behavioral and treatment research on marijuana withdrawal and dependence alan j. budney university...
TRANSCRIPT

Behavioral and Treatment Research on Marijuana Withdrawal and Dependence
Alan J. Budney University of Vermont
Supported by NIDA: DA08655, DA12471, DA12157, DA015186, T32DA07242
Marijuana is more similar than dissimilar to other drugs of abuse
Like other substances of abuse, a subset of persons who use marijuana go on to have problems…some not so serious, some serious
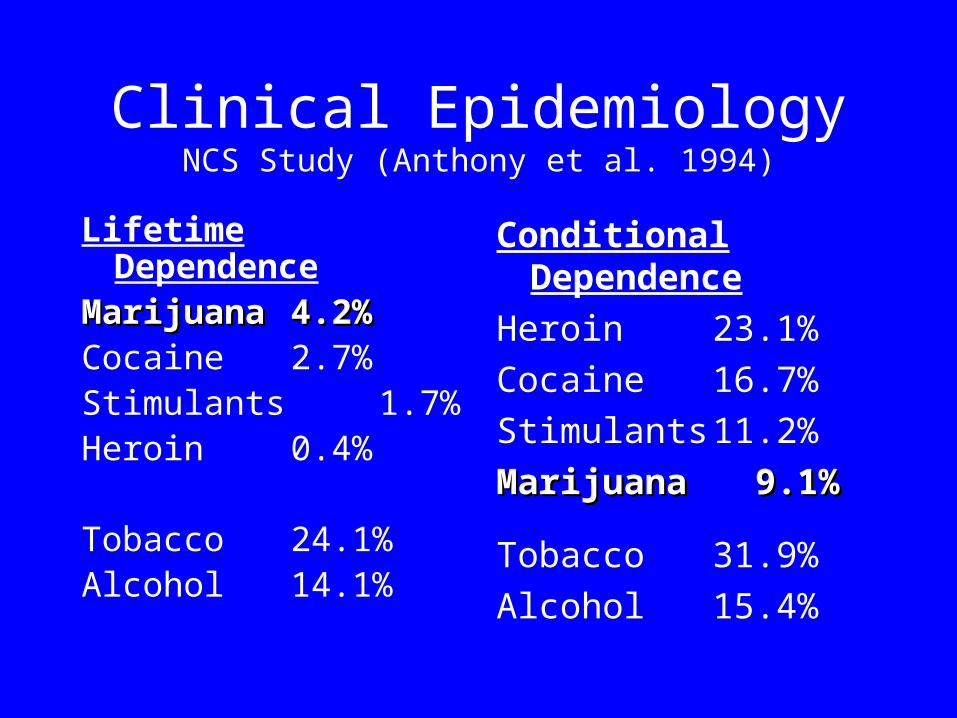
Clinical EpidemiologyNCS Study (Anthony et al. 1994)
Lifetime DependenceMarijuana Marijuana 4.2%4.2%Cocaine 2.7%Stimulants 1.7%Heroin 0.4%
Tobacco24.1%Alcohol 14.1%
Conditional Dependence
Heroin 23.1%
Cocaine 16.7%
Stimulants 11.2%
MarijuanaMarijuana 9.1% 9.1%
Tobacco31.9%
Alcohol 15.4%

Treatment Admissions (SAMHSA 2001)
0
10
20
30
40
50
60
Alcohol Cocaine Heroin Marijuana
199219962001
Treatment Outcome Studies
- 4 controlled studies (Adults)Stephens, Roffman et al. (1994, 2000)Budney, et al. (2000)Copeland et al. (2001) Australia
- 2 others in press or in preparationMarijuana Treatment Project(multi-site study)Budney et al.
Patient Characteristics
Age 32-35 (10.0) yrs
Male 75%
Employed (FT) 55-60%
