reproductive health update: encouraging students to use contraceptives john kulig, md, mph lead...
TRANSCRIPT

Reproductive Health Update: Reproductive Health Update: Encouraging Students to Use Encouraging Students to Use
ContraceptivesContraceptives
John Kulig, MD, MPHJohn Kulig, MD, MPH
Lead Medical SpecialistLead Medical Specialist
Sara Mackenzie, MDSara Mackenzie, MD
Regional Medical SpecialistRegional Medical Specialist
March 28, 2013March 28, 2013

OverviewGoals:Goals:
This webinar will provide an update on contraceptive methods, This webinar will provide an update on contraceptive methods, including long-acting reversible methods. Additionally, including long-acting reversible methods. Additionally, presenters will provide strategies to promote consistent use of presenters will provide strategies to promote consistent use of contraceptives by students.contraceptives by students.
Objectives:Objectives:
After this presentation, participants will be able to:After this presentation, participants will be able to:
Implement a comprehensive family planning program for female Implement a comprehensive family planning program for female and male students on center.and male students on center.
Counsel students about delaying pregnancy and parenting in Counsel students about delaying pregnancy and parenting in support of employability.support of employability.
Counsel students about current contraceptive options and Counsel students about current contraceptive options and provide access to all methods.provide access to all methods.

Family Planning ProgramPRH 6.11 R4
A family planning program shall be A family planning program shall be provided to all students on a voluntary provided to all students on a voluntary basis. At a minimum, this program shall basis. At a minimum, this program shall include counseling, health promotion include counseling, health promotion activities and medical services. The activities and medical services. The Center Director shall appoint a staff Center Director shall appoint a staff member to implement and monitor this member to implement and monitor this program.program.

Sexual Health MisinformationOne in five adolescents believe that birth control pills offer protection from STDsOne in five adolescents believe that condoms are “not effective” in preventing STD transmissionOne in six adolescents believe that sex without a condom once in awhile is “no big deal”One in ten adolescents believe that “you do not need to use condoms unless you have a lot of sexual partners.”Half of adolescents believe that raising the subject of condoms raises suspicions about both partners’ sexual history
Ref: Kaiser Family Foundation National SurveyRef: Kaiser Family Foundation National Survey
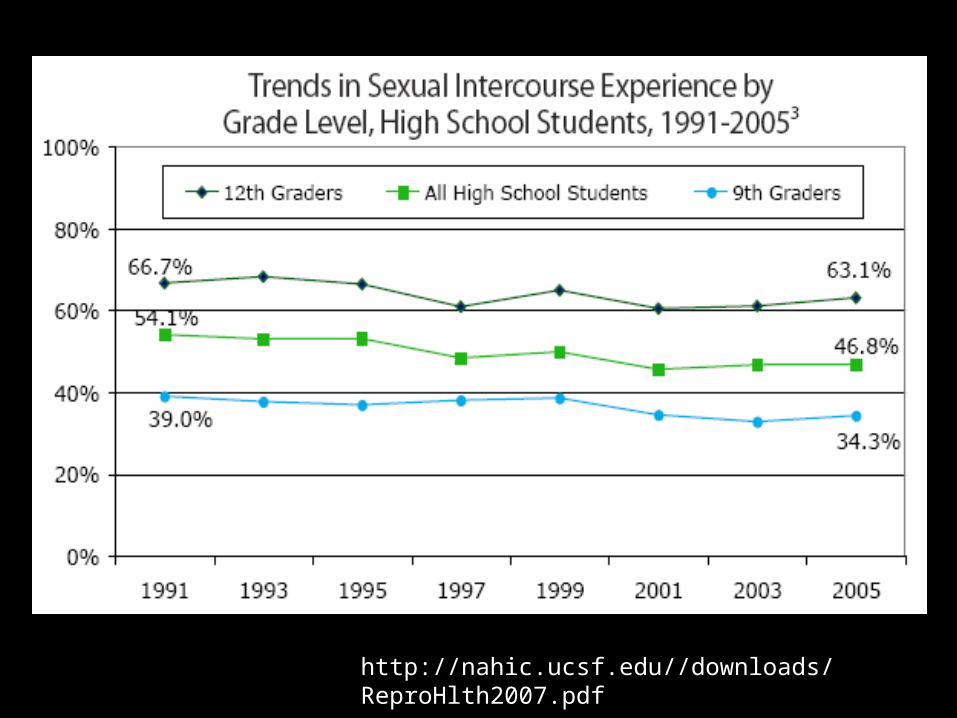
http://nahic.ucsf.edu//downloads/ReproHlth2007.pdf






