keele clinical trials unit - keele.ac.uk · sop 21: non-compliance: ... service or other...
TRANSCRIPT

SOP 21: Non-Compliance: © Keele University Deviations and Serious Breaches of GCP and/or the Trial Protocol
Ref: KCTU/SOP21/v4.0/27-Oct-2017 Page 1 of 13
Keele Clinical Trials Unit
Standard Operating Procedure (SOP) Summary Box
Title Non-Compliance: Deviations and Serious Breaches of GCP and/or the Trial Protocol
SOP Index Number SOP 21
Version 4.0
Approval Date 13-Oct-2017
Effective Date 27-Oct-2017
Review Date October 2019
Lead Author Steve Alcock
Reference KCTU/SOP21/v4.0/27-Oct-2017
DISCLAIMER
This SOP is the property of Keele Clinical Trials Unit (Keele CTU), Faculty of Health, Keele University and the content cannot be reproduced without specific permission from
the owner.
All SOPs and associated documents must be accessed through the dedicated SOP area of the Research Institute for Primary Care and Health Sciences (iPCHS) Intranet to
ensure the correct version is being used. If this document is being accessed through any other method, such as electronic copies saved onto a network drive or in printed form, it is only valid for use if the version number and effective date shown above is the same as
that shown on the iPCHS Intranet.
Any superseded versions of this document need to be promptly withdrawn from use.
All individuals undertaking functions outlined in this document are responsible for ensuring that they are trained in the procedures outlined in the correct version of this
document. SOP Template v6.0 date 18 Aug 2016
Signature Box
Print Name Signature Date
Research Integrity Manager
Emma Skinner Signed hard copy stored in
approved SOP file with Research Integrity office
13-Oct-2017
Senior Trial Manager
Susie Hennings Signed hard copy stored in
approved SOP file with Research Integrity office
13-Oct-2017

SOP 21: Non-Compliance: © Keele University Deviations and Serious Breaches of GCP and/or the Trial Protocol
Ref: KCTU/SOP21/v4.0/27-Oct-2017 Page 2 of 13
Version History Log
Version Date Approved
Reason(s) for Change Implementation Plan
1.0 22-Oct-2015 Approval of version 1.0 All Research Institute staff will be notified of the SOP release. Staff are expected to read the SOP, as applicable to their role. Study Coordinators are to cover the procedures at the next operations and management group meetings for the trials.
2.0 11-Jul-2016 Update to trial deviation form, and addition of conditions of sponsorship withdrawal
All Research Institute staff will be notified of the SOP release. Staff are expected to read the SOP, as applicable to their role. Trial Managers are to cover the procedures at the next operations and management group meetings for the trials.
3.0 31-Jan-2017 Update following serious breach notification to clarify process.
All Keele Health and Social Care Research QMS users will be notified of the new SOP. Staff are expected to read the new version of the SOP when it is released, as applicable to their role. The updated procedures are to be implemented from the SOP effective date
4.0 13-Oct-2017 Update following changes made to the forms for reporting and investigation, and the management of the process.
All Keele Health and Social Care Research QMS users will be notified of the new SOP. Staff are expected to read the new version of the SOP when it is released, as applicable to their role. The updated procedures are to be implemented from the SOP effective date Training sessions to be led by Lead Author focusing on the completion of the new form.
SOP 21: Non-Compliance: © Keele University Deviations and Serious Breaches of GCP and/or the Trial Protocol
Ref: KCTU/SOP21/v4.0/27-Oct-2017 Page 3 of 13
Table of Contents 1. Purpose ........................................................................................................................ 4
2. Scope and Applicability ................................................................................................. 4
3. Background .................................................................................................................. 4
4. Procedures ................................................................................................................... 6
4.1 All Studies ............................................................................................................... 6
4.1.1 Summary Flow Diagram ................................................................................... 6
4.1.2 Identification of potential non-compliance ........................................................ 7
4.1.3 [FOR25.1 - Initial Report] ................................................................................. 8
4.1.4 [FOR25.2 - Research Integrity Office Assessment] .......................................... 9
4.1.5 Additional Information ...................................................................................... 9
[FOR25.3 - Local PI Assessment] .................................................................... 9
[FOR25.4 - Further Assessment] ................................................................... 10
[FOR25.5 - Independent Review] ................................................................... 10
[FOR25.6 - Serious Breach Submission]........................................................ 10
[FOR25.7 - Urgent Safety Measures] ............................................................. 10
[FOR26 - Corrective and Preventative Action (CAPA) Plan] .......................... 10
4.1.6 [FOR25.8 - Deviation closure] ........................................................................ 10
4.1.7 Reporting deviations ...................................................................................... 11
4.2 Serious Breaches ................................................................................................. 11
4.3 Non-compliance Data ........................................................................................... 12
5. Key Personnel to whom this SOP Applies .................................................................. 12

