published ahead of print effectiveness of lumbopelvic...
TRANSCRIPT

. . . Published ahead of Print
Medicine & Science in Sports & Exercise® Published ahead of Print contains articles in unedited manuscript form that have been peer reviewed and accepted for publication. This manuscript will undergo copyediting, page composition, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered that could affect the content.
Copyright © 2016 American College of Sports Medicine
Effectiveness of Lumbopelvic Exercise in Colon Cancer Survivors
Irene Cantarero-Villanueva
1,2,3, Antonio Sánchez-Jiménez
3, Noelia Galiano-Castillo
3,
Lourdes Díaz-Rodríguez1,2,4
, Lydia Martín-Martín3, and Manuel Arroyo-Morales
1,2,3
1Institute for Biomedical Research ibs, Granada, Spain
2Mixed University Sport and Health Institute, iMUDS University of Granada, Spain
3Department of Physical Therapy, Health Sciences Faculty, University of Granada, Spain
4Department of Nursing, Health Sciences Faculty, University of Granada, Spain
Accepted for Publication: 22 February 2016
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
Effectiveness of Lumbopelvic Exercise in Colon Cancer Survivors
Irene Cantarero-Villanueva1,2,3
, Antonio Sánchez-Jiménez3, Noelia Galiano-Castillo
3, Lourdes
Díaz-Rodríguez1,2,4
, Lydia Martín-Martín3, and Manuel Arroyo-Morales
1,2,3
1Institute for Biomedical Research ibs, Granada, Spain
2Mixed University Sport and Health Institute, iMUDS University of Granada, Spain
3Department of Physical Therapy, Health Sciences Faculty, University of Granada, Spain
4Department of Nursing, Health Sciences Faculty, University of Granada, Spain
* Corresponding author: I. Cantarero-Villanueva
Department of Physical Therapy, Health Sciences Faculty, University of Granada, Parque
Tecnológico de la Salud. Avenida de la Ilustración,60 18016 Granada, Spain
Email address: [email protected]
Phone: +34958248764
Fax: +34 958 24 20 70
This study was supported by a grant from the Education Ministry and Economy, Innovation,
Science and Employment Counseling through the University of Granada CEI-BioTic. The results
of the present study do not constitute endorsement by the ACSM.
CONFLICT OF INTEREST: None declared.
Running title: Lumbopelvic exercise in cancer survivors
Medicine & Science in Sports & Exercise, Publish Ahead of PrintDOI: 10.1249/MSS.0000000000000917
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
ABSTRACT
Introduction: This study evaluated the effectiveness of lumbopelvic exercise in improving
health-related fitness, anthropometric measurements and body composition in colon cancer
survivors (CCS).
Methods: Forty-six CCS (35% female, n=14) were assigned to two groups for this randomized
controlled clinical trial: a trunk muscle stabilization exercise program group (CO-CUIDATE)
and a usual-care group. The CO-CUIDATE program was conducted for 8 weeks (3 times per
weeks). The primary endpoint was isometric abdominal strength measured using the trunk curl
test. The secondary endpoints used were isometric back strength, functional capacity, lower-body
flexibility, weight and anthropometric measurements evaluated at baseline, after the physical
exercise program and after 6 months of follow-up. A trained member of the research group with
5 years of experience working with cancer patients and who was blinded to the patient group
assessed the variables. All physical tests were carried out with multiple observations.
Results: The adherence to intervention was 88.36%, and 2 drop-outs (10.5%) were recorded.
Minor side effects, including discomfort with the exercises in the first sessions, were reported by
the participants. ANOVA demonstrated significant differences in group x time interactions for
isometric abdominal strength (F= 7.7; p= 0.001), functional capacity (F= 4.6; p= 0.015), lower-
body flexibility (right, F= 4.3, p= 0.021 and left, F= 3.6, p= 0.034) and waist circumference (F=
5.7; p= 0.07), which were the best values for the CO-CUIDATE group. No significant changes in
isometric back strength, weight, hip circumference or body composition were observed.
Conclusion: An 8-week program based on stabilization exercises is a promising strategy to
increase health-related fitness and reduce waist circumference in CCS. An exercise program
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
based on lumbopelvic exercise is a feasible intervention to improve the control of deep
abdominal muscles and health-related fitness.
KEYWORDS: colon cancer survivorship, health related fitness, anthropometric, physical
activity, stabilization exercise program
TRIAL REGISTRATION: Clinical Trials.gov NCT02052050 (available in
https://clinicaltrials.gov/ct2/show/NCT02052050?term=cantarero+villanueva&rank=1)
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
INTRODUCTION
Colorectal cancer is the cause of 13% of cancer deaths (13). The survival rate 5 years after
diagnosis can reach up to 90.3% when the tumor is detected at the initial stages (16). However,
recurrence rates can reach up to 60% (22). A recent study concluded that colon cancer in some
subgroups results in a similar survival rate to that of people without cancer, which highlights the
importance of cancer nonrecurrence (27). Physical activity and body composition play vital roles
in the prevention of cancer recurrence (23). Therefore, health support programs to control or
improve these risk factors are needed.
Colon cancer survivors (CCS) suffer from a reduction in health-related fitness, both objectively
and perceptively (31), including decreases in balance, flexibility, functional capacity and the
isometric strength of abdominal muscles. This decrease not only affects the patient’s functional
ability but is also accompanied by a decrease in abdominal muscle width (32), which could lead
to the development of chronic low back pain. Therefore, an effective choice of intervention for
these patients should consider the rehabilitation of the lumbopelvic area. However, we are not
aware of previous studies that describe a specific protocol for training this area of the body in
CCS.
Reduced isometric strength of the abdominal wall muscles in colon cancer patients who
underwent longitudinal abdominal incisions has been demonstrated (11). This reduction in
isometric strength in abdominal flexor muscle can reach up to 65% compared with the strength
of healthy controls (31). CCS also show a decrease in fatigue resistance in the soleus, a postural
muscle in the legs (28). Evidence indicates that a therapeutic approach to prevent this loss should
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
be directed at the stimulation of mitochondrial biogenesis and the reduction of muscle
proteolysis and inflammation (1). Physical activity reduces the loss of muscle mass and improves
mitochondrial content (4). Therefore, a muscle stabilization exercise program could improve
motor control in lower back and pelvic muscles. A physical activity program based on muscle
stabilization exercises, such as Pilates-based exercise programs, may be an option to solve this
problem. However, no studies have demonstrated the effects of this type of exercise program in
CCS.
Currently, gaining popularity, muscle stabilization programs promote improvements in the
strength and control of trunk muscles, endurance, flexibility, balance and breathing (17). Indeed,
the beneficial effects of these programs have been widely studied because these programs have
positive effects on quality of life (7,5), physical fitness, mood (5), postural balance (7), fall
prevention, (5) and body composition (29) in older people. However, few studies have used
muscle stabilization exercises in cancer patients.
