come l’endoscopia ha trasformato la gastroenterologia ... · pdf filecome...
TRANSCRIPT

COME L’ENDOSCOPIA HA TRASFORMATO LA
GASTROENTEROLOGIA PEDIATRICA
Salvatore Cucchiara,
Department of Pediatrics - Sapienza University of Rome
Pediatric Gastroenterology and Liver Unit
University Hospital Umberto I, Rome

TECHNICAL AND SCIENTIFIC EVOLUTION OF GASTROENTEROLOGY
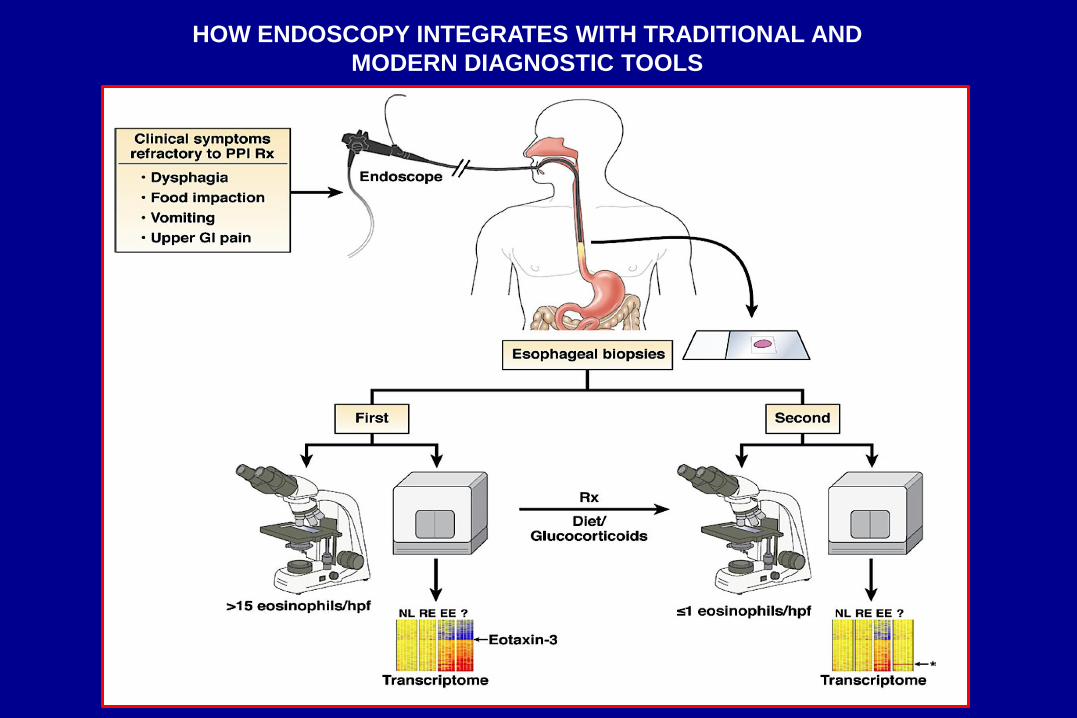
HOW ENDOSCOPY INTEGRATES WITH TRADITIONAL AND
MODERN DIAGNOSTIC TOOLS

HOW ENDOSCOPY INTEGRATES WITH TRADITIONAL
AND MODERN DIAGNOSTIC TOOLS
STOOL
CULTURE
MOLECULAR
MICROBIOTA
PROFILE
HISTOLOGY
MUCOSA
CYTOKINE
SCENARIO
MUCOSA
SPECIMEN
CULTURE

GI ENDOSCOPY IN PEDIATRIC GASTROENTEROLOGY: ITEMS
The indications for upper endoscopy in the pediatric age group are similar
to those for adult endoscopy, but…..
all infants, many children, and some adolescents cannot verbalize or
describe symptoms accurately
PEDIATRIC PECULIARITIES:
Training (acquisition and maintenance)
Equipment
Circumstances: i.e. ingestion of foreign bodies, caustic substances
Rigorous definition of indications
Preprocedure health evaluation
Sedation, analgesia and monitoring
Postprocedure monitoring and discharge

TRAINING IN PEDIATRIC GI ENDOSCOPY IS CRUCIAL !!!

