glut1 glucose transporter expression in the diabetic...
TRANSCRIPT

GLUT1 Glucose Transporter Expression in the Diabeticand Nondiabetic Human Eye
Arno K. Kumagai,* BenJ. Glasgow,-\% and William M. Pardridge*$
Purpose. The GLUT1 glucose transporter is expressed in endothelial and epithelial barriers,including the retinal capillary endothelium and the retinal pigment epithelium (RPE) of theeye. The present studies were undertaken to determine whether GLUT1 is expressed in addi-tional cell types within the human eye and whether retinal endothelial GLUT1 is aberrantlyexpressed in diabetic proliferative retinopathy in humans.
Methods. Immunohisiochemical staining of sections of human eyes obtained at surgery orautopsy from patients with and without diabetes was performed with polyclonal antisera di-rected against the human GLUT1 glucose transporter.
Results. In the course of this study, an unexpected multicellular localization of GLUT1 indifferent cellular barriers of the human eye was observed. In the nondiabetic eye, specificstaining for GLUT1 was seen in the nerve fiber layer, the ganglion and photoreceptor cellbodies, the capillaries and the RPE of the retina, the basal infoldings of the pigmented andnonpigmented layers of the ciliary body, the capillary cndoihelium and posterior epithelium ofthe iris, the corneal epithelium and endothelium, and the endothelium lining of the canal ofSchlemm. Miiller cells, a type of retinal glial cell identified by morphology and by parallelstaining for glial fibrillary acidic protein, also stained intensely positive for GLUT1. The pat-tern of GLUT1 immunoreactivity in the diabetic eyes was virtually identical to that in thenondiabetic specimens, with the notable exception that the neovascular endothelium of prolif-erative retinopathy did not stain for GLUT1.
Conclusions. These studies describe the heretofore unrecognized expression of immunoreac-tive GLUT1 in the ganglion cell layer of the retina, the endothelium lining the canal ofSchlemm, the corneal endothelium, and the basal cells of the corneal epithelium of the humaneye. The present study also provides evidence for immunoreactive GLUT1 in glial cells of thecentral nervous system. Because the expression of GLUT1 is characteristic of tissues thatpossess a barrier function, the absence of GLUT! immunoreactivity in the neovascular tissueof proliferative diabetic retinopathy suggests that the loss of selective permeability is associatedwith an absence of facilitated glucose transport in this disorder. Invest Ophthalmol Vis Sci.J994;35:2887-2894.
Otates of acute and chronic hyperglyceinia give rise topathophysiologic processes in various structures ofthe eye. Within these structures, glucose gradients arethought to be maintained by isoforms of the sodium-independent glucose transporter gene family.1
From the Departments oj "Medicine, ^Pathology, and %Ophthalmidogy, and theSliraiu Research Institute., UCLA School of Medicine, Los Angeles, Cnlijonim.Supported by National Institutes of Health grunt POI-NS-25554. AKK is therecepient of a Postdoctoral Fellowship from the Juvenile Diabetes Foundation.Submitted for publication /une 24. 1993; revised December 22. 199.3; acceptedJanuary II. 1994.Proprietary interest category: A1'.Reprint requests: Arno K. Kumagai, Ml), c./n William M. Pardndge, Ml).Department of Medicine, Division of F.ndorrinology, Mail Code 168217, UCLASchool of Medicine, Los Angeles. CA 90024.
