oulu 2011 d 1137 university of oulu p.o.b. 7500 fi-90014...
TRANSCRIPT

ABCDEFG
UNIVERS ITY OF OULU P.O.B . 7500 F I -90014 UNIVERS ITY OF OULU F INLAND
A C T A U N I V E R S I T A T I S O U L U E N S I S
S E R I E S E D I T O R S
SCIENTIAE RERUM NATURALIUM
HUMANIORA
TECHNICA
MEDICA
SCIENTIAE RERUM SOCIALIUM
SCRIPTA ACADEMICA
OECONOMICA
EDITOR IN CHIEF
PUBLICATIONS EDITOR
Senior Assistant Jorma Arhippainen
Lecturer Santeri Palviainen
Professor Hannu Heusala
Professor Olli Vuolteenaho
Senior Researcher Eila Estola
Director Sinikka Eskelinen
Professor Jari Juga
Professor Olli Vuolteenaho
Publications Editor Kirsti Nurkkala
ISBN 978-951-42-9666-6 (Paperback)ISBN 978-951-42-9667-3 (PDF)ISSN 0355-3221 (Print)ISSN 1796-2234 (Online)
U N I V E R S I TAT I S O U L U E N S I S
MEDICA
ACTAD
D 1137
ACTA
Marjo Tourula
OULU 2011
D 1137
Marjo Tourula
THE CHILDCARE PRACTICE OF CHILDREN’S DAYTIME SLEEPING OUTDOORSIN THE CONTEXT OF NORTHERN FINNISH WINTER
UNIVERSITY OF OULU,FACULTY OF MEDICINE,INSTITUTE OF HEALTH SCIENCES, NURSING SCIENCE,INSTITUTE OF BIOMEDICINE, DEPARTMENT OF PHYSIOLOGY;FINNISH INSTITUTE OF OCCUPATIONAL HEALTH, OULU;NORTHERN OSTROBOTHNIA HOSPITAL DISTRICT;KYUSHU UNIVERSITY, FACULTY OF DESIGN, DEPARTMENT OF HUMAN SCIENCE


A C T A U N I V E R S I T A T I S O U L U E N S I SD M e d i c a 1 1 3 7
MARJO TOURULA
THE CHILDCARE PRACTICE OF CHILDREN’S DAYTIME SLEEPING OUTDOORS IN THE CONTEXT OF NORTHERN FINNISH WINTER
Academic dissertation to be presented with the assent ofthe Faculty of Medicine of the University of Oulu forpublic defence in Auditorium 101 A of the Faculty ofMedicine (Aapistie 5 A), on 2 December 2011, at 12 noon
UNIVERSITY OF OULU, OULU 2011
Copyright © 2011Acta Univ. Oul. D 1137, 2011
Supervised byProferssor Arja IsolaProfessor Hannu RintamäkiProfessor Juhani Hassi
Reviewed byDocent Päivi KankkunenProfessor Randi Eidsmo Reinertsen
ISBN 978-951-42-9666-6 (Paperback)ISBN 978-951-42-9667-3 (PDF)
ISSN 0355-3221 (Printed)ISSN 1796-2234 (Online)
Cover DesignRaimo Ahonen
JUVENES PRINTTAMPERE 2011

Tourula, Marjo, The childcare practice of children’s daytime sleeping outdoors inthe context of Northern Finnish winterUniversity of Oulu, Faculty of Medicine, Institute of Health Sciences, Nursing Science; Instituteof Biomedicine, Department of Physiology, P.O. Box 5000, FI-90014 University of Oulu,Finland; Finnish Institute of Occupational Health, Oulu, Aapistie 1, FI-90220 Oulu, Finland;Northern Ostrobothnia Hospital District, P.O.Box 10, FI-90029 OYS, Finland; KyushuUniversity, Faculty of Design, Department of Human Science, 4-9-1 Shiobaru, Minami-ku,Fukuoka 815-8540, JapanActa Univ. Oul. D 1137, 2011Oulu, Finland
AbstractThe purpose of the study was to create a comprehensive view and add understanding about thechildcare practice of children sleeping outdoors in the context of Northern Finnish winter. Ageneral view of the topic was described, the thermal insulation of clothing of infants sleepingoutdoors in northern winter climate was evaluated and the relationships among thermalenvironment, infants’ skin temperatures and daytime outdoor sleep duration were described.
Mixed methods research design was used. A questionnaire was distributed to the parents(n=116) of children under 2 years of age in the city of Oulu. Skin temperatures of about three-month-old infants were recorded from seven skin sites throughout a daytime sleep outdoors (n=34)and indoors (n=33) in the families’ homes. The duration of the infant’s sleep was observed and airtemperature and velocity of the outdoor environment were recorded. Clothing data of infants werecollected and microclimate temperatures and humidity inside middle wear measured. Theinsulation of clothing ensembles was measured by using a baby-size thermal manikin. Therequired clothing insulation was estimated according to ISO 11079. Mothers (n=21) fromNorthern Finland were interviewed.
A fit can be found between family – cultural outdoor sleeping childcare practice – and NorthernFinnish winter environment, but also factors that decreased the fit existed. Winter environmentwas seen as an affordance for the child to sleep outdoors. Infants usually slept outdoors in thedaytime once a day in different kinds of environments, the best temperature being -5 °C. Outdoorsleeping was a self-evident and common culturally bound custom. Guidelines and encouragementwere given to mothers from different sources, and by sharing their own experiences, mothersparticipated in the cultural knowledge-building processes. The outdoor sleeping practice wascommonly accepted collective behavior. Many risk factors also existed, but when all securityperspectives were first taken into account it promoted family well-being by creating rhythm andstrengthening the fluency of everyday life. The optimal thermal insulation was difficult to adjustsystematically and both cooling and sweating existed. When ambient temperature decreased, thecooling rate of Tsk increased. Children slept longest outdoors when the cooling rate of Tsk wasminimal. The basic idea was that outdoor sleeping promoted children’s health.
A comprehensive view of the phenomenon was gathered into the evaluation model, which canbe utilized in nursing practice. The findings give detailed information that is utilized whenupdating guidelines. This study also creates ground for international comparative studies.
Keywords: child, child care, culture, mixed methods, Northern Finland, skintemperature, sleep, thermal insulation of clothing, winter


Tourula, Marjo, Lasten ulkona nukuttaminen talvella lastenhoitokäytäntönäpohjoissuomalaisessa kontekstissa Oulun yliopisto, Lääketieteellinen tiedekunta, Terveystieteiden laitos, Hoitotiede; Biolääke-tieteen laitos, Fysiologia, PL 5000, 90014 Oulun yliopisto; Työterveyslaitos, Oulu, Aapistie 1,90220 Oulu; Pohjois-Pohjanmaan sairaanhoitopiiri, PL 10, 90029 OYS; Kyushun yliopisto,Suunnittelun tiedekunta, Ihmistieeteet, 4-9-1 Shiobaru, Minami-ku, Fukuoka 815-8540, JapaniActa Univ. Oul. D 1137, 2011Oulu
TiivistelmäTutkimuksen tavoitteena oli muodostaa kokonaiskuva ja lisätä ymmärrystä lasten ulkona nukut-tamiskäytännöstä pohjoissuomalaisessa talvikontekstissa lasten ja perheiden hyvinvoinninlisäämiseksi. Tarkoituksena oli kuvata lasten ulkona nukuttamiskäytäntöä, ympäristön ja ihonlämpötilojen sekä unen pituuden yhteyttä ja arvioida vaatetuksen lämmöneristävyyttä.
Tutkimuksessa käytettiin mixed methods -lähestymistapaa monipuolisen kokonaiskuvantavoittamiseksi. Pilottikysely tehtiin alle 2-vuotiaiden lasten vanhemmille (n=116) Oulun alueel-la. Ihon lämpötiloja mitattiin seitsemästä eri kehon osasta noin kolmen kuukauden ikäisiltä lap-silta (n=34) heidän nukkuessaan kotona päiväuniaan sisällä ja ulkona Pohjois-Suomessa talvel-la. Unen pituutta havainnoitiin ja ympäristön lämpötilaa ja tuulen nopeutta mitattiin. Lasten tal-vivaatetuksesta kerättiin tietoa ja lämpötiloja mitattiin vaatetuksen eri kerroksista sekä kosteuttavälivaatetuksen alta. Vaatetuksen lämmöneristävyyksiä mitattiin lasten kokoa vastaavalla lämp-önukella. Vaadittava lämmöneristävyys arvioitiin ISO 11079 – standardin mukaisesti. Pohjois-suomalaisia lapsiperheiden äitejä (n=21) haastateltiin kulttuurisen tiedon esille tuomiseksi.
Yhteensopivuus perheen, kulttuurisen ulkona nukuttamiskäytännön ja pohjoisen talviympär-istön välillä voidaan saavuttaa, mutta toisaalta myös tasapainoa vähentäviä tekijöitä löytyi. Tal-viympäristö nähtiin tarjoumana lapsen rauhalliselle nukkumiselle sen puhtaan ja raikkaan ilmanja luonnon sekä hiljaisuuden ja rauhallisuuden takia. Talvinen sää vaihteli auringon paisteestakovaan lumipyryyn ja lämpötila muutamista lämpöasteista lähes kolmenkymmenen asteen pak-kaseen lasten nukkuessa vaunuissaan. Paras lämpötila ulkona nukkumiselle oli -5 °C. Ulkonanukuttamista pidettiin itsestään selvänä kulttuurisena tapana. Äidit saivat ohjeita ja kannustustalasten ulkona nukuttamiseen eri lähteistä. Vertailemalla ja jakamalla kokemuksiaan he osallistui-vat myös itse kulttuurisen tiedon rakenteluun. Lasten ulkona nukuttaminen talvella osoittautuiyleisesti hyväksytyksi kollektiiviseksi käyttäytymiseksi, joka toisinaan aiheutti paineita äideille.Lapsen ulkona nukkumiseen liittyi monia riskitekijöitä, mutta kaikki turvallisuusnäkökohdatensin huomioon ottamalla se edisti perheen hyvinvointia luomalla säännöllistä rytmiä ja vahvis-tamalla arjen sujuvuutta. Optimaalisen vaatetuksen lämmöneristävyyden löytäminen systemaat-tisesti eri lämpötiloissa oli vaikeaa; sekä jäähtymistä että hikoilua esiintyi. Ympäristön lämpöti-lan laskiessa keskimääräisen ihon lämpötilan jäähtymisnopeus lisääntyi. Lapset nukkuivat ulko-na pisimpään silloin, kun ihon lämpötilan jäähtyminen oli hitainta. Ensisijaisesti ulkona nukku-misen ajateltiin edistävän lapsen terveyttä.
Lasten ulkona nukuttamisen arviointimallia voidaan hyödyntää käytännössä ohjauksen yhte-ydessä ja tutkimuksen tuottamaa yksityiskohtaista tietoa ohjeistusten päivittämisessä. Tutkimusantaa lähtökohtia kansainväliselle vertailevalle tutkimukselle.
Asiasanat: ihon lämpötila, kulttuuri, lapsi, lastenhoito, mixed methods -lähestymistapa,Pohjois-Suomi, talvi, uni, vaatetuksen lämmöneristävyys


To Tuomo, Eetu, Olli, and Aaro

8

9
Acknowledgements
This study was carried in co-operation with the Institute of Health Sciences and
the Institute of Biomedicine at the University of Oulu as well as Finnish Institute
of Occupational Health, Oulu, Northern Ostrobothnia Hospital District and the
Department of Human Science at the Kyushu University.
Most importantly, I would like to thank all families for your participation. I
appreciate your interest in my study and your contribution to it making this thesis
possible. I want to thank those public health nurses and other persons who helped
me to contact the study families.
My warmest appreciation and the most grateful acknowledgements go to my
supervisors Professor Arja Isola, Professor Hannu Rintamäki and Emeritus
Professor Juhani Hassi. I want to express my deepest gratitude to Arja for your
encouragement, support and advice during my academic studies, especially
during these five years when I have been privileged to work as a doctoral
candidate at the Institute of Health Sciences. I am very grateful for your
enthusiasm when I presented the idea of my research, your trust and that you have
encouraged me to continue until the doctoral thesis. I want to express my special
gratitude to Hannu for inspiring me in the field of thermophysiology. I am very
grateful to you for helpful discussions and valuable support. I highly appreciate
that you always gave me time when I needed to reflect many kinds of issues. I
want to thank Juhani for introducing me to the field of cold research. You had a
significant role in encouraging me to do research in this field.
I would like to express my grateful acknowledgements to The Vice-President,
Professor, Yutaka Tochihara, at the Kyushu University. I highly appreciate that
you gave me the possibility to do the clothing insulation measurements at the
Faculty of Design. I am grateful to Takako Fukazawa, PhD, for your guidance,
valuable comments and patience when introducing me to the field of clothing
insulation measurements. I highly appreciate our cooperation. I wish to express
my gratitude to Koji Tabata as well as the students and the staff at the Research
center for human environmental adaptation for your help with thermal manikin
measurements. My family and I want to express our gratitude to Hitoshi
Wakabayashi, PhD, for sharing with us many unforgettable moments in Japan and
in Finland. I have been privileged to meet all of you.
I want to express my gratitude to Professor Leena Paasivaara and Docent
Sirkka Rissanen, members of the follow-up group, for your valuable comments. I
am grateful to the official referees of the dissertation, Professor Randi Eidsmo

10
Reinertsen and Docent Päivi Kankkunen, for your careful review and valuable
advice to improve this thesis.
I want to express gratitude to Risto Bloigu, MSc, for your statistical guidance,
Anna Vuolteenaho, MSc, for revising the language of my manuscripts and this
thesis, Pertti Tuhkanen, specialized occupational hygienist, for helping with the
measurement of relative humidity, Raija Heino, information specialist, for helping
me in literature searches and Aino-Maria Vuoti, senior in visual communication,
for graphic designing of figure 5.
I am grateful to the staff at the Institute of health sciences, department of
nursing science and health administration for all the support I got during these
years. Working with you and our fruitful discussions have been important to me. I
want to thank docent Tarja Pölkki for inspiring discussions about research among
children.
I warmly thank my fellow students and friends especially Hanna, Maire,
Eeva-Leena, Merja, Outi, Leena, Ulla, Pirjo and Jaana for our conversations that
have been very helpful for me, your support and sharing experiences with me. I
also express my gratitude to all doctoral candidates at the Finnish Post-Graduate
School in Nursing Science.
I would like to thank my friends, Helinä and Minna, for offering refreshing
company and support.
I want to thank my parents, Anni and Paavo, for your encouragement, support
and help throughout my life. Moreover, I want to thank my siblings, Kirsi, Satu,
Marko and Heli for everything. You and your families will always have a special
place in my life. I also thank Leena, Pentti, Tapio, Ilkka, Outi and your families
for your support.
My dearest gratitude is expressed to my husband, Tuomo. We have shared our
lives; thank you for your love and patience. Our sons, Eetu, Olli and Aaro are the
most important persons in my life. Thank you for richening my life in so many
ways.
This study was financially supported by the Finnish Post-Graduate School in
Nursing Science, the Graduate School of Circumpolar Wellbeing, Health and
Adaptation, Northern Ostrobothnia Hospital District and Health Science
Academic Leaders and Experts.
Oulu, October 2011 Marjo Tourula

11
List of abbreviations and definitions
BAT brown adipose tissue
°C Celsius
CI confidence interval
CIS cold injury syndrome
CLO thermal insulation of clothing, 0.155 m2 °C/W
CV coefficient of variation
Icl basic thermal insulation, m2 · K · W–1
Icle effective clothing insulation, m2 · K · W–1
IREQ required clothing insulation, m2 · K · W–1
ISO International Organization for Standardization
It total thermal insulation, m2 · K · W–1
M metabolic rate (W/m2)
REM rapid eye movement sleep
RH% relative humidity
rs Spearman’s rank correlation coefficient
SD standard deviation
SIDS sudden infant death syndrome
Tsk mean skin temperature (°C)
VO2 oxygen consumption

12

13
List of original publications
This thesis is based on the following articles, which are referred to in the text by
their Roman numerals:
I Tourula M, Isola A & Hassi J (2008) Children sleeping outdoors in winter: Parents’ experiences of a culturally bound childcare practice. International Journal of Circumpolar Health 67(2–3): 269–278.
II Tourula M, Isola A, Hassi J, Bloigu R & Rintamäki H (2010) Infants sleeping outdoors in a northern winter climate: skin temperature and duration of sleep. Acta Paediatrica 99(9): 1411–1417.
III Tourula M, Fukazawa T, Isola A, Hassi J, Tochihara Y & Rintamäki H (2011) Evaluation of the thermal insulation of clothing of infants sleeping outdoors in Northern winter. European Journal of Applied Physiology 111(4): 633–640.
IV Tourula M, Pölkki T & Isola A (2011) The cultural meaning of children sleeping outdoors in Finnish winter: A qualitative study from the viewpoint of mothers. Manuscript.
In addition, some unpublished data are presented in the thesis.

14

15
Table of contents
Abstract
Tiivistelmä
Acknowledgements 9
List of abbreviations and definitions 11
List of original publications 13
Table of contents 15
1 Introduction 17
2 Review of the literature 19
2.1 The concept of environment .................................................................... 19
2.2 Winter environment in Northern Finland ................................................ 21
2.3 Families’ cultural childcare ..................................................................... 22
2.4 Cultural clothing practice and thermal resistance ................................... 25
2.5 The well-being of children in the north ................................................... 27
2.6 Sleep of children ..................................................................................... 29
2.7 Thermal environment of children ............................................................ 34
2.7.1 Thermal balance and thermoregulation ........................................ 34
2.7.2 Interaction between sleep and thermoregulation .......................... 37
2.7.3 Symptoms of thermal stress .......................................................... 39
2.8 Summary of the literature........................................................................ 40
3 Aims and hypotheses of the study 43
4 Methodology 45
4.1 Mixed methods research design .............................................................. 45
4.2 Subjects and settings ............................................................................... 48
4.3 Procedures, data collection and analysis ................................................. 49
4.3.1 Children sleeping outdoors in winter from the viewpoint
of parents ...................................................................................... 49
4.3.2 Observation and physiological measurement of infants ............... 51
4.3.3 Microclimate and clothing insulation measurements ................... 54
4.4 Ethical considerations ............................................................................. 58
5 Results 61
5.1 Winter environment in Northern Finland ................................................ 63
5.2 Cultural knowledge-building .................................................................. 64
5.3 Family well-being ................................................................................... 66
5.4 Winter clothing of outdoor sleeping children .......................................... 69
5.5 Well-being of the children ....................................................................... 74

16
5.5.1 Children’s sleep ............................................................................ 74
5.5.2 Children’s skin temperatures ........................................................ 77
6 Discussion 81
6.1 Validity and reliability of the quantitative studies ................................... 81
6.2 Trustworthiness of the qualitative study .................................................. 85
6.3 Discussion of the results .......................................................................... 86
6.3.1 Winter environment in Northern Finland ..................................... 86
6.3.2 Cultural knowledge-building ........................................................ 87
6.3.3 Family well-being ......................................................................... 89
6.3.4 Winter clothing of outdoor sleeping children ............................... 91
6.3.5 Well-being of the children ............................................................ 94
6.4 Summary of the findings and conclusions .............................................. 97
6.5 Implementation and suggestions for future research ............................... 98
References 101
Appendices 121
Original publications 129

17
1 Introduction
”All people who coat their children with clay or butter, wrap them in buffalo hide
or tapa or silk, swaddle them or fasten them on cradle boards will give as the
primary reason for so doing their desire to protect the child” (Mead 1954: 400).
Cultural communities provide their own developmental pathways for their
children within a specific cultural context, and these cultural pathways are made
up of everyday routines of life (Weisner 2002). The goal of improving children’s
well-being is a common point of view, but consensus as to what is the best
sleeping arrangement for children cannot be found despite many decades of
research (Giannotti & Cortesi 2009).
Sleep problems in children are a major issue of concern to parents (Sadeh &
Anders 1993, Morrell 1999, Thunström 1999, Lam et al. 2003, Wake et al. 2006,
Bayer et al. 2007, Martin et al. 2007), and they experience low efficacy related to
infant’s daily rhythm and sleep (Salonen et al. 2008). Infants’ sleep problems
have more extensive effects on family well-being.
In Finland, the first guidelines pointing out how important and good it is for
children’s health to have them sleep outdoors in the winter came out in the 1920s
(Ylppö 1921); today it is a culturally bound custom. However, infants’ greater risk
for hypothermia due to their physiological characteristics (Pocock et al. 1999) as
well as the geographical location of Finland between the 60th and 70th northern
parallels of latitude and its cold winters (Finnish Meteorological Institute 2011)
highlight the safety aspects of this childcare practice.
Sleep is biological behavior of the child, as well as being strongly affected by
cultural values and beliefs (Jenni & O’Connor 2005). Cultural differences of
childcare practices dealing with children’s sleep and studies comparing cultures
can be found, but according to the review of Jenni & O’Connor (2005), scientific
literature is scant, widely scattered, and narrowly focused. Hardly any of the
previous studies have even mentioned children sleeping outdoors in the winter. To
our knowledge, this is the first study to focus on children’s daytime sleeping
outdoors, although it is a common childcare practice in the Nordic countries
(Reima group 2009). In Finland, 60,980 children were born in 2010, and there are
30,1621 children at the age of 0–4 years (Tilastokeskus 2011), which means that
the outdoor sleeping practice concerns many children and families in Finland. Just
like McKenna et al. (2007) considered in their article how several generations
have been influenced to treat their babies in a certain way and why it came to be
considered “normal”, in this study answers are sought to the meaning of children

18
sleeping outdoors in the winter. Without an understanding of sleep characteristics
in different cultures, it is difficult to provide guidelines and counseling on sleep
and what is normal or expected (Mindell et al. 2010b).
Sleep studies most often focus on nighttime sleep instead of assessing the
roles of daytime sleep (Schwichtenberg et al. 2011). The clothing and wrapping
of infants and thermal environment have been studied, as overheating is
associated with SIDS (sudden infant death syndrome) (Eiser et al. 1985, Bacon et
al. 1991, Wigfield et al. 1993, Watson et al. 1998, Vennemann et al. 2009).
Studies have also addressed newborn babies’ thermal environment in incubators
(Telliez et al. 1998, Bach et al. 2000ab, Bach et al. 2001, Telliez et al. 2004) as
well as using baby-size manikins (Elabbassi et al. 2001, Elabbassi et al. 2002,
Elabbassi et al. 2004) and infants’ thermal environment in the home setting in
New Zealand (Nelson & Taylor 1989, Baddock et al. 2004) and England (Eiser et
al. 1985, Nicoll & Davies 1986, Wailoo et al. 1989ab, Bacon et al. 1991, Wigfield
et al. 1993) during the day (Anderson et al. 1990) and night (Lodemore et al.
1992, Wigfield et al. 1993). McCullough et al. (2009) have developed a
temperature ratings model for children’s cold weather clothing from the age of
four years for the activity level of walking, but no studies were found about
infants’ thermal environment and winter clothing used outdoors during daytime
sleep in a northern country.
The purpose of this study is to create a comprehensive view and add
understanding about the childcare practice of children sleeping outdoors in the
context of Northern Finnish winter for enhancing the well-being of children and
families. A general view of the topic is described and created, the thermal
insulation of clothing of infants sleeping outdoors in the northern winter climate
is evaluated and the relationships between thermal environment, infants’ skin
temperatures and daytime outdoor sleep duration are described.
The paradigm of nursing science is defined through its essential concepts:
human being, health, nursing and environment (Kankkunen & Vehviläinen-
Julkunen 2010), all of which are concerned in this study. This doctoral thesis
belongs to the field of applied clinical nursing research, which begins with
practice-related questions (Polit & Beck 2010). Public health nurses have
counselled families about children's outdoor sleeping since the 20th century. This
study provides a basis for and viewpoints on this counseling.

19
2 Review of the literature
2.1 The concept of environment
Environment is a complex entity consisting of spatial, temporal and qualitative
characteristics. When the environment is viewed spatially, concentric circles can
be defined to be around the person in the center where some elements of the
environments have a direct impact upon the person’s life while some only
influence it in minor ways. Viewed temporally, the environment includes the
duration and manner of presence; elements exist continuously, intermittently or
fleetingly as well as regularly or randomly. Environment can be classified
qualitatively into physical, social and symbolic environment. The main concept in
the physical environment is ecosystem, which can be defined as a system of
interactions among the various human groups themselves and with the physical
and chemical components of the environment where the basic process is energy
transfer between and among elements of the environment. Physical environment
is composed of biotic elements ranging from viruses to human beings, and abiotic
elements, i.e. artifacts starting with clothing as the most proximal elements and
extending to satellites orbiting the earth. Individuals and groups with whom a
person interacts constitute the social environment, whereas symbolic environment
consists of ideational elements (ideas, values, beliefs, history, and knowledge),
normative elements (rules, laws, expectations, and constraints) and institutional
elements (roles, organizations, institutions, society, and culture). (Kim 2000.)
According to Bronfenbrenner (1977, 1979), children’s development should be
studied by taking account of the multilevel social, material and cultural context.
The most proximal first level is microsystem level, consisting of the physical,
social and symbolic characteristics of the environment determining the conditions
either promoting or inhibiting a child’s development. Mesosystems are collections
of a child’s daily environments’ microsystems and the synergetic effects of the
various components. Exosystems, such as the health care system, are not
necessarily a part of an individual’s system, but affect peoples’ lives nevertheless.
Macrosystem is the cultural level affecting the micro-, meso- and exosystems.
Background, age, culture, and conditions of life affect the meanings that we
give to the environment (Lindheim & Syme 1983), and for that reason everyone
experiences the environment in their own way, changing the objective
environment into subjective life space (Lewin 1917, cited by Bronfenbrenner

20
1977). Attachments are formed to places that fulfill emotional needs and make it
possible to develop and maintain people’s identities (Kaiser & Fuhrer 1996).
Favorite places affect psychological well-being and eventually health (Korpela
2002). Korpela (1989) has described that physical environments can be used to
regulate pleasure/pain and self-experience, and those regulation processes that
produce experiences and cognitions partly form a place identity. Proshansky et al.
(1983: 59) have described place identity as follows:
“These cognitions represent memories, ideas, feelings, attitudes, values,
preferences, meanings, and conceptions of behavior and experience which
relate to the variety and complexity of physical settings that define the day-
to-day existence of every human being. At the core of such physical
environment-related cognitions is the ‘environmental past’ of the person; a
past consisting of places, spaces, and their properties which have served
instrumentally in the satisfaction of the person’s biological, psychological,
social, and cultural needs.”
According to the study of Barker (1987) daily activities seemed to consist of
operational cycles, episodes with varying durations, most of which were
determined by environment and behavior setting. Episodes are series of
meaningful, goal-directed actions (Hoogsteder et al. 1998). According to
Leininger (1997), environmental context includes events with meanings and
interpretations in physical, ecological, sociopolitical and cultural settings.
Several child-rearing variables have been shown to have associations with the
presence of environmental affordances and demands, which play an important
role in influencing maternal behavior by acting as environmental cues for place-
related behavior (Miller et al. 1998). In the field of environmental psychology,
place rules for behavior are seen in situations when human actions fit into the
place in which they occur (Canter 1992). The term affordance can be defined as
what the environment offers to persons for actions to be undertaken (Gibson
1986). Affordances are prerequisite for action (Greeno 1994). There are potential
affordances and actualized affordances consisting of perceived, utilized and
shaped affordances (Heft 1989, Kyttä 2003). Related to the perception and
actualization of affordances are a person’s skills, practice, strength, goals and
intentions (Costall 1995). Affordances can be seen in different ways in different
cultures due to socialization (Reed 1996, Kyttä 2003). Each person may also see
uniquely apparent emotional coloring of affordances (Kyttä 2003) and due to

21
individuals’ different perceptions, affordances can be seen as positive or negative,
as benefits or injuries, as safeties or dangers (Gibson 1986).
A healthy environment provides a range of opportunities for its inhabitants to
shape the conditions that affect their lives (Lindheim & Syme 1983), safety,
opportunities for social integration, and the ability to predict and/or control
aspects of the environment, whereas unhealthy environments are those that
threaten safety and undermine the creation of social ties, and that are conflictual,
abusive, or violent (Taylor & Repetti 1997). Circumstances of the physical and
emotional environment impact children’s health and set the groundwork for future
vulnerabilities and resiliencies (Reading & Wien 2009). A quiet, safe living
environment has been described to increase families’ sense of well-being (Åstedt-
Kurki et al. 1999).
The term context has been defined as the contents of the immediate situation
but also broader contents of the neighborhood, community, and culture
(Bronfenbrenner 1979). In this study the term context means the surroundings
from the immediate physical level of infant’s skin and clothing to the more distant
levels of social and cultural surroundings and northern winter environment.
2.2 Winter environment in Northern Finland
The northern region can be defined to encompass the areas in the northern parts of
the United States, Canada, Denmark, Iceland, Norway, Sweden, Finland and the
Russian Federation (Young 2008). In this study, when the north is viewed
worldwide, areas located above 60°N latitude and thus the whole Finland is
defined as north, whereas when the north is viewed nationally, only the areas of
the Kainuu region, Northern Ostrobothnia and Lapland are located in the north.
The Finland’s geographical position between the 60th and 70th northern
parallels of the latitude in the Eurasian continent's coastal zone causes
characteristics of both a maritime and a continental climate, depending on the
direction of air flow. A quarter of the surface area of Finland lies to the north of
the Arctic Circle and is situated on the same latitudes as Alaska, the southern part
of Greenland and Siberia, but the mean temperature is several degrees higher due
to the Baltic Sea, inland waters and airflows from the Atlantic, which are warmed
by the Gulf Stream. However, the Asian continental climate can be seen in
Finland as severe cold in winter. The lowest temperature in Finland, recorded in
1999, is −51.5°C. Weather types can change rapidly in winter and snow- and
rainfalls are typical. (Finnish Meteorological Institute 2011.) Windy weather

22
increases the cooling effect on the skin that can be expressed as wind chill
temperature (ISO 11079 2007).
Winter can be defined to be the longest season in Finland, lasting from 100 to
200 days, as it begins when the mean temperature remains below 0°C. Permanent
snow covers open grounds about two weeks after winter begins and the lakes
freeze over in late November and early December. (Finnish Meteorological
Institute 2011.)
The "polar night" is the period lasting for 51 days, when the sun does not rise
above the horizon at all north of the Arctic Circle. The day is also short in
southern Finland, lasting only about 6 hours. (Finnish Meteorological Institute
2011.)
Climate can be defined as long-term average weather, and observations have
been made to indicate that the climate has changed. Earth’s average temperature
has increased, and the probabilities of certain types of weather phenomena have
become more frequent and intense, such as heat waves and heavy downpours,
while others have become less frequent and intense, such as extreme cold events.
(Le Treut et al. 2007.)
2.3 Families’ cultural childcare
Culture can be defined in a variety of ways (Kao et al. 2004), such as sets of
beliefs, norms, and expectations, but it is also more complex, the entire
nonbiological inheritance of human beings, everything that is socially constructed
and learned (Hufford 1990, cited by Jenni & O’Connor 2005). The definition of
culture is ambiguous, being sometimes too narrow, omitting salient viewpoints, or
too general, so that when it loses its real meaning (Kao et al. 2004). According to
Shore (1996: 44), culture can be defined as “an extensive and heterogeneous
collection of “models”, models that exist both as public artefacts “in the world”
and as cognitive constructs “in the mind” of members of a community”. Culture
can be seen in a static perspective as a system of rules that can be measured and
predicted. In a dynamic perspective culture is seen with no concrete reality
existing in a person’s mind as a cognitive system with shared symbols and system
of meanings. (Kao et al. 2004.)
Culture is dynamic and adaptive in response to the environment (Lenburg et
al. 1995), when people with cultural backgrounds and experiences actively
interact with their environments (Kao et al. 2004). Culture can be seen
comprehensively as a way of life over time and in different geographic locations

