hartmann's pouch: radiographic evaluation of postoperative ... · title: hartmann's...
TRANSCRIPT

RaviCherukuri1Marc S.Levine1Daniel D. Maki1StephenE.Rubesin1IgorLaufer1ErnestF.Rosato2
OBJECTIVE. The purposeof this studywas to determinethe usefulnessof contrast-enhanced radiography of the Hartmann's pouch for evaluating postoperative abnormalities.MATERIALS AND METHODS. We performeda retrospectivestudyof 84 patients
with a Hartmann's pouch who underwent contrast-enhanced radiography of the pouch duringa recent 7-year period. Sixty-four patients underwent single-contrast barium studies of thepouch, 17 underwent studies with a water-soluble contrast medium, and three underwent bothtypes of studies. The radiographic studies were reviewed to determine the types and frequencyof abnormalitiesinvolvingthe pouch.Medical recordswere also reviewedto determineclinicalpresentationandcourse.RESULTS. Abnormalitiesof the Hartmann'spouchwere detectedon contrast-enhanced
radiography in 16 (19%) of the 84 patients. Of the 70 patients who underwent routine contrast-enhanced radiography of the pouch, 11 (16%) had abnormalities, including diversioncolitis in three,leaksin two, adhesionsin two, recurrentcarcinomain two, ulcerativecolitisinvolving the pouch in one, and a stricture in one. In both patients with clinically silent leaks,the contrast-enhanced radiography was performed 3 months or more after creation of thepouch. Of the remaining 14 patients who underwent contrast-enhanced radiography becauseof suspectedcomplications involving the pouch, five (36%) had abnormalities revealed, including leaks in two, fistulas in two, and recurrent carcinoma in one.CONCLUSION. Contrast-enhancedradiographyof the Hartmann'spouchrevealedab
normalitiesof thepouchin 19%of patients,includingleaksor fistulas,diversioncolitis,adhesions, strictures, and recurrent tumor. Because two patients had clinically silent leaks thatwere detected during the late postoperative period, it may be prudent to perform these studieswith a water-soluble contrast medium to avoid the problems associated with extravasation ofbarium into the extra- or intraperitoneal spaces.
T he Hartmann's procedure is acommon surgical procedure inwhich a temporarydivertingco
lostomyand blind-endingrectal or colonicstump closed by suture (Hartmann's pouch)are created after partial colectomy or sigmoidectomy[1]. This procedureis usuallyperformed on an emergent basis in patientswith complicated diverticulitis, obstructingor perforated sigmoid carcinoma, or penetrating trauma [2, 3]. When such patients undergo sigmoid resection, a Hartmann'sprocedure is performed rather than primaryreanastomosis of the bowel because of therisk of anastomotic rupture associated withinadequate bowel preparation, complicatingperitonitis,or both.The creationof a tempo
rary diverting colostomy allows peritonealinflammationto subside;the colostomycanthen be taken down and reanastomosed to thepouch during the second stage of the procedure to restore colonic continuity.Leakage or even blowout ofthe blind-end
ing rectal or colonic stump can occur as a potentially life-threatening complication of theHartmann's procedure [4—7].Other complications include pouch fistulasor stricturesand diversion colitis [4, 8, 9]. Contrast-enhanced radiography of the Hartmann's pouchmay be performed to assess the anatomy andintegrity of the pouch and to rule out complicationsbefore takedownof the colostomy.To our knowledge, except for two previousarticles about diversion colitis I 10, 11], little
ReceivedApril29,1998;acceptedafterrevisionJune11,1998.
1Department of Radiology, Hospital of the University ofPennsylvania,3400SpruceSt.,Philadelphia,PA19104.Addresscorrespondenceto M.S.Levine.2DepartmentofSurgery,Hospitalof theUniversityofPennsylvania,Philadelphia,PA19104.AJR1998;171:1577—1582
0361—803X/98/1716—1577
©AmericanRoentgenRaySociety
AJR:171,December 1998 1577
Hartmann's Pouch: RadiographicEvaluation of Postoperative Findings
Dow
nloa
ded
from
ww
w.a
jronl
ine.
org
by D
artm
outh
- H
itchc
ock
Med
Ctr
on 0
2/28
/13
from
IP a
ddre
ss 1
30.1
89.1
0.63
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
right
s res
erve
d
•¿ ,@.1@@Flndingsin 84 PatIentsWho Underwent Contrast-EnhancedRadiographyof- . the Hartmann'sPouch.