The American College of Sports Medicine (ACSM) expressed the need in 2010 for increased
research to expand our knowledge of the safety and efficacy of Pilates in treating cancer patients
(34), in which motor control of the lumbopelvic area is addressed based on a specific training
philosophy. In addition, it has been shown that Pilates program gives similar results for
improving muscle endurance to those of traditional resistance programs in breast cancer patients
(20) and that it increases functional capacity and flexibility (12), shoulder functionality, quality
of life, mood and body image (38) in patients with this type of cancer. However, it is necessary
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
to enhance the effects of stabilization exercise programs based on Pilates in cancer patients,
especially in colon cancer patients.
The present study evaluated the effects of a physical activity program incorporating lumbar and
pelvic stabilization exercises on health-related fitness, anthropometric measurements and body
composition in CCS. We hypothesized that a CO-CUIDATE exercise program based on
lumbopelvic exercises would improve health-related fitness, anthropometric measurements and
body composition endpoints compared with the effects of the usual-care protocols.
METHODS
SUBJECTS:
For this randomized controlled clinical trial, 46 CCS (35% female, n=14) were assigned to one
of two groups within one year of their completion of primary treatment (Clinical Trials.gov
NCT02052050): a group undergoing a trunk muscle stabilization exercise program (CO-
CUIDATE group) and a usual-care group. The study was performed from September 2013 to
December 2014. Participants were recruited from the Department of Surgery at the University
Hospital San Cecilio, Granada (Spain), and they were eligible if they (1) were more than 18
years old, (2) received curative treatment due to cancer (surgery, chemotherapy and/or
radiotherapy), (3) were diagnosed with grades I to III A of colorectal cancer and (4) completed
coadjuvant treatment. Subjects were excluded if they presented cancer recurrence, underwent
previous abdominal surgeries or were diagnosed with concomitant conditions, such as previous
lower-back pain or musculoskeletal conditions (e.g., osteoarthritis, fibromyalgia or chronic
fatigue syndrome).
ACCEPTED
Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
Two oncology surgeons at the hospital encouraged patients to participate in the study to
stimulate subject participation (24). Interested participants were called and fully informed about
the study. An appointment was scheduled, and after passing a medical and physical examination,
patients signed a consent form. The Research Ethics Committee (Granada, Spain) granted ethical
approval (CEI2013-MP-18) for the study, and the trial followed the Helsinki Declaration for
biomedical research (14/2007).
Epidat 3.1 software (Xunta de Galicia, Spain) was used to calculate the sample size. The sample
size was based on detecting a minimum difference of 29.19 seconds in the post-treatment
abdominal isometric endurance scores, according to previous research using a similar exercise
program in breast cancer survivors (8), with an α-level of 0.05, a desired power of 80% and an
estimated standard deviation of ± 29 seconds. Each group included 18 participants. We chose 23
participants for each group assuming a 20% drop-out rate.
Participants were placed into two groups (CO-CUIDATE or control group) in two randomized
cycles (block size=23) using computer-generated numbers from Epidat 3.1 software (Xunta de
Galicia, Spain), and the sequence created was introduced in numbered, opaque, sealed envelopes
by an external researcher who did not participate in the study. The envelopes were opened to
obtain group assignments after the participants were evaluated.
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
INTERVENTION:
Two physiotherapy experts in oncological rehabilitation with more than 7 years of experience
working with oncology patients performed the CO-CUIDATE program, which was conducted in
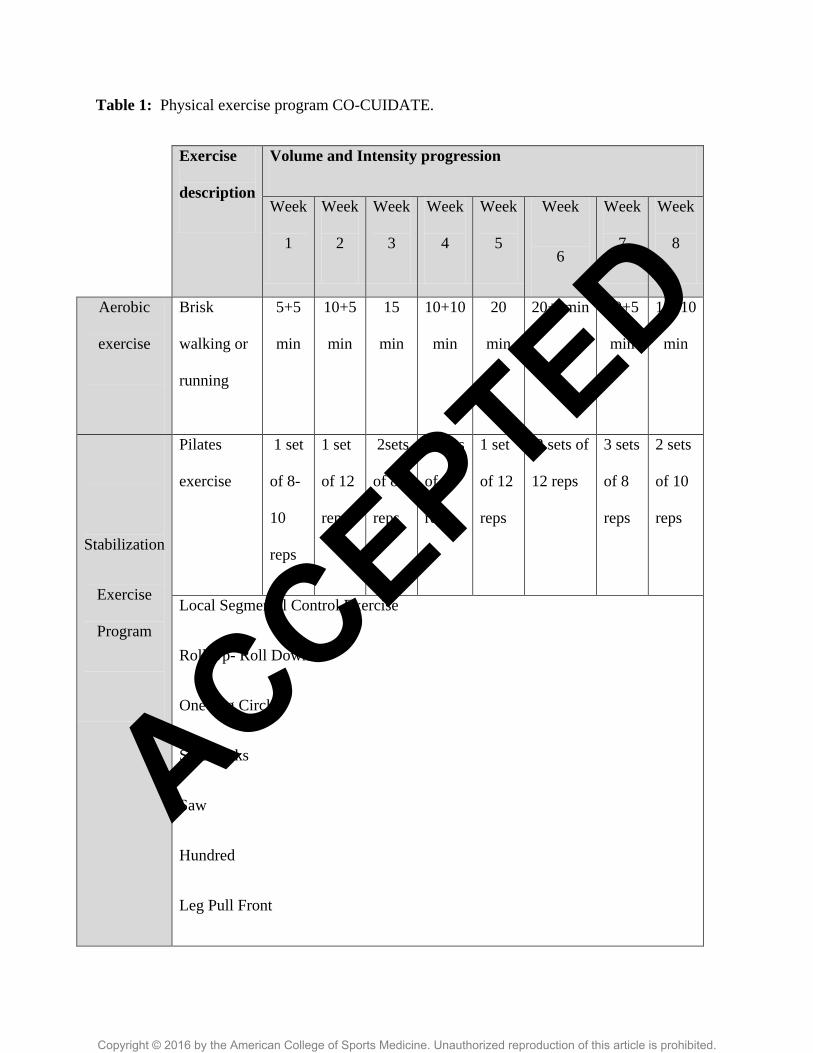
90 minute sessions 3 times per weeks for 8 weeks. Each session included warm-up exercises (10
to 20 minutes), core stabilization exercises (20 to 30 minutes) and stretching exercises (table 1).
The exercises were adapted to each participant’s potential. Each patient kept a diary throughout
the exercise program to register perceptions of fatigue (Borg Rating of Perceived Exertion Scale)
and adverse effects of the program. Adherence was defined based on the patient’s attendance of
the CO-CUIDATE sessions, and patients were considered as drop-outs if they did not participate
in at least 75% (18) of 24 sessions.
