don't forget sickled cells in the urine when investigating a patient for
TRANSCRIPT
Nephrol Dial Transplant (1996) 11: 723-725
The Interesting Case
NephrologyDialysis
Transplantation
Don't forget sickled cells in the urine when investigatinga patient for haematuria
G. B. Fogazzi, S.-O. Leong* and J. S. Cameron
Department of Nephrology, Guy's Hospital, London, UK
AbstractHaematuria is a well-known complication of sickle celldisease. A South African coloured patient withrepeated episodes of gross haematuria is described inwhom the diagnosis of sickle cell disease was suggestedafter the finding of sickled erythrocytes in the urinesediment. The diagnosis was then confirmed by haemo-globin electrophoresis, which revealed sickle cell trait(Hb-AS). It is concluded that sickled erythrocytesmust be looked for when urine is microscopicallyscrutinized to determine the source of a haematuria.
Introduction
Since the first report of Abel and Brown in 1948 [1]haematuria has been a well-known complication ofsickle cell disease [2-4]. Electrophoresis of haemo-globin and the demonstration of sickled cells in theperipheral blood are clues to the diagnosis. In onlya few cases so far have sickled erythrocytes beendescribed in the urine. Herein we report a casein whom it was the finding of sickled cells in theurine that suggested the diagnosis of sickle-cell carrierstatus, which was then confirmed by haemoglobinelectrophoresis.
Case report
A 16-year-old coloured South African male born inCape Town of parents born locally was evaluated forpainless gross haematuria. He presented a year previ-ously with the problem after a upper respiratory tractinfection. Since then he has had recurring episodes ofgross haematuria, occurring particularly after phys-ical exercise. The haematuria was not accompaniedby dysuria, frequency, or other urinary symptoms.
Correspondence and offprint requests to: G. B. Fogazzi, Divisione diNefrologia e Dialisi, Ospedale Maggiore, IRCCS, Via Commenda15, 20122 Milan, Italy.
*Permanent address: Department of Medicine, NationalUniversity Hospital, Singapore.
Microscopic haematuria was also noted by his doctorin between these episodes. He has been a healthy ladwithout any significant past medical history and hisfamily history was negative with respect to renal orhaematological diseases. Physical examination wasunremarkable, and blood pressure was 120/75 mmHg.
Urine was grossly bloody and showed trace albumin-uria on dipstick testing (Multistix 10 SG, Ames Inc.USA). After centrifugation of a 10-ml aliquot at2000r.p.m. for lOmin, phase-contrast microscopyat 400 x showed only red blood cells which weretoo numerous to be counted. They were isomorphicin morphology (spherocytes and crenated cells).Moreover in each microscopic field there were about15-20 sickled cells (Figure 1). A full blood countrevealed Hb of 14.5 g/dl; white count: 6.3 x 109/l; andplatelets: 154xlO9/l- Haemoglobin electrophoresis,performed after the urinary findings, revealed Hb-AS(sickle cell trait). Renal function was normal with aGFR of 99 ml/min. Imaging of the urinary tract withintravenous urography, ultrasonography and flexiblecystoscopy were all normal.
A diagnosis of haematuria associated with sickle-cell trait was made and patient was treatedconservatively.
Discussion
Haematuria occurs in 3-4% of patients with sickle celldisease [5]. It is far more common in heterozygoteswith sickle cell trait than in homozygotes with sicklecell anaemia, the reason being that the trait is 30-40times more frequent than the disease. Young adultblack people of North America and Africa are thetypical patients. However, Afro-Caribbean patients inthe West Indies [6] and white patients in different partsof the world, including Europe [6-10], as well aschildren have also been described [11,12]. Haematuriais typically macroscopic, of variable duration, recur-rent, and asymptomatic or associated with pain causedby the passage of clots. More frequently it is unilateral,originating from the left side. Microscopic haematuriais less common, and at times is found between oneepisode of gross haematuria and another [5,13]. The
© 1996 European Dialysis and Transplant Association-European Renal Association
Dow
nloaded from https://academ
ic.oup.com/ndt/article/11/4/723/1851406 by guest on 15 January 2022