SOP 21: Non-Compliance: © Keele University Deviations and Serious Breaches of GCP and/or the Trial Protocol
Ref: KCTU/SOP21/v4.0/27-Oct-2017 Page 4 of 13
1. Purpose This Standard Operating Procedure (SOP) describes the process for management and escalation of non-compliance and serious breaches of Good Clinical Practice (GCP) and/or the approved trial/study protocol. 2. Scope and Applicability This SOP applies to all individuals undertaking functions outlined herein. This includes all core Keele CTU staff and all other academic, research, management or admin staff, or students working on Keele University sponsored/Keele CTU managed clinical research projects through site agreements, service or other contractual arrangements.
This SOP must be followed in line with the NHS Research Governance Framework, and the
University, Research Institute and CTU policies.
Where applicable to Clinical Trials of Investigational Medicinal Products (CTIMPs) this SOP
must be followed in line with the UK Medicines for Human Use (Clinical Trials) Regulations
2004 and subsequent amendments, and the EU Clinical Trials Directive. This SOP must
also be followed in line with any current MHRA requirements as detailed on their website.
Where applicable to non-CTIMP studies this SOP must be followed in line with the principles
of Good Clinical Practice. Whilst elements of this SOP relate only to CTIMPs, e.g. reporting
Serious Breaches to the MHRA, the principles of identifying and managing non-compliance
apply to non-CTIMP studies.
For Keele University Sponsored research studies, operational responsibility for
identification, classification and reporting of non-compliance is delegated to the Chief
Investigator (CI) with the support of the Sponsor.
3. Background Deviations from study protocols and Good Clinical Practice (GCP) occur commonly in health
and social care research. The majority of these instances are technical non-compliances
that do not result in harm to participants, do not compromise data integrity, or significantly
affect the scientific value of the reported results of the study. These technical deviations
must be still be documented, and appropriate corrective and preventative actions must be
taken.
It is the responsibility of the sponsor to assess the impact of any serious breaches on the
scientific value of the study. The sponsor can terminate or suspend a study if there are
concerns around patient safety or study conduct (see HSCRC-POL-01 Policy for Health
and Social Care Research for further information).

SOP 21: Non-Compliance: © Keele University Deviations and Serious Breaches of GCP and/or the Trial Protocol
Ref: KCTU/SOP21/v4.0/27-Oct-2017 Page 5 of 13
Where Keele University is not the Sponsor but the function of reporting serious
breaches to the main REC and MHRA is delegated by the Sponsor to Keele University,
the arrangement does not affect the legal responsibility of the Sponsor. All reports
and correspondence relating to the issue must be collated and supplied to the
Sponsor.

SOP 21: Non-Compliance: © Keele University Deviations and Serious Breaches of GCP and/or the Trial Protocol
Ref: KCTU/SOP21/v4.0/27-Oct-2017 Page 6 of 13
4. Procedures 4.1 All Studies 4.1.1 Summary Flow Diagram
Identification of potential non-compliance (section 4.1.2)
Sponsor notified of non-compliance event via [FOR25.1 – Initial Report] submitted to
Research Integrity Office(section 4.1.4)
Sponsor records event on Edge workflow, assigns unique deviation code and completes
[FOR25.2 – Research Integrity Office Assessment] (section 4.1.4)
Local PI review [FOR25.3 – Local PI Assessment] (if required)
(section 4.1.5)
[FOR26 – Corrective and Preventative Action Plan] (if required) (section 4.1.5)
Further assessment carried out by CI or other relevant individual [FOR25.4 – Further
Assessment] (if required) (section 4.1.5)
Final sponsor review of non-compliance [FOR25.2 – Research Integrity Office
Assessment] (section 4.1.5)
Independent review of deviation if sponsor review does not agree with CI assessment
[FOR25.5 – Independent Review] (section 4.1.5)
Deviation closure and reporting [FOR25.8 - Closure]
(section 4.1.6)
Serious breach identified at any stage (section 4.2)
Serious Breach Notification Form completed by Sponsor and CI
(section 4.2)
Research Integrity Manager submits Serious Breach Notification Form to MHRA (CTIMPS) and NHS REC (section 4.2) and completes
[FOR25.6 – Serious Breach Submission]
CI completes [FOR25.1 – Initial Report] and e-mails to Research Integrity Office
(section 4.1.3)
7 c
ale
nd
ar
da
y d
ead
line

