submitted by lai tsz ning for the master of nursing at the ...nursing.hku.hk/dissert/uploads/lai tsz...
TRANSCRIPT

Abstract of thesis entitled
“An Evidence-based Guideline of using Superficial Heat therapy for
Adult patients with Acute Low Back Pain”
Submitted by
LAI TSZ NING
For the Master of Nursing
At The University of Hong Kong
In July 2014
Low back pain is a common health problem. Around 80% of adults experience an
episode of low back pain in their lifetime. The prevalence of low back pain is the
highest during middle age.
People who suffered from acute low back pain may have the problem resolved
within a few months.However, without proper intervention, the condition could
deteiorate and result in increasing disability, losing working productivity, thus
reducing the quality of life.
Superficial heat therapy is proved to be effective in reducing pain of patients with
acute low back pain, especially heat wrap therapy which was supported by six quality
studies. It was found to be superior to oral analgesic.
This dissertation is a translational nursing research which aims at developing an
evidence-based guidline of using Superficial heat therapy to relieve pain in patients

with acute low back pain.
Seven randomized controlled stuides were identified through searching database
and critically appraised by Scottish Intercollegiate Guidelines Network. Useful data
from the studies was summarised and analysed in this paper.
The proposed protocol are designated to be implemented in Orthopaedics and
Traumatology wards in a public hospital. Therefore, implementation potential
including transferability, feasibility and cost-benefit ratio are evaluated for
establishing the superficial heat therapy guidelines. A continuous low-level heat wrap
is recommended as a mean of superficial heat therapy. The heat wrap is suggested to
apply for 8 hours in daytime for 2 consecutive days.
Furthermore, a program team was formed to facilitate communication with the
stakeholders in order to seek their approval. A pilot test is conducted to assess the
feasibility of the protocol in the implementation plan. In order to assess the
effectiveness of the protocol, an evaluation plan was initied and outcomes to be
achieved was compromised by the program team.
By implementing this newly developed evidence-based superficial Heat Therapy
guideline for patients with acute low back pain, it is anticipated that the pain of those
patients can be alleviated and their quality of life be maintained.

An Evidence-based Guideline of using Superficial Heat
therapy for Adult patients with Acute Low Back Pain
by
LAI TSZ NING
B.Nurs. H.K.U.
A thesis submitted in partial fulfillment of the requirements for
The Master of Nursing
At The University of Hong Kong
July 2014

i
Declaration
I declare that this thesis represents my own work, except where due
acknowledgement is made, and that it has not been previously included in a thesis,
dissertation or report submitted to this University or to any other institution for a degree,
diploma or other qualifications.
Signed……………………………………………………………..
LAI TSZ NING

ii
Acknowledgements
I would like to express my deepest gratitude to my supervisor Ms. Rebecca Poon,
who has inspired me and provided tremendous support and encouragement. Without her
guidance, I would not be able to advance my professional knowledge and complete this
dissertation.
I would like to express my heartily thanks to my supervisor Dr. Angela Leung. She
has selflessly offered lots of assistance and advice throughout the preparation of this
dissertation. This dissertation would not be possible without her support.
Besides, I would like to express my sincere thanks to my partner, Miss Chan
Hoi-yan who has stood by me and provided the needed supports during these 2 years’
master programme.
Last but not the least, I would like to express my blessings to my family,
colleagues, friends and classmates, especially Mr. Lo Kwok-chun, for their tolerance,
encouragement and support in every aspect during my study of the master programme.

iii
Contents
Declaration…………………………………………………………………….....i
Acknowledgements……………………………………………………………...ii
Table of Contents…………………………………………………….………….iii
List of Appendices………………………………………………….…………..vii
Abbreviations………………………………………………………………… viii
CHAPTER 1 INTRODUCTION
1.1 Background .......................................................................... 1
1.2 Affirming Needs ................................................................... 2
1.3 Significance ........................................................................... 5
1.4 Objectives ............................................................................. 5
1.5 Research Question ............................................................... 6
CHAPTER 2 CRITICAL APPRAISAL
2.1 Search Strategy .................................................................... 7
2.1.1 Inclusion criteria ............................................................................................... 7
2.1.2 Exclusion criteria ............................................................................................. 7
2.1.3 Keywords and Search Engines ......................................................................... 7
2.2 Appraisal Strategies ............................................................. 8
2.3 Results ................................................................................... 8
2.3.1 Search Result .................................................................................................... 8
2.3.2 Data Extraction ................................................................................................. 9
2.3.3 Critical appraisal .............................................................................................. 9
2.4 Summary and Synthesis .................................................... 10

iv
2.4.1 Summary of data ............................................................................................ 10
2.4.2 Synthesis of Data............................................................................................ 12
2.4.2.1 Sample Characteristics ............................................................................................ 12
2.4.2.2 Interventions ........................................................................................................... 13
2.4.2.3 Effect of Interventions ............................................................................................. 14
2.4.2.4 Outcome measurements ......................................................................................... 17
2.5 Implications ........................................................................ 18
CHAPTER 3 IMPLEMENTATION POTENTIAL
3.1 Target setting ...................................................................... 22
3.2 Target Audience ................................................................. 22
3.3 Transferability .................................................................... 24
3.3.1 Proposed setting ............................................................................................. 24
3.3.2 Proposed audiences ........................................................................................ 24
3.3.3 Philosophy of care .......................................................................................... 25
3.3.4 Sufficiency of clients benefiting from innovation ......................................... 26
3.3.5 Time for Implementation & Evaluation ......................................................... 26
3.4 Feasibility ............................................................................ 27
3.4.1 Freedom of nurse to carry out the intervention .............................................. 27
3.4.2 Interfere current staff functions ...................................................................... 27
3.4.3 Administrative Support .................................................................................. 27
3.4.4 Consensus ....................................................................................................... 28
3.4.5 Requirement of special skills and staff training ............................................. 30
3.4.6 Availability of Essential equipment & facilities ............................................. 30
3.4.7 Availability of Evaluation tools ...................................................................... 30
3.5 Cost-Benefit Ratio .............................................................. 31
3.5.1 Potential Risk ................................................................................................. 31
3.5.2 Potential Risk of maintaining current practice ............................................... 31
3.5.3 Potential Benefits ........................................................................................... 32

v
3.5.4 Cost for implementation of protocol .............................................................. 32
3.5.4.1 Set up cost ............................................................................................................... 32
3.5.4.2 Operational Cost ...................................................................................................... 34
3.5.5 Cost –benefit ratios ........................................................................................ 34
CHAPTER 4 EVIDENCE-BASED PRACTICE PROTOCOL
4.1 Title ...................................................................................... 36
4.2 Objectives ........................................................................... 36
4.3 Target User ......................................................................... 36
4.4 Target Population ............................................................... 36
4.5 Rating system of Recommendations ................................ 37
4.6 Grades of Recommendations ............................................ 37
CHAPTER 5 IMPLEMENTATION PLAN
5.1 Communication Plan ......................................................... 40
5.1.1 Identifying Stakeholders ................................................................................ 40
5.1.2 Forming Program Team ................................................................................. 41
5.1.3 Process of Communication Plan .................................................................... 42
5.1.3.1 Initiation Stage......................................................................................................... 42
5.1.3.2 Guiding Stage ........................................................................................................... 45
5.1.3.3 Sustaining Stage ...................................................................................................... 45
5.2 Pilot Study .......................................................................... 46
5.2.1 Study Design .................................................................................................. 47
5.2.2 Objectives ....................................................................................................... 47

vi
5.2.3 Target Population and Program Intervention ................................................. 47
5.2.4 Outcomes Measurements ............................................................................... 48
5.2.5 Evaluation of the guideline ............................................................................ 49
CHAPTER 6 EVALUATION PLAN
6.1 Identifying Outcomes and Outcomes Measurements .... 50
6.1.1 Patient outcomes ............................................................................................ 50
6.1.2 Healthcare Provider Outcomes ...................................................................... 51
6.1.3 System Outcomes ........................................................................................... 52
6.2 Determining Nature and Number of Clients .................. 52
6.2.1. Nature of Clients ........................................................................................... 52
6.2.2 Sampling Method ........................................................................................... 52
6.2.3 Sample Size .................................................................................................... 53
6.2.4 Duration of Program ...................................................................................... 53
6.3 Data Collection and Method of Analysis ......................... 54
6.3.1 Data Analysis Designs.................................................................................... 54
6.3.2 Time for Outcome Measurements .................................................................. 54
6.3.3 Method of Analysis ........................................................................................ 54
6.4 Basis for an effective change of practice ......................... 55
CHAPTER 7 CONCLUSTION………………………………………….56
APPENDICES………………………………………………………………....58
REFERENCES…………………………………………………………….….91

vii
List of appendices
Appendix I: History of Searching Studies ............................................................... 58
Appendix II: Table of Evidence ................................................................................ 59
Appendix III: Methodology Checklists .................................................................... 66
Appendix IV: SIGN Grading System 1999-2012 ..................................................... 80
Appendix V: Summary table of Levels of Evidence of relevant studies ................ 81
Appendix VI: Cost for Implementation of protocol ................................................ 82
Appendix VII: Comparison of the cost between Current Practice and Superficial
Heat Therapy .................................................................................... 83
Appendix VIII: SIGN Grading System 1999 – 2012:
Grades of recommendations .......................................................... 84
Appendix IX: Timeframe for Superficial Heat Therapy Program for acute Low
Back Pain .......................................................................................... 85
Appendix X: Operational Flow of Superficial Heat therapy in Pilot Test ............ 86
Appendix XI: Pain Chart .......................................................................................... 87
Appendix XII: Assessment chart for Patient using Superficial Heat therapy ..... 88
Appendix XIII: Nurses’ Evaluation form for Superficial Heat Therapy
Program .......................................................................................... 89
Appendix XIV: Calculation of Sample Size ............................................................. 90

viii
Abbreviations
AC
APN
Assistant Concultant
Advanced Practice Nurse
CCE Cluster Chief Executive
COS Chief of Service
DOM Department Operation Manager
EN Enrolled Nurse
GMN
MO
General Manager of Nursing
Medical Officer
NC Nursing Consultant
NRS Numeric Rating Scale
O&T Orthopaedics and Traumatology
Q&A Question and Answer
RN Registered Nurse
SIGN Scottish Intercollegiate Guidelines Network
VRS Verbal Rating Scale
VAS Visual Analog Scale
WM Ward Manager

1
Chapter 1
Introduction
1.1 Background
Low Back pain is one of the common health problems. Around 80% of adults
experience once in a lifetime. The prevalence of low back pain is the highest
during middle age with the point prevalence of 11.9% and 1-month prevalence of
23.2% (Hoy et al., 2012).
There is no universal classification of low back pain. According to national
clinical guidelines from Europe and the United Kingdom, low back pain can be
classified as acute when it persists for less than 6 weeks, sub-acute between 6
weeks and 3 months and chronic when it lasts for longer than 3 months (Koes et
al., 2010). Signs and symptoms of low back pain may resolve within a few
months in 90% of cases with acute low back pain. However, without proper
intervention, some cases will proceed to recurrent or chronic problems and
residual trunk muscle dysfunction (Hides et al, 1994). These result in increasing
disability, losing working productivity and reducing quality of life (Pengel et al.,
2003). In addition, from a psychosocial prospective, anxiety and depression are
associated with low back pain. People with low back pain are more likely to
develop depression and anxiety disorder (Mok & Lee, 2008).

2
In order to prevent functional loss from acute low back pain, physical activity
and early initiation of rehabilitative exercises are recommended (Mayer et al.,
2005). However, people experience acute pain episode will be limited to perform
physical exercise, or even reluctant to participate.
Therefore, the alleviation of acute low back pain is important and necessary.
1.2 Affirming Needs
According to the admission statistical record at the Orthopaedics &
Traumatology departments of a public hospital where I work, over 70% patients
were admitted for acute low back pain. Current treatments for acute low back pain
include oral, intravenous or intramuscular analgesic, bed resting for 1-2 days and
referral to physiotherapy for physical exercise.
However, by clinical experience, over 40% of patients consider the current
treatment not effective in relieving the pain. Patients complain of epigastric pain,
nausea and vomiting after taking medications (Drug office, 2013a). Some patients
even request more medications for pain relief. This leads to more serious effect
such as gastrointestinal disturbance, poor appetite which induced poor nutrition
absorption (Drug office, 2013a). Dizziness and tiredness may cause as a result
which prolong bed resting time and delay of starting physical exercise.

3
Besides, sleep disturbance and insomnia are common associated problems in
patients with low back pain. Sleeping problem is associated with pain of 60%
prevalence (Alsaadi et al., 2011). Patients refuse to have physical exercise due to
lack of energy and prolong bed resting time, worsening the low back pain and
delay recovery (Waddell, Feder & Lewis, 1997). Moreover, they are more prone
to using sleeping pills which may cause severe side effects such as convulsion and
paranoid psychosis (Drug office, 2013b). The medical costs and length of
hospitalization are increased.
Superficial heat therapy is one of the common non-pharmacological
interventions for low-back pain. It is a safe and non-invasive treatment (Chou &
Huffman, 2007). Nurses can apply it to patients in need based on their
professional knowledge and judgments.
This superficial heat therapy is an application of topical heat by variety of
modalities over the pain area of the lower back. The heat stimulates
thermo-receptors in the skin and deeper tissues. According to the Gate Control
Theory (Melzack and Wall 1965), heat stimulates the impulse of large diameter
sensory fibers which close the gate in spinal cord. Transmission of painful signal
is thus decreased and pain reduced (Candler, Preece & Lister, 2002). There are
different modalities in superficial heat therapy, for example hot water bottles, hot

4
towels, electric heat pads and heat wrap (French et al., 2011).
Various studies have shown positive result of superficial heat therapy in
reducing low back pain (Kinkade, 2007). Some studies show that superficial heat
therapy is superior in pain relief to oral medications in treating low back pain
(Kettenmann et al., 2007; Nadler et al., 2002). Patients have preference in
superficial heat therapy to oral analgesic (Kettenmann et al., 2007). Other studies
also indicate that superficial heat therapy helps improve quality of sleep
(Kettenmann et al., 2007, Nadler et al., 2003).
Other countries, for example the United States, have recommended the use of
topical heat therapy in treatment of acute low back pain and applied it into clinical
practice (Chou et al., 2007). The Hospital Authority in Hong Kong also suggests
using heat therapy for relieving low back pain (HA, 2013) but it is not a common
routine practice in proposed ward.
Patients benefit from better pain controls are able to undergo earlier
rehabilitation exercise and maintain quality of life. Therefore, it is essential to
evaluate the effectiveness of using superficial heat therapy in reducing acute low
back pain and the methodology for application in local setting should also be
considered.

