le leucemie - chped.itchped.it/gico/ferrara_2013/la malattia neoplastica...
TRANSCRIPT

LE LEUCEMIE DELL’ADOLOSCENTE/GIOVANE ADULTO:
DALLA PARTE DEL BAMBINO Andrea Pession
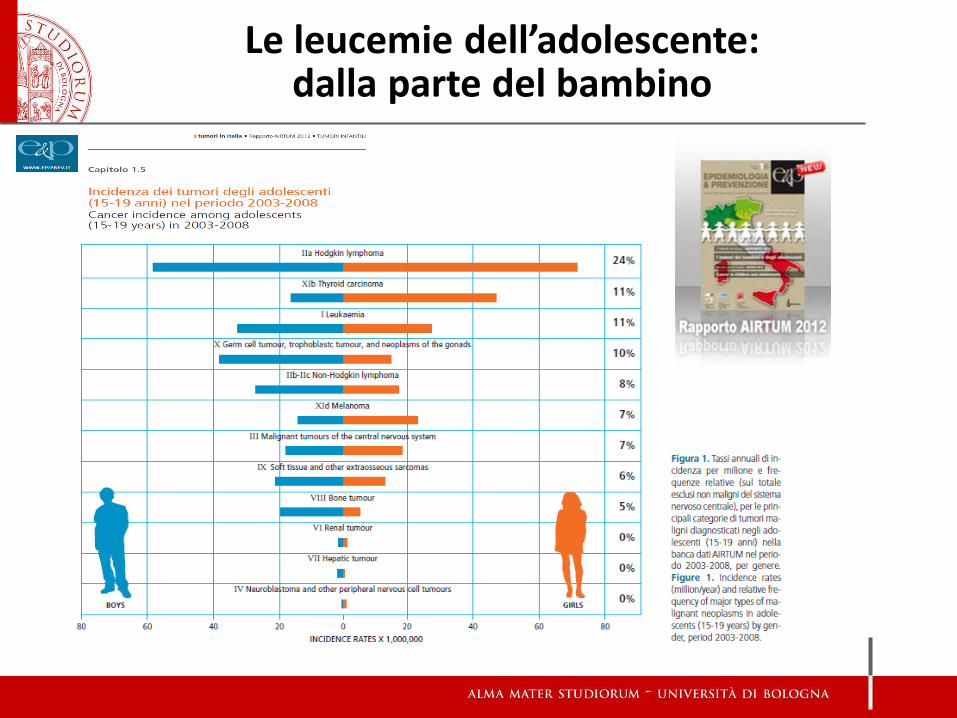
Le leucemie dell’adolescente: dalla parte del bambino
A remarkable triumph of modern medicine is the cure of most forms of
childhood cancer. By the turn of the century, it is estimated that 1 in 900
persons between 21 and 45 years of age will be a survivor of childhood
cancer. The defining event that initiated this awesome achievement
was the cure of acute lymphocytic leukemia.
The Cure of Childhood Leukemia: Into the age of miracles
N Engl J Med 1996; 334:275 January 25, 1996
Acute Lymphoblastic Leukemia
La LAL dell’adolescente: dalla parte del bambino
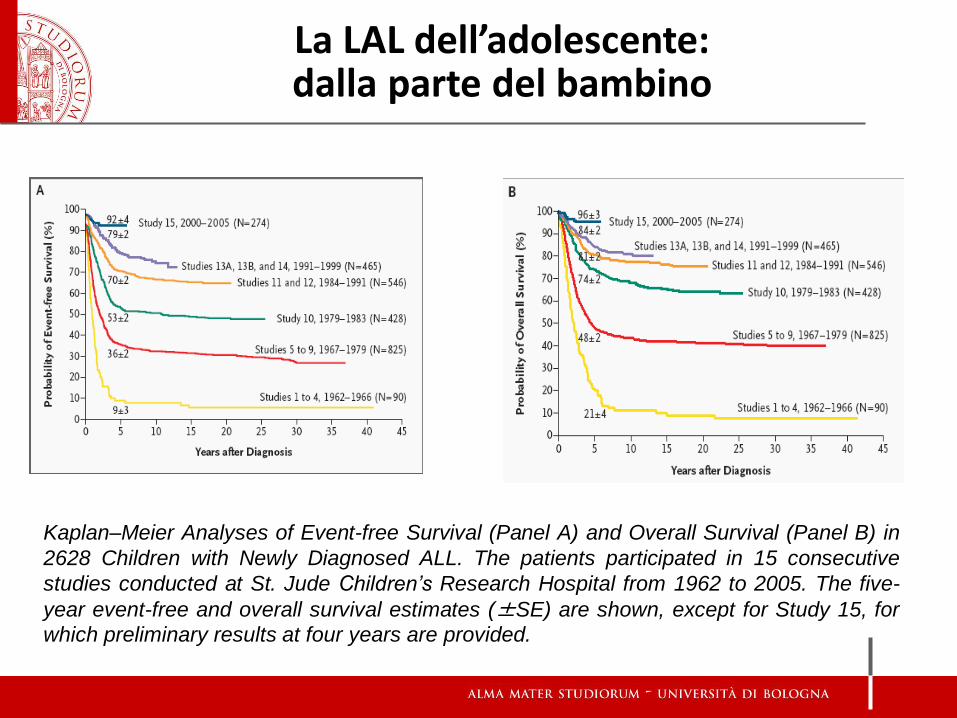
Kaplan–Meier Analyses of Event-free Survival (Panel A) and Overall Survival (Panel B) in
2628 Children with Newly Diagnosed ALL. The patients participated in 15 consecutive
studies conducted at St. Jude Children’s Research Hospital from 1962 to 2005. The five-
year event-free and overall survival estimates (±SE) are shown, except for Study 15, for
which preliminary results at four years are provided.