724 G. B. Fogazzi et al.
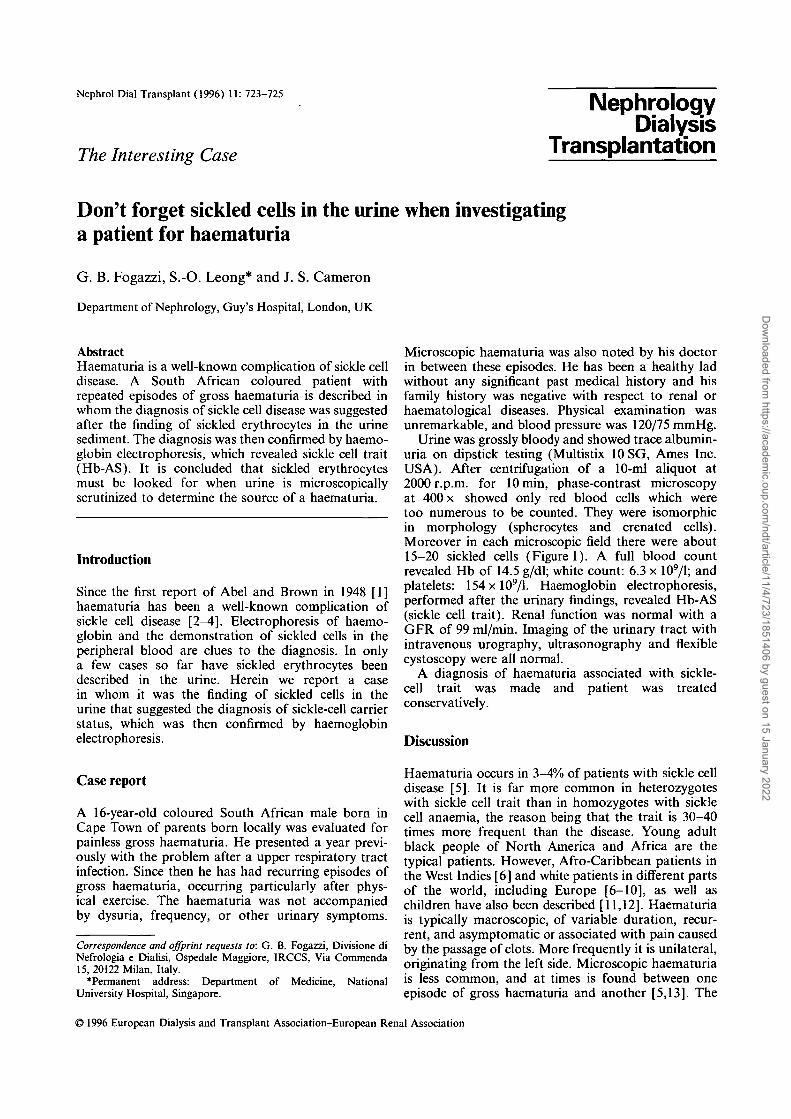
Fig. 1. Various types of sickled erythrocytes in the urine (arrows). Note the different appearance of isomorphic crenated erythrocytes(arrowheads) (phase-contrast microscopy, 400 x).
sickling of erythrocytes within the hypoxic, hypertonic,and acidotic renal medulla is considered the initiat-ing mechanism which leads to haematuria [14-16].Sickling in fact causes stasis within the peritubularcapillaries, which is followed by interstitial haemor-rhages with invasion into the tubular lumina [17].However, papillary necrosis and haemorrhages second-ary to erythrocyte sickling within the vessels of thepelvis or the ureter are other possible sources ofbleeding [18-20].
The finding of sickled erythrocytes in the urine ofour patient was the clue to the diagnosis of sickle celldisease. They appeared as sickles, crescents, 'holly-leaf shaped cells, or cells with 'pecked' contours, andclearly differed in morphology from the other erythro-cytes which may be found in haematuria of eitherglomerular, renal, or postrenal origin [21-23]. Theonly possible confusion is the differentiation of sicklederythrocytes with isomorphic crenated cells, which,however, have more regular and smaller protrusions(Figure 1). Instead, urinary sickled cells are identicalto sickled cells found in the peripheral blood and inthe vessels of the renal medulla [13,17].
Sickled cells in the urine have rarely been reportedso far. In fact in a review of the international Englishliterature containing information on the urinary sedi-ment findings in about one hundred patients withhaematuria and sickle cell disease, we were able toidentify only five papers in which sickled cells had beenobserved in the urine, in a total of seven patients only[9,13,15,16,24] (Table 1). In addition, in only one ofthese studies was the potential diagnostic role of thesecells considered [9]. In that paper sickled cells werefound in the urine of a Greek patient, and wereconfirmed in two subsequent analyses, the second beingperformed after gross haematuria subsided into micro-scopic haematuria. While Savige et al. [9] also found
Table 1. Patients with haematuria associated with sickle cell diseaseand sickled erythrocytes in the urine
Author [Ref.] Patients with urine Patients with sickledsediment described cells in urine
Goodwin et al. [13] 4Crone et al. [24] 7Knochel [15] 2Marynick et al. [16] 1Savige et al. [9] 1
urinary dysmorphic erythrocytes in association withsickled cells, we only found isomorphic erythrocytes.This finding, together with the lack of other elementssuch as erythrocyte or haemoglobin casts, suggestedthat there was no glomerular bleeding in our patient.This was also supported by the presence of only traceamounts of albuminuria.