5
1.3 Significance
Superficial heat therapy is a kind of non-pharmacological intervention and
could be applied to patients in need by nurses based on knowledge and assessment.
It enhances nurses’ autonomy to provide better care to patient and raise patient’s
satisfaction. In addition, patients can benefit from better pain control away from
increasing risk of medication’s side effect. Patients with acute low back pain can
remain active in participating physical activity and maintain quality of life.
Moreover, burden of hospital-based medical care expanse could also be relieved
due to reduced consumption of additional medications and decreased length of
hospitalization.
Besides, evidenced based practice integrates clinical expertise and patient’s
value with research evidence support. (Sackett et al., 1996) It improved patient’s
pain intensity by providing higher quality of care since it incorporates the latest
research evidence.
1.4 Objectives
The objectives of this study are
1) To review and critically appraise the published research which evaluate the
effectiveness of using superficial heat therapy in reducing pain of patients with

6
acute low back pain
2) To develop an evidence-based guidelines for nurses in providing quality care
to patients with acute low back pain.
3) To assess the implementation potential of the guidelines which include
transferability, feasibility and cost-effectiveness
4) To develop a plan for implementing new innovation including a
communication plan with stakeholders
5) To develop an evaluation plan to assess the effectiveness of the proposed
protocol
1.5 Research Question
Is superficial heat therapy effective in reducing pain of patients with acute low
back pain compared with usual orthopaedics care?

7
Chapter 2
Critical Appraisal
2.1 Search Strategy
2.1.1 Inclusion criteria
The studies should be published in English, accessible in full text and the
publication year after 2002. Only randomized controlled trials studies could be
selected.
2.1.2 Exclusion criteria
Studies included participants aged less than 18, with the complaint of chronic
low back pain were excluded. Studies that included participants with low back
pain with radiculopathy were also excluded
Trials of deep heating intervention, for example, microwave diathermy and
ultrasound, were excluded. Besides, studies which given co-interventions which
could not isolate the effects of heat from other therapy were excluded too.
2.1.3 Keywords and Search Engines
Keywords were used for searching eligible studies which include “Acute low

8
back pain”, “back pain”, “Superficial heat therapy”, “thermotherapy” and “pain”.
A total of 3 databases were used for systematic search which are Pubmed,
CINAHL via EBSCOHOST and British Nursing Index via Proquest.
2.2 Appraisal Strategies
Those randomized controlled trials were appraised by using Critical
Appraisal: Notes and Checklist (2012) from Scottish Intercollegiate Guidelines
Network (SIGN). The level of evidence of those selected studies would be rated
according to the Grading System 1999-2012 from Scottish Intercollegiate
Guidelines Network (SIGN).
2.3 Results
2.3.1 Search Result
After using those keywords separately and in combination with each other via
three databases with consideration of inclusion and exclusion criteria, a total of
seven randomized controlled studies were chosen which all from Pubmed
(Kettenmann et al., 2007; Tao & Bernacki, 2005; Mayer et al., 2005; Nuhr et al.,
2004; Nadler et al., 2003a; Nadler et al., 2003b; Nadler et al., 2002). No studies
were retrieved from CINAHL via EBSCOHOST and British Nursing Index via

9
Proquest. The search was done on 18th June, 2013. The searching history and
details were presented in Appendix I.
Those 7 randomized controlled studies were appraised and graded by using
SIGN. The details of methodology checklist and grading system were shown in
Appendix III & IV.
2.3.2 Data Extraction
All useful data from the studies would be extracted into Table of Evidence.
The details of the table were listed in Appendix II.
2.3.3 Critical appraisal
All seven trials reported as randomized. Only two studies described the
randomization methods by using computer-generated codes (Mayer et al., 2005;
Nuhr et al., 2004). Concealment method was used in only one of the studies (Nuhr
et al., 2004) while the remaining studies were not reported. Single blinding was
carried out in five of the studies which one study blinded to participants (Tao &
Bernacki, 2005) and four studies blinded to investigators. (Nuhr et al., 2004;
Nadler et al., 2003a; Nadler et al., 2003b; Nadler et al., 2002).

10
One trial reported zero dropout rate and all data were successfully analyzed
(Tao & Bernacki, 2005). The other six trials had an acceptable dropout rate ranged
from 2% to 21% (Kettenmann et al., 2007; Mayer et al., 2005; Nuhr et al., 2004;
Nadler et al., 2003a; Nadler et al., 2003b; Nadler et al., 2002). Intention to treat
was undertaken in four studies to analysis the data (Mayer et al., 2005; Nadler et
al., 2003a; Nadler et al., 2003b; Nadler et al., 2002) and per protocol analysis was
carried out in two studies (Kettenmann et al., 2007; Nuhr et al., 2004).
Seven selected studies were appraised by Scottish Intercollegiate Guidelines
Network (SIGN), the level of evidence were ranged from 1- to 1+. 6 studies were
rated as 1+ (Tao & Bernacki, 2005; Mayer et al., 2005; Nuhr et al., 2004; Nadler
et al., 2003a; Nadler et al., 2003b; Nadler et al., 2002) while 1 study was rated as
1- (Kettenmann et al., 2007). The Summary table of levels of evidence was listed
in Appendix V.
2.4 Summary and Synthesis
2.4.1 Summary of data
The sample size of seven studies varied from 30 to 371. The mean age of
participants varied from 30-56. The trials included patients with acute low back
pain or a mix of acute and sub-acute low back pain. All seven trials reported clear

11
inclusion and exclusion criteria. For example, eligible participants should be over
18 and able to follow the instructions, those with history of low back pain over 3
months must be excluded.
Two types of superficial heat therapy were examined in seven studies which
were continuous low-level heat wrap therapy and active warming with electric
blanket. Continuous low-level heat wrap therapy was a wearable heat wrap made
of layers of cloth-like material that contain heat-generating ingredients. These
ingredients heat up to 40oC when exposure to air within 30 minutes and this
temperature could maintain continuously for 8 hours. The heat wrap was applied
on the lumbar region and participants were allowed mobile while wearing it. This
device was safe and approved by Food and Drug Administration in the United
States (Kettenmann et al., 2007; Tao & Bernacki, 2005; Mayer et al., 2005; Nadler
et al., 2003a; Nadler et al., 2003b; Nadler et al., 2002). Heat wrap was used either
in the day time for 2-5 days or throughout 3 consecutive nights.
For the active warming with electric blanket therapy, the blanket temperature
was set to 42oC by heating system (Nuhr et al., 2004). The intervention time of
using electric blanket was during transportation.
Pain was assessed in all studies with different measurement tools which include
0-100mm visual analogue scale (VAS), 6-point verbal rating scale (VRS) and 0-10

12
numeric rating scale (NRS). The pain intensities were measured before and after
the treatment with subsequently measurement taken ranged from 2 to 14 days
(Kettenmann et al., 2007; Tao & Bernacki, 2005; Mayer et al., 2005; Nuhr et al.,
2004; Nadler et al., 2003a; Nadler et al., 2003b; Nadler et al., 2002).
2.4.2 Synthesis of Data
2.4.2.1 Sample Characteristics
The sample size was small in two trials which included 30 and 43 participants
respectively without formal power calculation (Kettenmann et al., 2007; Tao &
Bernacki, 2005). The remaining five trials had effective sample size with power
analysis. Four trials had a power of 80% or above at 5% level of confidence
(Mayer et al., 2005; Nuhr et al., 2004; Nadler et al., 2003a; Nadler et al., 2003b)
while one trial had a power of 90% at 2.5% level of confidence (Nadler et al.,
2002).
The mean of age of six trials ranged from 30-42 (Tao & Bernacki, 2005;
Mayer et al., 2005; Nuhr et al., 2004; Nadler et al., 2003a; Nadler et al., 2003b;
Nadler et al., 2002). One trial had older age group which the mean of age was 56
(Kettenmann et al., 2007).

13
All studies reported the participants were suffered from acute low back pain.
However, according to the classification approved by Europe and United
Kingdom, there was only one study included acute low back pain participants
(Nuhr, 2004), while a mix of acute and sub-acute low back pain participants was
included in six studies (Kettenmann et al., 2007; Tao & Bernacki, 2005; Mayer et
al., 2005; Nadler et al., 2003a; Nadler et al., 2003b; Nadler et al., 2002). Although
data of acute low back pain cannot be differentiated from those studies with mixed
population, superficial heat wrap therapy was proved to be effective for not only
acute low back pain, but also sub-acute low back pain patients.
2.4.2.2 Interventions
Six studies examined a continuous low-level heat wrap therapy as the
intervention (Kettenmann et al., 2007; Tao & Bernacki, 2005; Mayer et al., 2005;
Nadler et al., 2003a; Nadler et al., 2003b; Nadler et al., 2002) and one study used
active warming with electric blanket as intervention (Nuhr et al., 2004). Nuhr et al.
(2004) conducted a study by using active warming with electric blanket during
emergency transportation. Nadler et al. (2003b) examined the effect of overnight
use of heat wrap therapy for 3 consecutive nights. The remaining trials used the

14
heat wrap therapy for daytime use. Three trials used it for 2 (Nadler et al., 2002),
4 (Kettenmann et al., 2007) and 5 consecutive days (Mayer et al., 2005)
respectively and two trials used it for 3 consecutive days (Tao & Bernacki, 2005;
Nadler et al., 2003a).
Heat wrap therapy was well tolerated and no serious adverse events occurred
during the study. Three trials reported minor adverse effect of skin redness after
use of the heated wrap but all can be resolved without intervention (Nadler et al.,
2003a; Nadler et al., 2003b; Nadler et al., 2002). A total of 2 out of 208
participants who used heat wrap in the daytime experienced skin redness (Nadler
et al., 2003a; Nadler et al., 2002) and 4 participants out of 33 got erythema by
using heat wrap throughout the night (Nadler et al., 2003b) .There was no adverse
event occurred in the use of active warming with electric blanket.
2.4.2.3 Effect of Interventions
2.4.2.3.1 Comparison 1: Heat therapy versus non-heat therapy or oral
placebo
In the study of Nuhr et al. (2004), it compared the active warming electric
blanket with non-heat woolen blanket. The active warming group had
significantly reduction in pain. (p<0.01) It showed a statistically significant

15
benefit of a heated blanket compared to a non-heated woolen blanket immediately
after treatment (Pain score mean difference: -32.3 vs +0.8; Scale Range 0 to 100)
(Nuhr et al., 2004).
Two studies compared the effect of heated wrap with oral placebo. Results
showed that pain relief was significantly greater in heat wrap than the oral placebo.
In the study of Nadler et al. (2003a), heat wrap group was 2.89 times greater pain
relief than the oral placebo group. (p<0.04) Both studies also showed that there
was a significantly extended pain relief (on days 4 and 5) in heat wrap group even
the removal of intervention on day 3 (p<0.00001; p<0.00005) (Nadler et al.,
2003a; Nadler et al., 2003b).
2.4.2.3.2 Comparison 2: Heat therapy versus pharmacological interventions
Kettenmann et al. (2007) compared heat wrap with oral analgesics, the
heatwrap therapy treatment was more effective in reducing pain on day 3 and day
4 with statistically significance. (p<0.02; p<0.042) However, considering the
limitations of this study, such as small sample size (n=30) without formal power
calculations carried out, about 20% drop out rate and uneven sex distribution
between the control group and treatment group, the results would be in risk of bias
(Kettenmann et al., 2007).

