cdijournal - hcpro farewell 23 advisor board members offer reflections superstar cdi 26 tips for...
TRANSCRIPT

January 2013 Vol. 7 No. 1
Director’s note 4Agenda set for 2013 conference
Peer audits 5Co-worker reviews provide insight into query efforts
Sepsis syndrome 10Coding Clinic advice leads to query questions
ICD-10 guidance 12Coding Clinic provides first of ICD-10 insight
Healthcare climate 13Trey La Charité, MD, says hospitals could be endangered
Meet a member 15Katy Good, RN, BSN, CCDS, CCS
Concurrent coding 16Efforts limited according to survey
Travel CDI 18New opportunities arise
Physician education 20CDI staff craft documentation newsletters
Fond farewell 23Advisor Board members offer reflections
Superstar CDI 26Tips for excellence to start 2013
cdiJournalSandy survivors share stories of recovery
Nearly 200 people lost their lives. More than 300,000 either lost their homes completely or suffered significant damage. In the floods that came with Hurricane Sandy, New Jersey ACDIS Chapter leader Deborah Gardner-Brown lost the first floor of her home to significant water damage.
Although Sandy only reached Category 1 status, the October storm extended almost 1,000 miles in diameter, according to the National Oceanic and Atmospheric Administration. Esti-mates of damage from the storm range from $50 to $90 billion.
In the weeks following the storm, ACDIS reached out to area members and associates, but many members could not be contacted due to power outages and business closings. Many more, thankfully, suffered only minor damage or inconveniences.
Hospitals in Manhatten were evacuated. Perhaps the hardest hit, New York University Langone Medical Center, saw flooding reach nearly 15 feet, which decimated its research, radi-ology, and emergency departments, according to a New York Times article.
In addition to NYU, Bellevue Hospital Center, Coney Island Hospital, and VA New York Harbor Healthcare System all remained closed as of mid-December, according to newspaper articles and ACDIS members in the area. Nearby, facilities struggled to handle the influx of patients migrating from closed facilities.
“A few hospitals had to increase their nursing staffs due to the increased census and overflow,” says New York City’s Five-Borough ACDIS chap-
ter leader Wanda Mejias-Gonzalez, RN, DDS, director of quality assurance and regulatory services at Wyckoff Heights Medical Center in Brooklyn.
Her home did not suffer any structural dam-age, although several colleagues were either per-manently or temporarily displaced. For a week following the storm, she had no electricity, no water. Two weeks after the storm she still had no heat or hot water.
Vital servicesAt Wyckoff, the CDI team is composed of
nurses. Although CDI efforts are not considered “vital services,” those with nursing backgrounds were needed. So during the height of the storm Mejias-Gonzalez told staff first to take care of their homes and families, but if they lived in the vicinity and could help out, they should do so.
“Some people live on the other side of town. The transportation systems were all stopped, so any
How to help
Although Hurricane Sandy hit the east coast
nearly three months ago many remain homeless
and in need of basic services. Here are a few agen-
cies still providing assistance and looking for addi-
tional help:
» American Red Cross www.nyredcross.org
» The Salvation Army https://donate.salvationar-
myusa.org/disaster
» NYC Service www.nycservice.org/pages/pages/8
» United Way http://action.unitedwaynyc.org/
page/content/uwsandyrecovery

2 January 2013 © 2013 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Advisory Board Susan Belley, M.Ed., RHIA, CPHQProject Manager3M HIS Consulting ServicesAtlanta, [email protected]
Timothy N. Brundage, MDPhysician ChampionKindred Hospital North Florida DistrictSt. Petersburg, [email protected]
Cheryl Ericson, MS, RNManager of Clinical DocumentationIntegrityMedical University of [email protected]
Robert S. Gold, MDCEODCBA, Inc.Atlanta, [email protected]
Fran Jurcak, RN, MSN, CCDSDirector, CDI PracticeHuron HealthcareChicago, [email protected]
James S. Kennedy, MD, CCS, CDIPManaging DirectorFTI HealthcareBrentwood, [email protected]
Glenn Krauss, BBA, RHIA, CCS, CCS-P, CPUR, FCS, PCS, C-CDIS, CCDSIndependent ConsultantMadison, [email protected]
Trey La Charité, MDPhysician AdvisorUniversity of Tennessee at KnoxvilleKnoxville, [email protected]
Gail B. Marini, RN, MM, CCS, LNCManager, Clinical DocumentationSouth Shore HospitalWeymouth, [email protected]
Dee Schad, RN, BSN, CCDSDirector Care Coordination and CDIClark Memorial HospitalJeffersonville, [email protected]
Donna D. Wilson, RHIA, CCS, CCDSSenior DirectorCompliance Concepts, [email protected]
Lena N. Wilson, MHI, RHIA, CCS, CCDSHIM Operations ManagerClarian HealthIndianapolis, [email protected]
Previous ACDIS board members:Cindy Basham, MHA, MSCCS, BSN,CPC, CCS (2007–2010)
Shelia Bullock, RN, MBA, CCM, CCDS (2008–2011)
Gloryanne Bryant, BS, RHIA, RHIT, CCS, CCDS (2007–2010)
Jean S. Clark, RHIA (2007–2010)
Wendy De Vreugd, RN, BSN, PHN,FNP, CCDS (2007–2010)
Garri Garrison, RN, CPUR, CPC, CMC (2008–2011)
Colleen Garry, RN, BS (2007–2010)
Robert S. Gold, MD (2007–2010)
William E. Haik, MD (2007–2010)
Tamara Hicks, RN, BSN, CCS, CCDS (2007–2010)
Robin R. Holmes, RN, MSN (2009-2011)
Pam Lovell, MBA, RN (2007–2010)
Shannon E. McCall, CCS, CCS-P, CPC, CEMC, CPC-I, CCDS (2007–2010)
Lynne Spryszak, RN, CPC, CCDS (founding member)
Colleen Stukenberg, MSN, RN, CMSRN, CCDS (2008–2010)
Heather Taillon, RHIA (2007–2010)
CDI Journal (ISSN: 1098-0571) is published quarterly by HCPro, Inc., 75 Sylvan St., Suite A-101, Danvers, MA 01923. Subscription rate: $165/year for membership to the Association of Clinical Documentation Improvement Specialists. • Postmaster: Send address changes to CDI Journal, P.O. Box 3049, Peabody, MA 01961-3049. • Copyright © 2013 HCPro, Inc. All rights reserved. Printed in the USA. Except where specifically encouraged, no part of this publication may be reproduced, in any form or by any means, without prior written consent of HCPro, Inc., or the Copyright Clearance Center at 978-750-8400. Please notify us immediately if you have received an unauthorized copy. • For editorial comments or questions, call 781-639-1872 or fax 781-639-7857. For renewal or subscription information, call customer service at 800-650-6787, fax 800-639-8511, or email: [email protected]. • Visit our website at www.cdiassociation.com. • Occasionally, we make our subscriber list available to selected companies/vendors. If you do not wish to be included on this mailing list, please write to the marketing department at the address above. • Opinions expressed are not necessarily those of CDI Journal. Mention of products and services does not constitute endorsement. Advice given is general, and readers should consult professional counsel for specific legal, ethical, or clinical questions.
ACDIS Director: Brian Murphy, CPC [email protected]
Associate Director: Melissa [email protected]
Membership Services Specialist:
Penny Richards, CPC
kind of travel was nearly impossible. Many people had downed trees. For others, it was difficult to even get out of their own buildings,” she says.
In a time of crisis, CDI specialists with nursing back-grounds are often asked to resume their old clinical support roles, says Barbara Hinkle-Azzara, RHIA, vice president of HIM Solution Strategy for Meta Health Technology, a division of Streamline Health Solutions, Inc., based in New York City.
“Let’s face it, when the power goes out the goal is likely to obtain any documentation at all,” she says.
Hinkle-Azzara was also lucky to have survived the storm relatively unscathed at home in New Jersey, aside from a downed tree and some minor damage. Meta/Streamline’s New York City office on 7th Avenue also luckily did not suf-fer from the widespread power outages due to a transformer explosion during the storm.
“Our building was somehow spared. For some reason we were in a pocket of the Chelsea area that wasn’t affected by the power outages that swept many areas of downtown,” Hinkle-Azzara says.
Disaster readinessThe Joint Commission requires facilities to implement
detailed disaster plans—plans that not only plot responses to natural and man-made calamities, but that thoroughly explain the roles and responsibilities of nearly everyone in the hospital, says Hinkle-Azzara. (For more information on this, read the January edition of our sister publication Briefings on The Joint Commission.)
Not surprisingly, such preparations require an extensive effort.
“It requires redundancies and backups; plans for who will be required to be on duty, who will stay at the hos-pital, and how responsibilities will be allocated,” says Hinkle-Azzara.
Hinkle-Azzara has experienced similar disasters before, including the major New York City blackout in 2003 and several hurricane scares. Although improving clinical docu-mentation may not be considered “vital” during a disaster, every hospital department plays an important role in the mechanics of healthcare. In her previous role as director of HIM, she would work long hours prior to the storm’s

© 2013 HCPro, Inc. January 2013 3
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
arrival and make arrangements to remain at the hospital for several days to respond to facility needs, whether related to providing health information or otherwise.
In the management of health records, disaster plans differ depending on the infrastructure of the facility, she says. With most facilities operating with some ratio of hybrid medical records, disaster plans need to account for the variances.
“The old mantra in terms of disaster training was to pay attention to the physical plant,” says Hinkle-Azzara. “The ironic part about that is that HIM and coding assets, including the staff and the records themselves, were gene-rally consigned to the basement. That doesn’t make a lot of sense when it comes to flood-related disasaters considering flooding typically begins in the basement.”
Disaster recovery conversations associated with Hurricane Katrina included an increased emphasis on moving away from paper to electronic health records (EHR), but an EHR does not guarantee access to health records.
“Back then you heard people say that everything would be safe and sorted out once we migrate to electronic records, but clearly the concerns of the physical plant don’t go away,” Hinkle-Azzara says.
Redundant protectionEHRs that use redundancy might be the best bet in a
disaster. Referring to reports of how one uptown New York City hospital reportedly fared, Hinkle-Azzara points to its stated ability to recover patient medical records.
“According to reports the hospital had redundancy [servers housed in New Jersey] outside of the immediate area. In the past this maybe meant microfilm copies of medical records being house off-site. Now it may refer to cloud computing or remote servers,” she says. “While the response to prior disaster situations like Katrina might have been ‘We need electronic records.’ Here the call is really for redundancy and about clear identification of roles and responsibilities within the facility.”
That’s essentially what happened at Wyckoff, says Mejias-Gonzalez.
“Every hospital has a policy in place for when the power goes out,” she says. “Here everything gets reverted to paper ‘DownTime P&P’ at the time the power goes out. Every record has a paper counterpart.”
For HIM or CDI professionals on-site during an emer-gency, ensuring accessibility to information should be the first priority, says Hinkle-Azzara. If the facility primarily operates electronically, make sure to have printed backups or a way to access those records, or at least some core clinical information. If the facility is primarily paper, be sure to have those in a safe place.
“The essence of documentation improvement is the importance of there being accurate documentation of care,” Hinkle-Azzara says. “During a disaster, that means ensuring some process is in place and that staff members are aware of the procedures and are following them.”
Return to routine
By early December, routines were slowly being righted.Some CDI programs’ missions may have been diverted
to handle more pressing HIM or nursing concerns, says Hinkle-Azzara. Those CDI programs which continued should be moving forward with record reviews and not look-ing back.
“You step back into the role once the ‘all clear’ is given,” she says. Any paper generated during the disaster needs to be scanned and tied back to the electronic record system. If the patient was discharged during the disaster, the coding department will need to code based on what documentation they have. If the patient was still in the facility once the CDI team renewed its efforts, those records should be reviewed, says Hinkle-Azzara.
Mejias-Gonzalez nevertheless worries about her fellow CDI professionals at facilities that remain shuttered.
“It is a double loss for many people,” she says. “They may have been affected by the storm, and then, on top of that, their facility is closed and they are essentially out of work.”
Call Hurricane Sandy a perfect case of Murphy’s Law, where anything that could go wrong, did go wrong. At least that was the situation for many in the devastated areas—from flooding to fires, power outages and injuries, home destruction and hospital closings.
“It is grim for a lot of people,” says Mejias-Gonzalez. “For many, all that preparation by the city, by their facilities, just didn’t work out. For me, thankfully, Sandy was mostly an inconvenience. Many others weren’t so lucky.”

