plasmaskin rejuvenation ofthehands · pdf filecha~ter 47;:~ plasmaskin rejuvenation ofthehands...
TRANSCRIPT
CHA~TER 47;:~
Plasma Skin Rejuvenation of the HandsTina S. Alster
Photodamaged skin of the hands occurs as a result ofchronic exposure to ultraviolet light and is characterizedby roughened surface texture, dyspigmentation, telangi-ectasias, rhytids, and skin laxity. Although several differ-ent noninvasive procedures have been advocated for handrejuvenation (Table 47.1), many are characterized by anunattainable balance between effectiveness and morbidity.The necessity of epidermal removal during most skin resur-facing treatments leads to significant morbidity during thereepithelialization process, particularly in areas such as thehands, where limited pilosebaceous glands are present.
PLASMA SKIN REGENERATION TECHNOLOGY
Plasma skin regeneration is a novel process that involves thegeneration of plasma through the use of ionized energy thatthermally heats tissue. A pulse of ultrahigh-energy radio-frequency (RF) from the device generator (Portrait plasmaskin regeneration) converts nitrogen gas into plasma withinthe handpiece. The plasma emerges from the distal end ofthe device handpiece and is directed onto the skin area tobe treated. Rapid heating of the skin occurs as the excitedgas transfers heat to the skin, resulting in increased fibro-blast activity during dermal regeneration. The retainednecrotic epidermis effectively serves as a biological dressingfor the efficient formation of a new stratum corneum andepidermis.The essentially instantaneous generation of plasma with
controlled application of RF energy produces individualplasma pulses that heat tissue. Adjustment of RF powerand pulse width enables control of tissue effects by alter-ing the amount of energy delivered to tissue per pulse. Inpractice, the energy per pulse is adjustable between 1 and4]. The power and duration of each RF pulse are directlyproportional to plasma strength.
CLINICAL PROTOCOL
The skin areas to be treated are cleansed with mild soapand water to remove all surface debris. While intralesional
lidocaine can be used for anesthesia, application of a topi-cal anesthetic cream (e.g., EMLA or LMX-S) under plasticwrap occlusion for sixty minutes is often adequate. Oncethe cream has been thoroughly removed and the skin com-pletely dried, the treatment should commence within five toten minutes. Typical energy settings of 1.S-4 ] are appliedto the areas, holding the device handpiece perpendi-cular to the skin at a distance measuring approximatelyS mm from the skin surface. The areas are treated in asingle pass with a pulse overlap of 10 to 20%. An additionalpass should only be delivered if a low (I.S J) energy set-ting is used. Pulse repetition rates of 1-4 Hz are chosen,subject to the discretion of the operator. While skin can becooled with ice packs or cool water compresses posttreat-ment, intraoperative cooling of the skin is contraindicatedbecause of its negative impact on the tissue heating neces-sary to achieve optimal clinical effect.
POSTOPERATIVE COURSE
Immediately posttreatment, a petrolatum-based ointment(e.g., Aquaphor) can be applied to the skin. Patients shouldbe instructed to gently cleanse the treated areas with mildcleanser and water and to reapply the ointment at least threetimes daily to maintain a moist healing environment. Non-stick gauze dressings can be used to protect the treatedareas from ultraviolet light exposure or abrasion due toclothing. Patients should be advised to avoid sun expo-sure, prolonged water immersion, or exposure to harshchemicals for as long as the treated skin appears pink incolor.
