radiology business journal april/may 2011
DESCRIPTION
Welcome to Radiology Business Journal, a bi-monthly print journal published by ImagingBiz. This next-generation economics journal is published by the team that founded and developed Decisions in Imaging Economics, Curtis Kauffman-Pickelle and Cheryl Proval. We published our first quarterly issue in April 2008 and went to a bi-monthly frequency in 2009. The challenges ahead for health care, and, more specifically, for radiology, will require vision, strong leadership, and masterful business skills. Radiology Business Journal’s mission is to feed all of those competencies with insightful articles written by expert authors.TRANSCRIPT

FOR LEADERS IN MEDICAL IMAGING SERVICES
April/May 2011
www.imagingBiz.com
Featured in this issue
Financing Outpatient imaging:the new hospital Playbook | page 42
a Comprehensive approach toMitigating Malpractice risk | page 50
Plague of the Practice: Why democratic Governance no Longer Works | page 64
Sharks in the Case Pool
Teleradiology, The Practice, and the Purveyors

FOR LEADERS IN MEDICAL IMAGING SERVICES
April/May 2011
www.imagingBiz.com
Featured in this issue
Financing Outpatient imaging:the new hospital Playbook | page 42
a Comprehensive approach toMitigating Malpractice risk | page 50
Plague of the Practice: Why democratic Governance no Longer Works | page 64
Sharks in the Case Pool
Teleradiology, The Practice, and the Purveyors

be unlimited.
Support
To find out more about Hitachi’s customer support and how together we can be unlimited, visit www.HitachiMed.com


April/MAy 2011 | Volume 4, Number 2
4 Radiology BusiNess JouRNal | april/May 2011 | www.imagingbiz.com
CONTENTS
FEATurES
28 Sharks in the Case pool: Teleradiology, The practice, and the purveyor By George Wiley The lines are blurring and passions are running high between the practice and the teleradiology purveyor.
42 Financing Outpatient imaging initiatives: The Saint Thomas Health Services Experience By Tom Blankenship; Jason Dinger; and Sheila Sferrella, MAS, RT(R), CRA, FAHRA To prepare to meet future health-care–delivery needs, this nonprofit health-care system considered all of the options for financing an ambitious outpatient imaging center initiative.
50 Medical Malpractice: Are you Covered? By Howard Kessler, MD, and D. Scott Jones, CHC, LHRM By understanding the elements of medical-malpractice litigation and taking steps to mitigate risk, radiologists can reduce substantially their risk of being sued.
56 leveraging the Cloud in radiology By Julie Ritzer Ross As the price of storage declines and as hospitals and practices groan under the weight of responsibility for image storage and management, radiology is beginning to embrace the cloud.
64 Corporate practice Management in the 21st Century: Why Democratic Governance No longer Works By David F. Hayes, MD In these turbulent times, radiology practices cannot afford to indulge in the groupthink, wisdom of the crowd, and information cascade that are the byproducts of democratic governance.
28
42

PACS, RIS, Cardio – all the data for each patient – on one virtual desktop.Synapse® PACS, RIS and Cardiovascular have a lot in common. They’re all designed by Fujifilm.They’re all leaders in their fields. And, this is a big deal; they all have related architecture, toolsand interfaces. These three impressive systems work together so you can get the information youneed from a single workstation. With Synapse organizing your data by patient, everything is at yourfingertips. So your job is less administrative, more diagnostic. And that’s an idea worth sharing.Call 1-866-879-0006 or visit fujimed.com.
www.fujimed.com©2010 FUJIFILM Medical Systems USA, Inc.
Healthcare organized by patient. Brilliant.
1294_SynEnterAd_Radiology_Management:Layout 1 10/18/10 2:47 PM Page 1

6 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
CONTENTS April/MAy 2011 | Volume 4, number 2
publiShErCurtis Kauffman-Pickelle
EDiTOrCheryl Proval
ArT DirECTOr Patrick R. Walling
TEChNiCAl EDiTOrKris Kyes
ASSOCiATE EDiTOrCat Vasko
CONTribuTiNg WriTErSTom Blankenship; Jason Dinger;
Thomas W. Greeson, JD, Esq; David F. Hayes, MD;D. Scott Jones, CHC, LHRM; Howard Kessler, MD;
Amit Mehta, MD; Paul W. Pitts, JD, Esq;Julie Ritzer Ross;
Sheila Sferrella, MAS, RT(R), CRA, FAHRA;George Wiley
SAlES & MArkETiNg DirECTOrSharon Fitzgerald
prODuCTiON COOrDiNATOrJean Lavich
COrpOrATE OffiCEimagingBiz
17291 Irvine Blvd., Suite 105, Tustin, CA 92780(714) 832-6400
www.imagingbiz.com
prESiDENT/CEOCurtis Kauffman-Pickelle
Vp, publiShiNgCheryl Proval
Vp, ADMiNiSTrATiONMary Kauffman
Radiology Business Journal is published bimonthly by imagingBiz, 17291 Irvine Blvd., Suite 105, Tustin, CA 92780. US Postage Paid at Lebanon Junction, KY 40150. April/May 2011, Vol 4, No 2 © 2011 imaging-Biz. All rights reserved. No part of this publication may be reproduced in any form without written permission from the publisher. POSTMASTER: Send address changes to imagingBiz, 17291 Irvine Blvd., Suite 105, Tustin, CA 92780. While the publishers have made every effort to ensure the accuracy of the materials presented in Radiology Business Journal, they are not responsible for the correctness of the information and/or opinions expressed.
DEpArTMENTS
8 AdView health Care’s rubik’s Cube By Cheryl Proval
10 The bottom line The Compliance puzzle: New hot Topics By Thomas W. Greeson, JD, Esq, and Paul W. Pitts, JD, Esq
12 priors 12 Strategic planning | preparing for ACOs 16 Strategic planning | Anticipating the purchase or Sale 18 leadership | beyond the blame game 24 Clinical research | future Trends in Clinical-trial imaging By Amit Mehta, MD
26 Numeric | batten Down the hatches: Data Security and breach
70 Advertiser index
72 final read What google and rbJ have in Common By Curtis Kauffman-Pickelle
50
64

VISIT MMP AT BOOTH #406 DURING THE 2011 RBMA SUMMIT

The ACO proposal’s poison pill is the decision to assign patients based on their use of primary-care services provided only by primary-care physicians. Klar says that physicians working outside primary care provide 60% of all primary-care services to Medicare beneficiaries, and some patients with chronic conditions receive most of their primary care from specialists. The assignment model used in pre-ACO pilot projects, he says, included primary-care services provided by any physician.
Steven M. Lieberman’s assessment, by virtue of his work as a visiting scholar at the Brookings Institution’s Engelberg Center for Health Care Reform (see page 12), carries great weight. He believes that the proposed regulations will stifle—if not halt completely—the launch of the ACO as a new health-care provider.
Room at the tableAfter a tremendous investment of
time, expertise, and thought, CMS has explicitly asked for input and participation. Radiologists have much to bring to the table here, including IT expertise and infrastructure, management experience, and (of course) their specialty. You can’t have an ACO without a radiology service.
An article in this issue (see page 42) by a team from Saint Thomas Health Services (Nashville, Tennessee) describes the financing and rollout of a major outpatient imaging initiative, a joint venture with several participating radiology practices. This initiative is part of a strategic move by the health system to position itself as an ACO.
We have yet to see an ACO convened by a radiology practice, but I would not be surprised if there were discussions happening today between big radiology groups and multispecialty practices.
Radiology can help make this mythical unicorn real.
Cheryl [email protected]
The idea is at once simple and profound: An entirely new
health-care provider, given incentives by the Medicare Shared Savings Program to
defragment health-care delivery, improve quality and patients’ health, and reduce costs—thereby preserving Medicare and fee-for-service reimbursement. It’s the much-discussed but little-understood accountable-care organization (ACO), due to begin operating in January 2012.
This grand (and seemingly impossible) ambition has led some to call the ACO a unicorn. With the arrival of proposed ACO regulations on March 31, though, the concept took a giant step toward clarity. Physicians, hospitals, and payors are poring over the proposed rules and related regulatory statements to divine whether there is a place for them in this universe.
In creating the ACO, the Patient Protection and Affordable Care Act (PPACA) also authorized waiving certain laws governing fraud and abuse to make ACOs work. Consequently, statements from the US Federal Trade Commission (FTC) and the US Department of Justice (DOJ) on antitrust enforcement policy—and from the OIG and CMS on waiver designs that would relax antitrust and self-referral regulations—accompanied the rules.
Thomas Hoffman, JD, CAE, associate general counsel for the ACR®, is now (with his colleagues) knee deep in the proposed regulations and related statements, preparing a response before the June 6 deadline. He acknowledges that his team has never encountered a document as challenging and open ended as this proposal, and that the role of radiology in the ACO—as well as how it will share in the risks and rewards—is still unclear. Many policy wonks, meanwhile, predict that interest will be limited.
the Peanut GalleRyExperts’ initial reactions to the proposed
regulations ranged from highly critical to favorable (with caveats). The landmines can be categorized as the potential anticompetitive effects of encouraging consolidation (and the resulting upward pressure on costs); organizational requirements so onerous as to prevent participation, particularly by physician-led ACOs; requirements even more restrictive than those prescribed by the PPACA; and retrospective attribution of patients. This is intended to prevent imposing any restrictions on patient movement, but it means that an ACO will find out only at the end of three years the identity of the patients for which it was responsible.
The DOJ and the FTC plan to approach the issue of anticompetitive effects by invoking three levels of antitrust scrutiny, based on an ACO’s primary service area (PSA) share: ACOs with PSA shares of 30% or less will fall into a safety zone; ACOs with more than a 50% PSA share will require formal antitrust review by the agencies; and ACOs with PSA shares of 31% to 49% may voluntarily seek review when they apply to become ACOs.
The view of Joe Miller, general counsel of America’s Health Insurance Plans and a former assistant chief in the Antitrust Division of the DOJ, is that the screens are set too low—and that in encouraging consolidation, the policy does not do enough to discourage anticompetitive effects. He predicts that Medicare savings through ACOs would be unlikely to outweigh the cost increases that could be caused by reduced competition.
Ron Klar, longtime consultant to private-sector health plans and chief of health-systems innovation and performance for an academic medical practice, notes that by some estimates, an ACO’s startup expenses and first-year operating costs could exceed $1.7 million—a steep price for a program that offers a three-year commitment and no defined patient base.
8 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
Health Care’s Rubik’s CubeThe proposed ACO regulations could kill the program, making concerns about the relaxation of Stark regulations moot
AdView

Experts In Fair Market Value.Focused In Healthcare.Trusted by Clients.
www.vmghealth.com
Three Galleria Tow 13155 Noel Rd., St s, TX214-369-4888
3100 West End Ave., St hville, TN615-777-7300
VMG Health is a recognized leader in the valuation
of imaging centers. No one has more experience
and insight into the critical factors that drive
the value of an imaging center.

It is a daunting task to understand and stay current with the various Medicare rules that have an impact on the delivery of radiology and imaging
services. The fast-approaching effective date for the accreditation of advanced radiology services, the new supervision rules, and the proper use of radiologist extenders (radiologist assistants or radiology practice assistants) all illustrate this challenge. Given the many regulatory changes, it is understandable that some radiology practices remain uncertain how these rules work.
Accreditation will be required—beginning January 1, 2012—for nonhospital physician practices and IDTFs furnishing the technical component of certain advanced imaging procedures, including diagnostic MRI, CT, and nuclear medicine (including PET). Such technical-component services at accredited physicians’ offices (whether owned by radiologists or nonradiologists) will have to be supervised and performed only by qualified physicians and nonphysician personnel.
CMS will eventually develop rules to define what it means to be qualified, but for now, the three accrediting bodies (the ACR®, the Intersocietal Accreditation Commission, and the Joint Commission) are authorized to apply separate and differing standards. After January 1, 2012, the technical component of these services will no longer be billed globally; the technical component and the professional component will have to be billed separately. This will be required so that the claim submitted for the technical component will be able to carry the 95 code, to identify that it was performed at an accredited facility.
Don’t be surprised to see CMS issuing guidance on who should bill for the accredited technical-component service. Our best guess on what to expect is that for an accredited advanced imaging service that does not require direct or personal supervision (such as nuclear medicine, PET, or CT and MRI without contrast), the billing physician will be the performing physician. For accreditation purposes, this is the medical director, who is responsible for the overall direction and control of the imaging equipment and for all those tests that require general supervision.
For accredited advanced imaging services that require direct supervision (such as MRI or CT with contrast), the
billing physician will be the physician who was supervising by being present in the office suite during the performance of those tests. For an accredited advanced imaging study that requires personal supervision, the billing physician will be that physician who was present in the room throughout the performance of the test. We anticipate that the role of the supervising radiologist will be more defined as a result of accreditation.
This brings us to a related regulatory issue: How can a radiology group effectively use radiologist extenders? Feedback on our comprehensive summary of the rules1
indicates that many practices failed to understand the implications of the rules.
The BoTTom LineLet’s be clear: There is no Medicare
Part B coverage for services performed by physician-employed auxiliary personnel in a hospital setting, regardless of whether a radiologist supervises the performance of the services. As a result, payment for the services of nonphysician auxiliary personnel is made solely to the hospital, as part of its reimbursement by Medicare under the hospital prospective payment system (PPS).
To date, the Medicare program has not recognized radiologist extenders as medical professionals who may separately bill for their own services and be reimbursed at a percentage of the Medicare Physician Fee Schedule (MPFS). The limitation imposed on billing for the services of radiologist extenders has a significant impact on the use of these professionals—at a time when hospitals and radiologists seek opportunities to reduce the cost of health-care services. These concerns are further compounded by the requirements for personal supervision that apply to many diagnostic tests.
Radiologist extenders have been used by radiology groups to assist in the performance of diagnostic tests and in the performance of physician/surgical procedures. Both uses can create problems. In a hospital setting, diagnostic tests for Medicare outpatients must be performed under the appropriate level of physician supervision designated by CMS. There are three levels of supervision applicable to the hospital setting: personal, direct, and general.
A procedure specifying personal supervision requires that the radiologist be in attendance in the room during the performance of the procedure. If direct supervision is specified, the radiologist
must be immediately available to furnish assistance and direction throughout the performance of the procedure. The radiologist is not required to be present in the room when the procedure is performed. If general supervision is called for, the procedure is furnished under the radiologist’s overall direction and control, but the radiologist’s presence is not required during the performance of the procedure.
CMS confirmed, in the 2010 Hospital Outpatient PPS (HOPPS) rule, that nonphysician practitioners, such as nurse practitioners and physician assistants, cannot supervise diagnostic tests. Only physicians can supervise diagnostic tests for Medicare outpatients. It should be noted, of course, that the 2010 HOPPS rule does not require a physician of any particular specialty to perform the supervision of the test.
In addition, in a hospital setting, surgical or invasive procedures (with CPT® codes not in the 70000 series) must be performed by a physician who submits a claim for payment under the MPFS. The hospital submits a claim for its services to an outpatient under HOPPS; for inpatients, it submits a claim under the applicable DRG.
Any assistance rendered by a radiologist extender (as part of such a procedure in a hospital) is considered part of hospital services. The radiology group may not bill Medicare for a surgical or invasive procedure performed by the group’s employed radiologist extender, even if the procedure is within the radiologist extender’s scope of practice under state law.
Be cautious and follow the Medicare rules when working with radiologist extenders. To do otherwise could prove to be very costly in lost revenue, as well as in potential fines and penalties assessed against those radiology groups that bill inappropriately.
Thomas W. Greeson, JD, Esq, is an attorney with Reed Smith LLP (Falls Church, Virginia); [email protected]. Paul W. Pitts, JD, Esq, is an attorney with Reed Smith (San Francisco, California); [email protected].
Reference1. Greeson TW, Pitts P. Medicare payment is contingent on appropriate supervision of diagnostic tests and proper use of radiologist assistants: is your practice meeting the current requirements? J Am Coll Radiol. 2011;8(3):180-185.
10 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
The BoTTom Line
The Compliance Puzzle: New Hot Topics by THomas w. gReesoN, JD, esq,
aND Paul w. PiTTs, JD, esq

Nearly every radiology department or practice will be affected by accountable-care organizations (ACOs)—
because even if it chooses not to become part of one or more ACOs, it will probably be competing with them. Since some types of ACOs will be granted the ability to sidestep current price-fixing and self-referral restrictions, according to proposed ACO antitrust regulations1 released on April 19, 2011, the competition between ACO participants and nonaligned groups could become intense. ACOs are permitted to serve commercially insured patients as well as Medicare/Medicaid enrollees (under the same loosened self-referral restrictions), so they are likely to be competing, sooner or later, for most of the imaging volume in any area.
In “Building Regulatory and Operational Flexibility Into Accountable Care Organizations and ‘Shared Savings,’”2 published in Health Affairs, Steven M. Lieberman and John M. Bertko predicted much of what the March 31 proposed rule3 for ACOs and the April 19 antitrust proposal1 would contain. Lieberman is president of Lieberman Consulting Inc (Bethesda, Maryland) and Bertko is a senior fellow at the LMI Center for Health Reform (McLean, Virginia).
Both authors are visiting scholars at the Brookings Institution’s Engelberg Center for Health Care Reform (Washington, DC). They are working on a collaboration between the center and the Dartmouth Institute for Health Policy & Clinical Practice (Lebanon, New Hampshire) to develop workable models for ACOs.
They write, “ACOs have the potential to lower costs, improve the quality of care, facilitate delivery-system reform, and promote innovation in health care.” Those hopes first led to the creation of ACOs in 2010’s Patient Protection and Affordable Care Act (PPACA).
In January 2012, ACOs can begin three years of participation in Medicare’s Shared Savings Program, which is expected to return bonuses of $800 million during that period to ACOs that save CMS money. ACOs that cost Medicare more than it expects to pay could be required to return $40 million to CMS, however.
In return for fee-for-service payment, ACOs must provide comprehensive care to at least 5,000 Medicare enrollees, either by incorporating all necessary services in their organizations or by paying for non-ACO services. Enrollees must be free to choose providers, but ACOs will pay those providers, even if they are outside the ACO. CMS will assign Medicare enrollees to the ACOs to which their primary-care providers belong, and ACOs will have no ability to reject any Medicare beneficiary (but enrollees can reject an ACO by changing primary-care providers).
ACOs that meet predetermined quality standards will be eligible for bonuses of
up to 60% of Medicare savings if they are willing to risk repaying CMS 10% of its predicted cost of care, if they fail to save Medicare any money. If they are unwilling to take that risk for the program’s first two years, they can still qualify for bonuses of up to 50% (but during the program’s third year, they will have to return up to 7.5% of excess costs of care to CMS).
ACOs must also meet CMS criteria for organizational, legal, and management structure, and they are required to provide cost and quality data (and have the necessary information systems in place). Comments on the antitrust proposal and the ACO proposal will be accepted until May 31 and June 6, respectively.
Radiology’s PRosPectsBecause ACOs will be paying for
the services of specialists (including radiologists), many ACOs will encourage radiology departments and groups to become affiliated with them—but ACOs
12 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
{priors}Preparing for ACOss t r a t e g i c p l a n n i n g

Data is as vital for financial decisions as it is for clinical decisions. So we combine billing expertise and industry-changing technology — including our Client Analysis Center — to analyze your data and evaluate it against industry benchmarks. Call us today to learn how our experienced people and leading-edge processes can help you identify new opportunities, reduce costs and maximize billing accuracy and revenues.
Zotec Partners. The total solution.
P 317.705.5050F 317.705.5047
11460 N. Meridian St.Carmel, IN 46032
MAxIMIze your ProFItAbIlIty...
wIth ADvANCeD MetrICS & ProveN exPertISe.
[email protected] zotecpartners.com See us at the RBMA Radiology Summit – Booth #300

14 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
priors
are not allowed to create exclusive arrangements with specialists, so radiology groups can expect to work with multiple ACOs, instead of being tied to one (as some had previously planned).
The effect of ACOs on imaging volume is difficult to predict. Many ACOs will probably attempt to limit costs by reducing utilization of expensive services such as advanced imaging, but others might increase imaging volume, particularly for screening exams, in an attempt to improve documented quality of care (and reduce future costs of care through earlier diagnosis). Imaging providers might be wise to ensure that ACOs forming in their areas are fully aware of what they can offer, especially since the proposed relaxation of self-referral prohibitions1 would make in-office imaging outside radiology more attractive to some ACOs.
Providers participating in ACOs are not allowed to restrict, through their contracts with commercial insurers, the ability of those payors to steer patients to their chosen providers—typically, those that charge least for their services. Steering patients to the lowest-cost providers is considered, under the PPACA, to be an important means of reducing the overall cost of care,1 and one obvious result is that fewer imaging providers will be able to avoid making their charges public.
Flexibility and innovationThe PPACA section creating ACOs
takes, as its premise, the idea that innovation can produce the reductions in cost and improvements in quality that are among the primary goals of health-care reform. Remaining flexible enough to innovate (and to keep changing as health-care delivery evolves) will be vital to creating beneficial ACO models at the federal level, but ACO participants also will be called upon to exhibit the same ongoing flexibility, according to Lieberman and Bertko.
They write, “ACOs are designed to occupy a middle ground between providers who are paid on a fee-for-service basis and managed-care plans that are paid by capitation.” Although the proposed regulation3 maintains a fee-for-service model initially, the bonuses that can be earned through cost control
bring the ACO beyond the status quo, and participants planning to earn those bonuses will be unlikely to do so without remaining open to new structures, alliances, and methods.
“Especially if a newly formed ACO includes only primary-care physicians, some specialty physicians, and perhaps a community hospital, patients will receive a substantial amount of care from providers outside of the organization,” Lieberman and Bertko write. “Regardless of how many services are delivered by outside providers, the organization remains accountable for the cost and quality of all services received by the patients assigned to it.”
Existing large, highly integrated delivery systems (such as Intermountain Health Care in Salt Lake City, Utah) might not need to change appreciably. As Lieberman and Bertko write, such systems “already have highly developed infrastructure and leadership that allow them to analyze patient, clinical, and claims data; manage use; and improve the quality of clinical processes and other types of care.” Their existing providers, they add, might already by able to provide nearly all of the care required by the patients assigned to an ACO.
Smaller, less integrated providers will need to make more changes, and these will go beyond structure. Cultivating a culture that values innovation and flexibility—both of which are uncommon in many health-care organizations—will be important, too. “In some geographic areas, an important part of provider culture is working together in a system, regardless of its precise legal organization. In other areas, many providers operate as essentially stand-alone, independent practitioners,” Lieberman and Bertko write.
Bringing those independent providers together will call for changes in outlook. Many will need time to adjust to the idea of working with their former competitors as part of a larger system, the authors note. Some will need to buy (or enter contracts to obtain) the services that they cannot now provide and do not want to begin providing. All will need to adjust to a greater need to measure and improve quality of care and to control costs if they are to be successful ACO participants.
exPectationsLieberman and Bertko make a cautious
prediction of success for the Shared Savings Program and ACOs, noting that both Medicare savings and ACO bonuses are probable, based on their pilot-program experience. Much refinement and revision will be required, however, to ensure optimal results, and constant monitoring of new developments and models will be required.
They write, “CMS must be on guard against strategies that would effectively subvert the goals of accountable care, which could occur if a dominant hospital or specialty physician group organized an entity for the purpose of controlling referral patterns and enhancing revenues.”
They add that some patience will be needed in assessing the validity of the ACO model—but providers intending to become part of it should be preparing now. “Although some organizations are already in operation, most have to make plans, train leaders, establish infrastructure, and develop strategies to improve patient care,” they write. “Some organizations may need two to five years to prepare for participation in accountable care. CMS needs to accommodate different levels of preparedness around the country.”
—Kris Kyes
References1. US Federal Trade Commission, US Department of Justice Antitrust Division. Proposed statement of antitrust enforcement policy regarding accountable care organizations participating in the Medicare Shared Savings Program. http://federalregister.gov/a/2011-9466. Published April 19, 2011. Accessed April 19, 2011.2. Lieberman SM, Bertko JM. Building regulatory and operational flexibility into accountable care organizations and ‘shared savings.’ Health Aff (Millwood). 2011;30(1):23-31.3. US Centers for Medicare & Medicaid Services. Medicare Program; Medicare Shared Savings Program: accountable care organizations. http://federalregister.gov/a/2011-7880. Published April 7, 2011. Accessed April 19, 2011.

