wilm's tumour
TRANSCRIPT
Wilm’s tumor
By- Dr. Satyajeet RathGuided by-Prof Kamal Sahni
EPIDEMIOLOGY
• Most common intra-abdominal tumor of childhood. (6%)• Second most common extracranial solid tumor among children• Wilms tumour (nephroblastoma)-embryonic kidney tumor• Develop from persistent embryonal remnant (nephrogenic rests)• 470 to 500 new cases in the US per year• More prevalent among girls. (1:0.9 for unilateral and 1:6 for bilateral)• >75% patients present before 5 years of age• Median age at diagnosis 30 months for unilateral and 40 mon. for B/L.• Children present with more advanced disease in less developed nations• Majority of cases- sporadic• Hereditary – 15-20%• 7% bilateral
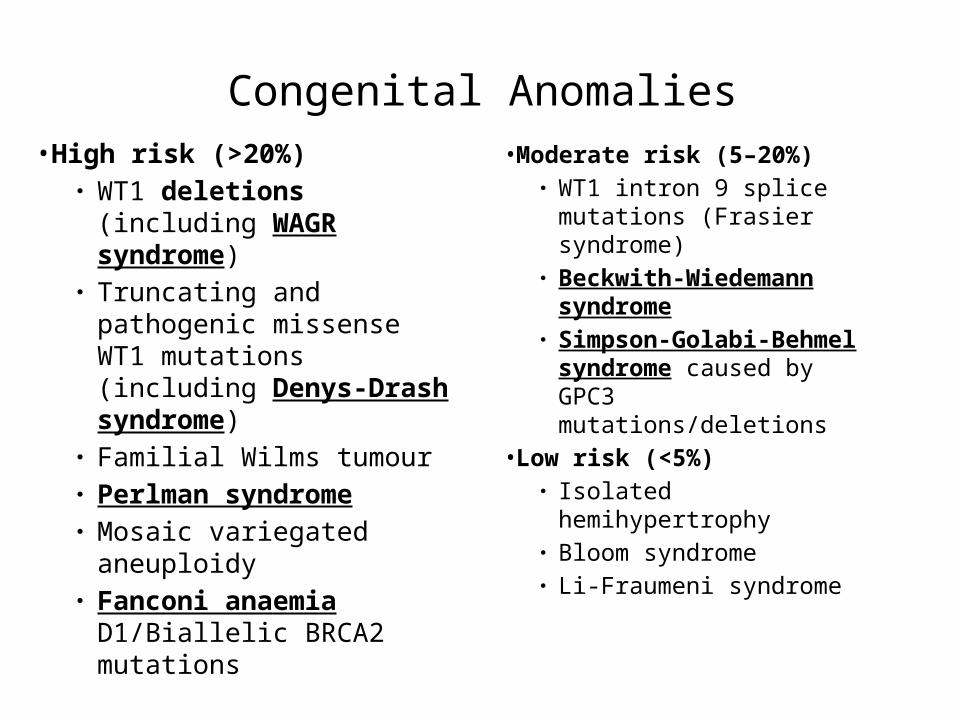
Congenital Anomalies•High risk (>20%)
● WT1 deletions (including WAGR syndrome)
● Truncating and pathogenic missense WT1 mutations (including Denys-Drash syndrome)
● Familial Wilms tumour● Perlman syndrome● Mosaic variegated aneuploidy● Fanconi anaemia D1/Biallelic
BRCA2 mutations
•Moderate risk (5–20%)● WT1 intron 9 splice
mutations (Frasier syndrome)● Beckwith-Wiedemann
syndrome● Simpson-Golabi-Behmel
syndrome caused by GPC3 mutations/deletions
•Low risk (<5%)● Isolated hemihypertrophy● Bloom syndrome● Li-Fraumeni syndrome
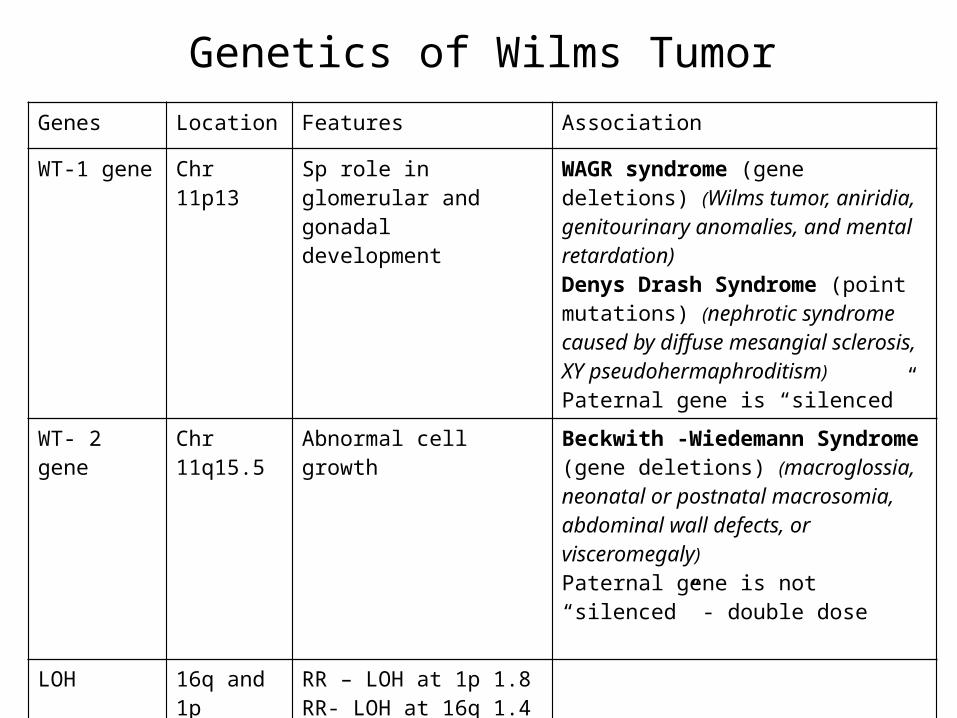
Genes Location Features Association
WT-1 gene Chr 11p13 Sp role in glomerular and gonadal development
WAGR syndrome (gene deletions) (Wilms tumor, aniridia, genitourinary anomalies, and mental retardation)Denys Drash Syndrome (point mutations) (nephrotic syndrome caused by diffuse mesangial sclerosis, XY pseudohermaphroditism)Paternal gene is “silenced”
WT- 2 gene Chr 11q15.5 Abnormal cell growth Beckwith -Wiedemann Syndrome (gene deletions) (macroglossia, neonatal or postnatal macrosomia, abdominal wall defects, or visceromegaly)Paternal gene is not “silenced” - double dose
