the ringlike structure of macular pigment in age-related...
TRANSCRIPT

The Ringlike Structure of Macular Pigment in Age-Related Maculopathy: Results from the Muenster Agingand Retina Study (MARS)
Martha Dietzel,1,2 Meike Zeimer,2 Britta Heimes,2 Daniel Pauleikhoff,2
and Hans-Werner Hense1
PURPOSE. The role of macular pigment (MP) in age-relatedmaculopathy (ARM) is still not clearly understood. Recentstudies have reported on variations in the spatial distribution ofMP optical density (MPOD) including a secondary peak (“ring”)in the slope of the MPOD profile. The authors investigated in across-sectional manner the presence of ringlike structures,their determinants, and their relationship with ARM.
METHODS. In all, 369 participants of the Muenster Aging andRetina Study were examined using dual-wavelength analysis ofautofluorescence images. ARM was graded using digital fundusphotographs according to the International Classification Sys-tem.
RESULTS. A ringlike structure was observed in 73 (19.8%) studyparticipants. The MP maximum of the ring was located onaverage at 0.85° and the minimum at 0.48° from the center ofthe fovea. Their concordance between pairs of eyes was highlysignificant. MPOD measured at eccentricities of 0°, 0.25°, and0.5° from the fovea was significantly lower in eyes with ring-like structure, whereas it was significantly higher at 1.0° and2.0° than that in eyes without the ring. Ringlike structureswere significantly more common in females and never smokersand were found significantly less often in eyes with ARM thanin healthy eyes, even after adjustment for influential factors(adjusted odds ratio, 0.347; 95% confidence interval, 0.196–0.617).
CONCLUSIONS. Ringlike structures in the MP spatial profile arefairly common, show a high degree of bilaterality, and ap-peared inversely related with ARM. (Invest Ophthalmol Vis Sci.2011;52:8016–8024) DOI:10.1167/iovs.11-7610
The macular pigment (MP) consists of three dietary carote-noids, lutein (L), zeaxanthin (Z), and meso-zeaxanthin
(MZ), which accumulate at high concentrations at the macula.1
L and Z are entirely of dietary origin, whereas MZ is largelyderived from retinal L. The MP acts as an antioxidant and as afilter of short-wavelength light, therefore limiting photooxida-
tive damage to retinal cells.1 Due to these properties, it issupposed that MP may protect against the development ofage-related maculopathy (ARM) and its late-stage, age-relatedmacular degeneration (AMD), the leading cause of blindness inpeople older than 50 years in the developed world.1
Corroborating histologic2 and clinical studies,3,4 we havepreviously reported on a wide variation of MP distribution.5
Recently, several research groups have shown that MP opticaldensity (MPOD) does not always steadily decline from thecenter of the fovea to the periphery. They observed ringlikestructures with a secondary peak of MP at a distance of 0.7°from the fovea.6,7 Others reported on “central dip” MP profileswith a dip of MPOD in 0.25° retinal eccentricity, followed by arise at 0.5°, and finally a steady decline to the periphery.8
Although the impact of those variations of MPOD profiles isstill unknown, there is first evidence that the spatial distribu-tion of MP might be associated with risk factors for ARM andAMD, respectively.8
We therefore investigated the ringlike structure in the spa-tial distribution of MPOD, its determinants, and its associationwith ARM in patients with ARM and eye-healthy controls whoparticipated in the first follow-up examination of the MuensterAging and Retina Study (MARS).
MATERIAL AND METHODS
Subjects
MARS is a longitudinal study designed to identify medical, environmen-tal, and genetic factors, with implications for the pathogenesis andprogression of ARM. Eligibility criteria were previously described indetail.9 A sample of 1060 residents of the Muenster (Germany) regionwith and without ARM were examined at baseline (MARS-I) of whom828 (85.5% of all eligible) took part in MARS-II.5 Median follow-up timewas 2.6 years. In MARS-II, we replicated the baseline study protocoland additionally measured the MPOD.5 For the present report, we usedonly data obtained at MARS-II in a cross-sectional manner.
As described previously,9 subjects were interviewed by trained staffmembers using a standardized risk factor questionnaire. Detailed infor-mation was obtained about smoking history, lifestyle, and the currentuse of supplements containing L and/or Z. Height and weight weremeasured. The spherical equivalent refractive error in each eye and thenumber of pseudophakic eyes were determined.
The recruitment and research protocols were reviewed and ap-proved by the Institutional Review Board of the University of Muen-ster, and written informed consent was obtained from all study partic-ipants, in compliance with the Declaration of Helsinki.
Grading of ARM
As previously described,9 30° stereoscopic digital color fundus photo-graphs were taken from both eyes after pupil dilatation with tropic-amide 0.5% and phenylephrine 2.5%. The diagnosis of ARM features
From the 1Institute of Epidemiology and Social Medicine, Univer-sity of Muenster, Muenster, Germany; and the 2Ophthalmology Depart-ment, St. Franziskus Hospital Muenster, Muenster, Germany.
Supported in part by Deutsche Forschungsgemeinschaft GrantsHE 2293/5-1, 5-2, 5-3, and PA 357/7-1; the Intramural InternationalMonetary Fund of the University of Muenster; the Pro Retina Founda-tion; and the Jackstaedt Foundation.
Submitted for publication March 23, 2011; revised June 10 andAugust 18, 2011; accepted August 18, 2011.
Disclosure: M. Dietzel, None; M. Zeimer, None; B. Heimes,None; D. Pauleikhoff, None; H.-W. Hense, None
Corresponding author: Martha Dietzel, Institute of Epidemiologyand Social Medicine, University Hospital Muenster, Domagkstrasse 3,48129 Muenster, Germany; [email protected].
Clinical and Epidemiologic Research
Investigative Ophthalmology & Visual Science, October 2011, Vol. 52, No. 118016 Copyright 2011 The Association for Research in Vision and Ophthalmology, Inc.