16
Nadler et al. (2002) conducted a study to compare the heat wrap therapy with
acetaminophen and ibuprofen, heat wrap group demonstrated significant
improvements in pain relief as compared with acetaminophen and ibuprofen.
(p=0.00001; p=0.00001) The effect was also sustained in the heat wrap group for
2 more days after removal of heat wrap (Nadler et al., 2002).
2.4.2.3.3 Comparison 3: Heat therapy versus non-pharmacological
interventions
Tao X. & Bernacki, R.J. (2005) conducted a study to compare heat wrap with
education. The pain intensity was taken at day 1-4, day 7 and day 14. The heat
wrap therapy had significantly reduced the pain intensity from day 1 to day 14
compared with education. (p<0.05) The pain intensity was dramatically reduced
during 3-day treatment. Pain relief was also taken at the same time. Pain relief
was significantly greater than education group during the 3-day treatment and the
day after. (p<0.05) However, no significant difference at day 7 (p=0.24) and day
14 (p=0.15) (Tao & Bernacki, 2005).
Study of Mayer et al. (2005) also compared the heat wrap with exercise alone
and educational booklet alone. The measurement was taken at day 2, day 4 and
day 7. No significance difference in pain relief at day 2. At day 4, the pain relief

17
was greater in heat wrap than education. (0=0.026) However, a greater number of
female were assigned to the control group compared with other treatment groups.
This gender imbalance may bias the outcome. There was also no blinding in this
study which weakened the results.
Besides, this study also combined the heat wrap with exercise, and compared it
with heat wrap alone, exercise alone and booklet alone. The heat wrap with
exercise group had significantly greater pain relief than exercise and booklet on
day 7. Heat wrap with exercise group had almost 30 times greater pain relief than
booklet (p=0.003) (Mayer et al., 2005).
2.4.2.4 Outcome measurements
Pain was assessed in all studies with either in the form of pain relief or pain
intensity. Four studies used 6-point verbal rating scale (VRS) to measure pain
relief (Mayer et al., 2005; Nadler et al., 2003a; Nadler et al., 2003b; Nadler et al.,
2002). Two studies used 0-100mm visual analog scale (VAS) to measure pain
intensity (Kettenmann et al., 2007; Nuhr et al., 2004). One study measured both
pain relief and pain intensity by using 6-point VRS and 0-10 numeric rating scale
(NRS) (Tao & Bernacki, 2005). All indicators evaluated the effect of superficial
heat therapy in reducing pain significantly with consistent or stable results.

18
In the study of Tao X. & Bernacki, E.J. (2005) which used both pain relief and
pain intensity measurements, the difference between these two indictors was
evaluated. It showed that pain intensity scale was more sensitive and stable
compared with pain relief. As the result in pain intensity showed dramatically
reduction at the beginning and kept consistent afterwards, the pain relief became
less useful. Pain intensity was a better indicator to show the rate of change in pain.
Both VAS and NRS are commonly used tools for measuring pain intensity.
They are reliable, valid and appropriate for use in clinical practice (Williamson &
Hoggart, 2005). NRS is easier for administration and recording comparatively.
Moreover, NRS is preferred by patient because of its simplicity (Williamson &
Hoggart, 2005). It is also widely used in hospital setting in Hong Kong.
2.5 Implications
Seven randomized controlled studies were appraised. Two types of superficial
heat therapy, which were continuous low level heat wrap therapy and electric
warm blanket, were examined for either acute low back pain participants or a
mixed population with acute and sub-acute low back pain. Both therapies were
better than non-heat therapies or oral placebo in pain relief. Six trials used heat
wrap as intervention and proved that heat wrap therapy was superior to either

19
pharmacological or non-pharmacological interventions with statistically
significant result.
Although 6 studies applied heat wrap as intervention, the duration of treatment
was different. Study of Kettenmann et al (2007) applied heat wrap for 4 hours for
4 consecutive days. The result was considered as low effectiveness due to the low
level of evidence comparatively. Another study applied heat wrap for 8 hours for 5
consecutive days (Mayer et al., 2005), the results of the study might be biased due
to the gender imbalance between groups. Therefore effectiveness of that study was
considered as low. Two studies used heat wrap therapy for 8 hours for 3
consecutive days showed dramatic reduction in pain but small sample size and
insufficient sample characteristics provided (Tao & Bernacki, 2005; Nadler et al.,
2003a). The effectiveness from these 2 studies was needed to be considered. Study
of Nadler et al, (2003b) showed greatest pain relief result by administration of
heat wrap for 8 hours for 3 consecutive nights. However, there was 12% risk of
minor adverse effect, like erythema occur compared with 0.9% risk used in the
daytime. One study with effective sample size exhibited significant pain relief by
using heat wrap for 8 hours for 2 consecutive days (Nadler et al., 2002).
All studies either use pain relief or pain intensity as an indicator of pain.
However, pain intensity was a better indicator as it could show the changes of

20
pain where pain relief became less useful. (Tao & Bernacki, 2005) Visual Analog
Scale and Numeric Rating Scale are commonly used tools in measuring pain
intensity. They are reliable and sensitive. Numeric Rating Scale is easier to use
and more preferable by patients because of its simplicity compared with Visual
Analog Scale. It is also widely used in clinical practice.
Heat wrap therapy allowed mobilization compared with electric warm blanket.
It was more appropriate for using in the clinical setting so as promoting early
rehabilitation exercise. Study of Mayer et al., (2005) indicated that heat wrap plus
exercise produce greater pain relief than exercise alone. Although there was no
sufficient data to prove that whether heat wrap plus exercise had more pain
reduction or similar result than heat wrap alone, this showed that with additional
heat wrap therapy, the effect of pain relief was enhanced.
On the other hand, study of Nadler et al. (2003b) showed that heat wrap therapy
was significantly beneficial to improve quality of sleep. Another study of
Kettenmann et al. (2007) also suggested that heat wrap therapy could help in
better night sleep. Further study on effectiveness of superficial heat therapy on
quality of sleep was encouraged in future.
To sum up, superficial heat therapy is effective in reducing pain among patients
with acute and sub-acute low back pain. Heat wrap therapy is more appropriate in

21
the clinical setting compared with using elective warm blanket. Patients can
remain active and can do the physical exercise when wearing heat wrap. Thus
their quality of life can be maintained.
In my clinical working place, an acute Orthopaedics & Traumatology (O&T)
ward in a public hospital, over 70% of patients were admitted with acute low back
pain. By clinical observation, people tend to seek for medical advice when the
pain persists for a week. Therefore, there are no patients admitted with sub-acute
low back pain. Considering the patient’s characteristics in target setting, it is
worthy and important to develop an evidence-based heat wrap protocol by
synthesizing all useful data for acute low back pain patients.

22
Chapter 3
Implementation Potential
There are several modalities in superficial heat therapy, for example, hot water
bottles and electric heat pad. Heat wrap therapy is proved to be effective with
evidence-based support in the last chapter. Therefore, heat wrap therapy is decided
to be introduced into proposed protocol.
This chapter will evaluate the implementation potential of proposed protocol.
The transferability, feasibility and cost-benefit ratio will be assessed (Polit & Beck,
2004).
3.1 Target setting
The target setting for the implementation of heat wrap therapy is Orthopaedics
and Traumatology (O&T) wards in a public hospital. There are totally 4 acute
O&T wards, including 2 male and 2 female wards. The bed stat of the O&T
department is over 200. People with acute low back pain are admitted to O&T
wards for orthopedics treatment such as medication and physiotherapy.
3.2 Target Audience
According to the statistical admission record, over 70% patients are admitted

23
with acute low back pain and the majority is adult patients. Those patients will be
the target population of the proposed program.
Moreover, they must be ambulatory and cognitive intact which can follow
instructions. Female patients are required to have negative urine pregnancy test.
Those patients with any evidences or history of radiculopathy, other neurologic
deficit or spinal surgery will be excluded to this protocol (Tao & Bernacki, 2005;
Mayer et al., 2005; Nadler et al., 2003a; Nadler et al., 2003b; Nadler et al., 2002).
According to the Gate Control Theory (Melzack and Wall, 1965), heat therapy is
effective in low back pain which caused by muscle spasm by reducing tension in
muscle trigger point (Candler, Preece & Lister., 2002). Therefore, those patients
who suffer from neurological pain are not benefited from this protocol.
Besides, patients with hypersensitivity to heat or any skin lesions on the lumbar
region must be excluded to this protocol (Kettenmann et al., 2007; Tao &
Bernacki, 2005; Mayer et al., 2005; Nadler et al., 2003a; Nadler et al., 2003b;
Nadler et al., 2002). Heat wrap is used and applied on the lumbar region to
provide superficial heat therapy. Continuously using heat wrap for those patients
will increase risk of skin abrasions and deterioration of wound condition. For the
sake of patient safety, this kind of patients is also not recommended for applying
this protocol.

24
3.3 Transferability
3.3.1 Proposed setting
The setting of studies included community-based research facilities,
(Kettenmann et al., 2007; Nadler et al., 2003a; Nadler et al., 2003b; Nadler et al.,
2002;), out-patient medical facilities (Mayer et al., 2005), out-patient clinic (Tao
& Bernacki, 2005) and during emergency transport (Nuhr et al., 2004). Although
those settings are not as same as the target settings, there are number of patients
with acute low back pain admitted in O&T wards. Therefore the innovation can be
transferred to the proposed setting.
3.3.2 Proposed audiences
The participants of 6 studies were a mix of sub-acute and acute low back pain
adult patients. Those eligible patients were ambulatory. Those studies excluded
patients with any evidence or history of radiculopathy or other neurologic deficits,
history of back surgery and skin lesions on the lumbar region. (Kettenmann et al.,
2007; Mayer et al., 2005; Tao & Bernacki, 2005; Nadler et al., 2003a; Nadler et al.,
2003b; Nadler et al., 2002). The inclusion and exclusion criteria of the studies are

25
similar with the characteristics of the target population. Therefore, the findings are
transferrable.
3.3.3 Philosophy of care
The mission of our Orthopaedics and Traumatology department is to enhance
and regain patient‘s capacity to get back to community by providing
“client-oriented holistic care” through continuous quality improvement, education
and research, multidisciplinary approach and professionals development. The
philosophy of superficial heat therapy is to relieve patient’s back pain in order to
enhance their rehabilitation and minimize the complications, such as residual
trunk muscle dysfunction and depression. (Hides et al., 1994; Mok & Lee, 2008)
This innovation is developed based on evidence and research with quality
justification. It aims at enhancing patient’s quality of life by improving current
practice which is corporate the mission of O&T department. This innovation is
client-oriented approach which their daily life activities can be maintained under
the intervention.
Those philosophies of care of the innovation are consistent with the philosophy
prevailing in practice setting. Therefore heat wrap therapy for patients with acute
low back pain is transferrable.

26
3.3.4 Sufficiency of clients benefiting from innovation
According to the admission statistics in O&T department, there are over 70%
patients admitted with acute low back pain. After considering the inclusion criteria
of this innovation, it is estimated that there is around 600 clients annually, which
is sufficiently a large number, benefiting from this heat wrap therapy.
3.3.5 Time for Implementation & Evaluation
The time for implementation is different in those 6 studies using heat wrap
ranged from 4 days to 14 days (Kettenmann et al., 2007; Tao & Bernacki, 2005;
Mayer et al., 2005; Nadler et al., 2003a; Nadler et al., 2003b; Nadler et al., 2002).
After considering the methodology and result among those 6 studies,the
findings from study of Nadler et al (2002) is the most precise with 90% power at
2.5% level of confidence. Therefore the time for implementation is set as 4 days
which includes 2-day intervention with 2 days of follow up (Nadler et al., 2002).
It is transferrable to the proposed setting as its short-term measurement.
Pain intensity will be used for impact evaluation. It will be first measured
before applying heat therapy, then daily measure for consecutive 4 days.

27
3.4 Feasibility
3.4.1 Freedom of nurse to carry out the intervention
Heat wrap therapy is a safe and non-pharmacological intervention. This
intervention has to be applied with doctor’s prescription. However, nurses have
the freedom to continue or terminate the superficial heat therapy according to
clinical judgment.
3.4.2 Interfere current staff functions
The workload of nursing staff might be slightly increased as they have to spend
time on education and applying the innovation. However, this innovation is
simply to apply which won’t take too long and evaluation of pain score and
education can be done during regular shift routine assessment , therefore current
staff functions will not be interfered.
3.4.3 Administrative Support
The administrators are supportive to research and evidence-based protocol. The
hospital set up a forum which allows all nurses to share their opinions and

28
suggestions in order to improve existing protocol. Moreover, nurses are welcomed
to develop a new protocol through this forum. Besides, each year our O&T
department encourages nurses to share different ideas and present the research in
the joint O&T nursing forum. The O&T department also reviews or develops
protocol regularly to maintain the standard of advanced nursing practice.
Therefore, the administrators would welcome this innovation which benefit to
clients.
3.4.4 Consensus
A protocol will not be success if work alone, a certain degree of consensus has
to be made. In the patient’s perspective, this new intervention is a
non-pharmacological treatment that they are in favor of as low risk of side effects.
In the nurse’s point of view, they agree this evidence-based innovation and
appreciate this simple intervention won’t occupy too much time which interfere
the routine work.
In doctor’s perspective, they support this intervention as less consumption of
analgesic which can reduce the potential complications induced by side effects.
Physiotherapists also welcome this innovation as their workload will be decreased
and the progress of physical exercise will become smoothly.