The control group received the usual treatment, which was stipulated by their oncologist. It
consisted of some general recommendations for a healthy lifestyle that were delivered at the start
of the program in paper format. Their physical activity level was controlled for during the study
period to avoid a possible bias through a follow-up assessment using the Spanish version of the
Minnesota Leisure questionnaire. Control subjects were assessed at the same times as the CO-
CUIDATE group (baseline, 8 weeks and 6 months). For ethical reasons, control patients were
allowed to participate in the same exercise program as the CUIDATE group once the study
period was completed, but these data were excluded from the analyses.
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
ENDPOINTS AND MEASUREMENTS
Health-related fitness endpoints
The primary outcome was isometric abdominal strength, which was assessed using the trunk curl
test. Patients remained in a supine position with a 90-degree flexion of both knees and hips and
with their arms extended without touching their knees. Patients performed a trunk curl and
maintained an isometric position that separated the inferior angle of the scapulae from the
stretcher for as long as possible up to a maximum of 90 seconds. This test exhibits an intraclass
correlation coefficient (ICC) > 0.97 (22).
Secondary endpoints
1. Physical endpoints
Isometric back strength was measured using a back dynamometer (TKK 5002 Back-A; Takey,
Tokyo, Japan) with a precision of 1 kg. Patients were measured in a standing position with a
lumbar flexion of 30º, and they performed an extension of the trunk three times. The average
value was used for analyses. This test showed acceptable to good reliability (ICC=0.81 and 0.85)
(14).
Functional capacity was determined based on a walking test used to measure the distance (m)
that patients could walk in 6 minutes. This test was performed using a treadmill (H-P-COSMOS
for graphics; Germany) after previous training, and patients were allowed to increase or decrease
the treadmill speed. This test is reliable in cancer patients (ICC>0.93) (33).
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
Lower-body flexibility was assessed using a chair sit-and-reach test. Patients were instructed to
slide their hands forward as far as possible to touch their toes. The distance between the tip of the
fingertips and the toes was measured. If the fingertips touched the toes, the score was zero. If the
fingertips did not touch the toes, the distance between the fingers and the toes was measured as a
negative score. If the fingers overlapped the toes, the distance of the overlap was measured as a
positive score. Two trials with each leg were performed, and the average of both legs was
included in the analysis (31). The reliability of this test exhibited an ICC=0.94 (9).
These physical tests have been used previously with colon cancer patients (31), and all of these
tests were carried out with multiple observations.
2. Anthropometric endpoints
Waist and hip circumferences were measured using a plastic tape measure. Waist circumference
was assessed midway between the lower rib margin and the top of the iliac crest (cm) at the end
of a normal breath. Hip circumference was measured at the level of the greater trochanter. The
ICC for waist and hip circumferences were 0.89 and 0.81, respectively (37).
Height and body composition was assessed using bioelectrical impedance (InBody 720;
Biospace, Gateshead, UK). Height, body fat percentage, skeletal muscle mass (kg) and body
mass indexes were recorded for analysis. The instrument used exhibits high reliability (39).
A trained member of the research group with 5 years of experience in taking these measurements
on cancer patients and who was blinded to patient group assessed these variables at the three
ACCEPTED
Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
time points. Measurements were performed in the physiotherapy laboratory of the Faculty of
Health Sciences at the University of Granada (Spain).
STATISTICAL ANALYSIS
Mean, coefficient intervals (confidence level, 95%) and standard deviations were used in
descriptive analyses. Student’s t and chi-square tests were used to assess the ability of the
randomization process to avoid differences between groups at baseline. The Shapiro-Wilk test
was used to assess the normality of the distribution of the variables.
A repeated-measure ANCOVA between the three time points (baseline, post-program and 6
months of follow-up) was used to examine the between-group and within-subject differences.
Patient age and tobacco and alcohol use were used as covariates to examine the influence of
these variables on the main analysis of this study. Cohen´s d was calculated to examine
intergroup effects and determine if there were small (d<0.2), negligible (0.2<d>0.5), moderate
(0.5<d>0.8) or large (d>0.8) differences (10).
The Statistical Program for Social Sciences (IBM, SPSS version 22.0) was used for statistical
analyses with a 1% level of significance for all statistical tests, and analyses were performed
according to the intention-to-treat principle (ITT) The worst-case value was used to replace
missing data, following a previously reported procedure (30).
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
RESULTS
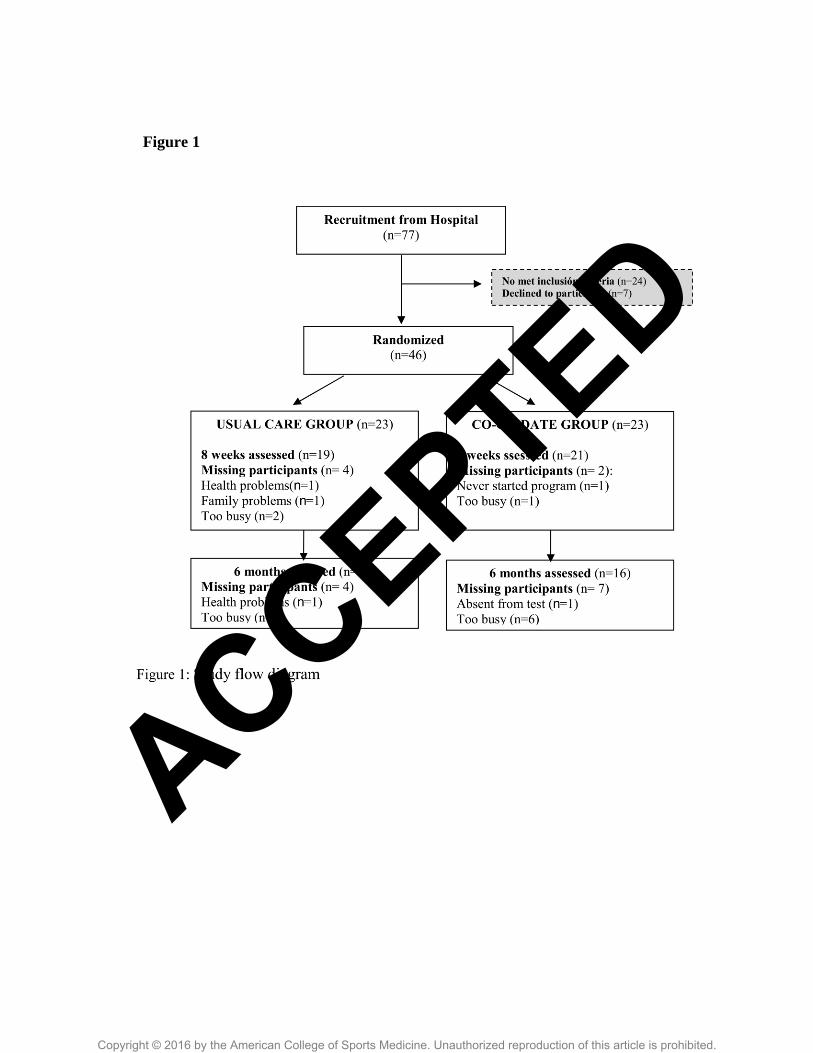
Seventy-seven CCS were evaluated with regard to the inclusion criteria. The 46 patients who met
the criteria were randomized into two groups: 23 patients in the CO-CUIDATE group and 23
patients in the Usual-care group. Figure 1 illustrates the number of CCS randomized into each
group; the number of and reasons for drop-outs are also shown. There were 2 drop-outs (10.5%)
in the CO-CUIDATE group (reasons: never started the program, n=1; too busy, n=1) and 4 drop-
outs (17.4%) in usual-care group (reasons: health problems, n=1; family problems, n=1; too
busy, n= 2). Table 2 shows the demographic, clinical and medical characteristics of the sample
group. There were no significant differences between groups for any variable at baseline (table
3). Adherence rates were calculated as the ratio of the number of exercise sessions performed
relative to the number of sessions prescribed. The average attendance of the CO-CUIDATE
group was 22.0±1.1 of the 24 sessions, with an adherence rate of 88.36%. Two participants in the
CO-CUIDATE group and one participant in the usual-care group experienced postoperative
ventral hernias. In the first sessions of the program, six patients expressed both neck and
abdominal discomfort with some of the exercises (roll up- roll-down and saw). They
subsequently underwent a slower progression and received more support to achieve the goals of
the program. Furthermore, one patient could not perform the aerobic exercise during one week
because he suffered a peripheral neuropathy. The average range of the perception of fatigue was
12 (6-17).