LOH 16q and 1p RR – LOH at 1p 1.8RR- LOH at 16q 1.4 RR – LOH at 1p and 16q, 2.9 for stage I-II and 2.4 for III-IV
Genetics of Wilms Tumor
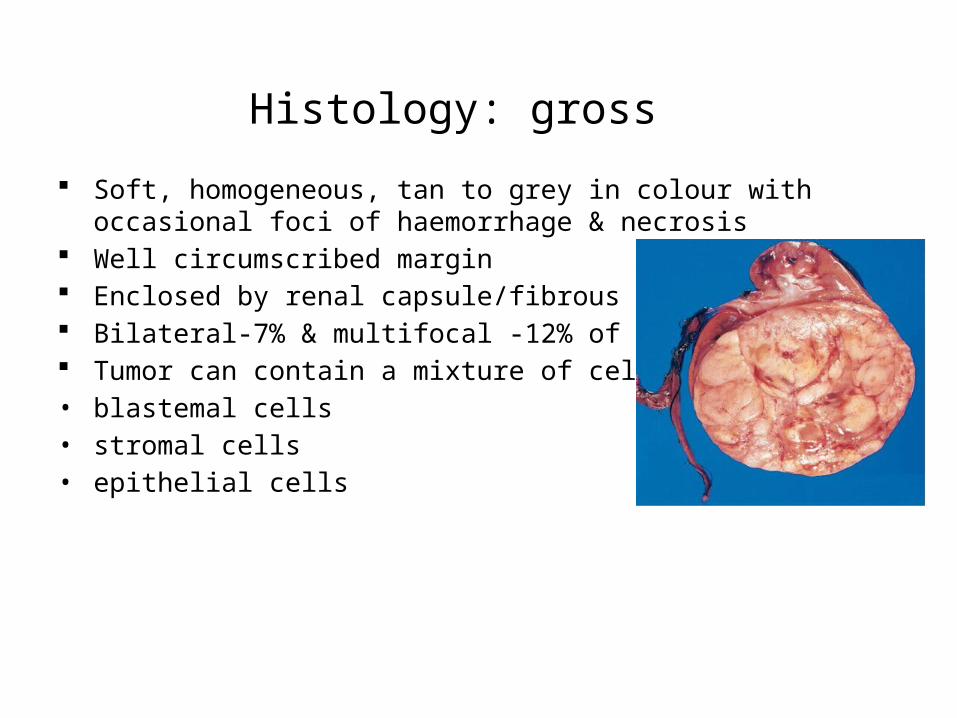
Histology: gross
Soft, homogeneous, tan to grey in colour with occasional foci of haemorrhage & necrosis
Well circumscribed margin Enclosed by renal capsule/fibrous pseudo-capsule Bilateral-7% & multifocal -12% of cases Tumor can contain a mixture of cells:• blastemal cells• stromal cells• epithelial cells
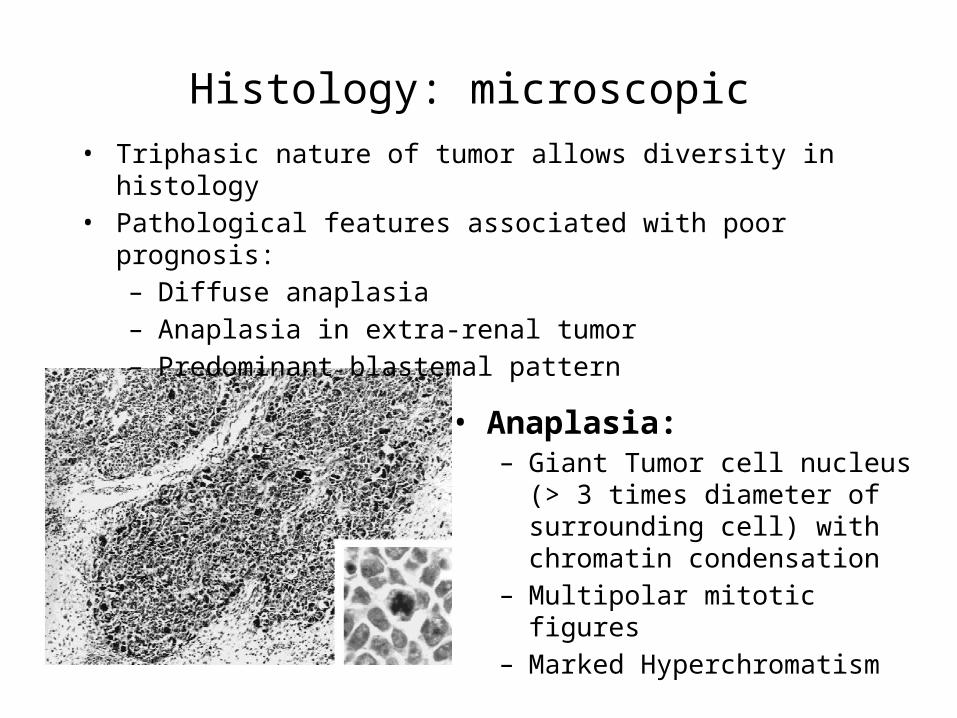
Histology: microscopic
• Anaplasia:– Giant Tumor cell nucleus (> 3 times
diameter of surrounding cell) with chromatin condensation
– Multipolar mitotic figures– Marked Hyperchromatism
• Triphasic nature of tumor allows diversity in histology• Pathological features associated with poor prognosis:
– Diffuse anaplasia– Anaplasia in extra-renal tumor– Predominant blastemal pattern
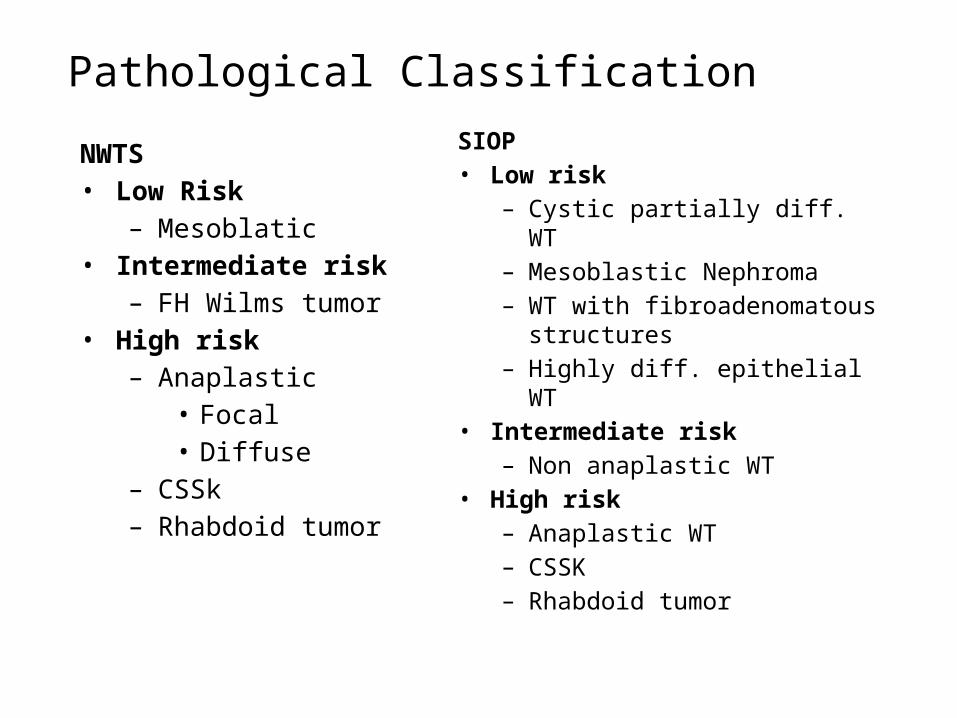
Pathological Classification
NWTS• Low Risk
– Mesoblatic• Intermediate risk
– FH Wilms tumor• High risk
– Anaplastic• Focal• Diffuse
– CSSk– Rhabdoid tumor
SIOP• Low risk
– Cystic partially diff. WT– Mesoblastic Nephroma– WT with fibroadenomatous
structures– Highly diff. epithelial WT
• Intermediate risk– Non anaplastic WT
• High risk– Anaplastic WT– CSSK– Rhabdoid tumor
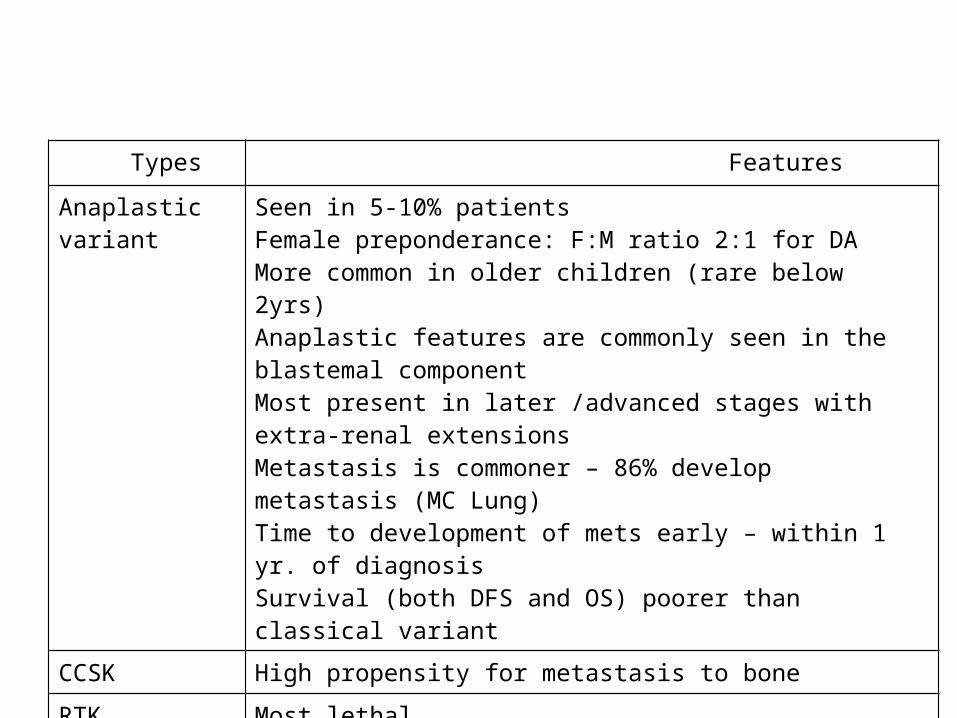
Types Features
Anaplastic variant Seen in 5-10% patients Female preponderance: F:M ratio 2:1 for DAMore common in older children (rare below 2yrs)Anaplastic features are commonly seen in the blastemal componentMost present in later /advanced stages with extra-renal extensionsMetastasis is commoner – 86% develop metastasis (MC Lung)Time to development of mets early – within 1 yr. of diagnosisSurvival (both DFS and OS) poorer than classical variant
CCSK High propensity for metastasis to bone
RTK Most lethal Associated with PNET of the cerebellum or pineal region in 10-15% of pts.
