assessment of hemorrhagic vs ischemic stroke as told by jj baumann ms, rn, cns
TRANSCRIPT
Assessment of Hemorrhagic VS Ischemic Stroke
As told by JJ Baumann MS, RN, CNS
Cerebral Vessel Vignettes

Couple of Clots• 70 year old female• Smoker • Mopping the floor
and started feeling dizzy and tired
• Witnessed sudden onset of aphasia, right sided weakness
12: 15 - last seen normal12:40 - stroke code activated – pre hospital
EMS states right side weakness12:45 - Handsome paramedic arrives with
patient who only has a right facial droop
Time to relax?
A. Don’t cancel stroke code. Let’s give tPA.B. Cancel stroke code, but still get imaging.C. Scold EMS for not knowing facial droop from
complete weakness.D. Get EMS call back number, the charge nurse
also thinks he is hot.
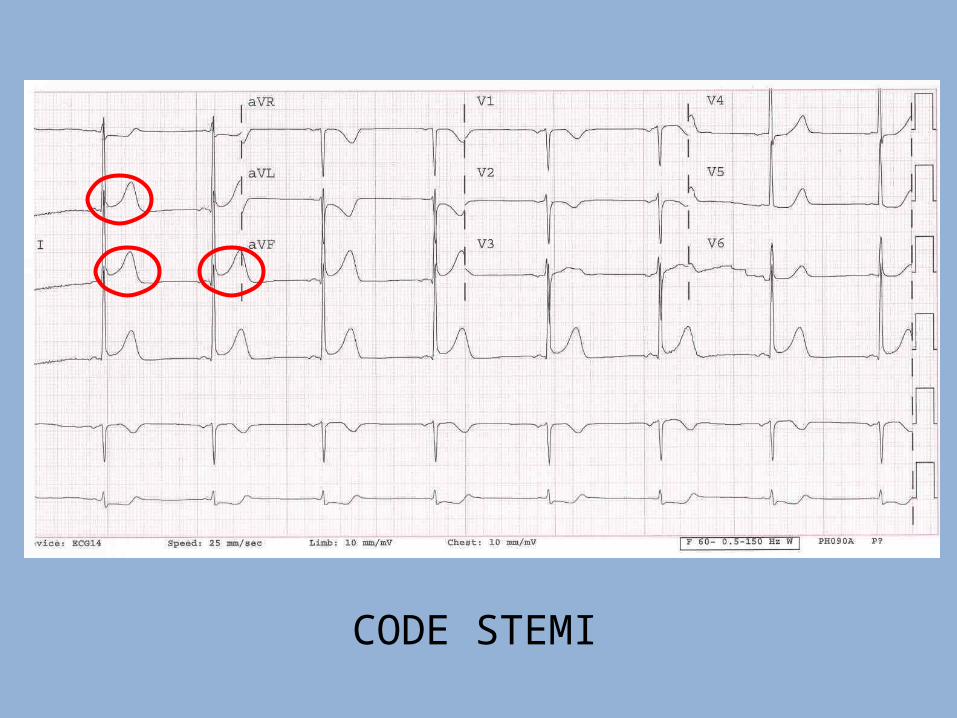
CODE STEMI

Déjà vu
Cardiac cath lab – heart fixed.
On the table, she suddenly stops talking and has right sided weakness.
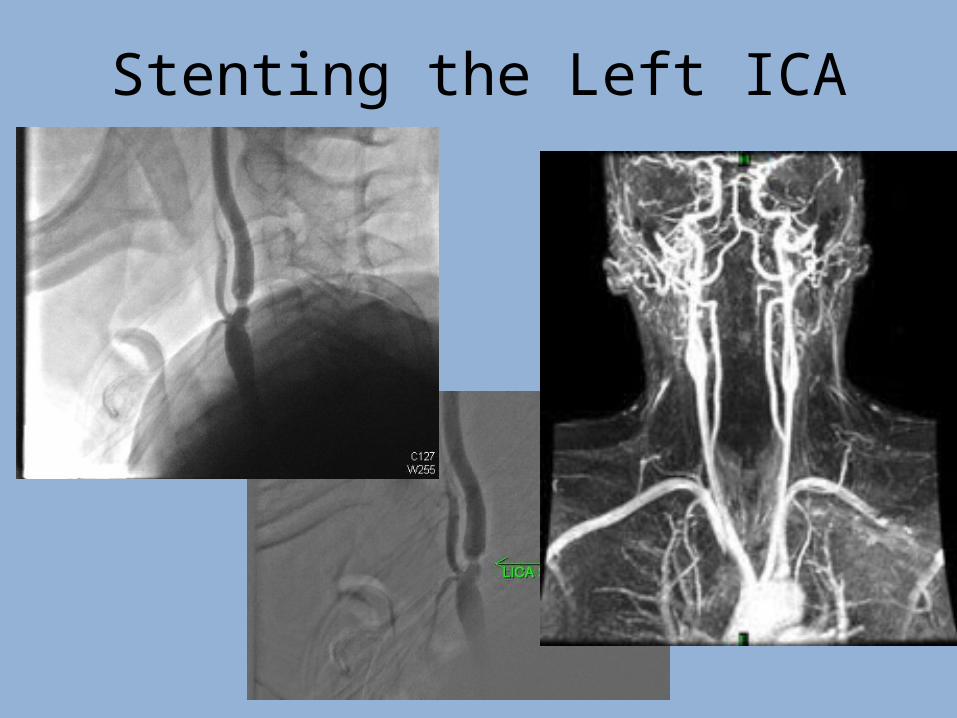
Stenting the Left ICA
48 Hours LaterHer requests:1. Thank paramedic that brought her to the
hospital so quickly2. Let her go home now
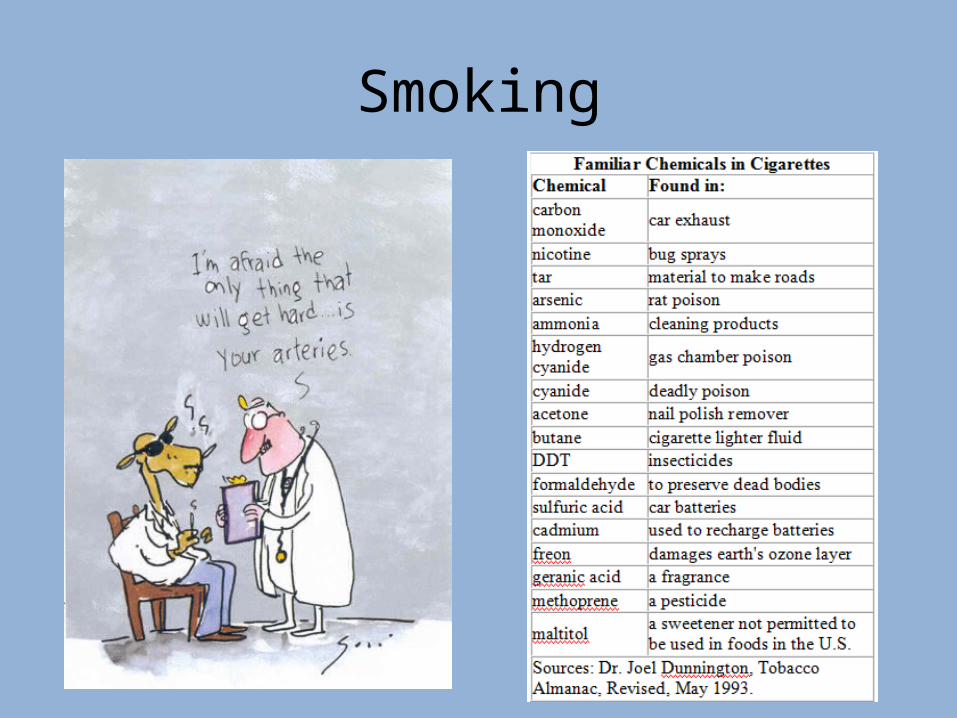
My request:1. Stop smoking!