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933458/ on 06/22/2018

was based on grading of the photographs according to the Interna-tional Classification and Grading System for ARM.10 In accordance withthe Rotterdam Study classification, ARM was classified into five severitystages.11 Eyes were classified as having no ARM (stages 0 to 1), ARM(stages 2 to 3), or as AMD (stage 4).12,13
Measurement of MPOD
The autofluorescence (AF) method for measuring MPOD has beenpreviously described.14–18 In brief, it is based on the AF of lipofuscin,which is located in the retinal pigment epithelium (RPE) cells.14,19
Lipofuscin is excited in vivo between 400 and 580 nm, to emit itsfluorescence in the 500- to 800-nm spectral range, whereas MP absorbsblue light for wavelengths shorter than 550 nm, with a peak absor-bance of 460 nm.16 In the fovea, excitation light within the absorptionrange of MP is partially absorbed by the carotenoids, resulting in anarea of reduced fluorescence. To measure the MPOD, the dual-wave-length approach of the AF method compares results from two excita-tion wavelengths that are differentially absorbed by the MP, therebytaking account of the nonuniform distribution of lipofuscin in theRPE.16
For quantitative imaging, we used a Heidelberg Retina Angiograph(HRA 1; Heidelberg Engineering, Heidelberg, Germany) that was mod-ified for the measurement of MP. This approach has previously beenused in clinical studies.5,15,17,18,20 In brief, alignment and focusing ofthe fundus were performed under 488-nm illumination. Retinal bleach-ing was conducted to minimize the influences of absorption of incom-ing light by the visual pigments.17 For bleaching, the central 20 � 20°area of the retina was illuminated with the 488-nm wavelength light ofthe HRA 1 for at least 30 seconds.17 After retinal bleaching, sequencesof 20° images were captured at 488 and 514 nm and MP density mapswere generated by digital subtraction of the log AF images, and meanMPOD values were calculated for circles centered on the fovea aspreviously described.17 In our analyses, these circles were located ateccentricities of 0.25°, 0.5°, 1.0°, and 2.0°. The reference locationwhere MPOD is optically undetectable was selected at an eccentricityof 6° because the profile normally plateaus for eccentricities largerthan approximately 4°.16
MP Density Profile and Ringlike Structure
To investigate the spatial distribution of MP, we analyzed the MPdensity maps and the radial density profiles. The latter were generatedand graphically displayed by plotting the mean MPOD values that werecalculated for each radius around the fovea, against the distance to thefovea21 (see Figs. 1a, 1c, 1e).
A ringlike structure was defined as the density profile showing abimodal pattern; the latter consists of a central peak of MPOD followedby a decline and a secondary peak of increased density on the slope ofthe profile (see Fig. 1a). The bimodal pattern of MPOD is also visible inthe associated MP density map as a “ringlike structure,” with a centralpeak of MPOD surrounded by a ring of increased density (Fig. 1b). Incases where the distribution of MPOD showed no strictly monotonicdecline from the center of the fovea to the periphery, and no explicitringlike pattern of MP (but, for example, an implied plateau on theslope of the profile), the eyes were marked as having “intermediatedistributions” (Figs. 1c, 1d). The absence of a ringlike structure wasdefined as a strictly monotonous decline of the density profile graphfrom the center of the fovea to the periphery without any plateauingor bimodal pattern (Fig. 1e), with the associated MP density mapshowing no ring patterns (Fig. 1f).
Density profiles were analyzed for the eccentricity at which themaximum and minimum of the ring occurred, and for the respectiveMPOD measured at these eccentricities; the “maximum” of the ringwas thereby defined as the secondary maximum of MP forming the ringand the “minimum” as the minimum density between the central peakof MPOD and the second peak. Furthermore, all MPOD profiles wereanalyzed for the “half width,” which indicates the eccentricity from thefovea where half of the peak of MPOD is reached.
Study Sample
MPOD measurements were taken in 609 of 828 participants of MARS-IIbecause the HRA 1 became available only after MARS-II had alreadystarted. AF images of inadequate quality and those with central AMD(i.e., with central geographic atrophies or choroidal neovasculariza-tions that affect the measurement of AF17) were excluded. From the659 eyes with valid AF measurements we excluded those with missinginformation in relevant study variables, such that data on 571 eyes of369 participants were available for analyses. Bilateral data were avail-able for 202 pairs of eyes.
Apart from the assessment of symmetry in pairs of eyes, we presentpatient-based analyses using the results obtained in one study eye:where measurements for single eyes only were available, we usedthese eyes as study eyes; if measurements for pairs of eyes wereavailable, we used the result of the right eye, with the exception ofcases with an “intermediate distribution” in the right eye and a clearattribution of the ringlike structure in the left eye (“ring” or “no ring”),in which case the latter was used in the analyses.
Statistical Analysis
The present report is a cross-sectional analysis of data obtained at theMARS-II examination, which included measurements of MPOD, spher-ical equivalent refractive error, body mass index (BMI), age, smokinghistory, current use of MP-containing supplements, status of the lenses(phakic, pseudophakic), and classification of ARM. Spearman’s rankcorrelation coefficients were computed to assess the association of thelocalization and the respective MPOD values of the ringlike structurebetween pairs of eyes. For analyses of single eyes, �2 tests werecomputed to compare categorical and t-tests for continuous variables.Pairwise U tests were used for unadjusted comparison of the three MPdistribution groups. The impact of influential factors and confounderson the presence of ringlike structures was evaluated by multivariablelogistic regression models. Adjusted odds ratios (ORs) and 95% confi-dence intervals (95% CIs) were calculated. A value of P � 0.05 wasconsidered statistically significant. A commercial analytical softwarepackage (SAS for Windows, version 9.1; SAS Institute Inc., Cary, NC)was used for analysis.
RESULTS
The 369 participants included in this report had a mean age of71.6 years. They were more often females and about half of thesingle study eyes were free of ARM (stage 0 to 1 according tothe Rotterdam Study classification). Other characteristics of theparticipants are contained in Table 1.
