overview of hiv/aids in ethiopia unit 1 hiv care and art: a course for healthcare providers
TRANSCRIPT

Overview of HIV/AIDS in Ethiopia
Unit 1HIV Care and ART: A Course for
Healthcare Providers

2
Learning Objectives
Describe the national HIV/AIDS epidemiological profile
Describe the Ethiopian national AIDS strategies, guideline for implementation of ART, and roadmap to accelerate care and treatment for PLWHA
List the major achievements, challenges and opportunities during the implementation of the ART program in Ethiopia

3
Learning Objectives (2)
Explain the Ethiopian National Policy on ARV drugs, supply and use
Convey the current status of the ART program in Ethiopia
List prevention strategies to reduce the spread of HIV infection in the country

Global and Ethiopian Summary of HIV/AIDS Epidemic

5
Global Summary of the AIDS Epidemic, December 2005
PLWHA 40.3 million (36.7 – 45.3) Adults 38.0 Million
(34.5-42.6) Women 17.5 Million
(16.2-19.3) Children <15 yrs 2.3
Million (2.1-2.8)
New infections 4.9 million (4.3–6.6) Adults 4.2 Million (3.6-5.8) Children <15 yrs 700,000 (630,000 – 820,000)
AIDS Deaths 3.1 million (2.8 – 3.6) Adults 2.6 Million (2.3 – 2.9 million) Children <15 yrs (570,000-670,000)

6
Global Picture of HIV/AIDS
Source: UNAIDS, 2006

7
Est. Number Newly Infected With HIV During 2005: 4.9 Million
North America44,00044,000
Caribbean53,00053,000
Latin America240,000240,000
Western Europe21,00021,000
North Africa& Middle
East92,00092,000
Sub-Saharan Africa
3.1 million3.1 million
Eastern Europe
& Central Asia210,000210,000 East Asia &
Pacific290,000290,000
South & South-
East Asia
890,000890,000Australia
& New Zealand5,0005,000
Source: UNAIDS/WHO

8
Est. Adult and Child Deaths From HIV/AIDS During 2005: 3.1 Million
North America16,00016,000
Caribbean36,00036,000
Latin America95,00095,000
Western Europe65,00065,000
North Africa& Middle
East28,00028,000
Sub-Saharan Africa
2.3 million2.3 million
Eastern Europe
& Central Asia60,00060,000 East Asia
& Pacific51,00051,000South
& South-East Asia490,000490,000
Australia & New Zealand
700700
Source: UNAIDS/WHO

9Source: UNAIDS/WHO 2004

10
Ethiopian Prevalence
National prevalence for 2003 ......... 4.4% National Prevalence for 2005 ........... 4.7%
Women….5.0% Men….3.8%
Urban prevalence in 2003...................12.6% Urban prevalence in 2005...................12.5%
Rural prevalence in 2003 .................. .2.6% Rural prevalence in 2005................... .3.0%
Addis Ababa prevalence in 2003 ........14.6% Addis Ababa prevalence in 2005 ........14.5%

11
HIV/AIDS Indicators in Ethiopia (2005)
Number of PLWHA 1.7 million Estimated AIDS cases 143,129 PLWHA requiring ARVs 286,258 Annual AIDS deaths 134,124 Adults and Children on ART 20,477

12
HIV/AIDS Indicators in Ethiopia (2005) (2)
AIDS orphans 678,936 Total orphans
4,801,219 Children living with HIV/AIDS 111,903
New HIV infections………39,886New AIDS cases…………29,359
Annual AIDS deaths in children 28,693 Children newly needing ART 58,718 Children on ART 654

13
Age & Sex Distribution of Reported AIDS Cases (1986 - June 2003, Ethiopia)
Source: AIDS in Ethiopia, 5th ed., MOH, July, 2004

