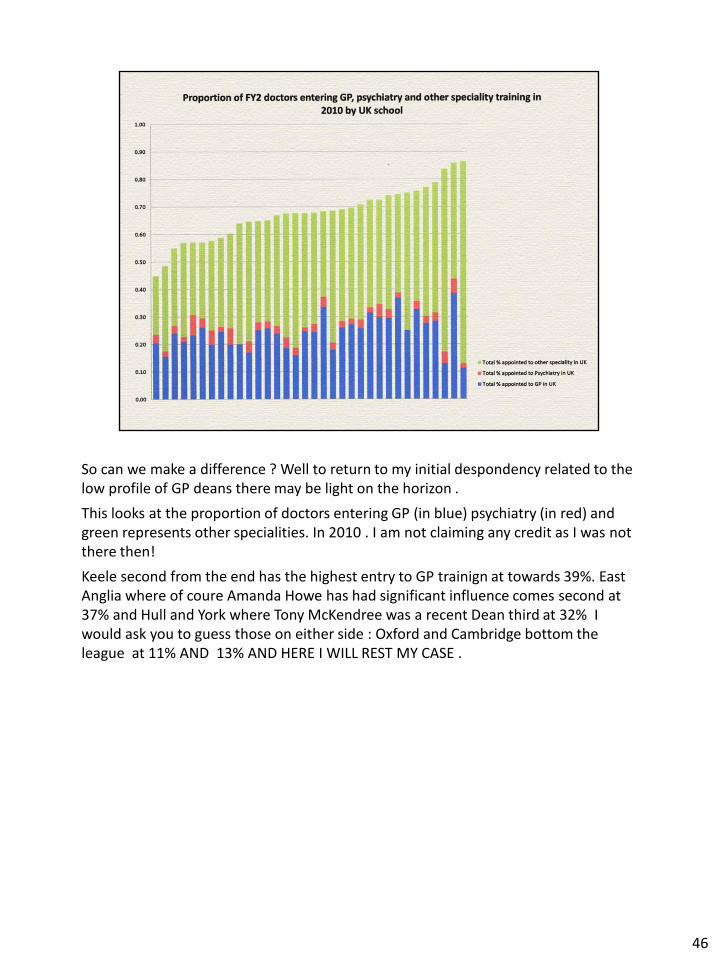
So can we make a difference ? Well to return to my initial despondency related to the low profile of GP deans there may be light on the horizon .
This looks at the proportion of doctors entering GP (in blue) psychiatry (in red) and green represents other specialities. In 2010 . I am not claiming any credit as I was not there then!
Keele second from the end has the highest entry to GP trainign at towards 39%. East Anglia where of coure Amanda Howe has had significant influence comes second at 37% and Hull and York where Tony McKendree was a recent Dean third at 32% I would ask you to guess those on either side : Oxford and Cambridge bottom the league at 11% AND 13% AND HERE I WILL REST MY CASE .
46

Slide 47
We need more GPs spending longer with patients and communities, with longer life-long training to ensure that patients receive the best possible care, in a timely and appropriate manner and in an environment that improves the quality of their lives.
Can we also ponder on looking beyond out time to that of the future : this requires I believe
We need more GPs spending longer with trainees offering longer life-long training to ensure that students receive the best possible understanding of their own interests, emotions and biases, in an environment that fosters the diversity of personal interaction and the complexity of future health care.
47

What I have illustrated is that much of working to the future requires the “heart” and connection with our inner feelings
This is the key message of Le Petit Prince : inscribed in here in French on a plaque in Memory of Antoine de Exupery
48
Yet the word “heart” is absoultely key toe the healtha genda of the future
49
Slide 50
I’ll end with the words of Antoine de Exupery : This seems even more apt as it has been pointed out to me that the last major international conference on medical educaiton (UG and PG) was held in Lyons where Antoine de Exupery was born and indeed has the airport named after him. I am grateful to Simon Gay for making the link and his photos
Antoine de Saint-Exupery
A civilization is a heritage of beliefs, customs, and knowledge slowly accumulated in the course of centuries, elements difficult at times to justify by logic, but justifying themselves as paths when they lead somewhere, since they open up for man his inner distance.
For me the key words here are inner distance which I have explored here as we look to the future at three levels.
The inevitable distance between ourselves and those we educate and the rather bizarre assumption often made that what was good for us is equally good for them as we confine them to our own learning. I hope I have illustrated the pitfalls of doing this, the impact it has and the importance of change to work as a college with universities to take generalism in the primary care context forward as an expanding media for undergraduate learning.
50

Secondly the inner distance between the doctor and patient and the need for educators to address this and move away from the mantra of patient centredness and acknowledge that there is a “doctor centredness” which must also be explored and which I believe patients also look to and value
And finally, as Einstein says, attaining the understanding and liberation from self to develop the flexibility and resilience needed to prepare for the challenges ahead. This is essential and needs to occur at an early stage in training.
The educational context of primary care where we are immersed, as Joanna and her colleagues framed, in generalist practice and offer the 1:1 supervision in a relatively safe ambience is where this can be achieved.
50

Slide 51
This wonderful new college gives the perfect context to establish much stronger relations with undergraduate students, medical schools and SAPC and drop the word postgraduate which seems to precede all our education initiatives.
Let’s move from confining students to our “own time” where medical education was secondary care dominated. Only then I believe will primary care gain global recognition.
We understand those values of the heart, invisible to the eye but so key to our shared belief that
“health is a human right which has equity at its heart”.
51

52