this work is licensed under a creative commons attribution...
TRANSCRIPT

Copyright 2007, The Johns Hopkins University and Richard Chaisson. All rights reserved. Use of these materials permitted only in accordance with license rights granted. Materials provided “AS IS”; no representations or warranties provided. User assumes all responsibility for use, and all liability related thereto, and must independently review all materials for accuracy and efficacy. May contain materials owned by others. User is responsible for obtaining permissions for use from third parties as needed.
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike
License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this site.
TB Epidemiology
Richard E. Chaisson, MDJohns Hopkins UniversityCenter for Tuberculosis Research

3
Richard E. Chaisson, MD
Professor of medicine, epidemiology, and international healthDirector of the Johns Hopkins University Center for Tuberculosis ResearchCo-founded the Johns Hopkins HIV Clinic cohortInterests focus on tuberculosis and HIV infection, including global epidemiology and control, prevention, clinical trials, and public health interventionsPrincipal investigator of the Consortium to Respond Effectively to the AIDS/TB Epidemic (CREATE)
Section A
General Epidemiology and Natural History

5
Statistics
“There are two kinds of statistics. The kind you look up and the kind you make up.”
— Archie Goodwin in Rex Stout’s Nero Wolfe
mystery Death of a Doxy, 1966

6
Highlights of 2006 Global TB Report
About 9 million new cases in 2004−
Sixteen million prevalent cases
−
Ninety-eight percent in developing countriesMore than 10% increase since 1997Increasing rates in Africa and Eastern Europe−
Decreasing elsewhere
1.9 million deaths−
Leading cause of death in people with HIV
Progress in case detection, but >50% still not diagnosed and treated!

7
Growth of TB in Africa and Eastern Europe

8
Estimated Number of TB Cases by Country, 2004

9
Estimated Incidence of TB by Country, 2004

10
Twenty-Two High-Burden Countries

11
Reported TB Cases, United States, 1982–2003

12
TB Case Rates* by Age Group and Sex, United States, 2003
*Cases per 100,000

13Source: Comstock GW. Frost Revisited: The Modern Epidemiology of
Tuberculosis: The Third Wade Hamptom
Frost Lecture. Am. J. Epidemiol..1975; 101: 363-382. By permission of Oxford University Press. All Rights Reserved.
Cohort Analysis of Effect of Age on TB Incidence

14*Cases per 100,000
TB Case Rates* by Race/Ethnicity

15
U.S.-Born vs. Foreign-Born

16
Length of U.S. Residence Prior to TB Diagnosis, U.S.

17
Epidemiology of TB Fundamentals
Reservoir of infection humans (cattle)−
Virtually all transmission is person to person
Two-stage process−
Initial infection with M. tuberculosis
−
Progression from infection to disease

18
Epidemiology of TB Fundamentals
Risks for initial infection−
Source case factors
−
Environmental factors−
? Recipient factors
Risks for disease once infected−
Inoculum size
−
Cellular immunity−
Body habitus
−
Genetics

19
Exposure(close contact)
No infection70%
Infection~30%
Risk factors –
Close contact, BR>HH>Casual
–
Duration of contact –
Severity of disease, cough, cavities
Risk of Infection and Disease among Exposed Individuals