CLINICAL PRESENTATION• Abdominal mass (80-90%)• Abdominal pain (30-40%)• Haematuria (20-25%)• Fever (20-25%)• Hypertension• Varicocele• Metastatic symptoms-rare
• Triad of Wilms Tumour : • Lump, Pain, Haematuria
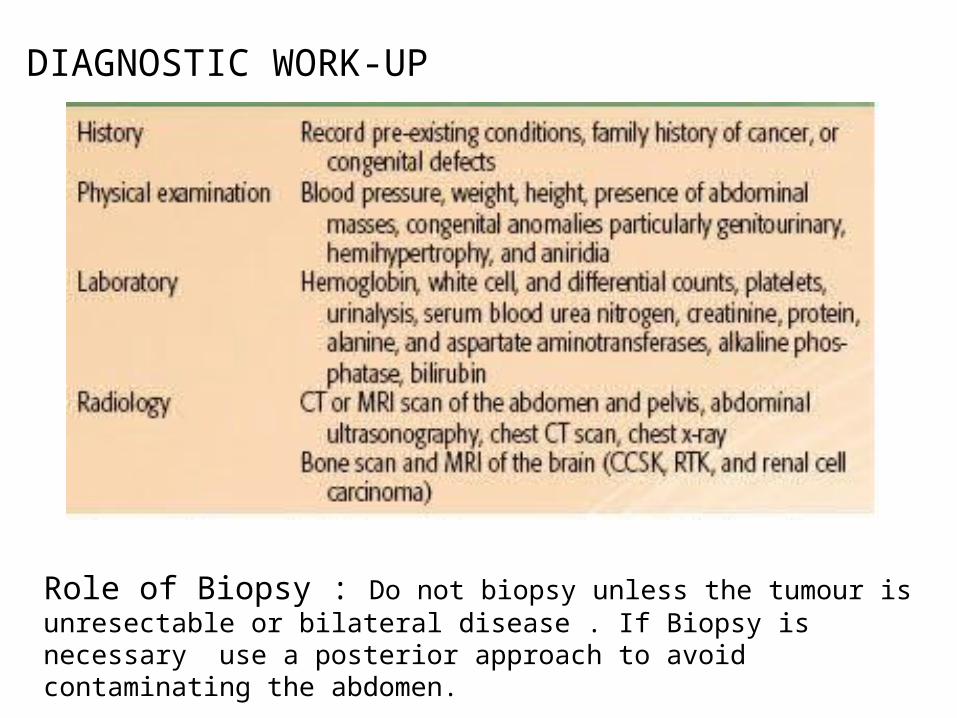
DIAGNOSTIC WORK-UP
Role of Biopsy : Do not biopsy unless the tumour is unresectable or bilateral disease . If Biopsy is necessary use a posterior approach to avoid contaminating the abdomen.
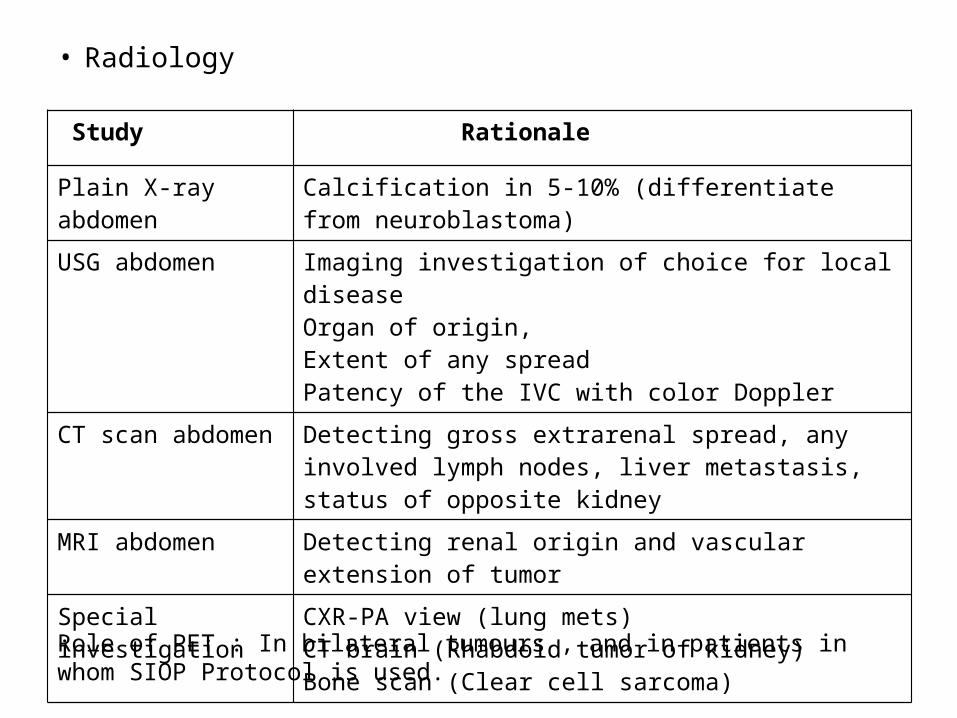
• Radiology
Study Rationale
Plain X-ray abdomen Calcification in 5-10% (differentiate from neuroblastoma)
USG abdomen Imaging investigation of choice for local diseaseOrgan of origin,Extent of any spreadPatency of the IVC with color Doppler
CT scan abdomen Detecting gross extrarenal spread, any involved lymph nodes, liver metastasis, status of opposite kidney
MRI abdomen Detecting renal origin and vascular extension of tumor
Special investigation CXR-PA view (lung mets)CT brain (Rhabdoid tumor of kidney)Bone scan (Clear cell sarcoma)
Role of PET : In bilateral tumours , and in patients in whom SIOP Protocol is used.
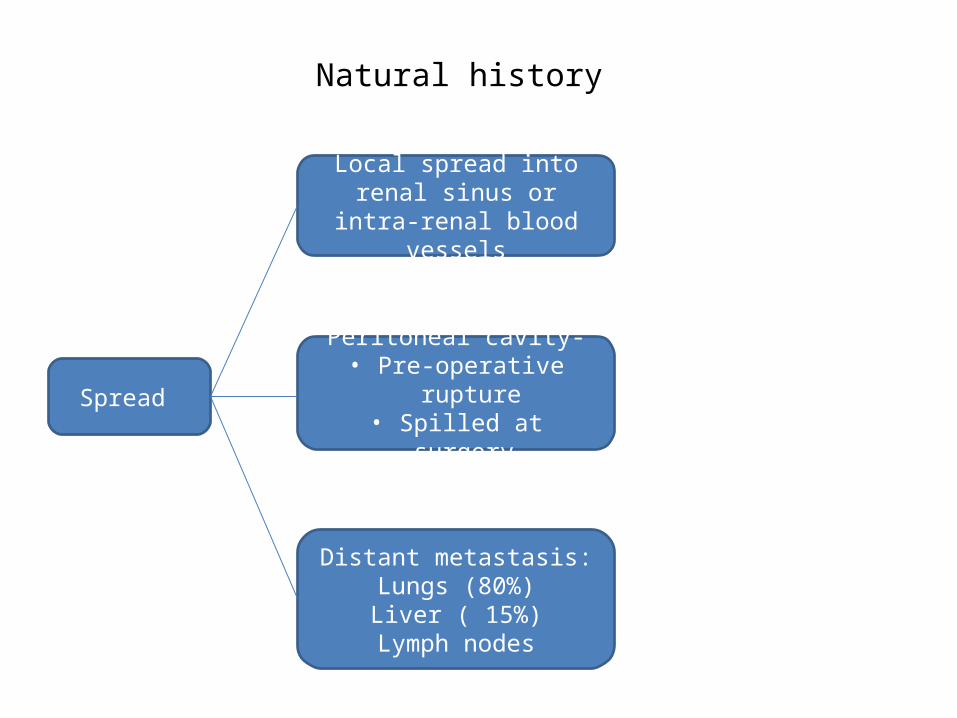
Natural history
Spread
Local spread into renal sinus or intra-renal blood vessels
Distant metastasis:Lungs (80%)Liver ( 15%)
Lymph nodes
Peritoneal cavity-• Pre-operative rupture
• Spilled at surgery

Staging : Given by NWTSG and still followed by COG Group
Treatment
• Treatment options: Surgery Radiotherapy Chemotherapy
Multimodality Management:• Surgery to remove the bulk of the disease • Chemotherapy to eliminate metastatic disease • Radiation therapy to eliminate the risk of local recurrence• Multimodality, stage and risk adapted approach is the standard of care.