In conclusion, we suggest that sickled cells must belooked for when urine erythrocytes are microscopicallyscrutinized to determine the source of a haematuria.In the case of a positive finding the appropriate bloodtests must be carried to confirm the diagnosis of asickle cell disease.
References
1. Abel MS, Brown CR. Sickle cell disease with severe hematuriasimulating renal neoplasm. JAMA 1948; 136: 624-625
2. Lucas WM, Bullock WH. Hematuria in sickle cell disease. J Urol1960; 83: 733-741
3. Chaplin H. Hematuria in hemoglobin S disorders. Arch InternMed 1980; 140: 1573
4. Mcinnes BK. The management of hematuria associated withsickle hemoglobinopathies. / Urol 1980; 124: 171-174
5. Allen TD. Sickle cell disease and hematuria: a report of 29cases. J Urol 1964; 91: 177-183
Dow
nloaded from https://academ
ic.oup.com/ndt/article/11/4/723/1851406 by guest on 15 January 2022

Sickled cells in the urine in haematuria 725
6. Bennett MA, Heslop RW, Meynell MJ. Massive haematuriaassociated with sickle-cell trait. Br Med J 1967; 1: 677-679
7. Chiorazzi N, Mailloux LU, Susin M et al. Recurrent hematuria.Occurrence in a white woman with sickle cell trait. JAMA 1974;230: 582-584
8. Richie JP, Kerr WS. Sickle cell trait: forgotten cause of hematu-ria in white patients. J Urol 1979; 122: 134-135
9. Savige JA, Birch DF, Fairley KF. Haematuria associated withureaplasma infection in sickle cell trair. Aust NZ J Med 1982;12: 293-295
10. Oksenhendler E, Bourbigot B, Desbazeille F et al. Recurrenthematuria in 4 white patients with sickle cell trait. J Urol 1984;132: 1201-1203
11. Vernier RL. Hematuria as manifestation of sickle-cell anemia inchildren. Am J Dis Child 1955; 89: 221-225
12. Tarry WF, Duckett JW, McC Snyder III. Urological complica-tions of sickle cell disease in a pediatric population. J Urol 1987;138: 592-594
.13. Goodwin WE, Alston EF, Semans JH. Hematuria and sicklecell disease: unexplained, gross unilateral, renal hematuria inNegroes, coincident with the blood sickling trait. J Urol 1950;63: 79-96
14. Perillie PE, Epstein FH. Sickling phenomenon produced byhypertonic solutions: a possible explanation for the hypostenuriaof sicklemia. J Clin Invest 1963; 42: 570-580
15. Knochel JP. Hematuria in sickle cell trait. The effect of intraven-ous administration of distilled water, urinary alkalinization, anddiuresis. Arch Intern Med 1969; 123: 160-165
16. Marynick SP, Ramsey EJ, Knochel JP. The effect of bicarbonateand distilled water on sickle cell trait hematuria and in vitrostudies on the interaction of osmolality and pH on erythrocytesickling cell trait. J Urol 1977; 118: 793-796
17. Mostofi FK, Bruegge CFV, Diggs LW. Lesions in kidneysremoved for unilateral hematuria in sickle-cell disease. ArchPathol 1957; 63: 336-351
18. Harrow BR, Sloane JA, Liebman NC. Roentgenologic demon-stration of renal papillary necrosis in sickle-cell trait. N EnglJ Med 1963; 268: 969-976
19. Harrison FG, Harrison FG Jr. Hematuria with sickle celldisease. J Urol 1952; 68: 943-949
20. Lund HG, Cordonnier JJ, Forbes K.A. Gross hematuria in sicklecell disease. J Urol 1954; 151-158
21. Fairley KF, Birch D. Haematuria: a simple method for identify-ing glomerular bleeding. Kidney Int 1982; 21: 105-108
22. Kholer H, Wandel E, Brunck B. Acanthocyturia. A characteristicmarker for glomerular bleeding. Kidney Int 1991; 40: 115-120.
23. Tomita M, Kitamoto Y, Nakayama M et al. A new morpholo-gical classification of urinary erythrocytes for differential dia-gnosis of glomerular hematuria. Clin Nephrol 1992; 37: 84-89
24. Crone R, Jefferson SC, Pileggi VJ et al. Gross hematuria insickle-cell trait. Arch Intern Med 1957; 100: 597-603
Received for publication: 29.8.95Accepted: 6 9.95
Dow
nloaded from https://academ
ic.oup.com/ndt/article/11/4/723/1851406 by guest on 15 January 2022