.FindingsRoutineRadiographyRadiography
forSuspected
ComplicationsTotalNo.%No.%No.%Abnormal
findingsLeaksorfistulasDiversion proctitisUlcerative proctitisRecurrent carcinomaAdhesionsStrictures2
312212
412214
001005
001006
313217
4142
1Totatabnormalities
Normalfindings11 5913 705 96 1116 681981Total
no. of patients7083141784100
PatientsIndicationNo.%Complicated
diverticulitis4149Gunshotwound1518Perforated
sigmoidcarcinoma911Pericolicabscess56Inflammatory
boweldisease34lschemicboweldisease34Atonic
megacolon22Steroid-relatedbowel22perforationMetastatic
ovariancarcinoma11latrogenictrauma11Colonicvarices11Obstructing
neurofibroma11
Cherukuri etal.
data exist in the radiology literature concerning the usefulness of contrast-enhanced radiography for evaluating the Hartmann'sprocedure or its complications. The purposeof this study was to determine the findings ofcontrast-enhancedradiographyof the Hartmann's pouch in a large series of patientswho underwent this surgical procedure.
Materials and MethodsPatientPopulation
We performed a retrospective study of 84 patients with a Hartmann's pouch who underwentcontrast-enhanced radiography of the pouch at ouruniversity hospital or affiliated Veterans Affairshospital during a 7-year period between 1990 and1997.The patients included 58 male patients and26 female patients with an average age of 51years(range, 15—85years). The indications for creatinga Hartmanns pouch are summarized in Table I.The proximal diverting colostomy was subsequently taken down and reanastomosed to thepouch in 63 patients (75%). Excluding one patientin whom the colostomy was taken down 25 yearsafter the first stage of the procedure, the averageinterval between creation of the Hartmann's pouchand takedown of the colostomy was 8 months(range. 2—42months). In all cases, medical recordswere reviewed to determine the clinical presentation and course of these patients.
RadiographicStudies
Each of the 84 patients underwent contrast-enhanced radiography of the Hartmann's pouch, including single-contrast barium studies in 64patients, studies with water-soluble contrast medium in 17 patients, and both in three patients. Ex
cluding the one patient in whom a Hartmann@spouch was created 25 years earlier, the average durationbetweencreationof thepouchandcontrastenhanced radiography was 10 months (range. 1—67months). Seventy patients (83%) underwent routineexaminations to assess the anatomy of the pouchbefore takedown of the colostomy. The remaining14patients (17%)underwentcontrast-enhancedradiography to rule out postoperative abnormalitiesbecause of abdominal pain and fever in four patients, abdominal pain and diarrhea in one, abdominal pain alone in two, diarrhea and fever in one,diarrhea alone in two. fever alone in two, rectal painin one, and a pelvicmass on CT in one. In these 14patients, the average duration between creation ofthe pouch and contrast-enhancedradiographywas12 months (range. 1—42months).Radiographic examination of the Hartmann's
pouch was performed using the following technique: An anteroposterior scout film of the abdomen and pelvis was initially obtained. A Foleycatheter was then inserted via the anus into thepouch, and either barium sulfate or a water-solublecontrast medium (Hypaque [diatrizoate sodiuml:Nycomed. Princeton, NJ; or Gastroview [diatrizoate meglumine and diatrizoate sodiuml;Mallinckrodt Medical, St. Louis, MO) was introduced into the pouch under fluoroscopicguidance.Radiographic imaging of the pouch included spotfilms of the pelvis in frontal, lateral, and obliqueprojections: frontal and lateral overhead radiographs of the pelvis: and a lateral postevacuationradiograph of the pelvis to assess functional emptying of the pouch.The original radiology reports from all 84 pa
tients were reviewed to determine the findings ofcontrast-enhanced radiography of the pouch. Theradiographs from 78 examinations (including allthe studies showing abnormalitiesdescribed in theradiologyreports)werereviewedretrospectively.
In those 78 cases, the blind-ending Hartmann'spouch was found to extend as far as the proximalrectum or rectosigmoid junction in six patients(8%). the sigmoid colon in 61 (78%). the descending colon in eight (10c/()and the transverse colonin three (4%). In six patients with normal findingsonpostoperativestudies.theradiographswerenotavailable for review.
ResultsPostoperativeStudieswith Normal Findings
Sixty-eightpatients(81%) who underwentcontrast-enhancedradiographyof the Hartmann's pouch had normal findings on postoperative studies.Of these 68 patients,41(60%) had an uncomplicated takedown ofthe diverting colostomy; 14 (2 1%) had takedown of the colostomy complicated by postoperativewoundinfections(ii = 7). abscesses(n = 3), or anastomotic leaks (ti = 4) that necessitatedsurgicalor percutaneousdrainage;six (9%) did not have takedown of the cobstomy for various medical reasons; and the remaining seven (10%) were lostto follow-up.