Management protocol varies according to: Age of patient Preoperative extent on imaging Operative stage Post operative histology
Surgery followed by adjuvant chemotherapy ± RT
Surgery• Operability should be determined on the table – imaging overestimates
inoperability• Radical nephrectomy and lymph node sampling via a transabdominal or
thoracoabdominal incision is the procedure of choice• The standard procedure includes:
– Unilateral radical nephrectomy– Excision without spillage – Selective sampling of nodes (RPL dissection doesn't alter outcome)– Renal vein and IVC (6% involvement) should be palpated to exclude
intravascular tumor extension– Exploration of the opposite kidney
TREATMENT OPTIONS: NWTS VS SIOP
NWTS• Treatment principle: Nephrectomy
adjuvant chemo ±RT• Advantages: Avoidance of
Administration of chemo to a patient with benign disease
Administration of chemo to a patient with a different histological type of malignant tumour
Modification of tumour histology
Loss of staging information
SIOP• Treatment Principle: Pre-op chemo
Nephrectomy adjuvant chemo ±RT• Advantages:
Tumour downsizing thereby making surgery simpler and ↓ing intra-op tumor rupture & intra-abd recurrence
Makes nephron sparing surgery possible
Moderator: Dr Sushmita Ghoshal
18
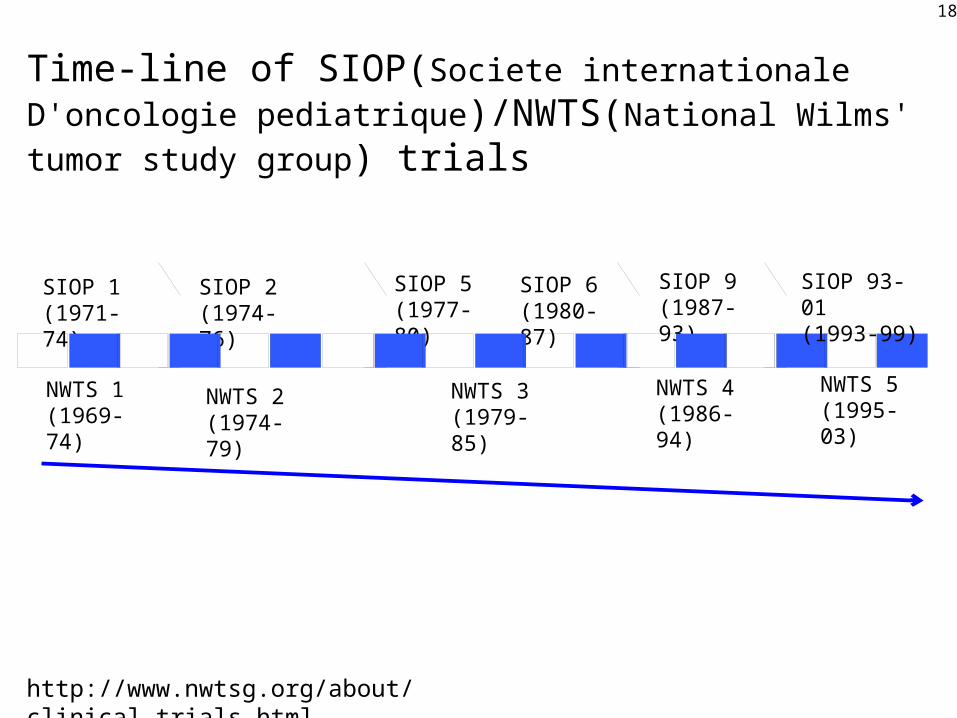
Time-line of SIOP(Societe internationale D'oncologie pediatrique)/NWTS(National Wilms' tumor study group) trials
SIOP 1(1971-74)
SIOP 2(1974-76)
SIOP 5(1977-80)
SIOP 6(1980-87)
SIOP 9(1987-93)
NWTS 1(1969-74)
NWTS 2(1974-79)
NWTS 3(1979-85)
NWTS 4(1986-94)
NWTS 5(1995-03)
SIOP 93-01(1993-99)
http://www.nwtsg.org/about/clinical_trials.html
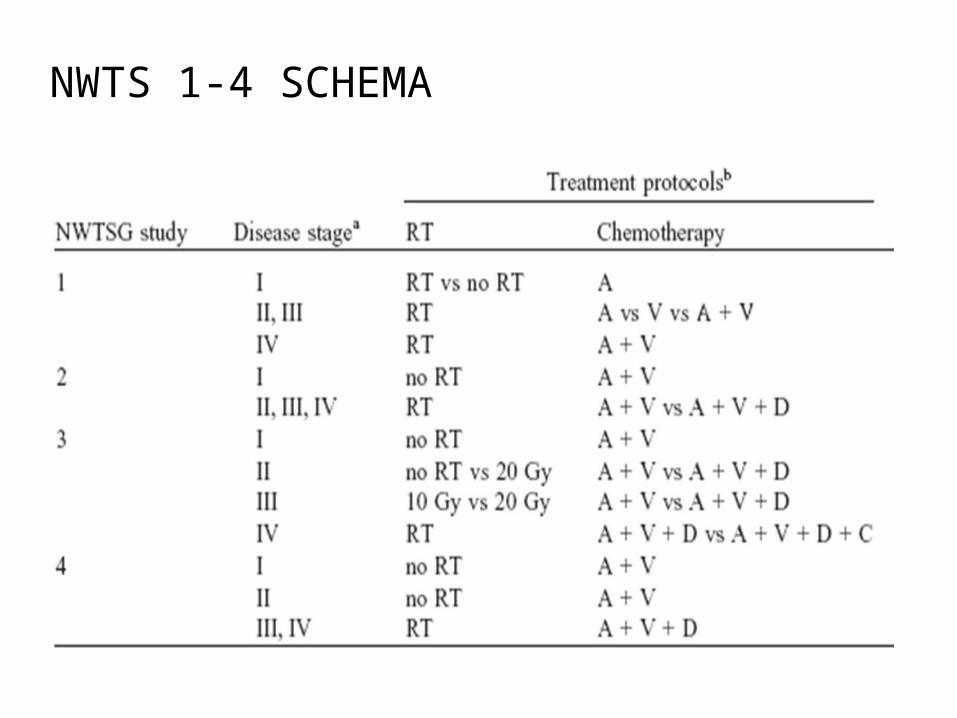
NWTS 1-4 SCHEMA
NWTS STAGE Evaluation
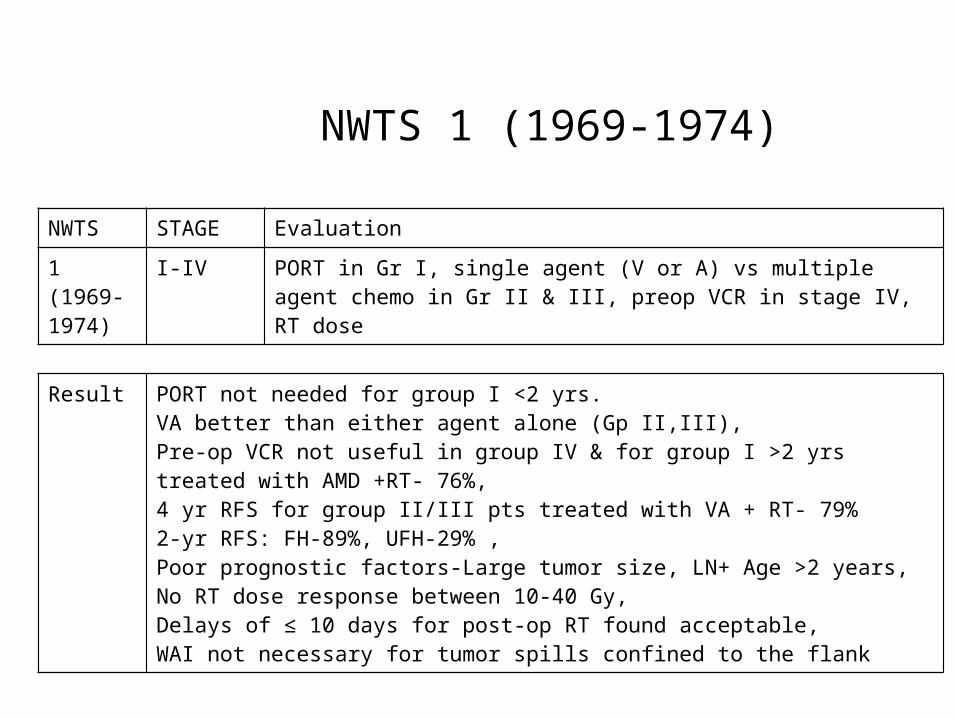
1 (1969-1974)
I-IV PORT in Gr I, single agent (V or A) vs multiple agent chemo in Gr II & III, preop VCR in stage IV, RT dose
Result PORT not needed for group I <2 yrs. VA better than either agent alone (Gp II,III), Pre-op VCR not useful in group IV & for group I >2 yrs treated with AMD +RT- 76%, 4 yr RFS for group II/III pts treated with VA + RT- 79%2-yr RFS: FH-89%, UFH-29% , Poor prognostic factors-Large tumor size, LN+ Age >2 years, No RT dose response between 10-40 Gy, Delays of ≤ 10 days for post-op RT found acceptable, WAI not necessary for tumor spills confined to the flank
