you can't forget the patient— in patient safety
TRANSCRIPT

Inside Medical LiabilityA P I A A P U B L I C A T I O N F O R T H E M E D I C A L P R O F E S S I O N A L L I A B I L I T Y C O M M U N I T Y
2 0 1 4 T H I R D Q U A R T E R W W W . P I A A . U S
ERM for MPLA N D
You Can’t Forget the Patient—
in Patient Safety
Covers 3Q 2014 FINAL USE _Layout 1 8/8/14 11:43 AM Page 2

PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:00 PM Page 1

PIAA polls its members on a regular basis, to keep up to date on
the issues that matter most to the community. In our most
recent survey, an old, but perennially important, topic was top
of mind for many PIAA members: patient safety.
Patient safety has long been a central concern for everyone who
is part of the Association. In fact, back in the 1970s, the founding
companies that joined together to launch PIAA broke new ground, in
many areas, when it came to developing a safer environ-
ment for healthcare. Innovative risk management and
loss prevention initiatives comprised the foundation of
these efforts, along with the analysis of MPL claims and
cause-of-loss data.
Today, in light of the ongoing transformation of the
healthcare system, and the intense focus on reducing the
cost of healthcare while at the same time increasing its
quality, patient welfare is arguably more central than
ever for those in healthcare and in the MPL arena. The interests of
healthcare professionals and their patients are squarely aligned when it
comes to safety. Nobody in the chain of care is more focused on a pos-
itive outcome than the healthcare professional. So, in this instance, the
interests of patients, healthcare professionals, and the MPL community
truly are in sync.
For this reason, in this issue of Inside Medical Liability, our cover
story examines the top ten patient safety concerns for healthcare
organizations. It then goes on to provide details about three of
these—care coordination, reporting test results, and drug shortages.
The article can help healthcare organizations in determining where
they can most usefully focus their patient safety efforts, and will assist
them in selecting priorities and devising corrective action plans that
can minimize adverse outcomes. You will also hear from two of your
peers—PIAA member companies that offer some illustrative stories
about what they’ve done to advance their progress in patient safety.
These are, of course, only two instances of the contributions that
PIAA members have made to a safer healthcare environment. We hope
that this discussion will serve as a springboard for a fruitful dialogue
and the sharing of new ideas on patient safety. We urge you to keep us
informed of your progress in this area.
It goes without saying that your feedback is the single most
important driver in all that we do at PIAA. In the latest
member survey, you told us about what you anticipate
will be your most daunting challenges over the next
three years: for example, the evolving healthcare land-
scape, the shifting MPL marketplace, operating and
defense costs, and state regulation and legislation.
You also told us what we are doing best at this
point: providing unique MPL data, leadership of the
MPL community, offering exceptional continuing educa-
tion for MPL professionals, and providing networking and relationship
building opportunities, among others.
In addition, and perhaps most important, you helped us under-
stand how we can assist you with your business, both now and in the
future: we should sustain our focus on patient safety, provide cutting-
edge information on loss prevention and risk management, expand
our data collection and research capabilities, favorably influence legis-
lators and public policy makers, and serve as a connecting point for
the larger MPL community, to name a few.
We will keep all of this clearly in mind, in the months ahead, as
we ensure that PIAA serves your needs to the best of our ability—and
provides even greater value for each PIAA member. As your trade
association, we endeavor to see for you, hear for you, and represent you
whenever a need arises. Nothing is more important to us than meet-
ing your needs.
Patient safety has longbeen a central concern foreveryone who is part of theAssociation.
PATIENT SAFETY AND YOUR NEEDS—ALWAYS MOVING FORWARD
P R E S I D E N T , B R I A N A T C H I N S O N
P E R S P E C T I V E
I N S I D E M E D I C A L L I A B I L I T Y 1 T H I R D Q U A R T E R 2 0 1 4
“”
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:01 PM Page 2

F e a t u r e s22 Cover Story: Using PSO Data to Identify the Leading Patient
Safety Concerns—and Lessons LearnedBy Cynthia Wallace, CPHRM, and Karen P. Zimmer, MD, MPH, FAAP
28 Feature: The ‘Seven Deadly Sins’ of Large-Scale IT Project Management By Martin Lippiett
31 Feature: Transparency: Changing the World We Live In, for the BetterBy Kevin Bingham, Mark Bethke, Greg Chrin, and Josh Merck
34 Feature: Enterprise Risk Management for MPL SpecialistsBy Gerry Glombicki
S p e c i a l S e c t i o n
54 2014 PIAA Medical Liability Conference
D e p a r t m e n t s
10 On MarketingThe Measure of Your Brand By David Kinard
14 Legislative Update
16 Case and CommentThe Dental Professional Review and Evaluation Program: Lessons and Implications for Professional License Defense By Thomas Bright, Esq., and Vincent Dunn, Esq.
39 Alternatives for RisksQ&A with Nathan Reznicek, Assurance Partners
43 Insights on AccountingLoss Reserves: The IRS’ Kryptonite or Gold Mine?By Brandy Vannoy and Derek Freihaut
47 International PerspectiveApproaching Risk in the Information AgeBy Dr. Thom Petty
50 By the NumbersA Pause in TimeBy Richard B. Lord and Stephen J. Koca
60 Last Word
U p F r o n t1 Perspective
4 Events & Calendar
6 Observer
8 PIAA DSP Data SnapshotMost Prevalent and Expensive Outcomes
A PIAA PUBLICATION FOR THE MEDICAL PROFESSIONALLIABILITY COMMUNITY
2014 THIRD QUARTER
“By collecting data from many providers,PSOs can spot problems and trends thatan individual organization, with a limitedpool of data, may be unable to detect.”—Cover story
I N S I D E M E D I C A L L I A B I L I T Y 2 T H I R D Q U A R T E R 2 0 1 4
28
Andrew N. Brown, M.D.2051 Idaho Ave., N.W.Washington, DC
31
34
Inside Medical Liability
22
contents
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:02 PM Page 3
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:02 PM Page 4
■ 2014 Claims and Patient Safety/Risk Management WorkshopSessions on high-risk situations in the ER, and successful courtroomstrategies
“Common Complaints/Catastrophic Outcomes”This is an essential topic for managing risk inevery MPL enterprise: how to identify the com-mon patient complaints in the ER that may signala high-risk situation. Michael J. Gerardi, MD,FAAP, FACEP, President, American College ofEmergency Physicians, will discuss what can gowrong in responding to symptoms such as abdom-inal pain, back pain, vomiting, headache, rash,
syncope and more. He will then explain how risk management canlower, or even prevent, catastrophic outcomes in the ER.
“In the Courtroom, but Outside the Box”You can also learn about the occasions when a successful outcome in thecourtroom requires something novel—a nontraditional technique orstrategy. In this session two experts will tell you when to use these, andhow to deploy them to maximum effect, based on actual cases. TracieM. Dorfman, Esq., Associate, Hancock, Daniel, Johnson & Nagle, P.C.and Richard L. Nagle, Esq., Director, Hancock, Daniel, Johnson &Nagle, P.C., will help you become more innovative in finding newapproaches to persuading a jury.
■ 2014 Underwriting Workshop Sessions on advanced-practice nurses,and use of the da Vinci robot inhealthcare
“The Expanding Role of Advanced-Practice Nurses” More of the tasks that were once restricted tophysicians are now done by advanced-practicenurses. This raises important questions for MPLentities. Melissa Joy Roberts, JD, MSN, FNPBC,Associate Dean, UMKC School of Nursing andHealth Studies, will discuss the crucial issueswith advanced-practice nursing for MPL. Forexample, how will states modify their scope-of-practice restrictions in response to physician shortages? As standalonenurse practitioner practices proliferate, what impact will that have onMPL exposures and rates?
“The da Vinci Robot: The Rest of the Story”Physicians and patients are bombarded with advertisements promotingnew medical technology like the da Vinci “robot.” In light of the volumeof these procedures, it is time to examine their actual impact for MPL.Barry N. Gardiner, MD, will provide full coverage of this complex topic,including a roster of the surgical specialties that now use robotic surgery,rates of complications, and product defects. He will provide an insider’sview of the strategies that plaintiff ’s attorneys use in claims of allegedharm from robot-assisted surgical procedures.
EVENTS & CALENDAR
C O M I N G A T T R A C T I O N S
I N S I D E M E D I C A L L I A B I L I T Y 4 T H I R D Q U A R T E R 2 0 1 4
September 10–12, 2014THRF WorkshopFairmont Olympic HotelSeattle, WA
September 30–October 1, 2014Introduction to MPLIWorkshopOmni San Diego HotelSan Diego, CA
October 1–3, 2014Underwriting WorkshopOmni San Diego HotelSan Diego, CA
October 8–10, 2014International ConferenceRenaissance Hotel AmsterdamAmsterdam, the Netherlands
October 16–17, 2014Corporate CounselWorkshopFairmont Hotel VancouverVancouver, Canada
November 5–7, 2014Claims/Risk ManagementWorkshopBaltimore Marriott Waterfront HotelBaltimore, MD
March 11–14, 2015CEO/COO MeetingThe Westin Kierland Resort & SpaScottsdale, AZ
March 12–15, 2015Board GovernanceRoundtableThe Westin Kierland Resort & SpaScottsdale, AZ
April 8–10, 2015Marketing WorkshopThe Ritz CarltonCharlotte, NC
April 8–10, 2015Dental WorkshopThe Ritz CarltonCharlotte, NC
May 13, 2015Leadership CampCaesars PalaceLas Vegas, NV
May 13–15, 2015Medical Liability ConferenceCaesars PalaceLas Vegas, NV
MICHAEL J. GERARDI MELISSA JOY ROBERTS
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:03 PM Page 5

Join the many medical professional liability insurance carriers, captives, and risk retention groups who rely on ECRI Institute for unbiased advice and proven risk reduction strategies. Healthcare professionals across the continuum of care refer to ECRI Institute as the “gold standard” for risk management and patient safety resources. Partner with a trusted healthcare research agency whose sole mission is to improve patient care.
Let ECRI Institute be your source for:
Online guidance and tools
Evidence-based best practices
Patient Safety Organization reporting and federal protection
Risk assessment services
Online CME and webinars
Healthcare technology decision support
Access to our 450-person interdisciplinary staff
Make claims reduction more than wishful thinking.
Jump start your risk management and patient safety initiatives today.
Visit www.ecri.org/insurance, e-mail [email protected], or call (610) 825-6000, ext. 5145.
MS14062
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:03 PM Page 6

How can you not love this one? Robotsthat shoot ultraviolet light onto roomsurfaces proved sufficiently powerfulto drive down rates of the hospital-
acquired infections (HAIs) that are caused bymultidrug-resistant organisms or Clostridiumdifficile. The study confirming this happy factwas published in the venerable AmericanJournal of Infection Control.
Ultraviolet disinfection (UVD) technologyuses mercury bulb devices or pulsed-xenonbulbs. The pulsed-xenon devices were firstused in May 2011, at a 643-bed New York hos-pital. Teams from several departments—infec-tion prevention, environmental services, andperformance management—monitored theresults weekly.
More than 11,000 applications of UVDbetween July 2011 and April 2013 resulted ina 20% decrease in overall HAIs related to mul-tidrug-resistant organisms, despite the factthat the researchers had missed nearly a quar-ter of the possible opportunities to use thetechnology.
Adult inpatient rooms at the hospital areroutinely cleaned with sodium hypochlorite0.55% disinfectants, and pediatric rooms arecleaned with a quaternary ammonium com-pound. During the study period, UVD wasadded to the regimen.
Study lead author Janet P. Haas, PhD,RN, director of infection prevention and controlat Westchester Medical Center in Valhalla,New York, says that because UVD seems to
work everywhere else in the hospital, it couldplausibly do the same in operating rooms.However, she warns that the current clinicalevidence for using UVD in the operating roomis less compelling; more research is needed to fully assess how effective it might be in surgical-care areas.
Despite their challenging financial circumstances, reinsurers havecontinued to report attractive results in recent quarters. Lowcatastrophe losses and positive reserve developments have helped.But can this be sustained? Not surprisingly, opinions differ.
The market, at any rate, has weighed in on the matter: reinsuranceshare prices have begun to slip as the abundant levels of traditional andalternative capital have exerted pressure on reinsurance rates.
Recently, presenters at a seminar sponsored by the CasualtyActuarial Society, in New York, offered their take on the relative extent ofdisruption in the reinsurance market resulting from the entry of newcapital. Two of the analysts, Alan Zimmerman, managing director of
Assured Research, and Matthew Mosher,SVP rating services at A.M. Best, suggestedthat the best option was to simply moveon—to explore new opportunities. Theynoted that both insurers and reinsurers needto work hard to remain relevant—even ifthat means abandoning segments of the
market to the new capital. There was a dissenting opinion from MeyerShields, of Keefe, Bruyette and Woods. He suggested less drastic action,advising that insurers and reinsurers investigate the possibility of prof-itable niches within the affected market segments.
But it was Zimmerman who came up with the most memorableimage for the market. He depicted the stark difference between the pre-Hurricane Andrew situation and today. Reinsurers in the prior era werelike “huge, impregnable castles,” he said, with a broad base and under-writing depth. Today, he suggested, they seem more like “mobile homes,”with a greater number than ever before, and more competition.
Reinsurance: From Impregnable Castles to Mobile Homes
Source: Artemis, June 24, 2013
N O T A B L E N E W S A N D T R E N D S
I N S I D E M E D I C A L L I A B I L I T Y 6 T H I R D Q U A R T E R 2 0 1 4
Source: American Journal of Infection Control,June 2014
OBSERVERUV Light Lowers Hospital-Acquired Infections
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:05 PM Page 7
Tacking against the headwinds of general consensus, University ofCincinnati College of Law professor Jim O’Reilly believes that theAffordable Care Act will actually transform MPL litigation into an uphillbattle for the plaintiff ’s attorney. When the huge influx of new patients is
fully in effect, O’Reilly says, we can expect to see a corresponding proliferation oftelemedicine, as well as grocery and convenience store clinics that are staffed bynurses, not doctors.
“There will be errors and there will be compensation,” O’Reilly notes, “but itwon’t be anything like what we’ve seen where patients win millions of dollars.”Speaking as a professor of future attorneys, he cautions, “For lawyers to better servetheir patients, they need to understand that the system has changed. If they don’tknow about it, their client loses.”
Overall, O’Reilly predicts, there will be fewer and fewer cases where a patientgoes to court directly against his family doctor.
The other big factor in the possible decline of MPLclaims, he says, is the rise of large hospital-basedaccountable care organizations (ACOs). The thoughtof taking on a mega-hospitals cadre of lawyers maywell be intimidating to a plaintiff ’s attorney contem-plating whether or not to take on a particular case.
The way out of this quandary? Well, this isAmerica, where the answers to so many problemsare revealed in a steady stream of brand-new pub-lications. O’Reilly offers his: The New MedicalMalpractice. Described by his employer, theUniversity of Cincinnati, as “groundbreaking,” thebook will supposedly help lawyers negotiate whatO’Reilly sees as a whole new healthcare scenario,with a “more diverse set of defendants and a muchmore complicated decision for compensation.”
Department of Upbeat Predictions: In-Store Clinics, Telemedicine—and the Death of Windfall MPL Judgments
Quiz Time! Students’ Concernsre MPL and Defensive Medicine
Compliance with hand hygiene is animportant goal in infection preven-tion. And yet the hand-to-handtransfer of infectious bacteria is
still a common public health hazard. Asdraconian as it sounds, some clinicians arepushing to prohibit the familiar greeting, thehandshake, between providers and patients.
According to a recent proposal published online in JAMA,hospitals, surgical centers, and office practices would be designated“handshake-free zones.” The authors, clinicians from the DavidGeffen School of Medicine in Los Angeles, propose some possiblesubstitutes: open-handed waves, bowed heads, hands over the heart,and yoga-style “Namaste” gestures.
There is actually some research toback up the proposal. Last year,researchers from the University of WestVirginia compared the infection-transferpotential of fist bumps vs. handshakes, andfound that the fist bumps were less likely to pass on infecting agents.
The UCLA clinicians are quite insistent about the impor-tance of the no-handshake policy. “Removing the handshake fromthe healthcare setting may ultimately become recognized as animportant way to protect the health of patients and caregivers,” they say, “rather than a personal insult to whoever [sic] refusedanother’s hand.”
Arecent report in the Western Journal of EmergencyMedicine (William F. Johnson et al., Hackensack UniversityMedical Center) noted the responses of third-year medicalstudents to a series of statements about defensive medi-
cine and their related medical liability concerns (MLC).The study employed a five-point Likert scale, and their
responses were tabulated as percentages, with a 95% confidenceinterval. Now it’s your turn. Match the statements in the first sec-tion with your guesses on the percentage of students who agreed,in the section below. The answers appear at the end of this article.The statements1. I rarely worry about being sued ____2. The faculty are concerned about MPL ____3. The faculty teach defensive medicine ____4. My satisfaction as a doctor will be decreased by MLC
and lawsuits ____5. My choice of medical specialty will be influenced by MLC ____6. My enjoyment of learning medicine is lessened by MLC ____7. I worry about practicing and learning procedures because
of MLC ____Percentage of students who agreed
I N S I D E M E D I C A L L I A B I L I T Y 7 T H I R D Q U A R T E R 2 0 1 4
Let’s Shake on It: Ban the Handshake
Source: Outpatient Surgery magazine, May 27, 2014
Source: Western Journal of Emergency Medicine, May 2014. Source: Medical Xpress, May 22, 2014
a. 51.0%b. 32.4%c. 21.6%d. 85.3%
e. 16.7%f. 55.9%g. 23.5%
Answers: 1, d; 2, f; 3, b; 4, a; 5, c; 6, g; 7, e.
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:05 PM Page 8

F O R E S I G H T
In conjunction with the cover story on page 22, Using PSO Data to Identify the Leading Patient
Safety Concerns—and Lessons Learned, ECRI Institute ranked “retained devices and unretrieved
fragments” as number seven on its 2014 Top 10 Patient Safety Concerns for Healthcare
Organizations. A review of closed claims in the PIAA Data Sharing Project from 2008–2012
revealed “foreign body, surgical, left in patient during a procedure” as the fourth most prevalent
patient outcome. This outcome is similar to “retained devices and unretrieved fragments” as iden-
tified in the previously named ECRI publication and also in ECRI’s 2014 Top 10 Health Technology
Hazards. Among these claims, 28% totaled more than $20 million in indemnity payments. The
claims had an average indemnity payment of $85,427.
I N S I D E M E D I C A L L I A B I L I T Y 8 S E C O N D Q U A R T E R 2 0 1 4
MPL DATA—MOSTPREVALENT AND EXPENSIVEOUTCOMES
P I A A D S P
When compared to the most expensive outcomes, “foreign body, surgical, left in patient during a procedure” was not among the top five and was
less than 1% of the total indemnity ($8.2 million) for all claims paid between 2008 and 2012; however, it’s critical to consider these claims as
they impact areas for improvement in patient safety.
The PIAA Data Sharing Project provides information on claim trends for the most recent ten-year period and other timeframes.
For more information, please visit the PIAA website at www.piaa.us.
MOST PREVALENT RESULTINGMEDICAL CONDITIONS
Closed Paid % Paid-to- Total AverageClaims Claims Closed Indemnity Indemnity
2,814 726 25.8 $252,065,722 $347,198
1,021 200 19.6 $54,810,736 $274,054
952 120 12.6 $14,286,539 $119,054
880 243 27.6 $20,758,861 $85,427
863 285 33.0 $132,015,648 $463,213
Cardiac/cardiorespiratory arrest
Postoperative infection
Emotional distress only
Foreign body, surgical, left in patient during a procedure
Breast cancer
MOST EXPENSIVE RESULTINGMEDICAL CONDITIONS
Closed Paid % Paid-to- Total AverageClaims Claims Closed Indemnity Indemnity
2,814 726 25.8 $252,065,722 $347,198
607 233 38.4 $172,109,686 $738.668
590 246 41.7 $132,480,940 $538,540
863 285 33.0 $132,015,648 $463,213
650 231 35.5 $96,639,029 $418,351
Cardiac/cardiorespiratory arrest
Brain damaged infant
Birth trauma
Breast cancer
Acute myocardial infarction
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:06 PM Page 9

Wells Fargo Advisors, LLC, Member SIPC, is a registered broker-dealer and a separate non-bank affiliate of Wells Fargo & Company. ©2013 Wells Fargo Advisors, LLC 0211-1214A 03/13
at the top of your game requires focus, foresight and the ability to act
your
Joe Montgomery, Judy Halstead, Christine Stiles, TC Wilson, Bryce Lee,
Robin Wilcox, Cathleen Duke, Kathryn Jenkins, Brian Moore, Loughan Campbell,
Karen Hawkridge, Evan Francks, Vicki Smith and Brad Stewart
428 McLaws Circle, Suite 100 Williamsburg, Virginia 23185757-220-1782 888-465-8422
of Wells Fargo Advisors
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:06 PM Page 10