Of the 369 single study eyes, 73 (19.8%) showed a ringlikestructure, 245 (66.4%) had no ring, and 51 (13.8%) displayed an“intermediate distribution.” Figure 2 shows the mean MPOD indensity units (D.U.) at six eccentricities from the fovea (0°,0.25°, 0.5°, 1.0°, 2.0°, and 6.0°) and the mean “half width”according to these three types of spatial MPOD patterns. Themean eccentricity of the minimum of ringlike structures was at0.48 � 0.09°, whereas the maximum was at 0.85 � 0.15°; thecorresponding mean MPOD values were 0.45 � 0.16 and0.56 � 0.17 D.U., respectively (Fig. 2a).
Table 2 shows the mean MPOD at different eccentricitieswithin the three groups. Mean MPOD measured at 0°, 0.25°,and 0.5° from the fovea was significantly lower in eyes with aring than in those without a ring. In contrast, eyes with a ringhad significantly higher mean MPOD measured at 1.0° and 2.0°compared with that of the no-ring group. Likewise, the mean“half width” was significantly higher in eyes with a ring patternthan that in eyes without a ring pattern. MPOD values of eyeswith intermediate distributions were rather consistently inbetween the values found in eyes with and without a ring.
In 202 pairs of eyes, ringlike patterns were highly symmet-rical: 41 (20.3%) had a bilateral ringlike structure, 108 (53.5%)
IOVS, October 2011, Vol. 52, No. 11 Ringlike Structure of Macular Pigment and ARM 8017
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933458/ on 06/22/2018

had no ringlike structure, and 22 (10.9%) had an intermediateMP distribution in both eyes; by contrast, only 14 (6.9%)showed a ringlike structure in solely one eye and 17 (8.4%) hadan intermediate distribution in one and no ring in the other eye(P � 0.0001). Similarly, the localization of the ringlike struc-
ture, the respective MPOD values, and further characteristicsof the ring pattern showed a high degree of symmetry betweenright and left eyes (see Table 3).
We found no difference in the presence of ringlike struc-tures in phakic and pseudophakic eyes (P � 0.6992). Likewise,
FIGURE 1. Radial density profiles of macular pigment (MP) optical density (MPOD) (a, c, e) and associated MP density maps (b, d, f) with andwithout ringlike structures. (a, b) A bimodal distribution of MPOD with a secondary peak of MPOD forming the ringlike structure. (c, d) Anintermediate distribution of MP without strictly monotonic decline of MPOD but with an implied plateau in the slope of the profile. (e, f) A steadydecline of MPOD from the center of the fovea to the periphery without any ringlike signs.
8018 Dietzel et al. IOVS, October 2011, Vol. 52, No. 11
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933458/ on 06/22/2018

we found no association between the spherical equivalentrefractive error in phakic eyes and MPOD values measured at0°, 0.25°, 0.5°, 1.0°, and 2.0°, the mean half width, and thelocalization of the minimum or maximum of the ringlike struc-ture (correlation analyses, each P � 0.05).
Females and never smokers showed significantly more oftenringlike structures than did males and ever smokers (Table 4).In contrast, other potential influential factors such as currentuse of supplements containing L and/or Z, overweight (definedas BMI � 30 kg/m2), and age older than 70 years were notsignificantly associated with the presence of ringlike struc-tures.
Interestingly, a ringlike structure was clearly less commonin the presence of ARM (Table 4). Further detailed analyseswith logistic regression models revealed an unadjusted OR of0.343 (95% CI, 0.196–0.603; P � 0.0002) for the occurrenceof a ringlike structure compared with the group with no ring oran intermediate distribution, when ARM was present (seeTable 5, model 1). Thus, the ringlike structure seemed almostthree times less common in eyes with ARM than that in healthyeyes. Adjustment for the influential factors sex and smoking didnot materially alter the magnitude of this association (Table 5,model 2).
Of note, drusen size, drusen type, and area covered bydrusen (within the central foveal field [radius: 500 �m] of thestandard grid used for ARM classification by fundus photo-graphs) showed no statistically significant differences in ARMpatients with a ring, without a ring, or with intermediatedistribution (data not shown). Likewise, in study eyes withringlike structure, the localization of the maximum and mini-mum of the ring and the respective MPOD values were notstatistically significantly different between participants withand without ARM (data not shown).
DISCUSSION
We used quantitative analyses of AF images and identifiedringlike structures in the spatial distribution of MP, whichshowed a high degree of symmetry between right and left eyesand occurred significantly more often in females, never smok-ers, and in eyes without ARM.
The first systematic evaluation of the ringlike structure ofMPOD was presented by Staurenghi G, et al. (IOVS 2003;44:
ARVO E-Abstract 5188) and Delori FC, et al. (IOVS 2004;45:ARVO E-Abstract 1288). By analyzing AF images, Delori et al.7
described bimodal spatial distributions of MP that were char-acterized by a central peak of highest MP density surroundedby a ring with high-density values at approximately 0.7° fromthe fovea. These results were confirmed by Berendschot andvan Norren,6 who additionally used the technique of reflec-tance spectroscopy, and by Wolf-Schnurrbusch et al.,21 whoobserved ringlike structures at 0.66°. These findings are wellcompatible with our observations. We determined the meanmaximum of ringlike structures at 0.85° from the center of thefovea, whereas we found the minimum, like Delori et al.,7 at0.48°. In the latter report, the MPOD values at the maximumand minimum were 81% and 75% of the peak MPOD, respec-tively, which is also in the same range of magnitude as ourresults in 41 pairs of eyes with bilateral ring. Moreover, Deloriand colleagues7 reported on the “MPOD at maximum to min-imum ratio” of 1.09, which was lower than our results of 1.27in right and 1.23 in left eyes. Thus, the differences of MPOD atmaximum and minimum of the ringlike structure were slightlymore pronounced in our study.