What is this?
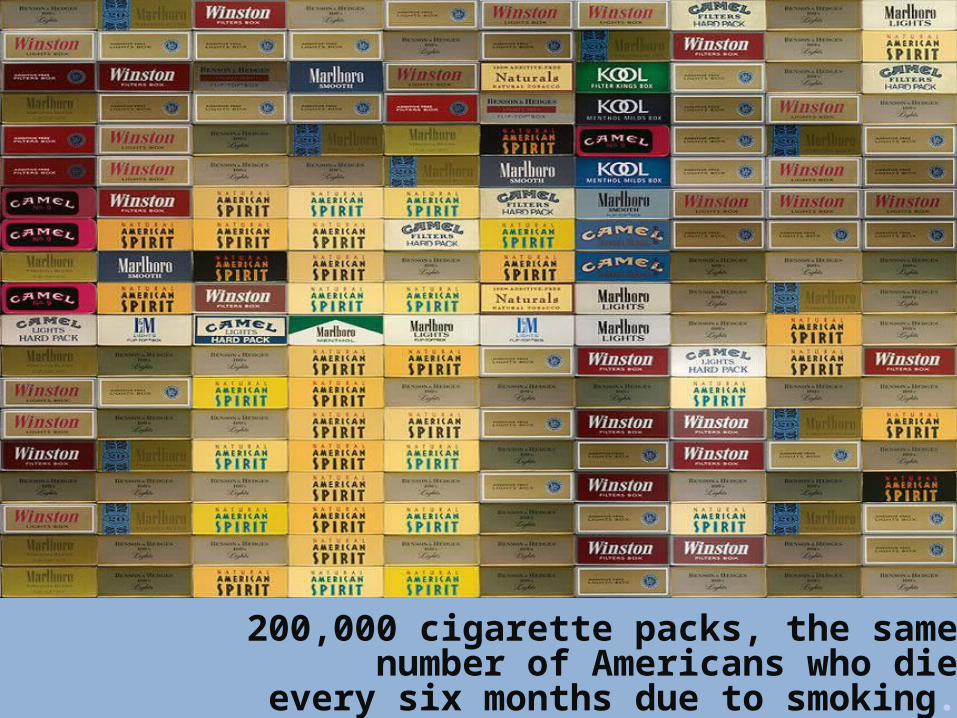
200,000 cigarette packs, the samenumber of Americans who die
every six months due to smoking.
Under Pressure
62 year old malePMHx:
Diabetes Hypertension
Renal issues?Medications:
2 blood pressure medications1 oral antiglycemicaspirin
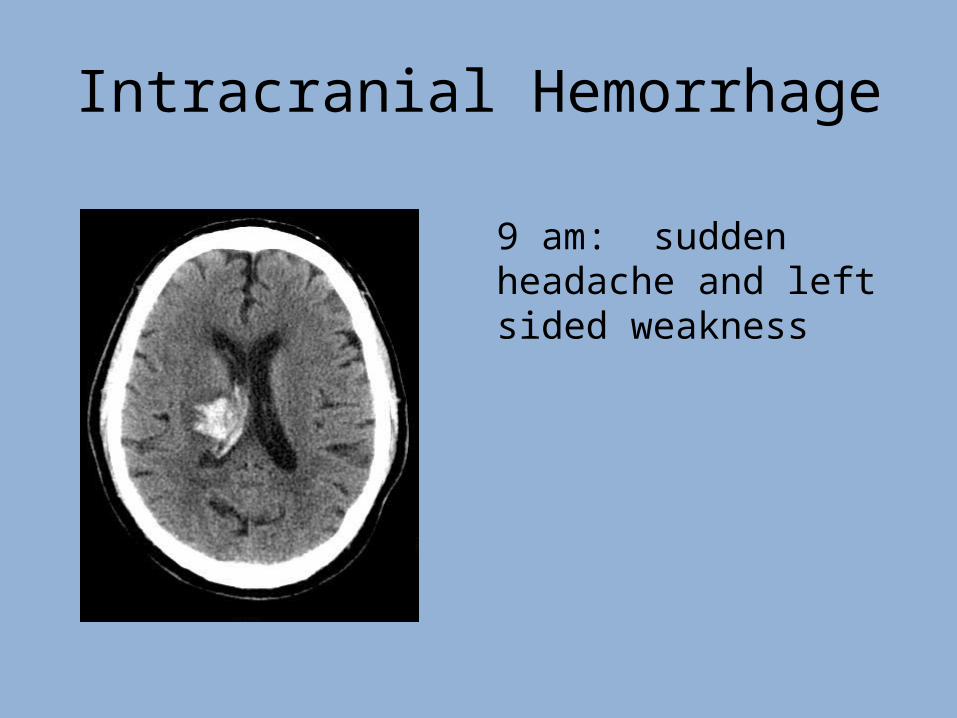
Intracranial Hemorrhage
9 am: sudden headache and left sided weakness
Now what?