NWTS 1 (1969-1974)
NWTS STAGE Evaluation
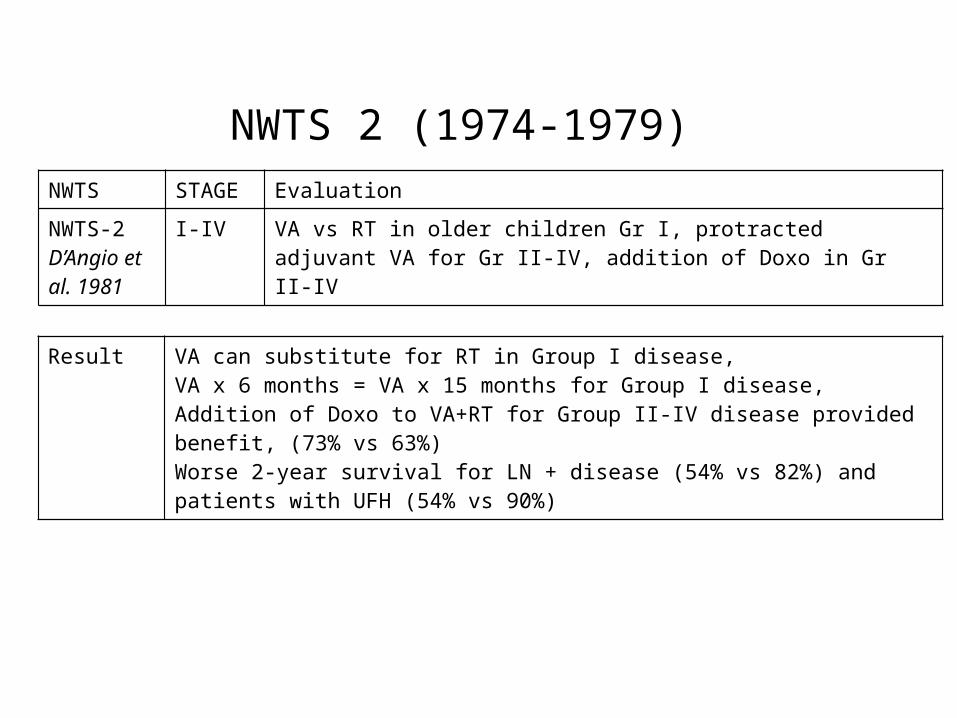
NWTS-2 D’Angio et al. 1981
I-IV VA vs RT in older children Gr I, protracted adjuvant VA for Gr II-IV, addition of Doxo in Gr II-IV
Result VA can substitute for RT in Group I disease, VA x 6 months = VA x 15 months for Group I disease, Addition of Doxo to VA+RT for Group II-IV disease provided benefit, (73% vs 63%)Worse 2-year survival for LN + disease (54% vs 82%) and patients with UFH (54% vs 90%)
NWTS 2 (1974-1979)
NWTS STAGE objective
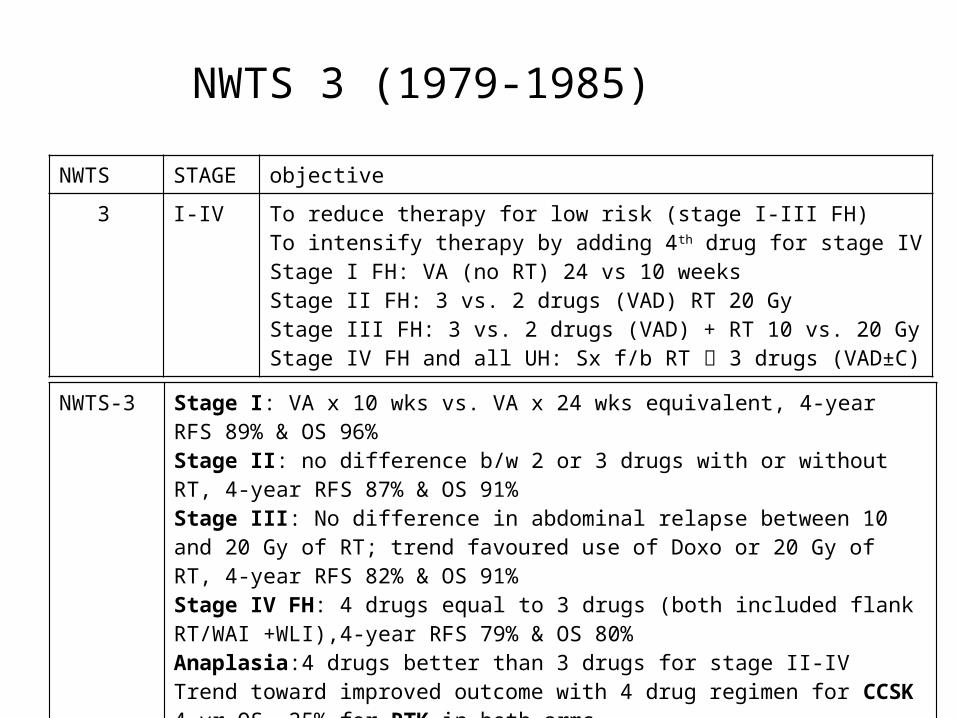
3 I-IV To reduce therapy for low risk (stage I-III FH) To intensify therapy by adding 4th drug for stage IV Stage I FH: VA (no RT) 24 vs 10 weeksStage II FH: 3 vs. 2 drugs (VAD) RT 20 Gy�Stage III FH: 3 vs. 2 drugs (VAD) + RT 10 vs. 20 Gy�Stage IV FH and all UH: Sx f/b RT 3 drugs (VAD±C)
NWTS-3 Stage I: VA x 10 wks vs. VA x 24 wks equivalent, 4-year RFS 89% & OS 96%Stage II: no difference b/w 2 or 3 drugs with or without RT, 4-year RFS 87% & OS 91%Stage III: No difference in abdominal relapse between 10 and 20 Gy of RT; trend favoured use of Doxo or 20 Gy of RT, 4-year RFS 82% & OS 91%Stage IV FH: 4 drugs equal to 3 drugs (both included flank RT/WAI +WLI),4-year RFS 79% & OS 80%Anaplasia:4 drugs better than 3 drugs for stage II-IVTrend toward improved outcome with 4 drug regimen for CCSK4 yr OS -25% for RTK in both arms
NWTS 3 (1979-1985)

NWTS STAGE objective
4Green et al, 1998
I-IV Addressed issues of minimization of therapy and customization bystage & histologyEvaluate the role of pulse dosed intensive chemotherapy
Result Similar survival among pts who received standard course (5 days) or single dose pulse-intensive dactinomycin chemotherapyPulse-intensive therapy was associated with less haematological toxicity and marked reduction of treatment doses.
NWTS 4 (1986-1994)
NWTS STAGE objective
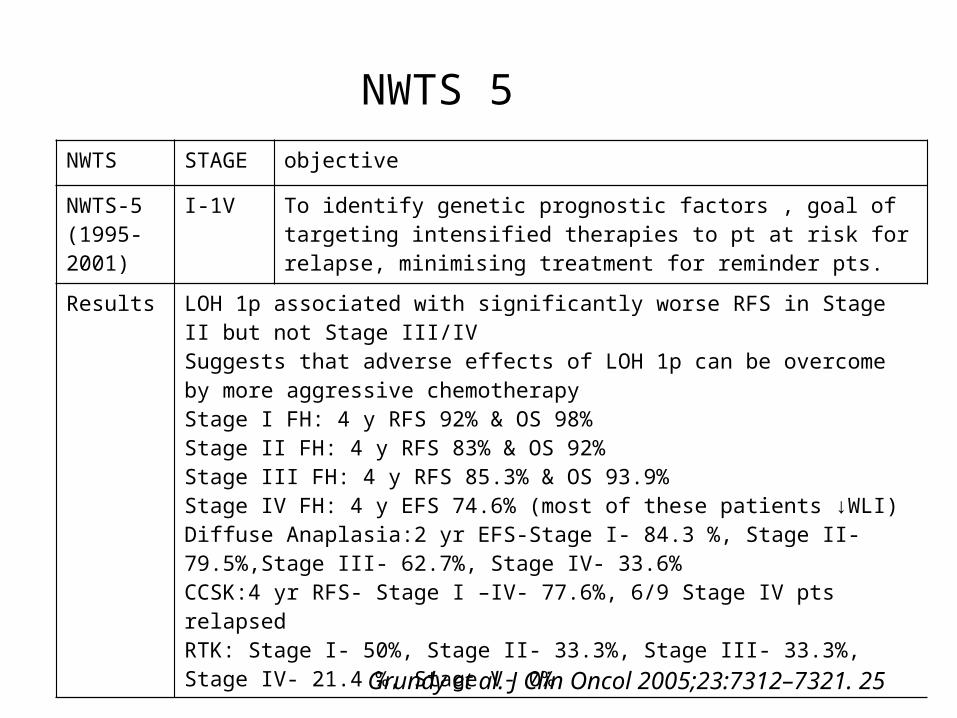
NWTS-5(1995-2001)
I-1V To identify genetic prognostic factors , goal of targeting intensified therapies to pt at risk for relapse, minimising treatment for reminder pts.
