sunshine health tango plan long-term care (ltc) · objective 2 • overview of our long-term care...
TRANSCRIPT

1
Sunshine Health Tango Plan
Long-Term Care (LTC)
Objective
2
• Overview of our Long-Term Care (LTC) product.
• Discuss how services are accessed - Integrated Care Model.
• Discuss care coordination and case management.
• Discuss trainings for providers and staff.
• Define both behavioral management and behavioral health.
• Answer any questions and address concerns regarding Integrated
Care Model.

Long-Term Care (LTC)
Overview
3
Nassau
Sumter
Clay
Charlotte
Polk
Flagler
Hardee
DeSoto
St.Johns
Volusia
Orange
Okeechobee
Brevard
IndianRiver
Palm Beach
St.Lucie
Broward
Miami-Dade
Okaloosa Walton
Escambia
Wakulla
Madison
Franklin
Jackson
Calhoun
Hamilton
Lafayette
Dixie
Suwannee
Gilc
hrist
Citrus
Pasco
Hernando
Bra
dford
Marion
Hillsborough
Manatee
Sarasota
Duval
Putnam
Lake
Lee
Osceola
Monroe
Seminole
Collier
Highlands
Glades
Hendry
Martin
SantaRosa
Leon
Jeffer
son
Bay
Gulf
Holmes
Was
hingt
on
Liberty
Gadsden
Taylor
Levy
Col
um
bia
Alachua
Baker
Union
PinellasRegion 1
3/1/14
Region 3
3/1/14
Region 4
3/1/14
Region 5
2/1/14
Region 6
2/1/14
Region 7
8/1/13
Region 8
9/1/13
Region 9
9/1/13
Region 10
11/1/13
Region 11
12/1/13
Nassau
Sumter
Clay
Charlotte
Polk
Flagler
Hardee
DeSoto
St.Johns
Volusia
Orange
Okeechobee
Brevard
IndianRiver
Palm Beach
St.Lucie
Broward
Miami-Dade
Okaloosa Walton
Escambia
Wakulla
Madison
Franklin
Jackson
Calhoun
Hamilton
Lafayette
Dixie
Suwannee
Gilc
hrist
Citrus
Pasco
Hernando
Bra
dford
Marion
Hillsborough
Manatee
Sarasota
Duval
Putnam
Lake
Lee
Osceola
Monroe
Seminole
Collier
Highlands
Glades
Hendry
Martin
SantaRosa
Leon
Jeffer
son
Bay
Gulf
Holmes
Was
hingt
on
Liberty
Gadsden
Taylor
Levy
Col
um
bia
Alachua
Baker
Union
Pinellas
LTC Service
Area 1
LTC Service
Area 2
LTC Service
Area 3
LTC Service
Area 4
Orlando/
Pensacola
Jacksonville
Tampa
Sunrise

LTC Leadership
4
Regions 1 & 7
Roni Zaletel, Executive Director
Carolyn Smith, Dir., Case Mgmt.
Regions 3
Donna Melogy, Executive Director
Pam Bertwell, Dir., Case Mgmt.
Regions 9, 10, 11
Amie Fernandez, Executive Director
Mayra Infanzon, Dir., Case Mgmt.
Regions 5, 6, 8
Greg Abdouch, Executive Director
Erica Colon, Dir., Case Mgmt.
Pam VanKoevering, Mgr., Ops &
Enrollment
Kathy Rupp, Mgr., Provider Relations
Carey Merzlicker, Dir., Finance
Tracy Celebrado, Mgr., LTC Contracting
Denise O’Driscoll, Mgr., Claims
Dona Leith, Cenpatico Clinical Mgr.
Sunshine Health LTC Provider Services
Phone # 877-211-1999
David Wagner, VP of LTC