14
Pregnant Women Testing HIV Positive: Urban, 2001
Source: Aids in Ethiopia, 4th ed., MOH, October 2002

15
Pregnant Women Testing HIV Positive: Rural, 2001
Source: Aids in Ethiopia, 4th ed., MOH, October 2002
16
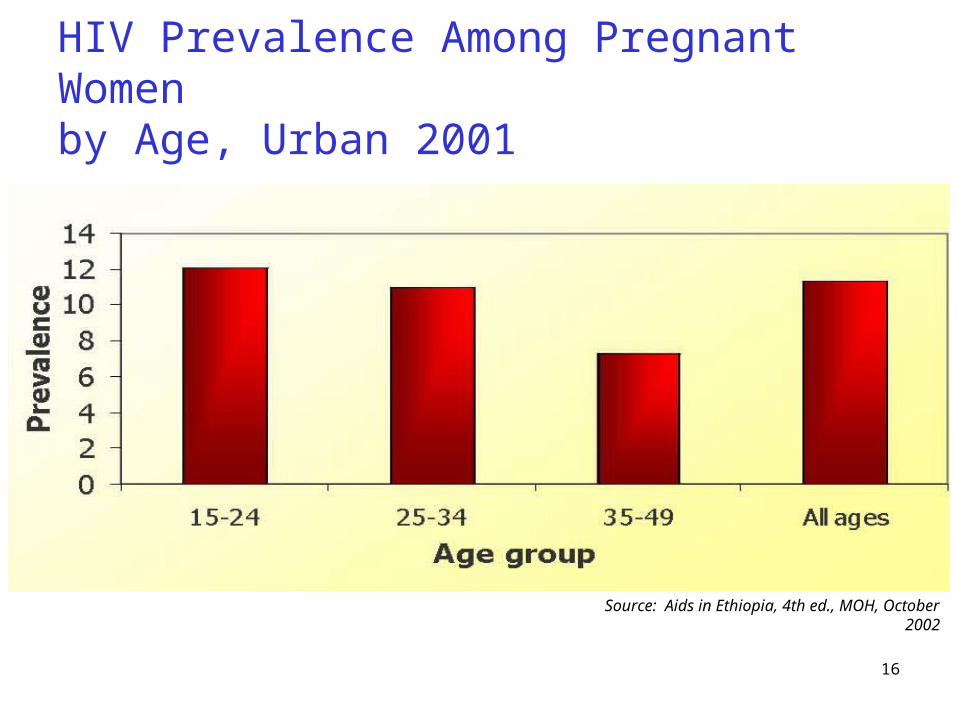
HIV Prevalence Among Pregnant Women by Age, Urban 2001
Source: Aids in Ethiopia, 4th ed., MOH, October 2002

17
Impact on Rural Households
Loss of income (50% or more)Loss of laborLoss of skilled manpower and knowledgeLoss of landLoss of remittances
Reduction in savings and investmentExpenses for treatment, funeral, teskarNeed to sell livestock to meet expenses

18
Impact on Industry
Loss of workersExpenses for recruiting and training replacementsReduced productivity in cases of skilled workers or
managers
Lost work days due to sickness and funeral leave
Increased health care costs50% illness due to AIDSLoss of skilled professionals

HIV/AIDS Treatment in Ethiopia

20
Historical Overview of HIV/AIDS in Ethiopia
1984: The first evidence of HIV infection in Ethiopia
1986: The first two AIDS cases reported to the Ministry of Health
1989: HIV/AIDS surveillance started March, 2005: Free ART program started Currently, approximately:
129 surveillance sites73 ART sites658 VCT sites

21
VCT Site Distribution by Region, 2005

22
ART Site Distribution by Region
Total =73

23
Regional Distribution of ART
Tigray9%
Amhara19%
Addis Ababa48%
Others6%
SNNPR6%
Oromia12%

24
PMTCT Site Distribution, by Region
Total site = 129

25
National Response
HIV/AIDS Policy formulated by MOH and adopted by the Council of Ministers in 1998Enabled HIV/AIDS prevention and controlSupplemented existing health, women’s, and
education and training policyCalled for a multisectoral responseGuaranteed rights of PLWHA
ARV Drugs Supply & Use Policy formulated July 2002

26
National Response (2)
HIV/AIDS Prevention & Control Office (HAPCO) established June 2002Restructured from NACS (April 2000)Sits under Prime Minister’s OfficeEstablished at all levels of government
Runs the daily activities of NACResource mobilizationAdvocacyCoordination of the sectoral responses
27
National Response (3)
HIV/AIDS Strategic plan for five years2004 - 2008
Social mobilization & community involvementCommunity ownership
Scaled up ART programAIDS fund was initiatedFree ART program was scaled up

28
HIV/AIDS Intervention Strategies
PreventionSocial mobilization
• IEC/BCCHIV counseling and testing
• Voluntary (VCT)• Provider initiated (PIHCT)
STI prevention and controlCondom promotionInfection preventionPrevention of mother to child transmission (PMTCT)Post exposure prophylaxis

29
HIV/AIDS Intervention Strategies (2)
Care and TreatmentPalliative care Community home based careOpportunistic infection treatmentTuberculosis treatmentTreatment of AIDS patients
Support forOrphans and vulnerable children (OVC)People living with HIV/AIDS (PLWHA)