Marital Status 55-60% never married
Marijuana Dependence Severity
# of DSM-III-R criteria 6.3 (1.8)Continued Use 97%Cut Down 86%Larger Amounts 80% Excessive time 73%Withdrawal 75%Tolerance 63%Reduced Activities 41%
Marijuana Use
Days Used/mo 25.6 (7.2) Times per day 3.9 (2.5) Years of Use 13.8 (8.3)$ spent (mo) $123 (185)
Cigarette smoker 46%
Problems Associated with Marijuana(MTP Study, 2000)
Feeling Bad or Guilty 90%
Low Energy Level 86%
Procrastination 86%
Memory loss 76%
Low productivity 75%
Low self-esteem/confidence 70%
Interpersonal 58%
Financial 49%
Family 44%

Reasons for Quitting(Stephens et al, 1993)
• Self-control
• Health concerns
• Self-image
• Not socially acceptable
• Legal problems
• Direct social pressure (family, children)
• Drug testing at work
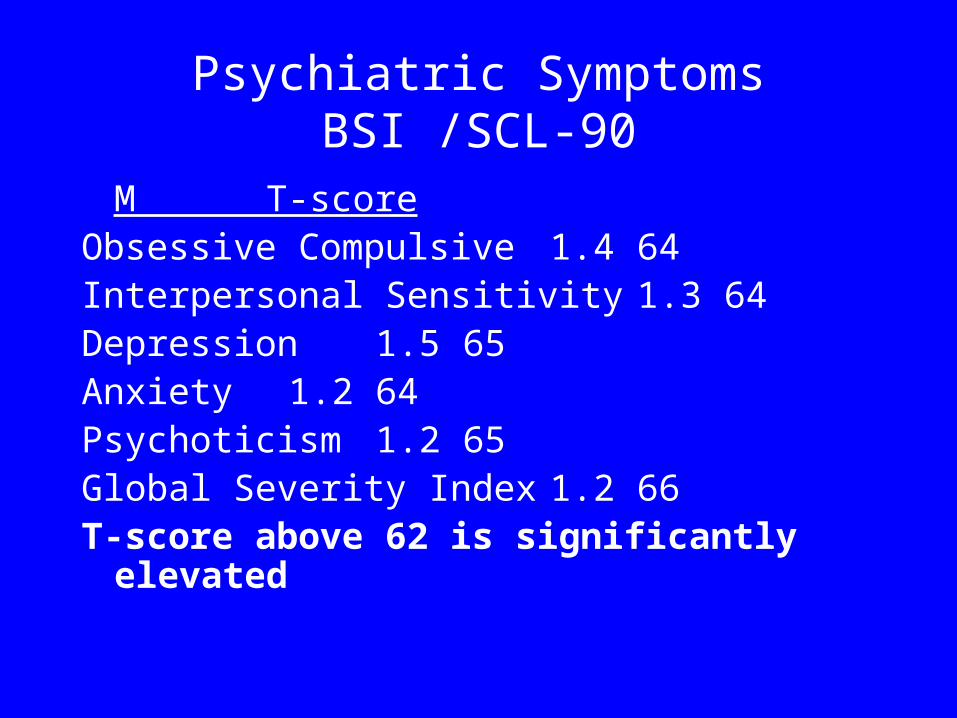
Psychiatric SymptomsBSI /SCL-90
M T-score Obsessive Compulsive 1.4 64Interpersonal Sensitivity 1.3 64Depression 1.5 65Anxiety 1.2 64Psychoticism 1.2 65Global Severity Index 1.2 66T-score above 62 is significantly elevated
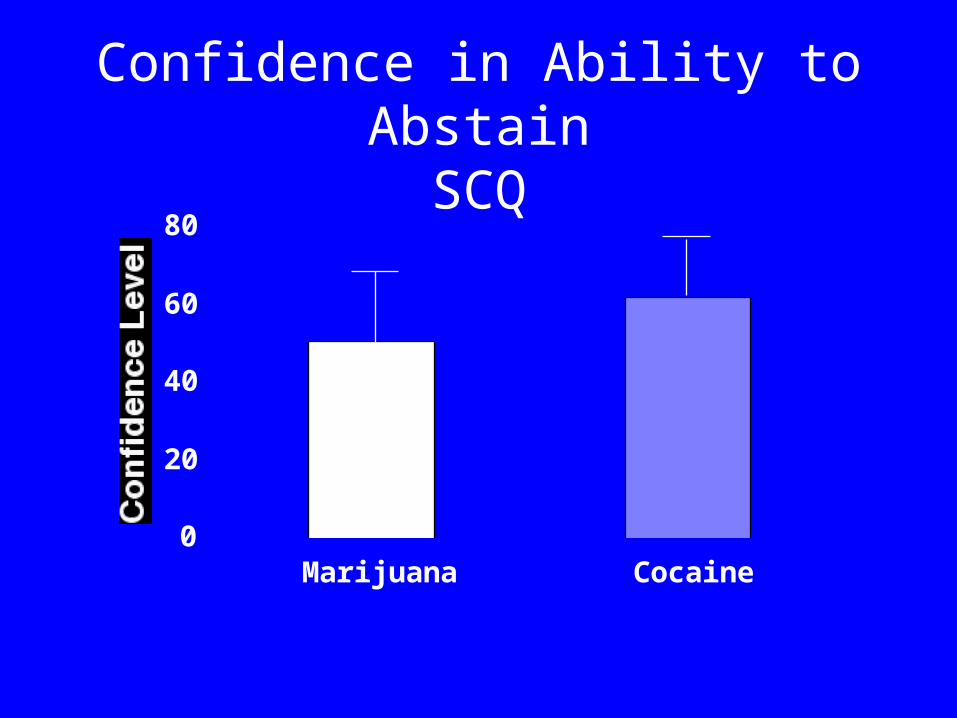
Confidence in Ability to AbstainSCQ
0
20
40
60
80
Marijuana Cocaine
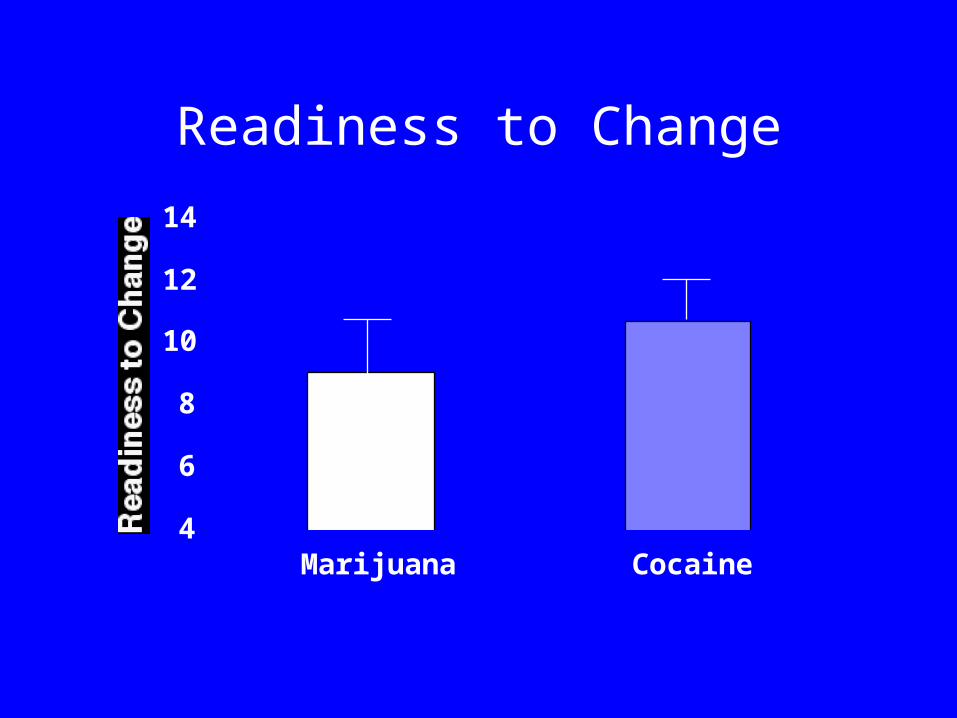
Readiness to Change
4
6
8
10
12
14
Marijuana Cocaine
Adult Treatment Seekers