Abnormalitiesofthe PouchAbnormalities were detected on contrast-en
hanced radiography ofthe Hartmann's pouch in16 ( 19%) of 84 patients (Table 2). Of 70 patients who underwent routine contrast-enhanced radiography before takedown of thecolostomy,I I (16%) hadabnormalities,including diversion colitis in three, leaks in two, adhesions in two, recurrent carcinoma in two.ulcerative colitis involving the pouch in one,and a stricture in one.Of the other 14 patients
1578 AJR:171,December1998
= PrimaryIndicationsfor£: Hartmann's Procedure in 84
Patients
Dow
nloa
ded
from
ww
w.a
jronl
ine.
org
by D
artm
outh
- H
itchc
ock
Med
Ctr
on 0
2/28
/13
from
IP a
ddre
ss 1
30.1
89.1
0.63
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
right
s res
erve
d
Radiography of Hartmann's Pouch
who underwent contrast-enhanced radiographybecause of suspected complications involvingthe pouch. five (36%) had abnormalities, ineludingleaksin two, flstula.sin two,andrecurrentcarcinomainone.
Leaksor FistulasOf six patients with leaks or fistulas from
the Hartmann's pouch. two were asymptomatic: these two underwent routine bariumstudies of the pouch before planned takedown of the colostomy. In one of the asymptomatic patients. a study 3 months aftercreation of the pouch showed focal extravasationof barium from the proximal end ofthe pouch into a 6 x 3 cm collection in thepresacral space (Fig. I ). In the second patient. a study 7 months after creation of thepouch showed free extravasation of bariumfrom the blind end of the sigmoid pouch intothe peritoneal cavity (Fig. 2). The first patient underwent surgical revision of thepouch and subsequent takedown of the cobostomy: the second was admitted to the hospital for 5 days of IV antibiotic therapy andwas scheduled for surgical revision and takedown of the colostomy.In fourpatientswhopresentedwithclinical
signsof a leak(e.g..abdominalpain.fever,or
leukocytosis), studies with water-soluble contrastmediashowedleaksor fistulasinvolvingthe pouch.One of thesepatientshad a 2.5-cmtract from the posterior wall of the rectalpouch intO a tiny collection in the presacralspace; a second had focal extravasation fromthe end of a long transverse cobonic stumpinto a sealed-off 5-cm collection (Fig. 3); anda third had an enterocutaneous fistula from theanterior border of the pouch to the anterior abdominalwall.After treatmentwithantibiotics.these three patients had successful closure ofthe colostomy. In the fourth patient. a studywith water-soluble contrast medium showed along fistula between the right superolateralborder of the rectosigmoid pouch and the distab ileum. The fistula was repaired surgically.
DiversionColitisIn three asymptomatic patients. barium
studies of the pouch revealed diversion colitis, a distinct pathologic entity involving thepouch in which nonspecific inflammatorychanges occur in colonic segments divertedfrom the fecal stream [121. In all three patients,markednarrowingof the pouchwasnoted. In addition, the pouch had a nodular,spiculated contour in two of these patients(Fig. 4) and a smooth, featureless appearance
in one. The latter patient was found at sigmoidoscopy to have findings of diversioncolitis. with erythema and friability of thepouch. The other two patients did not undergo endoscopy; one had an uncomplicatedtakedown of the pouch and was subsequentlylost to follow-up. and the other was not acandidate for a takedown procedure becauseof his overall health.
UlcerativeColitisInvolvingPouchOne patient developed a pericolic abscess
after resection of a retroperitoneal sarcoma,necessitatinga partial left hemicolectomyand creation of a Hartmann's pouch. The patient had rectal bleeding 6 months later andunderwent sigmoidoscopy. Endoscopic biopsy specimens revealed findings compatiblewith ulcerative colitis involving the pouchrather than diversion colitis. The patient wastreated with steroid enemas, and his symptoms resolved. Follow-up contrast-enhancedradiography of the pouch 6 months latershowed continued proctitis with thickened,edematous folds in the pouch.