GLUT], the first such isoform to be cloned,2 is ex-pressed in high density on the membranes of humanerythrocytes and on the brain capillaries that comprisethe blood-brain barrier.3 In addition to the blood-brain barrier, GLUT1 is expressed in other tissues pos-sessing barrier functions, including the endothelia ofthe retinal capillaries of the eye.4:> Because the neovas-cularization of the retina found in proliferative dia-betic retinopathy is characterized by "leaky" retinalvessels (that is, by a loss of barrier function)/' we inves-tigated whether GLUT] expression is preserved in theneovascularized diabetic retina. A second goal of thepresent study was to examine the expression of the
i1 Ophthalmology & Visual Srii-ix c. May I '.104, Vol. !*">, No. (>Copyright © Association lor Research in Vision and Ophihalmolog) 2887
Downloaded From: https://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933404/ on 08/23/2018
2888 Investigative Ophthalmology & Visual Science, May 1994, Vol. 35, No. 6
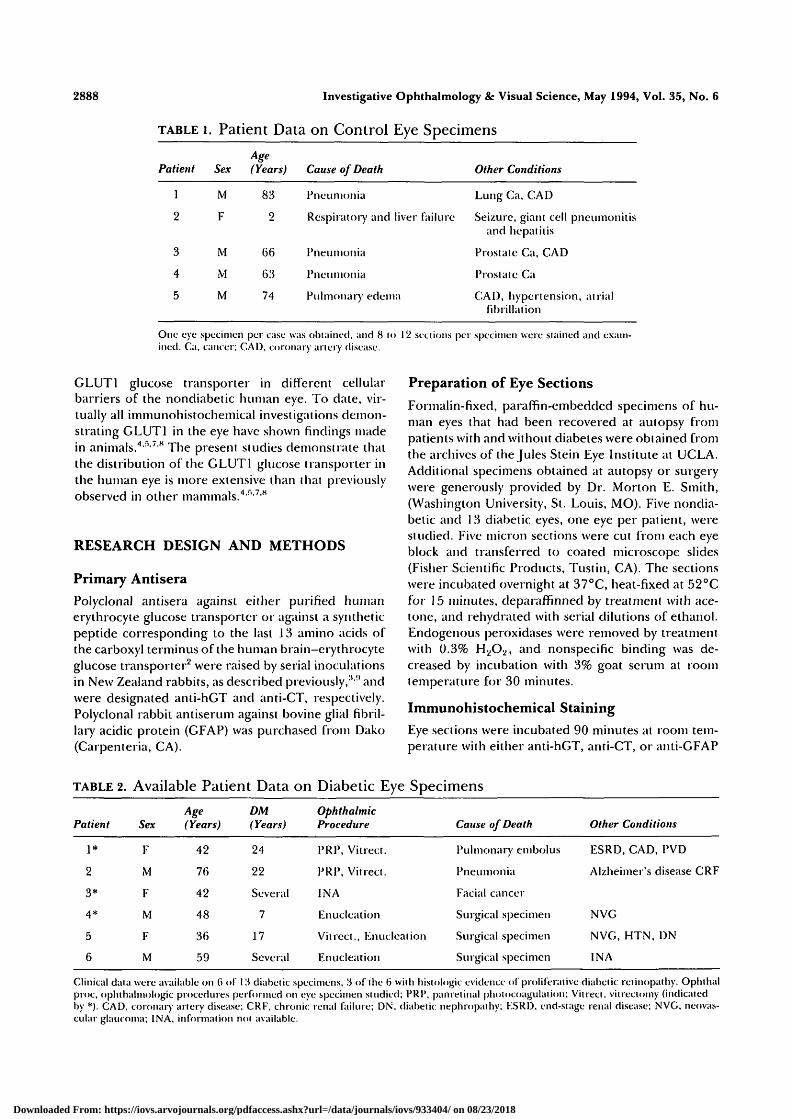
TABLE l. Patient Data on Control Eye Specimens
Patient
1
2
3
4
5
Sex
M
F
M
M
M
Age(Years)
83
2
66
63
74
Cause of Death
Pneumonia
Respiratory and liver failure
Pneumonia
Pneumonia
Pulmonary edema
Other Conditions
Lung Ca, CAD
Seizure, giant cell pneumonitisand hepatitis
Prostate Ca, CAD
Prostate Ca
CAD, hypertension, at rialfibrillation
One eye specimen per case was obtained, and 8 (<> 12 sections per specimen were stained and exam-ined. Ca, cancer; CAD, coronary artery disease.
GLUT1 glucose transporter in different cellularbarriers of the nondiabetic human eye. To date, vir-tually all immunohistochemical investigations demon-strating GLUT1 in the eye have shown findings madein animals.4">/S The present studies demonstrate thatthe distribution of the GLUT1 glucose transporter inthe human eye is more extensive than that previouslyobserved in other mammals.4•'•'•'•*
RESEARCH DESIGN AND METHODS
Primary Antisera
Polyclonal antisera against either purified humanerythrocyte glucose transporter or against a syntheticpeptide corresponding to the last .13 amino acids ofthe carboxyl terminus of the human brain—erythrocyteglucose transporter2 were raised by serial inoculationsin New Zealand rabbits, as described previously/" andwere designated anti-hGT and anti-CT, respectively.Polyclonal rabbit antiserum against bovine glial fibril-lary acidic protein (GFAP) was purchased from Dako(Carpenteria, CA).
Preparation of Eye Sections
Formalin-fixed, paraffin-embedded specimens of hu-man eyes that had been recovered at autopsy frompatients with and without diabetes were obtained fromthe archives of the Jules Stein Eye Institute at UCLA.Additional specimens obtained at autopsy or surgerywere generously provided by Dr. Morton E. Smith,(Washington University, St. Louis, MO). Five nondia-betic and 13 diabetic eyes, one eye per patient, werestudied. Five micron sections were cut from each eyeblock and transferred to coated microscope slides(Fisher Scientific Products, Tustin, CA). The sectionswere incubated overnight at 37°C, heat-fixed at 52°Cfor 15 minutes, deparaffinned by treatment with ace-tone, and rehydrated with serial dilutions of ethanol.Endogenous peroxidases were removed by treatmentwith 0.3% H.2O2, and nonspecific binding was de-creased by incubation with 3% goat scrum at roomtemperature for 30 minutes.