SOP 21: Non-Compliance: © Keele University Deviations and Serious Breaches of GCP and/or the Trial Protocol
Ref: KCTU/SOP21/v4.0/27-Oct-2017 Page 7 of 13
4.1.2 Identification of potential non-compliance
Potential non-compliance identified
For all research, non-compliance may be identified
through any study activity, but in particular through:
Central monitoring procedures such as consent form
review or data management (SOP 14: Monitoring)
Site visits
Self-reporting by a study site or participant
Potential non-compliance reported to the Chief Investigator
A potential non-compliance event affecting a study must
be reported to the Chief Investigator (CI) as soon as any
member of the study team becomes aware of an event.
This must be followed up in writing (e.g. via email or a
logged telephone call). The CI or delegated individual
must then follow up the event and is classed as the
‘investigator’ for the purposes of this SOP.
Confirm non-compliance
The investigator must collect information to assess
whether the event is a true non-compliance event or
could be a misunderstanding or otherwise not a non-
compliance event. For example, a protocol written
broadly to cover variation in activity at site may cause
activity to be misinterpreted as non-compliance by a
local study team.
Investigator completes Section A of [FOR25.1
– Initial Report]
If the CI wishes to initiate an urgent safety measure, (see SOP 20: Safety Reporting and Pharmacovigilance) to protect participants from any immediate hazard to their health and safety, this must be indicated in Section A of [FOR25.1 – Initial Report].