23
(Leininger 2006). Cultural practices are often taken for granted by its members,
but may seem strange and not understandable to persons outside the culture
(Connolly et al. 2006).
The idea of locally rational action can be found in ecocultural theory (Shore
1996). Local situations are comprised of everyday routines and activities where
connected, schematized and shared cultural knowledge is used to adapt and make
complex decisions to survive in local communities. It is possible to enter families’
cultural pathways by interviewing and observing their daily routines. (Weisner
2002.) Chess and Thomas (1984: 21) defined the interaction with environmental
demands by using the concept of “goodness of fit”, which can be attained “when
the organism’s capacities, motivations and style of behaving and the demands and
the expectations of the environment are in accord”. Environmental situations may
have a positive effect on well-being by enhancing fit between a person’s goals,
activities, and surroundings or negative effects by reducing the level of person-
environment fit (Wicker 1972).
In a study of Winch et al. (2005) where local knowledge from Bangladesh
related to newborn period was studied, newborns were seen as vulnerable to cold
and cold was thought to cause many problems. However, some of their practices,
such as keeping the infant on a mat on the floor could increase the risk of
hypothermia. (Winch et al. 2005.) At the same time, Swedish mothers considered
the outdoors an appropriate and desired environment for their infants and
achieved good health for infants by daily walks, provided healthy doses of fresh
air and toughened the child to the cold climate. This was in contrast to Italian and
American mothers, who prevented exposure to cold. (Welles-Nyström et al. 1994.)
Culture in different contexts is influenced by how mothers see affordances, and
these affordances and demands create cues for appropriate place-related behavior
(Miller et al. 1998).
History is part of our shared cultural knowledge. Childcare practices and the
meanings of these practices have varied in different eras. At the time of Greeks
and Romans, for example, it was thought necessary for infants to be exposed to
cold and heat and to harden the baby’s skin by salting it with soda ash (Lipton et
al. 1965). Spartan-like hardening after birth by bathing newborns in very cold
water disappeared in the second quarter of the 19th century (Korones 2004). Until
in 1958, lower environmental temperature was found to associate with higher
mortality of infants (Silverman et al. 1958). Infants have slept tightly swaddled
and in different kinds of beds; infant baskets and cradleboards, such as woolen
canoe-like cradles, have been used, and infants have been carried on parents’

24
backs by the Sami people in Lapland while tending reindeer herds. (Lipton et al.
1965.) However, little attention has been paid to the historical point of view in
terms of sleeping arrangements (Stearns et al. 1996).
The interest in child development and the significance of children’s sleep
started to increase internationally in the late 19th century, focusing first on
physical health issues and material arrangements. For example, popular health
columns in women’s magazines discussed how much covering should be use to
avoiding overheating and underprotection of the child. Parents were told to avoid
getting children’s feet cold, because this was associated with dangerous
conditions such as fatal sore throat. Children were thought to need regularity and
rituals as well as appropriate physical arrangements: proper ventilation, covers,
mattress and isolation. The use of cradles declined as the use of cribs increased,
the design of which was widely discussed in magazines in the 1920s and 1930s.
Children were also moved to separate bedrooms when housework became noisier
due to vacuum cleaners and sewing machines, noise from the radio, and more
vivid lighting due to electricity. (Stearns et al. 1996.)
During this time, in 1920, a pediatrician called Arvo Ylppö had as him aim to
reduce high infant mortality in Finland by distributing childcare guidelines to
mothers (Ylppö 1921). Poor air quality inside the home, preventing rickets and
creating sound blood were reasons why the childcare practice of having children
sleep outdoors was recommended. Fresh and cold air was thought to increase
blood circulation in the linings of the nose and mouth and thus increase immunity
to bacteria. Sunlight was thought to be an important preventive factor against
diseases as well. Infants were able to get wind, fresh air and sunlight in their faces
without any harm if they were regularly familiarized with cold air at an early
stage. (Ylppö 1939.) Only newborn children were regarded as too sensitive to
cold, but infants only a few weeks old were already allowed to sleep outside
without worrying at temperatures of −10°C…−15°C (Ylppö 1947). At the
beginning of the 20th century it was not so common to see children sleeping
outdoors during the winter. Public health nurses met children who had not been
outdoors during the first year of their lives. There were not enough clothes for the
children, and the few garments there were made of adults’ old ones. Children had
to be outdoors by turns due to lack of shoes. (Punto 1991.)
Public health nurses first had to disseminate the bases of the importance of
outdoor sleeping on a child’s health and well-being in the 1940s and 1950s; after
that, they changed the emphasis of counseling from stressing the importance of
outdoor sleeping to practical instructions and advice about duration and suitable

25
clothing in the 1960s (Varjoranta 1992). The viewpoint that mothers should put
their children outside to sleep was disseminated in parenting manuals and
information was distributed by public health nurses, so that parents adopted the
practice in their everyday lives. Little by little experience and social knowledge
has increased. Today, the practice of children sleeping outdoors is common in the
Nordic countries, being most common in Denmark and Finland (Reima group
2009). In the study by the Reima group (2009), most Finnish parents thought that
it is very important for children to be outdoors every day. As Lipton et al. (1965)
have written: “infant care practices are deeply rooted in culture and represent the
end results of generations of experience and conviction”.
2.4 Cultural clothing practice and thermal resistance
Cultural traditions and beliefs influence the thermal environment in which infants
are cared (Watson et al. 1998, Nelson et al. 2000). For example, infants in Japan
and Korea sleep indoors in bedding combinations of greater insulation than
infants in New Zealand in comparable season (Wilson & Chu 2005). Traditional
outdoor infant care practices, such as swaddling and living in traditional tents
called “Ger” in the Mongolian winter (Tsogt et al. 2006) and using a form of
dressing called “manta pouch” in Peru (Tronick et al. 1994) have been
represented as protecting the infant from the cold.
Swaddling, a form of some degree of infant motor restraint by using bands or
clothes wrapped around an infant was widely used worldwide before the 18th
century (Lipton et al. 1965). Today its prevalence varies in different countries; in
England, for example, it is hardly endorsed (Morrell & Cortina-Borja 2002). van
Sleuwen et al. (2007) have compiled information about swaddling and evaluated
its benefits and disadvantages in their systematic review. Swaddling has been
shown to calm infants; excessively crying infants cry less, it may sooth pain and
increase daytime sleep duration and decrease arousing. It has been suggested that
the restraint of arms may inhibit full extensor movements that startle the infant.
Swaddling has been shown to improve neuromuscular development, motor
organization and ability to self-regulation and increase physiologic distress in
preterm infants. Swaddling can be helpful for temperature control, but it can also
cause risk for hyperthermia when misapplied. Supine position decreases the risk
for SIDS more in swaddled babies than in those without swaddling, but increases
the risk if the baby is overdressed and the head is covered. Other adverse effects
that were mentioned in the review were an increased risk of the development of

26
hip dysplasia, which is related to legs in extension, higher risk of respiratory
infections related to tightness of swaddling and deficiency of vitamin D in some
countries. (van Sleuwen et al. 2007.)
In Finland the outdoor sleeping childcare practice in winter is commonly
endorsed, indicated by the fact that the Social Insurance Institution of Finland
distributes maternity packages including infants’ winter clothing and sleeping
bags to expecting mothers without any charge. The maternity package is common:
annually about 40,000 packages are distributed in Finland. Families have been
very content with the package. (Bogdanoff & Hämäläinen 2011.)
In the study of Wailoo et al. (1989a) parents received advice on how to clothe
their babies from a number of sources, such as other parents and health care
workers, mainly given at the time of birth, whereas in the study of Wigfield et al.
(1993) parents seemed to instinctively provide appropriate thermal conditions for
their infants to sleep in. Correlations were found in both studies with clothing
insulation of infants and room temperature, with parents applying more insulation
on colder nights with lower bedroom temperatures (Wailoo et al. 1989a, Wigfield
et al. 1993), and also applying more insulation in winter than in summer
(Wigfield et al. 1993). Contrary to these studies, some infants had also been
dressed inappropriately indoors when perceptions of expected weather conditions
and temperature outdoors had affected in parents’ decisions when making
assessments of ambient temperature (Nicoll & Davies 1986, Tuohy & Tuohy
1990, Bacon et al. 1991, Wigfield et al. 1993).
According to the study of Eiser et al. (1985), most mothers thought that
infants got colds from other people, but almost half of the mothers felt that infants
could get colds by being cold or wet. Bacon (1983) suggests that although
according to this folklore that infants should be well wrapped to prevent them
from getting a cold, wrapping them well may lead to overheating and fever. On
the contrary, Grover et al. (1994) found that bundling a healthy infant caused a
rise in skin temperature, but not in rectal temperature, suggesting that elevated
rectal temperature should rarely be attributed to bundling, in contrast to infections.
Clothing provides thermal resistance between the child and its environment,
maintaining the body in an acceptable thermal state in a variety of environments.
Thermal insulation is provided by the garments themselves, and especially the air
trapped in them, as well as by the layers of air trapped between the skin and
clothing layers. (Parsons 2003.) When a clothing ensemble consists of many
layers the total insulation is much higher than could be expected from the
insulation of the material layer alone (Havenith 1999). Many factors affect the

27
thermal characteristics of clothing, such as dry thermal insulation, transfer of
moisture and vapor through clothing, heat exchange with clothing, compression,
pumping effects, air penetration and subject posture (Parsons 2003).
2.5 The well-being of children in the north
The concept of well-being is broad and sometimes used as a synonym for health,
quality of life, life satisfaction, wellness and happiness. The definition of health
has shifted away from viewing health in terms of freedom from disease to an
emphasis on the individual’s ability to perform daily activities, and further to an
emphasis on the positive themes of happiness, social and emotional well-being,
and quality of life (McDowell & Newell 1996). Heath is described as an integral
part of the everyday life of families consisting of various dimensions of
experienced well-being and unwell-being, security and different life-habits
(Åstedt-Kurki et al. 1999). The determinants of health can be seen as proximal,
intermediate and distal. Proximal determinants of health include conditions that
have a direct impact on physical, emotional or spiritual health (e.g. health
behaviors, physical and social environment), intermediate determinants can be
seen as the origin of those proximal determinants (e.g. health care systems,
educational systems, community infrastructure, environmental stewardship,
cultural continuity), while distal determinants have profound influence on the
health of populations because they represent political, economic, and social
contexts that construct both intermediate and proximal determinants (e.g. historic,
political, social and economic contexts). (Reading & Wien 2009.) The well-being
of humans is influenced by many factors of the environment as well as a variety
of personal attributes, and that is why promotion of well-being should be based on
an understanding of interplays between these factors, not focusing exclusively on
one just factor (Stokols 1992).
In order to attain an overview of scientific studies related to the well-being of
children in the north, a literature search was performed using the Ovid Medline,
Cinahl, Arctic & Antarctic Regions (EBSCO), and PsycINFO databases. The
search was limited to April 2011 using the following search terms: infant* welfare
/ infant* well-being / child* welfare / child* well-being / toddler* welfare /
toddler* well-being / teen* welfare / teen* well-being / youth welfare / youth
well-being / adolescent* welfare / adolescent* well-being / famil* welfare /
famil* well-being / social welfare (limit all child or family) AND arctic / arctic
regions / northern / north / circumpolar / cold / cold climate / polar. Inclusion

28
criteria were as follows: 1) the place where the data was collected was located ≥
60 degrees northern latitude; 2) scientific empirical article or systematic literature
review; 3) the article was in English; 4) an abstract was available; 5) search terms
were included in the title and/or abstract and/or MeSH-term. Altogether 52
articles fulfilled inclusion criteria after duplicates were excluded (Table 1).
Table 1. The result of literature search related to the well-being of children in the north
by different databases.
Database Potentially relevant citations (n) Studies meeting inclusion criteria (n)
Ovid Medline 796 35
Cinahl 172 2
Arctic & Antarctic Regions 211 5
PsycINFO 755 10
The phenomenon of children’s well-being in the north consisted of studies dealing
with five main categories. Health care studies (n = 14) consisted of interventions
concerned for example with the prevention of childhood farm injuries in North
America (Hartling et al. 2004) and outdoor wintertime sun safety education
(Walkosz et al. 2007). Also studies about health services such as children’s use of
general practitioner services in Finland (Vuorinen et al. 1991), and using
telehealth in rural communities in Canada (Ens et al. 2010) were found.
Environmental health studies (n = 12) concerned exposures that were detrimental
to health, such as metals in the soil of children’s urban environment in Sweden
(Ljung et al. 2006) and infants’ blood lead concentrations and iron deficiency in
Canada (Willows & Gray-Donald 2002), as well as associations between diseases
and geographic (Samuelsen et al. 1993) and seasonal variations (Stephenson et al.
2002). Studies about diseases (n = 11) such as allergy in relation to pet ownership
(Braback et al. 2001) and well-being in children with for example symptoms of
ADHD (attention deficit hyperactivity disorder) (Taanila et al. 2009) emerged.
The fourth biggest group comprised studies about lifestyle and health habits
(n = 9). Our study of children sleeping outdoors (Study I) was placed in this
category. No other studies about sleep were found; instead, studies for example
about nutrient intake (Nakano et al. 2005) and life goals among adolescent (Lekes
et al. 2010) were found. The fifth category include children in research (n = 6),
such as ethical, legal and social issues in birth cohort studies (Ries et al. 2010)
and methodological issues in interviewing families (Åstedt-Kurki et al. 2001).

29
The topics of the studies on children’s well-being were versatile. However,
there was a lack of studies about the associations between climatic factors and
child health (Bunyavanich et al. 2003), and especially studies related to children’s
cold exposure in the area of children’s environmental health, even though it
comprises important physical environmental factors, such as air pollution, lead,
chemicals and noise, which all have effects on children’s health (Pond et al. 2007).
Growing evidence can be found that climate-health relationships pose increasing
health risks under future projections of climate change (Patz et al. 2005), and
children are especially vulnerable to these risks because of their greater exposure,
sensitivity, and dependence on caregivers for appropriate preparedness and
response (Sattler 2003, Ebi & Paulson 2007).
2.6 Sleep of children
The development and effects of sleep. During the first years of life sleep patterns
develop fast (Armstrong et al. 1994, Acebo et al. 2005, Sadeh et al. 2009). The
sleep cycles, during which REM (rapid eye movement sleep, active sleep) and
non-REM (quiet sleep) sleep stages alternate, last about 50 minutes in infants,
compared to about 90–110 minutes in adults. Newborn infants’ sleep is different
from that in older children as they fall directly into REM sleep (Hill et al. 2007).
More than half of their sleep consists of REM sleep (Roffwarg et al. 1966, Anders
et al. 1995), which decreases throughout childhood, while non-REM sleep
increases steadily (Roffwarg et al. 1966).
Multiple sleep periods around the clock consolidate progressively to one
main continuous nighttime sleep (Burnham et al. 2002) and well-defined daytime
naps by about three months of age (Parmelee et al. 1964). At about six months of
age the sleep cycle starts with non-REM sleep and infants have learn to move
from one sleep phase to another without waking (Hill et al. 2007).
Three-month-old children still spend most of their time sleeping; total sleep
duration is about 14.5 hours and daytime sleep duration about 4.5 hours
(Iglowstein et al. 2003, Sadeh et al. 2009) divided into two or more naps per day
(Iglowstein et al. 2003). Children usually give up taking daytime naps between 3
and 5 years of age, but some children not until the age of 7 (Weissbluth 1995,
Iglowstein et al. 2003) or later (Crosby et al. 2005). Total sleep duration
continues to decrease from about 14 hours at 6 months of age to about 8 hours at
16 years of age (Iglowstein et al. 2003). However, large individual variation can
be found in sleep duration especially during the first year of life (Iglowstein et al.

30
2003, Sadeh et al. 2009) indicating variability in sleep need or sleep opportunity
(Sadeh et al. 2009).
It has been hypothesized that sleep has a restorative effect on brain
metabolism and effects on memory consolidation, learning (Maquet 2001, Gómez
et al. 2006), as well as emotion and behavior regulation (Bates et al. 2002, Ward
et al. 2008). Sufficient sleep quantity and good sleep quality have been associated
with higher levels of optimism and self-esteem, thus affecting well-being in
children (Lemola et al. 2011). Reduced total sleep time might cause adverse
effects on normal cognitive (Dahl 1996) and social development (Lavigne et al.
1999). Daytime sleep has been shown to have similar beneficial effects on visual
learning as sleeping during the night among adults (Mednick et al. 2003), and
infants’ daytime sleep has appeared to promote abstraction in learning of
language (Gómez et al. 2006). Wake et al. (2006) found that most sleep problems
in the first two years of life are transient, but infants’ sleep problems have also
been associated with neurodevelopmental disorders later in childhood (Thunström
2002), and sleep problems in childhood may even associate with poor psychiatric
state in adulthood (Gregory et al. 2005). Less sleep during infancy has been
associated with weight gain and obesity in infants (Tikotzky et al. 2010), in
preschool-aged children (Taveras et al. 2008) and in adulthood (Landhuis et al.
2008).
The transactional model of sleep in socio-cultural contexts. In their
transactional model of sleep-wake regulation Sadeh & Anders (1993) have
emphasized that infants need to be viewed as part of a system where bidirectional
links between parenting and infant sleep can be seen. Infants’ sleep is affected by
maturational, intrinsic constitutional, biological, temperamental and medical
factors affect, but also by parental interactive behaviors. Parents’ socio-cultural
and environmental context, developmental history and memories, personality and
psychopathology as well as infant’s age, developmental characteristics and sleep
patterns affect parents’ beliefs, expectations, emotions and behaviors related to
infants’ sleep. (Sadeh et al. 2010.)
According to the transactional model, infants’ sleep, parenting competence
and well-being are influenced by complex relationship systems (Sadeh et al.
2010). Maternal cognitions about difficulty with limit setting, anger at the infant’s
demands, and increased doubts about parenting competence have been
significantly associated with infant sleep problems by Morell (1999). Parents
have experienced low efficacy related to infants’ daily rhythm and sleep (Salonen
et al. 2008) and during the stage when sleep patterns are developing, sleep

31
problems are a major issue of concern to parents (Sadeh & Anders 1993, Morrell
1999, Thunström 1999, Lam et al. 2003, Wake et al. 2006, Bayer et al. 2007,
Martin et al. 2007) in many cultures (Mindell et al. 2010b). Cultural norms affect
definitions as to what can be seen as normal or problematic sleep behavior (Jenni
& O'Connor 2005).
In addition to the direct effects of sleep problems to infants, they may also
cause adverse effects in a broader context. Infants’ sleep problems have been
associated with mothers’ depression (Armstrong et al. 1998, Hiscock & Wake
2001, Lam et al. 2003, Bayer et al. 2007), poorer general health in both mothers
and fathers (Martin et al. 2007) and parents’ marital conflicts (Richman 1981, El-
Sheikh et al. 2006, Meijer & van den Wittenboer 2007). However, in the study of
Lam et al. (2003) families functioned well despite having children with sleep
problems that resulted in an increase in maternal depressive symptoms.
Schwichtenberg et al. (2011) found in their study that those infants who took
more naps experienced more positive maternal affect, involvement, and
verbalizations. Sleeping more during the daytime may give infants and their
mothers a break, promoting optimal parenting. (Schwichtenberg et al. 2011.) It
has been shown that it is possible to reduce maternal symptoms of depression by
using behavioral infant sleep improving interventions (Hiscock & Wake 2002). In
general, infants’ sleeping problems cause substantial costs to health services
(Morris et al. 2001).
The method of falling asleep and sleep location have been shown to predict
sleep duration (Sadeh 2004). Parental involvement at bedtime has been correlated
with an increased number and duration of night waking of infants (Touchette et al.
2005, Sadeh et al. 2009, Tikotzky & Sadeh 2009), and infants who sleep in a crib
in a separate room have been reported to have fewer night wakings and shorter
settling times (Sadeh 2004). High level of parental interactions and soothing
routines are assumed to prevent infants from developing their own self-regulation
and self-soothing skills, resulting in shorter and more fragmented sleep (Sadeh et
al. 2010). Parenting practices that encouraged infants to independence and self-
soothing were associated with extended and more consolidated sleep by Sadeh et
al. (2009) in a study where a large (5,006 infants and toddlers) sample from the
United Stated and Canada was examined. Moreover, as bidirectional links exist
between parenting and infant sleep, interpretations that infants with sleep
problems require more parental involvements have also been presented (Tikotzky
& Sadeh 2009). According to McKenna et al. (2007) and McKenna & Volpe
(2007), expectations of self-soothing of infants and sleeping separately from

32
parents do not promote infants’ biological and emotional needs. Bedsharing has
been described to enhance the emotional connection between mother and infant
(Abel et al. 2001, McKenna & Volpe 2007), when infants need comfort and
regulation from their parents especially during the first months of life (Anders
1994).
The socio-cultural context has an important role in shaping parental
expectations and practices (Sadeh & Anders 1993, Sadeh et al. 2010). Cultural
norms, ethnicity and background may influence for example whether certain sleep
behaviors among children are determined as problematic (Jenni & O'Connor 2005,
Mindell et al. 2010b, Sadeh et al. 2010) and what is regarded as an appropriate
sleep environment (McKenna et al. 2007). Mindell et al. (2010a) provided a
picture of parenting and sleep ecology using a large global sample of parents of
29,287 infants and toddlers from predominantly Caucasian (Australia, Canada,
New Zealand, United Kingdom, and United States) and predominantly Asian
(China, Hong Kong, India, Indonesia, Japan, Korea, Singapore, Malaysia,
Philippines, Taiwan, Thailand, and Vietnam) regions. Striking cultural differences
were found, as 57% of children in predominantly Caucasian regions fall asleep
independently, compared to 4% of children in predominantly Asian regions
(Mindell et al. 2010a), who also had later bedtimes, shorter total sleep times,
increased parental perception of sleep problems, and were more likely to bed-
share and room-share. Minimal differences were found for daytime sleep with all
children (Mindell et al. 2010b).
Cultural values, parental expectations and infant’s developmental needs affect
the distance between the sleep locations of parents and infant; physical proximity
ranges from cosleeping in the same bed to sleeping independently in a separate
room. According to the findings of Nelson et al. (2000) 23 of 26 nonindustrialized
societies used separate beds for their infants (cradles, cots, mats, or hammocks) in
which the baby was placed during the day. According to the study of Morelli et al.
(1992), Mayan parents, who let their children sleep in their mothers’ bed,
described it in terms of the value of closeness with the baby, regarding the U.S.
families’ practice of having babies sleep in separate rooms as “tantamount to child
neglect” (Morelli et al. 1992), whereas having babies sleep in a separate room
was explained by the mothers from the U.S. to be of value for babies’
independence (Morelli et al. 1992, Germo et al. 2007). According to Anders &
Taylor (1994) many U.S. families shortened this distance by using baby monitors
designed to help parents hear their children sleep.

33
Seasons and children’s sleep. Few studies can be found comparing physical
environmental factors, such as seasons with children’s sleep. In the study of Javo
et al. (2004) cross-cultural differences in parenting among Sami and Norwegian
parents of four-year old children were studied. They found that compared
Norwegian mothers, Sami mothers regulated their children’s bedtime more
according to the season, letting children stay up much longer during the summer.
Carscadon & Acebo (1993) have described in their study parental reports of
seasonal mood and behavior changes in children aged about ten, some of whose
sleeping times were described as lengthening in the fall and winter.
Seasonal variation in sudden infant death syndrome (SIDS) with winter peaks
has been reported in both the northern and southern hemispheres in several
countries, such as Norway (Vege et al. 1998, Arnestad et al. 2001), Sweden
(Milerad et al. 1993, Haglund et al. 1995), Britain (Douglas et al. 1996, Douglas
et al. 1998), Ireland (Douglas et al. 1998), Italy (Montomoli et al. 2004), New
Zealand (Schluter et al. 1998), the United States (Malloy & Freeman 2004)
Hawaii (Mage 2004), California (Chang et al. 2008) and Ohio (Strimer et al.
1969), Kuwait (Douglas & Al-Sayer 1991) and Israel (Sivan et al. 1992). Outdoor
sleeping was mentioned in only three studies, where more deaths occurred
indoors compared with deaths occurring outdoors (Milerad et al. 1993, Vege et al.
1998, Arnestad et al. 2001), the proportion of which fluctuated from 40% to 9%
over different time periods. Outdoor deaths were more common during the winter
than during the summer. (Milerad et al. 1993, Vege et al. 1998.) Sleeping in prone
position is known to be a major cause of SIDS (Gilbert et al. 2005), and prone
sleeping has been associated with a greater risk in winter than in summer
(Mitchell et al. 1999). The seasonal variation of SIDS has also been associated
with cold meteorological temperature (Jones et al. 1994, Leiss & Suchindran
1996), but not with Föhn winds (Macey et al. 2000), thermal stress due to excess
thermal insulation (Nelson et al. 1989, Fleming et al. 1990) or having the head
covered (Beal 2000), viral infection (Harrison et al. 1999, Lindgren 1999), or
outdoor air pollution (Hoppenbrouwers et al. 1981, Klonoff-Cohen et al. 2005)
with highest levels in the winter (Hoppenbrouwers et al. 1981). However, a trend
of a diminishing rate of seasonal variation has been seen (Arnestad et al. 2001,
Malloy & Freeman 2004, Chang et al. 2008).
A literature search was performed using the Ovid Medline, Cinahl, Arctic &
Antarctic Regions (EBSCO), and PsycINFO databases in order to ensure a broad
scope of the literature in addition to articles gained through manual searches. The
search was limited to April 2011 using the following search terms: cold

34
temperature, arctic regions, cold climate, arctic, circumpolar, polar, north, cold
AND child*, infant*, toddler*, babies, baby AND sleep*, nap. Scientific
empirical articles or systematic literature reviews written in English were
included, and after duplicates were excluded, 29 articles fulfilled inclusion criteria
(Table 2). The included articles were related to thermal environment,
thermoregulation and/or circadian rhythm of infants (n = 15), sudden infant death
syndrome (n = 10) and child care (n = 4).
Table 2. The results of the literature search related to children’s sleep by different
databases.
Database Potentially relevant citations (n) Studies meeting inclusion criteria (n)
Ovid Medline 192 14
PsycINFO 564 7
Cinahl 68 1
Arctic & Antarctic Regions 110 7
2.7 Thermal environment of children
2.7.1 Thermal balance and thermoregulation
Thermoregulation is physiological ability to maintain body temperature within a
restricted range under conditions involving variable internal and external heat
loads (IUPS Thermal Commission 2001). Human response is influenced by air
temperature, radiant temperature, humidity and air movement, which constitute
the basic environmental parameters. Human activity and clothing are the personal
factors that influence the heat loads (Parsons 2003). The relationship with heat
production and heat transfers between the body and environment can be viewed
as heat balance equation (Parsons 2003, ISO 11079 2007):
M – W = E + R + C + K + S [W/m2],
where M is metabolic rate, which provides energy to do mechanical work (W).
The rest of the energy is released as heat. The body loses heat by radiation (R)
from the skin and by the evaporation (E) of water from the skin and the
respiratory tract. Heat is also lost to cooler environment by convection (C). Heat
loss to cooler objects in direct contact is conductive (K) heat flow, which becomes
a relevant factor when infants sleep in supine position. The sum of heat
production and loss provides the body heat storage rate (S), which is zero in heat

35
balance, positive in heat gain and negative in net heat loss. The heat balance
equation describes how the body can maintain a core body temperature (Parsons
2003), which in low birth weight infants at rest should be between 36.7 and
37.3°C, and the core temperature and Tsk change less than 0.2 and 0.3°C/hour,
respectively, in thermoneutral ambient temperature. When the infant becomes
older and the body weight increases, the temperature of a neutral thermal
environment decreases (Sauer et al. 1984). Also interindividual variability (Bach
et al. 2000a), metabolic rate (oxygen consumption) (Hey & O'Connell 1970) and
sleep variables, which are more sensitive to a mild cold exposure (Telliez et al.
1997, Bach et al. 2000a), should be observed when defining thermoneutrality.
Temperature regulation processes are activated when the environmental
temperature is not in the thermoneutral zone (Parsons 2003).
Removal to a relatively cold environment at birth causes temperature drops in
neonates, and increased heat production is essential for survival. The temperature
regulation response begins within minutes of birth, with oxygen consumption and
heat production increasing two- to three-fold. Basic heat production is generated
through metabolic activity and additional heat production through shivering and
nonshivering thermoregulation. (Asakura 2004.)
Newborn infants’ primary source of heat production is based on nonshivering
thermogenesis in brown adipose tissue (BAT), which is mainly located in the
interscapular region, neck, between the ribs and around the kidneys, serving as a
warming mechanism for the blood supply of vital organs (Aherne & Hull 1966,
Wehrli et al. 2007). The activation of nonshivering thermogenesis is dependent on
oxygen supply and thus it results in an increase in oxygen consumption
(Schubring 1986). Because of reduced demands for nonshivering thermogenesis
when shivering takes place, the importance and prevalence of BAT diminishes
with age (Johansson 1959, Wehrli et al. 2007). In the study of Hassi (1977) the
prevalence of BAT was about 90% in the samples from study children from the
fetal stage to the age of one year, diminishing to 43% in 1- to 13-year-old children,
when for example only single brown adipose cells or cell clusters were found in
the interscapular adipose tissue. Aherne and Hull (1966) have also suggested that
infants cared for in an ambient temperature lower than neutral may have gradual
depletion of BAT. The heat production increase cannot be continued in prolonged
cold exposure (Bach et al. 1994, Bach et al. 2002), but it has also been suggested
that the thermal resistance of neonates is improved by prolonged exposure to a
cool environment (Glass et al. 1968, Perlstein et al. 1974).

36
Infants are at increased risk of heat loss due to a large surface area in relation
to weight, a thin insulating fat layer and poor shivering mechanism (Pocock et al.
1999) due to relatively immature skeletal muscles (Herpin et al. 2002, Asakura
2004). Shivering has only been observed in infants when the body temperature
has decreased considerably (Darnall 1987) or in extreme cold exposures
(Adamson et al. 1965). Temperature sensitive receptors have been identified in
the skin, hypothalamus, spinal cord, blood vessels and in other body regions
(Hensel 1974), being either warm or cold types and sending signals to the
hypothalamic thermoregulatory center (Parsons 2003). According to Mestyàn et
al. (1964), the skin on infants’ face is sensitive to environmental temperature
changes, so that cooling of the face increases oxygen consumption.
Heat is transferred from the deeper tissues of the body to the surface of the
body where it can be lost to the environment. Vasoconstricted skin creates more
effective insulation compared with vasodilated skin. When the body becomes cold,
the heat is preserved by vasoconstriction, and if necessary, heat is generated by
shivering and nonshivering, whereas when the body becomes hot it loses heat
through vasodilation, and if required, through sweating. (Parsons 2003.) Skin
blood flow is well developed in infants (Hey 1972); in very low birthweight
infants it develops over the first two to three days of life (Lyon et al. 1997).
Cooling-induced vasoconstriction first takes place in peripheral vessels, seen as
falling skin temperatures in the extremities (Wissler 2008), and thus central-
peripheral skin temperature difference can be used as an indicator of cold stress
(Lyon et al. 1997). Skin temperatures in the extremities and trunk have been
shown to fall sharply in a heat-losing cool environment in infants, whereas the
temperature of the nape remains warmer because it contains brown adipose tissue
(Silverman et al. 1964, Rylander et al. 1972). Tsuzuki et al. (2008) found that
children had a greater decline in skin temperature of the hand and foot than adults
during exposure to cold, suggesting greater vasoconstriction in children.
Newborns are able to exhibit behavioral responses by changing posture and
modifying the body surface area exposed to the surroundings, thus changing
convective and radiative heat loss; e.g. crouch prone position reduced the body
surface area to 69% in cool environment (Stothers & Warner 1984).
Already a small 1.5°C decrease below thermoneutrality in air temperature has
been shown to affect body temperature, sleep, and restlessness without increase in
VO2 (oxygen consumption) (Bach et al. 2000a), suggesting that peripheral and
central thermal responses are evoked in cool exposure, but are not large enough to
induce heat production in brown adipose tissue (Telliez et al. 1997).