Immunohistochemical Staining
Eye sections were incubated 90 minutes at room tem-perature with either anti-hGT, anti-CT, or anti-GFAP
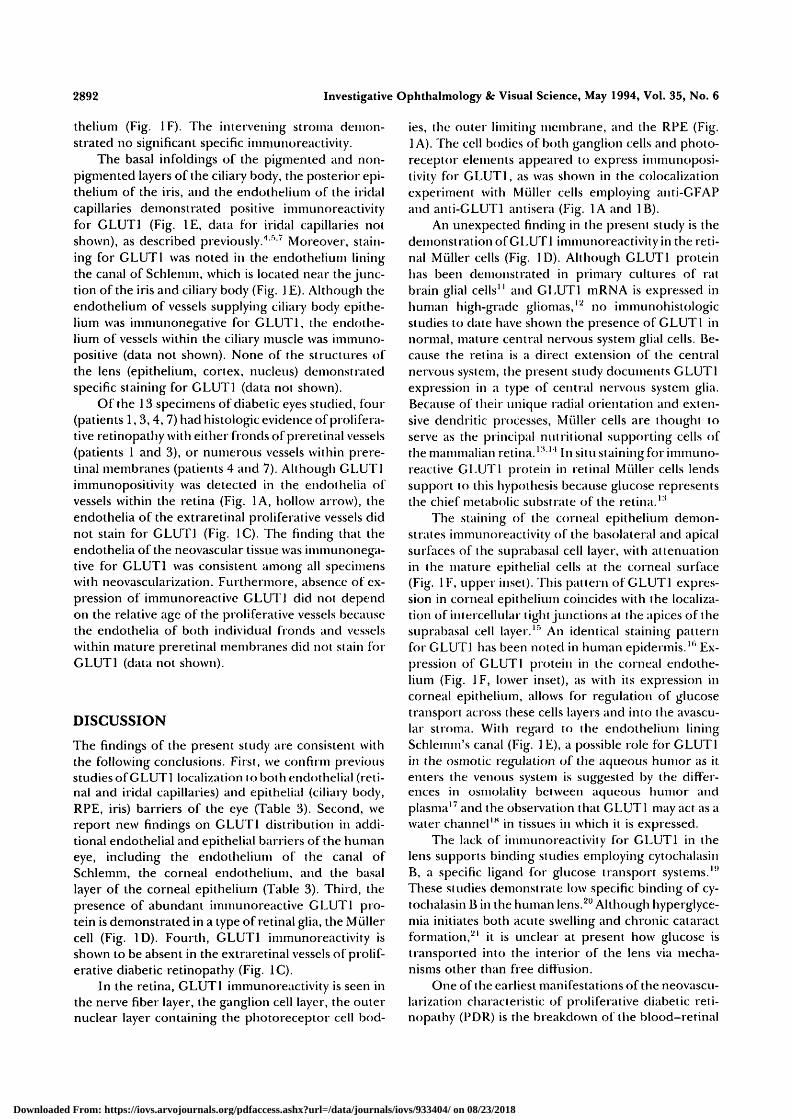
TABLE 2. Available Patient Data on Diabetic Eye Specimens
Patient
1*
2
3*
4*
5
6
Sex
F
M
F
M
F
M
Age(Years)
42
76
42
48
36
59
DM(Years)
24
22
Several
7
17
Several
OphthalmicProcedure
PRP, Vilrect.
PRP, Vitrect.
IN A
lilnucleation
Vitrect., Knucleaiion
Enucleation
Cause of Death
Pulmonary embolus
Pneumonia
Facial cancer
Surgical specimen
Surgical specimen
Surgical specimen
Other Conditions
ESRD, CAD, PVD
Alzheimer's disease CRF
NVG
NVG, HTN, DN
INA
Clinical data were available on (> of 1U diabetic specimens, !•$ of the (5 with histologic evidence of proliferative diabetic retinopathy. Ophlhalproc, opluhaliiiologic procedures performed on eye specimen studied; PRP, panretiual pholocoagulalion; Vitrect. vilreciomy (indicatedby *). CAD, coronary artery disease; CRF, chronic renal failure; DN, diabetic nephropathy; KSRD, end-stage renal disease; NVG, neovas-cular glaucoma; INA, information not available.
