undp/unfpa/who/world bank hrprhr reproductive health and research oral contraceptives and cvd...
TRANSCRIPT

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
Oral Contraceptives and CVDOral Contraceptives and CVDEpidemiologic EffectsEpidemiologic Effects
TMM FarleyTMM Farley
Department of Reproductive Health and ResearchDepartment of Reproductive Health and ResearchWorld Health OrganizationWorld Health Organization
Geneva

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
OverviewOverview
• Rationale for WHO Collaborative Study of Rationale for WHO Collaborative Study of Cardiovascular Disease and Steroid Cardiovascular Disease and Steroid Hormone ContraceptionHormone Contraception
• Venous thromboembolism, stroke and Venous thromboembolism, stroke and myocardial infarctionmyocardial infarction
• Supplement with data from other recent Supplement with data from other recent studiesstudies
• Overall cardiovascular riskOverall cardiovascular risk

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
• OC composition and patterns of use have OC composition and patterns of use have changed since late 1970schanged since late 1970s
• Most information refers to older products Most information refers to older products
• No information available on risks in women No information available on risks in women from developing countriesfrom developing countries
• ““What are the cardiovascular risks associated What are the cardiovascular risks associated with modern OCs used in modern ways?”with modern OCs used in modern ways?”
WHO Study of Cardiovascular Disease and WHO Study of Cardiovascular Disease and Steroid Hormone Contraception - 1986Steroid Hormone Contraception - 1986

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
WHO Study of Cardiovascular Disease WHO Study of Cardiovascular Disease and Hormonal Contraceptionand Hormonal Contraception
UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
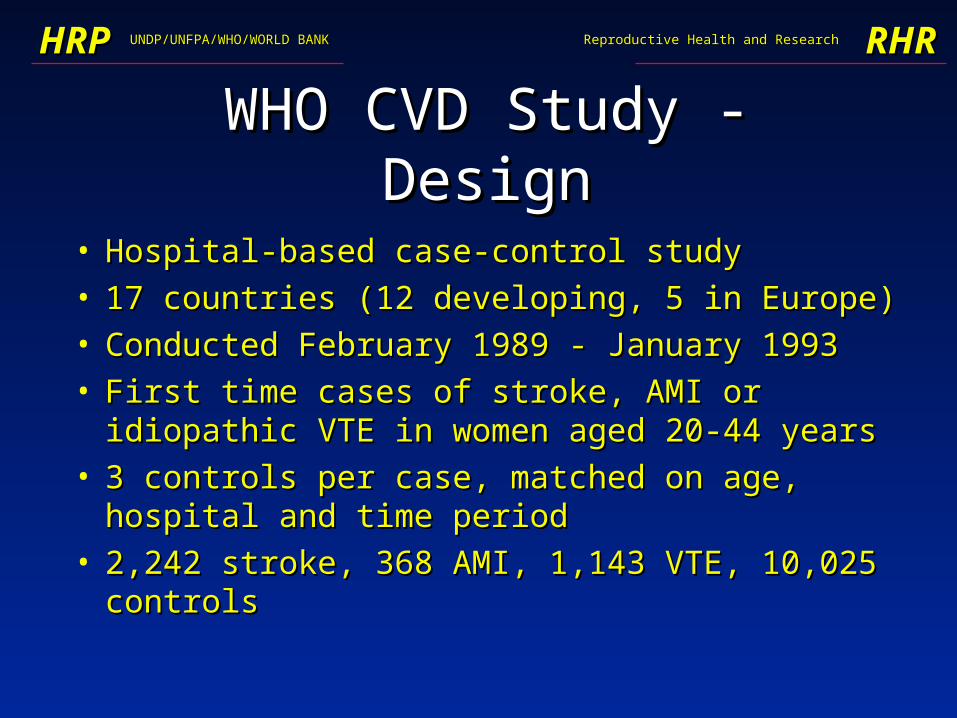
WHO CVD Study - DesignWHO CVD Study - Design
• Hospital-based case-control study Hospital-based case-control study • 17 countries (12 developing, 5 in Europe)17 countries (12 developing, 5 in Europe)• Conducted February 1989 - January 1993Conducted February 1989 - January 1993• First time cases of stroke, AMI or idiopathic VTE in First time cases of stroke, AMI or idiopathic VTE in
women aged 20-44 yearswomen aged 20-44 years• 3 controls per case, matched on age, hospital and 3 controls per case, matched on age, hospital and
time periodtime period• 2,242 stroke, 368 AMI, 1,143 VTE, 10,025 controls2,242 stroke, 368 AMI, 1,143 VTE, 10,025 controls

