treatment of temporomandibular joint dysfunction with a visible
TRANSCRIPT

General Dentistry
Treatment of temporomandibular joint dysfunction with a visiblelight-cured resin overlay denture: A case report
Siong-Beng
Abstract A woman presented with temporomandibular dysfunction caused by a markedoverchsure of her mandible. She complained of pain and clicking noises in hertemporomandibular ¡oint. After initial assessment and treatment with a provisionalocclusal acryhc resin splint, the patient was provided with a definitive overlaydenture with visible light-cured resin as occlusal overlays. The denture was stable inthe mouth and ¡iie occlusal resin material showed some occlusal wear at the 2-yearexamination. (Quintessence lnt 1996:27:105-109.)
Introduction
Sphnt therapy is one of the most commonly usedmodalities of treatment in patients presenting withtemporomandibular dysllinction (TMD). Patients withthis condition may complain of some of the followingsymptoms: pain at or around the temporomandibularjoint (TMJ), clicking noises, limited range of motion,or an occasional locking of the TMJ. After the initialstabihzation of these patients and the concomitantreduction in the signs and symptoms, the definitivetreatment plan in many of these patients may be therehabilitation of the occlusion with fixed partialdenmres, multiple crowns,'' or removable dentures.'
The vertical dimension of occlusion of patientssuffering from TMD is often reduced and may sometimes cause problems during movement of the TM.!."""''This article describes an alternative treatment ap
' Associate Professor, Department of Restorative Dentistry, NationalUniversity of Singapore, Faculty of Dentistry. National UniversityHospital, Singapore.
Reprint requests: Dr Siong-Beng Keng. Associate Professor, Departmentof Restoralive Dentistij, National University of Singapore. Faeulty ofDentistry, National University Hospiral. Lower Kent Ridge Road.Singapore 0511.
proach for the management of a patient requiring therestoration of the vertical dimension of occlusion. Thepatient was provided with an overlay visible light-cured (VLC) resin partial denture.
Case report
Patient history
A 40-year-old woman was experiencing clicking noisesin her joint associated with pain. She had beensuffering from this condition for 1 year and decidedthat her symptoms needed treatment. She had noticedjoint noises, especially during chewing, and occasionalcatching sensations when she opened her mouth. Shealso complained of occasional pressure in her earduring wide opening of her mouth.
Examination
Examination revealed a grossly overdosed position ofthe mandible. Examination of her joints revealedreciprocal clicking in her left TMJ. The initial clickoccurred at 10-mm opening and the closing click at5 mm. The area of the left TMJ was tender to palparion,especially during movements that accentuated thesounds. Neuromuscular examination revealed tender
Quintessence International Volume 27, Number 2/1996 105

Fig 1 Reduced vertical dimension o1 occiusion. Themandibular anterior teeth almost contact the upper ridge.
Fig 2 Partial overlay denture framework with meshworkdesign over the occiusal surfaces of posterior teeth.
ness of her left and right masseter muscles. There wereno unusual findings in the joint or articular surfaces onthe transcranial radiographs.
Occiusal examination revealed an edentulous spacein the maxillary anterior ridge and the loss of hermandibular left first molar and right second premoiar.Deep anterior overbite was evident, and the mandib-ular leeth almost contacted the maxillary alveoiar ridge(Fig 1). The vertical dimension of occlusion wasassessed to be decreased by 3 to 4 mm. The patient waswearing an existing cobaU-chromium partiai dentureto replace three maxiilary anterior teeth for estheticreasons; it provided no change to her present verticaldimension of occlusion.
Treatmenl
At the initial assessment of the patient's occlusion, twotongue blades were placed between the posterior teethto increase the vertical dimension of occlusion. Thistest eliminated the joint sounds. A complete-coveragemandibular acrylic resin anterior repositioning splintwas then fabricated and positioned to eliminate theclick. The patient was instructed to wear this appliancecontinuously, even while eating. If she felt discomfort,she was to restrict mandibular movements to withinpainless limits. A mild analgesic was prescribed to betaken on a regular basis for 7 days.
At the 1-week recall, she reported that her joint hadonly occasional "pops" and her mandibular openingwas smoother and less restricted. The fit of theprosthesis was checked and minor adjustments weremade to the occiusal surfaces of the acrylic resin splint.
