vascularized organoid engineered by modular assembly ... · vascularized organoid engineered by...
TRANSCRIPT

Vascularized organoid engineered by modularassembly enables blood perfusionAlison P. McGuigan and Michael V. Sefton*
Department of Chemical Engineering and Applied Chemistry and Institute of Biomaterials and Biomedical Engineering, University of Toronto,164 College Street, Toronto, ON, Canada M5S 3G9
Edited by Robert Langer, Massachusetts Institute of Technology, Cambridge, MA, and approved June 15, 2006 (received for review April 5, 2006)
Tissue engineering is one approach to address the donor-organshortage, but to attain clinically significant viable cell densities inthick tissues, laboratory-constructed tissues must have an internalvascular supply. We have adopted a biomimetic approach andassembled microscale modular components, consisting of submil-limeter-sized collagen gel rods seeded with endothelial cells (ECs)into a (micro)vascularized tissue; in some prototypes the gelcontained HepG2 cells to illustrate the possibilities. The EC-coveredmodules then were assembled into a larger tube and perfused withmedium or whole blood. The interstitial spaces among the modulesformed interconnected channels that enabled this perfusion. Via-ble cell densities were high, within an order of magnitude of celldensities within tissues, and the percolating nature of the flowthrough the construct was evident in microcomputed tomographyand Doppler ultrasound measurements. Most importantly, the ECsretained their nonthrombogenic phenotype and delayed clottingtimes and inhibited the loss of platelets associated with perfusionof whole blood through the construct. Unlike the conventionalscaffold and cell-seeding paradigm of other tissue-engineeringapproaches, this modular construct has the potential to be scalable,uniform, and perfusable with whole blood, circumventing thelimitations of other approaches.
collagen gel modules � endothelial cells � tissue engineering
H ierarchical structures self-assembled from discrete mod-ular components are widespread in nature at both the
molecular and macroscopic scales. Organs, for example, arebuilt up from modular components such as the nephron or liverlobule. Adapting this principle, mesoscale modular arrange-ments have been self-assembled artificially for a range ofengineering applications (1). Here we have devised a biomi-metic modular approach to create a previously undescribed,potentially scalable tissue-engineered construct that ultimatelymight address donor-organ shortages or could be used as avascularized in vitro 3D culture model. Laboratory-engineeredtissues with dimensions greater than a few hundred microme-ters require an internal vascular supply to attain clinicallysignificant viable cell densities. We have assembled microscalemodular components with thrombosis-inhibiting characteris-tics into a vascularized tissue, which was perfused with wholeblood without significant platelet loss. The modular constructcontained a uniform cell distribution and enabled the incor-poration of multiple cell types in a form that is theoreticallyscalable, unlike other scaffold methods.
Engineering an artificial tissue conventionally involves seed-ing healthy cells into a preformed, porous, and biodegradablescaffold (2). The utility of such constructs, as a potential organsource to alleviate donor shortages, is limited, however, by theabsence of an internal vascular supply, such that cell viabilityis maintained exclusively by oxygen diffusion from the sur-rounding host. At the cell densities of normal tissues, thisdiffusion limitation restricts viable engineered constructs to�100–200 �m in thickness (3). Devices with larger dimensionsare possible only by reducing cell density or by tolerating a verylow oxygen concentration. Moreover, achieving a high-density,
uniform cell distribution throughout a scaffold is difficultbecause cells primarily populate the periphery (�1 mm) of thescaffold (4). Furthermore, typical scaffolds do not facilitatethe controlled mixing of multiple cell types, which may pro-mote long-term cell function through paracrine and otherinteractions, because the specific growth rates of the differentcell types can alter their ratio and relative location. Strategiesthat enable fabrication of large vascularized constructs withhigh, uniform cell densities, within which multiple cell typescan be incorporated, are essential for engineering wholeorgans comprised of highly metabolic cells. Although each ofthese scaffold-related problems is being addressed separatelyelsewhere (4–9), here we report the development of modularassembly as a theoretically scalable strategy to provide avascularized construct with uniform cell density, here con-taining two cell types. Furthermore, we demonstrate thecapacity of the endothelial cell (EC)-seeded construct to beperfused with whole blood in vitro, which has not previouslybeen reported for a (micro)vascularized engineered construct.
Instead of seeding a preformed scaffold with cells, HepG2cells (as a model cell) were encapsulated in short cylindricalcollagen gel modules (Fig. 1 a and b), and the outer surface ofthese modules was covered with a conf luent layer of humanumbilical vein endothelial cells (HUVEC) (Fig. 1 a and c).These modules then were assembled randomly into a largerstructure (here a tube) to form the modular construct (Fig.1d). The interstitial spaces, formed between the assembledmodules, constituted HUVEC-lined interconnected channels,on the order of a few hundred micrometers in size, thatpermeated the modular construct, enabling f luid and partic-ularly blood perfusion. Even though these channels are notcapillary-like in scale or structure, and they do not replicatethe ‘‘tree-like’’ native vascular structure, the seeded ECs(uniform throughout the construct, unlike native vasculature)were expected to control the dynamic balance of pro- andanti-thrombogenic factors to maintain continuous blood f lowwithout thrombosis. We envision that the modular construct,in an appropriate organ-like shape, will be connected to thevascular supply of the host by using appropriate host vessels orartificial vascular grafts. Modular constructs (albeit on a muchsmaller scale) resemble packed beds, a common and wellunderstood component in chemical engineering (10).