• Meet 5-7 DSM-III-R criteria (Budney, 2000, 2003;
Stephens et al., 2000, 2002, Copeland et., 2001)
• Associated problems are comparable to other substance dependent populations
• Measures of Readiness to Change and Confidence in Ability to Quit are not high
• Majority not dependent on other substances
Marijuana Withdrawal
Patient concerns and complaints
Old literature, both human and nonhuman
Withdrawal Study 1 (Budney et al. (1999)
Structured survey of 54 adults seeking treatment for marijuana dependence
Marijuana Withdrawal Checklist (22 items) – rate perception of withdrawal severity on
a 0-3 scale (none to severe)
9.6 + 5.1 symptoms of at least mild severity
57%: > 5 symptoms of > moderate severity
47%: > 3 symptoms rated as severe
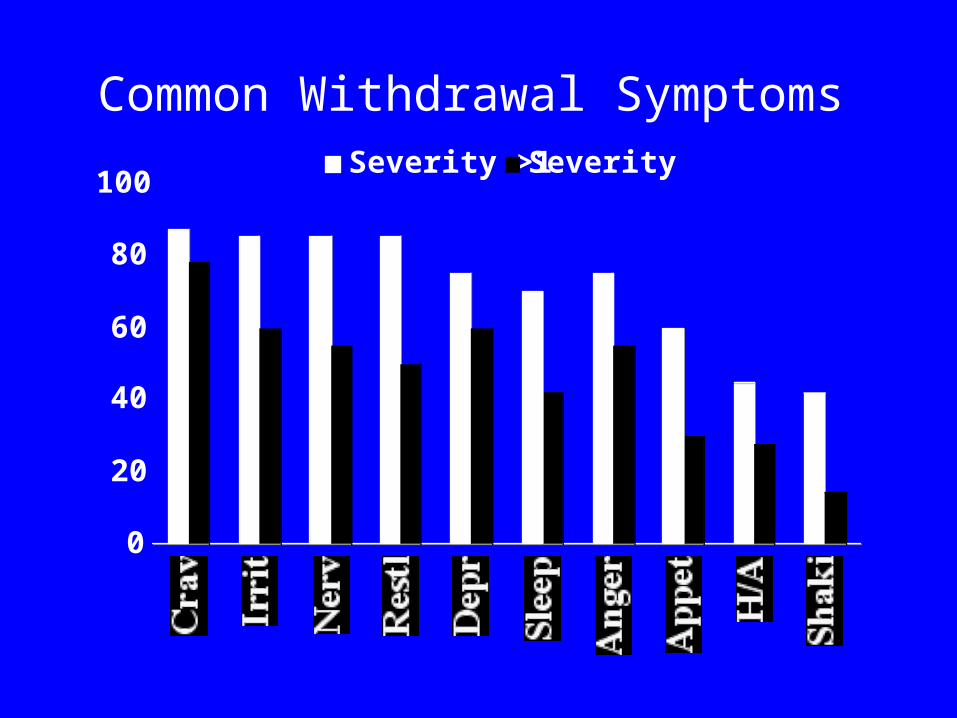
Common Withdrawal Symptoms
0
20
40
60
80
100Severity >1 Severity >2
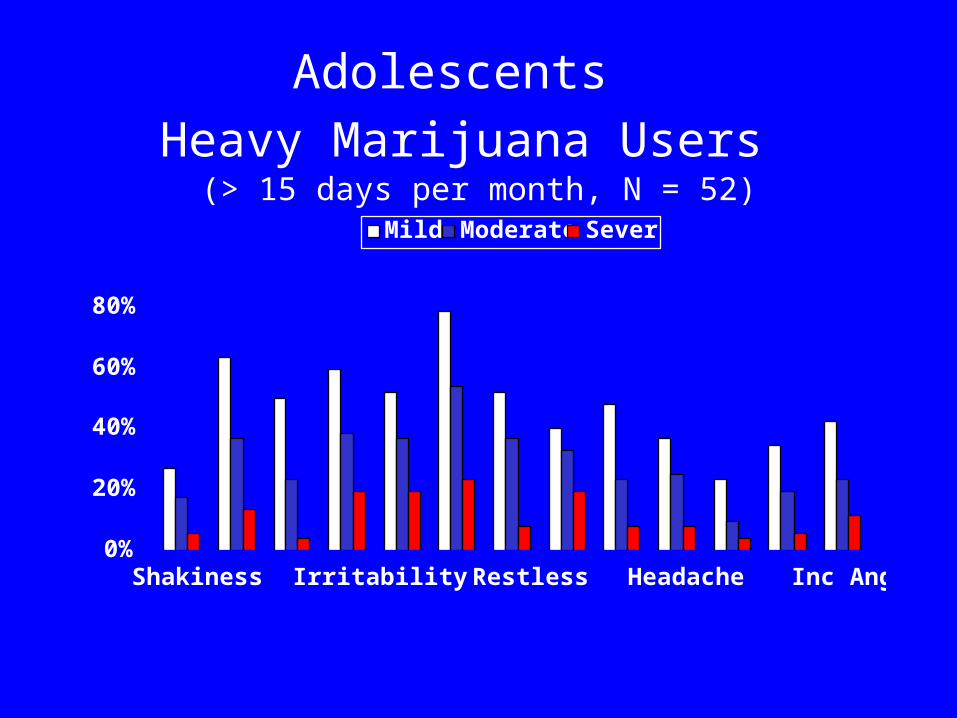
Adolescents
Heavy Marijuana Users (> 15 days per month, N = 52)
0%
20%
40%
60%
80%
Shakiness Irritability Restless Headache Inc Anger
Mild Moderate Severe
These data suggest that marijuana withdrawal
is experienced by the majority of those
seeking treatment for marijuana dependence,
and its severity may warrant clinical
intervention.
Timecourse Study(Budney et al, 2003)
