annandale public schools january 1, 2020 health …...january 1, 2020 health insurance renewal...
TRANSCRIPT

Annandale Public Schools
January 1, 2020 Health Insurance Renewal Analysis
November 1, 2019
Mark Beltz, cpa (651) 480-1501

Annandale Public School District 876 2020 Health Insurance Rates
6) == Fsr H s-; f/CII/ '"' -s: .. , f< 'l',v I; 10 (J..J _1e-+-1*)... CfS".(" ,11\.f.o Y"(/~ H~A- s'"''! ~cciJ.;..._.f- f:/t fk._ y~r. per H:1t.. h ... / y•v p~., to J.~ j.ef 10
~ tt {o yIN' S 4 v:j s o..e6-lf1Jtf;-
Q) p-.r I{ S.# f '·~) "~ r .... : '7 y-~ f( ,; D .... I s~-+ ~ .)(,'{ ~II\{. y~.,, HsA- ~ct..,)~,.r IA~eov"'-f; 'f:,r
f-IJ !. Pt~"'-, \j , v f "'/ ~ & ;tS. g, rr ~ h'l~~ +t... ~k·'c.~ fcfa(s 1t,,'3Jo P,/ +k7ec.£,

@ Annandale Public School District 876
2019 Health Insurance Rates

innesota Public Employees Insurance Program (PEIP) M. A dvantage Health Plan 2020- 2021 Benefits Schedule- HSA Compatible
Benefit Provision Cost Level1- You Pay Cost Level2- You Pay A. Preventive Care ~ervices • Routin~ medical ell:ams, cancer screening • Child lre'alth preventive services, routine Nothing Nothing
immunizations • Prenatal and postnatal care and exams ¥ ( uff<-1.._, • Adult immunizations • Routine eve and hearinQ exams B. Annual First Dollar Deductible * $1,500 $2,000
Combined Medical/Pharmacy (single coverage)
Combined Medical/Pharmacy (family coverage) ~800 per family member $3,200 per family member $3,000 per family $4,000 per family
C. Office visits for Illness/Injury, for Outpatient 4 Physical, Occupational or Speech Therapy, ~~~oa and Urgent Care
• Outpatient visits in a physician's office $45 capay per visit $55 capay per visit • Chiropractic services annual deductible applies annual deductible applies • Outpatient mental health and chemical
~~D f~o dependency • Urqent Care clinic visits (in & out of network) D. Network Convenience Clinics & Online Care $0 capay $0 capay
annual deductible applies annual deductible applies E. Emergency Care (in or out of network) $150 capay $150 capay • Emergency care received in a hospital
emergency room annual deductible applies annual deductible applies
F.lnpatient Hospital Copay $400 capay $650 capay annual deductible applies annual deductible applies
G. Outpatient Surgery Copay $250 capay $400 capay annual deductible applies annual deductible applies
H. Hospice and Skilled Nursing Facility Nothing after Nothing after annual deductible annual deductible
I. Prosthetics and Durable Medical 20% coinsurance 25% coinsurance Equipment annual deductible applies annual deductible applies
J. Lab (including allergy shots), Pathology, and X-ray (not included as part of preventive 20% coinsurance 25% coinsurance care and not subject to office visit or facility annual deductible applies annual deductible applies copayments)
K. MRI/CT Scans 20% coinsurance 25% coinsurance annual deductible applies annual deductible applies
L. Other expenses not covered in A- K above, including but not limited to:
• Ambulance • Home Health Care • Outpatient Hospital Services (non-surgical) 20% coinsurance 25% coinsurance • Radiation/chemotherapy
annual deductible applies annual deductible applies • Dialysis • Day treatment for mental health and
chemical dependency • Other diagnostic or treatment related
outpatient services M. Prescription Drugs $30 tier one r .2 "" $30 tier one fJ 9 S'"
30-day supply of Tier 1, Tier 2, or Tier 3 $50 tier two .:f ~ 0 $50 tier two +1 0 prescription drugs, including insulin; or a $75 tier three t (e. ~ $7 5 tier three C. ~ 3-cycle supply of oral contraceptives. annual deductible applies annual deductible applies
N. Plan Maximum Out-of-Pocket Expense•• $3,000 $3,000 (including prescription drugs) Single Coverage
Family Coverage $5,000 per family member $5,000 per family member
$6,000 per family $6,000 per family
(!~i) ~
Cost Level3- You Pay Cost Level4- You Pay
Nothing Nothing
' lc.:C:Fck••t ' - 'teo.r , "" '"" ~).::1-3,"' I v ' ~-~~ ( D<;,f /'f!:vt/
$3,000 $4,0~ $4,800 per family member $6,400 per family member
$6,000 per family $8,000 per family
$105 capay per visit $130 capay per visit annual deductible applies annual deductible applies
f/oo ~ /9.-D
$0 capay $0 capay annual deductible applies annual deductible applies
$150 capay 50% coinsurance annual deductible applies annual deductible applies
$1,500 co pay 50% coinsurance annual deductible applies annual deductible aQ!Jiies $800 capay 50% coinsurance annual deductible applies annual deductible applies Nothing after Nothing after annual deductible annual deductible 30% coinsurance 50% coinsurance annual deductible applies annual deductible applies
30% coinsurance 50% coinsurance annual deductible applies annual deductible applies
30% coinsurance 50% coinsurance annual deductible applies annual deductible applies
30% coinsurance 50% coinsurance annual deductible applies annual deductible applies
$30 tier one ! ::l r $30 tier one ~ :;) (' $50 tier two f Lf l) $50 tier two ~ ~ 0 $75 tier three ... (,;f $75 tier three 4 (:. .(" annual deductible applies annual deductible applies
$4,000 $5,000
r,t~6,900 per family member ~ ~~li$8,000 per family
,900 per family member $10,000 per family
Emergency care or urgent care at a hospital emergency room or urgent care center out of the plan's seiVICe area or out of network IS covered as descnbed m sect1ons C and E above. 1fl,1 Q S' O
This chart applies only to in-network coverage. Point of Se/Vice coverage is available only to members whose permanent residence is both outside the State of Minnesota and the Advantage Plan's seNice area. This category includes employees temporarily residing outside Minnesota on temporary assignment or paid leave pncluding sabbatical/eaves] and college students. It is also available to dependent children and spouses permanently residing outside these/Vice area. Members pay a $1,500 single or $3,000 family deducfible (separate and distinct from the deductibles listed in section 8 above) and 30% coinsurance that will apply to the out-of-pocket maximums described in section N above. Members pay the drug copayment described at section M above to the out-of-pocket maximum described at secffon N. This benefit must be requested.