20
Number of Droplets Produced by Different Activities

21
TB Infection in Children by Type of Contact

22
TB Infection among Inflight Personnel

23
Risk of Infection and Disease among Exposed Individuals

24
HIV and Risk of TB Disease among Infected Individuals

25
Diagnostic Standards for Tuberculosis
Latent TBTuberculin skin test−PPD-S−Cutpoints
for positive−Nonspecific
Interferon-gamma assays
Active TBCXRSputum smear−Sensitivity 50%
Sputum cultureClinical criteria
26
TST Quantiferon
PPDQuantiferon
Gold
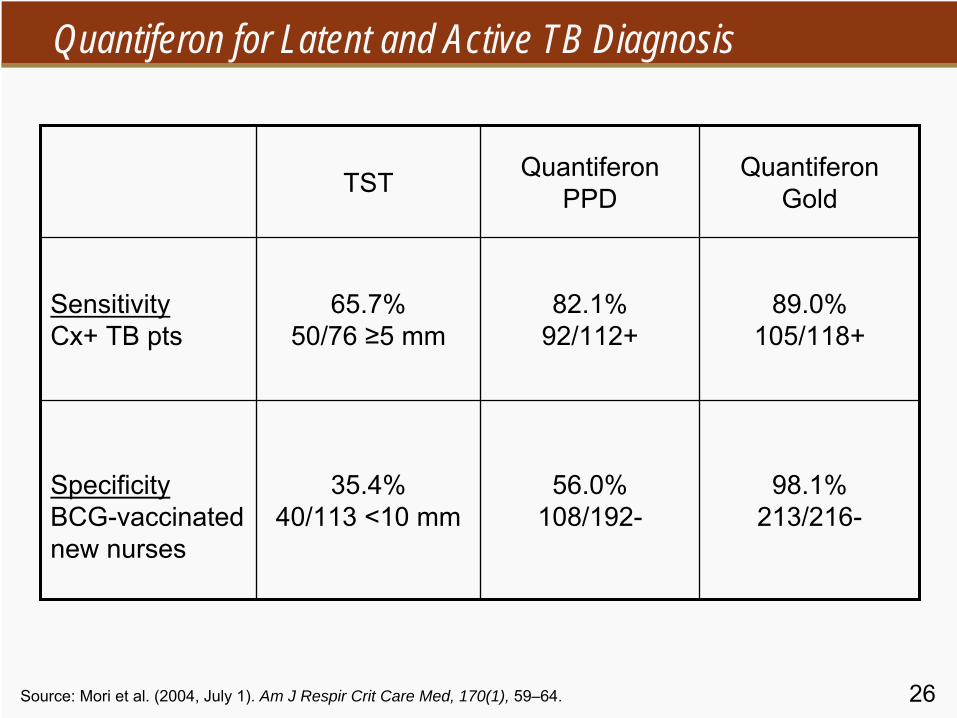
SensitivityCx+ TB pts
65.7%50/76 ≥5 mm
82.1%92/112+
89.0%105/118+
SpecificityBCG-vaccinated new nurses
35.4%40/113 <10 mm
56.0%108/192-
98.1%213/216-
Source: Mori et al. (2004, July 1). Am J Respir Crit Care Med, 170(1), 59–64.
Quantiferon for Latent and Active TB Diagnosis

27
ELISPOT and TST in School Contacts of Infectious TB

28
Response to ELISPOT or TST by BCG Vaccination Status
Vaccinated
(n = 467)Unvaccinated
(n = 68)
p for vaccinated
vs. unvaccinated
ELISPOTPositive
Negative131 (28.1%)
336 (71.9%)16 (23.5%)
52 (76.5%)0.44
Heaf
grade
4
3
2
1
0
52 (11.1%)
81 (17.6%)
110 (23.6%)
116 (24.8%)
108 (23.1%)
10 (14.7%)
2 (2.9%)
10 (14.7%)
13 (19.1%)
33 (48.5%)
0.002*
*χ2
test for trend across all five Heaf
gradesSource: Ewer et al. (2003, April 5). Lancet, 361(9364), 1168–1173.
Response to ELISPOT or TST by BCG vaccination status in a school TB outbreak