LTC Members
5
• Individuals 65 years of age or older who need a nursing facility
level of care.
• Individuals 18 years of age or older who are eligible for Medicaid
by reason of a disability and need a nursing facility level of care.
• Individuals who live in a nursing facility.
• Individuals enrolled in one of the following programs:
• Aged and disabled adult waiver
• Consumer-Directed Care Plus for individuals in the above
waiver
• Adult day health care waiver
• Assisted living waiver
• Channeling services for frail elders waiver
• Program of all-inclusive care for the elderly
• Nursing home diversion waiver

Who is on the team?
6
Integrated Care Team Members (IC T)
• Member
• Family / Natural Supports
• Medical Directors
• Integrated Leadership team
• Case Manager
• Program Coordinator / Specialist
• BH Coordinator
• Disease Management Health Coach
• Pharmacy Director
• Utilization Managers
• Member Connections Representative
• LTC Trainer & Behavior Management Specialist

Collaboration
7
Working together for the good of the enrollee.

8
The Sunshine Health case management model is based on
supporting our members in a holistic manner.
The model considers the member’s physical health and
behavioral health conditions and diagnoses as well as their
social, environmental, financial, cognitive, spiritual, cultural
and functional status.
Integrated Holistic Approach

9
Some members have both physical and behavioral health
conditions. The presence of these conditions may have an impact
on the member’s ability to access care and manage their conditions.
In many cases, both physical health and behavioral staff are
supporting the member. Ongoing and frequent dialog occurs
between the staff managing the member and with the member’s
treating providers.
Overview of Integrated Care

10
Coordinated physical health, mental health, and substance abuse
treatment to provide the best possible outcomes for our members.
Integrated Healthcare
11
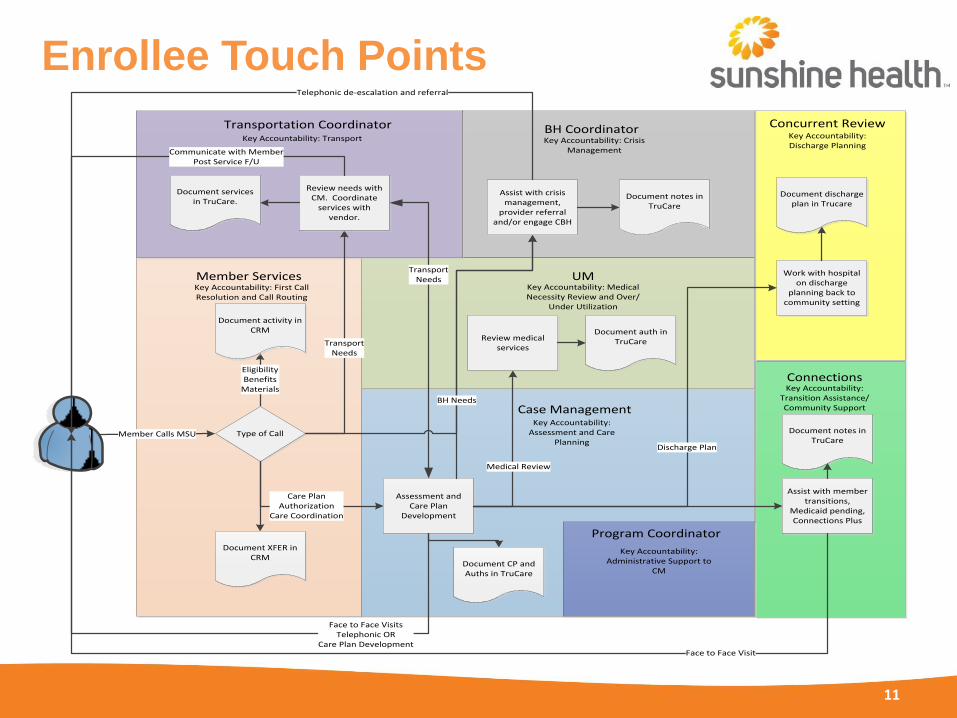
Enrollee Touch Points
Document CP and Auths in TruCare
Member Calls MSU
EligibilityBenefits
Materials
Care PlanAuthorization
Care Coordination
Type of Call
Document activity in CRM
Connections
Member Services
Transportation Coordinator BH CoordinatorKey Accountability: Transport Key Accountability: Crisis
Management
Key Accountability: Transition Assistance/Community Support
Key Accountability: First Call Resolution and Call Routing
Document services in TruCare.
TransportNeeds
Review needs with CM. Coordinate
services with vendor.
Assessment and Care Plan
Development
TransportNeeds
Communicate with MemberPost Service F/U
Assist with crisis management,
provider referral and/or engage CBH
Review medical services
Assist with member transitions,
Medicaid pending, Connections Plus
UMKey Accountability: Medical Necessity Review and Over/
Under Utilization
Document notes in TruCare
Concurrent ReviewKey Accountability: Discharge Planning
Work with hospital on discharge
planning back to community setting
Document discharge plan in Trucare
Discharge Plan
Medical Review
Key Accountability: Assessment and Care
Planning
Case Management
Document XFER in CRM
Document auth in TruCare
Face to Face Visit
Face to Face VisitsTelephonic OR
Care Plan Development
Document notes in TruCare
Telephonic de-escalation and referral
BH Needs
Key Accountability: Administrative Support to
CM
Program Coordinator