Health-related fitness endpoints
ANOVA revealed a significant difference (F= 7.7, p= 0.001) in the group x time interaction for
isometric abdominal strength. The CO-CUIDATE group experienced a greater increase in
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
isometric abdominal strength compared with that of the usual-care group after discharge (table
4). The intergroup effect size was large after the 8-week program (d = 1.2; 95% CI, -4.9 to 7.5).
The covariates did not influence these results. Analysis of isometric back strength (F= 2.1, p=
0.13) revealed a non-significant trend for the group x time interactions, with a greater increase in
the CO-CUIDATE group compared with that in the usual-care group (table 4).
Physical endpoints analyses:
Statistical analyses revealed significant differences in group x time interactions for the remaining
physical variables: functional capacity (F= 4.6, p= 0.015) and right and left lower-body
flexibility (F= 4.3, p= 0.021 and F= 3.6, p= 0.034, respectively). The CO-CUIDATE group
exhibited a higher increase in functional capacity and lower-body flexibility compared with the
results in the usual-care group after discharge (table 4). Intergroup effect sizes observed after the
exercise program were large for functional capacity (d = -0.8; 95% CI, -27.7 to -26.0) and for
right and left lower-body flexibility (d = -0.8; 95% CI, -2.7 to 1.0 and d = -0.8; 95% CI, -3.5 to
1.7, respectively). Effect sizes at the 6-month follow-up were large for functional capacity (d = -
0.9; 95% CI, -27.5 to 29.3). The inclusion of age as a co-variable in the analysis influenced right
(F= 2.8, p= 0.068) and left lower-body flexibility (F= 2.1, p= 0.135).
Anthropometric endpoint analyses
A significant group x time interaction was found for waist circumference (F= 5.5, p= 0.007). The
CO-CUIDATE group experienced a greater decrease in this variable compared with results in the
usual-care group (table 5). Intergroup effect sizes for waist circumference were large after the
exercise program (d = 0.9; 95% CI, -0.7 to 2.6) and moderate at the 6-month follow-up (d = 0.7;
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
95% CI, -0.3 to -1.7) (table 5). The inclusion of additional covariates did not significantly change
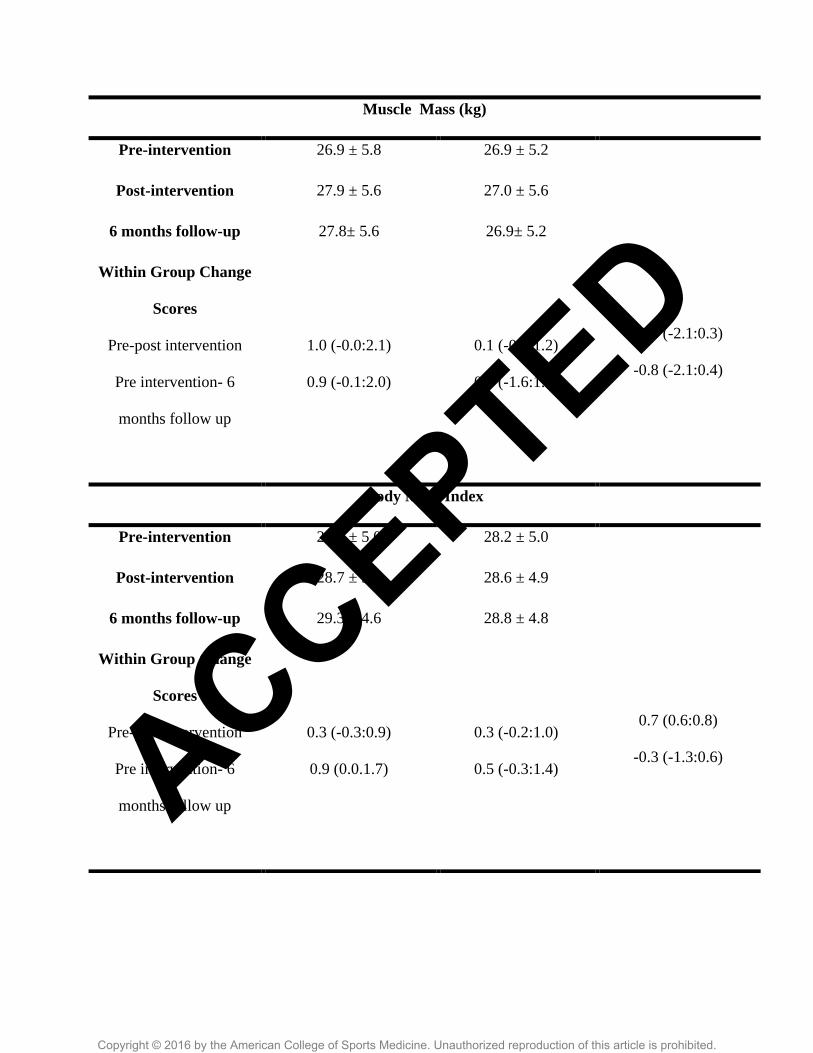
these results. There were no significant differences in the group x time interactions for the
variables of hip circumference, weight or body composition.
DISCUSSION
The results of this randomized trial partially confirm our hypothesis that the CO-CUIDATE
program widely improves isometric abdominal strength, functional capacity, and lower-body
flexibility and reduces waist circumference in CCS compared with the usual-care group after
completion of the exercise program and at a 6-month follow-up. No significant changes in
isometric back strength, hip circumference, body fat percentage or muscle mass were found.