37
In a warm environment, sweat is secreted over the skin to allow cooling by
evaporation (Parsons 2003). The sweat gland density in infants is larger than in
adults, but the sweating response is much more ineffective. Sweating nearly
always occurs first, and profusely, on the head, accounting for 85% of the total
body heat loss in supine position; the trunk and limbs start sweating later. (Foster
et al. 1969.) The threshold is lower for the rate of fall than the rate of rise in skin
temperature (Libert et al. 1979) when all body sites are more sensitive to cold
than to warm (Stevens & Choo 1998).
When Eiser et al. (1985) asked mothers how they checked whether the baby
was too hot, most mothers relied on feeling the baby or checking the baby’s color.
Some mothers mentioned also that the baby become irritable if too hot or were
sweaty. Only few mothers used their own feelings of hot as a guide to the baby’s
temperature. It was more difficult for mothers to estimate whether the infant was
too cold. Almost all mothers felt the baby while others relied on color or observed
when the baby became irritable when too cold.
2.7.2 Interaction between sleep and thermoregulation
Wailoo et al. (1990) suggest that thermal discomfort could cause awakenings in
infants as some poorly wrapped babies woke early, and especially heavily
wrapped babies in warm rooms did so even more frequently. According to other
studies, exposure to warm temperature did not disturb sleep, but the duration of
REM sleep has been observed to increase in a cold environment (Bach et al. 1994,
Telliez et al. 1997, Bach et al. 2000ab, Bach et al. 2001, Telliez et al. 2004) at the
expense of non-REM sleep (Azaz et al. 1992, Telliez et al. 1997, Bach et al.
2000ab, Bach et al. 2001, Telliez et al. 2004), decreasing the total sleep time
(Telliez et al. 1997, Bach et al. 2000ab, Bach et al. 2001). Cold exposure delays
sleep onset (Bach et al. 1996) and enhances awakenings (Azaz et al. 1992, Telliez
et al. 2004).
It has been found that overall sleep movements decrease in warm conditions
(Bach et al. 1994), while small body movements increase during cold exposure
(Hey 1969, Azaz et al. 1992, Bach et al. 1994, Telliez et al. 1997, Bach et al.
2000a), often causing the lightly clothed infant to wake up, especially at 1 to 3
months of age (Azaz et al. 1992) and during REM sleep (Bach et al. 1994). This
is in contrast to the findings of Hey & O’Connell (1970) where clothed infants did
not cry or move in response to cooling.

38
Higher levels of VO2 have been found due to larger metabolic heat
production during REM sleep than during non-REM sleep in short cool exposure
suggesting that thermoregulation could be maintained mainly by vasoconstriction,
but partly also by increasing REM sleep (Telliez et al. 2004), the
thermoregulation of which is not impaired, as it is in adults (Bach et al. 1994,
Telliez et al. 2004).
Infants sleeping in the prone position have been found to have a lower
metabolic rate than those sleeping in the supine position (Ammari et al. 2009),
although infants in the supine position have lower heart rate and peripheral skin
(Skadberg & Markestad 1997, Ammari et al. 2009) and rectal temperature (North
et al. 1995). According to the findings of Baddock et al. (2004), bed-sharing
infants experienced warmer thermal conditions than cot-sleeping infants, but they
were still able to maintain a normal core temperature.
Apneas have been observed more frequently in warm conditions than during
exposure to cool temperatures (Bach et al. 1994). It has also been found that
infants’ auditory thresholds increased in warm rooms (Franco et al. 2001) and
when the face was covered (Franco et al. 2002).
The biorhythm is immature in newborns and requires functional maturity of
the central nervous system components. Parents and other family members in a
home environment are governed by the circadian rhythm, and it is an important
developmental step for the newborn baby to fit into this tempo. (Thomas & Burr
2002.) The daily body temperature rhythm develops earliest (McGraw et al.
1999). According to the findings of Lodemore et al. (1991), rectal temperature
changed little in the first two weeks of life, but by 6 weeks of age rectal
temperature was higher at bedtime than later in the night, and those whose rectal
temperature fell below 36.5°C also slept longer. The fall has been shown to be
greater during nighttime sleep than during the day, even when infants have had
similar sleep durations (Anderson et al. 1990). The characteristic pattern of
decreased nighttime deep body temperature is exhibited by infants by 4 months of
age (Wailoo et al. 1989b, Lodemore et al. 1991, Lodemore et al. 1992); this rate
of fall is unaffected by environmental conditions (Wailoo et al. 1989a, Anderson
et al. 1990). Skin temperatures change less than rectal temperature during nights
(Wailoo et al. 1989b); for example, no significant circadian variation rhythm in
abdominal skin temperature was found in the study of Glotzbach et al. (1994).

39
2.7.3 Symptoms of thermal stress
Neonatal hyperthermia can develop when the infant is in an environment that is
too hot and the core body temperature rises above 37.5°C. This should be
differentiated from fever caused by infection with microorganisms or other
sources of inflammation. Hyperthermia is less frequent than hypothermia,
although both situations can occur equally easily in neonates. (World Health
Organization 1997.) Overheating has been associated with increased risk for
SIDS, and it has been suggested that cultural child care practices may facilitate
hyperthermia, partly causing the disparate rates of SIDS in different countries
(Nelson et al. 1989, Ponsonby et al. 1992).
The newborn can be defined to be under cold stress when a body temperature
is 36.0–36.4°C, under moderate hypothermia with a temperature of 32.0–35.9°C,
and severe hypothermia with a temperature below 32°C (World Health
Organization 1997). Hypothermia has also been defined as a core body
temperature of 35°C or lower (Culic 2005). Accidental hypothermia called cold
injury syndrome (CIS) has been described to exist in neonates and infants due to
exposure to cold (Mann & Elliot 1957). Children with CIS have had cold skin and
limbs along with red facial skin and some of them have been sleepy, hypotonic
and inactive. Most of those patients have also been cyanotic with bradycardia and
bradypnea, and have had scleredema (Culic 2005). In a 10-year cohort study
between 1976 and 1985 in Croatia by Culic (2005), 103 children, most of them
between 0–15 days old, were diagnosed with CIS. Behavioral customs and
insufficient home heating could have affected the frequency of CIS when most of
the children were hospitalized in the winter. The frequency of CIS in Split has
decreased, as only 5 infants were hospitalized between 1991 and 1995. (Culic
2005.) Neonatal hypothermia has also been reported to exist in many other
countries (Goldsmith et al. 1991), being a common problem especially in
developing countries (Dragovich et al. 1997). In Ladakh, India, most of the
pediatric hospital deaths have been reported to occur in the winter months (Wiley
2004).
According to Glass et al. (1968), the rate of increase in body weight and
length among newborn infants was faster in warmer conditions. Hypothermia
may cause psychological and neurodevelopmental disturbances (Culic 2005) and
it is associated with increased morbidity for example from infections (Dagan &
Gorodischer 1984), and it has been seen as a contributing factor to mortality

40
among newborns (Mann & Elliot 1957) and premature infants even in mild cold
stress (Day et al. 1964).
Chilblains, also known as pernio, are a moderately severe form of cold injury
characterized by localized inflammatory skin lesions with cyanosis and
subcutaneous swelling in areas exposed to prolonged nonfreezing temperatures
and damp conditions (Long et al. 2005). Chilblains are usually located in the
peripheral parts (fingers, toes, and ears) of the body (Weston & Morelli 2000,
Gardinal-Galera et al. 2010), but chilblains have also been found on the cheek of
a child (Giusti & Tunnessen 1997). Color changes (white, blue, red) of the distal
extremities in response to cold are defined as Raynaud’s phenomenon, the
symptoms of which can begin in childhood (Nigrovic et al. 2003, Tsai et al. 2010).
Due to an oversensitive reaction to cold by vasoconstriction and thus reduced
circulation in peripheral parts of the body, people with Raynaud’s phenomenon
have an increased risk of frostbite, among other physiological, behavioral and
environmental factors predisposing for frostbite (Rintamäki 2000).
When the temperature of tissue is reduced below the freezing point, frostbite
emerges, producing localized necrosis. Although children are particularly
vulnerable to cold injury and frostbites, only few cases have been reported
(Brown et al. 1983, von Heimburg et al. 2001, Krishnamurthy et al. 2009).
Gangrene resulting from frostbite in neonates is an extremely rare event
(Krishnamurthy et al. 2009). In the study of Koljonen et al. (2004) where
frostbite injuries in the Helsinki area from 1995 to 2002 were studied, children
under 13 were not mentioned. Instead, Juopperi et al. (2002) studied the incidence
of patients admitted to hospitals in Finland with frostbite during the period 1986–
1995 and found that frostbites increased linearly with age: 0.9% (n = 11) of the
patients who were 0–9 years old and 8.3% (n = 106) of the patients who were 10–
19 years old had frostbites, respectively. Frostbites in childhood can cause long-
term consequences in the joints and bones (Brown et al. 1983, Ervasti et al. 1993).
Because of the importance of thermoregulation in infants the World Health
Organization (1996, 1997) has published some information for the prevention of
hypothermia aimed at health professionals as well as parents.
2.8 Summary of the literature
Environment can be viewed as a multilevel context (Bronfenbrenner 1979, Kim
2000), which creates affordances and demands acting as cues for place-related
behavior (Miller et al. 1998). Cultural context shapes parental expectations and

41
childcare practices influencing infants’ clothing, sleep and thermal environment.
Infant’s sleep has broad effects on the family well-being. Infants are a vulnerable
population group due to their fast developing sleep patterns and special
characteristics of thermoregulation. This study is based on the view of multilevel
context (Figure 1).
Fig. 1. The childcare practice of children sleeping outdoors is viewed within a
multilevel context.
Level IChildsleep,
thermoregulation
Level IIClothing
Level IIIFamily
Level IVCulture
Level VNorthern environment

42

43
3 Aims and hypotheses of the study
The purpose of the study was to create a comprehensive view and add
understanding about the childcare practice of children sleeping outdoors in the
context of Northern Finnish winter in order to enhance the well-being of children
and families.
The detailed aims, research questions and hypotheses were as follows:
1. To describe and create a general view of the childcare practice of children
sleeping outdoors in winter in Northern Finland.
a) What is the childcare practice of children sleeping outdoors like?
(Studies I, IV)
b) How prevalent is the childcare practice of children sleeping outdoors in
the city of Oulu? (Study I)
c) Why do parents let their children sleep outdoors in winter? (Studies I, IV)
d) What is the meaning of the childcare practice of children sleeping
outdoors? (Study IV)
2. To describe the relationships between thermal environment, infants’ skin
temperatures and daytime outdoor sleep duration in the northern winter
climate.
a) Hypothesis: Duration of infants’ daytime sleep is longer outdoors in the
winter compared with the daytime sleep they take indoors (Studies I, II).
b) Hypothesis: Infants wearing conventionally used thermal insulation have
lower skin temperatures at the end of outdoor sleep than at the end of
indoor sleep (Study II).
3. To evaluate the thermal insulation of the clothing of infants sleeping outdoors
in the northern winter climate.
a) Hypothesis: Deficiency in thermal insulation increases in colder ambient
air temperatures while overdressing increases in warmer ambient air
temperatures (Study III).
b) Hypothesis: Conventional winter clothing of infants does not ensure
thermal balance during outdoor sleeping (Study III).

44

45
4 Methodology
4.1 Mixed methods research design
There is a complex human environment surrounding this study phenomenon. In
health research various levels of human environments can be found from
immediate to more distant environments, emphasizing the need to use
multidisciplinary and multimethod analyses (Stokols 1992) and more complex
research designs to capture the complexity of human phenomena (Sandelowski
2000). A multidisciplinary mixed methods research design has been used in this
study in order to provide a more comprehensive view and better understanding of
the study phenomenon than would have been provided by single methods alone
(Creswell & Plano Clark 2007, Denscombe 2008). Mixed methods allow the use
of all methods possible, both qualitative and quantitative, to address the research
problems and questions. Both numbers and words are important and necessary to
clarify subtleties and provide a broader perspective on the research topic of this
study. (Creswell & Plano Clark 2007.) Pragmatism as a paradigm is associated
with mixed methods research. It is a pluralistic worldview that is focused on the
consequences of actions, real-world practice-oriented, and problem-centered.
(Tashakkori & Teddlie 1998, Creswell 2003, Creswell & Plano Clark 2007,
Denscombe 2008.)
Mixed methods consist of four major types: triangulation, embedded,
explanatory, and exploratory design. The division is dependent on the timing,
weighting and mixing decisions between qualitative and quantitative methods. In
this study, triangulation has been used due to concurrent timing in qualitative and
quantitative data collection. (Creswell & Plano Clark 2007.) In addition,
sequential timing has been used in quantitative studies, where the pilot study
(Study I) gave rise to the hypothesis that was tested in the next quantitative study
(Study II), while the hypothesis that emerged there was tested in the next study
(Study III). Quantitative methods have been used in Studies I–III, and qualitative
methods mainly in Study IV, and partly in Study I (Figure 2). The findings of the
pilot study (Study I) were also used as an aid in sampling when participants were
screened for inclusion in the interview (Study IV) (Denscombe 2008).
Methodological triangulation in the form of quantitative (quan) and qualitative
(qual) methods have been used, as well as data triangulation, due to the variety of
data (time, space and person) (Patton 1990, Kimchi et al. 1991) (Figure 2).

46
Fig
. 2. S
tud
y d
es
ign
an
d t
he
co
urs
e o
f th
e r
es
ea
rch
.
Pil
otS
tud
yI
2004
-200
5A
im:
Des
crib
epa
rent
s’
opin
ions
abou
tthe
irch
ildr
ensl
eepi
ngou
tdoo
rsdu
ring
Fin
nish
win
ter
Su
bje
cts:
Par
ents
of
chil
dren
unde
r2
year
sof
ag
e(n
=11
6)M
eth
od:
A c
ross
-se
ctio
nal
stud
yus
ing
ques
tion
nair
e, q
uan
(qua
l)A
nal
ysis
:O
ne-s
ampl
et-
test
, cro
ss-t
abul
atio
n, χ
2,
Man
n-W
hitn
eyte
st,
cont
enta
naly
sis
Stu
dy
II
2007
-200
8A
im:
Des
crib
eth
e re
lati
onsh
ips
amon
gth
erm
alen
viro
nmen
t, sk
inte
mpe
ratu
rean
d in
fant
s’
outd
oor
slee
pdu
rati
onS
ub
ject
s:34
abo
ut3.
5 m
onth
old
infa
nts
Met
hod
s: C
ross
-ove
rob
serv
atio
nal
stud
y, T
sk,
Ta, q
uan
An
alys
is:
Mea
n, S
D,
corr
elat
ions
, pai
red-
sam
ples
t-te
st,
inde
pend
ent-
sam
ples
t-te
st
Stu
dy
III
2008
-200
9A
im: E
valu
ate
the
ther
mal
insu
lati
onof
clo
thin
gof
in
fant
ssl
eepi
ngou
tdoo
rsin
w
inte
rS
ub
ject
s: 3
4 ab
out3
.5
mon
thol
din
fant
s, a
bab
y-si
zeth
erm
alm
anik
inM
eth
ods:
Cal
cula
tion
sof
It
, Icl
e, I
RE
Q, d
iffe
renc
ebe
twee
nob
serv
edcl
othi
ngin
sula
tion
and
IRE
Q, R
H%
, qu
anA
nal
ysis
: P
aire
d-sa
mpl
est-
test
, cor
rela
tion
s, l
inea
rre
gres
sion
Pub
lica
tion
IP
ubli
cati
onII
Pub
lica
tion
III
Pub
lica
tion
IV
Stu
dy
IV20
07-2
010
Aim
: Exp
lore
the
mea
ning
of c
hild
ren
slee
ping
outd
oors
in
Fin
nish
win
ter
from
the
view
poin
tof
mot
hers
Su
bje
cts:
21
Fin
nish
mot
hers
Met
hod
s:E
xplo
rati
vede
scri
ptiv
est
udy
desi
gn u
sing
unst
ruct
ured
inte
rvie
ws,
qua
lA
nal
ysis
: C
onte
nt a
naly
sis
Su
mm
ary
2011
Ove
rall
inte
rpre
tati
on
Doc
tora
lth
esis

47
Qualitative methods have been used to understand the broader context of the
childcare practice of children sleeping outdoors in winter by paying attention to
the voice of the parents who let their child sleep outdoors. Study IV provides a
culturally sensitive subjective point of view. Quantitative methods have been used
to obtain an objective view of interaction between the child and winter
environment. Both methods have been given equal weight when qualitative and
quantitative data have been analyzed separately and merged together during the
interpretation in the summary.
The childcare practice of outdoor sleeping in winter comprises five levels,
from microlevel to a more distant cultural and environmental level, as well as
interactions between these levels. Although the phenomenon is described as levels
within each other, all levels also have a direct contact to the child. The northern
winter environment has been in evidence in all Studies I–IV. Study results are
presented according to these levels. (Figure 3.) The triangulation design-
multilevel model has been used in order to form a general view of the system by
collecting different types of data from different levels of the system (Creswell &
Plano Clark 2007).
Fig. 3. The phenomenon of outdoor sleeping childcare practice and the studies
involved.
Level IChild
Level IIClothing
Level IIIFamily
Level IVCulture
Level VNorthern environment
Study II
Study I Study III
Study IV

48
4.2 Subjects and settings
Study I was carried out as a questionnaire study in the city of Oulu in November
and December 2004. The questionnaire was distributed to the parents of children
under 2 years of age using the services of child health clinics. Background
information of the study families (n = 116) is presented in Table 3.
The persons interviewed in Study IV between 2007 and 2010 were mothers
(n = 21), who described their family as consisting of themselves, husband (90%)
and 1 to 10 children aged between 2.5 months and 21 years. They lived in
Northern Finland (Kainuu region, Northern Ostrobothnia and Lapland) in towns
(33%), in municipal centers (43%) and in the countryside (24%). Some families
had earlier lived in southern parts of Finland and the USA. The families selected
to Study IV had similar characteristics and backgrounds as those who participated
in Studies I–III.
Physiological measurements of the infants and measurements of
environments (Studies II–III) were conducted in the natural settings of the
families’ homes in town and country settings in Northern Finland (Kainuu region,
Northern Ostrobothnia and Lapland) between January and March 2007 and
between December 2007 and March 2008. Thirty-four families (Table 3)
participated; 33 infants during both outdoor and indoor daytime sleep and one
during outdoor sleep only.
A baby-size thermal manikin (Kyoto Electronics manufacturing Co., Ltd) was
used for the calculations of the insulation of clothing ensembles in the thermal
chamber at the Research Center for Human Environment Adaptation at the
Faculty of Design, Kyushu University, Fukuoka, Japan in December 2008. The 8-
segmented manikin represented an about 4-month-old infant with a body surface
area of 0.311 m2, a weight of 5.7 kg, and height of 60 cm.

49
Table 3. Background information of the subjects in Studies I–III (n, %).
Background variables Study I Study II, III
Mother Father Mother Father
n (%) n (%) n (%) n (%)
Age
20–29 67 (58) 54 (47) 15 (44) 11 (33)
30–39 46 (40) 50 (44) 17 (50) 18 (55)
40–60 3 (2) 10 (9) 2 (6) 4 (12)
Education
No occupational education 13 (11) 6 (5) 2 (6) 1 (3)
Occupational education 26 (23) 43 (39) 8 (24) 15 (47)
Polytechnic school 43 (37) 25 (23) 12 (35) 7 (22)
University 34 (29) 36 (33) 12 (35) 9 (28)
Number of children Family
1 58 (50) 14 (41)
2–3 49 (42) 16 (47)
4–9 9 (8) 4 (12)
Housing
Apartment building 51 (44) 9 (27)
Semi-detached or terrace house 47 (41) 10 (29)
One-family house 17 (15) 15 (44)
Country where the family had lived
Only in Finland 99 (86) 28 (82)
In the Nordic countries 3 (3) 2 (6)
In other countries 13 (11) 4 (12)
Characteristics of the infant Infant
17/17
14.3 (3)
60.9 (3.9)
6215 (1001)
Gender girl/boy
Age (weeks, mean, (SD)
Height (cm, mean, (SD)
Weight (g, mean, (SD)
4.3 Procedures, data collection and analysis
4.3.1 Children sleeping outdoors in winter from the viewpoint of parents
Parents’ opinion, attitudes, beliefs and experiences about the childcare practice of
children sleeping outdoors in winter were studied quantitatively and qualitatively.
Data were collected using a questionnaire compiled for the purpose (Study I) and
by interviewing mothers (Study II).

50
The questionnaire was developed by interviewing four parents who had
experiences about this childcare practice and by using theoretical background
information and questionnaires (Raatikka et al. 2001) designed for adults and
adolescents to obtain information about cold exposure. The questionnaire was
evaluated by a researcher specializing in cold exposure and tested by bachelor’s
degree students (n = 15) from the Department of Nursing Science and Health
Administration at the University of Oulu.
The questionnaire consisted of three items: the background information of the
family (7 questions), children’s outdoor sleeping practices during the winter (23
questions) and parents’ opinions and grounds for having the child sleep outdoors
in the winter (21 statements). A description of variables is given in Publication I
as appendices. The questionnaire includes Nominal, Interval and Likert Scales as
well as open questions.
The questionnaires were distributed to public health nurses in seven areas of
child welfare clinics in the city of Oulu. Nurses were advised to distribute
questionnaires systematically to all those parents who came to the reception of the
clinic and had children under 2 years of age. Both mother and father had a
possibility to complete the questionnaire at home or at the clinic and return it
anonymously in a closed envelope to the nurse.
The material analyzed consisted of 116 questionnaires (45%). Quantitative
data were analyzed using SPSS for Windows version 12.0 (SPSS Inc., Chicago,
IL, USA) and MS Excel. Cross-tabulation and the χ2 test were used when follow-
up density and using a baby monitor to listen to the baby were compared as well
as when children who slept longer outdoors and those children who slept longer
indoors were compared with the number of siblings and the types of housing. The
one-sample t-test was used for testing the hypothesis. Non-responder (n = 10)
analysis was conducted for testing whether non-responder bias affected the results
(Kotaniemi et al. 2001). Data from those who responded to the questionnaire and
those who did not were compared using cross-tabulation, the χ2 test and the
Mann-Whitney test. Data of open questions were content-analyzed.
There was a need to understand profoundly the meaning of children sleeping
outdoors in winter as there existed conflicts between some viewpoints in the
results in Study I, such as parents’ opinions that there are no disadvantages to
letting the child sleep outdoors in winter, although parents also evaluated that
their child had had cold hands or feet after outdoor sleeping.
Finnish mothers who let their child sleep outdoors and who lived in Northern
Finland constituted the inclusion criteria for interviews (Study IV). Purposive

51
sampling with potential to provide rich data was used when cases with a wide
range of variation on the experiences of outdoor sleeping practice were selected
purposefully (Patton 1990, Giacomini & Cook 2000, Côté & Turgeon 2005, Polit
& Beck 2010); mothers living in the countryside and in cities in a large
geographic area in Northern Finland, mothers with different family sizes, and
mothers who regularly put their children out to sleep as well as mothers who did
not let their children sleep outdoors so often were selected for the interviews.
Snowball sampling was used, i.e. some mothers recruited other mothers who
conformed to the selection criteria (Parahoo 2006, Polit & Beck 2010). In
addition, public health nurses asked mothers to volunteer, and announcements of
the possibility to participate in the study were placed on notice boards at child
welfare clinics.
A qualitative design was adopted, and unstructured interviews were used to
collect the data. The location where the interview took place was selected by the
participants when mothers were interviewed once face-to-face at home or in the
researcher’s office between 2007 and 2010. The data were collected until
saturation was reached (Dey 1996, Parahoo 2006, Polit & Beck 2010). The
interviews were recorded, except for one mother whose interview was written
down. The average duration of the interviews was 36 min (range 20–61 min),
which constituted 254 transcribed A4 pages.
Inductive content analysis was used for the purpose of building up conceptual
categories (Hsieh & Shannon 2005, Elo & Kyngäs 2008). A meaning unit (a word,
part of a sentence, a sentence or a paragraph) which constituted a central meaning
was selected as the unit of analysis (Graneheim & Lundman 2004). Data were
reduced by coding, and comparisons were made for finding similarities and
differences between codings. These were organized into relevant sub-categories.
Generic categories were created through interpretation by grouping sub-categories
that belonged together, and by continuing the process of abstraction and
combining generic categories, the main category was formed and conceptualized.
(Dey 1996.)
4.3.2 Observation and physiological measurement of infants
Measuring infants’ skin temperatures and observing sleep durations gave a chance
to obtain information about the sleeping child in the winter environment.
Observational studies and defining the characteristics and risks of environments
of people’s everyday lives are needed for enhancing environmental health and

52
protection (Lebowitz et al. 2008, Barrett 2009). Measurements in this study were
as noninvasive as possible, and they did not affect the normal sleeping habits
when recordings were made in the natural settings of the families’ homes under
weather conditions and wrapping type chosen by the parents. Event sampling
included in structured observation was done when data were collected to
document specific events (Parahoo 2006, Polit & Beck 2010) of infants’ daytime
sleep outdoors and indoors. This study was a nonexperimental study where the
researcher did not intervene with the independent variable (Polit & Beck 2010).
Selection criteria included healthy outdoor-sleeping infants aged about 3
months (Studies II–III). At that age, infants’ sleep has developed so that well-
defined daytime naps can be specified (Parmelee et al. 1964) and the outdoor
sleeping practice in families was thought to already have developed (Study I).
The sampling was nonprobability convenience sampling (Polit & Beck 2010) as
the voluntary families were recruited through public health nurses in child welfare
clinics and using parents’ social networks and snowball sampling.
Normal skin temperature values in children are undetermined (Azaz et al.
1992, Svedberg et al. 2005); therefore Study II was designed to assess skin
temperatures during outdoor as well as indoor sleeping in the same infants. Study
II was conducted as a crossover study where subjects (n = 33) served as their own
controls (daytime sleep indoors and outdoors). Moreover, measurements of one
child were done only outdoors. Outdoor and indoor measurements were
performed at a time corresponding to daytime sleep, and depending on the
weather conditions, the parents decided whether the infants first slept outdoors or
indoors. Measurements were performed during weekdays due to the same rhythm
of the day, with the exception of measurements in two families, which were done
on weekends, as they had the same kind of rhythm during the week and on
weekends. The mean (SD) interval between measurements for each infant was 7
(5) days; the first test was done outdoors in 22 families, indoors in 11 families,
and only outdoors in 1 family.
Quantitative data were collected as objectively and accurately as possible
(Parahoo 2006) when in vivo measures were performed, i.e. measures performed
directly within or on living organisms (Polit & Beck 2010). Skin temperatures
were measured at 7 sites on skin areas on the forehead (T1), cheek (T2), chest (T3),
lower arm (T4), back of the hand (T5), shin (T6) and dorsal foot (T7) using
thermistor probes (Dräger skin temperature sensor, part number 2M21916,
2M21943, Drägerwerk Aktiengesellschaft, Germany). The probes were securely
attached to the infant’s skin with adhesive tape using thicker tape for insulation on

53
the forehead and cheek during outdoor sleep. The probes were always placed at
the same lefthand body side as skin temperatures have been shown to be
symmetrical on both sides of the body (Svedberg et al. 2005). A data-logger
(SmartReader 8; ACR Systems Inc., Vancouver, Canada) recorded temperatures at
one-minute intervals throughout the infant’s sleep. During outdoor sleep, the
recording started when the child was taken outdoors and during indoor sleep
when the child was laid in the cot. Recordings were discontinued when the child
woke up and was taken indoors.
The mean skin temperature (Tsk) was calculated by weighing the local skin
temperatures by representative areas according to the following equation
(Solomon 1985, Puhakka et al. 1994):
Tsk = 0.14 × T1 + 0.05 × T2 + 0.34 × T3 + 0.14 × T4 + 0.05 × T5 + 0.21 × T6 + 0.07 × T7
A structured observation data collection procedure was done: background
information, environmental circumstances, clothing information, the general
condition of the child and events during the child’s daytime sleep were written
down. The infants were closely monitored during sleep by the same experimenter
and the mothers, both to check security because of the probes and to take notes on
events during the infants’ naps. When the infant was settled, with eyes closed
sleep was defined as starting; the infant was defined as being awake when the
eyes were open and the infant was babbling, crying or moving. The duration of
sleep was observed and the precise time of sleep onset and the end of sleep
written down. Subjective temperature assessment was carried out by palpating the
infant’s hands and feet immediately after sleep and estimating if the hands and
feet were felt cool or cold or if the infant was sweaty. Photographs were taken of
the child and the environment for creating a possibility to go back and check the
observations and measurements procedures.
SPSS for Windows version 16.0 (SPSS Inc., Chicago, IL, USA) was used in
statistical analysis. In serial measurements, summary measures are analyzed in the
same way as in the original observations and raw data (Altman 1990, Matthews et
al. 1990), and the results are given as means, standard deviations and correlations
calculated by the Spearman correlation coefficient. The paired-samples t-test was
used to compare durations of sleep, ambient temperatures, Tsk between sleep onset
and end of sleep, and changes in Tsk for 33 infants. The rate of change of Tsk
(°C/min) was defined by calculating the difference between the mean Tsk value of
a 6-minute period from the end of sleep and a 6-minute period from the onset of
the infant’s peaceful sleep. The same 6-minute period at the end of sleep was used

54
for calculating central (T3) – peripheral (T7) skin temperature differences. The
Independent-Samples t-test was used to test the relationship with outdoor sleep
duration and going for a walk during outdoor sleep by mother as well as carryover
effect between treatments’ order (outdoor/indoor sleep) with outdoor sleep
duration. Results were considered significant at a level of p < 0.05.
4.3.3 Microclimate and clothing insulation measurements
Microclimate temperatures of the infants’ clothing (Study III) were recorded at
the same time as skin temperatures (Study II), and ambient air temperature, air
velocity, and humidity between clothing layers were recorded. Specific data were
collected about the type and amount of clothes, which were based on prevailing
weather conditions and experiences of the parents. For the evaluation of the
thermal insulation of the clothing of infants sleeping outdoors in the northern
winter connections between Study II and Study III were needed (Figure 4).
Fig. 4. Connections between Study II and Study III.
Study II
CHILD
Clothing information
Activity level
Tsk
ENVIRONMENT
Temperature
Air velocity
Study III
IREQGeneral
calculationsfor different
ambienttemperatures
THERMALMANIKINClothinginsulation
measurements
INSULATION OFOBSERVEDCLOTHING
INDIVIDUAL CALCULATIONSOF IREQ-VALUES
EVALUATION