In a nutshell, AAU looks at these:Awareness. The percentage of your targetaudience (customers or potential customers)who recognize your organization or its brand,either aided or unaided. It also measures howmuch knowledge the target audience hasabout your organization’s products and serv-ices. So, not only do you look to see if theyknow about you, you measure what theyknow about you.
Attitudes. This is a combination of what yourtarget audience believes and how strongly theybelieve it. Measurements cover the target audi-ence’s perceptions of quality, effectiveness, andvalue as they relate to your organization, andalso cover intention to make a purchase orbecome involved with your cause.
Usage. This is simply the target audience’s self-reported behavior, as it relates to yourorganization.
So, how do you get this type of informa-tion? Here are two ideas.
But first, a caveat: make sure you specificallyidentify the target audience you want to meas-ure. I can’t overemphasize the need for specifici-ty in this step. Saying you want to measureawareness among the physicians will not giveyou actionable data, because your organizationprobably doesn’t have the marketing budget forthat large a study. Think specifically about the
If you ask 25 marketing professionals whata brand is, you’ll likely get 25 differentanswers. The best definition of a brand I’veheard is this: “a promise held in the mind
of the consumer, of an expected, consistent,and personal experience from a product, per-son, or organization.” But, despite the vast vol-ume of words written about brands (Amazonhas more than 5,000 books on the subject), itseems that many marketers today find it chal-lenging to define their brand, let alone meas-ure its impact.
The first brands were literally justthat—names of companies burned intopacking barrels, so they could be identifiedduring the loading and unloading of ships inport. Some have said that the first brand totruly take root was that of the NationalBiscuit Company, which burned its abbreviat-ed name—NABISCO—into these barrels to sort theirs from the other cargo morequickly.
More recently, however, branding funda-mentally changed and became a marketingstaple in the early 1980s, when Jack Trout andAl Ries published their seminal book,Positioning: The Battle for Your Mind. Thatsimple paperback redefined the role of brand-ing and put the business-customer relation-ship front and center in the purview of the
marketing department, thereby sparking awhole new series of efforts meant to createspecific associations and evoke positive feel-ings for brands in consumers’ minds.
The challengeThe challenge facing insurance marketerstoday is how to refresh our brands in a waythat keeps them out of the general commodi-ty market and viewed instead by the buyerand consumer as essential to their success.But how do you, as a marketer, know whatthat promise is—the one that is in the mindof the consumer? How do you unlock thepower of your brand, if that power isn’t fun-damentally yours to begin with?
The best place to start assessing yourbrand’s capabilities is with a simple metricdesigned to tell you how many people areaware of your brand, find out their attitudesabout it, and reveal their behaviors in regardto your brand.
Typically referred to as AAU (“aware-ness,” “attitudes,” and “usage”), this metric ismost useful when results are set against someform of comparator—that is, data from aprior term (e.g., year-over-year), differentmarkets (e.g., geographic or demographic), orinformation from your competitor(s). AnAAU metric by itself is meaningless, until youhave a pivot point from which to demonstratemovement. In that light, several data sets areessential for identifying valid trends andmovement in AAU.
O N M A R K E T I N G
B Y D A V I D K I N A R D
David Kinard is Vice President of BusinessDevelopment at Physicians Insurance A MutualCompany, Seattle, Washington.
I N S I D E M E D I C A L L I A B I L I T Y 10 T H I R D Q U A R T E R 2 0 1 4
The Measure ofYour Brand
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:06 PM Page 11

CREATE A WIN WHEN YOU CHOOSE THE IMPERIAL PFS INSTALLMENT SOLUTIONS PROGRAM
To find out more about the advantages of the Imperial PFS Installment Solutions Program, call:
For information on all other Imperial PFS programs, visit: ipfs.com
JACK MERRIMAN312.205.4838
DICK CRNKOVICH253.466.3583
JASON SANDERS312.205.4821
1. INSTALLMENT PLAN FLEXIBILITY/OPTIONS
• When a consumer finances a purchase, the focus is on the amount down and the monthly payment.
• Offering more down payment and monthly installment options correlates to higher sales success for carriers.
• Add significant value to your product offerings by dramatically improving your billing options.
2. REDUCE BILLING & CUSTOMER SERVICE EXPENSES
• Collect premium payments UP FRONT.
• Eliminate the cost of billing and servicing deferred installments.
• Imperial PFS handles customer service calls.
3. FINANCIAL BENEFITS• Cash flow, liquidity and investment income all grow when
full premium is collected UP FRONT.
• No deferred installments means reduced operating expenses and credit risk.
HAPPIER CUSTOMERS.MORE PROFITS.
LESS RISK. THAT’S A WIN.
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:07 PM Page 12

finite group you want to study, for example,radiologists in Arizona.
You can use surveys conducted byresearch organizations that know how toreach your target audience. These might beonline, intercept, mail, or telephone surveysthat ask a series of questions. Use the sameset of questions over time, so you have datapoints to measure against.
Yes, you can administer a survey your-self if you’re measuring your internal con-stituents, but I’d still suggest that you employa true researcher to help with the set-up, col-lection, and analysis. They’re the experts atthis type of work—you’re likely not.
Or, you can scan discussion boards andsocial sites for first-hand comments andreviews. You can gather a wealth of knowledgejust by becoming a quiet participant in userforums and sites that are talking about you.Resist the urge to defend and comment. Justlisten and regularly monitor the tone of theposts, and the information shared.
Here are three kinds of data streams youmight get and what to do about them.
■ High awareness, high attitude, lowusage. In essence, these people are saying, “Iknow about you, but I do not think highly ofyou and will not engage with you.” How to respond. These people may notknow how to engage with your organization.Maybe your communications are unclearabout your educational opportunities. Maybeyour opportunities for learning are not whatthis audience wants. Go to them, find out howthey want to engage with you, and then createthe opportunities they’re looking for.
■ High awareness, low attitude, lowusage. These individuals may know aboutyou, but they don’t think highly of you andwill not engage with you. How to respond. These people should be leftalone; instead, you should focus your energieson higher-yield opportunities. Seriously, themore you try to engage this population, themore likely you are to annoy them and createnegative brand experiences.
■ Low awareness, low attitude, lowusage. Basically, these individuals don’t know
you exist, and therefore do not engage with you.How to respond. An awareness campaignmight move the members of this group intoanother, more fruitful category for your mar-keting efforts. But you’ll need to evaluate thecost of a program compelling enough to breakthrough the noise in the market space as youcompete for attention. Make sure you have aplan in place to engage with (or disengagefrom) these people once you do.
Bottom line For many insurers, the commonly acceptedidea is that if more people are aware of anorganization, there will be more prospectsand, ultimately, more buyers. These insurersequate awareness with moving the organiza-tion forward and enhancing success. Rather,the opportunity with branding is to createengagement, not awareness. Because if aware-ness were the name of the game, we’d all beshoveling pamphlets out of airplanes—from30,000 feet.
O N M A R K E T I N G
I N S I D E M E D I C A L L I A B I L I T Y 12 T H I R D Q U A R T E R 2 0 1 4
For related information, seewww.phyins.com.
CEN
EPL
Learn more about our actuarial services at www.oliverwyman.com/actuaries or email us at [email protected].
THE ACTUARIAL PRACTICE OFOLIVER WYMANOur more than 90 credentialed actuaries provide customized actuarial services and strategic insight, supporting healthcare clients as they strive to exceed their business objectives. Our exceptional client and employee retention exemplifies our commitment to relationships built on trust, responsiveness and clear communication.
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:07 PM Page 13
CENTER FOR QUALITY IMPROVEMENT IN RADIOLOGY INTERPRETATIONS
The Center for Quality Improvement
in Radiology Interpretations
offers two ways toimprove outcomes in
medical liability litigation
STRENGTHEN EXPERT TESTIMONYWe provide your expert with the litigation study hidden
among multiple control studies for interpretation
BLINDED CLAIMS ASSESSMENTHave your litigation study read and reported by 10 ABR certified radiologists in the course of their daily routine
■ ■ ■
Visit our website, www.VeritasReporting.comor contact us at [email protected]
ELIMINATE HINDSIGHT BIASPLAIN FILMS • CT • MRI • MAMMOGRAPHY • ULTRASOUND
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:07 PM Page 14

While regular readers of“Legislative Update” will recallprevious articles about PIAA’slobbying efforts in
Washington, D.C., that represents only a por-tion of what it takes to advance the PIAA agen-da and defend our companies from groups thatoppose your interests. To be truly effective,advocacy efforts must include three compo-nents—grassroots, lobbying, and politicalfundraising. Unless we engage all three, it isnearly impossible to achieve legislative successin the nation’s capital.
GrassrootsIn 2011, the Congressional ManagementFoundation (defined by them as an “organiza-tion founded to aid in management-relatedissues in Congress”) released a report on howwell various types of advocacy efforts are per-ceived on Capitol Hill. Congressional stafferswere nearly unanimous in saying that an in-per-son visit from a constituent had at least someinfluence over the Member of Congress.Compared with a meeting with a lobbyist (moreon that later), nearly six times as many stafferssaid the constituent visit had “a lot of positiveinfluence” on the legislator. Hill staffers also payattention when an individual represents the
views of multiple constituents. The same reportnoted that 96% of staffers said “contact from aconstituent who represents other constituents”has an influence on the Member’s views.
With this information in mind, onSeptember 15 and 16, PIAA will host a CapitolHill Advocacy Day. The event will feature anetworking dinner on the evening of the firstday, so attendees can connect with their med-ical professional liability (MPL) colleaguesfrom around the country. The next morning,participants will be briefed on the most press-ing MPL issues facing Congress, and then meetwith their elected legislators. Because the mid-term elections will be less than two monthsaway at that point, and many Congressmen willalready be thinking about which issues they’llneed to deal with first during the anticipatedpost-election lame duck session, PIAAAdvocacy Day will be perfectly timed to getMembers of Congress thinking about impor-
tant MPL issues.To find out more information about this
special event, or to learn how you can helpeven if you can’t come to Washington, D.C., see www.piaa.us.
LobbyingGrassroots advocacy is critical, but PIAAknows you have many important things to doin keeping your company prosperous. This iswhy PIAA has a full-time GovernmentRelations Department that connects withCongress and the Administration throughoutthe year. The lobbyist’s responsibility is torepresent you and your interests when youcannot be there to represent yourself. In prac-tical terms, this means meeting with Hillstaff, Members of Congress, and officials fromthe Administration, to help shape policy.
Lobbyists’ efforts span a broad array of tasks, for example, working with a
Understanding the Advocacy Process
L E G I S L A T I V E U P D A T E
B Y M I C H A E L C . S T I N S O N
Michael C. Stinsonis Director ofGovernmentRelations at PIAA.
I N S I D E M E D I C A L L I A B I L I T Y 14 T H I R D Q U A R T E R 2 0 1 4
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:07 PM Page 15

Congressional office to draft legislation, writing up talking points or questions for aCongressional hearing, developing strategy foradvancing a particular piece of legislation (orto stop its progress), and explaining the impactof proposed regulation.
It is probably most accurate, however, todescribe lobbyists as educators whose pri-mary function is to ensure that governmentofficials know as much about an issue as pos-sible before they take action on it.
To many people, the lobbying process issomehow tainted, but in fact it’s a vital ele-ment in governing. For starters, no Memberof Congress, Hill staffer, or regulator can knowall the ramifications of a piece of legislation orproposed rule. In the case of Congress, legis-lators and their staffs are asked to consider lit-erally thousands of bills over every two-yearcycle, and there is simply not enough man-power on Capitol Hill to permit every office tohave an expert on all possible issues. In addi-tion, as noted above, you, as PIAA members,can’t be expected to serve as the resource foryour Member of Congress on every issue ofimportance to you. You’ve got other things todo. Lobbyists ensure that your voice is heardand your issues are understood by the peoplewho are making important policy decisions.
CampaignsThe third element in advocacy is politicalfundraising. While nearly every lobbyist Iknow would rather focus on his role as aneducator, rather than spend time at campaignfundraising events, it is a sad truth thatmoney is very often necessary to get access.That does not mean that money will neces-sarily influence a given official, however(more often than not, money is used to sup-port a candidate who already holds a specificview, rather than in trying to convince thatindividual to change his mind). Instead, cam-paign contributions are used to pay for atten-dance at fundraising events, where you canfocus a candidate’s attention on a key policyissue. These discussions are usually quitebrief and superficial, but they can open thedoor for more in-depth conversations at somelater point—and this was the actual objectiveof the initial discussion in the first place.Admittedly, this is not the ideal approach togetting things done, but overly zealous ethics
“reforms” enacted several years ago bannedmany lobbying activities that were perfectlylegitimate, leaving advocates with few optionsother than paying what may be large sums toattend fundraisers.
In this regard, PIAA maintains a politicalaction committee (PIAAPAC) just for this pur-pose. Annual fundraising efforts from withinthe PIAA membership (federal law prohibitsPIAAPAC from accepting funds from non-members and even a substantial number ofindividuals directly affiliated with a PIAAmember company) provide the revenue neededto attend political fundraising events. To maxi-mize the effectiveness of our extremely limitedPAC dollars, PIAA focuses its attention on thosecandidates who sit on specific important com-mittees or otherwise hold positions that willallow them to influence their colleagues. Allfunds given to campaigns from PIAAPAC arefirst approved by the PAC Board of Directors,and are donated without regard to the political
affiliation of the candidate or their views onissues outside the scope of PIAA interests.
ConclusionWhile PIAA is small compared with manyother interest groups and associations, itstrives to make the most of its resources.Utilizing grassroots advocacy, lobbying, andpolitical contributions, PIAA has achievedremarkable success in recent years. Amongthese victories has been successfully defendingMPL insurers from efforts to limit or eliminatelimited antitrust exemptions for insurers andobtaining bipartisan support for efforts to pre-vent the misuse of federal guidelines/regula-tions in MPL lawsuits.
Advocacy is a key component of PIAA’sservices to its membership—and one thatPIAA takes very seriously. Only the strategicimplementation of all three elements of ouradvocacy program will enable us to sustain our current success.
I N S I D E M E D I C A L L I A B I L I T Y 15 T H I R D Q U A R T E R 2 0 1 4
PIAA thanks the following companiesfor participating in the PAC this year:
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:07 PM Page 16
The Dental Professional Review andEvaluation Program, or D-PREP, wasrecently developed by the AmericanAssociation of Dental Boards (AADB)
as a tool for evaluating the competency ofdental professionals. The program may begood idea in theory, but a recentMassachusetts case highlights the seriouslegal issues and difficulties that its applicationposes for dental professionals and insurersalike.
D-PREP presents unique challenges forprofessional licensing defense. The sanctionis so severe—and the results of it so unpre-dictable—that taking a matter to a hearingwill likely prove more desirable than agreeingto D-PREP as a settlement term. Generally,going through a full adjudicatory hearinggreatly increases the costs of defending anaction. The D-PREP program itself is very
expensive, however, and insurers and practi-tioners should be mindful of who will bestuck with the hefty fees associated with theprogram, should it be required.
This case note discusses the issuesraised by D-PREP and offers some insightsfrom our experience in successfully defendingagainst it recently in Massachusetts.
What is D-PREP?D-PREP was created by the AADB and mod-
The Dental Professional Review and Evaluation Program:
C A S E A N D C O M M E N T
B Y T H O M A S B R I G H T, E S Q . , A N D V I N C E N T D U N N , E S Q .
eled after the Physician Assessment andClinical Education (PACE) program designedfor physicians. D-PREP consists of the follow-ing six phases, with fees totaling nearly$20,0001 : 1. A dentist is referred by a licensing boardand applies to the program at one of threehost universities. 2. The dentist undergoes a full mental andphysical examination, the results of whichmust be provided to the AADB for their
Thomas Bright, Esq., and Vincent Dunn,Esq., are with Hamel Marcin Dunn Reardon & Shea, P.C.
Lessons and Implications for Professional License Defense
I N S I D E M E D I C A L L I A B I L I T Y 16 T H I R D Q U A R T E R 2 0 1 4
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:08 PM Page 17

review. 3. The AADB assembles all the informationavailable about the dentist. 4. The dentist travels to one of the host uni-versities, in Wisconsin, Louisiana, orMaryland. There, they undergo a full evalua-tion, including written and clinical testing,over the course of four to five days. 5. The reviewers write a comprehensiveanalysis of the dentist’s competency for thereferring dental board. The dentist will receiveone of three grades: a pass, a pass with rec-ommendations, or fail. A pass with recom-mendations will include suggested remedia-tion. A fail is a determination that he cannotpractice dentistry at a level of minimumpatient safety, and in all likelihood will func-tion as a complete revocation of the dentist’slicense. 6. The dentist completes the remediation rec-ommended in the D-PREP evaluation once ithas been approved by the board.
There is no appellate procedure oropportunity to obtain an appellate review atany stage of the program. The evaluation isfinal, and there is no mechanism for challeng-ing the D-PREP report.
D-PREP is still in its relative infancy. As of January 2014, only approximately tenindividuals had enrolled in D-PREP for serious issues that had cast doubt on theircompetency.
Legal implications of D-PREPGenerally, licensing boards are creatures ofstatute and must have a statutory grant ofauthority for any action they take. Dueprocess requires that when a board seeks torevoke a license, the licensee be given a hear-ing on the allegations against him. These fun-damental legal principles are called into ques-tion by the very nature of D-PREP.
First, while boards are frequently givenwide discretion in fashioning an appropriatesanction, such discretion is not unlimited. InMassachusetts, the action of at least one licens-ing board has been overturned by a reviewingcourt, when it attempted to require a licensee totake and pass an industry examination as a con-dition for maintaining licensure.2 InMassachusetts, there is nothing in the dentalboard’s enabling statute giving them authority
to order a dentist to undergo assessment by athird party. Compare this to the MassachusettsBoard of Registration in Medicine’s statute,which explicitly allows the board to utilize reme-diation programs like the Physician Assessmentand Clinical Education Program (PACE), buteven then, only on a voluntary basis.3
Second, the D-PREP report is used bythe board to determine whether a dentist willbe able to retain his license. The evaluation isnot limited to the issues that caused the caseto be referred to D-PREP in the first place.Thus, a dentist enrolled in the D-PREP pro-gram risks losing his license completely forissues on which a hearing was never held andfor which no appellate review was available.
This possibility flies directly in the faceof traditional notions of due process andessentially outsources the hearing process toan unaccountable third party.
A case studyOur client dealt with a difficult patient popu-lation. He had received a series of patientcomplaints that, we believe, were motivated bya desire for free care, as the patients’ insur-ance program had recently cut benefits sub-stantially. In response to the complaints, theboard conducted a thorough investigation,which included an unannounced complianceinspection of our client’s office. Ultimately,the board did not move forward on the quali-ty-of-care issues raised in the patient com-plaints, except for one allegation that involvedan overfilled root canal. Instead, the boardsought discipline for recordkeeping deficien-cies and other issues discovered during thecompliance inspection.
The board’s proposed sanction, from the
beginning, was to require that our clientenroll in D-PREP. We viewed this as highlydraconian; after all, our client was only beingaccused of a single clinical deficiency. D-PREP was designed for dentists with seri-ous competency problems, not bad recordkeepers. Furthermore, if our client were toenroll in D-PREP, he would need to pay nearly$20,000 and spend a week away from his fam-ily. He would lose any type of control over theprocess, and also risked losing his ability topractice entirely, should the D-PREP assess-ment come back negative.
Keeping in mind that board cases rarelybenefit from a full hearing, we sought toaddress the board’s concerns by proposingthat our client complete additional continuingeducation in the areas noted by the board. Wealso proposed to demonstrate that he had nophysical or mental impairments that mightimpact his ability to practice. The board con-tinued to insist on D-PREP, however, and, con-sequently, this became one of the rare caseswhere a hearing appeared the more attractivealternative to a negotiated resolution.
Our primary theory of the case was thatD-PREP was not warranted under the facts.Nearly all the violations of which our clientwas accused were minor or entirely defensi-ble. In particular, our expert was fully sup-portive of our client’s treatment of the singleoverfilled root canal, which is a known com-plication of root canal therapy.
We also vigorously disputed the board’sauthority to order D-PREP as a sanction.There was evidence, developed through discov-ery, that tended to show that the board was notactually familiar with what D-PREP entailed.We attacked the board’s position on both pro-cedural and substantive grounds. Because webelieved the board would go forward with itsintention to order D-PREP, we thoroughlydeveloped a number of issues for appeal.
In one final push, shortly before thehearing commenced, the case went back tothe board for reconsideration. Our messagewas clear: this was not a case that warrantedD-PREP, and we would challenge it. Shouldwe prevail on appeal, the board risked losingD-PREP as an option in the future in caseswhere a D-PREP assessment might be a farmore appropriate remedy. Ultimately, theBoard relented and accepted our initial coun-
I N S I D E M E D I C A L L I A B I L I T Y 17 T H I R D Q U A R T E R 2 0 1 4
Generally, licensing
boards are creatures
of statute and must
have a statutory grant
of authority for any
action they take.
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:09 PM Page 18

teroffer. This was only after substantial andintense efforts and expenditures needed toprepare the case and highlight the issues D-PREP raised, however.
Insights and lessonsLike outright revocation of a dental license,when D-PREP is proposed as a settlementterm, taking the case through a full adjudica-tory hearing may be the preferable option.The defense will be far more costly, but thisapproach does ensure some limitation in thescope of the issues considered, some level ofdue-process protection for the licensee, andappellate options not available with D-PREP.
If you are confronted with D-PREP as asettlement option, conduct a thorough evalu-ation and assessment of your client’s case.This is an extreme sanction, with whollyunpredictable, and possibly disastrous, conse-quences for your client. Your board’s enablingact may not authorize third-party assess-ments; your client may not be willing to sacri-fice his substantive and procedural dueprocess rights to the unknown individuals at
the D-PREP centers; and you may obtain amore predictable result for your clientthrough the established procedures of anadjudicatory hearing.
D-PREP may serve a suitable purposefor those whose clinical competency is inserious doubt, but it is likely not an appropri-ate option for practitioners facing more rou-tine allegations.
D-PREP can be a useful tool for theboards, and offers an attractive alternative torevocation when the facts warrant it. Theboards need to understand, however, that ifthey order it when it is not warranted and
subsequently lose on appeal, they may fore-close the possibility of ever ordering it.
ConclusionIt remains to be seen how D-PREP will be uti-lized by the boards as the program maturesand boards become more familiar with it. If,as in the Massachusetts case, the boards seekto require it for routine violations, it willimpede the ability to reach negotiated resolu-tion, and defense of professional licensuremay become far more costly. If, however, theboards use it sparingly, and only where seri-ous issues warrant it, the program could bean attractive alternative to the ultimate sanc-tion of revocation.
References1. See http://dentalasp.com/D-PREP.htm.2. George v. Board of Registration of HomeInspectors, 27 Mass. L. Rptr. 186, 2010 WL 3038729(Mass.Super. May 26, 2010). 3. See M.G.L. c. 112, § 5.
C A S E A N D C O M M E N T
I N S I D E M E D I C A L L I A B I L I T Y 18 T H I R D Q U A R T E R 2 0 1 4
For related information, seewww.hmdrslaw.com.
Due process requiresthat when a boardseeks to revoke alicense, the licenseebe given a hearing onthe allegationsagainst him.
AAA
Our handshake means more than an engagement. It means commitment.
MEDICAL PROFESSIONAL LIABILITYALTERNATIVE MARKETSENTERPRISE RISK MANAGEMENTLEGISLATIVE COSTINGLITIGATION SUPPORT LOSS RESERVING
Commitment Beyond Numbers
Commitment Beyond Numbers
Commitment Beyond Numbers
Empathetic Customer Service.elationships, not just transactions. Wr
consulting services in every aspect of medical prinsurance at the local, state and national levels.
e about our medical pro learn morTTovisit us at pinnacleactuaries.com.
Empathetic Customer Service. At Pinnacle, we believe in ovided actuarial e have prelationships, not just transactions. W
ofessional liability consulting services in every aspect of medical prinsurance at the local, state and national levels.
ofessional liability expertise, e about our medical prpinnacleactuaries.com.
MEDICAL PROFESSIONAL LIABILITYTERNALLT
ENTERPRISE RISK MANAGEMENTLEGISLA
TION SUPPORLITIGALOSS RESERVING
At Pinnacle, we believe in ovided actuarial
ofessional liability
ofessional liability expertise,
MEDICAL PROFESSIONAL LIABILITYTIVE MARKETSNAAT
ENTERPRISE RISK MANAGEMENTTIVE COSTINGLEGISLA
TTION SUPPORLOSS RESERVING
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:09 PM Page 19

