better data for better outcomes: the importance of process
TRANSCRIPT
DEBATE Open Access
Better data for better outcomes: theimportance of process mapping andmanagement in CRVS systemsDaniel Cobos Muñoz1,2*, Don de Savigny1,2, Renee Sorchik3, Khin Sandar Bo4, John Hart3, Viola Kwa5,Xavier Ngomituje6, Nicola Richards3 and Alan D. Lopez3
Abstract
Background: Despite attempts to apply standard methods proven to work in high-income nations, nearly all civilregistration and vital statistics (CRVS) systems in low- and middle-income countries are failing to achieve adequatelevels of registration completeness or produce the high-quality vital statistics needed to support better healthoutcomes and monitor progress towards the 2030 Sustainable Development Goals. This suggests that, rather thansimple technical issues, these countries are facing additional or different systemic challenges, including duplicationof roles and responsibilities, inefficient methods of data collection, and a reluctance to change.
Applying process management: Process management is a valuable tool that strengthens the production of vitalstatistics by providing a visualisation of data flow from start to finish. It helps identify gaps and bottlenecks in theprocess, allowing stakeholders to work collaboratively to find solutions and target interventions. As part of theBloomberg Philanthropies Data for Health Initiative at the University of Melbourne, 16 countries were supported inmapping the varied processes required in registering a birth or death. Comparative analysis exposed severallimitations in the design of CRVS systems that hinder their performance — from ‘passive’ systems, to overlycomplex and fragmented system design, through to poor collaboration and duplication of efforts.
Conclusions: The experiences from Myanmar, Papua New Guinea and Rwanda reported in this paper illustrate thebenefits of process management to improve CRVS. While these three countries are at different stages of systemdevelopment, each uniquely benefited. Process management is a useful tool for all CRVS systems, from the mostrudimentary to the most developed. It can strengthen CRVS systems and improve the quality and completeness ofvital statistics, resulting in more robust, reliable and timely vital statistics for health planning and better monitoringof the 2030 Sustainable Development Goal agenda.
Keywords: Cause of death, Civil registration and vital statistics, Mortality, Myanmar, Papua New Guinea, Processmanagement, Process mapping, Rwanda, Sustainable development goals
BackgroundNearly all civil registration and vital statistics (CRVS)systems in low- and middle-income countries (LMICs)are failing to achieve adequate levels of registration com-pleteness and produce high quality vital statistics despiteattempts to apply standard methods proven to work inhigh-income nations [1]. This greatly reduces the policy
value of this important and routine data source. Further-more, it suggests that, rather than simple technical is-sues, LMICs are facing additional or different systemicchallenges to those faced by high-income countries.CRVS systems differ from other health-related data sys-tems in that they are more complex and often comprisedof a multitude of stakeholders, including the ministriesof health, interior, planning, justice and security as wellas local government. The consequence of this is a stron-ger tendency to create and maintain separate, often par-allel, information systems to collect and store data on
© The Author(s). 2020 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
* Correspondence: [email protected] Tropical and Public Health Institute, Socinstrasse 57, Basel CH-4002,Switzerland2University of Basel, Petersplatz 1, Basel CH-4002, SwitzerlandFull list of author information is available at the end of the article
Cobos Muñoz et al. BMC Medicine (2020) 18:67 https://doi.org/10.1186/s12916-020-01522-z

vital events. However, stakeholders must work harmoni-ously in order to register all vital events and produce us-able, robust vital statistics that can inform health policy.Thus, a systems-level approach is needed to achieve last-ing improvements and meet the increased demand forvital statistics, particularly with respect to the 2030 Sus-tainable Development Goal (SDG) agenda.