55
During outdoor sleeping, microclimate temperatures were recorded inside the
middle layer (T8), inside the infant’s snowsuit (T9), inside the sleeping bag (T10),
10 cm from the infant’s face (T11), and 50 cm from the pram (Ta). During indoor
sleeping probes were inside the middle layer if used (T12), inside the covering
(T13), 10 cm from the infant’s face (T14) and 50 cm from the cot (Ta). The probes
(NTC DC95, type 22520HM, DIGI-KEY, Thief River Falls, MN, USA) were
placed on the left side on the infant’s chest and connected to a data-logger
(SmartReader 8; ACR Systems Inc., Vancouver, Canada), which was set to make
recordings at one-minute intervals. Air velocity was recorded 100 cm from the
pram by using an anemometer (Testo 491, Testoterm GmbH & Co., Lenzkirch,
Germany). Humidity (RH%) was recorded at five-minute intervals with a
miniature temperature and humidity recorder (OM-CP-MicroRHTemp, OMEGA,
USA) placed on the infant’s underclothing, on the infant’s abdomen during sleep
indoors (n = 24) and outdoors (n = 25).
An 8-segmented baby thermal manikin (Kyoto Electronics manufacturing Co.,
Ltd) was used for the calculation of clothing ensembles’ insulation. Thermal
manikins are used for analyzing thermal relationship between the human body
and its environment and in determination of thermal insulation of clothing
(Holmer 2004). The manikin was placed in a climatic chamber (The Research
Center for Human Environment Adaptation at the Faculty of Design, Kyushu
University, Fukuoka, Japan) with air temperature set at −10°C and relative
humidity at 50% for clothing ensembles No 3–9 and at +22°C for clothing
ensembles No 1–2 (see Appendix 1). The manikin was laid on 3 mattresses
(Appendix 1, Test No 1–5) or on one mattress with the pram (Appendix 1, Test
No 6–9) in supine position, which was how most infants slept while napping
outdoors. Segments of the manikin were heated to 33.0°C, and after reaching
steady state, the computer system recorded the temperatures of each segment and
supplied heating energy every minute over ten-minute periods.
The clothing insulation measurements with the manikin consisted of nine
ensembles (see Appendix 1), where No 1 represented a clothing ensemble worn
indoors, No 7 the least and No 8 the most clothing that an infant might wear
outdoors in winter. No 9 consisted only of clothes from the Maternity package
version 2008 (Kela 2009). Clothes were washed twice before measurements,
because especially in families with more than one child clothes had been washed,
and washing may decrease the thermal insulation due to reduced thickness (ISO
9920 2007).
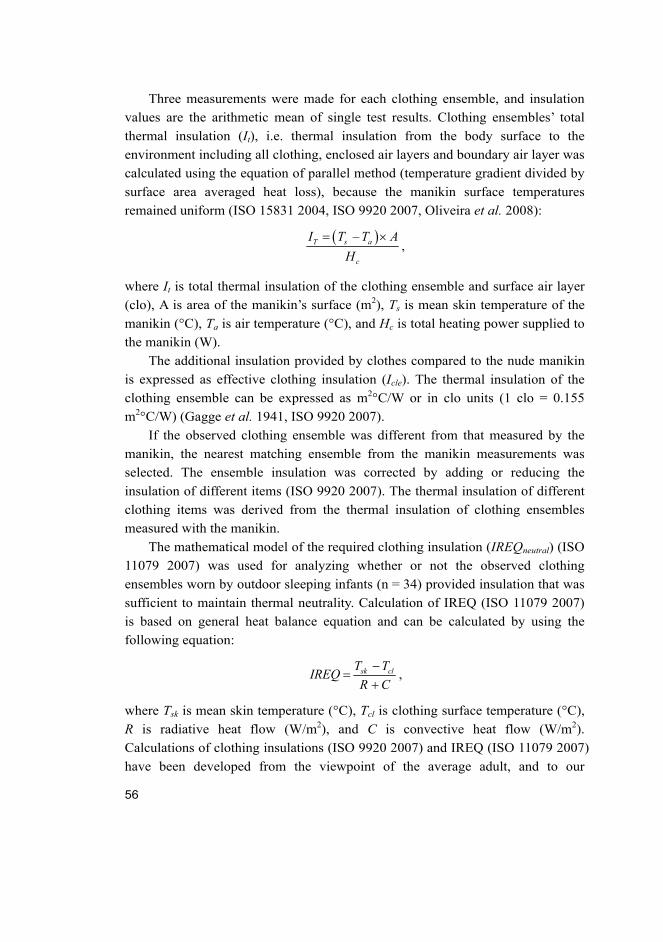
56
Three measurements were made for each clothing ensemble, and insulation
values are the arithmetic mean of single test results. Clothing ensembles’ total
thermal insulation (It), i.e. thermal insulation from the body surface to the
environment including all clothing, enclosed air layers and boundary air layer was
calculated using the equation of parallel method (temperature gradient divided by
surface area averaged heat loss), because the manikin surface temperatures
remained uniform (ISO 15831 2004, ISO 9920 2007, Oliveira et al. 2008):
–T s a
c
I T T A
H
,
where It is total thermal insulation of the clothing ensemble and surface air layer
(clo), A is area of the manikin’s surface (m2), Ts is mean skin temperature of the
manikin (°C), Ta is air temperature (°C), and Hc is total heating power supplied to
the manikin (W).
The additional insulation provided by clothes compared to the nude manikin
is expressed as effective clothing insulation (Icle). The thermal insulation of the
clothing ensemble can be expressed as m2°C/W or in clo units (1 clo = 0.155
m2°C/W) (Gagge et al. 1941, ISO 9920 2007).
If the observed clothing ensemble was different from that measured by the
manikin, the nearest matching ensemble from the manikin measurements was
selected. The ensemble insulation was corrected by adding or reducing the
insulation of different items (ISO 9920 2007). The thermal insulation of different
clothing items was derived from the thermal insulation of clothing ensembles
measured with the manikin.
The mathematical model of the required clothing insulation (IREQneutral) (ISO
11079 2007) was used for analyzing whether or not the observed clothing
ensembles worn by outdoor sleeping infants (n = 34) provided insulation that was
sufficient to maintain thermal neutrality. Calculation of IREQ (ISO 11079 2007)
is based on general heat balance equation and can be calculated by using the
following equation:
sk clT TIREQ
R C
,
where Tsk is mean skin temperature (°C), Tcl is clothing surface temperature (°C),
R is radiative heat flow (W/m2), and C is convective heat flow (W/m2).
Calculations of clothing insulations (ISO 9920 2007) and IREQ (ISO 11079 2007)
have been developed from the viewpoint of the average adult, and to our

57
knowledge this is the first time when calculation of IREQ is used for estimation
of thermal insulation of infants’ clothing ensembles together with a pram. The
large outer surface area reduced the insulation (ISO 9920 2007). The insulation of
the pram and its greater surface area has been taken into account by calculating
the total insulation (It) and the effective clothing insulation (Icle) by using thermal
manikin measurements, which includes the reduced insulation effect of the
surface area (ISO 9920 2007). This represented an about 0.5 clo decline in
insulation of clothing ensembles with pram. The basic insulation (Icl), where the
effect of the surface area has been taken away, was calculated.
Individual IREQ (Icl) values of each outdoor sleeping infant were defined by
using the values of mean outdoor air temperature and air velocity measured
during each sleeping situation. The metabolic rate of sleeping infants in
thermoneutral conditions was estimated to be 50 W/m2 based on earlier studies:
28–55 W/m2 (Arkell et al. 2007), mean (SD) 45 (10) W/m2 (Hull et al. 1996a,
Hull et al. 1996b), and 53–60 W/m2 (Rising et al. 2003). For the estimation of
sufficient clothing insulation in use the difference between observed clothing
insulation and IREQ [observed clothing insulation (clo) – required clothing
insulation (clo)] was calculated.
General IREQ was calculated by using air velocity of 0.4 m/s, which was the
mean value during the outdoor sleeping situations of infants (n = 34), and relative
humidity of 85%, which was the mean value in Northern Finland from November
to March (Finnish Meteorological Institute 2009).
SPSS version 16.0 for Windows (SPSS Inc., Chicago, IL, USA) was used in
statistical analysis. Infants slept for a shorter time indoors than outdoors (Studies I,
II), and for that reason the most stabile moment was selected when comparing
mean temperatures at the point of 60 min (T8–10) outdoors with mean temperatures
at the point of 30 min (T13) indoors by using Paired-samples t-test. Comparisons
between observed (clothing in use) and predicted (IREQ) insulations of clothing
ensembles were calculated by using Paired-samples t-test as well. The Spearman
correlation coefficient was used for calculating correlations. Relationships
between cooling rate of Tsk and the difference between observed and required
insulations as well as between outdoor air temperature and the difference between
observed and required insulation were predicted by using Linear regression. The
effect of exposure time for cooling was assessed by calculating mean difference
between central (T3) and peripheral (T7) skin temperature in the course of time.

58
4.4 Ethical considerations
There are ethical considerations at every stage of the research process, from the
choice of topic to publication (Parahoo 2006). The choice of the research topic of
children sleeping outdoors in winter was based on the findings of previous
research among adults that cold exposure causes adverse health effects on humans
(Näyhä 2000, Rytkönen et al. 2005) as well as on lack of information as to
whether infants are exposed to cold environment during outdoor sleeping.
Physiological measurements of infants were needed due to their different
thermoregulation, stage of development and smaller size compared to adults, and
observations in the natural settings were conducted to evaluate the risk of cold
exposure of outdoor sleeping infants.
Observing children who might be exposed to risks in their environment can
create ethical dilemmas for the researcher (Resnik & Wing 2007, Resnik & Zeldin
2008, Resnik 2009). Observational studies in daily environment are an
appropriate scientific method of determining exposures such as cold exposure in
this study, when purposeful exposures and increased risk is not involved
(Lebowitz et al. 2008). Infants would have faced the same risks even if they had
not participated in the study (Resnik 2009). The same lowest outdoor air
temperatures in which parents let their children sleep outdoors were seen in the
findings of the questionnaire study (Study I) as when the skin temperature
measurements were done in Study II. We also knew that allowing children to
sleep outdoors in the winter is a common childcare practice (Tourula et al. 2008).
However, if the well-being of the participants is found to be at risk during the
conduct of the observational study, it should be stopped (The International
Society for environmental Epidemiology 2009, Resnik 2009). Skin temperatures
were controlled while the infants were sleeping outdoors, and the limits of lowest
skin temperatures were determined beforehand. Once we advised taking the child
indoors before it woke up. If considerable evidence for risks can be found
according to earlier studies, participants should be informed about those risks
(Resnik & Wing 2007, Resnik 2009). The parents were informed that the
childcare practice of children sleeping outdoors in winter had not been studied
earlier and thus we did not know whether children were exposed to cold during
outdoor sleeping. We discussed with parents that according to studies among
adults, cooling was found to cause adverse health effects.
In order to ensure the reliability of the findings, the collection of the data of
physiologic measurements was continued after winter 2007 to winter 2008.

59
According to analysis after the first winter when skin temperature measurements
were conducted in 16 infants it was estimated that sample size and the minimum
necessary number of participants had to be increased. However, there should be
as few children as possible recruited to studies to attain reliable findings (ETENE
2003). The calculation of power analysis for sample size was not performed,
because skin temperature levels of infants during outdoor sleeping were not
available due to lack of earlier studies (see Scheinin 2001, Uhari & Nieminen
2001).
This study was estimated to provide benefit both to the participants and to the
same age group (ETENE 2003, Medical Research Act No. 488/1999). The curves
of skin temperatures of all 7 skin sites and preliminary analysis were given to the
parents of participating infants after measurements, and advice about clothing and
temperature limits was given if needed. The findings of this study can be utilized
when updating guidelines on infants’ of outdoor sleeping.
Responding to the questionnaire (Study I) was based on voluntariness and
informed consent, where assumption of implied consent was used, i.e. returning
the questionnaire reflected voluntary consent to participate (Polit & Beck 2010).
Written and verbal information was provided and informed consent obtained from
the parent of each infant by having participants sign a consent form stating
voluntariness and willingness to participate (Studies II–III) and from all
interviewed mothers (Study IV). The ethical procedure of the study was approved
by the Ethical Committee of the Northern Ostrobothnia Hospital District (84/2006)
and the study plan was approved by the postgraduate research committee at the
Faculty of Medicine, University of Oulu. In those cases where public health
nurses asked voluntary participants in child welfare clinics, approval was given
by the chief of the health care unit. The privacy of participants was maintained
through possibility to answer the questionnaire anonymously (Study I).
Permissions for tape recording during interviews (Study IV) were requested, and
the tapes were transcribed without the names of the participants. The data from
physiological measurement of infants were also analyzed and the findings
reported without names. All the data of Studies I–IV were treated in confidence.
No monetary incentive for participation was provided in studies I–IV. Possibility
to contact the researcher as well as to withdraw from the study at any time was
brought out to the participants. The principles of research ethics were taken into
consideration during the research processes (Academy of Finland 2008, World
Medical Association 2008).

60

61
5 Results
There is fluctuation in children’s sleeping episodes from day to day and between
different families. The outdoor sleeping childcare practice binds juggling acts on
the part of the family on different levels. In general, a fit was found between
family – cultural outdoor sleeping childcare practice – Northern Finnish winter
environment, constituting a coherent whole. However, balance was not found
during some sleep episode causing an increase in adverse effects.
Different points of view and results on every level are gathered in the
evaluation model of outdoor sleeping episode (Figure 5). Evaluation on each level
shifts the pointer of goodness of fit either to the direction of beneficial or adverse
effects.
Detailed results are presented from level to level, starting from the
description of the environment to the skin temperature of the infants.

62
Fig
. 5. T
he
eva
luati
on
mo
de
l o
f o
utd
oo
r s
lee
pin
g e
pis
od
e.

63
5.1 Winter environment in Northern Finland
The quality of the northern winter environment. Mothers described the northern
environment as consisting of four distinct seasons, with typical features of winter:
lots of snow and freezing temperatures when the coldness of the weather was
increased due to wind (Study IV). The outdoor sleeping children were exposed to
many kinds of environments, from sunshine to heavy snowfall in the winter. The
temperature limits for allowing the child to sleep outdoors varied quite a lot from
family to family, the coldest being about −30°C. (Studies I–IV.) The best
temperature was evaluated to be about −6°C (ranging from +7 to −15°C), and the
largest group of parents answered that −5°C was the best temperature for having a
child sleep outdoors (Study I). Mean air velocity was 0.4 m/s; air velocity ranged
instantly from 0 to 9 m/s during the skin temperature measurements and mean
velocity from 0 to 2.23 m/s (Study II). When staying indoors, infants slept in cots
or prams (Studies II, IV), the mean (SD) room ambient air temperature (Ta)
ranging from 17.7 to 24.8°C [mean (SD) 22.1 (1.5)°C] and outdoors from −25.9
to 2.2°C [mean (SD) −5.9 (5.9)°C]. During the measurements in Study II, the
mean temperature difference between Ta outdoors and indoors was 27.9°C (95%
CI: 25.7 to 30.0°C, p < 0.001); the maximum difference was 47°C. The mean
temperature difference (T11–T14) was slighter near the infants’ face outdoors and
indoors: 19.7°C (95% CI: 18.0 to 21.4°C, p < 0.001).
In winter the days were short and darkness came early. The winter
environment was described as providing an ideal and favourable setting for
children to sleep calmly, because it was sleepy, silent and peaceful and there was
fresh and clean nature and pure air. Especially rural surroundings were considered
ideal for sleeping outdoors, with only natural sounds being heard:
In the winter environment there are no disturbing sounds. There was only the
sound of footfall as dry snow creaked under the soles of my shoes. (Mother,
Study IV.)
On the contrary, the harsh and changeable weather posed challenges to families.
The greenhouse effect caused different, shorter, “strange” winters that came later
than normal. The northern city environment was also described as sometimes
noisy and the air polluted. (Study IV.)
The countryside in Northern Finland was described to be safe, but the social
context of the downtown was considered insecure – however, less so than in

64
southern Finland. In general, Finland was described to be safer than some other
countries. (Study IV.)
Dimensions of the northern winter experiences. The natural northern winter
environment was highly valued and mothers were satisfied with their living place
expressing that they were “a people of the north”. The northern life-style was
described as being close to nature and mothers wished that their children would
learn the same respectful attitude towards nature that they had, and their aim was
to make outdoor activities an enjoyable part of the life-style of their children
throughout their lives. The relationship between the child and the natural
environment got a start by sleeping outdoors, and this connection was gradually
reinforced through engaging in many kinds of outdoor activities in the expanding
milieu. The winter environment was seen as an affordance for the child to sleep
outdoors and produced many affordances for older siblings. Families with little
children spent much of their time outdoors playing and engaged in different kinds
of activities:
We have a one-family house and we have outbuildings there and a slide just
there in our own yard; we have built it up after the plough truck drove from
there. What we usually do when we go out, we dig snow with a spade,
because we dig a path to the sauna and warehouse. And then we make snow
cakes, glide and go to the grocery store by kick sled. It takes about 15
minutes when for example the younger child is in a baby sling and the older
is sitting on the kick sled or uses the kick sled herself. We walk a lot. (Mother,
Study IV.)
Negative attitudes were also mentioned when the winter environment was felt to
limit and make going outdoors cumbersome if a lot of snow had fallen. The cold
winter also meant higher costs to families; for example appropriate clothes and
prams cost a lot, putting a strain on families’ economic resources.
5.2 Cultural knowledge-building
Families have generated shared knowledge about children sleeping outdoors in
winter during some generations. Social knowledge building involved comparisons
between experiences and opinions with grandmothers, friends, other mothers, and
cultures as well. Practical details, temperature limits, duration of sleep, possible
correlations with outdoor sleeping and falling ill have been discussed. During
they walks mothers made observations on how other mothers managed and had

65
dressed their children. The mothers had noticed how differently people can see
the cold winter outdoor environment when they had been abroad or met families
who had moved to Finland. Place rules for behavior were different in different
cultures and the outdoor sleeping practice had caused wonder. For example a
mother from Brazil had said: “What on earth? People will freeze here!” while
Finnish woman who had moved to the USA had realized that no children slept
outdoors there. It was not easy to continue with outdoor sleeping childcare
practice then, for example due to lack of walkways and appropriate prams and
winter clothing. (Study IV.)
Culturally bound custom. Having children sleep outdoors is self-evident
(Studies I, IV) and common in the city of Oulu (95%) (Study I). Some of those
who did not take their child to sleep outdoors thought that this practice was of no
use and did not want to adopt it as a habit, or it was prevented by someone
smoking on the next balcony (Study I). Usually the mothers expressed that it was
natural to continue with the outdoor sleeping practice as it had been used by
earlier generations, e.g. one mother described how they had let their children
sleep outdoors at least during three generations since a Finnish pediatrician, Arvo
Ylppö, had recommended it. The mothers described old family photos showing
that having a baby sleep outdoors had been a moment worth taking a picture of in
those days. (Study IV.) Parents’ experiences were mainly positive (Study I) and
the interviewed mothers were going to recommend the outdoor sleeping childcare
practice to their children and friends as well (Study IV).
Outdoor sleeping as a norm. Guidelines, advice and encouragement about
having children sleep outdoors were given to mothers from different sources;
grandparents were the biggest group (39%) giving lots of advice, and a great
number of guidelines were also received from friends (33%) and from public
health nurses (28%) in child welfare clinics, which held an authoritative position,
especially from the point of view of first-time mothers. An important source of
support came from female family members and friends. Guidelines were also
found in books and magazines. (Studies I, IV.) Directions on how to dress the
baby were found in the Finnish maternity package as it contained a winter
clothing ensemble and sleeping bag. Some mothers were not able to mention a
single source from where they have received advice, as it had always been so
generally encouraged (Study IV); only 3% of parents had been advised not to take
the child out to sleep in the winter (Study I). The childcare practice of having
children sleep outdoors in the winter has gradually become a commonly accepted

66
collective, a type of behavior that is sometimes felt to be compulsory. The outdoor
sleeping childcare practice has been described as a myth (Study IV).
5.3 Family well-being
Outdoor sleeping episode as one building block of everyday life. Outdoor sleeping
usually took place once a day (52%) (range 3 times a month to twice a day)
(Study I). The episode consisted of three phases: preparing, getting to sleep and
waking up. Mothers fed their babies, looked for appropriate clothing, dressed
their babies carefully and laid them peacefully down in a pram. (Study IV.)
Infants usually slept in prams on the balcony, veranda or in the garden (Studies I–
IV). The babies who cried needed to be swayed to sleep and the mothers went for
a walk with them. The families did their outdoor activities while the babies took
their daytime naps. Sometimes the mothers stayed indoors with the rest of the
family while the baby was sleeping outdoors alone (Studies I–IV). Some children
woke up peacefully babbling, with some older children calling for mother from
the pram outdoors, whereas others cried (Study IV).
The mothers had “season babies”: winter babies had to wait about two weeks
until they were allowed to sleep outdoors, as opposed to spring babies who were
let to sleep outdoors at once (Study IV). Outdoor sleeping was usually
commenced when the child was two weeks old (range 3 days to 7 months) (Study
I). Some children expressed their wish to sleep outdoors, even saying it out loud,
telling the mother how the blankets should be placed. Babies learned to sleep
longer periods outdoors in prams so well that some mothers encountered
problems when they tried to have the babies sleep indoors, and the mothers had to
trick the babies into believing that they were outdoors by dressing them in
outdoor clothes and putting them in the pram. (Study IV.) The age of the child
when the outdoor sleeping practice was stopped varied between families (Studies
I, IV), the oldest children being about 3 years then (Study I). When the child grew
taller and the prams got too tight or the child started to move more in the pram
were reasons for ending the practice (Study IV).
Fluency of everyday life. Having children sleep outdoors was a daily routine
in the families creating rhythm for the day, and this way regularity and fluency of
everyday life was strengthened. Mothers also described how they needed to get
outdoors; they got a possibility to take care of their social relationships when
allowing the baby to sleep outdoors and go for a walk with the child, and at the
same time they improved their fitness and shed weight. It helped to combine

67
different outdoor activities of other members of the family as well. The outdoor
sleeping childcare practice was an important factor enhancing the family’s well-
being. (Study IV.)
Mother’s personal knowledge-building. Mothers built their personal
knowledge of outdoor sleeping as their experience increased. During pregnancy
they already intended to let their child sleep outdoors, as it represented one aspect
of healthy childcare and was fraught with big expectations, similarly to
breastfeeding. Especially young mothers followed guidelines and advice they had
received to the letter, as well as learning the practice through experience, by
trying and discovering their own ways of doing it. They were motivated to do
their best for their children and to fulfill their needs, striving to be good mothers.
Mothers were sometimes very resilient when trying to get their babies to sleep
outdoors every day by pushing prams in the snow while pulling a sibling in a
sledge and often also walking the family dog on a leash. There were experiences
of a sense of being forced to do outdoor activities against one’s own will. (Study
IV.)
Some of the mothers wanted to use their common sense and intuition and
make independent decisions, for example when estimating when it was too cold
for sleeping outdoors. They explained how they did not want to be given so much
advice and how the everyday life of the family was not planned so strictly in
advance. Doubts concerning the necessity of this practice also came up. (Study
IV.)
The gamut of feelings fluctuated from “nothing special” to “very emotional”
and from positive to negative. Confidence in own skills, fluency of everyday life,
and success in attaining goals were positive feelings evoked by the practice,
whereas negative feelings consisted of uncertainty of one’s own ability to take
care of the baby correctly. When the mother was not able to put her baby outdoors
to sleep for different reasons, feelings of failure and guilt were experienced as
they felt that they failed to attain the goals of healthy childcare. Feelings of being
“bad mothers” and lazy were experienced. From time to time mothers had to give
up after trying hard, and they were dissatisfied when their idea of the baby
sleeping peacefully outdoors did not come true. The outdoor sleeping practice
was sometimes quite exhausting and burdensome; the baby had to be dressed in
so many articles of clothing and the mothers feared for their babies’ safety and
were on the alert for the many risks that might occur during outdoor sleeping that
it would have been much easier if the baby had slept indoors. This part of the day

68
and stage of life was very busy, especially in families with many children, and the
mothers with children with sleeping problems had a hard time, getting very tired.
The relationship between the mother and the baby fluctuated from unity to
separate. Mutual feelings and identification with the child were experienced by
mothers; for example when the child slept well and everything was all right, the
mother was also satisfied and happy; likewise, when mothers felt invigorated
during a walk, they assumed it as having the same effect on the baby. Outdoor
sleeping was described as a shared good experience. The relationship was
separate when mothers left their babies to sleep alone in the pram outdoors while
being indoors themselves. On the other hand, the distance was not described to be
a problem, as the distance was shortened by placing the baby within sensory
distance. During this daily separation when the baby was sleeping outdoors,
mothers had a moment of their own; they had a change to do some housework or
take a brief respite, read, rest and have flow experiences. During this time the
baby’s siblings also got more attention from their mothers. (Study IV.)
Safety. Many parents (88%) had not encountered any potentially dangerous
situations related to sleeping a child outdoors (Study I); however, mothers were
conscious of potential risks and had to take notice of many security perspectives
(Study IV). Cold environment could cause general, facial or bronchial cooling or
cooling of the extremities as well as frostbites (Study IV), and clothing, such as
gloves and hat staying in place and generally appropriate clothing in view of
weather, was observed by the mothers (Study I). Some mothers connected cooling
with the common cold. On the other hand, sweatiness of the baby caused by
overdressing was a risk which was sometimes described as being more common.
The baby’s activity also caused dangerous situations, as one mother described
how her baby had fallen to the ground from the pram. An older child could have
climbed down from the pram and walked off somewhere. Mothers were conscious
of the possibilities of social problems, such as kidnapping. (Study IV.) Animals
(cats, small birds, squirrels, mice and rats) in the immediate vicinity were named
as a risk factor (Studies I, IV), and there was even a risk that the pram might be
knocked down by the family’s pony (Study IV). Problems with well-being
technology had been encountered, as in some situations baby monitoring had been
broken off while the child was sleeping outdoors (Studies I, IV).
Protection against risk factors. It was not always possible to let children
sleep outdoors due to many reasons related to the child, the mother or the
environment; child’s illness, such as fever (97%) or otitis (85%) was according to
most of the parents an obstacle to taking the child outdoors, but a mild sniffle

69
(36%) or cough (38%) was not (Studies I, IV). Mother’s lack of know-how was
named as one obstacle. Environmental preventive factors which prevented
sleeping outdoors were poor air quality, noise from the surroundings, and bad
weather conditions.
Security and the physical factors of the environment as well as practical
perspectives affected mothers’ choice of location for having their child sleep
outdoors. The wind and which way it was blowing and where the sun was shining
were observed by the mothers, trying to find a sheltered, peaceful spot. Children
usually slept under windows, in the same familiar and constant prams, but if it
was difficult to get somewhere by using prams, also in sledges and wheelbarrows.
One mother told how their baby was laid in a basket hanging from the branch of a
spruce. (Study IV.)
The outdoor sleeping practice required more frequent observing than indoor
sleeping. When mothers were indoors they watched the prams through the
window and usually also used baby monitors. Mothers went outside to check that
everything was fine every 15 minutes (58%) or every half an hour (40%) in those
families who used a baby monitors. The sleeping child was frequently observed;
the frequency of going outside to observe the sleeping child was reduced by using
a baby-monitor. The child’s breathing, babble, moving and the amount and quality
of sleep were noted. The child’s temperature was evaluated by touching the
child’s skin from the neck or using a thermometer inside the pram. During the
child’s sleep also wind, the direction of the wind, rain, sunshine, changes in
weather and the climate as a whole were kept watched by the parents. (Study I,
IV.)
Mothers protected the children against harmful effects; first of all came cold
protection and using layered winter clothing (Studies I–IV).
5.4 Winter clothing of outdoor sleeping children
Mothers learned to know their babies, all of whom were unique individuals,
noticing how some children needed more clothes than others, for example one
child with Down’s syndrome reacted differently to cold. An attempt was made to
regulate the amount and quality of babies’ clothing ensembles and coverings
according to weather conditions. This was easy in the fall and spring, but became
challenging and difficult in the variable weather conditions in the wintertime
(Study IV), as was confirmed when clothing insulations in use (n = 34) were not
found to correlate with ambient air temperature (see Figure 1 in Publication III).

70
On the contrary, according to questionnaire (Study I), clothing insulation was
seen to be higher in colder conditions, and some mothers described that they had
a special clothing solution when it was colder than −20°C. Mothers took into
account the effect of the wind by adding extra covers on the pram, and some
mothers also limited the duration of the child’s sleeping time in cold weather.
(Study IV.)
The children were clad in layered clothing (Studies I–IV). Outdoor sleeping
infants’ (n = 34) mean (SD) clothing insulation (Icle) was estimated to be 5.54
(0.52) clo (range 4.35 to 6.47 clo) (Study III). Clothes and beddings did not vary
much indoors, where infants were usually clad in a bodysuit, disposable nappy,
footed leggings (sometimes tights, or leggings with socks or a romper suit) and
covers (blanket and duvet cover or sleeping bag). The same kind of underwear
was worn with the outdoor clothing ensembles. The middle layer had greater
variability in amount and quality, sometimes consisting of handmade woolens.
(Studies I, III.) According to the interviews, grandmothers knitted woolens for
their grandchildren and underwent the process of becoming grandmothers.
Clothing tradition was passed on from earlier generations and at the same time,
giving handmade pieces of clothing was a positive sign for outdoor sleeping.
(Study IV.) The middle layer also consisted of a balaclava hat, socks (usually
woolen, handmade), mittens (cotton or woolen), shirt and pants / overall (cotton,
fleece or woolen). Outer garments consisted of a hat, snowsuit with hood and
insulated mittens and booties. Sleeping bags were usually those included in the
maternity package (62%), but sometimes a thicker padded winter footmuff was
used. Some infants slept on a sheepskin. In nearly all cases (82%) the hood of the
pram was covered with gauze, net or cloth when using different kinds of pram
models. (Study III.)
Layered clothes, sleeping bags, other covers and the pram formed something
like swaddling clothes, restraining infants’ movements. When infants took their
daytime naps indoors, they slept under a blanket in cots or prams. The outdoor
used clothing ensembles’ (see Appendix 1, measurement no. 6–9) total thermal
insulation (It) with the pram ranged from 5.67 to 8.07 clo. The pram increased the
insulation of the clothed manikin by 1.44 clo / 0.22 m2°CW−1. The thermal
insulation of the clothing ensemble was divided so that underwear accounted for
10%, middle layer for 16%, outerwear for 35%, covers for 13% and the pram for
26% of the insulation. (Study III.)
The cold ambient air temperature came in close contact with the outdoor
sleeping child. When the child had slept outdoors for 60 min the mean
71
temperature inside the middle layer was 1.6°C (95% CI: 0.4 to 2.9°C, p = 0.014)
warmer than inside the blankets when the child had slept indoors for 30 min,
whereas the mean temperature inside the snowsuit was 3.5°C (95% CI: 5.6 to
1.5°C, p = 0.002) colder and mean temperature inside the sleeping bag 18.2°C
(95% CI: 20.3 to 16.2°C, p < 0.001) colder outdoors than indoors inside the
blankets. The temperature inside the middle layer decreased when cold ambient
air temperature cooled it down (rs = 0.442, p = 0.011), which led to a decrease
(rs = 0.533, p = 0.002) in Tsk. The observed and required thermal insulation of
clothing was equal at about −5°C. An increased difference between observed and
required clothing insulation was found when Ta decreased below −5°C, meaning
that the deficit of clothing insulation increased in colder ambient air temperatures.
On the contrary, overdressing existed when Ta was higher than −5°C (rs = 0.739,
p < 0.001, see Figure 2, Publication III), supporting hypothesis number 3a. When
the difference between observed and required clothing insulation increased the
cooling rate of Tsk increased linearly (rs = 0.605, p < 0.001, see Figure 3,
Publication III), supporting hypothesis number 3b. When the difference between
observed and required clothing insulation increased the infants also slept for a
shorter time (rs = 0.524, p = 0.001).
IREQ calculation (ISO 11079, 2007) shows the required clothing insulation
in different ambient air temperatures when infant’s metabolic rate is 50 W/m2
during sleep (Figure 6).
Fig. 6. IREQ-values have been calculated by using air velocity of 0.4 m/s, which was
the mean value during the outdoor sleeping of infants (n = 34). Relative humidity of 85%
was used as it represented the mean value in Northern Finland from November to
March (FMI 2009).
0
1
2
3
4
5
6
7
8
9
10
11
-34 -32 -30 -28 -26 -24 -22 -20 -18 -16 -14 -12 -10 -8 -6 -4 -2 0 2
IRE
Q (
clo)
Temperature (°C)

72
When the insulation is less than IREQneutral the infant cannot maintain thermal
equilibrium without limiting outdoor sleeping time (ISO 11079 2007). For
example, when the infant is dressed in a clothing ensemble with about 5clo
insulation and laid in pram, the infant is allowed to sleep at −1°C outdoors
without time limits from the viewpoint of thermal equilibrium, but is also allowed
to stay outdoors when it is colder than −1°C for a shorter time. Maximum amount
of clothes gave appropriate insulation in ambient temperature of about −17°C
(Table 3.)
Table 4. Examples of required clothing ensembles in different temperatures
(Clo/m2°CW−1, °C).
Clothing ensembles Icle
Clo/m2°CW−1
Temperature limits
(°C)
Bodysuit, disposable nappy, footed leggings, mittens, socks,
balaclava hat, woolen hat, snowsuit, sleeping bag, pram
5.01/0.78 −1
Bodysuit, disposable nappy, footed leggings, playsuit, mittens,
socks, overall with wadding, balaclava hat, insulated mittens,
insulated booties, insulated hat, snowsuit, sleeping bag, pram
5.40/0.84 −4
Bodysuit, disposable nappy, footed leggings, mittens, woolen
socks, woolen cardigan and pants, balaclava hat, insulated
booties, woolen hat, snowsuit, sleeping bag, pram
5.60/0.87 −5
*Bodysuit, disposable nappy, footed leggings, mittens, woolen
socks, woolen cardigan and pants, balaclava hat, insulated
booties, woolen hat, snowsuit, padded winter footmuff,
sheepskin, pram
6.44/1.00 −10
*Bodysuit, disposable nappy, footed leggings, mittens, woolen
socks, playsuit (shirt and pants), woolen cardigan and pants,
balaclava hat, insulated booties, woolen hat, snowsuit, padded
winter footmuff, sheepskin, pram
6.86/1.07 −13
Bodysuit, disposable nappy, footed leggings, mittens, socks,
woolen socks, woolen mittens, playsuit (shirt and pants),
woolen cardigan and pants, overall with wadding, balaclava hat,
insulated booties, insulated mittens, insulated hat, snowsuit,
padded winter footmuff, sheepskin, pram
7.41/1.15 −17
* The thermal insulation of clothing ensemble is derived from the thermal manikin measurements, but not
measured directly by using the thermal manikin.