Downloaded From: https://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933404/ on 08/23/2018

GLUT1 Expression in the Human Eye 2889
antisera in dilutions from 1:500 to 1:2000 in 50 mMTris-buffered saline (TBS), pH 8.0. Control slideswere stained with identical dilutions of preiininuneserum (for anti-hGT, anti-GFAP) or with anti-CT anti-serum that had been preabsorbed with synthetic: pep-tide. After incubation with the primary antisera, three5-minute washes in TBS were performed, followed byincubation at room temperature for SO minutes withbiotinylated goat anti-rabbit fgG (Vector Laborato-ries, Burlingame, CA) at a concentration of 50 ^g/111'in TBS. Three 5-minute washes in TBS were repeated,followed by treatment with an avidin-biotin-peroxi-dase complex (ABC Elite, Vector) for 30 minutes.After a washing procedure identical to those describedabove, the eye sections were developed for 15 to 20minutes at 37°C in peroxidase substrate, which con-sisted of 0.02 M sodium acetate (pH 5.1), 0.1 7 mg/ml3-amino-9-ethylcarbazole (AL'C, Sigma, St. Louis,MO), 10% dimethyl sulfoxide, and 0.20% H2O2. Theslides were briefly counterstaincd with Mayer's hema-toxylin (Sigma), mounted with glycerol, and viewedunder light microscopy.
Semiquantitative analysis of the intensity of thereaction product seen in the various eye structuresstudies was performed. The intensity of GLUT1 immu-noslaining of the various structures was compared tothe staining intensity of structures known to expressGLUT1. The reference structures employed in thisscoring system were: 1 + = the human erythrocyte, 2+= the cytoplasm of the nonpigmented layer of the cili-ary body, and 3+ = the basolateral surface of the non-pigmented layer of the ciliary body. The grading sys-tem allowed for a convenieni internal reference foreach slide in which the reference structures were pres-ent. An individual score was assigned to each eyestructure studied, which ranged from 0 (total absenceof staining) to 3+ (most intensely stained). The accu-racy of this scoring system was tested by an indepen-dent review of the slides by an observer who wasmasked to the previous staining intensity scores, theuse of anti-GLUTf or preimmune antisera, and thepresence or absence of diabetes in the patients fromwhom the specimens were obtained. In addition, amasked comparison was made between the stainingpatterns of adjacent sections of eye specimens stainedwith either anti-hGT or anti-CT antisera or with therespective control antisera (preimmune antiserum oranti-CT antisera preabsorbed with CT peptide, respec-tively). Between 8 and 12 slides per specimen werestudied.
RESULTS
The clinical data for all patients without diabetes andfor all patients with diabetes for whom data were avail-able (6 of 13) are given in Tables 1 and 2.A list of the
eye structures studied in both diabetic and nondia-betic specimens, with the respective relative intensitystaining scores, is presented in Table 3. The relativescores made by the investigators and a masked ob-server were virtually identical for all structures listed.The staining patterns were consistent among all speci-mens examined, and slight variations in staining couldbe attributed to pre-embedding necrosis or artifact.With the notable exception of the staining pattern ofthe preretinal vessels of the diabetic eyes with prolifer-ative diabetic retinopathy (PDR, discussed below), the
TABLE 3. GLUT1 Glucose TransporterImmunoreactivity in the Human Diabeticand Nondiabetic EyeStructure
VesselsRetinal enclotheliuinPreretinal tieovascular endothelium*Iriclal enclolheliumChoroid enclotheliuinCiliary enclotheliuin
RetinaInner limiting membrane*Nerve liber layer*Miiller cells*Ganglion tell bodies*Cell bodies of rods and tones*Outer limiting membrane*Outer segments, rods and tones*Retinal pigmented epithelium (a, b)
Ciliary bodyI'iginentecl epitheliumNonpigmented epithelium
Score
2-3+02-3+00
03 +3+1-2+2+2-3+03+
1-2+3+ (R)
Canal of SchlemmI:'.ii(lol helium*
IrisPigmenled posterior epitheliumAnterior epithelium
CorneaEpithelium (a, b)*Knclolhelium (a, b)*
LensKpithelium*Cortex and nucleus*
Human erythrocyte
3+
0-1 +0
1-3+ (var.)2-3+
00
l+(R)
* Nt:w findings of this study.Semi-quantitative scoring of staining intensity of iinmunoperoxi-dasi' reaction product from iininunocyiochc-mical staining of fi-^msections of human diabetic and nondiabetic eyes with polyclonalantiserum directed against purified human eryllirocyte glucosetransporter. The scoring .system was based on (he relative intensityof staining of eye structures in comparison to reference structures(R) in which GLUT1 expression is well documented.1 r<7 The grad-ing scale rellects total absence of staining (0) to most intensestaining (!i+). The reproducibility of the scale was verified bymasked comparison, a, apical membrane; I), basolateral membrane.
