universal access to care: healthy san francisco american public health association
DESCRIPTION
Universal Access to Care: Healthy San Francisco American Public Health Association 136 th Annual Meeting – San Diego, CA Tangerine Brigham, Director of Healthy San Francisco San Francisco Department of Public Health October 28, 2008. Presenter Disclosures. Tangerine M. Brigham. - PowerPoint PPT PresentationTRANSCRIPT
1
Universal Access to Care:
Healthy San Francisco
American Public Health Association
136th Annual Meeting – San Diego, CA
Tangerine Brigham, Director of Healthy San Francisco
San Francisco Department of Public Health
October 28, 2008
2
Presenter Disclosures
The following personal financial relationships with commercial interests relevant to this presentation existed during the past 12 months:
Tangerine M. Brigham
No relationships to disclose
3
The Problem
Magnitude of problem: 45 million uninsured in United States6.5 million uninsured in California73,000 uninsured adults in San Francisco
Uninsured persons have:Less access to medical carePresent for care at later stages of illnessGreater mortality and morbidity due to illnessFragmented health care delivery system
4
San Francisco’s Response: Universal Health Care Access
Health Care Security Ordinance:
Employer Spending Requirement: Requires certain employers to make health care expenditure on behalf of designated employees. Implemented January 9, 2008.
Healthy San Francisco Program: Universal health care access program for uninsured residents. Debuted July 2, 2007 and City-wide implementation September 17, 2007.

5
Healthy San Francisco Program
6
Healthy San Francisco (HSF)
Provides health care for uninsured San Francisco adults (18 – 64 years old), regardless of: Employment Immigration status Pre-existing conditions Income level
Offers comprehensive, affordable health care services
Is not a health insurance plan/product
Restructures County indigent health system to encourage preventive care and continuity in primary care
Participants must be ineligible for publicly-funded health insurance
7
For Participants, HSF is an Organized Health Care Program
Select and receive primary care medical home
Streamlines the eligibility and enrollment
Accessible and clear information on services and the costs
Coordinated health care delivery network of providers
Customer service (e.g., call center, HSF ID card, newsletter)
8
HSF Services
INCLUDEDPreventive Care Primary Care Specialty Care
Emergency/Urgent Inpatient Care Pharmacy
Diagnostics DME Mental Health
Substance Abuse Laboratory X-rays
EXCLUDED (partial listing)Allergy Testing Cosmetic Services Dental
Infertility Tx Long-term Care
Organ Transplants Vision
9
HSF Provider Network
Primary Care Medical Homes 14 public health clinics 8 private non-profit community clinics (13 different locations) 1 private, non-profit hospital-affiliated clinic 1 private physicians association
Hospitals San Francisco General Hospital (public-County)
Hospitals linked to specific medical homes California Pacific Medical Center (private, non-profit) Saint Francis (private, non-profit) St. Mary’s (private, non-profit) Chinese Hospital (private, non-profit)
Hospitals providing specific services Univ. of CA San Francisco (public-State) – Radiologic
10
HSF Population and Enrollment
Estimated uninsured adults: 73,000 (2005 CHIS)
Expected enrollment: 60,000
Currently enrollment (10/08): 31,000 Phased enrollment strategy – focuses on those with lowest income first Over 100 HSF application assistors using
One-e-App 35,000 HSF applications processed 5% of all applications (9% of all applicants)
processed are for other health programs
11
HSF Participant Demographics
74% incomes below 100% FPL; 26% above 100% FPL
51% male; 49% female
38% Asian/PI; 24% Hispanic; 16% White; 9% Afr-Amer.; 2% Other; 11% Not Provided
8% under 25 years old; 65% b/w 25 - 54 years of age; 27% b/w 55 - 64 years of age
12