4 January 2013 © 2013 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Director’snote
ACDIS 2013: Are you ready for Nashville?I’m writing this director’s note
in the final cold days of 2012, but my heart is already warming to thoughts of Nashville in springtime, the site of our 6th annual confer-ence. Save the date(s): May 21–23, 2013, at the Renaissance Nashville Hotel.
The dates above are correct: We have expanded this year’s conference to two and a half days to accommodate more of the great speakers and sessions you’ve come to expect from ACDIS. And we’ve kept the price of the con-ference the same.
What types of sessions will you find at the conference? Here’s a sample:
» A case study presented by a lawyer who successfully defended a hospital against allegations of fraud related to alleged improper physician queries and upcoding to document kwashiorkor.
» A session reviewing the new ASPEN malnutrition consensus guidelines and the physical components of today’s clinically based nutritional status evaluation.
» A panel session presenting results of a large-scale study, conducted by the University HealthSystem Consortium, to assess the accuracy and consistency of the documentation and coding of Agency for Healthcare Research and Quality Patient Safety Indicators. » A session focusing on the different types of encephalopathy and capturing brain-related severity of illness. It will cover “midline shift” radiographic findings that indicate vasogenic/cerebral edema when treated, along with identification of poten-tial underlying causes of the symptom diagnosis “altered mental status.”
» A number of ICD-10 sessions, from specific docu-
mentation requirements under the new coding system to assessing your vulnerabilities and devel-oping an educational action plan.
» Sessions on merging CDI processes and procedures with electronic health records.
» Reviewing medical records for quality measures, present-on-admission indicators, outpatient procedures, medical necessity admission criteria, and documentation of discharge codes.
» A number of sessions on engaging your physicians in CDI efforts.
» Sessions on RAC defense and compliance.
As usual, we will award the 2013 CDI Professional of the Year and two winners of Recognition of CDI Professional Achievement. We’re also bringing back our popular poster session and Day 2 Chapter Networking Lunch.
I owe great deal of gratitude to our 2013 Conference Committee for putting together such a great list of speakers. This group worked very diligently to review all submitted applications, call selected presenters, and decide on the best possible lineup. The committee includes the following members: Carol Beehler, Colleen Martin, Sharon Krug, Peggy Reap, Karen McKaig, Joyce Mosier, Andrea Majewski, Leah Taylor, Sherri Clark, Jennifer Love, Wendy Clesi, Jennifer Noel, Lynne Spryszak, and Shelia Bullock.
If you have any questions about the 2013 conference, please don’t hesitate to contact me. And I hope to see you all in Nashville!Take care,
Brian D. Murphy, [email protected], Ext. 3216

© 2013 HCPro, Inc. January 2013 5
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
“Documentation can be greatly improved by a properly functioning query process,” AHIMA says in its 2008 “Managing an Effective Query Process” practice brief.
But how can you tell whether your query process works? Peer-to-peer review of query practices and outcomes may provide a low-cost, effective option.
“Every profession that exists has some form of peer review processes,” says Donna Kent, RN, BSN, CCDS, CDI manager at Torrance (Calif.) Memorial Medical Center. “Healthcare is no different. CDI programs should be no different either.”
Laying the groundworkBefore you develop a peer review process, first establish
policies and procedures for how and when to query. These policies should be clearly communicated to the CDI staff and reviewed annually to appropriately reflect changes in industry guidance. Because query policies and procedures define standards for the query process, they serve as a gener-ally accepted common ground, says Donald Butler, RN, BSN, CDI program manager at Vidant Medical Center in Greenville, N.C.
Use those policies as a starting point for your audit processes, Butler says. The audit forms and actions need not repeat facility policy language verbatim, but they can and should refer to facility-specific documents and original industry recommendations, he says.
Without this source material guiding the peer audit process, CDI staff members may question its legitimacy.
“Those who want to do well in the CDI role will know about these standards and view the audit as an effort to obtain a level of professionalism within the CDI pro-gram that demonstrates an effective process,” says ACDIS Advisory Board member Fran Jurcak, RN, MSN, CCDS, CDI director at Huron Healthcare Consulting Group in Chicago.
Engaging staffEnsuring that CDI specialists support the audit process
is the second step. Kent remembers performing peer reviews as a nurse in the hospital. When she made the move to CDI, she lamented the lack of such audits. For some time Kent’s
staff was too small to make the peer audit process successful. With the recent addition of a temporary third CDI reviewer, however, the time seemed perfect to establish one.
Staff members, however, were skeptical, Kent says. They worried about the intent of the reviews. And they worried about the potential of punitive measures associated with mistakes.
“All of us, at one time or another, have experienced reviews that were punitive just for the sake of being punitive,” says Kent. “For peer-to-peer audits to be successful, they must be used as a learning and evaluation tool, not as some
sort of gotcha game.”“The value of peer-to-peer review comes from the abil-
ity of CDI staff members to learn from each other, to see what each other is doing and support process improvement,” Jurcak says.
Each person has his or her own style, strengths, and foibles, says Kent, who can look at a query and tell which staff member created it.
For example, in reviewing a record regarding excisional
Conduct peer audits to provide query practice insight
“Forpeer-to-peerauditstobesuccessful,theymustbeusedasalearningandevaluationtool,notassomesortofgotchagame.”
—Donna Kent, RN, BSN, CCDS
6 January 2013 © 2013 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
DEMOGRAPHIC Information
CDS Admit date D/C date Encounter # Reviewer
Date of review Final working DRG Billed DRG
General CDI process items
1 Initial review conducted <48 hrs Yes No
2 Adequate re-reviews (dependent on clinical condition and documentation status; anywhere from
daily to 2x weekly)
Yes No
3 Final working DRG (after any query resolution) matches billed DRG Yes No
3 A Appropriate PDX and procedures recognized Yes No N/A
3 B ODX influencing DRG assignment recognized Yes No N/A
3 C Significant ODX influencing ROM/SOI/LOS recognized Yes No N/A
4 Relevant clinical factors were identified during reviews (pertinent positive & negative/
normal) and relevant trends in documentation were recognized
Yes No
General CDI process items
5 No missed query opportunity (details in comments)
(alternative diagnoses were recognized, considered, and either queried or appropriately refrained
from query)
Yes No
6 Comments: N/A
Query specific items (N/A if no query posed) Each query contains or complies with:
7 If query forms utilized: appropriate form used AND form content was customized to the specific
case documentation, circumstances, and data
Yes No N/A
8 Nature of query (PDX, proc, CC/MCC, 2nd CC/MCC, SOI/ROM/LOS, clarify, POA, etc.) is identified
and recorded appropriately
Yes No N/A
9 Reason(s) for query:
* The clinical symptoms, indicators, or information are included;
* The specific documentation issue is described (legibility, consistency, etc.)
* Treatment is described that lacks a diagnosis
* Other:
Yes No N/A
Query specific items (N/A if no query posed) Each query contains or complies with:
10 The clinical indicators firmly support the query (i.e., not stretched)
(including recognition and use of broadly recognized clinical literature standards)
Yes No N/A
11 Succinct, clear wording of the query with a clear question posed Yes No N/A
12 Formatted in a user-friendly manner (appropriate use of bullets, avoidance of run-on sentences, etc.) Yes No N/A
13 Timely presentation
(i.e., adequate time for workup results to be in the record; initial physician documents
must be in record prior to the query posed)
Yes No N/A
14 Working DRG at time of query is appropriate to existent documentation Yes No N/A
CDI Audit Form—DRAFT

© 2013 HCPro, Inc. January 2013 7
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
debridement, one CDI specialist may read the record and see no query opportunities. Another CDI specialist may remem-ber a Coding Clinic reference regarding excisional debridement and determine a query opportunity does exist.
There may not be a right or wrong to this scenario, Kent says. Instead, there is an opportunity for the two staff mem-bers to discuss their views and the various options open to them during the query process. Through that dialogue, she says, comes learning.
“Over time I really hope that [the audit process] will [help us] come to a type of consensus about to how to conduct a medical record review and to do reviews consis-tently,” says Kent.
Although peer audits are not meant to be punitive, Kent still plans to provide oversight and regular reviews of the process to see what trends, if any, the audits illustrate.
“Otherwise you might have staff members say, ‘You had me do this extra work but you’re not doing anything with that information, so what difference does it make?’ ” Jurcak says. “The results of the audit need to be communicated and used to identify solutions for process improvement.”
Highlighting trends illustrated by the peer reviews allows managers to dig deeper into process problems, support the
need for additional CDI education efforts, provide evidence of physician noncompliance, and insight for educational opportunities, Jurcak says.
Creating an audit plan, toolTo launch her peer review process, Kent asked members
of her team to review five to 10 of each other’s charts per month. Jurcak suggests the same. Butler, who has nine CDI specialists, suggests requiring reviews of roughly 10% of total staff queries per month.
“It depends on how large the staff is,” says Jurcak. “They can do a couple of chart audits a week on a Friday afternoon, and they’ll have done five to 10 without it adversely affecting their productivity.”
Make sure the charts staff review are a random sample, says Butler, so that a good cross section of queries are examined. Audit queries for representation of disease types and representation of query reasons (e.g., specificity, legibility, lack of diagnosis).
If the staff is large enough, Butler also suggests having each chart reviewed blindly by two different peers to establish inter-rater reliability.
“If there is disagreement on any one case, then that record
15 Suggested answer options are presented appropriately
(Note: If was to confirm or rule out a diagnosis documented as possible/etc., then format of
options may be appropriate to differ from standard multiple choice)
Yes No N/A
15 A Open-ended question posed Yes No N/A
15 B Multiple choice: At least 2 clinically reasonable options for this pt diagnosis presented Yes No N/A
15 C Multiple choice answer format: includes other ______ and clinically undetermined Yes No N/A
16 Provider’s response was appropriately recorded in tracking software or tool Yes No N/A
17 Final result/impact of query appropriately recorded Yes No N/A
18 Inclusion of required data elements (patient identifiers, person posing query, contact phone #, etc.) Yes No N/A
19 Overall, query was non-leading Yes No N/A
20 Other query comments:
ADMINISTRATIVE SECTION
Inter-rater reliability: 90% agreement on findings between 2 peers conducting reviews
If no, third-level review 90% agreement with findings?
Source: Donald Butler, RN, BSN, CDI program manager at Vidant Medical Center in Greenville, N.C.

8 January 2013 © 2013 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
can be referred to the CDI team leader or manager,” he says. “If the CDI program is a one-person shop, consider reaching out to a team member in coding or compliance to help.”
Involve CDI staff in crafting the program’s auditing process from the start. This step helps win their support, but also, as the adage goes, “two heads are better than one” and staff members may offer interesting ideas about how to proceed, says Kent.
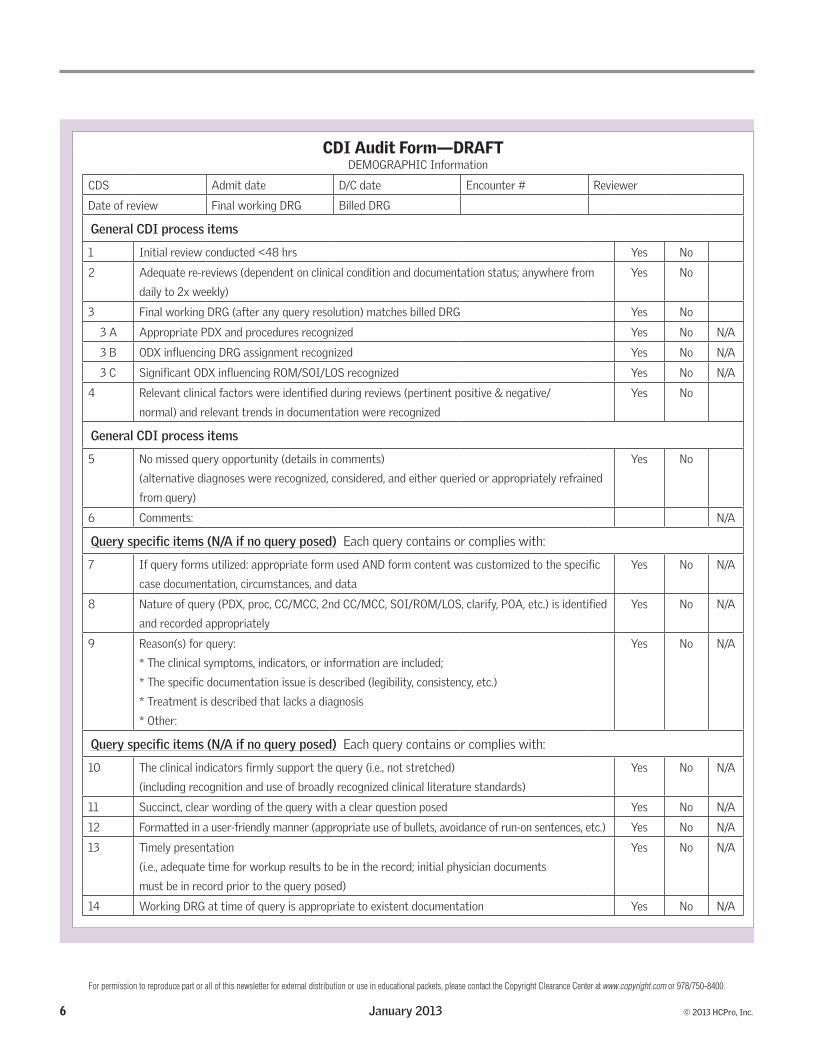
Regardless, a standard form used by all staff makes the effort less subjective, Butler says. In his sample form (see p. 6), specific questions include only “yes,” “no,” or “not applicable” responses. This particular tool can be adapted to the focus of your audit be it purely query compliance, accura-cy of outcomes data, or analysis of the entire CDI program. Butler suggests starting with a smaller, more concentrated focus to support the long-term auditing efforts.
“This allows you to load the information into a database and calculate percentages for an entire team as well as for the individual CDI specialist over time. The percentages, graphs, and comparison of trends helps set standard levels of performance as well as to identify variances,” Butler says. “Ideally, there would be national benchmark data to compare yourself to.”
Jurcak’s sample audit tool (see p. 9) also includes yes and no responses. However, she assigns a point system—“yes” answers receive one point, “no” responses receive zero—that totals 20 points. A passing grade is 18–20, she says. “It makes it more objective than a simple ‘I disagree with the way you handled that query.’ ”
Both samples begin with general query process questions, such as the time frame of the initial record review. This should coincide with your facility’s policies—some require initial review within 24 hours, others 48 hours. Both tools ask about accurate/appropriate capture of initial working DRG and any potential secondary diagnoses.
The audit tools also ask staff to determine the following: » Whether the query was necessary » Whether the language used in the query was leading or otherwise inappropriate
» Whether the query introduced new information from the health record
Both audit forms also look for inclusion of relevant clinical factors in the query and both delve into the structure
of the query forms themselves. “Through the process you may find that staff pose a lot
of queries but they aren’t following up with physicians,” says Jurcak. “If they aren’t following up, there isn’t any learning going on, there isn’t a lot of anything going on. What’s the point of leaving a bunch of queries if they aren’t valid or if the physician isn’t responding?”
Offering educationThe environment where peer reviews takes place needs
to be nurturing, says Kent. There are any number of ways to foster this. If the staff is small and the number of audited records reasonable, consider including audit reviews as an agenda item in monthly team meetings.
For larger staffs, a separate monthly meeting focused on sharing thoughts and lessons learned during the auditing process can help.
CDI team leaders or managers should review data quarterly for a more neutral overview, identify trends, and report those trends back to the team seeking their input on opportunities for improvement.
Through self-auditing, it may become apparent that an individual either doesn’t have the interpersonal or analytical skills required for the position. The audit process can help identify those deficiencies, says Jurcak. It is then incumbent on the management/leadership of the program to provide the educational opportunities to help.
“Maybe they are doing what they are told to do, but the process isn’t working. Then you need to investigate fur-ther to see how the program is perceived within the facility and work with staff to resolve those problems,” says Jurcak.
Determine whether the concern is a process issue, an educational concern, or external/temporary oversight, she says.
To ensure program success, you need a plan for remedia-tion of any identified concerns. First, identify the nature of the problem. Then create an action plan for improvement. Set a reasonable timeline to meet those goals and make sure that success can be concretely measured, Jurcak says. Then start the whole process over again.
“You need to use the audit process to help CDI special-ists and process improvement resulting in overall program improvement,” Jurcak says.