The PE/P Advantage Plans offer a standani set of benefits regardless of the selected carrier. There are some differences in the way each carrier administers the benefits, including the transplant benefits, in the referral and diagnosis coding patterns of primary care clinics, and in the definition of Allowed Amount.
*The family Deductible is the maximum amount that a family has to pay in deductible expenses in any one calendar year. The family Deductible is not the amount of expenses a family must incur before any family member can receive benefits. Individual family members only need to satisfy their individual deductible once to be eligible for benefits. Once the family Deductible has been met, deductible expenses for the family are waived for the balance of the year.
"The family Out-of-Pocket Maximum is the maximum amount that a family has to pay in any one calendar year. The per-family member embedded Out-of-Pocket Maximum is the maximum amount that a family has to pay in any one calendar year on behalf of any individual family member.
08/19
~

3 innesota Public Employees Insurance Program (PEIP) M
A
~~pz.~ 4'<"\ )
dvantage Health Plan 2020- 2021 Benefits Schedule -Benefit Provision Cost Level1 -You Pay Cost Level2- You Pa_y Cost LeveiJ- You Pay Cost Level 4 -You Pay A. Preventive Care Services • Routine medical exams, cancer screening • Child health preventive services, routine Nothing Nothing Nothing
riF~t:y) immunizations ~ C'utf-.oAt " ' lc-• Prenatal and postnatal care and exams year , "' '"'
• Adult immunizations (es f kvP/ .?1'3 .,,/.., "'7~ • Routine eve and hearinq exams B. Annual First Dollar Deductible *
... $250 /50J J400~00/. I; $750 /1 ,5~~ I
(single/family) )1 ,500 I 3,0~0 r~n I"'~ r ..... -·
C. Office visits for Illness/Injury, for Outpatient rJ~Vj3D0 -"f..> -- 1fJ. - ., .,~..,, -, ... Physical, Occupational or Speech Therapy, and Urgent Care
$30 copay per visit • Outpatient visits in a physician's office $35 copay per visit $65 co pay per visit $85 copay per visit • Chiropractic services annual deductible applies annual deductible applies annual deductible applies annual deductible applies • Outpatient mental health and chemical t)s- ~3D ~ ft,o ~eo dependency • Urgent Care clinic visits (in & out of network) D. Network Convenience Clinics & Online Care Nothinq Nothinq Nothinq Nothing E. Emergency Care (in or out of network)
$100 copay $100 copay $100 copay 25% coinsurance • Emergency care received in a hospital emerqency room annual deductible applies annual deductible applies annual deductible applies annual deductible applies
F. Inpatient Hospital Copay $100 copay $200 copay $500 ,copay 25% coinsurance annual deductible applies annual deductible agplies annual deductible applies annual deductible applies
G. Outpatient Surgery Copay $60 copay $120 copay $250 copay 25% coinsurance annual deductible applies annual deductible applies annual deductible applies annual deductible applies
H. Hospice and Skilled Nursing Facility Nothinq Nothinq NothinQ Nothino I. Prosthetics and Durable Medical
20% coinsurance 20% coinsurance 20% coinsurance 25% coinsurance
Equipment annual deductible applies J. Lab (including allergy shots), Pathology,
and X-ray (not included as part of preventive 10% coinsurance 10% coinsurance 20% coinsurance 25% coinsurance care and not subject to office visit or facility annual deductible applies annual deductible applies annual deductible applies annual deductible applies copayments) ~% s-9o
K. MRI/CT Scans ( p 10% coinsurance ( ~ 15% coinsurance ( ~5% coinsurance ; ~ ~ 30% coinsurance
annual deductible applies annual deductible applies annual deductible applies annual deductible applies L. Other expenses not covered in A- K ...__..s,.~ ............ /0~ '?"'~ ~'--~s~
above, including but not limited to: • Ambulance • Home Health Care • Outpatient Hospital Services (non-surgical) 5% coinsurance 5% coinsurance 20% coinsurance 25% coinsurance • Radiation/chemotherapy
annual deductible applies annual deductible applies annual deductible applies annual deductible applies • Dialysis • Day treatment for mental health and
chemical dependency • Other diagnostic or treatment related
outpatient services M. Prescription Drugs ~,., $18 tier one J"' $18 tier one I a./ $18 tier one If.,~ $18 tier one 30-day supply of Tier 1, Tier 2, or Tier 3
~s $30 tier two ?~ $30 tier two :>~ $30 tier two ~!15 $30 tier two prescription drugs, including insulin; or a 3-cvcle supply of oral contraceptives. _r;> $55 tier three . ~() $55 tier three ~ s-0 $55 tier three S1J $55 tier three
N. Plan Maximum Out-of-Pocket Expense for Prescription Drugs (excludes PKU & Infertility) 4$1,050/2,po ~ $)a050'i.100 f$1~roo 4 $1~50 ~1100 (single/family) Qcc IL.cE) (}f) lhtUJ )I..IJ21 DO I ~-o
0. Plan Maximum Out-of-Pocket Expense ,
$2,~00 I 4f30 • $~,6~0~·70~ ~~ (excluding prescription drugs) (single/family) !1$1 ,7~0 /3,4JO • L $1 ,7oo 13,jDO 1.. ,.,.,...,. ""' .. . , I .,_ -, ""'""""' '
.,, .,~7ft' \ ,,,.,..,I ;),;,.H'CI ,,- I " Emergency care or urgent care at a hospital emergency room or urgent care center out of the plan's service area or out of network is covered as described in sections C and E above.