Results LOH 1p associated with significantly worse RFS in Stage II but not Stage III/IVSuggests that adverse effects of LOH 1p can be overcome by more aggressive chemotherapyStage I FH: 4 y RFS 92% & OS 98%Stage II FH: 4 y RFS 83% & OS 92%Stage III FH: 4 y RFS 85.3% & OS 93.9%Stage IV FH: 4 y EFS 74.6% (most of these patients ↓WLI)Diffuse Anaplasia:2 yr EFS-Stage I- 84.3 %, Stage II- 79.5%,Stage III- 62.7%, Stage IV- 33.6%CCSK:4 yr RFS- Stage I –IV- 77.6%, 6/9 Stage IV pts relapsedRTK: Stage I- 50%, Stage II- 33.3%, Stage III- 33.3%, Stage IV- 21.4 %, Stage V- 0%
NWTS 5
Grundy et al. J Clin Oncol 2005;23:7312–7321. 25
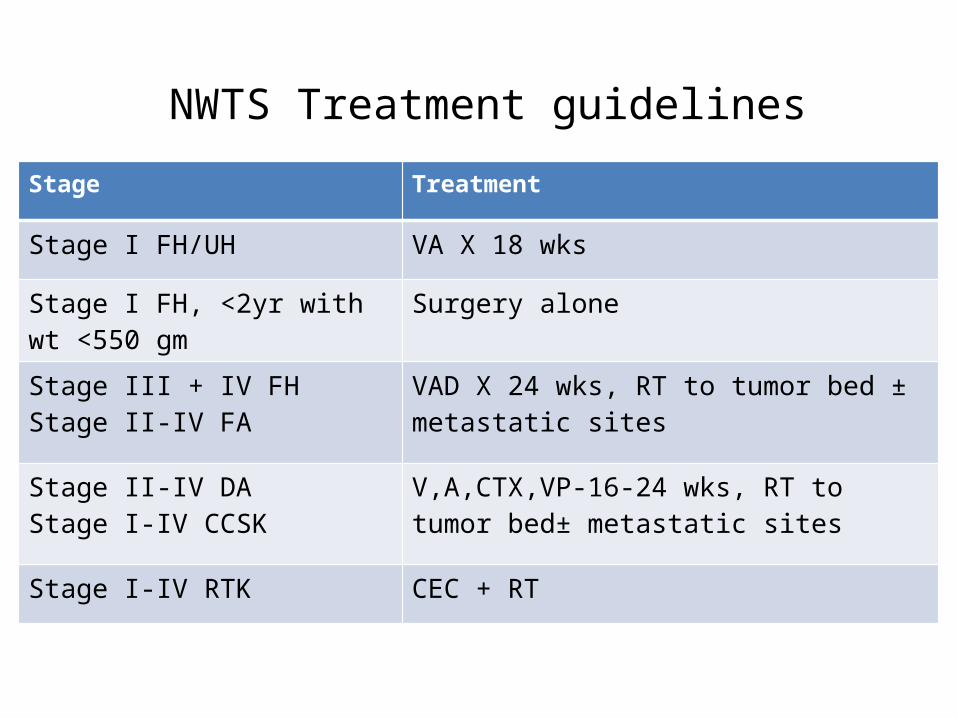
NWTS Treatment guidelines
Stage Treatment
Stage I FH/UH VA X 18 wks
Stage I FH, <2yr with wt <550 gm
Surgery alone
Stage III + IV FHStage II-IV FA
VAD X 24 wks, RT to tumor bed ± metastatic sites
Stage II-IV DAStage I-IV CCSK
V,A,CTX,VP-16-24 wks, RT to tumor bed± metastatic sites
Stage I-IV RTK CEC + RT
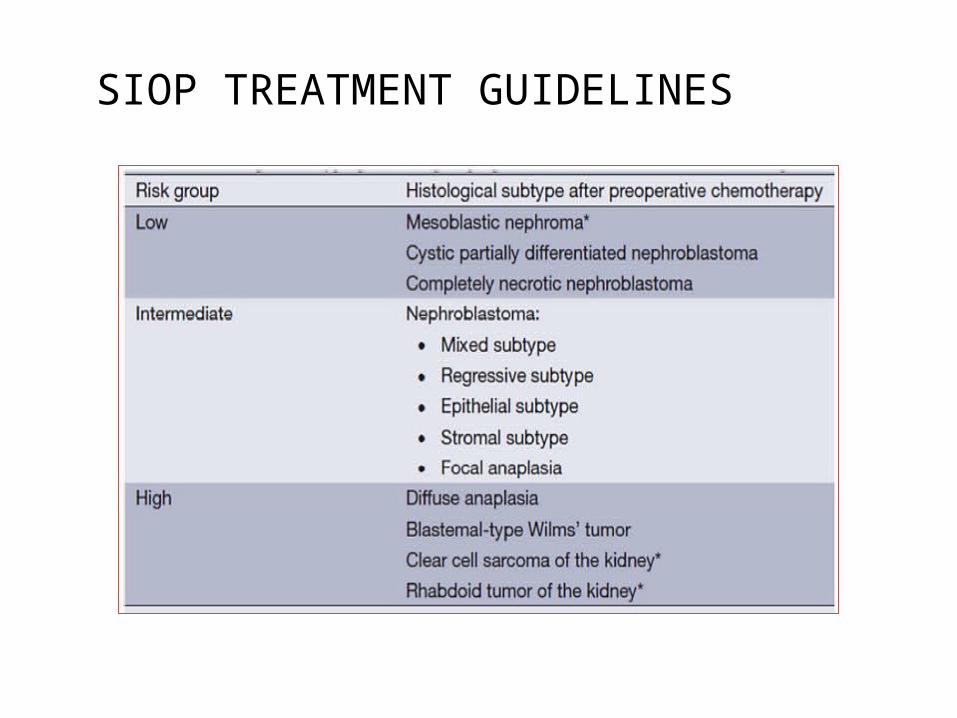
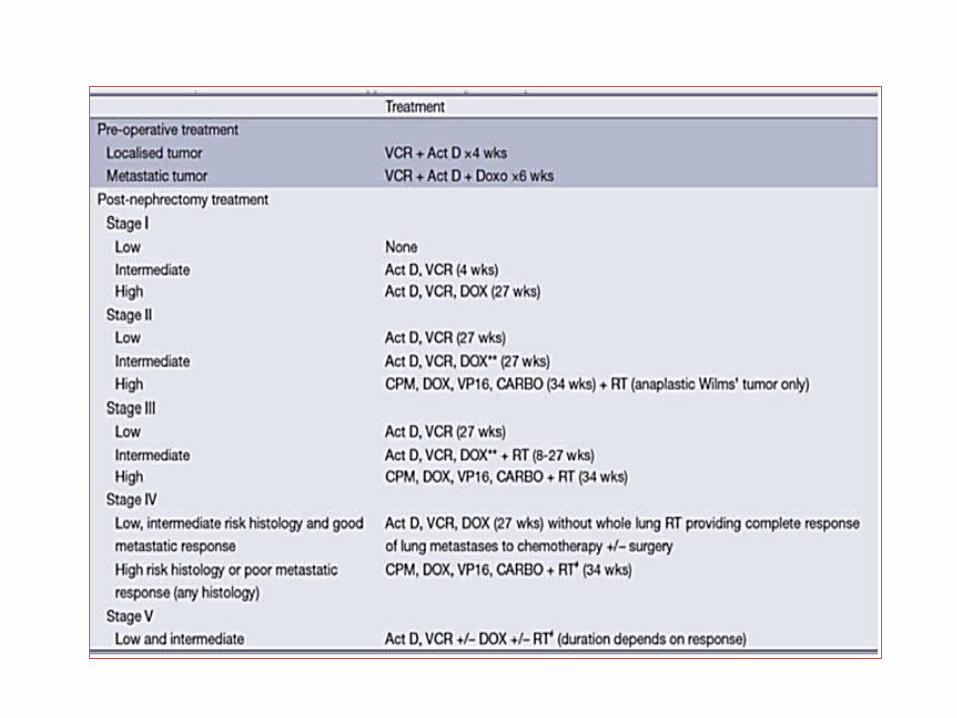
SIOP TREATMENT GUIDELINES
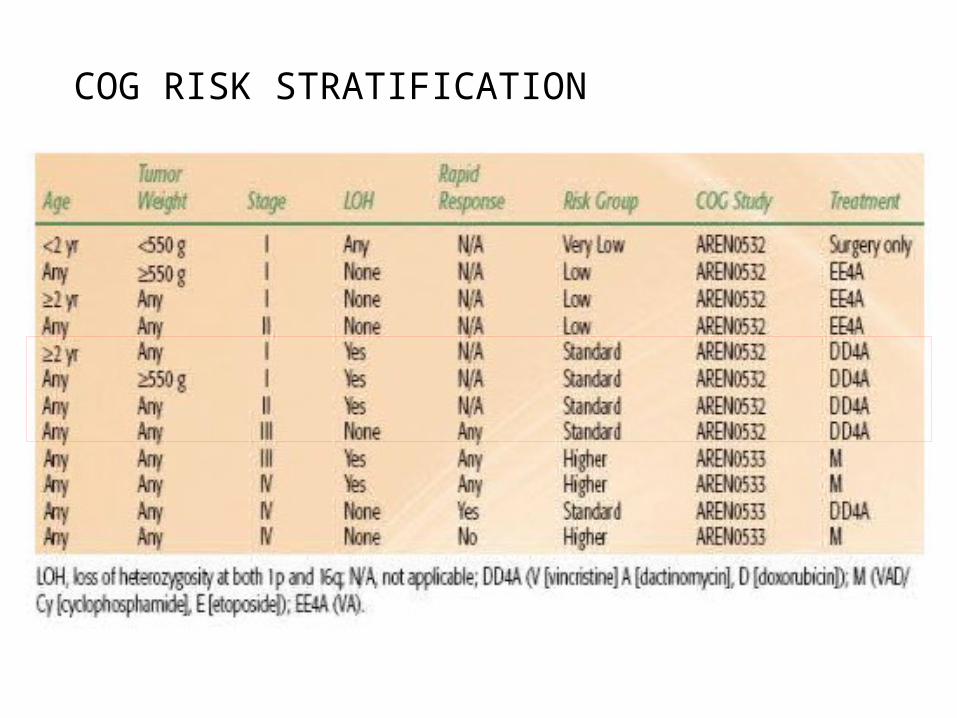
COG RISK STRATIFICATION
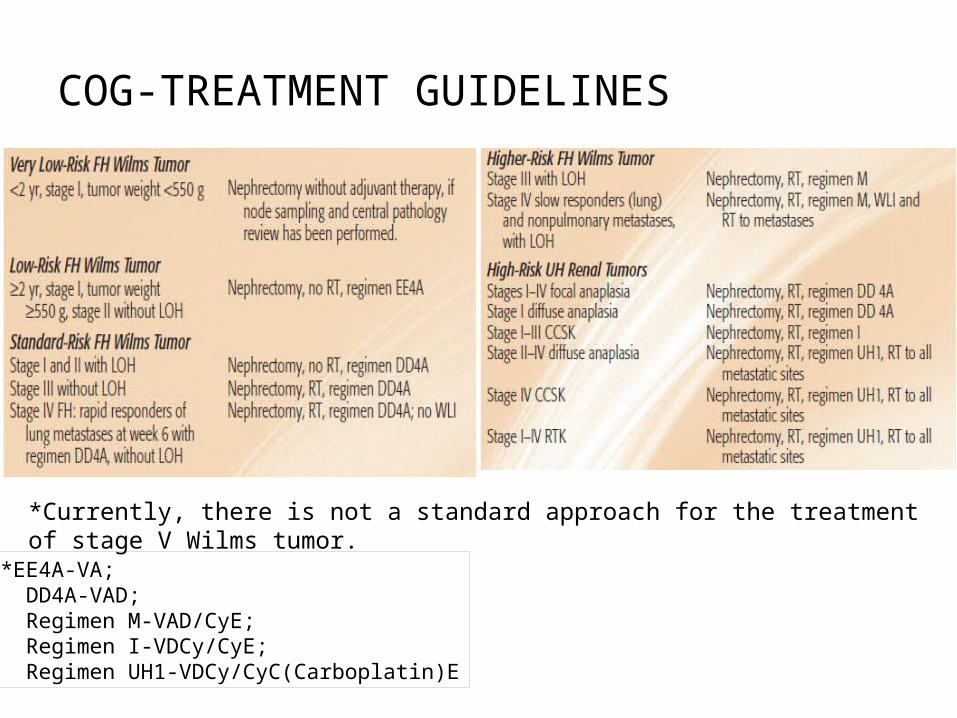
COG-TREATMENT GUIDELINES
*EE4A-VA; DD4A-VAD; Regimen M-VAD/CyE; Regimen I-VDCy/CyE; Regimen UH1-VDCy/CyC(Carboplatin)E
*Currently, there is not a standard approach for the treatment of stage V Wilms tumor.