© 2013 HCPro, Inc. January 2013 9
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
F. Jurcak, 9/2012
CDI Quality Review CDI Specialist Name__________________________________ Date Reviewed_____________________
Account Number_____________________________Coder_____________________________________
TOPIC
SCORE Yes = 1 No = 0
CDS Initial Review Process Record reviewed within one business day of admission
Yes
No
Initial and potential DRG assignment supported with treatment, monitoring, and/or evaluation etc.
Yes
No
Initial and potential secondary diagnoses (CC/MCC) supported with treatment
Yes
No
Patient demographics entered accurately into the CDI Tool? Yes No Identified query opportunity initiated? Yes No All potential queries were identified Yes No Initial DRG and potential DRG accurately reflect query impact Yes No Query Process Was the query necessary, based on the need for Present On- Admission status, clinical indicators for a higher degree of specificity, and/or conflicting, incompl ete, or ambiguous (diagnoses that may have multiple impressions) documentation?
Yes
No
Does the query include accurate patient risk factors? Yes No Does the query include accurate signs and symptoms? Yes No Does the query include accurate patient treatment? Yes No Was the query addressed to the appropriate provider (based on the query policy)?
Yes
No
Follow-up Process Query response identified? Yes No Follow-up documentation reflects physician response or required next steps to ensure physician response
Yes
No
Additional physician documentation is noted in CDI Tool Yes No Follow-up documentation in CDI Tool reflects the current DRG Yes No Escalation of query occurred appropriately Yes No Reconciliation Answering physician is identified in CDI Tool Yes No Type of query is accurate in CDI Tool Yes No Missed coding opportunity is identified by the CDS and communicated via policy and documented in the follow-up notes
Yes
No
TOTAL SCORE (out of possible 20) Acceptable score is 18 of 20
For any "No" responses, please explain in the comments section.
Source: Fran Jurcak, RN, MSN, CCDS, CDI director at Huron Healthcare Consulting Group in Chicago.

10 January 2013 © 2013 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Coding Clinic prompts fresh sepsis educationThe phrase “sepsis syndrome” is starting to appear in
medical records these days, but unfortunately it’s a term that requires further clarification. When it’s used, CDI staff/ coders should query the physician to clarify the condition being treated. That’s the latest guidance from AHA’s Coding Clinic for ICD-9-CM released in Second Quarter 2012 (pp. 21–22).
“Sepsis is something we all struggle with,” says Katy Good, RN, BSN, CCDS, CCS, AHIMA-Approved ICD-10-CM/PCS Trainer and CDI program coordinator at Flagstaff (Ariz.) Medical Center. Physicians at Flagstaff understand the documentation requirements related to sepsis, she says. And her CDI staff doesn’t typically have to query for clarification, although it does sometimes need additional specifi city to iden-tify the underlying cause of the infection.
However, the latest guidance which calls out “sepsis syndrome” poses new difficulties for Good and her team.
“We were never even aware that physicians used the term ‘sepsis syndrome’ before, and now it is popping up in docu-mentation all over the place,” Good says. “It’s interes ting, from time to time some rogue physician will start using a term and if you don’t catch it, all of a sudden everyone is using it.”
The original definition of sepsis syndrome was “septic shock,” says ACDIS Advisory Board member Robert S. Gold, MD, CEO of DCBA, Inc., in Atlanta.
“The term has been played with and manipulated and now has little resemblance to the original intent of the clini-cal language. Just as the term ‘urosepsis’ evolved, so has this and many physicians consider it merely equivalent to sys-temic inflammatory response syndrome,” says Gold.
The trick is how to ask physicians to provide clarification without appearing to lead them to a diagnosis of “sepsis” or “septic shock.”
Querying for urosepsis is easier, says Good, because there are clearly other options for the physician. However, in this instance, simply posing the question could be seen as leading.
“Physicians want to be helpful and compliant. I am nervous we’ll end up with a situation where we query for sepsis syndrome because the physician doesn’t understand why we’re asking the question. He or she will think we are looking for something completely different, document that in the record, and we will end up with something else entirely that is not clinically supported at all,” Good says.
To resolve the matter, Good and her team have revised their sepsis-related query templates. Unified templates pro-vide one way to ensure that the whole team communicates the same message in the same method. “It makes it more defensible on our side when either physicians raise questions about the clinical aspect of the query or if the results of the record are contested by auditors,” says Good.
But drafting a consensus-driven template takes time. In the interim, Flagstaff CDI specialist used its typical sepsis query form.
Gold offers similar advice. Specifically, he recommends reviewing the sample sepsis query included in AHIMA’s Guidelines for an Effective Query Process. “If your medical staff doesn’t know what sepsis syndrome is, and you introduce the term, then all you’re doing is leading them down potentially dangerous garden paths,” Gold says.
However, understanding the specific condition—such as simple pneumonia or sepsis due to pneumonia, or whether the patient has a simple urinary tract infection or sepsis due to an indwelling urinary catheter, or whether the patient
Additional resources
» Q&A: Sepsis vs. SIRS
Ω www.hcpro.com/acdis/details.cfm?content_id=245973
» Address these common Q&As related to SIRS documentation
Ω www.hcpro.com/acdis/details.cfm?content_id=229305
» Tip: Take time for a sepsis refresher
Ω www.hcpro.com/acdis/details.cfm?content_id=241295
» Tip: Maintain sepsis focus under RAC scrutiny
Ω www.hcpro.com/acdis/details.cfm?content_id=244199
» “Sepsis Coding and Documentation: Case Studies to Prev ent
Common Mistakes”
Ω www.hcmarketplace.com/prod-8353

© 2013 HCPro, Inc. January 2013 11
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
has simple pancreatitis or a pancreatic abscess—will help the CDI staff draft a more accessible query and enable the team to solicit the needed information from the physician, Gold says.
Although Coding Clinic guidance clearly spells out the need to query the physician when the term “sepsis syn-drome” appears, it does not dictate when or how to query. At times, says Good, physicians may write “sepsis syndrome” in the medical record but in the discharge summary simply document “sepsis” or “septic shock,” which the coder can then use to code the condition. She suggests that queries for “sepsis syndrome” might best be left for situations where the phrase is used in the discharge summary.
Like so many other situations, providing clarity may come down to education.
“We simply need to educate the physicians not to use this term, just the way we did with urosepsis, because the guidance says sepsis syndrome lacks specificity,” says Good.
She created a quick poster and hung it around the facility (see below). You can use the emergence of “sepsis syndrome” as an opportunity, Good says. Explain that this term is not an adequate term to code sepsis, and inform physicians that you will have to query for clarification if that phrase is document-ed. Add some additional reminder language regar ding guidance around documentation for systemic inflammatory response syndrome, septicemia, and septic shock, too.
The Tip for this Week is: Sepsis Syndrome
Source: Katy Good, RN, BSN, CCDS, CCS, CDI program coordinator at Flagstaff (Ariz.) Medical Center.
Per coding guidelines, the term “SEPSIS SYNDROME” is not adequate to code SEPSIS.
If possible, please refrain from using this phrase when referring to the subset of symptoms generally associated with SEPSIS.
When this phrase is seen in the documentation, the CDS or Coder will be required to submit a query to the physician to clarify the diagnosis. As a reminder, Systemic Inflammatory Response Syndrome (SIRS) is defined as two or more of the following:
1. Fever 2. Tachycardia 3. Tachypnea 4. Leukocytosis
SIRS with a (suspected) infectious source = SEPSIS SEPSIS with Organ Dysfunction = SEVERE SEPSIS Suggested documentation of Sepsis is (for example): “patient presents with leukocytosis and fever, suspect UTI as source, meets criteria for Sepsis”.
Questions? Call/E-mail _______
Source: Katy Good, RN, BSN, CCDS, CCS, CDI program coordinator at Flagstaff (Ariz.) Medical Center.

12 January 2013 © 2013 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
ICD-10codingcorner
Recap of Coding Clinic, Fourth Quarter 2012AHA Coding Clinic for ICD-9-CM released its first ICD-
10 coding guidance in its Fourth Quarter 2012 issue. The guidance is welcome as the first official coding regulations concerning ICD-10 to come out to date, other than the ICD-10 Official Guidelines for Coding and Reporting.
HCPro CDI education director Cheryl Ericson, MS, RN, CCDS, CDIP, says the guidance, while helpful, does not address big issues such as defining chronic conditions (i.e., COPD, diabetes, obesity), so they are considered reportable/always clinically significant in the inpatient setting regardless of the “absence of documented interven-tion or further evaluation, (see Coding Clinic, Third Quarter 2011, p. 4, and Third Quarter 2007, pp. 13–14). Nor does it address whether you can consider the term “acute exacer-bation of a chronic condition (heart failure)” as acute-on-chronic (see First Quarter 2009, p. 7), for example.
Coding Clinic for ICD-9-CM provides such direction, but that guidance does not carry over to ICD-10, Ericson notes.
The following is a recap of the issue with an eye toward what it means for CDI specialists.
Acute exacerbation of asthma and status asthmaticusCoding Clinic clarifies that you should only assign a code
for the more severe condition (i.e., status asthmaticus) if a physician documents “acute exacerbation of asthma and status asthmaticus” together. This concept applies more broadly to ICD-10 as well.
“We’re going to see a trend of that in ICD-10—you start with the more severe condition and code to the greatest depth of severity,” Ericson says. “For example, ICD-10-CM chapter-specific coding guidelines for Chapter 1 indicate that once SIRS of a noninfectious origin becomes sepsis or severe sepsis, then you no longer code the SIRS.”
The tabular list reinforces this chapter-specific guideline as both sepsis and severe sepsis follow an Excludes1 note, meaning that these codes are mutually exclusive with SIRS.
Rib resection with reconstruction of anterior chest wallThis entry underscores the changing nature of procedure
coding under ICD-10-PCS and how coders (and CDI
specialists reviewing operative notes) will have to be on their toes regarding the nature of root operations. In this case, even though a physician documented the term “resec-tion,” the coder has to report the root operation “excision” in order to comply with ICD-10-PCS requirements. That’s because the physician removed a segment of the rib but did not cut it out completely, without replacement, which is what defines “resection” in ICD-10.
“The whole premise of this Q&A reinforces the A11 coding guideline for PCS that states, ‘It is the coder’s respon-sibility to determine what the documentation in the medi-cal record equates to in the PCS definitions. The physician is not expected to use the terms used in PCS ... ’ ” Ericson says. “Even though the physician specifically used the term ‘resection,’ the root operation is ‘excision.’ You can’t just code what the physician writes.”
In short, your ICD-10-PCS education should not focus on teaching providers the root operations, Ericson says. Rather, focus on ensuring that the documentation is suffi-cient for the coder to apply the correct root operation.
Sequencing of acute MI with subsequent infarctionAlthough also spelled out in the ICD-10 Official Guidelines
for Coding and Reporting, this entry makes it clear that you should report an initial (new) myocardial infarction (MI) using an I21 code, and an I22 code for a subsequent MI. A subsequent MI is defined as any MI that occurs within 28 days (four weeks) of an initial MI.
Note that under ICD-9-CM, a subsequent MI is defined as occurring within eight weeks of an initial MI, so the change in ICD-10 to four weeks/28 days is a significant change.
“I stress that four weeks is not a month—a month is 30 or 31 days, not four weeks,” Ericson says.
An immediate takeaway is to start asking your physicians to document how many weeks it has been since the patient had his or her initial MI, if they are not already doing so. Better yet, ask them to document the date of the initial MI.
“Start asking now and get the physicians in the habit of providing that information,” she says.