This chart applies only to in-network coverage. Point of SeiVice coverage is available only to members whose permanent residence is outside both the State of Minnesota and the Advantage Plan's service area. This categoty includes employees temporarily residing outside Minnesota on temporal}' assignment or paid leave [including sabbatical/eaves] and college students. It is a/so available to dependent children and spouses permanently residing outside the service area. Members enrolled in this categoty pay a $350 single or $700 family deductible (separate and distinct from the deductibles listed in section B above) and 30% coinsurance that will apply to the out-of-pocket maximums described in section 0 above. Members pay the drug copayment described at section M above to the out-of-pocket maximum described at section N. This benefit must be requested.
The PEIP Advantage Plans offer a standard set of benefits regardless of the selected carrier. There are some differences in the way each carrier administers the benefits, including the transplant benefits. in the referral and diagnosis coding patterns of primaty care clinics, and in the definition of Allowed Amount.
• This Plan uses an embedded deductible: If any family member reaches the individual deductible then the deductible is satisfied for that family member. If any combination of family members reaches the family deductible, then the deductible is satisfied for the entire family.
08/19

Step by Step Instructions for Enrollment in the Public Employees Insurance Program Advantage Plan
To help explain your options in the Public Employees Insurance Program, we have created the following guide.
"§><> Step 1- Choose Your Plan level ~
The Public Employees Insurance Program Advantage Plan has cost sharing features that will help you and your employer to better control health care costs while maintaining flexibility in access to doctors and clinics. The Public Employees
(j)surance Program offers three Plan choices:
• Advantage (High) • Value (Medium) • HSA (Low)
Choose the Benefit Level that best fits your needs. The premium and cost sharing will vary based on the Benefit Level you choose. You may change your Benefit Level each year during your group's annual open enrollment.
"§><> Step 2- Choose Your Health Plan/Network ~
The Public Employees Insurance Program offers three different Health Plans/Networks to choose from:
(i;} • HealthPartners • Blue Cross Blue Shield • Preferred One
Choose the network carrier that best fits your needs. Your network selection will not affect the cost of the plan; nor will it affect the premium rate. The benefits are similar under each network (HP includes a benefit for treatment of infertility). You may change your Health Plan/Network level each year during your group's annual renewal.
':9'- Step 3- Choose Your Primary Care Clinic ~
Primary Care Clinics have been placed into one of four cost levels, depending on the care system in which the provider participates and that care system's total cost/quality of delivering health care. The amount of cost sharing that is paid for health care services varies depending upon the cost level of the Health Plan and Network that you choose.
@ • Select a primary care clinic (PCC) for each family member ::l('- '/61) 0" C (,<•je ,..,+J.Iy Each family member must select a primary care clinic (PCC). Family members may choose different PCCs- even in a different cost level, but all family members must enroll with the same Plan Level and Network choice. Your enrollment form should include the primary care clinic# associated with your network carrier.
All primary care clinics are broken into four tier levels that determine the benefits received by that family member. A list of participating clinics is available online to help you make your primary care clinic selection. This list includes your primary care clinic's clinic number that you will need in order to enroll. You can change clinics by calling the phone number on your ID card (changes are effective on the 1st day of the following month).
Most medical care is coordinated through a Primary Care Clinic (PCC) and you will generally need a referral to see a specialist (referrals to a specialist's office will be covered at the same cost level as your PCC). You may self-refer to certain specialists including OBGYN, chiropractors, and mental health/chemical dependency practitioners, providing the practitioner is part of the carrier's self-referral network. No referrals needed for urgent care and emergencies.
A statewide primary care clinic listing and health plan documents, including the Summary Benefit Comparisons (SBC's) for all plan levels, are available online at www.innovomn.com/plan_information.html.
IMPORTANT! Once enrolled. you will receive TWO ID cards. One card will be sent from your health plan (HP, BCBS, POne) which is to be used for medical services. The second card from CVS is to be used for all pharmacy charges. If you have questions please call us at 952.746.3101 or 800.829.5601 or email us at [email protected].