Section B
Epidemiologic Basis for TB Control

30
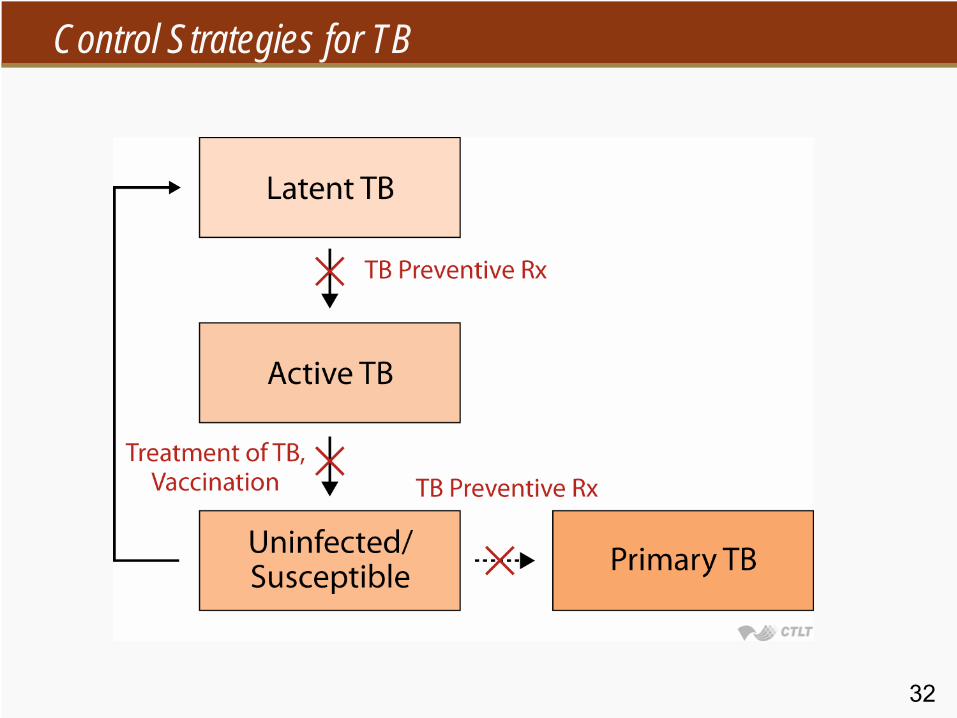
Strategies for Control of Tuberculosis
Detection and treatment of casesTreatment of latent infectionVaccination

31
Definitions of Tuberculosis Control
Diagnosis of 70% of all cases, with cure rates of 85%(WHO/IUATLD)
R0 <1−
Less than one secondary case for each new case
(Frost, 1937, Anderson and May, 1982)The incidence of tuberculosis goes down
32
Control Strategies for TB

33
Use Dots More Widely

34
DOT vs. DOTS
Directly Observed Therapy−
Supervision of all doses of TB medication by a health team member
Directly Observed Therapy, Short Course−
WHO policy for TB control, with programmatic imperatives to strengthen TB control efforts

35
What Is DOTS?
Governmental commitment to TB controlSystem for registration and follow-up of TB casesReliable supply of TB drugsMicrobiologic confirmation of TB diagnosisSupervision of at least the initial phase of TB therapy
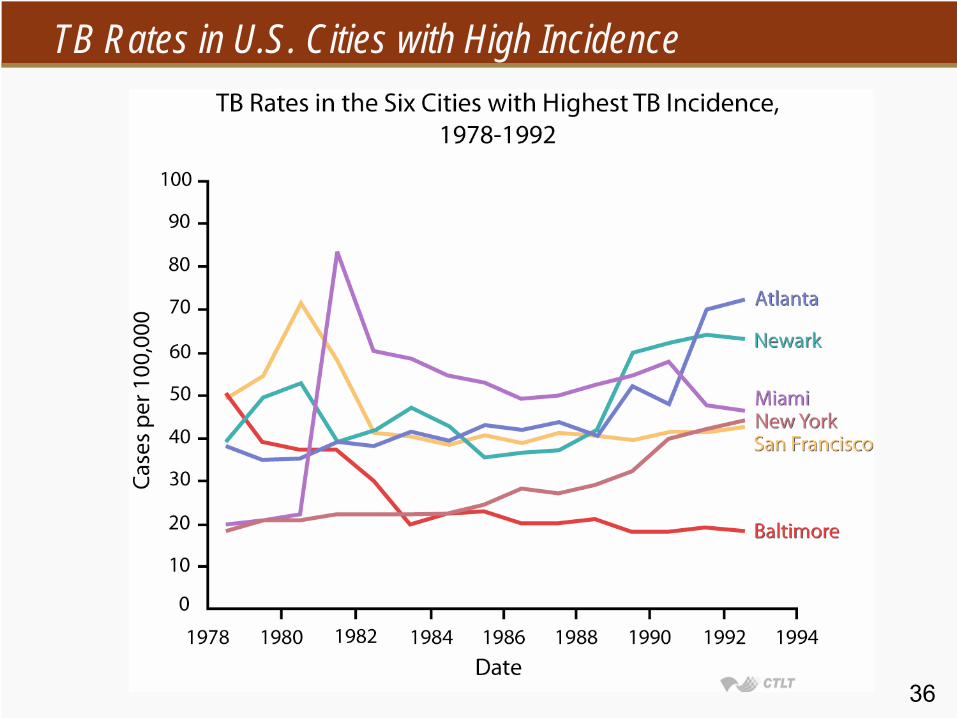
36
TB Rates in U.S. Cities with High Incidence