Since unbleached cone pigment could theoretically influ-ence the profile of the MP distribution,7 retinal bleaching wasperformed before taking the first MPOD measurements in ourstudy, in accordance with procedures previously described.17
Although the ringlike structure and its localization can beconsistently observed with different imaging modalities,7 theanatomic basis of the ringlike structure is not yet fully under-stood. Snodderly et al.22 measured the MP density profiles inretinal layers of macaque and cebus monkeys and found insome animals a “trimodal” distribution with secondary maximaat 200–300 �m (i.e., around 0.8° eccentricity) from the fovea.The main peak was associated with MP along the photorecep-tor axons, whereas the secondary maxima followed the innerplexiform layer. The authors hypothesized that profile variabil-ity in different species might be the result of differences in theshape of the foveal depression.22 Interestingly, Kirby et al.23
recently reported on an association between “secondarypeaks” in the MP spatial profile measured by heterochromaticflicker photometry (HFP) and wider foveae measured by opti-cal coherence tomography (OCT) in a small group of healthyindividuals (n � 16), indicating a relationship between spatialdistribution of MPOD and foveal architecture. They measuredthe MPOD at five distinct eccentricities from the fovea (i.e., at0.25°, 0.5°, 1.0°, 1.75°, and 7°) and defined profiles with lowerMPOD at 0.25° than at 0.5° as “secondary peaks,” thus alsoconfirming variations in spatial distribution of MPOD. On theother hand, the location of these “secondary peaks” differedfrom the “ringlike structures” found in our study and thementioned studies6,7,21 and reasons for this difference need tobe further elucidated.
Whereas other studies reported a mean MPOD of 0.28 D.U.measured at 1.0° eccentricity from the fovea24 and 0.54 D.U. at0.25°, 0.44 D.U. at 0.5°, and 0.32 D.U. at 1.0°,25 using devicessimilar to the one used in our study, our MPOD measurementresults were slightly higher. On the other hand, our MPODvalues are well compatible with the results of Lima et al.,15
who reported on MPOD of 0.51 D.U. measured at 0.5°, and ofTrieschmann et al.,17 who reported on a mean MPOD of 0.50D.U. measured at 0.5° eccentricity. Interestingly, in the latterstudy, oral supplementation with lutein raised MPOD on aver-age by 0.1 D.U., which is comparable with our results; wefound that MPOD at 0.5° was on average 0.09 D.U. higher inusers of L/Z supplements compared with nonusers (0.64 vs.0.55 D.U.).5 These findings support our contention that sup-plement use by study subjects may explain higher values in ourstudy.
TABLE 1. Characteristics of Study Participants (n � 369)
Characteristic Value*
Mean age, y 71.6 (5.3)Female; n (%) 227 (61.5)Mean BMI, kg/m2 27.3 (4.1)Smoking
Never smokers; n (%) 243 (65.9)Ever (current, former) smokers; n (%) 126 (34.1)
Current users of supplements containing luteinand/or zeaxanthin; n (%)
56 (15.2)
Study eyes; showing a ringlike structure ofMPOD; n (%)
73 (19.8)
Pseudophakic study eyes; n (%) 65 (17.6)Spherical equivalent refractive error in phakic
study eyes�0.53 (2.38)
ARM stage according to RotterdamClassification (in study eye):
Stage 0; n (%) 99 (26.8)Stage 1; n (%) 95 (25.7)Stage 2; n (%) 89 (24.1)Stage 3; n (%) 86 (23.3)
* Values are given as mean (SD), unless otherwise noted.
IOVS, October 2011, Vol. 52, No. 11 Ringlike Structure of Macular Pigment and ARM 8019
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933458/ on 06/22/2018
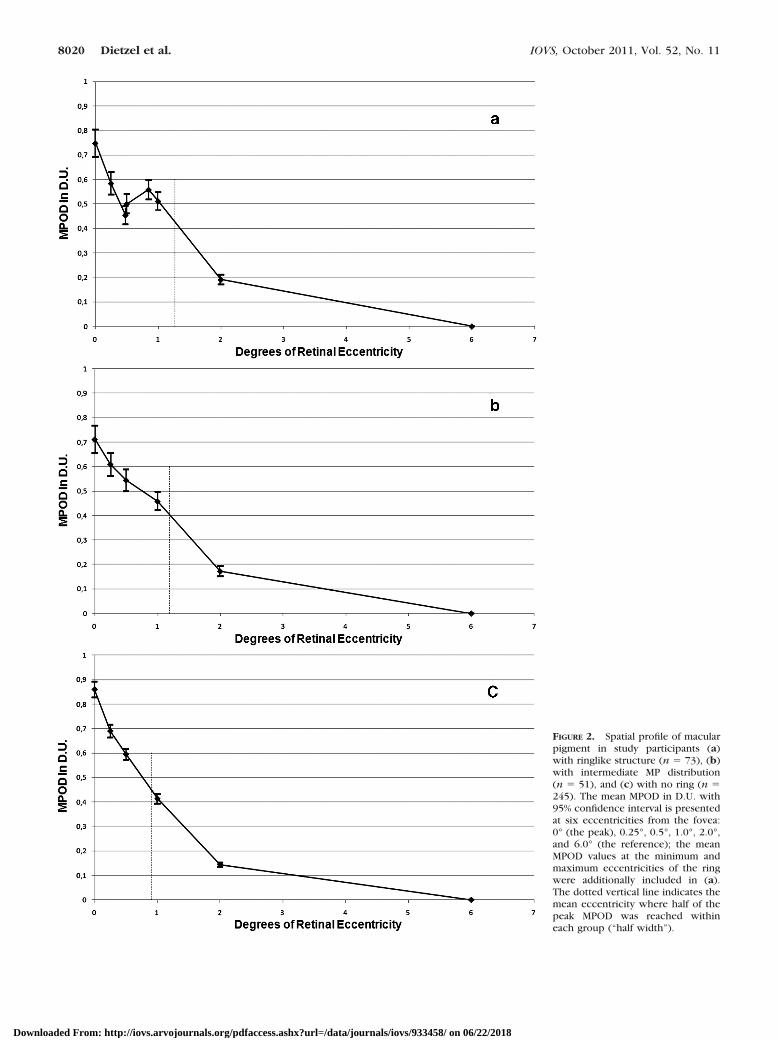
FIGURE 2. Spatial profile of macularpigment in study participants (a)with ringlike structure (n � 73), (b)with intermediate MP distribution(n � 51), and (c) with no ring (n �245). The mean MPOD in D.U. with95% confidence interval is presentedat six eccentricities from the fovea:0° (the peak), 0.25°, 0.5°, 1.0°, 2.0°,and 6.0° (the reference); the meanMPOD values at the minimum andmaximum eccentricities of the ringwere additionally included in (a).The dotted vertical line indicates themean eccentricity where half of thepeak MPOD was reached withineach group (“half width”).