AdhesionsIn one asymptomaticpatient, a barium
study of the pouch revealed beaklike narrow
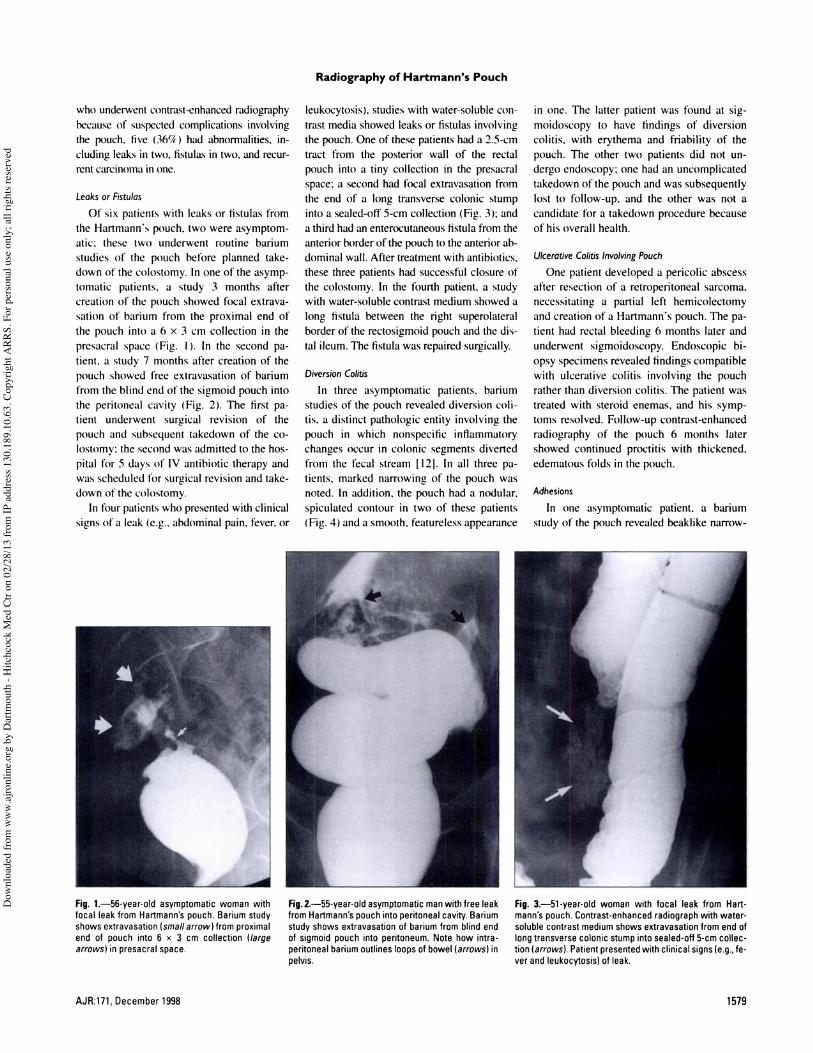
Fig.1—56-year-oldasymptomaticwomanwithfocal leak from Hartmann'spouch. Barium studyshowsextravasation(smallarrow) from proximalend of pouch into 6 x 3 cm collection (largearrows)inpresacralspace.
Fig.2—55-year-oldasymptomaticmanwithfreeleakfromHartmann'spouchintoperitonealcavity.Bariumstudy shows extravasationof bariumfrom blind endof sigmoid pouch into peritoneum. Note how intraperitonealbariumoutlinesloopsofbowel(arrows)inpelvis.
Fig.3—51-year-oldwomanwithfocalleakfromHartmann'spouch.Contrast-enhancedradiographwith watersoluble contrast mediumshows extravasationfrom end oflongtransverse colonic stumpinto sealed-off 5-cmcollection (arrows). Patientpresentedwith clinical signs(e.g.,fever and leukocytosis)of leak.
AJR:171,December1998 1579
Dow
nloa
ded
from
ww
w.a
jronl
ine.
org
by D
artm
outh
- H
itchc
ock
Med
Ctr
on 0
2/28
/13
from
IP a
ddre
ss 1
30.1
89.1
0.63
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
right
s res
erve
d
Cherukuri etal.