© 2013 HCPro, Inc. January 2013 13
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Don’t try to explain the ICD-10 change from eight weeks to four weeks, since physicians will likely view it as an obscure coding rule.
Ericson also notes that if a physician documents the term AMI rather than specifying the event as a STEMI or NSTEMI, chapter-specific guidelines direct a coder to report the event as a STEMI of unspecified site.
This guidance can negatively affect the American Heart Association’s Mission: Lifeline® quality measures, which may result in an artificial increase in STEMIs in your facility.
“You may not have favorable data with the inclusion of all unspecified AMIs,” Ericson says. To avoid this situation, ask your physicians to be specific in their documentation, differen-tiating STEMI vs. NSTEMI, transmural MI vs. nontransmu-ral MI, as well as providing the location of the infarction.
Crohn’s disease with rectal abscessCoding Clinic clarifies that you can assign combination code
K50.014 (Crohn’s disease of the small intestine with abscess) along with code K61.1 (rectal abscess) to identify the specific location of the abscess when a patient presents with Crohn’s disease of the small intestine with a rectal abscess.
The takeaway for CDI specialists: Ask your physicians to link the Crohn’s disease with the abscess.
Initial encounter for fracture malunionThis entry highlights episodes of care, noting that it’s
more important to accurately capture the episode of care than the current condition of the fracture in the event of a patient who delays seeking treatment until after a fracture has begun to heal.
Even though the initial episode of care code (S62.002A) does not allow the coder to capture the status of the fracture as a malunion, Coding Clinic declares it is more important to record whether the event was an initial episode of care.
“As long as it’s the first time you’re seeking treatment, then it’s an initial episode of care,” Ericson says.
Editor’s note: Ericson is the CDI education director for HCPro, Inc., in Danvers, Mass. She teaches the ICD-10 for CDI Boot Camp, details of which can be found at www.hcprobootcamps.com/ courses/10051/overview. Contact her at [email protected].
by Trey La Charité, MD
Medical schools exist to train physicians to care for sick people. I chose to be a hospitalist path because I see the value of managing issues found only in an acute care setting. I
am the most professionally satisfied when I see a patient with a problem list of 20–25 medical conditions and know that I can help him or her.
As my career in medicine progresses however, I find myself doing more and more that does not involve direct patient care. How did this happen? I have come to the unsettling conclusion that my hospital is under attack. If you haven’t noticed, your facility is as well. Furthermore, as a physician advisor to CDI, I feel obligated to protect and defend my hospital.
The simple fact is that if I can’t help keep my hospital’s
Hospital status: Endangered!doors open, I will not have a place to treat sick, complicated patients. More importantly, the patients in my area of the country may not get the care they need. Simple economics is the root of my fear of hospital closure. Hospitals, as they exist today, are on the endangered species list.
Changing habitatThe constant struggle medical facilities face has several
facets. First, the Medicare trust fund is projected to run out of money in 2024. Will our government fix Medicare? With no tangible solution in sight, CMS is desperately trying to extend the available Medicare dollars as far as possible. How does one extend something? You use less of it by carefully rationing it.
In our world, this means reducing reimbursements to providers, both physicians and hospitals. In addition, CMS has also developed an aggressive strategy of trying to take back previously earned reimbursements through its Recovery

14 January 2013 © 2013 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Auditor programs. The private insurers, taking their cue from CMS, have instituted similar review programs in the hopes they, too, can regain funds they previously paid out.
The combined result of reduced reimbursements and the auditor efforts means that your facility has fewer resources year after year to provide the care your ever increasing patient population desperately needs.
The second component of this troubling conundrum is the rising expectation that our providers and facilities must provide “better care.” What is “better care?” As a broad generalization, this means improved patient outcomes, fewer complications, and lower costs. Every year CMS, the Agency for Healthcare Research and Quality, The Joint Commission, Leapfrog, and others add additional performance metrics that facilities must meet or risk losing some portion of needed reimbursements.
While all hospitals can improve their safety records, outcomes, complication rates, and costs per case, I have to wonder whether these financial ties to quality reporting represent the best mechanism to push for the achievement of these noble improvement goals. Failure to meet these goals means hospitals have reduced operating margins to effect the necessary changes. Our facilities are expected to per-form better and better each year while receiving less and less reimbursement to achieve that performance level.
Third, our government has embarked on a strategy of driving healthcare reform by encouraging direct provider competition. The theory goes that if two facilities’ data are available on the Web for public scrutiny, patients will choose the facility whose data shows better outcomes, fewer compli-cations, and lower costs.
Therefore, your facility is probably spending great sums of money, as mine is, in the effort to make your publicly reported data look better than the competition down the street. The obvious risk is that if your data doesn’t look as good as or better than your competition’s, your patient popu-lation may migrate away from your doors.
What about that competition down the street? They are trying equally hard to make their data look better than yours.
Whether you are for or against this approach, this sort of Consumer Reports strategy is here to stay.
The fourth problem facing our hospitals is the private insurers. Private insurance companies are trying their own version of influencing patient choice by adjusting copays
based on provider performance. Their plans mean that “poor performing” providers will have a reduced percent-age of their services covered by the insurer while the “better performing” providers will have their services fully covered. A patient is more likely to choose a provider whose insurance will pay 100% of the bill versus a provider where the insur-ance will only pay 80% of that same bill. The reality is that most patients simply cannot afford to go to a provider whose services are not fully covered. Additionally, if a provider does get “downgraded” by an insurer, getting back into that insurer’s good graces will take significant time and effort. Obviously, improving a provider’s performance data takes time as most of the reported metrics are averages. Will your facilities or your physicians have time to improve those metrics before the flow of new patients dries up?
Environmental impactWhile I am not an economist, the combination of
attacks that hospitals now face seems to be an untenable long-term situation. Unless mitigated in some fashion, I am fearful of what the face of healthcare will look like when I need inpatient hospitalization. For me, all this raises a series of concerns:
Will there be any hospitals left open to take care of me? Will those remaining open hospitals have any empty
rooms, or I will I be stuck in a hall stretcher for the duration of my hospitalization due to overcrowding?
Will hospitals be forced to band together into only a handful of “super” systems sharing the resources to survive?
Remember what happened to American car manufactu-rers? During the 20th century, they were economically squeezed down to four companies and then to just the current three survivors. Will hospitals then have to face a “bailout” similar to the automobile industry?
Will qualified people pursue careers in medicine?In my own situation, I was 30 years old before I ever
made more than $12,000 in a year. Additionally, I had over $100,000 in school loans to pay off when I finished my medical training. Should I encourage my children to pursue careers as physicians?
Today’s hospitals are a dying breed. A hospital is an amazing and wonderful “animal” that accomplishes fantastic things. I cannot imagine working outside of the hospital

© 2013 HCPro, Inc. January 2013 15
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Meetamember
Contributor finds ‘gold mine’ in networkingEditor’s note: If you spend any time on the ACDIS networking
group “CDI Talk,” you’ve seen Katy Good’s frequent commentary. She’s very active in CDI matters, both through ACDIS and at Flagstaff (Ariz.) Medical Center, where she is the CDI program coordinator. Now, you can get to know a little more about her in this quarter’s “Meet a member” feature.
Katy Good, RN, BSN, CCDS, CCS, AHIMA-Approved ICD-10-CM/PCS Trainer, has been in the CDI field since January 2011. She began her career as a critical care nurse at Massachusetts General Hospital in Boston before moving to northern Arizona, where she worked for Indian Health Services in a rural ER and in primary/ prenatal care.
CDIJ: Why did you get into this line of work? KG: To be honest, I didn’t even know what CDI or a
DRG was when I decided to apply. I was approached by a
former coworker who was looking to fill this position and she asked me to apply. I will admit I was mainly intrigued by the promise of a flexible schedule. However, I have found that this area suits me and I have been very happy in this new adventure.
CDIJ: What has been your biggest challenge?KG: Adjusting out of patient care. I now work from
home and I miss the social interaction of work.CDIJ: What has been your biggest reward?KG: I look back on the knowledge I have gained in less
than two years and I am amazed by how far we have come. We started with a program that had gone unstaffed and forgotten and now have a small but growing team and are seeing the direct impact of our work.
CDIJ: Can you mention a few nuggets of information you’ve received from colleagues on “CDI Talk” or through ACDIS?
KG: When I first took this position, I literally spent
environment. I love my hospital, and I am the physician and person I am today because of the training and experiences I have had the good fortune to receive at my facility.
We provide excellent patient care. I worry that this facility will not be able to withstand the collapse of our healthcare system that looms in the distance.
Who will take care of me and my family when we need medical care?
What is the United States patient population going to do without hospitals?
These thoughts keep me up at night. I would like to see our system fixed before my fears become reality.
How to adaptWhy do I see fewer patients these days? I make more of
a difference for my facility’s patients in the non-patient care roles I perform than I do as a practicing physician. How? It’s simple math. By working hard to make sure my hospital’s data looks better than the competition’s and by defending this facility against the various unscrupulous recovery raid-ers, I ensure that my hospital and my colleagues have the
resources needed to take the best care possible of our patient population.
As a hospitalist, I might have anywhere from 17 to 24 patient care encounters a day. However, since my hospital has more than 500 licensed beds, I consider myself to actually have about 500 patient care encounters a day in my non-direct patient care roles.
I like that math. I believe I better protect my hospital as a physician advisor than as a physician. If you were missing some enthusiasm for your role in the world of CDI, perhaps my fears will infuse you with some added vigor for the new year.
Editor’s note: La Charité is a hospitalist at the University of Tennessee Medical Center at Knoxville and a member of the ACDIS Advisory Board. He is board certified in internal medicine, a clini-cal assistant professor with the Department of Internal Medicine, and serves as the physician advisor for his facility CDI program, coding and Recovery Auditor response teams. His comments do not necessar-ily reflect those of UTMCK or ACDIS. Contact him at [email protected].