8020 Dietzel et al. IOVS, October 2011, Vol. 52, No. 11
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933458/ on 06/22/2018
Regarding the symmetry in the spatial distribution of MPbetween pairs of eyes, Snodderly et al.22 examined retinalsections of a monkey and found a similar shape of the MPdensity profile (i.e., the “trimodal” distribution mentioned ear-lier) in both foveae. Similarly, Staurenghi and colleagues (IOVS2003;44:ARVO E-Abstract 5188) reported a high degree ofsymmetry of the ring pattern in 36 study subjects measured invivo by AF imaging (P � 0.002). Our study confirms theseresults, showing a high degree of symmetry of the localizationof the ring, the respective mean MPOD values, the peak MPODat 0°, and the “half width” in pairs of eyes with ringlikestructures. Thus, a substantial part of retinal MP levels may begenetically closely regulated, as suggested by Liew et al.24 in atwin study on the heritability of MPOD. Although these authorsdid not explicitly analyze the spatial distribution of MPOD,
they observed a high degree of correlation of MPOD measuredat 1° eccentricity by AF imaging that was more pronounced inmono- than that in dizygotic twins.24
We observed significant differences in MPOD measured ateccentricities of 0°, 0.25°, 0.5°, 1.0°, and 2.0° between partic-ipants with and without a ring. These differences are likely dueto diverse MP profiles: the broader distribution in individualswith a ringlike structure (i.e., a secondary peak at 0.85°) is alsotransferred to higher MPOD values at 1.0° and 2.0° and higher“half width” values; conversely, lower MPOD values at 0.25°and 0.5° are a reflection of the minimum of the ring at 0.48°.Interestingly, the intermediate distribution group rather con-sistently showed mean MPOD values in between those of thering and the no-ring groups. The mean “half width” of theintermediate group was similar to that of the ring group,
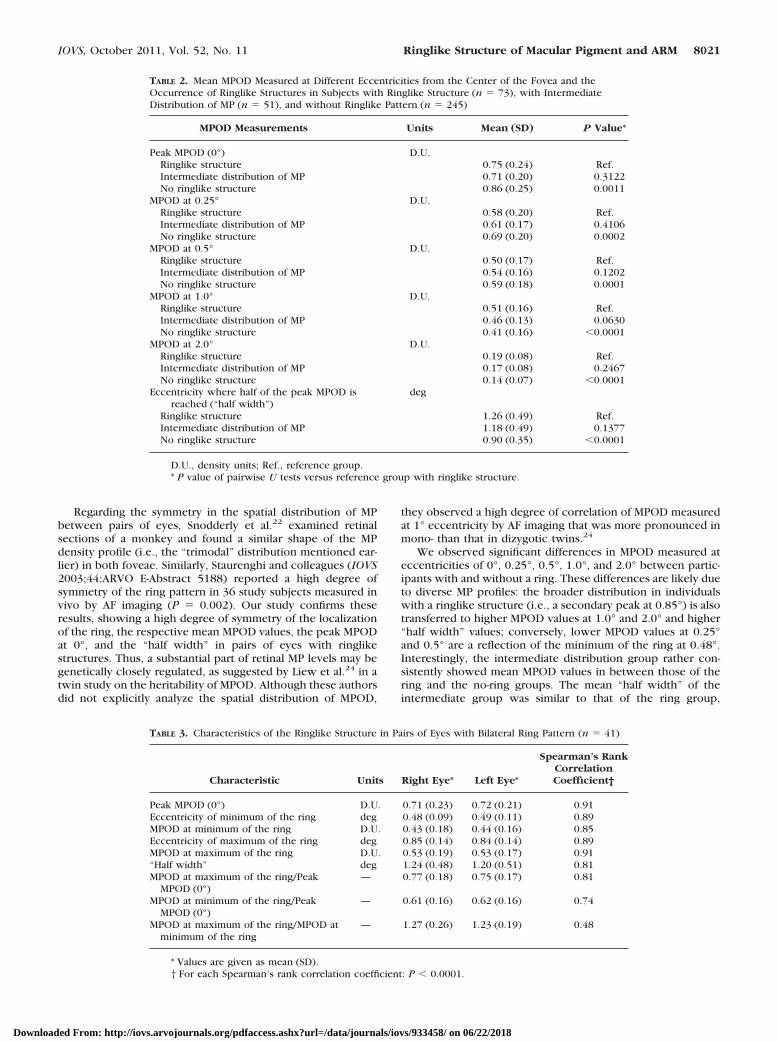
TABLE 2. Mean MPOD Measured at Different Eccentricities from the Center of the Fovea and theOccurrence of Ringlike Structures in Subjects with Ringlike Structure (n � 73), with IntermediateDistribution of MP (n � 51), and without Ringlike Pattern (n � 245)
MPOD Measurements Units Mean (SD) P Value*
Peak MPOD (0°) D.U.Ringlike structure 0.75 (0.24) Ref.Intermediate distribution of MP 0.71 (0.20) 0.3122No ringlike structure 0.86 (0.25) 0.0011
MPOD at 0.25° D.U.Ringlike structure 0.58 (0.20) Ref.Intermediate distribution of MP 0.61 (0.17) 0.4106No ringlike structure 0.69 (0.20) 0.0002
MPOD at 0.5° D.U.Ringlike structure 0.50 (0.17) Ref.Intermediate distribution of MP 0.54 (0.16) 0.1202No ringlike structure 0.59 (0.18) 0.0001
MPOD at 1.0° D.U.Ringlike structure 0.51 (0.16) Ref.Intermediate distribution of MP 0.46 (0.13) 0.0630No ringlike structure 0.41 (0.16) �0.0001
MPOD at 2.0° D.U.Ringlike structure 0.19 (0.08) Ref.Intermediate distribution of MP 0.17 (0.08) 0.2467No ringlike structure 0.14 (0.07) �0.0001
Eccentricity where half of the peak MPOD isreached (“half width”)
deg
Ringlike structure 1.26 (0.49) Ref.Intermediate distribution of MP 1.18 (0.49) 0.1377No ringlike structure 0.90 (0.35) �0.0001
D.U., density units; Ref., reference group.* P value of pairwise U tests versus reference group with ringlike structure.