A. Get frequent neuro exams?B. Have neurosurgery fix it?C. Stop the bleeding?D. Find the cause?
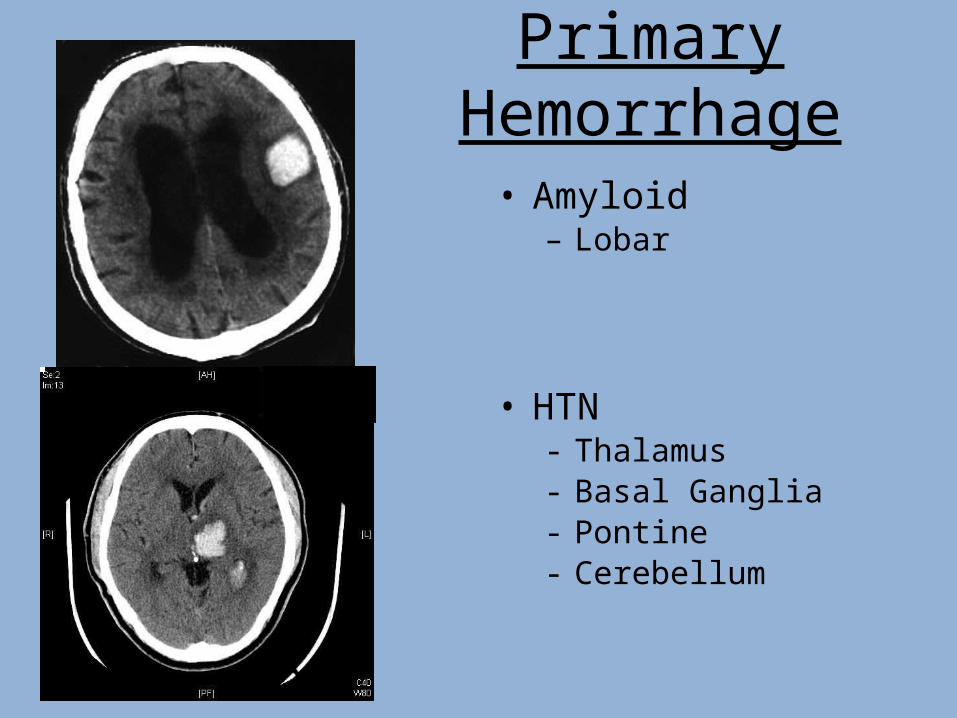
Primary Hemorrhage
• Amyloid– Lobar
• HTN- Thalamus- Basal Ganglia- Pontine- Cerebellum
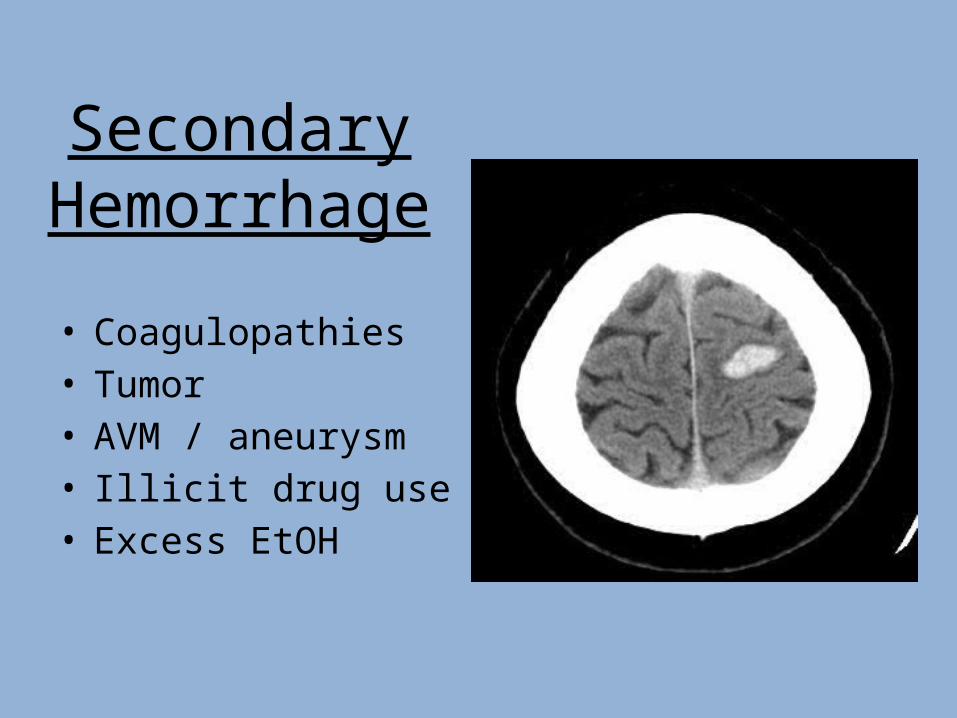
Secondary Hemorrhage
• Coagulopathies• Tumor• AVM / aneurysm• Illicit drug use• Excess EtOH
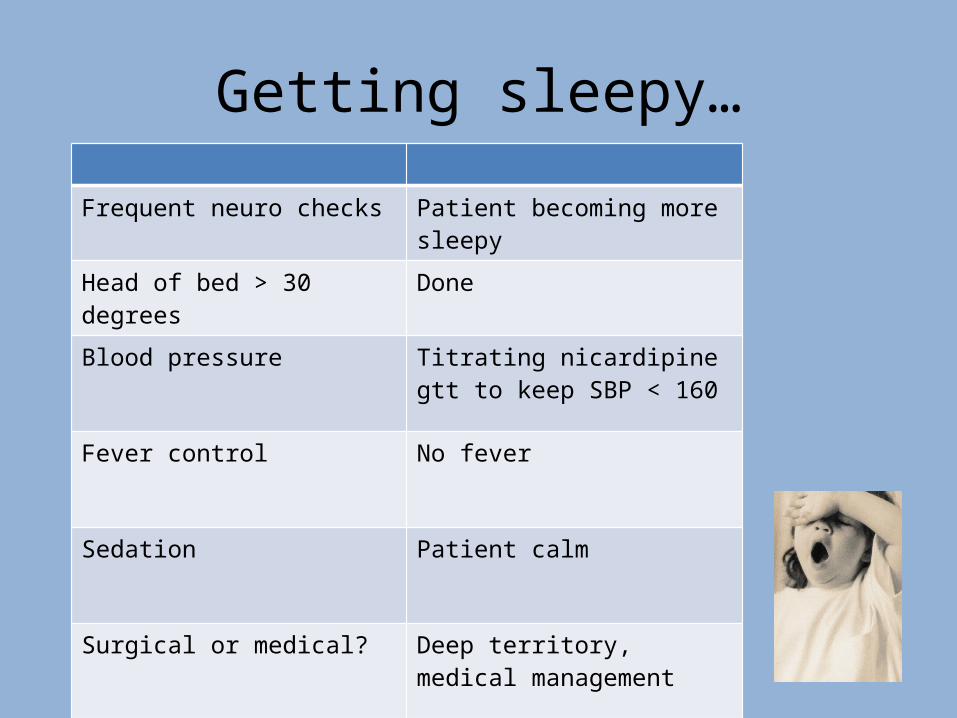
Getting sleepy…
Frequent neuro checks Patient becoming more sleepy
Head of bed > 30 degrees Done
Blood pressure Titrating nicardipine gtt to keep SBP < 160
Fever control No fever
Sedation Patient calm
Surgical or medical? Deep territory, medical management
CT scan
• Bleed is stable• More swelling• Ventricles – no change
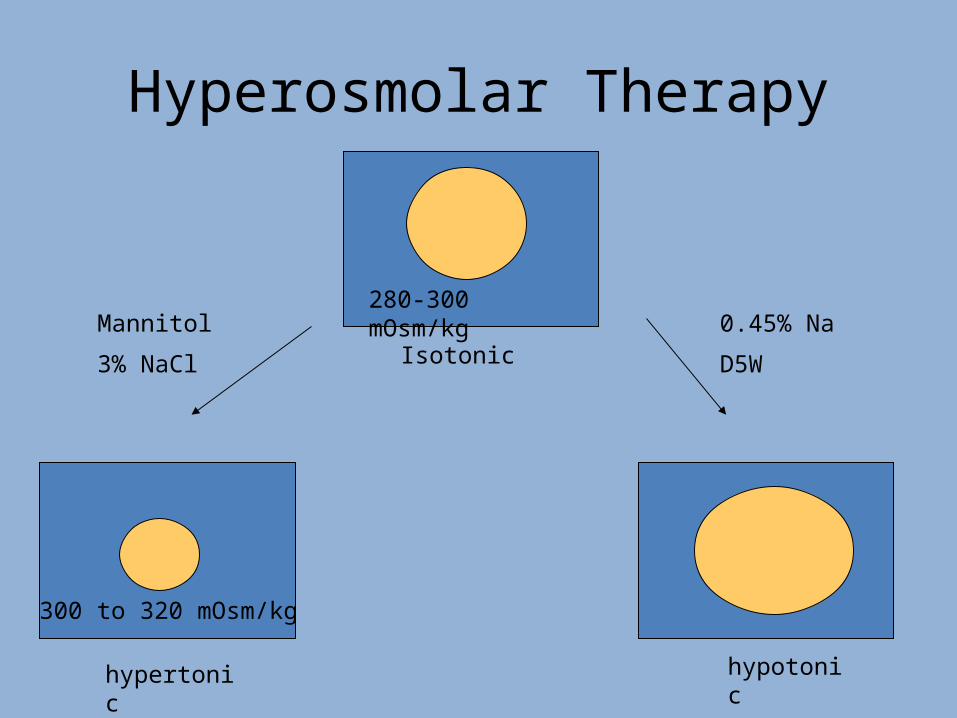
Hyperosmolar Therapy
Isotonic
hypertonic hypotonic
300 to 320 mOsm/kg
280-300 mOsm/kg0.45% Na
D5W
Mannitol
3% NaCl

DO IT FOR THE BRAIN !
• Neuro exam• Blood pressure control• Head of bed• Hyperosmolar therapy• Sedation• Fever control• Prepare for EVD placement
Stroke Code on ortho
• 72 yo male• Hip fx • POD 2• Sudden onset
left facial droop & slurred speech
Increased risk of MI/ PE 1 week after surgery and stroke 1-2 weeks after surgery.
Patient is at increased risk of stroke after surgery if:
They have had a stroke.They have atrial fibrillation.
Risky Business?
• Hypertension• Diabetes – type 2• Overweight• There was something
else, but….
Exacerbation of Old Symptoms
• Metabolic– Electrolytes– Medications– Hypercarbia
• Infectious– WBC– Fever
Exacerbation of stroke symptoms by infection and metabolic perturbations – A diffusion-weighted MRI studyS. Iyadurai, K. Knievel, M. Flaster (St. Louis, Phoenix, Las Vegas, US)
If a Tree Falls in the Forest…87 year old female
EMS: Trauma! AMS following a non-witnessed fall at about 7 pm
Family: Patient got up to get ready for bed. There was a loud thud in the bedroom, and she was found "down" by her vanity table gripping tightly unto her walker and chair and "shaking."
Trauma Team: She sustained multiple lacerations, the worst of which is on her R forearm.
Medications
• diltiazem (CARDIZEM CD) 120 mg sustained release capsule
• losartan (COZAAR) 25 mg tab • furosemide (LASIX) 20 mg tab • pantoprazole (PROTONIX) 40 mg delayed
release tablet • acetaminophen (TYLENOL) 325 mg tab • Multi vitamin
• Paroxysmal AF • CVA with residual R
visual field neglect• High blood pressure• Congestive heart failure• Dementia
Seeing the Trees for the Forest
• Not clear if fall was mechanical
• Fall not witnessed
Pre-syncope? Seizure? TIA?