SOP 21: Non-Compliance: © Keele University Deviations and Serious Breaches of GCP and/or the Trial Protocol
Ref: KCTU/SOP21/v4.0/27-Oct-2017 Page 8 of 13
4.1.3 [FOR25.1 - Initial Report]
CI or delegate completes Section B of
[FOR25.1 – Initial Report] within 24
hours of being notified of event.
This section is used by the CI to assess the severity of
the non-compliance event, in accordance with the study
protocol.
Investigator completes Section C of [FOR25.1 – Initial Report] (if known at this time)
Completion of section C should NOT delay submission of
[FOR25.1 – Initial Report] to the Research Integrity
Office and should therefore only be completed at this
time if the information necessary to classify the deviation
and / or root cause is already available when Section B
is completed.
CI completes and signs Section D of [FOR25.1 – Initial Report], for
CTU managed studies a Senior Trials
Manager must also sign, and they (or the Investigator) send to
the Research Integrity Office.
Submit to the Research Integrity Office via e-mail to
[email protected] with a subject
heading of “[RG/sponsor code: study acronym/short
title] – Non-compliance notification”.
The judgement on whether an instance of non-compliance is likely to have a significant
impact on the scientific value of the study depends on a variety of factors e.g. the design of
the study, the type and extent of the data affected by the breach, the overall contribution of
the data to key analysis parameters, the impact of excluding the data from the analysis etc.
For examples of what is classed as a serious breach see guidance for the notification of
serious breaches of GCP or the study protocol on the MHRA website.
SOP 21: Non-Compliance: © Keele University Deviations and Serious Breaches of GCP and/or the Trial Protocol
Ref: KCTU/SOP21/v4.0/27-Oct-2017 Page 9 of 13
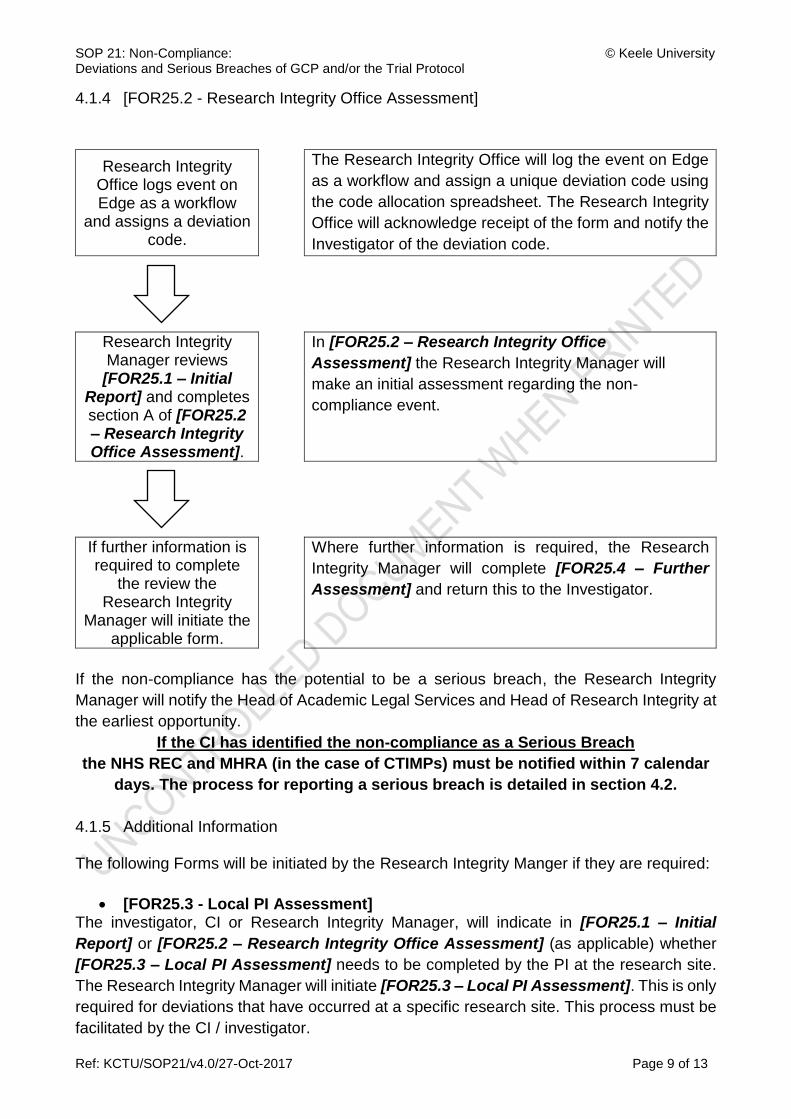
4.1.4 [FOR25.2 - Research Integrity Office Assessment]
Research Integrity Office logs event on Edge as a workflow
and assigns a deviation code.
The Research Integrity Office will log the event on Edge
as a workflow and assign a unique deviation code using
the code allocation spreadsheet. The Research Integrity
Office will acknowledge receipt of the form and notify the
Investigator of the deviation code.
Research Integrity Manager reviews [FOR25.1 – Initial
Report] and completes section A of [FOR25.2 – Research Integrity Office Assessment].
In [FOR25.2 – Research Integrity Office
Assessment] the Research Integrity Manager will
make an initial assessment regarding the non-
compliance event.
If further information is required to complete
the review the Research Integrity
Manager will initiate the applicable form.
Where further information is required, the Research
Integrity Manager will complete [FOR25.4 – Further
Assessment] and return this to the Investigator.
If the non-compliance has the potential to be a serious breach, the Research Integrity
Manager will notify the Head of Academic Legal Services and Head of Research Integrity at
the earliest opportunity.
If the CI has identified the non-compliance as a Serious Breach
the NHS REC and MHRA (in the case of CTIMPs) must be notified within 7 calendar
days. The process for reporting a serious breach is detailed in section 4.2.
4.1.5 Additional Information The following Forms will be initiated by the Research Integrity Manger if they are required:
[FOR25.3 - Local PI Assessment] The investigator, CI or Research Integrity Manager, will indicate in [FOR25.1 – Initial
Report] or [FOR25.2 – Research Integrity Office Assessment] (as applicable) whether
[FOR25.3 – Local PI Assessment] needs to be completed by the PI at the research site.
The Research Integrity Manager will initiate [FOR25.3 – Local PI Assessment]. This is only
required for deviations that have occurred at a specific research site. This process must be
facilitated by the CI / investigator.