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
Venous ThromboembolismVenous Thromboembolism
Europe Developing
Cases / controls 433 / 1044 710 / 1954
OC use(case/cntl)
61% / 34% 29% / 12%
Risk cf non-users 4.1 (3.1 - 5.6) 3.3 (2.6 - 4.1)
Adjusted odds ratio (95% CI)WHO, Lancet 1995; 346:1575

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
Risk Factors for Idiopathic VTERisk Factors for Idiopathic VTE
• Increased relative risk withIncreased relative risk with– OC useOC use– elevated body mass indexelevated body mass index– hypertension in pregnancyhypertension in pregnancy
• No effect on relative riskNo effect on relative risk– smoking, age, hypertensionsmoking, age, hypertension– duration of OC useduration of OC use– previous OC useprevious OC use
WHO, Lancet 1995; 346:1575
UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
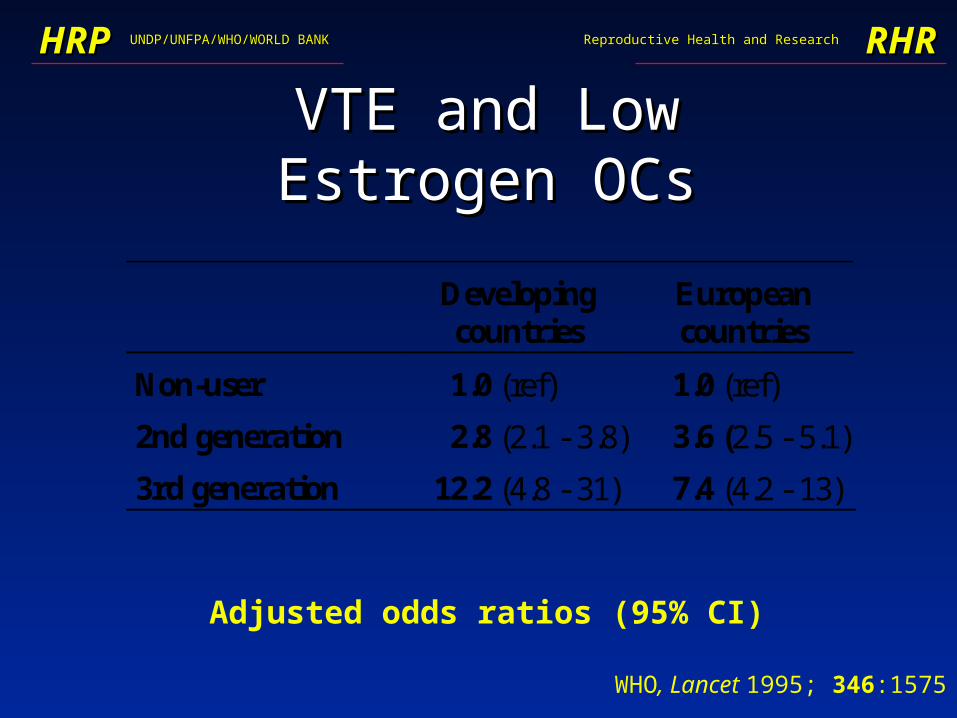
VTE and Low Estrogen OCsVTE and Low Estrogen OCs
Adjusted odds ratios (95% CI)
Developingcountries
Europeancountries
Non-user 1.0 (ref) 1.0 (ref)
2nd generation 2.8 (2.1 - 3.8) 3.6 (2.5 - 5.1)
3rd generation 12.2 (4.8 - 31) 7.4 (4.2 - 13)
WHO, Lancet 1995; 346:1575

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
VTE and Low Estrogen OCs VTE and Low Estrogen OCs
• Excess risk with desogestrel & gestodene Excess risk with desogestrel & gestodene compared with levonorgestrel compared with levonorgestrel – About 2.5 About 2.5 higher risk higher risk – Similar excess risk for the two productsSimilar excess risk for the two products– Bias or confounding unlikely explanationBias or confounding unlikely explanation
• Unexpected, Unexplained, Unwelcome, Unexpected, Unexplained, Unwelcome, UncomfortableUncomfortable
• ““Must be confirmed by independent research”Must be confirmed by independent research”

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
33rdrd Gen vs. Levonorgestrel Gen vs. Levonorgestrel
Adjusted risks relative to non-users (crude risk)
Lancet 1995; 346:1582, 1589, 1593; BMJ 1996; 312: 83; Contraception 1998; 57: 291
Study Levong. Third Ratio
WHO CVD Study 3.4 8.6 2.6
UK General Practice Research Database
-(4.2)
-(7.6)
2.1
Leiden Thrombophilia Study
3.8 8.7 2.2
Transnational Study 3.0 5.4 1.8
Denmark 1.8 3.2 1.8
Overall risk ratio (95% CI) 1.9 (1.5, 2.2)