She was reviewed again at 4 weeks. At that time, theappliance was thinned slightly to allow the mandible to
move backward to a more retruded position. Thepatient was stabilized in this position for another 2months, and the appliance was adjusted again. After 4months with the patient in this comfortable positionand an acceptable vertical dimension of occlusion, amore permanent prosthesis was suggested.
Permanent alteration to maintain the occiusal rela-tionship in this position requires conventional pros-thodontic rehabilitation with multiple crowns andprostheses. However, following discussion with thepatient concerning extensive fixed restorations andthe associated financial and time commitments, it wasdecided to restore the vertical height of occlusion inthe symptom-free position with an overlay removablepartial denture.
The partial denture was designed with conventionalcircumferential clasping and the use of a casting meshdesign over the teeth to be overlaid (Fig 2). Themandibular framework was fitted in the mouth and theappropriate adjustments were made to the framework.The position of the mandible with the provisionalacrylic resin splint in place was used as a guide toestablish the height of occiusal increase. The maxiUo-mandibular position was then recorded with a waxwafer in the predetermined vertical dimension. Thecast with the overlay framework was mounted togetherwith the opposing maxillary cast on the articulator.
The tooth contour was huilt up in wax over theframework on the cast in proper oeclusion with theopposing maxillary teeth. To ohtain the anatomy of thewaxed tooth surfaces, an occiusal index was made. Thewax on the metal framework was later removed withboiling water. The rope of Triad VLC tooth-coloredmaterial (Dentsply) was then applied to the framework
106 Quintessence International Volume 27, Number 2/1996
Keng
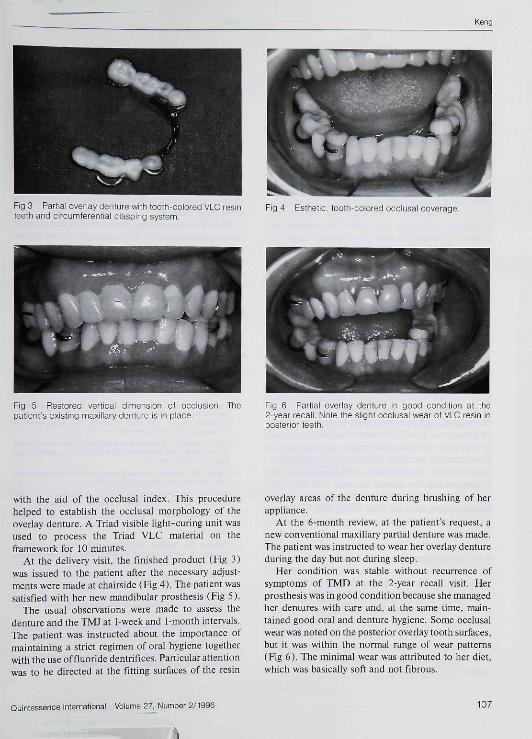
Fig 3 Partiai overiay denture with tooth-colored VLC resin Fig 4 Esthetic, tooth-coiored occiusai coveiage.teeth and circumferential clasping system
Fig 5 Resiored verficai dimension of occlusion. Tbepatient's existing maxiiiary denture is in place.
Fig 6 Partiai overiay denture in good condition at tfie2-year recail. Note the slight occlusai wear of VLC resin inposterior teeth.
with the aid of the occlusal index. This procedurehelped to establish the occlusal morphology of theoverlay denture, A Triad visible light-curing unit wasused to process the Triad VLC material on theframework for 10 minutes.
At the dehvery visit, the finished product (Fig 3)was issued to the patient after fhe necessary adjust-ments were made at chairside (Fig 4). The patient wassatisfied with her new mandibular prosthesis (Fig 5),
The usual observations were made to assess thedenture and the TMJ at 1-week and 1-month intervals.The patient was instructed ahout the importance ofmaintaining a strict regimen of oral hygiene togetherwith the use of fluoride dentrifices. Particular attentionwas to be directed at the fitting surfaces of the resin
overlay areas of the denture during brushing of herappliance.
At the 6-month review, at the patient's request, anew conventional maxillary partial denture was made.The patient was instructed to wear her overlay dentureduring the day but not during sleep.