30
Major Achievements
National HIV/AIDS Policy National AIDS Council Secretariat Five editions of “AIDS in Ethiopia” National ARV Policy (revised and published in
January 2005) Roadmap to accelerate access to HIV/AIDS care
and treatment M&E framework

31
Major Achievements (2)
Five-year strategic plan revised & updatedUsed as main input for the National Strategic
Framework adopted by NACContains strategic outline of interventions at federal
and regional levels
Key guidelines developed:HIV Surveillance GuidelineHIV Surveillance Training ManualVoluntary Counseling & Testing Guideline

32
Major Achievements (3)
Key guidelines (continued):AIDS Case Management GuidelineSTI Management GuidelineHome-Based Care Guideline Private HIV Labs Licensing GuidelinePMTCT GuidelineHome Care Training ManualCounseling Training ManualARV GuidelineUniversal Precautions & Post Exposure Prophylaxis

33
Major Achievements (4)
658 VCT sites established 129 sentinel surveillance sites established MOH has been the primary advocate for a multi-
sectoral response to HIV/AIDS:Formulated and disseminated HIV/AIDS and ARV
Drugs Supply & Use PoliciesActs as a catalyst for several multi-sectoral HIV/AIDS
committees that pre-dated the NAC

34
Major Achievements (5)
Integrating HIV/AIDS into health programs:Reproductive healthMother and child healthHospital hygieneHealth educationIntegrated disease surveillanceTB/HIV Initiative

35
Limitations
Synchronizing pharmacy & patients reports Absence of laboratory reports Inadequate Pre and ART registers Employing ART coordinators and Data
managers Sending reports to RHBs and MOH AIDS patients on waiting lists

Policy of ARV Supply and Use in Ethiopia

37
Introduction
Care and support of PLWHA plays an important role in preventing the spread of HIV/AIDS
ART is an important component of care for PLWHA
ARVs also have an important place in PMTCT and PEP
ARVs have enormous benefits, but affordability, toxicity, adherence and resistance are challenging

38
National ARV Policy
Policy approved in July 2002 Objectives of the policy:
Reduce MTCTProlong and improve the quality of lives of PLWHAReduce accidental HIV infection within health
institutions

39
General Policy
Determines type of ARVs that will be used in health care services
The Government of Ethiopia:Coordinates & facilitates the supply of ARVsBuilds capacity for making available safe, effective
and quality antiretroviral drugs, and for ensuring proper use of these drugs
Ensures sustainable supply of ARVs by encouraging involvement of all stakeholders
40
General Policy (2)
The Government of Ethiopia (cont):Nurtures international partnerships to strengthen
sustainable supply and use of ARVsEncourages research on modern and traditional
HIV/AIDS treatmentEstablishes strong systems to monitor ARV supply
and use

41
General Strategies
1. Selection of ARVs Determine the type of ARVs to be used in Ethiopia Incorporate selected ARVs into the national drug list Permit the import of ARVs that are not included in
the national drug list

42
General Strategies (2)
2. Supply of ARVs ARVs for ART:
• Exempted from taxation• Supplied at reduced prices through government
negotiation with manufacturers, importers and distributors
• Purchased by a system of bulk and generic substitution
Local production of ARVs encouraged Benefaction of ARVs facilitated by the Ethiopian
Government Ethiopian Government supplies ARVs for PMTCT

43
General Strategies (3)
3. Drug Use Prepare and implement standardized prescription
paper Prepare and implement national guidelines for safe
and effective use of ARVs Sustainable public education on ARV drugs

44
General Strategies (4)
4. Research and Development Government of Ethiopia encourages research on
modern and traditional HIV/AIDS treatment Government of Ethiopia shall make efforts to
strengthen the capacity of research institutions Rights and benefits of citizens that enroll in research
studies shall be respected National and international ethical norms and values
in human experimentations shall be observed

45
Scaling up ART Uptake
Need capacity development to:Initiate treatmentHelp patients adhere to their treatment regimensMonitor the efficacy and toxicity of the regimens Diagnose treatment failureMonitor overall resistance in society
ART program must be implemented at Health Center level
Nursing initiative to prescribe ARVs is being piloted
46
Key Points
AIDS is a global, regional, and national crisis The national HIV seroprevalence rate in Ethiopia
is 4.7% Urban rate is 12.5% Rate in Addis Ababa is 14.5%
Approximately 20,500 people in Ethiopia are currently receiving ART

47
Key Points (2)
ARV guidelines have been written, policies have been adopted, and training is being conducted in Ethiopia
ARVs have enormous benefits and challenges. The challenges include:Developing capacity to initiate treatmentSupporting adherenceMonitoring efficacy and toxicityDiagnosing treatment failureMonitoring resistance