8/17
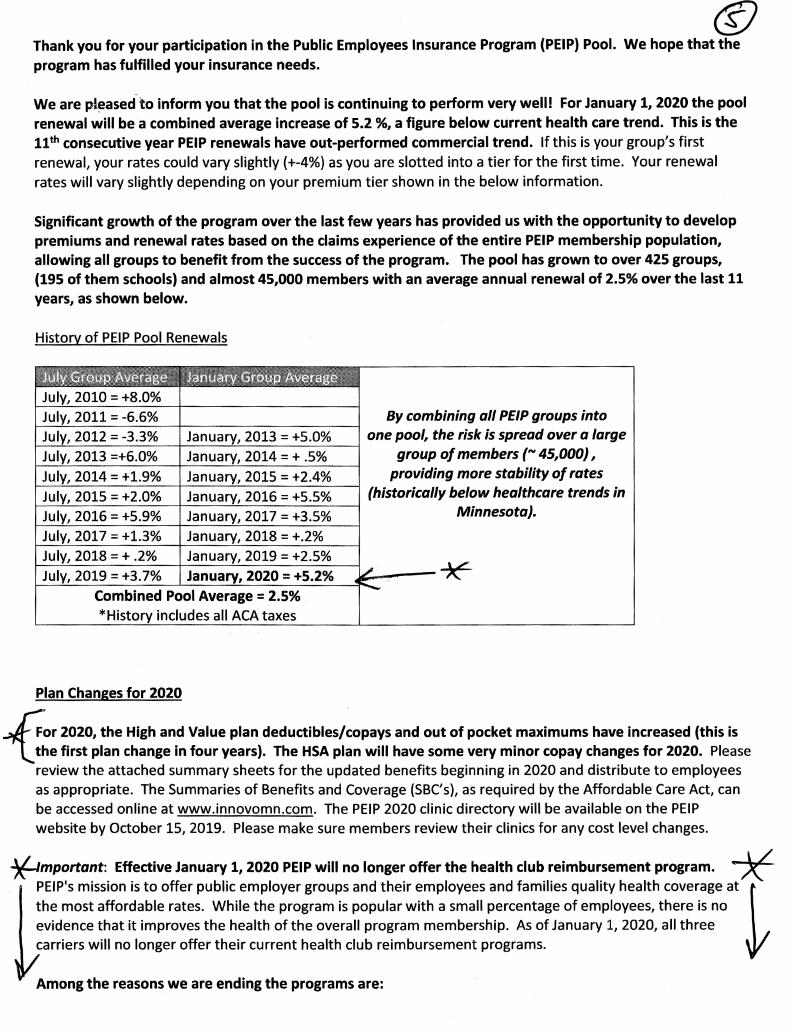
@ Thank you for your participation in the Public Employees Insurance Program (PEIP) Pool. We hope that the program has fulfilled your insurance needs.
We are pieased,to inform you that the pool is continuing to perform very well! For January 1, 2020 the pool renewal will be a combined average increase of 5.2 %, a figure below current health care trend. This is the 11th consecutive year PEIP renewals have out-performed commercial trend. If this is your group's first renewal, your rates could vary slightly (+-4%) as you are slotted into a tier for the first time. Your renewal rates will vary slightly depending on your premium tier shown in the below information.
Significant growth of the program over the last few years has provided us with the opportunity to develop premiums and renewal rates based on the claims experience of the entire PEIP membership population, allowing all groups to benefit from the success of the program. The pool has grown to over 425 groups, (195 of them schools) and almost 45,000 members with an average annual renewal of 2.5% over the last 11 years, as shown below.
History of PEIP Pool Renewals
By combining all PEIP groups into
~~------------~----~--------~~ one pool, the risk is spread over a large
group of members ("' 45,000), providing more stability of rates
2015 = +2.0% 2016 = +5.5% (historically below healthcare trends in ~~-2-0_1_6_=_+_5_.-9°-%--~----~2-0_1_7_=_+_3 ___ 5.:....:%---1 Minnesota).
2017 = +1.3% 2018 = +.2% 2018 = + .2%
Plan Changes for 2020
hor 2020, the High and Value plan deductibles/copays and out of pocket maximums have increased (this is l ~he first plan change in four years). The HSA plan will have some very minor copay changes for 2020. Please review the attached summary sheets for the updated benefits beginning in 2020 and distribute to employees as appropriate. The Summaries of Benefits and Coverage (SBC's), as required by the Affordable Care Act, can be accessed online at www.innovomn.com. The PEIP 2020 clinic directory will be available on the PEIP website by October 15, 2019. Please make sure members review their clinics for any cost level changes.
7{-lmportant: Effective January 1, 2020 PEIP will no longer offer the health club reimbursement program. * PEIP's mission is to offer public employer groups and their employees and families quality health coverage at } the most affordable rates. While the program is popular with a small percentage of employees, there is no evidence that it improves the health of the overall program membership. As of January 1, 2020, all three carriers will no longer offer their current health club reimbursement programs.
Among the reasons we are ending the programs are:

(f) 1. Because Blue Cross is no longer able to offer its fitness center reimbursement program, we would be unable to continue to provide a consistent member experience across all three carriers (HP/BC/Pl). 2. The alt~rnativ-e programs we explored were estimated to cost four to five times more than the fitness center reimbursement programs. 3. Only 9.4% of eligible contract holders received a health club reimbursement during the quarter ending June 30,2019. 4. The IRS ruling that clarified that monetary incentives are taxable has reduced the benefit to the member by about one third. 5. The work required to include the fitness award for tax purposes has placed a large burden on employer groups, the carriers, and PEIP staff.
COMING SOON/I In early 2020 PEIP will offer online enrollment access for all groups. You will receive more information soon about this new administrative tool.