• 50 days, AB design outpatient studyA: 5-day, Baseline (smoking-as-usual) PhaseB: 45-day, Marijuana Abstinence Phase
• 2 groups– 18 chronic, heavy marijuana smokers
(>25/month)– 12 ex-marijuana smokers (abstinent >1 year)
• Previous heavy use
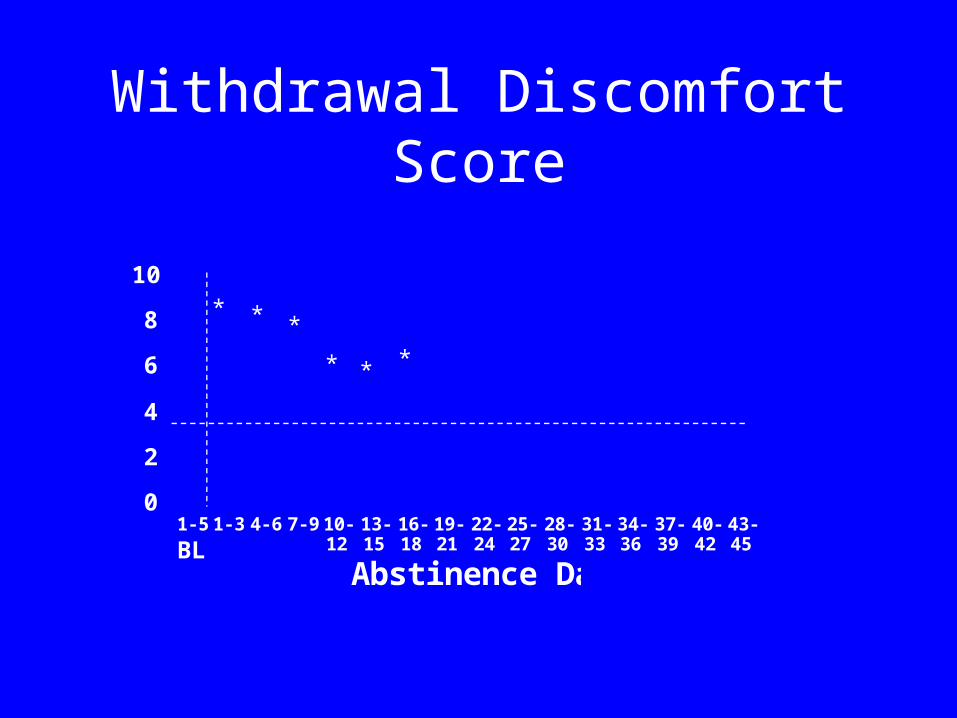
Withdrawal Discomfort Score
0
2
4
6
8
10
1-5 1-3 4-6 7-9 10-12
13-15
16-18
19-21
22-24
25-27
28-30
31-33
34-36
37-39
40-42
43-45
Abstinence Days
*
*
* *
*
BL
*
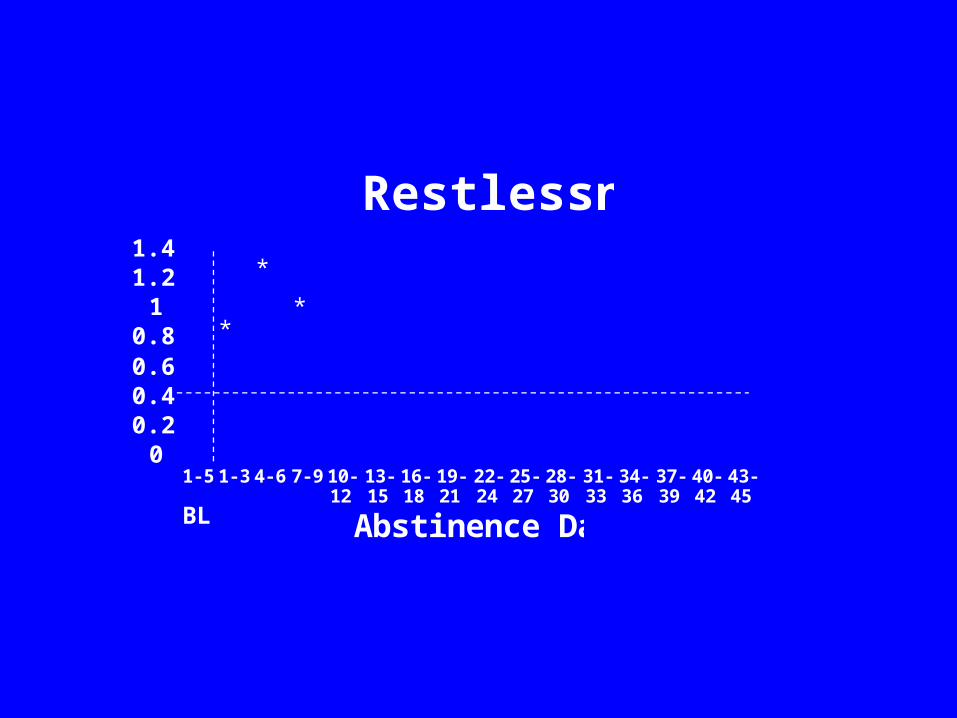
Restlessness
00.20.40.60.8
11.21.4
1-5 1-3 4-6 7-9 10-12
13-15
16-18
19-21
22-24
25-27
28-30
31-33
34-36
37-39
40-42
43-45
Abstinence Days
*
**
BL
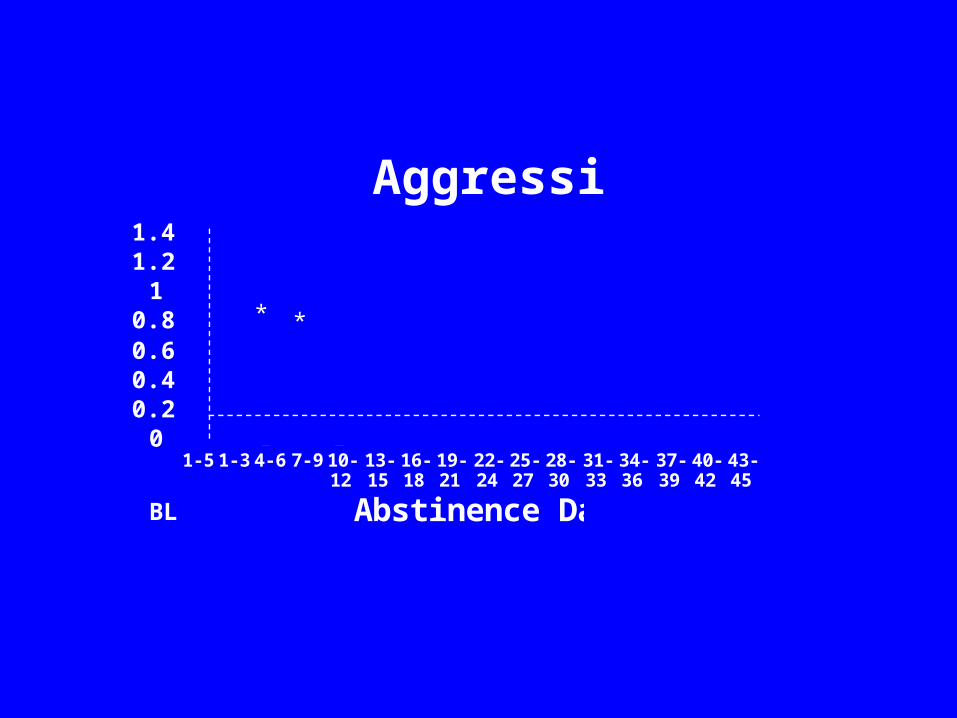
Aggression
00.20.40.60.8
11.21.4
1-5 1-3 4-6 7-9 10-12
13-15
16-18
19-21
22-24
25-27
28-30
31-33
34-36
37-39
40-42
43-45
Abstinence Days
**
*
BL
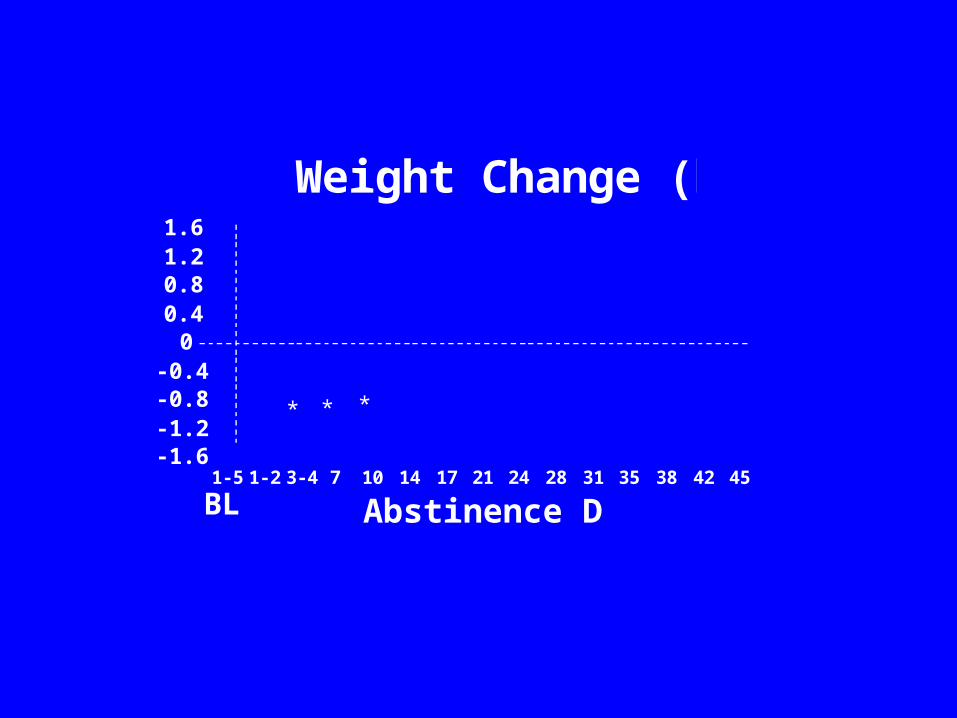
Weight Change (kg)
-1.6-1.2-0.8-0.4
00.40.81.21.6
1-5 1-2 3-4 7 10 14 17 21 24 28 31 35 38 42 45
Abstinence Days
* * *
BL
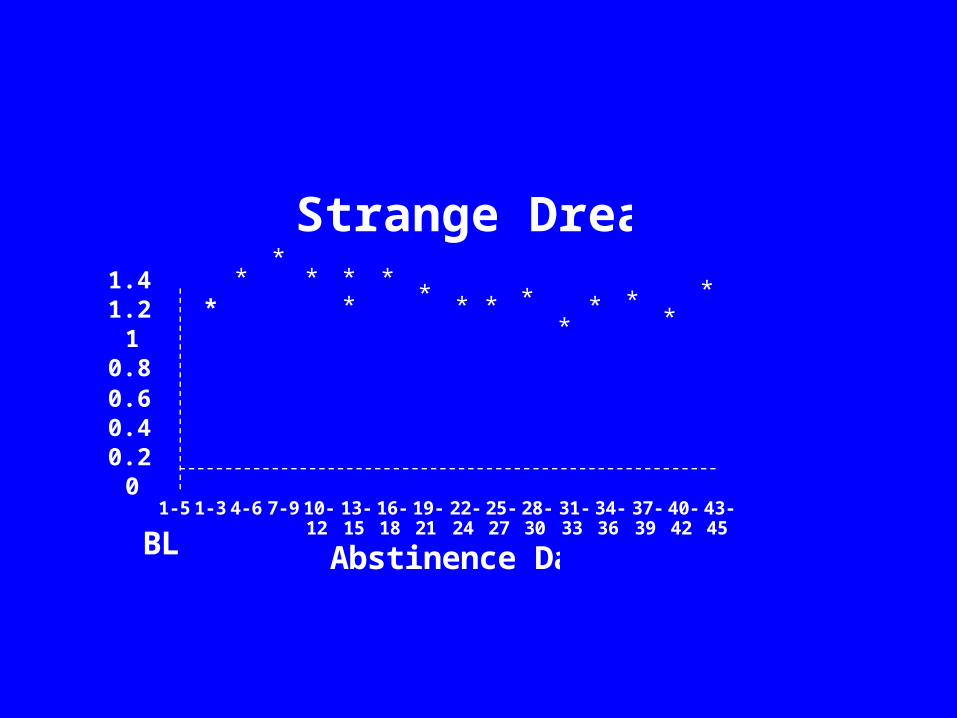
Strange Dreams
00.20.40.60.8
11.21.4
1-5 1-3 4-6 7-9 10-12
13-15
16-18
19-21
22-24
25-27
28-30
31-33
34-36
37-39
40-42
43-45
Abstinence Days
**
**
*** *
*
***
** *
BL
*
Timecourse and Magnitude
- Peak Effects occur between Days 2-6