How will yourradiology department fareafter healthcare reform?
Radisphere is the radiology partner that can help you prepare today for the sharp realities ahead.
A strong radiology strategy is critical in today’s environment of declining reimbursements, increased competition and the uncertainty of ACO and P4P strategies.
Radisphere National Radiology Group provides you with a higher level of radiology services. Our local, on-site radiologists and extensive network of U.S.-based subspecialists collaborate with your physicians to deliver thor-ough, decisive, high quality final reports and consultations that improve medical staff satisfaction and allow your facility to differentiate itself in the market. Our unparalleled technology enables us to significantly improve report turnaround time as well as provide transparency and accountability across a variety of key performance metrics including discrepancy rates, turnaround times, critical findings, and referral physician patterns.
Healthcare reform doesn’t have to be traumatic. You can be prepared by evaluating and improving your radiology services with Radisphere today.
866-437-7237 www.radisphere.net
1385_Rad2011Trade_ImagingBiz.indd 1 3/29/11 3:09 PM

16 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
priors
After a period of hypergrowth from 1994 to 1996, hospital mergers and acquisitions declined from a height of more than 450
transactions in 1996 to a mere 50 in 2009. John Reiboldt, managing director of Coker Capital Advisors (Alpharetta,
Georgia), says that the merger/acquisition market is heating up once again with the return of many of the factors that drove the action in the early 1990s:
pressure from payors, the threat of managed care, greater regulatory burdens and government intervention, physician employment, physician integration, and economic uncertainty.
In Orlando, Florida, on February 22, 2011, Reiboldt presented “Mergers and Acquisitions in the Hospital Market” at the annual meeting of the Health Information and Management Systems Society. He says that he did not expect to see the number of deals experienced in 1996, but that hospitals will increasingly engage in merger/acquisition activity as
s t r a t e g i c p l a n n i n g
Anticipating the Purchase or Sale
a strategic alternative. The total number of hospital transactions in 2010 was 77, with a total value of $12.7 billion—a dramatic increase over the total values of $2.6 billion for 2008 and $1.7 billion for 2009. Reiboldt refers to these as the lost years.
DeAl ChArACteristiCsAn interesting wrinkle in the latest
go-round is the widely dispersed types of transactions (see table) that occurred in 2010, with not-for-profit entities buying for-profit organizations (and vice versa), and with new participants and deal structures.
“What really surprised us was the acquisition of Caritas Christi Health Care System (Boston, Massachusetts), an $830 million acquisition by a private-equity company, Cerberus Capital Management LP (New York, New York),” Reiboldt says, noting the 2006 investment that the company made in the GMAC division of General Motors.
Reiboldt believes that, based on demographics, the for-profit providers are gearing up for volume-based medicine—rather than the accountable-care organization (ACO) concept—with
dispersion of costs, economies of scale, and economies of scope as the strategic objectives.
On the other hand, in-market consolidation has been an earmark of not-for-profit acquisitions, supporting the ACO concept of delivery of care on multiple levels. Both for-profit and not-for-profit providers, however, are thinking about the impending demographic surge as more of the baby-boom generation reaches retirement age; the percentage of people in the United States who are over 65 years old is set to soar from 13% in 2009 to 19% in 2030. “The number of people who are entering our health-care system, who are asserted to be high utilizers, is absolutely staggering,” Reiboldt states. “Right now, hospitals are not prepared for that.”
Care for most of these patients will be paid for under Medicare rates, which is why Reiboldt believes that the ACO concept is not coming into play in a big way in the current round of acquisitions. “What you see is people preparing for volume-based medicine instead of value-based medicine,” he says.
Reiboldt also notes a good balance between buyers and sellers, which has
With deal activity heating up in health care, radiology practices, imaging centers, and hospitals are well advised to have a strategy in place before acquisition opportunities—and suitors—come calling
John reiboldt
Announced target Acquirer transaction size status
November 12 ......... Tenet Healthcare .................................... Community Health Systems ............... $7.4 billion ................. announced
March 19 ............... Detroit Medical Center ........................... Vanguard Health Systems .................. $1.3 billion .................. closed
March 25 ............... Caritas Christi Health Care System ......... Cerberus Capital Management ........... $830 million ............... closed
March 31 ............... University Community Health ................. Adventist Health System .................... $200 million ............... closed
March 1 ................. Jewish Hospital (Cincinnati, OH) ............. Catholic Healthcare Partners .............. $180 million ................ closed
July 26 ................... Wuestoff Health System ......................... Health Management Associates ......... $152 million ................ closed
February 23 ........... Coffee Health Group ............................... RegionalCare Hospital Partners .......... $145 million ................ closed
April 30 ................. Summer Regional Health System ........... LifePoint Hospitals ............................. $145 million ................ closed
September 10 ........ Pikes Peak Ragional Hospital and .......... IASIS Healthcare ................................ $95 million ................. closed Wadley Regional Medical Center
August 30 .............. St Joseph’s Health System ...................... to be determined ................................ unknown .................... announced (Catholic Health East)
table. Selected 2010 Hospital Transactions
i believe
“Itistimetogivesomethingback. Callitkarmicobligation. Callittikkunolam.Itreallydoesn’tmatter whatyoucallit—
itissimplytherightthingtodo.”
Allen Rothpearl, MDFounder, Complete Radiology Reading Services
OrganizedthedigitaltransmissionofimagesfromapediatrichospitalinHaititoCRRSafterthedevastatingearthquakein2010.Dr.Rothpearlandhisassociatesreadtheexaminationsanddonatetheirinterpretationstothehospitaltothisday.
Allen Rothpearl uses eRAD PACS. www.erad.com

PrePAring for A trAnsACtionWhether you are planning to buy or to
sell, the merger/acquisition process should be part of your strategic plan. “Going out and selling your hospital doesn’t have to be your strategy,” Reiboldt says. “Going out and buying other hospitals doesn’t have to be your strategy. All it has to be is a component of your long-term strategy.”
Reiboldt recommends taking four steps. First, outline and adhere to your transaction goals before and during the process. Second, recognize what drives value, and don’t be afraid to drive value—which doesn’t always mean monetary value. It could be as simple as investing in the physical plant, in the IT infrastructure, or in building the physician network.
Third, think ahead, plan for an auction, and create a market. Fourth, consider other methods of affiliation, such as joint ventures, that might be more appropriate.
There are seven key components of a successful transaction process, beginning with confidentiality, which must be maintained internally and externally. The other six are the development of a strategy (your play book), thorough due diligence (the most money does not translate into the highest stability), the identification of prospective partners, buyer due diligence, maintaining competition among multiple potential partners, and a negotiation
18 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
priors
sent valuation multiples slightly higher. Sellers are selling because the financial crisis has sent many community and government owners running for the exit. Preparing and paying for stages 1, 2, and 3 of meaningful use under the Health Information Technology for Economic and Clinical Health Act have been factors, Reiboldt believes.
“You go to some of these hospitals, and you have unfunded pension liabilities and significant financial risk, so they are going to people with deeper pockets, both on the for-profit and nonprofit sides,” he says. “I’m a big believer that the days of the single hospital are over.”
All of this has made executives and boards more amenable to these transactions. “They are finding that it is a good way to maintain quality health care in their communities,” Reiboldt says. “Merger and acquisition are no longer dirty words.” In addition, many hospitals have no choice but to consider selling. Reiboldt recommends that you avoid finding yourself backed into a corner with no options.
Buyers, on the other hand, are acquiring entities to build economies of scale, to enter new geographic markets, to add new services, to attract and retain physicians (probably among the biggest drivers), and to diversify patient and payor mixes, as well as because they have the financial backing to do so.
process that optimizes economic and noneconomic terms.
Sellers can use one of three transaction-process alternatives: a negotiated process with one to two buyers, a targeted auction marketed to a select group of targeted buyers, or a broad auction marketed to a wide range of potential buyers. The first alternative ensures speed and confidentiality, but is unlikely to achieve maximum value. A targeted auction is both expedient and likely to achieve full value, while a broad auction maximizes competition.
Reiboldt advises hospital buyers to be clear about their long-term strategies, to understand their financial capabilities, to know their competitive environments, to know why they want other hospitals, and to identify opportunistic targets (those with reasonable valuations that are viable acquisition targets).
Be prepared to invest the time and money that it takes to conclude the deal properly. One of Reiboldt’s clients spent $5 million on IT integration alone for a large hospital acquisition. It’s not about the deal; it’s about the integration, which doesn’t begin the day you sign definitive agreements, but at least 120 days earlier. “The day you start thinking about buying a hospital is the day you should start thinking about integration,” Reiboldt concludes.
—Cheryl Proval
l e a d e r s h i p
Beyond the Blame Game
If at first you don’t succeed, then go ahead and fail, but do it intelligently. Failure, in fact, not only should be dissected and analyzed, but
should be planned for—and, if done well, celebrated. That’s because failure, according to Amy C. Edmondson, not only is inevitable in complex systems (such as a busy hospital emergency department), but is a key innovation tool. The tragedy occurs when organizations fail to learn from failure, and most of them do, she writes in the April 2011 issue of Harvard Business Review.1
As health care embarks on a period of great experimentation, the lessons that Edmondson imparts are well timed
for this market. The author reviews the role and spectrum of failure (from deviance to exploratory testing), but she also addresses ways to limit the liabilities associated with failure.
Edmondson lays the responsibility for the inability to learn from failure squarely at the feet of leaders, who are invariably guilty of viewing failure as something bad (though not all failures are) and are unable to embrace the lessons of failure due to cultural beliefs and stereotypical notions of success. “In organizational life it is sometimes bad, sometimes inevitable, and sometimes even good,” she says.
Begin by understanding how the blame game gets in the way of learning from
mistakes. Executives Edmondson has interviewed in a range of organizations, including hospitals, worry that without the fear of blame, people will not do their best work. The author identifies a spectrum of reasons for failure to explain why a culture in which it is safe to admit blame can—and in some organizations, must—exist in an organization that adheres to the highest standards.

› Uncertainty. You don’t like it because it obscures your vision for the future. Yet uncertainty is the order of the day in radiology.
Just›consider:›government›is›poised›to›impose›
further›limitations›on›how›much›imaging›you›can›
perform›and›under›what›circumstances,›while›
private›payors›are›contemplating›putting›up›
extra›hoops›and›hurdles›to›further›complicate›
the›reimbursement›process.›On›top›of›that,›the›
economy›continues›to›struggle,›in›some›parts›
of›the›country›the›radiologist›shortage›shows›
no›sign›of›abating,›and›capital›resources›are›
stretched›to›the›limit.›Uncertainty›is›everywhere›
you›look.
One›thing›that›is›certain,›though:›all›this›
uncertainty›is›impairing›your›ability›to›meet›the›
demands›of›referring›physicians,›their›patients›
and›your›other›customers›or›partners.
Despite›that,›you›do›have›an›advantage›against›
uncertainty.›Imaging On Call.›We›bring›into›
sharp›view›the›advanced›diagnostic›imaging›
solutions›you›need›to›make›your›path›forward›
clearly›visible,›your›footing›sure,›and›your›
progress›certain.
Uncertainty. Take›the›edge›off›it.
See things differently.www.imagingoncall.net

We help yoU exceed›expectations›around-the-clock›with›premier›teleradiology›services›and›radiology›department›support.› Save time and resources on staff supplementation. We›step›in›to›help›you›recruit›
and›vet›the›extra›radiologists›you›need›on›site›as›well›as›appropriately›augment›the›staff›required›
at›your›facilities.›This›is›key›to›your›ability›to›provide›the›level›of›diagnostic›interpretation›expertise›
your›medical›staff›and›referring›providers›expect›as›they›strive›to›achieve›the›highest›standards›in›
patient›care.
› Deliver higher quality care. To›do›that,›you›first›need›the›
ability›to›quickly›yet›thoroughly›read›images›from›all›types›of›
modalities›involving›all›manner›of›studies,›which›means›you›must›
have›extensive›sub-specialty›expertise.›The›sub-specialist›network›
we›bring›to›you›consists›of›over›400›board-certified›and›Joint›
Commission-accredited›radiologists›from›every›field›of›diagnostic›
and›interventional›imaging.›They›work›hand-in-glove›with›our›select›
team›of›40-plus›fellowship-trained,›board-certified›teleradiologists›
to›cover›you›day›and›night›for›sub-specialty›readings›–›as›well›as›for›
readings›involving›emergent,›routine›and›overflow›studies.

› Expand into new service lines without expanding your radiologist staff. Our›
financial›expertise›helps›you›procure›new›modalities›
and›enlarge›your›facilities.›No›need›to›hire›more›
radiologists›since›our›teleradiology›and›sub-speciality›
networks›provide›that›expertise›for›you.
› Lower your costs. We›reduce›your›need›to›make›
capital›investments›in›hardware›and›software.›Our›
services›are›delivered›to›you›through›our›economical›
yet›full-function,›web-based›PACS›system.›With›it,›
you’ll›be›able›to›consolidate›all›your›DICOM-›and›
HL7-compliant›images›and›reports›into›a›centrally›
managed›work›list›and›at›last›experience›the›benefits›of›high-availability›information.
› Lighten the load on your staff. We›offer›departmental›administrative›support›to›handle›
many›of›your›most›time-consuming›and›labor›intensive›clerical›tasks›–›except›that›our›powerful›
efficiencies›of›scale›allow›us›to›do›it›for›a›fraction›of›what›your›non-physician›personnel›have›likely›
been›costing›you.
› A name you trust. Imaging›On›Call›is›a›division›of›RadNet,›Inc.,›an›outpatient›diagnostic-
imaging›facilities›owner/operator›that›started›in›1980›and›is›currently›responsible›for›more›than›200›
centers›across›the›nation.›At›Imaging›On›Call,›we’ve›been›serving›radiology›departments›like›yours›
since›2002.
See things differently.
www.imagingoncall.net

Let Imaging On Call›restore›your›vision›for›the›future›with›the›
advanced›teleradiology, information management›and›personnel
support solutions›you›need›today.›You›can’t›completely›end›the›
uncertainty›that›threatens›your›organization,›but›you›can›at›least›take›
the›edge›off›it›with›Imaging›On›Call.
Learn more about us. See for yourself what a difference we make.For›More›Information››Call›Beth›Jackson
(845)›891-2146
695 Dutchess Turnpike, Suite 105, Poughkeepsie, NY 12603 Corporate Offices: 1510 Cotner Avenue, Los Angeles CA 90025
Uncertainty›demands›you›respond›with›certainty.
See things differently.
www.imagingoncall.net

www.imagingbiz.com | april/May 2011 | Radiology Business JouRnal 23
On the blameworthy end of the spectrum, it begins with deviance, followed by inattention, lack of ability, and process inadequacy. Task challenge is at the center of the spectrum, followed by (and progressing toward the praiseworthy) process complexity, uncertainty, hypothesis testing, and exploratory testing, the most praiseworthy reason for failure.
Very few of the reasons for failure on this spectrum are purely blameworthy, and in fact, most executives acknowledge that the percentage of blameworthy failures is in the low single digits. Because 70% to 90% are treated as blameworthy, however, many failures go unreported and therefore are likely to recur.
three flAvorsFailures fall into three broad categories:
preventable in predictable operations, unavoidable in complex systems, and intelligent at the frontier. Preventable failures are to be avoided and usually involve deviations from specified processes in high-volume or routine operations. Training, checklists, and systems that adapt processes (based on what is learned from small mistakes) are measures that are successful in preventing such failures.
Unavoidable failures in complex systems can usually be attributed to an unpredictable combination of factors that might never have occurred simultaneously before in a complex environment, such as a hospital emergency room, a battlefield, or a fast-moving startup. Such failures are inevitable, Edmondson believes, and the best approach is to identify them rapidly, so that they do not trigger consequential, larger failures. “Most accidents in hospitals result from a series of small failures that went unnoticed and unfortunately lined up in just the wrong way,” she notes.
Intelligent failures occur when experimentation is required, providing an organization with valuable new knowledge. At the frontier, managers hope for experiments that fail quickly, thereby preventing the failure of a larger-than-necessary experiment, which is what Edmondson calls an unintelligent failure.
the leADer’s roleTolerating the failures that provide
knowledge requires leadership that can
shift the organization away from blame and toward a culture of learning—in which managers seek the reason for a failure, rather than the perpetrator. All organizations learn from failure through three activities: detection, analysis, and experimentation.
Detection, however, can be tricky. Big failures are easy to spot, but the small failures that are unlikely to cause serious harm stay hidden, in many organizations. Edmondson relates an anecdote about Alan Mulally, president and CEO of Ford Motor Company (Dearborn, Michigan), who instituted a new system for detecting failure by color coding reports green for good, yellow for caution, and red for problems. Mulally grew increasingly frustrated during the first several meetings, as all reports were coded green. After one manager delivered a yellow-coded report about a problem that could delay a launch, Mulally broke into applause, and a greater openness ensued.
The attitude of the manager plays a significant role in the willingness of nurses to discuss failures in hospitals, Edmondson writes. How midlevel managers respond to failures and whether they encourage open discussion, welcome questions, and display humility and curiosity were the differentiators.
She also reports that failure analysis is frequently ineffective, even in hospitals. An exception to that rule is Intermountain Healthcare (Salt Lake City, Utah), where physicians’ deviations from care protocols are routinely analyzed. Allowing deviation and sharing the data on whether care is improved encourage physician buy-in; multidisciplinary teams can go beyond the superficial to root out second- and third-order causes of failure.
The third activity necessary for learning from failure is experimentation—but only in the right place and at the right time. “Too often, managers in charge of pilots design optimal conditions rather than representative ones,” Edmondson writes. “Thus the pilot doesn’t produce knowledge about what won’t work.”
In communicating the kinds of failures that can be expected in a particular work environment, it is important for leaders to craft the right message for a given work context. Most organizations engage in the kinds of work associated with all three
categories of failure: routine, complex, and experimental.
BuilDing A sAfe environmentJulie Morath, former COO of
Children’s Hospitals and Clinics of Minnesota (St Paul), led a successful campaign to reduce medical error during her tenure (1999–2009), illustrating five practices that Edmondson identifies as critical to building a psychologically safe environment: Frame the work accurately, embrace the messengers, acknowledge limits, invite participation, and set boundaries and hold people accountable.
Morath began by accurately framing the safety issues in the hospital environment through sharing US medical-error rates, building teams of influencers, and conducting discussion groups. She also implemented a system of blameless reporting, in which employees were encouraged to reveal medical errors and near misses anonymously. She encouraged employees to learn from failure and always assigned a team to analyze each incident, and the rate of reported failures spiked.
By acknowledging her limited knowledge of how things worked and encouraging thoughtful discussions about the safety of the patient experience, she helped employees recognize that there was room for improvement, thus enlisting many willing helpers.
When Morath launched blameless reporting, she held the staff accountable by specifying the behaviors that were not blameless—including reckless conduct, conscious violation of standards, and failing to ask for help when overwhelmed.
Courage is required by those individuals and organizations intent on learning from their failures, but most managers are loath to move beyond the blame game, at the risk of creating a lax workplace. Edmondson believes that failure is inevitable in today’s complex work environments, and those who can learn from it are the ones who will succeed.
—Cheryl Proval
reference1. Edmondson AC. Strategies for learning from failure. Harv Bus Rev. 2011;89(4):49-55.