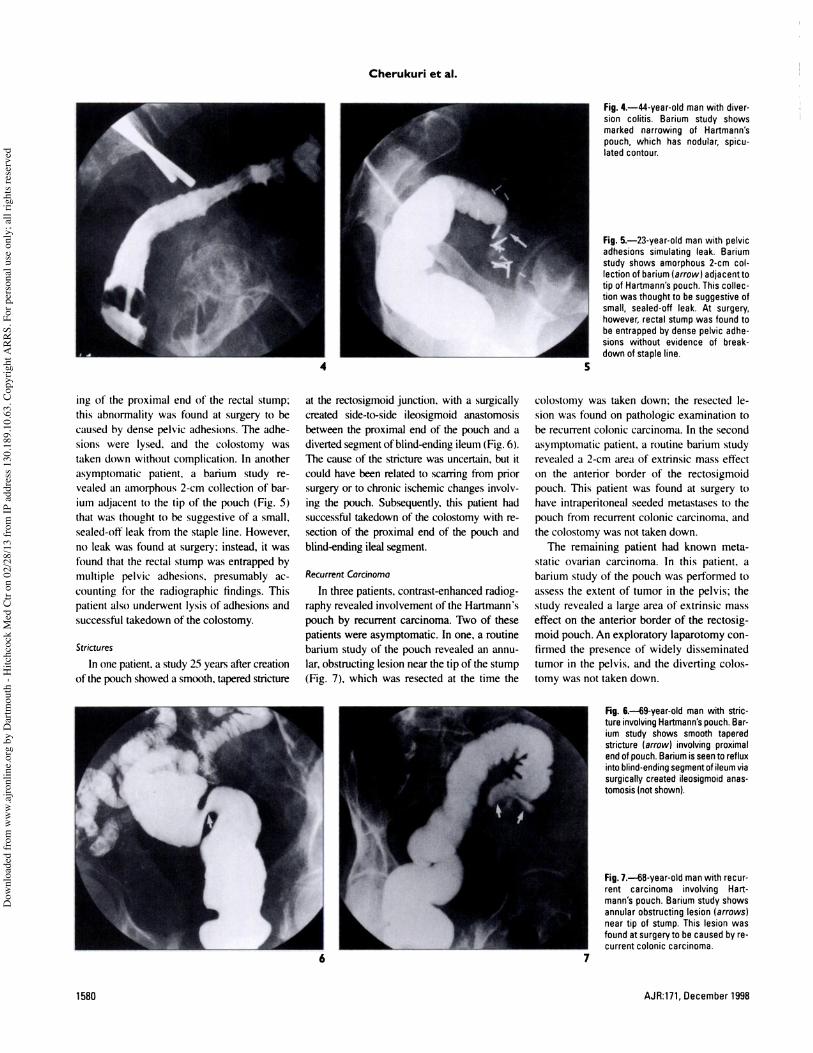
Fig.4—44-year-oldmanwithdiversion colitis. Barium study showsmarked narrowing of Hartmann'spouch, which has nodular, spiculated contour.
Fig.5—23-year-oldmanwithpelvicadhesions simulating leak. Bariumstudy shows amorphous 2-cm collection of barium(arrow) adjacent totip of Hartmann'spouch.This collection was thought to be suggestiveofsmall,sealed-offleak.At surgery,however, rectal stumpwas found tobe entrapped by dense pelvic adhesions without evidence of breakdown of staple line.
f..4@.,
;@ s
1.@4 5
ing of the proximal end of the rectal stump:this abnormality was found at surgery to becausedby densepelvicadhesions.The adhesions were lysed. and the colostomy wastaken down without complication. In anotherasymptomaticpatient. a barium study revealedan amorphous2-cm collectionof barium adjacent to the tip of the pouch (Fig. 5)that was thought to be suggestive of a small.sealed-off leak from the staple line. However,no leak was found at surgery: instead, it wasfound that the rectal stump was entrapped bymultiple pelvic adhesions, presumably accounting for the radiographic findings. Thispatientalsounderwentlysisof adhesionsandsuccessfultakedownof the colostomy.
StricturesIn one patient, a study 25 years after creation
of thepouchshoweda smooth,taperedstricture
at the rectosigmoid junction. with a surgicallycreated side-to-side ileosigmoid anastomosisbetween the proximal end of the pouch and adiverted segment ofblind-ending ileum (Fig. 6).The cause of the stricture was uncertain, but itcould have been related to scarring from priorsurgery or to chronic ischemic changes involving the pouch. Subsequently, this patient hadsuccessfultakedownof the colostomy with resection of the proximal end of the pouch andblind-ending ileal segment.
RecurrentCarcinomaIn three patients, contrast-enhanced radiog
raphy revealed involvement of the Hartmann'spouch by recurrent carcinoma. Two of thesepatients were asymptomatic. In one, a routinebarium study of the pouch revealed an annubar, obstructing lesion near the tip of the stump(Fig. 7), which was resected at the time the
colostomywas takendown; the resectedbesion was found on pathologic examination tobe recurrentcoloniccarcinoma.In thesecondasymptomaticpatient,a routinebariumstudyrevealed a 2-cm area of extrinsic mass effecton the anterior border of the rectosigmoidpouch.This patientwas foundat surgerytohave intraperitoneal seeded metastases to thepouch from recurrent cobonic carcinoma, andthe colostomy was not taken down.The remaining patient had known meta
static ovarian carcinoma. In this patient. abariumstudyof the pouchwasperformedtoassessthe extentof tumor in the pelvis; thestudy revealed a large area of extrinsic masseffect on the anterior border of the rectosigmoid pouch.An exploratory laparotomy confirmed the presence of widely disseminatedtumor in the pelvis, and the diverting cobstomywasnottakendown.
