the anxiety disorders a patient-centered, evidence-based diagnostic and treatment process 1 kendall...
TRANSCRIPT

The Anxiety DisordersA Patient-Centered, Evidence-Based Diagnostic and Treatment Process1Kendall L. Stewart, MD, MBA, DLFAPASeptember 20, 2013
1 This is problem-oriented learning with numerous links to supporting resource material.

Why should you learn about these disorders?
• They are the most common mental disorders.• These disorders are frequently missed, ignored or mistreated.• These disorders cause substantial distress and impairment.1
• Patients with these disorders over-utilize other medical services.2,3
• Many physicians still lump these disorders and minimize them as “nerves.”
• These disorders can usually be effectively treated.
1 Significant distress and/or impairment are required to make a psychiatric diagnosis.2 Anxiety and depression are frequently masked by physical complaints.3 One of my elderly patients never talked about her anxiety, only the “burning in my head.”

What are some of the physical manifestations of anxiety?
• Diarrhea• Dizziness or light-
headedness• Hyperhidrosis• Hyperreflexia• Hypertension• Palpitations• Pupillary mydriasis
• Restlessness• Syncope• Tachycardia• Tingling in the extremities• Tremors1,2,3
• Upset stomach (“butterflies”)
• Urinary frequency, hesitancy, urgency
1 Most tremors are worsened by anxiety.2 I admitted a man from the ED who developed a significant conduction disturbance.3 I unexpectedly experienced panic when undergoing MR imaging.
What are some of the mental manifestations of anxiety?
• Apprehension• Vigilance • Scanning• Shame• Confusion• Distortion of perception• Decreased concentration• Poor recall• Impaired association• Selective inattention• False assumption1,2
1 Anxious patients always assume the worst.2 One of my patients noted, “You don’t look so good.”

What clinical algorithm1,2 will assist you in making a correct anxiety diagnosis?
“Normal”Anxiety
Anxiety
AnxietyDisorders
Anxiety 2o toGen Med Cond
Substance-InducedAnxiety
Anxiety AssocWith Another
Mental Disorder
Etc.
Gen Anxiety Disorder
Etc. Etc. Etc.
PTSD
OCD
Social Anxiety Disorder
Specific Phobia
Agoraphobia
Panic Disorder
Adjustment Disorders Hypoglycemia
Hypothyroidism
CHF
Pulmonary Embolism
COPD
Caffeine
Alcohol
Stimulants
Anesthetics
Sedatives
Mood Disorder
Cognitive Disorder
Dissociative Disorder
Etc.
1 These categories form an excellent conceptual algorithm for evaluating psychiatric symptoms in clinical practice. 2Always remember to ask about caffeine.

What is the difference between normal and pathologic anxiety?
• It is often impossible to tell at the time.• Consider whether the anxiety or fear promotes adaptation
or causes impairment.• Consider the trigger, the duration and the degree of
impairment.• Whether a given distress is judged normal or pathologic
depends on one’s resources, psychological defenses, and coping mechanisms.1,2
• “Is this more than the usual ups and downs of life?” will often point the physician in the right direction.
1 Strong emotion of any sort impairs your ability to think clearly and act rationally.2 One of my patients came out of the restroom to find the atrium door locked. The sign on my door mayhave discouraged potential rescuers. All she needed to do was turn the deadbolt and walk out.

What disorders are included in the Anxiety Disorders category?
• Separation Anxiety Disorder• Selective Mutism• Specific Phobia• Social Anxiety Disorder (Social Phobia)• Panic Disorder• Panic Attack Specifier (not a diagnosis)• Agoraphobia• Generalized Anxiety Disorder• Substance/Medication-Induced Anxiety Disorder• Anxiety Disorder Due to Another Medical Condition • Other Specified Anxiety Disorder• Unspecified Anxiety Disorder

What disorders are included in the Obsessive-Compulsive category?
• Obsessive-Compulsive Disorder• Body Dysmorphic Disorder• Hoarding Disorder• Trichotillomania (Hair-Pulling Disorder)• Excoriation (Skin-Picking) Disorder• Substance/Medication-Induced Obsessive-Compulsive
and Related Disorder• Other Specified Obsessive-Compulsive and Related
Disorder• Unspecified Obsessive-Compulsive and Related
Disorder