CLINICAL RESUL T5
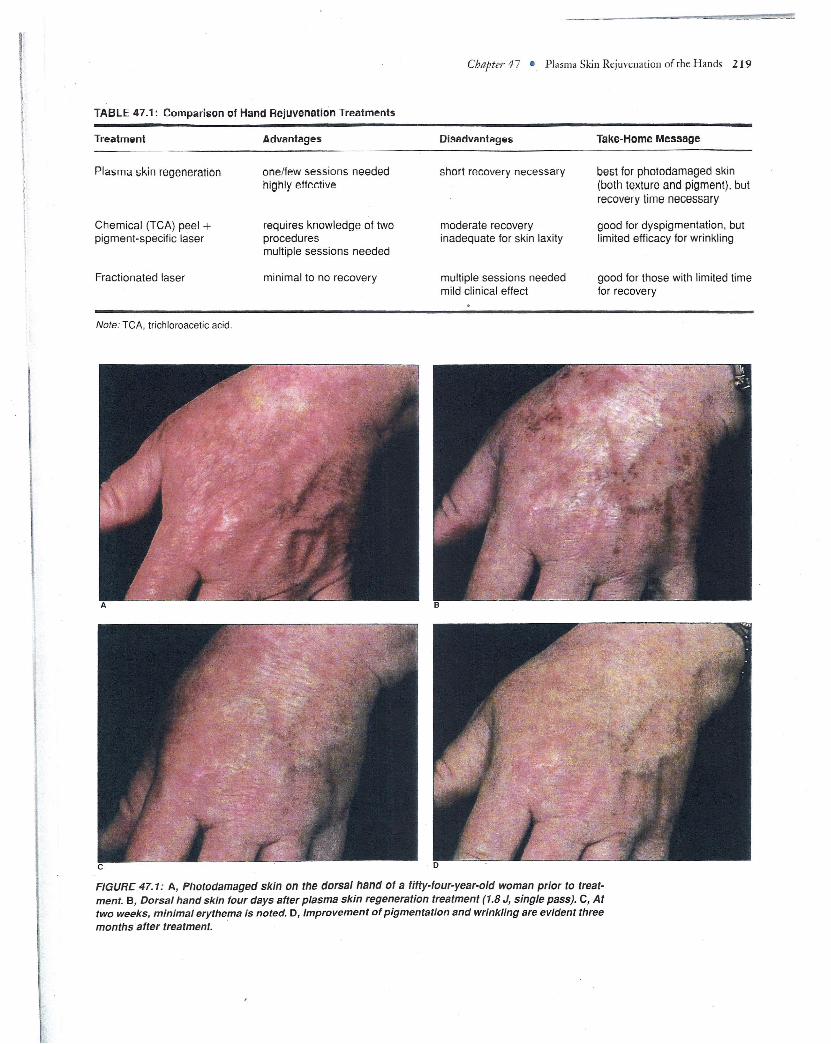
Clinical improvement of SO% is typically observed, withsignificant reduction in wrinkle severity and hyperpig-mentation within one month after a single treatment(Figure 47.1). Most patients also experience increased skinsmoothness. Additional treatments can be delivered for
page 218
\
\
TABLE 47.1: Comparison of Hand Rejuvenation Treatments
Chapter 47 • PlasmaSkin Rejuvenation of the Hands 219
Treatment Advantages Disadvantaqes Take-Home Message
Plasma skin regeneration one/few sessions neededhighly effective
Chemical (TeA) peel +pigment-specific laser
requires knowledge of twoproceduresmultiple sessions needed
Fractionated laser minimal to no recovery
short recovery necessary best for photodamaged skin(both texture and pigment), butrecovery lime necessary
moderate recoveryinadequate for skin laxity
good for dyspigmentation, butlimited efficacy for wrinkling
multiple sessions neededmild clinical effect
good for those with limited timefor recovery
Note: TeA, trichloroacetic acid.
FIGURE 47.1: A, Photodamaged skin on the dorsal hand of a fiHy-four-year-old woman prior to treat-ment. B, Dorsal hand skin four days after plasma skin regeneration treatment (1.8 J, single pass). C, Attwo weeks, minimal erythema is noted. D, Improvement of pigmentation and wrinkling are evident threemonths after treatment. .

220 OFFICE-BASED COSMETIC PROCEDURES AND TECHNIQUES
further enhancement and maintenance of clinical effect butshould be delayed at least one month to assess the resultsof prior treatment and to give the skin ample time to heal.
SIDE EFFECTS
The use of higher energy settings or multiple passes yieldsgreater clinical benefit, but also prolonged tissue healing(fourteen days versus seven days). Side effects of erythema,edema, and desquamation are uniformly experienced. Epi-dermal sloughing with clinical evidence of a superficial der-mal wound is evident within forty-eight hours of treat-ment. Reepithelialization with normalization of externalskin architecrure occurs within a few days. Mild erythema istypical for two to four weeks. While infection, dyspigmen-tation, and scarring are potential risks of the procedure,the incidence is extraordinarily low when the intraoper-ative and postoperative protocols outlined previously arefollowed. No prophylactic antibiotics are recommended;
however, if a postoperative infection is suspected, broad-spectrum antibiotics can be prescribed.
SUMMARY
Plasma skin regeneration is a highly effective rejuvenativeskin treatment. Its excellent clinical efficacy and safety pro-file in cutaneous sites that have notoriously been difficultto treat with ablative laser technology make it my preferredtreatment for photodamaged skin of the hands.
SUGGESTED READING
Alster TS, Konda S. Plasma skin resurfacing for regeneration ofneck, chest, and hands: investigation of a novel device. Derma-tol. SU1"g. 2007;33:1-5.
Bogle MA, Arndt KA, Dover )S. Evaluation of plasma skin regen-eration technology in low-energy full-facial rejuvenation.Arch. Dermatol. 2007;143:168-74.