Fig. 6.—69-year-oldman with stricture involvingHartmannspouch.Barium study shows smooth taperedstricture (arrow) involving proximalendof pouch.Bariumisseento refluxintoblind-endingsegmentof ileumviasurgically created ileosigmoidanastomosis(notshown).
Fig.1—68-year-oldmanwithrecurrent carcinoma involving Hartmann'spouch. Barium study showsannular obstructing lesion (arrows)neartip of stump.Thislesionwasfound at surgeryto be causedby recurrent colonic carcinoma.
4:@@ r -@k lb
I
I
6 7
1580 AJR:171,December 1998
:
Dow
nloa
ded
from
ww
w.a
jronl
ine.
org
by D
artm
outh
- H
itchc
ock
Med
Ctr
on 0
2/28
/13
from
IP a
ddre
ss 1
30.1
89.1
0.63
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
right
s res
erve
d

Radiography of Hartmann's Pouch
DiscussionRoutinecontrast-enhancedradiographyof
the Hartmann's pouch is often requestedbythe surgeon to assessthe anatomy and integrity of the pouch before takedownof the proximal diverting colostomy. Many radiologistserroneously believe that the pouch consistsofa blind-ending rectal or rectosigmoid stump.In fact,theHartmann'spouchisdefinedin thesurgical literature as a rectal or colonic stumpthat can extend as far proximally as the transverse colon [I, 13, 14]. In ourseries, the Hartmann's pouch extended beyond the level ofthe sigmoidcolon in 14% of patients.Thelengthof thepouchis of particularinteresttothe surgeon because the stump can slowlyshortenovertime, affectingits locationin relationtotheproximaldivertingcolostomy[5];this information is important when planningthesurgicaltechniqueto takedownthecobstomy and reanastomosethe proximal colon tothepouch.The most important causeof morbidity
andmortalityafter the firststageof theHartmann'sprocedureis breakdownof the rectalstump [4, 8]. In various series, the rate ofleakage from the Hartmann's pouch hasranged from 2% to 9% [4—7].Most suchleaks involve the blind end of the oversewnstump (Figs. 1—3).Depending on the location of the stump,theseleakscan be extraperitoneal or intraperitoneal. Patients withshort rectal stumpsmay haveextraperitonealbeakswith associated pelvic abscesses.Insuch patients, options for treatment includeantibiotics,percutaneousor surgicaldrainage of the abscess,or surgical repair of theleak. In contrast, patients with long pouchesmay have intraperitoneal leaks from theblind-endingstump,with abscessformationor even peritonitis. When peritonitis occurs,surgical repair of the leak usually is requiredbecauseof the life-threateningnatureof thiscomplication [15].Surprisingly,it is difficult to find guide
lines about the appropriateuse of contrastagentsfor radiologicevaluationof the Hartmann's pouch. In general, water-soluble contrast media (e.g.. Hypaque or Gastroview)are used to rule out leaks from the pouchduring the early postoperativeperiod (i.e.,days to weeks after surgery), whereas bariumsulfate is used to evaluate the pouch duringthe late postoperative period (i.e., months toyearsafter surgery).In our study,however,two of six patients
with breakdown of the pouch had clinicallysilent leaks (Figs. I and 2) that were detected
3 monthsormoreaftercreationof thepouch.One of the leakswasextraperitoneal(Fig. I)and the other was intraperitoneal (Fig. 2).Both patients were asymptomatic, presumably becausethe pouch had been divertedfrom thefecalstream;the leaksthereforeoccurred in a relatively sterile environment.Clinically silent leaks or fistulas have alsobeen shown to occur from an ileal pouch after total proctocolectomy and ileoanal pullthrough with a diverting ileostomy [16]. Insuch patients, delayed closure of the ileostomy hasbeenadvocatedto allow time forhealing before exposingthe ileal pouch tothe fecal stream [16, 17]. Similarly, delayingtakedown of the colostomy in patients withasymptomaticleaks from the Hartmann'spouchshouldallow theseleaks to heal, decreasing the risk of pelvic infection after coIoniccontinuityhasbeenrestored.Some investigatorsbelievethat peritonitis
occurs only as a complication of barium studies in patients with perforated bowel whenbarium and feces simultaneously enter theperitoneal cavity [18, 19]. However, animalexperimentshaveshown that evenasepticadministrationof intraperitonealbarium maycause peritonitis [20]. The use of barium sulfate to evaluate the Hartmann's pouch couldalsocompromisefollow-upstudiesin patientswith leaksbecausebarium (unlike water-soluble contrastmedium) is not resorbedfrom theextra- or intraperitoneal spaces.For thesereasons, we favor the use of water-soluble contrast media for radiographic evaluation of theHartmann's pouch even during the late postoperative period because clinically silent leaksoccasionally may be found in these patients.