What disorders are included in the Trauma- and Stressor-Related category?1,2
• Reactive Attachment Disorder• Disinhibited Social Engagement Disorder• Posttraumatic Stress Disorder• Acute Stress Disorder• Adjustment Disorders• Other Specified Trauma- and Stressor-Related
Disorder• Unspecified Trauma- and Stressor-Related
Disorder
1 A number of us are concerned about diagnosis inflation.2If you would like to read more about this concern, read Saving Normal by Allen Frances.
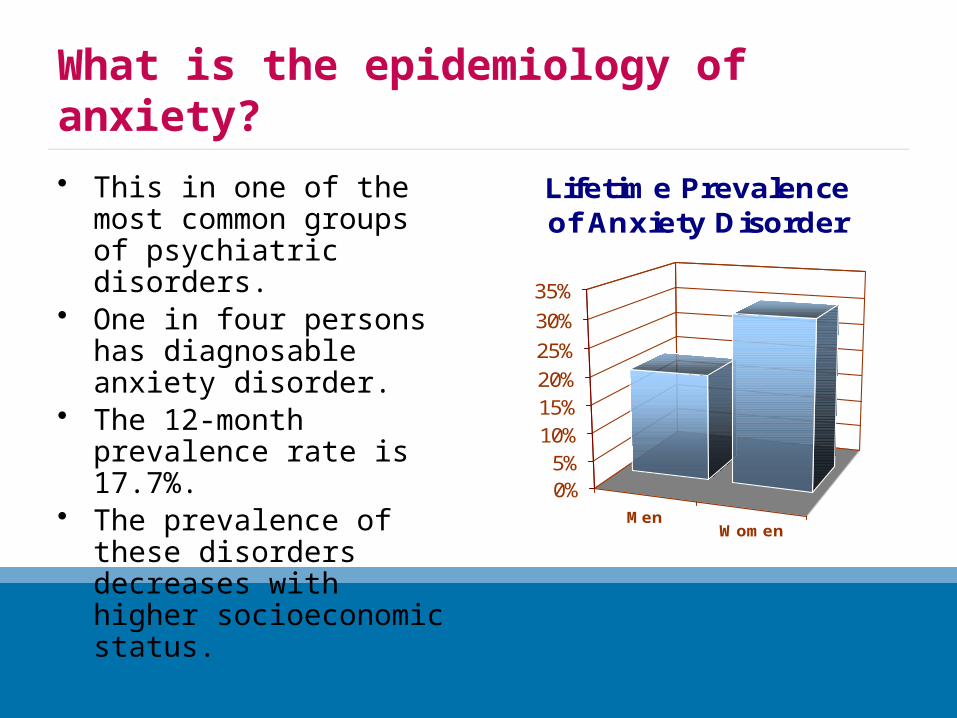
What is the epidemiology of anxiety?
• This in one of the most common groups of psychiatric disorders.
• One in four persons has diagnosable anxiety disorder.
• The 12-month prevalence rate is 17.7%.
• The prevalence of these disorders decreases with higher socioeconomic status.
MenWomen
0%5%10%15%20%25%
30%
35%
Lifetime Prevalence of Anxiety Disorder

What is the biological basis of anxiety?1,2
• Autonomic Nervous System– Increased sympathetic tone in anxious patients
• Neurotransmitters– Norepinephrine– Serotonin– γ- aminobutyric acid (GABA)
• Brain-Imaging Studies– Some patients with anxiety disorders have functional or anatomical changes.
• Genetic Studies– Some genetic component clearly contributes to the development of anxiety
disorders.
• Neuroanatomical Considerations– The locus ceruleus and raphe nuclei project to the limbic system.– The limbic system contains a high concentration of GABAA receptors.
– The frontal cerebral cortex is connected with the parahippocampal region, the cingulate gyrus, and the hypothalamus.
1 Kaplan & Sadock, 20082These observations are true for all of the anxiety disorders.

What about Anxiety Disorder Due to Another Medical Condition?
1 Most tremors are worsened by anxiety.2 I admitted a man from the ED who developed a significant conduction disturbance.3 I unexpectedly experienced panic when undergoing MR imaging.
• Anxiety commonly accompanies many different general medical conditions.
• These underlying conditions cause anxiety via the noradrenergic and perhaps the serotonergic systems.
• Paroxysmal bouts of anxiety should make clinicians suspicious.
• The clinical features can be identical to those of the primary anxiety disorders.
• Primary anxiety disorders generally have their onset before age 35.
• Anxiety symptoms may persist after the primary disorder is treated.
• The underlying disorder should be treated first, but the anxiety may need to be addressed separately.1,2
1 If you decide up front that the patient is a crock, this will set you up for some serious mistakes.2 One of my “crock” patients presented to the ED with the history of a dilated pupil.