The importance of process management in CRVSsystemsEnterprise architecture is an established methodologywithin the business sector that provides a frameworkand approach to describe the fundamental concepts orproperties of a system, thus bridging the vision and ob-jectives of a system with its actual operating model [1].Process management, one of the tools used in enterprisearchitecture(EA) to describe and analyse the architectureof a system, is critical in helping to understand CRVSsystems at a systems level by capturing the complexity ofthe multiple interactions among different stakeholders.The first step in process management is the develop-ment of process maps — graphical representations ofend-to-end processes outlining the stakeholders and ac-tivities needed to complete a process (Table 1). Processmapping engages the various, and often siloed, stake-holders and brings them together to collaboratively de-velop and agree upon a common understanding of theprocesses of the current CRVS system. It also helps toidentify areas where there is no shared understandingand why different stakeholders may not agree upon theprocesses at any given step. As such, a critical pre-condition to the successful creation of process maps isthe identification of all relevant stakeholders; while thisgenerally includes ministries of health, civil registrationand justice departments, and national statistical offices,sectors as varied as immigration departments, funeralhomes and community-based organisations may also beinvolved, depending on country context.Process mapping strengthens the production of vital sta-
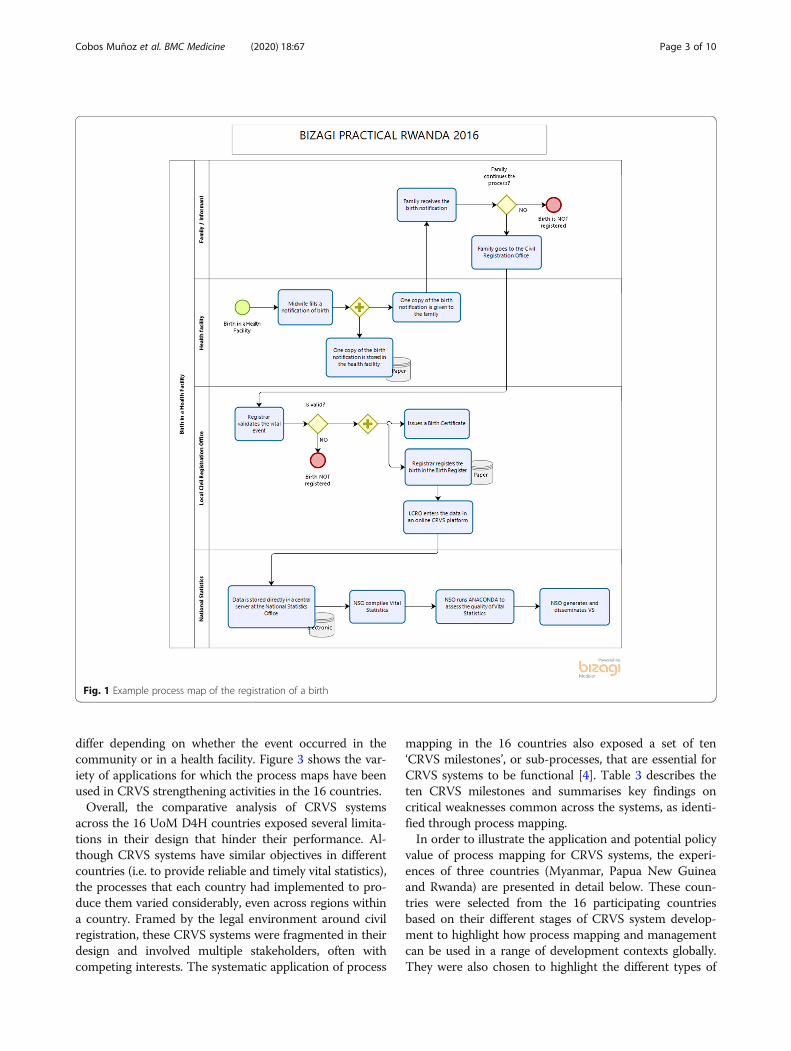
tistics by providing a visualisation of the flow of data fromstart (occurrence of a vital event) to finish (publication of
vital statistics) whilst identifying process gaps and bottle-necks (Figs. 1 and 2), allowing stakeholders to work col-laboratively to find solutions and target interventions —the next step in effective process management. Stake-holders can start by developing ‘as-is’ process maps, show-ing current operations in the system [2], followed by ‘as-desired’ maps in order to achieve a shared vision and goalfor improvement. As process maps show how data flowsfrom start to finish, they can pinpoint sub-processeswhere data is lost or not being shared with the appropriatestakeholders (Table 2), ultimately benefiting the produc-tion of vital statistics.Process management is a critical first step in strength-
ening CRVS systems to monitor and achieve several ofthe indicators and targets of the SDGs. Indeed, strongCRVS systems capable of registering practically everybirth and death are specifically defined as SDG targetsand indicators (SDG Target 16.9 and Indicator 17.19.2).Furthermore, 7 of the 17 SDGs, and 17 of their corre-sponding indicators, will require cause-specific mortalitydata from CRVS systems [3]. Achieving the targets re-lated to 102 of the indicators greatly depends on peoplehaving access to birth, death and marriage certificates —a critical service that only CRVS systems can provide[3]. Additionally, mapping out processes for deaths thatrequire further investigation, such as those due to trafficaccidents or suicide and homicide, will support a morecomprehensive and reliable picture of mortality, andallow for stronger and more timely reporting on SDG in-dicators requiring cause-specific mortality. Process man-agement allows individual actors to gain an appreciationof the importance of the information for other stake-holders, supporting collaborative solutions to improvedata sharing and data quality, both of which are criticalin generating reliable vital statistics.