- 10%-45% increases across symptoms(+ 0.4 to 1.8 pt on the 4-pt severity scale)
- 78% of Ss show > 1-pt change on 5 or more symptoms
- Duration of elevation 5-21 days for most symptoms
Collateral ReportsAggressionIrritability
RestlessnessSleep DifficultyStrange Dreams
Marijuana vs. Tobacco Withdrawal Vandrey et al. (in preparation)
Total Withdrawal Discomfort
0
2
4
6
8
10
B2 B3 B4 A1 A2 A3
TobaccoMarijuana
*Sig diff by condition (p<.001); no interaction by group
Irritability
0
0.2
0.4
0.6
0.8
1
1.2
1.4
B2 B3 B4 A1 A2 A3
TobaccoMarijuana
*Sig diff by condition (p<.001); no interaction by group
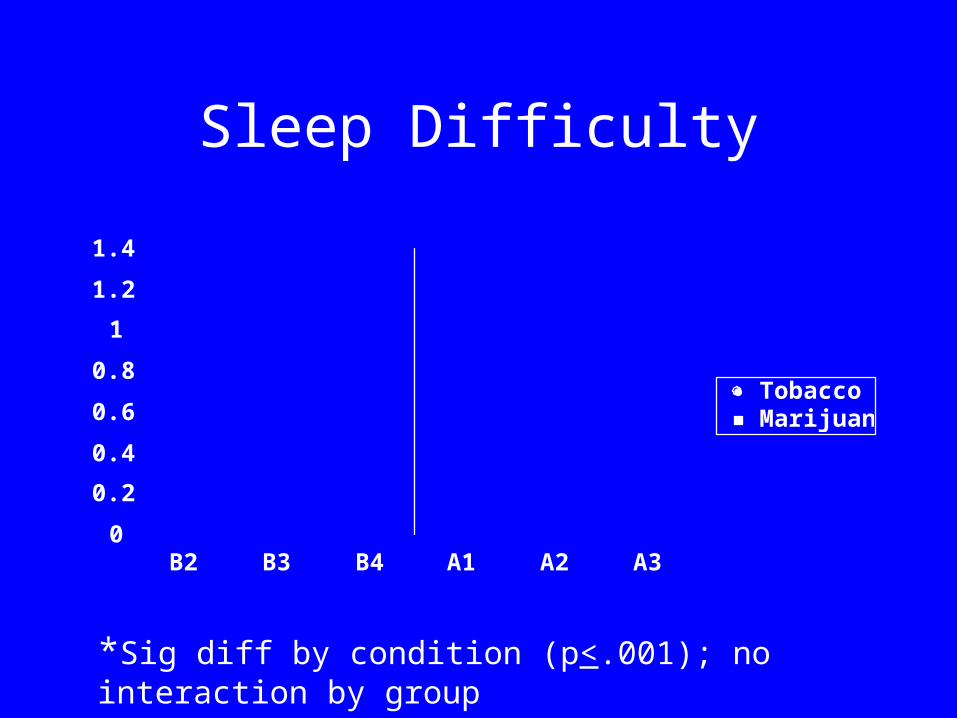
Sleep Difficulty
0
0.2
0.4
0.6
0.8
1
1.2
1.4
B2 B3 B4 A1 A2 A3
TobaccoMarijuana
*Sig diff by condition (p<.001); no interaction by group
Pharmacological SpecificityDronabinol (Oral THC) Attenuates
Marijuana Withdrawal
Outpatient study
7 daily marijuana smokers
ABACAD design
Dronabinol (0, 10, 30mg tid)

Withdrawal Discomfort Score
01
2345
67
Base Placebo Base 10mg Base 30mg
***
**
* diff from base, * diff from 10mg, * diff from 30mg
Symptoms suppressed by 10mg and 30mg
Increased AggressionIncreased AngerIrritabilitySleep DifficultyViolent Outbursts
Symptoms suppressed by 30mg dose only:
– Craving to Smoke Marijuana– Decreased Appetite– Nervousness/Anxiety
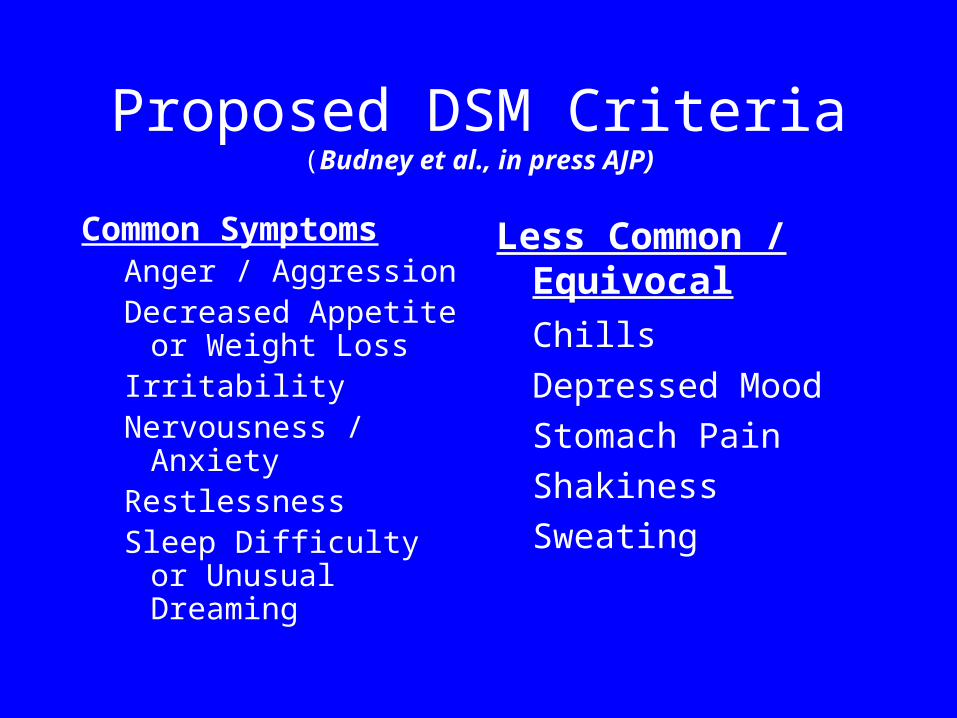
Proposed DSM Criteria(Budney et al., in press AJP)
Common SymptomsAnger / AggressionDecreased Appetite or
Weight LossIrritabilityNervousness / AnxietyRestlessnessSleep Difficulty or
Unusual Dreaming
Less Common / Equivocal
Chills
Depressed Mood
Stomach Pain
Shakiness
Sweating
Treatment Outcome Research Adult Marijuana Dependence
Types of Treatment Studied
• Social Support Group
• CBT Group
• CBT Individual
• Brief Motivational
• Voucher-based Contingency Management
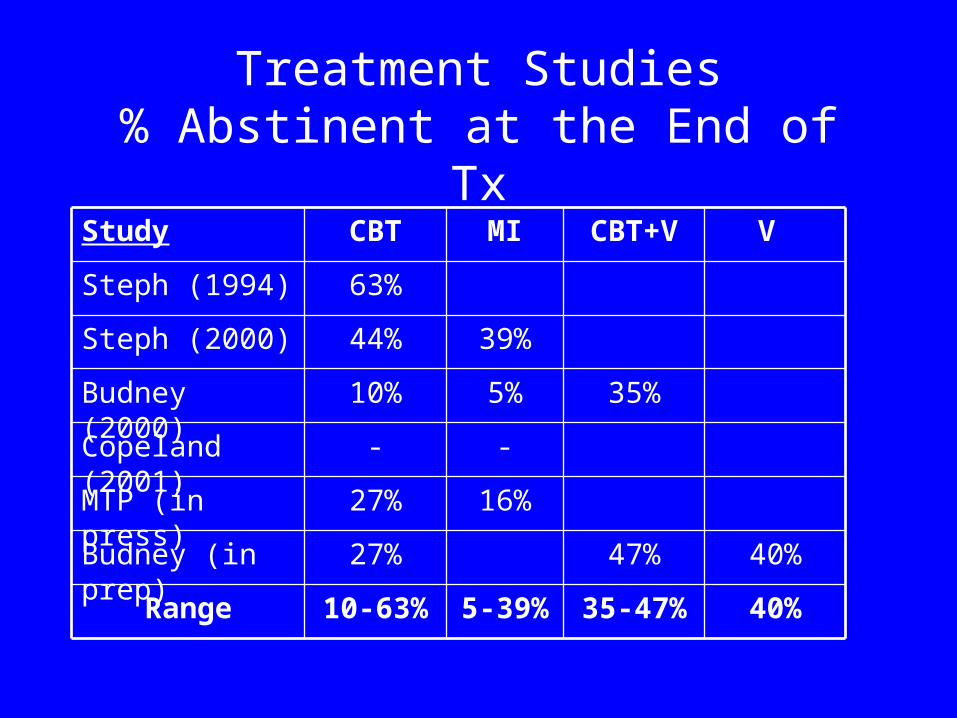
Treatment Studies% Abstinent at the End of Tx
16%27%MTP (in press)
--Copeland (2001)
40%35-47%5-39%10-63%Range
40%
V
47%27%Budney (in prep)
35%5%10%Budney (2000)
39%44%Steph (2000)
63%Steph (1994)
CBT+VMICBTStudy
Treatment Outcome Research Summary to Date
Types of effective treatments are similar to those observed with other substances...- behavioral-based and motivational
therapies
Magnitude of treatment effect appears similar
Primary Aim of our Treatment Research
Develop interventions that can enhance treatment outcomes
Application of Contingency Management
- voucher-based incentive program
Why contingency management?