La LAL dell’adolescente: dalla parte del bambino
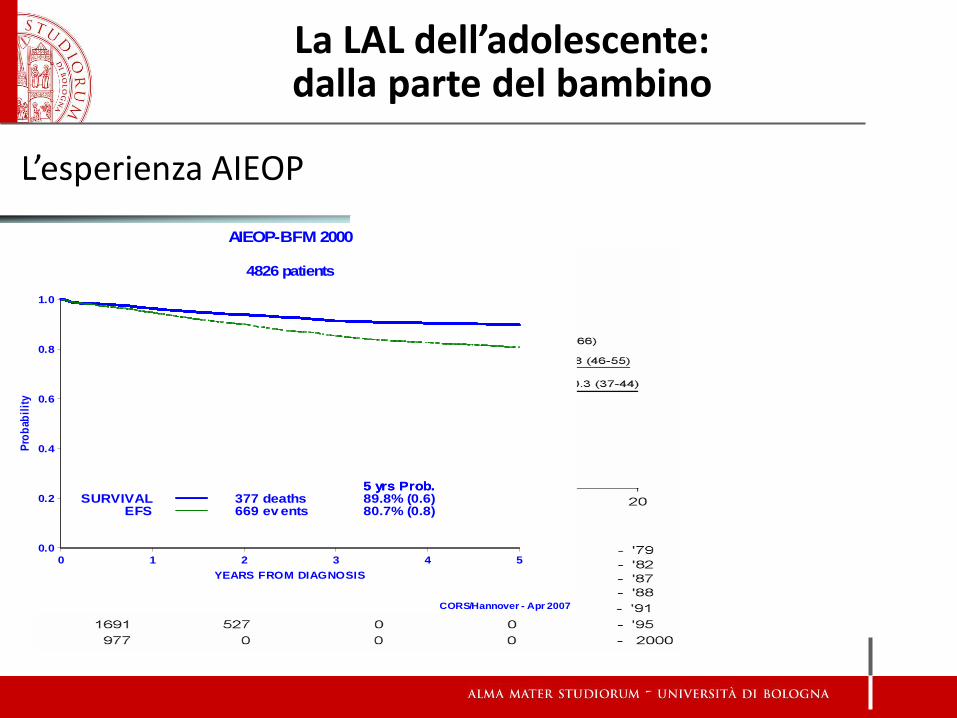
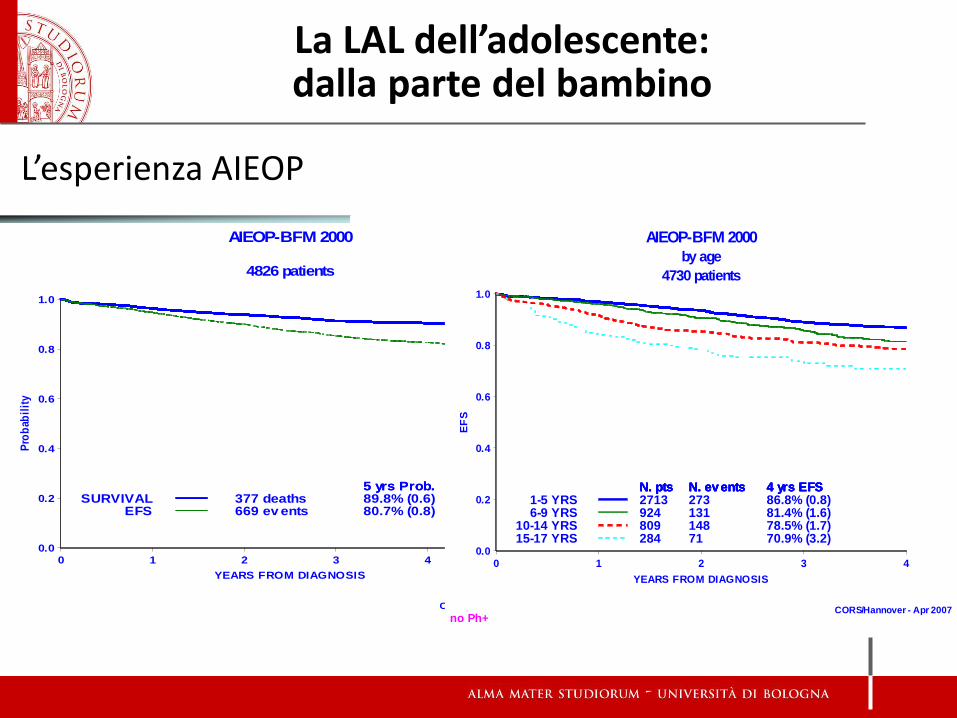
L’esperienza AIEOP
377 deaths 89.8% (0.6)5 yrs Prob.
SURVIVAL669 ev ents 80.7% (0.8)
5 yrs Prob.
EFS
AIEOP-BFM 2000
4826 patients
CORS/Hannover - Apr 2007
Pro
bab
ilit
y
0.0
0.2
0.4
0.6
0.8
1.0
YEARS FROM DIAGNOSIS
0 1 2 3 4 5
La LAL dell’adolescente: dalla parte del bambino
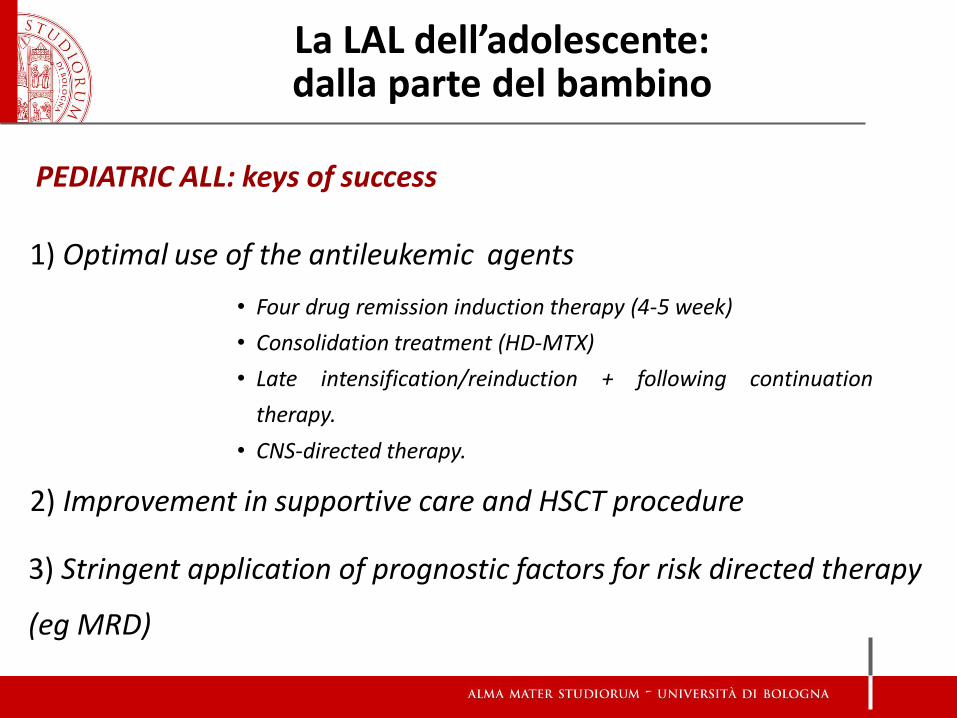
1) Optimal use of the antileukemic agents
2) Improvement in supportive care and HSCT procedure
3) Stringent application of prognostic factors for risk directed therapy
(eg MRD)
• Four drug remission induction therapy (4-5 week)
• Consolidation treatment (HD-MTX)
• Late intensification/reinduction + following continuation
therapy.
• CNS-directed therapy.
PEDIATRIC ALL: keys of success
La LAL dell’adolescente: dalla parte del bambino
La LAL dell’adolescente: dalla parte del bambino
Le leucemie dell’adolescente: dalla parte del bambino
L’esperienza AIEOP
377 deaths 89.8% (0.6)5 yrs Prob.
SURVIVAL669 ev ents 80.7% (0.8)
5 yrs Prob.