StoneHill
Advancing Your Business. Ensuring Success.
Inquire. Collaborate. Execute.
www.stonehi l l re.com
ancAdvva
our BusinessYancing
Ensuring Successour Business
Ensuring Success
Ensuring Success
ancAdvva
StoneHill
our BusinessYancing
StoneHill
Ensuring Success.our Business
StoneHill
Ensuring Success
. Ensuring Success
CollaboraInquire.
www
te.Collaboraat
.come.stonehi l l rwww
Execute.
.com
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:10 PM Page 20

H E R C U L E SHIGH SOUTHERN SKYOH SGIH
REHH
RYKN SREHTUO
SELC U
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:10 PM Page 21

Bulk up.Gain capital and scale by becoming a mutual owner of Constellation.If you’re feeling a bit insignificant in the universe of physician-owned medical liability companies, you’re not alone. Many are finding it increasingly tough to compete against large stock companies.
That’s why we formed Constellation, a mutual holding company created for like-minded medical liability insurers and other types of health care organizations. As a joint owner of Constellation, you’ll enjoy significant benefits, such as increased scale, efficiencies, capital and support.
With this kind of strength, you’ll be protected from consolidation and more able to compete against commercial carriers. Most importantly, you’ll remain independent and maintain your customary
operations, allowing you to continue focusing on improving patient outcomes and serving the unique needs of your market.
Find out more about how your company can shine brighter as a part of Constellation. Contact us at 888.965.0503 or visit ConstellationMutual.com.
brighter together
l
klk
B
luB
klkk
puup
p.
p
p.
sniage atpemocna. Menolt aonenwo-niacisyhhypgnielee ffer’uof yI
tipan ciaG ap
.seinapmok ccotrge sat lsylgnisaercnt ig inidne firy annapmoy ctilibial lacided mene uhn tt inacfiinigsnt iig a b
ey be blacd snl aat y b
ruof ys odeenag pnivorpmil, asnoitarpeo
oh tguoy ter’uo, yseinfse orevvein
autug a mnimoec
goe
m
t.ekrar mgnivrd sens aemoctuut oneitaacoe ffounitnoo cu tog yniwooll
etsnof Cr oenwl oa
euqine uhg tng onisuc
.noitlale
uq
n
s eicneicffi, eelacso nigy sojnl el’uoy
. Ar snoitazinargosi rerusny itilibiallnapmog cnidloh
e fy ws whhy’taaTh
gp
nj
t.rpopud snl aatipa, csecns ih acu, sstfient benacfiinleltsnof Cr oenwt onios a jA
h tlaef hs opeyr tehtd ons ad ednime-kir lod ffoetaaery cnu, a mnoitaleltsnod Cemroffo
pg
3050.569.888s a pr aethhigrb
rot muud oniF
dseaerc,noitaal
eraclacidem
lautuu
sn
i
tuMnoitaleltsnot Cisir v3 otno. Cnoitaleltsnof Ct orapynapmor cuow yoot huboe ar
.moc.lauts aat uact
enihn say c
mtaai
npeednn iiamerral ciacremmoc
n aoitaadilosnocd nis kihh ttiWWi
ur cuon yiatniad mnt anedno, yyy,ltnatrpomt iso. Msreirrge atpemoo ce tlbe arod mn
etorl be pl’uo, yhtgnertf so
yramotsull’u
tsniagmord ffretc
olnd
rehttheogge ttorehttegghirb r ig
PIAA 3Q 2014 AFRONT _Layout 1 8/8/14 12:10 PM Page 22
Cynthia Wallace, CPHRM, and Karen P. Zimmer, MD, MPH, FAAP,are with ECRI Institute.
I N S I D E M E D I C A L L I A B I L I T Y 22 T H I R D Q U A R T E R 2 0 1 4
C O V E R S T O R Y
Using PSO Data toIdentify the LeadingPatient SafetyConcerns—and Lessons Learned
Patient safety is a top priority for every healthcare
organization, but knowing where to direct patient
safety initiatives can be daunting. To help organiza-
tions decide where to focus their patient safety
efforts, ECRI Institute has developed a list of the top
ten patient safety concerns confronting healthcare
organizations (Figure 1).
B Y C Y N T H I A WA L L A C E , C P H R M , A N D
K A R E N P. Z I M M E R , M D , M P H , FA A P
PIAA 3Q 2014 Features_Layout 1 8/8/14 2:52 PM Page 1

I N S I D E M E D I C A L L I A B I L I T Y 23 T H I R D Q U A R T E R 2 0 1 4
We’ve been collecting events since 2009, and with closeto 400,000 events, we’re at a point where it’s impor-tant to share where we’re seeing recurring themes,”says Karen P. Zimmer, MD, MPH, FAAP, medicaldirector of ECRI Institute’s patient safety, risk, and
quality group and of ECRI Institute PSO. The initiative underscores the intent of the Patient Safety and
Quality Improvement Act of 2005, which laid the groundwork forproviders to voluntarily report patient safety events and other informa-tion (e.g., root-cause analyses) to Patient Safety Organizations (PSOs)in a protected environment. The PSOs aggregate, analyze, and share
findings and lessons learned. By collecting data from many providers,PSOs can spot problems and trends that an individual organization,with a limited pool of data, may be unable to detect.
The list as a starting pointThe list, which highlights risks to patient safety that stem from issueswith processes and systems, is not intended to be comprehensive, andnot all of the patient safety concerns will be applicable at all healthcarefacilities. “We encourage facilities to use the list as a starting point forpatient safety discussions and for setting their patient safety priori-ties,” says Zimmer.
“
PIAA 3Q 2014 Features_Layout 1 8/8/14 2:53 PM Page 2

Although many of the organizations reporting to ECRI Institute PSOare hospitals, the list of patient safety concerns, such as drug shortages,mislabeled specimens, and care coordination, also applies to non-hospitalsettings, such as physician practices and long-term care settings.
This article highlights three of ECRI Institute’s 2014 Top 10: carecoordination, test result reporting, and drug shortages.
Where to find the full listThe complete 2014 ECRI Institute Top 10 Patient Safety Concerns list,which ECRI Institute plans to update annually, is available for freedownload at https://www.ecri.org/Products/PatientSafetyQuality
RiskManagement/Pages/Free-Reports-Advisories.aspx. It includesstrategies for mitigating each of the ten concerns and is accompaniedby a poster, PowerPoint presentation, and other tools.
Care coordinationCare coordination is a “shared responsibility” of all providers involvedin a patient’s care, says Lorraine Possanza, DPM, JD, MBE, patient safe-ty, risk, and quality analyst at ECRI Institute. However, events reportedto ECRI Institute PSO reveal gaps in communication—between hospi-tals and providers, among providers, and between long-term care set-tings and hospitals or other providers. For example, in one event, an
P A T I E N T S A F E T Y C O N C E R N S
I N S I D E M E D I C A L L I A B I L I T Y 24 T H I R D Q U A R T E R 2 0 1 4
On June 13, 2014, more than 200 patientsafety advocates from across the coun-
try gathered to participate in a day-longsymposium that was focused on how culturecan progressively impact patient safety inhealthcare organizations. Sponsored byCRICO, the goal was to gain a better under-standing of the ways by which culture canenhance or inhibit safety improvements, andhow organizations can affect their own envi-ronment by learning to “Walk This Way.”
In a unique opening segment, a skitcomprising a series of acts depicted the evo-lution of smoking behavior in the hospitalsetting. Many of you may recall a time in thenot so distant past when it was commonpractice for clinicians and patients to smokeon the wards, in the break room, and at nurs-ing stations. This practice evolved—slowly,but surely—to remote smoking rooms at theend of the hallway, outside designated smok-ing areas, and finally, to present-day smoke-free campuses around the country.
Looking back, it’s difficult to believe weever smoked on the ward, drove our childrenaround without car seats, or allowed them toride their bicycles helmet-free. However,through years of research, education, and per-sistence, all of these safety risks have indeedbeen recognized and changes introduced, andpeople have adapted. This premise segued toa robust program that captured an array ofperspectives and impactful lessons for creat-ing a stronger safety culture, including:
Paul McTague, Esq.: Culture as aContributing Factor to Legal Defense■ Three “Cs” for MDs: be Competent,Confident, and Caring—in court and in practice.■ Follow policies; it’s difficult to defend aclaim when they’re not followed.■ Document, as needed, to provide forgood medical care, not what you think willprotect you in court.
Asaf Bitton, MD: Envisioning YourFuture Work Environment■ If we want to make drastic changes, weneed to take drastic steps. ■ Imagine a patient-centered medicalhome that was designed for maximumteamwork and connected by robust IT systems. ■ Establish the goal of your culturethrough seven habits: co-location, huddles,warm handoffs, weekly meetings, staffingthat matches the culture, work force devel-opment, and committed leadership.
Tracy Granzyk: What’s Your Story?The Power of Narrative■ Storytelling can change attitudes andbeliefs, because it breaks down cognitiveresistance.■ Data helps us focus on “what” to fix;storytelling gives us the emotional connec-tion to “why” it matters.■ Honor patient and caregiver stories
through actions respectful of their lesson.
Jerry Hickson, MD: How to Recognize and Remove Obstacles■ Establish an infrastructure that promotes reliability and professionalaccountability.■ Fix your faulty systems and promoteprofessional behavior to set the right balance. ■ Respond to every incident of unprofes-sional behavior with a consistent construc-tive response.
At lunch, attendees were asked to envisionevolved cultural events five to ten years fromnow that may be as difficult to believe as the“smoking story.” The day wrapped up with asummary of the myriad submissions on thegeneral topic: It’s hard to believe there was atime when…■ We did not always wash our handsbefore seeing a patient.■ We did not do formal timeouts forevery surgery. ■ We were afraid to report adverse events.■ We did not have efficient systems fortracking/follow-up on abnormal test results.■ We did not consider patients part oftheir own care team.
Missy Padoll is Director, Strategic Analysisand Communication, CRICO.
By Missy Padoll
For related information, see www.rmf.harvard.edu.
“Walk This Way”: Impacting the Culture of Safety through Time and Example
PIAA 3Q 2014 Features_Layout 1 8/8/14 2:54 PM Page 3

infant’s discharge summary andfollow-up care information werenot provided to the patient’s pri-mary care physician:
An infant who died from sud-den infant death syndrome had pre-viously been seen in the hospital for alife-threatening event. Because ofabnormal findings on the patient’s CTscan, the patient’s discharge summaryindicated the patient should have anMRI exam. The discharge summarywas not sent to the patient’s primaryphysician. The patient did not under-go the MRI study.
While a best practice is forhospitals to send a patient’s dis-charge information to all thepatient’s providers, staff can beoverwhelmed trying to identifythose providers. “It’s not only the hospital’s responsibility,” saysPossanza, who previously had a podiatry practice and has experiencewith care coordination challenges. “It’s also on me as the patient’sprovider to communicate with the patient’s other providers,” she says,recalling that in addition to communicating with patients’ providers asneeded, she used to “touch base” with her patients’ other providers atleast once a year “so they know I’ve been involved in the patient’s care.”
One “simple and basic” strategy to improve care coordinationbetween hospitals and ambulatory settings is for practices to providecurrent contact information, such as phone and fax numbers, on theirwebsites. Possanza adds: “Identify the providers in your practice. If thehospital needs to contact you, the information is right there.”
Linda C. Wallace, BSN, MSN, CPHRM, a consultant in aging serv-ices risk management at ECRI Institute, notes some of the strategiesshe has seen put in place to improve care coordination between hospi-tals and post-acute care providers. They include:■ Preadmission nurses from the postacute care setting evaluate thepatient before discharge and prepare the post-acute care provider formeeting the patient’s needs.■ Hospital representatives visit the post-acute care organization toensure an understanding of the services available there and to mini-mize the risk of transferring patients whose condition cannot be man-aged at that post-acute care facility.■ There are closer affiliations between hospitals and post-acute careproviders, through accountable care organizations or other means.
As providers develop more arrangements to ensure care coordina-tion, Possanza reminds them, “You can’t forget the patient. The patientis overwhelmed by their disease process and by navigating the
system . . . someone needs to helpthat person, especially an elderlypatient, to remind them to makeappointments, to take medications,and to help them know what to askand expect at their next healthcarevisit.”
Reporting test resultsBreakdowns in reporting test resultscan occur for many reasons.Sometimes, the ordering providernever gets the results or receivesthem after a delay. Or, the reportingprovider may be unavailable, andorganizations may not have a backupplan for ensuring that results withimportant findings are communicat-ed to someone else who can act onthem. These breakdowns can con-tribute to “bigger issues of delays inpatient care, as well as delays in diag-
nosing an acute condition,” says Christine M. Callahan, RN, MBA, physi-cian practice management consultant for ECRI Institute.
Examples of test result reporting errors reported to ECRI InstitutePSO include:■ A baby’s treatment with antibiotics was delayed because the testresults confirming an infection were not reported promptly to theordering clinician.■ Prompt management of a patient with C. difficile infection washindered because of a delay in reporting test results confirming theinfection.■ A patient’s seizure due to a low sodium level could have been avoid-ed if blood chemistry results had been provided on a timely basis.
Callahan observes that breakdowns in test results reporting, par-ticularly in physician practices, typically have one or more of threecauses: ■ Technology limitations, such as an inadequate interface betweenan electronic health record (EHR) system and a laboratory system thatprovides the results electronically■ Provider-to-provider communication gaps, such as those thatoccur when no backup plan is in place to designate a provider toreview test results for another provider who is unavailable.■ Staffing and training failures, for example, requiring that a staffmember periodically check an EHR system for test results but notinforming him about the volume of test results he can expect to see.
As more healthcare organizations adopt EHR systems, Callahanwarns against being lulled into thinking the systems can prevent testreporting failures. “It’s another tool,” she says. “It won’t improve test
I N S I D E M E D I C A L L I A B I L I T Y 25 T H I R D Q U A R T E R 2 0 1 4
Figure 1 ECRI Institute’s Top 10Patient Safety Concerns for 2014
MS1
4036
PIAA 3Q 2014 Features_Layout 1 8/8/14 2:54 PM Page 4

I N S I D E M E D I C A L L I A B I L I T Y 26 T H I R D Q U A R T E R 2 0 1 4
results reporting if it’s not used correctly.”Whether test results are reported on paper, electronically, or in
some combination of both, organizations must have policies and pro-cedures to guide reporting of the results and must educate and trainstaff about the policies, says Debra Ann Maleski, MBA, senior associatewith ECRI Institute’s Applied Solutions Group, which provides cus-tomized consulting. The policy should address key questions:■ Who gets the results?■ What is the process for reporting abnormal findings?■ Is there a designated backup provider to review the results if theordering provider is unavailable or does not review the results within aspecified time frame?■ What is the expected time frame for providers to review results?■ How are findings communicated to the patient?■ What is the policy for ensuring that information gets to the
patient if that person is unavailable?
In addition, organizations must audit staff compliance, Maleskiadvises. “You may have a great policy, but if it’s not enacted or followed,the organization needs to be aware and implement corrective action.”
Drug shortagesThe potential implications of drug shortages for patient care werehighlighted when a hospital contacted ECRI Institute PSO about asevere shortage of emergency drugs. Unable to replenish its supply ofinjectable unit-dose medications stored on crash carts, the hospitalwanted to know whether its remaining supply of expired drugs couldbe used instead.
“In the intervening months, the topic remained on our radar andshowed an escalating level of interest from healthcare providers,” says
With a supporting pledge of $50 millionfrom MagMutual Insurance Company,
the MagMutual Patient Safety Institute wasestablished this past October, to facilitate in-depth study and analysis of patient safetyissues confronting MagMutual policyholders.The institute endeavors to create evidence-based resources and practical tools to pro-mote the adoption of best practices in orderto improve safety among its policyholdersand decrease their exposure to risk.
“We believe the best defense againstmedical error is to proactively assist physi-cians and other healthcare providers in thecreation of environments conducive to opti-mal care and outcomes,” said Dr. Joe WilsonJr., MagMutual’s chairman and chief execu-tive officer. “Patient safety is one of the mostpressing challenges in healthcare today. “
In addition to analyzing historicalclaims data, the institute facilitates riskassessments for the more than 19,000 physi-cians insured by MagMutual and its affiliate,Professional Security Insurance Company.This number includes solo practitioners aswell as physicians employed by larger prac-tices and hospitals. The data derived fromthese assessments serves as the basis for con-tinuing medical education (CME), as well asspecialty-specific and even practice-specific
tools and resources.Dr. Mary Gregg, senior vice president
and chief medical officer of MagMutual,serves as president of the institute. Dr. Greggpreviously served as medical director forquality and patient safety and vice presidentof medical affairs with Swedish HealthServices in Seattle, one of the largest nonprof-it health systems in the Pacific Northwest. Shewas also medical director for ClinicalOutcomes Assessment and Performance(COAP) at the Foundation for HealthcareQuality (FHCQ), and medical director of clin-ical quality at Swedish Heart and VascularInstitute.
“Physicians appreciate the power ofeducation and collaboration, and by tappinginto our network of policyholders, we are tak-ing our patient safety and quality efforts tonew levels,” said Gregg. “We help them under-stand their areas of greatest risk, and then wedesign tools to help address them.“
So what are some of the key patientsafety risks identified by the Institute so far?“Two of the most common of the many con-cerns we encounter are medication errorsand issues with electronic medical records[EMRs],” explained Gregg.
“Not only do physicians need to cross-check multiple lists of medications at every
step of the prescribing and dispensingprocess; they also need to be more aware ofdrug interactions and side effects.”
“With regard to EMR issues, caregiversneed to ensure that their system works forthem. Technology can greatly enhance thequality of patient care, but there are risks aswell. We encourage healthcare professionalswho are prescribing and treating to take anactive role in the formatting of order sets,progress notes, procedure notes, and careplans. Providers need to make the ‘right thing’the easiest thing to do.”
“At the end of the day, our goal is to helpour policyholders create a culture of safetycharacterized by transparency and trust, allgrounded in the creation of a database that isfocused on root causes,” added Gregg. “We arelearning as we go, but we aspire to be the go-to organization for new ideas, solutions, andmodels that promote patient safety and mitigate risk, and to attract partners who are willing to pilot new processes.”
Terrell McCollum is Director, MarketingCommunications, MagMutual InsuranceCompany.
By Terrell McCollum
MagMutual Patient Safety Institute Researches Safety Concerns
For related information, see MagMutual.com/patient-safety/resource-library.
P A T I E N T S A F E T Y C O N C E R N S
PIAA 3Q 2014 Features_Layout 1 8/8/14 2:54 PM Page 5

I N S I D E M E D I C A L L I A B I L I T Y 27 T H I R D Q U A R T E R 2 0 1 4
Patricia Neumann, RN, MS, patient safety analyst/consultant for ECRIInstitute PSO. An event reported to ECRI Institute PSO shows the needfor established policies that will guide pharmacists, nurses, and physi-cians on what to do when a drug is unavailable:
A patient in intensive care had a critical phosphate level. The physi-cian ordered an intravenous sodium phosphate for the patient. The phar-macist could not fill the order because the drug was unavailable and didnot tell the patient’s nurse or the ordering physician about the shortage. Thepatient had a seizure due to abnormally low phosphate levels in the blood.
Neumann advises healthcare organizations to develop a proac-tive plan for managing drug shortages. The plan should assign a taskforce to monitor impending shortages, she says. Two good resourcesfor identifying potential drug shortages are the U.S. Food and DrugAdministration’s (FDA) website on drug shortages, which provides alist of national shortages for which there are no substitutes, and theAmerican Society of Health-System Pharmacists’ (ASHP) drug short-ages website, which provides information on regional drug shortages.1
In addition to tracking shortages that can affect the organiza-tion’s supplies, the action plan should address these areas:■ Documenting drug shortages and approving alternatives todrugs that are unavailable or in short supply■ Monitoring adverse drug events to determine whether any mayhave been caused by shortages■ Keeping the quality improvement and pharmacy and therapeu-tics committees informed of any shortages■ Providing an annual report on shortages and their impact on the organization to its leaders.
Information about drugs in short supply or substitute drugsmust be communicated to clinical staff. All ordering providers mustknow what drugs are in short supply, when regular distribution ofthem will resume, what alternatives or substitutes are available, andbasic information on each alternative drug, including its current for-mulations, contraindications, and potential for error.
To keep clinical staff informed about any shortages and the orga-nization’s planned response, it should consider posting updates on anIntranet site available to clinical staff at all times, suggests Neumann.In addition, it should ensure that a pharmacist is available to clinicalstaff to answer any questions. Components of the organization’s healthIT system—EHR systems, electronic drug ordering, and electronicmedication administration records—must be kept up-to-date as drugavailabilities change. Although time-consuming, system updates arevital for preventingmedication errors,says Neumann.
Reference1. FDA’s website on drug shortages is athttp://www.fda.gov/Drugs/DrugSafety/DrugShortages/default.htm. ASHP’s website is at http://www.ashp.org/shortages.
For related information, see www.ecri.org.
PIAA 3Q 2014 Features_Layout 1 8/8/14 2:54 PM Page 6