Strengthening the efficiency and quality of CRVSsystems through process management — countryexperiencesProcess management is important in strengthening effi-cient and sustainable CRVS systems as well as to produceaccurate and timely data for policy. As part of the Bloom-berg Philanthropies Data for Health (D4H) Initiative atthe University of Melbourne (UoM), between March 2015and March 2019, 16 countries1 were supported in map-ping four CRVS processes (birth in a health facility, birthin the community, death in a health facility and death inthe community). These four types of vital events were se-lected since the processes for notifying and registeringbirths and deaths differ; furthermore, the processes also
Table 1 Key terms [1]
Business process: the set of activities and tasks that logically grouptogether to accomplish a goal or produce something of value for thebenefit of the organisation, stakeholder or customer.
Enterprise architecture: a methodology that provides a conceptualblueprint of the structure and operation of a system. The aim ofenterprise architecture is to determine how an organisation can mosteffectively achieve its current and future objectives.
Process map: a visual snapshot of an end-to-end description of the ac-tivities, stakeholders and requirements of a process.
Process management: a systematic approach to understand, analyse andoptimise processes within complex adaptive systems in order to achieveintended system goals.
1Bangladesh, Brazil, China (Shanghai), Colombia, Ecuador, Ghana,India (Mumbai), Myanmar, Papua New Guinea, Peru, Philippines,Rwanda, Solomon Islands, Sri Lanka, Tanzania and Zambia.
Cobos Muñoz et al. BMC Medicine (2020) 18:67 Page 2 of 10
differ depending on whether the event occurred in thecommunity or in a health facility. Figure 3 shows the var-iety of applications for which the process maps have beenused in CRVS strengthening activities in the 16 countries.Overall, the comparative analysis of CRVS systems
across the 16 UoM D4H countries exposed several limita-tions in their design that hinder their performance. Al-though CRVS systems have similar objectives in differentcountries (i.e. to provide reliable and timely vital statistics),the processes that each country had implemented to pro-duce them varied considerably, even across regions withina country. Framed by the legal environment around civilregistration, these CRVS systems were fragmented in theirdesign and involved multiple stakeholders, often withcompeting interests. The systematic application of process
mapping in the 16 countries also exposed a set of ten‘CRVS milestones’, or sub-processes, that are essential forCRVS systems to be functional [4]. Table 3 describes theten CRVS milestones and summarises key findings oncritical weaknesses common across the systems, as identi-fied through process mapping.In order to illustrate the application and potential policy
value of process mapping for CRVS systems, the experi-ences of three countries (Myanmar, Papua New Guineaand Rwanda) are presented in detail below. These coun-tries were selected from the 16 participating countriesbased on their different stages of CRVS system develop-ment to highlight how process mapping and managementcan be used in a range of development contexts globally.They were also chosen to highlight the different types of
Fig. 1 Example process map of the registration of a birth
Cobos Muñoz et al. BMC Medicine (2020) 18:67 Page 3 of 10

issues and challenges found within CRVS systems as wellas the potential interventions to address these.
MyanmarMyanmar has made substantial progress in improving itsCRVS system over the twentieth century [6]. The CRVS
system was initially established in lower townships in thelate nineteenth century, eventually extending to upper-Myanmar during 1906–1907 [7]. Two main institutionsare responsible for Myanmar’s CRVS system, the Minis-try of Health and Sports and the Central Statistics Or-ganisation (CSO). Birth and death data are collected by
Fig. 2 Example process map of the registration of a death
Cobos Muñoz et al. BMC Medicine (2020) 18:67 Page 4 of 10

basic health staff, such as midwives and health assistants,under the authority of the Department of Public Health,Ministry of Health and Sports. This data is then sent tothe CSO, which compiles, tabulates and analyses thedata and publishes reports [8]. Legislation introduced in2012 obligates families to report births and deaths to thelocal General Administrative Department office within 3days of occurrence [9]; however, in practice, this doesnot always happen as communities generally have lowlevels of awareness about birth and death registrationprocedures or the value of death certificates. Withoutadequate monitoring and enforcement as well as withoutappropriate data collection and transfer procedures, ap-proximately 30% of births and 40% of deaths continue togo unrecorded by the civil registration system [8].