The primary finding of this randomized controlled trial is that participants exhibited a large
effect size and a significant improvement in isometric abdominal strength after the CO-
CUIDATE program. These results are consistent with a previous study investigating the
stabilization of deep abdominal muscles in breast cancer survivors (8). CCS exhibit alterations in
abdominal deep muscles of more than 50% relative to healthy controls (31), high levels of lower-
back pain and muscle hyperalgesia up to 6 months after surgery (32). However, we have not
found any previous studies that report improvement in abdominal isometric strength despite
improvement in muscle strength using other exercise modalities in CCS (35). One plausible
explanation for our positive results is that CO-CUIDATE was performed under the supervision
of two physiotherapists with an expertise in oncological rehabilitation who encouraged the
patients during the exercises and ensured that each patient correctly executed the exercise
program. Furthermore, all exercise prescriptions (intensity, sets and repetitions) were generated
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
based on individual capabilities, which is a relevant requirement of exercise programs to achieve
better success. The changes found in this study support the possible inclusion of lumbopelvic
stabilization exercises in supportive physical exercise guides for colon cancer.
The CO-CUIDATE program resulted in large improvements in functional capacity and
flexibility. The gain of functional capacity is an important result of our trial (CO-CUIDATE
group = 79.7 meters vs. control group = 4.9 meters), and an improvement in walking distance of
54 meters is clinically relevant (26). Our results demonstrated improvements in muscle strength
and control that produced functional improvements, even though the program was not
specifically designed to improve functional capacity. These results are consistent with the results
found by Yuen and collaborators (40) in breast cancer survivors. These researchers demonstrated
that a 12-week exercise program performed at home increased functional capacity to a greater
extent when using resistance training (36.1 meters) than when using an aerobic program (11.5).
These results may be due to the selection of resistance exercises and improvements in the
muscular state to increase function and improve cardiorespiratory capacity. Functional capacity
is a very important modifiable risk factor after colorectal surgery (18), and it should be
considered in all support strategies in CCS. The benefits observed in functional capacity after
participation in the 8-week CO-CUIDATE program were maintained six months later (large size
effect), demonstrating that supportive strategies of physical activity are needed to improve
health-related fitness in colon cancer patients. Although the CO-CUIDATE program did not
focus on the improvement of functional capacity, functional capacity was improved.
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
The CO-CUIDATE participants exhibited a similar performance in the flexibility test as healthy
subjects in a previous study (31), but these values were below the standard values for adults (2.1
cm for women and 0.6 cm for men) (15). A probable explanation for this difference is that CCS
suffer abdominal pain after cancer treatment (32) because of illness and that they experience
more difficulty in performing trunk flexion. The inactivity experienced by cancer patients
because of treatment side effects may also lead to reduced physical functionality, which may
explain the differences between the studies. Our results suggest that the CO-CUIDATE program
resulted in positive effects on the health-related fitness, which usually decreases, of colon cancer
patients (31). Our results showing changes in flexibility were influenced by age because physical
fitness naturally decreases with age.
Isometric back strength was also improved after the CO-CUIDATE program, but these results
were not significant. Strength exercises effectively improve lumbar extension muscle activity
when the pelvis is stabilized (36). CCS suffer muscle alterations after interventions (11, 31, 32)
and experience lumbar pain and widespread hyperalgesia pressure pain in their muscles (32).
These results support the need for physical activity programs that include stabilization exercises
in CCS.
We also found significant differences after the CO-CUIDATE program in waist circumference,
with a large effect size, which is an important finding because abdominal obesity is a greater
predictor of colon cancer risk than general obesity (19). Our improvements are consistent with
more specific and longer lifestyle modification programs (35, 3) and programs that include
dietary changes (3). Bourke and collaborators (3) used a 12-week lifestyle program with a
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
greater volume of work per week as a method to further guide weight loss or control (30 minutes
of aerobic exercise and 2 or 4 sets of 8 to 12 repetitions along with dietary recommendations).
The CO-CUIDATE program obtained similar results in less time and with a lower exercise
volume and less specific weight loss management. Similar previous studies also found a
reduction in waist circumference (6), but we did not find any studies that used stabilization
exercise programs in CCS. Therefore, our CO-CUIDATE program may provide adequate
support for reducing the risk of colon cancer through a decrease in waist circumference and a
reduction in mortality (2). Future studies using this exercise modality combined with dietary
recommendations to maximize the effectiveness of both strategies on body composition in CCS,
which is the primary objective in this population, are warranted.
The limitations of the trial include the fact that the CO-CUIDATE program may require
significant resources for implementation. Two specialists led the exercise program, which is a
significant cost over time. Another limitation is the enrollment of patients with a tumor between
stage I and IIIa in a single hospital. Therefore, our participants could have some specific
characteristics that make extrapolation of our results difficult. To the best of our knowledge, this
study is the first randomized trial to demonstrate the benefits of a physical exercise program
using the stabilization of deep abdominal muscles in CCS, and the results provide evidence of
the necessity of a physical activity program in the rehabilitation of CCS. Few studies have
examined the short- and long-term effects of a physical exercise program based on stabilization
exercises in cancer patients (12, 20, 38), and no studies have investigated exercise in CCS.
Another strength of the study is the high adherence rate and the low dropout rate. The adherence
of the CO-CUIDATE group (88.36%) may be explained by the encouragement of oncologists to
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
participate (24). This adherence was similar to another supervised physical exercise intervention
with CCS (90%) (3), though it is slightly lower than adherence to exercise by patients with other
types of cancer (95%) (25).
In conclusion, the CO-CUIDATE program, which is an 8-week physical activity program based
on stabilization exercises, is a promising strategy for improving health-related fitness and
reducing waist and hip circumferences in CCS. These results are evident in the short and long
term.
CLINICAL IMPLICATIONS:
An exercise program based on lumbopelvic exercise improves the control of deep
abdominal muscles and health-related fitness.
An exercise program based on lumbopelvic exercise is adaptable to individual
capabilities.
The CO-CUIDATE program does not require expensive material.
ACCEPTED
Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
ACKNOWLEDGMENTS
The authors acknowledge the patients for their participation, and we are also grateful to the
Sporting Activities Centre of the University of Granada. This study was supported by a grant
from the Education Ministry and Economy, Innovation, Science and Employment Counseling
through the University of Granada CEI-BioTic. The results of the present study do not constitute
endorsement by the ACSM.
CONFLICT OF INTEREST AND SOURCE OF FUNDING
None declared.
ACCEPTED
Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
REFERENCES
1. Altman DG. Practical Statistics for Medical Research. London: Chapman & Hall;
1991.396-435 p.
2. Argilés JM, Busquets S, Stemmler B, López-Soriano FJ. Cachexia and sarcopenia:
mechanisms and potential targets for intervention. Curr Opin Pharmacol.
2015;22:100-106.