Unintended pregnancy in U.S. Unintended pregnancy in U.S. (all age groups)(all age groups)
82% of teen pregnancies unintended82% of teen pregnancies unintended
49% of 49% of allall pregnancies unintended pregnancies unintended 29% mistimed29% mistimed 19% unwanted19% unwanted 43% end in abortion43% end in abortion

Teen child bearing associated with:Teen child bearing associated with:
School dropoutSchool dropout
Infants of teens more likely to have low Infants of teens more likely to have low birth weight, lower academic achievement, birth weight, lower academic achievement, and increased likelihood of becoming teen and increased likelihood of becoming teen parentparent

Case 1:Case 1:
Student presents to wellness center Student presents to wellness center requesting pregnancy test – worried she requesting pregnancy test – worried she might be pregnant. You review chart and might be pregnant. You review chart and see prescribed oral contraceptives at see prescribed oral contraceptives at entrance. She says: “I started it but my entrance. She says: “I started it but my period started after a couple of weeks, so I period started after a couple of weeks, so I stopped for a week, then started the next stopped for a week, then started the next package but had bleeding again, so I package but had bleeding again, so I stopped.”stopped.”

Of teens with live birth:Of teens with live birth:
50% not using contraception at time 50% not using contraception at time pregnancy – of these 1/3 thought could not pregnancy – of these 1/3 thought could not get pregnant at that timeget pregnant at that time
21% using highly effective contraceptive 21% using highly effective contraceptive (although only 1% with IUD)(although only 1% with IUD)
24% moderately effective contraceptive24% moderately effective contraceptive
5% rhythm or withdrawal method5% rhythm or withdrawal method
REF: Prepregnancy contraceptive use among teens with unintended pregnancies REF: Prepregnancy contraceptive use among teens with unintended pregnancies resulting in live births 2004-2008 MMWR v61/No.2 January 20, 2012resulting in live births 2004-2008 MMWR v61/No.2 January 20, 2012

To decrease teen pregnancy:To decrease teen pregnancy:
Reduce or delay onset of sexual activityReduce or delay onset of sexual activity
Provide factual information about Provide factual information about conditions in which pregnancy occursconditions in which pregnancy occurs
Increase motivation and negotiation skills Increase motivation and negotiation skills for preventionfor prevention
Increase access to contraceptives Increase access to contraceptives
Increase use of most effective Increase use of most effective contraceptivescontraceptives
REF: Prepregnancy contraceptive use among teens with unintended pregnancies REF: Prepregnancy contraceptive use among teens with unintended pregnancies resulting in live births 2004-2008 MMWR v61/No.2 January 20, 2012resulting in live births 2004-2008 MMWR v61/No.2 January 20, 2012

AbstinenceAbstinence

Teenage Births
teenage birth rate had fallen “below any teenage birth rate had fallen “below any level previously recorded in the US” as of level previously recorded in the US” as of 2005, 2005, butbut increased 3.4% in 2006 and 1.4% increased 3.4% in 2006 and 1.4% in 2007 (15-19 year-olds), then lower in 2008in 2007 (15-19 year-olds), then lower in 200830% overall decline in the past decade30% overall decline in the past decade40% decline among African American 40% decline among African American teenagers since 1991teenagers since 1991abortion rate among women 15-19 declined abortion rate among women 15-19 declined from 40 per 1,000 in 1990 to 24 per 1,000 in from 40 per 1,000 in 1990 to 24 per 1,000 in 20002000attributed to less sexual activity and more attributed to less sexual activity and more effective use of contraceptioneffective use of contraception

Changes in marriage
The proportion of 25-year-olds who have never been married has
increased steadily since the 1970s. Source: The Brookings Institution, 2007