73
The average humidity (RH%) between clothing layers was 35.3% (range 22.6 to
64.5%) during outdoor sleeping, whereas during indoor sleeping it was 32.6%
(range 21.0 to 62.9%). Humidity was on average 40% at sleep onset, and
individual variations were found in the humidity trends; in general there was a
decreasing trend, but in some cases (n = 4) humidity increased during outdoor
sleeping. There was a clear association with maximum Tsk and humidity
(rs = 0.747, p ≤ 0.001) during outdoor sleeping, but this was not found indoors
(rs = 0.107, p = 0.619). Mean humidity was > 30 RH% when mean Tsk
was > 32.5°C (Figure 7). The biggest correlation was seen between mean
temperature of cheek and humidity (rs = 0.587, p = 0.002) when different skin
sites and humidity were compared. Mean humidity correlated with the
temperature of middle layer (rs = 0.471, p = 0.023), whereas correlation was not
noticed with clothing insulations (rs = 0.088, p = 0.677) or outdoor temperature
(rs = 0.102, p = 0.627).
Fig. 7. The correlation between mean relative humidity (RH%) and mean Tsk.
30 31 32 33 34 35
20
30
40
50
60
70
RH
%
Tsk (°C)
rs = 0.566
p = 0.003

74
5.5 Well-being of the children
Mothers described the surroundings of their child sleeping outdoors in the pram to
be a closed and safe nest with limited stimuli. Babies were bundled up and the
prams were veiled so that they could not see anything but the pattern on the hood
of the pram. The microclimate temperature and the motion when the wind rippled
the pram or the mother moved it created haptic stimulations to the child. At the
same time, the movements of the child were restricted by clothing and sleeping
bags as if they were swaddled. (Study IV.)
It was thought to be important for the child’s development to be outdoors in
nature. The children’s environmental health consisted of the beneficial health
effects of cool, fresh, humid and clean air as well as the sun shining in the later
stages of winter. (Study IV.) Some parents (29%) and interviewed mothers saw
outdoor sleeping as toughening the child to the harsh climate (Studies I, IV), and
fresh air was thought by most of the parents (94%) to be healthy for the outdoor
sleeping child. The better quality of sleep and being outdoors was thought to
enhance the child’s appetite (Studies I, IV), as well as growth and learning, and
have effects on mental development and better mood (Study IV). According to
parents (66%), children were more active after outdoor sleeping. Parents (88%)
evaluated that the child clearly enjoyed sleeping outdoors. (Study I.) The baby’s
mental security was promoted by foreseeable and familiar routines and regular
rhythm of everyday life. Some interviewed mothers had experiences of children
having fewer infections and illnesses when they had slept outdoors (Study IV);
however, most parents (65%) were not able to say whether their child might
remain healthier because of outdoor sleeping (Study I). The interviewed mothers
had a strong belief that outdoor sleeping promoted health of the baby; it was one
part of the wholeness of a healthy way of life, and the good of the child was the
basis for this childcare practice (Study IV).
5.5.1 Children’s sleep
Infants usually slept in a supine position both outdoors (74%) and indoors (55%).
Prone sleeping did not exist. (Study II.) The mothers had noticed that sleeping
outdoors improved the quality of sleep of their child, making it fall asleep quickly
and sleep soundly and longer, without interruptions (Study IV). Children took
significantly longer naps outdoors compared with naps taken indoors according to
both the questionnaire study (mean difference 34 min, 95% CI: 21–47 min,

75
p < 0.001) (Study I) and the observational study (mean difference 92 min, 95% CI:
74–110 min, p < 0.001) (Study II) supporting hypothesis number 2a (Figure 8).
Fig. 8. Outdoor sleeping durations in Study I (n = 106) and in Study II (n = 33).
The longer the baby slept indoors the longer he/she also slept outdoors (rs = 0.405,
p = 0.019) (Study II). The number of children in the families had an effect on the
difference in sleeping durations; according to the questionnaire, most of the
children (57%) in the group that slept longer outdoors had siblings, while most of
the children (74%) in the group that slept longer indoors were the family’s only
child (p = 0.05). Children slept longer outdoors than indoors in all types of
housing (p = 0.004). (Study I.) No significant differences between outdoor sleep
durations were found, whether the mothers went for a walk or not (p = 0.297)
(Study II).
Some external factors, such as noise from the surroundings or physiological
factors of the child, e.g. sweatiness or coldness were described as causing

76
awakening. Long duration of sleep was a sign of thermoneutrality, while shorter
and discontinuous sleep indicated coldness, according to some interviewed
mothers (Study IV):
If they felt cold, they woke up. Of course this could sometimes happen.
(Mother, Study IV.)
This was also noticed in the skin temperature measurements as infants reacted to
the increased cooling rate of Tsk by waking up; the cooling rate of Tsk had a
significant correlation with outdoor sleeping duration (rs = 0.611, p < 0.001) (See
Figure 3, Publication II). Infants were especially sensitive even to a slow cooling
rate of the chest (Figure 9). A slight correlation (rs = 0.352, p = 0.041) could be
seen between outdoor ambient air temperature and sleeping duration, but no
correlation (rs = −0.168, p = 0.351) was found between room temperature and
duration of sleep. (Study II.)
Fig. 9. The correlation between the cooling rate of chest (°C/min) and outdoor
sleeping duration (min).
50
100
150
200
250
300
Out
door
sle
epin
g du
rati
on (
min
)
Cooling rate of chest (°C/min)
rs = 0.658
p < 0.001
-0.020 -0.015 -0.010 -0.005 0.000 0.005

77
5.5.2 Children’s skin temperatures
Mean Tsk of all measurements in Study II decreased during outdoor sleeping and
increased during indoor sleeping. At the beginning of the recordings, higher level
in mean Tsk was seen outdoors compared to indoors due to clothing. (See Figure 2,
Publication II.) Tsk was significantly lower at the end of outdoor sleep compared
with indoor sleep (mean difference 1.23°C, 95% CI: 0.72–1.74, p < 0.001). The
mean difference of the rate of change of Tsk between outdoors and indoors was
0.025°C/min (95% CI: 0.018 to 0.033°C/min, p < 0.001) (Figure 10). During
outdoor sleeping the mean cooling rate varied at different skin sites, being fastest
in the cheek (−0.049°C/min) and slowest in the chest (−0.007°C/min). In the
extremities, the cooling rate was highest in the distal parts (−0.02°C/min). (Study
II.)
Fig. 10. The rate of change (°C/min) of Tsk indoors and outdoors.
Outdoor ambient air temperature had a clear effect on the cooling rate of Tsk
(rs = 0.628, p < 0.001) (See Figure 1, Publication II). Moreover, the difference

78
between outdoor air temperature and temperature near the infants’ face (T11)
decreased with increasing air velocity, (rs = −0.491, p = 0.004). At the same time,
the T11 affected the mean temperature of the cheek (rs = 0.524, p = 0.001). Air
velocity also slightly affected the cooling rate of the dorsal foot (rs = 0.384,
p = 0.028).
Skin temperatures of all measured sites were lower at the end of outdoor
sleep compared with indoor sleep, being significantly lower in the cheek (mean
difference 8.54°C, 95% CI: 6.73–10.36°C, p < 0.001), lower arm (mean
difference 1.46°C, 95% CI: 0.67–2.25°C, p = 0.001), back of the hand (mean
difference 2.12°C, 95% CI: 0.89–3.35°C, p = 0.001), shin (mean difference
0.79°C, 95% CI: 0.22–1.37°C, p = 0.009), and dorsal foot (mean difference
2.57°C, 95% CI: 1.41–3.73, p < 0.001), supporting in this respect hypothesis
number 2b. (Study II.)
According to the subjective reports of the parents in the questionnaire study,
children had cold fingers in 3% of the cases at 0°C and 25% at −15°C or colder,
but cold toes were observed less frequently, in 3% and 16% of the cases,
respectively (Study I). Frequencies of cool hands were recorded after outdoor
sleeping in Study II: 9% had cool (27.0–27.6°C) and another 9% had cold (21.4–
22.7°C) hands. Cool (26.3–28.9°C) feet were recorded in 15% and cold (21.2–
23.7°C) feet in 9% of the infants. The coldest area was the cheek with 47 % of the
infants having cool (20.1–24.8°C) and 18% cold (12.2–18.4°C) cheeks. (Study II.)
A white area on the cheek was uncommon; it was seen in none at 0°C and in 4%
at −15°C or colder (Study I). Frostbite of cheek came up in the interviews with
the mothers:
Once my own child got a frostbite on his cheek when the weather was frosty.
He had moved in the pram so that his cheek was exposed and dribble-soaked.
The cheek was frostbitten in a small area; it was a kind of bluish area in the
cheek that lasted the whole winter. (Mother, Study IV.)
Frostbites of other parts of the body or hypothermia did not come up in any data
in this study.
Increased differences between chest and peripheral (dorsal foot) skin
temperatures were seen at the end of outdoor sleep, suggesting the effect of
vasoconstriction. The mean (SD) temperature difference between chest and dorsal
foot was 3.7 (3.2), ranging from −0.3 to 12.4°C. Smaller differences were seen
between the lower arm and back of the hand and between the shin and dorsal foot.
The colder the outdoor air temperature, the bigger the maximal differences

79
between the lower arm and back of the hand (rs = −0.454, p = 0.007) as well as
between the shin and dorsal foot (rs = −0.387, p = 0.024). Differences were found
in skin temperatures’ cooling between different skin sites: the mean (SD)
difference of cooling between the lower arm and back of the hand was −0.9
(2.0)°C (95% CI: −1.6 to −0.2°C, p = 0.012), between the shin and dorsal foot
−1.8 (2.0)°C (95% CI: −2.5 to −1.1°C, p < 0.001), and between the chest and
dorsal foot −1.8 (2.5)°C (95% CI: −2.7 to −0.9°C, p < 0.001). (Study II.) The
mean difference between central and peripheral skin temperature exceeded the
start difference (2°C) when infants (n = 10) had been outdoors about 200 min or
longer (Figure 11).
Fig. 11. Central-peripheral temperature difference (Td) over the course of time. All
results for subjects were summarized in composite graphs. Sample size decreases
over the course of time.
-2
-1
0
1
2
3
4
5
6
7
8
9
0 30 60 90 120 150 180 210 240 270 300
Skin
tem
pera
ture
diff
eren
ces
(°C
)
Time (min)
lower arm - back of the hand
shin - dorsal foot
chest - dorsal foot

80
On the other hand, also sweatiness of the children was observed during outdoor
sleeping. According to the questionnaire study, almost half of the children had
sweaty necks at 0°C, with decreasing prevalence in colder temperatures (Study I),
and according to Study II, 32% of the infants were estimated to be warm or
sweaty, compared to none after indoor sleeping.

81
6 Discussion
The use of mixed methods approach elicited new, different and complementary
findings between qualitative and quantitative methods. The qualitative part of this
study contributed to connecting the findings of physiological measurements to the
broader context, with all parts and levels of the study constituting a
comprehensive view. For example, if only skin temperature measurements had
been done, the emphasis would have been more on the negative effects, ignoring
the promotion of family well-being. A combination of quantitative and qualitative
research provides a better understanding of the research problem than either
approach by itself (Creswell 2005). On the other hand, if only one level of the
phenomenon had been studied, there would have been a possibility to study it
more profoundly. The quality of mixed methods research could be considered by
examining whether the chosen methods are correct in terms of providing answers
to the research questions, whether different parts of the study are implemented
and data analyzed appropriately as well as how smoothly different parts are
connected to the whole (Tashakkori & Teddlie 2008).
The similarities in the qualitative and quantitative parts helped to confirm the
data. For example, parents estimated that their child slept longer outdoors than
indoors and reacted to the cold by waking up earlier (Study I, IV), findings which
were confirmed in the observational study (Study II). Parents also evaluated in the
questionnaire study (Study I) that the best temperature for letting their child sleep
outdoors was about −5°C, which was confirmed by the clothing insulation study
(Study III), showing that parents usually clothed their child appropriately at about
−5°C; the maternity package also gave insulation at −5°C. The mixed methods
approach strengthens the validity of findings by obtaining similar results via each
of the methods employed (Greene 2005).
In the contemplation of the rigor of the study both factors related to
quantitative (validity, reliability) and qualitative study (credibility, dependability,
confirmability and transferability) should be taken into account (Tashakkori &
Teddlie 2008).
6.1 Validity and reliability of the quantitative studies
Validity refers to the degree to which inferences are accurate and well-founded as
well as the degree to which an instrument measures what it is intended to measure.
Content validity concerns the degree to which the items in an instrument

82
adequately represent the completeness of the content of the concept being
measured. (Polit & Beck 2010.) Content validity was taken into account when the
questionnaire (Study I) aimed to provide a comprehensive view of children
sleeping outdoors in winter was compiled by first interviewing mothers and then
using a panel of experts and pilot test. However, the larger interview study (Study
IV) and skin temperature (Study II) and clothing insulation (Study III)
measurements showed that the questionnaire could be more comprehensive and
thus needs to be improved for additional researches.
In Study II, the validity of measurements of Tsk was increased when Tsk was
measured at seven skin sites instead of two, such as the cheek and abdomen, as is
usually the case (Telliez et al. 1997, Bach et al. 2000a, Bach et al. 2001, Telliez et
al. 2004). Core temperature measurements could have provided more specific
information about thermoneutrality, but they would have reduced volunteers’
willingness to participate in the study (Baddock et al. 2004), and above all the
possibility of risk for adverse effects to the infants could have increased.
Actigraphic sleep measures, which have been considered a reliable and
accurate data collection method in children, could have been used for the data
collection of infants’ sleep durations (Tikotzky & Sadeh 2001, Asaka & Takada
2011). However, when actigraphy and parental daily sleep logs have been
compared, similar data for sleep duration have been obtained (Sadeh 1996,
Tikotzky & Sadeh 2001), and an attempt was made to make the measurements in
Study II as non-invasive as possible. A limitation of the study is that an
observational design was used in natural settings instead of an experimental
design with more constant conditions; furthermore, more detailed study of sleep
stages and total diurnal sleep duration was missing. At the same time, data
collections in natural settings strengthen the study, because the sleeping
environment of the infants was familiar and did not cause any additional stimulus.
Before the use of the probes and data loggers in Study II, accuracy was tested
by placing the probes in water at known temperature. The system of using
equipment was tested in one child before primary measurements. These kinds of
probes and data loggers have been used for a long time for the purpose of
measuring thermal conditions of the human body and there have not been any
validity problems. Physiological measurements are objective, relatively accurate
and precise, providing valid measures of targeted variables (Polit & Beck 2010).
Selection bias may pose a threat to internal validity (Polit & Beck 2010).
Nonprobability sampling was used in quantitative studies (Studies I – III). This
increases the possibility of sampling bias (Polit & Beck 2010). An attempt was

83
made to evaluate the possibility of bias by using nonresponding analysis in Study
I. It gave the assumption that there was no essential bias. In Study II, the lack of
nonprobability sampling might have caused a bias in which a disproportional
amount of families taking good care of their babies and infants without sleep
problems took part. Those mothers whose infants were used to sleeping outdoors
for a long time might have chosen to participate. This can be seen when looking
at the findings on sleeping duration (Figure 6), as much longer outdoor sleeping
durations where seen in the Study II than in Study I. On the other hand, infants
were about three month of age in Study II and under two years of age in Study I
causing different daytime sleep durations because of the decrease in the duration
of daytime sleep with increasing age (Iglowstein et al. 2003, Sadeh 2004).
In quantitative studies, an attempt is made by researchers to control
potentially confounding variables. Study participants’ characteristics could form
extraneous variables which are important to control. (Polit & Beck 2010.) The
crossover design used in Study II added validity when infants served as their own
controls and thereby controlled all confounding characteristics. It was not
possible to randomly assign infants to different order of treatments (outdoor and
indoor sleeping), which decreased the power of the crossover design. It is possible
that the ”first night effect” influences behavioral and physiological recordings
(Agnew et al. 1966), as the second condition is influenced by experiences in the
first (Polit & Beck 2010), but no carryover effect was found between outdoor
sleep duration and treatment order in the study, in line with other recent
publications (Kronholm et al. 1987, Katz et al. 2002).
Although the sample size was quite small in Studies I–III, it provided
significant correlational findings on some variables. Statistical conclusion validity
concerns the extent to which the conclusions about relationships and differences
drawn from statistical analyses reflect reality. There is a greater risk of a Type II
error with small samples, which can lead to the false conclusion that there are no
differences between the groups, even though the groups are different in reality.
(Burns et al. 2011.) It should be noticed that the correlations in Studies II and III
do not imply causality, even if relationships between variables were strong (Polit
& Beck 2010, Burns et al. 2011). The relationships in correlational research are
the means for generating hypotheses to guide experimental studies for examining
cause-and-effect relationships (Burns et al. 2011).
External validity concerns the degree of generalizability of the results (Polit
& Beck 2010). With caution, the findings of Study I are generalized to concern all
children under two years of age and the findings of Study II and III all children

84
about three months of age who sleep outdoors in the winter. Because of the
possibility of selection bias, i.e. that only those families who had higher well-
being and who had children with no sleeping problems participated in Study II,
the results are generalized at least to such families. The results of the
questionnaire study showed that almost all parents (91%) thought that they were
happy to have their child sleep outdoors. The proportion of families with good
experiences about children sleeping outdoors in winter is thus high, increasing
external validity. Study II was performed in natural settings, which increases the
generalizability of the findings to everyday lives of the families. If tight control
aimed to maximize internal validity would have been exercised in the study, the
setting could have become too artificial to be generalized into a more naturalistic
environment (Polit & Beck 2010).
Reliability means the consistency of the measurement method (Burns et al.
2011). Internal consistency of the questionnaire (Study I) was evaluated by
calculating Cronbach’s alpha, the results of which ranged between 0.6 and 0.81.
As reliability of 0.80 is usually considered to show a strong coefficient for a scale
(Burns et al. 2011), some parts of the questionnaire are reliable, while some parts
still need restructuring. The degree of error and bias in temperature readings is
low. The tests can be repeated by other researchers and the results should be the
same. Therefore they are verifiable and replicable.
The reliability in structure observations refers to the consistency of how
strictly observations and records could be performed in the same way each time
they take place (Parahoo 2006). All observations were done by the same
researcher with several years of experience in pediatric nursing. Also infants’
mothers were present, observing and evaluating the falling asleep and awakenings
of their infants.
The use of a thermal manikin for measuring heat loss is relevant, reliable and
accurate, and the method is quick, easily standardized and repeatable. Thermal
manikins have been used for research purposes for more than 60 years. (Holmer
2004.) Manikin measurements have produced good reproducibility and agreement
with clothing trials (Anttonen et al. 2004, Meinander et al. 2004). However, the
manikin had a simple shape without toes, fingers, eyes, mouth, ears and nose, all
of which would increase the heat transfer. Only measurements on human subjects
in natural settings and actual conditions of movements and wind would directly
provide correct insulation results (Havenith 1999). Thermal insulation of specific
bedding will vary according to its arrangement over the baby; whether the covers
are loosely draped over the body or tucked in tightly (Kerslake 1991). To ensure

85
the reliability of the clothing insulation study, three measurements were made for
each clothing ensemble, and the results given in this study are the arithmetic mean
of single test results. The coefficient of variation (CV) of clothing ensembles’
insulation (It) was less than 7%. Replications should be within 10% of the mean
value of the three measurements (ISO 9920 2007).
6.2 Trustworthiness of the qualitative study
Trustworthiness of Study IV was discussed through credibility, dependability,
confirmability and transferability, which are the criteria developed for the
evaluation of qualitative research (Lincoln & Guba 1985).
Credibility means confidence in the truth of the data and their interpretations
(Polit & Beck 2010). Finnish mothers who had varying amounts of experience
about children sleeping outdoors in winter were recruited from a large geographic
area. Sometimes it was hard for a researcher who is also a mother of children who
sleep outdoors to see something that was obvious because cultural thinking
shapes our interpretations (Connolly et al. 2006). On the other hand, having
similar experiences made it easier to understand the phenomenon more deeply.
The researcher familiarized herself more closely with the study phenomenon
during the observational study and skin temperature measurements, which helped
to formulating research questions and with analysis. The same researcher
conducted and analyzed all interviews. During the development of categories
looking forwards towards the overall results of the analysis as well as looking
backwards towards the data was needed. It was not possible to have a holistic
view just somehow simply emerge from an accumulation of detailed
categorization. (Dey 1993.) Two participants in the interviews performed
member-checking for increased credibility (Lincoln & Cuba 1985). The contents
of the generic and main categories were agreed by participants; only some sub-
categories were combined.
Dependability concerns the stability of data over time and over conditions
(Polit & Beck 2010). Three pilot interviews were conducted to test the research
questions. Similar question areas, but sometimes in different order, were used
with all the participants, and supportive questions were used to help the mothers
describe their perceptions. The analysis process was discussed and agreed with
the co-authors of Study IV.
Confirmability is concerned with the objectivity and neutrality of the data, so
that the findings reflect the participants’ voice and conditions of the inquiry (Polit

86
& Beck 2010). Mothers’ original expressions were used in reporting. The
limitation in confirmability is that the mothers used local dialects, and the rich
nuances of the expressions they used were lost when they were translated into
English. Confirmability was also confirmed by two participants’ member
checking and agreement on the information provided by the participants.
Transferability deals with the extent to which the findings from the data can
be transferred to other settings or groups (Polit & Beck 2010). The context,
inclusion criteria and participants’ characteristics have been described as clearly
as possible (Polit & Beck 2010). The findings can be transferred to families with
outdoor sleeping children in a northern winter environment.
6.3 Discussion of the results
6.3.1 Winter environment in Northern Finland
The winter environment in Northern Finland was highly valued, and parents
wished that their children would also adopt a life-style that was close to nature. A
strong northern place-identity was formed, which emerged when mothers
described their dimensions of northern winter experiences. Mother’s
‘environmental past’ (Proshansky et al. 1983) had an effect on how they
experienced the cold environment, what their place-identity was like and how the
harsh environment also created psychological well-being and health (Korpela
2002). This respectful attitude towards nature partly affected the experiences of
some mothers in that winter environment was seen as a positive affordance, as
described by Gibson (1986), and as an ideal setting for children to sleep although
the weather was harsh and changeable and it was dark in the winter.
Fresh air was thought to be healthy for the child and one of the main reasons
for letting the child sleep outdoors in the winter. Already Florence Nightingale’s
first rule of nursing was: “to keep the air he breathes as pure as the external air,
without chilling him” (p. 34) and she emphasized that “the main want of baby is
always to have fresh air” (Nightingale & McDonald 2001: 148). However, during
the winter temperature inversions may play a major role in air quality when
pollutants are trapped near the ground, leading to poor air quality (National
weather service forecast office 2011). The air of northern city environment was
sometimes observed by mothers to be polluted, and this viewpoint highlights the

87
question of the healthfulness of outdoor sleeping during frosty weather with calm
winds.
The temperature of infants’ outdoor and indoor daytime sleeping environment
and the weather outdoors varied markedly in Northern Finland during the winter.
Point of comparisons between other cultures with ambient air temperatures
outdoors during the infants sleep was not found. The measured room temperatures
in which study infants slept were higher during daytime sleep than those
measured in Britain in the winter (Wailoo et al. 1989b) and during the nights in
New Zealand (Baddock et al. 2004). The temperature difference between outdoor
and indoor ambient air can be 50°C in Finland posing challenges to the families
for offering appropriate sleeping arrangements to their child and require
knowledge and experiences to manage.
The interviewed mothers in this study described how greenhouse effects had
caused different shorter winters with warmer weather. This could cause
decreasing experiences of cold weather events and how to protect from cold.
Climate change affects all people (Guidotti & Gitterman 2007), but still there is a
lack of empiric data on the specific effects of climate change on children
(Bunyavanich et al. 2003). Weather conditions such as storms, heat waves and
cold snaps, create increasing challenges and responsibility for protecting children
(Guidotti & Gitterman 2007, Pronczuk & Surdu 2008). In the news, there was
reported for example that in Peru, at least 46 children died during one of the
coldest spells in 30 years in 2004 (BBC NEWS 2004) and in Chile, the coldest
July since 1908 was in 2010 (MercoPress 2010a) causing increase of respiratory
problems in children (MercoPress 2010b). Knowledge of cold protection of
children is a current topic despite global warming and even because of it
highlighting the importance of sharing “snow-how” globally.
6.3.2 Cultural knowledge-building
The premise of the childcare practice of children sleeping outdoors in winter is
nowadays generally in accordance with the earlier premise introduced by
pediatricians such as Arvo Ylppö since the 1920s. It has always been considered a
practice that promotes children’s well-being, although the aims have shifted from
the prevention of diseases, such as rickets, to the promotion of health and
comprehensive well-being of children and families. The reasons behind and
meanings assigned to particular practices can change over time as culture is
historically produced through interaction with changing economic, social, and

88
political factors. Infant care practices can differ between cultures and yet be
justified in similar ways or practices may be similar but the meanings of those
practices may vary. (Abel et al. 2001.)
This culturally bound childcare practice has its historical backgrounds (Ylppö
1921, Ylppö 1939, Ylppö 1947), the know-how on which has traditionally been
passed on from one generation to another. The guidelines have been based on this
historical background and have been distributed to the parents by the public
health services. Female family members and friends have had an important role
and influence on infant care practices in New Zealand (Abel et al. 2001) just like
in this study in Northern Finland. Parents’ own positive experiences have
strengthened continuity and their desire to recommend practices to their own
children as well.
Cultural knowledge-building related to children sleeping outdoors in the
winter has been a prerequisite for the practice, as knowledge grew little by little
with increased experience in a changing society. When lack of clothes could
earlier prevent mothers from letting their children sleep outdoors (Punto 1991),
there are now many kinds of prams available and the maternity package is
distributed to parents (Kela 2009). Without this growing knowledge, more
adverse effects could exist among infants. Stahl (2000) described the knowledge-
building process as consisting of cycles of personal and social knowledge-
building. Personal beliefs are entered into a social process of interaction with
other people and shared culture. Alternatives expressed in public statements and
other people’s statements are discussed, providing a rationale for different points
of view and converging to a shared understanding. Collaborative knowledge is
formed, formalized and objectified into cultural artifacts, which are used in
activity (Stahl 2000). Shared knowledge is the understanding of the same
historically accumulated knowledge, values, perspectives artifacts and ways of
life (Stahl & Hesse 2009).
In the city of Oulu, almost all parents let their children to sleep outdoors
showing the practice to be common. This was consistent with a study by the
Reima group (2009), which showed it to be more common in Denmark and a
popular practice in Norway and Sweden as well. No other international studies of
the prevalence of the outdoor sleeping practice were found. Instead, cultural
comparisons have been made between bedsharing, cosleeping and sleeping in
separate rooms, and different kinds of arguments for and against can be found. In
cold environments such as in Mongolia (Tsogt et al. 2006), Peru (Tronick et al.