What about Substance/Medication-Induced Anxiety Disorder?
1 Most tremors are worsened by anxiety.2 I admitted a man from the ED who developed a significant conduction disturbance.3 I unexpectedly experienced panic when undergoing MR imaging.
• This is a common consequence of recreational and prescription drug abuse.
• You must think about it and ask about it every time.
• Don’t forget about caffeine.• The associated clinical features may
vary with the substance involved.1,2
• Cognitive impairments in comprehension, calculation and memory usually disappear when the substance is discontinued.
• The differential diagnosis includes– Primary anxiety disorders– Anxiety due a general medical
condition (for which the patient may be receiving the implicated drug)
– Mood disorders– Personality disorders– Malingering
• Removal of the offending substance is the preferred treatment
1 People who take a lot of speed become overtly paranoid.2 I evaluated a patient at a MHC who was convinced that the FBI was landing UFOs in his backyard.

What about patients who present with mild mixed anxiety and depression?
1 Most tremors are worsened by anxiety.2 I admitted a man from the ED who developed a significant conduction disturbance.3 I unexpectedly experienced panic when undergoing MR imaging.
• These are patients that don’t meet full criteria for either a mood or an anxiety disorder.
• They are particularly common in primary care practices.
• On careful examination, they often are depressed; the accompanying anxiety is misleading.
• This controversial presentation is not a separate diagnosis.
• This combination of symptoms leads to considerable functional impairment.
• Up to 2/3 of depressed persons are also anxious and up to 9/10 of panic patients experience depression.
• If this emerges as a specific diagnosis, it may affect about 1% of the population.
• The serotonergic drugs are helpful for both the anxiety and depression.1,2,3
1 These “mixed syndromes” can be very challenging.2 When in doubt, treat for depression. It is very hard to get patients off benzodiazepines.3A number of these patients will report definite benefit from one of the SSRIs.

What treatment options are available?
1 Most tremors are worsened by anxiety.2 I admitted a man from the ED who developed a significant conduction disturbance.3 I unexpectedly experienced panic when undergoing MR imaging.
• Non-medication interventions• No treatment• Distractions• Sensory override strategies• Meditation• Progressive relaxation
exercises• Cognitive behavioral
therapy
• Medication• Antidepressants• Benzodiazepines• Atypical antipsychotics• Buspirone (Buspar)• Antihistamines
What practical guidelines should you follow when prescribing medication for anxiety?
1 Most tremors are worsened by anxiety.2 I admitted a man from the ED who developed a significant conduction disturbance.3 I unexpectedly experienced panic when undergoing MR imaging.
• Make the correct diagnosis first; the treatment differs.
• Fix the problem that is causing the anxiety if you can.
• Try every reasonable nonmedical intervention first unless the severity of the symptoms will not allow that.
• The SSRIs and SNRIs are currently considered the medications of first choice for most anxiety disorders.
• If you need to block panic attacks immediately, clonazepam (Klonopin) is the go-to drug.
• Use benzodiazepines for only a brief period of time before tapering—if possible.
• Encourage exposure and cognitive therapy from the start; pills are rarely the answer by themselves.
• Support your patients in their management of their chronic illnesses.
• Use the atypical antipsychotic medications and anticonvulsants for anxiety ONLY as a last resort and after a psychiatric consultation.

1 Most tremors are worsened by anxiety.2 I admitted a man from the ED who developed a significant conduction disturbance.3 I unexpectedly experienced panic when undergoing MR imaging.
What problems will you face when prescribing antidepressants?
Problem Solution
Your anxious patients may become even more anxious after starting the drug.
Lower the starting dosage, reassure them and counsel patience.
Your patients may complain of unpleasant side effects.
If possible, recommend persistence and completion of an adequate trial.
Your patients may need immediate blockage of panic attacks.
Don’t hesitate to add clonazepam (Klonopin) and taper it later.
Your patients may want to try the same drug a family member took with benefit.
Agree to try it. This is a very good idea.
Your patients may not want to take ANY medication long term.
The rare PRN use of benzodiazepines makes some sense. PRN SSRIs do not.