3. Bourke L, Thompson G, Gibson DJ, et al. Pragmatic lifestyle intervention in patients
recovering from colon cancer: a randomized controlled pilot study. Arch Phys Med
Rehabil. 2011;92(5):749-55.
4. Broskey NT, Greggio C, Boss A, et al. Skeletal muscle mitochondria in the elderly:
effects of physical fitness and exercise training. J Clin Endocrinol Metab.
2014;99(5):1852-61.
5. Bullo V, Bergamin M, Gobbo S, et al. The effects of Pilates exercise training on
physical fitness and wellbeing in the elderly: A systematic review for future exercise
prescription. Prev Med. 2015;75:1-11.
6. Cakmakçi O. The effect of 8 week pilates exercise on body composition in obese
women. Coll Antropol. 2011;35(4):1045-50.
7. Campos de Oliveira L, Gonçalves de Oliveira R, Pires-Oliveira DA. Effects of Pilates
on muscle strength, postural balance and quality of life of older adults: a randomized,
controlled, clinical trial. J Phys Ther Sci. 2015;27(3):871-6.
8. Cantarero-Villanueva I, Fernández-Lao C, Cuesta-Vargas AI, Del Moral-Avila R,
Fernández-de-Las-Peñas C, Arroyo-Morales M. The effectiveness of a deep water
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
aquatic exercise program in cancer-related fatigue in breast cancer survivors: a
randomized controlled trial. Arch Phys Med Rehabil. 2013;94(2):221-30.
9. Carbonell-Baeza A, Álvarez-Gallardo IC, Segura-Jiménez V, et al. Reliability and
feasibility of physical fitness tests in female fibromyalgia patients. Int J Sports Med.
2015;36(2):157-62.
10. Cohen J. A power primer. Psychological Bulletin. 1992;112: 155-159.
11. DuBay DA, Choi W, Urbanchek MG, et al. Incisional herniation induces decreased
abdominal wall compliance via oblique muscle atrophy and fibrosis. Ann Surg.
2007;245(1):140-6.
12. Eyigor S, Karapolat H, Yesil H, et al. Effects of pilates exercise on functional
capacity, flexibility, fatigue, depression and quality of life in female breast cancer
patients: a randomized controlled study. Eur J Phys Rehabil Med. 2010;46(4):1–7.
13. Global Health Observatory of the World Health Organization Web site [Internet].
Ginebra: World Health Organization; [cited 2015 May 14]. Available
from:http://www.who.int/gho/en/.
14. Gruther W, Wick F, Paul B, et al. Diagnostic accuracy and reliability of muscle
strength and endurance measurements in patients with chronic low back pain. J
Rehabil Med. 2009;41(8):613-9.
15. Kirkham AA, Neil-Sztramko SE, Morgan J, et al. Health-related physical fitness
assessment in a community-based cancer rehabilitation setting. Support Care Cancer.
2015;e25617069.
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
16. Klimentidis YC, Bea JW, Lohman T, Hsieh PS, Going S, Chen Z. High genetic-risk
individuals benefit less from resistance exercise intervention. Int J Obes (Lond).
2015;e25924711.
17. Latey P. The Pilates method: history and philosophy. J Bodyw Mov Ther.
2001;5(4):275-82.
18. Li C, Carli F, Lee L, et al. Impact of a trimodal prehabilitation program on functional
recovery after colorectal cancer surgery: a pilot study. Surgical
Endoscopy.2013;27:1072–82.
19. MacInnis RJ, English DR, Hopper JL, Gertig DM, Haydon AM, Giles GG. Body size
and composition and colon cancer risk in women. Int J Cancer. 2006;118(6):1496–
1500.
20. Martin E, Battaglini C, Groff D, Naumann F. Improving muscular endurance with the
MVe Fitness Chair™ in breast cancer survivors: a feasibility and efficacy study. J Sci
Med Sport. 2013;16(4):372-6.
21. McGill SM, Childs A, Liebenson C. Endurance times for low back stabilization
exercises: clinical targets for testing and training from a normal database. Arch Phys
Med Rehabil.1999; 80(8):941–944.
22. Meyerhardt JA, Heseltine D, Niedzwiecki D, et al. Impact of physical activity on
cancer recurrence and survival in patients with stage III colon cancer: findings from
CALGB 89803. J Clin Oncol. 2006;24(22): 3535-3541.
23. Otto SJ, Korfage IJ, Polinder S, et al. Association of change in physical activity and
body weight with quality of life and mortality in colorectal cancer: a systematic
review and meta-analysis. Support Care Cancer. 2015;23(5):1237-50.
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
24. Park JH, Lee J, Oh M, et al. The effect of oncologists' exercise recommendations on
the level of exercise and quality of life in survivors of breast and colorectal cancer: A
randomized controlled trial. Cancer. 2015; e 25965782.
25. Rajarajeswaran P, Vishnupriya R. Exercise in cancer. Indian Journal of Medical and
Paediatric Oncology : Official Journal of Indian Society of Medical & Paediatric
Oncology. 2009;30(2):61–70.
26. Redelmeier DA, Bayoumi AM, Goldstein RS, Guyatt GH. Interpreting small
differences in functional status: the Six Minute Walk test in chronic lung disease
patients. Am J Respir Crit Care Med. 1997;155:1278–82.
27. Renfro LA, Grothey A, Kerr D, et al. Survival following early-stage colon cancer: an
ACCENT-based comparison of patients versus a matched international general
population†. Ann Oncol. 2015;26(5):950-8.
28. Roberts BM, Frye GS, Ahn B, Ferreira LF, Judge AR. Cancer cachexia decreases
specific force and accelerates fatigue in limb muscle. Biochem Biophys Res Commun.
2013;435(3):488-92.
29. Rogers K, Gibson AL. Eight-week traditional mat Pilates training-program effects on
adult fitness characteristics. Res Q Exerc Sport. 2009;80(3): 569-74.
30. Rydeard R, Leger A, Smith D. Pilates-based therapeutic exercise: effect on subjects
with nonspecific chronic low back pain and functional disability: a randomized
controlled trial. J Orthop Sports Phys Ther. 2006;36(7):472-84.
31. Sánchez-Jiménez A, Cantarero-Villanueva I, Delgado-García G, et al. Physical
impairments and quality of life of colorectal cancer survivors: a case-control study.
Eur J Cancer Care (Engl). 2014;e 25055886.
ACCEPTED
Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
32. Sánchez-Jiménez A, Cantarero-Villanueva I, Molina-Barea R, Fernández-Lao C,
Galiano-Castillo N, Arroyo-Morales M. Widespread pressure pain hypersensitivity
and ultrasound imaging evaluation of abdominal area after colon cancer treatment.
Pain Med. 2014;15(2):233-40.
33. Schmidt K, Vogt L, Thiel C, Jäger E, Banzer W. Validity of the six-minute walk test
in cancer patients. Int J Sports Med. 2013;34(7):631-6.