The quiescent, nonthrombogenic EC lining within the chan-nels of the modular construct is critical to enable whole bloodto percolate around the modules with a significantly lowerlevel of thrombosis than that associated with biomaterialsurfaces. HUVEC are useful in this context because theyexpress low basal levels of tissue factor, a potent coagulationinitiator (11). Collagen was selected for the module base
Conflict of interest statement: No conflicts declared.
This paper was submitted directly (Track II) to the PNAS office.
Abbreviations: EC, endothelial cell; HUVEC, human umbilical vein ECs; AB, Alamar blue; PE,polyethylene.
*To whom correspondence should be addressed. E-mail: [email protected].
© 2006 by The National Academy of Sciences of the USA
www.pnas.org�cgi�doi�10.1073�pnas.0602740103 PNAS � August 1, 2006 � vol. 103 � no. 31 � 11461–11466
APP
LIED
BIO
LOG
ICA
LSC
IEN
CES
ENG
INEE
RIN
G
material in the prototype because HUVEC naturally reside ona type IV collagen membrane, albeit not the same type as that(type I) which is readily available. It is possible to incorporateother extracellular matrix components, such as type IV colla-gen, elastin peptides, and glycosaminoglycans, during modulefabrication to further enhance the function of the modules.
This biomimetic modular design strategy has several intrin-sic benefits. Constructs are potentially scalable: High-cell-density modules can be assembled into any overall size andshape with a uniform cell distribution simply by using moremodules. The small dimensions of the modules and the inter-connected channels through which blood f lows are expected toallow for relatively high mass transfer coefficients [followingthe extensive engineering literature on f low through packedbeds (10)] and hence good nutrient and oxygen supply to theencapsulated cells, which ideally should be within �100–200�m of a f low channel. Furthermore, modules encapsulatingdifferent cell types can be mixed to prepare constructs withmultiple cell types in controlled ratios and in different loca-tions within the overall construct.
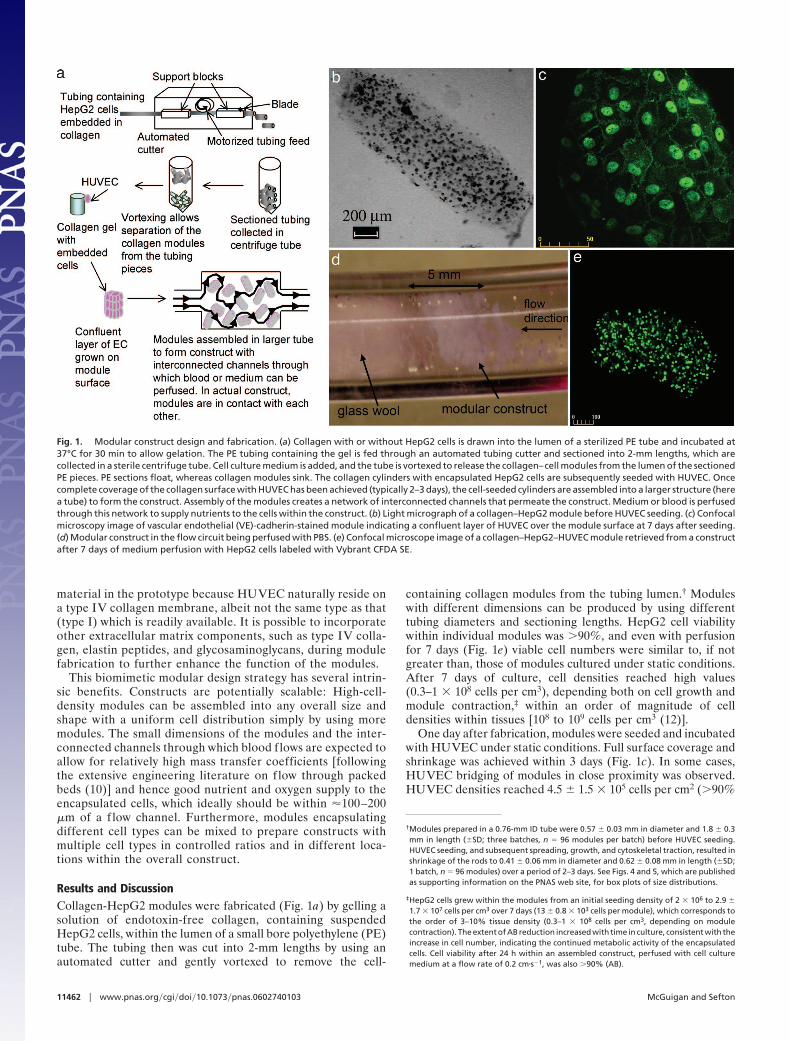
Results and DiscussionCollagen-HepG2 modules were fabricated (Fig. 1a) by gelling asolution of endotoxin-free collagen, containing suspendedHepG2 cells, within the lumen of a small bore polyethylene (PE)tube. The tubing then was cut into 2-mm lengths by using anautomated cutter and gently vortexed to remove the cell-
containing collagen modules from the tubing lumen.† Moduleswith different dimensions can be produced by using differenttubing diameters and sectioning lengths. HepG2 cell viabilitywithin individual modules was �90%, and even with perfusionfor 7 days (Fig. 1e) viable cell numbers were similar to, if notgreater than, those of modules cultured under static conditions.After 7 days of culture, cell densities reached high values(0.3–1 � 108 cells per cm3), depending both on cell growth andmodule contraction,‡ within an order of magnitude of celldensities within tissues [108 to 109 cells per cm3 (12)].