TABLE 3. Characteristics of the Ringlike Structure in Pairs of Eyes with Bilateral Ring Pattern (n � 41)
Characteristic Units Right Eye* Left Eye*
Spearman’s RankCorrelationCoefficient†
Peak MPOD (0°) D.U. 0.71 (0.23) 0.72 (0.21) 0.91Eccentricity of minimum of the ring deg 0.48 (0.09) 0.49 (0.11) 0.89MPOD at minimum of the ring D.U. 0.43 (0.18) 0.44 (0.16) 0.85Eccentricity of maximum of the ring deg 0.85 (0.14) 0.84 (0.14) 0.89MPOD at maximum of the ring D.U. 0.53 (0.19) 0.53 (0.17) 0.91“Half width” deg 1.24 (0.48) 1.20 (0.51) 0.81MPOD at maximum of the ring/Peak
MPOD (0°)— 0.77 (0.18) 0.75 (0.17) 0.81
MPOD at minimum of the ring/PeakMPOD (0°)
— 0.61 (0.16) 0.62 (0.16) 0.74
MPOD at maximum of the ring/MPOD atminimum of the ring
— 1.27 (0.26) 1.23 (0.19) 0.48
* Values are given as mean (SD).† For each Spearman’s rank correlation coefficient: P � 0.0001.
IOVS, October 2011, Vol. 52, No. 11 Ringlike Structure of Macular Pigment and ARM 8021
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933458/ on 06/22/2018

indicating a broader MPOD distribution but without a second-ary peak in the slope of the MPOD profile.
We further noted that the presence of ringlike structureswas not associated with eyes being phakic or pseudophakic.Likewise, we found no association between the sphericalequivalent refractive error and MPOD in phakic study eyes.The issue of refractive defect has been previously ad-dressed,26,27 with results similar to those reported in our study.
Our results of ringlike structures being significantly morecommon in females are compatible with the work of Delori etal.7 These authors hypothesized that shapes and sizes of thefovea differ between males and females, with a more openfoveal depression in females.7 However, this was not sup-ported by a recent study reporting a reduced central subfieldthickness in females compared with that in males, but nosex-dependent differences in foveal pit morphology, as mea-sured by spectral-domain (SD) OCT.28 Moreover, Berendschotand van Norren6 did not find any differences between malesand females with regard to the presence of ring structures.
The relationship between age and MPOD has been previ-ously investigated,5,20,29 but with inconsistent results: al-though some studies reported a decline of MPOD with age,20
we found a slight increase of MPOD (measured at 0.5° and2.0°) with age,5 whereas others found no age dependence atall.29
The presence of ringlike structures was not associated withage in our elderly study individuals with a mean age of 71.6years (range, 62–85 years). Despite examining younger sub-jects with a mean age of 50 years (range, 19–76 years), Be-rendschot and van Norren6 also found no effect of age on thering structure in the spatial distribution of MPOD. Interest-ingly, although not explicitly mentioning age dependence ofthe ringlike structure in individuals ranging in age from 20 to70 years, Delori et al.7 reported on a broadening of the MPdistribution with age; the occurrence of “intermediate distri-butions,” which included plateaus on the slopes of the profiles;and a distribution pattern that “is often fragmented at old age.”These results seem to concur with those in our elderly studypopulation, where we also found “intermediate distributions”in the spatial distribution of MPOD.
To our knowledge, this study is the first to evaluate therelationship between smoking and the ringlike structure in alarge study population. We report here that never smokersshowed significantly more often a ringlike structure than didever smokers. Of note, Delori et al.7 studied 41 individuals anddid not detect an effect of smoking on the ring pattern. To ourknowledge, there are also no studies that investigated theimpact of supplementation with L and/or Z on the ringlikestructure. We found no statistically significant relationship be-tween current supplementation with L and/or Z and the pres-ence of ring patterns in our cross-sectional study. However, wedid not have data on duration of supplement use and its dosagein current users, and this lack of detailed information maypartly account for the absence of such an association. On theother hand, Connolly et al.30 recently reported on the disap-pearance of “central dips” (i.e., lower MPOD at 0.25° than thatat 0.5° of eccentricity) after 8 weeks of oral supplementationwith L, Z, and MZ in four study participants, measured by HFP,thus suggesting an influence of supplementation on spatialdistribution of MPOD. These results might indicate that envi-ronmental factors related to oxidative stress could modify thespatial distribution of MPOD. However, further studies areobviously warranted in this area.