16 January 2013 © 2013 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Concurrent coding efforts are limited in CDI practices
hours poring through the ACDIS site. I asked a million questions (which now seem ridiculous) on “CDI Talk.” I would say my experience has been less about finding nuggets than the gold mine of assistance and knowledge shared by ACDIS and its members throughout the site.
CDIJ: If you could have any other job, what would it be? KG: It’s hard for me to imagine my life as anything other
than what it is. This is just my personality. I have a lot of interests though and entered college intent on studying Latin American studies and joining the Foreign Service.
CDIJ: What was your first job?KG: I didn’t work in high school; my first job was
working in the university library during my freshman year of college.
CDIJ: Do you mind telling us a little bit about your family.KG: My husband, David, and I have been married for
seven years. He is also a nurse and is currently in graduate school to become a CRNA. Our son, Griffin, turned 5 in August and our daughter, Rozlyn, will be 3 in December. We are expecting our third child, a boy, in December.
CDIJ: Tell us about a few of your favorite things:KG: Vacation spots: We have not done any big international
trips since having our children. We try to fit in an annual ski vacation every winter as well as a trip to the Gulf Islands in the summer. We live far from all our family, so we spend much of our time off visiting family.
Hobbies: I spent a lot of time cooking! Also, basic sewing, knitting, crafting, and reading.
Non-alcoholic beverage: Root beer.Foods: All of it! I love to cook … and eat! I especially
enjoy seafood and fruit. I have an enormous sweet tooth.Activity: I enjoy going to the gym, skiing/snowboarding,
hiking, and enjoying family activities. Editor’s note: CDI Journal introduces an ACDIS member in
each issue. If you would like to be featured or know someone who would, please email ACDIS Member Services Specialist Penny Richards at [email protected].
Katy Good, of Arizona, with her family, son Griffin, husband David, and
daughter Rozlyn on a winter outing.
Concurrent coding. It’s a process whereby coders assign ICD-9-CM codes throughout the patient’s stay, rather than after discharge. But the practice isn’t a common one. According to a recent CDI poll on the ACDIS website, only 13% of nearly 170 respondents perform concurrent coding at their facility. The bulk of respondents (50%) indicated they do some concurrent coding primarily in order to assign a working MS-DRG, but coders perform coding retrospec-tively (See Figure 1.)
Effective concurrent coding efforts require additional staff, place additional expectations on coders, and require
policy and procedure revisions, says Paul Evans, RHIA, CCS, CCS-P, supervisor of clinical documentation integ-rity in the quality department at California Pacific Medical Center in San Francisco.
“It can be a good idea, but only if you have the technology and skilled manpower to do it right,” he says.
That means: » Working efficiently (preferably electronically) so that CDI staff members receive their census on a daily basis for assigned patients. » Examining the charts and coding concurrently based on

© 2013 HCPro, Inc. January 2013 17
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
all documentation, in a thorough manner. This takes addi-tional time and may require additional staff, or staff may need to limit the type of charts they review. Staff will need to perform an initial review on day one of admission and continue to add codes daily, as warranted by subsequent documentation. » Querying the physician when and if significant conditions need to be clarified and/or the documentation for such con-ditions do not support coding guidelines/requirements. » Sending the CDI specialist’s proposed codes electronically at discharge to an HIM professional/coder for final review, coding, and bill drop. This person should have the final say on code assignment and should be responsible for incorpo-rating any last-minute changes to the discharge summary or late dictations or amendments if needed, Evans says.
“The obvious advantage [of the concurrent coding model] for us was the enhanced opportunity to perform concurrent queries,” says Evans.
A similar process takes place at a 60-bed facility in Iowa, says Rachel April, a pseudonym. She prefers to remain anonymous since, she confides, this method has not worked very well in her facility.
In April’s facility the CDI team includes a combination of coding and nursing staff— two RNs who work three eight-hour days, one coder who works four six-hour days, and one coder who works two eight-hour days—who per-form rotating duties of concurrent coding.
The team reviews all patients on every floor. Each staff member is assigned a floor to review every day, and the next day the assignment rotates. A tracking sheet on each unit documents which CDI specialist reviewed the record last and whether the diagnosis changed.
Each staff member reviews roughly 10 new patients and conducts about 11 re-reviews of the charts, essentially follow-ing up on a patient’s record every three days. They track the initial, working, and final DRG.
The idea of rotating the responsibility for the record review over the course of the patient stay may have been intended to ensure both clinical and coder expertise were accounted for; however, without assigned accountability, individuals frequently left tricky questions for the next reviewer to resolve, April says.
Janet Gentle, RN, BSN, MSN, CCDS, says the concur-
1%
Figure 1: Does your CDI/HIM program perform concurrent coding along with concurrent record reviews?
50%
Yes, but we only assign codes associated with working DRGs; coders assign final codes retrospectively
Don’t know
Source: ACDIS CDI poll, December 10, 2012.
36% No
Yes13%
1%
rent review and coding process at her previous facility (a program similar in structure to that which Evans describes) worked very well.
“The relationship between the CDI nurses and the cod-ers became very collaborative over time,” Gentle says.
HIM and CDI staff sat in close proximity. Coders made the final coding determination the day after discharge and the same day, CDI staff reviewed the chart to ensure every-one agreed on the final DRG assignment.
“This prevented delays in dropping the bill and reduced days in accounts receivable. I know this type of CDI pro-gram is in the minority but it worked well in this situation,” Gentle says.
Now CDI coordinator for Munson Medical Center in Traverse City, Mich., Gentle’s current CDI program uses employs CDI nurses to perform concurrent reviews/working DRG assignment and retrospective coding is completed post discharge by inpatient coders.
“The change in program methodology has been a big learning curve for me,” says Gentle.
“I now can appreciate that there is a lot to be said for both styles of CDI programs. Each has advantages and dis-advantages, but the decision to use either depends on the needs of the facility, the focus of the CDI program, and the talents and backgrounds of the staff.”
18 January 2013 © 2013 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
When you think of a travel nurse, perhaps you picture a fresh-faced RN graduating from college and setting off to see the country. Maybe you think seeing different cities would be great but feel like it has been too many years since your feet fit into those traveling boots. And being an interim staff member means job insecurity, long hours, and head-aches, right? Perhaps you think such a position is probably a better fit for those just leaving college than someone with your expertise. Not so, says George Klimis, vice president at MedPartners CDI based in Tampa, Fla.
“Those who chose a career as a travel/interim CDI specialist are actually at the height of their careers. They have worked in the field, worked their way up the career ladder in their facility. They want to take the next step, to be challenged in a way they simply may not have been challenged before,” Klimis says.
That’s what prompted Sheri Blanchard, RN, CCDS, cur-rently a CDI specialist at Wexner Medical Center at The Ohio State University in Columbus, to join Alpharetta, Ga.–based MedAssets. The large consulting firm provides a number of healthcare services but was just branching out into the CDI realm, says Blanchard. Her primary duties included helping facilities implement CDI programs of their own.
“So I took a leap and loved it. I’ve always loved the CDI role and I have a passion for teaching and working with
See the world: Become a travel CDI specialist others, so this was a perfect fit,” Blanchard says.
Wendy Frushon Tsaninos, ASN, BA, CMSRN, CCDS, an employee with Maxim Health Information Services (MHIS) based in Columbia, Md., was “over the moon excit-ed” about the opportunity to travel for work.
After working as a nurse, Tsaninos moved into a CDI role in Chicago, and then changed careers to teach nursing before coming back to CDI in a position in Scottsdale, Ariz. There she assisted hospitalists with documentation, and performed physician education and training. When she was ready to make another professional transition she opted to give travel CDI a try.
“There is so much to learn and so much opportunity to teach others as well,” Tsaninos says. “With my background and interests, travel CDI was just the perfect fit.”
Staffing expectationsTo be accepted into the travel/interim role, CDI
specialists must have multiple years’ worth of experience and demonstrated leadership in the field, says Steven Robinson, MS, PA, RN, CDIP, CPUR, CDI senior director for MHIS.
The reason for such expectations stems from one of the most frequent requests for hiring interim staff—programs need someone to fill in for existing staff members due to extended illness, leave of absence, or staffing shortfalls.
“Facilities want staff able to hit the ground running” in such situations, Robinson says. “They don’t want any lag time in getting a CDI specialist up to speed.”
In a vacancy situation, the host facility has a solid CDI program in place and knows what’s lost when a staff member is absent, says Klimis. “To them, the cost of an interim CDI specialist is minute compared to potential loss in producti-vity,” he says.
Hospitals may choose to hire travel/interim CDI special-ists for any number of other reasons. For example, MHIS contracts with several facilities to essentially operate the entire CDI program. CDI specialists then are considered MHIS employees who work at a given facility. MHIS tracks their successes and shares outcomes with the host hospital and staff.
“It can be a convenience for the facility,” says Robinson.
Wendy Frushon Tsaninos, a travel CDI specialist with Maxim Health
Information Services (MHIS) based in Columbia, Md., enroute to her
assignment in Boston.

© 2013 HCPro, Inc. January 2013 19
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
“Administrators understand the importance of CDI but don’t want to expend the effort internally to run the program.”
MHIS’s travel/interim CDI staff members also get hired to perform concurrent record review and act as tutors or mentors for new hires while new programs are established.
“Onboarding” CDI programs represents an important opportunity for interim/travel CDI specialists, Klimis says. “Finding qualified CDI specialists is difficult. It is a growing profession, but [experienced professionals] don’t grow on trees. You cannot just tap someone on the shoulder and ask them to come to your facility.”
So, as a new program trains its physicians and hires and educates new CDI staff, interim/travel employees ensure that CDI efforts continue effectively until newer staff members are able to take over.
Having that expertise makes travel/interim CDI specialists flexible, adept at problem solving, Klimis says.
“These individuals are well versed in CDI,” he says. “They know what to do and have seen enough different types of programs to be able to adapt best practices to the current needs of a given facility. They also look forward to that challenge. They want to be exposed to different compo-nents and learn new things. They want to get into the muck and solve problems.”
That level of awareness also makes them uniquely capable of completing special projects. For example, several interim CDI staff members from MedPartners CDI are helping with a documentation-related record audit at one facility.
Other programs may hire interim CDI specialists to test results on program expansion, Klimis says. So, a program looking to expand into outpatient or emergency department record reviews could employ interim specialists to perform those tasks. After a few months, the facility can review the results and determine whether the expansion makes sense before hiring additional full-time permanent staff of its own.
“The CDI specialists I have been privileged to work with really like to see how different sites work in different ways,” says Robinson. “It takes a certain amount of awareness and flexibility to be able to drop into a facility and adapt to their processes while still bringing the best of your awareness and background to a job.”
Such high-level expectations come with some high-level salaries in addition to other benefits, Klimis says. “Let’s face it, other than a few locations, travel/interim work can nearly
double an average CDI specialist’s annual salary.”
Travel perksThe primary benefit to taking a travel/interim CDI
position may be the most obvious one: traveling. As Blanchard and Tsaninos suggest, most travel employees fly to their assign-ment on Sunday night or Monday morning and fly home again on the weekends.
Every Sunday, for example, Blanchard boarded a plane sometimes to Arizona, sometimes to New York. Ideal weeks, she worked at a given facility Monday through Thursday and spent the weekend back at home in Ohio. Most assignments lasted roughly six to eight weeks.
Tsaninos’s first assignment was at Alexian Brothers Health System in Illinois, which happened to be the facility where she started her nursing career.
“They all remembered me and it was really a terrific first experience in my new role,” says Tsaninos. After that she headed to Cambridge (Mass.) Health Alliance, a position that at first intimidated her. Rumor was all the Harvard medical students interned there, and she worried her credentials might not warrant their respect. She quickly learned otherwise.
“The attendings, residents, and nurses all call each other by their first names. In that simple fact alone, I came to real-ize that it must be a caring group,” she says.
Now the Cambridge Health Alliance CDI program is primarily a remote one and Tsaninos spends most of her working time at home in Arizona, traveling to Massachusetts on a quarterly basis.
The opportunity to tour a host town, stay the weekend, and take in the sights adds entertaining experiences to travel/interim staff members’ lives. Knowing your own habits can help in that regard, Tsaninos suggests.
For her part, she enjoys getting out, trying new restau-
“FindingqualifiedCDIspecialistsisdifficult.Youcannotjusttapsomeoneontheshoulderandaskthemtocometoyourfacility.”
—George Klimis
20 January 2013 © 2013 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
rants, and even taking in an occasional Celtics game in her host hometown. Those whose habits tend toward the con-servative side might want to work in a more rural location, Tsaninos suggests.
Finding the right fit between host facilities and CDI specialists’ preferences is part of the role of the staffing firm negotiating with the hospital.
“Not every individual can work with every facility,” says Klimis. “There has to be the right fit, the right match of staffing for the facility. Fit really matters in these situations.”
Flying lessonsTsaninos points to a number of travel lessons she
learned during her experiences. One tip: Know which hotels provide frequent flier miles and make sure to get credit for them. Another tip: If you are staying in the same hotel over multiple weeks, have the hotel keep your luggage and travel back and forth with just the essentials.
“A certain amount of life skills can be gained as an individual becomes adept at traveling also,” says Robinson. “Personally, I’ve learned to be a bit more relaxed about it,” he jokes. “I’ve learned there is always another plane.”
The parent company/host facility cover costs for almost all travel expenses, says Klimis, and they typically make travel arrangements taking staff preferences into consideration.
Nevertheless, the staff member often gets to keep his or her travel perks such as frequent flier miles and credit card bonus points, which can add up to significant additional compensa-tion, Klimis says.
“We’ve had quite a few people heading off to vacation in Hawaii, let’s just put it that way,” he says.
The return homeAlthough Blanchard ultimately returned to a typical
CDI position close to home, the education her experi-ence afforded her will no doubt continue to influence her professional life.
“I really feel I blossomed in the role,” she says. “People don’t get a chance to see the global picture, to see the impact they have. As I met different people I was able to find comfort in the fact that although we all came from different backgrounds, we all experience the same difficulties and joys about the job.”
Such life experiences do have the potential to enhance professional development, Robinson agrees.
“I particularly enjoy seeing individuals mature in their roles,” he says. “I love seeing how they grow professionally due to the rigors of this aspect of the work. They took this job to learn and to explore. Once they become acclimated they really begin to shine.”
Who doesn’t love all those crafty ideas on Pinterest or home improvement projects on HGTV? For those CDI professionals working alone in small facilities, or just getting a program off the ground, creating your own physician edu-cation program can seem daunting. But crafting newsletters, tip sheets, or educational posters for your physicians can yield positive results.
Success simply depends on starting small, focusing in on important documentation concerns, and using available models shared by peers. Learning from others’ experiences, such as those that follow, doesn’t hurt either.
Poster, plus 15 minutesAlthough she has three years’ worth of experience, Karen
Macey, RN, CDI specialist at Champlain Valley Physicians Hospital (CVPH) in Plattsburgh, N.Y., still considers herself a newbie. Her self-assessment is due primarily to her limited formal CDI training. Like many new CDI specialists, Macey received a case log and spreadsheet when she started, and little else. “It was ‘Here is your log and here is your doc-umentation, go to it,’ ” she laughs. “And there I was trying to figure out what CDI was all about.”
Macey joined ACDIS, researched articles, reviewed the Forms & Tools Library, and began developing physician education materials. As she puts it, “I like to muck around with things until I become comfortable with them.”
To start, she recognized that her facility needed orienta-tion programs not only for future CDI staff, but also for the physicians.
DIY: Make your own CDI newsletters