Oral Oral Contraceptive Contraceptive PillsPills

Noncontraceptive Benefits of OCs
decrease menstrual flow (lighter, shorter periods)decrease menstrual flow (lighter, shorter periods)
decrease menstrual cramps (no ovulation)decrease menstrual cramps (no ovulation)
improve anemia (lighter, shorter periods)improve anemia (lighter, shorter periods)
improve acne (estrogen effect)improve acne (estrogen effect)
protect against ovarian and endometrial cancerprotect against ovarian and endometrial cancer
decrease benign breast disease decrease benign breast disease
decrease ovarian cyst formationdecrease ovarian cyst formation
prevent ectopic pregnancyprevent ectopic pregnancy
protect against some causes of PIDprotect against some causes of PID
protect against osteoporosisprotect against osteoporosis

Contraindications to Use of OCs
deep vein thrombosisdeep vein thrombosis
pulmonary embolismpulmonary embolism
cerebrovascular disease cerebrovascular disease
coronary artery diseasecoronary artery disease
factor V Lyden mutation or other known thrombophiliafactor V Lyden mutation or other known thrombophilia
migraine headache with aura or neurologic changesmigraine headache with aura or neurologic changes
estrogen-dependent cancerestrogen-dependent cancer
active liver diseaseactive liver disease
major surgery or immobilizationmajor surgery or immobilization
pregnancy or breastfeedingpregnancy or breastfeeding

Drug Interactions with OCs
carbamazepine (Tegretol)carbamazepine (Tegretol)
griseofulvin (Grifulvin)griseofulvin (Grifulvin)
phenobarbital (Luminal)phenobarbital (Luminal)
phenytoin (Dilantin)phenytoin (Dilantin)
primidone (Mysoline)primidone (Mysoline)
rifampin (Rifadin)rifampin (Rifadin)
rifabutin (Mycobutin)rifabutin (Mycobutin)
ritonavir (Norvir)ritonavir (Norvir)
St. John’s wort St. John’s wort

Extended Cycling
fewer and shorter menstrual periods – fewer and shorter menstrual periods – one or four per yearone or four per year
shorter hormone-free intervalsshorter hormone-free intervals
better ovarian suppression (PCOS)better ovarian suppression (PCOS)
decreased premenstrual dysphoric decreased premenstrual dysphoric disorder (PMDD), premenstrual syndrome disorder (PMDD), premenstrual syndrome (PMS), acne vulgaris, endometriosis, (PMS), acne vulgaris, endometriosis, menstrual migrainemenstrual migraine
preferred by athletespreferred by athletes

Seasonale®
Seasonique®

Seasonale®
extended regimen combined oral extended regimen combined oral contraceptive pills with ethinyl contraceptive pills with ethinyl estradiol 0.03 mg and levonorgestrel estradiol 0.03 mg and levonorgestrel 0.15 mg0.15 mg
91 day cycles - 84 days on – 7 days off91 day cycles - 84 days on – 7 days off
4 menstrual cycles per year - one each 4 menstrual cycles per year - one each seasonseason

Seasonique®
extended regimen combined oral extended regimen combined oral contraceptive pills with ethinyl estradiol contraceptive pills with ethinyl estradiol 0.03 mg and levonorgestrel 0.15 mg0.03 mg and levonorgestrel 0.15 mg
91 day cycles - 84 days on both – 91 day cycles - 84 days on both –
7 days on ethinyl estradiol 0.01 mg7 days on ethinyl estradiol 0.01 mg
4 menstrual cycles per year - one each 4 menstrual cycles per year - one each seasonseason

Oral Contraception: Red Flags
Mnemonic: ACHES
Abdominal pain (severe)
Chest pain (severe), cough, shortness of breath
Headache (severe), dizziness, weakness, or numbness
Eye problems (vision loss or blurring), speech problems
Severe leg pain (calf or thigh)

Emergency Emergency ContraceptionContraception

Plan B


Does knowledge of EC alter adolescent sexual behavior?
study of 916 male and 852 female students age study of 916 male and 852 female students age 14-15 in 12 schools in UK14-15 in 12 schools in UK
single lesson on emergency contraceptionsingle lesson on emergency contraception
improved knowledge persisted six months improved knowledge persisted six months later in comparison with controlslater in comparison with controls
no difference in sexual activity, intent to use no difference in sexual activity, intent to use EC or use of EC EC or use of EC
Ref: Ref: BMJBMJ 2002:324:1179-1183 2002:324:1179-1183