24 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
priors
This is the final article in a series of three providing a primer for radiologists and imaging professionals interested in clinical trials.
Over the past two decades, there has been a significant evolution in the methodology of clinical trials, specifically as
it applies to the use of medical imaging as a surrogate endpoint or biomarker. While the use of medical imaging has now garnered mainstream acceptance in clinical-trial arenas to make trials more effective and accurate, the actual use of imaging in trials remains in its infancy.
In order to satisfy regulatory requirements and access the most widely available technology, imaging contract-research organizations (CROs) have primarily advocated the use of conventional modalities and methods, as they are easily translatable from the clinical sphere to research protocols. As mainstream acceptance has widened, however, investigators have begun to look into new modalities, newer protocols, and new methods for using medical imaging in clinical trials.
HardwareAs most current clinical trials involve
oncology, the workhorse modalities are CT and MRI (due to the validation and acceptance of response-evaluation criteria in solid tumors). CT technology has evolved to allow isometric voxel imaging and reproducible 3D imaging, and MRI allows evaluation of a broad range of imaging elements, from metabolism and physiology to tissue microstructure.
CT: The main developments in CT have been related to the introduction of multidetector spiral CT. Multidetector imaging allows multiplanar and 3D rendering of anatomical structures with a level of detail that is on par with that of other planar modalities—conventional angiography, for example, when compared with CT angiography.
The evolution of CT technology has produced improvements in multiple areas, including better spatial resolution, reduced radiation dose, in-vivo high-resolution CT imaging, flat-panel–detector CT, and dual-energy CT. As
these technologies are vetted and gain acceptance in clinical practice, they will become involved in protocols for trial imaging.
MRI: The evolution of MRI
technology has seen the use of both 1.5T and 3T magnets become conventional. For body applications, while 1.5T remains the current standard, the benefits of increased resolution at 3T ultimately will translate to trial imaging. The exquisite imaging obtained on 3T units for neuroimaging and the reproducibility available for cardiac imaging have already caused 3T MRI to make its way into limited clinical trials.
Ultrahigh-field (7T) imaging systems are currently in research use, typically for neuroimaging applications, but these are unlikely to find acceptance as a clinical technology (and, consequently, in clinical trials) due to their high overhead and limited scope of utility for clinical applications.
Since the introduction of multichannel coils, eight and 16-channel devices have become increasingly common, and modern systems are designed to accommodate upgrades to 24 or 32 channels (or more). Devices that are specific to laboratory research have been taken up to 100 channels. The higher-channel devices allow research protocols to focus on specific organs or specific disease processes, permitting imaging charters to be more precise in the impact of drugs being studied.
Integrated modalities: These (especially PET/CT and PET/MRI) are a particular focus for oncology applications. While PET, as a stand-alone modality, has been validated for use in clinical trials, radiologists have limited its use primarily to diagnosis (due to the lack of anatomical data). Integrating PET and CT provides the anatomical detail that helps imaging CROs to decrease the level of adjudication required across time points.
Manufacturers have surmounted incredible challenges in coupling the high magnetic fields of the MRI magnets
with PET equipment. As this challenge is overcome, PET/MRI will make the natural progression from the clinical sphere to trial methodology, promoting a more accurate understanding of the relationship of metabolic and structural data through a higher spatial resolution than is possible with PET/CT.
SoftwareImprovements in software relate
primarily to management of trials and trial imaging. This field also has witnessed an explosion in the use of software, on dedicated workstations, that allows improved visualization of imaging data.
Trial-management software: Clinical trials were once managed using stand-alone, proprietary information systems. This reliance resulted in the use of legacy systems that are slow, outdated, and ineffective. Newer, improved technology can reduce trial turnaround times tenfold.
Image collection: The key areas of differentiation for newer software are improved processes for image collection and image submission, as well as for removal of individuals’ identification. With the use of distributed networks, multiple sites can submit real-time data to a central imaging repository—with unparalleled security.
The key ingredients of newer imaging CRO systems include tools that allow monitoring of sites, acquisitions, and quality-assurance (QA) and quality-control (QC) processes in real time. These systems allow sponsors, project managers, and other key personnel full access to images and information.
Web-based viewers: For radiologists interpreting studies for clinical trials, these newer systems allow real-time monitoring of studies, as well as improving the activity of interpretation. Given the instantaneous nature of these systems, radiologists can participate in a complex protocol, reviewing images on patients as they are acquired and providing QC.
For example, if a sequence in a complex protocol is performed incorrectly, a radiologist could be involved while the patient is on the table (in a different location), making adjustments accordingly. In addition, the use of decentralized Web-
future trends in Clinical-trial Imaging By amit meHta, md
c l i n i c a l r e s e a r c h
amit mehta, md

Choose the Gold Standard. Choose ACR.
“ACR accreditation demonstrates
that our equipment meets the
highest clinical standards and
our patients receive the safest and
Þ nest quality imagi
ng available.”
— Michael J. Kelley, MD, FACR, FSIR,
Take time to prepare for accreditation … don’t delay. Apply by
June 30 or you could miss the CMS accreditation deadline and put your
reimbursements at risk. The ACR online application is quick and easy —
with no surprises. We outline what’s needed up front and provide you every
resource you need to succeed.
Only ACR delivers medical imaging accreditation from medical
imaging experts. To apply, visit .
The ACR advantage
Unmatched imaging review by radiologists
Peer-reviewed, educationally focused
Designed by radiologists and medical physicists
Guided by expert technologists
Multi-site, multi-modality pricing
7759 4.11
ADIS Accreditation
The time is now!

26 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
priors
based viewers allows geographically unrestricted interpretation.
While meeting FDA standards and maintaining good clinical practice, these newer systems allow radiologists with subspecialty expertise in geographically disparate locations to participate in trials. Involving subspecialty radiologists improves the overall quality of interpretation. This ultimately leads to fewer patients being dropped from trial protocols due to incorrect understanding of imaging findings, and it improves the characterization of response (versus nonresponse) to the use of drugs or devices. High-quality interpretations by subspecialty radiologists increase the efficiency—and decrease the cost—of trials.
Data integration and reporting: As the volume of data generated by advanced scanners proliferates, workstations and clinical-trial software need to be able to integrate, analyze, and report the data better. Next-generation management software provides new methods for data integration across the clinical-trial platform, allowing better integration of the medical images as they relate to patients enrolled in the trial. In addition, it offers improved tools for analysis and reporting that provide a broader scope, while maintaining the ability to find an individual treatment at a specific time.
Study-specific workflow configuration: As trial protocols evolve around newer technologies and better methodologies, clinical-trial software needs to allow for sponsor-driven, imaging CRO controlled specific workflow configurations. As legacy modalities from clinical practice and new modalities in the trial practice gain wider use, many protocols need to be configured to address particular issues regarding certain tools.
For example, newer PET radiopharmaceuticals have half-lives measured in minutes. As this mandates that a clinical-trial acquisition site be near a cyclotron, it is of great benefit to be able to configure workflow prior to transmitting test images or enrolling a patient.
Storage: Conventionally, imaging CROs have used paper-based storage or, more recently, limited hard-drive storage (with redundant backup) at a single physical location. Next-generation imaging CROs have embraced the use of off-site redundant SAN technology. This allows for the utmost security of data.
Other advances: As popular services such as Twitter have gained market share,
systems that incorporate similar real-time notifications in their software have become available to alert project managers or QA/QC personnel of potential problems. This allows imaging CROs to capture cleaner data and to decrease the number of patients/cases that need to be discarded due to improper acquisition or screening.
Workstations: While using subspecialty radiologists is a key to getting better data in clinical trials, these radiologists, in their clinical work, have begun to use specialized workstations to interrogate the data generated by improved modalities.
These workstations allow radiologists to provide more detailed analyses of structures affected by drugs or devices. Other workstation technologies that are raising the interest of trial-methodology architects include computer-aided detection, in-vivo modeling, fusion software, and physiologic measurement.
The integration of medical imaging into clinical trials is now validated and accepted. Legacy imaging CROs have helped to build this acceptance, but next-generation providers have begun to employ tools that promise to improve, accelerate, and reduce costs for the trials that bring drugs and devices to the marketplace.
As shown by the development of the Metrics Champion Consortium (www.metricschampion.org), imaging CROs are trying to standardize clinical trials. As we integrate newer modalities, technologies, and processes into clinical trials, we will improve our ability to bring drugs and devices to the public in record time.
Amit Mehta, MD, FRCP, is a vascular and interventional radiologist with the South Texas Radiology Group in San Antonio and is vice president of an imaging contract-research organization; [email protected].
n u m e r i c
Batten down the Hatches: Data Security and Breach
Do not underestimate the importance of physical and administrative safeguards when securing patient data. According
to Adam Greene, JD, MPH, attorney with the US DHHS Office of Civil Rights, 66% of patient-data breaches involving 500 patients or more were due to theft and loss (Figure 1). Just 7% were due to the more sensational category of hacking/IT incidents. Do not overlook paper records, either, as they accounted for 21% of large data breaches (Figure 2). Greene presented “HIPAA and Health IT: New Challenges, New Opportunities,” at the annual meeting of the Health Information
and Management Systems Society on February 21, 2011, in Orlando, Florida.
There were 8,524 privacy complaints in 2010, up from 6,534 in 2004, the first full year that HIPAA regulations were in place. The top five privacy issues are impermissible uses and disclosures, lack of reasonable and appropriate safeguards, failure to provide an individual with access to a designated record set, failure to use or disclose the minimum necessary information, and inadequate complaint processes. As of December 31, 2010, there were 221 reports involving more than 500 individuals and more than 14,000 reports involving fewer than 500 individuals.
figure 1. Data breaches involving 500 or more individuals since 2003, by type of breach, according to information from the US DHHS Office of Civil Rights.
figure 2. Data breaches involving 500 or more individuals since 2003, by location of breach, according to information from the US DHHS Office of Civil Rights.
improper disposal 6%other 0%
Hacking/itincident 7%
theft51%
Unauthorizedaccess/disclosure
21%
Loss 15%
Laptop24%
Paper records 21%
desktop computer
16%
Portable device 13%
Network server 11%
email 3%
electronic health record 2%
other 10%

INTEGRATEDMedicalPartners
RCM
10850W.ParkPlace,Suite1100,Milwaukee,WI53224•877-816-1467•www.integratedmp.com
ACHIEVESUSTAINEDSUCCESSBYBECOMINGINTEGRATED...&MOREEFFICIENT,STABLE&PROFITABLE.Aswithanybusiness,radiologypracticesareonacontinualmissiontomaximizeperformance,protabilityandsuccess.Yet,diagnostic imaging isn’t justanybusiness…especiallytoday.
Fromdeclining reimbursementand risingcosts topayerscrutinyandnewregulatorymandates, radiologypracticesareundersiege.Inaddition,youfaceuniquechallenges,notjustwithinyourpracticebutalsorelatedtobeingpartoftheoverallhealthcarepuzzle.
At IntegratedMedicalPartners,wehelpyouovercomethesechallengesbymaximizingyourpractice’sefciency,profitability and long-term stability and success.Withdemonstratedexpertiseanddiverse services,weenableyouto integratetoday’sbestpractices intoeveryaspectofyourorganization.Ourteamincorporatesitsindustry-leadingexperienceand intelligence intoyourpractice so itcanbecomeatrulyintegratedpartofthehealthcareenvironmentandaself-integrated,complete,successfulenterprise.
IntegratedMedicalPartnersgivesyouthepowertoachieve—andevensurpass—yourbusinessobjectivesandaspirations.ACHIEVEINTEGRATION—Callustoday.
TELERADIOLOGY:Maximizeefciency&utilization.
REVENUECYCLEMANAGEMENT:Increaseprotability&stability.
STRATEGY&LEADERSHIP:Optimizepositioning&success.
ANALYTICS&INFORMATICS:Operateintelligently.
ACHIEVEINTEGRATION

The lines are blurring and passions are running high between the practice and the teleradiology purveyor
Teleradiology | The Practice and the Purveyor
Wilson Wong, MD, was there when teleradiology took off, almost 15 years ago. Back then, there was a radiologist
shortage, and Wong saw a way to increase the efficiency of coverage and bring some relief to other radiologists who were laboring (as he was) under the constant burden of on-call night work.
In 1997, Wong started a company called Teleradiology Diagnostic Service (TDS), Inc, to serve the Southern California market; soon, he and three or four radiologists were issuing nighttime preliminary reports for hospital and radiology-group clients, mostly for emergency-department work. “I started TDS because I was tired of taking call,” Wong says. “Imagine working all night, and then you have to work the next day—another full-time job.”
It was more than a matter of ending night work for clients, though. It was a matter of streamlining after-hours reading, too. “If we could centralize, one radiologist could take more calls,” Wong recalls. Under the old on-call system, a radiologist at one hospital might spend half the night sitting idle. Wong says, “With the interruptions and the ups and downs, there were a lot of dead periods. The radiologist might sit there for 15 or 20 minutes.”
With TDS, a few radiologists soon were reading for 80 West Coast hospitals at night. Wong says, “There was no competition; everybody was clamoring to be a customer of ours.” In the
28 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
By George Wiley
Sharks in the Case Pool:Teleradiology, the Practice, and the Purveyor

Deliver Remarkable Results
Intelerad® Medical Systems is a recognized leader in medical imaging PACS, archiving and workflow solutions.
www.intelerad.com/rbj | 1-888-246-9774 | [email protected]
Accelerate. Stand Out. Breathe.RADIOLOGY TRANSFORMED
Imag
es b
y In
tele
rad
Med
ical
Sys
tem
s. A
ll rig
hts
rese
rved
.
Delight your referring physicians by delivering timely results with your organization’s branding. Mobile users can receive notification of critical results on the go with InteleConnect™, a zero footprint PACS-agnostic referring physician web portal. With InteleViewer™, physicians with image-intensive requirements get high performance across all modalities and bandwidths. PC and Mac compatible, it excels in any local or remote configuration through its smart streaming technology and allows instant messaging with the appropriate radiologist.
Come and visit us at SIIM 2011, Booth# 814.

Teleradiology | The Practice and the Purveyor
30 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
beginning, TDS used film digitizers to create electronic images at the hospitals and then transported them by telephone to radiologists at a centralized reading station.
TDS fashioned its own software for its RIS to create reports. It followed the technology curve upward until its image-transport and reporting systems were server based. “We became one of the largest (if not the largest) California-based teleradiology companies,” Wong says. He ran TDS for nine years; then, he sold the company to a major, national teleradiology company. He says. “I have done extremely well. People think I was smart to sell. The truth is that I was lucky.”
He was lucky because the rosy teleradiology world that Wong helped create has, some critics say, turned sullen and predatory. According to a 2011 article by Levin and Rao,1 more than 50% of US radiology practices are now outsourcing some of their work to teleradiology providers.
Fears Come TrueAccording to Levin and Rao,1 this
escalating adoption of teleradiology has created many ill effects for the imaging industry. Among them are the commoditization of imaging interpretations, the lowering of fees per interpretation, and the vulnerability of radiology groups’ existing hospital
contracts to predation by teleradiology providers.
Wong says that it is all true; the worst fears of teleradiology opponents have been realized—but it’s not all bad, he adds. While Levin and Rao1 warn that teleradiology might lower the quality of image interpretation, Wong argues that the opposite has been the case, at least in the late-night emergency-department venues where most teleradiology takes place.
Teleradiologists have become experts in emergency-care imaging—so much so that Wong expects them, one day, to have a subspecialty society of their own. Competition from teleradiologists has caused all radiologists to raise their standards, he argues. “Several sites have done reviews of accuracy and found that teleradiology is as good as the local radiology groups, if not better,” Wong says. “It’s the opposite of what the ACR® has predicted. It’s ironic.”
Wong agrees that competition from teleradiologists has been at least one force in cutting the price of interpretations. “When it started, the price was as high as $50 per case,” he says, “and now, the average price is below $30 per case.”
Some of that might be due to generally lower reimbursements, Wong says. He adds that the downward pressure on reimbursements isn’t going away. Where once there was a radiologist shortage,
today’s young radiology graduates sometimes can’t find jobs. He says, “The demand slows, and the supply comes up; the profit margin is going to be a lot less.”
Since selling his teleradiology company, Wong has gone back to being a radiologist. He is now a partner in Arcadia Radiology Medical Group in California. “My subspecialty is body imaging; I do some interventional work,” he says. “I don’t do any teleradiology, but I still read for them once in a while.”
He says that there are so many teleradiology providers in the market now that potential customers won’t even open their doors. He explains, “The customers don’t want to talk because they’re inundated with phone calls.” He says that it’s understandable that radiology groups would fear teleradiology companies stealing their hospital contracts. He says, “What people fear is that teleradiology is disruptive because it insinuates itself between the radiology group and the community it serves.”
That predation of contracts does happen, Wong says, but he argues that the truly predatory companies will get such bad reputations that they will fail. “The ACR is right in that teleradiology enables administrators of hospitals to bargain much harder with their radiology groups. What we have to learn is that knowing we can be replaced, we have to provide the best service to our hospitals so we won’t be replaced,” Wong says.
He adds that teleradiology is in a state of flux now, and it’s hard to tell how permutations in the service are going to play out—but teleradiology won’t go away. Emergency-department turnaround times for interpretations are much shorter, industrywide, than they were before teleradiology providers put pressure on everyone to produce results more rapidly, he says.
“Even the ACR people who say they don’t like teleradiology use it,” Wong says. He points to medical schools that offer subspecialized teleradiology as part of their services. He says, “The ultimate truth is that teleradiology enables you to get the best service for the price that you paid. It’s disruptive to contracts, but it improves patient care.”
The ultimate truth is that teleradiology enables you to get the best service for the price that you paid. It’s disruptive to contracts, but it improves patient care.
—Wilson Wong, Md arcadia radiology Medical group
We will never be a client of teleradiol-ogy providers. We are opposed to that whole model of providing partial service. We think it’s destructive to the relation-ship with providers. It’s our work, and we figure out a way to get it done.
—gregory C. Karnaze, Md, FaCr austin radiological association

Teleradiology | The Practice and the Purveyor
32 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
ruining radiologyThere are those—besides Levin and
Rao1— who take a far less sanguine view of teleradiology than Wong does. They think that the practice of radiology is being diminished by teleradiology providers who skim the interpretation-fee fat away from the other work that radiology groups must perform. Gregory C. Karnaze, MD, FACR, is a vascular and interventional radiologist with Austin Radiological Association (ARA) in Texas. ARA reads for 15 outpatient centers and 17 hospitals and has about 90 radiologist partners, Karnaze says.
“Not only are we not a client of teleradiology providers,” Karnaze says, “but we will never be a client. We are opposed to that whole model of providing partial service. We think it’s destructive to the relationship with providers. We follow the model that our practice takes care of our practice. It’s our work, and we figure out a way to get it done.”
Karnaze says that hiring teleradiology providers to do nighttime preliminary reports for an emergency department and leaving the exams to be overread (on final interpretation) the next day makes radiology groups look pampered and unprofessional. “I can tell you the emergency-department physicians are getting one interpretation at night—and having that changed the next day. They feel that’s bad patient care. Preliminary interpretation is a very flawed model and provides inferior care,” Karnaze says.
He continues, “Radiologists are just like any other physicians: We have an obligation to patients, the hospital, and our other medical colleagues to provide much more than interpretations. We serve as medical directors, set protocols, consult with physicians, and help with case management. We provide a full service, of which interpretation is a small subset. To extract that small subset and turn it into a commodity, bought and sold based on price, is to offer less than full service. It strips away the husk of rice to a lifeless kernel and sells that as a commodity.”
Karnaze makes a big distinction between teleradiology and distributed reading, wherein images are transmitted electronically to available radiologists or subspecialists within a defined network.
In that sense, “There’s no difference, whether the image is acquired next door or 10 miles away,” he says.
ARA has designated night readers for its hospitals’ emergency departments, but they do final reports, Karnaze says. ARA also markets its professional interpretation services, as well as infrastructure, such as PACS and IT, to nonradiology physician groups that have their own scanners. “We offer a world-class system to small medical practices,” Karnaze says.
Strategic advantageARA also is a member of what can
be called a loosely fashioned national radiology group. Named Strategic Radiology, it is headquartered in St Paul, Minnesota. Strategic Radiology is composed of 15 prominent radiology groups around the United States that
have joined forces to augment services and preserve full-service traditional radiology while gaining clout and payor leverage through size. Karnaze says that the vision within Strategic Radiology is eventually to provide distributed reading services among member groups and to outside clients that might choose to join the network.
Strategic Radiology’s members are in the process of ending all contracts with outside teleradiology providers and developing an after-hours service among members instead, Karnaze says. “It’s the number-one topic on the Strategic Radiology agenda,” he adds. Strategic Radiology will offer more than emergency-department interpretations and subspecialized interpretations, Karnaze says. It will help members develop best practices and achieve cost efficiencies in purchasing. One thing that it definitely will not do is go after other radiology groups’ hospital contracts.
Karnaze says that the radiologists in ARA are working hard with client hospitals to prepare for new forms of health-care delivery, such as accountable-care organizations (ACOs), that might be able to reduce the cost of health care. He says, “We are having discussions with all our hospitals to do everything we can to shorten patient stays. If we get reports to them faster, then patients can be turned over faster and treated at lower cost. We’ve already begun that dialogue.”
What ARA (and groups like it) do not want to see is nighttime teleradiology providers morphing into day readers, offering both night preliminary interpretations and daytime final interpretations to hospitals that might be struggling with provision of 24/7 imaging services. That’s exactly what’s happening, Karnaze says. Night services are now
beginning to challenge existing providers for lucrative hospital radiology contracts. “The teleradiology market is saturated, and many teleradiology providers have turned predatory on their customers and are beginning to pursue those hospital contracts,” Karnaze says.
Boots on the groundChristopher G. Ullrich, MD, FACR, is a
neuroradiologist with Charlotte Radiology PA in North Carolina, an 80-radiologist practice that is also a member of Strategic Radiology. Ullrich says that the big teleradiology companies face a grow-or-die cash-flow dilemma. If all they get from serving a small-to-medium hospital is a dozen or so night cases, the revenue isn’t sufficient to support the technological and administrative outlay that they must put in place for that client.
“They have to have enough IT infrastructure to go in and out with minimal human intervention—or the
We merged with another group to address our system with one voice. That added 17 radiologists to our group. That’s a trend that going to continue, where it makes sense.
—Christopher g. Ullrich, Md, FaCr Charlotte radiology Pa

overhead goes up, and the error rate goes up—and they’ve got to get people credentialed who are outside the state,” Ullrich says. The bottom line is that night-coverage teleradiology “is not a very attractive book of business, unless they also have the daytime work,” he adds.
To stay solvent, the big providers must become predatory. They have to go after radiology contracts at the hospitals that they serve, Ullrich says, but doing so puts them in another bind, which has nothing to do with the ethics of displacing an existing radiology group.
To get the daytime contracts, the teleradiology companies have to put at least a skeleton crew of live radiologists at the site. There has to be a face or two that referring physicians can see, somebody to do interventional radiology one or two days a week, and somebody to handle a face-to-face consultation.
Ullrich says that this is not easy. “The struggle to find the boots on the ground: That’s the Achilles heel of the national integrated practice,” he says. “There are lots of people who want to work nights so they can do something else during the day, but it’s hard to find a radiologist to go to a smaller community, take that practice, and run it while working for a national company. It’s hard to assemble even a medium-sized team if you’re going to take a lot of work out of the practice.”
The endgame for those who strictly supply teleradiology might be to compete for sites where reading volumes are high enough to yield a profit without displacing radiology groups. “There are books of work that don’t need boots on the ground,” Ullrich says.
For the rest of radiology, Ullrich sees continued consolidation, whether through a model like Strategic Radiology or through mergers of smaller groups into larger ones. Charlotte Radiology has already gone through one of those.
“We merged with another group to address our system with one voice,” Ullrich says. “That added 17 radiologists to our group. That’s a trend that’s going to continue, where it makes sense. Getting big is not the goal; it’s operational efficiency. Teleradiology has caused no groups to think they can’t be replaced, and if you’re small, you’re really replaceable.”
We did a survey in California and the feedback to us was that there’s still a need for night reading and a lot of groups need daytime subspecialized interpretation, so we said we’ve got to do the night to get the day.
—Fred gaschen, MBa radiological associates of Sacramento Medical group inc