29
Before establishing a new protocol, approval from administrators which
includes Chief of Service (COS), General Manager of Nursing (GMN),
Department Operation Manager (DOM), Nursing Consultant (NC) and Ward
Manager (WM) must be obtained. The protocol must be turned down without their
support. Therefore, the rationale, significance, effectiveness and advantages of
superficial heat therapy supported by evidence-based research should be
explained. In order to persuade them, the implementation potential of an
innovation proposal with budget plan must also be presented. It is importance to
allow time for them to ask and clarify any misunderstand.
Moreover, gaining support from orthopaedics medical officer is an essential
element of this protocol as the heat wrap therapy is initiated with Orthopaedics
medical officer’s prescription. Studies of Kettenmann (2007) and Nadler (2002)
showed that heat wrap therapy is superior to oral medications in pain relief and
patient tends to less use of oral analgesic when receiving heat wrap therapy.
Doctors can consider the effect of heat wrap therapy when prescribing analgesic.
Therefore, details and significant of protocol must be explained to them. They are
welcomed for raising their concerns and sharing opinions on developing protocol
in order to increase the compliance of patient to new intervention.
Nurses who are responsible to carry out the protocol are also another important

30
professionals towards success. Some nurses may reluctant to change or adopt the
new techniques, therefore the details and advantages of protocol must be
explained. The skills of applying this new innovation have also to be introduced.
3.4.5 Requirement of special skills and staff training
Heat wrap therapy is an evidence-based practice with new innovated
technology to nursing staff. The skills of applying heat wrap are required to
introduce to nursing staff. Therefore one-hour training workshop will be provided
with compensation hour and continuous nursing education point.
3.4.6 Availability of Essential equipment & facilities
The superficial heat therapy requires continuous low-level heat wrap which is
not available in the current setting. Therefore, an estimated amount of heat wrap
should be purchased. A store room is already available for storage of equipment
3.4.7 Availability of Evaluation tools
The outcome measurement is pain intensity and it is measured by Numeric
Rating Scale which is available in the pain score charting. The charting is

31
currently used in the ward setting.
3.5 Cost-Benefit Ratio
3.5.1 Potential Risk
There is no serious adverse effects occurred in using superficial heat therapy
during studies. Mild erythema is rarely noted but can be resolved without
intervention (Nadler et al., 2003a; Nadler et al., 2003b; Nadler et al., 2002).
3.5.2 Potential Risk of maintaining current practice
Patients will request for more analgesic if the pain is not relieving. The risk of
side effects of analgesic, for example, peptide ulcer is increased (Drug Office,
2013a). Those complications will increase the duration of hospitalization and
prolong the bed resting time which delay the recovery and increase disability.
Undoubtedly, the quality of life of patients is reduced.
The medical cost will be increased due to the increased consumption of
medication and prolonged hospitalization.

32
3.5.3 Potential Benefits
The superficial heat therapy can relieve low back pain effectively. Patient will
tend to less use of oral analgesic which lowers the risk of complication
development. Moreover, the sleep quality will be improved. Patient can start
rehabilitation exercise earlier and maintain quality of life. These benefits can
shorten the length of hospital stay and decrease medication use, thus reduce the
medical cost of the hospital. Besides, this evidence-based superficial heat therapy
can enhance the professionalism of nurses. Nurses can strengthen their confidence
to handle patients with low back pain.
3.5.4 Cost for implementation of protocol
3.5.4.1 Set up cost
Material cost
The superficial heat therapy requires heat wrap which cost 0.99US Dollars per
each. (Approximately $8 HK dollars) According to admission statistics record of
O&T department, there are estimated 600 patients per year fit for this intervention.
Each patient will use 2 packs of heat wrap for 2 consecutive days in this protocol.
An extra amount of 100 heat wrap also has to be ordered for replacement as there

33
are risks of broken or not functioning of heat wrap. Therefore, the total amount of
1300 heat wrap is required annually which costs $10400.
The printing of leaflets about heat wrap therapy for patient’s education cost
$0.2 per each. 600 printings are required which cost $120 in total.
The stationary and computer component used in the workshop are available
which is free of charge. Evaluation from is also available in the ward setting, no
extra cost will be charged.
The total amount of set up cost is $10,520. The detail of calculation is attached
in Appendix VI.
Non-material cost
There are two one-hour training workshops provided to all responsible nurses,
the venue and manpower are the non-material cost in this protocol. The venue for
holding the workshop is available and free of charge after getting the hospital’s
approval. Two RN trainers will be responsible for providing training to all nurses.
Compensate hour and continuous nursing education point will be offered to all
nurses who attended the workshop, as well as trainers. Therefore, no extra salary
costs will be charged.

34
3.5.4.2 Operational Cost
This protocol is implanted by nurse and the heat wrap can be applied during
routine work. Therefore, no extra operational salary has to be spent. Besides, a
store room is available for storage of heat wrap which is also free of charge.
3.5.5 Cost –benefit ratios
According to clinical observation, the average length of stay of patients with
low back pain is 7 days and the hospital stay cost for each day is around $4900.
Panadol is the common drug prescription for pain relief. However, most
patients request more pain killers for pain control on the next day. The common
regimen for additional analgesics includes oral tramadol and voltaren. Pepcidine
will also be prescribed at the same time for prophylactic use of peptic ulcer.
Follow up appointment will be given to patient which is 14 days after discharge in
average with medications prescribed.
The costs of maintaining current practice of each patient is $34331.2.
Patients would have better pain control and remains active when applying heat
wrap, therefore they can start rehabilitation exercise 2 days earlier instead of
taking bed rest for 2 days in current practice of physiotherapist. By clinical

35
experience, the earlier starting physical exercise, the less duration of
hospitalization. Therefore, it is believed that the estimated length of stay after
implementing heat therapy is 5 days. The unit cost of applying the intervention is
$24516.2. The details of calculation are in Appendix VII.
This heat wrap therapy can save $9815 per person and the annual cost saving is
($9815 x 600 patients/ year) = $5,889,000. The cost-benefit ratio is ($10,520 /
$5,889,000) = 0.0018.

36
Chapter 4
Evidence-based Practice Protocol
4.1 Title
An evidence-based protocol of using superficial heat therapy for adult patients
with acute low back pain in reducing pain
4.2 Objectives
The objective of this evidence-based protocol is to relieve pain in adult patients
with acute low back pain by using continuous low-level heat wrap. Secondly, it
optimizes the pain management in a safe and cost-effective way. Thirdly, it
provides guidelines for nurses when applying superficial heat therapy.
4.3 Target User
All O&T nurses, including Registered Nurse (RN) and Enrolled Nurse (EN)
will be the target users of this guideline.
4.4 Target Population
The target population is adult patients admitted with acute low back pain. Those
eligible patients must be ambulatory and cognitive intact which can follow the

37
instructions and agree for the superficial heat therapy. Female patients are
required to have negative urine pregnancy test. Patients with any evidences or
history of radiculopathy, other neurologic deficit or spinal surgery must be
excluded in this protocol. Patients with hypersensitivity to heat or had any skin
lesions on the lumbar region are also excluded.
4.5 Rating system of Recommendations
The recommendations of this guideline are graded with consideration of level
of evidence by using SIGN grading System 1999-2012. (Appendix IV, V and
VIII)
4.6 Grades of Recommendations
4.6.1 Using Continuous low-level heat wrap as a mean to provide superficial
heat therapy.
Heat wrap is effective in reducing pain for treating low back pain (Kettenmann
et al., 2007; Tao & Bernacki, 2005; Mayer et al., 2005; Nadler et al., 2003a;
Nadler et al., 2003b; Nadler et al., 2002). It is a safe and non-pharmacological
device which approved as FDA class I medical device (Tao & Bernacki, 2007). It
delivers continuous low-level heat to the low back and allow patients to remain

38
mobility when wear (Mayer et al., 2005).
4.6.2 Wearing a Heat wrap for approximately 8 hours continuously in the
daytime.
Heat wrap provides constant heat at 40OC for at least 8 hours continuously (Tao
& Bernacki, 2005; Mayer et al., 2005; Nadler et al., 2003a; Nadler et al., 2003b;
Nadler et al., 2002). There is no serious adverse effect occurred and the risk of
minor adverse effects is much lower when using in the daytime (Kettenmann et al.,
2007; Tao & Bernacki, 2005; Mayer et al., 2005; Nadler et al., 2003a; Nadler et al.,
2002).
4.6.3 Applying heat wrap for 2 consecutive days.
The duration of applying heat wrap therapy ranged from 2 to 5 consecutive
days (Kettenmann et al., 2007; Tao & Bernacki, 2005; Mayer et al., 2005; Nadler
et al., 2003a; Nadler et al., 2003b; Nadler et al., 2002). Using heat wrap for 2
consecutive days can exhibit significant pain relief with high level of evidence
(Nadler et al., 2002).

39
4.6.4 Routine assessment to evaluate effectiveness of heat wrap in pain
intensity for 4 consecutive days.
The heat wrap therapy has significant pain improvement in the first 4 days and
kept consistent afterwards (Kettenmann et al., 2007; Tao & Bernacki, 2005;
Mayer et al., 2005; Nadler et al., 2003a; Nadler et al., 2003b; Nadler et al., 2002).
Routine assessment allows nurses to examine the effectiveness which does not
increase their workload and prevents undesired adverse event.
4.6.5 Using Numeric Rating Scale to measure pain intensity for evaluation.
Pain intensity is a better indicator for showing the rate of change in pain (Tao &
Bernacki, 2005). Numeric Rating scale is a sensitive and reliable measurement for
pain. It is easier to use and available in current practice.

40
Chapter 5
Implementation Plan
After developing the evidence-based practice protocol, it comes to the
implementation. Before implementing the new intervention, we have to obtain
approval from the administrators. Besides, we have to explore and consider
solutions to any issues or problems that may arise during the implementation
process. Therefore, a thorough planning of communication with stakeholders and
the process of implementation is important and will be discussed in this chapter
5.1 Communication Plan
5.1.1 Identifying Stakeholders
Stakeholders are people who are interested in the program, have impact on the
implementation or affected by the proposed changes of the new interventions.
Initially, stakeholders should be identified and prioritized for interviews. The
stakeholders in this program include:
1. Administrators who are the decision maker: Ward Managers, Nurse
Consultant of Orthopaedics and Traumatology (O&T) (NC), Department
Operating Manager of O&T (DOM), Chief of Service of O&T (COS),

41
General Manager Nursing (GMN), Cluster Chief Executive (CCE)
2. Frontline Nurses who are the target users of the protocol: Nursing
Officer(NO), Advanced Practice Nurse (APN), Registered Nurse(RN),
Enrolled Nurse(EN)
3. Orthopaedics Doctors who are the supporter of the protocol by giving
prescription of the heat wrap therapy: Consultants, Assistant Consultants
(AC), Medical Officer (MO)
4. Physiotherapist who can be benefited from the intervention as their
workload will be reduced if the protocol worked out
5. Patients who can be benefited from the intervention
5.1.2 Forming Program Team
The program proposer cannot proceed the protocol alone. It is crucial to gain
support from others and form a team in order to facilitate communications.
The program team will involve 1 APN and 3RNs corresponding to different
targeted acute wards. A meeting will be held to introduce the current situation and
practice to treat low back pain, the affirming needs of developing new
interventions and details of heat wrap therapy supported by research finding.
Moreover, we will review the evidence-based protocol by discussing the

42
implementation potential and making compromise according to different ward
practice and the comments received from ward staff. Eventually, a program team
including 1 APN as the team advocator, 4 RNs including myself as team
coordinators, and a program proposer will be formed.
5.1.3 Process of Communication Plan
The process of communication can be divided into 3 phases which are initiation,
guiding and sustaining stages.
5.1.3.1 Initiation Stage
5.1.3.1.1 Communication plan with Ward Managers
The target setting of the intervention is 4 acute O&T wards. It is important to
obtain an approval from the ward managers first. Four RN team coordinators
should invite their respective ward managers for meetings. The APN team
advocator will be responsible for administration tasks such as reserving the
meeting venue, sending invitations and proposal to the concerned ward managers.
During the meeting, throughout materials should be presented, objectives be
explained and questions be answered. Details of the new intervention with
research support, the needs of change, the benefits of the new method, the

43
transferability and feasibility of the evidence-based protocol with budget plan.
The ward managers will share their ward situation and offer advices. The proposal
and guideline will then be revised and redistributed for approval. The APN team
advocator will then approach NC, DOM, Consultants and COS with the revised
proposal and seek their approval for presenting the new interventions during the
department meeting.
5.1.3.1.2 Communication plan with NC, DOM, Consultants and COS
The team advocator and the proposer will present the new, evidence-based
intervention at the department meeting. Every participant should receive a hard
copy of the proposal. The proposer will present data such as the admission rate of
low back pain by using figures and charts, the current treatment and the new
interventions with research support. The implementation potential, the benefits
and budget plan should also be explained in details. Furthermore, the proposer
will present the revised protocol and follow-up plans such as training workshop
for frontline nurses in applying the new intervention. The department meeting
should conclude with a sharing session for collecting comments and advice.
If this evidence-based protocol is endorsed, it will be sent to GMN and CCE by
DOM for seeking final approval and funding.

44
5.1.3.1.3 Communication plan with GMN and CCE
Although DOM has the responsibility of presenting the proposal to GMN and
CCE, the proposer has to take the initiative to present revised details of the new
intervention at the department conference. Meanwhile, the program team should
provide the necessary support and strategize solutions to any problems arise
throughout the process of communications.
5.1.3.1.4 Communication plan with Frontline Nurses and Physiotherapist
After obtaining all the required approval, it is essential to announce the
guidelines to frontline nurses and physiotherapist before implanting the pilot study.
A luncheon talks will be held in the theatre with compensation hours for
attendants. Poster of invitation will be displayed on the notice board in all acute
O&T wards as promotion. The vision, relevant details, benefits of the new
intervention and flow of protocol will be introduced during the session. A Q&A
sessions would be held for clarifying any misunderstanding and collecting
opinions.
5.1.3.1.5 Communication plan with Patients
The contents of heat wrap therapy and its benefit will be printed on leaflets
which would be placed on the information shelf for patients’ information. Nurse
staff should deliver and explain the contents of the leaflets before applying heat

45
wrap therapy.
5.1.3.2 Guiding Stage
The evidence-based protocol will be printed and distributed to targeted acute
ward setting. The protocol will also be uploaded to the department website for
referencing and a forum will be set up for opinions, information exchange and
answering any queries.
There are total 80 nurses responsible for executing the new interventions. Two
1-hour training workshops will be delievered. Each workshop will be held by 2
RN team coordinators including the proposer. Each nurse has to attend either
session. The training workshop will explain the contents of the protocol, the time
of measurement and its method. Moreover, the session will demonstrate the
method of using heat wrap therapy and re-demonstration session.
Four RN team coordinators are responsible for providing support or dealing
with any difficulties related to heat therapy faced by frontline nurses,
physiotherapist, as well as patients.
5.1.3.3 Sustaining Stage
Four RN team coordinators have to monitor any misfiling of patient’s charting,

46
for example pain scale chart and discharge date in admission statistical record, in
order to prevent missing data. They also have to monitor any adverse events
induced by heat therapy by collecting staff reporting or documentation. They are
responsible for encouraging frontline nursing staff to apply this heat therapy by
appreciation and giving positive reinforcement with evidence of patient’s
progress.
The proposer is responsible for monitoring the quantity of heat wrap to ensure
there is enough supply during the pilot test and estimating the demands in the
future. The team advocator has to collect feedback from ward managers, doctors
and physiotherapist. Regular meetings will be held by the program team
bi-weekly to follow up the progress and revise the protocol. Those meeting
minutes will be reported to DOM. The time frame of implementation plan is
attached in Appendix IX.
5.2 Pilot Study
Pilot Study plays an important role in implementing a new intervention. It is
used to test the feasibility of the intervention which intended to use in a larger
scale in the future. It helps in evaluating any modifications needed in the future
planning. (Leon, Davis & Kraemer, 2011)

47
5.2.1 Study Design
A Quasi-experimental design will be used in the pilot study.
5.2.2 Objectives
The objectives of the pilot study are:
1. Testing the feasibility of the superficial heat therapy guidelines
2. Assessing nurses’ attitude to new guidelines
3. Assessing patient’s satisfaction to the new interventions
4. Identifying any unpredictable problems or obstacles
5.2.3 Target Population and Program Intervention
The Superficial heat wrap therapy protocol will be executed in 4 acute O&T
wards, including 2 male and 2 female wards, within a public hospital.
Adult patients admitted with acute low back pain, ambulatory and cognitive
intact which are able to follow the instructions of using heat wrap therapy will be
recruited to the program. For female patients, only those with negative urine
pregnancy test will be recruited.