Contraceptive Contraceptive PatchPatch

Ortho Evra
Ortho Evra
seven day contraceptive patchseven day contraceptive patch
113/4 3/4 inch three-layer adhesive patchinch three-layer adhesive patch
releases ethinyl estradiol 20 µg and releases ethinyl estradiol 20 µg and norelgestromin 150 µg dailynorelgestromin 150 µg daily
applied to the buttocks, lower abdomen or applied to the buttocks, lower abdomen or upper body – not breastsupper body – not breasts
newly applied weekly for three weeks, then newly applied weekly for three weeks, then one week off for mensesone week off for menses
less effective in women over 198 poundsless effective in women over 198 pounds

Ortho Evra
The pharmacokinetic profile for the ORTHO EVRA The pharmacokinetic profile for the ORTHO EVRA patch is different from oral contraceptives in that it patch is different from oral contraceptives in that it has higher steady state concentrations (60% higher) has higher steady state concentrations (60% higher) and lower peak concentrations (25% lower) of and lower peak concentrations (25% lower) of ethinyl estradiol (EE) compared with an oral ethinyl estradiol (EE) compared with an oral contraceptive containing 35 mcg EE. contraceptive containing 35 mcg EE.
Increased estrogen exposure may increase the risk Increased estrogen exposure may increase the risk of adverse events, including venous of adverse events, including venous thromboembolism. thromboembolism.
Safety information added 2007

Ortho Evra
The results of epidemiologic studies evaluating the The results of epidemiologic studies evaluating the risk of venous thromboembolism (VTE) among risk of venous thromboembolism (VTE) among women using ORTHO EVRA compared to those women using ORTHO EVRA compared to those using oral contraceptives containing 30-35 mcg EE using oral contraceptives containing 30-35 mcg EE and either levonorgestrel or norgestimate reported and either levonorgestrel or norgestimate reported odds ratios ranging from 0.9 (no increase in risk) to odds ratios ranging from 0.9 (no increase in risk) to 2.4 (approximate doubling of risk). 2.4 (approximate doubling of risk).
Safety information added 2007

Ortho Evra
Side effects leading to discontinuation:Side effects leading to discontinuation:nausea (2%)nausea (2%)moodiness (1.5%)moodiness (1.5%)headache (1.1%)headache (1.1%)breast discomfort (1%)breast discomfort (1%)irritation at application site (1.9%)irritation at application site (1.9%)
Inadvertent detachment uncommon (1.9%), Inadvertent detachment uncommon (1.9%), even with exercise, humid climates, saunas, even with exercise, humid climates, saunas, hot tubs.hot tubs.

Contraceptive Contraceptive Vaginal Vaginal RingRing

NuvaRing

NuvaRing
contraceptive vaginal ring - 2 inch diametercontraceptive vaginal ring - 2 inch diameter
worn for 21 days => removed for 7 days to allow worn for 21 days => removed for 7 days to allow menses => replaced with new ringmenses => replaced with new ring
releases 120 mcg of etonogestrel and 15 mcg of releases 120 mcg of etonogestrel and 15 mcg of ethinyl estradiol dailyethinyl estradiol daily
one size only - does not require fitting one size only - does not require fitting
cannot be inserted incorrectlycannot be inserted incorrectly
no increase in vaginal infections/dischargeno increase in vaginal infections/discharge
3 hour window for reinsertion after inadvertent 3 hour window for reinsertion after inadvertent removalremoval


Long acting reversible Long acting reversible contraceptives (LARCs)contraceptives (LARCs)
IUDs and contraceptive implantsIUDs and contraceptive implants
Highly effective and safeHighly effective and safe
High satisfaction and continuation ratesHigh satisfaction and continuation rates
Underutilized in U.S.Underutilized in U.S.
Recent study noted significant reduction in Recent study noted significant reduction in abortions, repeat abortions, teen birth abortions, repeat abortions, teen birth rates with use of LARCsrates with use of LARCs
Preventing Unintended Pregnancies by Providing No-cost contraception; Preventing Unintended Pregnancies by Providing No-cost contraception; Obstetrics and Gynecology vol 120, no 6, 1291-1297 December 2012Obstetrics and Gynecology vol 120, no 6, 1291-1297 December 2012