SOP 21: Non-Compliance: © Keele University Deviations and Serious Breaches of GCP and/or the Trial Protocol
Ref: KCTU/SOP21/v4.0/27-Oct-2017 Page 10 of 13
[FOR25.4 - Further Assessment] If there is a need for further assessment this will be indicated by the CI on [FOR25.1 – Initial
Report] or the Research Integrity Manager on [FOR25.2 – Research Integrity Office
Assessment]. [FOR25.4 – Further Assessment] will be initiated by the Research Integrity
Manager and must be completed by the CI or their delegate.
[FOR25.5 - Independent Review] Where additional expertise is required to assess the severity of an event, the Research
Integrity Manager will initiate [FOR25.5 – Independent Review]. For CTIMPs; if the
Research Integrity Manager’s review of seriousness is different from the CI’s decision, an
independent reviewer must be asked to complete [FOR25.5 – Independent Review]. If the
outcome of the independent review is that a serious breach has occurred and this had not
been previously reported the processes in Section 4.2 of this SOP must be followed.
[FOR25.6 - Serious Breach Submission] (See section 4.2)
[FOR25.7 - Urgent Safety Measures] Where an USM is required in relation to the deviation, [FOR25.7 – Urgent safety Measures]
is completed by the Research Integrity Manager. USMs are managed in accordance with
SOP 20: Safety Reporting and Pharmacovigilance.
[FOR26 - Corrective and Preventative Action (CAPA) Plan] It may be sufficient for all CAPA to be detailed in [FOR25.1 – Initial Report] Section A.
Where a full CAPA is required, the Research Integrity Manager will initiate [FOR26 –
Corrective and Preventative Action Plan]. This must be completed by the investigator
through liaison with the CI and study team. The CAPA must describe what actions are
required to correct the deviation and how to prevent it happening again in the future. If the
separate [FOR26 - Corrective and Preventative Action Plan] has been used, the CAPA
code must be referenced in the respective box in [FOR25.2 – Research Integrity Office
Assessment]. The Research Integrity Manager will review the proposed CAPA and
associated timeframes to ensure that actions are completed in a reasonable period. The
Research Integrity Manager may escalate breaches of timeframes or other issues to the
Head of Research Integrity.
4.1.6 [FOR25.8 - Deviation closure] The Research Integrity Manager will review the information provided in all completed forms.
If unsure about any aspect of the information, the Research Integrity Manager may contact
the CI, Investigator, Lead Statistician or appropriate Trial Manager for further clarification
using [FOR25.4 – Further Assessment]. The Research Integrity Manager will complete
Section B of [FOR25.2 – Research Integrity Office Assessment]
Once the deviation has been resolved [FOR25.8 - Closure] must be completed by the
Research Integrity Manager. For CTIMPs, any serious breaches must be considered as
ongoing until confirmed closed by the MHRA Inspector. The original completed GCP and
Protocol Deviation Forms must be filed in the Study Master File and copies with the
Research Integrity Office.