Downloaded From: https://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933404/ on 08/23/2018

2890 Investigative Ophthalmology 8c Visual Science, May 1994, Vol. 35, No. 6
distribution and intensity of GLUTl immunoreactivityin various eye structures were virtually identical be-tween tbe nondiabetic and diabetic specimens. Thisfinding was confirmed by masked observation. Fur-thermore, no significant difference could be detectedon masked comparison between specimens stainedwith either anti-hGT or anti-CT GLUTl antisera.
In the retina, intense specific immunostaining forGLUTl (2 to 3+) was seen in the nerve fiber layer, theMiiller cells, and the outer limiting membrane, whichseparates the photoreceptor cell bodies from the moredistal inner and outer segments (Fig. 1A; individualretinal layers are identified in Fig. IB, right panel).Less intense (2+) but specific staining was also ob-served in the ganglion cell layer and in the cell bodiesof the rods and cones (Fig. 1A). In confirmation ofprevious findings,45 the endothelia of retinal capillar-ies and the apical and basolateral surfaces of the reti-nal pigment epithelium (RPE) stained intensely (2 to3+) for GLUTl (Fig. 1A); in contrast, the endotheliaof the choriocapillaris did not stain (Fig. 1A, large ar-rowhead). The inner and outer segments of the pho-toreceptor cells (Fig. 1A, small arrow), as well as theinner limiting membrane (Fig. 1 A, large arrow) did notshow GLUTl immunoreactivity. Sections treated witheither preimmune serum or anti-CT antiserum preab-sorbed with CT synthetic peptide showed an absenceof staining in all structures of the eye (Fig. IB, rightpanel).
Miiller cells, a type of retinal glia, are orientedradially and possess cytoplasmic processes that spanthe retina between the inner and outer limiting mem-
branes. On the basis of their unique morphology andorientation, the Muller cells could be distinguishedwithin the immunopositive retina. These cells stainedintensely for GLUTl in both diabetic and nondiabeticeyes (Fig. ID).
Muller cells have numerous dendritic processesthat contact and encircle various structures within theretina, including the neuronal axons of the nerve fiberlayer, retinal vessels, and the cell bodies of the gan-glion and photoreceptor cells.10 Because of thesecharacteristics, it was difficult to determine whetherthe axons of the nerve fiber layer and the ganglion andphotoreceptor cell bodies themselves stained forGLUTl, or whether the immunoreactivity in thesestructures was due to overlying or surrounding retinalglial cell dendritic processes. To clarify this issue, adja-cent sections of nondiabetic retina were stained withanti-GLUTl (Fig. 1A, right panel) and anti-GFAP an-tisera (Fig. 1B, left panel). As can be seen in Figures 1Aand IB, although Muller cells and ganglion and pho-toreceptor cell bodies stained for GLUTl, immunore-activity for GFAP could be clearly detected only in theradial extensions of the Muller cells and in the nervefiber layer. This differential staining pattern sup-ported initial impressions that the cell bodies of theganglion cells and photoreceptor elements expressedGLUTl. It could not be determined, however,whether or not the staining of the axons in the nervefiber layer was due to staining of glial elements.
In the cornea, specific staining for GLUTl wasalso observed in the apical and basolateral surfaces ofthe suprabasal epithelial layer and of the corneal endo-
FIGURE 1. Immunocytochemical staining of human eyes with anti-GLUTl or anti-GFAP anti-sera. (A) GLUTl immunoreactivity in cross-section of nondiabetic whole retina (lefi panel) orinner layers of retina (right panel). Large arrow, inner limiting membrane; small arrow, distalsegments of photoreceptor cells; hollow arrow, retinal capillary endothelium; large arrow-head, choriocapillaris with GLUTl positive erylhrocytes. Specific retinal layers are identifiedin (B), right panel. Bar in left panel, 30 /im; bar in right panel, 20 /urn. (B), left panel. GFAPimmunosiaining of eye section adjacent to that shown in (A), right panel. Bar, 20 nm. Rightpanel, control slide of nondiabetic retina stained with preimmune serum: (1) inner limitingmembrane; (2) nerve fiber layer; (3) ganglion cell layer; (4) inner plexiform layer; (5) bipolarcell layer; (6) outer plexiform layer; (7) layer of the photorecepior cell bodies; (8) externallimiting membrane; (9) retinal pigment epithelium, v, vitreous; c, choroid. Bar, 30 fim. (C)Left panel, GLUTl iminunostaining of diabetic retina with proliferative retinopathy contain-ing extrarelinal vessels. Erylhrocytes within the lumen of the extraretinal vessels stain posi-tively for GLUTl. Right panel, control slide from same eye stained with preimmune serum.Bar, 30/im. (D) GLUTl immunostaining of slightly disrupted nondiabetic retina demonstrat-ing positive staining of Muller cells, v, vitreous. Bar, 20 /zni. (E) GLUT! immunostaining ofnondiabetic eye showing canal of Schlemm (hollow arrow); ciliary body (Cb) with staining ofbasilar infoldings of nonpigmented cell layer (small arrows); and iris (I). AC, anteriorchamber. Bar, 125 /xm. Inset, high-power magnification of endothclial lining of canal ofSchlemm. Bar, 20 /im. F. GLUTJ immunostaining of nondiabetic cornea. Right panel, low-power magnification. Large arrow, corneal epithelium; small arrow, corneal endothelium; S,stroina; AC, anterior chamber. Bar, 125 i/m. Insets, high-power magnification of cornealepithelium (upper) and endothelium (lower). Bar, 10 ixm.