Teleradiology | The Practice and the Purveyor
34 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
That’s a lesson that’s being learned all the time. Ullrich mentions locations in Virginia, Florida, and California where radiology groups have lost hospital contracts to replacement entities that are composed, at least partially, of teleradiologists. A lot of this activity has to do with what hospitals see as the changing health-care landscape, Ullrich says. “Hospitals believe in the ACO world; they can only function if they own the network,” Ullrich says.
a New Service lineIf any radiology group might have
been viewed as unassailable in a contract-takeover bid, it would have been Radiological Associates of Sacramento (RAS) Medical Group, Inc, in California, an 80-radiologist practice that is nearly a century old. RAS had a long history of providing interpretations for a string of central California hospitals operated by Sutter Health (Sacramento).
The Sutter Health contract was foundational to RAS, but the radiology group also ran a network of more than a dozen outpatient imaging centers, a handful of PET and nuclear-medicine centers, and about half a dozen centers providing radiation-oncology services. RAS seemed to have it all. It was a force to be reckoned with in the region; like ARA and Charlotte Radiology, it was a founding member of Strategic Radiology. Then, early in 2010, RAS lost its Sutter Health contract. Sutter Health decided to take its radiology operation in-house, under hospital ownership, and at least part of its staffing solution was reliance on teleradiology providers.
RAS has held its group together, but it has lost partners and has had to maximize its other ventures. Now, it has launched its own teleradiology service to make further use of its group, illustrating the statement of Mohandas Ghandi (1869–1948) that you become what you hate. As Fred Gaschen, MBA, RAS executive vice president, explains, “I’ve got a lot of mouths to feed.”
Gaschen says that the service primarily has concentrated, so far, on offering teleradiology services to the group’s own centers and a few other centers owned by others in the region—but it is branching
out, he adds. “We did a survey in California,” he says, “and the feedback to us was that there is still a need for night reading and a lot of groups need daytime subspecialized interpretation, so we said we’ve got to do the night to get the day.”
The teleradiology service will operate as a separate profit center, Gaschen says, and one of the early decisions regarding
it was to limit the number of radiologists doing interpretations (to simplify obtaining state licensure and hospital credentials). For the RAS service, the number of dedicated teleradiologists is 11. As Gaschen points out, these radiologists don’t just do teleradiology; they also perform daytime duties, when scheduled. They are full members of the RAS team, no different in standing than any other radiologists in the group.
This is an important distinction, Gaschen says, because part of the RAS marketing strategy is to emphasize that all the quality-control programs used at RAS will extend to the teleradiology service as well. A teleradiology client will be hiring an integral group with solid accumulated expertise.
“Part of the issue with teleradiology,” Gaschen says, “is determining whether you are hiring a commodity or contracting with an existing group that is also providing night interpretations and is there to help you be successful. That’s the approach that we take. We will do whatever the client wants. Right now, that’s all final interpretations, but some clients don’t
want those. It depends on the group. You have to give the group what it wants.”
infrastructure and iT HurdlesTeleradiology tends to be viewed
as a business with a low cost of entry: All radiologists need is an Internet connection for their home workstations, and off they can go. This turns out to be a misperception. Craig Roy is CIO at RAS, and he says that one of the limiting factors in implementing the RAS teleradiology service has simply been the amount of IT that he and his team can implement in a given time. Right now, Roy says, he’s putting together the technology to serve one major out-of-state teleradiology client. “We have four outside clients,” he adds, “but there are a bunch more just waiting on me.”
Over its long years with Sutter Health, RAS learned the landscape of putting together a community shared-image service so that prior exams and patient data could be accessed from any point in the RAS network. That legacy knowledge has been leveraged to incorporate the local imaging centers that the practice serves in a WAN, accessed via VPN. This allows patients in the client system to be integrated into the teleradiology billing array, and it lets those cases appear on the teleradiologist’s worklist.
Roy also employs a voice-recognition server with a workflow engine to integrate reports with the worklist. Finished
We have four outside clients, but there are a bunch more just waiting on me.
—Craig royradiological associates of Sacramento Medical group inc

reports can be delivered electronically or by fax. File-transfer methods are secure; electronic reports are ready for integration into the electronic health record at the client facility.
Roy recently finished implementation of a more difficult IT installation that will transfer both the exam images and the teleradiology report to an out-of-state client as a single package. Even though the images originated with the client, sending them back in concert with the report allows the client to access the images without having to devote staff time to matching images and reports. “Once our physician’s dictation is finished, that will go, via HL7 interface, to our PACS; it will become a DICOM object associated with the patient study, so both the images and the results can be sent to our client,” Roy says.
Automating ProcessesIt’s this sort of timesaving service,
Roy says, that will give RAS an edge in
the teleradiology market—but it doesn’t come easily. “What if we receive the same medical-record numbers from two different out-of-state clients in different states? Our PACS can’t process that, since it uses the medical-record number,” Roy says. He explains that if the teleradiology service distinguishes between such records simply by attaching a prefix or suffix, when the case is sent back to the client, that client’s software won’t recognize its own patient’s file.
“That’s the nut I’m trying to crack. We may have to build, through an interface engine, a new system that will recognize a prefix and then strip it off before it’s sent back,” Roy says. It’s also important to RAS for files on its end to be populated automatically, so that it doesn’t have to add information manually. “That eliminates three minutes to scan and retype that into our order system,” Roy explains.
Getting software programs to do this requires working with equipment vendors, which raises more difficulties.
Roy doesn’t want his staff rewriting vendors’ code because then warranties can become void and contract violations can come into play. The vendors have to be brought into the effort.
It’s hurdles like these that make teleradiology less than easy to implement these days, Roy says. He estimates it costs at least $1 million to obtain the necessary software and equipment—and far more to pull together the support of technologists, radiologists, and support staff. “I don’t know if there’s enough business out there,” he says. “I think the landscape is getting more and more competitive.”
The Size FactorNobody seems to know quite how
many teleradiology providers are out there. Levin and Rao1 cite 2008 advertising that shows at least 33 teleradiology vendors. The Joint Commission accredits more than 30 teleradiology companies, according to Michael Kulczycki,
www.imagingBiz.comYour Destination Portal for News about the Business of Radiology Bookmark It Now!
imagingBiz.com17291 Irvine Blvd., Ste. 105, Tustin, California
714.832.6400
• Frequent news updates• Perspectives on the news• StatRead Blog• Archives ·ImagingBiz.comnewsletter ·Radiology Business Journal ·Radinformatics.com ·MedicalImagingReview ·RadAnalytics ...andthenewlylaunched ·HealthCXO
Submit news to Web News Editor Julie Ritzer Ross at
For advertising information, contact Sales & Marketing Director
Sharon Fitzgerald at [email protected];
330.835.3640

Teleradiology | The Practice and the Purveyor
36 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
executive director of the Ambulatory Care Accreditation Program.
RadNet, Inc, Los Angeles, California, which operates a multistate network of 200 outpatient imaging centers, estimates that there are more—with as many as 200 teleradiology vendors in the market today. RadNet recently purchased, intact, a national teleradiology service, and it is marketing the service through its network, effectively creating a new outpatient imaging delivery model. Its 40 teleradiologists are already reading for 100 hospitals, and the service will eventually be integrated into the RadNet electronic backbone, turning RadNet into a giant multiservice provider where images and text data can be exchanged.
The question is whether it and some of the other national teleradiology vendors will turn out to be unwieldy because of their size. Wong says that one of the most perplexing questions about teleradiology vendors is their optimal size.
“When I first looked into teleradiology, I thought the big company seemed to be better,” he says. “I thought the small company might not survive. Now, the small company seems to have a unique advantage—in the long run, all of medicine and radiology is local.”
What’s happening now, other than the big national teleradiology companies trying to build and hold onto turf, is that a lot of prominent regional radiology practices (such as ARA and RAS) are organizing teleradiology ventures aimed at bringing efficiency and expertise into the market without infringing on existing radiology practices.
The rria ModelAnother large regional practice that
has grown through the use of its internal teleradiology services is Riverside
Radiology and Interventional Associates (RRIA), Inc, Columbus, Ohio. Marcia Flaherty is RRIA’s CEO, and Mark Alfonso, MD, a body imager, is president of the physician-owned group.
RRIA has 70 radiologists in its practice. It reads for about 15 regional hospitals, including the 1,000-bed Riverside Methodist Hospital in Columbus, Flaherty says. It also interprets for imaging centers and for medical practices that have their own imaging equipment. Like ARA and RAS, RRIA is a founding member of Strategic Radiology. “We only provide telemedicine as it pertains to our practice,” Flaherty says, adding that the practice provides only final (not preliminary) interpretations.
Alfonso adds, “We started doing after-hours interpretations, at the request of Riverside Methodist Hospital, 14 years ago. We started in-house because it was a tremendous service to patients and referrers to provide final interpretations contemporaneously with the study.”
RRIA has invested more than $1 million, Alfonso says, in the development of a software solution to link all the sites it handles to a single database that is organized around the radiologists’ workflow solution.
“Anyplace that we provide radiology coverage, our IT solution will integrate those databases, and a patient will be automatically picked up,” Alfonso says. “Our PACS will query the patient by descriptors (such as date of birth and name); it almost never pulls up the wrong patient. If the patient was in another facility, we can see if he or she had exams. Patients do move around, to our surprise.”
Flaherty says, “The system shows the radiologist where the patient may have been. That automatically appears on the
worklist, and the radiologist can access any prior studies. This also allows the radiologists to organize their workflow for greater efficiency.” RRIA’s teleradiology solution is a hybrid of proprietary technology and custom software developed in-house. “We couldn’t find it on the market, so we built it,” Flaherty says.
RRIA can provide a PACS solution or integrate its systems with a client’s existing PACS, Alfonso says. Clients receive the final report on their systems. RRIA uses voice-recognition technology, but a transcriptionist edits and corrects the dictation. Alfonso adds, “They’re two or three minutes behind us; it doesn’t add much to the time, but it adds to the quality of the report.”
Flaherty says, “Quality is an important part of our practice and of pending health-care initiatives, such as ACOs. We have a robust quality-assurance (QA) function, including a medical director dedicated to QA across our sites. We want to be ahead of the curve when reimbursement changes require demonstration of the quality of services. With the creation of our IT infrastructure, we believe we’ve made our radiologists much more productive. We feel we can make the transition to bundled care and new reimbursement models.”
RRIA expects that as a member of Strategic Radiology, it will eventually become part of a larger delivery network. “The whole purpose is not to compete with other radiology groups, but to benefit radiology practices,” Flaherty says. “We feel Strategic Radiology is a longer-lasting solution than an investor-owned teleradiology company.”
Alfonso expects the consolidation of health-care entities to accelerate as the push continues for economies of scale. He says, “There will be fewer players in the market and significantly bigger—much larger—networks. The days of the two- or three-, or even 10-person radiology group are becoming history.”
RRIA wants enough size to reside on the right side of history, but it’s also mindful of the dictum that all health care is local. “We have a sphere of influence in Ohio. We’re not trying to be a national radiology corporation,” Flaherty says.
There will be fewer players in the market and significantly bigger—much larger—networks. The days of the two- or three-, or even 10-person radiology group are becoming history.
—Mark alfonso, Md riverside radiology and interventional associates inc

Thin-client speed and accessibility when and where you need it. Rich clinical tools, automation and ease of use for fast, accurate quality care.
Imaging anytime, anywhere.
www.vitalimages.com®
®
Visit us at SIIM 2011, booth # 609

The challenges of running imaging operations are increased by market changes and multiple disparate IT systems. To succeed, you must have good intelligence … and know how to use it.
For over 15 years, Regents Health Resources has helped more than 500 imaging clients develop and optimize their services, facilities, operations and technology. Today, we are leaders in imaging business intelligence who leverage considerable data and experience to help our clients achieve market dominance.
Regents is also the management and resources behind National Imaging Network, an imaging collaborative formed to improve the efficiency, utilization and long-term stability for medical imaging providers nationwide.
Improve your performance with industry-leading expertise trusted by imaging providers and hospitals everywhere. Call today.
Thrive and grow
Optimizing imaging businesses with comprehensive services ...Market analysis & planningStrategic planning · Financial modelingTechnology & RIS/PACS assessment & planningOperations assessment · Customer-service planningHealthcare business-intelligence tools/softwareImaging center sales, acquisitions & developmentProcurement services · ValuationsJoint-venture planning · Project management
(615) 550-2633 · Toll-Free (800) 423-4935810 Crescent Centre Drive, Suite 100Franklin, TN 37067www.RegentsHealth.comwww.NationalImagingNetwork.com
The Standard in Medical Imaging Intelligence
with industry-leading business intelligence.
Regents_final.indd 1 4/20/11 10:26:21 PM

Hospital-based Versus Freestanding Outpatient Imaging Services
During the first half of the first decade of the 21st century, freestanding outpatient imaging
grew at an accelerated rate, capturing market share from hospital outpatient imaging departments. After years of losses to what were typically more nimble freestanding outpatient provid-ers, hospitals have taken a renewed interest in this service line.
Introduction: The first installment in the Imaging Market File is based on data from the National Imaging Network (NIN), an outgrowth of the hospital and radiology-practice consulting work of Regents Health Resources, a medical-imaging consultancy based in Franklin, Tennessee. In 2009, Regents Health Resources began developing the Web-based tools that would constitute the back end of the network and enable members to access their own disparate data easily while comparing their results to national and regional performance benchmarks, as well as to those from similar settings. Fed
The trend toward hospital-based imaging: Deep cuts to imaging reimbursement rates in the MPFS have led many imaging centers to exit the business, while others struggle to survive. Meanwhile, hospitals have been acquiring centers in their markets. Eight of last year’s top 20 diagnostic imaging center chains were hospital owned, up from five in 2006.1
The drivers: The migration of outpatient imaging from freestanding to hospital based is being driven by deep cuts to reimbursement for the 7000 CPT® codes paid under the MPFS, by health systems’ interest in recouping ground lost to service-oriented outpatient imaging operators over the past decade, and by more favorable reimbursement under the Hospital Outpatient Prospective Payment System (HOPPS).
Note: Rates are blended and include all commercial and government payors for each provider, excluding professional revenues. Outpatient imaging center global revenue was reduced by estimated professional percentages using the following reductions: MRI, 18%; CT, 19%; ultrasound, 20%; radiography, 30%; mammography, 30%; nuclear medicine, 19%; and PET/CT, 18%.
Average Revenue (Blended) per Procedure, Comparing Hospital and Outpatient Imaging Center Technical-component Reimbursement
Modality Hospital outpatient average reiMburseMent iMagingcenter revenue reiMburseMent differential
MRI $832.46 $460.95 1.8
CT $626.66 $245.83 2.54
Ultrasound $241.23 $87.01 2.77
Radiography $106.45 $44.55 2.39
Mammography $121.44 $78.07 1.55
Nuclear medicine $634.71 $181.72 3.49
PET/CT $2,898.95 $1,243.64 2.33
Overall average 2.41
Exam mix: According to the NIN database, 63 CPT codes represent 80% of all hospital exam volume, and 56 CPT codes represent 80% of all outpatient imaging company exam volume. MRI exams account for more than 2.5 times the percentage of total volume in the outpatient setting than they do in the hospital setting. Conversely, CT exams represent one-fifth of the volume in the hospital setting, but slightly less than 14% of the volume in the outpatient setting. Mammography represents twice the percentage of total volume in the outpatient setting that it represents in the hospital setting. Advanced imaging (MRI, CT, PET, and nuclear medicine) accounts for roughly the same percentage of total exams in both settings: 29.9% in the outpatient setting and 30.2 in the hospital setting.
by blinded data from 96 of Regents Health Resources’ 500 clients, the initial database represents 6.9 million exams acquired in diverse settings from 2008 to the present, including hospital-based outpatient imaging centers and freestanding outpatient imaging centers in 72 communities (in 21 states). Access to the NIN is available through a subscription service to hospitals, imaging-center owners, and physician practices and is designed to provide ongoing active business support and intelligence, including access to referring physician, financial, and clinical data.
Hospitals Outpatient Imaging Centers
Exam mix, by modality and percentage of total, in hospitals and outpatient imaging centers.
Radiography50.49%
Ultrasound10.78%
CT20.07%
MRI5.97% PET
0.13%
Nuclear medicine4.03%
Mammography8.28%
Dual-energy x-ray absorptiometry0.26%
Radiography35.88%
Ultrasound16.96%
CT13.93%
MRI13.59%
PET0.92%
Nuclear medicine1.46%
Mammography15.07%
Dual-energy x-ray absorptiometry2.19%
1. Kyes K. The top 20 imaging-center chains. Radiology Business Journal. 2010;4:30-35.
Imaging Market File
Spo
nSo
red
Su
pple
men
t

Comparison: The top 10 CPT codes by volume for hospitals and outpatient imaging centers were compared, representing 1.9 million exams out of the 6.9 million in the NIN database, collected from 2008 through 2010. To illustrate the differences, MPFS and HOPPS reimbursement rates for the state of Maryland were used from 2010 and 2011. HOPPS rates show a 1.7% to 177% premium over the MPFS. In the cases in which the rates are higher for the MPFS (mainly MRI), the procedure is reimbursed at the lower HOPPS rate. The two codes for the exams performed most frequently in the hospital setting are associated with radiography. Significantly, those codes display the greatest variance between HOPPS and MPFS reimbursement.
Top 10 CPT Codes by Volume, Hospital Outpatient
cpt description percentage 2010 2011 2010 2011 2011Hopps/ oftotal Mpfs($) Mpfs($) Hopps($) Hopps($) Mpfsvariance
71020........Chest x-ray ........................................8.9% ..............20.23 ............22.12 ............. 44.79 ............. 45.04 ................ 103.6%71010........Chest x-ray ......................................... 8% ................14.89 ............16.23 ............. 44.79 ............. 45.04 ................ 177.5%70450........Ct head/brain w/o Contrast ...............3.1% ..............158.3 ...........168.34 ............ 194.6 ............ 193.85 ................ 15.2%G0202 .......sCreeninG mammoGraphy, diGital ..........2.4% ..............99.56 ............114.2 ............. 99.56 ............. 114.2 ....................0%72193........Ct pelvis w/Contrast ..........................2.1% .............241.06 ..........257.47 ............ 296.3 ............ 299.81 ................ 16.4%74160........Ct abdomen w/Contrast .....................2.1% .............274.25 ..........294.66 ............ 296.3 ............ 299.81 ................. 1.7%74000........x-ray exam of abdomen .......................1.4% ..............16.41 .............17.7 .............. 44.79 ............. 45.04 ................ 154.5%76700........Us exam, abdomen, Complete ...............1.2% ..............97.27 ...........109.78 ............ 97.06 ............. 96.28 ................ –12.3%72192........Ct pelvis w/o Contrast .......................1.1% .............194.15 ...........205.9 ............. 194.6 ............ 193.85 ................ –5.9%74150........Ct abdomen w/o Contrast ................... 1% ...............192.62 ..........204.43 ............ 194.6 ............ 193.85 ................ –5.2%
Top 10 CPT Codes by Volume, Outpatient Imaging Center
cpt description percentage 2010 2011 2010 2011 2011Hopps/ oftotal Mpfs($) Mpfs($) Hopps($) Hopps($) Mpfsvariance
71020.........Chest x-ray ......................................2.5% ............... 20.23 ...........22.12 ............ 44.79 ..............45.04................ 103.6%71010.........Chest x-ray ....................................... 2% ................. 14.89 ...........16.23 ............ 44.79 ..............45.04................ 177.5%G0202 ........sCreeninG mammoGraphy, diGital ........1.7% ............... 99.56 ...........114.2 ............ 99.56 ..............114.2....................0%77057.........mammoGram, sCreeninG .....................0.9% ................ 45.4 ............50.11 ............. 45.4 ...............50.11....................0%76700* .......Us exam, abdomen, Complete .............0.8% ............... 97.27 ..........109.78 ........... 97.05 ..............96.28................ –12.3%70450.........Ct head/brain w/o Contrast .............0.7% ............... 158.3 ..........168.34 ........... 194.6 .............193.85................ 15.2%74160.........Ct abdomen w/Contrast ...................0.7% .............. 274.25 .........294.66 ........... 296.3 .............299.81................. 1.7%72148* .......mri lUmbar spine w/o Contrast .........0.7% ............... 369.6 .........427.62 .......... 348.68 ............342.93............... –19.8%72193.........Ct pelvis w/Contrast .......................0.6% .............. 241.06 .........257.47 ........... 296.3 .............299.81................ 16.4%73562.........x-ray exam of knee, 3 .......................0.6% ............... 25.18 ...........29.12 ............ 44.79 ..............45.04................. 54.7%
* Because of the lesser-of rule governing MPFS reimbursement, this CPT code is reimbursed at the lower HOPPS rate.
Scheduling and registration
Reports: turnaround time and quality
Preauthorization
Quality of and access to radiologists
Imaging technology
Top reasons for referring physicians’ dissatisfaction.
The prize: Referring-physician relationships that ensure a steady stream of business are the lifeblood of both hospital radiology departments and radiology practices. The follow-ing figures and tables are based on customer-service surveys of more than 1,200 referring-physicians conducted by Regents Health Resources for multiple clients. They identify the top customer-service issues and preferences for imaging provider location.
Top 10 Reasons to Refer Patients to Specific Imaging Locations
1. Patient preference .......................... 49.8%
2. Location ........................................ 49.8%
3. Insurance carrier ........................... 47.6%
4. Cost to patient ............................... 21.3%
5. Technology .................................... 19.7%
6. Customer service ........................... 19.3%
7. Radiologists ................................... 14.4%
8. Patient customer service .................. 8.4%
9. No preauthorization needed ............ 4.6%
10. No insurance verification needed .. 2.2%
Imaging Market File
21.4%
23.4%
32.8%
34.2%
53.5%
About the sponsor: Regents Health Resources (www.regentshealth.com) was formed in 1996 to assist hospitals and physicians in the development and management of their medical-imaging and oncology services. The consultancy has served more than 500 clients nationwide with a diverse range of services, from strategic planning and operational assessments to joint-venture planning, valuations, and imaging-center sales and acquisitions.
The Standard in Medical Imaging Intelligence