48
Patients with hypersensitivity to heat, evidence or history of neurologic deficit,
radiculopathy or spinal surgery, any skin lesions over lumbar region must be
excluded to the program.
The operational flow of superficial heat wrap therapy is attached in Appendix
X.
Sixteen eligible patients from 4 target ward settings will be recruited to the pilot
study. Considering the admission statistical record, the duration of pilot study will
be set at 1 month.
5.2.4 Outcomes Measurements
The following outcomes will be measured and evaluated, which are:
1. Pain intensity
2. Sleep quality
3. Nurse’s satisfaction level
4. Patient’s satisfaction level
5. Length of Hospital Stays

49
5.2.5 Evaluation of the guideline
After the pilot test, the program team will hold an evaluation meeting to discuss
the results of outcomes and feedback from various disciplines. The program team
will revise the protocol and offer suggestions. The revised protocol will then be
presented to ward managers and DOM during department meeting and final
decision will be announced by DOM.
Besides, the program team will evaluate the effectiveness of the measuring
tools and the feasibility of the measuring time. Although the risk of adverse effect
of heat wrap such as blister and erythema is low, an emergency plan has to be set
up including actions such as removing heat wrap immediately, soothing with cold
water and assessing by doctor for medication prescription if necessary.

50
Chapter 6
Evaluation Plan
An evaluation plan helps to clarify the measureable outcomes of program in
order to determine effectiveness of the program by the evaluation results.
Outcomes are identified from 3 different perspectives include patient, health care
provider and the health care system. The method and the timeframe for outcome
measurements are also to be decided. Furthermore the nature and number of
clients are determined. The data collected are analyzed with specified methods
and the basis of considering the effectiveness of program is compromised.
6.1 Identifying Outcomes and Outcomes Measurements
The outcomes of the protocol can be divided into 3 aspects: patient, healthcare
provider and the health care system.
6.1.1 Patient outcomes
The aim of the superficial heat wrap therapy protocol is to reduce acute low
back pain among adult patient which is supported by the 7 evidence-based studies.
(Kettenmann et al., 2007; Mayer et al., 2005; Tao & Bernacki, 2005; Nuhr et al.,
2004; Nadler et al., 2003a; Nadler et al., 2003b; Nadler et al., 2002) Therefore, the

51
primary outcome is pain intensity. Pain intensity will be measured by using the
0-10 Numeric Rating Scale in currently used pain chart which is attached in
Appendix XI.
Secondary outcome is the sleep quality. Although there is insufficient research
proved that heat therapy helps in improving sleep quality, (Tao & Bernacki, 2005;
Nadler et al., 2003b), this program determines to examine its effectiveness on
sleeping. Sleep quality will be assessed with the 6-point Verbal Rating Scale in
response to a question “How well did you sleep last night?” ; ranging from 0=
very poor to 5 = excellent (Nadler et al., 2003b).
Patient’s satisfaction is another secondary outcome and it will be reflected by
satisfaction level to the protocol. Satisfaction level will be assessed by using the
5-point Verbal rating scale ranging from” Not at all satisfied” from “Very
satisfied”. Comments from patients will also be evaluated if provided.
Both sleep quality and patient’s satisfaction level will be charted in a specific
assessment form which comprised by the program team. The assessment from is
attached in Appendix XII
6.1.2 Healthcare Provider Outcomes
Nurse’s satisfaction level will be assessed by ranking few statements in a

52
questionnaire ranging from “strongly disagree” to “strongly agree”. Those
questions can reflect their attitude towards the protocol. The questionnaire will be
set up by the program team and approved by DOM. The nurses’ evaluation
questionnaire is attached in Appendix XIII.
6.1.3 System Outcomes
Length of hospital stays will be evaluated by tracing the admission statistical
record at the end of the program. The reduction in the length of hospital stays
helps to prove the cost-effectiveness of the program.
6.2 Determining Nature and Number of Clients
6.2.1. Nature of Clients
According to the result of pilot study, there is no modification of requirement of
target population. The nature of clients is the same as those in the pilot study
which was mentioned in Chapter 5.
6.2.2 Sampling Method
Non-probability purposive sampling will be used in this program. Patients who

53
meet the inclusion criteria of the protocol are recruited.
6.2.3 Sample Size
The sample size is calculated by G*Power 3.1.9.2. In order to estimate sample
size, p-value, power, mean difference and standard deviation are adapted from
relevant studies (Kettenmann et al., 2007; Mayer et al., 2005; Tao & Bernacki,
2005; Nuhr et al., 2004; Nadler et al., 2003a; Nadler et al., 2003b; Nadler et al.,
2002).
Eventually, 41 participants are required for the program with medium effect
size (d=0.5) at the p≤0.05 level of significance with a power of 90% and attrition
rate of 10% in a one tailed test. The detail of calculation is attached in Appendix
XIV.
This program are used by all nurses, therefore the calculation of sample size of
nurses are not needed.
6.2.4 Duration of Program
According to the admission statistical record, the program will be carried out
for 2 months in order to collect sufficient data.

54
6.3 Data Collection and Method of Analysis
6.3.1 Data Analysis Designs
An intention-to-treat analysis was conducted among all subjects with any
efficacy data.
6.3.2 Time for Outcome Measurements
Pain intensity measurement is a daily routine. Pain intensity will be measured at
pre-intervention (Day 0) and 4 days post-intervention(Day 1-4). Sleep Quality
will be measured daily from Day 0 to Day 4. Patient’s satisfaction will be asked
on Day 4. Questionnaire for evaluating nurses’ satisfaction will be carried out
after the program. Length of Hospital stays of each patient will be traced at the
end of the program.
6.3.3 Method of Analysis
Statistical analytical software IBM SPSS Statistics 22.0 will be used for data
analysis. Patient’s demographic data will be presented by using descriptive
statistical method. The pain intensity and sleep quality will be tested by using 1

55
tailed paired t-test at the p≤0.05 significance level. Patient satisfaction and nurse
satisfaction will be analyzed by using descriptive statistical method. The mean of
length of hospitals stays will be calculated and compared with previous years.
6.4 Basis for an effective change of practice
The program of superficial heat therapy will be considered as successful if the
followings are achieved. Those achievements are based on relevant
evidence-based research studies and compromised by program team.
1. Pain intensity is reduced by over 3 points (Tao & Bernacki, 2005)
2. The mean of Sleep quality is scored at 3 or above (Nadler et al., 2003b)
3. 90% of nurses satisfied with the superficial heat protocol.
4. 80% of patients satisfied with the superficial heat protocol.
5. The mean of length of hospital stays is reduced by 2 days or more

56
Chapter 7
Conclusion
According to the reviewed studies, superficial heat therapy is proved as an
effective intervention in reducing pain among adult patients with acute low back
pain. Continuous low-level heat-wrap therapy is suggested as a safe,
non-pharmacological and cost-effective measure. Patients wearing heat-wrap
experienced better pain control than taking analgesic. Moreover, patients can
remain active to carry out physical exercise, daily living and maintain their quality
of life. However, heat wrap therapy is not a common practice in local public
hospital settings. In this regards, this translational nursing research is conducted to
develop an evidence-based guideline for nurses to provide high quality of care to
patients with acute low back pain.
The guidelines are based on the relevant data extracted from high quality of
research studies which critically appraised by Scottish Intercollegiate Guidelines
Network. The results suggested that the application of heat wrap therapy for 8
hours for 2 consecutive days in daytime is the most effective method in pain
reliefing among adult patients with acute low back pain.
After considering the implantation potential of the protocol, it is transferrable

57
and feasible to the proposed ward setting with clearly inclusion and exclusion
criteria. A plan of implantation and evaluation is also discussed in this paper for
implementing and evaluating the effectiveness of the guidelines. The newly
developed superficial heat therapy guidelines are beneficial to adult patients with
acute low back pain, by reducing their pain and reserving their quality of life, as
well as relieving the medical burden.
Sleep disturbance and insomnia are common associated problems of low back
pain. There is little evidence proved that heat wrap therapy improves quality of
sleep. Further studies investigating the effect of heat wrap therapy on sleep quality
is encouraged. Moreover, there is lacks of evidence-based research studies about
Superficial Heat Therapy to acute low back pain patients in Hong Kong. Further
investigations are encouraged as people gradually prefer non-pharmacological
approach which may become a new evolution towards current health care system.

58
Appendix I: History of Searching Studies
Date of search: 18/6/2013 Database searched
Pubmed CINAHL via
EBSCOHOST
British
Nursing
Index via
Proquest
Search Terms
Low back pain or
Back pain or
Acute low back pain
44683 8174 609
Superficial heat therapy or Heat therapy or
Hot therapy or Thermotherapy or
Heat treatment or Heat management or
Heat or Hot or Heat pack or Hot pack or
Heat pads or Hot pads or Heat wrap or
Heatwrap or Continuous thermotherapy or
Continuous heat therapy or
Continuous hot therapy or Warm or
Warming
300705 23661 542
Pain or
pain management or
pain measurement or
pain intensity or
pain scale
536773 80062 8011
AND 673 106 10
Limit to year 2002 - 2013 414 89 6
Limit to RCT 92 26 1
Screened by title or abstract 13 2 0
Screened by full text 7 0 0
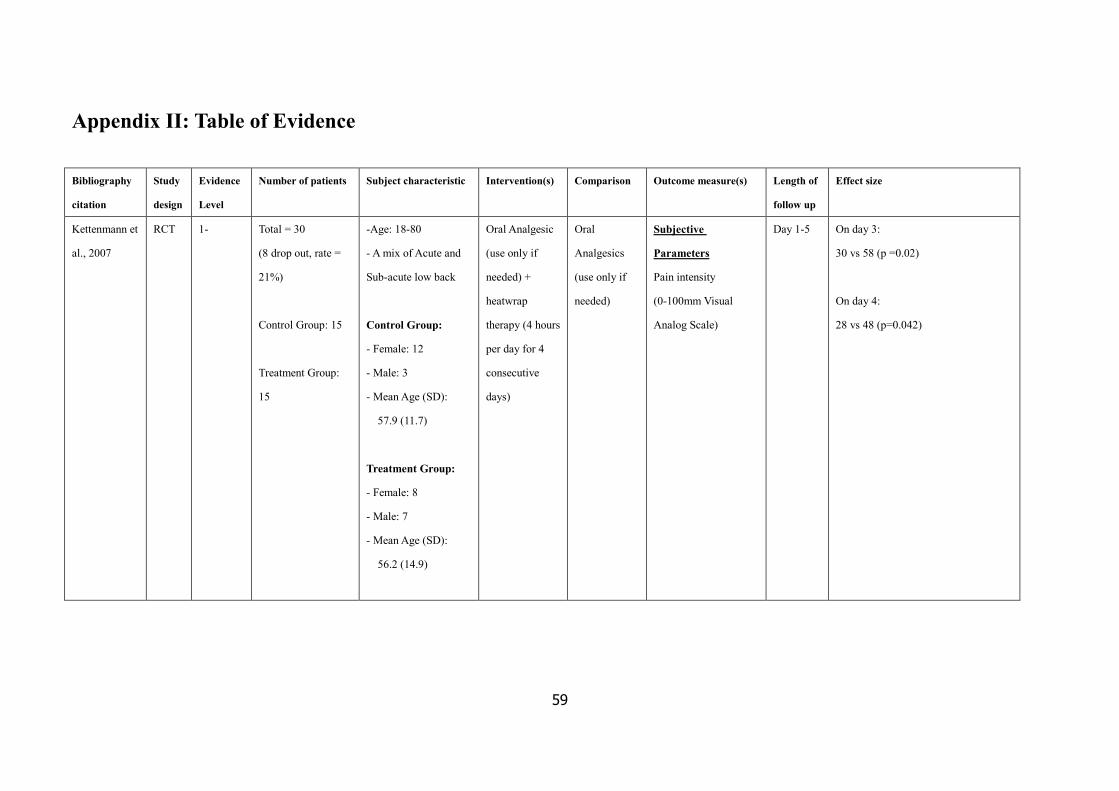
59
Appendix II: Table of Evidence
Bibliography
citation
Study
design
Evidence
Level
Number of patients Subject characteristic Intervention(s) Comparison Outcome measure(s) Length of
follow up
Effect size
Kettenmann et
al., 2007
RCT 1- Total = 30
(8 drop out, rate =
21%)
Control Group: 15
Treatment Group:
15
-Age: 18-80
- A mix of Acute and
Sub-acute low back
Control Group:
- Female: 12
- Male: 3
- Mean Age (SD):
57.9 (11.7)
Treatment Group:
- Female: 8
- Male: 7
- Mean Age (SD):
56.2 (14.9)
Oral Analgesic
(use only if
needed) +
heatwrap
therapy (4 hours
per day for 4
consecutive
days)
Oral
Analgesics
(use only if
needed)
Subjective
Parameters
Pain intensity
(0-100mm Visual
Analog Scale)
Day 1-5 On day 3:
30 vs 58 (p =0.02)
On day 4:
28 vs 48 (p=0.042)