The most important finding of our study was that ringlikestructures were significantly more common in persons without
TABLE 4. Association of the Ringlike Structure of MPOD with Other Factors among 369 StudyParticipants, �2 Test
Factor
Ringlike Structure
P ValuePresent, n (%)Intermediate
Distribution, n (%) Absent, n (%)
SexFemale 57 (25.1) 27 (11.9) 143 (63.0)Male 16 (11.3) 24 (16.9) 102 (71.8) 0.0039
SmokingNever 60 (24.7) 33 (13.6) 150 (61.7)Ever 13 (10.3) 18 (14.3) 95 (75.4) 0.0040
Current use of supplements*Yes 13 (23.2) 8 (14.3) 35 (62.5)No 60 (19.2) 43 (13.7) 210 (67.1) 0.7580
Body mass index, kg/m2
�30 59 (21.1) 39 (14.0) 181 (64.9)�30 14 (15.6) 12 (13.3) 64 (71.1) 0.4737
Age group, y�70 38 (23.0) 25 (15.2) 102 (61.8)�70 35 (17.2) 26 (12.7) 143 (70.1) 0.2328
Age-related maculopathyNo 53 (27.3) 30 (15.5) 111 (57.2)Yes 20 (11.4) 21 (12.0) 134 (76.6) 0.0001
*Containing lutein and/or zeaxanthin.
TABLE 5. Association of the Ringlike Structure of MPOD withAge-Related Maculopathy
Predictor Variables OR 95% CI P Value
Unadjusted, model 1ARM 0.343 0.196–0.603 0.0002
Adjusted, model 2ARM 0.347 0.196–0.617 0.0003Sex (female) 2.214 1.178–4.162 0.0136Smoking (ever smokers) 0.453 0.230–0.889 0.0213
This table provides results of logistic regression models compar-ing the presence of a ringlike structure of MPOD with that of anintermediate distribution/no ring; n � 369 study participants.
8022 Dietzel et al. IOVS, October 2011, Vol. 52, No. 11
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933458/ on 06/22/2018

ARM. It may be worth noting that all the studies on ringlikestructures of MPOD mentioned earlier involved only personswith normal retinal status,6,7,21 whereas we were able to com-pare groups of subjects with and without ARM. As reportedearlier, mean MPOD was not different between our studyparticipants with and without ARM after adjustment for con-founders and exclusion of users of L/Z supplements.5
In our study setting, 1.0° eccentricity from the fovea corre-sponded to 270- to 305-�m eccentricity from the fovea. Thus,the central field of the standard grid used for ARM classifica-tion, which has a radius of 500 �m, included the ringlikestructures whose mean peak was found at 0.85° eccentricityfrom the fovea. Of note, morphologic characteristics of drusen,such as type, number, and area covered by drusen within thecentral radius of 500 �m of the macula, were not differentbetween ARM patients with and without ringlike structures.Likewise, we found no differences in the localization of thering and the respective MPOD values between participantswith and without ARM when a ringlike structure was present.
Recently, first evidence was presented that indicated thatthe spatial distribution of MP might be associated with riskfactors for ARM and AMD.8 Using HFP, Kirby et al.8 observed“central dip” MP profiles (defined by a dip of MPOD at 0.25°,a rise at 0.5°, and then a steady decline to the periphery) moreoften in older subjects and in smokers. They concluded thatthe “central dip” might represent an undesirable feature ofmacular pigmentation. Contrary to our study, Kirby and col-leagues8 included persons ranging in age from 18 to 70 yearswithout any ocular pathology.
Interestingly, former studies that involved younger and oph-thalmologically healthy subjects found the ringlike structuremore frequently (in approximately half of the subjects6,7) thanwe did in our elderly study participants (in approximately 20%)who, in addition, relatively often showed intermediate distri-bution patterns. Therefore, we hypothesize that the ringlikestructure of MP may be interpreted as an individual character-istic of the fovea that tends to change or even disappear in thecourse of life and, in particular, in combination with ARM; thismay be potentially related to alterations in absorption andstorage of MP, especially in the parafoveal area.
In conclusion, we have performed extensive analyses onthe ringlike structure of MPOD as a specific pattern of spatialdistribution of MP, comparing persons with and without ARM.We have shown that ringlike structures exhibited a high de-gree of symmetry between right and left eyes and were morecommon in females, never smokers, and persons free of ARM.The reasons and mechanisms of these relationships are pres-ently not clearly understood. Therefore, longitudinal studiesshould investigate how the spatial distribution of MPODchanges individually over the course of time. Furthermore,longitudinal studies including the techniques of high-resolutionSD-OCT might help to better understand whether changes inthe spatial distribution of MP are the sequelae of developingARM or whether the ringlike structure in the spatial distribu-tion is protective against ARM. Similarly, the impact of MP-containing supplements on the spatial distribution of MPODand their potential effect on the occurrence or progression ofARM need to be further explored in longitudinal trials. We areconfident that further analyses of the prospective long-termobservation of the MARS cohort will be able to contribute to abetter understanding of the processes involved.
References
1. Loane E, Kelliher C, Beatty S, Nolan JM. The rationale and evidencebase for a protective role of macular pigment in age-related macu-lopathy. Br J Ophthalmol. 2008;92:1163–1168.
2. Trieschmann M, van Kuijk FJ, Alexander R, et al. Macular pigmentin the human retina: histological evaluation of localization anddistribution. Eye. 2008;22:132–137.
3. Robson AG, Moreland JD, Pauleikhoff D, et al. Macular pigmentdensity and distribution: comparison of fundus autofluorescencewith minimum motion photometry. Vision Res. 2003;43:1765–1775.
4. Trieschmann M, Spital G, Lommatzsch A, et al. Macular pigment:quantitative analysis on autofluorescence images. Graefes ArchClin Exp Ophthalmol. 2003;241:1006–1012.
5. Dietzel M, Zeimer M, Heimes B, Claes B, Pauleikhoff D, Hense HW.Determinants of macular pigment optical density and its relation toage-related maculopathy: results from the Muenster Aging andRetina Study (MARS). Invest Ophthalmol Vis Sci. 2011;52:3452–3457.
6. Berendschot TT, van Norren D. Macular pigment shows ringlikestructures. Invest Ophthalmol Vis Sci. 2006;47:709–714.
7. Delori FC, Goger DG, Keilhauer C, Salvetti P, Staurenghi G. Bi-modal spatial distribution of macular pigment: evidence of a gen-der relationship. J Opt Soc Am A Opt Image Sci Vis. 2006;23:521–538.