One day after fabrication, modules were seeded and incubatedwith HUVEC under static conditions. Full surface coverage andshrinkage was achieved within 3 days (Fig. 1c). In some cases,HUVEC bridging of modules in close proximity was observed.HUVEC densities reached 4.5 � 1.5 � 105 cells per cm2 (�90%
†Modules prepared in a 0.76-mm ID tube were 0.57 � 0.03 mm in diameter and 1.8 � 0.3mm in length (�SD; three batches, n � 96 modules per batch) before HUVEC seeding.HUVEC seeding, and subsequent spreading, growth, and cytoskeletal traction, resulted inshrinkage of the rods to 0.41 � 0.06 mm in diameter and 0.62 � 0.08 mm in length (�SD;1 batch, n � 96 modules) over a period of 2–3 days. See Figs. 4 and 5, which are publishedas supporting information on the PNAS web site, for box plots of size distributions.
‡HepG2 cells grew within the modules from an initial seeding density of 2 � 106 to 2.9 �
1.7 � 107 cells per cm3 over 7 days (13 � 0.8 � 103 cells per module), which corresponds tothe order of 3–10% tissue density (0.3–1 � 108 cells per cm3, depending on modulecontraction). The extent of AB reduction increased with time in culture, consistent with theincrease in cell number, indicating the continued metabolic activity of the encapsulatedcells. Cell viability after 24 h within an assembled construct, perfused with cell culturemedium at a flow rate of 0.2 cm�s�1, was also �90% (AB).
Fig. 1. Modular construct design and fabrication. (a) Collagen with or without HepG2 cells is drawn into the lumen of a sterilized PE tube and incubated at37°C for 30 min to allow gelation. The PE tubing containing the gel is fed through an automated tubing cutter and sectioned into 2-mm lengths, which arecollected in a sterile centrifuge tube. Cell culture medium is added, and the tube is vortexed to release the collagen–cell modules from the lumen of the sectionedPE pieces. PE sections float, whereas collagen modules sink. The collagen cylinders with encapsulated HepG2 cells are subsequently seeded with HUVEC. Oncecomplete coverage of the collagen surface with HUVEC has been achieved (typically 2–3 days), the cell-seeded cylinders are assembled into a larger structure (herea tube) to form the construct. Assembly of the modules creates a network of interconnected channels that permeate the construct. Medium or blood is perfusedthrough this network to supply nutrients to the cells within the construct. (b) Light micrograph of a collagen–HepG2 module before HUVEC seeding. (c) Confocalmicroscopy image of vascular endothelial (VE)-cadherin-stained module indicating a confluent layer of HUVEC over the module surface at 7 days after seeding.(d) Modular construct in the flow circuit being perfused with PBS. (e) Confocal microscope image of a collagen–HepG2–HUVEC module retrieved from a constructafter 7 days of medium perfusion with HepG2 cells labeled with Vybrant CFDA SE.
11462 � www.pnas.org�cgi�doi�10.1073�pnas.0602740103 McGuigan and Sefton
viable) within 7 days, consistent with confluent HUVEC den-sities observed on tissue culture polystyrene.
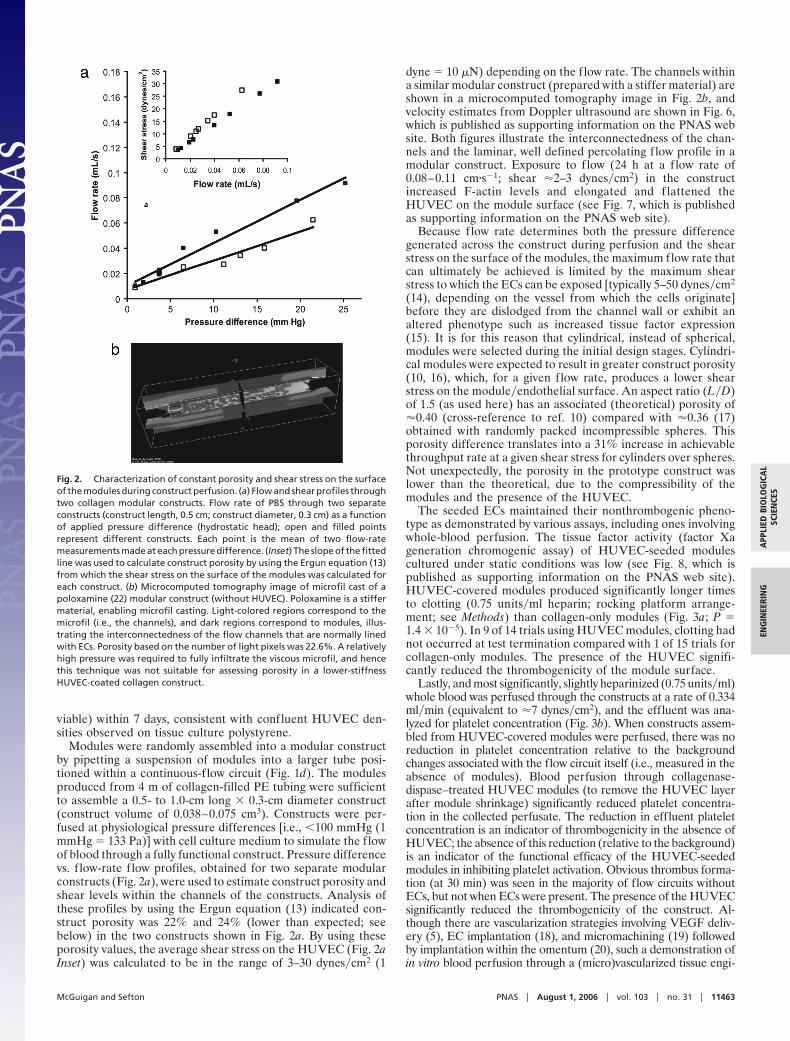
Modules were randomly assembled into a modular constructby pipetting a suspension of modules into a larger tube posi-tioned within a continuous-f low circuit (Fig. 1d). The modulesproduced from 4 m of collagen-filled PE tubing were sufficientto assemble a 0.5- to 1.0-cm long � 0.3-cm diameter construct(construct volume of 0.038–0.075 cm3). Constructs were per-fused at physiological pressure differences [i.e., �100 mmHg (1mmHg � 133 Pa)] with cell culture medium to simulate the flowof blood through a fully functional construct. Pressure differencevs. f low-rate flow profiles, obtained for two separate modularconstructs (Fig. 2a), were used to estimate construct porosity andshear levels within the channels of the constructs. Analysis ofthese profiles by using the Ergun equation (13) indicated con-struct porosity was 22% and 24% (lower than expected; seebelow) in the two constructs shown in Fig. 2a. By using theseporosity values, the average shear stress on the HUVEC (Fig. 2aInset) was calculated to be in the range of 3–30 dynes�cm2 (1
dyne � 10 �N) depending on the flow rate. The channels withina similar modular construct (prepared with a stiffer material) areshown in a microcomputed tomography image in Fig. 2b, andvelocity estimates from Doppler ultrasound are shown in Fig. 6,which is published as supporting information on the PNAS website. Both figures illustrate the interconnectedness of the chan-nels and the laminar, well defined percolating flow profile in amodular construct. Exposure to flow (24 h at a flow rate of0.08–0.11 cm�s�1; shear �2–3 dynes�cm2) in the constructincreased F-actin levels and elongated and f lattened theHUVEC on the module surface (see Fig. 7, which is publishedas supporting information on the PNAS web site).
