reaching the poorest – what role for cash...
TRANSCRIPT

REACHING THE POOREST –
WHAT ROLE FOR CASH TRANSFERS
TO ATTAINING UHC
ANDI ZA DULUNG
GENERAL DIRECTOR OF SOCIAL PROTECTION
AND SECURITY
MINISTRY OF SOCIAL AFFAIRS

Area: 5.193.250 km2. The sixth widest
country after Canada, USA , China,
Brazil, Australia
More than 13.000 islands
Population: more than 240 millions, the
four highest in the world after China,
India and USA
INDONESIA Data of Poverty
2013

SOCIAL PROTECTION INITIATIVES
1 A significant
number of the Poor
2 From commodity
subsidy to
household subsidy
3 Unconditional Cash
Transfer (UCT)
transformed to CCT
(Conditional Cash
Transfer) in 2007 ,
health insurance,
scholarship, and
rice for the poor.
4 Large poverty
dimension in
Indonesia
1. CCT & CCT Nutrition for
the poorest
2. Scholarship for the poor
3. Supplemental food for
school children program
4. Subsidized rice
5. For disabled
6. Children with adversity
7. Neglected old ages
8. Indigenous community
9. National Program on
Community
Empowerment (PNPM),
& PNPM Generation +
Nutrition)
10.Credit Facility to SMEs
1.Pension
2.Old age
security
3.“HEALTH”
4.Work Injury
5.Death
Social
Assistance
Social Insurance
NATIONA
L SOCIAL
INSURAN
CE
SYSTEM
(SJSN) -
UHC
Backgrounds

PKH (Family Hope Program) is a national priority program in
Indonesia.
The objective is to reduce poverty through improvement of life
quality in the field of health and education as well as to give ability
to the family to improve their consumption expense/economy.
PKH design elements:
1 PKH is a social protection program providing conditional cash
transfers (CCT) for the poorest families.
2 PKH is expected to change poorest families behavior in health
and education covering medical check up for women with
pregnancy/post natal/children under five and sending the
children to school.
3 PKH works on the principle that health is a human right and long
term investment which is expected to cut the link of poverty tothe next generation.

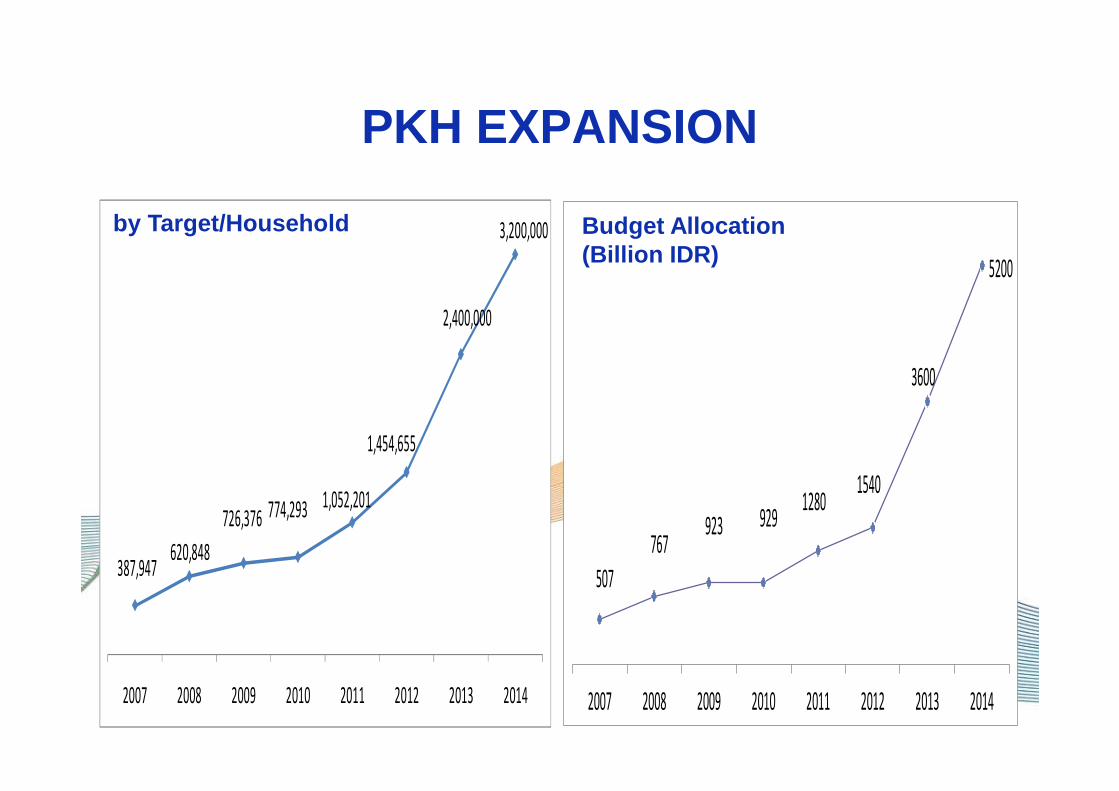
387,947 620,848
726,376 774,293 1,052,201
1,454,655
2,400,000
3,200,000
2007 2008 2009 2010 2011 2012 2013 2014
507
767 923 929
1280 1540
3600
5200
2007 2008 2009 2010 2011 2012 2013 2014
Budget Allocation(Billion IDR)
by Target/Household
PKH EXPANSION