EFS
AIEOP-BFM 2000
4826 patients
CORS/Hannover - Apr 2007
Pro
bab
ilit
y
0.0
0.2
0.4
0.6
0.8
1.0
YEARS FROM DIAGNOSIS
0 1 2 3 4 5
La LAL dell’adolescente: dalla parte del bambino
2713N. pts
273N. ev ents
86.8% (0.8)4 yrs EFS
1-5 YRS924
N. pts
131
N. ev ents
81.4% (1.6)
4 yrs EFS
6-9 YRS809
N. pts
148
N. ev ents
78.5% (1.7)
4 yrs EFS
10-14 YRS284
N. pts
71
N. ev ents
70.9% (3.2)
4 yrs EFS
15-17 YRS
AIEOP-BFM 2000
by age
4730 patients
no Ph+CORS/Hannover - Apr 2007
EF
S
0.0
0.2
0.4
0.6
0.8
1.0
YEARS FROM DIAGNOSIS
0 1 2 3 4
ALL – ADOLESCENTS vs. YOUNGER CHILDREN
Higher incidence of T cell immunophenotype:
25% vs 10%
Higher incidence of PH+ ALL: 1.3-3.3% vs >3.5
Lower incidence of hyperdiploidy and TEL-
AML1 translocations
AVN a significant complication
La LAL dell’adolescente: dalla parte del bambino
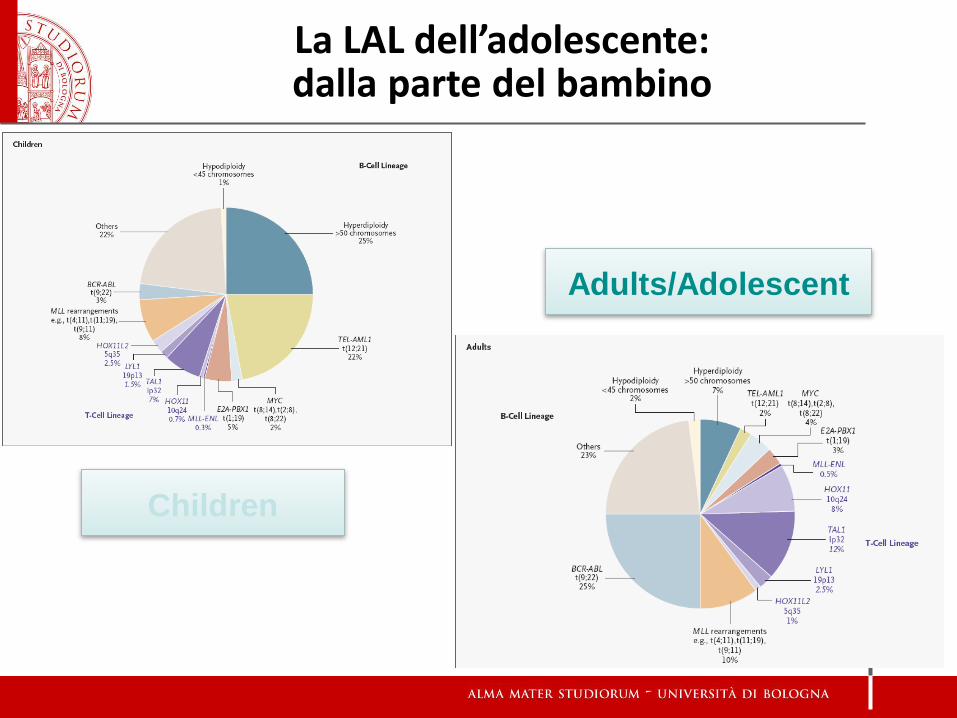
Children
Adults/Adolescent
La LAL dell’adolescente: dalla parte del bambino
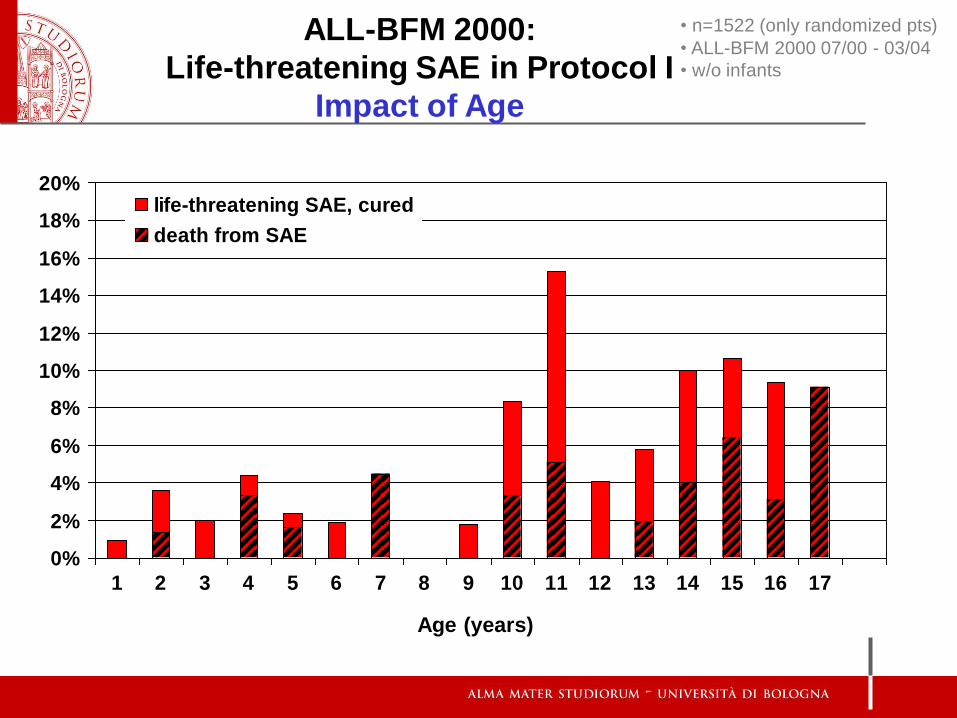
• n=1522 (only randomized pts)
• ALL-BFM 2000 07/00 - 03/04
• w/o infants
ALL-BFM 2000:
Life-threatening SAE in Protocol I
Impact of Age
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
life-threatening SAE, cured
death from SAE
Age (years)
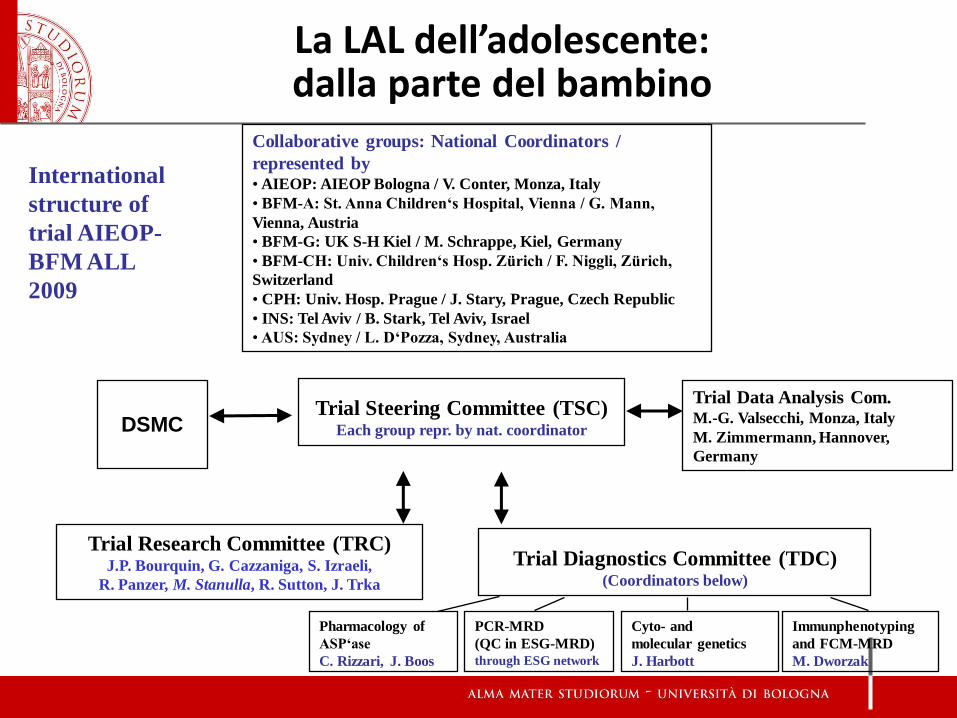
Trial Steering Committee (TSC) Each group repr. by nat. coordinator
Trial Data Analysis Com. M.-G. Valsecchi, Monza, Italy
M. Zimmermann, Hannover,
Germany