X-rays, labs, spot EKG, MRI…
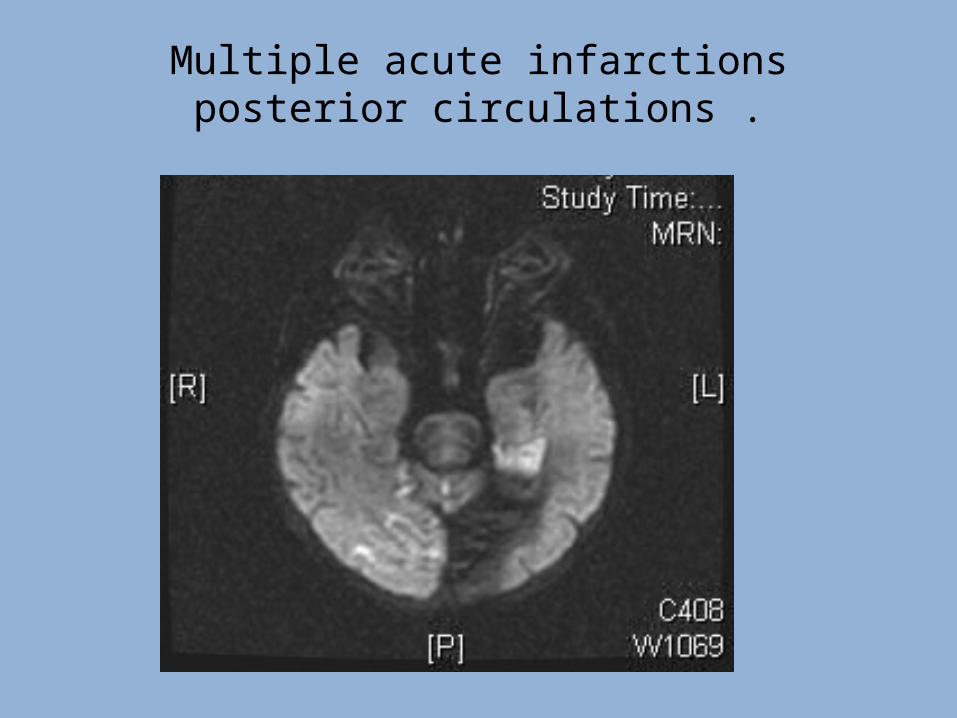
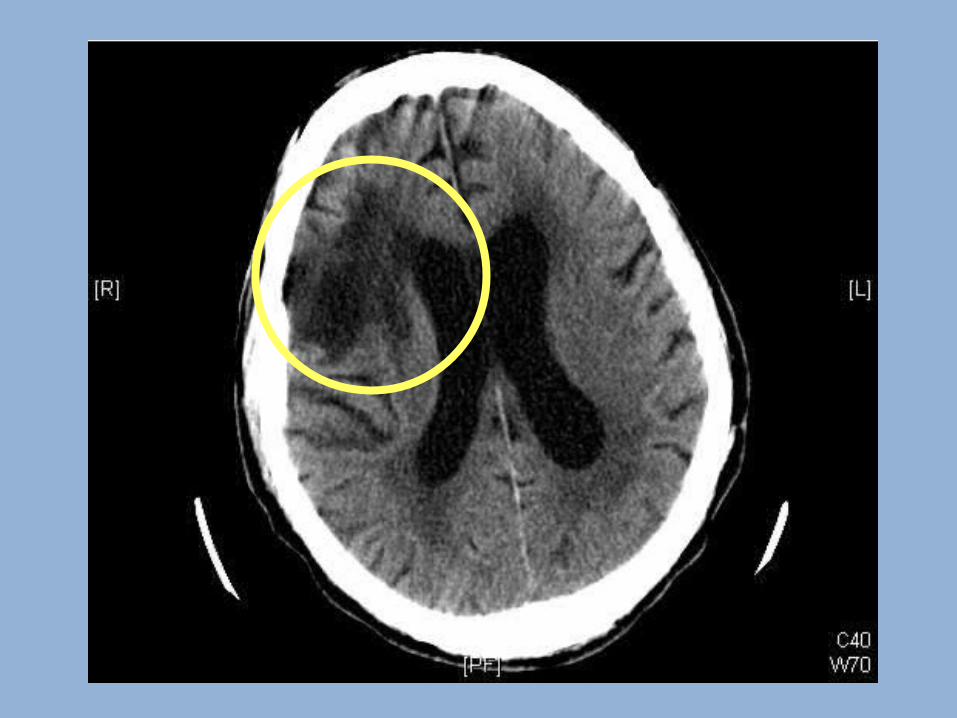
Multiple acute infarctions posterior circulations .
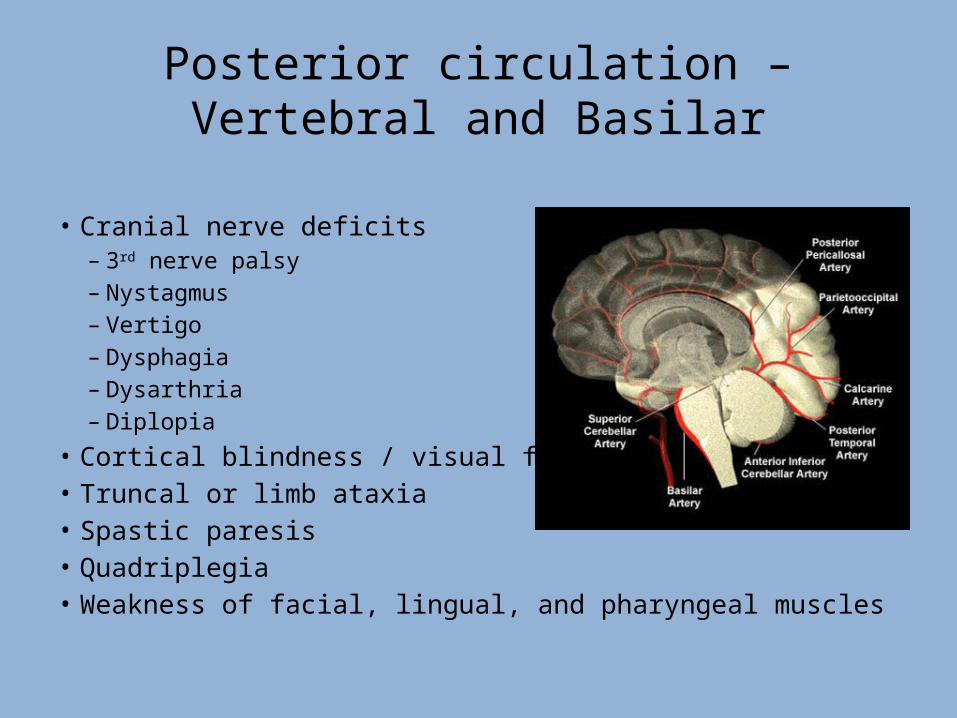
Posterior circulation – Vertebral and Basilar
• Cranial nerve deficits – 3rd nerve palsy– Nystagmus– Vertigo– Dysphagia– Dysarthria– Diplopia
• Cortical blindness / visual field loss• Truncal or limb ataxia• Spastic paresis• Quadriplegia• Weakness of facial, lingual, and pharyngeal muscles

Now what?