Improving overall system function and coordination isa top priority for Myanmar. In 2015, the Government ofMyanmar, in collaboration with D4H, officially commit-ted to strategically strengthening its CRVS system. FromJanuary to August 2016, a series of process managementexercises were undertaken to evaluate the existing CRVSsystem. Given the complexity of the CRVS system, sev-eral stakeholder groups were involved, including generaladministrators, auxiliary midwives, community healthworkers, traditional birth attendants, community in-formers, free funeral service associations, basic healthstaff, immigration staff, CSO staff and members ofcommunity-based organisations.The exercises uncovered several key gaps, the most
prominent of which was the lack of a proactive notifica-tion system for births and deaths, which is critical to at-tain 100% registration completeness in a timely manner.Additionally, the mapping exercise found data validationand sharing to be absent as there was no formalised sys-tem among key government agencies. The lack of datavalidation was reinforced when data discrepancies, in-completeness and inaccuracies were found after compar-ing information on vital events from different datasources. Furthermore, the exercise highlighted the ab-sence of a formalised data quality assurance system tocorrect for incomplete information and inaccuraciessuch as missing values in birth notification forms as wellas age heaping or errors in medical certificates of causesof death (COD).
Table 2 Examples of key questions addressed during processmanagement
Design flaws, inefficiencies and bottlenecks in civil registration and vitalstatistics (CRVS) processes are identified and documented as part ofprocess management, with potential solutions and new interventionsdiscussed. Key questions include:• Is the current CRVS system process aligned with the vision, mission,
legal authority and objectives of the system and the various actorswithin it?• Is the current CRVS process producing what is expected? That is,
high-quality and reliable data for population health policy andplanning?• Are there bottlenecks or dead-ends in the current CRVS system?• Are there duplications or parallel systems?• Is there room for gains in efficiency in the current CRVS system; that
is, room for savings in time, resources, technology and cost?
Fig. 3 Applications of process mapping among Data for Health countries
Cobos Muñoz et al. BMC Medicine (2020) 18:67 Page 5 of 10

Process mapping also revealed that, while basic healthstaff did an acceptable job of registering births as part oftheir routine tasks, they did not always register deathsand rarely provided awareness on death registration tothe community. Midwives had substantial workloads andcould not fill in birth and death forms completely for allevents, resulting in reduced efficiency of the registrationprocess and the loss of relevant epidemiological informa-tion. Furthermore, as COD information for the registra-tion of community deaths was collected through aninformal interview with the deceased’s family, vague
diagnoses were often given, and the resulting COD datawere not useful for policy and planning purposes. Otherbottlenecks identified included the paper-based storageand archiving system, and the high transfer rate oftrained mortality coders in the CSO, which led to delaysin vital statistics reports.By undertaking process management, stakeholders were
able to identify gaps and bottlenecks in the MyanmarCRVS system, and collaboratively determine innovativestrategic interventions to improve the system. One suchintervention included the introduction of automated verbal
Table 3 Summary of key weaknesses and challenges identified across UoM D4H countries through process mapping [5]
CRVS milestone Definition Common weaknesses and challenges
1. Notification The capture and onward transmission of minimum essentialinformation on the fact of birth or death by a designatedagent or official of the CRVS system, using a CRVS authorisednotification form (paper or electronic) with that transmissionof information being sufficient to support eventualregistration and certification of the vital event
The notification of vital events was one of the least consistentsub-processes across countries; the stakeholders involved var-ied from country to country (even among different regionswithin a country) and some countries did not have a SOP forhow to notify a vital eventIt was difficult to find regulations or SOPs describing how thenotification of vital events should be done or whichinstitution or individuals were entitled/responsible to notifyvital events; globally, there is a paucity of guidance forcountries on the international standards for notification ofvital events
2. Validation The act by which a relevant authority confirms that allnecessary documentation to prove the vital event is correctand that the registration process can continue
The validation of the vital event, although present in allcountries as a sub-process, was not consistent across coun-tries or even among different regions within a country; least-developed CRVS systems did not have written procedures tosupport their local civil registration offices in the validationprocess; it was also difficult to find global recommendationson what the minimum requirements should be to validate avital event