30
CURRENT PROTOCOLS
• AREN 0532– FH Stage I through FH Stage III Standard Risk
31
AREN 0533 & AREN 0321
• AREN 0533 FH Stage III High RiskFH Stage IV
• AREN 0321 UH Wilms’CCSKRTKRCC
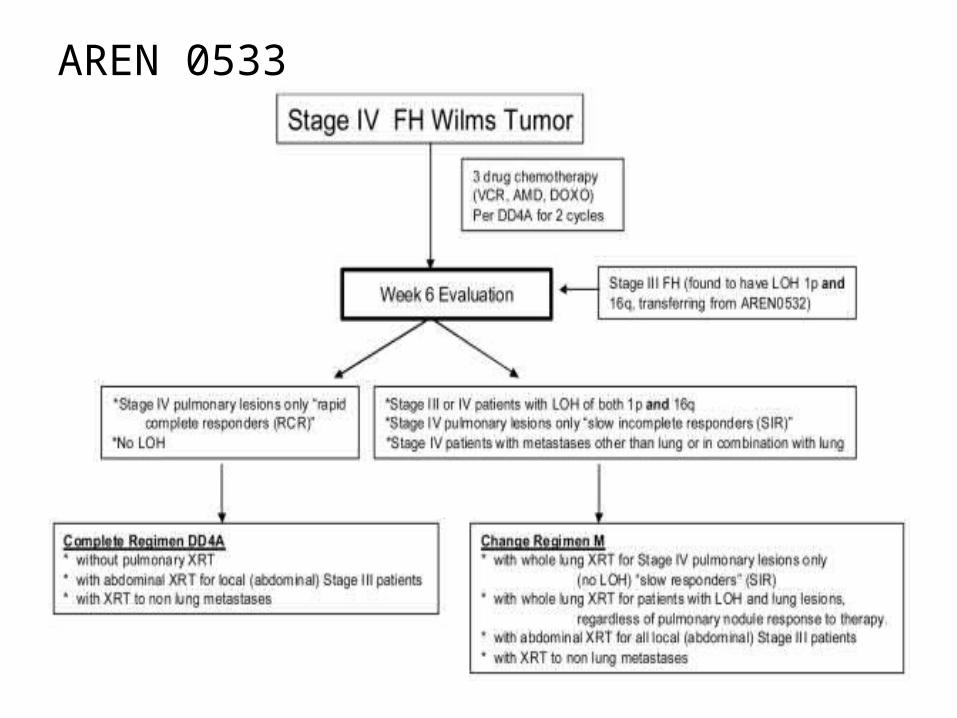
AREN 0533
Radiation techniques
Flank Radiation• The technique mostly utilized is a parallel opposing AP arrangement• Patient is planned and treated in the supine position.• Pediatric anesthesia is sometimes necessary• Treatment Portal design:
– Should encompass the tumor bed and the site of the excised kidney
– 2-3 cm margins should be given circumferentially– The medial border must cross the midline to include the entire
width of the vertebrae• Beam energy: Best treated with beam energies of 4-6 MV• Dose : 10.8 Gy in 1.8 Gy per fraction over 6 fractions.
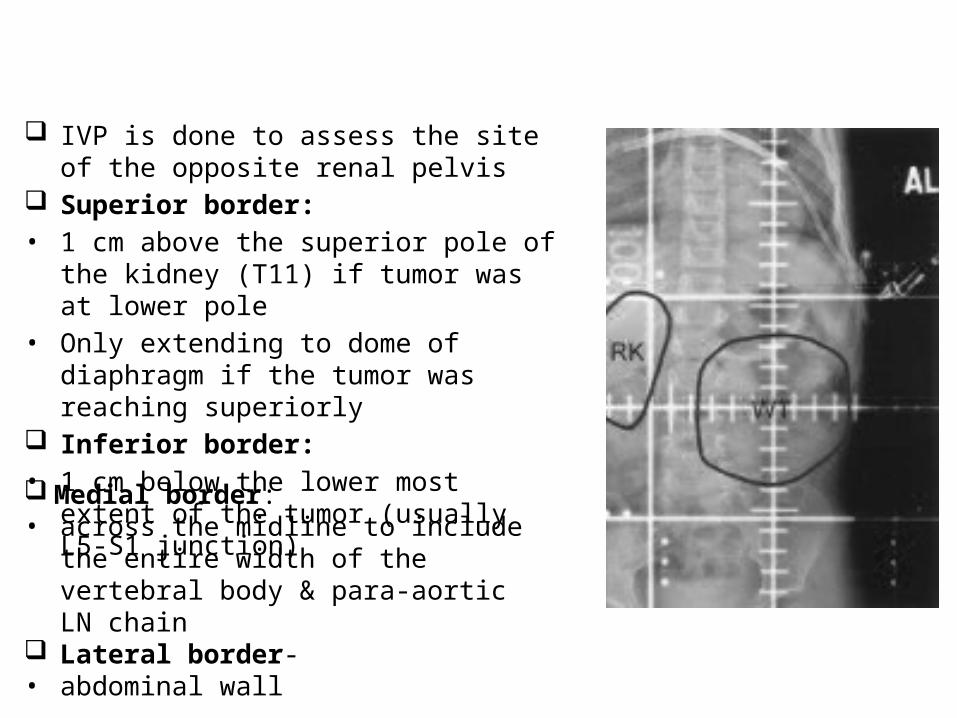
IVP is done to assess the site of the opposite renal pelvis
Superior border:• 1 cm above the superior pole of the kidney
(T11) if tumor was at lower pole• Only extending to dome of diaphragm if the
tumor was reaching superiorly Inferior border:• 1 cm below the lower most extent of the
tumor (usually L5-S1 junction) Medial border:• across the midline to include the entire width
of the vertebral body & para-aortic LN chain Lateral border- • abdominal wall
Whole Abdomen Irradiation (WAI)• The indications are:
– Diffuse peritoneal implantation– Diffuse tumor spillage during surgery– Preoperative tumor rupture
• Dose prescribed is 10.8 Gy in 1.5 Gy / # - this can be followed by a selected boost of 10.5 Gy to the Tumor bed.