60
Bibliography
citation
Study
design
Evidence
Level
Number of patients Subject characteristic Intervention(s) Comparison Outcome measure(s) Length of
follow up
Effect size
Tao X. &
Bernacki, E.J.,
2005
RCT 1+ Total = 43
Control Group: 18
Treatment Group:
25
-Age: 20-62
-A mix of Acute and
Sub-acute low back
Control Group:
- Female: 15
- Male: 3
- Average Age: 35
Treatment Group:
- Female:21
- Male: 4
- Average Age: 36.2
Education +
Heat Wrap ( 8
hours per day
for 3
consecutive
days)
Education Primary Outcome:
1. Pain Intensity (0 -10
Numeric Rating
Scale)
2. Pain Relief (6-point
Verbal Rating
Scale)
Day 1-3
Day 4,
Day 7,
Day 14
1.
Day Difference
(95%CI)
p-
value
1 -1.73 (-2.83,-0.65) 0.0029
2 -1.43 (-2.70,-0.16) 0.0293
3 -2.33 (-3.73,-0.94) 0.0019
4 -1.78 (-3.31,-0.26) 0.0237
7 -1.69 (-3.18, -0.21) 0.0257
14 -1.75 (-3.33, -0.18) 0.0305
2.
Day Difference
(95%CI)
p-
value
1 1.55 (0.58,2.52) 0.0027
2 0.73 (-0.05,1.51) 0.0631
3 1.40 (0.54,2.25) 0.0022
4 1.13 (0.11,2.14) 0.0299
7 0.63 (-0.47.1.72) 0.2491
14 0.80 (-0.33,1.93) 0.1567

61
Bibliography
citation
Study
design
Evidence
Level
Number of patients Subject characteristic Intervention(s) Comparison Outcome measure(s) Length of
follow up
Effect size
Mayer et al.,
2005
RCT 1+ Total: 100
(Dropped:8, rate:
8%)
Heat Wrap Group: 25
(Completed: 22
Dropped: 3)
Exercise Group: 25
(Completed: 24
Dropped: 1)
Heat + Exercise
Group: 24
(Completed: 21
Dropped: 3)
Control Group: 26
(Completed: 25
Dropped: 1)
-Age: 18-55
- A mix of Acute and
Sub-acute low back
Heat Wrap Group:
Female: 17 Male: 8
Age (SD): 29.3 (9.9)
Exercise Group:
Female: 15 Male: 10
Age (SD): 32.6 (10.3)
Heat + Exercise
Group:
Female: 15 Male: 9
Age (SD): 31.8 (11.8)
Control Group
Female: 24 Male: 2
Age (SD): 31.2 (10.9)
Heat Wrap
Group: Heat
Wrap for 8 hours
per day for 5
consecutive days
Exercise Group:
Directional
Preference-based
exercise once
every hour while
awake for 5
consecutive days
Heat + Exercise
Group:
Heat wrap for 8
hours per day and
exercise once
every hour while
awake for 5
consecutive days
Educational
Booklet
Secondary Outcome:
Pain Relief
(6-point Verbal Rating
Scale)
Day 2
Day 4
Day 7
Day 2:
No significant difference (p=0.111)
Day 4:
Heat wrap vs Education
1.9 vs 0.8 (p=0.026)
Pain relief score difference: 1.1
Heat + Exercise vs Education.
2.5vs 0.8 (p=0.000)
Pain relief score difference: 1.7
Day 7:
Heat + Exercise vs Exercise
3.2 vs 2 (p=0.007)
Pain relief score difference: 1.2
Heat + Exercise vs Education
3.3 vs 1.3 (p<0.001)
Pain relief score difference: 2
Incidience of pain relief:
Heat + Exercise vs Education
95.2% vs 40% (p=0.003; odds
ratio=29.85)

62
Bibliography
citation
Study
design
Evidence
Level
Number of patients Subject characteristic Intervention(s) Comparison Outcome measure(s) Length of
follow up
Effect size
Nuhr et al.,
2004
RCT 1+ Total: 90
(10 drop out, rate =
9%)
Active warming
group : 47
Passive warming
group: 43
-Age >19 years old
- Acute low back pain
Active warming group:
Female: 21
Male : 26
Age (SD) : 36.8 (8.2)
Passive Warming group:
Female: 12
Male: 31
Age (SD) : 41.7 (12)
Heating blanket
with 42 oC
Woolen
blanket
Pain Intensity
(0-100mm Visual
Analog Scale)
--- Active Warming group:
74.2 (95% CI, 71.7-76.7) to
41.9 (95% CI, 36.5-47.5)
(p<0.01)
Passive warming group:
73.3 (95% CI, 69.7-76.9) to
74.1 (95% CI, 70.4-77.8)
Pain score mean difference:
-32.3 vs +0.8

63
Bibliography
citation
Study
design
Evidence
Level
Number of
patients
Subject characteristic Intervention(s) Comparison Outcome measure(s) Length of
follow up
Effect size
Nadler et al.,
2003a
RCT 1+ Total: 219
(Dropped: 24,
Rate :10.9)
Heat wrap group:
95
(Completed: 92
Dropped: 3)
Oral Placebo: 96
(Completed: 88
Dropped: 8)
(For Blinding)
Oral Ibuprofen: 12
(For Blinding)
Unheated Wrap:
16
(Completed:15
Dropped: 1)
-Age: 18-55
- A mix of Acute and
Sub-acute Low Back
Pain
Heat wrap group:
Age (SD): 35.55 (11.57)
Oral Placebo:
Age (SD): 36.73 (10.82)
Oral Ibuprofen:
Age (SD): 36.25 (11.56)
Unheated Wrap:
Age (SD): 34.88 (11.32
Heat wrap for 8
hours per day for 3
consecutive days
Oral Placebo
-2 tablets for 3 times
per day with 6 hour
apart for 3
consecutive days
Oral Ibuprofen
- 2oomg x 2 tablets
for 3 times per day
with 6 hour apart for
3 consecutive days
Unheated wrap
8 hours per day for 3
consecutive days
Primary Outcome:
Pain relief
(6-point Verbal Rating
Scale)
Day 1-5 On Day 1:
1.76 +/- 0.10 vs 1.05 +/- 0.11 (p<0.001)
Pain relief score difference:
0.61
Incidence of complete pain relief over
1-5 days:
15.4% vs 6.6% (p=0.04; odd ratio =
2.89)
On days 4 and 5:
2.5 +/- 0.16 vs 1.56 +/- 0.18 (p<0.0001)
Pain relief score difference:
0.94

64
Bibliography
citation
Study
design
Evidence
Level
Number of patients Subject characteristic Intervention(s) Comparison Outcome
measure(s)
Length of
follow up
Effect size
Nadler et al.,
2003b
RCT 1+ Total: 76
(Dropped: 6,
Rate :7.8%)
Heat wrap group: 33
(Completed: 31
Dropped: 2)
Oral Placebo: 34
(Completed: 32
Dropped: 2)
(For Blinding)
Oral Ibuprofen: 4
(For Blinding)
Unheated Wrap: 5
(Completed:3
Dropped: 2)
-Age: 18-55
-A mix of Acute and
Sub-acute Low Back Pain
Heat wrap group:
Female: 21 Male: 12
Age (SD): 42.21 (9.38)
Oral Placebo:
Female: 21 Male:13
Age (SD): 41.53 (9.76)
Oral Ibuprofen:
Female:3 Male: 1
Age (SD): 42.5 (2.65)
Unheated Wrap:
Female: 4 Male: 1
Age (SD): 34 (8.37)
Heat wrap for 8
hours during
sleep for 3
consecutive
nights
Oral Placebo
-2 tablets 15-20mins before
sleep for 3 consecutive nights
Oral Ibuprofen
- 2oomg x 2 tablets
15-20mins before sleep for 3
consecutive nights
Unheated wrap
8 hours during sleep for 3
consecutive nights
Primary Outcome:
1) Morning Pain
relief
(6-point Verbal
Rating Scale)
Secondary Outcome:
2) Mean Daytime
Pain relief
(6-point Verbal
Rating Scale)
3) Mean extended
Pain relief
(6-point Verbal
Rating Scale)
Day 2-5 1) 2.75 +/- 0.25 vs 1.45 +/- 0.23
(p<0.00005)
Pain relief score difference:
0.7
2) 2.69 +/- 0.24 vs 1.46 +/- 0.23
(p<0.00005)
Pain relief score difference:
1.23
3) 2.90 +/- 0.29 vs 1.60 +/- 0.27
(p<0.0001)
Pain relief score difference:
1.3

65
Bibliography
citation
Study
design
Evidence
Level
Number of patients Subject characteristic Intervention(s) Comparison Outcome
measure(s)
Length of
follow up
Effect size
Nadler et al.,
2002
RCT 1+ Total: 371
(Dropped: 8,
Rate :2.16%)
Heat wrap group: 113
(Completed: 111
Dropped: 2)
Acetaminophen: 113
(Completed: 111
Dropped: 2)
Ibuprofen: 106
(Completed: 102
Dropped: 4)
(For Blinding)
Oral Placebo :20
(For Blinding)
Unheated Wrap: 19
-Age: 18-55
- A mix of Acute and
Sub-acute Low Back Pain
Heat wrap group:
Female: 66 Male: 47
Age (SD): 35.82 (10.54)
Oral Acetaminophen:
Female: 64 Male: 49
Age (SD): 34.9 (11.29)
Oral Ibuprofen:
Female: 63 Male: 43
Age (SD): 36.61 (10.4)
Oral Placebo:
Female: 12 Male: 8
Age (SD): 38.00 (9.07)
Unheated Wrap:
Female: 11 Male: 8
Age (SD): 36.79 (9.32)
Heat wrap for 8
hours per day for 2
consecutive days
Acetaminophen
- 2 tablets for 4 times
per day for a total dose
of 4000mg for 2
consecutive days
Ibuprofen
- 200 mg x 2 tablets for
3 times per day for total
dose of 1200mg + 2
tablets placebo for 1
time per day for
blinding for 2
consecutive days
Oral Placebo
- 2 tablets for 4 times
per day for 2
consecutive days
Unheated wrap
8 hours per day for 2
consecutive days
Primary Outcome:
Pain relief
(6-point Verbal
Rating Scale)
Day 1-4 Heat vs Acetaminophen vs
ibuprofen
On Day 1:
2 vs 1.32 (p=0.0001) vs 1.51
(p=0,0007)
Pain relief score difference:
0.68 and 0.49
On Day 2:
2.78 vs 2 (p=0.0001) vs 2.06
(p=0.0001)
Pain relief score difference:
0.78 and 0.72
Day 3-4:
2.61 vs 1.95 (p=0.0009) vs 1.68
(p=0.0001)
Pain relief score difference:
0.66 and 0.93

66
Appendix III: Methodology Checklists
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Kettenmann B., Wille C., Lurie-Luke E., Walter D. & Kobal G. (2007). Impact of Continuous Low
Level Heatwrap Therapy in Acute Low Back Pain Patients: Subjective and Objective
Measurements. Clin J Pain, 23(8), 663-668. doi: 10.1097/AJP.0b013e31813543ef
Guideline topic: Superficial Heat Therapy in pain relieving
for patients with low back pain
Key Question No:
N/A
Reviewer:
LAI TSZ NING
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study� Does this study do it?
1.1 The study addresses an appropriate and clearly focused question
Yes ����
Can’t say �
No �
1.2 The assignment of subjects to treatment groups is randomised
Yes �
No �
Can’t say ����
Reported but method
not described
1.3 An adequate concealment method is used
Yes �
Can’t say �
No ����
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
Yes �
Can’t say �
No ����
1.5 The treatment and control groups are similar at the start of the trial. Yes �
Can’t say
����
No �
1.6 The only difference between groups is the treatment under
investigation.
Yes ����
Can’t say �
No �
1.7 All relevant outcomes are measured in a standard, valid and reliable
way.
Yes ����
Can’t say �
No �

67
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was
completed?
21%
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).
Yes � � � � No �
Can’t say � Does not
apply �
Per protocol Analysis
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Yes �
Can’t say �
No �
Does
not
apply ����
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows.
High quality (++)�
Acceptable (+)����
Unacceptable – reject 0 �
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain
that the overall effect is due to the study
intervention?
Yes.
Sex distribution was not even between
groups. Greater number of female in
control group
Small sample size with about 20% drop
out rate
2.3 Are the results of this study directly applicable to
the patient group targeted by this guideline?
yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of
the study, and the extent to which it answers your question and mention any areas of
uncertainty raised above.
Heatwrap Therapy was effective in reducing pain and better night’s sleep. No significant
difference in use of oral analgesics but a trend toward less use in heatwrap group.