Downloaded From: https://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933404/ on 08/23/2018

GLUTl Expression in the Human Eye
A $
2891
Downloaded From: https://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933404/ on 08/23/2018
2892 Investigative Ophthalmology & Visual Science, May 1994, Vol. 35, No. 6
thelium (Fig. 1F). The intervening stroma demon-strated no significant specific imniunoreaclivity.
The basal infoldings of the pigmented and non-pigmented layers of the ciliary body, the posterior epi-thelium of the iris, and the endothelium of the iridalcapillaries demonstrated positive immunoreactivityfor GLUT1 (Fig. IE, data for iridal capillaries notshown), as described previously.'1 '7 Moreover, stain-ing for GLUT1 was noted in the endothelium liningthe canal of Schlemm, which is located near the junc-tion of the iris and ciliary body (Fig. J E). Although theendothelium of vessels supplying ciliary body epithe-lium was immunonegative for GLUT1, the endothe-lium of vessels within the ciliary muscle was immuno-positive (data not shown). None of the structures ofthe lens (epithelium, cortex, nucleus) demonstratedspecific staining for GLUT1 (data not shown).
Of the 13 specimens of diabetic eyes studied, four(patients 1,3,4, 7) had histologic evidence of prolifera-tive retinopathy with either fronds of pi eretinal vessels(patients 1 and 3), or numerous vessels within prere-tinal membranes (patients 4 and 7). Although GLUT1immunopositivity was detected in the endothelia ofvessels within the retina (Fig. 1A, hollow arrow), theendothelia of the extraretinal proliferative vessels didnot stain for GLUT1 (Fig. 1C). The finding that theendothelia of the neovascular tissue was immunonega-tive for GLUT1 was consistent among all specimenswith neovascularization. Furthermore, absence of ex-pression of immunoreactivc GLUT! did not dependon the relative age of the proliferative vessels becausethe endothelia of both individual fronds and vesselswithin mature preretinal membranes did not stain forGLUT1 (data not shown).
DISCUSSION
The findings of the present study are consistent withthe following conclusions. First, we confirm previousstudies of GLUT1 localization tobothendothelial (reti-nal and iridal capillaries) and epithelial (ciliary body,RPE, iris) barriers of the eye (Table 3). Second, wereport new findings on GLUT1 distribution in addi-tional endothelial and epithelial barriers of the humaneye, including the endothelium of the canal ofSchlemm, the corneal endothelium, and the basallayer of the corneal epithelium (Table 3). Third, thepresence of abundant immunoreactive GLLJT1 pro-tein is demonstrated in a type of retinal glia, the Miillercell (Fig. ID). Fourth, GLUT1 immunoreactivity isshown to be absent in the extraretinal vessels of prolif-erative diabetic retinopathy (Fig. 1C).
In the retina, GLUT1 immunoreactivity is seen inthe nerve fiber layer, the ganglion cell layer, the outernuclear layer containing the photoreceptor cell bod-
ies, the outer limiting membrane, and the RPE (Fig.1 A). The cell bodies of both ganglion cells and photo-receptor elements appeared to express immunoposi-tivity for GLUT1, as was shown in the colocalizationexperiment with Muller cells employing anti-GFAPand anti-GLUTl antisera (Fig. 1A and IB).