During the next six weeks, your insurance eligible employees will have the opportunity to change health plans and carrier
www.innovomn.com.
networks. Updated plan summaries and an employee Enrollment Form is attached as well as a new Group Application. Forms can also be found on PEIP's website at
Employees and dependents who wish to change health plans or networks must complete an Enrollment Form or the chan e. A rimar care clinic number for each member is re uired. Participants staying with the
same carrier who wish to change their primary care clinic must contact the carrier directly. Primary care clinics can be changed at any time by calling the customer service number on the member's ID card.
All completed Enrollment Forms and any changes to your group's eligibility requirements must be submitted to lnnovo Benefits Administration, PEIP's administrator, by November 12, 2019 (please plan your open enrollment to meet that deadline).
**** Please send forms for those employees making a plan, carrier or family change only. No form is required for those employees maintaining current coverage. *****
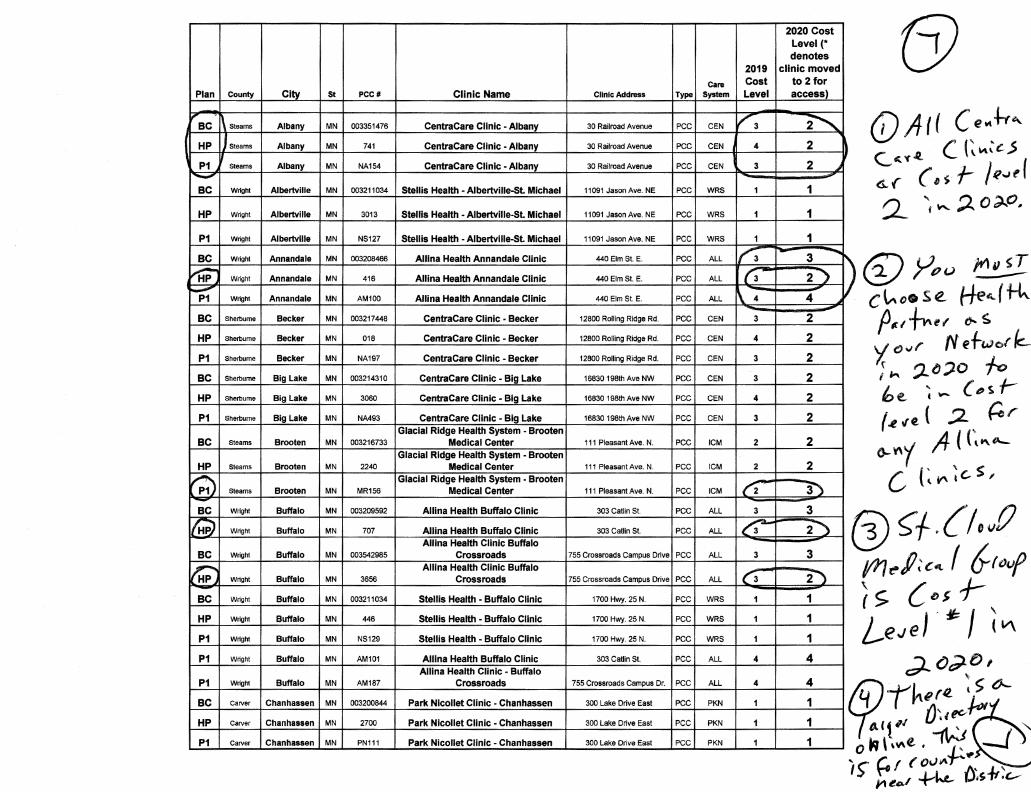
Plan County City St PCCII Clinic Name
BC Steams Albany MN 003351476 CentraCare Clinic - Albany
HP Steams Albany MN 741 CentraCare Clinic -Albany
P1 Steams Albany MN NA154 CentraCare Clinic -Albany -BC Wright Albertville MN 003211034 Stellis Health -Albertville-St. Michael
HP Wnght Albertville MN 3013 Stems Health - Albertville-St Michael
P1 wnght Albertville MN NS127 Stellis Health -Albertville-St. Michael
BC Wright Annandale MN 003208466 Allina Health Annandale Clinic
~ Wright Annandale MN 416 Allina Health Annandale Clinic
P1 wnght Annandale MN AM100 Allina Health Annandale Clinic
BC Sherburne Backer MN 003217448 CentraCare Clinic - Becker
HP Sherburne Becker MN 018 CentraCare Clinic • Becker
P1 Sherburne Becker MN NA197 CentraCare Clinic - Becker
BC Sherburne Big Lake MN 003214310 CentraCare Clinic - Big Lake
HP Sherburne Big lake MN 3060 CentraCare Clinic • Big Lake
P1 Sherburne Big Lake MN NA493 CentraCare Clinic - Big Lake Glacial Ridge Health System - Brooten
BC steams Brooten MN 003216733 Medical Center Glacial Ridge Health System - Brooten
HP Steams Brooten MN 2240 Medical Center
~ Glacial Ridge Health System - Brooten
steams Brooten MN MR156 Medical Center
BC Wnght Buffalo MN 003209592 Allina Health Buffalo Clinic
t.WJ Wright Buffalo MN 707 Allina Health Buffalo Clinic Alllna Health Clinic Buffalo
BC Wnght Buffalo MN 003542985 Crossroads
1;1 Alllna Health Clinic Buffalo Wright Buffalo MN 3656 Crossroads
BC Wright Buffalo MN 003211034 Stellis Health - Buffalo Clinic
HP Wright Buffalo MN 446 Stellis Health • Buffalo Clinic
P1 Wnght Buffalo MN NS129 Stems Health - Buffalo Clinic