© 2013 HCPro, Inc. January 2013 21
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
“The physicians needed to know what my little papers [queries] were all about, what I was all about, how the CDI program works, and why it is so important,” says Macey.
So she started asking questions about the CVPH phy-sician orientation program and earned her proverbial 15 minutes of fame by gaining that segment of time as a one-on-one introduction to the program during the physician orientation process.
Macey next developed a CDI brochure, essentially a doc-umentation tip sheet, to pass out to physicians as reminders of appropriate documentation and crafted posters to hang in the physician lounge. (Download her sample brochure sample chest pain poster from the Form & Tools Library www.acdis.org.)
Ideally, she’d love to have more than 15 minutes with the physicians. But for now, she’s definitely making headway, she says.
Information and laughterAlthough the CDI program at Park Nicollet Health
Services in Minneapolis, is nearly 10 years old, providing physician documentation improvement tips via newsletter was a new idea for the crew.
The facility recently implemented Epic as its electronic health record and 3M software to capture SOI and ROM measures. The shift to electronic systems meant some added conveniences for the seven-person team—some of whom may now work remotely—but it also meant fewer face-to-face interactions and more electronic prompts to the physician, says Kim MaGee, RN, the CDI program’s team leader.
“We really believe that our constant and consistent educational efforts are part of the reason our CDI program has been so successful,” MaGee says. “When we went elec-tronic we were looking for ways to update those efforts, to do something that would catch our physicians’ attention, and to keep our CDI efforts visible.”
Through networking, the CDI team hit upon the idea of a monthly newsletter and worked with its physi-cian advisor to bring it to fruition. One of the first top-ics covered in the newsletter was congestive heart failure, “which continues to be one of our top queries,” says MaGee. They’ve since covered documentation concerns regarding sepsis, chest pain, renal failure, and other com-mon documentation concerns.
In addition to the month’s main focus, the newsletter includes some tips and reminders, a joke of the month, and a featured physician “star.”
“We choose a physician that is dedicated to CDI efforts and highlight them,” MaGee says. The feature includes a photo of the physician, which the team sometimes takes from the facility archives. “Sometimes the photos are out of date and that generates some conversation and laughter,” she says. “We want them to be talking about the newsletter because if they pick it up for one reason, they’ll continue to read it and maybe get a tip or two as well.”
And of course, the newsletter includes the CDI team members’ names and contact information.
Each CDI team member shares the duties associated with the monthly newsletter’s creation. The individual assigned to that month’s issue works with the team’s physician advi-sor to determine the topic and scope. When a draft is done, it is brought back to the team for edits and suggestions. Although work on the newsletter begins 30 days prior to publication, MaGee estimates the whole process only takes about three to four hours total.
When complete, the physician advisor emails the facility’s physicians the final draft and the hospital prints several dozen copies for CDI team members to distribute. At the physicians’ request, MaGee even collects the newsletter in a binder that she leaves in the physician lounge.
“This has been really successful for us. It’s been a really interactive opportunity for us to keep communication open for the whole team,” says MaGee.
The Champlain Valley Physicians Hospital CDI team in Plattsburgh, N.Y.,
includes Mark Dixon, Doreen Curtin, Patricia Alrimawi, Karen Macey,
Janelle Pachter and seated Mafe Upton and Cheryl Mesick.

22 January 2013 © 2013 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
It took more than 100 hours and four-plus months to create the 60-plus page UNC Healthcare Clinical Documentation: Handbook for Physicians and other Licensed Healthcare Providers, recently donated to the ACDIS Forms & Tools Library (www.acdis.org).
In it, the Chapel Hill, N.C.–based CDI team explores the importance of CDI programs, outlines physician query basics and general documentation guidelines, and discusses top documentation concerns by diagnosis, including enceph-alopathy, pneumonia, sepsis, anemia, and dementia, among others. It includes information about ICD-10 implementa-tion, explains CC/MCC concepts, and offers examples of good documentation habits.
How does a five-person team develop such a compre-hensive product? Teamwork and dedication, says Tiffany H. Estes, RHIA, CCDS, UNC’s CDI supervisor.
Evolution of an ideaEstes has been with UNC since the inception of its
CDI program in 2005. Today, the CDI team is a mix of nurses, RHIT, RHIA, and CPC certified professionals who support the 850-bed teaching facility.
In 2009, Estes came up with the idea of creating tip cards for each service line. Along the way, a ring clip was added and the “cards” were laminated. The idea morphed again when the cards became too bulky. Estes downsized them and created a booklet with a spiral binding. Then, in January 2012, the facility made the decision to update the handbook annually.
“We’ve been blessed to have good support from the chief executive officer and chief financial officer for our CDI program,” Estes says. Such support affords the UNC CDI team with consistent staffing levels, CDI education materi-als, and a budget for physician education which pays for the handbook publication. Because UNC is a teaching facility, administration pushed to have the handbook ready for the season’s influx of residents last June.
The new handbook serves as a unified (and unifying) source of documentation improvement information. It can be used by coders attempting to understand clinical indicators for given diseases, by physicians trying to determine documenta-
tion requirements, and even by the CDI specialists themselves.“I’ve been using it a lot,” says Kathy Kinser, RHIT, CCS,
CDI specialist at UNC. “We wanted this to be a book that we [as CDI specialists] could have in our hands. That way, when the physicians ask us why we are querying, when they ask us to show them where the definitions are, we have the material with us and we can look it up and respond to them immediately.”
Devil in the detailsEstes decided to “share the love” and involve her CDI
team in the 2012 revision/creation process.“Working on this book with this group was tremendous,”
Estes says. “They showed a passion for making it the best it could be, took the challenge, and did a wonderful job.”
They met every other week and divided the work up equally among themselves. The team looked at the existing structure and decided to make it a 5-by-7-inch spiral-bound book with colored tabs to make it easy to find information. UNC Healthcare has a print shop on campus that worked with the team on the finished project.
The CDI staff reviewed the previously existing content against current documentation trends and trouble spots. They worked with physician advisors on clinical indicators, and with the medical staff on the floor by specialty to build consensus and support for the handbook, Estes says.
“It was a fun group project,” says Kinser. “We had an open discussion about what to include, and we each took portions of that discussion out onto the floors.”
Such involvement was essential, says Carolyn Smith, RN, MSN, also a CDI specialist and member of the team. “With the physician advisor input, it helped us all have a set of uniform information that we can use to approach the physicians.”
For her part, Kinser points to the joint learning process that took place due to the inclusivity of the project.
“There is an open learning environment here that enabled everyone to learn something, to take something away,” she says. “In our program we really are supported and told what is needed to be successful; I think this project is just one aspect of that. I am really proud of it.”
Handbook offers education and clinical support for staff

© 2013 HCPro, Inc. January 2013 23
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Each year, four new Advisory Board members step forward to lend leadership to the ACDIS membership, and four trusted members take a step back from their roles. These board members shared their thoughts on the growth of ACDIS and the CDI profession as a whole during their three-year tenure on the board. This January, outgoing board members include:
» James S. Kennedy, MD, CCS, managing director at FTI Healthcare in Brentwood, Tenn. Contact him at james. [email protected].
» Glenn Krauss, RHIA, CCS, CCS-P, CPUR, FCS, PCS, CCDS, C-CDI, independent revenue cycle consultant based in Madison, Wis. Contact him at [email protected].
» Gail B. Marini, RN, MM, CCS, LNC, manager of clinical documentation at South Shore Hospital in Weymouth, Mass. Contact her at [email protected].
» Lena N. Wilson, MHI, RHIA, CCS, CCDS, HIM operations manager at Clarian Health in Indianapolis. Contact her at [email protected]. (Note: Wilson was unable to provide comments for this publication.)
CDIJ: What prompted you to volunteer for the ACDIS Advisory Board?
JK: At the time I joined, I found ACDIS to be the only organization that holistically promoted clinical documenta-tion improvement among all professional groups. Given that I enjoy public service—I was the volunteer chairman of my county’s 911 system and served as my county’s medical examiner when I was in practice—serving on the ACDIS Advisory Board coincided with my natural desire to see CDI grow as a profession.
GK: I volunteered to serve on the ACDIS Advisory Board because I have a real passion for this profession. I believe in the efforts of CDI professionals and their poten-tial to help improve the quality of the healthcare record. As an advisory board member, you really have an opportunity to shape the direction of the profession and the association.
GM: I enjoyed my time helping get the New England ACDIS Chapter going and I wanted to play a larger role in the profession and the association. I wanted to be more than just a member who benefits from all the great material and knowledge available through ACDIS, I wanted to be a par-ticipant, a driver of growth for the profession.
CDIJ: What surprised you most about being an advisory board member?JK: Every individual involved with ACDIS is passionate
about their professional practice and the integrity to which they execute it. It was like being with family.
GK: I guess I was surprised by the number of opportuni-ties there are to become more involved in the development of the association and to the professional development of the ACDIS membership.
For example, during my service on the advisory board I was able to participate on the quarterly conference calls, to offer insight in presentation on outpatient CDI efforts dur-ing one of the calls, and to help the board develop policies around electing new board members to promote transpar-ency.
GM: The amount of an impact you can have on individual lives by being a member of the advisory board surprised me most, I think. When I spoke during a quar-terly conference call, or when my name appeared in a CDI Journal article or on the “CDI Talk” message board, people
Fondfarewell
Advisory Board members share memories of service

24 January 2013 © 2013 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
would often respond directly to me and either ask me to fol-low up questions or just thank me for my input.
I feel like I am a “grassroots” sort of girl, and that kind of impact and feedback loop really made me feel like I was making a difference to people.
CDIJ: What do you feel the greatest benefit of being affiliated with ACDIS has been for you, personally?
JK: Personally, it’s been having the opportunity to work with ACDIS Director Brian Murphy and everyone on the ACDIS administrative team, to have a channel by which HIM professionals and physicians can be more fully engaged in the CDI practice, and to make great friends.
GK: The networking and educational opportunities afforded to me via volunteering have been tremendous.
It takes a special person to be on the ACDIS Advisory Board. You need to be dedicated to the role of CDI special-ists and energized, passionate about that effort. You need to be willing to share your experience and willing to continue to learn new information. When you serve on a committee of that caliber, you cannot help but learn and grow from and with them. Being an advisory board member is a wonderful opportunity if you just take advantage of it.
GM: I have made some lasting and significant relation-ships through my involvement with ACDIS and I was able to work on some tremendous projects. Because of my involve-ment with ACDIS, I was picked to work on the AHIMA Clinical Documentation Improvement Toolkit with a number of other highly involved individuals. Because of my involvement with ACDIS, I was able to meet on a regular basis with some of the clinical experts in this field. I am very grateful for each of those experiences and what they have afforded me both personally and professionally.
CDIJ: What do you feel the greatest benefit of being an ACDIS mem-ber is, generally?
JK: Networking and professional growth. We all learn from each other.
GK: As I mentioned before, education and network-ing definitely are two of the greatest benefits of being an ACDIS member. I’ve been privileged to also work on the CDI Roadmap Committee, which developed roles and responsibilities for rolling out a CDI program, and honored to serve on the CDI Week Planning Committee
twice. These tools that are now available to all the ACDIS members will help provide a cohesive set of tools and serve to energize CDI specialists about their roles. At least, that’s what it does for me.
GM: I cannot begin to list out all the benefits of being an ACDIS member or what it has meant to me as I have grown in this profession. I’ve been doing this type of work for more than 10 years now, but the community that has developed around ACDIS to support CDI professionals is tremendous.
The resources that are available to ACDIS members regardless of your experience are also invaluable. If you are a new CDI specialist, there are tools, articles, and network-ing opportunities for you. Similarly, for those who have several years of experience, there is always some regulatory change and shift in focus that ACDIS brings forward.
CDIJ: What aspect of ACDIS’ growth are you most proud of being involved with during your tenure?
JK: I am most proud of ACDIS’ growing advocacy of the coder who, at the end of the day, affixes his or her initials to the coding report and is ultimately responsible for the codes that are submitted. I was gratified to see AHIMA and ACDIS working together to write a new CDI practice brief that will be published in 2013 to address common challenges of both the concurrent and retrospec-tive reviewer.
Even in Tennessee, our state HIM and ACDIS associa-tions cosponsored seminars promoting CDI practice, which I was proud to be part of.
Finally, I enjoy seeing new physicians join the CDI movement, demonstrated by the strong attendance at ACDIS’ physician advisor meetings and their engagement at their facilities.
GK: I’ve been proud and grateful for the opportunity to contribute to the variety of news outlets, such as the ACDIS Blog, the email newsletter CDI Strategies, the online message board system “CDI Talk,” among other ven-ues that ACDIS provides.
I am also proud of having been a member of the board during the time it created new policies around the election process. I believe that transparency and inclusiveness will benefit the overall association as it continues to grow.
GM: I am very proud of the work we did on the CDI