UPDATING TRAINING OF PEDIATRIC GI ENDOSCOPISTS JPGN 2004;39:S589-S595
Use of GI and hepatobiliary-pancreatic endoscopy in children has
advanced during the past decades
Specific techniques for diagnosis and interventional procedures.
Training in pediatric endoscopy must keep pace with these
developments
Responsibility of national and international PEDGI
organizations to guide its membership in the skill acquisition during
fellowship training and in the maintenance-enhancement of those
skills.

Procedures are an integral
part of the practice of
pediatric gastroenterology
(trainees expected to demonstrate
competency in the performance of a
wide array of procedures).
Endoscopy and related procedures (eg, motility procedures), in continual state of evolution (technological advances in equipment, changes in other diagnostic disciplines, i.e. imaging, and shifts in the health care delivery system).
It remains important to establish
guidelines for pediatric
gastroenterology training
programs so that trainees are up to
date in the most current techniques
available.

………essential aspect of all
training programs is to
ensure that each trainee is
adequately exposed to
relevant procedures….
i.e. diagnostic and therapeutic upper
and lower GI endoscopy, percutaneous
endoscopic gastrostomy tube
placement, diagnostic and therapeutic
colonoscopy, endoscopic examination
of the SB (capsule endoscopy and/or
SB enteroscopy), ERCP, percutaneous
liver biopsy, rectal biopsy………………...,
manometry (esophageal,
antroduodenal, colonic and
anorectal), esophageal pH and
impedance monitoring, and breath
test analysis….


After completion of a training program in Pediatric Gastroenterology, Level 1
trainees should be able to do (JPGN 2013;56: S1-S38):
Recommend procedures on the basis of personal consultation and consideration
of specific indications, contraindications, and diagnostic and therapeutic
alternatives
Counsel the patient and family on bowel preparation and other pre-procedure
requirements as indicated
Select and apply appropriate sedation as indicated
Identify age-, size-, and condition-appropriate endoscopy equipment
Perform each indicated procedure safely, completely, independently, and
expeditiously
Interpret and describe endoscopic findings accurately
Integrate endoscopic findings or therapy into the management plan

After completion of a training program in Pediatric Gastroenterology, Level 1
trainees should be able to do (JPGN 2013;56: S1-S38):
Understand the inherent risks of endoscopic procedures, and counsel the patient
and family on the expected risks of benefits of, and alternatives to various
procedures
Recognize personal and procedural (including equipment) limitations and know
when to request assistance
Recognize and manage complications, including requesting assistance from
colleagues in related disciplines such as pediatric anesthesia, critical care,
pediatric surgery, or adult gastroenterology as required
Know how to clean and maintain endoscopic equipment and be familiar with the
Joint Commission and institutional standards for quality improvement, infection
control, sedation, and monitoring
Understand how an endoscopy unit is run, including how the unit interfaces with
the inpatient and outpatient gastroenterology practice and other services
(including pediatric anesthesiology)

GASTROINTESTINAL ENDOSCOPY AND GUIDELINES OF THE
MOST COMMON PEDIATRIC GI DISORDERS-CONDITIONS
FUNCTIONAL GASTROINTESTINAL DISORDERS
HELICOBACTER PYLORI
GASTROESOPHAGEAL REFLUX DISEASE
EOSINOPHILIC ESOPHAGITIS
CELIAC DISEASE
INFLAMMATORY BOWEL DISEASE
INTERVENTIONAL ENDOSCOPY

GASTROINTESTINAL ENDOSCOPY AND GUIDELINES OF THE
MOST COMMON PEDIATRIC GI DISORDERS-CONDITIONS
FUNCTIONAL GASTROINTESTINAL DISORDERS
HELICOBACTER PYLORI
GASTROESOPHAGEAL REFLUX DISEASE
EOSINOPHILIC ESOPHAGITIS
CELIAC DISEASE
INFLAMMATORY BOWEL DISEASE
INTERVENTIONAL ENDOSCOPY

OBJECTIVES: appropriateness of indications for upper gastrointestinal (UGI)
endoscopy in children with dyspepsia.
CONCLUSIONS: UGI endoscopy appropriate only for cases with a family history of
peptic ulcer and/or HP infection, > 10 year age, with symptoms persisting > 6 months
and affecting activities of daily living.
A) INDICATIONS TO UPPER GASTROINTESTINAL ENDOSCOPY IN CHILDREN WITH
DYSPEPSIA. Guariso G et al. JPGN 2010;50:493-9
VALIDATION OF PEDIATRIC ROME III CRITERIA OF FUNCTIONAL DYSPEPSIA
B) IMPACT OF PEDIATRIC ROME III CRITERIA OF FUNCTIONAL DYSPEPSIA ON THE
DIAGNOSTIC YIELD OF UPPER ENDOSCOPY AND PREDICTORS FOR A POSITIVE
ENDOSCOPIC FINDING. Tam YH et al. JPGN 2011;52:387-91
Rome III recommendations in dyspeptic children for alarm features and investigation
for HP: effective to identify children with a higher likelihood of organic diseases and
require upper endoscopy before a diagnosis of FD (HP and nocturnal pain)