I N S I D E M E D I C A L L I A B I L I T Y 28 T H I R D Q U A R T E R 2 0 1 4
Martin Lippiett is VicePresident of Business
Consulting, Delphi Technology, Inc.
The main news
item, a few months
ago, was the failure
of the Affordable
Care Act website to
perform as intend-
ed. There were
many reasons for
this, and each
failed project has
its own story. But
the following fac-
tors are almost
always in play, to
varying degrees,
when the implemen-
tation of an enter-
prise-level system
ends up in trouble.
The “Seven Deadly Sins” of Large-Scale IT Project Management
B Y M A R T I N L I P P I E T T
F E A T U R E S T O R Y
PIAA 3Q 2014 Features_Layout 1 8/8/14 2:54 PM Page 7
Poor governance
This is probably the number-one reason why projects fail. Theproject is begun without an adequate and achievable planwith respect to requirements, budget, and resources. Then, asthe work continues, control over changes in the plan is poorlymanaged, and mid-course corrections are made with politics,
face-saving, extreme optimism, and other undesirable considerationsassuming priority in decision-making.
The keys to effective project governance are these: ■ It’s critical to incorporate scenario modeling into the initial pre-project analysis, so that different options can be evaluated and the one
that is most realistic—and shows optimal benefits—is selected. Inother words, make sure the project you are planning in the first place isthe right one for the business.■ Project criteria, roles, processes, and outcomes must be estab-lished early and then actively monitored to enhance project success.Have an escalation strategy in mind; nothing goes exactly as planned.■ Governance must be accepted and supported by all levels of management.■ Warning signs should be recognized and effective action takenearly to avoid a snowballing failure.
Changes in scope and budget If the content of the project can be easily changed, the rate of changewill in time exceed the rate of progress. When this happens, the proj-ect managers have in effect abandoned the plan established at the out-set, and the new plan will be compromised with short cuts, and expedient thinking, often done in a futile attempt to accomplish theimpossible.
The work plan should be reviewed regularly, to track progressagainst time and budget. To do this effectively, on a project that hashundreds of tasks and dozens of participants, project planning andtime tracking software is essential. Where there is slippage, the criticalpath must be identified, and corrective action should be taken as soonas possible.
These are some of the tell-tale signs of a project in trouble:■ There are small variances in schedule or budget that gradually getbigger over time; this is especially concerning in the early days.■ Activities noted as complete still are in fact being worked on.■ Team morale, quality, and service start to slide.■ Time allotted for quality control and project management gets cutback, to make up for lost ground.
Poor communication between business users and IT A sustained focus on the value of the project to the company is essen-tial, and any turf issues need to be put aside. The IT staff shouldremember to talk to the user community in business, not technical,terms. Project plans should be based on facts and business metrics,not opinions and assumptions, about the current status of the enter-prise, as well as the objectives of the new project.
Gaining insight upfront from a variety of internal resources isessential for creating a project plan that encompasses all aspects of thebusiness. Without that input, tools and processes may be developedthat are incomplete or even unnecessary; also, the inclusion of usersearly on encourages buy-in to the project.
Unclear expectations If expectations about the project are in any way ambiguous, whatmight start out as a minor piece of work could expand into a major
I N S I D E M E D I C A L L I A B I L I T Y 29 T H I R D Q U A R T E R 2 0 1 4
PIAA 3Q 2014 Features_Layout 1 8/8/14 2:55 PM Page 8

I N S I D E M E D I C A L L I A B I L I T Y 30 T H I R D Q U A R T E R 2 0 1 4
undertaking. Expectations not onlydefine the final outcome; they also affectthe process of getting there. If some ofthose working on a project worry thatexpectations will not be met, the projectwill become a lot harder to manage.
The first step in expectation-set-ting is to ensure that the project’s deliv-erables are actually going to meet therequirements of the project. Failure to doso means an unsuccessful project. Butthe need to manage stakeholder expec-tations goes beyond the delivery of spec-ified requirements: It covers all aspectsof a project’s work and the manner inwhich it's accomplished. The next stepis to map the expectations of the keystakeholders. This requires carful listen-ing and the ability to decipher what'smeant, not just what's said.
Expectations generally will fall into two groups—the realistic andthe unrealistic. But even the realistic expectations need managing; theymust be fulfilled, and the stakeholder must be made aware that theyhave been met. Communication requires delivering the right informa-tion to the right stakeholder in the right manner. Unrealistic expecta-tions are obviously more difficult to manage, since they are unlikely tobe met. Fortunately, expectations are not fixed, but fluid; they reside ina person’s mind, and they can be influenced or changed by fact-basedcommunication.
Personnel issues Project management is one of the most challenging tasks in the mod-ern IT organization; the potential for payback makes it one of the mostimportant functions. The project management function must be ade-quately staffed, and the individuals fulfilling that function must beadequately trained. A qualified person must also be allowed the timeto do his work properly—the involvement of staff in major projects—not only the project manager, but also the users and developers. Theamount of time required is often underestimated, and managers maynot recognize the conflict that some team members face, between proj-ect work and their “everyday” duties.
In addition to selecting the right individual to lead the project,project managers should make sure that the staff engaged in it have theright credentials, with the required degree of expertise. Don’t forgetthat turnover during a project can have serious repercussions—one ofmany reasons for good documentation.
Inadequate attention to risk managementFor most software development projects, the five main risk-impactareas are: (1) the use of new and unproven technologies, (2) softwaresystem requirements, (3) software system architecture, (4) software
system performance, and (5) organiza-tional and non-functional areas.
Risk management is generally notgiven as much attention as it shouldwhen planning a project—all too oftenit’s, “Trust the project manager,” and offwe go! Risks to success should be identi-fied early in the planning stage. Forexample, the use of an emerging technol-ogy might be a risk; there are othersrelating to the competence of the team,the availability of users to articulaterequirements, the commitment to qualityassurance (QA), the relative scalability ofthe solution, reliability of a vendor, busi-ness impact, and so on. Once risks havebeen identified, they should be priori-tized, and the ownership of each shouldbe assigned to a project team member. Risks can be avoided, minimized (the
most common case), or simply accepted. Not all risks will be identi-fied ahead of time, but most can, and some preventive actions can betaken—or at least a possible response can be considered beforehand.
Inadequate QC and QAWhen projects get into trouble, the most tempting areas for shortcutsare usually the ones that are related to the quality and integrity of thedelivered software. “Hope for the best” thinking is a temptation whendeadlines have to be met.
Quality control (QC) is used to verify the quality of the output;QA is the process of managing for quality. Achieving success in a proj-ect requires both QA and QC. If only QA is applied, then there is a set ofprocesses that can be applied to ensure great quality in our deliveredsolution, but the delivered solution itself is never actually quality-checked. Likewise, if the sole focus is on QC, then tests are simply conducted without any clear vision for making them repeatable, forunderstanding and eliminating problems in testing, and for, generally,driving improvement into the vehicle used to deliver the new system.
ConclusionFinally, here are some (potentially) comforting data, from a survey byIBM, of successes and failures in 1,500 large-scale projects:■ Only 40% of projects met schedule, budget, and quality goals.■ Biggest barriers to success were listed as these:
• People factors: Changing mindsets and attitudes, 58%
• Corporate culture, 49%.
• Lack of support from senior management, 32%.■ Underestimation of complexity was listed as a factor in 35% of projects.
I T P R O J E C T M A N A G E M E N T
For related information, seewww.Delphi-Tech.com.
If the content of the project can be easilychanged, the rate ofchange will in timeexceed the rate of
progress.
PIAA 3Q 2014 Features_Layout 1 8/8/14 2:58 PM Page 9
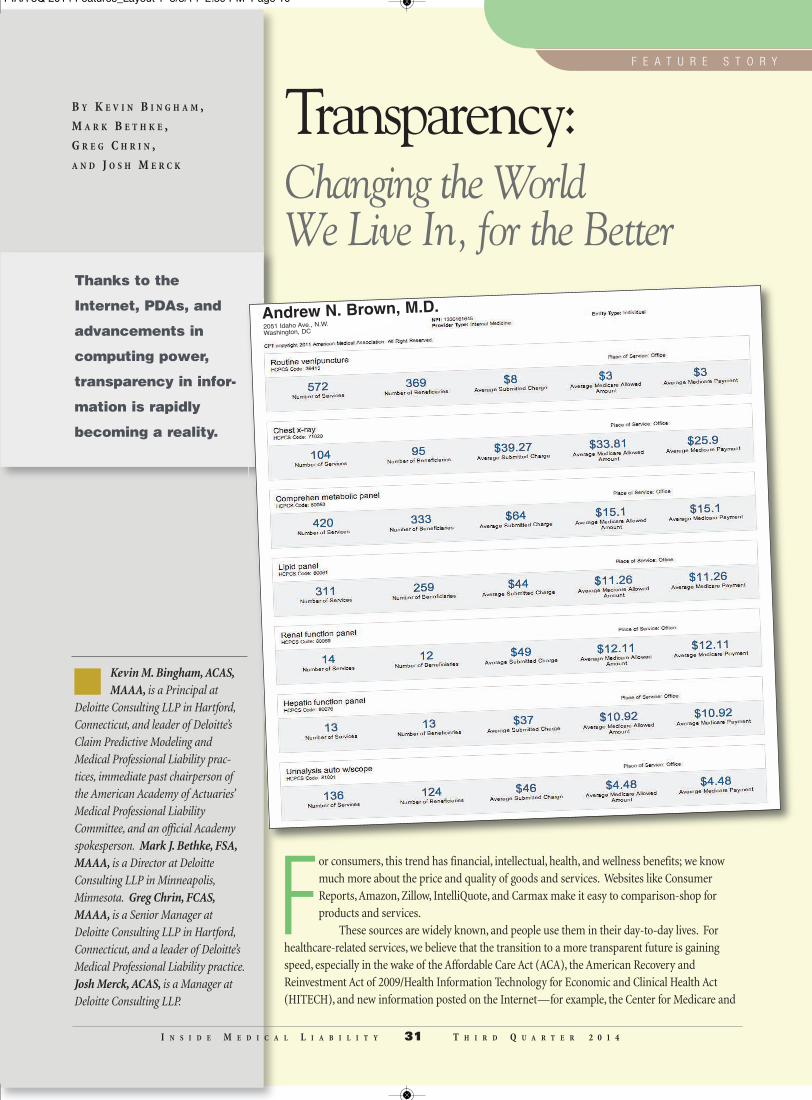
B Y K E V I N B I N G H A M ,
M A R K B E T H K E ,
G R E G C H R I N ,
A N D J O S H M E R C K
I N S I D E M E D I C A L L I A B I L I T Y 31 T H I R D Q U A R T E R 2 0 1 4
Kevin M. Bingham, ACAS,MAAA, is a Principal at
Deloitte Consulting LLP in Hartford,Connecticut, and leader of Deloitte’sClaim Predictive Modeling andMedical Professional Liability prac-tices, immediate past chairperson ofthe American Academy of Actuaries’Medical Professional LiabilityCommittee, and an official Academyspokesperson. Mark J. Bethke, FSA,MAAA, is a Director at DeloitteConsulting LLP in Minneapolis,Minnesota. Greg Chrin, FCAS,MAAA, is a Senior Manager atDeloitte Consulting LLP in Hartford,Connecticut, and a leader of Deloitte’sMedical Professional Liability practice.Josh Merck, ACAS, is a Manager atDeloitte Consulting LLP.
Thanks to the
Internet, PDAs, and
advancements in
computing power,
transparency in infor-
mation is rapidly
becoming a reality.
Transparency: Changing the World We Live In, for the Better
For consumers, this trend has financial, intellectual, health, and wellness benefits; we knowmuch more about the price and quality of goods and services. Websites like ConsumerReports, Amazon, Zillow, IntelliQuote, and Carmax make it easy to comparison-shop forproducts and services.
These sources are widely known, and people use them in their day-to-day lives. Forhealthcare-related services, we believe that the transition to a more transparent future is gainingspeed, especially in the wake of the Affordable Care Act (ACA), the American Recovery andReinvestment Act of 2009/Health Information Technology for Economic and Clinical Health Act(HITECH), and new information posted on the Internet—for example, the Center for Medicare and
F E A T U R E S T O R Y
Andrew N. Brown, M.D.2051 Idaho Ave., N.W.
Washington, DC
PIAA 3Q 2014 Features_Layout 1 8/8/14 2:59 PM Page 10
Medicaid Services’ (CMS) release of information on 880,000 distincthealthcare providers in April of this year1 and the 100 most frequentlybilled discharges at more than 3,000 hospitals in May of 2013.2
This article explains how transparency in healthcare may welltransform our lives.
Forces at workAchieving transparency in the healthcare market has been an uphillbattle for consumers, for many years. Before the spike in numbers ofhigh-deductible plans, most healthcare consumers in America probablydidn’t pay much attention to the cost of visiting a doctor’s office orambulatory care center. The small percentage of consumers who didtry and figure it out were likely to be confused about how health servic-es are priced and what they had actually paid for the diagnoses andtreatments they received.
However, many Americans have switched to high-deductibleplans, wherein a significant amount of first-dollar costs are born bypatients. Consumers are learning that a visit to the doctor’s office or theemergency room can be quite expensive. Now, armed with apps/web-sites like Yelp, Healthgrades, myHealthcare Cost Estimator, SmartPatient, and state-sponsored sites like New Hampshire Health Cost, con-sumers are becoming savvy buyers of healthcare. Just as the availabilityof information changed the way we buy cars (i.e., transparency on pricehas replaced the “let me ask the manager” haggle), we believe thattransparency in this market will, in time, transform the discussionbetween consumers and hospitals and physicians.
The ACA states: “(c) STANDARD HOSPITAL CHARGES—Eachhospital operating within the United States shall for each year establish(and update) and make public (in accordance with guidelines developedby the Secretary) a list of the hospital’s standard charges for items andservices provided by the hospital, including for diagnosis-related groupsestablished under section 1886(d)(4) of the Social Security Act.”3
We believe that this is definitely a step in the right direction!
States taking actionIn the short term, we expect to see a gradual increase in both federal- andstate-level efforts to enhance transparency. Some states have passed lawsrequiring that healthcare providers either report information to a central
repository or be able to answer consumer queries about their prices, byprocedure. The breadth, depth, and relative effectiveness of these lawsvary, but there is no doubt that states are making strides toward a trans-parent future, in the name of reducing costs and improving patient out-comes. One state, New Hampshire, has required that all providers reportinsurance-claim payments to an All Payer Claims Database. This data-base supplies the information for a website, NH Health Cost, where anyconsumer can search for costs by provider based on zip-code radius andprocedure type (e.g., get a detailed cost estimate for outpatient arthro-scopic knee surgery within 50 miles of Zip Code 03302).
In North Carolina, Section 131E-212.7 of the Health Care CostReduction and Transparency Act of 2013 addresses disclosure of pricesfor the most frequently reported Diagnostic Related Groups (DRG),Current Procedural Terminology (CPT), and Health Care CommonProcedure Code System (HCPCS) codes. Beginning on June 30, 2014,and quarterly thereafter, each hospital must disclose, to the Departmentof Health and Human Services, the amount charged to a patient foreach DRG, average negotiated settlements, Medicaid reimbursementsfor each DRG, etc. In addition, hospital and ambulatory surgical facili-ties must provide information on the total cost for the 20 most com-monly performed surgical procedures and the 20 most commonly usedimaging procedures, by volume, that are performed in hospital outpa-tient settings or in ambulatory surgical facilities, along with the relatedCPT and HCPCS codes.4
In 2012, Massachusetts added a new Chapter 224 titled An ActImproving the Quality of Health Care and Reducing Costs ThroughIncreased Transparency, Efficiency and Innovation, which becameeffective January 1, 2014.5 Section 206 of the law requires that all man-aged care health insurance carriers “establish a toll-free telephone num-ber and website” so that insureds can find out the “estimated or maxi-mum allowed amount or charge” and out-of-pocket cost that theinsured member [consumer] shall be responsible to pay for a proposedadmission, procedure, or service. Carriers are encouraged to do this inconsumer-friendly ways and are generally expected to respond topatients’ queries within two business days.
Hospitals taking the leadSome hospitals and healthcare providers have also been early adopters
I N S I D E M E D I C A L L I A B I L I T Y 32 T H I R D Q U A R T E R 2 0 1 4
T R A N S P A R E N C Y I N H E A L T H C A R E
In 1989, the Health Commissioner of NewYork, Dr. Mark Chassin, required that all
hospitals disclose their death rates aftercoronary artery bypass graft (CABG) proce-dures. In this way, New York became the firststate to measure and share information onhospital CABG performance. The programidentified hospitals with significantly higher
mortality rates (e.g., one hospital had an18% mortality rate) and informed con-sumers that surgeons with low volumes ofCABG procedures were linked with a mortal-ity rate that was four times higher than thestate average.
As a result of New York’s push for trans-parency during the first four years of New
York’s public reporting program, deathslinked with CABG fell by 41%.
Marty Makary, MD, noted in his bookUnaccountable: “Introducing transparency toNew York’s heart centers brought somethingvery novel and powerful to health care: pub-lic accountability.”Source: Unaccountable, by Marty Makary, MD
The Power of Transparency
PIAA 3Q 2014 Features_Layout 1 8/8/14 2:59 PM Page 11

I N S I D E M E D I C A L L I A B I L I T Y 33 T H I R D Q U A R T E R 2 0 1 4
of transparency.In an article in The Blaze magazine, “Free Market at Work: Okla.
City Hospital Causes Bidding War by Posting Surgery Prices Online,” wesee what happens when people find out about the actual cost of surgery.6
For the past five years, the Surgery Center of Oklahoma has been post-ing surgery prices online. Since then, the center’s owners have noticedsome interesting things about the market for surgical procedures: first,their costs were much lower than those of their competitors (e.g., one-sixth to one-eighth the cost); second, people were willing to travel a longway to get treatment at a lower price (e.g., from Canada); and third, theyhad had a deflationary effect on prices, as their competitors were forcedto match the center’s prices.
There’s also been pressure on prices from outside the U.S., drivenby lower-priced foreign hospitals and medical tourism. According toPatients Beyond Borders, it is estimated that 1.2 million Americans willtravel to foreign countries for medical services each year.7 There aremany issues involved in traveling outside the U.S. to get care, but thedifferences in costs are substantial enough that some patients are will-ing to deal with those issues. It is not uncommon to see magazine adshighlighting how Americans can save 50% to 80% on quality medicalcare in locations such as Mexico, the Bahamas, Costa Rica, India,Singapore, Thailand, and Jordan. Although many of us might prefer tobe treated in the U.S., the new price transparency helps consumersmake the best overall choice for themselves.
Evolution of quality metrics in risk-based contracting The last several years have seen major advances in the field of qualitymetrics. With the emergence of the star quality-rating system forMedicare Advantage plans,8 which arose from the ACA, quality metricsnow plays a lead role in payer and provider contracting. The star quali-ty-rating system was developed to educate consumers on healthcarequality and to make the data included in the metrics more transparent.Further, it provided quality bonuses to higher-scoring plans and alsohelps lower member premiums.
Then, CMS Medicare Shared Savings Program (MSSP) account-able care organizations (ACOs) developed their own set of quality met-rics.9 To be eligible for CMS Shared Savings, an ACO must report on the33 quality standards, and meet prescribed quality-performance thresh-olds for each of four quality domains:■ Patient/caregiver experience (seven measures)■ Care coordination/patient safety (six measures)■ Preventative health (eight measures)■ Measures for 12 at-risk populations (e.g., diabetes, hypertension,ischemic vascular disease, heart failure and coronary artery disease).
With Medicare taking the lead, it’s not surprising that quality met-rics have become a more common feature in commercialpayer/provider contracts that contain some form of gain and/or risksharing of financial results. These quality metrics are often some varia-tion of, or slight deviation from, those used in the STAR program for
Medicare Advantage plans or the ACOs metrics. Organizations need tobe able to track, report on, and exceed at these metrics, to become eligi-ble for the financial savings they are striving for, and all of this adds anextra layer of administrative complexity and additional risk.
ConclusionAs healthcare providers become more transparent about costs, prices,and even outcomes, the demand for their various services will likelychange as well. After the release of the first CABG mortality rates inNew York, the hospitals reporting the worst mortality needed to doalmost everything in their power to improve their performance in heartoperations. For the hospital that had reported the 18% mortality rate,changes in their medical staff and internal review processes, over theyears, ultimately decreased their observed mortality rate to less than1%, based on 2009–2011 hospital and surgeon outcomes for isolatedCABG data.10 That is 18 times lower than in their pre-reporting days,back when there was no transparency on outcomes after CABG procedures. Thus: the power of transparency at work!
As ACOs mature, the types of patients seen, the types of proceduresperformed, the use of defensive medicine, and even in what is used toreach their patients will evolve, as more information is made available topatients. Depending on whether healthcare providers lead from thefront with transparency, or become late adopters because of necessity,the decision is in their hands. As we have observed in virtually everyindustry over time, the physicians, hospitals, and surgical centers thatcan provide the highest-quality service at the lowest price will eventuallygain a competitive advantage, in a marketplace where information flowsmore freely. As Gary Hamel and C.K. Prahalad observed in Competingfor the Future, “One doesn’t get to the future first by letting someone elseblaze the trail.” Transparency is already all around us. It’s just a matterof making sure yourorganization is one of thetrailblazers.
References1. http://www.cms.gov/Newsroom/MediaReleaseDatabase/Press-releases/2014-Press-releases-items/2014-04-09.html. 2. http://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/Medicare-Provider-Charge-Data/Inpatient.html. 3. http://www.gpo.gov/fdsys/pkg/BILLS-111hr3590enr/pdf/BILLS-111hr3590enr.pdf. 4. http://www.ncdhhs.gov/dhsr/ahc/pdf/memo082913.pdf. 5. https://malegislature.gov/Laws/SessionLaws/Acts/2012/Chapter224. 6. http://www.theblaze.com/stories/2013/07/12/free-market-at-work-okla-city-hospital-causes-bidding-war-by-posting-surgery-prices-online/#.7. http://www.patientsbeyondborders.com/medical-tourism-statistics-facts. 8. http://www.medicare.gov/Publications/Pubs/pdf/11226.pdf. 9. http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/sharedsav-ingsprogram/index.html?redirect=/. 10. http://www.health.ny.gov/statistics/diseases/cardiovascular/heart_disease/docs/2009-2011_adult_cardiac_surgery.pdf.
For related information, seewww.deloitte.com.
PIAA 3Q 2014 Features_Layout 1 8/8/14 2:59 PM Page 12