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
Ischaemic StrokeIschaemic Stroke
• Major risk factorsMajor risk factors– smokingsmoking– hypertensionhypertension– rheumatic heart diseaserheumatic heart disease– diabetesdiabetes
• Overall risk with OC use 2.9 (2.2 - 3.9)Overall risk with OC use 2.9 (2.2 - 3.9)
• No effect of past OC use or duration of useNo effect of past OC use or duration of use

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
Ischaemic Stroke - smokingIschaemic Stroke - smoking
Non-user OC-User
Non-smoker 1.0 (ref) 2.5 (1.8 – 3.5)[70%] [9%]
Smoker 1.3 (0.9 – 1.7) 5.5 (3.5 – 8.7)[17%] [3%]
Pooled adjusted odds ratio (95% CI) [% controls]
WHO, Lancet 1996; 348: 498
UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
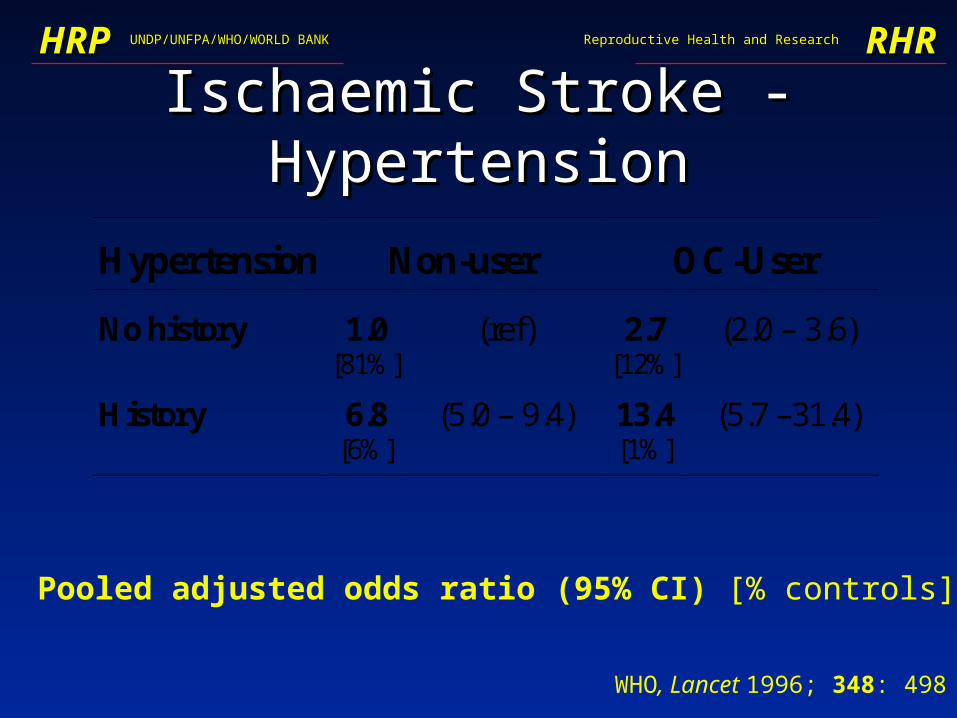
Ischaemic Stroke - HypertensionIschaemic Stroke - Hypertension
Hypertension Non-user OC-User
No history 1.0 (ref) 2.7 (2.0 – 3.6)[81%] [12%]
History 6.8 (5.0 – 9.4) 13.4 (5.7 –31.4)[6%] [1%]
Pooled adjusted odds ratio (95% CI) [% controls]
WHO, Lancet 1996; 348: 498

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
Ischaemic Stroke and Low Estrogen OCsIschaemic Stroke and Low Estrogen OCs
• Kaiser, CAKaiser, CA 1.2 (0.5, 2.6)1.2 (0.5, 2.6)
• Washington StateWashington State 1.4 (0.5, 3.8)1.4 (0.5, 3.8)
• DenmarkDenmark 1.6 (1.1, 2.4)1.6 (1.1, 2.4)
• WHO WHO Europe Europe 1.4 (0.6, 3.1)1.4 (0.6, 3.1) Developing countries Developing countries 3.4 (2.2, 3.1)3.4 (2.2, 3.1)
• TransNationalTransNational 2.8 (2.0, 3.8)2.8 (2.0, 3.8)
RR (95% CI) compared with non-users