COMPOSITION OF MEMBER PARTICIPATION FOR PKH FAMILY
Source : Center UPPKH , 2011
Positive Impact for Health
1. Number of women with pregnancy/post natal visitin g health facility improved 7 – 9 percentage points;
2. Number of children under five measured is improve d around 15-22 percentage points;
3. Delivery helped by medical person improved 5 percentage points;
4. Delivery helped by trained health personal improv ed 6 percentage points;
5. Impact of PKH is stronger in the regions with bet ter health service :
6. Impact in urban area is better than in rural. 7. Improvement of health facilities (Puskesmas, Pust u,
Pusling, Posyandu, dll)
collected from TNP2K 2011

PKH Health Impacts…PKH Health Impacts (% of baseline value)
-0,05
0,05
0,15
0,25
0,35
0,45
1 2 3 4 5 6 7 8 9 10 11 12 13 14
Direct PKH Beneficiaries
Non-beneficiaries in PKHareas
1. Pre-natal visits
2. Pre-natal visits ≥ 4
3. Delivery at facility
4. Post-natal visits
5. Post-natal visits ≥ 2
6. Weighings ≥ 1 (1-3 yrs)
7. Weighings ≥ 1 (0-5 yrs
8. Public health facility outpatient visits
9. Public health facility outpatient visits (all HH members)
10. Private health facility outpatient visits (all HH members)
11. Body Weight
12. Diarrhea 13. Treated Diarrhea.
14. Fever
Program and Public Expenditure Review The World Bank , 2011
How did PKH contribute to improved health and
access to health service?
PKH contributed to the increased use of Posyandu in rural areas in NTT
because there were a more significant number of PKH recipients and
facilitators threatened to cut of PKH funding to recipients if they did not
routinely attend Posyand
Source: SMERU Research Report
Which design issues of the programs support these impacts?
The involvement of actors that influenced the utilization of MCH services including village officials, midwives, posyandu staff, PKH facilitators, and religious leaders
Source: SMERU Research Report
What are future challenges in this field (i. e. how to better
coordinate health sector and social protection/cash transfers)?
1 Increase the availability of MCH services so that this is adequate and easily
accessible by all communities.
2 Increase the number of MCH professionals and personals as well as improve
the incentive for them.
3 Improve rural infrastructure including buildings, roads, bridges, electricity, and
clean water.
4 Renew the awareness raising efforts of PKH to village officials, service
providers and recipient and non-recipient households. Midwives and Posyandu
cadres should also be involved in the monitoring of program beneficiaries.
5 Improve the relationship between facilitators and beneficiaries by defining
facilitator’s regions, not only on the number of beneficiaries, but also taking
into account the geographical area and number of villages beneficiaries.
6 Ensuring transparency in the targeting of beneficiaries and renewing
awareness raising efforts amongst program recipients and non-recipients.
7 Source: SMERU Research Report

EFFORT OF PROGRAM IMPROVEMENT AND SYNCHRONIZATION
SYNCHRONIZATION OF SUPPORTED
PROGRAM BETWEEN PKH,
KUBE AND ASKESOS
IMPROVEMENT OF BETTER
PKH ACHIEVEMENT AND
SUSTAIN
CONDUCTING FAMILY
DEVELOPMENT
SESSION
RE-CERTIFICATION

THANK YOU…..