I N S I D E M E D I C A L L I A B I L I T Y 34 T H I R D Q U A R T E R 2 0 1 4
F E A T U R E S T O R Y
Medical professional liability (MPL) insurers have
enjoyed operating success over the last decade.
However, accident-year results are beginning to
deteriorate, and MPL specialists face a challeng-
ing operating environment that could lead to larger
underwriting losses in the future, as well as an
erosion of capital.
B Y G E R R Y G L O M B I C K I
Enterprise Risk Management for MPL Specialists
Primary threats to MPL underwriters include a persistentlyweak pricing environment that contrasts with the hardeningmarket noted in the U.S. commercial lines market for the lastthree years and challenges in various states that would over-turn legislative reforms that have helped stabilize loss severity
over time. Also, with the implementation of the Affordable Care Act(ACA), healthcare providers are organizing their practices and obtain-ing liability coverage in new ways.
Property/casualty insurers continue to incorporate enterprise risk management (ERM) into their risk and strategic managementpractices. For MPL specialists, adopting a more disciplined approachto risk management and planning can provide benefits in assessingstrategic options, preserving capital, and reducing volatility in performance.
What’s included in ERMERM is a process of systematically identifying, measuring, managing,controlling, and reporting on the various risks to which an organiza-
tion is exposed.ERM empha-sizes risk evalu-ation on anenterprise, oraggregate, level, rather than in isolated departments or business func-tions. Considering risks on an individual basis ignores the potentialfor interaction of risks that may seem unrelated but, in extreme events,may impact each other.
The ability to measure and assess risk is essential for effectivemanagement. For less quantifiable exposures, such as regulatory andreputational risks, insurers are utilizing risk dashboards more fre-quently, to consider the nature of the exposure and promote effectivemonitoring and risk mitigation. Assessment of operational risks canmake it easier to develop contingency plans for recovery from naturaldisasters or information-systems failures. Stress-testing analysis isused to assess the potential impact of individual events, or a conflu-ence of events, on capital.
Over time, more sophisticated risk measurement tools havedeveloped for insurers. Economic capital models have become increas-Gerry Glombicki, CPA, is Director, Fitch Ratings.
PIAA 3Q 2014 Features_Layout 1 8/8/14 2:59 PM Page 13

I N S I D E M E D I C A L L I A B I L I T Y 35 T H I R D Q U A R T E R 2 0 1 4
ingly popular as tools that can help analyze risk on an integrated basis.Economic capital models can provide unique insights into the keyfinancial risks that an insurer faces and its ability to withstand anadverse confluence of events. These capital models look at all of themajor risks in an integrated fashion, using a stochastic simulationprocess that weighs the interconnectedness of risks and gives weight tothe impact of diversification.
The outcome of ERM activity provides insights that can help anorganization in establishing risk limits and tolerances for its variousoperating areas and in allocating capital more efficiently. Over thelonger term, information garnered from ERM processes may promptadjustments in a company’s risk profile in several areas, including:■ Product terms■ Business mix■ Claims and reserving processes
■ Asset allocation.
While the ultimate success of an ERM endeavor may prove difficult tomeasure, its essential worth hinges on limiting large losses and reduc-ing volatility of earnings to boost risk-adjusted returns on capital.
New requirements for risk reporting As insurance risk management practices evolve, so does the number ofcompliance and reporting requirements that insurers must deal with.The NAIC’s Solvency Modernization Initiative (SMI) includes theadoption of the Own Risk and Solvency Assessment (ORSA), which ismanagement’s self-assessment of the insurer’s risk management andcorporate governance framework.
Unlike historical regulatory reporting, ORSA represents an ongo-ing review of risk exposures and capital adequacy. Insurers must
Insurershave begunto makegood use of riskdashboards.
PIAA 3Q 2014 Features_Layout 1 8/8/14 3:00 PM Page 14

describe the elements of their ERM framework and ORSA results in anannual “Summary Report.” Three key sections (1) describe an insurer’srisk management framework, (2) provide the insurer’s risk exposureassessment, and (3) show the company’s evaluation of its risk capitaland future solvency.
Looming in the near future are more comprehensive risk-report-ing requirements; these are spurring more insurers to embrace andexpand their ERM practices. The first ORSA reports are required in2015, but a number of insurers participated in 2013 pilot projects withthem. The smaller MPL specialists will not be included in the initialORSA reporting requirements, but it is likely that the ORSA mandatewill expand over time.
MPL more volatile than other casualty segmentsA review of multi-year results for assessing volatility, by business seg-ment, in underwriting and loss reserves reveals that the MPL, claims-made, segment is the second-most-volatile major P/C product line(from the standpoint of underwriting profits/losses and reserves),
exceeded only by product liability, occurrence and well ahead of othervolatile segments, including workers’ compensation and other liability,occurrence (Figure 1).
A deeper look at historical industry accident-year underwritingexperience in the MPL, claims made, line provides a vivid portrait ofhow volatile this business truly is (Figure 2), with periods of verystrong underwriting profits, as well as severe and extended losses.From 1987–2011, the developed accident-year loss and loss adjustmentexpense (LAE) ratio ranged from 47% to 125%.
Loss reserve experience, as measured by the change in loss ratiofrom initial estimates to the latest reported estimate, reveals just howdifficult it is to estimate claims costs in a long-tail line that has sub-stantial litigation-related exposures. In the most extreme cases, from accident year 1987 to accident-year 2011, the P/C industry-reported incurred losses, for an individual underwriting period, wereadjusted over ten years of development by 37%, favorably, and 25%,unfavorably.
Changes in risk selection, geographic mix, pricing, and under-writing practices and policy form may offer some opportunities
I N S I D E M E D I C A L L I A B I L I T Y 36 T H I R D Q U A R T E R 2 0 1 4
E R M F O R M P L
Figure 2 MPL Claims Made—Historical Accident Year Results
Figure 1 Average Loss Ratio Volatility vs. Reserve Volatility by Segment
Figure 3 MPL Underwriters—RBC and Leverage Trends
Figure 4 MPL Underwriters Prism Results Gross Target Capital Distribution
Source: SNL Financial, Fitch. Source: SNL Financial, Fitch. Note: P/C Industry Aggregate
Loss Ratio Change (Original vs Latest Reported)Latest Loss Ratio
Aver
age
Loss
Res
erve
Vol
atili
ty
Source: SNL Financial. Note: RBC - Risk-based capital. Source: SNL Financial. Fitch Ratings.
Average Loss Ratio Volatility
RBC (Left Axis) Operating Leverage (Right Axis) Net Leverage (Right Axis)
Other7%
Reinsurance3%
Investments11%
Operational Risks8%
Underwriting24%
Reserves47%
PIAA 3Q 2014 Features_Layout 1 8/13/14 2:18 PM Page 15
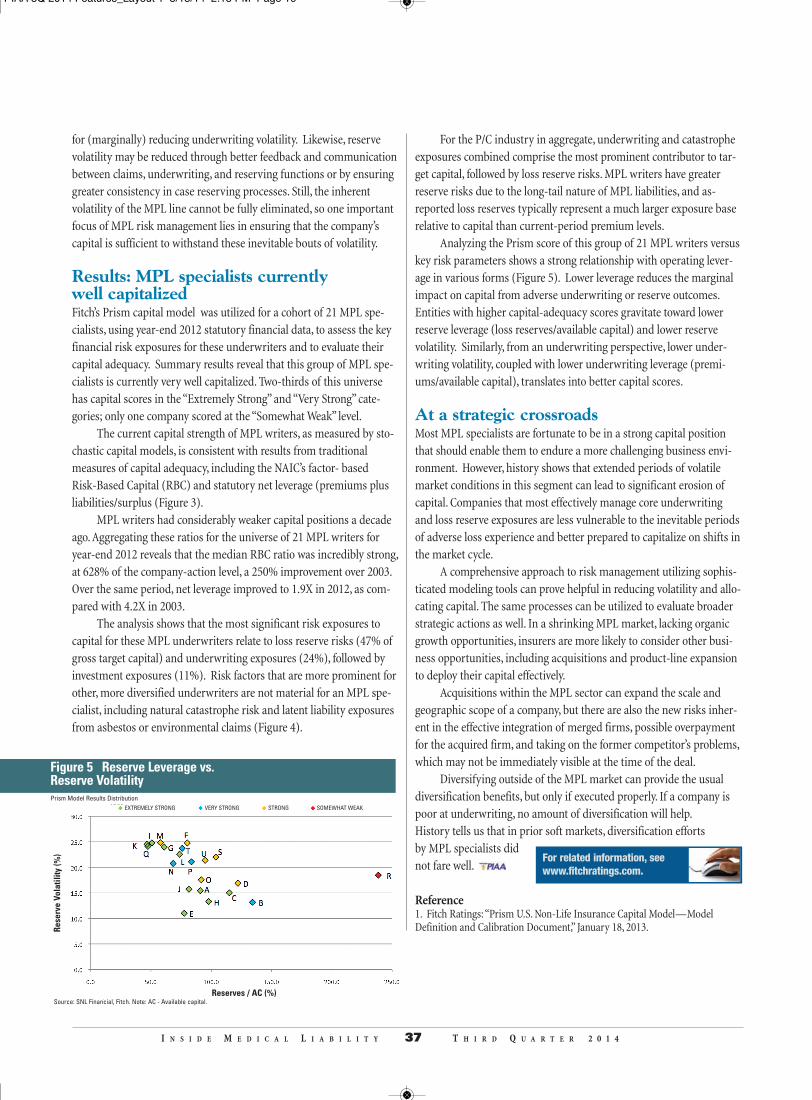
for (marginally) reducing underwriting volatility. Likewise, reservevolatility may be reduced through better feedback and communicationbetween claims, underwriting, and reserving functions or by ensuringgreater consistency in case reserving processes. Still, the inherentvolatility of the MPL line cannot be fully eliminated, so one importantfocus of MPL risk management lies in ensuring that the company’scapital is sufficient to withstand these inevitable bouts of volatility.
Results: MPL specialists currently well capitalized Fitch’s Prism capital model was utilized for a cohort of 21 MPL spe-cialists, using year-end 2012 statutory financial data, to assess the keyfinancial risk exposures for these underwriters and to evaluate theircapital adequacy. Summary results reveal that this group of MPL spe-cialists is currently very well capitalized. Two-thirds of this universehas capital scores in the “Extremely Strong” and “Very Strong” cate-gories; only one company scored at the “Somewhat Weak” level.
The current capital strength of MPL writers, as measured by sto-chastic capital models, is consistent with results from traditional measures of capital adequacy, including the NAIC’s factor- based Risk-Based Capital (RBC) and statutory net leverage (premiums plusliabilities/surplus (Figure 3).
MPL writers had considerably weaker capital positions a decadeago. Aggregating these ratios for the universe of 21 MPL writers foryear-end 2012 reveals that the median RBC ratio was incredibly strong,at 628% of the company-action level, a 250% improvement over 2003.Over the same period, net leverage improved to 1.9X in 2012, as com-pared with 4.2X in 2003.
The analysis shows that the most significant risk exposures tocapital for these MPL underwriters relate to loss reserve risks (47% ofgross target capital) and underwriting exposures (24%), followed byinvestment exposures (11%). Risk factors that are more prominent forother, more diversified underwriters are not material for an MPL spe-cialist, including natural catastrophe risk and latent liability exposuresfrom asbestos or environmental claims (Figure 4).
For the P/C industry in aggregate, underwriting and catastropheexposures combined comprise the most prominent contributor to tar-get capital, followed by loss reserve risks. MPL writers have greaterreserve risks due to the long-tail nature of MPL liabilities, and as-reported loss reserves typically represent a much larger exposure baserelative to capital than current-period premium levels.
Analyzing the Prism score of this group of 21 MPL writers versuskey risk parameters shows a strong relationship with operating lever-age in various forms (Figure 5). Lower leverage reduces the marginalimpact on capital from adverse underwriting or reserve outcomes.Entities with higher capital-adequacy scores gravitate toward lowerreserve leverage (loss reserves/available capital) and lower reservevolatility. Similarly, from an underwriting perspective, lower under-writing volatility, coupled with lower underwriting leverage (premi-ums/available capital), translates into better capital scores.
At a strategic crossroadsMost MPL specialists are fortunate to be in a strong capital positionthat should enable them to endure a more challenging business envi-ronment. However, history shows that extended periods of volatilemarket conditions in this segment can lead to significant erosion ofcapital. Companies that most effectively manage core underwritingand loss reserve exposures are less vulnerable to the inevitable periodsof adverse loss experience and better prepared to capitalize on shifts inthe market cycle.
A comprehensive approach to risk management utilizing sophis-ticated modeling tools can prove helpful in reducing volatility and allo-cating capital. The same processes can be utilized to evaluate broaderstrategic actions as well. In a shrinking MPL market, lacking organicgrowth opportunities, insurers are more likely to consider other busi-ness opportunities, including acquisitions and product-line expansionto deploy their capital effectively.
Acquisitions within the MPL sector can expand the scale andgeographic scope of a company, but there are also the new risks inher-ent in the effective integration of merged firms, possible overpaymentfor the acquired firm, and taking on the former competitor’s problems,which may not be immediately visible at the time of the deal.
Diversifying outside of the MPL market can provide the usualdiversification benefits, but only if executed properly. If a company ispoor at underwriting, no amount of diversification will help. History tells us that in prior soft markets, diversification efforts by MPL specialists didnot fare well.
Reference1. Fitch Ratings: “Prism U.S. Non-Life Insurance Capital Model—ModelDefinition and Calibration Document,” January 18, 2013.
For related information, seewww.fitchratings.com.
I N S I D E M E D I C A L L I A B I L I T Y 37 T H I R D Q U A R T E R 2 0 1 4
Figure 5 Reserve Leverage vs. Reserve Volatility
Rese
rve
Vola
tility
(%)
Source: SNL Financial, Fitch. Note: AC - Available capital.Reserves / AC (%)
Prism Model Results DistributionEXTREMELY STRONG VERY STRONG STRONG SOMEWHAT WEAK
PIAA 3Q 2014 Features_Layout 1 8/13/14 2:18 PM Page 16

I N S I D E M E D I C A L L I A B I L I T Y 56 T H I R D Q U A R T E R 2 0 1 3
Don’t Miss the PIAA Fall Workshops!
October 1-3, 2014Underwriting WorkshopOmni San DiegoSan Diego, California
September 10–12, 2014 Technology, HumanResources, and FinanceWorkshop Fairmont Olympic HotelSeattle, Washington
November 5–7, 2014 Claims and PatientSafety/Risk ManagementBaltimore Marriott Waterfront HotelBaltimore, Maryland
Visit sunny San Diego! It boasts a new city center, world-class museums, the world-famous San Diego Zoo, and more than 70 miles of beautiful coastline.
■ Featured speakers:
Melissa Joy Roberts, JD, MSN,FNPBC, Associate Dean, UMKCSchool of Nursing and HealthStudiesSession: The Expanding Role of
Advanced Practice Nurses
Daniel P. Groszkruger, JD, CPHRM,DFASHRM, Principal, President &CEO, rskmgmt.incSession: Electronic Medical Records =Safer, Better, Cheaper? Not So Much!
Other sessions include:
■ Understanding Error and Mitigating Injuryand Loss in Diagnostic Imaging. Diagnostic error in medical imaging can be broadly categorized aserrors of perception, of interpretation, and of communication. All threecan result in injury and loss. This session will examine the MPL costsassociated with these several types of errors, the human factors thatgive rise to them, and potential strategies to mitigate them.
■ The da Vinci Robot: The Rest of the Story.Today, the volume of procedures performed with the assistance of theda Vinci Robot has significantly increased, which suggests a criticalquestion, “How have PIAA companies fared with this new technolo-gy?” The speaker will share the latest news about the da Vinci robot,including the surgical specialties that have adopted it, rates of com-plications, product defects, and the strategies employed by plaintiff’sattorneys who have dedicated their practices to patients who haveallegedly been harmed during robot-assisted surgical procedures.
Come to Baltimore and you will be charmed by Harbor East, a spectacular stretch of waterfront just east of Balti- more’s Inner Harbor that features dining, entertainment, great shopping, and more!
■ Featured speakers:
Michael J. Gerardi, MD, FAAP,FACEP, President, American Collegeof Emergency PhysiciansGeneral session: CommonComplaints/Catastrophic Outcomes
Dean F. Sittig, PhD, Professor,Biomedical Informatics, University of Texas Health Science Center atHoustonGeneral Session: EMRs: How to UseThem with Maximum Safety
Other sessions include:
■ Claims: Why Winners Win: The Why, When, and What of Witness Preparation. This session will focus on the application of a research-basedapproach to the why, when, and what of witness preparation.Research shows that juries decide first about the person (usually thedefendant) and then decide which side’s experts they will rely on forunderstanding the medicine involved in the case. How the witnesshandles the plaintiff’s attorney on cross-examination is crucial towhether the jury will give the defendant the benefit of the doubtabout what transpired with the medical care provided in the case.And this is the point when the witness needs to be at his best—because the way he presents himself is crucial to the success of the trial.
■ Patient Safety/Risk Management: mHealth:Claims, Patient Safety, and Risk ManagementRamifications. Among the many drivers of potential lawsuits against physicians,mobile/smart phones and electronic medical records (EMRs) haveassumed a new importance recently. This session will demonstratehow some adverse outcomes may occur because of basic errors intreatment and/or dysfunctional office systems. In addition, with theadvent of mobile healthcare technology and its integration with EMRs,there are new issues for patient safety and MPL claims.
Seattle, the “Emerald City,” is two cities in one! It’s a world-class metropolis—featuring the Space Needle and a monorail—that is set within the shadow of stunning Mount Rainier!
■ Featured speakers:
Jamie Naughton, Speaker of theHouse/Employee EngagementStrategist, Zappos.comKeynote session: Building a Brand That Matters
Spence Byrum, Managing Partner, Convergent, HRS, LLCGeneral session: New Strategies for THRF Leaders
Other sessions include:
■ Information Technology: Integrating CloudServices into Your Computing Environment. How do you get started in working with the cloud? In this session,you will learn the nuts-and-bolts of what you need to do to inte-grate cloud services like AWS and Azure into an existing computingenvironment. You will find out how servers, storage, and databasesare provisioned; how to decipher the pricing models; and somepractical suggestions for your first cloud projects.
■ Finance: MPL Industry Results andInvestment Market Opportunities. This session will present an overview of the current investment mar-ket as this pertains to PIAA companies, and will also offer a lookahead to some developing trends. It will provide detailed numberson the year-over-year financial performance for the MPL industry,and discuss some of the essential considerations in developingportfolio strategies.
■ Human Resources: Legal Update: SocialMedia, Employee Leave, and More! Human resources professionals are continuously challenged tokeep abreast of evolving legal requirements when making personneldecisions. This session will identify what is, and is not, employeeprotected activity, including specific guidance on employee use ofsocial media, and help attendees understand when an employee’sleave can be lawfully terminated, while feeling confident that theyare in compliance with the Fair Labor Standards Act. The speakerwill also explore other current legal pitfalls for HR professionals.
Information and strategies that will help you succeed in MPL!
To view the complete agendas for any of these workshops, or to register online, go to www.piaa.us.
PIAA 3Q BACK 2014_Layout 1 8/8/14 12:36 PM Page 1