3. Registration The act of formally registering an event at a civil registrationoffice; at this point, the details of the event are entered intothe official civil register by the registrar
Registration of the vital event by civil registrars was quiteconsistent across countries and aligned with globalrecommendations
4. Certification The issuance by the civil registrar of a legal documentcertifying a birth or death
Certification of the vital event by civil registrars was quiteconsistent across countries and aligned with globalrecommendations
5. Sharing ofinformation
All activities in which some information about the individualevent is shared with other systems (i.e. ID)
Several initiatives were identified among the countries toshare civil registration information with other institutions suchas the national ID system or the health sector
6. Storage andarchiving
Activities where all or part of the information captured aboutthe vital event is stored either digitally or in paper
The storage of vital records was fragmented and there wereno consistency checks among the different databases inmultiple countries; although the global recommendations areclear about the ideal storage system and minimumrequirements for archiving vital event records, this was notconsistently applied in many countries
7–10. Compilation todissemination of vitalstatistics
The process of condensing and summarising information onvital events by classifying and tabulating data withincategories or groups to produce vital statistics according to apredetermined tabulation programmeTimely publication of an annual national vital statistics reporton births and deaths disaggregated by age, sex and sub-national region, including numbers and completeness (cover-age) rates, with trends and patterns of leading CODs, in apublic repository
Although all countries mapped a step where the quality ofthe data compiled is assessed and improved, it was difficultto get accurate information about the type of checksperformed or if these were done in a systematic way; thisactivity is either done by the health sector/civil registrationauthority directly on the main database or by the NSO in ananonymised databaseOnce the database is clean, the NSO generates the vitalstatistics report and publishes it in different formats; a fewcountries conduct some form of matching among differentdatabases containing information about vital events (usuallyhealth sector notification database and civil registrationrecords) aiming to obtain a more complete set of vitalstatistics
COD causes of death, CRVS civil registration and vital statistics, ID National Identification, NSO National Statistics Office, SOP standard operating procedure
Cobos Muñoz et al. BMC Medicine (2020) 18:67 Page 6 of 10

autopsy (VA) to improve the efficiency of death registra-tion by midwives and generate accurate information oncauses of community deaths, which account for approxi-mately 84% of deaths in the country. Other interventionsincluded advocacy for, and establishment of, a community-led notification system as well as campaigns to increasecommunity awareness about the importance and benefitsof birth and death registration. Additionally, following theprocess mapping exercise, the Myanmar Governmentrecognised the need for a quality assurance system andstandard operating procedures for data analysis. Going for-ward, the process maps developed can be used to system-atically monitor improvements due to implementation ofinterventions over time [1].
Papua New GuineaPapua New Guinea (PNG) is a large and culturally di-verse country comprising the eastern half of the islandof New Guinea and multiple islands in the surrounds.Principal government stakeholders in the CRVS systeminclude the Ministry of National Planning and Monitor-ing, which oversees the Civil and Identity Registry Officeand the National Statistics Office; the Ministry of Healthand HIV/AIDS, which oversees the National Departmentof Health, the Performance Monitoring and EvaluationBranch, the PNG Institute of Medical Research, and theAIDS Council; and the Department of Provincial andLocal Level Government Affairs [9]. Due, in part, to thecomplexity of providing effective public services underchallenging conditions, with 80% of the country’s 8 mil-lion people living in rural or remote areas, CRVS pro-cesses in PNG have been mostly dysfunctional in recentdecades. While it is estimated that approximately 38% ofbirths and 20% of deaths are captured within the healthsystem, less than 5% of these events ever become offi-cially registered [10]. The Civil Registration Act wasinterpreted by civil registration offices as a guideline tomaximise coverage of the national ID card rather than alegislative framework mandating registration of birthsand deaths, and while the health sector collects relativelyextensive data on births and deaths at health facilities,this information is not linked with the CRVS system.Furthermore, medical certification of COD is not com-pulsory in PNG. Thus, there is no comprehensive sourceof data for the calculation and compilation of vitalstatistics.