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
• With Blood Pressure checkWith Blood Pressure check WHO Europe WHO Europe 1.3 (0.5, 3.5)1.3 (0.5, 3.5) WHO Developing WHO Developing 2.1 (1.1, 3.8)2.1 (1.1, 3.8) TransNational TransNational 2.1 (1.4, 3.1)2.1 (1.4, 3.1)
• Without Blood Pressure checkWithout Blood Pressure check WHO Europe WHO Europe 1.5 (0.5, 4.6)1.5 (0.5, 4.6) WHO Developing WHO Developing 5.2 (2.9, 9.1)5.2 (2.9, 9.1) TransNational TransNational 4.5 (2.6, 8.0)4.5 (2.6, 8.0)
Ischaemic Stroke and Low Estrogen OCsIschaemic Stroke and Low Estrogen OCs
RR (95% CI) compared with non-users

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
Ischaemic stroke - ConclusionIschaemic stroke - Conclusion
• Some excess risk associated with low Some excess risk associated with low estrogen dose OCsestrogen dose OCs
• Smoking and hypertension potentiate OC-Smoking and hypertension potentiate OC-associated riskassociated risk
• Lower risk when screened for hypertensionLower risk when screened for hypertension
• No evidence of difference in risk according No evidence of difference in risk according to OC type (2to OC type (2ndnd vs. 3 vs. 3rdrd generation) generation)

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
Haemorrhagic StrokeHaemorrhagic Stroke• No difference according to BP checkingNo difference according to BP checking• No impact on risk in women < 35 yearsNo impact on risk in women < 35 years• About 2 About 2 risk in women over 35 years risk in women over 35 years• Higher (relative) risk among older women, smokers, Higher (relative) risk among older women, smokers,
women with hwomen with hx x of hypertension of hypertension
• Smoking has greater impact on risk of haemorrhagic Smoking has greater impact on risk of haemorrhagic than ischaemic strokethan ischaemic stroke
• Consistent with data from Kaiser, CA (Petitti, 1996) Consistent with data from Kaiser, CA (Petitti, 1996)

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
Myocardial InfarctionMyocardial Infarction
• Major risk factorsMajor risk factors– smoking, hypertension, rheumatic heart smoking, hypertension, rheumatic heart
disease, diabetes, hyperlipidaemiadisease, diabetes, hyperlipidaemia
• Overall risk with OC use 4.9 (3.1 - 7.8)Overall risk with OC use 4.9 (3.1 - 7.8)
• No effect of past OC use or duration of useNo effect of past OC use or duration of use
• Lower risks with low compared with high Lower risks with low compared with high dose OCs dose OCs

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
AMI - Hypertension & OC useAMI - Hypertension & OC use
Hypertension Non-user OC-User
No history 1.0 (ref) 3.8 (2.3 –6.2)[81%] [12%]
History 7.6 (4.5 – 12.8) 23.7 (6.5 – 86.7)[6%] [1%]
Pooled adjusted odds ratio (95% CI) [% controls]
WHO, Lancet 1997; 349: 1202

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
AMI - smoking & OC useAMI - smoking & OC use
Non-user OC-User
Non-smoker 1.0 (ref) 4.2 (2.2 – 8.1)[62%] [8%]
Smoker 4.4 (3.0 – 6.4) 44.9 (21 – 96)[25%] [5%]
Pooled adjusted odds ratio (95% CI) [% controls]
WHO, Lancet 1997; 349: 1202