When evaluating the esophagus for possibleperforation, esophagographywith barium subfate can detect leaks that are missed with water-soluble contrast media [21]. Therefore, it isrecommendedthat esophagographybe repeated with barium sulfate when no leak is detected with water-soluble contrast media inpatients with suspected esophageal perforation[21]. In theory, a similar approach could beused to evaluate the Hartmann's pouch withcontrast-enhanced radiography. However,manypatientswouldbeunableorunwillingtotolerate two sequential contrast-enhanced examinationsof the pouch (i.e., a studywith water-soluble contrast medium immediatelyfollowed by a barium study), and it would bedifficult to obtain optimal barium coating of apouch that contained residual water-solublecontrast medium. Therefore, this approachwould be impractical for most patients.
When a high level of clinical suspicion cxistsof a pelvic abscessin a patient with aHartmann'spouchor when a leak from thepouch is shown on contrast-enhanced radiography, CT is the imaging technique of choicefor confirming the presence of an abscessand determiningits extent [4, 15]. Depending on the size and location of the abscess,itcan be drained surgically or percutaneouslywith CT guidance.Some patients with a Hartmann's pouch
may developdiversioncolitis, a nonspecificinflammatory processoccurring in cobonicsegmentsthat havebeendiverted from the fecal stream I12]. It has been postulated that diversioncolitis is causedby a deficiencyofshort-chainfatty acids,which normally areusedby the colonic mucosafor nutrition [22].Diversion colitis may be extremely difficult todifferentiate from Crohn's colitis on pathologic grounds[23]. In our series,diversioncolitiswasmanifestedby decreaseddistensibility andnodularityof the pouchon bariumstudies (Fig. 4). Others have previously described a nodular mucosaon double-contrastexaminations of the pouch, most likely due tolymphoid follicular hyperplasia of the cxcluded colonic segment [10, 11]. Diversioncolitis is a relatively common condition at endoscopy,but mostofthese patientsareasymptomatic [12, 23]. In almost all cases, diversioncolitisspontaneouslyremitsafterthedivertingcolostomy has been taken down and coloniccontinuity restored [ 12, 23, 24].Although uncommon, dense pelvic adhe
sions may prevent complete filling of theHartmann'spouch.Rarely,contrastmediumin the deformed pouch may erroneouslysuggest a leak, as occurred in one of our patients (Fig. 5). When the Hartmann's procedure is performed on patients with sigmoidcarcinoma or other pelvic malignancies, contrast-enhancedradiographymay show involvement of the pouch by recurrent tumorin the pelvis (Fig. 7).Several investigatorshave reportedcases
of primary rectal carcinoma developing in aHartmann's pouch one or more years aftersurgery for benign disease[8, 25, 26]. It hasbeenpostulatedthatchronicinflammationofthe pouch in patientswith diversioncolitisincreasesthe risk of malignant degeneration[26]. These investigators therefore advocateperiodicevaluationof thepouchwith endoscopy or contrast-enhancedradiography, evenin asymptomatic patients, so that developingcancers can be detected at the earliest possiblestage[8, 25, 26]. However,long-termfob
AJR:171,December1998 1581
Dow
nloa
ded
from
ww
w.a
jronl
ine.
org
by D
artm
outh
- H
itchc
ock
Med
Ctr
on 0
2/28
/13
from
IP a
ddre
ss 1
30.1
89.1
0.63
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
right
s res
erve
d

low-up of a large series of patients withHartmann'spouchesis requiredto determinewhetherthe incidenceof rectalcarcinomaisincreasedin thesepatients.
In summary, contrast-enhanced radiographyof theHartmann'spouchrevealedabnormalities of the pouch in 16 ( I9%) of 84patients, including leaks or fistulas, diversioncolitis, adhesions,strictures,and recurrenttumor. Because two patients had clinicallysilent beaks that were detected during the latepostoperative period, it may be prudent toperform these studies with water-solublecontrastmediumto avoidtheproblemsassociated with extravasation of barium into theextra-or intraperitoneabspaces.