Teleradiology | The Practice and the Purveyor
www.imagingbiz.com | april/May 2011 | Radiology Business JouRnal 41
“We focus on our corner of the world—and that’s critical.”
Finding the right SolutionWith national teleradiology companies
expanding turf and regional players carving out market segments, what does the small radiology practice do to fill its after-hours interpretation needs? Nancy Holland, MBA, MHA, is practice administrator at High Point Radiological Services, PA, in North Carolina. The group has eight radiologists, and it reads for two hospitals and a joint-venture imaging center. It interprets approximately 185,000 studies per year.
Faced with finding a nighttime service to do preliminary interpretations, Holland says, she did phone interviews with about 10 teleradiology providers and invited three to undergo on-site interviews. High Point Radiological Services chose a national provider that uses only US-based teleradiologists (a requirement of one of its hospitals).
Holland says that a key determinant of the choice was making sure that the teleradiology company would not try to take over the practice. “That was a real concern; a lot are now doing daytime work,” she says. “We included a noncompete clause. That threat is still out there.” Holland says that the relationship has worked well and that the hospitals have been satisfied. The teleradiology vendor installed the necessary equipment in the hospitals, and its discrepancy rate has been within reason, she adds.
Finding the right teleradiology vendor was critical. She says, “It saves us two FTE radiologist positions.” She adds that High Point Radiological Services was careful to work closely with the hospitals throughout the process. “If there’s a contentious relationship with your hospital, you’re always in danger of losing that contract. Communication is the key to keeping it,” she says.
Full CircleAlicia Vasquez, CRA, FRMBA, is
administrator at Arcadia Radiology Medical Group, the same nine-physician California practice where Wong is now a radiologist partner. She also serves as president of the RBMA. Vasquez says
that Arcadia Radiology Medical Group continues to use the same national teleradiology vendor to which Wong sold his smaller teleradiology company—not out of loyalty, but because it is a good provider.
Vasquez says that she audits her teleradiology vendor and compares it to others on the market, even if she’s satisfied with the service. “Every other year, we put out a request for proposals, talk to the other vendors, and weigh the pros and cons of switching,” she says. “We want the ability to look at apples-to-apples comparisons.”
She advises caution in switching vendors, however. “If you were to change your teleradiology provider and that new provider put the relationship you have with your hospital in jeopardy, it wouldn’t be worth the change,” she says. Key factors in choosing a nighttime teleradiology provider are turnaround times for reports on emergency-department cases and flexibility in working with the radiologists in your group, Vasquez explains.
Turnaround time is critical because keeping patients flowing through the emergency department is a major concern of hospitals, she says. Flexibility is important because some radiologists want extra work to supplement their incomes. At Arcadia Radiology Medical Group, some of the younger physicians take on night work to earn additional income, and Vasquez says that the teleradiology vendor has to understand that. On the other hand, if there’s an event or an illness that reduces radiologist availability, the teleradiology vendor has to be willing to step in with extra help. Vasquez says that her vendor is good about that.
“There are a lot of radiologists out there available and wanting to work,” Vasquez
says. “They will go where they find jobs. That being said, I haven’t seen a major proliferation of teleradiology vendors. I think the market is already saturated.”
There is no doubt that teleradiology predators—the sharks in the case pool—are out there. Daytime final-interpretation volumes are the engine projected to provide growth for many of the large teleradiology providers. Some of those companies are not averse to poaching contracts from entrenched radiology practices (a consequence of a competitive market).
It is also clear that radiology, as it is practiced today, would be seriously disrupted if teleradiology providers suddenly disappeared. In filling staffing and subspecialty gaps, teleradiology providers are ensured a market among hospitals and radiology practices. This opportunity is not lost on large, technically savvy practices that have the resources needed to enter the fray. As health care moves into an uncertain future, will all teleradiology practices find enough food to stay afloat?
George Wiley is a contributing writer for Radiology Business Journal.
reference1. Levin DC, Rao VM. Outsourcing to teleradiology companies: bad for radiology, bad for radiologists. J Am Coll Radiol. 2011;8(2):104-108.
There are a lot of radiologists out there available and wanting to work. They will go where they find jobs. That being said, I haven’t seen a major prolif-eration of teleradiology vendors. I think the market is already saturated.
—alicia Vasquez, arcadia radiology Medical group, Ca

To prepare to meet future health-care–delivery needs, this nonprofit health-care system considered all of the options for financing an ambitious outpatient imaging center initiative
HealtH SyStem | Outpatient Imaging Initiatives
While there have been significant changes in the imaging market over the past 20 years, we continue
to witness sea changes within the sector, increasing pressure on operators, administrators, and physicians. Within Saint Thomas Health Services (STHS), Nashville, Tennessee, inpatient and outpatient imaging services are available predominantly in three large system hospitals: Baptist Hospital and Saint Thomas Hospital in Nashville and Middle Tennessee Medical Center (MTMC) in Murfreesboro.
The hospitals’ campus-based imaging services are not physically or organizationally distinct for outpatients, but serve both inpatients and outpatients. STHS does, however, have some ownership experience in two freestanding outpatient imaging center joint ventures in the primary market of MTMC.
Freestanding imaging centers (including those owned by competing health systems, physicians, and proprietary companies) are prevalent in the Nashville and Murfreesboro markets. From fiscal year (FY) 2007 to FY 2009, outpatient volumes for MRI and CT at the three large STHS hospitals declined by 19% and 3%, respectively, creating motivation to increase market share. Long-term strategic considerations, including health-care reform, technology, and other factors, also concentrated
our attention on outpatient imaging opportunities.
Strategic ContextBeginning in 2009, plans were
developed by the STHS strategic-development team led by Wesley O. Littrell, president and CEO of Saint Thomas Affiliates and chief strategy officer for STHS. This series of plans involved STHS and various potential equity partners.
Plan A: As part of a five-year strategic assessment in FY 2009, STHS proposed the development of a network of medical villages that would consolidate outpatient imaging and other ambulatory services near the campus of its Nashville hospitals, with a similar village to be implemented adjacent to its replacement hospital at MTMC (which was under construction). Both projects, with the potential to generate strong returns on investment, were capital intensive; consequently, they were not approved due to competition with other system projects.
Plan B: In late spring 2009, STHS entered into discussions with a corporate partner regarding a joint venture in which the partner would acquire four local imaging centers. In addition, the partner would contribute sufficient cash to develop the original medical-village initiative, and STHS would contribute future hospital outpatient imaging volume for equity in the venture. The two
existing, joint-venture imaging centers near MTMC would be contributed and physically consolidated into the village in that market. While this plan was creative and sound in concept, the partner was unable to acquire the local imaging centers and required extraordinary control and management rights in the potential venture, which led to a termination of those negotiations.
Plan C: STHS reached out to both of the radiology groups that provided inpatient coverage to the system’s hospitals and to Premier Radiology (Nashville)—a direct competitor operating three large freestanding centers in this market—regarding their interest in discussing a joint-venture network of imaging centers. A four-party confidentiality agreement was signed, and all parties commissioned separate fair-market valuations of their respective imaging enterprises, which would be consolidated in the potential venture. The valuation process involved numerous and frequent meetings between STHS and the radiology groups from September through November 2009.
Part of the challenge, for hospital executives, in funding the growth of outpatient business is that such capital investments are usually made at the expense of the traditional and genuine hospital needs. Plans B and C represented a decision to pursue creative options to fund outpatient imaging growth for the system. A process that started
42 RadIOlOgy BusIness JOuRnal | april/May 2011 | www.imagingbiz.com
By Tom Blankenship; Jason Dinger; and Sheila Sferrella, MAS, RT(R), CRA, FAHRA
Financing Outpatient Imaging Initiatives:The Saint Thomas Health Services Experience

www.imagingbiz.com | april/May 2011 | RadIOlOgy BusIness JOuRnal 43
with identifying three venture-capital companies ultimately yielded the lesson that having the money was only one piece of the equation—a large piece, but not the only one of significance.
Identifying and selecting the right partners were pivotal for this venture. The system reached out to a competitor (Premier Radiology) based on its outstanding reputation for service, its experience in the market, and the success of its existing centers. The cultures of Premier Radiology and MidState Radiology (Murfreesboro)—already an STHS partner—were found to be consistent and based on shared values.
In March 2011, STHS announced the formation of Saint Thomas Outpatient Imaging, a $100 million joint venture of STHS, Premier Radiology, and MidState Radiology that will provide outpatient imaging services to patients at eight locations, making it the largest network of outpatient imaging centers in Middle Tennessee.
transactional ChallengesIt’s not surprising that the transaction
process, even among these compatible partners, included three significant challenges: valuations, going-forward projections, and definitive-agreement development. It was relatively easy, even with two separate valuation consultants representing different parties, to agree on a valuation approach for existing imaging centers.
In the end, analyses of discounted cash flow (based on consistent methods and assumptions) were used to assign value to the existing imaging centers and to establish the contribution value for the new venture. A similarly consistent approach was taken in determining the value of the contributed future hospital outpatient volumes, based on agreed-upon capital investments necessary to provide service to those volumes under nonhospital revenue and operating-expense assumptions.
Obviously, the parties had a mutual
interest in determining how well they would do as partial owners of the venture (compared with the status quo), so the development of a well-vetted common set of operating projections was essential to reaching a shared confidence level and a shared position on the ultimate go/no-go assessment.
There is no good substitute for excellent and knowledgeable counsel; involved early, these individuals can transform a shared vision and operating model into an appropriately constructed vehicle for the venture (in this case, a limited-liability company) and the stacks of corollary contribution agreements, assignments, schedules, and exhibits. Painstaking definition of what one hopes are remote occurrences—such as unwind provisions and agreements for termination of professional services agreements—can be uncomfortable, but it is essential to resolve these questions as early as possible.
Traditionally, nonprofit health-care

HealtH SyStem | Outpatient Imaging Initiatives
44 RadIOlOgy BusIness JOuRnal | april/May 2011 | www.imagingbiz.com
organizations form a conservative group, so the creative financing that led up to the March announcement establishing a joint-venture outpatient imaging company is something of a departure from business as usual. We thank the team that supported us and helped us bring this deal to closure, beginning with Mike Schatzlein, MD, CEO of STHS, who arrived in the middle of negotiations, and our executive sponsor, Wesley O. Littrell, who helped us every step of the way.
We thank our colleagues at Ascension Health (St Louis, Missouri), who assisted us with board approvals and with financing, capital, and legal issues. The team at STHS includes Alan Straus, STHS CFO; Jay Galbreath, director of strategic financial planning; Cindy Williams, director of joint-venture contracting for managed care; and our three acute-care hospitals’ CEOs, Bernard Sherry, Dawn Rudolph, and Gordon Ferguson.
Our partners at Premier Radiology include Chad Calendine, MD, president; Michael Moreland, CEO; and Mark Gaw, CFO. Our partners at MidState Radiology include Max Moss, MD; Rick Smith, MD; and Holly Ramsey. We also had tremendous support and guidance from our legal colleagues, E. Berry Holt, Kevin Campbell, and Abbie DeBlasis.
Financing the Imaging VentureThere are three primary vehicles used,
alone or in combination, for financing new imaging ventures: debt, private equity, and the joint venture. Both hospitals or physician groups have aggressively pursued unique debt vehicles over the past decade. Low interest rates offered by equipment manufacturers, the desire to retain the majority of equity, and the ability to make independent decisions have made debt an attractive option to many imaging leaders.
Physician practices, however, often have limited cash-flow levels and find it difficult to raise enough debt to continue rapid expansion. Tightening of the credit markets has also made it difficult for centers to gain access to low-cost debt opportunities, further restricting growth and development. Debt financing entails material guarantees, in the form of personal property and assets, to be provided by physicians and other independent owners who want to continue expansion and growth; these guarantees are something that most want to keep to a minimum.
The realities and constraints of debt financing have created a number of new partnerships between large imaging companies and private-equity companies. In this instance, private-equity groups or venture-capital companies provide an influx of cash and resources to accelerate the growth of new and existing centers. In return, most companies take a majority stake in the imaging company, hold most of the governing board seats, and—while perhaps not requiring operating control—can make significant changes in leadership, should performance not meet expectations.
These terms can be very attractive to imaging companies that want to grow aggressively and need a new influx of cash to move into new markets or help fund enough growth to let them become attractive to private buyers or the public market. Many physicians and hospitals,
however, have little experience with the private-equity market and are leery of partnering with experienced investment bankers who are solely focused on generating strong returns for their limited partners.
Others have found the forfeiting of control and of the sole ability to dictate a path forward to be the most difficult challenge in working with financing partners. It should also be noted that outside of their financial strength, private-equity and venture-capital companies might provide limited strategic strength in the local and national markets. They might have limited access to new markets, might have few relationships with physicians, and might lack the operational expertise to help with IT integration and other long-term strategic initiatives.
the Joint VentureFor imaging companies looking for
a long-term strategic partner that will help with same-store growth and the development of new centers, a joint-venture structure might be the best alternative. In these cases, imaging centers might come together with hospitals or large physician groups. The entities sometimes merge their existing assets into a new company, while in other instances, one entity might provide assets and the other might provide financing.
A joint-venture partner differs from a private-equity company in that it almost always brings a strategic asset and outlook to growing the imaging venture. Some partners might be able to open up new markets where they have hospitals or employed physicians; others will provide financing with better terms, less need for operating control, or unique IT infrastructure to tie the imaging center more closely to its current and potential referral streams.
It should be emphasized that joint ventures come in all shapes and sizes, with equity levels, governance, and operating control varying widely. It is precisely this flexibility that can be the model’s greatest strength, allowing partners to craft a unique structure that meets both entities’ strategic terms.
It is important to note, however, that the three structures described (debt, private
It should also be noted that outside of their financial strength, private-equity and venture-capital companies might provide limited strategic strength in the local and national markets.
—tom BlankenshipSaint thomas Health Services

GROWTH GUARANTEED
Chances are, your imaging center’s revenue growth is being hindered by fairly common problems. Workflow inefficiencies. Front-end denials. Prolonged collections. Revana is committed to helping you overcome these challenges and capture more revenue—in fact, we guarantee you’ll see revenue growth. With our proven combination of systems and services, your medical imaging center can achieve better results.
Revana. You take care of your patients. We’ll take care of your revenue. Guaranteed.
www.revanahealth.com
888.973.8262
REV11988-4_LaunchAd3_8125x10875_F.indd 1 4/14/11 9:13:15 AM

HealtH SyStem | Outpatient Imaging Initiatives
46 RadIOlOgy BusIness JOuRnal | april/May 2011 | www.imagingbiz.com
equity, and the joint venture) are not mutually exclusive. Many (if not all) joint ventures take on some debt to continue expansion and preserve an adequate cash balance. A private-equity company might also partner with an existing joint venture to help it expand regionally or nationally, increasing its chances of being acquired by a larger player or of eventually entering the public market.
Private-equity companies might also invest in a management company that helps form local joint ventures between hospitals and physicians, taking a minority stake in each venture formed. This has been an especially popular structure, during the past decade, for parties looking for financing and management experience.
Whichever option is chosen, the key is understanding how much you’re willing to invest, what level of control you will require, and how large you hope your entity will become. These three fundamental areas not only will dictate which partner will be best over the long run, but will also dictate the areas in which you will most probably need to compromise.
acquisitions and alternativesOne of the perennial questions in our
industry is whether to acquire existing centers or build new centers in order to ensure long-term growth. Our view is that both are necessary for long-term growth and sustainable financial returns—but each option should be used to respond to unique short-term circumstances.
Acquisitions can provide immediate cash flow and existing customer and referral bases—key factors if the company
is in a highly competitive market and is trying to grow while minimizing risk. Acquisitions, however, are typically more expensive than new centers; therefore, they do not offer the same amount of benefit, in comparison.
This, however, might not be an issue if the partners are looking for relatively low (but stable) returns in a rather competitive or volatile market. Acquisitions can be a great way to gain a foothold in a new market while avoiding the challenge of marketing and developing a new center or brand. It can also be easier to gain financing for acquisitions, as existing centers have assets and cash flows against which lenders can make loans.
New centers are dramatically cheaper than acquisitions, but are much more risky, since there is no existing business (and referral trends are yet to be defined). New centers are, therefore, desired by partners looking for the highest possible returns—and willing to bear commensurate risks.
These risks can be mitigated based on whether existing referrers will support the new center, on whether the company is familiar with the existing market, and on the degree of competition that is currently in place for the new center. Starting from scratch, however, is always riskier than
an acquisition—and therefore, financing a new center will be more difficult.
With respect to the question of buying versus leasing, we think it’s hard to find a reason to buy real estate. Certainly, if the imaging center is a single tenant, and you can’t think of an instance in which you would ever move, buying a building can make financial sense. In nearly every opportunity we’ve examined, however, it has been much better to lease the building and use cash or other available debt to open or acquire new centers. The return on existing or new centers is much greater than the return on any real-estate investment that we’ve evaluated.
Financing has also been much easier to identify and secure for growth than it has been for acquisition of an existing building. This is even more likely to be the case with imaging equipment. Given how quickly imaging assets depreciate, using precious cash or financing on an imaging asset is likely to provide much lower returns than investing in expansion or growth in the marketplace could.
Present and FutureClearly, the financial meltdown and
subsequent recession have changed the game for any business that wishes to raise capital. We have found that the current economic environment has produced three primary effects in the health-care marketplace. First, imaging centers must have higher net margins and greater cash balances to qualify for debt financing.
Second, the ability to negotiate better terms depends on the operating history of the company—specifically, on its performance over the past 24 months—giving lenders a baseline for how the organization responds to a down market. Third, if you are working with an asset-based lender, the quality and number of assets can determine how quickly a transaction can take place (and the amounts of any loans that will be made available to the company).
There is no doubt that health-care reform and the escalating cost of health care have resulted in serious debate, within and between health systems, regarding how to position their imaging strategies. Likewise, there is no doubt that the Florida market is behaving very differently than that of
One of the perennial questions in our industry is whether to acquire existing centers or build new centers in order to ensure long-term growth. Our view is that both are necessary for long-term growth and sustainable financial
returns—but each option should be used to respond to unique short-term circumstances.
—Jason DingermissionPoint Health Partners

Revenue Cycle Management Coding
Credentialing
Experience Service Technology Information
The APS DifferenceAffiliated Professional Services, Inc.
2527 Cranberry Hwy.Wareham, MA 02571
866.914.8719www.affilprof.net
Free BillingProgram Consultation
Call Toll Free:866.914.8719
Practice Financial Challenges:
Control Spiraling Costs
Maximize Practice Revenue
Increase Practice Profitability
Since 1982, APS has helped practices across the country by offering billing program solutions.
A Medical Billing Alternative

HealtH SyStem | Outpatient Imaging Initiatives
48 RadIOlOgy BusIness JOuRnal | april/May 2011 | www.imagingbiz.com
North Dakota, so there is certainly not a single answer to any question concerning the years ahead. We believe, however, that certain truths do exist.
Hospital outpatient-department rates are unsustainable. These rates, we’re certain, will exist for different lengths of time, depending on the market forces in the local community. It is only a matter of time, however, before someone enters the market and competes directly with hospitals—at half the price. Payors might be unwilling, in the short term, to put pressure on their strongest hospitals, but
eventually, employers and others will begin narrowing networks to include only the lower-cost providers.
Patient access and prompt physician response are gaining strength in the market. We are seeing more and more hospital-loyal physicians send patients to independent imaging centers. At many (if not all) of these centers, patients can park easily, get their exams done quickly, and be out the door in 45 minutes. The same centers often read studies more quickly, provide more rapid report turnaround, and offer easy access to the image. In
these environments, hospitals with strong outpatient-department rates are suffering tremendously from volume declines, rather than pricing pressure—and payors are willing to make concessions on those rates because they are at decreasing risk of paying them.
Given these factors, centers with the lowest costs, highest patient satisfaction, and greatest integration with referring physicians will win in the market, over the long term. Lower costs will drive new volume to these centers, and the experience of patients and physicians will keep them there.
Tom Blankenship is vice president of business development for Saint Thomas Health Services (STHS), Nashville, Tennessee. Jason Dinger is CEO of MissionPoint Health Partners, the accountable-care organization of STHS. Sheila Sferrella, MAS, RT(R), CRA, FAHRA, is vice president of nonacute care operations for STHS.
Payors might be unwilling, in the short term, to put pressure on their strongest hospitals, but eventually, employers and others will begin narrowing networks to include only the lower-cost providers.
—Sheila Sferrella, maS, Rt(R), CRa, FaHRaSaint thomas Health Services
Saint Thomas Health Services (STHS), Nashville, Tennessee, announced on March 14, 2011, the formation of Saint Thomas Outpatient Imaging, a new joint venture between the five-hospital system and two of the area’s leading radiology groups, Premier Radiology (Nashville) and MidState Radiology (Murfreesboro). Once the transaction of $100 million is complete, Saint Thomas Outpatient Imaging will be the largest network of outpatient imaging centers in Middle Tennessee.
The newly formed imaging provider began offering services on April 1, giving patients access to more than 40 radiologists at eight locations in Nashville and in Cool Springs, Hermitage, Nolensville, Mt Juliet, Smyrna, and Murfreesboro. Several additional sites are under development. Saint Thomas Outpatient Imaging will also serve as the outpatient radiology provider for STHS stand-alone imaging centers, and it will be an integral part of an accountable-care organization. Volume for the venture is projected to exceed 250,000 imaging procedures in its initial year of operation.
Wesley O. Littrell, president and CEO of Saint Thomas Affiliates and chief strategy officer for STHS, considers the transaction
StHS launches Imaging Partnership
to be consistent with the STHS operating philosophy of collaboration and physician alignment. “STHS brings to the partnership a network of five hospitals and other affiliated providers throughout the region, as well as our own outpatient imaging centers,” he notes. “Partnering with Premier Radiology and MidState Radiology will result in greater access to lower-cost imaging services and a superior experience for our patients and the physicians we serve.”
Premier Radiology, a 30-member radiology group, brings six imaging centers in the Nashville area to the new joint venture. Premier Radiology provides inpatient radio-logy services at area hospitals in Nashville, at Williamson Medical Center in Franklin, at University Medical Center in Lebanon, and at STHS’ Hickman Community Hospital in Centerville. It also offers teleradiology services to more than 90 hospitals and other sites across the United States.
Chad Calendine, MD, president of Premier Radiology, says, “In STHS, we found a joint-venture partner that is as dedicated as we are to building processes and infrastructure that lower health-care costs for our community, and we believe this joint venture will change the face of imaging
in the region. We’ve invested our time and resources in building a model of excellent service delivery that focuses on the needs of our patients and physicians.”
Max Moss, MD, medical director and radiologist with MidState Radiology, corroborates Calendine’s comments. MidState Radiology is an 11-member group of physicians that is currently a joint-venture partner with STHS in the ownership of two outpatient imaging centers in Rutherford County; both facilities will become a part of the new venture. MidState Radiology is also the sole provider of radiology professional services at Middle Tennessee Medical Center in Murfreesboro, a hospital member of STHS. “MidState Radiology and our practices in Murfreesboro and Smyrna have proudly worked with STHS since 1971,” Moss says. “This partnership allows us to streamline our operations and extend our business beyond the communities we currently serve.”
—Julie Ritzer Ross
This article has been adapted from an imagingBiz Newswire entry that was posted on March 15, 2011, at www.imagingbiz.com/articles/newswire/st.-thomas-health-launches-imaging-partnership.