Acute treatment?- tPA- NIR
Prevention? - ASA- Plavix / Aggrenox- Coumadin / Pradaxa
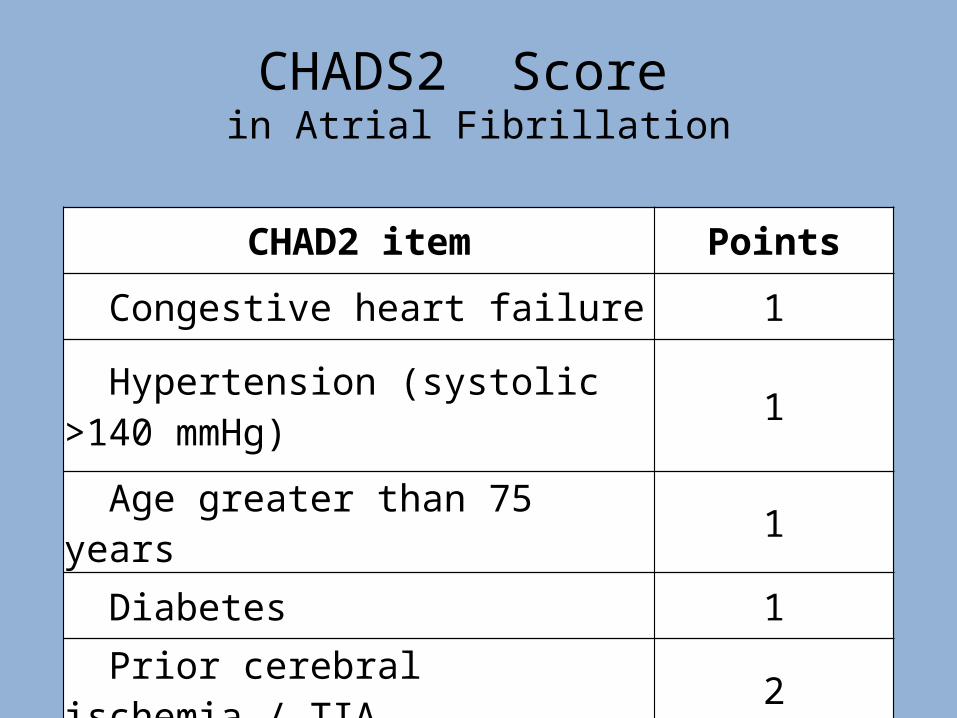
CHADS2 Score in Atrial Fibrillation
CHAD2 item Points
Congestive heart failure 1
Hypertension (systolic >140 mmHg) 1
Age greater than 75 years 1
Diabetes 1
Prior cerebral ischemia / TIA 2
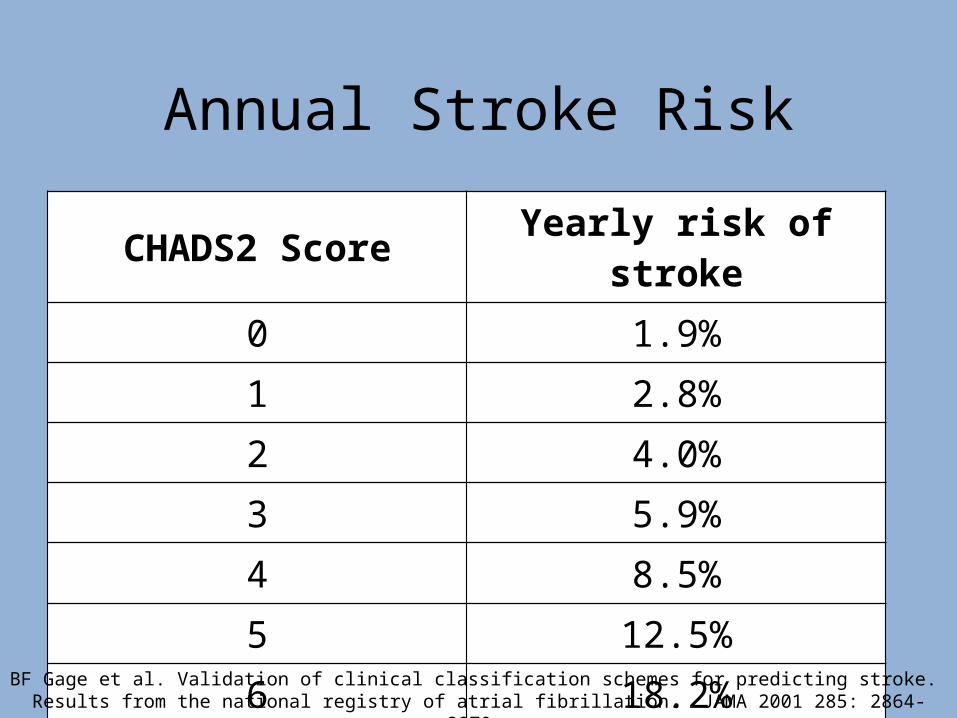
Annual Stroke Risk
CHADS2 Score Yearly risk of stroke
0 1.9%1 2.8%2 4.0%3 5.9%4 8.5%5 12.5%6 18.2%
BF Gage et al. Validation of clinical classification schemes for predicting stroke. Results from the national registry of atrial fibrillation. JAMA 2001 285: 2864-2870.
Balancing Act
CHADS Score is 5, 12.5% chance per year will have a stroke
Two GI Bleeds requiring hospitalization in past 3 months

Grandma
82 year-old woman who lives with her daughter’s family. She needs help with groceries and preparing meals, but she
is otherwise independent and enjoys life. Grandkids love her.
Treat?
1:45 pm Unable to talk, right
hemi
(NIH – 22)2:30 pm
EMS arrivesStroke Code
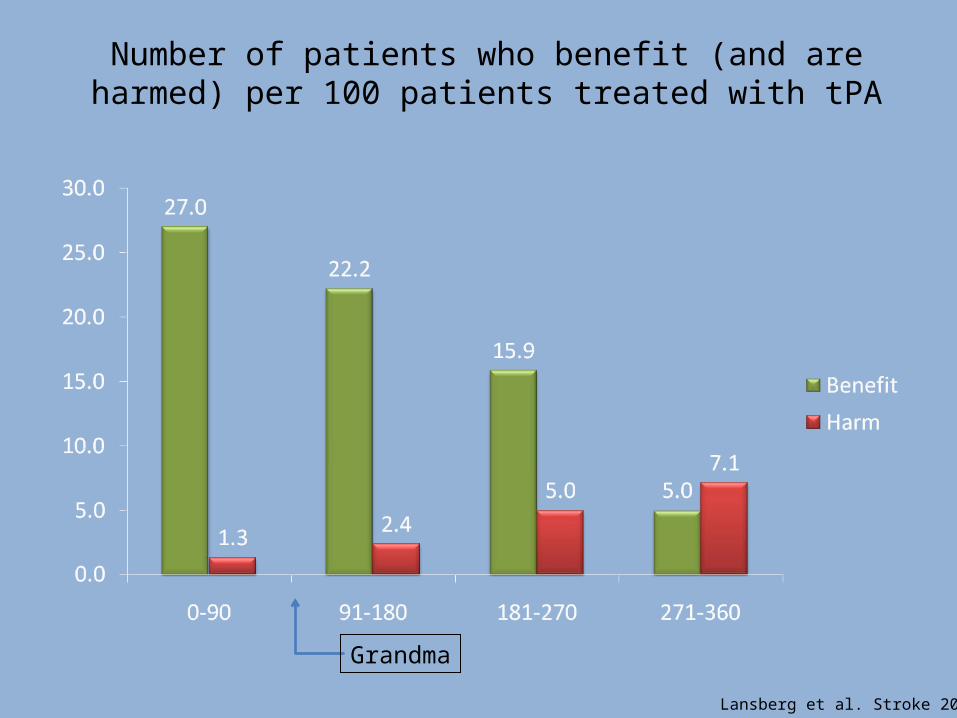
Number of patients who benefit (and are harmed) per 100 patients treated with tPA
Lansberg et al. Stroke 2009
Grandma
4:13 pm: tPA complete!