UoM D4H has been working with the government ofPNG since 2015 to improve CRVS in the country. A keyaspect of the work plan has been to link the CRVS andnational ID systems to help ensure data is accurate andup to date. Process management was also used as part ofa broader legal review aimed at developing a new civilregistration bill to better reflect the situation and provide
guidance on more effective birth and death registrationprocesses.Process mapping became an integral part of the legal re-
view, enabling government stakeholders to come togetherand understand the processes required for notificationand registration as well as to plan what the ideal processesshould be. Stakeholders from several government bodiesattended, including from the National Department ofHealth, the Department of National Planning and Moni-toring, the Department of Provincial and Local Level Gov-ernment Affairs, the National Statistics Office, the Civiland Identity Registry, and the Constitution and Law Re-form Commission. Key outcomes were stakeholders’ ac-knowledgement of their lack of understanding of thenotification and registration processes as well as recogni-tion of the many barriers individuals and families experi-ence when attempting to register their vital events.During the mapping exercise, stakeholders had diffi-
culty in defining the exact processes required for the no-tification and registration of births and deaths. This wasdue to the complexities involved and how infrequentlycertain events are notified and registered. For example,for community deaths, three letters signed by commu-nity leaders are required for the local civil registry officeto start the registration processes. Similarly, for births,while the health system and church parish registries holdrecords of many births, there is no formalised system forsharing these with civil registration. The difficulty, costand onus solely on the family to initiate and continuethe process were identified as clear obstacles to attaininggood coverage of notification and registration, especiallyin a setting where the benefits of birth and death regis-tration are not yet clear for the population.As a first step to overcome some of these barriers,
stakeholders produced as-desired process maps. Healthsector involvement was identified as essential to create anotification system able to achieve good coverage ofbirths and deaths. The Constitution and Law ReformCommission was able to recognise, from the final as-desired maps, certain amendments required to the newlegislation to facilitate the processes, for example, re-moving the requirement for a COD in order to completeregistration and permitting various agents to notify com-munity births and deaths.Bringing all stakeholders together in this way to
understand the current systems and design as-desiredprocesses was a significant step in getting governmentdepartments to work together, recognise each other’sroles and enable them to begin planning for improvedfuture CRVS processes. The new civil registration bill,following good stakeholder participation, is expected tofacilitate future CRVS processes in PNG. A processmanagement technical working group with membersfrom all attending government departments has been
Cobos Muñoz et al. BMC Medicine (2020) 18:67 Page 7 of 10

created to continue updating the process maps with fu-ture developments and will report regularly to the na-tional CRVS Committee.
RwandaIn Rwanda, as in most of Africa, registration of vitalevents began during the colonial period, although regis-tration laws only applied to nationals of the colonialpowers and not to indigenous Rwandans. Subsequentlaws regulating civil registration evolved along with thestages of its political and administrative history. From in-dependence in 1962 until 2006, the district level was thelowest administrative level to perform civil registration.With the second phase of the decentralisation processinitiated in 2006, the responsibilities of civil registrationwere extended to the Sector which is a lower administra-tive level in the government. The Sector Executive Sec-retary (who is the highest ranking official in the Sector)was added to the list of country civil registrars with theaim of bringing the most needed services closer to thepopulation [11].Rwanda has good national level coordination among
key entities such as the Ministry of Health and the Na-tional Institute of Statistics of Rwanda (NISR); however,coordination at the sector level is less functional. The in-complete notification and registration of births anddeaths that occur in the community is problematic, par-ticularly so for the latter, as they are more likely to occurat home and minimal information is available for theCODs occurring outside of health facilities. In responseto this, in 2016, Rwanda conducted a comprehensive as-sessment of the CRVS system [12], which included thedevelopment of a series of process maps to inform theCRVS National Strategic Plan for 2017–2018 to 2021–2022 [13].The process management exercise identified signifi-
cant gaps in birth and death notification and registrationprocesses, particularly between health facility notificationand official registration at the sector level. This realisa-tion led to an intervention to support the NISR andRwandan Ministry of Health to develop clear pathwaysfor notification and registration of the events in both thecommunity and health facilities. The process maps de-veloped were used to re-design information flows forbirths and deaths from the community and health facil-ity levels to the sector level registration offices.Process mapping also uncovered extremely low rates
of registration of deaths that occurred outside of healthfacilities, leading to difficulties in capturing informationregarding fact of death and COD and significantlyimpacting the quality of mortality statistics. To addressthis, a second intervention to improve information oncommunity deaths and COD was introduced in 2017. AHome-Based Care Practitioner programme using VA
was introduced to generate information on COD forcommunity deaths where physicians were not able toprovide a reliable cause. As part of the integration of VAactivities into the CRVS system, the NISR ‘opened a win-dow’ in their digital CRVS system to allow Home-BasedCare Practitioners to notify sector civil registration of-fices and health facilities about deaths that occurred intheir catchment area. Process management was instru-mental in the development of this activity and helped tocreate a reliable and systematic flow of information,which also helped to improve death registration com-pleteness. As it was a collaborative endeavour, processmaps went through five iterations of development beforean agreed-upon map was created and used for imple-mentation. Process mapping was critical in helping regu-lators understand considerations for the flow ofnotification of deaths and conducting VAs and was anexceptionally valuable tool to understand the CRVS sys-tem as a whole and strengthen its performance.