International
structure of
trial AIEOP-
BFM ALL
2009
DSMC
Trial Diagnostics Committee (TDC) (Coordinators below)
Collaborative groups: National Coordinators /
represented by • AIEOP: AIEOP Bologna / V. Conter, Monza, Italy
• BFM-A: St. Anna Children‘s Hospital, Vienna / G. Mann,
Vienna, Austria
• BFM-G: UK S-H Kiel / M. Schrappe, Kiel, Germany
• BFM-CH: Univ. Children‘s Hosp. Zürich / F. Niggli, Zürich,
Switzerland
• CPH: Univ. Hosp. Prague / J. Stary, Prague, Czech Republic
• INS: Tel Aviv / B. Stark, Tel Aviv, Israel
• AUS: Sydney / L. D‘Pozza, Sydney, Australia
PCR-MRD
(QC in ESG-MRD)
through ESG network
Cyto- and
molecular genetics
J. Harbott
Immunphenotyping
and FCM-MRD
M. Dworzak
Pharmacology of
ASP‘ase
C. Rizzari, J. Boos
Trial Research Committee (TRC) J.P. Bourquin, G. Cazzaniga, S. Izraeli,
R. Panzer, M. Stanulla, R. Sutton, J. Trka
La LAL dell’adolescente: dalla parte del bambino
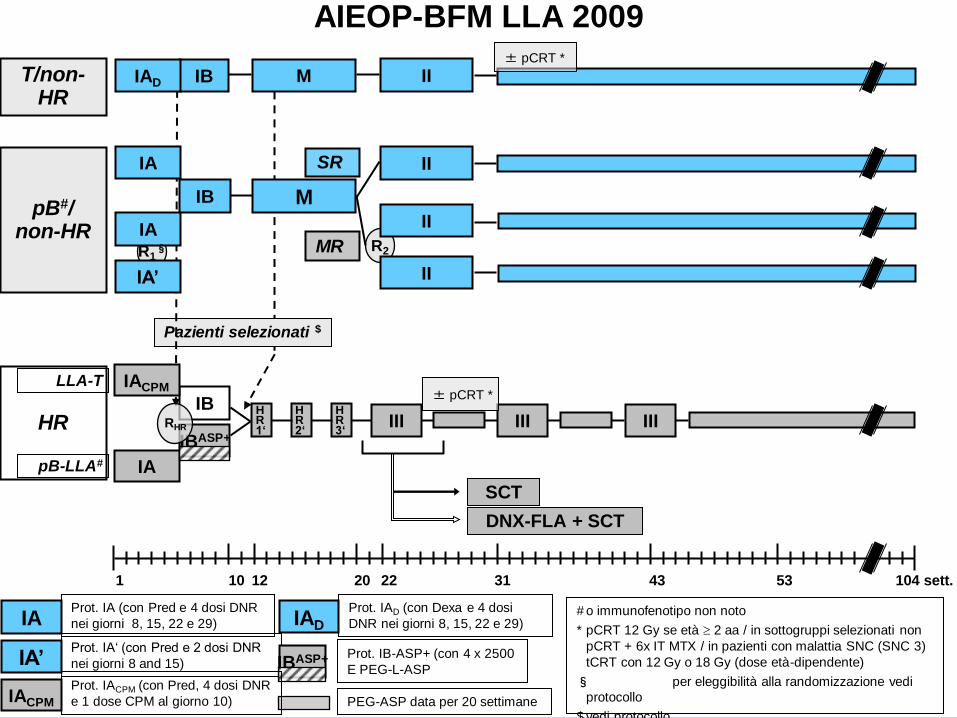
AIEOP-BFM LLA 2009
PEG-ASP data per 20 settimane
Prot. IB-ASP+ (con 4 x 2500
E PEG-L-ASP
Prot. IA‘ (con Pred e 2 dosi DNR
nei giorni 8 and 15)
Prot. IA (con Pred e 4 dosi DNR
nei giorni 8, 15, 22 e 29)
IBASP+
IAD IA
IA’
Prot. IAD (con Dexa e 4 dosi
DNR nei giorni 8, 15, 22 e 29)
IACPM
Prot. IACPM (con Pred, 4 dosi DNR
e 1 dose CPM al giorno 10)
T/non-HR
pB#/ non-HR
53 104 sett. 12 1 22 31 43 20 10
Pazienti selezionati $
M
M
HR 1‘
HR 2‘
HR 3‘
MR
II
II
R2
II SR
II