SOP 21: Non-Compliance: © Keele University Deviations and Serious Breaches of GCP and/or the Trial Protocol
Ref: KCTU/SOP21/v4.0/27-Oct-2017 Page 11 of 13
4.1.7 Reporting deviations The Research Integrity Manager will notify the Head of Academic Legal Services and Head
of Research Integrity of potential and confirmed serious breaches.
All deviations must be reported to the Trial Management Group (TMG), Trial Steering
Committee (TSC) and Data safety Monitoring Committee (DMC). TSC and DMC reports
must include data regarding deviations in accordance with SOP 33: Trial Steering
Committees and Data Monitoring Committees.
In addition, deviations should be included and considered when producing the final
CONSORT diagram, which describes how such deviations have been handled during
analysis, and their impact on patient safety and the conduct of the analysis reported in the
applicable Study Report (SOP 16: Analysis).
4.2 Serious Breaches
A “serious breach” is defined as a breach of the protocol or of the conditions or principles of
Good Clinical Practice (or equivalent standards for conduct of non-CTIMPs) which is likely
to affect to a significant degree the safety or physical or mental integrity of the trial subjects,
or the scientific value of the research.
For CTIMPs, Where it is confirmed that a Serious Breach of the trial protocol or GCP has
occurred, or there is uncertainty, the CI must complete the MHRA’s Notification of Serious
Breaches of GCP or the Trial Protocol Form, the current version of which is available on the
MHRA’s Website and send it to the Research Integrity Office (via
The MHRA and NHS REC must be notified of a confirmed serious breach within 7
calendar days of becoming aware of the breach.
The Research Integrity Manager will notify the MHRA GCP Inspectorate of the serious
breach via the email provided on the MHRA website using the notification form which the CI
has completed. If there are any queries the Research Integrity Manager, as sponsor
representative, will telephone the MHRA Inspectorate to discuss the serious breach. The CI
must also notify the Research Ethics Committee of the serious breach via e-mail.
The Research Integrity Office will continue to be the contact for the allocated MHRA
Inspector. [FOR25.6 – Serious Breach Submission] will be used by the Research Integrity
Manager to record serious breach submission information. The Research Integrity Manager
will notify the Head of Academic Legal Services and Head of Research Integrity.
Consideration will be made regarding notifying the University’s insurance broker.
For serious breaches in non-CTIMPs the CI must notify the NHS REC. Time lines for reporting of serious breaches in non-CTIMPs are the same as those for CTIMPs.

SOP 21: Non-Compliance: © Keele University Deviations and Serious Breaches of GCP and/or the Trial Protocol
Ref: KCTU/SOP21/v4.0/27-Oct-2017 Page 12 of 13
The CI must respond with urgency to any actions or queries relating to a serious breach.
4.3 Non-compliance Data
The data collated by the Research Integrity Office regarding non-compliance events for all
health and social care research studies, whether CTIMP or not, will be reviewed for trends
and to identify any critical activity that may require further training or an audit to be
performed.
5. Key Personnel to whom this SOP Applies
Responsibility of
Undertaken by Activity
1 All staff to which SOP applies
Users of SOP
Identification of non-compliance with trial protocol
and /or GCP and highlighting to the Trial
Manager/Study Coordinator and CI
2 Chief Investigator
Chief Investigator (with support of Research Integrity Manager)
Assessment
Assessment of impact of non-compliance on
participant safety and scientific integrity of the trial
Escalation of any non-compliance that is
potentially a serious breach of the trial protocol or
GCP
Completion of MHRA’s Notification of Serious
Breaches of GCP or the Trial Protocol Form as
required
Reporting of confirmed Serious Breaches to the
NHS REC
Oversight of agreed Corrective and Preventative
Action Plans [FOR26 - Corrective and
Preventative Action Plan]

SOP 21: Non-Compliance: © Keele University Deviations and Serious Breaches of GCP and/or the Trial Protocol
Ref: KCTU/SOP21/v4.0/27-Oct-2017 Page 13 of 13
Responsibility of
Undertaken by Activity
Trial Manager/Study Coordinator (with support of, CI and Research Integrity Manager)
Maintenance of record of all non-compliance
occurring within the trial
Investigation into instances of non-compliance
Reporting
Reporting confirmed and potential serious
breaches to the CI and Research Integrity Office
for assessment
Supporting the CI in completion of serious breach
report for submission to MHRA and REC
Development and implementation of Corrective
and Preventative Action plan [FOR26 -
Corrective and Preventative Action Plan] as
agreed with all parties
3 Sponsor Research Integrity Office
Support CIs and trial teams in investigations into
non-compliance
Maintenance of a central University record of all
non-compliance across all trials
Support CIs and trial teams to develop
appropriate corrective and preventative action
plans [FOR26 - Corrective and Preventative
Action Plan] as necessary
Report confirmed serious breaches to MHRA on
behalf of the University within regulatory
timeframes
Point of contact for MHRA for correspondence
relating to serious breach reports
Report all non-compliances assessed as potential
serious breaches to the Head of Academic Legal
Services and the Head of Research Integrity.
Report all non-compliances and CAPA plans (if
appropriate) to the appropriate University
Committee(s)