References1. Corman ML. Diverticular disease. In: Corman
ML, ed. Colon and rectal surgery, 3rd ed. Philadelphia: Lippincott, 1993:817—859
2. Wedell J, BanzhafG, Chaoui R, Fischer R, ReichmannJ. Surgicalmanagementof complicatedcolonicdiverticulitis.BrJ Surg1997;84:380—383
3. DociR,AudisioRA,BozzeutiF,GennariL.Actual role of Hartmann'sresection in elective surgical treatment of carcinoma of rectum andsigmoid colon. Surg GynecolObstet 1986;163:49—53
4. CarterFM,McleodRS,CohenZ. Subtotalcolectomy for ulcerativecolitis:complicationsrelatedto the rectal remnant. Dis Colon Rectum 1991:
34:1005—10095. ChuaCL.Surgicalconsiderationsin theHartmannprocedure.AustNZJSurg 1996;66:676—679
6. Lubbers EtC. de Boer HMM. Inherent complicationsof Hartmann'soperation.SurgGynecolObstet1982;l55:7l7—721
7. Bakker FC, Hoitsma HFW, Den Otter 0. TheHartmann procedure. Br) Surg 1982;69:580—582
8. HaasPA,FoxTA.The fateof the forgottenrectalpouch after Hartmann's procedure without reconstruction. Am J Surg 199019:106—111
9. OakleyJR. LaveryIC, FazioVW,JagelmanDO,Weakley FL, Easley K. The fate of the rectalstumpafter subtotalcolectomy for ulcerativecolitis. Dis ColonRectum1985;28:394—396
10. Lechner GL, Wolfgang F, Jantsch H, et al. Lymphoid follicular hyperplasia in excluded colonicsegments: a radiologic sign of diversion colitis.Radiology 1990;176:135—136
11. ScottRL, PinsteinML.Diversioncolitisdemonstrated by double-contrast barium enema. AiR1984;143:767—768
12. Glotzer DJ, Glick ME, GoldmanH. PrOctitisandcolitis following diversion of the fecal Stream.Gastroentemlogy1981;80:438—44l
13. RosenmanLD. Hartmann's operation: how I doit. Am J Surg 1994;l68:283—284
14. NunesGC. RobnettAN, KremerRM, AhiquistRE. The Hartmann procedure for complicationsof diverticulitis. Arch Surg 1979;l 14:425-429
15. ScheinM, KopelmanD, Nitecki 5, HashimonaiM.Management of the leaking rectal stump after Hartmann'sprocedure.AmJSurg 1993;l5:285—287
16. lIning JM,LevineMS.RombeauJL, RubesinSE,Laufer I. Total proctocolectomy and ileoanal pouch:the role ofcontrast StUdieSfor evaluating postopera
tive leaks.Abdom imaging 1998;23:375—37917. Alfisher MM, Scholz FJ, Roberts PL, Counihan
1. Radiologyof ileal pouch-anal anastomosis:normal findings. examination, pitfalls, and complications. RadioGraphics 1997;17:81—98
18. YamamuraM, Nishi M, FurubayashiH, Hioki K,YamamotoM.Bariumperitonitis:reportof a caseand reviewof the literature.Dis ColonRectum1985;28:347—352
19. Grobmeyer Al, Kerlan RA. Peterson CM, Dragstedt LR. Barium peritonitis. Am Surg 1984:50:116—120
20. Henrich MH. Barium peritonitis in animal experiments.Chirurg 1986;57:801—804
21. BueckerA, WeinBB, NeuerburgJM, GuentherRW.Esophagealperforation:comparisonof useof aqueous and barium-containing contrast media.Radiology1997;202:683—686
22. Sartor RB, Murphy ME, Rydzak E. Miscellaneous inflammatory and structural disorders ofthecolon.In:Yamada1, ed.Textbookofgastroentemlogy. 2nd ed. Philadelphia: Lippincou, 1995:1806—1832
23. Murray FE, O'Brien MJ, Birkett DH, KennedySM, Lamont JT. Diversion colitis: pathologicfindingsin a resectedsigmoidcolonand rectum.Gastmentemlogy 1987;93:1404—1408
24. Scholz FJ. Postoperative colon. In: Gore RM, LevineMS.LauferI, eds.Textbookofgastrointestinal radiology Philadelphia: Saunders, 1994:1342—1350
25. Lafreniere R, Ketcham AS. Hartmann's pouchcarcinoma.J SurgOncol1985;29:26—27
26. ThaemertBC, KiskenWA.Neoplasmsin longterm Hartmann'spouches.WisMed J 1996:95:105—107
1582
Cherukuri et al.
AJR:171,December1998
Dow
nloa
ded
from
ww
w.a
jronl
ine.
org
by D
artm
outh
- H
itchc
ock
Med
Ctr
on 0
2/28
/13
from
IP a
ddre
ss 1
30.1
89.1
0.63
. Cop
yrig
ht A
RR
S. F
or p
erso
nal u
se o
nly;
all
right
s res
erve
d