P1 Wright Buffalo MN AM101 Allina Health Buffalo Clinic Allina Health Clinic • Buffalo
P1 Wright Buffalo MN AM187 Crossroads
BC Carver Chanhassen MN 003200844 Park Nicollet Clinic - Chanhassen
HP Carver Chanhassen MN 2700 Park Nicollet Clinic - Chanhassen
P1 Carver Chanhassen MN PN111 Park Nicollet Clinic - Chanhassen
2019
Care Cost Clinic Address Type System Level
30 Railroad Avenue PCC CEN v-3
30 Railroad Avenue PCC CEN 4
30 Railroad Avenue PCC CEN 3
11091 Jason Ave. NE PCC WRS 1
11091 Jason Ave. NE PCC WRS 1
11091 Jason Ave. NE PCC WRS 1
440EimSt. E. PCC ALL 1'3
440 Elm St E. PCC ALL (3
440EimSt. E. PCC ALL \ 4
12600 Rolling Ridge Rd. PCC CEN 3
12800 Rolling Ridge Rd. PCC CEN 4
12800 Rolling Ridge Rd. PCC CEN 3
16830 198th Ave NW PCC CEN 3
16830 198th Ave NW PCC CEN 4
16830 198th Ave NW PCC CEN 3
111 Pleasant Ave. N. PCC ICM 2
111 Pleasant Ave. N. PCC ICM 2
111 Pleasant Ave. N. PCC ICM ('2
303Catlin St. PCC ALL 3
303Catlin St PCC ALL c3
755 Crossroads Campus Drive PCC ALL 3
755 Crossroads Campus Drive PCC ALL c3
1700 Hwy. 25 N. PCC WRS 1
1700 Hwy. 25 N. PCC WRS 1
1700 Hwy. 25 N. PCC WRS 1
303 CaUin St PCC ALL 4
755 Crossroads Campus Dr. PCC ALL 4
300 Lake Drive East PCC PKN 1
300 Lake Drive East PCC PKN 1
300 Lake Drive East PCC PKN 1
2020 Cost Level(* denotes
clinic moved to 2 for access)
~ 2 ~
2
1
1
1 - 3 .....
2")
4
2
2
2
2
2
2
2
2
3")
3
2~
3
2~ 1
1
1
4
4
1
1
1
(j) (j)Atl Cet4+r~ c...~ v.t. ( (~ ~:c..s c;.. (" (' s f- / ~..~ e (
2.. ~ "'- :;2.. 0 ~0"
(i) yp u }t1" !I c~o.se. f1e ... (tk p~, ~t( (Jo. s 'f ()vr N ef-,.,or fc_ j k ~lJ~O fo be. ~- c-s f(.e "e. ( :2 Per
G-Y\1 A- ((~~A... c (~"'~e-S,
(i) ~f.{/,,l) mr!'R:c ... I Gr"vf (s. {Dsf-L,e J e J . ~ / ( II\
""') ()~t>, <::?-- ' r ().._ . h (ll t ~ 9?-r oi~ec-~~«
't'' ~ --f. "' ,Y\e. • .P.·
.. o f'.t (ovk... ():s.ft~t:-1) lf'lt!cs.l +-
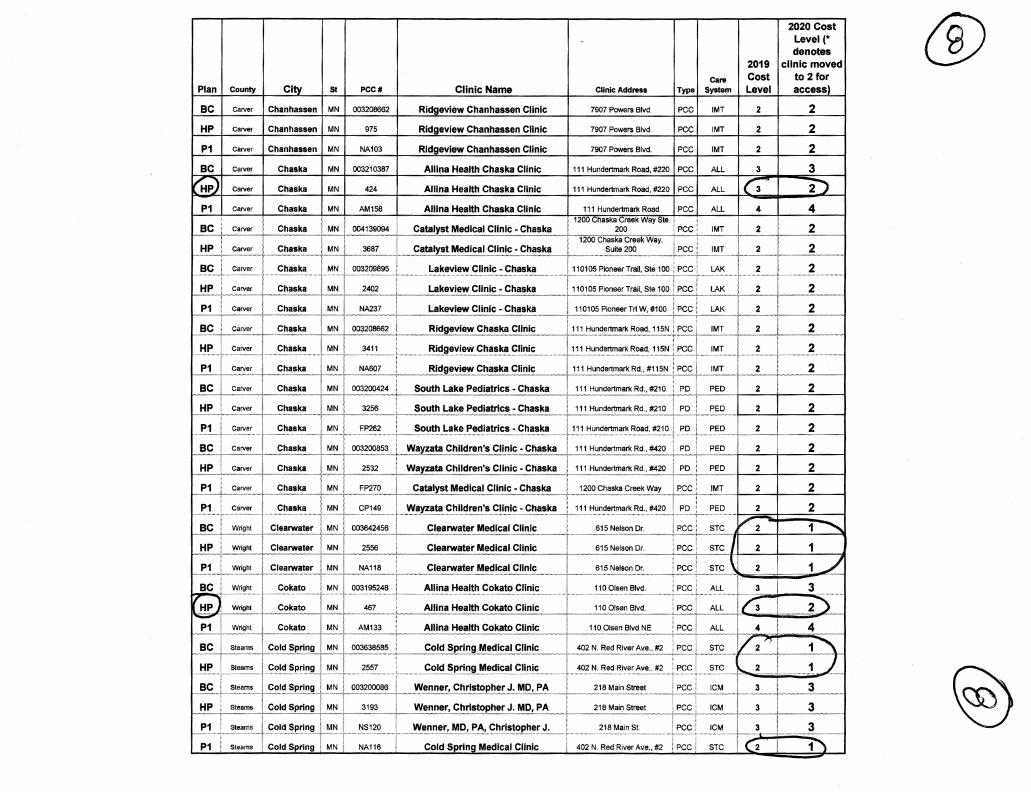
@ 2020 Cost Level(* denotes
2019 clinic moved
Care Cost to 2 for Plan County Citv I St PCC# Clinic Name Clinic Address Type System Level access)
BC Carver Chanhassen I MN 003208662 Ridgeview Chanhassen Clinic 7907 Powers Blvd. PCC IMT 2 2
HP I Carver Chanhassen I MN 975 Ridgeview Chanhassen Clinic 7907 Powers Blvd. PCC IMT 2
~a rver Chanhassen MN NA103 Ridgeview Chanhassen Clinic 7907 Powers Blvd. PCC /MT 2
Carver Chaska MN 003210387 Allina Health Chaska Clinic 111 Hundertmark Road, #220 PCC --Carver Chaska MN 424 Allina Health Chaska Clinic 111 Hundertmark Road, #220 PCC --Carver Chaska MN I AM158 I Allina Health Chaska Clinic I 111 Hundertmark Road I PCC --Carv~r
HP Carver
1 ! ! 1200 Chaska Creek Way Ste i ! ~~~.:.C..chccasc..k~a . .-J~L 004139094~L~talyst Med~C:al Clinic::~Ch!!!~~~~l~-··~··-··2.~-~·-·--~-.1~_9C ,
' i ' j 1200 Chaska Creek Way, ! ' 3687 . C~J~I}'~t.'Y'I!~!~!Ig!!!l~iC:_:g~!'~~~~ ; Suite 200 i PCC Chaska