SCT
DNX-FLA + SCT
III
± pCRT *
III III HR
LLA-T
pB-LLA#
± pCRT *
# o immunofenotipo non noto
* pCRT 12 Gy se età 2 aa / in sottogruppi selezionati non
pCRT + 6x IT MTX / in pazienti con malattia SNC (SNC 3)
tCRT con 12 Gy o 18 Gy (dose età-dipendente)
§ per eleggibilità alla randomizzazione vedi
protocollo
$ vedi protocollo
IBASP+
IB
IB IAD
IA
IB
IA’
IA
R1§
IA
IACPM
RHR
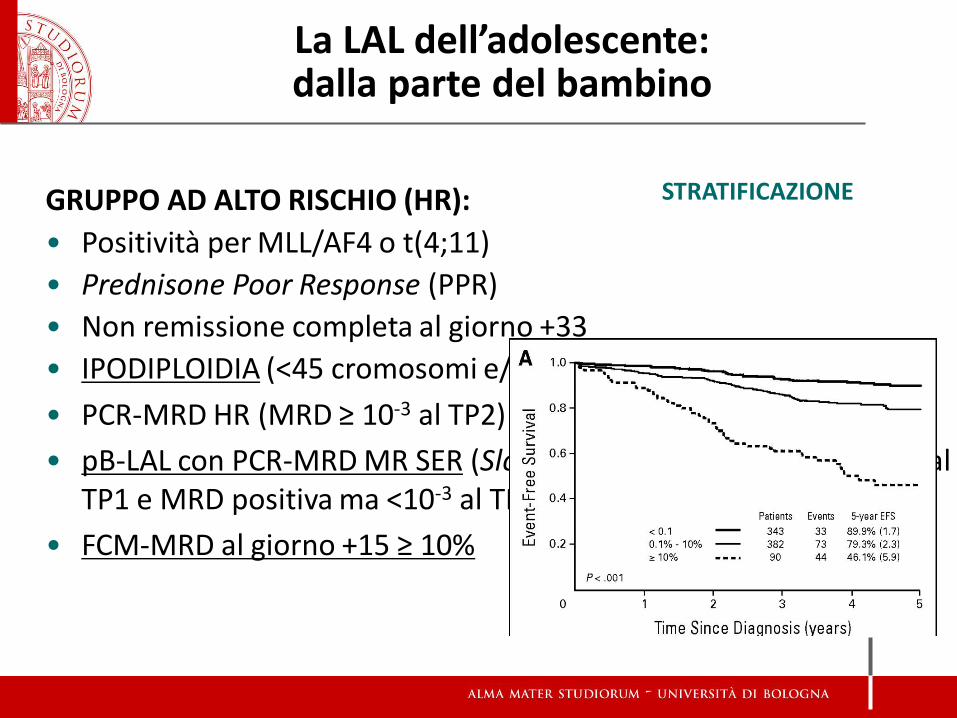
STRATIFICAZIONE GRUPPO AD ALTO RISCHIO (HR):
• Positività per MLL/AF4 o t(4;11)
• Prednisone Poor Response (PPR)
• Non remissione completa al giorno +33
• IPODIPLOIDIA (<45 cromosomi e/o DNA index < 0.8)
• PCR-MRD HR (MRD ≥ 10-3 al TP2)
• pB-LAL con PCR-MRD MR SER (Slow Early Responders: MRD ≥10-3 al TP1 e MRD positiva ma <10-3 al TP2)
• FCM-MRD al giorno +15 ≥ 10%
La LAL dell’adolescente: dalla parte del bambino
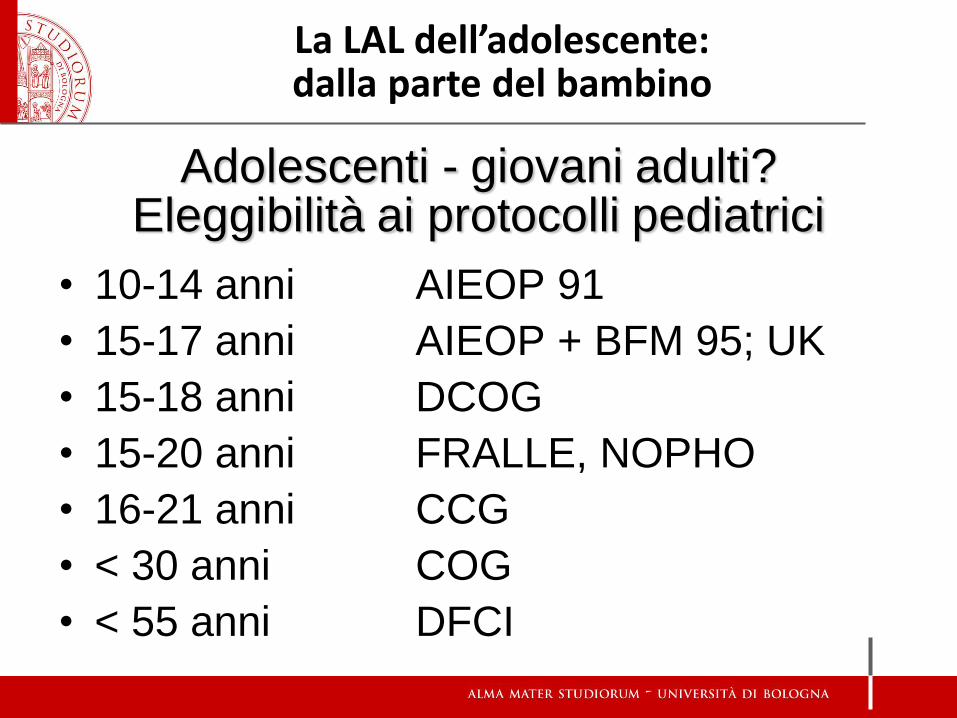
Adolescenti - giovani adulti? Eleggibilità ai protocolli pediatrici
• 10-14 anni AIEOP 91
• 15-17 anni AIEOP + BFM 95; UK
• 15-18 anni DCOG
• 15-20 anni FRALLE, NOPHO
• 16-21 anni CCG
• < 30 anni COG
• < 55 anni DFCI
La LAL dell’adolescente: dalla parte del bambino
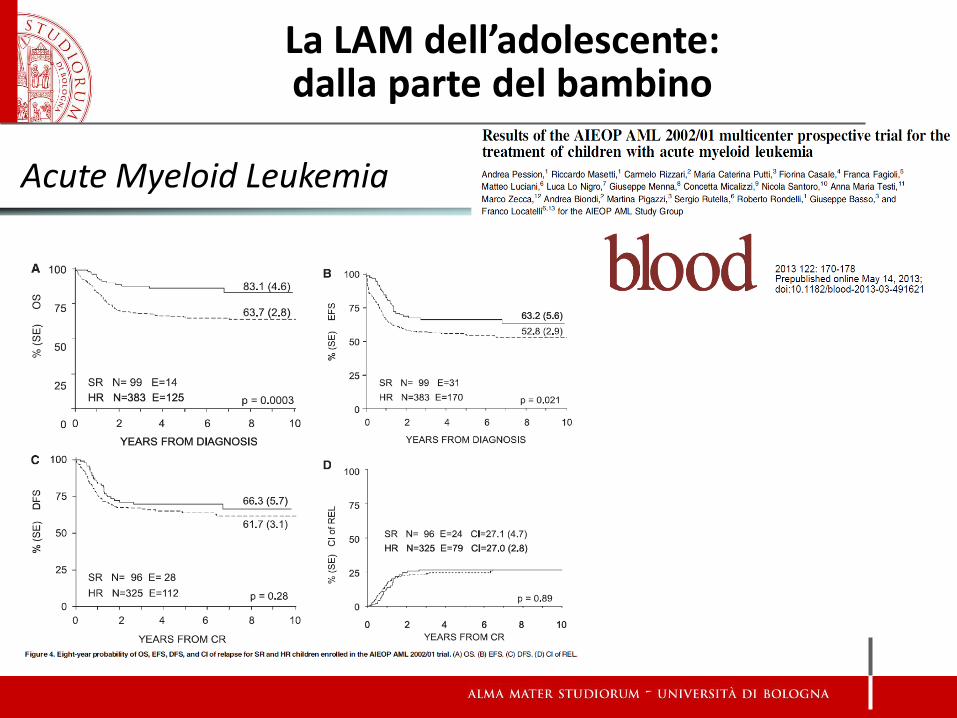
Acute Myeloid Leukemia
La LAM dell’adolescente: dalla parte del bambino
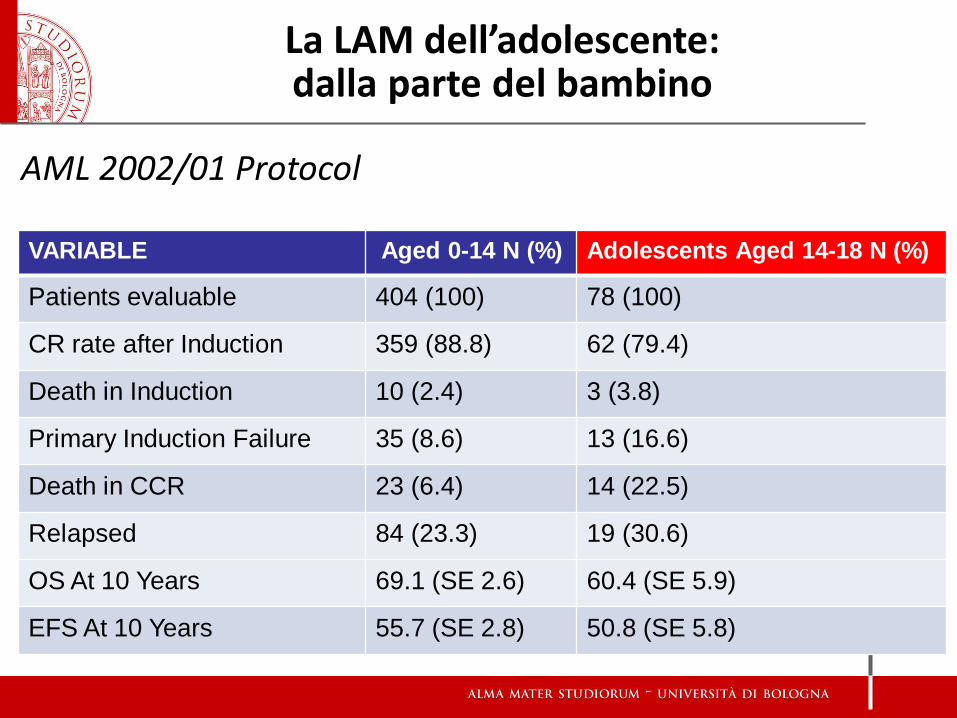
VARIABLE Aged 0-14 N (%) Adolescents Aged 14-18 N (%)
Patients evaluable 404 (100) 78 (100)
CR rate after Induction 359 (88.8) 62 (79.4)