12
Case Management
What to expect?
• Case Manager (CM) will contact facility to notify them of assigned
members – Administrator, Director of Nursing, Social Worker, and
Business Office Manager are potential contacts for the CM’s.
• CM will contact member’s responsible party if necessary to review new
enrollee handbook, member benefits, required forms, etc.
• Consent from member’s responsible party is not required to complete
member needs assessment and the CM will proceed in order to meet
ACHA requirements and to complete service authorizations.
• Based on facility membership only 1-2 CM’s will be assigned for
continuity of care and consistent communication.

13
Case Management What to expect?
• CM will review meet with the member and review the medical record
including the MDS, MAR’s, Care Plan, Progress Notes, MD Orders, etc.
• Copies of Demographic Sheet, MAR’s, POA, Advanced Directives may be
requested.
• SNF members are to be seen within seven business days of enrollment date
and ALF/Home members within five business days
• Case Manager will complete a new member Needs Assessments and
develop a member centered plan of care.
• Reassessment of members needs is completed on at least a quarterly basis.
• Contact by phone or in person is made on a monthly basis to each member
to ensure their safety, well being and if any additional services are needed.
• Enrollees residing and remaining in the nursing home setting are exempt
from the annual level of care redetermination requirement.

14
Care Coordination
Sunshine Health has mechanisms in place to promote coordination and
communication across disciplines and departments, with particular
emphasis on ensuring coordinated approaches with medical management
and quality management. This includes such mechanisms as the following:
• Interdepartmental communication among staff with Enrollee contact,
Case management, Enrollee Services, Utilization Management, Med
Management and Quality Management. CM and QM and MM staff (as
well as other staff with Enrollee contact) have access to TruCare and
are able to share data.
• Case Manager’s participate in weekly Clinical Rounds which are
attended by the Medical Director, Clinical Resource Specialist, BH
Coordinator, Director of CM and Interdisciplinary staff to review complex
cases & facilitate coordination of care, appropriate utilization of services,
and identify additional service options based on IDT recommendations.
15
Case Management – Home Based Care Plan Management
• Initiated Weekly Discharge Planning Rounds (Acute Care/Rehab).
• Attendees: CM, CM Supervisors, Medical Director,
Behavioral Health CM, Clinical Resource Specialist (CRS),
CR (NHT CM Sup), DCM, and ED
• Created Discharge Planning Tool (v4).
• Weekly Complex Case Discussion (placement, high cost care
plans, under utilization/over utilization (two hours).
• Case Conferences as needed.
• Attendees: CM Supervisor, appeals and grievance
coordinator, CRS, CM, and Directors
• Fair hearings
• Appeals/Grievances
• Behavioral Health – integrated to all meetings as needed.