89
1994) and Finland, different childcare practices can be found, all of which have
the same aim, i.e. to protect the child.
In this study, mothers who were interviewed were stimulated to discussion
when they had been in contact with different cultures where the outdoor sleeping
practice was not common; it was not understood by persons outside the culture
although it was taken for granted in the Nordic cultures. This was consistent with
the thought of Connolly (2006), who discussed cultural practices. Cultural
similarities and differences can be found in infant care practices and beliefs (Abel
et al. 2001), which goes to the core of cultural understanding of children’s health
and well-being (Morelli et al. 1992).
Adverse and beneficial health effects should be weighed and evidence-based
information provided to fit the individual needs as well as complex cultural
contexts of families (Morgan et al. 2006). Nelson et al. (2000) highlight the
significance of understanding child care from a cross-cultural perspective in SIDS
research pointing out the need to modify health educational messages for certain
cultural groups. Weaving the safety needs of the infant into family dynamics and
culture is a challenging task (Casey 2007), and more important than ever during
this time of international migration. As Melendez (2005) has discussed in her
review, immigrant families in the United States have to make choices concerning
childcare practices between their own values and the practices of their host
society and surrounding culture. Cultural sensitivity is needed by those who work
with families. (Melendez 2005.) It is important to be aware of the background and
meanings of childcare routines, not only take them as a self-evident practice. This
makes it possible to see even possible adverse effects more exactly and protect
the child effectively. Understanding is needed on how parents structure infants’
sleep, and what their goals and expectations are, and through awareness of these
factors parents may choose certain sleeping arrangements over others. (McKenna
& Volpe 2007.) It is important to understand cultural differences in beliefs and
practices for successful delivery of health recommendations (Abel et al. 2001).
6.3.3 Family well-being
A prerequisite for family well-being was safety perspectives, which had to be
taken into account accurately. Many risk factors related to the child, physical and
social environment were mentioned. Mothers had to observe their outdoor
sleeping babies frequently and protect them against risk factors. However, many
parents had not encountered dangerous situations and when comparing different

90
cultures, they felt the Finnish northern environment to be safe, which is one of the
factors of a healthy environment (Taylor & Repetti 1997) that impact beneficially
on the family’s sense of well-being (Åstedt-Kurki et al. 1999).
Shared cultural knowledge is seen in everyday routines (Weisner 2002).
Mothers act according to the cues from Finnish culture letting their child sleep
outdoors in the winter, which is seen as appropriate place-related behavior (Miller
et al. 1998). “Goodness of fit” between mother’s goals, activities, and
surroundings (Wicker 1972) can be reached enhancing family well-being.
Sometimes negative effects were also experienced.
In addition to satisfying the child’s sleep needs, mothers had wider goals of
providing healthy childcare and wanting their children to adopt a lifestyle that
would be in tune with the natural environment. As Like Wells & Lekies (2006: 13)
have described: “When children become truly engaged with the natural world at a
young age, the experience is likely to stay with them in a powerful way – shaping
their subsequent environmental path” (Wells & Lekies 2006). When concrete
goals are being attained it also promotes reaching larger, more abstract goals, thus
increasing the importance of concrete goals (Carver & Scheier 1998) such as
mothers’ everyday goal of putting their children outdoors to sleep.
According to McKenna et al. (2007) the majority of parents feel that it is an
alien idea to have the infant sleep alone. Yet, in the postindustrial west, solitary
sleep is thought to be modern, healthy, and normal way (McKenna et al. 2007).
Cosleeping promotes closeness in cultures where interdependence is the goal of
the childcare practice, whereas solitary sleeping promotes individualism in other
cultures (Morelli et al. 1992). The connection between the outdoor sleeping
practice and promotion of desirable socialization goals such as independence in
American families (Jenni & O'Connor 2005) did not exist in the data of this study,
despite the great distance when the child is sleeping outdoors in the garden and
the parents are indoors. Families with outdoor sleeping practice may also have
habit of bedsharing during other sleep episodes.
Positive attitude on the part of the community towards outdoor sleeping have
confirmed that the practice is now firmly rooted in our culture and is popular.
This strong attitude may have caused that sometimes the outdoor sleeping
practice has been felt as an activity of “good mothers”, leading to feelings of
failure and guilt if it is not successful. In the study of Morelli et al. (1992),
mothers justified their infant sleeping arrangements with reference to norms of
good parenting and the infant’s needs and development. The mothers they
interviewed who were not able to achieve the goal of traditional sleeping
91
arrangements of infants were unhappy because they were aware that they did not
comply with conventional practices. Salonen et al. (2008) found that parents in
Finland experienced low self-efficacy related to infants’ daily rhythm and sleep.
The outdoor sleeping episode has become a building block of everyday life
creating fluency by its rhythm and regularity, which children were found to need
as early as the late 19th century (Stearns et al. 1996) and which is seen as one of
the characteristics of good childcare in Dutch parenting (Super et al. 1996). Daily
routines are an important aspect of family health (Denham 1999, Denham 2002,
Fiese et al. 2006) and well-being (Vuori & Åstedt-Kurki 2009).
Furthermore, when the child takes longer daytime naps outdoors and his/her
sleep need satisfied, it has broader effects on family well-being. Mothers have a
moment of their own and get a chance to have a break that could promote
parenting, according to Schwichtenberg et al. (2011). Children who take more
naps may experience more positive maternal attention (Schwichtenberg et al.
2011), showing that infant sleep and parenting competence and well-being are
influenced by complex relationship systems, as shown by the transactional model
(Sadeh et al. 2010). At its best, the outdoor sleeping episode is a shared good
experience that evokes larger positive effects to family well-being. Mothers tried
to find a balance between the child’s and parents’ needs in the northern winter
environment and it was possible to reach the situation of goodness of fit. The
outdoor sleeping childcare practice is a desirable custom when it promotes family
well-being, but the child’s needs and safety come first.
6.3.4 Winter clothing of outdoor sleeping children
The selection of thermal insulation of clothing was not always sufficiently based
on outdoor air temperature, and traditional infant care practice was not always
precise enough to maintain infants’ thermal comfort in a cold outdoor
environment. In the study of Wailoo et al. (1989a) and Wigfield et al. (1993)
mothers applied more insulation when it was colder, instinctively providing
appropriate thermal conditions, whereas studies were also found where infants
were dressed inappropriately (Nicoll & Davies 1986, Tuohy & Tuohy 1990,
Bacon et al. 1991). All these studies were implemented indoors in quite stabile
thermal condition while mothers in northern winter encountered more challenges
in varying weather conditions.
The infants were like swaddled during outdoor sleeping when mothers
bundled them up in layered clothing and sleeping bags, restraining their

92
movements when they slept in the pram. Cold environment makes it possible to
use this kind of swaddling without overheating of the infants.
Mothers found the most appropriate thermal insulation of clothing at around
−5°C when the observed and required insulation values were equal. The Finnish
maternity package and pram gives appropriate insulation at −5°C, providing
explanation for this. Our findings in the questionnaire study (Study I) also support
the notion that the best temperature for letting the child sleep outdoors is about
−5°C. There is a bigger risk that infants do not reach thermal balance when it is
colder or warmer than −5°C. Fine adjustment is needed in the selection of thermal
insulation of clothing in other outdoor temperatures than −5°C.
The maximum amount of clothes gave appropriate insulation in ambient
temperature of about −17°C, but it should be noticed that by limiting the duration
of cold exposure, letting the child be outdoors is possible, but not desirable, in
colder weather. When the insulation of infant’s clothing is less than the required
insulation, the body cannot maintain thermal balance during a long nap outdoors,
which is why sleeping time has to be limited to prevent progressive cooling (ISO
11079 2007).
Our study shows that the thermal insulation of the clothing of infants sleeping
outdoors has important significance in terms of reaching goodness of fit between
the child, family and northern winter environment. The cooling rate of Tsk.
increased when the deficiency in thermal insulation increased, and in this kind of
situation, infants slept for a shorter time. This is in line with the study of Eiser et
al. (1985), in which mothers reported that the infants became irritable when too
cold.
A slow cooling of Tsk was observed even when the difference between
observed and required thermal insulation was ≥ 0 clo caused by either diurnal
variation, a sleep-induced decrease in body temperature or return to normal
temperature after initial overheating due to dressing procedures indoors. Before
going outdoors, infants were dressed in layered winter clothes and put in prams
indoors, causing heat accumulation and higher skin temperature at sleep onset
when compared to indoor sleeping.
Vasoconstriction showed that infants were not always sleeping at
thermoneutral temperature and their thermoregulation processes were activated.
Sometimes infants were also too heavily clothed, which was seen as higher level
of Tsk and relative humidity inside the clothing. This is consistent with the
findings of Grover et al. (1994), where bundling a healthy infant in a temperate
environment caused an increase in skin temperature. Of the different skin sites,

93
cheek temperature showed the biggest positive correlation with microclimate
humidity measured on the chest. This suggests that the head plays an important
role in heat loss, as also shown by previous studies where most of the heat loss in
dressed infants has occurred via the head (Stothers 1981, Elabbassi et al. 2002),
especially via the face (Nelson et al. 1989). Elabbassi et al. (2002) have cautioned
against reducing heat loss from the head of heavily dressed newborns, which was
suggested to contribute to overheating of the brain, and Mitchell et al. (2008)
have recommended avoiding head covering as part of SIDS prevention strategies.
Special attention should therefore be given therefore to cold protection of the
head of outdoor sleeping infants to avoid overheating and cooling alike.
Excessive bedding and clothing causes overheating, and its relevance to SIDS
has been widely studied (Nelson et al. 1989, Fleming et al. 1990, Ponsonby et al.
1992, Wigfield et al. 1993, Wilson et al. 1994, Watson et al. 1998, Baddock et al.
2004, Wilson & Chu 2005), but hardly any studies were found related to the
association between SIDS and too little thermal insulation (Williams et al. 1996).
It should be taken into account in interpretations that children are individuals,
as pointed out by one of the interviewed mothers who had noticed that her child
who had Down’s syndrome reacted differently to cold. The type and intensity of
cold exposure and many individual factors interact with cold-related symptoms
(Stocks et al. 2004). Special attention should be paid to thermal insulation of
clothing in the case of children with neurological disorders with cold extremities
(Svedberg et al. 2005) and Raynaud’s phenomenon (Nigrovic et al. 2003) because
of their increased risk of frostbite and higher level of stress reaction if they are
allowed to sleep outdoors. Moreover, facial cooling alone with inhalation of warm
air can increase bronchoconstriction in children with mild asthma (Zeitoun et al.
2004).
Scientifically based guidelines of children’s cold protection and sleeping in
varying weather conditions should still be considered. Hull et al. (1996a,b) have
suggested to giving general advice and reinforcing parents’ awareness of infants’
sweatiness and coldness and adjusting the amount of clothing insulation in
accordance with ambient air temperature, rather than giving more specific advice,
due to the individuality of infants and wide variation in their sleeping metabolic
rates.

94
6.3.5 Well-being of the children
Sleep. The findings of both the questionnaire and the observational study show
that among well-clothed children, the duration of outdoor sleep is longer
compared to indoor sleep. The average duration of outdoor sleep episode was
longer and that of indoor sleep shorter when compared to other studies of children
at the age of about three months sleeping indoors (Iglowstein et al. 2003, Sadeh
2004, Sadeh et al. 2009). Morgan (2006) has brought out the thought that long
sleep duration would not be the best practice nutritionally. It would also be a new
viewpoint in terms of SIDS research in Scandinavia that if long outdoor sleep
duration were taken into account the SIDS risk per slept hour might in many cases
be greater outdoors than indoors.
One suggestion for the long duration of outdoor sleeping could be restriction
of movements by winter clothing and sleeping bag, as swaddling has been shown
to increase duration of sleep (Gerard et al. 2002, Franco et al. 2005) and may help
infants return to sleep spontaneously, limiting parental intervention (Gerard et al.
2002). During outdoor sleeping auditory stimuli are reduced by hats, sleeping
bags and prams, preventing the effect of less intense auditory stimuli needed to
incur arousal when swaddled (Franco et al. 2005).
Soothing techniques and the location of sleep have been shown to affect
infant sleep (Sadeh 2004). Sleeping in a pram outdoors could be the same kind of
situation as falling asleep and sleeping alone in a crib in a separate room, which
has been shown to improve the possibilities of infants to sleep through the night,
with fewer night awakenings. It has been suggested that parents of such infants
are less likely to notice when their infant wakes up because of the distance and
visual separation (Sadeh 2004). Outdoor sleeping could promote infants’ own
self-regulation and self-soothing skills, the lack of which could cause shorter
sleep (Sadeh et al. 2010).
Parents familiarized their children with outdoor sleeping by starting with a
short duration. Children may learn to sleep outdoors so well that it is difficult to
try to have them sleep indoors. An antecedent stimulus may encourage the
behavior that has been linked with the stimulus. The stimulus serves as a trigger
for the desired behavior. Over time, bedtime routines in a familiar environment
become associated with the onset of sleep. (Wiggs 2009.) In the same way,
dressing the child in winter clothing and putting the child out serve as an
antecedent stimulus and help the child fall asleep.

95
Interaction between sleep and thermoregulation. Cold exposure was not the
factor that made children sleep longer. This study showed infants’ high sensitivity
to cold, when a slight cooling rate caused awakening and decreased the total sleep
time in a cool environment. Previous studies confirm this, as findings show a
decrease in total sleep time in unclothed neonates due to cold exposure (Bach et
al. 1994, Telliez et al. 1997). However, Hey and O’Connell (1970) have presented
a contrasting finding: well-clothed infants who were exposed to a cold
environment slept quietly even when heat production was increased, suggesting
that swaddled infants may not cry or call for attention even if they are under
severe cold stress. It could be hypothesized that a slow enough cooling rate due to
good clothing is under the infants’ threshold and during long duration of sleep
skin temperature can decrease without awakening the child. The skin is quite
insensitive to slow rates of temperature changes that cause adaptation (Parsons
2003). The thresholds for warm and cold stimuli increase when the rate of
temperature change becomes small (Kenshalo 1990). In previous studies on
infants’ sleep in cool exposure (Azaz et al. 1992, Telliez et al. 1997, Bach et al.
2000a, Bach et al. 2001, Telliez et al. 2004), the correlation between cooling rate
of Tsk and sleep duration has been ignored, although it is essential in relation to
sensations in a cold environment.
A correlation was not found between the rate of rise of Tsk and sleep duration
indoors. This is in line with the findings of Bach et al. (1994), where neonates’
sleep was not disturbed by exposure to warm temperatures. The threshold is
higher for the rate of rise than the rate of fall in skin temperature (Libert et al.
1979), and there is stronger sensitiveness to cold than to warm in all body sites
(Stevens & Choo 1998). During outdoor sleeping sweating of infants was
observed, and humidity increased quite evenly when Tsk increased. In the study of
Werner and Reents (1980), evaporation started to increase rapidly when the
ambient air temperature rose above 30°C.
Central-peripheral temperature difference has been shown to be a better
indicator of the thermal state of the child than a single skin temperature
measurement alone (Lyon et al. 1997). Those infants who had a slow cooling rate
and were outdoors for about 200 min or more (n = 10) had an increase of more
than 2°C in central-peripheral temperature difference. A difference of more than
2°C may have an effect on heart rate and blood pressure of very low birth weight
infants (Lyon et al. 1997). For this reason it would be better to limit the duration
of outdoor sleep to less than 200 min, especially if it is colder than −5°C. The

96
cooling-induced awakening of infants may interrupt the cold exposure before
cooling appears if the cooling rate crosses the threshold.
The findings indicate that the infants had in some cases cold stress; peripheral
vasoconstriction was found as there was a significant increase in the central-
peripheral skin temperature difference during outdoor sleeping and significantly
lower temperatures of the extremities at the end of outdoor sleeping compared to
indoor sleeping. Coldness of hands and feet was also observed by palpation.
Thermoneutrality was not maintained in 85% of the infants sleeping outdoors, as
Tsk fell more than 0.3°C/hour, if the definition of thermoneutrality is viewed
according to Sauer et al. (1984). However, the proportion of infants who reached
thermoneutrality could be higher because study infants were older and body
weight greater than in the study of Sauer et al. (1984). Skin temperature of the
chest at the end of outdoor and indoor sleep did not differ significantly, which
shows that cooling-induced vasoconstriction had first taken place in peripheral
vessels, but cooling had not proceeded to hyporthermia. The interviewed mothers
described how they checked their outdoor sleeping infants’ temperature by
palpating the cheeks and nape. It is possible to feel sweatiness by palpating the
nape, but it is not the right place to feel coldness, because nape temperature
remains warm during cold exposure due to the action of brown adipose tissue
(Silverman et al. 1964, Rylander et al. 1972).
It was interesting to find that mothers tried to protect their children from
cooling as they had noticed a correlation between cooling and the common cold.
An association was found between cold outdoor temperature and humidity and
respiratory tract infections among adults in the study of Mäkinen et al. (2009). On
the other hand, some mothers saw sleeping in a cold environment as toughening
the child, which is line with findings among Swedish mothers (Welles-Nyström et
al. 1994).
A white and bluish area on the child’s cheek was reported by some parents. A
white area seems to be frostnip, which is superficial cooling of tissues without
cellular destruction (Marx et al. 2010), whereas a bluish area might be a chilblain,
a form of cold injury representing the next stage of severity (Giusti & Tunnessen
1997). The low amount of frostbite injuries reported in previous studies in
Finland (Juopperi et al. 2002, Koljonen et al. 2004) was confirmed in this study,
as no other frostbite injuries came up.
97
6.4 Summary of the findings and conclusions
1. The winter environment in Northern Finland with pure air and peaceful, fresh
and clean nature can be seen as an affordance for the child sleeping outdoors.
2. During daytime, infants usually sleep outdoors once a day in different kinds
of conditions, from sunshine to heavy snowfall, with ambient air temperature
decreasing almost to −30°C.
3. The best temperature for outdoor sleeping was shown to be −5°C.
4. Outdoor sleeping is a self-evident and common culturally bound custom in
Northern Finland.
5. Guidelines, advice and encouragement about having children sleep outdoors
were given to mothers from different sources. Mothers built their own
personal knowledge through their experiences and shared it with others, at the
same time participating in the cultural knowledge-building processes. The
outdoor sleeping childcare practice is a commonly accepted collective, a type
of behavior that is sometimes felt to be compulsory.
6. There are many risk factors involved with the outdoor sleeping practice, but
when all security perspectives are taken into account it can promote family
well-being by creating a rhythm and strengthening the fluency of everyday
life.
7. It was difficult to adjust systematically the optimal thermal insulation for
outdoor sleeping infants during northern winter. When ambient temperature
decreased, the cooling rate of Tsk increased, suggesting that the cold
protection of the clothing compensated only partly for the increased heat loss.
Both cooling and sweating existed.
8. Specific guidelines on clothing are needed for parents.
9. Maximum amount of clothes combined with a pram can provide appropriate
insulation in ambient temperature of about −17°C.
10. Children sleep longest sleep outdoors when the cooling rate of Tsk is minimal.
11. Outdoor sleeping promotes satisfying children’s daytime sleep needs as it
increased the duration of sleep.
12. Infants should not sleep outdoors for more than three hours because a slow
cooling rate that remains under threshold could increase cold stress.
13. Outdoor sleeping was thought to promote children’s health.
14. A comprehensive view of the phenomenon was gathered in the evaluation
model of outdoor sleeping episode (Figure 5). It provides a tool for
systematic evaluation on each different level and between levels, shifting the

98
pointer of goodness of fit either to the direction of beneficial or adverse
effects.
6.5 Implementation and suggestions for future research
This study gives information about outdoor sleeping that can be applied to
practical problems encountered by parents. Families who move to Finland can
familiarize themselves with a childcare practice that they may even never have
heard of by reading this study. It also provides support to families who move
abroad, helping them describe a practice that is self-evident to them, but which
may seem peculiar to others.
The evaluation model of outdoor sleeping episode can be utilized in nursing
practice when public health nurses give counseling to families. It helps to identify
relationships between different levels and broader aspects that should be noticed
in guidelines. The model (Figure 5) can be used as a tool when giving counseling.
More specific guidelines are needed in Finland, and the study findings also
provide detailed information, for example about required clothing insulation in
different outdoor temperatures.
In nursing science, when mixed methods are used to study different kind of
phenomenon, findings can be compiled and utilized with the mixed methods
evaluation model (Figure 5), developed in this study. The questionnaire used in
Study I still needs improvements, and the evaluation model of outdoor sleeping
episode need testing.
This study prepares the ground for international comparative studies. Cultural
comparisons allow us to understand better children’s sleep in different contexts
and to evaluate the benefits and consequences of different cultural sleeping
practices (Giannotti & Cortesi 2009). Hardly any other studies addressing the
outdoor sleeping childcare practice can be found, and for that reason it would be
of great significance to add questions about outdoor sleeping into international
questionnaires, such as the Brief Infant Sleep Questionnaire (BISQ), used to study
bed sharing and room sharing (Sadeh 2004, Mindell et al. 2010a). Internationally
collaborative and broadly interdisciplinary studies are needed (Jenni & O’Connor
2005) using both qualitative and quantitative approaches in the field of SIDS
research, where there is still a lack of knowledge dealing with correlations
between outdoor sleeping, cooling and SIDS.
This study concentrated on the thermal environment, but not on the quality of
indoor and outdoor air, which are also important factors when evaluate the

99
healthfulness of the outdoor sleeping practice. Information about connections
between morbidity, such as falling ill due to infections, and cooling caused by
outdoor sleeping is still needed. In the next phase, more extensive
epidemiological studies and experimental research is needed to attain inferences
from causal relationships.
Future research is needed to find out the effects of extreme weather events on
children and to gain more knowledge about children’s environmental health.

100

101
References
Abel S, Park J, Tipene-Leach D, Finau S & Lennan M (2001) Infant care practices in New Zealand: a cross-cultural qualitative study. Soc Sci Med 53(9): 1135–1148.
Academy of Finland (2008) Academy of Finland Guidelines on Research Ethics. URI: http://www.aka.fi/Tiedostot/Tiedostot/Julkaisut/Suomen Akatemian eettiset ohjeet 2003.pdf. Cited 2010/12/10.
Acebo C, Sadeh A, Seifer R, Tzischinsky O, Hafer A & Carskadon MA (2005) Sleep/wake patterns derived from activity monitoring and maternal report for healthy 1- to 5-year-old children. Sleep 28(12): 1568–1577.
Adamson SK, Gandy GM & James LS (1965) The Influence of thermal factors upon oxygen consumption of the newborn human infant. J Pediatr 66: 495–508.
Agnew HW, Webb WB & Williams RL (1966). The first night effect: an EEG study of sleep. Psychophysiology 2: 263–6.
Aherne W & Hull D (1966) Brown adipose tissue and heat production in the newborn infant. J Pathol Bacteriol 91(1): 223–234.
Altman GD (1990) Serial measurements. In Practical Statistics for Medical Research. London, Chapman and Hall: 426–433.
Ammari A, Schulze KF, Ohira-Kist K, Kashyap S, Fifer WP, Myers MM & Sahni R (2009) Effects of body position on thermal, cardiorespiratory and metabolic activity in low birth weight infants. Early Hum Dev 85(8): 497–501.
Anders T, Sadeh A, Appareddy V (1995) Normal sleep in neonates and children. In Ferber R & Kryger MH (eds) Principles and practice of sleep medicine in the child. Philadelphia, Saunders: 7–18.
Anders TF & Taylor TR (1994) Babies and their sleep environment. CYE 11(2): 66–84. Anders TF (1994) Infant sleep, nighttime relationships, and attachment. Psychiatry 57(1):
11–21. Anderson ES, Petersen SA & Wailoo MP (1990) Factors influencing the body temperature
of 3–4 month old infants at home during the day. Arch Dis Child 65(12): 1308–1310. Anttonen H, Niskanen J, Meinander H, Bartels V, Kuklane K, Reinertsen RE, Varieras S
& Soltynski K (2004) Thermal manikin measurements–exact or not? Int J Occup Saf Ergon 10(3): 291–300.
Arkell S, Blair P, Henderson J & Fleming P (2007) Is the mattress important in helping babies keep warm?–Paradoxical effects of a sleeping surface with negligible thermal resistance. Acta Paediatr 96(2): 199–205.
Armstrong KL, O'Donnell H, McCallum R & Dadds M (1998) Childhood sleep problems: Association with prenatal factors and maternal distress/depression. J Paediatr Child Health 34(3): 263–266.
Armstrong KL, Quinn RA & Dadds MR (1994) The sleep patterns of normal children. Med J Aust 161(3): 202–206.
Arnestad M, Andersen M, Vege A & Rognum TO (2001) Changes in the epidemiological pattern of sudden infant death syndrome in southeast Norway, 1984–1998: implications for future prevention and research. Arch Dis Child 85(2): 108–115.

102
Asaka Y & Takada S (2011) Comparing sleep measures of infants derived from parental reports in sleep diaries and acceleration sensors. Acta Paediatr 100(8): 1158–1163.
Asakura H (2004) Fetal and neonatal thermoregulation. J Nippon Med Sch 71(6): 360–370. Åstedt-Kurki P, Hopia H & Vuori A (1999) Family health in everyday life: a qualitative
study on well-being in families with children. J Adv Nurs 29(3): 704–711. Åstedt-Kurki P, Paavilainen E & Lehti K (2001) Methodological issues in interviewing
families in family nursing research. J Adv Nurs 35(2): 288–293. Azaz Y, Fleming PJ, Levine M, McCabe R, Steward A, Johnson P (1992) The relationship
between environmental temperature, metabolic rate, sleep state, and evaporative water loss in infants from birth to three months. Pediatr Res 32(4): 417–423.
Bach V, Bouferrache B, Kremp O, Maingourd Y & Libert JP (1994) Regulation of sleep and body temperature in response to exposure to cool and warm environments in neonates. Pediatrics 93(5): 789–796.
Bach V, Telliez F, Krim G & Libert JP (1996) Body temperature regulation in the newborn infant: interaction with sleep and clinical implications. Neurophysiol Clin 26(6): 379–402.
Bach V, Telliez F, Leke A, Chiorri C, Libert J-P (2001) Interaction between body temperatures and the direction of sleep stage transition in neonates. SRO 4(1): 43–49.
Bach V, Telliez F, Leke A & Libert JP (2000) Gender-related sleep differences in neonates in thermoneutral and cool environments. J Sleep Res 9(3): 249–254.
Bach V, Telliez F & Libert JP (2002) The interaction between sleep and thermoregulation in adults and neonates. Sleep Med Rev 6(6): 481–492.
Bach V, Telliez F, Zoccoli G, Lenzi P, Leke A & Libert JP (2000a) Interindividual differences in the thermoregulatory response to cool exposure in sleeping neonates. Eur J Appl Physiol 81(6): 455–462.
Bacon CJ (1983) Over heating in infancy. Arch Dis Child 58(9): 673–674. Bacon CJ, Bell SA, Clulow EE & Beattie AB (1991) How mothers keep their babies warm.
Arch Dis Child 66(5): 627–632. Baddock SA, Galland BC, Beckers MG, Taylor BJ & Bolton DP (2004) Bed-sharing and
the infant's thermal environment in the home setting. Arch Dis Child 89(12): 1111–1116.
Barker R (1987) Prospecting in Environmental Psychology: Oskaloosa Revisited. In Stokols D & Altman I (eds) Handbook of Environmental Psychology, vol 2. New York, John Wiley & Sons: 1413–1432.
Barrett JR (2009) DOUBLE PROTECTION: reaching accord on the ethical conduct of child observational research. Environ Health Perspect 117(8): A354–7.
Bates JE, Viken RJ, Alexander DB, Beyers J & Stockton L (2002) Sleep and adjustment in preschool children: sleep diary reports by mothers relate to behavior reports by teachers. Child Dev 73(1): 62–74.
Bayer JK, Hiscock H, Hampton A & Wake M (2007) Sleep problems in young infants and maternal mental and physical health. J Paediatr Child Health 43(1): 66–73.
BBC NEWS (2004) Children die in Peruvian freeze. URI: http://news.bbc.co.uk/2/hi/ americas/3923731.stm. Cited 2011/6/6.

103
Beal SM (2000) Sudden infant death syndrome: is the winter prepoderance due to some infants having the head covered? J Paediatr Child Health 36(6): 612.
Bogdanoff P & Hämäläinen U (2011) Bodyt, potkarit ja perhevapaat. Äitiyspakkaus-kyselyn tuloksia. Nettityöpapereita/2011, Kela. URI: https://helda.helsinki.fi/ bitstream/handle/10138/25046/Nettityopapereita22.pdf?sequence=1. Cited 2011/5/19.
Braback L, Kjellman NI, Sandin A & Bjorksten B (2001) Atopy among schoolchildren in northern and southern Sweden in relation to pet ownership and early life events. Pediatr Allergy Immunol 12(1): 4–10.
Bronfenbrenner U (1979) The Ecology of Human Development. Experiments by Nature and Design. Cambridge, Harvard University Press.
Bronfenbrenner U (1977) Lewinian space and ecological substance. J Soc Iss 33(4): 199–212.
Brown FE, Spiegel PK & Boyle WE,Jr (1983) Digital deformity: an effect of frostbite in children. Pediatrics 71(6): 955–959.
Bunyavanich S, Landrigan CP, McMichael AJ & Epstein PR (2003) The impact of climate change on child health. Ambul Pediatr 3(1): 44–52.
Burnham MM, Goodlin–Jones BL, Gaylor EE & Anders TF (2002) Nighttime sleep–wake patterns and self–soothing from birth to one year of age: a longitudinal intervention study. J Child Psychiatry Allied Disciplines 43(6): 713–725.
Burns N, Grove SK & Gray J (2011) Understanding nursing research : building an evidence-based practice. St. Louis MO, Elsevier.
Canter D (1992) Understanding, Assessing, and Acting in Places: Is an Integrative Framework Possible? In Garling T & Evans G (eds) Environment, Cognition, and Action: An Integrated Approach. Cary NC USA: 191–209.
Carskadon MA & Acebo C (1993) Parental reports of seasonal mood and behavior changes in children. J Am Acad Child Adolesc Psychiatry 32(2): 264–269.
Carver CS & Scheier MF (1998) On the self-regulation of behavior. New York, Cambridge University Press.
Casey TC (2007) Separate sleep environment for infants. J Obstet Gynecol Neonatal Nurs 36(4): 362–363.
Chang RK, Keens TG, Rodriguez S & Chen AY (2008) Sudden infant death syndrome: changing epidemiologic patterns in California 1989–2004. J Pediatr 153(4): 498–502.
Chess S & Thomas A (1984) Origins and evolution of behavior disorders from infancy to early adult life. New York,NY, Brunner/Mazel.
Connolly M, Crichton-Hill Y & Ward T (2006) Culture and child protection Reflexive Responses. London, Jessica Kingsley Publishers.
Costall A (1995) Socializing affordances. Theory & Psychology 5(4): 467–481. Côté L & Turgeon J (2005) Appraising qualitative research articles in medicine and
medical education. Med Teach 27(1): 71–75. Creswell JW (2003) Research design: qualitative, quantitative, and mixed methods
approaches. Thousands Oaks CA, SAGE.

104
Creswell JW (2005) Educational research: Planning, conducting, and evaluating quantitative and qualitative research. 2nd ed. Upper Saddle River NJ, Pearson Education.
Creswell JW & Plano Clark VL (2007) Designing and conducting mixed methods research. Thousand Oaks (CA), SAGE Publications.
Crosby B, LeBourgeois MK & Harsh J (2005) Racial differences in reported napping and nocturnal sleep in 2- to 8-year-old children. Pediatrics 115(1 Suppl): 225–232.
Culic S (2005) Cold injury syndrome and neurodevelopmental changes in survivors. Arch Med Res 36(5): 532–538.
Dagan R & Gorodischer R (1984) Infections in hypothermic infants younger than 3 months old. Am J Dis Child 138(5): 483–485.
Dahl RE (1996) The impact of inadequate sleep on children's daytime cognitive function. Semin Pediatr Neurol 3(1): 44–50.
Darnall RA (1987) The thermophysiology of the newborn infant. Med Instrum 21(1): 16–22.
Day RL, Caliguiri L, Kamenski C & Ehrlich F (1964) Body temperature and survival of premature infants. Pediatrics 34: 171–181.
Denham SA (1999) Part I: The Definition and Practice of Family Health. J Fam Nurs 5(2): 133–159.
Denham SA (2002) Family Routines: A Structural Perspective for Viewing Family Health. Adv Nurs Sci 24(4): 60–74.
Denscombe M (2008) Communities of practice: A research paradigm for the mixed methods approach. MMR 2(3): 270–283.
Dey I (1996) Qualitative data analysis: a user-friendly guide for social scientists. London, Routledge.
Douglas AS, Allan TM & Helms PJ (1996) Seasonality and the sudden infant death syndrome during 1987–9 and 1991–3 in Australia and Britain. BMJ 312(7043): 1381–1383.
Douglas AS & Al-Sayer H (1991) Seasonality of disease in Kuwait. Lancet 337(8754): 1393.
Douglas AS, Helms PJ & Jolliffe IT (1998) Seasonality of sudden infant death syndrome in mainland Britain and Ireland 1985–95. Arch Dis Child 79(3): 269–270.
Dragovich D, Tamburlini G, Alisjahbana A, Kambarami R, Karagulova J, Lincetto O, Malla DS, Mello MJ & Vani NS (1997) Thermal control of the newborn: knowledge and practice of health professional in seven countries. Acta Paediatr 86(6): 645–650.
Ebi KL & Paulson JA (2007) Climate change and children. Pediatr Clin North Am 54(2): 213–226.
Eiser C, Town C & Tripp J (1985) Dress and care of infants in health and illness. Arch Dis Child 60(5): 465–470.
Elabbassi EB, Bach V, Makki M, Delanaud S, Telliez F, Leke A & Libert JP (2001) Assessment of dry heat exchanges in newborns: influence of body position and clothing in SIDS. J Appl Physiol 91(1): 51–56.