Scan here with a code reader on yoursmartphone to learn about our full arrayof products and professional services.
Or visit AllAboutPACS.com/rbj01
Visit Booth #301 during SIIM to find out how McKesson
can help you reach new levels of success. It’s about your success.
It’s about making healthcare better.
Everyone notices when you are successful. Care delivery gets better. Business operations get better. But how do you
achieve “better” in light of current challenges? Increasing patient care demands and resource utilization. Shrinking
budgets and ongoing changes in technology. Learn how to get better information, enjoy better workflow and deliver
better patient care with medical imaging solutions from McKesson. See why thousands of healthcare enterprises like
yours have put their trust in McKesson.
©2011 McKesson Corporation and/or one of its subsidiaries. All rights reserved.

By understanding the elements of medical-malpractice litigation and taking steps to mitigate risk, radiologists can reduce substantially their risk of being sued
Medical Malpractice | Risk Mitigation
Many factors have contributed to radiology’s increasingly important role in our health-care system and to the
specialty’s contributions to medicine. Demographics suggest that radiology will continue to be demanded by the physicians who will care for an aging and expanding population.
Likewise, new indications for existing technology have accelerated the utilization of diagnostic-imaging procedures in both elective and emergency situations. For example, physicians’ reliance on imaging to arrive at a prompt diagnosis can be seen in the unprecedented rise in the use of CT in US emergency departments—from 2.7 million exams in 1995 to more than 16 million in 2007, representing an average growth rate of 16% per year.1
Other factors contributing to increased utilization of imaging include patient expectations, the use of diagnostic-imaging procedures (including mammography) in screening programs, defensive medicine, the financially motivated ordering of unnecessary or noncontributory diagnostic tests, and the recommendation by radiologists of follow-up studies (of which the value is frequently questioned by referring physicians). In a 2008 report,2 America’s Health Insurance Plans estimated that 20% to 50% of diagnostic-imaging procedures fail to provide information that improves the patient’s diagnosis.
While much has been written about the financial burden of unnecessary imaging exams, less attention has been focused on the increasing exposure to the risk of litigation for radiologists. They can
be exposed either directly (for example, through failure to diagnose or incorrect diagnosis) or as defendants in cases that seem tangential to the performance and/or interpretation of radiological exams (in circumstances where counsel for the plaintiff sues all who were involved in the medical care delivered, even where their performance was not the proximate cause of the injury).
Medical MalpracticeMedical malpractice is professional
negligence, by act or omission, by a health-care provider, in which care provided deviates from accepted standards of practice in the medical community and causes injury or death to the patient, with many cases involving medical error. Standards and regulations for medical malpractice vary by country and by jurisdiction within countries.
The plaintiff must establish all four elements of the tort of negligence for a successful medical-malpractice claim: First, a duty was owed. A legal duty exists whenever a hospital or health-care provider undertakes care or treatment of a patient. Second, a duty was breached. The provider failed to conform to the relevant standard of care. The standard of care is proved by expert testimony or by obvious errors (the doctrine of res ipsa loquitur, or the thing speaks for itself).
Third, the breach caused an injury. The breach of duty was a proximate cause of the injury. Fourth, there are damages. Without damages (losses that might be pecuniary or emotional), there is no basis for a claim, regardless of whether the medical provider was negligent. Likewise, damages can occur without
50 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
By Howard Kessler, MD, and D. Scott Jones, CHC, LHRM
Medical Malpractice:Are You Covered?

www.imagingbiz.com | April/May 2011 | RAdiology Business JouRnAl 51
negligence—for example, when someone dies of a fatal disease.
Most settled malpractice claims (73%) involve medical error, according to a 2006 study.3 The authors discovered that claims without evidence of error are not uncommon, but most plaintiffs in such cases (72%) are denied compensation. The vast majority of expenditures (54%) go toward litigation over errors and payment for them. An examination of records of 1,452 closed malpractice claims revealed that an overwhelming majority (97%) were associated with injury; in those cases, 73% of plaintiffs received compensation. Just 3% of the claims were not associated with injuries; in those cases, 16% of plaintiffs received compensation.
Well over half of the claims (63%) were associated with errors; in those cases, 73% of plaintiffs received compensation (with an average payment of $521,560). The other 37% of claims were not associated with errors; in those cases, 28% of plaintiffs got compensation (with an average payment of $313,205). Claims not associated with errors accounted for 13% to 16% percent of the total costs. For every dollar spent on compensation, $0.54 went to administrative expenses (including lawyers, experts, and courts). Claims involving errors accounted for 78% of administrative costs.2,3
Separating Myth From RealityUntil recently, little information was
available regarding the direct and indirect costs assumed at the level of the practice or individual health-care practitioner—including loss of productivity for medical personnel, as defendants in litigation, related to communication and meetings with lawyers, trial preparation, and lost income—when cases go to trial.
The Physician Insurers Association of America (PIAA), Rockville, Maryland, is a leading insurers’ trade association that represents domestic and international medical professional liability insurance companies owned and/or operated by physicians, hospitals, dentists, and other health-care providers. PIAA domestic member companies include large national insurance companies, midsized regional writers, single-state insurers, and specialty companies that serve specific
niche markets in health-care provision. Collectively, these companies provide insurance protection to more than 60% of US private-practice physicians, and they write approximately 46% (or $5.2 billion) of the total annual industry premium.4
In a long-term analysis5 of radiology data from 1985 through 2008 provided by the PIAA, the most common condition for which claims were filed against radiologists was female breast cancer, resulting in an indemnity payment almost 39.2% of the time and representing 33.7% of the total paid for all radiology claims. The second most prevalent condition was cancer of the bronchus and lung, which resulted in a payment 36.3% of the time and accounted for 12.6% of total indemnity payments (Table 1).
In 2008 (the last year for which reportable data are complete), the average indemnity payment for radiology
($358,349) is comparable to the overall average indemnity of $345,498. These figures represent the portion of the radiology contribution to total judgments or settlements, many of which involve multiple defendants.
Radiology ranks sixth among the 28 specialties in the number of claims paid and monies paid for cases that closed between 1985 and 2008 (Table 2) and sixth in number of claims closed (Table 3). Radiology did not, however, rank in the top 10 specialties for average size of indemnity: It ranked 13th (Table 4).
The percentage of claims that result in payment has remained remarkably stable over time and is not much higher than the average across specialties: 31.2% of the radiology claims that closed in 2008 resulted in an indemnity payment, compared with 31.7% a decade ago and 28.4% for all physician specialty groups.5
Claims Percentage
Malignant neoplasm, breast 1,255 29%
Malignant neoplasm, bronchus and lung 678 15.7%
Neoplasm, breast, malignant/benign unknown 458 10.6%
Fracture, vertebral column 341 7.9%
Symptoms, abdomen/pelvis 326 7.5%
Injury, multiple body parts 300 6.9%
Screening, malignant neoplasms 286 6.6%
Radiological exam 249 5.8%
Fracture, foot 219 5.1%
Back disorders (including lumbago and sciatica) 217 5.0%
Table 1. Most Prevalent Conditions in Radiology Claims, 1985–2008
In a long-term analysis of radiology data from 1985 through 2008 provided by the PIAA, the most common condition for which claims were filed against radiologists was female breast cancer, resulting in an indemnity payment
almost 39.2% of the time and representing 33.7% of the total paid for all radiology claims.
—Howard Kessler, MDRadiology Solutions
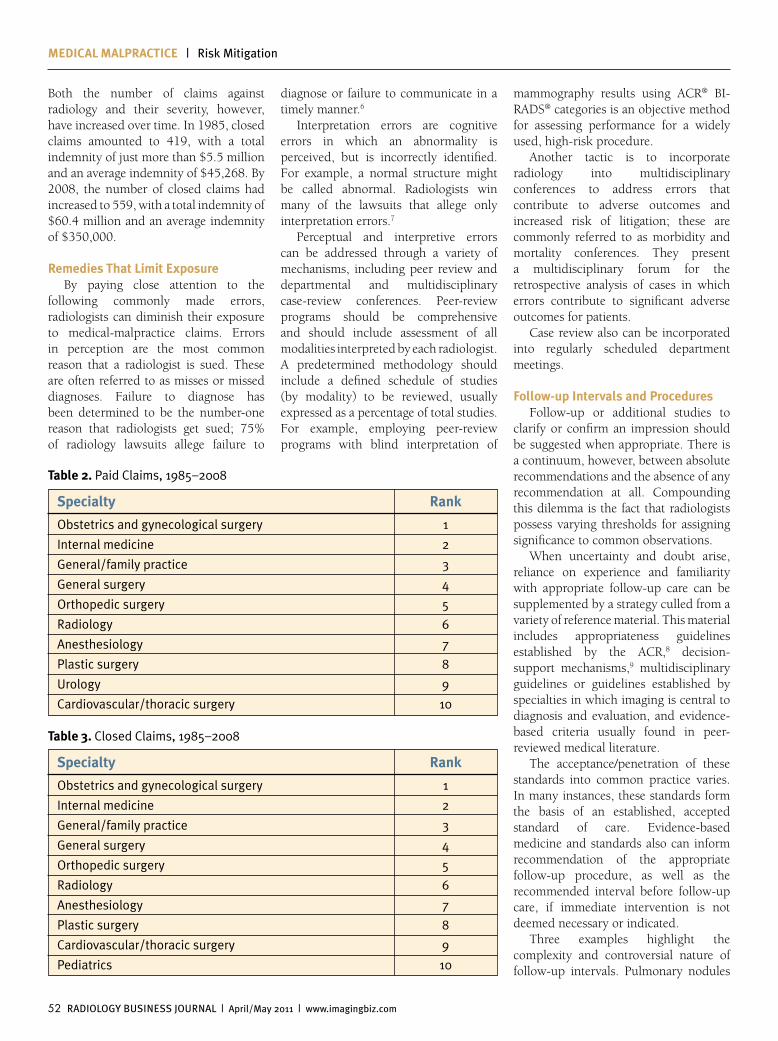
Medical Malpractice | Risk Mitigation
52 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
Both the number of claims against radiology and their severity, however, have increased over time. In 1985, closed claims amounted to 419, with a total indemnity of just more than $5.5 million and an average indemnity of $45,268. By 2008, the number of closed claims had increased to 559, with a total indemnity of $60.4 million and an average indemnity of $350,000.
remedies that limit exposureBy paying close attention to the
following commonly made errors, radiologists can diminish their exposure to medical-malpractice claims. Errors in perception are the most common reason that a radiologist is sued. These are often referred to as misses or missed diagnoses. Failure to diagnose has been determined to be the number-one reason that radiologists get sued; 75% of radiology lawsuits allege failure to
diagnose or failure to communicate in a timely manner.6
Interpretation errors are cognitive errors in which an abnormality is perceived, but is incorrectly identified. For example, a normal structure might be called abnormal. Radiologists win many of the lawsuits that allege only interpretation errors.7
Perceptual and interpretive errors can be addressed through a variety of mechanisms, including peer review and departmental and multidisciplinary case-review conferences. Peer-review programs should be comprehensive and should include assessment of all modalities interpreted by each radiologist. A predetermined methodology should include a defined schedule of studies (by modality) to be reviewed, usually expressed as a percentage of total studies. For example, employing peer-review programs with blind interpretation of
mammography results using ACR® BI-RADS® categories is an objective method for assessing performance for a widely used, high-risk procedure.
Another tactic is to incorporate radiology into multidisciplinary conferences to address errors that contribute to adverse outcomes and increased risk of litigation; these are commonly referred to as morbidity and mortality conferences. They present a multidisciplinary forum for the retrospective analysis of cases in which errors contribute to significant adverse outcomes for patients.
Case review also can be incorporated into regularly scheduled department meetings.
Follow-up intervals and proceduresFollow-up or additional studies to
clarify or confirm an impression should be suggested when appropriate. There is a continuum, however, between absolute recommendations and the absence of any recommendation at all. Compounding this dilemma is the fact that radiologists possess varying thresholds for assigning significance to common observations.
When uncertainty and doubt arise, reliance on experience and familiarity with appropriate follow-up care can be supplemented by a strategy culled from a variety of reference material. This material includes appropriateness guidelines established by the ACR,8 decision-support mechanisms,9 multidisciplinary guidelines or guidelines established by specialties in which imaging is central to diagnosis and evaluation, and evidence-based criteria usually found in peer-reviewed medical literature.
The acceptance/penetration of these standards into common practice varies. In many instances, these standards form the basis of an established, accepted standard of care. Evidence-based medicine and standards also can inform recommendation of the appropriate follow-up procedure, as well as the recommended interval before follow-up care, if immediate intervention is not deemed necessary or indicated.
Three examples highlight the complexity and controversial nature of follow-up intervals. Pulmonary nodules
Specialty rank
Obstetrics and gynecological surgery 1
Internal medicine 2
General/family practice 3
General surgery 4
Orthopedic surgery 5
Radiology 6
Anesthesiology 7
Plastic surgery 8
Urology 9
Cardiovascular/thoracic surgery 10
table 2. Paid Claims, 1985–2008
Specialty rank
Obstetrics and gynecological surgery 1
Internal medicine 2
General/family practice 3
General surgery 4
Orthopedic surgery 5
Radiology 6
Anesthesiology 7
Plastic surgery 8
Cardiovascular/thoracic surgery 9
Pediatrics 10
table 3. Closed Claims, 1985–2008
RBJ_World-RFA_Full-page-ad.indd 1 4/6/11 3:01 PM
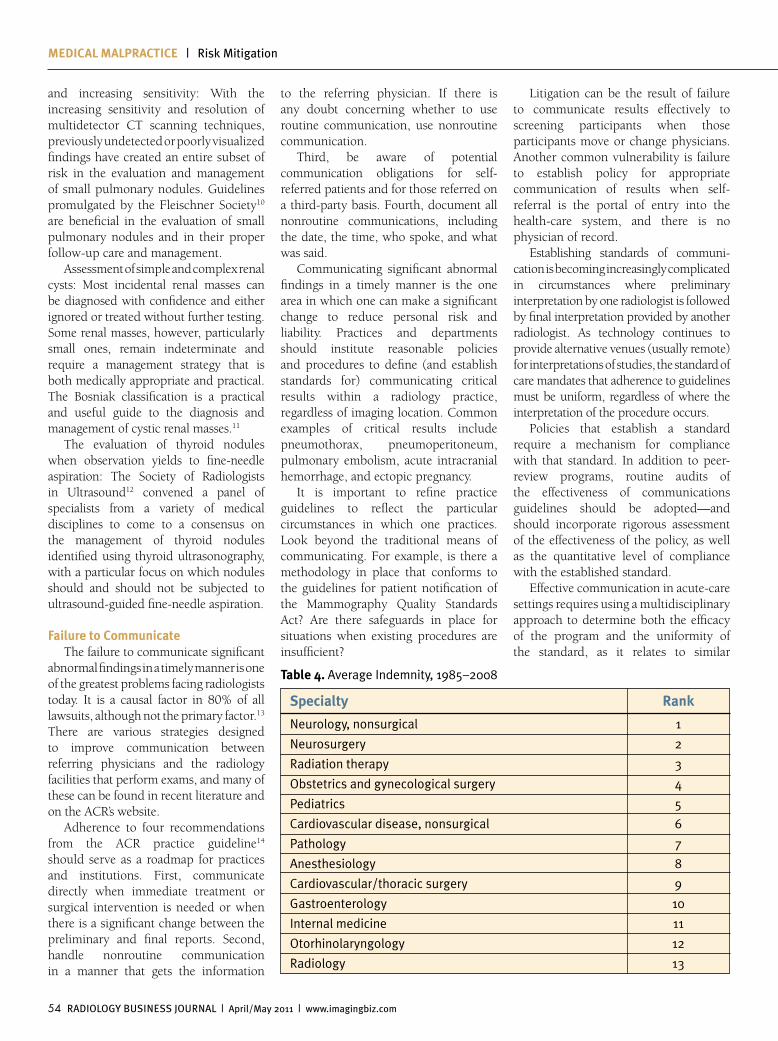
Medical Malpractice | Risk Mitigation
54 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
and increasing sensitivity: With the increasing sensitivity and resolution of multidetector CT scanning techniques, previously undetected or poorly visualized findings have created an entire subset of risk in the evaluation and management of small pulmonary nodules. Guidelines promulgated by the Fleischner Society10 are beneficial in the evaluation of small pulmonary nodules and in their proper follow-up care and management.
Assessment of simple and complex renal cysts: Most incidental renal masses can be diagnosed with confidence and either ignored or treated without further testing. Some renal masses, however, particularly small ones, remain indeterminate and require a management strategy that is both medically appropriate and practical. The Bosniak classification is a practical and useful guide to the diagnosis and management of cystic renal masses.11
The evaluation of thyroid nodules when observation yields to fine-needle aspiration: The Society of Radiologists in Ultrasound12 convened a panel of specialists from a variety of medical disciplines to come to a consensus on the management of thyroid nodules identified using thyroid ultrasonography, with a particular focus on which nodules should and should not be subjected to ultrasound-guided fine-needle aspiration.
Failure to communicateThe failure to communicate significant
abnormal findings in a timely manner is one of the greatest problems facing radiologists today. It is a causal factor in 80% of all lawsuits, although not the primary factor.13 There are various strategies designed to improve communication between referring physicians and the radiology facilities that perform exams, and many of these can be found in recent literature and on the ACR’s website.
Adherence to four recommendations from the ACR practice guideline14 should serve as a roadmap for practices and institutions. First, communicate directly when immediate treatment or surgical intervention is needed or when there is a significant change between the preliminary and final reports. Second, handle nonroutine communication in a manner that gets the information
to the referring physician. If there is any doubt concerning whether to use routine communication, use nonroutine communication.
Third, be aware of potential communication obligations for self-referred patients and for those referred on a third-party basis. Fourth, document all nonroutine communications, including the date, the time, who spoke, and what was said.
Communicating significant abnormal findings in a timely manner is the one area in which one can make a significant change to reduce personal risk and liability. Practices and departments should institute reasonable policies and procedures to define (and establish standards for) communicating critical results within a radiology practice, regardless of imaging location. Common examples of critical results include pneumothorax, pneumoperitoneum, pulmonary embolism, acute intracranial hemorrhage, and ectopic pregnancy.
It is important to refine practice guidelines to reflect the particular circumstances in which one practices. Look beyond the traditional means of communicating. For example, is there a methodology in place that conforms to the guidelines for patient notification of the Mammography Quality Standards Act? Are there safeguards in place for situations when existing procedures are insufficient?
Litigation can be the result of failure to communicate results effectively to screening participants when those participants move or change physicians. Another common vulnerability is failure to establish policy for appropriate communication of results when self-referral is the portal of entry into the health-care system, and there is no physician of record.
Establishing standards of communi-cation is becoming increasingly complicated in circumstances where preliminary interpretation by one radiologist is followed by final interpretation provided by another radiologist. As technology continues to provide alternative venues (usually remote) for interpretations of studies, the standard of care mandates that adherence to guidelines must be uniform, regardless of where the interpretation of the procedure occurs.
Policies that establish a standard require a mechanism for compliance with that standard. In addition to peer-review programs, routine audits of the effectiveness of communications guidelines should be adopted—and should incorporate rigorous assessment of the effectiveness of the policy, as well as the quantitative level of compliance with the established standard.
Effective communication in acute-care settings requires using a multidisciplinary approach to determine both the efficacy of the program and the uniformity of the standard, as it relates to similar
Specialty rank
Neurology, nonsurgical 1
Neurosurgery 2
Radiation therapy 3
Obstetrics and gynecological surgery 4
Pediatrics 5
Cardiovascular disease, nonsurgical 6
Pathology 7
Anesthesiology 8
Cardiovascular/thoracic surgery 9
Gastroenterology 10
Internal medicine 11
Otorhinolaryngology 12
Radiology 13
table 4. Average Indemnity, 1985–2008

www.imagingbiz.com | April/May 2011 | RAdiology Business JouRnAl 55
policies across the entire medical milieu. Coordination with risk management is also key in ensuring that standards and policies are applicable beyond the scope of the institution and are compliant with new or established guidelines promulgated by state and federal regulatory agencies.
Be PreparedRadiologists will continue to be
defendants in both meritorious and frivolous malpractice suits. Society is becoming more litigious, resulting in an increase in the frequency of medical-malpractice lawsuits. Understanding the basis for medical malpractice in radiology is a good place to start. Enterprise-wide commitment to risk management is the most effective and efficient mechanism for the development of successful strategies to improve risk and deliver high-quality care
While many cling to the holy grail of tort reform with limits on awards, this approach is not likely to be realized at the national level, nor is there a mandate for comprehensive tort reform at the state level. While there are examples where legislation at the state level mitigates the magnitude of damages, these examples fail to address why radiology is fertile ground for medical-malpractice claims.
Understanding why radiologists are sued is vital in planning an effective risk-management program. Knowledge about the most likely areas where litigation occurs can direct efforts, at a practice or institutional level, to apply risk-management techniques. Comprehensive assessment of policies and procedures is a good starting point for addressing matters such as communication of results. Addressing the other areas where
risk can be improved is less concrete and is more related to individual performance in interpretation and in making follow-up recommendations.
Nonetheless, there is great potential in pursuing a methodical approach to lowering risk and improving the quality of care provided. This requires integration of many disciplines within the radiology milieu. In the past, little attention was focused on the educational value that the lawyers who defend these cases and the companies that provide medical-malpractice insurance can offer.
Integrating this information with that provided through risk-management resources will be limited by the willingness of the targets of malpractice suits to embrace the notion that managing risk benefits everyone in the health-care system. Radiologists can lower their risk primarily through communication, education, and constructive feedback from others involved in the delivery of health care.
Howard B. Kessler, MD, is medical director, Radiology Solutions, New Jersey and Pennsylvania divisions, Philadelphia, Pennsylvania. D. Scott Jones, CHC, LHRM, is vice president, corporate compliance and risk management, Healthcare Providers Insurance Exchange and American Healthcare Providers Insurance Services, Philadelphia.
References1. Larson DB, Johnson LW, Schnell BM, Salisbury SR, Foreman HP. National trends in CT use in the emergency department: 1995–2007. Radiology. 2011;258(1):164-173.2. America’s Health Insurance Plans.
Ensuring quality through appropriate use of diagnostic imaging. http://www.ahip.org/content/default.aspx?docid=24057. Published July 2008. Accessed April 2, 2011.3. Studdert DM, Mello MM, Gawande AA, et al. Claims, errors, and compensation payments in medical malpractice litigation. N Engl J Med. 2006;354:2024-2033.4. Bloom JB. Medical malpractice study: disproving frivolous myth. National Law Journal. July 3, 2006:12-15. 5. Risk Management Review: Radiology. Rockville, MD: Physician Insurers Association of America; 2009.6. Berlin L, Berlin JW. Malpractice and radiologists in Cook County, IL: trends in 20 years of litigation. AJR Am J Roentgenol. 1995;165(4):781-788.7. Raskin MM. Why radiologists get sued. Applied Radiology. 2001;30(8):19-21.8. ACR appropriateness criteria. h t t p : / / w w w. a c r . o r g / s e c o n d a r y mainmenucategories/quality_safety/app_criteria.aspx. Accessed April 2, 2011.9. Sistrom CL, Dang PA, Weilburg JB, Dreyer KJ, Rosenthal DI, Thrall JH. Effect of computerized order entry with integrated decision support on the growth of outpatient procedure volumes: seven-year time series analysis. Radiology. 2009;25(1):147-155.10. MacMahon H, Austin JH, Gamsu G, et al. Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the Fleischner Society. Radiology. 2005;237(2):395-400.11. Silverman AG, Israel GM, Herts BR, Richie JP. Management of the incidental renal mass. Radiology. 2008;249(1):16-31.12. Frates MC, Benson CB, Charboneau JW, et al. Management of thyroid nodules detected at US: Society of Radiologists in Ultrasound consensus conference state-ment. Radiology. 2005;237(5):794-800.13. Berlin L. Communication of the significant but not urgent finding. AJR Am J Roentgenol. 1997;168(2):329-331.14. ACR practice guideline for communication of diagnostic imaging findings. http://www.acr.org/SecondaryMainMenuCategories/quality_safety/guidelines/dx/comm_diag_rad.aspx. Published 2010. Accessed April 2, 2011.
Understanding why radiologists are sued is vital in planning an effective risk-management strategy. Knowledge about the most likely areas where litigation occurs can direct efforts, at a practice or institutional level, to apply risk- management techniques.
—D. Scott Jones, CHC, LHRMHealthcare Providers Insurance Exchange