8. Kirby ML, Beatty S, Loane E, et al. A central dip in the macularpigment spatial profile is associated with age and smoking. InvestOphthalmol Vis Sci. 2010;51:6722–6728.
9. Dasch B, Fuhs A, Schmidt J, et al. Serum levels of macular carote-noids in relation to age-related maculopathy: the Muenster Agingand Retina Study (MARS). Graefes Arch Clin Exp Ophthalmol.2005;243:1028–1035.
10. Bird AC, Bressler NM, Bressler SB, et al. An international classifi-cation and grading system for age-related maculopathy and age-related macular degeneration. The International ARM Epidemio-logical Study Group. Surv Ophthalmol. 1995;39:367–374.
11. van Leeuwen R, Klaver CC, Vingerling JR, Hofman A, de Jong PT.The risk and natural course of age-related maculopathy: follow-upat 6 1⁄2 years in the Rotterdam study. Arch Ophthalmol. 2003;121:519–526.
12. Kanis MJ, Berendschot TT, van Norren D. Influence of macularpigment and melanin on incident early AMD in a white population.Graefes Arch Clin Exp Ophthalmol. 2007;245:767–773.
13. Kanis MJ, Wisse RP, Berendschot TT, van de Kraats J, van NorrenD. Foveal cone-photoreceptor integrity in aging macula disorder.Invest Ophthalmol Vis Sci. 2008;49:2077–2081.
14. Delori FC, Goger DG, Hammond BR, Snodderly DM, Burns SA.Macular pigment density measured by autofluorescence spec-trometry: comparison with reflectometry and heterochromaticflicker photometry. J Opt Soc Am A Opt Image Sci Vis. 2001;18:1212–1230.
15. Lima VC, Rosen R, Maia M, et al. Macular pigment optical densitymeasured by dual wavelength autofluorescence imaging in dia-betic and non-diabetic patients: a comparative study. Invest Oph-thalmol Vis Sci. 2010;51:5840–5845.
16. Trieschmann M, Heimes B, Hense HW, Pauleikhoff D. Macularpigment optical density measurement in autofluorescence im-aging: comparison of one- and two-wavelength methods.Graefes Arch Clin Exp Ophthalmol. 2006;244:1565–1574.
17. Trieschmann M, Beatty S, Nolan JM, et al. Changes in macularpigment optical density and serum concentrations of its constitu-ent carotenoids following supplemental lutein and zeaxanthin: theLUNA study. Exp Eye Res. 2007;84:718–728.
18. Wustemeyer H, Jahn C, Nestler A, Barth T, Wolf S. A new instru-ment for the quantification of macular pigment density: first resultsin patients with AMD and healthy subjects. Graefes Arch Clin ExpOphthalmol. 2002;240:666–671.
19. Delori FC, Dorey CK, Staurenghi G, Arend O, Goger DG, WeiterJJ. In vivo fluorescence of the ocular fundus exhibits retinal pig-ment epithelium lipofuscin characteristics. Invest Ophthalmol VisSci. 1995;36:718–729.
20. Jahn C, Wustemeyer H, Brinkmann C, Trautmann S, Mossner A,Wolf S. Macular pigment density in age-related maculopathy.Graefes Arch Clin Exp Ophthalmol. 2005;243:222–227.
21. Wolf-Schnurrbusch UE, Roosli N, Weyermann E, Heldner MR,Hohne K, Wolf S. Ethnic differences in macular pigment densityand distribution. Invest Ophthalmol Vis Sci. 2007;48:3783–3787.
IOVS, October 2011, Vol. 52, No. 11 Ringlike Structure of Macular Pigment and ARM 8023
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933458/ on 06/22/2018

22. Snodderly DM, Auran JD, Delori FC. The macular pigment. II.Spatial distribution in primate retinas. Invest Ophthalmol Vis Sci.1984;25:674–685.
23. Kirby ML, Galea M, Loane E, Stack J, Beatty S, Nolan JM. Fovealanatomic associations with the secondary peak and the slope ofthe macular pigment spatial profile. Invest Ophthalmol Vis Sci.2009;50:1383–1391.
24. Liew SH, Gilbert CE, Spector TD, et al. Heritability of macularpigment: a twin study. Invest Ophthalmol Vis Sci. 2005;46:4430–4436.
25. Canovas R, Lima VC, Garcia P, Morini C, Prata TS, Rosen RB.Comparison between macular pigment optical density measure-ments using two-wavelength autofluorescence and heterochro-matic flicker photometry techniques. Invest Ophthalmol Vis Sci.2010;51:3152–3156.
26. Ciulla TA, Hammond BR Jr, Yung CW, Pratt LM. Macular pigmentoptical density before and after cataract extraction. Invest Oph-thalmol Vis Sci. 2001;42:1338–1341.
27. Gallaher KT, Mura M, Todd WA, et al. Estimation of macular pigmentoptical density in the elderly: test–retest variability and effect of opticalblur in pseudophakic subjects. Vision Res. 2007;47:1253–1259.
28. Wagner-Schuman M, Dubis AM, Nordgren RN, et al. Race- andsex-related differences in retinal thickness and foveal pit morphol-ogy. Invest Ophthalmol Vis Sci. 2011;52:625–634.
29. Iannaccone A, Mura M, Gallaher KT, et al. Macular pigment opticaldensity in the elderly: findings in a large biracial Midsouth populationsample. Invest Ophthalmol Vis Sci. 2007;48:1458–1465.
30. Connolly EE, Beatty S, Thurnham DI, et al. Augmentation of macularpigment following supplementation with all three macularcarotenoids: an exploratory study. Curr Eye Res. 2010;35:335–351.
8024 Dietzel et al. IOVS, October 2011, Vol. 52, No. 11
Downloaded From: http://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933458/ on 06/22/2018