Time lines
• Case Manager is assigned immediately upon member enrollment
• Case Manager must make initial onsite visit and complete Care Plan within 5 business days
• Case Manager must follow up with enrollee or representative telephonically within 7 business days after initial contact and Care Plan development
16

Time lines
• Monthly telephone contact
• Review of Care Plan in a face-to-face visit every 90 days (more often if enrollee requires changes to be made)
• Annual face-to-face visit to reassess enrollees needs and develop a new Plan of Care
• Case Manager must forward Plan of Care within 10 business days of development to PCP and ALF
17

Time line for Case Managers
18
• Review of Care Plan in a face-to-face visit every 90 days (more often if enrollee requires changes to be made)
• Annual face-to-face visit to reassess enrollees needs and develop a new Plan of Care
• Case Manager must forward Plan of Care within 10 business days of development to PCP and ALF
• If the recipient is enrolled in both an MMA and LTC plan, the LTC plan is responsible for CC.

19
Case management [Assessing and Care
planning]
Behavioral Health
Coordinator [Crisis
management]
Clinical Resource Specialist [Medical necessity review]
Enrollee connections
[Transition assistance/Enroll
ee support]
Program Coordinator [Case mgmt.
admin support needs]
Transportation Coordinator
[Transportation scheduling]
Concurrent Review
[Discharge planning]
Integrated Care Team Approach and Support Staff

20
• Case Manager during assessment process will determine behavioral
health need
• Case Manager will staff case during weekly meeting with ICT
• Once need is identified BHC will contact member and
identify/coordinate services within 48 hours
• BHC will either telephonically or in person contact member and will
also contact facility for behavioral management services & training
• BHC is used as a resource for the Case Manager to determine needs
• Participates in case review during Clinical Rounds
Case Management – LTC Behavioral Health Coordinator

21
Service Planning and Coordination
The case manager collaborates with the Enrollee/representative, family,
Primary Care Physician (PCP), network, and non-network providers
and community resources to develop, implement and monitor a
comprehensive, cost-effective plan of care based on enrollee/family
strengths, needs, goals, and preferences.

22
• Trainings
• Behavioral Health
• Behavioral Management
Cenpatico Services

23
Behavioral Management : A short term intervention to assist with the management of a new or change in a behavior.
• Identify triggers to specific behaviors.
• Short term behavioral modification and facility trainings.
• Support to the member and facility/caregiver through the development of a plan to modify behaviors.
• Provided by a Cenpatico contracted Community Mental Health Centers (CMHC).
Behavioral Health: Ongoing treatment of a psychiatric illness or a mental health diagnosis.
• Treatment to include crisis intervention of a psychiatric crisis, counseling/therapy, targeted case management, and medication management.
• Accessed through the Medicaid Managed Care Organization (MCO).
Behavioral Management vs. Behavioral Health

24
We use behavioral management to help our member stay in their
placements and have the highest quality of life.
Behavioral Management Services

25
• If an enrollee is having a behavioral issue, during regular
business hours or after hours the caregiver or facility may
contact the Community Mental Health Care (CMHC) directly.
• There is no referral needed and will receive up to eight hours of
behavioral management help.
• The CMHC is required to respond within two hours of the
request.
Behavioral Management Services Access
26
How do I request this?
• During office hours you may contact the member’s case manager
at Tango to initiate the request.
• After hours you may contact the CMHC contact for your regional
area to initiate the request.
Behavioral Management Services Access

27
The services are used to maximize reduction of the enrollee’s disability
and restoration to the best possible functional level and may include,
but are not limited to:
• Evaluation of the origin and trigger of the presenting behavior.
• Development of strategies to address the behavior.
• Implementation of an intervention by the provider.
• Assistance for the caregiver in being able to intervene and
maintain the improved behavior.
Behavioral Management