Why has she not improved?Cath lab? Completed her stroke?tPA did not work?
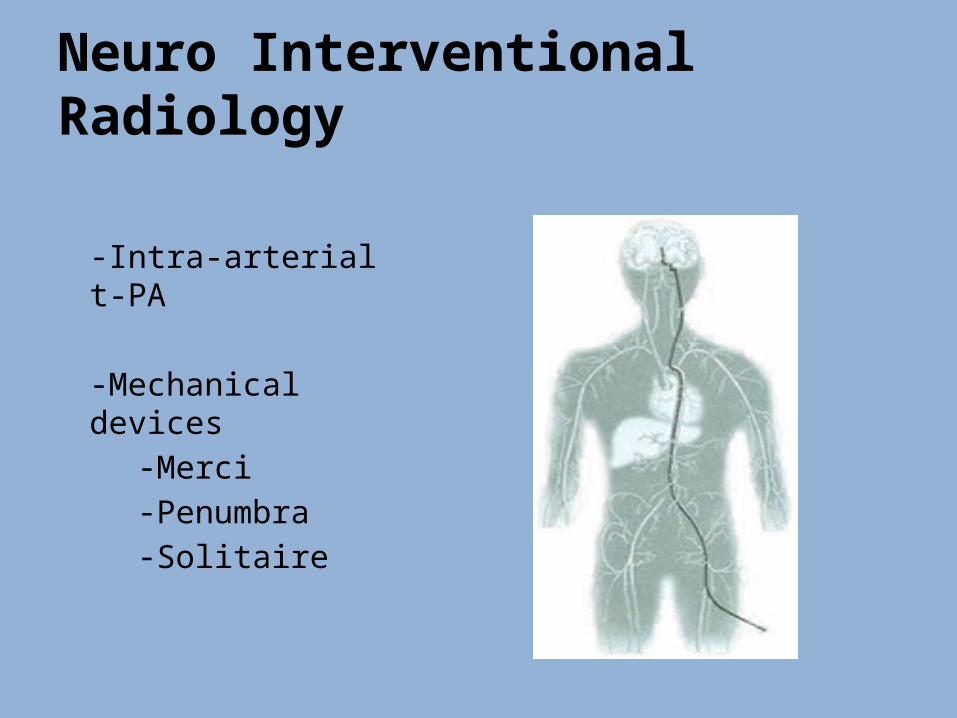
Neuro Interventional Radiology
-Intra-arterial t-PA
-Mechanical devices-Merci-Penumbra-Solitaire
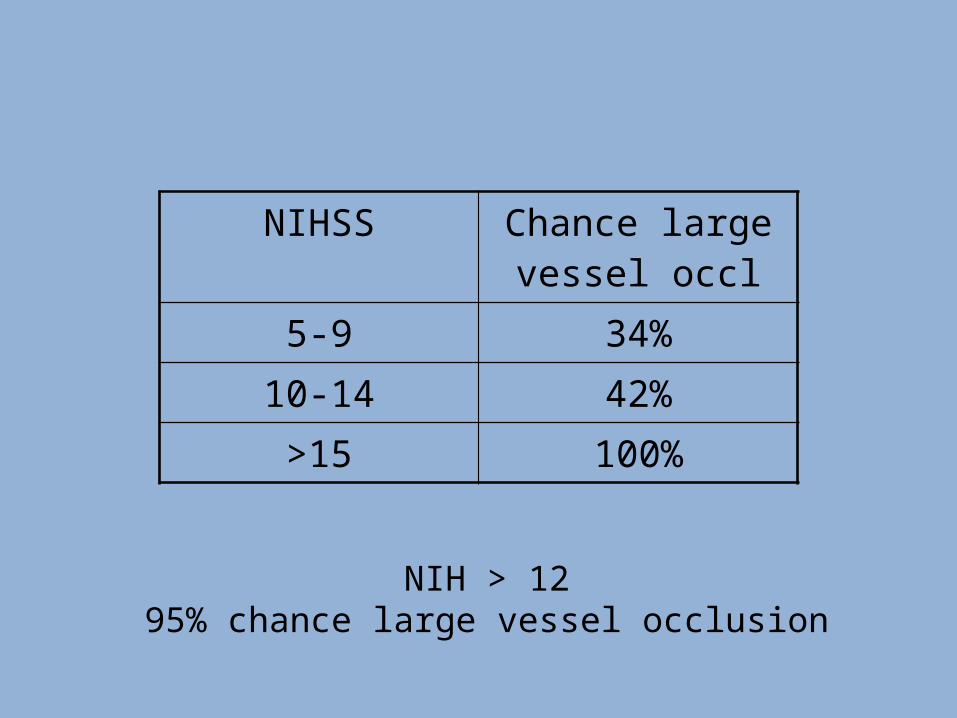
NIH > 1295% chance large vessel occlusion
NIHSS Chance large vessel occl
5-9 34%
10-14 42%
>15 100%
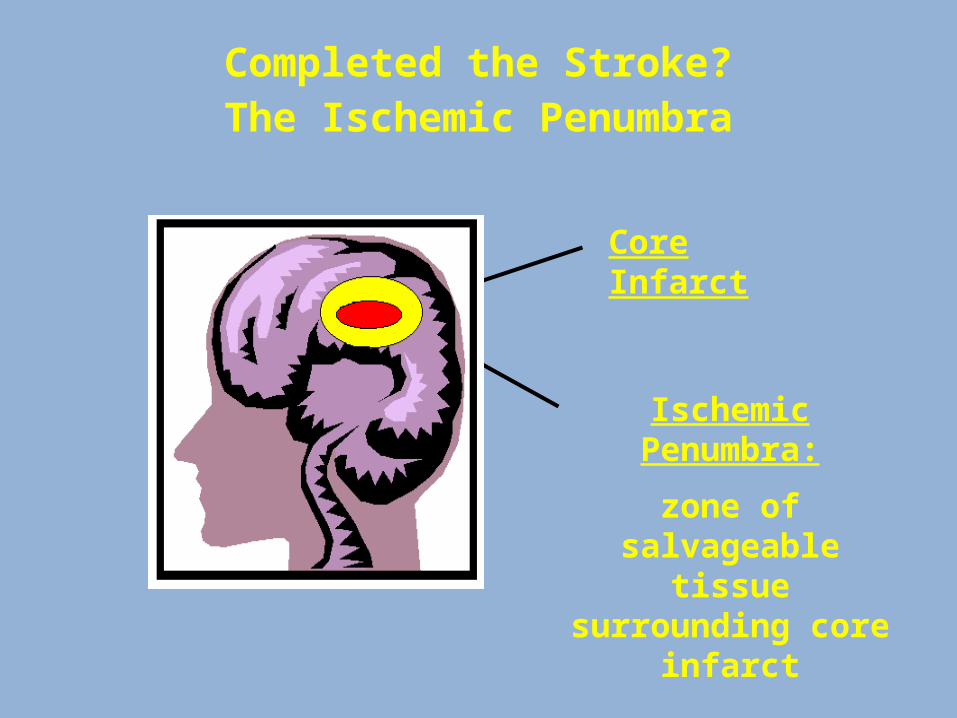
Completed the Stroke?The Ischemic Penumbra
Core Infarct
Ischemic Penumbra:
zone of salvageable tissue surrounding
core infarct