GASTROINTESTINAL ENDOSCOPY AND GUIDELINES OF THE
MOST COMMON PEDIATRIC GI DISORDERS-CONDITIONS
FUNCTIONAL GASTROINTESTINAL DISORDERS
HELICOBACTER PYLORI
GASTROESOPHAGEAL REFLUX DISEASE
EOSINOPHILIC ESOPHAGITIS
CELIAC DISEASE
INFLAMMATORY BOWEL DISEASE
INTERVENTIONAL ENDOSCOPY
EVIDENCE-BASED GUIDELINES FROM ESPGHAN AND NASPGHAN FOR
HELICOBACTER PYLORI INFECTION IN CHILDREN. JPGN 2011;53:230-243
Recommendation 1:
Primary goal of clinical investigation of GI symptoms is to determine the
underlying cause of the symptoms (not solely HP infection presence)
Recommendation 6:
For the diagnosis of HP infection during EGD, gastric biopsies (antrum and
corpus) for histopathology must be obtained
Recommendation 7:
The initial diagnosis of HP infection should be based on either positive
histopathology + positive rapid UBT or a positive culture
Recommendation 14:
A “test and treat” (T&T) strategy is not recommended in children.
Primary goal of testing is to diagnose the cause of clinical symptoms…….a “T&T” strategy will not
provide this information in children…….current evidence does not support this practice in children.

GASTROINTESTINAL ENDOSCOPY AND GUIDELINES OF THE
MOST COMMON PEDIATRIC GI DISORDERS-CONDITIONS
FUNCTIONAL GASTROINTESTINAL DISORDERS
HELICOBACTER PYLORI
GASTROESOPHAGEAL REFLUX DISEASE
EOSINOPHILIC ESOPHAGITIS
CELIAC DISEASE
INFLAMMATORY BOWEL DISEASE
INTERVENTIONAL ENDOSCOPY

European Society for Pediatric Gastroenterology, Hepatology and Nutrition:
GUIDELINES FOR THE DIAGNOSIS OF CELIAC DISEASE, JPGN 2012;54:136-60

GASTROINTESTINAL ENDOSCOPY AND GUIDELINES OF THE
MOST COMMON PEDIATRIC GI DISORDERS-CONDITIONS
FUNCTIONAL GASTROINTESTINAL DISORDERS
HELICOBACTER PYLORI
GASTROESOPHAGEAL REFLUX DISEASE
EOSINOPHILIC ESOPHAGITIS
CELIAC DISEASE
INFLAMMATORY BOWEL DISEASE
INTERVENTIONAL ENDOSCOPY

Am J Gastroenterol. 2013 Apr 9. doi: 10.1038/ajg.2013.71. [Epub ahead of print]

ENDOSCOPIC FEATURES OF EOSINOPHILIC ESOPHAGITIS
furrowing and
vertical lines
mucosal rings and
whitish exudates

ACG Clinical Guideline: Evidenced Based Approach to the Diagnosis and Management of
Esophageal Eosinophilia and Eosinophilic Esophagitis (EoE). Am J Gastroenterol 2013 Epub

GASTROINTESTINAL ENDOSCOPY AND GUIDELINES OF THE
MOST COMMON PEDIATRIC GI DISORDERS-CONDITIONS
FUNCTIONAL GASTROINTESTINAL DISORDERS
HELICOBACTER PYLORI
GASTROESOPHAGEAL REFLUX DISEASE
EOSINOPHILIC ESOPHAGITIS
CELIAC DISEASE
INFLAMMATORY BOWEL DISEASE
INTERVENTIONAL ENDOSCOPY