1 Most tremors are worsened by anxiety.2 I admitted a man from the ED who developed a significant conduction disturbance.3 I unexpectedly experienced panic when undergoing MR imaging.
What problems might you face when prescribing benzodiazepines?
Problem Solution
You may not be comfortable prescribing benzodiazepines at all.
Refer the patient to a more flexible, mature and experienced provider.
You may not feel comfortable prescribing benzodiazepines long-term.
Seek a consultation from a psychiatrist.
Your patient may insist that you prescribe when you don’t agree.
Refer to a colleague BEFORE anyone gets mad.
You may discover that your patient is abusing your medication.
Confront them respectfully, then taper and discontinue the medication.
You may need to taper the medication. Warn about relapse, rebound, withdrawal and taper slowly.
You may conclude that the benefits of long-term use outweigh the risks.
Document your unsuccessful attempts to taper and monitor carefully.

The Psychiatric InterviewA Patient-Centered, Evidence-Based Diagnostic and Treatment Process
• Review my laboratory data and other available records.
• Tell me what diagnoses you have made.• Reassure me.• Outline your recommended treatment
plan while making sure that I understand.• Repeatedly invite my clarifying questions.• Be patient with me.• Provide me with the appropriate
educational resources.• Invite me to call you with any additional
questions I may have.• Make a follow up appointment.• Communicate with my other physicians.
• Introduce yourself using AIDET1.• Sit down.• Make me comfortable by asking some
routine demographic questions.• Ask me to list all of my problems and
concerns.• Using my problem list as a guide, ask me
clarifying questions about my current illness(es).
• Using evidence-based diagnostic criteria, make accurate preliminary diagnoses.
• Ask about my past psychiatric history.• Ask about my family and social histories.• Clarify my pertinent medical history.• Perform an appropriate mental status
examination.
1Acknowledge the patient. Introduce yourself. Inform the patient about the Duration of tests or treatment. Explain what is going to happen next. Thank your patients for the opportunity to serve them.
How can you access the OU-HCOM psychiatry flash cards online?
• Go to Quizlet.• Create a free account.• When you receive a confirmatory email, click on the link
to activate your new account.• With your activated account open in another browser
window, click on this link to join the class.• You can download the free Quizlet app to your iPhone or
import these learning sets to the more robust Flashcards Deluxe app.
• Enjoy. I hope you find these cards helpful.• Please post your feedback or suggestions on the Quizlet
site.

Where can you learn more?• American Psychiatric Association,
Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, 2013• Sadock, B. J. and Sadock V. A.,
Concise Textbook of Clinical Psychiatry, Third Edition, 2008• Stern, et. al., Massachusetts General Hospital Comprehensive Clinical
Psychiatry, 2008. You can read this text online here.• Flaherty, AH, and Rost, NS, The Massachusetts General Hospital
Handbook of Neurology, 2011• Stead, L, Stead, SM and Kaufman, M, First Aid© for the Psychiatry Clerkship,
Third Edition, 2011• Klamen, D, and Pan, P, Psychiatry PreTest Self-Assessment and Review,
Thirteenth Edition, 2012• Blitzstein, Sean, Lange Q&A Psychiatry, 2011• Ratey, JJ, Spark: The Revolutionary New Science of Exercise and the Brain,
2008• Medina, John,
Brain Rules: 12 Principles for Surviving and Thriving at Home, Work and School, 2010
Where can you find evidence-based information about mental disorders?
• Explore the site maintained by the organization where evidence-based medicine began at McMaster University here.
• Sign up for the Medscape Best Evidence Newsletters in the specialties of your choice here.
• Subscribe to Evidence-Based Mental Health and search a database at the National Registry of Evidence-Based Programs and Practices maintained by the Substance Abuse and Mental Health Services Administration here.
• Explore a limited but useful database of mental health practices that have been "blessed" as evidence-based by various academic, administrative and advocacy groups collected by the Iowa Consortium for Mental Health here.
How can you contact me?
Kendall L. Stewart, MD, MBA, DLFAPAVPMA and Chief Medical OfficerSouthern Ohio Medical Center
Chairman & CEOThe SOMC Medical Care Foundation, Inc.
1805 27th StreetWaller Building
Suite B01Portsmouth, Ohio 45662
740.356.8153
[email protected] [email protected]
www.somc.orgwww.KendallLStewartMD.com

Are there other questions?1,2
Safety Quality Service Relationships Performance
1Learn more about Southern Ohio Medical Center.2Learn more about our Family Medicine and Emergency Medicine Residencies.
Justin Greenlee, DODirectorFamily Medicine Residency
Thomas Carter, DODirectorEmergency Medicine Residency