the garba tulla htsp project: increasing contraceptive uptake in northern kenya
TRANSCRIPT

Sub-awardee logo here
Devina Shah, MPH Jan 28th 2016
www.worldvision.org/our-impact/health
The Garba Tulla HTSP Project: Increasing Contraceptive Uptake in Northern Kenya
International Conference on Family Planning Nusa Dua, Indonesia

Sub-awardee logo here
Overview
• Background/Context • Program Interventions • Early results/Lessons
Learned

Sub-awardee logo here
Sub-awardee logo here
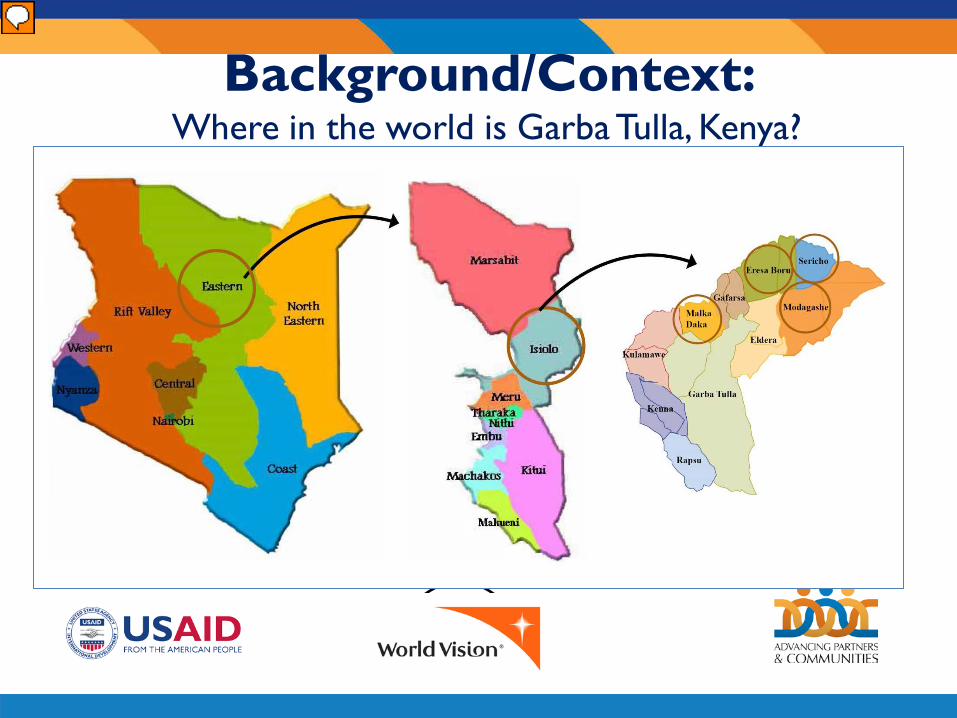
Background/Context: Where in the world is Garba Tulla, Kenya?
Sub-awardee logo here
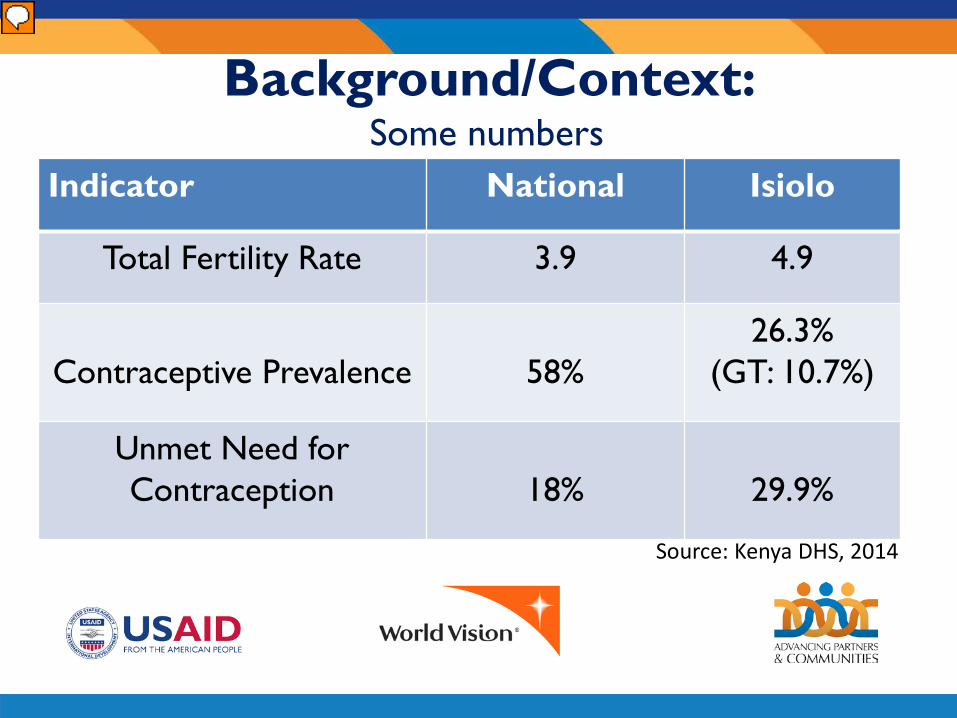
Background/Context: Some numbers
Indicator National Isiolo
Total Fertility Rate 3.9 4.9
Contraceptive Prevalence
58%
26.3% (GT: 10.7%)
Unmet Need for Contraception
18%
29.9%
Source: Kenya DHS, 2014

Sub-awardee logo here
Background/Context: What does Garba Tulla look like?