• Growing literature on CM interventions with adult substance abusers
• CM usually combined with effective behavioral therapies to enhance outcomes
Behavioral Treatment - Study 2(Budney et al. in prep)
Three Group Design
- Behavioral coping-skills (BT)- BT plus vouchers (BTV)- Vouchers only (V)
14-week outpatient programProvided urine specimens twice weekly
*Post-tx follow-up assessments (12 months)
Study 2Replication: vouchers enhance the effect of
behavioral therapy (BTV vs BT) (Budney et al. 2000)
To determine if effects endure post-treatment
To determine if behavioral counseling enhances the effect of the voucher program (V - BTV)
To examine the feasibility of providing the voucher program alone (V)
Study 2Participants
MJ-dependent individuals seeking treatment
N = 9069 men and 21 womenMean Age = 32.7 years
Marijuana useDays used / month: 25.3 + 7.4Times used / day: 3.9 + 3.2 Years of regular use: 13.6 + 10.5

Treatment Acceptability(Budney et al., in prep)
0
20
40
60
80
100
BTBTVVouchers
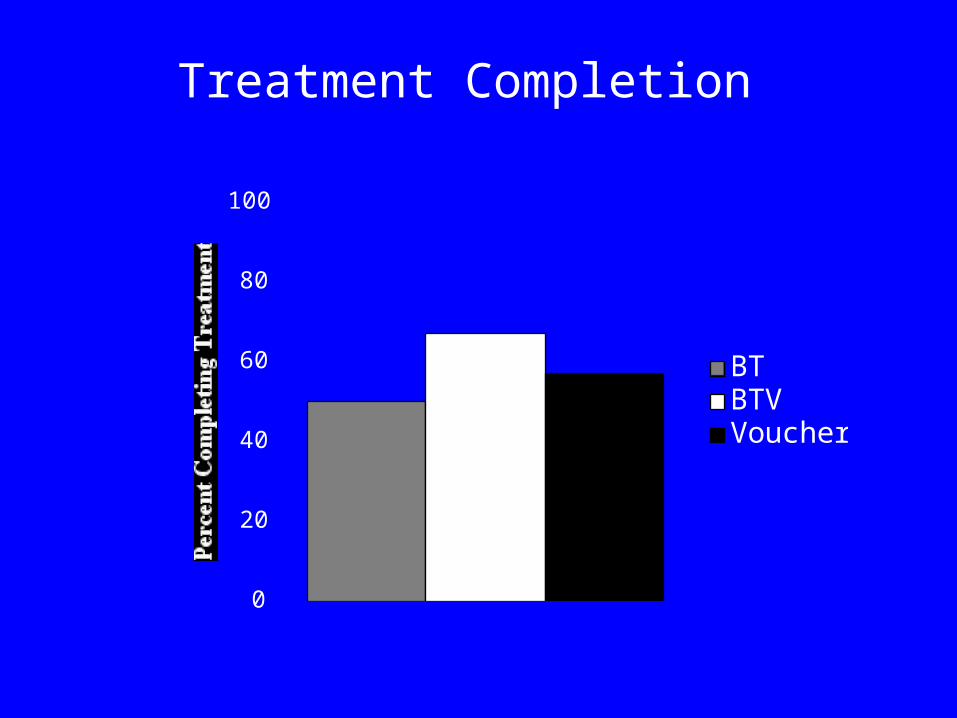
Treatment Completion
0
20
40
60
80
100
BTBTVVouchers
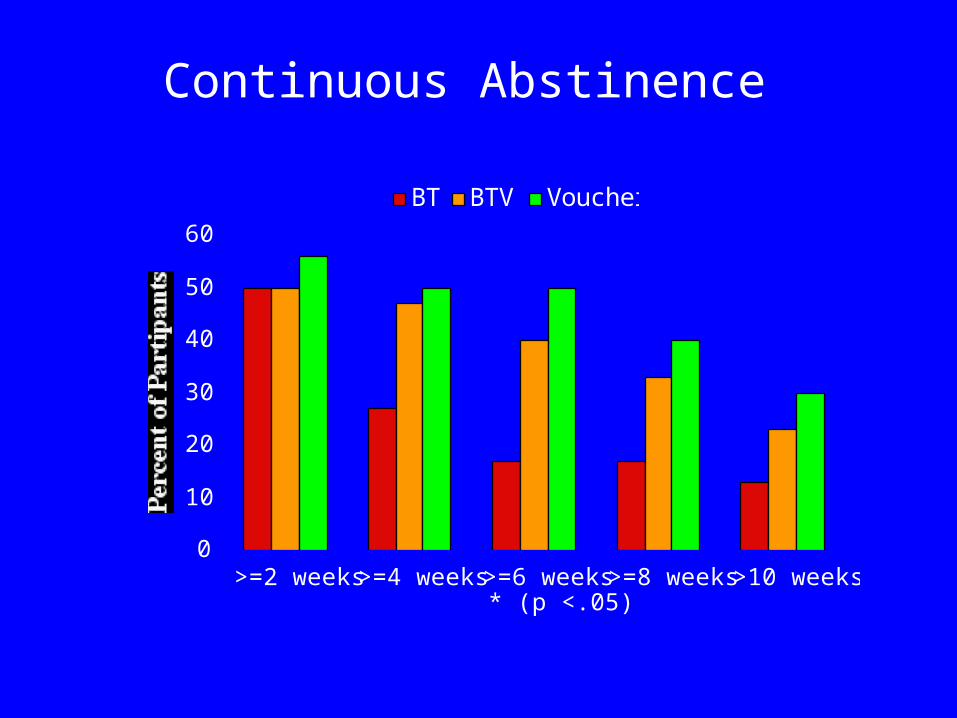
Continuous Abstinence
0
10
20
30
40
50
60
>=2 weeks >=4 weeks >=6 weeks* (p <.05)
>=8 weeks >10 weeks
BT BTV Voucher
Marijuana Abstinence(marijuana-negative urinalysis)
0
10
20
30
40
50
wk1
wk2
wk3
wk4
wk5
wk6
wk7
wk8
wk9
wk10
wk11
wk12
wk13
wk14
Voucher BT BTV
Marijuana Abstinence (marijuana-negative urinalysis)
0
10
20
30
40
50
ETX 1-Month
3-Month
6-Month
9-Month
12-month
BT BTV Voucher
Days of Use per Month
0
10
20
30
Baseline M1-TX M2-TX M3-TX M1-FU M3-FU M12-FU
Voucher BT BTV
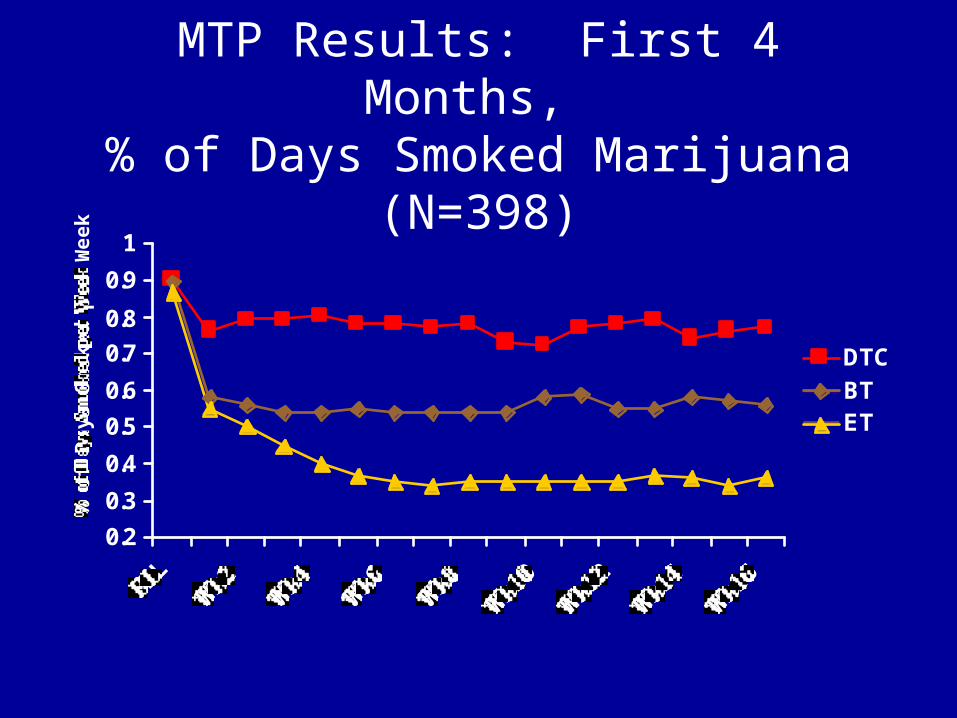
MTP Results: First 4 Months, % of Days Smoked Marijuana (N=398)
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
BLW
k2W
k4W
k6W
k8
Wk10
Wk12
Wk14