Reflux esophagitis as the presence of endoscopically visible breaks in the
esophageal mucosa at or immediately above the GEJ.
Visible breaks in the esophageal mucosa: signs of greatest interobserver
reliability (operator experience is a component of interobserver reliability).
Grading severity of esophagitis useful for grading esophagitis and
response to treatment (the LA classification generally used for adults, but
suitable for children).
Endoscopically normal esophageal mucosa does not exclude NERD or
esophagitis of other etiologies
PEDIATRIC GERD CLINICAL PRACTICE GUIDELINES: JOINT
RECOMMENDATIONS OF THE NASPGHAN AND ESPGHAN. JPGN 2009; 49:498-547

Diagnostic yield of endoscopy greater if multiple samples of good size and
orientation are obtained from biopsy sites
Variables influencing validity of histology as a diagnostic tool for RE:
sampling error (patchy changes); no standardization of biopsy location,
tissue processing, and morphometric interpretation.
Histology may be normal or abnormal in NERD because GERD is an
inherently patchy disease. Histologic findings of eosinophilia, elongation
of papillae (rete pegs), basal hyperplasia, and dilated intercellular spaces
(spongiosis) are neither sensitive nor specific for RE
PEDIATRIC GERD CLINICAL PRACTICE GUIDELINES: JOINT
RECOMMENDATIONS OF THE NASPGHAN AND ESPGHAN. JPGN 2009; 49:498-547