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
AMI - ConclusionAMI - Conclusion
• Majority of cases (78%) occur in smokers Majority of cases (78%) occur in smokers
• Lower risk with low dose OCs, in women Lower risk with low dose OCs, in women without CV risk factors and who reported without CV risk factors and who reported BP check (similar observations in BP check (similar observations in TransNational study)TransNational study)
• Among women with no cardiovascular risk Among women with no cardiovascular risk factors who do not smoke, RR = 1.1 in factors who do not smoke, RR = 1.1 in women with BP checkwomen with BP check
UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
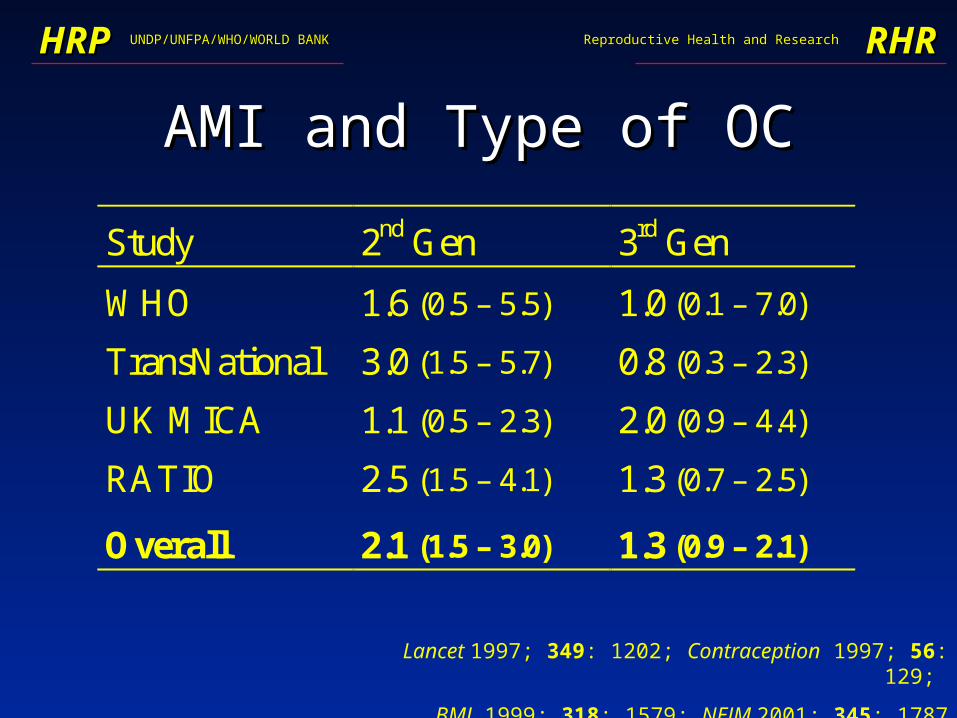
AMI and Type of OCAMI and Type of OC
Study 2nd Gen 3rd Gen
WHO 1.6 (0.5 – 5.5) 1.0 (0.1 – 7.0)
TransNational 3.0 (1.5 – 5.7) 0.8 (0.3 – 2.3)
UK MICA 1.1 (0.5 – 2.3) 2.0 (0.9 – 4.4)
RATIO 2.5 (1.5 – 4.1) 1.3 (0.7 – 2.5)
Overall 2.1 (1.5 – 3.0) 1.3 (0.9 – 2.1)
Lancet 1997; 349: 1202; Contraception 1997; 56: 129;
BMJ 1999; 318: 1579; NEJM 2001; 345: 1787
UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
Overall Cardiovascular RiskOverall Cardiovascular Risk
• Different risk factors for VTE and stroke Different risk factors for VTE and stroke or MIor MI
• Age distribution of VTE, stroke and MI Age distribution of VTE, stroke and MI cases very different over 15 - 44 age rangecases very different over 15 - 44 age range
• Any reduction in MI risk for third Any reduction in MI risk for third generation OC users more important for generation OC users more important for older women and smokersolder women and smokers

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
0.0
4.0
8.0
20-24 25-29 30-34 35-39 40-44
Age group (years)
Inci
den
ce (
per
100
000
wyr
s)
Observed CVD Incidence Oxford
VTE
Haemorrhagic stroke
Ischaemic stroke
AMI
J Epidemiol Comm Health 1998; 52: 775

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
CVD Incidence - Non-smokerCVD Incidence - Non-smoker
0
100
200
300 VTE
I Str
H Str
MI
20-24y 30-34y 40-44y 20-24y 30-34y 40-44y
Eve
nts
per
106 w
yrs
Non-OC user OC user

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
0
20
40
CVD Mortality - Non-smokerCVD Mortality - Non-smoker
Non-OC user OC user
20-24y 30-34y 40-44y 20-24y 30-34y 40-44y
Dea
ths
per
106 w
yrs

UNDP/UNFPA/WHO/WORLD BANKUNDP/UNFPA/WHO/WORLD BANKHRPHRP RHRRHRReproductive Health and ResearchReproductive Health and Research
OCs and CVDOCs and CVD
• OCs most widely studied pharmacologic agentOCs most widely studied pharmacologic agent• In young women without cardiovascular risk factors, In young women without cardiovascular risk factors,
OCs are safeOCs are safe• Excess risk seen in older women, smokers and those Excess risk seen in older women, smokers and those
with pre-existing risk factorswith pre-existing risk factors• Risk-benefit of 2Risk-benefit of 2ndnd vs. 3 vs. 3rdrd generation OCs generation OCs
– VTE risk more important in younger womenVTE risk more important in younger women
– MI risk more important in older women and smokersMI risk more important in older women and smokers