Because flow rate determines both the pressure differencegenerated across the construct during perfusion and the shearstress on the surface of the modules, the maximum flow rate thatcan ultimately be achieved is limited by the maximum shearstress to which the ECs can be exposed [typically 5–50 dynes�cm2
(14), depending on the vessel from which the cells originate]before they are dislodged from the channel wall or exhibit analtered phenotype such as increased tissue factor expression(15). It is for this reason that cylindrical, instead of spherical,modules were selected during the initial design stages. Cylindri-cal modules were expected to result in greater construct porosity(10, 16), which, for a given flow rate, produces a lower shearstress on the module�endothelial surface. An aspect ratio (L�D)of 1.5 (as used here) has an associated (theoretical) porosity of�0.40 (cross-reference to ref. 10) compared with �0.36 (17)obtained with randomly packed incompressible spheres. Thisporosity difference translates into a 31% increase in achievablethroughput rate at a given shear stress for cylinders over spheres.Not unexpectedly, the porosity in the prototype construct waslower than the theoretical, due to the compressibility of themodules and the presence of the HUVEC.
The seeded ECs maintained their nonthrombogenic pheno-type as demonstrated by various assays, including ones involvingwhole-blood perfusion. The tissue factor activity (factor Xageneration chromogenic assay) of HUVEC-seeded modulescultured under static conditions was low (see Fig. 8, which ispublished as supporting information on the PNAS web site).HUVEC-covered modules produced significantly longer timesto clotting (0.75 units�ml heparin; rocking platform arrange-ment; see Methods) than collagen-only modules (Fig. 3a; P �1.4 � 10�5). In 9 of 14 trials using HUVEC modules, clotting hadnot occurred at test termination compared with 1 of 15 trials forcollagen-only modules. The presence of the HUVEC signifi-cantly reduced the thrombogenicity of the module surface.
Lastly, and most significantly, slightly heparinized (0.75 units�ml)whole blood was perfused through the constructs at a rate of 0.334ml�min (equivalent to �7 dynes�cm2), and the effluent was ana-lyzed for platelet concentration (Fig. 3b). When constructs assem-bled from HUVEC-covered modules were perfused, there was noreduction in platelet concentration relative to the backgroundchanges associated with the flow circuit itself (i.e., measured in theabsence of modules). Blood perfusion through collagenase-dispase–treated HUVEC modules (to remove the HUVEC layerafter module shrinkage) significantly reduced platelet concentra-tion in the collected perfusate. The reduction in effluent plateletconcentration is an indicator of thrombogenicity in the absence ofHUVEC; the absence of this reduction (relative to the background)is an indicator of the functional efficacy of the HUVEC-seededmodules in inhibiting platelet activation. Obvious thrombus forma-tion (at 30 min) was seen in the majority of flow circuits withoutECs, but not when ECs were present. The presence of the HUVECsignificantly reduced the thrombogenicity of the construct. Al-though there are vascularization strategies involving VEGF deliv-ery (5), EC implantation (18), and micromachining (19) followedby implantation within the omentum (20), such a demonstration ofin vitro blood perfusion through a (micro)vascularized tissue engi-
Fig. 2. Characterization of constant porosity and shear stress on the surfaceof the modules during construct perfusion. (a) Flow and shear profiles throughtwo collagen modular constructs. Flow rate of PBS through two separateconstructs (construct length, 0.5 cm; construct diameter, 0.3 cm) as a functionof applied pressure difference (hydrostatic head); open and filled pointsrepresent different constructs. Each point is the mean of two flow-ratemeasurements made at each pressure difference. (Inset) The slope of the fittedline was used to calculate construct porosity by using the Ergun equation (13)from which the shear stress on the surface of the modules was calculated foreach construct. (b) Microcomputed tomography image of microfil cast of apoloxamine (22) modular construct (without HUVEC). Poloxamine is a stiffermaterial, enabling microfil casting. Light-colored regions correspond to themicrofil (i.e., the channels), and dark regions correspond to modules, illus-trating the interconnectedness of the flow channels that are normally linedwith ECs. Porosity based on the number of light pixels was 22.6%. A relativelyhigh pressure was required to fully infiltrate the viscous microfil, and hencethis technique was not suitable for assessing porosity in a lower-stiffnessHUVEC-coated collagen construct.