• Biweekly hemogram is necessary.• Typical energy selected is 4-6 MV photons
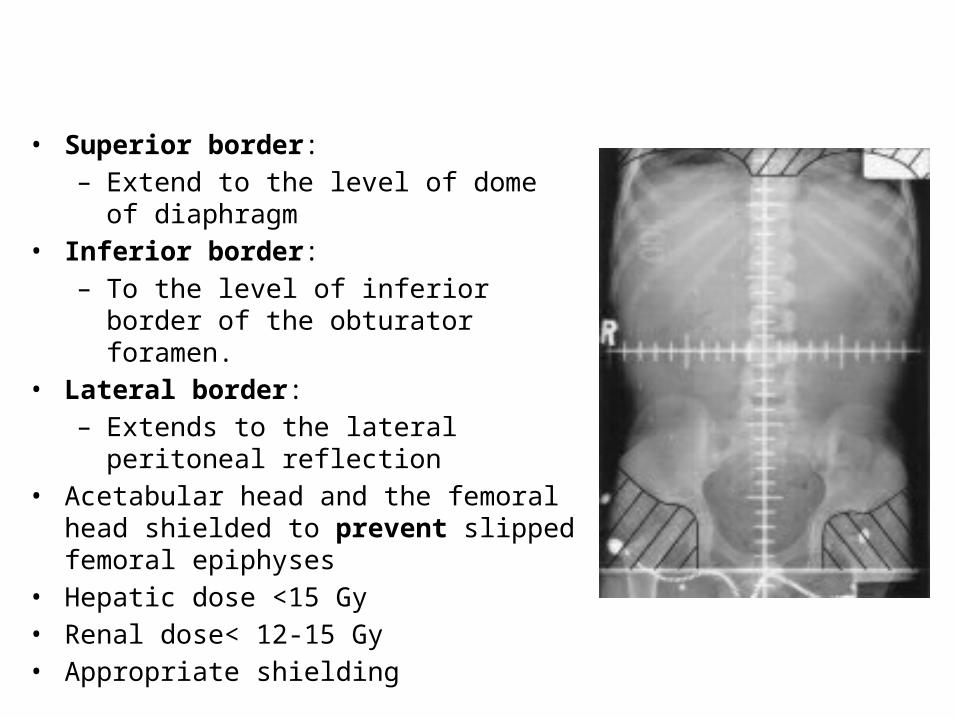
• Superior border:– Extend to the level of dome of diaphragm
• Inferior border:– To the level of inferior border of the
obturator foramen.• Lateral border:
– Extends to the lateral peritoneal reflection• Acetabular head and the femoral head shielded
to prevent slipped femoral epiphyses• Hepatic dose <15 Gy• Renal dose< 12-15 Gy• Appropriate shielding
CONFORMAL PLANNING
• GTV Pre-op tumour volume using co-registered MR-CT scans
• CTVGTV+1 cm isotropic expansion
• PTVCTV+SM+IM
• AP-PA beam arrangement with MLC shaping
• Aim Adequate target coverage with symmetrical irradiation of vertebrae, avoidance of contralateral kidney & minimisation of whole body dose
• IMRT rarely needed & conformal treatment adequate

Whole Lung Irradiation (WLI)
• Recommended in the NWTS protocol in patients with CXR defined* lung mets
• WLI indicated when there is no CR seen on CT at wk 6 after 3-drug chemo
• Pulmonary RT complications:– Radiation pneumonitis : CCT dose reduction by 50%
recommended– Pneumocystis carinii pneumonia (TMP-SMX Px)
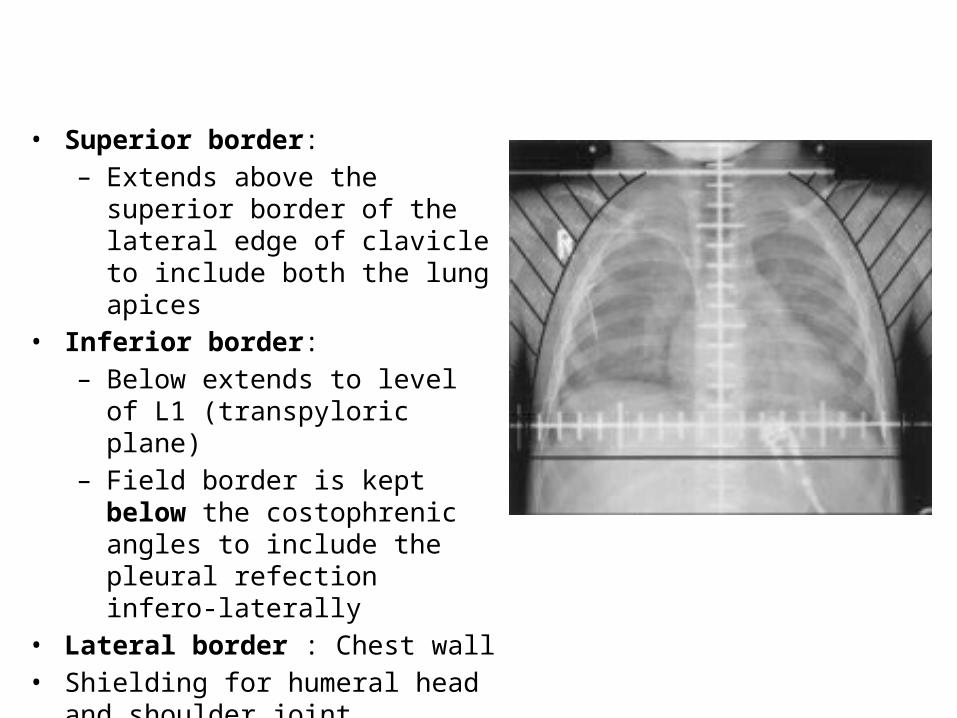
• Superior border:– Extends above the superior border
of the lateral edge of clavicle to include both the lung apices
• Inferior border:– Below extends to level of L1
(transpyloric plane)– Field border is kept below the
costophrenic angles to include the pleural refection infero-laterally
• Lateral border : Chest wall• Shielding for humeral head and
shoulder joint necessary bilaterally.• Some add a midline shield for larynx.
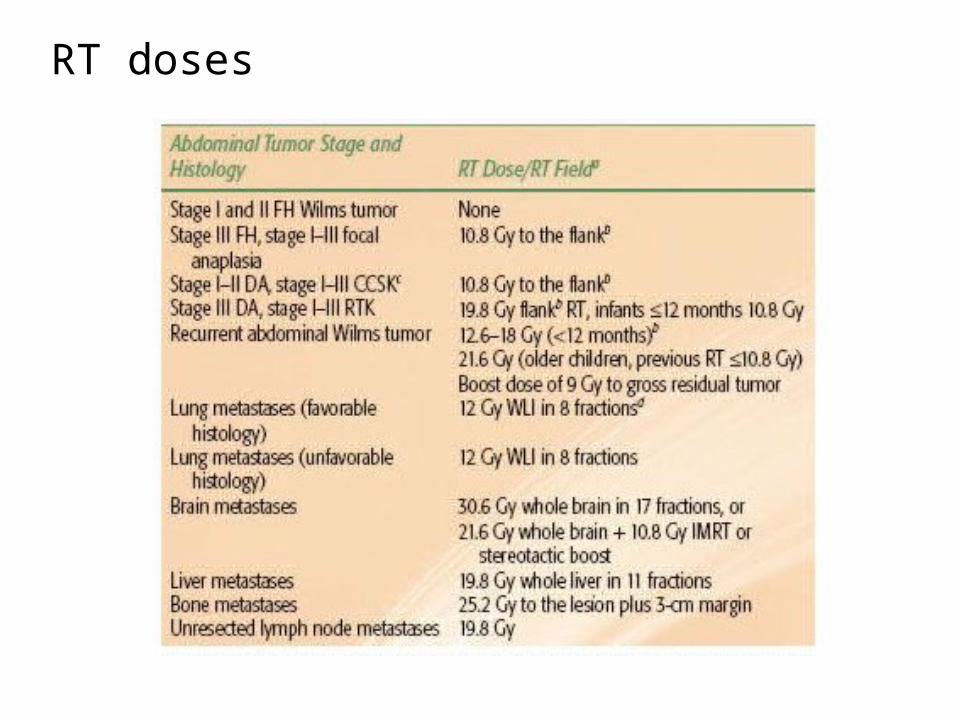
RT doses
LATE EFFECTS OF TREATMENT
• Scoliosis - 54% in patients treated with a median dose of 30Gy - Thomas et al. IJROBP 1983;9:651-57.
• CHF-4.4% at 20 years (NWTS1-4) - Green et al. JCO 2001;19:1926-34.
• End stage renal disease (ESRD)-20 year cumulative incidence• 74% in children with Denys-Drash syndrome• 36% in children with WAGR syndrome• 7% in children with GU abnormalities• 0.6% in children without any syndrome/ abnormality - Breslow NE et al. J Urol 2005;174:1972-75.
• Second malignant neoplasm (SMN)-15 year cumulative incidence 1.6%• Leukaemia/ lymphoma incidence 0.4% at 8 years with no case thereafter• Solid malignancy incidence continued to rise sharply with time• 73% of the solid malignancies arose in previous RT field• Associated factors: higher dose of RT, use of Doxorubicin & Rx of relapse - Breslow et al. JCO 1995;13:1851-59.
• Adverse pregnancy outcome-• Foetal malposition• Premature labour• LBW baby• Congenital malformation - Green et al. JCO 2010;28:2824-30.
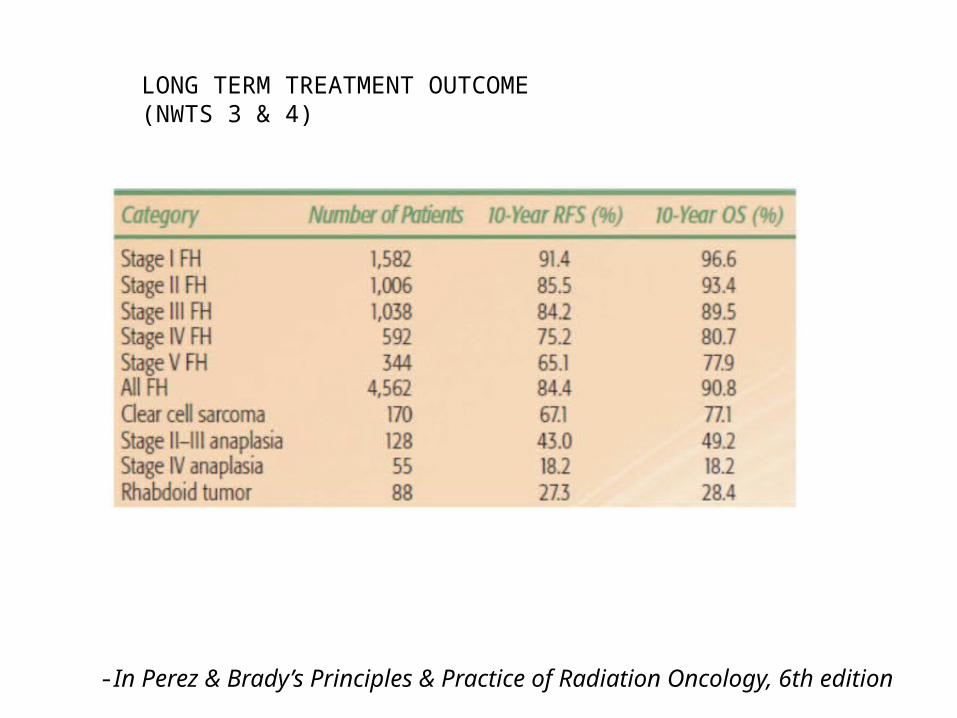
LONG TERM TREATMENT OUTCOME(NWTS 3 & 4)
-In Perez & Brady’s Principles & Practice of Radiation Oncology, 6th edition
THANK YOU