© 2013 HCPro, Inc. January 2013 25
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Roadmap. That was a very intensive project and I feel like it was an extremely worthwhile endeavor.
I am also very proud to have been able to help people out. For the longest time, when I first started in this role, I felt like I was alone. There are newcomers out there, pro-grams that haven’t had an opportunity to fly yet that still need to reach out to someone for a helping hand.
This association puts all of us together to help one another. It’s a good thing.
CDIJ: What challenges do you feel the association faces in 2013 and beyond?
JK: ACDIS as an organization must continue to evolve into a professional organization that strongly advocates excellence in CDI practice in concert with the Cooperating Parties for ICD-9-CM/ICD-10.
This means we must be proactive in assessing these associated transaction sets and providing feedback and advice with these empowered agencies as to what mechanics and principles best serve the medical community and the nation.
Consequently, ACDIS must introduce itself to and part-ner with the AMA and other physician groups as HIPAA transaction code sets are increasingly used to measure, moni-tor, and reward provider outcomes and efficiency as part of the Patient Protection and Affordable Care Act, all the while continuing to nurture its relationship with AHIMA and other members of the Cooperating Parties.
ACDIS must also invest in informatics, considering a partnership with Healthcare Information and Management Systems Society to better deploy CDI principles integral to the electronic health record to ease the burdens of the pro-vider, coder, and others involved in the CDI process.
I see ACDIS potentially having a lobby arm in Washington to monitor legislation and rulemaking, attend meetings affecting HIPAA transaction sets, and/or perhaps share resources with other associations attuned to these mat-ters. Doing this will require ACDIS members to conti nue to invest in the CDI practice and the provision of industry standard education and professional practice materials suit-able for reference.
Last but not least, we must never forget our primary mission, which, in my mind, is to selflessly advocate the rela-
tionship between the provider and the coder that best pro-motes the clinically congruent and compliant submission of HIPAA transaction sets in the most cost- and time-efficient manner. I believe ACDIS will do this as it continues its legacy of servant and principled leadership.
GK: I think ACDIS needs to continue to be a voice for the growth of the profession, to consistently review the mis-sion of CDI professionals to meet the challenges of a chang-ing world of healthcare business and reimbursement reforms. If we don’t challenge the traditional expectations of simply capturing CC/MCC documentation in exchange for reviews focused more on quality, severity of illness/risk of mortality, across all payers, the ethical impetus of our endeavors could be called into question.
Furthermore, I believe that expanding the CDI scope to areas of outpatient services, ED, and other clinical settings needs to be explored more fully. As we migrate into this new arena, CDI specialists will continue to grow their skill sets
and expand the quality of the documentation and care being provided.
GM: Keeping up with the changing role of CDI special-ists will undoubtedly be a challenge for the association and for CDI programs in general. The changing landscape of reimbursement measures means we have to evolve and begin to review records for quality and to include case management and utilization review in our efforts.
As we delve into electronic health records, CDI special-ists need to keep the story of the patient’s care at the fore-front so that the picture the data is meant to create doesn’t get lost.
Combining the clinical with the coding aspects of medi-cal record review allows us to capture what’s happening with that patient in the bed.
We cannot let go of that clinical aspect of care and allow it to disappear as technology changes our day-to-day functions. I worry about these challenges, but I know that ACDIS has the power to keep the CDI role relevant.
“Thechanginglandscapeofreimbursementmeasuresmeanswehavetoevolve…”
—Gail B. Marini, RN, MM, CCS, LNC

26 January 2013 © 2013 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
We asked ACDIS members to explain what it takes to be an exemplary CDI specialist, to excel at not only medi-cal record reviews, but also at incorporating the underlying purpose of CDI efforts into even seemingly mundane, everyday tasks. We heard from quite a few folks who shared some sound, sage advice. Read on and consider implement-ing some of this advice into your personal job or your larger program—and you just might find yourself becoming a “Superstar CDI” in 2013.
Focus on teamworkDon’t forget that you’re part of a team. The CDI specia-
lists, coders, providers, quality, nursing, compliance, utiliza-tion review teams all work together for the patient to make sure that the record is as complete and accurate as it can possibly be.
I believe that real success comes from keeping the lines of communication open, showing mutual respect, and main-taining your focus on what’s important: the patient.
Keep up with trends, continue to educate yourself on your job, and communicate new information to other members of the team.
And, perhaps more importantly, listen when they com-municate information to you. If you do that, show respect, listen, and remember that you’re only one cog in the wheel that moves around the patient, you’ll do great.
—Robert S. Hodges, BSN, MSN, RN, CCDS, CDI specialist at Aleda E. Lutz VAMC, Saginaw, Mich.
Expand beyond the ‘typical’When our department started, we learned how to assess
the chart for the primary diagnosis, determine sufficient doc-umentation to capture CC/MCCs. We developed queries for areas of uncertainty. We learned about CDI metrics to judge our benefit to the health system against cost of the program, such as coder-CDI specialist agreement rates, physician response rate, and our affect on MS-DRG assignments.
As we progressed into our second year we sought infor-mation from CMS, ACDIS, HealthGrades data, and other resources to learn about current RAC initiatives in our region and nationwide. We learned about the effect of government reimbursement initiatives such as value-based purchasing, bun-dling payments, and quality initiatives. This knowledge gave us further support to expand our record reviews and query efforts to look for clinical relevance, not just CC/MCC capture.
Our goal was to develop a quality medical record document that could withstand the rigors of government audits, private payer review, and sustain our request for reim-bursement. Furthermore, this helps improve our facility and physician’s HealthGrades scores and prevents revenue loss from value-based purchasing issues.
Our team is considered the hospital’s leading base of knowl-edge regarding medical necessity documentation verification and education for all services regarding prevention of denials/audits.
We have grown from beginning as “chart auditors” into a team of “quality documentation specialists” providing more than financial improvement in the case-mix index. We provide assurance of a quality medical record. The focus of our position shifted from perusing for clinically appropriate diagnosis documentation to ensuring all components of the medical record reflect the most accurate severity of illness and risk of mortality levels.
In addition, we perform a concurrent audit for core measure and patient safety indicators. We would rather have a preemptive challenge in working with clinicians on the medical record than a post-chart chase.
—Sara Baine, MSN-Ed, CCDS, quality documentation specialist at Southeast HEALTH in Cape Girardeau, Mo., and president of the
Heartland ACDIS Chapter
SuperstarCDI
Start 2013 with an eye toward excellence

© 2013 HCPro, Inc. January 2013 27
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Examine records of all patientsWith the presence of value-based purchasing and the
knowledge that “as Medicare goes, so go all other payers,” folks who isolate their CDI efforts to Medicare patients only with the goal of increasing revenues from that one payer will inevitably place their hospital and their medical staff in the unenviable perception of providing bad care to anyone else. Patients are patients, their diseases and data all count. Doctors are doctors, their patients and data all count. Review all payers, not just Medicare, and your CDI program will be more compliant and effective.
—Robert S. Gold, MD, president and CEO of DCBA, Inc., Atlanta, and founding ACDIS Advisory Board member
Take advice from othersEnjoy your CDI position. Most CDI specialists say it is
the best position they have ever had. Not only do you get to use your clinical experience as you review charts, you learn new diagnoses, procedures, terminology, medications, and more, and that keeps your medical knowledge current and your brain stimulated. Furthermore, the position allows you to use your creative flair by designing educational newsletters, tip cards, and PowerPoint® presentations to educate physi-cians, other departments, and fellow CDI staff members.
Earn your CCDS credential and learn about career ladders within the industry.
Relationship building with physicians requires some mutual understanding. Read journal articles from sources that the physicians read, such as The Wall Street Journal, Journal of the American Medical Association, and The New England Journal of Medicine. You will become aware of what physicians are thinking and can be understanding and empathize with their needs. Speak to your physicians about more than just queries. Ask them questions related to their specialty so you can learn from them and build rapport.
Don’t take it personally when physicians rant and rave or are rude to you regarding queries. Use the shoulders of fellow CDI staff to comfort you and give you the wisdom and fortitude to face the next encounter with grace.
Seek mentors. Join your state ACDIS chapter and participate in the networking opportunities afforded to you by your national ACDIS membership. For example, partici-pate in “CDI Talk.” Email someone from “CDI Talk” who has listed their contact information.
Network with coders and other CDI specialists. Attend meetings and conferences. When you do, gather business cards and give out yours.
You may be surprised at how much you know and how much of an expert you may already be on the CDI industry, trends, and new horizons. Be a mentor. Volunteer on ACDIS committees or submit an idea for a poster session at the ACDIS national convention. Offer to present an idea you’ve worked on at your facility to an upcoming local chapter meeting.
Share things you learn.Help those you see struggling.Educate everyone about the importance of CDI.Celebrate CDI Week each September.Learn what your CDI program metrics mean. Keep track
of the number of reviews, the number of queries, physician response rate, and physician agree rate. Monitor both physi-cians who answer with helpful information and those who need further education.
Participate in ACDIS surveys and read the results so you know how your program compares to others.
Remember that hospital size, nonprofit and for-profit status, teaching hospital or not, specialty programs and trauma can make your program very different from other programs.
Be proud of what you do. Know that a complete and accurate medical record helps with patient care and safety. It helps the next provider to know the patient’s medical history. It clarifies diagnoses ruled out or ruled in. It establishes present-on-admission status versus hospital-acquired conditions. It reflects the great care your physi-cians gave to the patient. It justifies the length of stay, resource utilization, and helps support the physician’s E/M billing level. It protects the physicians and the hospital from recoupment.
As a CDI specialist you are the bridge between the medical terminology and coding language for the physician. You are a partner and a resource for the patient, the physi-cian, coding, quality, case management, and many other teams within your facility.
—Charrington “Charlie” Morell, RN, CCDS, director of case management and clinical documentation integrity for HCA West
Florida Division CDI Manager at HCA West Florida Palm Harbor, and past vice president of the Florida ACDIS Chapter.

28 January 2013 © 2013 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Build relationshipsCDI success is all about the relationship you have with
your service/physician/nurse practitioner (NP). Under-standing that when you have a strong relationship with your service/physician/NP, it gives you the opportunity to edu-cate them on the “why you are asking, who you are, and the benefits of what you do.”
This is a marketing job. You should always be selling the concepts of CDI and talking the CDI lingo to anyone and everyone when the opportunity arises.
It is not a desk job. Interacting with your services, physi-cians, NP, and other providers allows you to educate, whether in a passing moment or at length in a meeting, about the various specificities we look for and why we look for them.
CDI efforts are all about ensuring a complete chart. CDI reviews should not be about the payer source or focused on a designated service line. Success, in all aspects of healthcare, means finding and taking the opportunity to showcase how sick the patient is and what care was provided to help them get well. Concise and accurate documentation supports every aspect of what we do.
CDI specialists understand what is missing in the chart from a potential diagnosis/coding standpoint and also what is missing from a case management staff/medical necessity standpoint. Together, these strengths can bridge the gaps for documentation success.
—Sheri Blanchard, RN, CCDS, CDI specialist at Wexner Medical Center at The Ohio (Columbus) State University and leader of the
Columbus (Ohio) ACDIS Chapter
Develop interdepartmental collaborationWhat a great time to be a part of the synergy necessary
to propel clinical documentation into an enhanced quality product. Collaboration, strong leadership, and top-down support are all required to ensure the healthcare provider’s documentation reflects the severity of the conditions in order for the coder to assign accurate codes. Continuous skill building will enable the entire healthcare team to deliver a quality product that insurance companies across the nation will be proud to partner with and purchase our valued quality healthcare. All of us want the very best healthcare for our patients.
Together with administrative support, great leadership, excellent software systems, and skilled staff, we will achieve
best practices in clinical documentation, which is the root of successful healthcare transition and change.
—Marie A. Thomas, RHIT, CCS, CPC-H, CCDS, AHIMA-Approved ICD-10-CM/PCS Trainer, Duke University
Health System, Durham, N.C.
Be flexible, innovateCDI specialists can’t be all things to all people. Just
because you’re “in the chart” it doesn’t mean that you should necessarily review quality measures or patient safety indicators or monitor length of stay. Eventually, however, your CDI program should become advanced enough to where you can do more than clarify principal or secondary diagnoses.
For example, you may realize that your ED documenta-tion is nonspecific, a vulnerability that results in take-backs from Recovery Auditors. Maybe your hospital doesn’t have the necessary documentation to capture drug administration charges and is missing out on billing for expensive drugs.
If so, consider expanding your duties to include the ED or other neglected departments. Propose to administration a new role for a CDI reviewer exclusive to the ED. Advocate for a CDI specialist whose job is to review outpatient claims. Present the facts in a sound business case, and you’ll get folks to listen.
In short, innovate. Help grow the profession and show your facility how valuable you are. It may just lead to increased recognition and a promotion.
CDI is a new and evolving profession and I believe its boundaries and potential are limitless.
—Brian Murphy, ACDIS director, Danvers, Mass.
Stay informedIt is so easy to get into a routine of reviewing charts,
leaving queries, finding MS-DRGs, and then going home. Instead, participate in “CDI Talk” on the ACDIS site. Attend your state chapter meetings to exchange ideas and thoughts. Participate in the ACDIS quarterly conference calls. Take time to read updated information.
When you learn something new or discover something insightful, share your information. Do not be afraid to com-municate with your peers, whether it is at your facility, over “CDI Talk,” or at a state chapter meeting. No question is ever stupid. When you ask it, someone else in the group