McGuigan and Sefton PNAS � August 1, 2006 � vol. 103 � no. 31 � 11463
APP
LIED
BIO
LOG
ICA
LSC
IEN
CES
ENG
INEE
RIN
G

neering construct together with evidence of low thrombogenicityhas not been described previously.
The potential for scalability arises because, unique to the mod-ular approach, the underlying design principles can be delineated.The three main constraints that influence the design of the modularconstruct are nutrient supply, incorporating clinically significantnumbers of cells within a construct of implantable volume, and theshear force on the HUVEC layer. Nutrient supply, determined bymass transfer within the construct, was estimated not to be asignificant design constraint. Channel dimensions are expected tobe of the same size as the modules (i.e., on the order of a fewhundred micrometers) allowing good oxygen mass transfer, thelikely limiting nutrient (12), within the construct channels. More-over, HepG2 cells remained viable within an assembled constructover 7 days, suggesting that mass transfer to the encapsulated cellswas sufficient, at least for the cell-seeding density and module sizeused. Because it has been predicted that a patient could survive on10% of normal liver function (12), an engineered liver with the celldensities achieved in our construct (3–10% of tissue densities) couldconceivably have sufficient cell mass to support patient survival.Studies of liver cell function and comparison with other liverconstructs were beyond the scope of this investigation.
Controlling shear stress is the most critical constraint to achievinga quiescent, confluent, nonthrombogenic layer of HUVEC. Qui-escent cells are unlikely to overgrow and block the channels of theconstruct. Here, HUVEC growth on module surfaces reached aplateau, which suggests that overgrowth is not a concern. Mainte-nance of a confluent layer of HUVEC, under flow, is also criticalto allow long-term blood flow through the interconnected channelsof the construct. A major limitation of endothelialized vasculargrafts is incomplete cell coverage under flow conditions due toinsufficient adhesion (21), resulting in limited protection fromthrombosis. Full coverage of the modules was achieved within 3days of seeding, and strong adhesion to collagen films was observed,as expected, in a centrifugation assay.§ Most importantly, the
HUVEC must exhibit a nonthrombogenic phenotype. Whole-blood perfusion of a prototype construct, assembled from HU-VEC-covered modules, at shear rates equivalent to �7 dynes�cm2,resulted in no significant increases in platelet loss above backgroundlevels, whereas constructs assembled from modules from whichECs were removed showed significant platelet loss within a shortperiod. Together with the tissue factor and clotting time results, thisresult suggests that a functional nonthrombogenic layer of EC wasgenerated on the module surface that was sufficient to maintaincontinuous blood flow through the engineered modular tissue.
We have demonstrated the use of microscale modular com-ponents in a biomimetic fashion to assemble uniform, potentiallyscalable (micro)vascularized tissue-engineered constructs con-taining multiple cell types, which were perfused with wholeblood. The current prototype enabled maintenance of cellviability at high cell densities and whole-blood perfusion withminimal blood activation. The next step is exploiting the modularconcept in a form that is suitable for in vivo use (e.g., addingcomponents to enable anastomoses to the host vasculature; usingbiocompatible components) and understanding how the modu-lar construct and the EC-lined channels remodel once im-planted. Subsequently, it will be necessary to demonstrate thehigher-level functions (e.g., polarity, spatial heterogeneity) andlonger-term nonthrombogenicity of the endothelialized chan-nels (at different shear stresses) and ultimately the utility of thisapproach to create functioning tissue or organ (e.g., liver,pancreas) equivalents, including extending the concept beyondHUVEC�HepG2 cells. Modular tissue assembly is a biomimeticalternative to traditional scaffold-based strategies, which offersmany advantages for engineering whole-organ and large-tissuegrafts and potentially transforms the conventional cell seeding�porous scaffold paradigm of tissue engineering.
MethodsCell Culture. The human hepatoma cell line, HepG2 (AmericanType Culture Collection, Manasses, VA), was cultured in 25-cm2
tissue culture flasks in RPMI 1640 culture medium with L-glutamine (Invitrogen Canada, Burlington, ON, Canada) sup-plemented with 15% bovine calf serum (HyClone) and 2%penicillin�streptomycin (Invitrogen Canada) at 37°C in a 5%CO2�95% air humidified atmosphere. HUVEC (Cambrex,Walkersville, MD) were cultured in 75-cm2 tissue culture flasks
§When HUVEC (25 � 103 cells per well) seeded on collagen films in a 96-well plate weresubjected to centrifugation (in an inverted orientation) at �175 � g, no significant cell losswas observed (cell numbers in centrifuged plates were compared with noncentrifugedcontrols to obtain percent cell loss), indicating that HUVEC adhered strongly to collagenfilms, as expected. Furthermore, strong pipetting was necessary to separate modules thathad bridged together with a HUVEC layer.