105
Elabbassi EB, Belghazi K, Delanaud S & Libert JP (2004) Dry heat loss in incubator: comparison of two premature newborn sized manikins. Eur J Appl Physiol 92(6): 679–682.
Elabbassi EB, Chardon K, Telliez F, Bach V & Libert JP (2002) Influence of head position on thermal stress in newborns: simulation using a thermal mannequin. J Appl Physiol 93(4): 1275–1279.
Elo S. Kyngäs H (2008) The qualitative content analysis process. J Adv Nurs 62(1): 107–115.
El-Sheikh M, Buckhalt JA, Mize J & Acebo C (2006) Marital Conflict and Disruption of Children's Sleep. Child Dev 77(1): 31–43.
Ens CD, Hanlon-Dearman A, Millar MC & Longstaffe S (2010) Using telehealth for assessment of fetal alcohol spectrum disorder: the experience of two Canadian rural and remote communities. Telemed J E Health 16(8): 872–877.
Ervasti O, Hassi J & Manelius J (1993) Frostbite-induced changes in bones and joints. Duodecim 109(1): 60–63.
ETENE National Advisory Board on Health Care Ethics (2003) Valtakunnallisen terveydenhuollon eettisen neuvottelukunnan asettaman työryhmän loppuraportti. Näkökulmia lääketieteellisistä tutkimuksista lapsilla. URI: http://www.etene.fi/c/ document_library/get_file?folderId=17165&name=DLFE-538.pdf. Cited 2011/03/25/.
Fiese BH, Foley KP & Spagnola M (2006) Routine and ritual elements in family mealtimes: contexts for child well-being and family identity. New Dir Child Adolesc Dev 111(111): 67–89.
Finnish Meteorological Institute (2009). Climatological statistics for the normal period 1971–2000. URI: http://www.fmi.fi/saa/tilastot_7.html. Cited 2009/12/22.
Finnish Meteorological Institute (2011) Finland's Climate. URI: http://legacy.fmi.fi/ weather/climate.html. Cited 2011/5/24.
Fleming PJ, Gilbert R, Azaz Y, Berry PJ, Rudd PT, Stewart A & Hall E (1990) Interaction between bedding and sleeping position in the sudden infant death syndrome: a population based case-control study. BMJ 301(6743): 85–89.
Foster KG, Hey EN & Katz G (1969) The response of the sweat glands of the newborn baby to thermal stimuli and to intradermal acetylcholine. J Physiol 203(1): 13–29.
Franco P, Lipshutz W, Valente F, Adams S, Scaillet S & Kahn A (2002) Decreased arousals in infants who sleep with the face covered by bedclothes. Pediatrics 109(6): 1112–1117.
Franco P, Scaillet S, Valente F, Chabanski S, Groswasser J & Kahn A (2001) Ambient temperature is associated with changes in infants' arousability from sleep. Sleep 24(3): 325–329.
Franco P, Seret N, Van Hees JN, Scaillet S, Groswasser J & Kahn A (2005) Influence of swaddling on sleep and arousal characteristics of healthy infants. Pediatrics 115(5): 1307–1311.
Gagge AP, Burton AC & Bazett HC (1941) A practical system of units for the description of heat exchange of man with his environment. Science 94: 428–430.

106
Gardinal-Galera I, Pajot C, Paul C & Mazereeuw-Hautier J (2010) Childhood chilblains is an uncommon and invalidant disease. Arch Dis Child 95(7): 567–568.
Gerard CM, Harris KA & Thach BT (2002) Spontaneous arousals in supine infants while swaddled and unswaddled during rapid eye movement and quiet sleep. Pediatrics 110(6): e70.
Germo GR, Chang ES, Keller MA & Goldberg WA (2007) Child sleep arrangements and family life: perspectives from mothers and fathers. Infant Child Dev 16(4): 433–456.
Giacomini MK & Cook DJ (2000) Users' guides to the medical literature: XXIII. Qualitative research in health care A. Are the results of the study valid? Evidence-Based Medicine Working Group. JAMA 284(3): 357–362.
Giannotti & Cortesi (2009) Family and Cultural Influences on Sleep Development. Child Adolesc Psychiatr Clin N Am 18(4): 849–861.
Gibson JJ (1986) The ecological approach to visual perception. Hillsdale NJ, Lawrence Erlbaum.
Gilbert R, Salanti G, Harden M & See S (2005) Infant sleeping position and the sudden infant death syndrome: systematic review of observational studies and historical review of recommendations from 1940 to 2002. Int J Epidemiol 34(4): 874–887.
Giusti R & Tunnessen WW,Jr (1997) Picture of the month. Chilblains (pernio). Arch Pediatr Adolesc Med 151(10): 1055–1056.
Glass L, Silverman W, Sinclair J (1968) Effect of the thermal environment on cold resistance and growth of small infants after the first week of life. Pediatrics 41(6): 1033–1046.
Glotzbach SF, Edgar DM, Boeddiker M & Ariagno RL (1994) Biological rhythmicity in normal infants during the first 3 months of life. Pediatrics 94(4 Pt 1): 482–488.
Goldsmith JR, Arbeli Y & Stone D (1991) Preventability of neonatal cold injury and its contribution to neonatal mortality. Environ Health Perspect 94: 55–59.
Gómez RL, Bootzin RR & Nadel L (2006) Naps Promote Abstraction in Language-Learning Infants. Psychol Sci 17(8): 670–674.
Graneheim UH & Lundman B (2004) Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today 24(2): 105–112.
Greene JC (2005) Synthesis: A reprise on mixing methods. In Weisner TS (ed) Discovering successful pathways in children's development: Mixed methods in the study of childhood and family life. Chicago, University of Chicago Press: 405–419.
Greeno JG (1994) Gibson's affordances. Psychol Rev 101(2): 336–342. Gregory AM, Caspi A, Eley TC, Moffitt TE, Oconnor TG & Poulton R (2005) Prospective
longitudinal associations between persistent sleep problems in childhood and anxiety and depression disorders in adulthood. J Abnorm Child Psychol 33(2): 157–163.
Grover G, Berkowitz CD, Lewis RJ, Thompson M, Berry L & Seidel J (1994) The effects of bundling on infant temperature. Pediatrics 94(5): 669–673.
Guidotti TL & Gitterman BA (2007) Global pediatric environmental health. Pediatr Clin North Am 54(2): 335–350.
107
Haglund B, Cnattingius S & Otterblad-Olausson P (1995) Sudden infant death syndrome in Sweden, 1983–1990: season at death, age at death, and maternal smoking. Am J Epidemiol 142(6): 619–624.
Harrison LM, Morris JA, Telford DR, Brown SM & Jones K (1999) The nasopharyngeal bacterial flora in infancy: effects of age, gender, season, viral upper respiratory tract infection and sleeping position. FEMS Immunol Med Microbiol 25(1–2): 19–28.
Hartling L, Brison RJ, Crumley ET, Klassen TP & Pickett W (2004) A systematic review of interventions to prevent childhood farm injuries. Pediatrics 114(4): e483–96.
Hassi J (1977) The brown adipose tissue in man. Structural and functional aspects in relation to age. Oulu, Acta Universitatis Ouluensis D 21.
Havenith G (1999) Heat balance when wearing protective clothing. Ann Occup Hyg 43(5): 289–296.
Heft H (1989) Affordances and the body: An intentional analysis of Gibson's ecological approach to visual perception. J Theory Soc Behav 19(1): 1–30.
Hensel H (1974) Thermoreceptors. Annu Rev Physiol 36: 233–249. Herpin P, Lossec G, Schmidt I, Cohen-Adad F, Duchamp C, Lefaucheur L, Goglia F &
Lanni A (2002) Effect of age and cold exposure on morphofunctional characteristics of skeletal muscle in neonatal pigs. Pflugers Arch 444(5): 610–618.
Hey EN (1969) The relation between environmental temperature and oxygen consumption in the new-born baby. J Physiol 200(3): 589–603.
Hey EN (1972) Thermal regulation in the newborn. Br J Hosp Med (8): 51–64. Hey EN & O'Connell B (1970) Oxygen consumption and heat balance in the cot-nursed
baby. Arch Dis Child 45(241): 335–343. Hill CM, Hogan AM & Karmiloff-Smith A (2007) To sleep, perchance to enrich learning?
Arch Dis Child (92): 637–643. Hiscock H & Wake M (2002) Randomised controlled trial of behavioural infant sleep
intervention to improve infant sleep and maternal mood. BMJ 324(7345): 1062–1065. Hiscock H & Wake M (2001) Infant Sleep Problems and Postnatal Depression: A
Community-Based Study. Pediatrics 107(6): 1317. Holmer I (2004) Thermal manikin history and applications. Eur J Appl Physiol 92(6): 614–
618. Hoogsteder M, Maier R & Elbers E (1998) Adult-Child interaction, joint problem solving
and the structure of cooperation. In Woodhead M, Faulkner D & Littleton K (eds) Cultural Worlds of Early Childhood. London and New York, Routledge: 178–196.
Hoppenbrouwers T, Calub M, Arakawa K & Hodgman JE (1981) Seasonal relationship of sudden infant death syndrome and environmental pollutants. Am J Epidemiol 113(6): 623–635.
Hsieh HF & Shannon SE (2005) Three approaches to qualitative content analysis. Qual Health Res 15(9): 1277–1288.
Hull D, McArthur AJ, Pritchard K & Goodall M (1996a) Metabolic rate of sleeping infants. Arch Dis Child 75(4): 282–287.
Hull D, McArthur AJ, Pritchard K & Oldham D (1996b) Individual variation in sleeping metabolic rates in infants. Arch Dis Child 75(4): 288–291.

108
Iglowstein I, Jenni OG, Molinari L & Largo RH (2003) Sleep duration from infancy to adolescence: reference values and generational trends. Pediatrics 111(2): 302–307.
ISEE The International Society for environmental Epidemiology (2009) ISEE Statement on the White Paper titled: The Necessity of Observing Children’s Exposure to Contaminants in Their Real-World Environmental Settings. URI: http://www.iseepi.org/ChildrensExposureWhitePaper&ISEEResponse-4-09.pdf. Cited 2011/03/24.
ISO 15831 (2004) Clothing – Physiological effects – Measurement of thermal insulation by means of a thermal manikin. Geneva, International Standards Organisation.
ISO 11079 (2007) Ergonomics of the thermal environment – Determination and interpretation of cold stress when using required clothing insulation (IREQ) and local cooling effects. Geneva, International Standards Organisation.
ISO 9920 (2007) Ergonomics of the thermal environment – Estimation of thermal insulation and water vapour resistance of a clothing ensemble. Geneva, International Standards Organisation.
IUPS Thermal Commission (2001) Glossary of terms for thermal physiology. 3rd ed. Jpn J Physiol 51(2): 245–280.
Javo C, Ronning JA & Heyerdahl S (2004) Child-rearing in an indigenous Sami population in Norway: a cross-cultural comparison of parental attitudes and expectations. Scand J Psychol 45(1): 67–78.
Jenni OG & O'Connor BB (2005) Children's sleep: an interplay between culture and biology. Pediatrics 115(1 Suppl): 204–216.
Johansson B (1959) Brown fat: a review. Metabolism 8(3): 221–240. Jones ME, Ponsonby AL, Dwyer T & Gilbert N (1994) The relation between climatic
temperature and sudden infant death syndrome differs among communities: results from an ecologic analysis. Epidemiolog 5(3): 332–336.
Juopperi K, Hassi J, Ervasti O, Drebs A & Näyhä S (2002) Incidence of frostbite and ambient temperature in Finland, 1986–1995. A national study based on hospital admissions. Int J Circumpolar Health 61(4): 352–362.
Kaiser FG & Fuhrer U (1996) Dwelling: Speaking of an unnoticed universal language. New Ideas Psychol 14(3): 225–236.
Kankkunen P & Vehviläinen-Julkunen K (2010) Tutkimus hoitotieteessä. Helsinki, WSOYpro.
Kao HF, Hsu MT & Clark L (2004) Conceptualizing and critiquing culture in health research. J Transcult Nurs 15(4): 269–277.
Katz ES, Greene MG, Carson KA, Galster P, Loughlin GM, Carroll J & Marcus CL (2002) Night-to-night variability of polysomnography in children with suspected obstructive sleep apnea. J Pediatr 140(5):589–594.
Kela the Social Insurance Institution of Finland. (2009). Maternity package for 2009 features recycled materials. URI: http://www.kela.fi/in/internet/english.nsf/NET/ 030409090408ML?OpenDocument. Cited 2009/12/7.
Kerslake D (1991) The insulation provided by infants' bedclothes. Ergonomics 34: 893–907.

109
Kim HS (2000) The nature of theoretical thinking in nursing. New York, Springer Publishing Company.
Kimchi J, Polivka B & Stevenson JS (1991) Triangulation: operational definitions. Nurs Res 40(6): 364–366.
Klonoff-Cohen H, Lam PK & Lewis A (2005) Outdoor carbon monoxide, nitrogen dioxide, and sudden infant death syndrome. Arch Dis Child 90(7): 750–753.
Koljonen V, Andersson K, Mikkonen K & Vuola J (2004) Frostbite injuries treated in the Helsinki area from 1995 to 2002. J Trauma 57(6): 1315–1320.
Korones SB (2004) An encapsulated history of thermoregulation in the neonate. NeoReviews 5(3): e78–e85.
Korpela KM (1989) Place-identity as a product of environment self-regulation. J Environ Psychol (9): 241–256.
Korpela KM (2002) Children's environment. In Bechtel RBCA (ed) Handbook of environmental psychology. New York, John Wiley & Sons: 363–373.
Kotaniemi JT, Hassi J, Kataja M, Jonsson E, Laitinen LA, Sovijärvi AR & Lundback B (2001) Does non-responder bias have a significant effect on the results in a postal questionnaire study? Eur J Epidemiol 17(9): 809–817.
Krishnamurthy S, Singh V & Gupta P (2009) Neonatal Frostbite with Gangrene of Toes. Pediatr Dermatol 26(5): 625–626.
Kronholm E, Alanen E & Hyyppä MT (1987) Sleep movements and poor sleep in patients with non-specific somatic complaints. I. No first-night effect in poor and good sleepers. J Psychosom Res 31: 623–9.
Kyttä M (2003) Children in outdoor contexts: affordances and independent mobility in the assessment of environmental child friendliness. Academic dissertation, Helsinki University of Technology, Centre for Urban and Regional Studies, Espoo.
Lam P, Hiscock H & Wake M (2003) Outcomes of infant sleep problems: a longitudinal study of sleep, behavior, and maternal well-being. Pediatrics 111(3): e203–7.
Landhuis CE, Poulton R, Welch D & Hancox RJ (2008) Childhood sleep time and long-term risk for obesity: a 32-year prospective birth cohort study. Pediatrics 122(5): 955–960.
Lavigne JV, Arend R, Rosenbaum D, Smith A, Weissbluth M, Binns HJ & Christoffel KK (1999) Sleep and behavior problems among preschoolers. J Dev Behav Pediatr 20(3): 164–169.
Le Treut H, Somerville R, Cubasch U, Ding Y, Mauritzen C, Mokssit A, Peterson T & Prather M (2007) Historical Overview of Climate Change. In Solomon S, Qin D, Manning M, Chen Z, Marquis M, Averyt KB, Tignor M & Miller HL (ed) Historical Overview of Climate Change. In: Climate Change 2007: The Physical Science Basis. Contribution of Working Group I to the Fourth Assessment Report of the Intergovernmental Panel on Climate Change. Cambridge, United Kingdom and New York NY, USA. URI: http://www.ipcc.ch/pdf/assessment-report/ar4/wg1/ar4-wg1-chapter1.pdf. Cited 2011/5/24. Cambridge University Press: 95–122.

110
Lebowitz M, Lioy P, McKone T, Spengler J, Adgate J, Bennett D, Fenske R, Freeman N, Graham J, Kissel J, Neutra R, Al-Delaimy W & Weisel C (2008) The necessity of observing children's exposure to contaminants in their real-world environmental settings. URI: http://www.iseepi.org/ChildrensExposureWhitePaper&ISEEResponse-4-09.pdf. Cited 2011/03/23.
Leininger M (1997) Overview of the theory of culture care with the ethnonursing research method. J Transcult Nurs 8(2): 32–52.
Leininger MM (2006) Culture Care Diversity and Universality Theory and Evolution of the Ethnonursing Method. In Leininger MM & McFarland MR (eds) Culture Care Diversity and Universality. Boston, Jones and Bartlett Publishers: 1–41.
Leiss JK & Suchindran CM (1996) Sudden infant death syndrome and local meteorologic temperature in North Carolina. Am J Epidemiol 144(2): 111–115.
Lekes N, Gingras I, Philippe FL, Koestner R & Fang J (2010) Parental autonomy-support, intrinsic life goals, and well-being among adolescents in China and North America. J Youth Adolesc 39(8): 858–869.
Lemola S, Räikkönen K, Scheier MF, Matthews KA, Pesonen A-K, Heinonen K, Lahti J, Komsi N, Paavonen JE & Kajantie E (2011) Sleep, quantity, quality and optimism in children. J Sleep Res 20(1): 12–20.
Lenburg CB, Lipson JG, Demi AS, Blaney DR, Stern PN, Schultz PN & Gene L (1995) Promoting cultural competence in and through nursing education: A critical review and comprehensive plan for action. Washington DC, American Nurses Association, American Academy of Nursing.
Libert JP, Candas V & Vogt JJ (1979) Effect of rate of change in skin temperature on local sweating rate. J Appl Physiol 47(2): 306–311.
Lincoln YS, & Guba EG (1985). Naturalistic inquiry. Newbury Park CA, Sage Publications.
Lindgren C (1999) Respiratory control during upper airway infection mechanism for prolonged reflex apnoea and sudden infant death with special reference to infant sleep position. FEMS Immunol Med Microbiol 25(1–2): 97–102.
Lindheim R & Syme SL (1983) Environments, people, and health. Annu Rev Public Health 4: 335–359.
Lipton EL, Steinschneider A & Richmond JB (1965) Swaddling, a child care practice: historical, cultural and experimental observations. Pediatrics 35:SUPPL: 519–567.
Ljung K, Selinus O & Otabbong E (2006) Metals in soils of children's urban environments in the small northern European city of Uppsala. Sci Total Environ 366(2–3): 749–759.
Lodemore M, Petersen SA & Wailoo MP (1991) Development of night time temperature rhythms over the first six months of life. Arch Dis Child 66(4): 521–524.
Lodemore MR, Petersen SA & Wailoo MP (1992) Factors affecting the development of night time temperature rhythms. Arch Dis Child 67(10): 1259–1261.
Long WB 3rd, Edlich RF, Winters KL & Britt LD (2005) Cold injuries. J Long Term Eff Med Implants 15(1): 67–78.

111
Lyon A J, Pikaar M E, Badger P, Mclntosh N (1997) Temperature control in very low birthweight infants during first five days of life. Arch Dis Child Fetal Neonatal Ed (76): F47–F50.
Macey PM, Schluter PJ & Ford RP (2000) Weather and the risk of sudden infant death syndrome: the effect of wind. J Epidemiol Community Health 54(5): 333–339.
Mage DT (2004) Seasonal variation of sudden infant death syndrome in Hawaii. J Epidemiol Community Health 58(11): 912–916.
Mäkinen TM, Juvonen R, Jokelainen J, Harju TH, Peitso A, Bloigu A, Silvennoinen-Kassinen S, Leinonen M & Hassi J (2009) Cold temperature and low humidity are associated with increased occurrence of respiratory tract infections. Respir Med 103(3): 456–462.
Malloy MH & Freeman DH (2004) Age at death, season, and day of death as indicators of the effect of the back to sleep program on sudden infant death syndrome in the United States, 1992–1999. Arch Pediatr Adolesc Med 158(4): 359–365.
Mann T & Elliot RIK (1957) Neonatal cold injury due to accidental exposure to cold. Lancet 1: 229–234.
Maquet P (2001) The Role of Sleep in Learning and Memory. Science 294(5544): 1048. Martin J, Hiscock H, Hardy P, Davey B & Wake M (2007) Adverse associations of infant
and child sleep problems and parent health: an Australian population study. Pediatrics 119(5): 947–955.
Marx J, Hockberger R, Walls R, Adams J, Barsan W, Biros M, Danzl D, Gausche-Hill M, Ling L & Newton E (2010) Rosen's emergency medicine: concepts and clinical practice. 7th edition. Philadelphia PA, Elsevier.
Matthews JN, Altman DG, Campbell MJ & Royston P (1990) Analysis of serial measurements in medical research. BMJ 300(6719): 230–235.
McCullough EA, Eckels S & Harms C. (2009) Determining temperature ratings for children's cold weather clothing. Appl Ergon (40): 870–877.
McDowell I & Newell C (1996) Measuring health: a guide to rating scales and questionnaires. New York, Oxford University Press.
McGraw K, Hoffmann R, Harker C & Herman JH (1999) The development of circadian rhythms in a human infant. Sleep 22(3): 303–310.
McKenna JJ, Ball HL & Gettler LT (2007) Mother-infant cosleeping, breastfeeding and sudden infant death syndrome: what biological anthropology has discovered about normal infant sleep and pediatric sleep medicine. Am J Phys Anthropol Suppl 45(Suppl 45): 133–161.
McKenna JJ & Volpe LE (2007) Sleeping with baby: an internet-based sampling of parental experiences, choices, perceptions, and interpretations in a western industrialized context. Infant Child Dev 16(4): 359–385.
Mead M (1954) The swaddling hypothesis: Its reception. American Anthropol 56: 395–409.
Medical Research Act (No. 488/1999). Ministry of Social Affairs and Health, Finland. URI: http://www.finlex.fi/en/laki/kaannokset/1999/en19990488.pdf. Cited 2011/03/25.

112
Mednick S, Nakayama K & Stickgold R (2003) Sleep-dependent learning: a nap is as good as a night. Nat Neurosci 6(7): 697.
Meijer AM & van den Wittenboer GL (2007) Contribution of infants' sleep and crying to marital relationship of first-time parent couples in the 1st year after childbirth. J Fam Psychol 21(1): 49–57.
Meinander H, Anttonen H, Bartels V, Holmer I, Reinertsen RE, Soltynski K & Varieras S (2004) Manikin measurements versus wear trials of cold protective clothing (Subzero project). Eur J Appl Physiol 92(6): 619–621.
Melendez LME (2005) Parental Beliefs and Practices Around Early Self-regulation: The Impact of Culture and Immigration. Infant Young Child 18(2): 136–146.
MercoPress (2010a) Santiago suffering the coldest July since 1908: 2 degrees below monthly average. URI: http://en.mercopress.com/2010/08/03/santiago-suffering-the-coldest-july-since-1908-2-degrees-below-monthly-average. Cited 2011/6/6.
MercoPress (2010b) Chile's hospitals anticipate wave of respiratory infections. URI: http://en.mercopress.com/2010/07/10/chile-s-hospitals-anticipate-wave-of-respiratory-infections. Cited 2011/6/6.
Mestyan J, Bata G, Jarai I & Fekete M (1964) The significance of facial skin temperature in the chemical heat regulation of premature infants. Biol Neonat 7: 243–254.
Milerad J, Norvenius G & Wennergren G (1993) SIDS outdoors and seasonality in Sweden 1975–1987. Acta Paediatr 82(12): 1039–1042.
Miller PC, Shim JE & Holden GW (1998) Immediate contextual influences on maternal behavior: Environmental affordances and demands. J Environ Psychol 18(4): 387–398.
Mindell JA, Sadeh A, Kohyama J & How TH (2010a) Parental behaviors and sleep outcomes in infants and toddlers: a cross-cultural comparison. Sleep Med 11(4): 393–399.
Mindell JA, Sadeh A, Wiegand B, How TH & Goh DY (2010b) Cross-cultural differences in infant and toddler sleep. Sleep Med 11(3): 274–280.
Mitchell EA, Clements M, Williams SM, Stewart AW, Cheng A & Ford R (1999) Seasonal differences in risk factors for sudden infant death syndrome. Acta Paediatr 88(3): 253–258.
Mitchell EA, Thompson JM, Becroft DM, Bajanowski T, Brinkmann B, Happe A, Jorch G, Blair PS, Sauerland C & Vennemann MM (2008) Head covering and the risk for SIDS: findings from the New Zealand and German SIDS case-control studies. Pediatrics 121(6): e1478–83.
Montomoli C, Monti MC, Stramba-Badiale M, Marinoni A, Foglieni N, Carreri V, Amigoni M & Schwartz PJ (2004) Mortality due to sudden infant death syndrome in Northern Italy, 1990–2000: a baseline for the assessment of prevention campaigns. Paediatr Perinat Epidemiol 18(5): 336–343.
Morelli GA, Rogoff B, Oppenheim D & Goldsmith D (1992) Cultural Variation in Infants' Sleeping Arrangements: Questions of Independence. Dev Psychol 28(4): 604–613.
Morgan KH, Groer MW & Smith LJ (2006) The controversy about what constitutes safe and nurturant infant sleep environments. JOGNN 35(6): 684–691.

113
Morrell J (1999) The Role of Maternal Cognitions in Infant Sleep Problems as Assessed by a New Instrument, the Maternal Cognitions about Infant Sleep Questionnaire. J Child Psychol Psychiatry Allied Disciplines 40(2): 247.
Morrell J & Cortina-Borja M (2002) The developmental change in strategies parents employ to settle young children to sleep, and their relationship to infant sleeping problems, as assessed by a new questionnaire: the parental interactive bedtime behaviour scale. Infant Child Dev (11): 17–41.
Morris S, James-Roberts IS, Sleep J & Gillham P (2001) Economic evaluation of strategies for managing crying and sleeping problems. Arch Dis Child 84(1): 15–19.
Nakano T, Fediuk K, Kassi N, Egeland GM & Kuhnlein HV (2005) Dietary nutrients and anthropometry of Dene/Metis and Yukon children. Int J Circumpolar Health 64(2): 147–156.
National weather service forecast office (2011) What are temperature inversions? http://www.wrh.noaa.gov/slc/climate/TemperatureInversions.php. Cited 2011/6/7.
Näyhä S (2000) Seasonal variation of deaths in Finland–is it still diminishing? Int J Circumpolar Health 59(3–4): 182–187.
Nelson EA, Schiefenhoevel W & Haimerl F (2000) Child care practices in nonindustrialized societies. Pediatrics 105(6): E75.
Nelson EA & Taylor BJ (1989) Infant clothing, bedding and room heating in an area of high postneonatal mortality. Paediatr Perinat Epidemiol 3(2): 146–156.
Nelson EA, Taylor BJ & Weatherall IL (1989) Sleeping position and infant bedding may predispose to hyperthermia and the sudden infant death syndrome. Lancet 1(8631): 199–201.
Nicoll A & Davies L (1986) How warm are babies kept at home? Health Visitor 59(4): 113–114.
Nightingale F & McDonald L (2001) Florence Nightingale on public health care. Waterloo, Ont, Wilfrid Laurier University Press.
Nigrovic PA, Fuhlbrigge RC & Sundel RP (2003) Raynaud's phenomenon in children: a retrospective review of 123 patients. Pediatrics 111(4 Pt 1): 715–721.
North RG, Petersen SA & Wailoo MP (1995) Lower body temperature in sleeping supine infants. Arch Dis Child 72(4): 340–342.
Oliveira AV, Gaspar AR & Quintela DA (2008) Measurements of clothing insulation with a thermal manikin operating under the thermal comfort regulation mode: comparative analysis of the calculation methods. Eur J Appl Physiol 104(4): 679–688.
Parahoo K (2006) Nursing research: principles, process and issues. Basingstoke, Palgrave Macmillan.
Parmelee AH Jr, Wenner WH & Schulz HR (1964) Infant sleep patterns: from birth to 16 weeks of age. J Pediatr 65: 576–582.
Parsons K (2003) Human thermal environments. The effects of hot, moderate and cold on human health, comfort and performance. 2nd ed. London and New York, Taylor & Francis.
Patton MQ (1990) Qualitative evaluation and research methods. Newbury Park CA, Sage Publ.

114
Patz JA, Campbell-Lendrum D, Holloway T & Foley JA (2005) Impact of regional climate change on human health. Nature 438(7066): 310–317.
Perlstein PH, Hersch C, Glueck CJ, Sutherland JM (1974) Adaptation to Cold in the First Three Days of Life. Pediatrics 54(4): 411–416.
Pocock G, Richards CD & Daly MB (1999) Human Physiology. The Basis of Medicine. New York, Oxford University Press.
Polit DF & Beck CT (2010) Essentials of nursing research: appraising evidence for nursing practice. Philadelphia PA, Wolters Kluwer Health/Lippincott Williams & Wilkins.
Pond K, Kim R, Carroquino MJ, Pirard P, Gore F, Cucu A, Nemer L, MacKay M, Smedje G, Georgellis A, Dalbokova D & Krzyzanowski M (2007) Workgroup report: developing environmental health indicators for European children: World Health Organization Working Group. Environ Health Perspect 115(9): 1376–1382.
Ponsonby AL, Dwyer T, Gibbons LE, Cochrane JA, Jones ME & McCall MJ (1992) Thermal environment and sudden infant death syndrome: case-control study. BMJ 304(6822): 277–282.
Pronczuk J & Surdu S (2008) Children's environmental health in the twenty-first century. Ann N Y Acad Sci 1140: 143–154.
Proshansky HM, Fabian AK & Kaminoff R (1983) Place-identity: physical world socialization of the self. J Environ Psychol (3): 57–83.
Puhakka K, Anttonen H, Niskanen J & Ryhänen P (1994) Calculation of mean skin temperature and changes in body heat content during paediatric anaesthesia. Br J Anaesth 72(5): 548–553.
Punto A (1991) The Development of Training and Counselling Work of Public Health Nurses in Finland from 1912–1944. University of Helsinki. Helsinki, Sairaanhoitajien koulutussäätiö.
Raatikka V-P, Hassi J, Remes J & Juopperi K (2001) Kylmäaltistus Suomessa – altistuksen yleisyys ja toiminta kylmässä. Tutkimuksia A5, taulukkoraportti, kylmätyöohjelma. Oulu, Työterveyslaitos.
Reading CL & Wien F (2009) Health inequality and social determinants of aboriginal peoples' health. National collaborating centre for aboriginal health. URI: http://www.nccah-ccnsaca/docs/social%20determinates/NCCAH-Loppie-Wien_Report pdf. Cited 2011/5/26.
Reed ES (1996) Selves, Values, Cultures. In Reed ES, Turiel E & Brown T (eds) Values and knowledge. Mahwah, New Jersey, Lawrence Erlbaum Associates, Publishers.
Reima group (2009) Pohjoismainen lasten ulkoilututkimus. URI: http://www.reima.fi/fi/ uutiset/#pohjoismainen_lasten_ulkoilututkimus. Cited 2011/5/4.
Resnik DB (2009) Environmental health research and the observer's dilemma. Environ Health Perspect 117(8): 1191–1194.
Resnik DB & Wing S (2007) Lessons learned from the Children's Environmental Exposure Research Study. Am J Public Health 97(3): 414–418.
Resnik DB & Zeldin DC (2008) Environmental health research on hazards in the home and the duty to warn. Bioethics 22(4): 209–217.