DiscussionReviewing CRVS processes is a necessary step in anyCRVS system reform effort. Process mapping can high-light missing or inefficient practices, such as duplicationof data collection across agencies, unclear processes, andlimited or poor data-sharing practices, among others.Process management in UoM D4H countries was criticalto identify gaps in the processes required to notify birthsand deaths and in developing appropriate interventions.In Myanmar, mapping demonstrated that there was noformalised notification process, while in PNG, it wasused to inform stakeholders about the onerous and oftenunclear procedures needed to notify a vital event. In thecase of Rwanda, significant gaps between notificationand registration were identified, particularly betweenhealth facility notification and official registration at thesector level. By identifying the issues in the notificationprocess, all three countries were able to use the informa-tion from the process maps to inform interventions toimprove the notification of vital events.Process mapping also enabled all stakeholders to con-
verge, often for the first time, to collaboratively discussand understand the current CRVS systems. A key outcomeof this, as was the case in PNG, was that stakeholderscould acknowledge where they lacked understanding ofthe notification and registration processes, and work to-wards more clearly defining and coordinating these pro-cesses. This collective understanding, or in some casesacknowledgement of areas of unknown or misunderstoodprocesses, allowed stakeholders to agree on and prioritiseinterventions to strengthen their CRVS systems in termsof the legal framework underpinning the system as well asfor the registration of vital events and generation of vitalstatistics.
Cobos Muñoz et al. BMC Medicine (2020) 18:67 Page 8 of 10

Coordination among stakeholders, more efficient useof services and more formalised data-sharing agreementsare often key outcomes of process management, as wasthe case in Rwanda and Myanmar. The mapping exer-cises in these countries supported better communicationand coordination among the different entities involvedin the notification and registration process. Furthermore,process management can be a useful tool for all CRVSsystems, from the most rudimentary to the most devel-oped. Systems in their infancy, with low levels of regis-tration completeness, can use process maps to identifythe most critical gaps to focus on for the improvementof registration of vital events. Improving registrationcompleteness will allow countries to work towards pro-ducing reliable vital statistics that can be used for report-ing on SDG indicators;, with Indicator 17.19.2 beingcritical in monitoring the improvement of birth anddeath registration completeness in the system [3].CRVS systems that are more developed can also use
process maps to improve registration completeness as wellas to identify system bottlenecks and weaknesses that canimpact the efficiency of services, data flow, quality andtimeliness. Improving the coordination and efficiency ofoperations and the flow of data will allow for more timelyproduction of vital statistics and reporting on the SDG in-dicators they support; better data quality will allow for im-proved health and SDG monitoring.
ConclusionCRVS systems in LMICs are struggling to produce thehigh-quality vital statistics needed for public health pol-icy and for monitoring and reporting on a variety of in-dicators. Process management can help stakeholdersshare a common view of the system, identify weak-nesses and work collaboratively to find solutions. Map-ping offers an opportunity to overcome the piecemealtreatment of CRVS systems across different, often si-loed, government agencies, allowing an aligned andend-to-end view of the system in its current operations;this is a key prerequisite to prioritising corrective inter-ventions and managing the necessary changes for theimprovement of system performance. Process mappinghas been shown to be a valuable tool to strengthenCRVS systems and increase the quality and complete-ness of vital statistics. Furthermore, it can be particu-larly useful in pinpointing weaknesses in reportingevents such as suspicious deaths and thus improve thereporting of cause-specific mortality for SDG indica-tors. Strengthening CRVS systems through processmapping and management results in more robust, reli-able and timely vital statistics that can be used forhealth planning and better monitoring of national andglobal health development goals.
AcknowledgementsNot applicable.
Authors’ contributionsDM and DS conducted the in-country process mapping, including data ana-lysis and validation, edited earlier versions of the manuscript, and contrib-uted to the final version of the manuscript. RS contributed to the analyticalframework, drafted earlier versions of the manuscript, and contributed to thefinal version of the manuscript. KB, JH, VK and XN were responsible for imple-menting activities under the Data for Health Initiative, including those onprocess mapping as described. They provided country-specific informationand edited earlier versions of the manuscript. NR and ADL conceptualisedthe manuscript, developed the analytical framework, drafted earlier versionsof the manuscript, and contributed to the final version of the manuscript. Allauthors have read and approved the final manuscript.