© 2013 HCPro, Inc. January 2013 29
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
may be thinking of the same question but be afraid to ask. If you have a particular query or suggestion that works for your facility, share it. This field is new and we are all looking for solutions.
Greet everyone you meet. I enjoy walking the hallways and saying “good morning” or “good afternoon” to everyone I see. I especially like to acknowledge the physicians. They need to realize we are people, not just the chart police.
This might encourage someone to ask you what you do each day. Not a week goes by that I don’t have a nurse or other staff member ask me what I am doing. This gives me a chance to talk about CDI.
—Lisa Romanello, RN, BSN, FNS, CCDS, CDI specialist at CJW Medical Center, Chippenham, Va.
Let your starlight shineThe definition of a “CDI Super Star” depends on
whom you ask. A corrected case mix may place you in the star category with your finance director or revenue cycle leadership. The quality department may hang a star on your door for your contribution to improved quality and core measure report cards. And what physician doesn’t consider you star material when you share your CDI wisdom in a courageous fashion? How kind are you to your other CDI professionals in the HIM department? Does your camarade-rie warrant a star status?
What about the improved outcomes for the septic patient diagnosed and treated in a timely fashion in part because of your early dialogue and diagnosis clarification with the physician? If this patient only knew, he too would rate you star quality.
Can you say that you keep your CDI practice patient-centric? Are you improving the data integrity of the medical record so essential to population health management? If you can answer yes to these questions, then you know you are a CDI super star in your own right.
—Melinda Tully, MSN, CCDS, CDIP, Nuance Communications, Healthcare Division, Atlanta
Maintain effective communication skillsTo be an effective CDI professional, you need to be a
businessperson. If you keep pace with the constant, ongoing Medicare changes and how they impact your physicians and the potential financial performance of their practices, you
can communicate those changes in a manner that earns their trust and respect.
Over time, physicians will recognize the added value CDI specialists have in promoting complete, accurate, and effective clinical documentation in support of the business of medicine instead of the traditional negative view of CDI staff attempting to get more money for the hospital.
Medicare Administrative Contractors, fiscal intermedi-aries and carriers consistently release results of widespread probe reviews, clinical documentation tips, and general reminders that impact physicians and hospitals. Recent examples include denials of physician E/M hospital services because the physician documentation did not demonstrate medical necessity (e.g., no diagnosis in the progress note or cloned progress notes).
CDI specialists must communicate these relevant, pivotal findings to physicians. Medicare contractors believe physi-cians are responsible for staying abreast of all updates to Medicare guidelines, policies, and regulations by reading and acknowledging contractor correspondence. Physicians are expected to be aware of these updates, yet they frequently do not have the time to devote to the constant barrage of emails and newsletters from Medicare.
CDI specialists can reinforce the educational benefits they provide to physicians by sharing tidbits obtained from reading these regular Medicare updates and notices. To this end, you’re not only helping their business, you’re looking out for the organization as well.
The material communicated by the Medicare contrac-tors affects the hospital as well as the physician. Presenting Medicare updates, findings from probe reviews, and tips for more effective clinical documentation in support of E/M assignment benefits both parties by reducing third-party denials. CDI specialists should incorporate this educational role into their regular duties and responsibilities.
Good communication requires open dialogue between all parties. Every member of the team should feel comfortable approaching another, whether for instruction, guidance, or further clarification. Questions are asked for good reason, and if someone is asking you for more detail, it means you didn’t provide enough in the first place.
—Glenn Krauss, BBA, RHIA, CCS, CCS-P, CPUR, FCS, PCS, C-CDI, CCDS, manager at Accretive Health, Madison, Wis.,
and leader of the Wisconsin ACDIS Chapter

30 January 2013 © 2013 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
New leaders step forward for local chaptersEditor’s Note: Local Chapter meetings and educational
efforts are a natural outgrowth of ACDIS’ mission to bring CDI specialists together to share the latest tested tips, tools, and strategies to implement successful CDI programs and achieve professional growth. Although the association fosters these efforts through regular leadership meetings, guidance, free products, and other give-a-ways, the success, and amaz-ing growth of ACDIS Local Chapters, stems from the dedi-cated efforts of dozens of volunteers.
These volunteers step forward to host and plan events, maintain membership contact information, apply for con-tinuing education credits, research speakers and assess the educational importance of potential presentations. Furthermore, they nurture and mentor their local chapter networking members offering a secure environment where professionals can comfortably ask questions about documen-tation improvement.
The following individuals recently stepped forward to lead networking groups in their region.
Children’s hospitals Valerie Bica, BSN, RN, CPN, CDI specialist at Nemours/A I duPont Hospital for Children, in Wilmington, Del., leads the Association of Pediatric Documentation Improvement Specialists (APDIS) networking group. She has 35 years of
pediatric/neonatal intensive care unit (NICU) nursing expe-rience, the last 10 years at the duPont Hospital for Children. Her previous experience includes case management, care management, managed Medicaid, acute care pediatrics, and high tech pediatric homecare. Bica helped establish the AI DuPont CDI program where she conducts concurrent clini-cal reviews of inpatients, education sessions for new attend-ing physicians, monthly education for residents, attends bedside rounds with treatment teams. Contact her at [email protected].
ArizonaGloria Richardson, RN, CDI special-ist at Scottsdale (Ariz.) Healthcare Osborn Medical Center, leads the Phoenix, Ariz., ACDIS Chapter. Born and raised in Sacramento, Calif., Richardson has been a nurse for more than 40 years, including time in sev-
eral acute care facilities. She has experience in disease management and utilization
review, claims review, and account management. A CDI specialist since 2004, she organized the first
Phoenix-area CDI networking meeting in September 2012 which gathered 22 CDI-related professionals. Contact her at [email protected].
ColoradoEric Ryland, MS, RHIA, CCDS, CHDA, CCS, CPC, manager of cod-ing at Denver Health Medical Center, serves as co-leader for the Colorado ACDIS Chapter. He has more than 20 years experience in coding and compliance related activities. A pre-
senter at the 2012 ACDIS Conference in San Diego, he is involved in his state with the Colorado Hospital Association and with the ICD-10 Task Force in Colorado. Contact him at [email protected].
Jane Hoyt, BA, BSN, RN, CCDS, manager of the CDI program at Denver Health Medical Center serves as co-leader of the Colorado ACDIS Chapter. A nurse for nearly 20 years, Hoyt joined the CDI team at the program’s incep-tion in 2008. She enjoys the challenge
of CDI and is committed to the integrity and mission of the CDI Profession. Contact her at [email protected].

© 2013 HCPro, Inc. January 2013 31
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
ConnecticutMaryAnn Shanley, RN, CCDS, CDI specialist at Saint Francis Hospital and Medical Center, in Hartford, leads the Connecticut ACDIS Chapter. A native of New Jersey, she has experience in various nursing and related management roles. Contact her at [email protected].
IdahoRobin Hetzler, RN, CDI specialist at Kootenai Health in Coeur d’Alene, leads the newly created Idaho ACDIS Chapter. A nurse for 20 years, Hetzler came to the CDI profession in June 2012. Contact her at [email protected].
IndianaTeresa Leap, RN, BSN, MBA, CDI specialist at Wishard Hospital in Indianapolis, recently became president of the Central Indiana ACDIS Chapter. Previously vice presi-dent of care management consulting for The Schumacher Group and national director for health advisory services for PricewaterhouseCoopers, Leap hopes to help local CDI programs advance their documentation improvement efforts. Contact her at [email protected].
Lisa A. Farhar, RN, MSN, CCDS, CDI liaison for Indiana University Health was recently named vice-pres-ident of the Central Indiana ACDIS Chapter. A nurse since 1995, her background includes cardiac, medical, and progressive care work. She joined
the CDI team at IU Health when it started and in 2000, and earned her CCDS credential in 2009. Contact her at [email protected].
Angie Green, ASN, BA, CDI special-ist at Community Hospital North in Indianapolis was recently named sec-retary of the Central Indiana ACDIS Chapter. Green’s experience includes time spent as director of nursing for
long term care, orthopedics and neurology, case management director, and quality/process improvement roles. Contact her at [email protected].
MassachusettsSarah T. Eby, RN, BSN, MHA-Inf, CDI specialist at Tobey Hospital, Southcoast Hospitals Group in Wareham, heads the newly re-launched Massachusetts ACDIS Chapter. A nurse for more than 15 years, Eby has experience in management for both
acute- and long-term care. Contact her at [email protected].
MichiganPatti Nemeth, BSN, RN, CCDS, CDI supervisor at Henry Ford Hospital in Detroit, co-leads the Michigan Chapter of ACDIS (MACDIS). She has more than 20 years experience in nursing, taking on a CDI role five years ago. Contact her
MissouriSara K. Baine, MSN-Ed, CCDS, CDI specialist at SoutheastHEALTH in Cape Girardeau, is president of the Heartland ACDIS Chapter which gathers CDI profession-als from a number of states at the joining of Kentucky, Tennessee, Illinois, Missouri, and Arkansas. A nurse since 1990, Baine joined the CDI profession in 2010 and eared her CCDS credential in 2012. Her background includes experience in cardiothoracic intensive care, surgical progres-sive care, as well as administrative roles as a nursing supervi-sor and manager of inpatient cardiac rehabilitation for the Department of Veterans Affairs Medical Center. Contact her at [email protected].
Christina Dunning, RN, BSN, CDI specialist at St. Francis Medical Center in Cape Girardeau, serves as the vice presi-dent of the Heartland ACDIS Chapter. A nurse since 2004, Dunning’s experience includes time as critical care nurse for cardiac, trauma, and dialysis. Contact her at [email protected].

32 January 2013 © 2013 HCPro, Inc.
For permission to reproduce part or all of this newsletter for external distribution or use in educational packets, please contact the Copyright Clearance Center at www.copyright.com or 978/750-8400.
Dawn Witty, RN, BSN, CDI specialist at SoutheastHEALTH, serves as secretary of the Heartland ACDIS Chapter. With 13 years experience in nursing includ-ing time in both inpatient and outpatient endoscopy, Witty came to CDI in 2010. Contact her at [email protected]. Vivian Bollinger, RN, BSN, CDI specialist at SoutheastHEALTH, serves as the treasurer of the Heartland ACDIS Chapter. Her 30-year nursing career includes experi-ence in medical-surgical, orthopedic-neurology, home health, among other specialties. She joined the CDI profession in 2010. Contact her at [email protected].
NebraskaCory Price, RN, BSN, case manager/CDI specialist at Nebraska Spine Hospital in Omaha, leads the Nebraska ACDIS networking group. She has more than 17 years of nursing experience, and nearly five years’ experience in CDI efforts. Contact her at [email protected].
OregonEileen Pracz, RN, CCDS, CDI specialist at Oregon Health & Science University serves as president of the chapter. With 17 years of nursing experience, Pracz moved to Portland to become a CDI specialist in 2004, earned her CCDS certification in 2010, and helped start the Oregon ACDIS Chapter serving as its first president. Contact her at [email protected].
Janet Barber, RN, BSN, MBA, CDI specialist at Providence Portland (Ore.) Medical Center serves as secretary for the nearly 4-year-old networking group. Barber, a past presi-dent of the group, has been a nurse for 35 years, working in intensive care, labor and delivers, home health, utilization management, compliance and other areas. She joined the CDI profession in 2010. Contact her at [email protected].
Virginia MaryLee Traver, RN, CDI special-ist at Henrico Doctors’ Hospital in Richmond, helps lead the Virginia ACDIS Chapter. A nurse since 1975, her experience includes time as medi-cal/surgical staff nurse, nurse man-ager, director of home health, and
director of oncology inpatient services among other roles. She has worked as a CDI specialist since 2010. Contact her at [email protected].
TexasBarbara Anne Presley, RN, CCDS, CDI Specialist at University Medical Center Brackenridge leads the Austin/San Antonia ACDIS Chapter. A nurse for more than 20 years, primarily in cardiology, she joined the CDI profes-sion in 2006. For information, con-
tact her at [email protected].