34. Schmitz KH, Courneya KS, Matthews C, et al. American College of Sports Medicine
roundtable on exercise guidelines for cancer survivors. Med Sci Sports Exerc.
2011;43(1):1409-26.
35. Sellar CM, Bell GJ, Haennel RG, Au HJ, Chua N, Courneya KS. Feasibility and
efficacy of a 12-week supervised exercise intervention for colorectal cancer survivors.
Appl Physiol Nutr Metab. 2014;39(6):715-23.
36. Smith D, Bissell G, Bruce-Low S, Wakefield C. The effect of lumbar extensión
training with and without pelvic stabilization on lumbar strength and low back pain. J
Back Musculoskelet Rehabil. 2011;24(4):241-9.
37. Sonnenschein EG, Kim MY, Pasternack BS, Toniolo PG. Sources of variability in
waist and hip measurements in middle-aged women. Am J Epidemiol.
1993;138(5):301-9.
38. Stan DL, Rausch SM, Sundt K, et al. Pilates for breast cancer survivors. Clin J Oncol
Nurs. 2012;16(2):131-41.
39. Thomas EL, Frost G, Harrington T, Bell JD. Validation of ‘InBody’Bioelectrical
Impedance by Whole Body MRI. Laboratory Report [Internet]. 2001. [cited 2015
May 14];1-2p. Available from:
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
http://www.fysiotest.se/swe/InBody_Studier_files/R%20Steiner%20validation_1.pdf.
40. Yuen HK, Sword D. Home-based exercise to alleviate fatigue and improve functional
capacity among breast cancer survivors. J Allied Health. 2007;36(4):e257-75.
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
FIGURE LEGENDS
Figure 1. Study flow diagram
ACCEPTED
Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
Figure 1
ACCEPTED
Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
Table 1: Physical exercise program CO-CUIDATE.
Exercise
description
Volume and Intensity progression
Week
1
Week
2
Week
3
Week
4
Week
5
Week
6
Week
7
Week
8
Aerobic
exercise
Brisk
walking or
running
5+5
min
10+5
min
15
min
10+10
min
20
min
20+5min 20+5
min
10+10
min
Stabilization
Exercise
Program
Pilates
exercise
1 set
of 8-
10
reps
1 set
of 12
reps
2sets
of 8
reps
2 sets
of 10
reps
1 set
of 12
reps
2 sets of
12 reps
3 sets
of 8
reps
2 sets
of 10
reps
Local Segmental Control Exercise
Roll Up- Roll Down
One Leg Circle
Side Kicks
Saw
Hundred
Leg Pull Front
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
Stretching
exercise
Specific and general exercises. The progression was performed for the feelings
(not pain) and autonomy
Notes All therapeuticexercises were focused to breathing and specific muscles
activation (mind-body exercise) and were made with instructor assist.
Intensity of exercises was quantified on the Borg Rating of Perceived Exertion
(RPE) scale
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
Table 2: Demographic, clinical and medical characteristics of the groups.
Characteristic CUIDATE group
(n= 21)
Control group
(n= 19)
P-value
Age (year), mean (SD)* 57.5±8.0 62.3±7.9 0.066a
Gender n (%)
Male
Female
13 (61.9)
6 (38.1)
13 (68.4)
8 (31.6)
0.294 c
Time since diagnosis (month)
mean(SD)*
13.8±7.8 17.1±11.3 0.293 a
Time since intervention
(month) mean(SD)*
12.0 ±7.4 14.6±10.0 0.436 a
Marital status, n (%)
Married
Unmarried
Divorced
19 (90.5)
1 (4.8)
1 (4.8)
15 (78.9)
2 (10.5)
2 (10.5)
0.294 b
Tumor stage, n (%)
II
IIIa
7 (33.3)
14 (66.7)
7 (36.8)
12 (63.2)
0.539 b
Educational level, n (%)
Primary schooling
Secondary schooling
University
9 (42.9)
6 (28.6)
6 (28.6)
14 (73.7)
3 (15.8)
2 (10.5)
0.200 b
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
Type of surgery, n (%)
Right hemicolectomies
Left hemicolectomies
Sigmoid colectomies
Anterior resections
6 (28.6)
3 (14.3)
5 (23.8)
7 (33.3)
6 (31.6)
0
8 (42.1)
5 (26.3)
0.269 b
Tobacco
No
Yes
Ex-smoker
7(33.3)
2 (9.5)
12 (57.1)
13 (68.4)
2 (10.5)
4 (21.1)
0.057 b
Alcohol Intake
Never
Monthly
Weekly
Dialy
7 (33.3)
5(23.8)
7 (33.3)
2 (9.5)
8 (42.1)
4 (21.1)
2 (10.5)
5 (26.3)
0.169 b
Physical activity (METS/h-d)
mean(SD)*
4.2±2.1 4.1±2.6 0.940 a
*values mean ± SD are expressed as mean (95% confidence interval) or as number and
percentage. P values for inter-group comparisons using t-student (a) and chi-square (
b) test.
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
Table 3: Comparison of variables data between groups at baseline
*P < 0.05 **P < 0.001 for ANOVA analysis between groups.
CO-CUIDATE program
group
(n= 21)
Control
group
(n=19)
P value
Health-related fitness
Trunk curl test (sec) 25.3 ± 10.5 24.3 ± 11.6 0.71
Back dynamometer (kg) 62.2 ± 36.5 54.8 ± 25.1 0.21
6-min walk test (m) 330.8 ± 137.2 288.8 ± 132.3 0.83
Modified Sit and Reach test
(right, cm)
-9.2 ± 10.9 -10.4 ± 12.1
0.61
Modified Sit and Reach test
(left, cm)
-10.0 ± 11.0 -6.3± 13.4
0.30
Anthropometric outcomes
Waist Circumference (cm) 102.5 ± 13.6 101.1 ± 11.2 0.60
Hip Circumference (cm) 108.3 ± 02.4 108.6 ± 02,5 0.72
Weight (kg) 74.7 ± 10.8 76.4 ± 14.2 0.30
Body Fat (%) 34.9 ± 10.5 32.6 ± 9.2 0.55
Muscle Mass (kg) 26.9 ± 5.8 26.9 ± 5.2 0.51
Body Mass Index 28.4 ± 5.0 28.2 ± 5.0 0.97 ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
Table 4: Pre-intervention, post-intervention, 6 months follow-up and change scores for mean
values ± standard deviation of health-related fitness.