I N S I D E M E D I C A L L I A B I L I T Y 39 T H I R D Q U A R T E R 2 0 1 4
Q:How have captives traditionallygone about earning investmentincome?
A: Captives have traditionallyearned their investment incomethrough the acquisition of U.S.Treasury bonds. This type of invest-ment is typically viewed as “safe,”provides a reasonable amount ofreturn, and satisfies domicile regula-tions, since they are relatively easy toturn back into cash to pay claims,should the need arise. Unfortunatelyfor these captives, recently, thisinvestment strategy has not beenproviding the rate of return that hasbeen expected or desired. Typical10-year long-term Treasury rateshave historically averaged around6.5%; at the end of 2013, the rate ofreturn (ROR) was less than 3%, and
it has been projected to remain thesame for the duration of 2014.
Q: Have you seen any changes inthe way that captives haveapproached their investments, inlight of this recent performance?
A: Given the low productivity of
Treasury bonds, captives have beenexploring alternate investmentstrategies, for example: intercompa-ny loans (loan-backs), hedges, realestate trusts, etc. For captives, thereis no one-size-fits-all investmentstrategy, as the investments depend
on the size of the reserve fund, therisk appetite of the captive owner,and the minimum capital require-ments of the domicile. Keep in mindthat investments are approved bythe domicile regulators to ensurethat a loss of capital doesn’t nega-tively impact the captive’s ability topay claims.
A good captive manager shouldbe able to put the necessary pieces inplace to present a captive owner withmultiple investment options that fitits appetite for risk and targetedROR, all while working with theapplicable regulators to ensure com-
pliance with domicile requirementsand the solvency of the captive.
Q:Are there risks, for captives, innot achieving a stipulated rate ofreturn on investments? Or, arereturns sufficiently separated, asfinancial items, from insurance-related aspects like premiums and
reserves, which are usually actuari-ally determined?
A: Well-managed captives havetheir premiums and associatedreserves actuarially determined onan annual basis. Gains in investment
Q&A WITH NATHANREZNICEK, ASSURANCEPARTNERS
Well-managed captives have their premi-ums and associated reserves actuariallydetermined on an annual basis. [ ]
Nathan Reznicek is the Client Services Coordinator atAssurance Partners. As one of the largest providers of alter-native risk transfer programs in the Midwest, AssurancePartners has particular experience designing solutions for captive companies. We wanted tofind out about the challenges that captives face in the current low-interest-rate environment,and how captives can strategize their portfolios to maximize yields within this environment.
NATHAN REZNICEK
A L T E R N A T I V E S F O R R I S K
PIAA 3Q BACK 2014_Layout 1 8/8/14 12:49 PM Page 2

I N S I D E M E D I C A L L I A B I L I T Y 40 T H I R D Q U A R T E R 2 0 1 4
income shouldn't really factor in,because the premium is determinedby the relative risk of the exposure,not the size of the reserve.
Since these items are sufficientlyseparated, the risks associated withunderperforming returns are typi-cally limited to the amount of theinvestment. This potential lossshould be considered by the captiveowner, as well as the regulator in theapproval process of the investment:neither of these entities would wantto put the captive in a positionwhere it would be unable to remainsolvent and pay claims.
Q: Are captives now moving intoequities to any significant extent?
A: It is not unusual for a captive tomake investments in equities. A typ-ical captive portfolio might actuallyclosely resemble that of an individ-ual’s 401(k) investment: T-bonds,notes, higher-grade corporate bonds,and a small amount in stocks/equi-ties. The size of the loss reserve,expected losses, and outstandingclaims all play a part in the particularpercentage of the portfolio that ismade up of equity investments.
Keep in mind that a captivecould need this money tomorrow, sothe ratio of stocks/equities (particu-larly real estate) is going to be much
lower than that of the dollars invest-ed in a more stable vehicle. Whendealing with money set aside to payclaims, the question isn’t only: “Whathappens if this investment fails?”More often, it is: “How quickly canwe get the money back to payclaims?”
Q: I was struck by the idea of a cap-tive entering the commercial lending
space. Is this happening now? Whatfactors would promote, or retard,this trend?
A: Captives have been players inthis arena for quite a while now, justin a very limited capacity. It is acommon practice (especially amongthe larger captives) to loan money tothe captive’s insureds. This practicehas a few additional complexities,
when compared with the otherinvestment vehicles a captive mightelect. In addition to ensuring captivesolvency, regulators also examine theinterest rates and payment terms setforth in the proposed agreementbetween the two entities. The inter-est rates of these loans are typicallyslightly higher than fair marketvalue rates, in order to avoid poten-tial regulatory issues. This type ofloan is attractive to the insureds,because the arrangements are notusually subject to the same level ofrestrictions that would be in placethrough a commercial lending institution.
Q: You mentioned the fact that
investment methods need to beapproved by the domicile regulators.Why is that, and are there notabledifferences in the regulations oncaptive investments, from one stateto another?
A: One of the charges that domicileregulators are tasked with is ensur-ing that the captives in their stateremain solvent. Captives fund their
investments by utilizing a portion oftheir loss reserves, which naturallyreduces the funds available to payclaims. A regulator will examine thetype of investment being proposed,and make a determination as to howthat transfer of funds will negativelyimpact the claims-paying ability ofthe captive.
Some domiciles are well-versedin the language of alternative invest-
ment strategies because their domicile is home to a substantialpopulation of massive captives withincredibly large loss reserves. Theprocess for approval through otherdomiciles could be significantlymore challenging, if they have nothad this experience. It all comesdown to how well the regulatorunderstands the proposal and howcomfortable he is with the ability ofthe captive to continue to pay claims.
Things can get very tricky quitequickly when the conversation turnsfrom U.S. to international domiciles.Some international domiciles areregulated in a fashion that is verysimilar to what is done in domesticlocations, while others are notorious
for their lack of regulation and order.A thorough review of the capabilitiesand compatibility of an internation-al domicile is very important wheninvestigating the potential home foran existing or future captive.
Q: More generally, do you thinkthat the use of cap-tives to hedge MPLrisk will expand dur-
ing the next five to ten years, and ifso, why?
A: Most definitely. Captive utiliza-tion has sustained a strong trend ofgrowth in recent years and is notanticipated to slow down. The con-cept of captive insurance is alsobecoming more widespread withinthe U.S., as more and more stateshave enacted captive legislation
(currently more than 30 states) toattract and keep this business withintheir borders.
The opportunity for an organi-zation to have full ownership of itsrisk management/transfer program,recent U.S. tax court rulings, and thecontinued trend wherein smallerorganizations are beginning to formtheir own captives would all indicatea strong trend of continued—andexpanded—captive utilization.
Q: How would you recommendthat existing and potential ownersapproach their captive investmentstrategy?
A: A captive is first and foremostan insurance company formed toprotect the interests and assets of itsinsureds; the availability of theunpaid premium dollars as a sourceof investment funds is an ancillarybenefit of proper captive operation.Find a domicile-neutral captivemanager who offers more than anjust an understanding of the liabilityside of captive—one who also has asolid grounding in best practices forthe asset side, and how to applythem.
A L T E R N A T I V E S F O R R I S K
For related information, seewww.yourassurance.com/captives.
Things can get very tricky quite quicklywhen the conversation turns from U.S. tointernational domiciles. [ ]
A captive is first and foremost an insurance company formed to protect theinterests and assets of its insureds.[ ]
PIAA 3Q BACK 2014_Layout 1 8/8/14 12:37 PM Page 3

You’ll find us listed in Best’s Directories of Recommended Insurance Attorneys andAdjusters and the Bar List Publishing Insurance Bar, Claim Services Guide, PIAA Affiliate
Defense Firm, and on the web at www.thuillezford.com
AFFILIATE PARTNER
PIAA 3Q BACK 2014_Layout 1 8/8/14 12:37 PM Page 4

I N S I D E M E D I C A L L I A B I L I T Y 42 T H I R D Q U A R T E R 2 0 1 4
Maybe mobile tech can be helpful: case study
Supported by mobile technology, trained health coaches at Elder Services of
Merrimack Valley (an Area Agency on Aging in Northeastern
Massachusetts) visit recently discharged Medicare patients in their homes
and monitored them via telephone to identify and address declines in health sta-
tus that increase the risk of readmission. Administered in partnership with area
hospitals, the four-week program begins with an in-hospital visit to determine the
risk of readmission.
Patients at medium or high risk for readmission receive an in-home visit
within 48 hours of discharge and a weekly phone call for each of the next three
weeks. During each encounter, the coach uses a tablet-based application that
provides suggested questions written in lay language based on the patient's
diagnoses, treatment, and overall risk profile. If the answers indicate a decline in health status, the system sends a real-time
alert to a nurse care coordinator, who subsequently uses a different component of the software to help the patient and coach
address the issue within 24 hours, including arranging for any needed services.
The use of health coaches supported by the tablet-based software significantly reduced readmissions among at-risk
Medicare patients, as compared with use of health coaches without the software. This reduction generated substantial cost
savings for partner hospitals and the healthcare system as a whole.
Source: AHRQ’s “Innovations “ newsletter, July 30, 2014
outtakes
Getting at the
Eleanor Kam -
Designing investment strategies to match the unique needs of medical professional liability providers.
markets
heart of the
PIAA 3Q BACK 2014_Layout 1 8/8/14 12:37 PM Page 5
I N S I D E M E D I C A L L I A B I L I T Y 43 T H I R D Q U A R T E R 2 0 1 4
Although the overall rate of IRS examinations oncorporations is at a three-year low, the focus oninsurance companies, and particularly theirdeduction of loss reserves,1 seems to be inten-
sifying. For most insurance companies, the tax deductiontaken for loss reserves is one of the largest tax benefits ontheir income tax return. As a result, this is an area offocus for the IRS, once a company comes under scrutiny.
The rulesSo what is the appropriate amount of tax loss deduction? IRS CodeSection 832(b)(5) defines losses incurred as the losses paid plus thechange in the discounted unpaid losses, less salvage/subrogation andreinsurance recoverable. Regulations Section 1.832-4(b) goes intomore detail, adding that the taxpayer must provide support that theunpaid losses represent only actual unpaid losses. These losses mustrepresent a “fair and reasonable” estimate of the amount the companywill be required to pay. The regulations alsostate that, “[T]he district director may requirean insurance company to submit detailed infor-mation with respect to its actual experience asis deemed necessary to establish the reason-ableness of the deduction.” The challenge totaxpayers is to determine what amount actuallyis “fair and reasonable.” Most taxpayers rely onthe amount of losses incurred as determined intheir National Association of InsuranceCommissioners (NAIC) Annual Statement,which is largely influenced by their annual actuarial report.
Case studyIn a recent tax court case, the IRS challenged this method. Fortunatelyfor the taxpayer, the court ruled against the IRS. In September 2013,the U.S. Tax Court ruled in favor of Acuity Mutual Insurance Company(“Acuity”), a property/casualty insurer, concurring with the companythat their loss reserve deduction was “fair and reasonable.”2 In their2006 income tax return, Acuity reported loss reserves of $660 million,which was within the acceptable range of the independent actuarialreport. As required by IRS Section 846, this amount was then discount-ed to $622 million on the tax return.
The Tax Court relied on the 7th Circuit’scase law3 (the same circuit where this case wasappealed) that the NAIC-approved annual state-ment should serve as the starting point for com-puting loss reserves. The IRS disagreed, statingthat the annual statement controls only what isincludable in loss reserves—but not the actualamount of the loss reserves themselves. The TaxCourt held that the taxpayer deducted the appro-priate amount of loss reserves, based on the rulesestablished by NAIC and Actuarial Standards ofPractice (ASOP), and asserted that they fell with-in a range of reasonable estimates determined bythe company’s appointed outside actuary.
The victory in this case was not just for thetaxpayer; it was also a win for insurance compa-nies in general, because it sets an example for therange of amounts that can be appropriately
Brandy Vannoy is a Partner with JohnsonLambert LLP, and Derek Freihaut is a Principaland Consulting Actuary with Pinnacle ActuarialResources, Inc.
LOSS RESERVES: THE IRS’ KRYPTONITEOR GOLD MINE?
BY BRANDY VANNOY AND DEREK FREIHAUT
The victory in
this case was
not just for the
taxpayer; it
was also a win
for insurance
companies in
general.
I N S I G H T S O N A C C O U N T I N G
I R S
PIAA 3Q BACK 2014_Layout 1 8/8/14 12:38 PM Page 6

I N S I D E M E D I C A L L I A B I L I T Y 44 T H I R D Q U A R T E R 2 0 1 4
deemed “fair and reasonable.” Although theAcuity case is only a Memorandum Decision ofthe Tax Court, and is therefore limited in prece-dential value, it does give insurance companiessome idea of the documentation and calcula-tions needed, based on an independent actuarialreport and NAIC and ASOP requirements, thatwould be needed to prevail against the IRS.Also, the case makes it more difficult for the IRSto assert that a company’s unpaid loss reservesinclude an “implicit margin” solely because theIRS’ actuaries determine a lower loss reserveamount.
The Acuity decision is significant in sup-porting a company’s ability to rely on its inde-pendent actuary. Acuity’s held reserves werewithin its opining actuary’s reasonable rangeand were also within the reasonable ranges as calculated by two differ-ent independent consulting actuaries, who testified in the case onAcuity’s behalf. The IRS countered, in the case, with two other actuari-al analyses that concluded that Acuity’s held reserves were outside of areasonable range.
After giving significant weight to the fact that Acuity’s heldreserves had been deemed reasonable by their independent actuaries,the Tax Court determined that Acuity had done enough to demon-strate that their held reserves were reasonable. After this determina-
tion, the court explicitly stated “our inquiryends,” and so the validity of the IRS’s actuarialreports was no longer relevant.
This is a significant result: reserve esti-mates are inevitably full of uncertainty, and it isnot uncommon to find varying results from dif-ferent actuarial analyses. This decision allows acompany to rely on its actuary’s reasonable rangeif the result is properly supported by the analysisand meets the appropriate standards of practice.This is a much more secure position to workfrom for a company; they do not have to be con-cerned about a potential duel between their actu-ary, and another opposing one, in court.
This decision also reinforces the impor-tance, for a company’s reserve analysis, of properdocumentation and adherence to the relevant
ASOPs. While managers may not be able to determine if a report ismeeting the necessary ASOPs, there are steps they can take to helpensure they are receiving a properly documented analysis. Any actuar-ial report the company receives should come from a credentialed actu-ary who is in good standing with his professional organizations andcurrent with the requisite continuing education. Best practices requirethat the actuarial report be exposed to the company board, and it isrecommended that the actuary be present in person, if possible. Thisgives management an opportunity to ask questions. Lastly, there are
I N S I G H T S O N A C C O U N T I N G
Best practicesrequire that the
actuarial report beexposed to the
company board,and it is recom-mended that the
actuary be presentin person, if
possible.
Visit us at www.wellscap.com
Wells Capital Management (WellsCap) is a registered investment adviser and a wholly owned subsidiary of Wells Fargo Bank, N.A. WellsCap
provides investment management services for a variety of institutions. For additional information on Wells Capital Management and its advisory
services, please view our web site at www.wellscap.com, or refer to our Form ADV Part II, which is available upon request by calling 415.396.8000.
WELLS CAPITAL MANAGEMENT® is a registered service mark of Wells Capital Management, Inc. 06/14
focused on institutional clients. Our diverse and autonomous teams provide a broad range of
investment solutions across multiple asset classes. We understand that managing investments
for insurance companies requires a specialized expertise to help navigate the regulatory
environment and address the unique needs of each client. We currently manage more than
$34 billion in assets for insurance companies around the world, ranging from property and
casualty to life and health.
The WellsCap advantage:
Dedicated insurance client relationship specialists, with an average of 24 years of experience.
For more information on how we can partner with you, please contact Larry Fernandes
at 415.396.0479 or [email protected] or visit www.wellscap.com.
PIAA 3Q BACK 2014_Layout 1 8/8/14 12:39 PM Page 7

I N S I D E M E D I C A L L I A B I L I T Y 45 T H I R D Q U A R T E R 2 0 1 4
often opportunities for other actuaries to review a company’s reserveanalysis. Leadership should request and review any report from a reg-ulator or an auditor that offers an opinion on the company’s actuarialreport. If these are not available, it is not uncommon to have an exter-nal peer review conducted by another independent actuary.
What the IRS will look forConsider this scenario: you open your mail and find a notice from theIRS that your company is going to be examined. What can you expectthe IRS will request in regard to loss reserves? On a typical insurancecompany exam, the IRS will request the actuarial report, AnnualStatement (including Schedule P), and the calculation of discountingfor tax purposes. As a standard request, they also ask for board min-utes. They are checking to determine how the reserves were booked inrelation to the independent actuary’s report. (We will discuss morelater on booking to range or point.) As seen in the Acuity case, theyare looking for any evidence that the loss reserves are higher than whatis “fair and reasonable.” They will examine the historic evidence to seeif the reserves have reversed and if the taxpayer has consistentlybooked to a higher estimate than actual.
In addition, they will look for trigger words in the board min-utes or actuary reports, such as “redundant” or “excess.” If the IRS con-sidered the reserves to be greater than an “estimate based on actualunpaid losses,” that estimate will likely be challenged.
The IRS has the advantage of hindsight when looking at thesereserves. In cases and exams, we have seen taxpayers successfullyargue that their reserve amounts were based on the best estimateavailable at the time, rather than with the intent of reporting an excess.Every exam and agent is different, but the important thing to be awareof is what they will be looking for in regard to loss reserves and thedocumentation needed to support the amounts claimed as your taxdeductions.
DocumentationThe amount of support necessary for a reserve estimate is detailed inthe ASOPs. The general guiding principle for an actuary is provided inSection 3.2 of ASOP 41, “Actuarial Communications”:
In the actuarial report, the actuary should state the actuarial findings,and identify the methods, procedures, assumptions, and data used by theactuary with sufficient clarity that another actuary qualified in the samepractice area could make an objective appraisal of the reasonableness ofthe actuary’s work as presented in the actuarial report.
Not every company uses their actuary’s or actuarial reports inthe same manner. ASOP 43, “Property/Casualty Unpaid ClaimsEstimates,” recognizes that it is appropriate for reserves to be provided“as a point estimate, a range of estimates, a point estimate with a mar-gin for adverse deviation, or a probability distribution of the unpaidclaim amount,” based on the intended purpose. If a company prefersto work with a point estimate or an estimate with a risk margininstead of a range, the opining actuary must still determine whetherthe held reserves make a reasonable provision for unpaid claims. It is
this determination of reasonableness in the Statement of ActuarialOpinion that a company, an auditor, the IRS, or a Tax Court will look tofirst to determine if reserves are reasonable.
One of the documents that will be helpful during an IRS examis support for how the loss reserves and losses incurred shown on theAnnual Statement translate to the amount shown on the income taxreturn. The easiest way to achieve this documentation is to prepare awork paper in conjunction with the annual tax return that shows a rec-onciliation between the components of losses incurred (losses paid,change in losses unpaid) on the Annual Statement and the lossesincurred that are deducted on the return. The main difference shouldbe the discounting of the unpaid losses as required by Code Section846, removal of any premium deficiency reserves, and any other lossreserve that is added in excess of the actuary’s reasonable range.
The important takeaway is to start thinking about the loss reserves your company is using in the calculation of taxableincome and understand that this is a highly targeted area during an IRS examination. An understanding of what the calculation oflosses incurred includes, Tax Court rulings on what is “fair and rea-sonable,” and what is needed for support if examined, will better pre-pare you in the eventthat the IRS doescome calling.
References1. “Loss reserves” include unpaid losses and loss adjustment expenses.2. Acuity Mutual Ins. Co. v. Commissioner, T.C. Memo. 2013-209.3. Sears, Roebuck & Co. v. Commissioner, 972 F.2d 858, 866 (7th Cir. 1992)).
For related information, seewww.johnsonlambert.com
The picture is worth at least1,000 words
Riba, a Japanese robot,aims to help withelder care. Japan has
one of the largest agingpopulations in the world, sothis is incredibly important.Designed to be nonthreatening in appearance,Riba lifts elderly patients out of bed, so theirlinens can be changed, among other tasks. Asimportant and difficult a task as this is, one hasto wonder what patients suffering from dementiawould think of a six-foot-tall robot bear liftingthem out of bed. Riba has gone through severaliterations and likely will go through more beforebeing put to heavy use.
— Source: Information Week, July 22, 2014
outtakes
PIAA 3Q BACK 2014_Layout 1 8/8/14 12:39 PM Page 8

PIAA 3Q BACK 2014_Layout 1 8/8/14 12:39 PM Page 9

I N S I D E M E D I C A L L I A B I L I T Y 47 T H I R D Q U A R T E R 2 0 1 4
I N T E R N A T I O N A L P E R S P E C T I V E
BY DR. THOM PETTY
Medical indemnifiers must accept that there will be a “nextbig thing.” All organizations experience periodic eruptionsof systemic risk, and we need only look to past experiencesfor confirmation. We have all seen how the actions of indi-
vidual practitioners, and also problems with technology, can affect largegroups of patients.
Enhanced data collection, evolving risk management, and sophis-ticated claims analysis are reassuring developments. However, denyingvulnerability to systemic risk, based on the premise that current meth-ods of risk assessment and analysis of cases are better than ever, isinadvisable at best.
Developments within medicine continue to accelerate: staff roles,treatments, technologies, and protocols for managing patients may berapidly introduced or changed. Within just a few months, a brand-newclinical approach to a certain medical condition may emerge. By con-trast, within an insured line such as auto insurance, safety improve-ments such as the introduction of seatbelts, airbags, and improved cardesign have evolved over a much longer timescale. Medicine works on aweeks-to-months basis. In addition, medical professional liability suf-fers from the inherent time lag between incurred and reported events
that one would not see in other insured areas.Accordingly, the need to anticipate and manage systemic risk
within medicine prospectively could not be greater. By the time theclaims notifications begin to pour in, the events have long since takenplace. At this stage, any steps to mitigate will be much less effective. Butnotwithstanding the financial liabilities for medical indemnifiers, thereis also the obligation to anticipate and manage risk in the interests ofpatients themselves.
“Information is not knowledge”2
There is one happy coincidence in play here, though. The higher preva-lence of clinical negligence litigation has emerged at the dawn of thedigital age. The landscape of publicly accessible information is unrecog-nizable compared with what was available only a decade ago. However,the new sources are so extensive and widespread, it is now essential formedical indemnifiers to develop systematic methods of review. Thedata is not tidy. It is often qualitative and highly clinically based, a farcry from neat tables of claims data.
Magic is everywhere, if you know where to lookSo where should medical indemnifiers look? Unhelpfully, the answer is“everywhere”: government and regulatory bodies, popular and medicalpress, the specialty-specific colleges, and clinicians themselves.
APPROACHINGRISK IN THEINFORMATION AGE
Niels Bohr, Nobel Laureate in physics, has said,“Predictions can be very difficult, especially aboutthe future.”1 Medical indemnifiers know only toowell that a new area of systemic risk can emergewith alarming speed. Consider the possibilities: an individual doctor or nurse with serial claims,repeated failures of a medical implant or device,and the breakdown of a healthcare institution’s systems or protocols—the scope is extremely broad.
Dr. Thom Petty, BSc (Hons), MBChB (Hons), Fellowship of the RoyalCollege of Anaesthetists, is Deputy Head of Underwriting, The MedicalDefence Union.
PIAA 3Q BACK 2014_Layout 1 8/8/14 12:39 PM Page 10