As the price of storage declines and as hospitals and practices groan under the weight of responsibility for image storage and management, radiology is beginning to embrace the cloud
EfficiEncy | Cloud Solutions
Health-care providers today have a heightened interest in streamlining operations and reducing capital outlays
to maintain or improve margins. In an increasing number of cases, cloud-based solutions and software as a service are being embraced by the radiology sector to meet these challenges—but not before a careful analysis that goes beyond cost considerations has been performed.
For some radiology players, a move to leverage the cloud stems from a desire to manage an increasing volume of imaging data more effectively, while simultaneously grappling with tight capital and operating budgets. Orlando Health in Florida—a 1,780-bed, not-for-profit private health network with 14,000 employees, multiple inpatient and outpatient facilities located across Central Florida, and 2,000 affiliated physicians—ranks among them.
Approximately two years ago, Orlando Health’s IT department acknowledged that shared cloud storage might, based on perceived total cost of ownership
(TCO), constitute a more viable means of addressing multiple data-storage challenges than a traditional product would. Brian Comp, MBA, PMP, is Orlando Health’s chief technology officer, information services. In calculating TCO, Comp and his team took into consideration not only the anticipated initial capital outlay, but maintenance costs and the very real possibility of the need to upgrade Orlando Health’s data-storage technology down the road.
The health network currently maintains two self-hosted data centers in Orlando that handle more than 200 terabytes of data. About 25% of total data storage is needed for PACS and for a separate cardiology PACS. Comp says, “Besides these demands, our data rate had been growing by 50% annually and continues to do so. Storage growth allocations in the IT capital budget range from approximately $1 million to $1.5 million per year—a tight squeeze—and changes in reimbursement mean that capital is harder to find.”
Comp and his team also looked at potential power savings in weighing
56 Radiology BuSineSS JouRnal | april/May 2011 | www.imagingbiz.com
By Julie Ritzer Ross
Leveraging the Cloud in Radiology

TakeYour Image Distribution to the Cloud
INTRODUCING ROENTGENWORKS ASP
View studies using:- BRIT’s WebWorks browser-based viewer- BRIT’s DoctorWorks iPad app
Locate and retrieve patient studies cross-enterprise
HIPAA access tracking by patient and/or user
For just pennies per study more, add additional services- Vendor Neutral Archive - Scheduling- Critical Results Reporting - Web-enabled PACS and RIS
Contact BRIT to learn how you can get started today!800-230-7227 • [email protected] • www.brit.com
Visit BRIT Systems at SIIM booth 608
Starting at $.50 per study.Zero Risk.
Zero Upfront Costs.Zero Maintenance.
BRIT takes a modular approach to image and radiology management – so you only payfor what you need. Add capacity and services as you grow.
iPad LOCAL APPLICATION
At a PriceYour CFOWill Love!
RoentgenWork_ASP_SIIM_Final:Layout 1 4/23/11 12:11 PM Page 1

EfficiEncy | Cloud Solutions
58 Radiology BuSineSS JouRnal | april/May 2011 | www.imagingbiz.com
whether Orlando Health would be better served by a cloud-storage solution or by an installed hardware/software configuration. He deems power and cooling for the data center significant issues in Florida, noting that these expenditures are likely to be three or four times higher than those incurred by providers in many other locations. “We figured that by reclaiming electricity that would otherwise be needed to power the systems and cool the equipment, we could do 25% better than now,” Comp reports. “That was a strong justification.”
The department, however, wasn’t willing to base its decision entirely on economics; other concerns came into play. Orlando Health wanted reasonable assurance that only authorized parties would have access to data stored in the cloud, that cloud-storage performance levels would rival those provided by its own data centers, and that the vendor would, as Comp put it, be around for the long haul.
“We are still in the midst of figuring out the best cloud-storage model for
us and discussing these issues with potential vendor partners, but the analysis definitely pushed us in that direction,” Comp states. “In our long-range plan for the next five to 10 years, our first step is to move our long-term storage to the data center of the cloud provider. We reduce the requirement for capital investment, we should be able to reclaim some electric power, our data-center floor space will be freed, we are hoping that our technical-support needs will be at least somewhat reduced, and we will be able to maintain our failover capability. If we have a loss at a primary data center, we want to be able to continue to provide service to our clinicians.”
He notes that Orlando Health’s planned transition to the cloud probably would not be possible if less-expensive, higher-bandwidth cloud-based solutions had not been introduced in recent years. “The original higher-bandwidth options were cost prohibitive—and thus, out of our reach,” he explains. “No analysis would have supported adopting them.”
Access insuranceAlta Vista Radiology (Phoenix, Arizona)
also saw the cloud as a panacea for its image-management and -storage ills. The provider offers teleradiology services to 80 hospitals in the Southwestern, Southeastern, and Midwestern regions of the United States, as well as along the East Coast. Alta Vista uses a PACS vendor’s software as a service to access a hosted version of the vendor’s PACS. The service is available on a pay-per-click basis.
Robert Ortega, MD, is Alta Vista Radiology’s CEO; he and his team looked at a number of factors in conducting cost justification for a hosted PACS (rather than a traditional PACS). A TCO analysis took into consideration the initial financial outlay for equipping a data center, as well as the costs of ongoing management, technical support, and anticipated upgrades. Because Alta Vista Radiology has two administrative employees whose responsibilities touch IT, but has no dedicated IT staff, the potential cost of hiring someone to manage the data center and the PACS, along with the costs of finding and training a replacement for that individual (should he or she leave the organization), were factored into the equation.
Ortega says, however, that the degree to which a hosted PACS would suit the provider’s business model and structure was a far more important criterion when contemplating a jump onto the cloud bandwagon. He notes, “Our model didn’t—and never will—include having a staff of network engineers, but our service promise necessitates near-perfect uptime. Our geographically diverse structure necessitated a data-center–based approach so that we are ready to read, no matter where hospitals are located, but we didn’t want to take the risk of having our own. Given the tight fit, we would have gone with the hosted PACS and the
We reduce the need for capital investment, we should be able to reclaim some electric power, our data-center floor space will be freed, and we will be able to maintain our failover capability. If we have a loss
at our primary data center, we want to be able to continue to provide service to our clinicians.
—Brian comp, MBA, PMP Orlando Health
Our geographically diverse structure necessitated a data-center–based approach so that we are ready to read, no matter where hospitals are located, but we didn’t want to take the risk of having our own. Given the tight fit,
we would have gone with the hosted PACS and the cloud even if that option cost us more than the do-it-yourself approach.
—Robert Ortega, MD Alta Vista Radiology

HPS uses GE Centricity® PACS-IW - ranked #1 PACS in 2008 and 2009 by Klas Research.
cloud even if that option cost us more than the do-it-yourself approach.”
While there was no concern about potentially extricating Alta Vista Radiology from its relationship with the vendor, based on the latter’s longevity in the market, other considerations were addressed in advance of signing on the dotted line. Ortega questioned how flexible the vendor would be, in terms of setting and enforcing minimum-usage volume requirements.
A guarantee from Alta Vista Radiology of a future uptick in usage volume enabled it to obtain the desired wiggle room at the beginning of the contract. Concerns about uninterrupted access to the hosted PACS were addressed by writing a guarantee of 99.99% uptime into the contract. The presence of a secure VPN connection between facilities and the data center appeased any worries about data compromise.
Like Comp, Ortega believes that
enhancements in Internet capabilities are pushing the cloud envelope, both within and beyond the radiology realm. He says, “Fiber-optic connectivity has done great things for uptime.” That, in turn, has bolstered the appeal of the cloud.
Share and Share AlikeOther health-care providers see the
cloud as the solution for image sharing. They include Baystate Health (Springfield, Massachusetts), which operates four
hospitals in the state—the 659-bed Baystate Medical Center in Springfield, Baystate Children’s Hospital within Baystate Medical Center, Baystate Mary Lane Hospital in Ware, and the Baystate Franklin Medical Center in Greenfield.
In addition, the system operates Baystate Radiology and Imaging and a number of other services and health centers. Baystate Medical Center is Western New England’s only level I trauma center and tertiary-care center.
We were looking for a better way to manage inbound CDs. Although they may have been DICOM compatible, they couldn’t always be read if we put them into a computer, leading to delays in patient care.
—Michael favreauBaystate Health

Hello, My Name is
Upcoming Deadline
Still need to meet the CMS imaging mandate?Start and end here.
Regardless of number of sites or modalities, you need only one
application, one survey, and pay one cost.
Meet the January 1, 2012 deadline with The Joint Commission.
Visit: www.jointcommission.org/onlyone
Get FREE trial of the standards!
AHC CMS AD 3-8_Layout 1 3/9/11 2:37 PM Page 1
EfficiEncy | Cloud Solutions
Its emergency department is the second-busiest such facility in Western Massachusetts, according to Michael Favreau, director of imaging and special projects.
In January 2010, after inking a deal with a startup image-sharing company, Baystate Health took a first step by installing the company’s product on its private network; this includes disc viewers, in addition to in-boxes that allow authorized users to hold data files obtained from patients’ CDs, as well as the tools needed to view, store, and share these files. Along with medical images,
the files can include physicians’ notes and reports.
Favreau explains, “We were looking for a better way to manage inbound CDs. Although they may have been DICOM compatible, they couldn’t always be read if we put them into a computer, leading to delays in patient care (and often, the need to expose patients to repeat studies).”
The solution helped immensely, making it possible to view 95% of the CDs that accompanied patients to Baystate Medical Center. It wasn’t enough, though: Baystate Health wanted to facilitate the sharing of images with community
physicians and hospitals outside its network. Favreau and his colleagues quickly concluded that implementing any solution other than one centered on the cloud would not make sense, from a logistical standpoint.
The health system had neither the staff resources nor the capital to build or buy (and manage) its own image-sharing application—especially one to which round-the-clock access was a must. Decision makers, however, determined that the hospital network’s IT budget and department could absorb the cost of a subscription-based image-sharing solution that was—by virtue of requiring minimal intervention by IT personnel and having minor equipment requirements—well within financial reach.
Accordingly, over the past few months, Baystate Health has moved image sharing to the vendor’s cloud, enabling referring hospitals to send imaging exams, reports, and associated documents to specialized departments at Baystate Medical Center through a secure online conduit. The data arrive in online drop boxes accessible only to authorized users who enter a password. Drop boxes, to which two hospitals can currently upload data, have recently been established for trauma and vascular services. Ultimately, the platform will serve as a conduit among five hospitals and for six to eight service lines, Favreau reports. “It’s still evolving,” he says.
Favreau emphasizes that a decision to handle image sharing via cloud should involve more than logistical and financial considerations and analyses. Open lines of communication must be established with any entity that will be sharing images with a given provider, and security concerns must be addressed with the solution vendor.
When the idea of migrating to the cloud first appeared on Baystate Health’s agenda, Favreau and his colleagues approached the potentially connected hospitals to discuss the project and explain how online image exchange would expedite and enhance patient care. The IT department requested (and received) from the image-sharing vendor a detailed description of security standards and protocols.
Every so often a solution comes along that absolutely revolutionizes an industry. PowerScribe 360 is that solution. For the first time ever in radiology, one single platform combines the industry’s best speech recognition technology, critical test result management, data capture, multi-site workflow, structured reporting and more to provide you with unprecedented speed, accuracy and control.
While the name might be familiar, the performance of this powerful new reporting solution is unlike anything you’ve ever seen before. For more than 10 years, our valued customers have shared their ideas for the perfect reporting platform. We listened, and the result is an unparalleled leap forward in speech recognition reporting. One that will help you create and turn around diagnostic imaging interpretations faster and with more control than you ever imagined possible.
© 2010 Nuance Communications, Inc. All rights reserved. Nuance, the Nuance logo and PowerScribe are trademarks or registered trademarks of Nuance Communications, Inc. or its affiliates in the United States and/or other countries.
Call us today at 1-800-350-4836, Ext. D792, or visit www.PowerScribe360.com to learn just how dramatically this next generation platform is going to improve your radiology workflow.

EfficiEncy | Cloud Solutions
62 Radiology BuSineSS JouRnal | april/May 2011 | www.imagingbiz.com
Tighter security around the Internet has made it a far more appealing platform for data sharing of any kind, Favreau concedes, emphasizing that the financial aspects are not all important. “Security, however, has to be scrutinized up front and is not worth sacrificing,” he adds.
Expanding ReachRadiologic Associates of Fredericksburg
(RAF) in Virginia has turned to the cloud in an effort to support an expansion of its services reach. The provider has a staff of 32 radiologists and two vascular surgeons; data pertaining to patients served at two hospitals, four outpatient imaging centers, and an interventional-radiology clinic reside in a conventional hospital-owned PACS—managed by a hospital-based IT department and backed up by an on-site database.
At one time, RAF provided the bulk of its interpretation services to MediCorp Health System (Fredericksburg), now known as Mary Washington Healthcare, which owns the hospitals to which RAF provides service in Fredericksburg and surrounding cities. Not long ago, however, it contracted to provide radiology services to an entity outside the hospital network. Neil Green, MD, director of nuclear medicine, says, “Because we were dealing with a group od urgent-care facilities not affiliated with Mary Washington Healthcare, we could not incorporate patient images and data into our hospital’s PACS and RIS. We asked ourselves how we could interpret the images easily.”
The practice looked at the cost of adding dedicated workstations and a full-blown RIS; in addition to the hardware
expenditure, this would have required maintaining a separate database on-site, with expensive server hardware (and no dedicated IT staff to support it), Green notes. Also factored in was the cost of system upgrades, which would probably become necessary as other nonaffiliated entities sought RAF’s services.
The TCO did not compare favorably with that of a hosted, turnkey, browser-based PACS, leading RAF to implement a Web-based image-management solution that allows on-site and off-site image availability. Along with the PACS capability, Green says, the solution offers the functionality of a RIS by enabling referring physicians to perform order entry.
A number of preimplementation meetings were held to iron out what Green calls “critical issues and concerns, when you’re talking about the cloud.” For example, the vendor was asked to provide training on the system for RAF’s staff, along with assurance that the solution would be sufficiently scalable to accommodate data-volume growth. An exit strategy—in case RAF ever wants to migrate images out of a separate system—was also developed, as were set triage procedures (in the event of system difficulties).
“The cloud is not an answer for everyone,” Green says. Nonetheless, he adds, if the price of training, maintenance, upgrades, troubleshooting, and related factors is compared with the cost of a turnkey solution, it becomes clear that the cloud is an excellent alternative.
Julie Ritzer Ross is a contributing writer for Radiology Business Journal.
Because we were dealing with a group of urgent-care facilities not affiliated with Mary Washington Healthcare, we could not incorporate patient images and data into our hospital’s PACS and RIS. We asked ourselves how we could
interpret the images easily.—neil Green, MD
Radiologic Associates of fredericksburg

Looking for a new riS/PaCS forraDioLogY or BreaST iMaging?
CHooSe THe MoST eXPerienCeD.
Sectra’s web-based RIS/PACS and Breast Imaging PACS core technology has been refined over the last 20 years. We’ve had plenty of time to add and custo-mize features and functionality as needs have changed.You can be sure our solution is ready to meet your demands – not just today, but far beyond tomorrow.
Perhaps that’s why some of the world’s largest healthcareproviders rely on our solutions. University Hospitals of Cleveland, several major hospitals in New York, Northern
Ireland and Greater London to name a few (out of more than 1,100). For them, workflow and system stability are top of mind. They don’t want delays, integration hassles or legacy migration problems.
And, we’re guessing, neither do you.So, if you’re looking for a partner to give your depart-
ment an efficiency booster, choose one that’s seen and done it all before. Many times. The journey to productivitywithout limits starts at sectra.com/medical.
VISIT US AT SIIM
BOOTH 824

Governance | The Practice
As a manifestation of their core DNA, physicians dislike being led. As a corollary, physicians dislike, to a greater or lesser
extent, their leader, particularly those leaders actually empowered to lead. To circumvent the leader problem, physicians tend to select a democratic form of governance for their practice, thus diluting the position of the leader.
The process of consensus building is the functional crux of the democratic governance model. It permits the partners to maintain an appearance of equality while, at the same time, allowing decisions to be made with only minimal direction by the leader.
Developing a consensus opinion is essentially a mathematical exercise: Members alter the proposal until the math works. The achievement of majority support for the proposal necessarily becomes the primary goal of the argument when, in reality, the primary goal should be the development of an opinion that improves the competitive stance of the group in its marketplace.
The very nature of the math of consensus development ensures that the content of the proposal is diluted until it is acceptable to a majority of voters. While proponents are looking
for enough residual content to make the desired change, opponents seek enough dilution to limit any undesirable effect. The proposition is watered down to a level that is acceptable to the majority of voters, and in the end, the corporate value of the proposal is lost.
Consider this hypothetical partnership meeting. Physician A (CEO and senior partner) says, “The clinicians in our office building want us to open our office on Saturday, from 9 am to 2 pm. Most of the physicians’ offices are open until 1 pm, but they are usually running late, so they want us there until 2 pm.”
Physician B replies, “It will cost us a fortune: $400 in technologists’ salaries, plus additional nontechnologist expenses. We will lose all kinds of money. Besides, many of these physicians send their patients to our competitor down the street during the week. I vote no.”
Physician C (who has a Saturday-morning golf game in the summer and who skis on Saturdays in the winter) adds, “I vote no, too.” Physician D (who is busy on Saturday mornings with family and church activities) says, “I vote no.”
Physician A says, “Rather than turning the physicians down completely, let’s work out something. We need a compromise.” After much haggling and complaining,
a compromise is reached in which the group will provide limited services (radiography and mammography) from 10 am to noon. The vote is carried with five in favor and four opposed.
Physician A informs the clinicians of the group’s decision. The physicians are furious; making mammography and radiography available until noon is insufficient. In the end, the extended hours fail. After six weekends of losing money every weekend and squandering the radiologists’ weekend time, they are stopped. How could a consensus decision—the product of such an elegant, human political process—produce such a bad outcome?
Mathematics to nowhereConsensus building is simply a cold,
objective mathematical process. Of itself, it has no capacity to ensure the propriety or validity of any decision. Even worse, our infatuation with the perceived wisdom conferred by consensus building allows us to select inappropriate conclusions, as we smugly envelop those conclusions with the crowd’s aggregated wisdom.
If the math is not damaging enough, two intrinsic weaknesses of the radiology partners are what ultimately sink the whole Saturday-hours endeavor. First,
64 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
By David F. Hayes, MD
In these turbulent times, radiology practices cannot afford to indulge in the groupthink, wisdom of the crowd, and information cascade that are the byproducts of democratic governance
Corporate Practice Management in the 21st Century:Why Democratic Governance No Longer Works

incomplete knowledge of the background issues is a devastating malady. The CEO is uncertain of the politics. Many of the other partners might have no understanding of the political implications of withholding needed clinical services from the referring physicians. If the knowledge is incomplete, it is very easy to get off track during the discussion phase, diluting the analysis with unsubstantiated opinion.
Second, the partners’ personal biases will readily fill any void created by incomplete knowledge. The discussion becomes all about the other issues: the Saturday golf outing, social and family issues, or any other competing pet project. The importance of Saturday office hours is lost, and the analysis is doomed.
It is readily apparent that consensus building is not a strong, useful management process in the competitive business marketplace. The math (and the inherent personal biases of the group) will inevitably compromise the group’s best deliberative efforts. When the group chooses to manage its affairs by consensus building, it must understand that while democratic consensus is a charming and elegant concept, it does not perform well in a competitive business marketplace.
The basic mathematical challenge of the process and the characteristics of
the individual partners are compelling weaknesses in the consensus model. There are, however, several additional elegant, subtle weaknesses in the consensus process. These characteristics, since they reflect more generalized human malfunctions, are difficult to recognize and control. They are characteristic of the human species at large, and are not limited to any individual radiology group or, for that matter, to the specific circumstance of weekend coverage. They are factors in virtually every partnership meeting (in every venue).
Wisdom of The crowdEver since the heyday of the ancient
Greek city-states, humans have been attracted to the democratic governance format, with its attendant consensus management. The elegance and appeal of democracy, however, do not—in any fashion—imply that consensus is an effective and functional management process. Specifically, can the democratic model identify and select the best answer to a difficult question even when there is no single popular option and when all choices will be distasteful to a significant segment of the partnership?
The wisdom of the crowd affirmatively declares that it can make that choice. Just
imagine that all the partners are bright, experienced individuals. When they convene as a partnership, they bring together not only all their knowledge and experience, but their wisdom as well. Magically, when they are gathered as a group, their wisdom is aggregated into a superwisdom of the crowd. It seems that when the group gathers for a meeting, two heads are better than one—and multiple heads are even better than two.
It is this attribute—the wisdom of the crowd—that allows the partnership to select the democratic process as its governance model. Without the hope of assumed wisdom, the group would hesitate to choose consensus management. Intrinsically, the democratic model has no specific capacity to resolve complex issues, and no one seriously makes that assertion.
In reality, the wisdom of the crowd rarely achieves fruition. Rather, the wisdom is diluted by imitative behavior, human emotions (peer pressure and the herd instinct), incomplete knowledge, personal bias, private agendas, and excessive homogeneity of the crowd. When so altered, the wisdom of the crowd becomes groupthink.
Groupthink and Information cascadeIrving Janis (1918–1990), a
psychologist who studied disasters in US foreign policy (such as failure to anticipate Pearl Harbor), identified groupthink as a mode of thinking that people engage in when the group’s pursuit of consensus overrides its interest in appropriate resolution of the question.
Compared with wisdom, groupthink is frightening indeed. More frightening is the subtle and slippery slope leading from wisdom to groupthink. Those involved in the process (for example, attending a partnership meeting) might feel only their collective wisdom and fail to perceive the looming groupthink. Conditions leading to groupthink are homogeneity of members’ social backgrounds and ideologies, along with isolation of the group from outside sources of information analysis.
Symptoms of groupthink include illusions of invulnerability (producing excessive optimism); rationalizing
www.imagingbiz.com | april/May 2011 | Radiology Business JouRnal 65