115
Richman N (1981) A community survey of characteristics of one- to two- year-olds with sleep disruptions. J Am Acad Child Psychiatry 20(2): 281–291.
Ries NM, LeGrandeur J & Caulfield T (2010) Handling ethical, legal and social issues in birth cohort studies involving genetic research: responses from studies in six countries. BMC Med Ethics 11(1): 4.
Rintamäki H (2000) Predisposing factors and prevention of frostbite. Int J Circumpolar Health 59(2): 114–121.
Rising R, Duro D, Cedillo M, Valois S & Lifshitz F (2003) Daily metabolic rate in healthy infants. J Pediatr 143(2): 180–185.
Roffwarg HP, Muzio JN & Dement W (1966) Ontogenetic development of the human sleep-dream cycle. Science 152: 604–619.
Rylander E, Pribylova H & Lind J (1972) A thermographic study of infants exposed to cold. Acta Paediatr Scand 61(1): 42–48.
Rytkönen M, Raatikka VP, Näyhä S & Hassi J (2005) Exposure to cold and the symptoms thereof. Duodecim 121(4): 419–423.
Sadeh A (1996) Evaluating night wakings in sleep-disturbed infants: a methodological study of parental reports and actigraphy. Sleep 19(10): 757–762.
Sadeh A (2004) A brief screening questionnaire for infant sleep problems: validation and findings for an Internet sample. Pediatrics 113(6): e570–7.
Sadeh A & Anders TF (1993) Infant Sleep Problems: Origins, Assessment, Interventions. Infant Ment Health J 14(1): 17–34.
Sadeh A, Mindell JA, Luedtke K & Wiegand B (2009) Sleep and sleep ecology in the first 3 years: a web-based study. J Sleep Res 18(1): 60–73.
Sadeh A, Tikotzky L & Scher A (2010) Parenting and infant sleep. Sleep Med Rev 14(2): 89–96.
Salonen AH, Kaunonen M, Åstedt-Kurki P, Järvenpää AL, & Tarkka MT (2008) Development of an internet-based intervention for parents of infants. J Adv Nurs 64(1): 60–72.
Samuelsen SO, Borge AI, Magnus P & Bakketeig LS (1993) Temporal and regional trends in fatal childhood injuries in Norway 1971–1989. Scand J Soc Med 21(1): 17–23.
Sandelowski M (2000) Combining qualitative and quantitative sampling, data collection, and analysis techniques in mixed-method studies. Res Nurs Health 23(3): 246–255.
Sattler B (2003) Children's environmental health. In Sattler B & Lipscomb J (ed) Environmental health and nursing practice. New York, Springer: 229–238.
Sauer PJ, Dane HJ & Visser HK (1984) New standards for neutral thermal environment of healthy very low birthweight infants in week one of life. Arch Dis Child 59(1): 18–22.
Scheinin H (2001) Riittääkö otoskoko? Finnanest 34(5): 566–567. Schluter PJ, Ford RP, Brown J & Ryan AP (1998) Weather temperatures and sudden infant
death syndrome: a regional study over 22 years in New Zealand. J Epidemiol Community Health 52(1): 27–33.
Schubring C (1986) Temperature regulation in healthy and resuscitated newborns immediately after birth. J Perinat Med 14(1): 27–33.

116
Schwichtenberg AJ, Anders TF, Vollbrecht M & Poehlmann J (2011) Daytime sleep and parenting interactions in infants born preterm. J Dev Behav Pediatr (32): 8–17.
Shore B (1996) Culture in mind: cognition, culture, and the problem of meaning. New York, Oxford University Press.
Silverman W, Fertig J & Berger A (1958) The influence of the thermal environment upon the survival of newly born premature infants. Pediatrics (22): 876–886.
Silverman WA, Zamelis A, Sinclair JC & Agate FJ (1964) Warm nape of the newborn. Pediatrics 33: 984–987.
Sivan Y, Shen G, Schonfeld T, Nitzan M & Nutman J (1992) Sudden infant death syndrome in the Tel Aviv and Petah Tikva districts. Isr J Med Sci 28(7): 430–435.
Skadberg BT & Markestad T (1997) Behaviour and physiological responses during prone and supine sleep in early infancy. Arch Dis Child 76(4): 320–324.
Solomon JR (1985) Pediatric burns. Crit Care Clin 1(1): 159–173. Stahl G (2000) A Model of Collaborative Knowledge-Building. In Fishman BOS (ed)
Fourth International Conference of the Learning Sciences: 70–77. Stahl G & Hesse F (2009) Paradigms of shared knowledge. Computer-Supported
Collaborative Learning (4): 365–369. Stearns PN, Rowland P & Giarnella L (1996) Children's sleep: Sketching historical change.
J Soc Hist 30(2): 345. Stephenson EA, Collins KK, Dubin AM, Epstein MR, Hamilton RM, Kertesz NJ,
Alexander ME, Cecchin F, Triedman JK, Walsh EP & Berul CI (2002) Circadian and seasonal variation of malignant arrhythmias in a pediatric and congenital heart disease population. J Cardiovasc Electrophysiol 13(10): 1009–1014.
Stevens JC & Choo KK (1998) Temperature sensitivity of the body surface over the life span. Somatosens Mot Res 15(1): 13–28.
Stocks JM, Taylor NA, Tipton MJ & Greenleaf JE (2004) Human physiological responses to cold exposure. Aviat Space Environ Med 75(5): 444–457.
Stokols D (1992) Establishing and maintaining healthy environments. Toward a social ecology of health promotion. Am Psychol 47(1): 6–22.
Stothers JK (1981) Head insulation and heat loss in the newborn. Arch Dis Child 56(7): 530–534.
Stothers JK & Warner RM (1984) Thermal balance and sleep state in the newborn. Early Hum Dev 9(4): 313–322.
Strimer R, Adelson L & Oseasohn R (1969) Epidemiologic features of 1,134 sudden, unexpected infant deaths. A study in the Greater Cleveland Area from 1956 to 1965. JAMA 209(10): 1493–1497.
Super CM, Harkness S, van Tijen N, van der Vlugt E, Fintelman M & Dijkstra J (1996) The three R's of Dutch Childrearing and the Socialization of Infant Arousal. In Harkness S & Super CM (ed) Parents' Cultural Belief Systems: Their Origins, Expressions, and Consequences. New York, NY, Guilford Press: 447–466.
Svedberg LE, Stener-Victorin E, Nordahl G & Lundeberg T (2005) Skin temperature in the extremities of healthy and neurologically impaired children. Eur J Paed Neurol (9): 347–354.

117
Taanila AM, Hurtig TM, Miettunen J, Ebeling HE & Moilonen IK (2009) Association between ADHD symptoms and adolescents' psychosocial well-being: a study of the Northern Finland Birth Cohort 1986. Int J Circumpolar Health 68(2): 133–144.
Tashakkori A & Teddlie C (2008) Quality of inferences in mixed methods research: Calling for an integrative framework. In Bergman MM (ed) Advances in mixed methods research. Theories and applications. London, Sage Publications: 113–114.
Tashakkori A & Teddlie C (1998) Mixed methodology: combining qualitative and quantitative approaches. Thousand Oaks (Calif.), Sage.
Taveras EM, Rifas-Shiman SL, Oken E, Gunderson EP & Gillman MW (2008) Short sleep duration in infancy and risk of childhood overweight. Arch Pediatr Adolesc Med 162(4): 305–311.
Taylor S & Repetti R (1997) Health psychology: What is an unhealthy environment and how does it get under the skin. Annu Rev Psychol 48: 411–447.
Telliez F, Bach V, Dewasmes G, Leke A & Libert J-P (1998) Sleep modifications during cool acclimation in human neonates. Neurosci Lett (245): 25–28.
Telliez F, Bach V, Krim G & Libert JP (1997) Consequences of a small decrease of air temperature from thermal equilibrium on thermoregulation in sleeping neonates. Med Biol Eng Comput 35(5): 516–520.
Telliez F, Chardon K, Leke A, Cardot V, Tourneux P & Bach V (2004) Thermal acclimation of neonates to prolonged cool exposure as regards sleep stages. J Sleep Res 13(4): 337–343.
Thomas KA & Burr R (2002) Preterm infant temperature circadian rhythm: possible effect of parental cosleeping. Biol Res Nurs 3(3): 150–159.
Thunström M (1999) Severe sleep problems among infants in a normal population in Sweden: prevalence, severity and correlates. Acta Paediatr 88(12): 1356–1363.
Thunström M (2002) Severe sleep problems in infancy associated with subsequent development of attention-deficit/hyperactivity disorder at 5.5 years of age. Acta Paediatr 91(5): 584–592.
Tikotzky L, DE Marcas G, Har-Toov J, Dollberg S, Bar-Haim Y & Sadeh A (2010) Sleep and physical growth in infants during the first 6 months. J Sleep Res 19: 103–110.
Tikotzky L & Sadeh A (2001) Sleep Patterns and Sleep Disruptions in Kindergarten Children. J Clin Child Psychol 30(4): 581–591.
Tikotzky L & Sadeh A (2009) Maternal Sleep-Related Cognitions and Infant Sleep: A Longitudinal Study From Pregnancy Through the 1st Year. Child Dev 80(3): 860–874.
Tilastokeskus (2011) Väestö. URI: http://www.stat.fi/tup/suoluk/suoluk_vaesto.html #lapset. Cited 2011/5/4.
Touchette E, Petit D, Paquet J, Boivin M, Japel C, Tremblay RE & Montplaisir JY (2005) Factors Associated With Fragmented Sleep at Night Across Early Childhood. Arch Pediatr Adolesc Med 159(3): 242–249.
Tourula M, Isola A & Hassi J (2008) Children sleeping outdoors in winter: parents' experiences of a culturally bound childcare practice. Int J Circumpolar Health 67(2–3): 269–278.

118
Tronick EZ, Thomas RB & Daltabuit M (1994) The Quechua manta pouch: a caretaking practice for buffering the Peruvian infant against the multiple stressors of high altitude. Child Dev 65(4): 1005–1013.
Tsai YY, Yang YH, Yu HH, Wang LC, Lee JH & Chiang BL (2010) Fifteen-year experience of pediatric-onset mixed connective tissue disease. Clin Rheumatol 29(1): 53–58.
Tsogt B, Manaseki-Holland S, Pollock J, Blair PS & Fleming PJ (2006) The development of thermoregulation in a harsh environment: a prospective controlled study of the effects of swaddling on infants' thermal balance in a Mongolian winter. Early Hum Dev 82: 621.
Tsuzuki K, Tochihara Y, Ohnaka T (2008) Comparison of thermal responses between yung children (1- to 3-year-old) and mothers during cold exposure. Eur J Appl Physiol (103): 697–705.
Tuohy PG & Tuohy RJ (1990) The overnight thermal environment of infants. N Z Med J 103(883): 36–38.
Uhari M & Nieminen P (2001) Epidemiologia ja biostatistiikka. Helsinki, Duodecim. van Sleuwen BE, Engelberts AC, Boere-Boonekamp MM, Kuis W, Schulpen TW &
L'Hoir MP (2007) Swaddling: a systematic review. Pediatrics 120(4): e1097–106. Varjoranta P (1992) Terveyssisarten kotikäynnit Suomalaisessa lastenneuvolatyössä
vuosina 1944–1972: Syöpäläisten torjunnasta keskosten huoltoon. Master´s thesis, University of Kuopio.
Vege A, Rognum TO & Opdal SH (1998) SIDS–changes in the epidemiological pattern in eastern Norway 1984–1996. Forensic Sci Int 93(2–3): 155–166.
Vennemann MM, Bajanowski T, Brinkmann B, Jorch G, Sauerland C, Mitchell EA & GeSID Study Group (2009) Sleep environment risk factors for sudden infant death syndrome: the German sudden infant death syndrome study. Pediatrics 123(4): 1162–1170.
von Heimburg D, Noah EM, Sieckmann UP & Pallua N (2001) Hyperbaric oxygen treatment in deep frostbite of both hands in a boy. Burns 27(4): 404–408.
Vuori A & Åstedt-Kurki P (2009) Well-being of mothers with children in Finnish low-income families–the mother's point of view. Scand J Caring Sci 23(4): 748–756.
Vuorinen HS, Makela M, Tuomikoski H & Floman P (1991) Core-periphery differences in children's health and use of general practitioner services in Finland from 1964 to 1987. Soc Sci Med 33(9): 1023–1028.
Wailoo MP, Petersen SA & Whittaker H (1990) Disturbed nights and 3–4 month old infants: the effects of feeding and thermal environment. Arch Dis Child 65(5): 499–501.
Wailoo MP, Petersen SA, Whittaker H & Goodenough P (1989a) The thermal environment in which 3–4 month old infants sleep at home. Arch Dis Child 64(4): 600–604.
Wailoo MP, Petersen SA, Whittaker H, Goodenough P (1989b) Sleeping body temperatures in 3–4 month old infants. Arch Dis Child (64): 596–599.

119
Wake M, Morton-Allen E, Poulakis Z, Hiscock H, Gallagher S & Oberklaid F (2006) Prevalence, stability, and outcomes of cry-fuss and sleep problems in the first 2 years of life: prospective community-based study. Pediatrics 117(3): 836–842.
Walkosz B, Voeks J, Andersen P, Scott M, Buller D, Cutter G & Dignan M (2007) Randomized trial on sun safety education at ski and snowboard schools in western North America. Pediatr Dermatol 24(3): 222–229.
Ward TM, Gay C, Alkon A, Anders TF & Lee KA (2008) Nocturnal sleep and daytime nap behaviors in relation to salivary cortisol levels and temperament in preschool-age children attending child care. Biol Res Nurs 9(3): 244–253.
Watson L, Potter A, Gallucci R & Lumley J (1998) Is baby too warm? The use of infant clothing, bedding and home heating in Victoria, Australia. Early Hum Dev 51(2): 93–107.
Wehrli NE, Bural G, Houseni M, Alkhawaldeh K, Alavi A & Torigian DA (2007) Determination of age-related changes in structure and function of skin, adipose tissue, and skeletal muscle with computed tomography, magnetic resonance imaging, and positron emission tomography. Semin Nucl Med 37(3): 195–205.
Weisner (2002) Ecocultural Understanding of Children's Developmental Pathways. Hum Dev 45(4): 275–281.
Weissbluth M (1995) Naps in children: 6 months-7 years. Sleep 18(2): 82–87. Welles-Nyström B, New R & Richman A (1994) The "good mother": A comparative study
of Swedish, Italian and American maternal behavior and goals. Scand J Caring Sci 8(2): 81–86.
Wells NM & Lekies KS (2006) Nature and the Life Course: Pathways from Childhood Nature Experiences to Adult Environmentalism. CYE 16(1): 1–24.
Werner J & Reents T (1980) A Contribution to the Topography of Temperature Regulation in Man. Eur J Appl Physiol (45): 87–94.
Weston WL & Morelli JG (2000) Childhood pernio and cryoproteins. Pediatr Dermatol 17(2): 97–99.
Wicker AW (1972) Processes which mediate behavior-environment congruence. Behav Sci (17): 265–277.
Wigfield RE, Fleming PJ, Azaz YE, Howell TE, Jacobs DE, Nadin PS, McCabe R & Stewart AJ (1993) How much wrapping do babies need at night? Arch Dis Child 69(2): 181–186.
Wiggs L (2009) Behavioural aspects of children's sleep. Arch Dis Child 94(1): 59–62. Wiley A (2004) Ecology of High-Altitude Infancy : A Biocultural Perspective. West
Nyack, NY, USA, Cambridge University Press. Williams SM, Taylor BJ & Mitchell EA (1996) Sudden infant death syndrome: insulation
from bedding and clothing and its effect modifiers. The National Cot Death Study Group. Int J Epidemiol 25(2): 366–375.
Willows ND & Gray-Donald K (2002) Blood lead concentrations and iron deficiency in Canadian aboriginal infants. Sci Total Environ 289(1–3): 255–260.
Wilson CA & Chu MS (2005) Thermal insulation and SIDS-an investigation of selected 'Eastern' and 'Western' infant bedding combinations. Early Hum Dev 81(8): 695–709.

120
Wilson CA, Taylor BJ, Laing RM, Williams SM & Mitchell EA (1994) Clothing and bedding and its relevance to sudden infant death syndrome: further results from the New Zealand Cot Death Study. J Paediatr Child Health 30(6): 506–512.
Winch PJ, Alam MA, Akther A, Afroz D, Ali NA, Ellis AA, Baqui AH, Darmstadt GL, El Arifeen S, Seraji MH & Bangladesh PROJAHNMO Study Group (2005) Local understandings of vulnerability and protection during the neonatal period in Sylhet District, Bangladesh: a qualitative study. Lancet 366(9484): 478–485.
Wissler EH (2008) A quantitative assessment of skin blood flow in humans. Eur J Appl Physiol 104(2): 145–157.
World Health Organization (1996) Safe motherhood. Mother - Baby Package: implementing safe motherhood in countries. Maternal Health and Safe Motherhood Programme. URI: http://whqlibdoc.who.int/hq/1994/WHO_FHE_MSM_94.11_Rev.1.pdf. Cited 2011/5/4.
World Health Organization (1997) Safe Motherhood. Thermal Protection of the Newborn: a practical guide. URI: http://whqlibdoc.who.int/hq/1997/WHO_RHT_MSM_97.2.pdf. Cited 2011/5/4.
World Medical Association (2008) World Medical Association Declaration of Helsinki. Ethical Principles for Medical Research Involving Human Subjects. URI: http://www.wma.net/en/30publications/10policies/b3/17c.pdf. Cited 2010/12/10.
Ylppö A (1921) Lapsista ja vanhemmista: neljä esitelmää. Helsinki, Kustannusosakeyhtiö Otava.
Ylppö A (1939) Äiti pikkulapsensa hoitajana ja ruokkijana. Helsinki, Kustannusosakeyhtiö Otava.
Ylppö A (1947) Miksi lapsi tarvitsee ulkoilmaa? Terveydenhoitolehti 59(2): 32–34. Young TK (2008) Circumpolar Health Indicators: Sources, Data, and Maps. Introduction.
Circumpolar Health Suppl (3): 10–16. Zeitoun M, Wilk B, Matsuzaka A, Knöpfli B, Wilson B, Bar-Or O (2004) Facial cooling
enhances exercise-induced bronchoconstriction in asthmatic children. Med Sci Sport Exerc (36): 767–771.

121
Appendix Clothing insulation tests and information about clothing
CL
OT
HIN
GIN
SU
LA
TIO
NT
ES
TS
:
B1.
AB
BR
EV
IAT
ION
S:
Type
ofcl
othe
s:L
isto
fcl
othe
s:U
1un
derc
loth
es1,
2,3
U1 UU1
2.
U2
unde
rclo
thes
1,2,
3,6
Bbl
anke
t5
M1
mid
-lay
er7,
8,12
,13,
M2
mid
-lay
er7,
8,9,
10,1
1,12
,13
U1
3.M
1
U1
M1
O1
4.
M3
mid
-lay
er7,
10,1
1,13
O1
oute
rwea
r14
a,15
b,17
O2
oute
rwea
r7,
14a,
15b
O3
oute
rwea
r14
b,15
a,16
,17
C18
U1
M1
O1
C1
5.
OC
C1
cove
rs18
C2
cove
rs19
Ssh
eeps
kin
20P
pram
21
U1
M1
O1
C1
6.P
U2
O2
C1
P7.
gabgnipeels.81
tiusydob.1ffu
mtoofretni
wdeddap.91
yppanelbasopsid.2
nikspeehs.02sgniggel
detoof.3marp.12
tiusrep
mor.4
U2
M2
O3
C2
S8.
UM
P
OC
P
5.bl
anke
tand
duve
tcov
er6.
sock
s7.
mit
tens
8.w
oole
nso
cks
9l
itt
U2
M3
9.O
3C
1P
9.w
oole
nm
itte
n10
.pla
ysui
t(s
hirt
and
pant
s)11
.ove
rall
wit
hw
addi
ng12
.woo
len
card
igan
and
pant
s13
bala
clav
aha
t13
.bal
acla
vaha
t14
a.sn
owsu
it14
b.w
arm
ersn
owsu
it15
a.in
sula
ted
hat
15b
woo
len
hat
15b.
woo
len
hat
16.i
nsul
ated
mit
tens
17.i
nsul
ated
boot
ies

122
Un
der
clot
hes
:
LIS
TO
FC
LO
TH
ES
4ro
mpe
rsu
it
1.bo
dysu
it•
wei
ght:
61.1
g•
60cm
•10
0%
cott
on
4.ro
mpe
rsu
it•
wei
ght:
78.4
g•
60cm
•10
0%
cott
on
•10
0%
cott
on
2.di
spos
able
napp
y
3.fo
oted
legg
ings
•w
eigh
t:44
.3g
•60
cm
5.bl
anke
tand
duve
tcov
er•
wei
ght:
671.
3g
•bl
anke
tfi
llin
g:10
0%
•10
0%
cott
onbl
anke
tfi
llin
g:10
0%
poly
este
r,•
cove
r:52
%po
lyes
ter,
48%
cott
on•
blan
ketc
over
:100
%co
tton

123
Mid
-lay
er:
6.so
cks
•w
eigh
t:19
.7g
•si
ze:1
9-21
•78
%co
tton
,20
%po
lyam
ide,
lycr
a
7.gl
oves
•w
eigh
t:18
.7g
78%
20%
lid
l
9.w
oole
nm
itte
n•
wei
ght:
40.7
g
•78
%co
tton
,20
%po
lyam
ide,
lycr
a
8.w
oole
nso
cks
•w
eigh
t:38
.0g
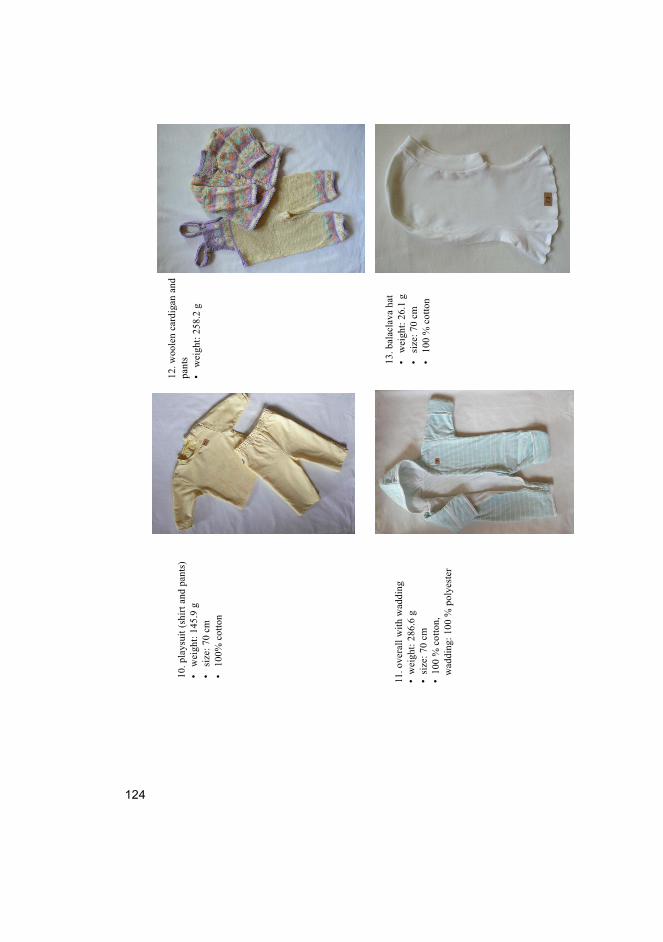
124
12.w
oole
nca
rdig
anan
dg
pant
s•
wei
ght:
258.
2g
10.p
lays
uit
(shi
rtan
dpa
nts)
•w
eigh
t:14
5.9
g•
size
:70
cm•
100%
cott
on
11.o
vera
llw
ith
wad
ding
•w
eigh
t:28
6.6
g•
size
:70
cm
13.b
alac
lava
hat
•w
eigh
t:26
.1g
•si
ze:7
0cm
•10
0%
cott
on•
100
%co
tton
,w
addi
ng:1
00%
poly
este
r

125
Ou
terw
ear:
14a
snow
suit
15a.
insu
late
dha
t14
a.sn
owsu
it•
wei
ght:
470.
5g
•si
ze:6
8cm
•co
ver:
100
%po
lyes
ter,
fill
ing:
100
%po
lyes
ter
•w
eigh
t:62
.6g
•si
ze:5
0•
cove
r:10
0%
poly
este
r,fi
llin
g:10
0%
poly
este
r,fi
llin
g:10
0%
poly
este
r,li
ning
:50
%po
lyes
ter,
50%
cott
on
lini
ng:
50%
poly
este
r,50
%co
tton
bi
14b.
war
mer
snow
suit
•w
eigh
t:66
7.0
g•
size
:68
cm
15b.
woo
len
hat
•w
eigh
t:36
.1g

126
16.i
nsul
ated
mit
tens
•w
eigh
t:46
.9g
•si
ze:1
•co
ver:
100
%po
lyes
ter,
fill
ing:
100
%po
lyes
ter,
lini
ng:5
0%
poly
este
r,50
%co
tton
17in
sula
ted
boot
ies
17.i
nsul
ated
boot
ies
•w
eigh
t:58
.5g
•si
ze:1
•co
ver:
100
%po
lyes
ter,
fill
ing:
100
%po
lyes
ter,
fill
ing:
100
%po
lyes
ter,
lini
ng:5
0%
poly
este
r,50
%co
tton
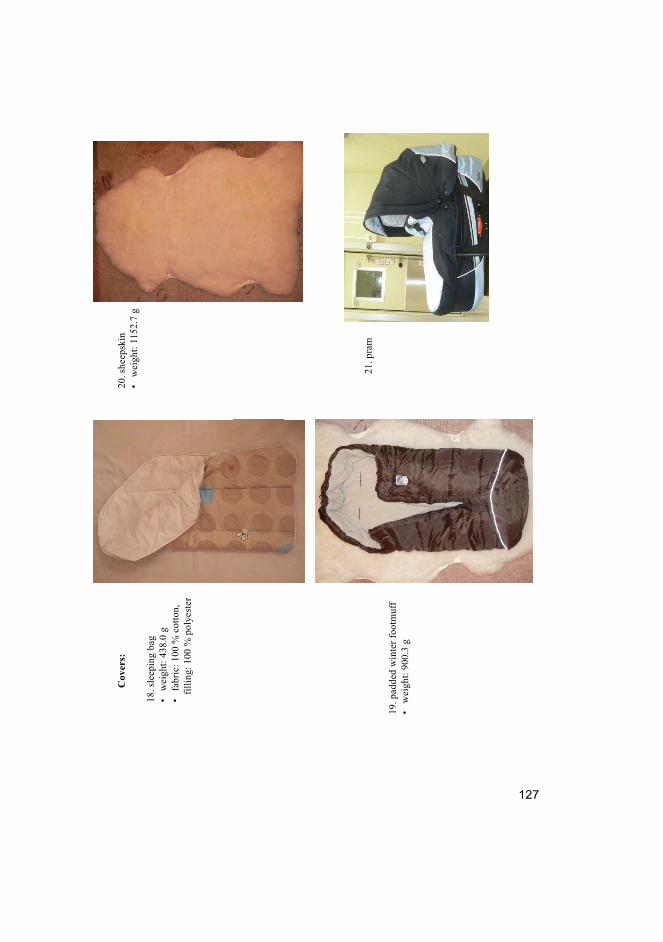
127
Cov
ers:
20.s
heep
skin
ih
1152
7
18.s
leep
ing
bag
•w
eigh
t:43
8.0
g•
fabr
ic:1
00%
cott
on,
•w
eigh
t:11
52.7
g
fill
ing:
100
%po
lyes
ter
21.p
ram
19.p
adde
dw
inte
rfo
otm
uff
•w
eigh
t:90
0.3
g

128

129
Original publications
I Tourula M, Isola A & Hassi J (2008) Children sleeping outdoors in winter: Parents’ experiences of a culturally bound childcare practice. International Journal of Circumpolar Health 67(2–3): 269–278.
II Tourula M, Isola A, Hassi J, Bloigu R & Rintamäki H (2010) Infants sleeping outdoors in a northern winter climate: skin temperature and duration of sleep. Acta Paediatrica 99(9): 1411–1417.
III Tourula M, Fukazawa T, Isola A, Hassi J, Tochihara Y & Rintamäki H (2011) Evaluation of the thermal insulation of clothing of infants sleeping outdoors in Northern winter. European Journal of Applied Physiology 111(4): 633–640.
IV Tourula M, Pölkki T & Isola A (2011) The cultural meaning of children sleeping outdoors in Finnish winter: A qualitative study from the viewpoint of mothers. Manuscript.
Reprinted with permission from International Association of Circumpolar Health
Publishers (I), John Wiley and Sons (II), Springer (III).
Original publications are not included in the electronic version of the dissertation.

130

A C T A U N I V E R S I T A T I S O U L U E N S I S
Book orders:Granum: Virtual book storehttp://granum.uta.fi/granum/
S E R I E S D M E D I C A
1120. Venhola, Mika (2011) Vesicoureteral reflux in children
1121. Naillat, Florence (2011) Roles of Wnt4/5a in germ cell differentiation and gonaddevelopment & ErbB4 in polarity of kidney epithelium
1122. Nurmenniemi, Sini (2011) Analysis of cancer cell invasion with novel in vitromethods based on human tissues
1123. Kangas-Kontio, Tiia (2011) Genetic background of HDL-cholesterol andatherosclerosis : Linkage and case-control studies in the Northern Finnishpopulation
1124. Cederberg, Henna (2011) Relationship of physical activity, unacylated ghrelin andgene variation with changes in cardiovascular risk factors during military service
1125. Miller, Brian (2011) Paternal age, psychosis, and mortality : The Northern Finland1966 Birth Cohort, Helsinki 1951–1960 Schizophrenia Cohort, and FinnishNonaffective Psychosis Cohort
1126. Tolvanen, Mimmi (2011) Changes in adolescents’ oral health-related knowledge,attitudes and behavior in response to extensive health promotion
1127. Pirilä-Parkkinen, Kirsi (2011) Childhood sleep-disordered breathing – dentofacialand pharyngeal characteristics
1128. Thevenot, Jérôme (2011) Biomechanical assessment of hip fracture : developmentof finite element models to predict fractures
1129. Moilanen, Kristiina (2011) Diagnostics and determinants of schizophrenia : TheNorthern Finland 1966 Birth Cohort Study
1130. Haapsamo, Mervi (2011) Low-dose aspirin therapy in IVF and ICSI patients
1131. Hyttinen, Laura (2011) Long-term effects of the cholesterol level and its drugtreatment
1132. Hannula, Samuli (2011) Hearing among older adults–an epidemiological study
1133. Paananen, Markus (2011) Multi-site musculoskeletal pain in adolescence:occurrence, determinants, and consequences
1134. Kaustinen, Teija (2011) Oulu-hoitoisuusluokitus ja hoitohenkilökunnan ajankäyttöhoitotyön laatuvaatimusten näkökulmasta
1136. Tölli, Hanna (2011) Reindeer-derived protein extract in the healing of bonedefects : Evaluation of various carrier materials and delivery systems

ABCDEFG
UNIVERS ITY OF OULU P.O.B . 7500 F I -90014 UNIVERS ITY OF OULU F INLAND
A C T A U N I V E R S I T A T I S O U L U E N S I S
S E R I E S E D I T O R S
SCIENTIAE RERUM NATURALIUM
HUMANIORA
TECHNICA
MEDICA
SCIENTIAE RERUM SOCIALIUM
SCRIPTA ACADEMICA
OECONOMICA
EDITOR IN CHIEF
PUBLICATIONS EDITOR
Senior Assistant Jorma Arhippainen
Lecturer Santeri Palviainen
Professor Hannu Heusala
Professor Olli Vuolteenaho
Senior Researcher Eila Estola
Director Sinikka Eskelinen
Professor Jari Juga
Professor Olli Vuolteenaho
Publications Editor Kirsti Nurkkala
ISBN 978-951-42-9666-6 (Paperback)ISBN 978-951-42-9667-3 (PDF)ISSN 0355-3221 (Print)ISSN 1796-2234 (Online)
U N I V E R S I TAT I S O U L U E N S I S
MEDICA
ACTAD
D 1137
ACTA
Marjo Tourula
OULU 2011
D 1137
Marjo Tourula
THE CHILDCARE PRACTICE OF CHILDREN’S DAYTIME SLEEPING OUTDOORSIN THE CONTEXT OF NORTHERN FINNISH WINTER
UNIVERSITY OF OULU,FACULTY OF MEDICINE,INSTITUTE OF HEALTH SCIENCES, NURSING SCIENCE,INSTITUTE OF BIOMEDICINE, DEPARTMENT OF PHYSIOLOGY;FINNISH INSTITUTE OF OCCUPATIONAL HEALTH, OULU;NORTHERN OSTROBOTHNIA HOSPITAL DISTRICT;KYUSHU UNIVERSITY, FACULTY OF DESIGN, DEPARTMENT OF HUMAN SCIENCE