Her condition was stable without recurrence ofsymptoms of TMD at the 2-year recall visit. Herprosthesis was in good condition because she managedher dentures with care and. at the same time, main-tained good oral and denture hygiene. Some occlusalwear was noted on the posterior overiay tooth surfaces,but it was within the normal range of wear patterns(Fig 6). The minimal wear was attrihuted to her diet,which was basically soft and not fibrous.
Quintessence International Volume 27, Number 2/1996 107
Keng
Discussion
The etiology of temporomandibular disorders is mulli-faclorial'*; the method of treatment thus depends onthe patient's situation. Sphnt therapy has been advo-cated as a reversible hne of treatment, the effects ofwhich can be studied in the patient.' Theories on thesphnt's mode of action include occlusal disengage-ment: mandibular realignment; restored vertical di-mension; TMJ repositioning; and cognitive awareness."'
In the patient in this case report, the increasedverticai dimension of occlusion resulting from theinitial splint therapy allowed her condyle-disc relation-ship to be stabilized. This treatment reduced hersymptoms of clicking and pain. The patient wasallowed to adjust to her new vertical height ofocclusion for 4 months before an occlusal overlaydenture was issued. The resultant increase and restor-ation of the vertical dimension of occlusion by the useof the overlay denture prosthesis was well tolerated bythe patient. Carlsson et al" reported that the verticaldimensiorr of occlusion in dentate patients can bealtered considerably with bite planes seetningly with-out affecting the resting tonus of the mandibularmuscles.
Base metal has its limitations in terms of pooresthetics and extreme hardness for occlusal overlays ofmultiple teeth, in the patient treated in this case, VLCtooth-colored material was used to mechanically bondto the meshwork.'^'^ The meshwork desigr: allowedthe required thickness of the tooth-colored material tobe light cured. Triad VLC resin is basically composedof a urethane dimethacrylate matrix with acr>'lic resincopolymer and micro tine silica fillers and a camphoro-quinone-amine photoinitiator. Tlie manufacturer re-commends that the material be cured with blue light(400 to 500 nm) using three high-intensity quartzhalogen lamps, as in the Triad curing unit. This high-intensity light results in deep curing of the material to adepth of 5 to 6 mm.
This material may have an advantage over conven-tional autopolymerizing resin, in that it is dimension-ally stable once polymerized,''' nontoxic, easy tomanipulate, and has greater wear resistance than doesacrylic resin. In another study of visible light-curedmaterial. Khan et al'̂ showed that Triad VLC materialhas superior transverse strength and microhardnesscompared with those of conventional denture baseacrylic resins. They obtained microhardness values of1S.93 kg/mm' arrd transverse strength values of 12.77kg/tnm^ for Triad VLC.
Examination of the patient's overlay denture re-vealed that the wear patterns on the occlusa! surfaces ofthe resin after 2 years' usage were within acceptablelimits, probably because the patient had a normalmixed diet and not a fibrous one. She also did not usethe denture during sleep, reducing the possible wearon the occlusal surfaces. No parafunctional or otheroral habit was observed in the patient. Similarly,Bledsoe'*' treated a patient with TMD by using thebonded VLC appliance as an intermediate splinttherapy, while Kolodney and Akerly" used the resincomposite veneer occlusal surface overlay partialdenture to manage a case of overclosure resulting fromgeneralized attrition.
The VLC resin overlay partial denture technique issimple and economical. The technique may be appro-priate in selected cases when time constraints andfinancial reasons make it an alternative to con-ventional crown and bridgework. The use of theoverlay partial denture, however, requires regularreviews to ensure that the denture is well maintainedand the patient's TMD is stable.
References
1. Hellsing G, Carlsson GE, Hollander LG, Johansson B. Temporo-mandibular joint adaplalion to mandibular reposilioning in aduKocdusal reliabiiilalion. J Craniomand Pract 1985-3:274-279.
2. Eltala-Yiitalo UM, Markkanen H. Syrjanen S. Functional disturb-ances of liie masticalory system and the effect of prosthetic treatmeniin patients treated with fixed prosthesis four years earlier. JCranioniand Pract 1987;i:44-49.