68
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Tao X. & Bernacki E.J. (2005). A Randomized Clinical Trial of Continuous Low-level Heat
Therapy for Acute Muscular Low Back Pain in the Workplace. J Occup Environ Med, 47(12),
1298-1306. doi: 10.1097/01.jom.0000184877.01691.a3
Guideline topic: Superficial Heat Therapy in pain relieving
for patients with low back pain
Key Question No:
N/A
Reviewer:
LAI TSZ NING
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study� Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
Yes ����
Can’t say �
No �
1.2 The assignment of subjects to treatment groups is randomised.
Yes �
No �
Can’t say ����
Reported but method
not described
1.3 An adequate concealment method is used.
Yes �
Can’t say �
No ����
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
Yes ����
Can’t say �
No �
1.5 The treatment and control groups are similar at the start of the trial. Yes ����
Can’t say �
No �
1.6 The only difference between groups is the treatment under
investigation.
Yes ����
Can’t say �
No �
1.7 All relevant outcomes are measured in a standard, valid and reliable
way.
Yes ����
Can’t say �
No �
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was
completed?
0 %

69
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).
Yes ����
Can’t say �
No �
Does not
apply �
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Yes �
Can’t say �
No �
Does
not
apply ����
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++)�
Acceptable (+)����
Unacceptable – reject 0 �
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain
that the overall effect is due to the study
intervention?
Yes.
Risk of Bias: Single Blinding
(Participants)
2.3 Are the results of this study directly applicable to
the patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of
the study, and the extent to which it answers your question and mention any areas of
uncertainty raised above.
Heat wrap therapy had significantly reduced pain intensity from day 1 to day 14. Heat
wrap therapy had increased pain relief from day 1 to day 4. Although no significant
difference on day 7 and day 14 on pain relief, it is less useful as the pain intensity was
reduced dramatically at the beginning to a low level and kept consistent afterwards.

70
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Mayer J. M., Raplh L., Look M., Erasala G. N., Verna J. L., Matheson L. N. & Mooney V. (2005).
Treating acute low back pain with continuous low-level heat wrap therapy and/or exercise: a
randomized controlled trial. The Spine Journal, 5(4), 395-403. doi:10.11016/j.spinee.2005.03.009
Guideline topic: Superficial Heat Therapy in pain relieving
for patients with low back pain
Key Question No:
N/A
Reviewer:
LAI TSZ NING
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study� Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
Yes ����
Can’t say �
No �
1.2 The assignment of subjects to treatment groups is randomised.
Yes � � � � No �
Can’t say �
Computer-generated
sheet
1.3 An adequate concealment method is used.
Yes �
Can’t say �
No ����
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
Yes �
Can’t say �
No ����
1.5 The treatment and control groups are similar at the start of the trial. Yes �
Can’t say ����
No �
1.6 The only difference between groups is the treatment under
investigation.
Yes ����
Can’t say �
No �
1.7 All relevant outcomes are measured in a standard, valid and reliable
way.
Yes ����
Can’t say �
No �
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was
completed?
Total: 8%
Heat Wrap : 12%
Exercise: 4%
Heat + Exercise: 12.5%
Control: 3.8 %

71
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).
Yes ����
Can’t say �
No �
Does not
apply �
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Yes ����
Can’t say �
No �
Does not
apply �
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++)�
Acceptable (+)����
Unacceptable – reject 0 �
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain
that the overall effect is due to the study
intervention?
Yes.
Risk of Bias: No Blinding, Gender
imbalance in control group but similar
gender characteristics
2.3 Are the results of this study directly applicable to
the patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of
the study, and the extent to which it answers your question and mention any areas of
uncertainty raised above.
No significance difference at day 2. Heat wrap was significantly greater than education in
pain relief at day 4. Heat wrap plus exercise was greater than exercise or education at
day 7 with significant difference

72
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Nuhr M., Hoerauf K., Bertalanffy A., Bertalanffy P., Frickey N., Gore C., Gustorff B. & Kober A.
(2004). Active warming During Emergency Transport Relieves Acute Low Back Pain. Spine,
29(14), 1499-1503. Retrieved from
http://ovidsp.tx.ovid.com.eproxy1.lib.hku.hk/sp-3.8.1a/ovidweb.cgi?T=JS&PAGE=fulltext&D
=ovft&AN=00007632-200407150-00002&NEWS=N&CSC=Y&CHANNEL=PubMed
Guideline topic: Superficial Heat Therapy in pain relieving
for patients with low back pain
Key Question No:
N/A
Reviewer:
LAI TSZ NING
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study� Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
Yes ����
Can’t say �
No �
1.2 The assignment of subjects to treatment groups is randomised.
Yes � � � � No �
Can’t say �
Computer-generated
codes
1.3 An adequate concealment method is used.
Yes � � � � No �
Can’t say �
Opaque Envelope
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
Yes ����
Can’t say �
No �
1.5 The treatment and control groups are similar at the start of the trial. Yes ����
Can’t say �
No �
1.6 The only difference between groups is the treatment under
investigation.
Yes ����
Can’t say �
No �
1.7 All relevant outcomes are measured in a standard, valid and reliable
way.
Yes � � � � No �
Can’t say �
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was
Total: 9%
Active warming: 6%

73
completed? Passive warming: 14%
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).
Yes � � � � No �
Can’t say � Does not
apply �
Per protocol analysis
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Yes �
Can’t say �
No �
Does
not
apply ����
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++)�
Acceptable (+)����
Unacceptable – reject 0 �
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain
that the overall effect is due to the study
intervention?
Yes.
Single blind: investigator
2.3 Are the results of this study directly applicable to
the patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of
the study, and the extent to which it answers your question and mention any areas of
uncertainty raised above.
Active Warming provide better pain relief and reduce anxiety than passive warming
during rescue transport

74
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Nadler S. F., Steiner D. J., Abeln S. B., Erasala G. N., Hengehold D. A. & Weingand K.W. (2003a).
Continuous low-level heatwrap therapy for treating acute nonspecific low back pain. Arch
Phys Med Rehabil, 84(3), 329-334. doi: 10.1053/apmr.2003.50102
Guideline topic: Superficial Heat Therapy in pain relieving
for patients with low back pain
Key Question No:
N/A
Reviewer:
LAI TSZ NING
Before completing this checklist, consider:
1. Is the paper a randomised controlled trial or a controlled clinical trial? If in doubt, check the
study design algorithm available from SIGN and make sure you have the correct checklist. If it is
a controlled clinical trial questions 1.2, 1.3, and 1.4 are not relevant, and the study cannot be
rated higher than 1+
2. Is the paper relevant to key question? Analyse using PICO (Patient or Population Intervention
Comparison Outcome). IF NO REJECT (give reason below). IF YES complete the checklist.
Reason for rejection: 1. Paper not relevant to key question � 2. Other reason � (please specify):
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study� Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
Yes ����
Can’t say �
No �
1.2 The assignment of subjects to treatment groups is randomised.
Yes �
No �
Can’t say ����
Reported but method
not described
1.3 An adequate concealment method is used.
Yes �
Can’t say �
No ����
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
Yes ����
Can’t say �
No �

75
1.5 The treatment and control groups are similar at the start of the trial. Yes �
Can’t say ����
No �
1.6 The only difference between groups is the treatment under
investigation.
Yes ����
Can’t say �
No �
1.7 All relevant outcomes are measured in a standard, valid and reliable
way.
Yes ����
Can’t say �
No �
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was
completed?
Total: 10.9%
Heat wrap :3.15%
Oral Placebo: 8.3%
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).
Yes ����
Can’t say �
No �
Does not
apply �
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Yes �
Can’t say ����
No �
Does not
apply �
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++)�
Acceptable (+)����
Unacceptable – reject 0 �
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain
that the overall effect is due to the study
intervention?
Yes.
Single blind: investigator
No gender described among groups
2.3 Are the results of this study directly applicable to
the patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of
the study, and the extent to which it answers your question and mention any areas of
uncertainty raised above.
1. No serious adverse events occurred. 1 subject in heat wrap group was found
progressed to definite redness on day 5 which resolved without treatment.
2. Pain relief over Day 1-5 was significantly greater for the heat wrap compared with
placebo

76
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Nadler S. F., Steiner D. J., Petty S. R., Erasala G. N., Hengehold D. A. & Weingand K.W. (2003b). Overnight
Use of Continuous Low-level Heatwrap Therapy for Relief of Low Back Pain. Arch Phys Med Rehabil,
84(3), 335-342. doi: 10.1053/apmr.2003.50103
Guideline topic: Superficial Heat Therapy in pain relieving
for patients with low back pain
Key Question No:
N/A
Reviewer:
LAI TSZ NING
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study� Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
Yes ����
Can’t say �
No �
1.2 The assignment of subjects to treatment groups is randomised.
Yes �
No �
Can’t say ����
Reported but method
not described
1.3 An adequate concealment method is used.
Yes �
Can’t say �
No ����
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
Yes ����
Can’t say �
No �
1.5 The treatment and control groups are similar at the start of the trial. Yes ����
Can’t say �
No �
1.6 The only difference between groups is the treatment under
investigation.
Yes ����
Can’t say �
No �
1.7 All relevant outcomes are measured in a standard, valid and reliable
way.
Yes ����
Can’t say �
No �
1.8 What percentage of the individuals or clusters recruited into each
treatment arm of the study dropped out before the study was
completed?
Total: 7.8%
Heat wrap :6%

77
Oral Placebo: 5.8%
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).
Yes ����
Can’t say �
No �
Does not
apply �
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Yes ����
Can’t say �
No �
Does not
apply �
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++)�
Acceptable (+)����
Unacceptable – reject 0 �
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain
that the overall effect is due to the study
intervention?
Yes.
Single blind: investigator
2.3 Are the results of this study directly applicable to
the patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of
the study, and the extent to which it answers your question and mention any areas of
uncertainty raised above.
1. Mild erythema without blister formation was noted in 4 subjects who wore the heat
wrap but resolved without intervention
2. The heat wrap group had significantly greater pain relief after 3 nights of treatment
compared with placebo and had extended pain relief 8 hours after waking and on day 4
and 5.

78
S I G N
Methodology Checklist 2: Controlled Trials
Study identification (Include author, title, year of publication, journal title, pages)
Nadler S. F., Steiner D. J., Erasala G. N., Hengehold D. A., Hinkle R. T., Goodale M. B., Abeln S. B.
& Weingand K. W. (2002). Continuous low-level heat wrap therapy provides more efficacy than
ibuprofen and Acetaminophen for acute low back pain. Spine, 27(10), 1012-1017. Retrieved
from
http://ovidsp.tx.ovid.com.eproxy1.lib.hku.hk/sp-3.8.1a/ovidweb.cgi?T=JS&PAGE=fulltext&D=
ovft&AN=00007632-200205150-00003&NEWS=N&CSC=Y&CHANNEL=PubMed
Guideline topic: Superficial Heat Therapy in pain relieving
for patients with low back pain
Key Question No:
N/A
Reviewer:
LAI TSZ NING
SECTION 1: INTERNAL VALIDITY
In a well conducted RCT study� Does this study do it?
1.1 The study addresses an appropriate and clearly focused question.
Yes ����
Can’t say �
No �
1.2 The assignment of subjects to treatment groups is randomised.
Yes �
No �
Can’t say ����
Reported but method
not described
1.3 An adequate concealment method is used.
Yes �
Can’t say �
No ����
1.4 Subjects and investigators are kept ‘blind’ about treatment
allocation.
Yes ����
Can’t say �
No �
1.5 The treatment and control groups are similar at the start of the trial. Yes ����
Can’t say �
No �
1.6 The only difference between groups is the treatment under
investigation.
Yes ����
Can’t say �
No �
1.7 All relevant outcomes are measured in a standard, valid and reliable
way.
Yes ����
Can’t say �
No �
1.8 What percentage of the individuals or clusters recruited into each Total: 2.16%

79
treatment arm of the study dropped out before the study was
completed?
Heat wrap :1.77%
Oral Acetaminophen:
1.77%
Oral Ibuprofen: 3.78%
1.9 All the subjects are analysed in the groups to which they were
randomly allocated (often referred to as intention to treat analysis).
Yes ����
Can’t say �
No �
Does not
apply �
1.10 Where the study is carried out at more than one site, results are
comparable for all sites.
Yes ����
Can’t say �
No �
Does not
apply �
SECTION 2: OVERALL ASSESSMENT OF THE STUDY
2.1 How well was the study done to minimise bias?
Code as follows:
High quality (++)�
Acceptable (+)����
Unacceptable – reject 0 �
2.2 Taking into account clinical considerations, your
evaluation of the methodology used, and the
statistical power of the study, are you certain
that the overall effect is due to the study
intervention?
Yes.
Single blind: investigator
2.3 Are the results of this study directly applicable to
the patient group targeted by this guideline?
Yes
2.4 Notes. Summarise the authors’ conclusions. Add any comments on your own assessment of
the study, and the extent to which it answers your question and mention any areas of
uncertainty raised above.
1. No serious adverse events occurred. 1 subject in heat wrap group was found minor
redness on day 1 which resolved 1 hour after removal of wrap.
2. Pain relief was significantly greater for the heat wrap and has higher extended pain
relief compared with oral acetaminophen and oral ibuprofen.