!'!<:;,. 003209895 Lakeview Clinic - Chaska 2
HP 2402 Lakeview Clinic - Chaska
37 Lakeview Clinic - Chaska
BC carver I Chaska I MN I 003208662 I Ridgeview Chaska Clinic ~-"j'··· ··-~·r-~···~--·~---·~-·-···:~~--~-~-~: -~~--··---.. --~-.~ ..... ~---·~-·~~-
Ridgeview Chaska Clinic
, ... ~~~.~! ··-"··---~~ge~ie,w <:;~aska_<:;Ji~i~ ....... . ' 003200424 i South Lake Pediatrics - Chaska +~-''"=~-,-~,,~,·~~~~~,.~~-~--~~~·~-·~--•wu'-~'"
South Lake Pediatrics - Chaska 111 Hundertmark Rd., #210
2 2
2 2
2 2
2 2
2 2
····.·~~~l!ll~!I!!'Y'I!.~!~!I .. CI!~!~ .•...•..... ,.~~·-6·1·5.!:Jel~;>~_()r: ... _ ..... 2 1
Clearwater Medical 2 1
Clearwater Medical 2 1
Allina Cokato Clinic 110
110
110 Olsen Blvd NE
i 003638585 Cold Spring Medical Clinic i 402 N. Red River Ave., #2 i PCC i ':,"m~~~-.~~ m ~ w.~~-~--.~-~~-"""""""""""'"""""~"~•""""~~---~-.--.-~-~---·~"""~"'-~"~'-""~-·~u·>~~··o-~wouuu-u-.w-.•u-... i~~"~-1'm
, 402 N. Red River Ave., #2 i PCC i ·····~···· ............................ ·········•·· ........... ~ .. . I 2557 i Cold Spring Medical Clinic r-···· ...... : ..... ··························································
NS120
I 003200086 I Wenner, Christopher J. MD, PA ! 218 Main Street i PCC' J~ .... ~~ ..... ~~ ................. r .... -··~ ......... ~ ............................... ~ ...... ~ .. ~~ ................................................. T ......... ~ .. ~ ........... ~ .. ~ ........ ~ ... ~ ...................... : ................ ~ .... . ~ ... ~!?.~ __ J ...... ~..!Ife~er, ~~-~!!~.~!r J.)'!'?.!I".~.J~ ....... ~18 M~~~r:.e~_ ....... , P~~L~ .. !'::~ ....... ~..J-~ ...... :'--+---.~-.........f ~ Wenner, MD, PA, ~hri~~()p~er J......... 218 Main St. i PCC
NA116 Cold Sprina Medical Clinic 402 N. Red River Ave., #2 j PCC STC

Plan 1 County Ci St PCC# Clinic Name Clinic Address
BC stearns .............. r ... P1 Steams
CentraCare Quick Care ... ~:::::~::: 1:: I 003643510
2749 Sexton Drive
CentraCare Clinic - St John's 2749 Sexton Drive
BC Wright Delano I MN Ridgeview Delano Clinic 916 Sl Peter Ave.
HP . Wria"' -~i-
Ridgeview Delano Clinic -m··· ! Delano~ 916 Sl Peter Ave.
P1 Wright ·---~~~Q~!'~P!'~r:'~.£1'':1.'~---·· Delano MN ·····-~j··· ............................... .
BC WliQht I Delano ! MN I 003200653 ! Wavzata Children's Clinic -Delano
HP Wlight
p
NW
NW
P1 I I I I HealthPartners RiverWay Clinics - Elk !
5303rdStNW
800 Freeport Avenue NW, River #100
iealth Clinic - Elk 800 Freeport Avenue NW, River #100
lealth Clinic - Elk P1 i Sherburne Elk River MN NM101 River 800 Freeport Ave. N., #100A
BC I Wright Howard Lake MN 003208682 Ridgeview Howard Lake Clinic 9006th St. #G
HP i Wright Howard Lake MN 2261 Rl~gevlew Howard La~!..._Ciinic 9006thSt.#G -~--r------0............ ~- .