Governance | The Practice
warnings that challenge group assumptions; unquestioned belief in the moral superiority of the group; stereotyping those opposed to the group as weak, evil, or stupid; and illusions of unanimity (consensus) in the decision (where a partner’s silence is viewed as tacit agreement).
An information cascade can be considered a variant of game theory. An information cascade develops in an open forum such as a partnership meeting. In the meeting, a decision is to be made by the group. The proposal is a simple binary question: Should we open the office on Saturday or not? Each member of the group, in sequence, must make a decision on the question. Since the meeting is open, each person knows the decision (and the opinions) offered by each of the preceding individuals.
The new information garnered by observing the preceding choices alters the participants’ preexisting knowledge base and leads them to follow their predecessors, believing they might be correct—even if their choices are contrary to the participants’ firmly held preexisting knowledge/bias. The herd instinct is a powerful one.
Even if most of the individual partners have primary information favoring the correct conclusion, the aggregated partners might reach the wrong conclusion because of the cascade effect of observing the sequential comments and votes of the other partners. If one of the early speakers is particularly powerful,
intimidating, or animated, that person can start the cascade. An information cascade is a compelling challenge to the knowledge and beliefs of the individual partner. An information cascade can overcome all but the strongest and best-prepared partners.
Keep in mind that the individual partners believe that they are acting rationally and making the right judgment. They fully trust the evolving wisdom of the crowd and ultimately deny their own privately held beliefs. They tell themselves that it feels good to see that so many of their bright partners share the same opinion. They really trust these knowledgeable and wise people.
Pluralistic ignorance is an additional influence: All those opposed to the
proposition think they are alone in their beliefs because they see the cascade developing—when, in fact, several (if not all) members, based on their primary knowledge before the meeting, are opposed to the cascade-based conclusion.
IndecisionAnalysis paralysis and paradox of
choice are common problems in a medical group. A yes-or-no choice is certainly the most efficient format. If there are possibilities other than aye and nay, however, failure to reach any decision is a common outcome. The group is paralyzed by too many choices.
Depending upon the difficulty of the question, resolution of the issue may be beyond the capacity of the consensus governance model. In this circumstance, making no decision is, in fact, a decision. It is firmly established that making no decision constitutes a decision—and, on occasion, the worst possible decision. Making no decision is a compelling indictment of the inadequacy of the consensus management process.
Lurking in the background in these prolonged indecisive meetings, look for incomplete knowledge, personal bias, and dysfunctional management personnel. Groupthink and information cascade are other extremely subtle developments in a partnership meeting.
Peer pressure and the herd instinct obviously will dilute the quality of discussion and impede a rational voting procedure. The wisdom of the crowd demands full participation by all attendees. Preparation beforehand, with complete and exhaustive research conducted by the partners, is a necessity.
Consensus management is a truly elegant management system that is very attractive to the educated, thoughtful physician. It has variously been celebrated for being inclusive, participatory, collaborative, cooperative, and egalitarian. The only problem is that consensus management doesn’t work, particularly when the issues are complex and difficult.
The concepts of wisdom of the crowd, groupthink, and information cascade are difficult and challenging. A medical
66 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
Depending upon the difficulty of the question, resolution of the issue may be beyond the capacity of the consensus governance model. In this circumstance, making no decision is, in fact, a decision. It is firmly established that
making no decision constitutes a decision—and, on occasion, the worst possible decision. Making no decision is a compelling indictment of the inadequacy of the consensus management process.
—David F. Hayes, MDWindsong radiology

IMAGINGACQUISITIONS
Old or unused imaging equipment is a business liability.
It consumes valuable space while being under- or
unutilized. On the other side, there is the high cost
of removal, low trade-in value and the challenge of
coordinating deinstallation and replacement.
At Imaging Acquisitions, we turn the replacement process
into an advantage for your business. We purchase and
deinstall your old or unused hardware at a fair price,
beating manufacturer trade-in by 15% or more. We also
focus solely on buying, have no interest in selling you
equipment and work closely with you and manufacturers
to ensure a seamless replacement... on your timeline.
For the most value for your out-of-date or idle equipment
and the flexibility, responsiveness and professionalism
you demand, call us today at (855) 411-7687.
(855) 411-7687
ReplAce Old equIpment. Get OptImAl vAlue. SeAmleSSly & On yOuR Schedule.
Optimal value. Unsurpassed professionalism. Seamless transition.

Governance | The Practice
68 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
group should not choose consensus management or any of its variants unless the partners fully understand these questions:
If democratic consensus governance doesn’t work, how can we ever acquire the benefit of the wisdom of the crowd? Is there such thing, or is it a myth? Is democratic governance valid if it is not accompanied by the wisdom of the crowd? Is groupthink an inevitable contaminant of the wisdom of the crowd and, consequently, the democratic governance process?
Can we get beyond groupthink? No matter what governance process we choose, whether democratic or otherwise, can we somehow benefit from the wisdom of the crowd? In its purest form, how could the wisdom of the crowd fail to be helpful?
Is it possible to build enough safeguards to forestall the apparently inevitable degeneration into groupthink? Furthermore, can we assure ourselves that our knowledge is complete, rather than incomplete? Can physicians assure themselves that when they vote, they will select the option that best serves the partnership, rather than ceding—under the protective cloak of a secret ballot—to their personal wants and needs?
By the time the hypothetical partnership’s meeting opens to discuss Saturday office hours, the wisdom of the crowd has descended upon the partners. They firmly believe that they can work out a solution that will best serve the purposes of the partnership. Although the aggregated partners believe that they possess superwisdom, their opinions are not based on wisdom, but on incomplete knowledge—further corrupted by personal agenda and bias. As regularly happens in these circumstances, an unstoppable information cascade develops. No one in the meeting possesses enough knowledge to turn back this cascade.
By the end of the meeting, the group’s wisdom has morphed into groupthink, leading the partners to choose to open the office, with limited services, from 10:00 am to noon, thereby offending the clinicians. The Saturday office-hours project is doomed from the beginning.
Even when the project fails, six weeks later, the partners have no insight whatsoever. Instead, they blame the clinicians. Such is the power of the wisdom of the crowd.
corporate ManagementIn the usual corporate management
system, the partners meet for the same purpose. The process of the corporate meeting, however, is completely different. In typical corporate settings, CEOs are fully authorized to act and are fully responsible and accountable for their actions. It is their responsibility alone to analyze and act upon a proposal.
To assist them in carrying out their responsibilities, CEOs call meetings of their expert advisors, seeking their knowledge and opinion. The purpose of these meetings, therefore, is to educate CEOs, not to develop policy (and certainly not to vote).
These meetings are educational events rather than voting exercises. The experts are interrogated aggressively, elevating the knowledge base of all in attendance, including CEOs. Note that there is negligible incomplete knowledge because only experts are allowed to speak, and those experts are thoroughly grilled to unmask any incomplete knowledge. Personal biases and personal agendas are similarly exposed. An appropriately conducted meeting is managed ruthlessly, and the experts are held accountable for the strengths and weaknesses of their opinions.
In The Effective Executive, Peter F. Drucker (1909–2005) stated that effective decision makers deliberately create dissent and disagreement rather than consensus. “Decisions of the kind the executive has to make are not made well by acclamation,” he wrote. “They are made well only if based on the clash of conflicting views.”1
Since this kind of meeting does not develop a formal opinion, groupthink is nonexistent. Rather, such meetings only develop facts and fact-based opinions. The final judgments are developed by CEOs alone, after they listen to the spirited, dissenting, and often contradictory arguments arising from the knowledgeable experts.
There is no information cascade because the opinions of the experts are based on fact and are subject to withering challenge by those attending the meeting. Furthermore, sequential comments (as spoken in consensus meetings) leading to an information cascade are not part of the usual corporate meeting. Rather, comments in the corporate meeting are data driven and are not sequential. They are not derived from the prior speaker’s opinion and do not influence the knowledge or comments of the following speakers.
Fully accountable CEOs develop the final opinions and policies based on the facts and fact-based opinions they gather at the meeting. The partners and experts at the meeting do not make the final judgment. There is no vote. Rather, they submit facts and fact-based opinions, leaving the decisions to the responsible and authorized CEOs. The CEOs, not the aggregated partners, implement the new policies. The CEOs alone are responsible for the initial analyses, the final decisions, and the implementation of the new policies.
Responsibility and authority to develop and implement policy are hugely important. Corporate CEOs are fully authorized to act and are fully accountable for their actions. Unfortunately, it is commonplace, in organizations managed by consensus, for no single individual to hold these responsibilities. Rather, accountability and authority to act are, as a signature of equality, intentionally
Different protocols
An awareness campaign of the American College of Radiology (ACR), the Radiological Society of North America (RSNA), the American Society of Radiologic Technologists (ASRT), and the American Association of Physicists in Medicine (AAPM).
Every patient and case is different, so perform only necessary imaging exams, make sure it’s the right scan for the indication and optimize the radiation dose delivered to each patient.
Radiation safety in adult imaging is vital to quality patient care. Take the pledge today at imagewisely.org.
Different patients
imagewisely.org I

Governance | The Practice
70 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
diffused throughout the partnership. Thus, the group of equals is paralyzed with indecision and inaction during its most difficult challenges.
When all options are difficult, consensus decisions and consensus actions are simply beyond the aggregated wisdom and knowledge of the arguing partners and their management process. They are crippled by incomplete knowledge, personal goals and wants, and a voting process that demands—absolutely demands—a mediocre, suboptimal outcome.
a Better ModelBecause of increasing challenges by
government entities, Byzantine behavior by enlarging hospital corporations, aggressive postures by insurance companies, and increasing intergroup and intragroup competition, it is in the best interest of the partnership that the group be managed as a typical corporate entity with an authorized and responsible CEO. Only then will the group be spared the alluring imperfections of consensus management.
Be aware, though, that any decision can occasionally become a failure, despite the best efforts of the management team. In that circumstance, it is easier to fire the dysfunctional CEO than it is to fire your own dysfunctional consensus opinion. Who takes the hit if the consensus opinion is wrong? Do you fire the group? Do you fire the management (consensus) process? Because you, the partner, are really at fault, do you simply fire yourself? Maybe you just move along, doing none of these.
Choosing the usual corporate management process is a large and bitter pill for the group. The comparison of corporate management with consensus
management can be accomplished more easily if it is viewed from a broader perspective. The group should schedule an evening meeting for this purpose, with a limited agenda (and unlimited food and drink).
At this meeting, review the vision statement and the mission statement as they were written at the time of the group’s founding. Understand their purpose. Understand their cultural and spiritual sources.
Partners should acknowledge that their professional careers and livelihoods (food and clothing, mortgages, children’s tuition fees, and retirement savings) depend on their fulfillment of the vision and mission statements. Put your heart and soul into these statements. Give them real meaning.
Have a knowledgeable discussion of the best management process to use to achieve those goals. Along the way, discard all preconceived notions. Put all options on the table. When stuck, reread the vision statement and the mission statement.
Consider hiring outside, knowledge-able experts to keep you focused on your goal of developing a functional and competitive group. Consider having a facilitator act as a referee—because it may be a difficult meeting.
What about the wisdom of the crowd? Is it only a myth? Since knowledge is a substrate of wisdom, and knowledge is incomplete in the consensus-managed partnership, wisdom can only be a myth in the consensus-managed group.
Does wisdom exist in the group with corporate management? Possibly; we trust that the knowledge level is adequate in the corporate setting. We know, however, that wisdom has other components, in addition to knowledge. All of us can only hope that those other segments come together in the corporate CEO. That’s why the CEO is given a contract, not a crown.
David F. Hayes, MD, is a radiologist practicing at Windsong Radiology, Williamsville, New York.
reference1. Drucker P. The Effective Executive. New York, NY: HarperCollins; 1967.
acr(800) 770-0145www.acr.org .......................................................... 25, 69
affiliated Professional Services(800) 841-5200www.affilprof.net ........................................................ 47
aHra(800) 334-2472www.ahraonline.org .................................................... 71
BrIT Systems(800) 230-7227www.brit.com ............................................................. 57
compone(800) 300-6717www.componeltd.com ............................................... 73
eraD(864) 234-7430www.erad.com ........................................................... 17
FujIFIlM Medical Systems(800) 431-1850www.fujimed.com ......................................................... 5
Ge Healthcare(800) 886-0815www.gehealthcare.com .............................................. 74
Hitachi Medical Systems america(800) 800-3106www.hitachimed.com ................................................... 2
Hosted PacS Solutions(888) 383-0388www.hostedpacs.com ................................................ 59
Imaging acquisitions(855) 411-7687 ........................................................... 67
imagingBiz(714) 832-6400www.imagingbiz.com ................................................. 35
Imaging on call(888) 647-5979www.imagingoncall.net ......................................... 19–22
Integrated Medical Partners(877) 816-1467www.integratedmp.com ............................................. 27
Intelerad Medical Systems, Inc(514) 931-6222www.intelerad.com ..................................................... 29
joint commission(630) 792-5286www.jointcommission.org/imaging ............................ 60
McKesson(800) 661-5885www.allaboutPACS.com ............................................ 49
Merge(877) 446-3743www.merge.com .......................................................... 3
MMP(800) 895-0002www.cbizmmp.com ...................................................... 7
nightshift(888) 318-8900www.nightshiftradiology.net ....................................... 31
nuance communications(781) 565-5000www.nuance.com/healthcare ..................................... 61
ProScan Imaging(877) PROSCANwww.proscan.com...................................................... 33
radisphere(866) 437-7237www.radisphere.net.................................................... 15
ramSoft(888) 343-9146 option 2www.ramsoft.com ...................................................... 53
regents Health resources, Inc(800) 423-4935www.regentshealth.com ........................................ 38–40
revana Health(888) 973-8262www.revanahealth.com .............................................. 45
Sectra(203) 925-0899www.sectra.com ......................................................... 63
virtual radiologic (vrad)(800) 737-0610www.virtualrad.com .................................................... 11
vital Images(952) 487-9500www.vitalimages.com ................................................ 37
vMG Health(214) 369-4888www.vmghealth.com .................................................... 9
Zotec Partners(317) 705-5050www.zotec.com .......................................................... 13
advertiserindex

The AHRA 39th Annual Meeting and Exposition will be held at the stunning Gaylord Texan Resort and Convention Center located in Grapevine, Texas near Dallas/Fort Worth.
There's a new, condensed schedule this year which offers the same number of CE opportunities while allowing you less time away from home and work. Also new this year will be a Practice Management Track presented by the Radiology Business Management Association (RBMA).
Register online now at: www.ahraonline.org.The full meeting brochure with a detailed schedule and program descriptions will be available in mid-April.
Save the date!August 14 17 2011
Building the Business of Radiology
- ,

It was interesting recent announce-ments1,2 from Google (Mountain
View, California) that got me thinking about our similarities. Google’s new ranking system
was not universally endorsed, especially by those organizations that are not in the business of creating and frequently updating original content. The company that virtually invented the modern weighted search has, over the years, developed grading systems that reward those websites that are rich in
content, those that update their sites with fresh information, and those that contribute to the body of knowledge.
In the eyes of Google, distinctions should be made between those organizations that merely show up and those that actually invest heavily in building content; in other words, those that actually add value. Google has announced new criteria and guidelines for ranking websites, based on tightening these distinctions.
We agree, and therefore applaud Google’s move, because we feel exactly the same way. In fact, we created this business based on the notion that radiologists, health-care executives, and those running hospitals and outpatient centers want and need much more than had been provided to them at the time. They (you) need content that is rich in depth, timely, relevant, and helpful in ways that will ensure that you have the information and tools necessary to compete effectively in a changing medical-imaging arena. Meeting this need was our primary vision when we launched Radiology Business Journal.
As a result, the publication that you hold in your hands is at least twice the size of most other publications vying for your attention in the radiology space. RBJ contains mountains of new and innovative editorial content—page after page of in-depth and relevant material that is written and edited by a team that is simply unmatched in the profession. Our editorial staff takes great pride in the fact that our articles are independent, unbiased, and vendor neutral. We consistently bring to life those stories that feature the credibility that only a team of objective journalists could provide. Unlike some who publish
with the old-media mindset, we have no quid pro quo; there is no trade-off between advertising and the editorial pages.
We know that this makes a difference because you need high-impact information that will help you navigate the quickly changing legislative, regulatory, business, and clinical landscape that is the new normal for the medical-imaging marketplace. RBJ has emerged as the go-to source for such top-level information.
Just as Google does, RBJ takes the time to sort through the maze of data, publishing only the information that adds to the debate and body of knowledge—and that rises above the mediocre, to bring you the articles that make a difference in the business of your practice. Our content is crisp, intelligent, and thought provoking. We know this because you have taken the time to tell us why you prefer to read RBJ. It is most gratifying to know that our effort and vision are hitting the mark and that you appreciate the difference that a commitment to high-quality journalism makes in this hectic industry.
72 Radiology Business JouRnal | april/May 2011 | www.imagingbiz.com
What Google and RBJ Have in CommonWe applaud Google’s attempt to scratch the surface and recognize quality in content, and we thank our readers and supporters who have done the same By Curtis Kauffman-Pickelle
FinalREAD
In the eyes of Google, distinctions should be made between those organizations that merely show up and those that actually invest heavily in building content; in other words, those that add value.
As you will notice in this issue, we continue to add the industry’s most important and enlightened vendors, manufacturers, and service organizations as our sponsors. We are grateful to those companies that also understand that their messages need to be seen and read within an editorial environment that is stimulating and relevant to their customers. They succeed when you succeed, and they truly understand that in order for you to succeed, you need solutions and support that go way beyond the rehash of press releases. You need case studies, success stories, and articles by thought leaders that resonate with your situation—that help you stretch to reach new levels of competence and achievement.
Thanks for your loyal readership over the years, and thanks to our growing list of advertisers for their support and endorsement of our concept. We are dedicated to guiding radiologists and health-care executives as you face new pressures, and it is our commitment to you that we will continue to add depth and breadth to all of our publications, based on the accumulated knowledge that these many years in medical imaging can provide.
Curtis Kauffman-Pickelle is publisher of ImagingBiz.com and Radiology Business Journal, and is a 25-year veteran of the medical-imaging industry.
References1. Singhal A, Cutts M. Finding more high-quality sites in search. http://googleblog.blogspot.com/2011/02/finding-more-high-quality-sites-in.html. Published February 24, 2011. Accessed April 14, 2011.2. Singhal A. High-quality sites algorithm goes global, incorporates user feedback. http://googlewebmastercentral.blogspot.com/2011/04/high-quality-sites-algorithm-goes.html. Published April 11, 2011. Accessed April 14, 2011.
ONE Easy Transition.
O K L A H O M A K A N S A S M I S S O U R I T E X A S N E W Y O R K F L O R I D A C O L O R A D O C A L I F O R N I A
Hassle-free practice management. Efficient, streamlined processes. Innovative technologies. A 14% increase in income.Interested? CompONE can deliver all this and more, and with our dedicated implementation team, it's never been easier to make the transition. Give us a call today.

There’s a clear path to a patient safe culture
GE Healthcare
GEHCDISV1001 8.125 x 10.875 Clear Path_RB Journal
Patient safety solutions from GE Healthcare Performance Solutions. One in 20 people will contract an infection during their hospital care in the United States, 90,000 of which die.1 Reducing this level of patient harm requires understanding not just adverse events, but also near misses.The GE Patient Safety Organization works with our members to capture best practices, share stories and see patterns in the data, in a safe community that reveals the path to a patient safe culture.
To see how we can help you perform at the next level, and to learn more about the GE PSO, visit www.ge.com/psopath.
1Leapfrog Hospital Survey Results. 2008:7.©2011 General Electric Company, doing business as GE Healthcare.