FundingThis study was funded under an award from Bloomberg Philanthropies tothe University of Melbourne to support the Data for Health Initiative. Thefunders had no role in study design, data collection and analysis, decision topublish, or preparation of the manuscript.
Availability of data and materialsNot applicable.
Ethics approval and consent to participateNot applicable.
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Author details1Swiss Tropical and Public Health Institute, Socinstrasse 57, Basel CH-4002,Switzerland. 2University of Basel, Petersplatz 1, Basel CH-4002, Switzerland.3Melbourne School of Population and Global Health, The University ofMelbourne, Carlton, Victoria 3053, Australia. 4Data for Health, Nay Pyi Taw,Myanmar. 5Data for Health, Port Moresby, Papua New Guinea. 6NationalInstitute of Statistics of Rwanda, Kigali City, Rwanda.
Received: 2 September 2019 Accepted: 11 February 2020
References1. de Savigny D, Cobos Muñoz D. Understanding CRVS Systems: The
Importance of Process Mapping. CRVS Development Series. The Universityof Melbourne. 2018. https://crvsgateway.info.myudo.net/file/9847/46.Accessed Aug 2019.
2. Cobos Muñoz D, Sant Fruchtman C, Miki J, Vargas-Herrera J, Botchway E,Woode S, Dake F, de Savigny D. Mapping Sources and Silos of MortalityData: Case Studies in Peru and Ghana. CRVS Technical Outcome Series. TheUniversity of Melbourne. 2019. https://crvsgateway.info/file/11077/3229.Accessed Aug 2019.
3. Richards N, Sorchik R, Brolan C. Why the Sustainable Development GoalAgenda Needs Strong Civil Registration and Vital Statistics Systems. CRVSDevelopment Series. Melbourne, Australia: Bloomberg Philanthropies Datafor Health Initiative, Civil Registration and Vital Statistics Improvement. NayPyi Taw: The University of Melbourne. 2018. https://crvsgateway.info.myudo.net/file/9849/1967. Accessed Aug 2019.
4. Cobos Muñoz D, Abouzahr C, de Savigny D. The ‘ten CRVS milestones’framework for understanding civil registration and vital statistics systems.BMJ Glob Health. 2018;3:e000673. https://doi.org/10.1136/bmjgh-2017-000673.
5. Cobos Muñoz D, Sant Fruchtman C, Renggli S, de Savigny D. CRVSInnovations: Assessing the Performance of CRVS Systems, CRVS TechnicalOutcome Series. The University of Melbourne. 2019. https://crvsgateway.info.myudo.net/file/10766/3136. Accessed Aug 2019.
6. Taw NP. CRVS system review report: Ministry of Health and Sports; Nay PyiTaw, 2014.
Cobos Muñoz et al. BMC Medicine (2020) 18:67 Page 9 of 10
7. Taw NP. Sample survey on evaluation of the completeness of vitalregistration Systems in Myanmar: Central Statistical Organization; Nay PyiTaw, 1995.
8. Mar, TZ. Fellowship Profile: Developing a Qualitative Study Protocol on VAInterviewer Experiences in Myanmar. CRVS Country Perspectives. TheUniversity of Melbourne. 2018. https://crvsgateway.info/file/9780/2232.Accessed Aug 2019.
9. Myint S, Lwin AM. Study on Completeness of Mortality Statistics inMyanmar: Department of Health Planning; Nay Pyi Taw, 2014.
10. Rouka I, Mathias E. Fellowship Report: An Analysis of Cause of Death Datafrom Papua New Guinea. CRVS Country Perspectives. The University ofMelbourne and National Department of Health of Papua New Guinea. 2018.https://crvsgateway.info.myudo.net/file/9785/2376. Accessed Aug 2019.
11. Presidential Order n° 57/01 of 15/10/2006, determining the Structure andFunctioning of Village, Cell and Sector (Art.74).
12. National Institute of Statistics of Rwanda. Rwanda Civil Registration and VitalStatistics Systems: Comprehensive Assessment Final Report Volume I. Kigali.2016. http://www.statistics.gov.rw/file/5059/download?token=4VFetbmn.Accessed Aug 2019.
13. National Institute of Statistics of Rwanda. CRVS National Strategic Plan.Kigali. 2018. https://statistics.gov.rw/publication/crvs-national-strategic-plan.Accessed Aug 2019.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Cobos Muñoz et al. BMC Medicine (2020) 18:67 Page 10 of 10