80
Appendix IV: SIGN Grading System 1999-2012

81
Appendix V: Summary table of Levels of Evidence of
relevant studies
Bibliography citation Study design Evidence Level
Kettenmann et al., 2007 RCT 1-
Tao X. & Bernacki, E.J., 2005a RCT 1+
Mayer et al., 2005b RCT 1+
Nuhr et al., 2004 RCT 1+
Nadler et al., 2003a RCT 1+
Nadler et al., 2003b RCT 1+
Nadler et al., 2002 RCT 1+

82
Appendix VI: Cost for Implementation of protocol
Set up Item Cost Operational Item Cost
Staff Training Workshop Venue Free / /
Computer Component + Stationary Free / /
2 RN Trainer Compensate
Hour x 2
/ /
Subtotal $16 Subtotal $0
Superficial Heat
Therapy
Heat wrap ($8 x 1300) $10400 Store Room Free
Patient’s Educational Leaflets ($0.2 x 600^) $120 Training Staff Salary Free (During
routine work)
Pain Chart Free
(Available in
ward setting)
/ /
Subtotal $10520 Subtotal $0
Total Set up Cost $10526 Total Operational Cost $0
Total $10526
Remarks:
# All costs are calculated in HK Dollars
* Attendance of Workshop: 80 responsible nurses
^ 600 patients each year receiving superficial heat therapy

83
Appendix VII: Comparison of the cost between Current Practice and Superficial Heat Therapy
Item Unit Cost Item Unit Cost
Maintaining
Current Practice
Hospital Fee
($4900 x 7 days)
$34300 Superficial Heat
Therapy
Hospital Fee
($4900 x 5 days)
$24500
Tramadol^ ($0.32/tab x 4) x
20 days*
$25.6 Heat wrap ($8 x 2) $16
Pepcidine^ ($0.06/tab x 2) x
20 days
$2.4 Educational Leaflets $0.2
Voltaren^ ($0.08/tab x 2) x
20 days
$3.2 / /
Total $34331.2 Total $24516.2
Remarks:
# All costs are calculated in HK Dollars
^ Additional Medicine regimen: Tramadol 50mg TDS + Nocte po, Pepcidine 20 mg BD po, Voltaren 25 mg BD po
* 6 days (During Hospitalization) and 14 days (Discharge medication till FU)

84
Appendix VIII: SIGN Grading System 1999 – 2012:
Grades of recommendations
At least one meta-analysis, systematic review, or RCT rated as 1++, and
directly applicable to the target population; or
A body of evidence consisting principally of studies rated as 1+, directly
applicable to the target population, and demonstrating overall consistency of
results
A body of evidence including studies rated as 2++, directly applicable to the
target population, and demonstrating overall consistency of results; or
Extrapolated evidence from studies rated as 1++ or 1+
A body of evidence including studies rated as 2+, directly applicable to the
target population and demonstrating overall consistency of results; or
Extrapolated evidence from studies rated as 2++
Evidence level 3 or 4; or
Extrapolated evidence from studies rated as 2+

85
Appendix IX
Timeframe for Superficial Heat Therapy Program for acute Low Back Pain
Gantt chart for Implementation Plan
Week 1-4 5-8 9-14 15-21 22-23 24-25 26-30 31-34 35-36 37-38 39-47 48-52
Forming Program Team X
Communication with Ward Managers X
Communication with NC, DOM,
Consultants and COS
X
Communication with GMN and CCE X
Program team meeting for revision X X X
Announcement to frontline nurse and
physiotherapist
X
2 Training workshops X
Announcement to Patients X
Pilot Test X
Analysis for collected data X
Department meeting for evaluation X
Full implementation of the program X
Analysis for collected data; evaluate and
report the results
X

86
Appendix X
Operational Flow of Superficial Heat therapy in Pilot Test
Day 0:
- Recruiting eligible patient following the guidelines
- Explaining the details of superficial heat therapy
- Getting verbal consent
- Assessing patient’s skin integrity before applying
- Obtaining baseline data of pain intensity and sleep quality
- Applying 1st heat wrap at daytimes for 8 hours only
- Regular Assessment and taking pain score during routine work
Day 1:
- Assessing sleep quality daily
- Continue assessing pain intensity level routinely
- Applying 2nd heat wrap at daytimes for 8 hours only
- Assessing any adverse events
Day 2-3:
- Continuing assessing pain intensity level and sleep quality
Day 4:
- Continuing assessment pain intensity level and sleep quality
- Assessing patient’s satisfaction level
-

87
Appendix XI
Pain Chart

88
Appendix XII
Assessment chart for Patient using Superficial Heat therapy
Department of Orthopaedics and
Traumatology
Superficial Heat Therapy
Assessment Chart
Name:
HKID:
HN No:
Sex/D.O.B.:
(Please affix HN label)
Sleep Quality Day 0 Day 1 Day 2 Day 3 Day 4
Date:
1. How well did
you sleep last
night?
(Verbal Rating
Scale)
0 = Very poorly
1 = poorly
2 = fair
3 = well
4 = very well
5= excellent
� Please complete the following assessment on Day 4
� Please circle the appropriate box
2. How satisfied
were you with
this therapy?
Very
Dissatisfied
Dissatisfied
Neutral
Satisfied
Very
Satisfied
3. Other
Comments:
(Optional)

89
Appendix XIII
Nurses’ Evaluation form for Superficial Heat Therapy Program
Department of Orthopaedics and Traumatology
Evaluation Form on Superficial Heat Therapy
Program
Name: (optional)
Rank:
*Please indicate your level of agreement with this statement
Strongly
Disagree
Disagree Neutral Agree Strongly
Agree
1. The content of
protocol is clear to
understand.
2. The protocol is easy
to follow
3. The workload is
acceptable.
4. Change is necessary
in my workplace
5. I feel that my
professionalism is
developing
6. I am satisfied with
the protocol
7. Other Comments:
(Optional)

90
Appendix XIV
Calculation of Sample Size
P-value is set at 0.05 which the result can be considered as significant difference. 5
studies set power from 80% to 90%, but 2 studies did not provide the value.( Mayer et
al., 2005; Nuhr et al., 2004; Nadler et al., 2003a; Nadler et al., 2003b; Nadler et al.,
2002) Therefore, Power will be set at 90% for the sake for more stringent result.
Mean difference and standard deviation are obtained from the study of Tao &
Bernacki (2005) as the outcome measure is same as the one used in this protocol.
According to the result of Tao & Bernacki (2005), the mean difference is 1.1.
However, standard deviation is not provided in the study. Pain intensity score is
chatted by using a 10-point Numeric Rating Scale, the standard deviation on a
10-point scale is 50% of the maximum possible variation. Standard deviation is 2.235
which obtained by calculation.
The mean of dropout rate 7 studies is 10%, therefore the attrition rate is also set at
10% for any dropped out of the program

91
References
Alsaadi S.M., McAuley H.H., Hush J.M. & Maher C.G. (2011). Prevalence of sleep
disturbance in patients with low back pain. European Spine Journal, 20, 737-743.
doi:10.1007/s00586-010-1661-x
Candler A., Preece J. & Lister S., (2002). Using heat therapy for management.
Nursing Standard, 17(9), 40-42. Retrieved from
http://rcnpublishing.com/doi/abs/10.7748/ns2002.11.17.9.40.c3297
Chou E., Qaseem A., Snow V., Casey D., Cross T., Shekelle P. et al. (2007). Diagnosis
and Treatment of Low Back Pain; A joint clinical practice guideline from the
American Colleage of Physicians and the American Pain Society. Annals of
Internal Medicine, 147(7), 478-491.
doi:10.7326/0003-4819-147-7-200710020-00006
Chou R. & Huffman L.H. (2007). Nonpharmacologic Therapies for Acute and
Chronic Low Back Pain: A review of the Evidence for an American Pain
Society/American College of Physicians Clinical Practice Guideline. Annals of
Internal Medicine, 147(7), 492-504.

92
doi:10.7326/0003-4819-147-7-200710020-00007
Drug office (2013a). Health and drug education: oral anagelsics. Retrieved from
http://www.drugoffice.gov.hk/eps/do/en/consumer/news_informations/dm_16.html
Drug office (2013b). Health and drug education: oral sleeping medicines. Retrieved
from
http://www.drugoffice.gov.hk/eps/do/en/consumer/news_informations/dm_07.html
French S.D., Cameron M., Walker B.F., Reggars J.W. & Esterman A.J. (2011).
Superficial heat or cold for low back pain(Review). Cochrane Database of
Systematic Review, 2, 1-13. doi: 10.1002/14651858.CD004750.pub2
Hoy D., Bain C., Williams G., March L., Brooks P., Blyth F.,et al. (2012). A
systematic review of the global prevalence of low back pain. Arthritis &
Rheumatism, 64(6), 2028-2037. doi: 10.1002/art.34347
Hides J.A., Strokes M.J., Jull H.A. & Cooper D.H. (1994). Evidence of lumbar
multifidus wasting ipsilateral to symptoms in patients with acute/subacute low

93
back pain. Spine, 19(2), 165-72. Retrieved from
http://www.ncbi.nlm.nih.gov/pubmed/8153825
Hospital Authority. (2013). Smart patient: chronic disease zone. Retrieved from
http://www21.ha.org.hk/smartpatient/en/chronicdiseases_zone/details.html?id=17
7
Kettenmann B., Wille C., Lurie-Luke E., Walter D. & Kobal G. (2007). Impact of
Continuous Low Level Heatwrap Therapy in Acute Low Back Pain Patients:
Subjective and Objective Measurements. Clin J Pain, 23(8), 663-668. doi:
10.1097/AJP.0b013e31813543ef
Kinkade S. (2007). Evaluation and Treatment of Acute Low Back Pain. American
Family Physician, 75(8), 1181-1188. Retrieved from
http://www.aafp.org/afp/2007/0415/p1181.html
Koes B.W., van Tulder M., Lin C.W.C., Macedo L.G., McAuley J. & Maher C.
(2010).An updated overview of clinical guidelines for the management of
non-specific low back pain in primary care. European Spine Journal, 19,

94
2075-2094. doi:10.1007/s00586-010-1502-y
Leon, Davis & Kraemer. (2011) The Role and Interpretation of Pilot Studies in
Clinical Research. J Psychiatr Res., 45(5), 626–629.
doi:10.1016/j.jpsychires.2010.10.008.
Mayer J. M., Raplh L., Look M., Erasala G. N., Verna J. L., Matheson L. N. &
Mooney V. (2005). Treating acute low back pain with continuous low-level heat
wrap therapy and/or exercise: a randomized controlled trial. The Spine Journal,
5(4), 395-403. doi:10.11016/j.spinee.2005.03.009
Mok L.C. & Lee F.K.I, (2008). Anxiety, depression and pain intensity in patients with
low back pain who are admitted to acute care hospitals. Journal of Clinical
Nursing, 17, 1471-1480. doi: 10.1111/j.1365-2702.2007.02037.x
Nuhr M., Hoerauf K., Bertalanffy A., Bertalanffy P., Frickey N., Gore C., Gustorff B.
& Kober A. (2004). Active warming During Emergency Transport Relieves Acute
Low Back Pain. Spine, 29(14), 1499-1503.
doi:10.1097/01.BRS.0000131439.87553.99

95
Nadler S. F., Steiner D. J., Abeln S. B., Erasala G. N., Hengehold D. A. & Weingand
K.W. (2003). Continuous low-level heatwrap therapy for treating acute
nonspecific low back pain. Arch Phys Med Rehabil, 84(3), 329-334. doi:
10.1053/apmr.2003.50102
Nadler S. F., Steiner D. J., Petty S. R., Erasala G. N., Hengehold D. A. & Weingand
K.W. (2003). Overnight Use of Continuous Low-level Heatwrap Therapy for
Relief of Low Back Pain. Arch Phys Med Rehabil, 84(3), 335-342. doi:
10.1053/apmr.2003.50103
Nadler S. F., Steiner D. J., Erasala G. N., Hengehold D. A., Hinkle R. T., Goodale M.
B., Abeln S. B. & Weingand K. W. (2002). Continuous low-level heat wrap
therapy provides more efficacy than ibuprofen and Acetaminophen for acute low
back pain. Spine, 27(10), 1012-1017. Retrieved from
http://www.oegpmr.at/wp-content/uploads/Heat-wrap-therapy-1.pdf
Pengel L.H.M., Herbert R.D., Maher C.G. & Refshauge K.M. (2003). Acute low back
pain: systematic review of its prognosis. bmj, 327, 323-327. doi:
96
10.1136/bmj.327.7410.323
Sackett D.L., Rosenberg W.M., Gray J.A., Haynes R.B and Richardson W.S. (1996).
Evidence based medicine: what it is and what it isn’t. BMJ, 312(7023), 71–72.
Retrieved from http://www.bmj.com/content/312/7023/71.full
Scottish Intercollegiate Guidelines Network. (2012).Critical appraisal: Notes and
checklists. Retrieved from http://www.sign.ac.uk/methodology/checklists.html
Scottish Intercollegiate Guidelines Network. (2012). SIGN Grading System
1999-2012. Retrieved from
http://www.sign.ac.uk/guidelines/fulltext/50/annexoldb.html
Tao X. & Bernacki E.J. (2005). A Randomized Clinical Trial of Continuous Low-level
Heat Therapy for Acute Muscular Low Back Pain in the Workplace. J Occup
Environ Med, 47(12), 1298-1306. doi: 10.1097/01.jom.0000184877.01691.a3
Waddell G., Feder G. & Lewis M. (1997). Systematic Reviews of bed rest and advice
to stay active for acute low back pain. British Journal of General Practice, 47,

97
647-652. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1410119/
Williamson A. & Hoggart B. (2005). Pain: a review of three commonly used pain
rating scales. Journal of Clinical Nursing, 14(7), 798-804.
doi: 10.1111/j.1365-2702.2005.01121.x