Wk16
% o
f D
ays
Smok
ed p
er W
eek
DTC
BTET
Relapse and Lapse(Moore and Budney, 2003)
• N = 152 • Adult MJ-Dependent Treatment Seekers• Across two trials
• N= 82 (54%) achieved 2 wks of abstinence– Self-report verified by urine test
• 90% achieved this 2-wk period with first 6 weeks
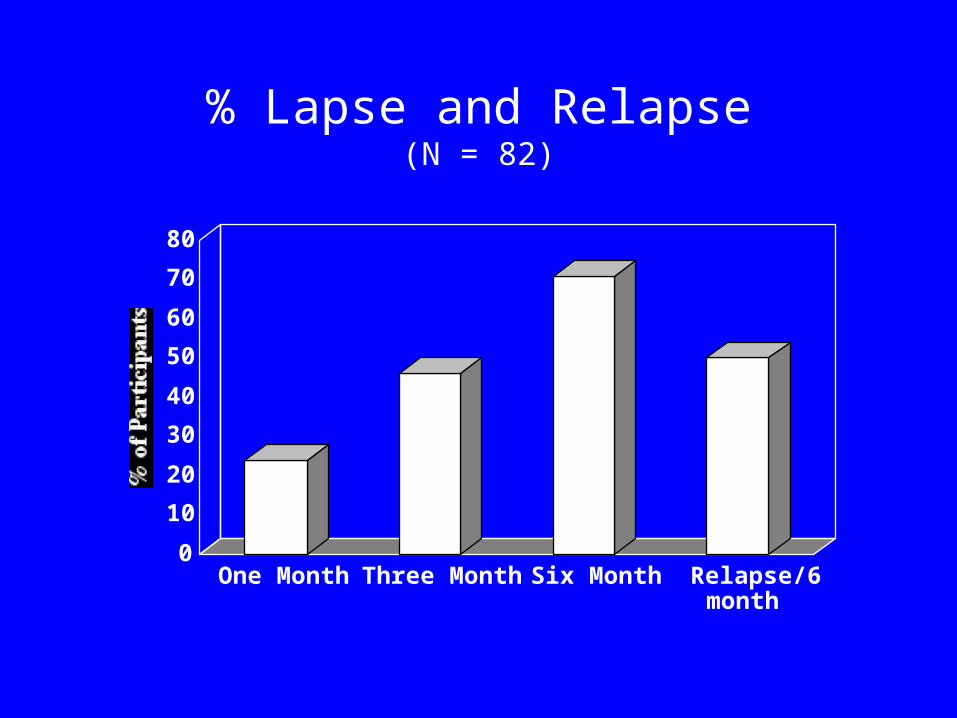
% Lapse and Relapse(N = 82)
0
10
20
30
40
50
60
70
80
One Month Three Month Six Month Relapse/6month
Adolescent Treatment
• Limited support for behavioral and family-based treatments with adolescents
• Only one study specifically focused on marijuana
CYT Adolescent Study
• Evaluate 5 outpt treatments for marijuana abuse• 600 adolescents 83% male 61% white• Age: M=16yrs (13-18yr)• 62% juvenile justice system referrals• Met at least 1 DSM abuse or dependence criteria
and used marijuana in past 90 days
CYT: Marijuana Use
0
10
20
30
40
50
0 3 6 9Months from Intake
MET/CBT5 ACRA MDFT MET/CBT12 MET/CB12+ FSN
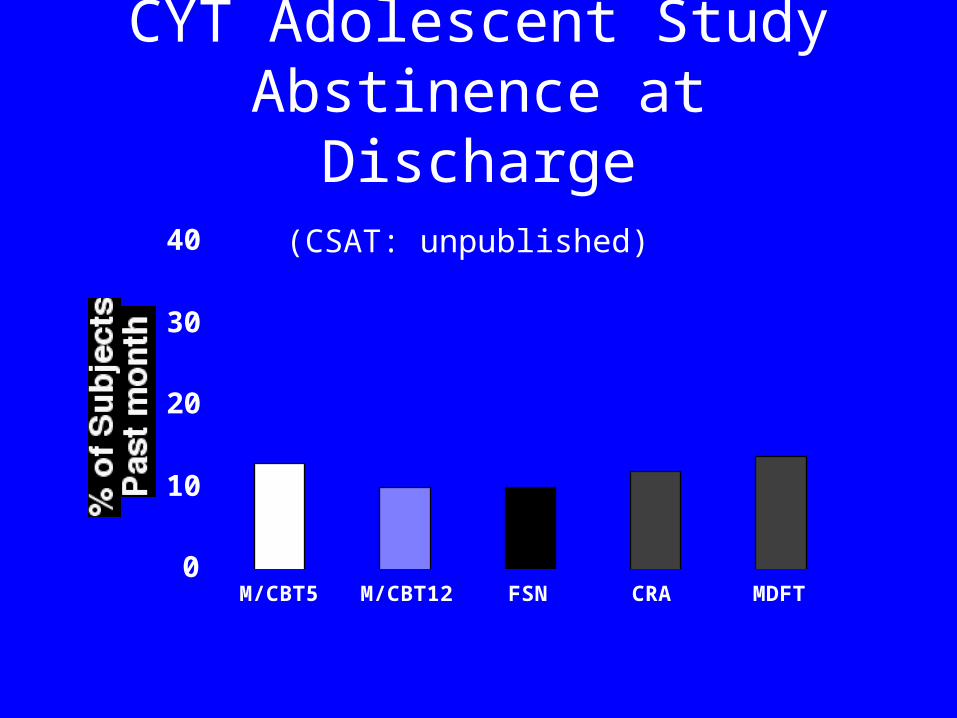
CYT Adolescent StudyAbstinence at Discharge
(CSAT: unpublished)
0
10
20
30
40
M/CBT5 M/CBT12 FSN CRA MDFT

NIDA-Funded Trial
Random assignment to one of two 14-wk treatments
CBT + Contingency Management and Parent Training
(Vouchers, Consequences)
CBT + Family Drug Education
Determine if combination of parent training and vouchers can enhance treatment outcome
Future Directions
• Continue search for more effective treatments
• Combine psychosocial treatments• Medication development
– Substitutes– Antagonists– Target mood
• Combine medication and psychosocial
Thanks to the Staff at the Treatment Research Center
• Heath Rocha Krestin Radonovich• Doris Ogden Pamela Novy• Allyson McGuire Andrea DeCoster• Betsy Bahrenburg Jason Revoir• Katherine Donahue Ann Greer
** John Hughes, Brent Moore, Catherine Stanger, Ryan Vandrey, Stephen Higgins