GASTROINTESTINAL ENDOSCOPY AND GUIDELINES OF THE
MOST COMMON PEDIATRIC GI DISORDERS-CONDITIONS
FUNCTIONAL GASTROINTESTINAL DISORDERS
HELICOBACTER PYLORI
GASTROESOPHAGEAL REFLUX DISEASE
EOSINOPHILIC ESOPHAGITIS
CELIAC DISEASE
INFLAMMATORY BOWEL DISEASE
INTERVENTIONAL ENDOSCOPY
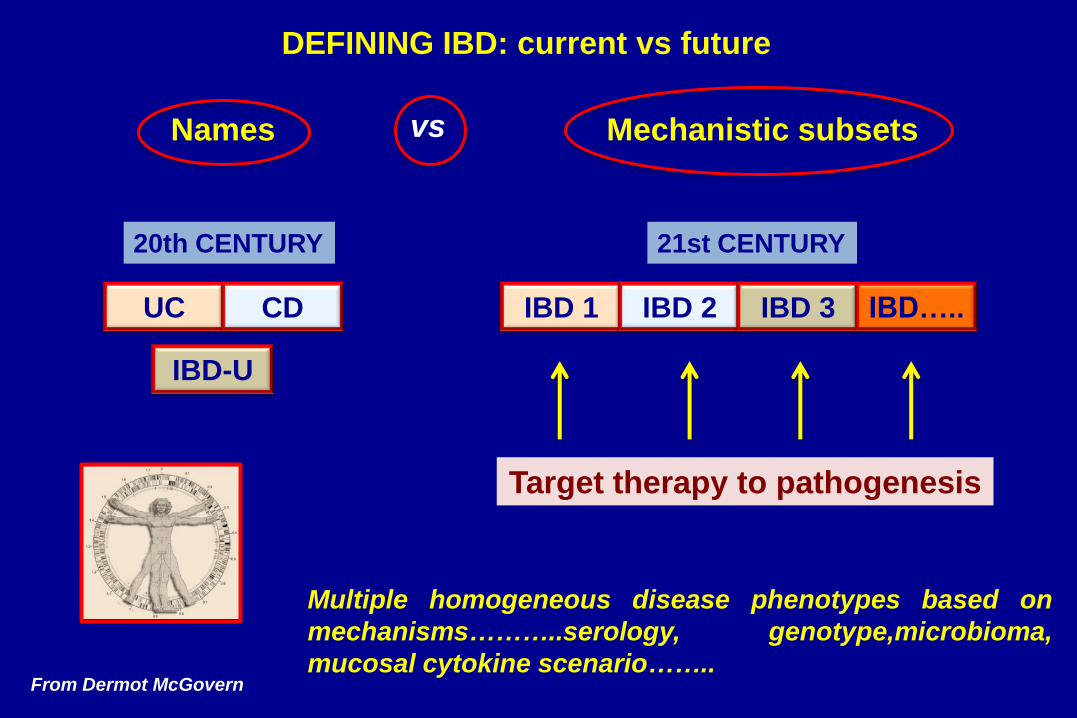
IBD 1 IBD 2 IBD 3 IBD….. UC CD
DEFINING IBD: current vs future
Names vs Mechanistic subsets
From Dermot McGovern
20th CENTURY 21st CENTURY
Target therapy to pathogenesis
Multiple homogeneous disease phenotypes based on
mechanisms………..serology, genotype,microbioma,
mucosal cytokine scenario……..
IBD-U
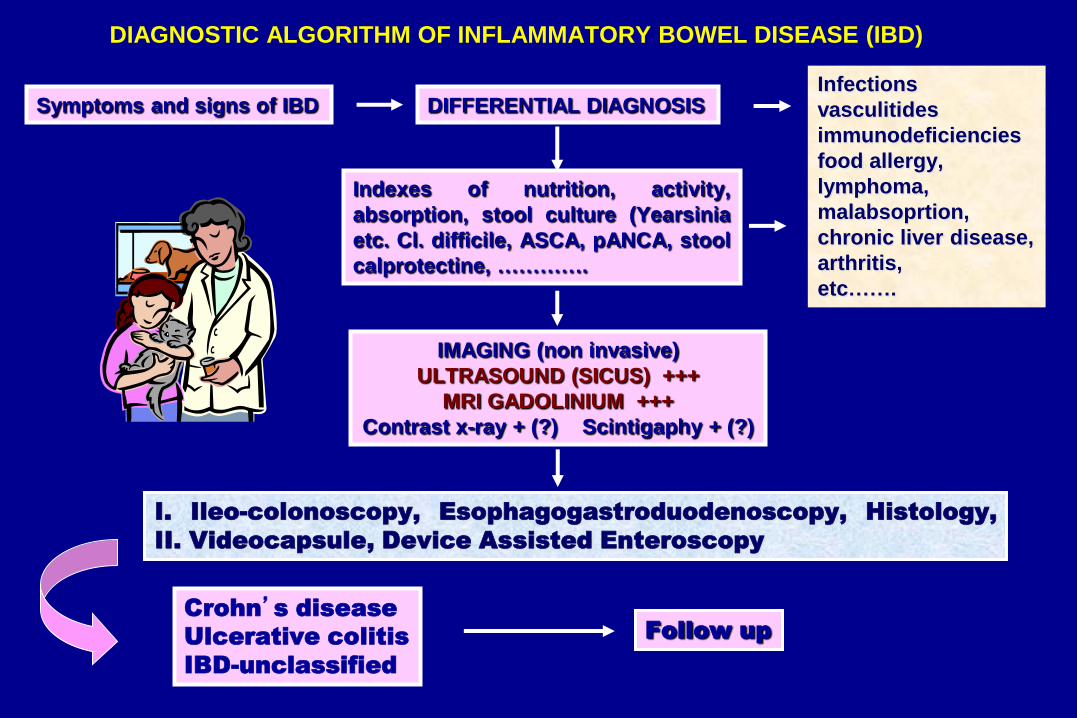
DIAGNOSTIC ALGORITHM OF INFLAMMATORY BOWEL DISEASE (IBD)
Symptoms and signs of IBD DIFFERENTIAL DIAGNOSIS Infections
vasculitides
immunodeficiencies
food allergy,
lymphoma,
malabsoprtion,
chronic liver disease,
arthritis,
etc…….
Indexes of nutrition, activity,
absorption, stool culture (Yearsinia
etc. Cl. difficile, ASCA, pANCA, stool
calprotectine, ………….
IMAGING (non invasive)
ULTRASOUND (SICUS) +++
MRI GADOLINIUM +++
Contrast x-ray + (?) Scintigaphy + (?)
I. Ileo-colonoscopy, Esophagogastroduodenoscopy, Histology,
II. Videocapsule, Device Assisted Enteroscopy
Crohn’s disease
Ulcerative colitis
IBD-unclassified
Follow up
Control symptoms
Mucosal healing (reduce inflammation)
Deep remission
Change disease course
Prevent relapse
Reduce complications
Optimize growth potential
Prevent surgery
Preserve bowel
Maintain adequate nutritional status
Improve quality of life
Short-Term
Long-Term
OLD & NEW THERAPEUTIC GOALS IN PEDIATRIC IBD

SURROGATE MARKERS FOR
MUCOSAL HEALING
AND DEEP REMISSION
• Fecal markers: calprotectin,
lactoferrin
• Serum markers: CRP
• Imaging methods: colonic US
• Capsule endoscopy: colonic WCE
• ………….HMGB1…
DDW 2013
Orlando, USA
DDW 2013
Orlando, USA