Sub-awardee logo here
Background/Context: What does Garba Tulla look like?
Programmatic Activities Focused on all Persons of Reproductive Age
Type Age Range Number of Beneficiaries
WRA 15-49 11,641
Married WRA 15-49 10,791
Men 15-49 21,990
Total Number of Beneficiaries 43,118

Sub-awardee logo here
Background/Context: Starting Strong Project
Starting Strong (2012-2017) is a five-year, $2 million Maternal and Child Health and Nutrition (MCHN) initiative privately funded by WV Canada.
• Improved uptake of MCHN services by mothers and their children
• Improved nutrition and WASH practices at community level
• Improved environment for MCHN services.
Sub-awardee logo here

Sub-awardee logo here
Sub-awardee logo here
Points of integration to increase utilization for HTSP/FP
• Antenatal care: 73% of women get tetanus toxoid coverage during the fourth antenatal care visit
• Immunization: High immunization coverage (72.6 percent) for fully immunized children under 2

Sub-awardee logo here
SO 1: Capacity Building of CHEWs and CHVs

Sub-awardee logo here

Sub-awardee logo here
Background/Context: What does Garba Tulla look like?

Sub-awardee logo here
SO 2: Community Mobilization: Male engagement

Sub-awardee logo here
SO 2: Community Mobilization: Faith Leaders

Sub-awardee logo here
SO 2: Community Mobilization: WRA

Sub-awardee logo here
Results
0
100
200
300
400
500
600
Capacity Building, Male-FPcounseling/services for CHWs
Capacity Building, Male-FPcounseling/services for other providers
working in health facilities
Cacacity Building, Female-FPcounseling/services for CHWs
Capacity Building, Female-FPcounseling/services for other providers
working in health facilities
Number of community health workers (CHWs) and/or other health providers trained or supported, disaggregated by gender

Sub-awardee logo here
Results
0
200
400
600
800
1000
1200
1400
Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15
Number of community members reached with family planning messages by type of provider
By CHEW (Other service providers in health facilities) By CHVs (Community health workers (CHWs)

Sub-awardee logo here
Results
0
500
1000
1500
2000
2500
3000
3500
4000
4500
10-14 15-19 20-24 25+March 2014 - Dec 2015
Number of clients of reproductive age receiving FP counseling, disaggregated by gender, age
Male Female

Sub-awardee logo here
Successes
0
100
200
300
400
500
600
700
Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15
# of clients receiving FP information integrated into MNCH services at the same location and time, disaggregated by sex
Male Female

Sub-awardee logo here
Successes
0
50
100
150
200
250
300
350
400
450
500
Jul-14 Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15
# of clients receiving FP services integrated into MNCH services at the same location and time, disaggregated by sex
Male Female

Sub-awardee logo here
Successes
2870
0
1867
184
3
0
45
1098
1
605
0
514
724
0 500 1000 1500 2000 2500 3000
Male condom, Male
Male Sterilization, Male
SDM, Male
Emergency Contraception, Female
Female condom, Female
Female Sterilization
Implants, Female
Injectables, Female
IUD, Female
Female Lactational Amenorrhea
Male condom, Female
Oral Contraceptive Pills, Female
Standard Days Method (SDM), Female
# of current users, disaggregated by sex and method
# of current users by gender and method

Sub-awardee logo here
Successes
18 89
376
179
451
757
0
200
400
600
800
1000
1200
Sep-14 Dec-14 Mar-16 Jun-16 Sep-16 Dec,2015
Male condom, Male Male Sterilization, Male SDM, Male
Emergency Contraception, Female Female condom, Female Female Sterilization
Implants, Female Injectables, Female IUD, Female
Female Lactational Amenorrhea Oral Contraceptive Pills, Female Standard Days Method (SDM), Female
# of current users over time, disaggregated by sex and method

Sub-awardee logo here
Challenges
• Hard to reach area: very tough terrain, scattered habitation, very low levels of literacy
• Socio-cultural factors: early child marriage, multiple marriages, religious factors,

Sub-awardee logo here
Lessons Learned • The pivotal importance of men in FP programs
In traditional societies, where men are the gate-keepers who control all access to resources, the initial focus of family planning programs must be on men – chiefs, elders, imams and fathers
• Increasing Contraceptive Use in conservative rural societies takes time
In cultures with no tradition of contraceptive use, the initial step succeeds when it focuses on culturally compatible methods like LAM and SDM. Introducing LARC and LAPM later in the program is much more effective, once communities are comfortable with and have reduced myths/misconceptions about hormonal methods.
• Socio-cultural factors like early child marriage must be taken into consideration
Need to work on issues underlying child marriage through social norm-change interventions as well as economic interventions

Sub-awardee logo here
Acknowledgements Project Staff: • Cynthia Nyakwama – WV Kenya • Shano Guyo – WV Kenya • Adrienne Allison – WVUS
We thank: • USAID • Advancing Partners & Communities • Ministry of Health - GOK

Sub-awardee logo here
Thank you!
Asante!
Shukriya!
Terima Kasih!
Dhonyawad!