Progestin-only Progestin-only Injectable Injectable ContraceptionContraception


Depo Provera
depot medroxyprogesterone depot medroxyprogesterone
acetate 150 mg IM once every acetate 150 mg IM once every
12 weeks – highly effective12 weeks – highly effective
inhibits ovulation, thickens cervical mucus, inhibits ovulation, thickens cervical mucus, thins the endometriumthins the endometrium
irregular bleeding/spotting => irregular bleeding/spotting =>
amenorrhea within 2 years (70%)amenorrhea within 2 years (70%)
concerns:concerns:– weight gain (54%)weight gain (54%)– osteoporosis risk, reversibleosteoporosis risk, reversible

Contraceptive Contraceptive ImplantImplant

Implanon => Nexplanon
progestin-only contraceptive implant progestin-only contraceptive implant
single flexible 4 cm rod inserted under the single flexible 4 cm rod inserted under the skin of the upper arm skin of the upper arm
contains 68 mg etonogestrel – releases 40 contains 68 mg etonogestrel – releases 40 mcg daily - 3 year efficacy mcg daily - 3 year efficacy
no pregnancies in 73,000 monthly cyclesno pregnancies in 73,000 monthly cycles
irregular menstrual bleeding common irregular menstrual bleeding common
clinician visit required for insertion and clinician visit required for insertion and removal – new insertion device for Nexplanonremoval – new insertion device for Nexplanon
Nexplanon is radiopaqueNexplanon is radiopaque

Implanon

Nexplanon

Intrauterine Intrauterine Contraceptive Contraceptive SystemSystem

Mirena
levonorgestrel-releasing intrauterine levonorgestrel-releasing intrauterine system - 20 mcg daily - 5 year efficacysystem - 20 mcg daily - 5 year efficacy
highest risk of PID within 20 days of highest risk of PID within 20 days of insertioninsertion
irregular menstrual bleeding common irregular menstrual bleeding common in first 3-6 monthsin first 3-6 months
clinician visit required for insertion and clinician visit required for insertion and removalremoval
Mirena

ParaGardParaGard®® T 380A T 380A
copper-releasing IUDcopper-releasing IUD
believed to work primarily by believed to work primarily by preventing sperm from reaching and preventing sperm from reaching and fertilizing the eggfertilizing the egg
10 year efficacy10 year efficacy
irregular menstrual bleeding common irregular menstrual bleeding common in first 3-6 monthsin first 3-6 months
clinician visit required for insertion clinician visit required for insertion and removaland removal

ParaGard® T 380A

Barrier Barrier MethodsMethods


Vaginal spermicides

FC2 Female Condom

Male latex condoms

Male polyurethane
condoms

Factors influencing condom useavailabilityavailabilitypartner negotiationpartner negotiationlow “cost” - reduction in pleasurelow “cost” - reduction in pleasurehigh benefit - partner’s appreciation, belief high benefit - partner’s appreciation, belief that condoms prevent STDsthat condoms prevent STDsfavorable male attitude toward responsibilityfavorable male attitude toward responsibilitycondom use condom use declinesdeclines with age and length of with age and length of the relationshipthe relationship23% of young men (17-22 yr) using condoms 23% of young men (17-22 yr) using condoms report at least one condom break during the report at least one condom break during the previous year => emergency contraceptionprevious year => emergency contraception

Condom use and hormonal contraception
Consistent condom useConsistent condom use
OCsOCs 21%21%
DMPADMPA 18%18%
NorplantNorplant 9% 9%
Condom use at last intercourseCondom use at last intercourse
hormonal contraception - 52%hormonal contraception - 52%
no hormonal contraception - 69%no hormonal contraception - 69%

Adherence
assure privacy and confidentialityassure privacy and confidentiality
discuss options and personal discuss options and personal preferencespreferences
connect to education and employmentconnect to education and employment
counsel about side effectscounsel about side effects
schedule monthly recall visitsschedule monthly recall visits
continue condom use!continue condom use!