MN I P1 Wright Howard Lake NA213 Ridgeview Howard lJI.~£1i~iC. ... ····t ..... . eoo 6th st.
- Melrose 525 w. Main St.
P1
.E.Lt-·-··--
BC o.:::.:.-":Z. I .... · I -------- I Lakeview Clinic West - Norwood 406 Faxon Road
HP ....... ·-- j MN 1 499 Lakevle~ Clinic West - Norwood 1 406 Faxon Road
BC Steams I Paynesville I MN I 003204253 CentraCare Health Paynesville -
Paynesville Clinic 200W.1st. St.
2019
Type
PCC
PCC
PCC
PCC
PCC HPR 1
PCC NOR 2
PCC NOR 2
PCC NOR 2
PCC IMT 2
PCC IMT 2
2020 Cost Level(* denotes
1
2
2
2
2
2
®
~ . '

Plan County City St PCC# Clinic Name Clinic Address
CentraCare Health Paynesville -HP Steams Paynesville Clinic ;
--~---"--'---~··········-~·--" ·"·•·-------·m~--···------·-·-········---- ····---.- ····--·-r·-·-··· . CentraCare Health Paynesville - -
MN 744 200 W. 1st. St.
P1 Steams MN NA600 Paynesville Clinic 200 W. 1st St.
ceiltiicareiieaiiilPciynesviiie~ , BC Steams Richmond MN 003204255 . ·····~- ·"·· -~---~~-~C:~.'!!~."~~JiiJ.i<: ................. L....... ~O..':'!"!~~!:."!.E_ ..
CentraCare Health Paynesville - ; HP ....... Richmond MN 870 St··~· Richmond Clinic i 130 First St. NE
P1 Steams
HP Steams
Steams --· ~-··
."!£ .. i---~eams I .=.:~:::;::;:""
HP Steams
P1 Steams
BC i s;_:~_.:::.:....:::.::.:::.::__ .. --. HP
, ... ·····c:eliiiicare.iieaiiilliavnesvilie:····· ····· Richmond Clinic : 130 First St. NE
iieaitilfiartlier&ceiliiiiTNiinile&otii· + Clinics 2251 Connecticut AveS
HealthPartners Central MN Clinic 2251 Connecticut Ave. S.
Pediatrics 111 Second St. South
Sartell Pediatrics
Sartell Pediatrics, PA
100 South 2nd S
·+~~W:.;c;.;illiams lntegracare Clinic i 1002ndStS . __ . ._... . centracare Health System·:sauk I -~----,-~----;
Centre Clinic ' 425 Elm St North -~~-centracarel=lealth sySieni- sau·il~'-·--~---~-
~--~--l..---~---~entre Elini<:. .......... ~-...1..... 425 E~:>t. North i CentraCare Healthcare System - Sauk i
NA184 ; Centre Clinic : 425 Elm St. North ~---: ~centracarecliliic~-NorthwayF .. amW·'--~---·~--
··-·----..M~~cine __ ~---····-L 1555 No_:tll~~-Drive, #1.0.0.""" CentraCare Clinic -Northway Family ·
Medicine CentraCare Clinic - Northway Famil
Medicine
2020 Cost Level(* denotes
2019 I clinic moved Cost to 2 for
2
2
;~--\--:~~~:-[--!!~~;::+:~+ -~:::~---+-~!:!~~:~:;!:~;~~::;:~~::::··· , 1555 Northway or. #2oo : Pcc'
~~l_:;~oo:~4""""''~--~~"";:;.E.~~~~J ~'"C;;,~;._;,:;:.-_:_j ~~~ .~ - . V HP steams St. Cloud i MN i 2554 St. Cloud Medical Group - South 1301 - 33rd St. South ! PCC ! STC "'7""
@
®

Plan I County City St PCC# Clinic Name Clinic Addrass
--~ ste~~T Cloud I MN t-00363867~-~~l.-~J~~-I!edical_~.':!l~ - Northwest 1 ... 2~~~~ty Roa!!,_ 120 -·
BC steams
HP I steams
255~ .. --i-S.~· Cloud Medical Group - Northwest
3690
d ! MN 3953
MN NA678
St. Cloud I MN ! NA117
FP148
..... ~.l~pl_i_~_i~ .. ~ltl'.~......... . . ........... + ........... :.:.:.:.:·:.:::~ ... :::.:.:: .. c., __ :: .. : .. c: ... ..
Simplicity Health CentraCare - Plaza Clinic lntemal
Medicine
Odam Medical Group
....... ~!~_p!i_~!~ ... l:!ltl'.~----····
~lt~!J!I.~I'.'.! .. ~!!~!~ ... : .. ~.~~~ItP~ .. ~I!'.'.i~---
3405 3rd St. N.
1360 Elm St. East IPCci ............. - ............................... ·············f····-· ... ··-··t·······
CentraCare Clinic - St. Joseph Clinic I 1360 Elm st. East i PCC i .... .. ... ~~~~~;;~;~::;.::;~:~;~;~::~;;~;~::::[:::_ ::::::~-~~~:.~~;;~~ ............ i'"" ···t···
llna Health St. Michael Clinic ~o Edgewood Dr. NE
I Clinic 4300 Edgewood Dr. NE
I Clinic 4300 Edgewood Dr. NE
FAI
2020 Cost Level(* denotes
2019 I clinic moved to 2for
2
2
2 2
2 2
(fj)
(31