An unexpected finding in the present study is thedemonstration of GLUT1 immunoreactivity in the reti-nal Muller cells (Fig. ID). Although GLUT1 proteinhas been demonstrated in primary cultures of ratbrain glial cells" and GLUT1 mRNA is expressed inhuman high-grade gliomas,12 no immunohistologicstudies to date have shown the presence of GLUT 1 innormal, mature central nervous system glial cells. Be-cause the retina is a direct extension of the centralnervous system, the present study documents GLUT1expression in a type of central nervous system glia.Because of their unique radial orientation and exten-sive dendritic processes, Muller cells are thought toserve as the principal nutritional supporting cells ofthe mammalian retina.1 u ' In situ staining for immuno-reactive GLUT1 protein in retinal Muller cells lendssupport to this hypothesis because glucose representsthe chief metabolic substrate of the retina.1'
The staining of the corneal epithelium demon-strates immunoreactivity of the basolateral and apicalsurfaces of the suprabasal cell layer, with attenuationin the mature epithelial cells at the corneal surface(Fig. IF, upper inset). This pattern of GLUT 1 expres-sion in corneal epithelium coincides with the localiza-tion of intercellular tight junctions at the apices of thesuprabasal cell layer.1* An identical staining patternfor GLUT1 has been noted in human epidermis."1 Ex-pression of GLUT1 protein in the corneal endothe-lium (Fig. IF, lower inset), as with its expression incorneal epithelium, allows for regulation of glucosetransport across these cells layers and into the avascu-lar stroma. With regard to the endothelium liningSchlemm's canal (Fig. 1 E), a possible role for GLUT1in the osmotic regulation of the aqueous humor as itenters the venous system is suggested by the differ-ences in osmolality between aqueous humor andplasma1' and the observation that GLUT1 may act as awater channel1" in tissues in which it is expressed.
The lack of iminunoreactivity for GLUT1 in thelens supports binding studies employing cytochalasinB, a specific ligand for glucose transport systems.11
These studies demonstrate low specific binding of cy-tochalasin B in the human lens.20 Although hyperglyce-mia initiates both acute swelling and chronic cataract.formation,21 it is unclear at present how glucose istransported into the interior of the lens via mecha-nisms other than free diffusion.
One of the earliest manifestations of the neovascu-larization characteristic of proliferative diabetic reti-nopathy (PDR) is the breakdown of the blood-retinal
Downloaded From: https://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933404/ on 08/23/2018
GLUT1 Expression in the Human Eye 2893
barrier (BRB), which is evidenced clinically by the leak-age of fluorescein into the vitreous during lluoresceinangiography.22 The BRB consists of two major compo-nents: the endothelial cells of the retinal capillaries(the inner BRB) and the cells of the retinal pigmentepithelium (the outer BRB), the barrier functions ofwhich are conferred by tight junctions (zonulae occlu-dens) between adjacent endothelial or epithelialcells.2' Although not settled conclusively, it appearsthat the compromise of BRB integrity associated withPDR occurs principally at the level of the retinal capil-lary endothelial cells.2'1
In the present study, we demonstrate the absenceof immunoreactive GLUT1 protein in the neovasculartissue characterizing PDR (Fig. 1C). Previous investi-gators have suggested that GLUT1 glucose trans-porter expression is a marker of tissues that serve abarrier function.'11' The results of the present studysuggest a corollary to this hypothesis: In tissues inwhich there is a pathologic loss of barrier function,such as the endothelia of the neovascular tissue ofPDR, there is an associated absence of immunoreac-tive GLUT.1 transporter expression. The observationmade in these studies that immunoreactive GLUT1transporter expression is absent in both preretinalneovascular fronds and in more mature preretinal fi-brovascular membranes suggests that absence ofGLUT1 expression is not characteristic of neovasculartissue per se but is associated with the permanent lossof the barrier properties seen in the pathologic vesselsof PDR. At present, it is unclear whether the absenceof GLUT1 expression is restricted to the proliferatevevessels themselves or is characteristic of the retinal vas-cular changes of nonproliferative diabetic retinopathyas well. Further investigations of GLLJT1 transporterexpression in early diabetic retinopathy may clarifythis issue.
Key Words
GLUT1, glucose transporter, rciinopathy, blood-retinalbarrier, Miiller cells, glia, neovascularization
Acknowledgments
The authors (hank Dr. Morton E. Smith for generously pro-viding diabetic eye specimens, Dr. Ana Maria Zaragosa andMs. Jing Yang for technical advice, Ms. Kathy Ryan for assis-tance in gathering clinical data, Drs. Ruben J. Roado andUlrich Bickel for helpful discussions, and Ms. Sherri Chienand Ms. Sara Morimoto for skillful preparation of the manu-script.
References
1. Mueckler M. Family of glucose transporter genes: Im-plications for glucose homeostasis and diabetes. Dia-betes. 1990; 39:6-11.
2. Mueckler M, Caruso C, Baldwin SA, et al. Sequenceand structure of a human glucose transporter. Science.1985:229:941-945.
3. Pardridge VVM, Boado RJ, Farrell CR. Brain-type glu-cose transporter (GLUT1) is selectively localized tothe blood-brain barrier. Studies with quantitativeWestern blotting and in situ hybridization. J liiolChem. 1990; 265:18035-18040.