3. Dibai N, Saint VU. Restoration of severe tooth wear and an unevenoeclusal plane using removable partial dentures. Compend ContinEdücDent l986i7:69-79.
4. Gibson MW. Reduced vertical dimension and temporomandibularpain. Dent Mag Oral Topics 1967;S4:149.
5. Shore N. Temporomandibular Joint Dysflinclion and OcclusalEquilibration, ed 2. Philadelphia: Lippincott, 1976:238-249.
6. Laskin DM, Greene CS. Tecluiologieal methods in the diagnosisand treatment of temporotnandibular disorders. Quintessence lnt1992;23:95-102.
7. Pullinger AG. Seligman DA, Solberg WK Temporomandibulardisorders. II. Occlusal factors associated wilh tetiip oro mandibularJoint tenderness and dysflinetion. J Proslhet Dent 1988;59;,16.1-367.
8. Greene CS, Marbach JJ. Epidemiológica! studies of mandibulardysfunction, J Prosthet Dent 1982i48: Í84- Í90.
9. Gray RJM, Davies SJ. Quayie AA. A clinical approaeh totemporomandibular disorders-Splint therapy. Br Dent J 1994̂177Tt3i-i42.
10. Clark GT A critical evaluation of orthopédie interocclusal appliancetherapy: Design, theory and overall effectiveness. J Am Dent Assoc19S4;108.359-364,
11. Carlsson GE, Ingervall B, Koeak G. Effect of increasing verticaldimension on the masticatory system in subjects with natural teeth. JPrnsthetDent l979;41;2S4-289.
108 Quintessence International Voiume 27, Number 2/1996
Kenc
12. Friedman MH, Howard 1, Framework design for overlay removablepartiai dentute, J Prosthet Dent I983:5O;866,
13. Tood R, Holt J. Metal frarrtework design for an onlay removablepartial denttire. J Prosthet Dent 19S7;57:116-117,
14. Ogle RE, Sorensen SE. Lewis EA, A new lighi-cured resin systemapplied to removable prosthodontics,J Prosthet Dent I9B6:56:497-506,
15. Kiian Z, Fraunhofer JA, Razavi R. The staining characteristics,transverse strength, and microhardness of a visible light-cureddenture base material, J Prosthet Dent 1937:57:384-386,
16. Bledsoe WS, The bonded visible light cured applianee intermediatesplint therapy for temporomandibular joint patient, J CraniomandPract 1989:7:126-131.
17. Kolodney H. Akerly WB, A composite resin veneer oeckisal surfaceon an overlay partial denture. Compend Contin Educ Dent L99I;12:66-70, G
ISBN 0-8S715-244-3;
Ouintessence Iniernafional Volume 27, Number 2/1996
Bonded Ceramic InlaysJean-François Roulet and Stefan Herder
Ceramic inlays have become an important treatmentmodality in modern dental practice becattse of theincreasing demand for esthetic posterior restorations andthe evolution of more complex ceramic systems. Thisbook serves as both textbook and manual to presentimportant principles atid procedures on the adhesivetechnique nsed with ceramic iiilay.s. The first part coversthe scientitic fundamentals of the dental materials used inthe ceramic inlay technique and forms the theoretical baseon which the subsequent procedures are built. The secondpart of the book describes the techniques necessary toproduce and seat a glass-ceramic inlay. Preparation andimpression techniqties can be used for all ceramic inlaysystems and so can the adhesive technique. BondedCeramic Inlays should be required reading for any student,dental laboratory technician, or dentist who gainssalisfaction and pride from esthetics and precision increating posterior restorations.
CALL OR FAX TO ORDER: Te(708) 6SZ-3223: Fax: 1708) 682-32HS
or fill out Ihi order form and send to;Quintessence Publistring Co, Inc351 N. Kimberly DriveCarul Stream, IL 60iaH-1881
(8U«¡ 621-0387 or
1copies of (2443) Bonded Ceramic 'Itilays at US $63/copy.
Name
Street
City .
Telephone
Zip
I 1 General Practitii I ISpeciaiist.I I Bill me, including shipping & hundiing[ I Charge to my credit card plus shipping &[ ] Visa/MastetCard [ ¡American Express
and I ing
Expires.
Signature.
, J