DDW 2013, Orlando, USA

DIAGNOSTIC ALGORITHM OF INFLAMMATORY BOWEL DISEASE (IBD)
Symptoms and signs of IBD DIFFERENTIAL DIAGNOSIS Infections
vasculitides
immunodeficiencies
food allergy,
lymphoma,
malabsoprtion,
chronic liver disease,
arthritis,
etc…….
Indexes of nutrition, activity,
absorption, stool culture (Yearsinia
etc. Cl. difficile, ASCA, pANCA, stool
calprotectine, ………….
IMAGING (non invasive)
ULTRASOUND (SICUS) +++
MRI GADOLINIUM +++
Contrast x-ray + (?) Scintigaphy + (?)
I. Ileo-colonoscopy, Esophagogastroduodenoscopy, Histology,
II. Videocapsule, Device Assisted Enteroscopy
Crohn’s disease
Ulcerative colitis
IBD-unclassified
Follow up
SIGENP MULTICENTER STUDY
2011;43:220-4

Rome Sapienza University, Naples Federico II University, Pescara PED-GI Hospital
Usefulness of wireless capsule endoscopy in paediatric inflammatory bowel disease. Dig Liver Dis
2011;43:220-4.


PATIENTS WITH SUSPECTED CROHN’S DISEASE (16) (GROUP A) (median age: 12.3 years; range: 7-18 years)
MRI – WCE: investigation of small intestine
CROHN’S DISEASE proximal jejunum (7), distal jejunum (4), proximal ileum (4), distal ileum (6)
Stricturing
Crohn’s disease,
successful EBD
Self-limited
enteropathy
Eosinophilic
Enteropathy in 2,
NSAID in 1
SINGLE BALLOON ENTEROSCOPY
10 patients - MRI: 7 with IWT and TE,
3 with IWT and SE; WCE: diagnostic of
CD in 3, suggestive of CD in 7
2 patients - MRI:
strictures (WCE
not performed)
3 patients - MRI:
normal; WCE:
unspecific
1 patient - MRI:
IWT and TE;
WCE: unspecific
Figure legend. CD: Crohn’s Disease; WCE: wireless capsule endoscopy; EBD: endoscopic balloon dilatation; NSAID: non steroid anti-inflammatory drugs; MRI: magnetic resonance imaging; MRI features: IWT= increased wall thickness; TE=transmural enhancement; SE=stratified enhancement.

Successful endoscopic
balloon dilatation
THERAPY: a) introduction of biologics in 10 patients on maintenance therapy with thioprine, b)
change of biological agent in 4 patients (from infliximab to adalimumab)
5 patients: IWT
and NSCE
3 patients: IWT and SE
3 patients: IWT and TE
3 patients:strictures
(2 with NSCE and 1 with SE)
SINGLE BALLOON ENTEROSCOPY
Inability to pass anastomosis
stricturoplasty in 4
(severe inflammation in areas
proximal to the MRI features)
Evidence of severe
inflammation
MRI: investigation of small intestine; WCE: not performed
Figure legend: MRI= magnetic resonance imaging; MRI features: IWT= increased wall thickness;
TE=transmural enhancement; SE=stratified enhancement; NCSE=non significant contrast enhancement
PATIENTS WITH ESTABLISHED CROHN’S DISEASE (14) (GROUP B) (previous surgery in 13) - (median age: 15.7 years; range: 12-18 years)

THE FUTURE OF PEDIATRIC GI ENDOSCOPY

GASTROINTESTINAL ENDOSCOPY AND GUIDELINES OF THE
MOST COMMON PEDIATRIC GI DISORDERS-CONDITIONS
FUNCTIONAL GASTROINTESTINAL DISORDERS
HELICOBACTER PYLORI
GASTROESOPHAGEAL REFLUX DISEASE
EOSINOPHILIC ESOPHAGITIS
CELIAC DISEASE
INFLAMMATORY BOWEL DISEASE
INTERVENTIONAL ENDOSCOPY

ADVANCES IN MODERN ENDOSCOPIC THERAPEUTICS
Important factors in performing successful
therapeutics
• Accessories
• Scope handling and experience
How often do we perform therapeutics and can we
predict what we will do ?
Interventions
• Haemostasis
• Injecting
• Argon plasma coagulation
• Heater probe or contact cautery
• Gluing
• Clipping and endolooping
• Polypectomy
• Stenting
• Dilatation
• Feeding tubes
• ERCP

Thank you for your
attention
Yesss, finally over !