4. Harik SI, Kalaria RN, Whitney PM, et al. Glucosetransporters are abundant in cells with 'occluding'junctions at the blood-eye barriers. Proc Natl Acrid SciUSA. 1990:87:4261-4264.
5. Takata K, Kasahara T, Kasahara M, Ezaki O, HiranoH. Erythrocyie/HcpG2-type glucose transporter isconcentrated in cells of blood-tissue barriers. BiochemBiophys lies Commun. 1990; 173:67-73.
6. Cunha-Vaz, JG. Studies on the pathophysiology of dia-betic retinopathy: The blood-retinal barrier in dia-betes. Diabetes. 1983;32(suppl):20-27.
7. Takata K, Kasahara T, Kasahara M, Ezaki O, HiranoH. Ultracytochemical localization of the erythrocyle/HepG2-type glucose transporter (GLUT1) in the cili-ary body and iris of the rat eye. Invest Ophthahnol VisSci. 1991;32:1659-1666.
8. Hsu S-C, Molday RS. Glucolylic enzymes and aGLUT1 glucose transporter in the outer segments ofrod and cone photoreceptor cells. J liiol Chem.1991;266:21745-21752.
9. Pardridge VVM, Triguero D, Farrell CR. Downrcgula-lion of blood—brain barrier glucose iransporier in ex-perimental diabetes. Diabetes. 1990;39:1040-1044.
10. Hollander H, Makarov F, Dreher Z, van Dricl D,Chan-Ling T, Stone J. Structure of the microglia of(he retina: Sharing and division of labour between as-trocytes and Miiller cells. J Comp Neural.1991;313:587-603.
11. Walker PS, Donovan JA, Van Ness BG, Fellows RE,Pessin JE. Glucose-dependent regulation of glucosetransport activity, protein, and mRNA in primary cul-tures of rat brain glial cells. J liiol Chem.1988; 263:15594-15601.
12. Nishioka T, Oda Y, Seino Y, et al. Distribution of theglucose transporter in human brain tumors. CancerRes. 1992; 52:3972-3979.
13. Kuwabara T, Cogan DG. Retinal glycogen. ArchOphthal. 1961:66:680-688.
14. Poitry-Yamate CL, Tsacopoulos M. Glucose metabo-lism in freshly isolated Miiller glial cells from a mam-malian retina. J Comp Neurol. 1992;320:257-266.
15. Maurice DM. The cornea and sclera. In: Davson H,ed. The Eye. 3rd ed. Orlando: Academic Press; 1984:9.
16. Gherzi R, Melioli G, De Luca M, et al. 'HepG2/ery-throid/brain' type glucose transporter (GLUT1) ishighly expressed in human epidermis: Keratinocytedifferentiation affects GLUT1 levels in reconstitutedepidermis. / Cell Physiol. 1992; 150:463-474.
17. Cole DF. Ocular fluids. In: Davson H, ed. The Eye. 3rded. Orlando: Academic Press; 1984:299.
18. FischbargJ, Kuang K, Vera JC, et al. Glucose trans-porters serve as water channels. Proc Natl Acad SciUSA. 1990:87:3244-3247.
Downloaded From: https://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933404/ on 08/23/2018

2894 Investigative Ophthalmology 8c Visual Science, May 1994, Vol. 35, No. 6
19. Wardzala LJ, Cushman SW, Salans LB. Mechanism ofinsulin action on glucose transport in the isolated ratadipose cell: Enhancement of the number of func-tional transport systems. / Biol Cham. 1 978; 253:8002-8005.
20. Kaulen P, Kahle G, Keller K, WollensakJ. Autoradio-graphic mapping of the glucose transporter with cyto-chalasin B in the mammalian eye. Invest Ophthalmol VisSci. 1991:32:1903-1911.
21. Kinosha JH. Mechanisms initiating cataract forma-tion. Invest Ophthalmol. 1974; 13:713-724.
22. Cunha-Vaz J, Faria de Abreu JR, Campos AJ, FigoGM. Early breakdown of the blood-retinal barrier indiabetes. Br J Ophlhalmol. 1975;59:649-656.
23. Cunha-VazJG, Shakib M, Aston N. Studies on the per-meability of the blood-retinal barrier: I: On the exis-tence, development and site of a blood-retinalbarrier. Br J Ophthalmol. 1966;50:441-453.
24. Vinores SA, Gadegbeku C, Campochiaro PA, GreenWR. Immunohistochemical localization of blood-reti-nal barrier breakdown in human diabetics. Am JPathol. 1989; 134:231-235.
Downloaded From: https://iovs.arvojournals.org/pdfaccess.ashx?url=/data/journals/iovs/933404/ on 08/23/2018