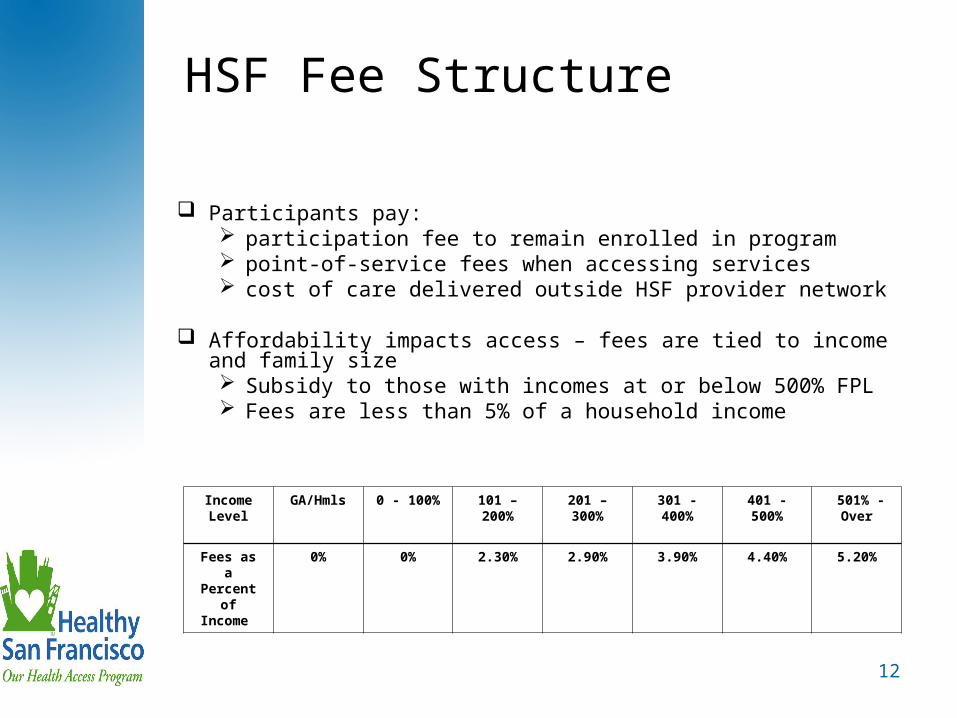
HSF Fee Structure
Participants pay: participation fee to remain enrolled in program point-of-service fees when accessing services cost of care delivered outside HSF provider network
Affordability impacts access – fees are tied to income and family size Subsidy to those with incomes at or below 500% FPL Fees are less than 5% of a household income
Income Level
GA/Hmls 0 - 100% 101 – 200%
201 – 300%
301 - 400%
401 - 500%
501% - Over
Fees as a Percent
of Income
0% 0% 2.30% 2.90% 3.90% 4.40% 5.20%
13
HSF Funding
Contributions from: Government
City & County (redirecting existing local dollars)State/Federal (existing funds to serve uninsured)Federal (Health Care Coverage Initiative award)
Participants
Employers
14
Employer Spending Requirement (ESR)
San Francisco employers are required to make health care expenditures. Can elect to: Offer health insurance Give Health Savings Accounts Reimburse employees for expenses Provide health care services Offer the City Option (incls. Healthy San Francisco)
Challenged by Golden Gate Restaurant Ass’n
Employer Spending Requirement went into effect on January 9, 2008
15
Employers are Selecting City Option
If an employer selects City Option, then their employee receives either: Healthy San Francisco or Medical Reimbursement Account
To date, over 1,000 employers have selected the City Option
In total, $18.5 million in health care expenditures committed for 27,500 employees One-half potentially eligible for HSF One-half eligible to receive a MRA
16
INTERSECTING POLICY WITH OPERATIONS
17
Moving HSF Policy Objective Toward Reality
A policy isn’t a program, a local ordinance isn’t a programPushing operations, technology, our
staff to achieve the policy objective
Crafting rules, regulations, processes, procedures, structure, etc. that take into account the existing infrastructure of your system(s)
18
Context for HSF Development
Aggressive timeline for HSF implementation
Coordination across multiple entities Three technology partners Third-Party Administrator (San Francisco Health Plan) Two other City/County agencies San Francisco Community Clinic Consortium
Highly visible program with significant public interest
GGRA Lawsuit
19
Lessons Learned
Manage change and expectations – frequent and consistent messaging required
Be clear about trade-offs – clarify prioritization since everything cannot be achieved
Clearly define program needs – designing program and developing technology simultaneously can create inefficiencies
Phase implementation – pilot and get the “kinks out”
High level of resources – extensive level of resources pre/post implementation
Linking programs and operational activities is complicated – more interfaces more complex systems more opportunities for system “glitches”
20
Replicability in
Other Communities
21
Factors in San Francisco’s Implementation
San Francisco’s environment has made effort achievable Political will and leadership Public support for addressing problem Financial resources available to leverage Safety net providers serving uninsured Geographic boundaries
Implementation has gone relatively smoothly
Too early to say if HSF is a success on all measures – program evaluation needed
22
HSF Evaluation Components
ParticipationAccessQualityUtilizationFinancial viability Replicability
23
Generalizable Features of HealthySan Francisco
Focus on primary care home to reduce duplication and improve coordination
Centralized eligibility system to maximize public entitlement and increase coordination of benefits
Centralized system of record creates accountability and comprehensive database for planning & evaluation purposes
Non-insurance (care) model potentially results in lower costs and leverages federal/state funds for localities
Establishment of predictable, affordable participation fees; may not be viewed as charity by participants
Public-private partnership maximizes available resources