CO-CUIDATE
program group
(n=21)
Control group
(n=19)
Between-Group
Differences
Trunk curl test (sec)
Pre-intervention 25.3 ± 10.5 24.3 ± 11.6
-26.0 (-39.2;-12.7)**
-7.2 (-7.2-21.8)
Post-intervention 54.0 ± 26.3 27.0 ± 12.6
6 months follow-up 42.0 ± 26.6 33.8 ± 23.9
Within Group Change
Scores
Pre-post intervention
Pre intervention- 6
months follow up
28.6 (17.4-39.9)
16.6 (4.2-29.6)
2.6 (-9.1-14.5)
9.4 (-3.6-22.4)
Back dynamometer (kg)
Pre-intervention 62.2 ± 36.5 54.8 ± 25.1
-4.6 (-16.2;-6.8)
Post-intervention 70.5 ± 30.8 58.5 ± 24.0
6 months follow-up 71.3 ± 37.3 53.3 ± 23.2
Within Group
Change Scores
8.2 (-1.5-18.1)
3.6 (-6.7-13.9)
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
Pre-post intervention
Pre intervention- 6
months follow up
9.1 (0.2-17.9)
-1.5 (-10.8-7.8)
-10.6 (-21.0-0,2)
6-min walk test (m)
Pre-intervention 330.8 ± 137.2 288.8 ± 132.3
-74.8 (-131.8;-17.3) *
-82.9 (-143.2;-22.6) *
Post-intervention 410.5 ± 130.8 293.7 ± 125.7
6 months follow-up 393.3 ± 148.4 279.8 ± 119.8
Within Group
Change Scores
Pre-post intervention
Pre intervention- 6
months follow up
79.7 (31.6-128.4)
62.4 (16.9-108.0)
4.9 (-46.2-56.0)
-8.9 (-56.8- - 38.9)
Modified Sit and Reach test (right, cm)
Pre-intervention -9.2 ± 10.7 -10.4 ± 12.1
-5.4 (-9.5;-1.4)*¥
-2.1 (-74.6-0.2)
Post-intervention -5.0 ± 10.9 -11.7 ± 11.8
6 months follow-up -7.7 ± 10.3 -11.1 ± 12.8
Within Group Change
Scores
Pre-post intervention
4.2 (0.7-7.6)
-1.2 (-4.8-2.3)
-0.7 (-2.8-1.4)
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
Values are expressed as mean ± standard deviation for pre, post-intervention and 6 months
follow up data and as mean (95% confidence interval) for within- and between-group change
scores. * Significant group × time interaction (repeated ANCOVA test, P < 0.05). . **
Significant group × time interaction (repeated ANCOVA test, P < 0.001). . ¥ influenced by aged.
Pre intervention- 6
months follow up
1.4 (-0.6-3.5)
Modified Sit and Reach test (left, cm)
Pre-intervention -10.0 ± 11.0 -6.3± 13.4
-7.5 (-13.1;-2.0)*¥
-4.4 (-9.3;0.4)
Post-intervention -6.1 ± 11.2 -9.9 ± 10.0
6 months follow-up -8.8± 10.4 -9.5 ± 13.8
Within Group Change
Scores
Pre-post intervention
Pre intervention- 6
months follow up
3.9 (-0.8-8.6)
1.2 (-2.9-5.4)
-3.6 (-8.6-1.1)
-3.2 (-7.6-1.1)
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
CO-CUIDATE
program group
(n=21)
Control group
(n=19)
Between-Group
Differences
Waist Circumference (cm)
Pre-intervention 102.5 ± 13.6 101.1 ± 11.2
5.1 (1.6:8.7) *
2.4 (0.1:4.6) *
Post-intervention 98.9 ± 12.7 102.7 ± 10.8
6 months follow-up 103.0 ± 12.5 104.0 ± 11.1
Within Group
Change Scores
Pre-post intervention
Pre intervention- 6
months follow up
-3.6 (-6.6:-0.5)
0.4 (-1.4:2.3)
1.5 (-1.6:-4.7)
2.9 (0.9:4.9)
Hip Circumference (cm)
Pre-intervention 108.3 ± 12.4 108.6 ± 9.3
2.4 (-0.4:04.5)
-0.5 (-2.4:1.4)
Post-intervention 106.5 ± 11.6 109.3 ± 10.1
6 months follow-up 109.2 ± 13.4 108.9 ± 9.1
Within Group
Change Scores
Pre-post intervention
Pre intervention- 6
-1.7. (-3.4; 00.0)
0.8 (-081:2.54)
0.7 (-0.0:3.4)
0.3 (-1.4:2.0)
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
months follow up
Weight (kg)
Pre-intervention 76.4 ± 14.2 74.7 ± 10.8
-0.2 (-3.1:2.6)
1.2 (-4.7:2.1)
Post-intervention 77.6 ± 13.3 75.7 ± 11.1
6 months follow-up 79.3 ± 13.2 76.4 ± 11.3
Within Group Change
Scores
Pre-post intervention
Pre intervention- 6
months follow up
1.2 (-1.2:3.7)
2.9 (0.0:5.8)
0.9 (-1.1:3.0)
1.6 (-1.3:4.7)
Body Fat (%)
Pre-intervention 34.9 ± 10.5 32.6± 9.2
1.5 (-0.1:3.3)
1.7 (-1.1:4.5)
Post-intervention 33.9 ± 10.5 33.3 ± 9.0
6 months follow-up 35.7 ± 9.9 35.2 ± 8.6
Within Group Change
Scores
Pre-post intervention
Pre intervention- 6
months follow up
-0.9 (-2.4:0.5)
0.8 (-1.5:3.2)
0.6 (-0.9:2.1)
2.5 (-0.0:5.1)
ACCEPTED
Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
Muscle Mass (kg)
Pre-intervention 26.9 ± 5.8 26.9 ± 5.2
-0.8 (-2.1:0.3)
-0.8 (-2.1:0.4)
Post-intervention 27.9 ± 5.6 27.0 ± 5.6
6 months follow-up 27.8± 5.6 26.9± 5.2
Within Group Change
Scores
Pre-post intervention
Pre intervention- 6
months follow up
1.0 (-0.0:2.1)
0.9 (-0.1:2.0)
0.1 (-0.9:1.2)
0.0 (-1.6:1.2)
Body Mass Index
Pre-intervention 28.4 ± 5.0 28.2 ± 5.0
0.7 (0.6:0.8)
-0.3 (-1.3:0.6)
Post-intervention 28.7 ± 5.0 28.6 ± 4.9
6 months follow-up 29.3 ± 4.6 28.8 ± 4.8
Within Group Change
Scores
Pre-post intervention
Pre intervention- 6
months follow up
0.3 (-0.3:0.9)
0.9 (0.0.1.7)
0.3 (-0.2:1.0)
0.5 (-0.3:1.4)
ACCEPTED

Copyright © 2016 by the American College of Sports Medicine. Unauthorized reproduction of this article is prohibited.
Table 5: Pre-intervention, post-intervention, 6 months follow-up and change scores for mean
values ± standard deviation of anthropometric measurement.
Values are expressed as mean ± standard deviation for pre, post-intervention and 6 months
follow up data and as mean (95% confidence interval) for within- and between-group change
scores. * Significant group × time interaction (repeated ANCOVA test, P < 0.05). ** Significant
group × time interaction (repeated ANCOVA test, P < 0.001). ¥ influenced by aged.
ACCEPTED