Fig. 3. Characterization of module thrombogenicity using whole-blood studies. (a) Clot formation times. The presence of HUVEC on the modules significantlyincreased the time to clot formation (P � 1.4 � 10�5) of slightly heparinized whole blood (0.75 units�ml) in a clotting test. In some cases, clot formation neveractually occurred, and the test was terminated between 4,500 and 5,400 s; in these instances, the recorded time was the test termination time. Mean clot timeis represented by the thick central line within the box. Open circles and stars represent outliers and extreme outliers, respectively. (b) Fresh whole blood (0.75units�ml heparin) perfused through a HUVEC-covered modular construct (filled circles) maintains platelet levels no different from those measured in the absenceof modules (open circles, flow circuit blank; includes polypropylene mesh required to keep modules in place). Blood perfusion through a control modularconstruct in which HUVEC have been removed by dispase–collagenase action (open squares), however, results in significant reductions in platelet number,indicating platelet activation and the thrombogenic response that occurs in the absence of HUVEC. Error bars indicate SEM (n � 3, 4, and 7 for background,dispase-treated modular constructs, and HUVEC-covered modular constructs, respectively).
11464 � www.pnas.org�cgi�doi�10.1073�pnas.0602740103 McGuigan and Sefton

in EGM-2 medium, as suggested by the suppliers, supplementedwith EGM-2 bullet kit (Cambrex) at 37°C in a 5% CO2�95% airhumidified atmosphere. In modules where both cell types werepresent, both cell types were cultured in HUVEC culturemedium.
Module Fabrication. Vitrogen collagen solution (Type I, bovinedermal, 3.1 mg collagen per ml; Cohesion Technologies, PaloAlto, CA) was mixed with 10� minimum essential medium (125�l of 10� medium per ml of collagen; Invitrogen Canada) andneutralized by using 0.8 M NaHCO3 (Sigma-Aldrich Canada).Pelleted HepG2 cells were mixed with the neutralized collagen(2 � 106 cells per ml), and the solution was drawn into the lumenof an ethylene oxide gas-sterilized PE tube (0.76 mm innerdiameter � 1.22 mm outer diameter) connected to a syringe atone end. After 30-min incubation to allow collagen gelation, thegel-filled tubing was cut into 2-mm lengths by using a custom-built automated cutter (Fig. 1a; FCS Technology, London, ON,Canada). Sections were vortexed gently in cell culture mediumto remove the gel-cell module cores from the tubing lumen. Thecollagen–cell modules were allowed to settle, separated from thePE tubing, and cultured in Petri dishes under static conditions.Collagen-only modules were fabricated identically (same colla-gen concentration) without the addition of the HepG2 cellpellet.
EC Seeding. HUVEC (Passage 1–6; 1.5–2.0 � 106 cells per ml ofsettled modules) were added to modules with or without encap-sulated HepG2 cells in a 15-ml centrifuge tube and incubated for60 min with gentle shaking every 10 min. Modules then weretransferred into a nontissue culture polystyrene Petri dish.Medium was replaced every 1–3 days.
Module Dimensions. After incubation overnight, a sample (n � 96)of modules containing HepG2 cells was selected, and lightmicroscopy images were taken of each module in a 96-well plate(one module per well) with an Olympus microscope. Modulesthen were seeded with �1.5 � 106 HUVEC per ml of settledmodules and incubated for 4 days, after which they werereimaged. Measurements of module diameter and length, beforeand after EC seeding, were made by using ImagePro software(Media Cybernetics, San Diego, CA).
Cell Viability and Enumeration Within Modules. Cell metabolism ofencapsulated cells was measured by using the Alamar blue (AB)assay at days 1, 3, and 7. Briefly, a micropipette was used to add10 modules (3 replicates) containing HepG2 cells in a 200-�lvolume into a 24 well plate. 10% AB (BioSource International,Camarillo, CA) was added, and the sample was incubated for 7 h.Supernatant samples were transferred into a 96-well plate andread by using a Sunrise ELISA plate reader (Tecan,Maennedorf, Switzerland) at 570 and 600 nm. Module samplesthen were digested with collagenase (final concentration 0.236mg�ml in culture medium; Sigma-Aldrich Canada), incubatedovernight, and stained with Trypan blue. The numbers of liveand dead cells were counted manually with a hemocytometer.
To assess cell viability within the assembled construct, mod-ules containing HepG2 cells or collagen-only modules seededwith HUVEC were cultured under static conditions for 6 daysand then within a flow circuit (see below) for 24 h. Modules wereretrieved from the circuit and tested immediately for viability bydigestion and staining with Trypan blue as above. The viabilityof HepG2 cells cultured within an assembled construct for 1week was assessed by using Vybrant carbofluorescein diacetatesuccinimidyl ester (CFDA) SE prelabeled cells (10 �M; Molec-ular Probes, Burlington, ON, Canada). One day after fabrication,the HepG2 modules were seeded with HUVEC and then, after2 days incubation, were assembled into a construct within a flow
circuit to allow module shrinkage. After 1 week of mediumperfusion, modules were retrieved from the flow circuit, fixed in3.7% paraformaldehyde–PBS (Electron Microscopy Science,Hatfield, PA) for 30 min, washed in PBS, and observed by usingfluorescence microscopy (Zeiss, Axiovert 135).