Death in Induction 10 (2.4) 3 (3.8)
Primary Induction Failure 35 (8.6) 13 (16.6)
Death in CCR 23 (6.4) 14 (22.5)
Relapsed 84 (23.3) 19 (30.6)
OS At 10 Years 69.1 (SE 2.6) 60.4 (SE 5.9)
EFS At 10 Years 55.7 (SE 2.8) 50.8 (SE 5.8)
AML 2002/01 Protocol
La LAM dell’adolescente: dalla parte del bambino
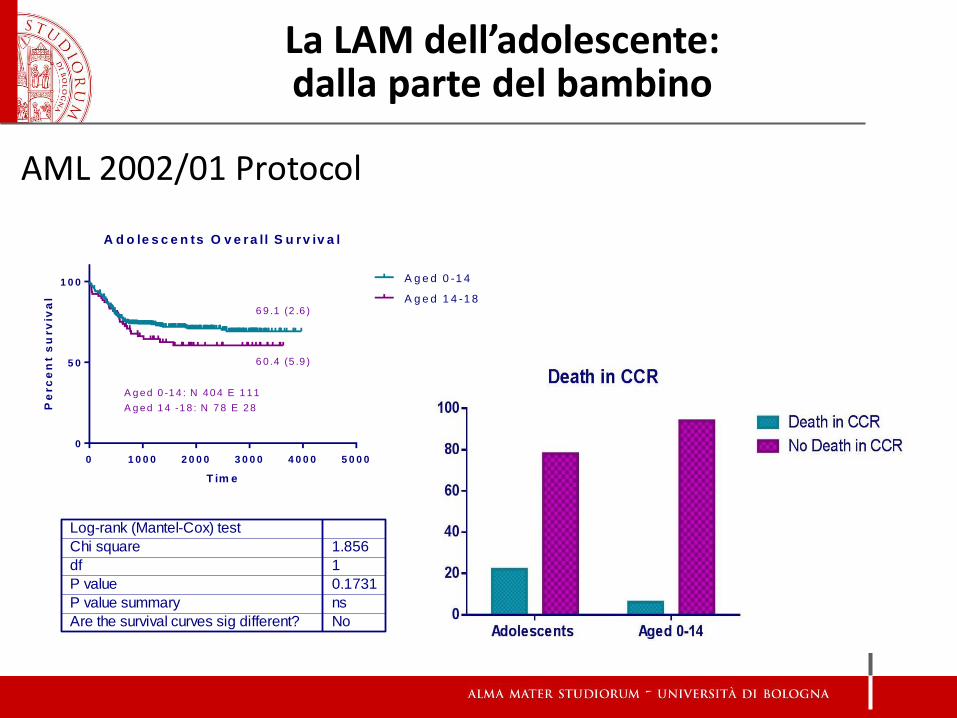
AML 2002/01 Protocol
A d o le s c e n ts O v e r a l l S u rv iv a l
T im e
Pe
rc
en
t s
urv
iva
l
0 1 0 0 0 2 0 0 0 3 0 0 0 4 0 0 0 5 0 0 0
0
5 0
1 0 0 A g e d 0 -1 4
A g e d 1 4 -1 8
Log-rank (Mantel-Cox) test
Chi square
df
P value
P value summary
Are the survival curves sig different?
1.856
1
0.1731
ns
No
A g ed 0 -1 4 : N 40 4 E 1 11
A g ed 1 4 -1 8 : N 7 8 E 28
6 9 .1 (2 .6 )
6 0 .4 (5 .9 )
La LAM dell’adolescente: dalla parte del bambino
La LAM dell’adolescente: dalla parte del bambino
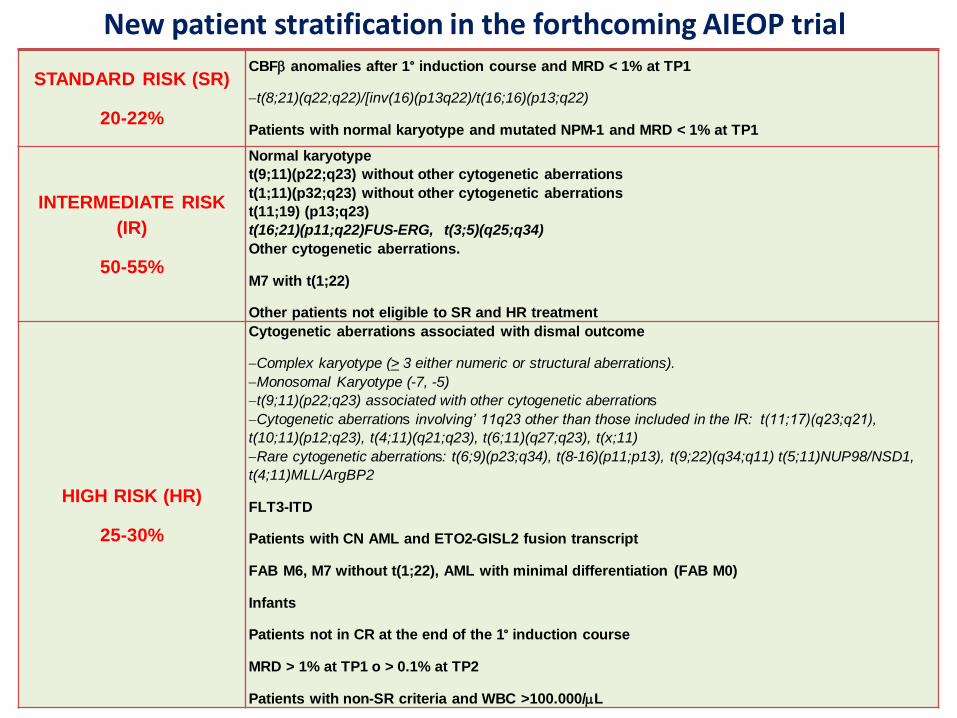
New patient stratification in the forthcoming AIEOP trial
STANDARD RISK (SR)
20-22%
CBFb anomalies after 1° induction course and MRD < 1% at TP1
t(8;21)(q22;q22)/[inv(16)(p13q22)/t(16;16)(p13;q22)
Patients with normal karyotype and mutated NPM-1 and MRD < 1% at TP1
INTERMEDIATE RISK
(IR)
50-55%
Normal karyotype
t(9;11)(p22;q23) without other cytogenetic aberrations
t(1;11)(p32;q23) without other cytogenetic aberrations
t(11;19) (p13;q23)
t(16;21)(p11;q22)FUS-ERG, t(3;5)(q25;q34)
Other cytogenetic aberrations.