I N S I D E M E D I C A L L I A B I L I T Y 48 T H I R D Q U A R T E R 2 0 1 4
By way of example, the Medicines and Healthcare productsRegulatory Agency (MHRA) is a U.K. governmental organization thatregulates medicines, devices, medical equipment, and blood and othertherapeutic products.3 In addition to licensing, the MHRA also reviewsand monitors reports from healthcare providers, manufacturers, andpatients. Of particular relevance are the rapid and regular medicaldevice alerts published online alongside the agency’s regulatory guid-ance. The MHRA also administers the Yellow Card Scheme, whichhealthcare professionals use to report adverse drug reactions. The prin-ciple is wide dissemination of information, urgently if required, and thewithdrawal or restriction of a product where deemed necessary. Itallows healthcare staff on the front line to take action and indemnifiersto take stock early on about potential implications and, from that point,to take steps to mitigate their impact. In April 2010, the MHRA was thefirst regulatory agency worldwide to issue advice to doctors about theissues with metal-on-metal hips.4 This followed their establishment ofan expert advisory group in 2008. They continue to provide updatedadvice about the matter.
Another example, the National Patient Safety Agency, provides acentralized adverse incident-reporting system.5 Anyone, healthcare staffand patients alike, can submit reports to the National Reporting andLearning System online. In turn, the agency releases rapid reports, safe-ty alerts, and guidance on best practice.
Align with the responsible bodyHealthcare providers now practice in an age of guidelines. In the U.K.,these are published by a variety of respected organizations, rangingfrom national and governmental bodies, such as the National Institutefor Health and Clinical Excellence,6 to the specialty-specific medical col-leges. A key assessment of negligence is the “Bolam test,” i.e., whether agiven clinician’s actions would be supported by a responsible body ofpractitioners.7 By definition, a guideline produced by one of these bod-ies represents the expected clinical management of the responsiblebody of practitioners. By adopting these guidelines in risk assessingand managing different areas of clinical work, indemnifiers may miti-gate the vulnerability to successful litigation.
However, guidelines provide guidance and not rules. If patients
with meningococcal meningitis routinely presented with a “text-book”set of symptoms, namely, severe headache, neck stiffness, photophobia,pyrexia, a positive Kernig’s sign, and a non-blanching rash, generalpractitioners would sleep more easily at night. It also remains the casethat litigants tend to quote guidelines “to the letter”—as literal, obliga-tory instructions—in pursuing cases. In fact, we know that it is impor-tant to respect the complexities of clinical practice, rather than usingguidelines rigidly and inflexibly.
Growing comfortable with qualitative dataThese are just a few examples of freely available information that canassist in our risk management processes. Medical indemnifiers are nostrangers to monitoring data, principally in relation to claims trends,damages and legal costs, and membership, but they will now need tobecome comfortable in utilizing this sort of qualitative information,which does not easily lend itself to actuarial analysis. The local andnational press, blogs, informal social media such as Twitter: any ofthese may contain that invaluable “heads up” about an emerging problem area.
Stay close to the profession So if an underwriter diligently surveys the scene as suggested, how doeshe translate this into a meaningful approach to risk assessment andmanagement? As medicine develops at breakneck speed, it is essentialthat medical indemnifiers stay close to the profession. Only by utilizingfrontline clinicians can we expect to understand medical developmentsin real time. The Medical Defence Union, for example, maintains a largecouncil of clinicians from all the specialty fields. They are an essentialreference point, providing unparalleled insight into new treatments,areas of emerging concern, and individual case management.
But in an ideal world, we would want to know about problemswith, for example, metal-on-metal hips, well in advance of 2010, or even2008. Again, clinicians themselves are in the best position to alert us.Discussions with colleagues, presentations at meetings, murmurings atconferences, and clinical experience: these may provide the first indica-tions of a problem, whether that risk lies with an individual clinician,device or a wider clinical area. Further, clinicians can offer practical
I N T E R N A T I O N A L P E R S P E C T I V E
New technologies, particularly auto-mated clinical procedures and robot-ics, have the potential to improve
patient safety by eliminating human error.However, if the original calibration is itselferroneous, the consequent repetition oferror can be devastating. In the French townof Epinal, because of a calibration error in anew radiotherapy machine at the JeanMonnet Hospital, approximately 450 patientswere subjected to radiation overdoses.12
Twelve patients died, and many were left
suffering from urinary and digestive prob-lems. Three of the doctors involved wereconvicted of manslaughter and imprisoned.
Fundamentally, protocols attempt to
standardize medical care and raise the qual-ity of it, while also reducing the risk oferrors. However, a single level mistake with-in a protocol, such as an erroneous medica-tion dose or even an erroneous referralmade by a computerized referral system, isquickly replicated in a large number ofpatients, with widespread implications. So itis more important than ever to front-load therisk management process—before an erroris incorporated and then repeated hundredsor thousands of times.
Man vs. Machine
PIAA 3Q BACK 2014_Layout 1 8/8/14 12:40 PM Page 11

I N S I D E M E D I C A L L I A B I L I T Y 49 T H I R D Q U A R T E R 2 0 1 4
advice in managing and mitigating the risk on the ground, which a riskmanager can then incorporate into underwriting policy.
“To expect the unexpected shows a thoroughly modern intellect” 8
Unsurprisingly, there remains no quick solution for anticipating riskareas within medical indemnity. However, in terms of the informationavailable to indemnifiers, the position has never been better.
Ultimately, there is no reason why the ghosts of the past will notrevisit us. It is likely that implants and medical devices will come to theforefront again at some point. We have seen metal-on-metal hips andPIP breast implants and there have been recent concerns raised aboutvaginal mesh procedures.9,10 Non-therapeutic areas of medicine, suchas cosmetic surgery, where patient expectations are high, will continueto be associated with high levels of litigation. There is an ever-increas-ing demand for novel cosmetic implants, such as pectoral and calf mus-cle prostheses. We have already been warned by the U.K. Department ofHealth about dermal fillers.11
Reviewing and making the best use of multiple, diverse sources ofinformation will require that medical indemnifiers shift their approach,from the reactive to the proactive. The MHRA will not come knockingat our doors, and the professional colleges will not alert us when theypublish new guidelines. Keeping up with these developments is a chal-lenging and time-consuming task, but it is no longer optional. Medicalindemnifiers must align themselves with the information available andthen call upon the medical profession to make sense of it.
Deutsche Asset & Wealth Management
Responsible for nearly $200 billion in assets under management and voted “Best Global Manager“ for six years in a row.
Deutsche Asset & Wealth Management –the global leader in insurance asset management.
Deutsche Asset & Wealth Management represents the asset management and wealth management activities conducted by Deutsche Bank AG or any of its subsidiaries. Clients will be provided Deutsche Asset & Wealth Management products or services by one or more legal entities that will be
or other documentation relevant to such products or services.
© 2014 Deutsche Asset & Wealth Management.All rights reserved. I-032672-1.0
Voted “Best Global Manager“ by the readers of Reactions magazine 2008-2013
For more information visit us atinsuranceam.db.com
at +1 212 250 9471or [email protected]
For related information, seewww.themdu.com.
References1. Niels Bohr, Danish physicist, quoted in H. Rosovsky, The University: AnOwners Manual (1991), 147.2. Albert Einstein, source unclear.3. www.mhra.gov.uk 4. http://www.mhra.gov.uk/Safetyinformation/Generalsafetyinforma-tionandadvice/Product-specificinformationandadvice/Product-specificinfor-mationandadvice–M–T/Metal-on-metalhipimplants/index.htm (accessed6/7/14).5. http://www.npsa.nhs.uk/. 6. http://www.nice.org.uk/. 7. Bolam v Friern Hospital Management Committee [1957] 1 WLR 583. 8. Wilde O. An Ideal Husband, 1899.9. Letter from the Chief Medical Officer for Scotland, Harry Burns, to ScottishNHS Board CEOs, Medical Directors and General Practitioners (dated 11/7/13).www.sehd.scot.nhs.uk/publications/DC20130711meshes.pdf (accessed 6/7/14).10. Letter from Acting Chief Medical Officer for Scotland, Aileen Keel, request-ing boards to consider suspending the use of synthetic mesh products forpelvic organ prolapse and stress urinary incontinence.www.sehd.scot.nhs.uk/cmo/CMO(2014)15.pdf (accessed 16/7/14).11. U.K. Department of Health. Review of the Regulation of CosmeticInterventions. April 2013. Available online: https://www.gov.uk/government/news/recommendations-to-protect-people-who-choose-cosmetic-surgery. 12. Chustecka Z. Docs in prison after radiation overdose in prostate cancer.Medscape, June 7, 2014; http://www.medscape.com/viewarticle/778862(accessed 6/7/14).
PIAA 3Q BACK 2014_Layout 1 8/8/14 12:40 PM Page 12

I N S I D E M E D I C A L L I A B I L I T Y 50 T H I R D Q U A R T E R 2 0 1 4
These results could continue over the next severalyears if trends in reserve releases hold. This revelation is likelyto give MPL insurers a brief reprieve from the impendingmarket change, but it doesn’t alter the fact that insurers’ tradi-
tional business models will likely be tested over the next five years.Which companies will endure? Which will prosper?
For the past eight years, reserve releases have made MPL insur-ers the darlings of the property/casualty industry, driving down theircombined ratio far below the industry’s breakeven point of 100%. Theyear 2013 was no exception, as MPL insurers posted a combined ratio
of 85%—5 percentage points better than the previous year. As in past years, overall profitability for calendar year 2013 was
largely the result of reserve releases from prior policies, which, at $2billion for the year, were in line with the previous five years. Over thepast eight years, MPL insurers have released some $16 billion inreserves on policies written since the beginning of the 2000s (Figure 1).In 2013, reserve releases contributed nearly 25 percentage points ofrelief to the industry’s combined ratio (Figure 2).
But even without the reserve releases, the MPL industry haslikely experienced profitable results, even if this fact hasn’t yet beenrecognized in the financial statements of insurers. This is because thesignificant trends in reserve releases that have been recognized afterthe initial recorded results are expected to continue for the current pol-icy year. And when all is said and done, we expect that calculations
will show that current pricinghas still been adequate to coverlosses and associated expenses.
Many observers mightbreathe a sigh of relief at thelikelihood of insurers’ continuedprofitability, especially in afiercely competitive market, if itweren’t for the fact that it stemsnot from renewed pricing disci-pline but, rather, from an aberra-tion in reported claim frequen-cy—which happened a decadeago, when the number of claimsreceived by insurers fell precipi-tously. Over the interveningyears, MPL insurers haveenjoyed the benefits of this sud-
Richard B. Lord, FCAS, MAAA, is a Principal and Consulting Actuary,and Stephen J. Koca, FCAS, MAAA, is a Principal and Actuary,Milliman.
A PAUSE IN TIME
B Y T H E N U M B E R S
BY RICHARD B. LORD AND STEPHEN J. KOCA
Developments in a soft market aren’t
often a pleasant surprise, but last year’s
improvement in medical professional lia-
bility (MPL) insurers’ results happened
for one of the best possible reasons: con-
tinued profitability, even on current-year
policies, based on our estimations.
Figure 1 Historical MPL Reserve Changes, As a Percent of Net Earned Premiums
Shaded areas represent hard market periodsSource: Medical Professional Liability Industry Aggregate, SNL Data / A.M. Best Aggregates & Averages
PIAA 3Q BACK 2014_Layout 1 8/8/14 12:41 PM Page 15

I N S I D E M E D I C A L L I A B I L I T Y 51 T H I R D Q U A R T E R 2 0 1 4
den and somewhat unexplained drop in frequency.Loss trends, however, have continued to rise, but as of2013 remain at levels that continue to yield profits forinsurers, in our estimation.
The fact remains that MPL insurers’ losstrends are rising, and have been for the past tenyears. And while the increase has admittedly beenfrom a much lower starting point because of theunprecedented drop in frequency, loss trends havesteadfastly continued their upward climb, whileincreasingly stiff competition has caused an erosionin rates and premium.
2013 was the seventh consecutive year thatearned premiums declined. These year-over-yearchanges, in fact, constitute the longest stretch of premium declines ofany in the past 30 years during which MPL results have been tracked.Since 2006, premiums have shrunk to $8.5 billion, and are nowapproximately 16% less than their 2006 level (Figure 3). At no othertime over the past 30 years have premiums declined to this extent. 1
Indeed, the exceptional decrease in premium happened for rea-sons that go beyond the sort of competition that perhaps defines mostsoft markets. Physician insurers have seen their markets shrivel asmore physicians—faced with rising operating expenses and flaggingrevenues—have left private practice to become employed by hospitalsor large medical groups. According to an Accenture study, the propor-tion of physicians in independent practice dropped from 57% in 2000
to 39% in 2012. The firm estimated we will likely findthat this figure has slipped to 36% when the year-end2013 data have been finalized.
With a growing number of physicians employedby large-group practices or hospital systems, many ofwhich self-insure their MPL exposures, physicianinsurers have seen their exposure base contract, asmore risks are removed from the primary commer-cial market. This trend has contributed to the pro-longed decline in premium revenues and raises thepossibility that expense problems could develop forsome insurers that now confront a smaller premiumbase for spreading their costs.
A tipping pointMPL insurers’ falling premiums have not yet converged with risinglosses to an extent that could lead to real problems, in our estimation.But in this evolving healthcare environment, this situation could rapidly change.
The biggest question centers on the impact of the AffordableCare Act (ACA), which could shift MPL claim frequency and averageclaim cost (severity) trends in either direction. In the interest of timeand space, let us just look at one in some detail—the introduction ofaccountable care organizations (ACOs). The goal of these organizationsis to improve the quality and efficiency of care. As such, their risk-based compensation model is intended to encourage physicians, hos-
The huge influx ofinsured individuals,which is expected totop 30 million by the
time ACA is fully imple-mented in 2016, couldlead to a shortage of
physicians.
CUSTOMIZED INSURANCE INVESTMENT MANAGEMENT SOLUTIONS THAT FIT CUSTOMM Z D NSSSNNIIDDEEZZIIMMOOTTSSUUCC URANCE NVESTMENNNEEMMTTSSEEVVNNIIEECCNNAARRUUSS T MMANAGEMENT SOOOSSTTNNEEMMEEGGAANNAAMMTTNN UTIONS THAT F TTTIIFFTTAAATATHHTTSSNNOOIITTUULLOO
PIAA 3Q BACK 2014_Layout 1 8/8/14 12:41 PM Page 16
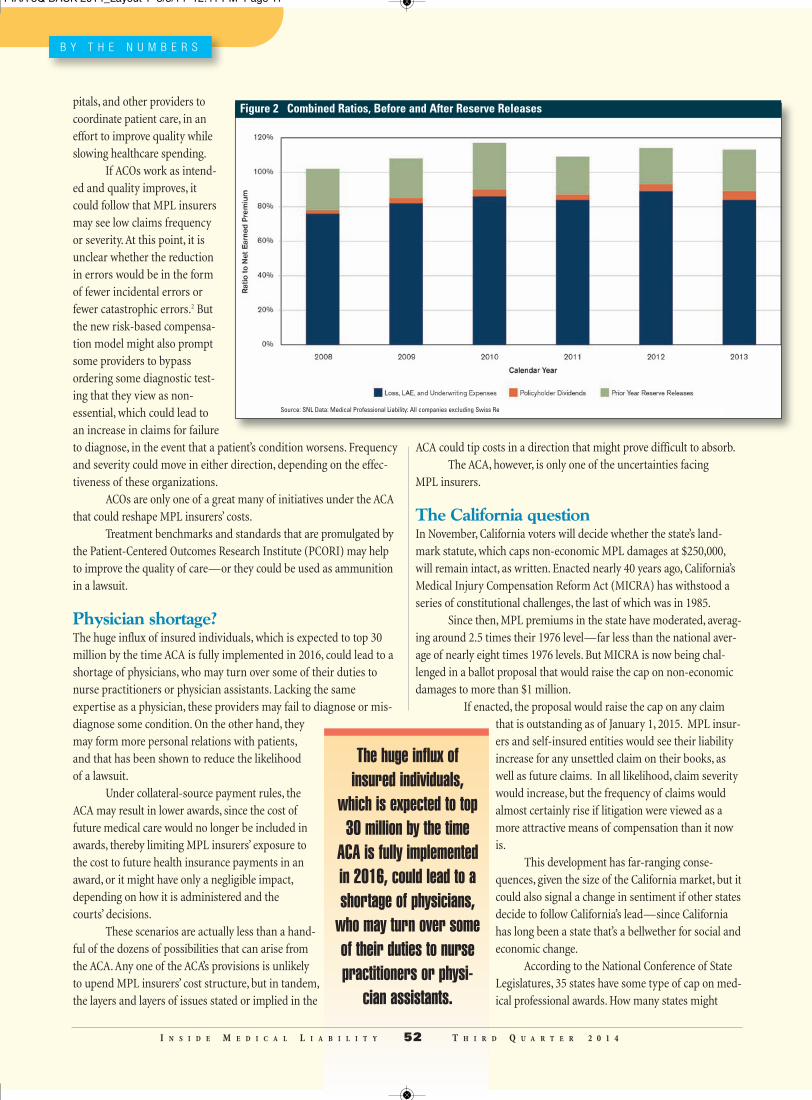
pitals, and other providers tocoordinate patient care, in aneffort to improve quality whileslowing healthcare spending.
If ACOs work as intend-ed and quality improves, itcould follow that MPL insurersmay see low claims frequencyor severity. At this point, it isunclear whether the reductionin errors would be in the formof fewer incidental errors orfewer catastrophic errors.2 Butthe new risk-based compensa-tion model might also promptsome providers to bypassordering some diagnostic test-ing that they view as non-essential, which could lead toan increase in claims for failureto diagnose, in the event that a patient’s condition worsens. Frequencyand severity could move in either direction, depending on the effec-tiveness of these organizations.
ACOs are only one of a great many of initiatives under the ACAthat could reshape MPL insurers’ costs.
Treatment benchmarks and standards that are promulgated bythe Patient-Centered Outcomes Research Institute (PCORI) may helpto improve the quality of care—or they could be used as ammunitionin a lawsuit.
Physician shortage?The huge influx of insured individuals, which is expected to top 30million by the time ACA is fully implemented in 2016, could lead to ashortage of physicians, who may turn over some of their duties tonurse practitioners or physician assistants. Lacking the same expertise as a physician, these providers may fail to diagnose or mis-diagnose some condition. On the other hand, theymay form more personal relations with patients, and that has been shown to reduce the likelihood of a lawsuit.
Under collateral-source payment rules, theACA may result in lower awards, since the cost offuture medical care would no longer be included inawards, thereby limiting MPL insurers’ exposure tothe cost to future health insurance payments in anaward, or it might have only a negligible impact,depending on how it is administered and the courts’ decisions.
These scenarios are actually less than a hand-ful of the dozens of possibilities that can arise fromthe ACA. Any one of the ACA’s provisions is unlikelyto upend MPL insurers’ cost structure, but in tandem,the layers and layers of issues stated or implied in the
ACA could tip costs in a direction that might prove difficult to absorb. The ACA, however, is only one of the uncertainties facing
MPL insurers.
The California questionIn November, California voters will decide whether the state’s land-mark statute, which caps non-economic MPL damages at $250,000,will remain intact, as written. Enacted nearly 40 years ago, California’sMedical Injury Compensation Reform Act (MICRA) has withstood aseries of constitutional challenges, the last of which was in 1985.
Since then, MPL premiums in the state have moderated, averag-ing around 2.5 times their 1976 level—far less than the national aver-age of nearly eight times 1976 levels. But MICRA is now being chal-lenged in a ballot proposal that would raise the cap on non-economicdamages to more than $1 million.
If enacted, the proposal would raise the cap on any claimthat is outstanding as of January 1, 2015. MPL insur-ers and self-insured entities would see their liabilityincrease for any unsettled claim on their books, aswell as future claims. In all likelihood, claim severitywould increase, but the frequency of claims wouldalmost certainly rise if litigation were viewed as amore attractive means of compensation than it nowis.
This development has far-ranging conse-quences, given the size of the California market, but itcould also signal a change in sentiment if other statesdecide to follow California’s lead—since Californiahas long been a state that’s a bellwether for social andeconomic change.
According to the National Conference of StateLegislatures, 35 states have some type of cap on med-ical professional awards. How many states might
B Y T H E N U M B E R S
The huge influx ofinsured individuals,
which is expected to top30 million by the time
ACA is fully implementedin 2016, could lead to ashortage of physicians,
who may turn over someof their duties to nursepractitioners or physi-
cian assistants.
I N S I D E M E D I C A L L I A B I L I T Y 52 T H I R D Q U A R T E R 2 0 1 4
Figure 2 Combined Ratios, Before and After Reserve Releases
Source: SNL Data: Medical Professional Liability: All companies excluding Swiss Re
PIAA 3Q BACK 2014_Layout 1 8/8/14 12:41 PM Page 17