Mean MTT 8 Mean XE-CT CBF 15 Mean Tmax 4s
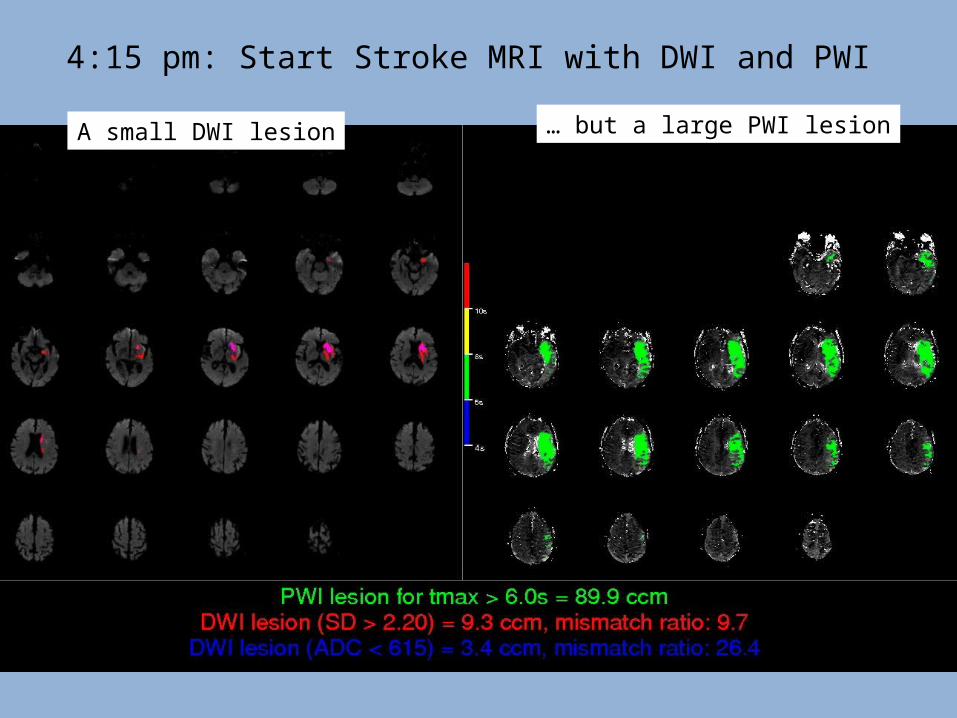
4:15 pm: Start Stroke MRI with DWI and PWI
A small DWI lesion … but a large PWI lesion

4:46 pm: Case start 5:38 pm: The vessel is open
Before Therapy After TherapyCourtesy of Maarten Lansberg, MD
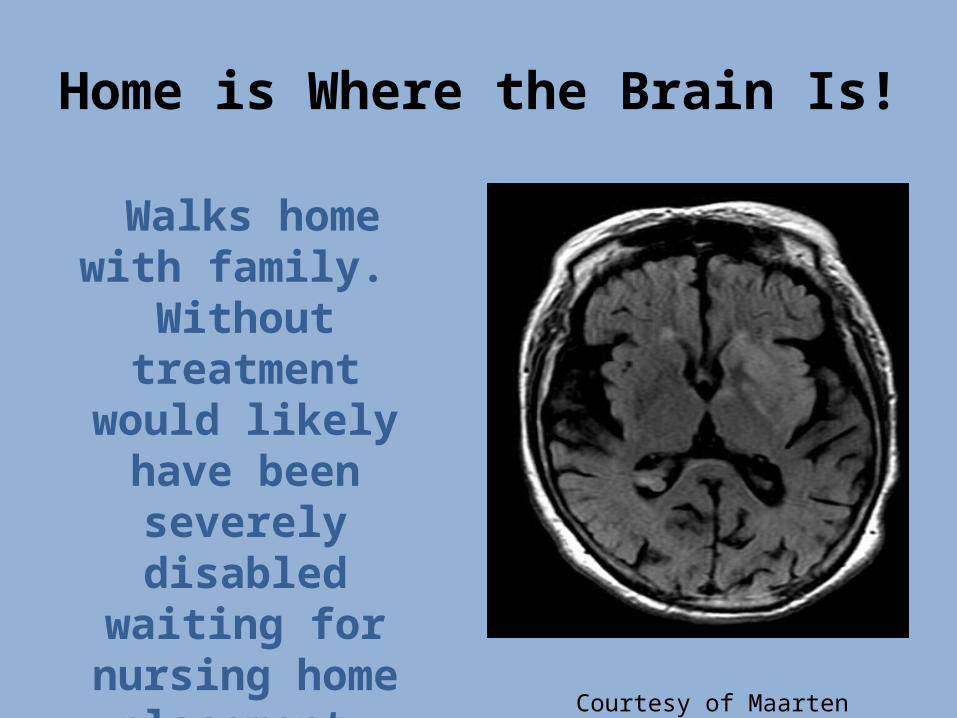
Home is Where the Brain Is!
Walks home with family. Without treatment would likely have been
severely disabled waiting for nursing home placement.
Courtesy of Maarten Lansberg, MD
Questions?