Construct Assembly and Flow Circuit Perfusion. Fifty-milliliter cen-trifuge tubes with two holes punctured in the cap through whichto thread Masterflex L�S-13 and L�S-16 tubing (Labcor, Anjou,QC, Canada) and �0.015 g of glass wool (�0.075 cm3) (to holdthe modules in place) were assembled into a continuous-loopflow circuit with a number of other connectors and stopcocks(various suppliers). A Masterflex peristaltic pump was used tocirculate medium through the flow loop from a 19-ml reservoir.Modules (0.5–1.0 ml) were loaded into the circuit (total circuitvolume 20 ml), within a laminar flow hood, by using a 10-mlpipette through a luer lock connector. Modules were maintainedin the flow circuit at 37°C in a 5% CO2�95% air humidifiedatmosphere for 24 h or 1 week. Medium was added to thereservoir every 1–2 days.
Flow Profile Measurements and Porosity Determination. Pressuredifference across the construct was recorded with low-pressuregauges (H. O. Trerice, Oak Park, MI) inserted on either side ofthe construct. Duplicate measurements of flow rate through theconstruct were measured for a range of pressure differences bythe timed collection of 0.5 ml of medium from the circuit througha T-connector output. The gradient of flow rate vs. pressuredifference (Darcy’s permeability) was calculated, and the gra-dient of similar curves measured in the absence of a construct(i.e., with glass wool only present) was subtracted to isolate thepressure difference contribution from the construct. The Ergunequation (13) then was solved for porosity by iteration using theSolver program in Microsoft Excel. The values used for constantspresent in this equation were as follows: length of construct, 0.5cm; fluid viscosity, 0.01 g�cm3; module diameter, 0.0411 cm; andshape factor, 0.874.
A construct of the same diameter and length was prepared byusing modules of a stiffer material (20% poloxamine modules,the preparation of which is described in ref. 22), which enabledperfusion with the viscous microfil solution (‘‘low viscosity’’;Flow Tech, Carver, MA; component:diluent ratio of 4:15, 10%curing agent) used for microcomputed tomography [Mice Im-aging Centre (MiCe), Hospital for Sick Children, Toronto, ON,Canada]. By using MicroView software (GE Healthcare, Chal-font St. Giles, U.K.), the number of pixels above the thresholdcorresponding to the microfil was used to calculate the volumefraction of microfil and hence the construct porosity.
Clotting Time. Fresh whole blood (10 ml) was collected fromconsenting donors (with ethics approval by the University ofToronto), who had not taken medication within 72 h of phle-botomy, into a syringe containing heparin (final concentration0.75 units�ml), after discarding the first milliliter. A 350-�lsample of slightly heparinized blood was mixed with 200 �l ofcollagen or HUVEC-coated modules in a microcentrifuge tube.A 400-�l sample of this mixture then was pipetted into a 25-cmlength of polypropylene tubing (1.57 mm ID) connected at eitherend with Silastic tubing (1.57 mm ID) to 200-�l pipette tipsconnected to a rocking platform (23). Rocking was initiated, andthe time until blood motion ceased or significant clot depositionoccurred within the tubing was recorded as the clotting time.
Construct Perfusion. Constructs were assembled from HUVEC-covered modules that were untreated or treated for 15 min in 100mg�ml collagenase dispase solution (Roche, Mississauga, ON,Canada) to remove all HUVEC from the surface (for controlmodules), yet retain the size and stiffness of the contracted
McGuigan and Sefton PNAS � August 1, 2006 � vol. 103 � no. 31 � 11465
APP
LIED
BIO
LOG
ICA
LSC
IEN
CES
ENG
INEE
RIN
G

collagen. The short treatment time ensured that module disso-lution did not occur, and microscope observation confirmedremoval of the HUVEC layer. Constructs were assembled withina 0.2-ml length of a 1-ml graduated pipette and held in place atboth ends with 1-cm2 sections of polypropylene mesh (PPM-3;Biomedical Materials, Slatersville, RI). Silastic tubing (10 cm,3.18 mm ID) was used to connect the pipette section to thesyringe pump (824E Infusion pump model A-99; Razel ScientificInstruments, Fairfax, VT). The construct was prefilled with PBSto prevent air bubble formation.
Blood was collected in a 10-ml syringe from consentingvolunteers that had taken no medication into 0.75 units�mlheparin. It was necessary to use a small amount of heparin (0.75units�ml is much less than the 5 units�ml needed to stop allcoagulation) to prevent premature clotting during the blooddraw or while the blood was sitting in the syringe pump. TheSilastic tubing was filled with blood from the syringe before beingconnected to the PBS prefilled pipette�construct section. Thesyringe then was placed on the syringe pump located on a rockingplatform (to minimize blood settling) within a 37°C oven, andblood was perfused through the construct at a rate of 0.334ml�min. At regular intervals during perfusion, 400-�l samples ofthe perfusate were collected in 0.6-ml graduated microcentrifugetubes containing 8 �l of 200 mM EDTA. An initial sample wascollected from the syringe before connecting it to the construct.The experiment was terminated when all of the blood from the
syringe had been used or if circuit blockage occurred. Constructswere removed and dissected for evidence of thrombus formationwithin the construct or the polypropylene mesh.