I N S I D E M E D I C A L L I A B I L I T Y 53 T H I R D Q U A R T E R 2 0 1 4
again follow California’s lead and challenge reforms? Time will shed more light on the answer, but the possibility that
the longstanding tort reforms might evaporate over the next few yearsadds another layer of challenge to an already fluid market.
Perhaps the one certainty that emerges from all the currentuncertainty is that traditional static business models that rely on what
has worked in the past arehighly unlikely to be up to thechallenges of the future. Thesechallenges require dynamicapproaches that leverage exist-ing expertise to judiciouslyexpand or diversify into newmarkets. Companies that knowhow to build on their expertise,and do more than just managerates, will be the insurers thatendure and most likely prosperin the future.
References1. Forray SJ, Karls CC. Profitabilitydeclines from previous levels;reserve releases fund dividendsand additions to surplus. InsideMedical Liability, Second Quarter2014. 2. Jones D. Medical professional
liability: The other insurance market affected by health reform. May 29, 2012.http://insight.milliman.com/article.php?cntid=8093
For related information, see www.milliman.com.
Figure 3 Historical MPL Net Earned Premiums
Source: Medical Professional Liability Industry Aggregate, SNL Data / A.M. Best Aggregates & Averages
Our niche is your niche.
flourish in their roles while they drive company success to new heights.talent to the right opportunity
sraey02roF
rofessional Liability Insurance RP
flourish in their roles while they drive company success to new heights.e take tremendous pride in seeing people. Wtalent to the right opportunity
ameerFtanoissimruo,s
uitingecrrofessional Liability Insurance R
flourish in their roles while they drive company success to new heights.e take tremendous pride in seeing people
tneebsahsesirpretnEn
flourish in their roles while they drive company success to new heights.e take tremendous pride in seeing people
p othctamo
PIAA 3Q BACK 2014_Layout 1 8/8/14 12:42 PM Page 18

2014 PIAA Medical Liability Conference
Reed V. Tuckson, MD, FACP
opics covered included finance, claims management, risk mitigation and patientsafety, and government and regulatory policy. Of particular interest at this year’s
conference were topics related to the notable changes in the healthcare market in the U.S.,such as the rapidly increasing percentage of physicians who are employed. Attendees leftthe meeting with a clear perspective on the present and future of the MPL business, andwith specific strategies for meeting the challenges of the evolving healthcare system, bothin the U.S. and around the world.
Keynote Session“Sustaining Cost-Effective, Patient-Centered Care in an Era of Transformation” We are in an unprecedented world of consumer/patient-driven healthcare, said Reed V.Tuckson, MD, FACP, delivering the address in the Keynote Session. At the same time,he said, for medical professionals, healthcare is in a volatile, unstable market, filled with
TT
The 2014 MedicalLiability Conference,May 14–16, in Toronto,Canada, brought togethermore than 500 insuranceprofessionals, all look-ing to gain key insightson the global—and day-to-day—issues facingthe medical professionalliability (MPL) communi-ty. The meetingaddressed the mostimportant topics theseprofessionals needed tolearn about and discuss.All of the conferenceproceedings were setamid the vibrant, cosmo-politan city of Toronto.
I N S I D E M E D I C A L L I A B I L I T Y 54 T H I R D Q U A R T E R 2 0 1 4
PIAA 3Q 2014 MLC Section_Layout 1 8/8/14 2:36 PM Page 1

risks. And yet, this disruption also makes possible new kindsof opportunities for innovation. In this sort of environment, hesaid, it is of critical importance that healthcare professionalssustain their traditional adherence to the Hippocratic Oath, andalso preserve their autonomy.
Tuckson is Managing Director, Tuckson HealthConnections, LLC; former Executive Vice President and Chief ofMedical Affairs, UnitedHealth Group; and former Senior VicePresident for Professional Standards, American MedicalAssociation.
One example of the emerging opportunities, Dr. Tucksonsaid, pertains to “big data.” Now, it will be possible to aggre-gate the clinical information on large numbers of patients, anduse techniques such as regression analysis to see which fac-tors are truly relevant for rigorously evidence-based diagnosisand treatment. That information can then be applied to indi-vidual patients, to ensure that they get the care they need,while scrupulously avoiding unnecessary care. Other recentdevelopments, such as mobile health apps, he pointed out, willalso enhance the specificity of diagnostics and treatments forpatients.
There are also some difficult issues for everyone inhealthcare, Dr. Tuckson said. There is now a medicine for hep-atitis C that cures the condition, rather than just treating thesymptoms. But its cost is $84,000; adding to the complexity indeciding whether to use this treatment is the fact that hepati-tis C occurs principally in addicts. There is also the new marketin molecular diagnostics and genetic testing, expected toemerge as a $15 billion to $20 billion industry by 2021. But, hepointed out, we don’t yet know what to do with the vastamount of data generated by these analyses.
In the midst of the ongoing evolution in the U.S. health-care system, Dr. Tuckson said, PIAA members should promotetheir work and all that it accomplishes. “You need to be muchmore public in your contribution to this discussion,” he said.
Peter Sweetland Award James L. Weidner was named as the 2014 Peter SweetlandAward of Excellence recipient for his significant contributionsand dedication to the MPL insurance industry and PIAA.Weidner has spent much of his extensive insurance career rep-resenting the interests of healthcare professionals and institu-tions through his work in the MPL industry. He is chief execu-tive officer of the Cooperative of American Physicians, Inc.(CAP), located in Los Angeles, California.
Weidner has dedicated countless hours of service to PIAA.He is a past member and chair of the PIAA Board of Directors.He also has also served on numerous PIAA committees: Audit,
Finance and Investment, Nominating, Strategic Planning, andRating Agency Relations committees. In addition, Weidner con-tinues to serve on the Data Sharing Advisory Committee and asthe liaison to the PIAA Board Fellows program.
“We are honored to present Jim with our most presti-gious award in recognition of his dedication and commitmentto PIAA and those who provide healthcare,” said Ted J. Clarke,MD, chair of PIAA. “Jim has been a passionate advocate onbehalf of the medical community and an unwavering supporterof PIAA.”
Brian K. Atchinson, president and CEO of PIAA, stated,“Jim is a great innovator and a true professional—and we areprivileged to recognize his many accomplishments on behalf ofboth the medical community and PIAA. Through his work atboth CAP and PIAA, Jim has been a driving force in bringingrisk management and patient safety programs to healthcareprofessionals and in assisting them in addressing businesschallenges.”
“The Peter Sweetland Award of Excellence was createdto recognize an exceptional individual from our ranks who hasprovided great leadership and has served as an inspiration toothers in the industry,” Atchinson continued. “Jim truly embod-ies the spirit of this award, and we thank him for his hard workand years of service.”
The Peter Sweetland Award of Excellence, established in1993 by PIAA’s Board of Directors, was created in honor ofPeter Sweetland, one of PIAA’s chief architects and ardent sup-porters. The Peter Sweetland Award of Excellence recognizesan individual who has provided great service to the industryand to PIAA, and who epitomizes the high ideals and ethics forwhich Peter Sweetland stood.
2014 Peter SweetlandAward of Excellencerecipient James L.Weidner (left) and PIAA Chair Ted Clarke,MD (right)
I N S I D E M E D I C A L L I A B I L I T Y 55 T H I R D Q U A R T E R 2 0 1 4
PIAA 3Q 2014 MLC Section_Layout 1 8/8/14 2:36 PM Page 2
PIAA President andCEO Brian Atchinson(left) with the 2014PIAA LeadershipAward recipients(left to right): ScottDiener, Mary Hedin,and Gordon Ownby.
I N S I D E M E D I C A L L I A B I L I T Y 56 T H I R D Q U A R T E R 2 0 1 4
PIAA Leadership AwardsAt the opening session, PIAA also presented its LeadershipAwards for major contributions to the Association by volun-teers from its member companies. This year, they included: • Scott Diener, NORCAL Mutual Insurance Company,
Data Sharing Advisory Committee• Donald J. Fager, Medical Liability Mutual Insurance
Company, Government Relations Committee • Mary Hedin, Mutual Insurance Company of Arizona,
Underwriting Section • Gordon Ownby, Cooperative of American Physicians, Inc.,
Leadership Camp Section
Focus on a Session“Hospital Employment: The Physician’s Changing Role” The Affordable Care Act (ACA) and theestablishment of accountable care organiza-tions (ACOs), as well as similar contractarrangements, are clearly influencing the delivery of health-care. Hospitals have been deploying their resources so as tomaintain market share and visibility in the market, throughthe employment of physicians. The panel of physicians inthis session discussed the evolving role of the physician inthis new healthcare market and considered as well itsimpact on the MPL community.
Hayes V. Whiteside, MD, FACS, Chief MedicalOfficer, Senior Vice President, Risk Management,ProAssurance, pointed out an interesting aspect to theincreasing employment of physicians: “Everything about thetrend of hospitals employing physicians is consistentlyinconsistent.” The statistics might seem to indicate clearpatterns. In 2012 and 2013 alone, he said, there was a 6%increase in physician employment and a corresponding 6%decrease in the ranks of solo practitioners. There was a25% increase in physician employment between 2004 and2011.
But there are many other factors that are inconsistentwith this trend. For example, Medicare has been crackingdown on services performed at hospitals that could be donemore cheaply in the office. Hospital CFOs are expecting, atleast in the short term, financial losses from acquiring physi-cian practices. Smaller community hospitals, affected bycuts in Medicare and Medicaid, cannot compete for physi-cian employees.
Physicians themselves may be uncertain about howthey want to practice medicine. Dr. Whiteside noted that,among other considerations, physicians do like the freedomfrom dealing with business issues that employment offers,but at the same time, they hate having to follow the rules of others.
Doctors will need to decide what matters most tothem in how they practice. If they do decide to opt foremployment, they should consider what is happening in all
PIAA 3Q 2014 MLC Section_Layout 1 8/8/14 2:37 PM Page 3

I N S I D E M E D I C A L L I A B I L I T Y 57 T H I R D Q U A R T E R 2 0 1 4
of the markets and competition in negotiating their terms ofemployment.
Luke Sato, MD, Senior Vice President and ChiefMedical Officer, CRICO/RMF and Assistant Clinical Professor ofMedicine, Harvard Medical School, offered the perspective ofan academic medical captive insurer on the issue of physicianemployment.
There are several issues shared by all of these captives,he said, as a result of acquisition activity, and these includeintegrating risk management and patient safety programs,developing a strategy for non-employed/affiliated physicians,and resolving the cost disadvantage vs. the current commercialmarket.
Uniquely, these entities have issues that stem from struc-tural program differences, such as separate physician limits indisparate MPL policies.
To deal with these issues, CRICO convened a workinggroup to discuss the implications of acquisitions; one goal wasto develop guidelines on underwriting, claims, and patientsafety. To date, they have established underwriting risk miti-gation and patient safety requirements for community hospi-tals. They are also developing a similar set of requirements forphysicians practice groups (PPGs). They addressed the riskmanagement and patient safety issues through a shared riskmanagement structure, primary care risk interventions, andwith that, a primary care incentive program. The next step, Dr.Sato said, is to establish a primary care risk reduction strategy,which will include data analytics on primary care risks.
Graham Billingham, MD, FACEP, Chief MedicalOfficer, Princeton Insurance Company, discussed some of thechallenges that healthcare professionals, and U.S. healthcareas a whole, will have to confront in the coming years. Giventhe emerging imbalance between numbers of primary careproviders—the ratio of such providers to patients is1:10,000—Dr. Billingham envisions that what is done to com-pensate for the paucity of physicians, e.g., moving older, more
complex patients faster through the system, ordering fewertests and consults, and not readmitting them, will drive up frequency.
He also points out that one consequence of the ACA,White House officials have said, will be this: the healthcaresystem will evolve into one of two forms—organized aroundhospitals or organized around large physician groups.Physicians will face challenges in areas like loss of control andoutcomes; hospital CEOs will face financial challenges andpotential personnel shortages.
Employed physicians will also need to learn new skills in,for example, the fine points in navigating the Stark law provi-sions and compliance with new standards of care. They willlikely play new roles, too. They will need to become tech- andpolitically savvy, adept at analytic skills and negotiation.
For traditional MPL carriers, some portion of their busi-ness is changing. In response, they will have to offer differentlayers of coverage and also pursue ongoing diversification ofproducts and services. Amid all of the seismic change inhealthcare, MPL companies will need to have “flexibility—butalso be selective” about what they pursue.
PIAAPAC Luncheon Attendees Hear ExpertAnalysis on 2014 Congressional Races and More Tom Bevan, co-founder and Executive Editor ofRealClearPolitics, the popular website for all matters on poli-tics and policy, spoke to a packed room at the PIAAPACLuncheon, on May 15 at the Medical Liability Conference.Bevan provided attendees with an objective, non-partisanassessment of the 2014 Congressional races and what is instore for the nation’s capital once the elections are over. Insearching for clues about the possible outcome of the elec-tions, he advised the attendees to keep close tabs on the latesteconomic figures, as well as presidential approval numbers, asthese will likely indicate whether one party will have nationalmomentum or whether races will be decided more on local
Conference sessionspeakers (left toright) Hayes V.Whiteside, MD,FACS; Luke Sato, MD;Graham Billingham,MD, FACEP; andPIAAPAC Luncheonspeaker Tom Bevan.
PIAA 3Q 2014 MLC Section_Layout 1 8/8/14 2:38 PM Page 4
The 2015 Medical Liability Conference will be held in Las Vegas, Nevada. Don’t miss the premiere conference for the MPL community. Make plans now to attend next year’s event!
2015 PIAA Medical Liability Conference • May 13-15, 2015 • Caesars Palace, Las Vegas, Nevada
S A V E T H E D A T E !
I N S I D E M E D I C A L L I A B I L I T Y 58 T H I R D Q U A R T E R 2 0 1 4
issues. He also noted that state and local races may havean “up ballot” impact on some Congressional contests aswell. Bevan concluded his presentation by fielding attendeequestions about specific races around the country. To learnmore about PIAAPAC, contact Mike Stinson [email protected] or visit www.piaa.us.
Focus on a Session“From Obstacles to Opportunities: UsingERM as a Platform for Business Success”This session was structured as a series of questions and
answers—the ones that the speakershear most often, and that are mostimportant for keeping companyfinances, and company ratings, on asound footing. This text offers a rep-resentative sample of what proved tobe a very lively and engaging dialogue.
First Question: What is “enterprise risk management”?Gerry Glombicki, CPA, a Director atFitch Ratings, offered a broad defini-tion. Enterprise risk management, hesaid, is “a set of business practicesthat supports a particular view of the
world.” This encompasses all of the activities that are donewith sufficient frequency to require control, and for which itis cost beneficial to exert such control. The key issue inthinking about ERM, he said, is what you hope to accom-plish with your ERM system. It is important to have a clearobjective in mind.
David Ingram, CERA, FRM, PRM, Executive VicePresident at Willis Re, explained how ERM should be done.
At the most fundamental level, he said, ERM can be under-stood as a control cycle. In an insurance company’s controlcycle, management needs to first identify the key risks, andthen determine the risk quantity they are willing to acceptand retain. It is imperative, he said, that the entity monitorthe risk taking throughout the year and react to actual situa-tions that are revealed by the monitoring.
Second question: What are the rating agencies looking for in reviewing insurers’ERM schemes?Mark Stephens, Managing Director-Corporate RiskAdvisory Services, Milliman, Inc. said that the rating agen-cies had in prior years been examining metrics like IRISratios; then the new item was risk-based capital; and mostrecently, it has been ERM. He noted that if every companydid ERM well, we could expect to see a more shallowunderwriting cycle.
Gerry Glombicki pointed out that although the ORSA[Own Risk and Solvency Assessment] is not yet required ofsmaller insurers, companies of all sizes have found it to bea very useful exercise for assessing and mitigating risk.
David Ingram asked if anyone had actually considered therisks involved in doing poor ERM. Had anyone actuallymeasured the impact, in terms of declining revenues?
Third question: Are there common hurdleswhen companies first attempt ERM?Mark Stephens said that companies tend to be good atestimating risks with underwriting and reserves, but otherrisks, like some operational risks, they can’t quite get theirarms around easily. He also noted that companies mayhave difficulty in seeing the relationship among the variousindividual risks. He advice on introducing ERM: “Don’t dotoo much too soon.”
PIAA 3Q 2014 MLC Section_Layout 1 8/8/14 2:39 PM Page 5
PIAA 3Q 2014 MLC Section_Layout 1 8/8/14 2:39 PM Page 6

WHAT’S THE PROBABILITYTHAT YOU’LL READ THIS COLUMN?
PIAA Board of DirectorsGLORIA H. EVERETT (CHAIR)PAUL C. MCNABB, II, MD (VICE CHAIR)RICHARD E. ANDERSON, MD (SECRETARY)KURT SCOTT (CHAIR, FINANCE AND
INVESTMENT COMMITTEE)THEODORE J. CLARKE, MDWILLIAM MCDONOUGH
MARY-LOU MISRAHY
JAAN E. SIDOROV, MDCHRISTOPHER SMITH
R. AUSTIN WALLACE, MDJOSEPH S. WILSON, JR., MD
Volume XXVIII, Number 3, Third Quarter, 2014.
Inside Medical Liability is published fourtimes per year by PIAA.
BRIAN K. ATCHINSONPresident
ERIC R. ANDERSONDirector of Public Relations and Marketing
DANA MURPHYEditor
Material contained herein may not be used in any formwithout written permission from PIAA. PIAA is theinsurance industry trade association that represents a fullrange of entities doing business in the medical profes-sional liability (MPL) arena. These include domestic andinternational MPL insurance companies, risk retentiongroups, captives, trusts, and other entities. PIAA mem-bers insure more than two-thirds of America's privatepracticing physicians as well as dentists, nurses and nursepractitioners, and other healthcare providers and provideindemnification and other services to more than 400,000healthcare professionals around the world. PIAA mem-bers also insure more than 3,000 hospitals. Inside MedicalLiability is mailed at no charge to PIAA members.
Contributed articles and letters to the editor are encour-aged, but may require editing for length. Please sendarticles, news releases, or address changes to: InsideMedical Liability, 2275 Research Blvd., Suite 250,Rockville, MD 20850. Opinions expressed under bylinedarticles do not necessarily represent those of PIAAand/or its member companies.
BY ERIC R. ANDERSON
L A S T W O R D
I N S I D E M E D I C A L L I A B I L I T Y 60 T H I R D Q U A R T E R 2 0 1 4
If you turn on your morning radio program, and the
show’s meteorologist tells you that the probability of
precipitation is 80% for the day, you’ll probably grab
your umbrella before you leave home.
When it comes to the decisions healthcare profes-
sionals make, do they have the same sort of luxury in
using statistical probability to help guide their diagnoses?
Or, do they have to work with absolutes, making deci-
sions on diagnoses or treatment regimens based purely
on “yes” or “no” answers?
The real-world answer may lie somewhere in
between. But the odds are good that in the courtroom,
the concept of absolutes will reign supreme—and work
against them.
Stepping away from clinicians for a moment, it is
interesting to consider epidemiology. The cornerstone of
public health, epidemiology includes investigations of all kinds of health-
related conditions, to determine who is affected by them, why, and what
can be done to treat and prevent them. Logic dictates epidemiologists
would use statistically based results in detailing their findings.
But researchers have to navigate a great number of hurdles before
they can establish the actual cause of a particular health outcome.
Correlation is not causation, as they say: How strong is the link between
event A and result B? Does A always take place after B? If A is changed, is
B altered too, and to the same degree? The more frequently researchers
can say “yes” to these sorts of questions, the closer they get to imputing
causation between A and B. This is why epidemiologists are often so cau-
tious when announcing their findings in anything but absolute terms.
Closer to home, in the MPL arena, probability is certainly a recurring
theme in the delivery of healthcare. Quite likely, not a
single day goes by when some healthcare professional
returning home from a busy day at the office, clinic, or
hospital suddenly has the uncomfortable sense that one
or more of his diagnoses may turn out to be wrong, or
that some of his recommended treatments may not pro-
duce the expected cure.
Encountering the unexpected is an occupational
hazard in clinical practice. It’s been said that healthcare
professionals, after some years of experience in their
profession, begin to accept the simple fact that there is
always some degree of uncertainty in any prognosis, and,
at best, it can only be expressed as a probability in any
particular case.
But, regardless of these realities, plaintiff ’s attor-
neys attempt to persuade jurors to think only in black
and white. They talk as if there were no middle ground in healthcare
decisions. Any given decision is either wrong or right. But we know, after
decades of study into the particular areas of medical care that give rise to
MPL claims, that this is not the case. There are no guarantees. There are
only informed decisions by healthcare experts—often the best and
brightest in their respective specialties.
In a world with a judicial system that demands “yes” or “no” answers,
and with the nearly countless pressures on healthcare professionals today,
what can we do to help? For starters, we can continue to strive to provide
them with the most up-to-date, comprehensive, and insightful patient-
safety data—so they can learn from prior outcomes and continue to
make the best decisions possible.
We can also hope that, at some point in the future, jurors will agree
that on a day when the probability of precipitation was forecast at 80%,
but skies happened to be sunny all day, a person who elected to take an
umbrella made a prudent decision.
Eric R. Anderson is Director of Public Relations and Marketing at PIAA;
In the MPL arena,
probability is certain-
ly a recurring theme
in the delivery of
healthcare.
PIAA 3Q BACK 2014_Layout 1 8/8/14 12:44 PM Page 25
The United States healthcare insurance market is undergoing rapid and profound change. Guy Carpenter is focused on this evolving and specialized market. As the recognized industry leader in casualty catastrophe reinsurance products, we are uniquely positioned to offer clients seamless and innovative coverage solutions that respond to known and emerging exposures.
We invite you to learn how our dedicated team of specialists leverages our industry experience, market intelligence and analytical expertise to customize solutions that can meet the unique strategic and reinsurance needs of the medical professional liability insurance market. Let us put our intellectual capital to work for you. Please contact Steve Underdal at (952) 820-1030 or [email protected] for more information.
BE CONFIDENT IN THE FACE OF UNCERTAINTY
Learn more at guycarp.comHEALTHCARE & LIFESPECIALTY PRACTICE
PIAA 3Q BACK 2014_Layout 1 8/8/14 12:44 PM Page 26

2275 Research Blvd., Suite 250Rockville, MD 20850
Medical Liability:The Good – Reducing RiskThe Bad – New LossesThe Ugly – The Unknown
Go to: www.piaa2014.com
Last Chance to Register !
OCTOBER 8–10, 2014Amsterdam, the NetherlandsRenaissance Hotel Amsterdam
INTERNATIONALCONFERENCE
Covers 3Q 2014 FINAL USE _Layout 1 8/8/14 11:40 AM Page 1