M7 with t(1;22)
Other patients not eligible to SR and HR treatment
HIGH RISK (HR)
25-30%
Cytogenetic aberrations associated with dismal outcome
Complex karyotype (> 3 either numeric or structural aberrations).
Monosomal Karyotype (-7, -5)
t(9;11)(p22;q23) associated with other cytogenetic aberrations
Cytogenetic aberrations involving’ 11q23 other than those included in the IR: t(11;17)(q23;q21),
t(10;11)(p12;q23), t(4;11)(q21;q23), t(6;11)(q27;q23), t(x;11)
Rare cytogenetic aberrations: t(6;9)(p23;q34), t(8-16)(p11;p13), t(9;22)(q34;q11) t(5;11)NUP98/NSD1,
t(4;11)MLL/ArgBP2
FLT3-ITD
Patients with CN AML and ETO2-GISL2 fusion transcript
FAB M6, M7 without t(1;22), AML with minimal differentiation (FAB M0)
Infants
Patients not in CR at the end of the 1° induction course
MRD > 1% at TP1 o > 0.1% at TP2
Patients with non-SR criteria and WBC >100.000/mL
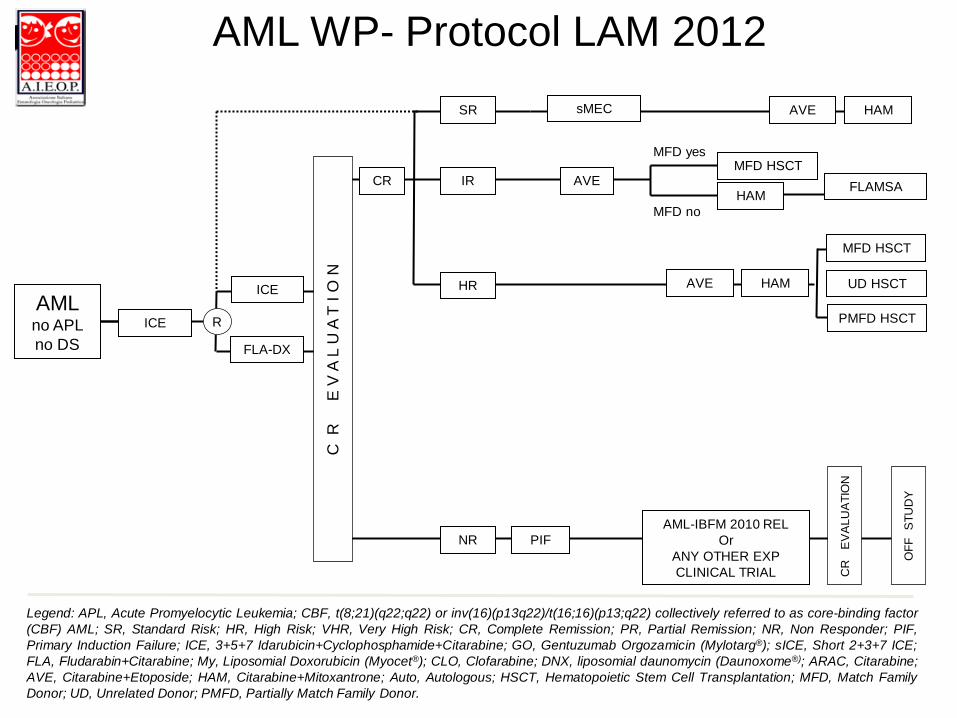
AML WP- Protocol LAM 2012
Legend: APL, Acute Promyelocytic Leukemia; CBF, t(8;21)(q22;q22) or inv(16)(p13q22)/t(16;16)(p13;q22) collectively referred to as core-binding factor
(CBF) AML; SR, Standard Risk; HR, High Risk; VHR, Very High Risk; CR, Complete Remission; PR, Partial Remission; NR, Non Responder; PIF,
Primary Induction Failure; ICE, 3+5+7 Idarubicin+Cyclophosphamide+Citarabine; GO, Gentuzumab Orgozamicin (Mylotarg®); sICE, Short 2+3+7 ICE;
FLA, Fludarabin+Citarabine; My, Liposomial Doxorubicin (Myocet®); CLO, Clofarabine; DNX, liposomial daunomycin (Daunoxome®); ARAC, Citarabine;
AVE, Citarabine+Etoposide; HAM, Citarabine+Mitoxantrone; Auto, Autologous; HSCT, Hematopoietic Stem Cell Transplantation; MFD, Match Family
Donor; UD, Unrelated Donor; PMFD, Partially Match Family Donor.
MFD HSCT
UD HSCT
PMFD HSCT
MFD yes
sMEC AVE HAM SR
AVE HAM HR
AML-IBFM 2010 REL
Or
ANY OTHER EXP
CLINICAL TRIAL
PIF
CR
E
VA
LU
AT
ION
OF
F
ST
UD
Y
NR
HAM FLAMSA
MFD HSCT AVE IR CR
C R
E V
A L
U A
T I
O N
ICE
FLA-DX
R
AML no APL
no DS
ICE
MFD no
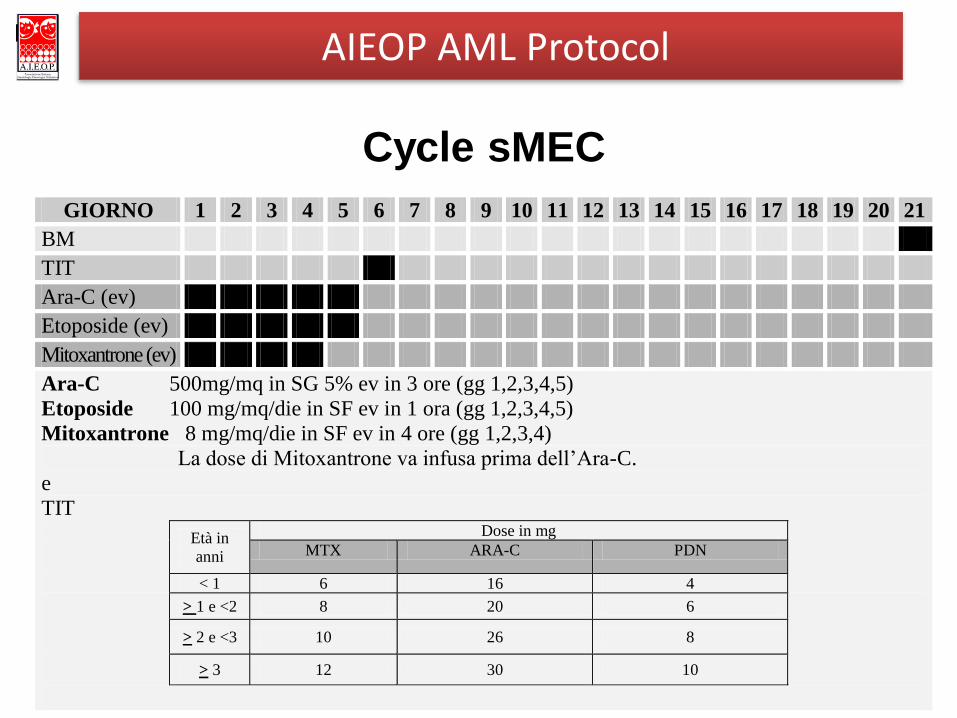
Cycle sMEC
GIORNO 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
BM
TIT
Ara-C (ev)
Etoposide (ev)
Mitoxantrone (ev)
Ara-C 500mg/mq in SG 5% ev in 3 ore (gg 1,2,3,4,5)
Etoposide 100 mg/mq/die in SF ev in 1 ora (gg 1,2,3,4,5)
Mitoxantrone 8 mg/mq/die in SF ev in 4 ore (gg 1,2,3,4)
La dose di Mitoxantrone va infusa prima dell’Ara-C.