Statistics. Student’s t test was used to determine significantdifference when only two treatment groups were being com-pared. ANOVA was used to test for significant differencesamong multiple test groups. Q-Q plots were used to assess thenormality of the data. Levene’s test for homogeneity was used totest for equal variance among samples (24). When equal variancecould be assumed, the Tukey HSD post hoc test was used toidentify significant differences among multiple test groups.When equal variance could not be assumed, the Games–Howell(25) post hoc test was used to identify significant differencesamong multiple test groups. All tests were two-tailed, and P �0.05 was considered significant. Further details on the methodsare available in Supporting Methods, which is published assupporting information on the PNAS web site.
We thank T. Fixler, O. Khan, B. Leung, C. Lo, and A. Rosenthal fortechnical assistance. This work was supported by National Institutes ofHealth Grant EB001013 (to Coinvestigators E. Yeo and A. Gotlieb) andthe Natural Sciences and Engineering Research Council. A.P.M. re-ceived fellowship support of the Province of Ontario, the CanadianInstitutes of Health Research Training Program in Regenerative Med-icine, and the Canadian Rhodes Foundation.
1. Whitesides, G. M. & Grzybowski, B. A. (2002) Science 295, 2418–2421.2. Langer, R. & Vacanti, J. P. (1993) Science 260, 920–926.3. Carmeliet, P. & Jain, R. K. (2000) Nature 407, 249–257.4. Kim, B. S., Putnam, A. J., Kulik, T. J. & Mooney, D. J. (1998) Biotechnol.
Bioeng. 57, 46–54.5. Richardson, T. P., Peters, M. C., Ennett, A. B. & Mooney D. J. (2001) Nat.
Biotechnol. 19, 1029–1034.6. Kaihara, S., Borenstein, J., Koka, R., Lalan, S., Ochoa, E. R., Ravens, M., Pien,
H., Cunningham, B. & Vacanti, J. P. (2000) Tissue Eng. 6, 105–117.7. Vunjak-Novakovic, G., Obradovic, B., Martin, I., Bursac, P. M., Langer, R. &
Freed, L. E. (1998) Biotechnol. Prog. 14, 193–202.8. Yarmush, M. L., Toner, M., Dunn, J. C., Rotem, A., Hubel, A. & Tompkins,
G. R. (1992) Ann. N.Y. Acad. Sci. 665, 238–252.9. Koike, N., Fukumura, D., Gralla, O., Au, P., Schechner, J. S. & Jain, R. K.
(2004) Nature 428, 138–139.10. Coulson, J. M., Richardson, J. F., Backhurst, J. R. & Harker, J. H. (1978)
Chemical Engineering (Pergamon, Oxford), 3rd Ed., Vol. 2, p. 127.11. Zwaginga, J. J., de Boer, H. C., Ijsseldijk, M. J., Kerkhof, A., Muller-Berghaus,
G., Gruhlichhenn, J., Sixma, J. J. & de Groot, P. G. (1990) Arteriosclerosis 10,437–448.
12. Avgoustiniatos, E. S. & Colton, C. K. (1997) in Principles of Tissue Engineering, eds.
Lanza, R. P., Langer, R. & Chick, W. L. (Landes, Austin, TX), pp. 333–346.13. Ergun, S. (1952) Chem. Eng. Prog. 48, 89–94.14. Paszkowiak, J. J. & Dardik, A. (2003) Vasc. Endovasc. Surg. 37, 47–57.15. Lin, M. C., Almus-Jacobs, F., Chen, H. H., Parry, G. C., Mackman, N., Shyy,
J. Y. & Chien, S. (1997) J. Clin. Invest. 99, 737–744.16. Milewski, J. V. (1978) Ind. Eng. Chem. Prod. Res. Dev. 17, 363–366.17. Jaeger, H. M. & Nagel, S. R. (1992) Science 255, 1523–1531.18. Levenberg, S., Rouwkema, J., Macdonald, M., Garfein, E. S., Kohane, D. S.,
Darland, D. C., Marini, R., van Blitterswijk, C. A., Mulligan, R. C., D’Amore,P. A. & Langer, R. (2005) Nat. Biotechnol. 23, 879–884.
19. Shin, M., Matsuda, K., Ishii, O., Terai, H., Kaazempur-Mofrad, M., Borenstein,J., Detmar, M. & Vacanti, J. P. (2004) Biomed. Microdevices 6, 269–278.
20. Ogawa, K., Ochoa, E. R., Borenstein, J., Tanaka, K. & Vacanti, J. P. (2004)Transplantation 77, 1783–1789.
21. Williams, S. K. (1995) Cell Trans. 4, 401–410.22. Sosnik, A. & Sefton, M. V. (2005) Biomaterials 26, 7425–7435.23. Gemmell, C. H., Ramirez, S. M., Yeo, E. L. & Sefton, M. V. (1995) J. Lab. Clin.
Med. 125, 276–287.24. Levene, H. (1960) in Contributions to Probability and Statistics, ed. Olkin, I.
(Stanford Univ. Press, Palo Alto, CA), pp. 278–292.25. Zolman, J. F. (1993) Biostatistics (Oxford Univ. Press, Oxford), p. 151.
11466 � www.pnas.org�cgi�doi�10.1073�pnas.0602740103 McGuigan and Sefton