37
Treatment Outcomes by WHO Region

38
DOTS Results in TB Incidence Decline

39
AFB Smears Performed by the TB Program, Peru

40
Full DOTS Implementation in Vietnam

41
What Can DOT(S) Do?
Increase treatment completion ratesReduce the emergence of drug-resistant TBImprove cost-effectiveness of TB controlIn conjunction with other interventions, reduce TB incidence

Section C
Challenges in TB Control

43
Challenges in the Control of Tuberculosis
HIV epidemicMDR tuberculosisHealth system weaknesses and lack of political will−
Poor infrastructure and lack of support
−
Weak organization of primary health services−
Private practitioners
−
Prisons

44
Tuberculosis and HIV

45
Tuberculosis and HIV
Estimated prevalence of HIV in adults (%)
Mea
sure
d pr
eval
ence
of H
IV in
TB
pat
ient
s (%
)

46
Uganda: Falling HIV Prevalence, Increasing TB Incidence
Rising TB incidence in setting of falling HIV prevalence in Uganda

47
TB in Botswana: Pre- and Post-DOTS, HIV

48
Reported TB Cases, U.S., 1979–1999
49
Major Challenges in HIV-Related TB
Case detection−
High prevalence of active TB in community
3% of HIV+ pregnant women8% of HIV VCT clients
−
Negative smears more commonTreatment of TB and HIV−
Drug interactions
−
Drug toxicity and adverse reactionsPrevention−
Use of preventive therapy

50Source: Espinal. (2001). N Engl J Med, 344, 1294–1303.
WHO/IAUTLD Survey of TB Drug Resistance, 1996–1999
Primary drug resistance—median 10.7%−
Primary MDR—median 1%
Acquired drug resistance—median 23%−
Acquired MDR—median 9.3%
MDR “hot spots” widespread

51Note: Based on initial isolates from persons with no prior history of TB. MDR TB defined as resistance to at least isoniazid and rifampin.
Primary MDR TB, United States, 1993–2002

52
MDR-TB and XDR-TB in HIV+ Patients, South Africa
41% of hospitalized patients in rural KwaZulu-Natal had MDR-TB25% of these had XDR-TB−
Resistant to first-
and second-line TB drugs
All HIV+52 of 53 diedMedian survival: 16 days
Source: Gandhi et al. (2006, August). International AIDS Conference, Toronto, Canada.

53
Global Approaches to MDR TB Control
Expansion and strengthening of DOTS−
Prevent creation of MDR cases through mismanagement
−
Assure access to drug supplyDOTS-Plus−
Second-line drugs for TB in setting of DOTS
−
Green Light Committee of WHOApproves proposals for national DOTS+ programs
New drug development−
Global Alliance for TB Drug Development
54
BCG* for Prevention of TB
Live attenuated vaccine derived from M. bovis early 1900s by Calmette and GuérinMost widely used vaccine in the worldEfficacy shown in clinical trials in 1930s–1950sRecent trials show lack of benefitGenetic evidence of attenuation of strain over years of laboratory passageNew vaccines in development, but will need to be compared with BCG
*Bacillus of Calmette
and Guérin (BCG)

55
Outcome/design Relative odds or risk 95% CI
TB preventionClinical trialsCase-control studies
0.490.50
0.34–0.700.39–0.64
Prevention of deathClinical trials 0.29 0.16–0.53
Meta-Analysis of BCG Effectiveness in 26 Studies
Source: Colditz
et al. (1994). JAMA, 271, 698–702.

56
Relationship to Lab Passage to BCG Efficacy

57
Strategies for Control of Tuberculosis: Limitations
Detection and treatment of cases−
Poor diagnostic capabilities
−
Poor compliance with treatment−
Emergence of drug resistance
−
HIV epidemicTreatment of latent infection−
Resources for screening and treatment
Vaccination−
Current vaccine doesn’t prevent disease or transmission

58
Imperatives for Controlling TB in the Coming Years
Expand DOTSIncrease case findingEvaluate and treat contacts of casesTreat high-risk patients with latent TBDecrease HIV prevalenceProvide effective treatment for HIVDevelop effective HIV and TB vaccines