e
TIT
Età in
anni
Dose in mg
MTX ARA-C PDN
< 1 6 16 4
> 1 e <2 8 20 6
> 2 e <3 10 26 8
> 3 12 30 10
AIEOP AML Protocol
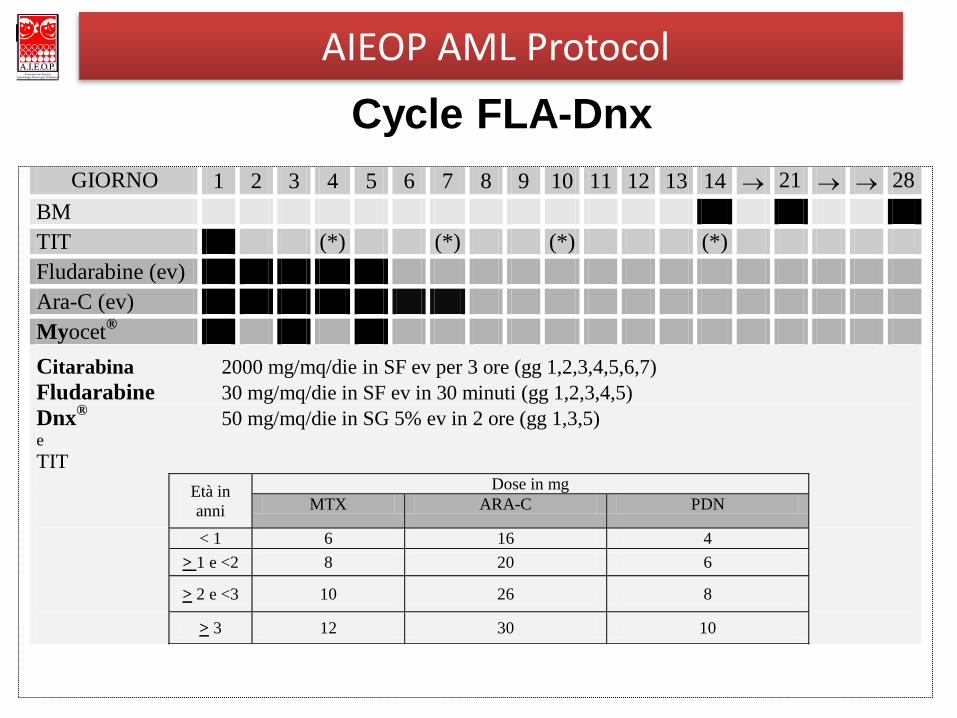
Cycle FLA-Dnx
GIORNO 1 2 3 4 5 6 7 8 9 10 11 12 13 14 21 28
BM
TIT (*) (*) (*) (*)
Fludarabine (ev)
Ara-C (ev)
Myocet®
Citarabina 2000 mg/mq/die in SF ev per 3 ore (gg 1,2,3,4,5,6,7)
Fludarabine 30 mg/mq/die in SF ev in 30 minuti (gg 1,2,3,4,5)
Dnx®
50 mg/mq/die in SG 5% ev in 2 ore (gg 1,3,5) e
TIT
Età in
anni
Dose in mg
MTX ARA-C PDN
< 1 6 16 4
> 1 e <2 8 20 6
> 2 e <3 10 26 8
> 3 12 30 10
AIEOP AML Protocol
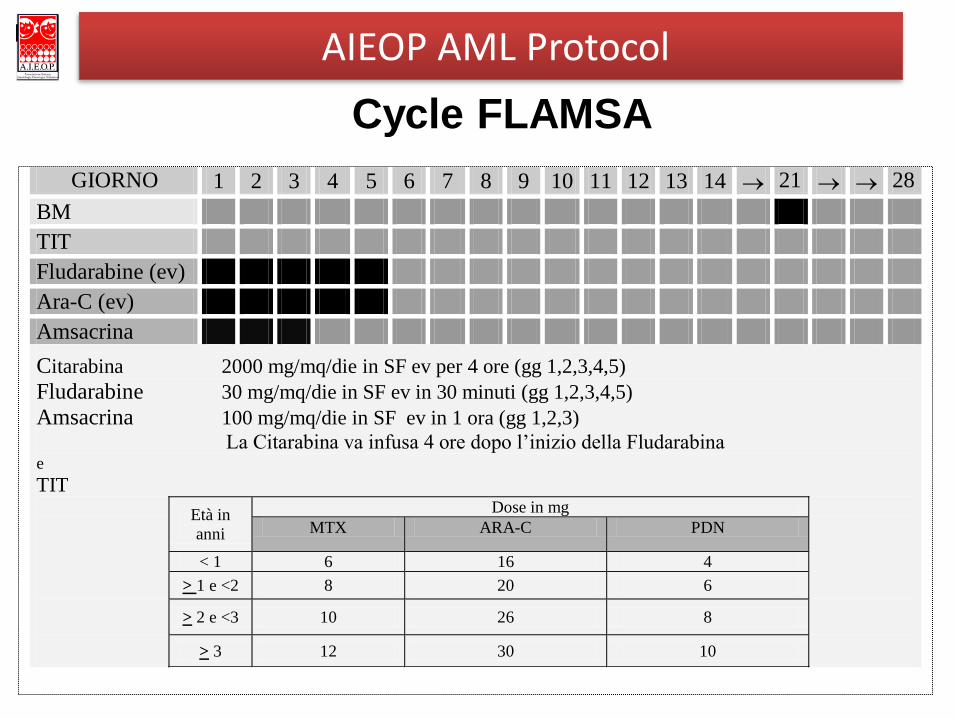
Cycle FLAMSA
GIORNO 1 2 3 4 5 6 7 8 9 10 11 12 13 14 21 28
BM
TIT
Fludarabine (ev)
Ara-C (ev)
Amsacrina
Citarabina 2000 mg/mq/die in SF ev per 4 ore (gg 1,2,3,4,5)
Fludarabine 30 mg/mq/die in SF ev in 30 minuti (gg 1,2,3,4,5)
Amsacrina 100 mg/mq/die in SF ev in 1 ora (gg 1,2,3)
La Citarabina va infusa 4 ore dopo l’inizio della Fludarabina e
TIT
Età in
anni
Dose in mg
MTX ARA-C PDN
< 1 6 16 4
> 1 e <2 8 20 6
> 2 e <3 10 26 8
> 3 12 30 10
AIEOP AML Protocol